- Published on
IEmergency And Acute Medicine – Duodenal Trauma
Basics Description
The duodenum is a 12-inch long, C-shaped structure extending from the pylorus to the ligament of Treitz and is divided into four sections. The distal portion of the first section and the remaining three sections are retroperitoneal. It lies mostly over the first three lumbar vertebrae, with the second portion being the most commonly injured. Types of injury include duodenal wall hematoma, wall perforation, hemorrhage including retroperitoneal bleeding, and crush injury. Duodenal trauma accounts for 3–5% of all traumatic abdominal injuries. Penetrating trauma causes approximately 75% of cases, with mortality ranging from 13–28%, often due to exsanguination. Blunt trauma carries higher mortality because of greater injury force and delayed diagnosis related to the retroperitoneal location. If diagnosed within 24 hours, mortality is approximately 11%; if delayed beyond 24 hours, mortality approaches 40%, with late deaths commonly due to sepsis.
Pediatric Considerations
Most pediatric duodenal injuries result from recreational trauma such as bicycle handlebar injuries. Intramural duodenal hematomas may be associated with nonaccidental trauma; suspected cases require immediate referral to child protective services. In children, hematomas most commonly involve the first portion of the duodenum.
Pregnancy Considerations
Retroperitoneal hemorrhage is more common due to increased abdominal and pelvic vascularity. The enlarged uterus may provide partial protection from bowel injury, and peritoneal irritation may be blunted, necessitating a higher index of suspicion.
Etiology
Blunt trauma mechanisms include shear strain from rapid acceleration–deceleration at points of fixation and tensile strain from direct compression or stretching. Penetrating trauma is the most common cause overall and may create cavitation with subsequent infection.
Diagnosis Signs And Symptoms
Symptoms may be minimal and nonspecific, including vague abdominal, flank, or back pain. High gastrointestinal obstruction may occur with duodenal hematomas.
History
Penetrating or blunt abdominal trauma.
Physical-Exam
Retroperitoneal injury may present subtly with right upper quadrant pain, nausea, vomiting, tachycardia, and fever. Intraperitoneal involvement presents with signs of peritonitis.
Essential Workup
Obtain basic laboratory studies including amylase. Perform an acute abdominal series or CT imaging. Diagnostic peritoneal lavage or exploratory laparotomy is indicated in unstable patients with high clinical suspicion.
Diagnosis Tests And Interpretation
Laboratory studies are generally nonspecific; approximately 50% of patients have elevated serum amylase, and rising leukocytosis may suggest missed injury. FAST examination is validated for hemoperitoneum but is unreliable for duodenal injury, with one-third of retroperitoneal injuries having a normal FAST. Upright chest and abdominal radiographs may show intraperitoneal or retroperitoneal air, air in the biliary tree, rightward scoliosis, loss of psoas shadow, or air around the right kidney. Air insufflation via nasogastric tube may enhance detection of retroperitoneal air. Intramural hematomas may show a coiled-spring appearance. CT with oral and IV contrast is the preferred diagnostic modality, identifying retroperitoneal gas, contrast extravasation, duodenal wall thickening, periduodenal fluid, sentinel clot, or sausage-shaped intramural masses. Exploratory laparotomy remains the definitive diagnostic test when suspicion persists despite negative studies. Diagnostic peritoneal lavage may reveal blood, bile, or bowel contents but has a false-negative rate of up to 65%.
Differential Diagnosis
Hollow viscus injuries involving stomach or intestines, liver and biliary injuries, vascular injuries including aortic or mesenteric vessels, and postoperative complications such as infection or suture dehiscence.
Treatment Pre Hospital
Follow standard trauma protocols. Clear documentation of mechanism of injury and transport to an appropriate trauma center are essential.
Initial Stabilization And Therapy
Secure the airway and initiate resuscitation as needed. Provide aggressive fluid resuscitation with warmed crystalloids and transfuse blood products when indicated. Place central venous access in unstable patients. Initiate nasogastric decompression and obtain early trauma surgery consultation.
Emergency Department Treatment And Procedures
Administer tetanus prophylaxis and broad-spectrum antibiotics for penetrating injuries. Definitive management typically requires laparotomy with duodenal exploration. Low-grade blunt injuries (grade I or II) are often managed nonoperatively, though up to 10% may fail conservative therapy. Antibiotics are essential in cases of perforation to prevent sepsis.
Medication
Cefoxitin 2 g IV every 6 hours (pediatric dose 40 mg/kg) or levofloxacin 750 mg IV or ciprofloxacin 400 mg IV daily combined with metronidazole 500 mg IV every 8 hours.
Follow-Up And Disposition
All patients with duodenal injury require admission to a trauma surgical service. Minor hematomas may require nasogastric decompression for obstruction for up to seven days with close observation for expansion or rupture. No patient with confirmed duodenal trauma should be discharged from the emergency department. Complications include intra-abdominal abscess, duodenal fistula, pancreatic fistula, and sepsis.
Issues For Referral
Duodenal injuries are graded using the American Association for the Surgery of Trauma Duodenal Injury Scale, with most injuries being grade II or III. Approximately 80% are managed with primary repair.
Follow-Up Recommendations
All confirmed injuries require inpatient management. If diagnostic studies are negative, arrange follow-up with a primary care physician within 24–48 hours. Begin with clear liquids and advance diet as tolerated.
Pearls And Pitfalls
Delayed or missed diagnosis significantly increases morbidity and mortality. Physical examination may be misleading due to the retroperitoneal location of the duodenum. Persistent clinical suspicion warrants immediate surgical consultation even with negative diagnostic tests.

- Published on
Emergency And Acute Medicine – Drowning
Basics Description
Drowning is a process resulting in primary respiratory impairment from submersion or immersion in a liquid medium. Fatal drowning refers to death at any time as a result of the drowning process, while nonfatal drowning occurs when the victim survives after interruption of submersion. Water rescue describes submersion or immersion without respiratory impairment. All drowning victims aspirate some amount of liquid; previously used terms such as “wet” and “dry” drowning are obsolete. The final common pathway is hypoxia, with no clinically significant difference between freshwater and saltwater drowning.
Pathophysiology
Aspiration of small volumes of water decreases lung compliance, causing ventilation–perfusion mismatch and intrapulmonary shunting, usually without major electrolyte disturbances. Grossly contaminated water increases the risk of pulmonary infection. Hypoxemia leads to lactic acidosis, multisystem organ dysfunction, noncardiogenic pulmonary edema, myocardial dysrhythmias, coagulation abnormalities including disseminated intravascular coagulation, acute renal failure, and cerebral hypoxia resulting in cerebral edema and increased intracranial pressure.
Pediatric Considerations
Hypothermia is more common in children due to a higher body surface area–to–mass ratio and may be neuroprotective by lowering metabolic rate. The diving reflex, particularly in young children exposed to cold water, causes bradycardia and preferential blood flow to the heart and brain, delaying hypoxic injury.
Alert
Risk factors include inadequate supervision, alcohol or drug use, limited swimming ability, trauma, seizure disorder, risky behavior, pre-existing medical conditions, suicide attempt, and poor water safety education.
Diagnosis Signs And Symptoms
Findings include cardiopulmonary arrest, cyanosis, dyspnea, copious pulmonary secretions, altered mental status or loss of consciousness, hypothermia, cerebral edema or neurologic injury, and evidence of trauma. Cervical spine injury is rare.
Essential Workup
Obtain witness and EMS information, initiate early airway management and cardiopulmonary resuscitation when indicated, and measure core temperature to assess hypothermia.
Diagnostic Tests And Interpretation
Laboratory studies include arterial blood gas, complete blood count, electrolytes, blood urea nitrogen, creatinine, glucose, and alcohol or toxicology screening. Imaging includes chest radiography, which may show infiltrates or acute respiratory distress syndrome but can be normal initially, electrocardiography showing bradyarrhythmias or tachyarrhythmias, and computed tomography of the brain or cervical spine when indicated.
Differential Diagnosis
Consider dysrhythmias such as long QT syndrome, myocardial infarction, seizure, syncope, trauma, or suicide attempt as causes of submersion. In pediatric patients, always consider abuse or neglect, particularly in bathtub incidents.
Treatment Prehospital
Address airway, breathing, and circulation, avoid further aspiration, secure the airway, initiate early cardiopulmonary resuscitation, apply cervical spine precautions when indicated, and begin rewarming. Abdominal thrusts are not recommended as they delay effective resuscitation and increase aspiration risk.
Initial Stabilization And Therapy
Manage airway and oxygenation, remove wet clothing, initiate rewarming, and support circulation.
Emergency Department Treatment
Correct hypoxemia, intubate with positive end-expiratory pressure if needed, treat acidosis, and evaluate for traumatic injuries. In cardiac arrest, follow advanced cardiac life support protocols and continue resuscitation until core temperature exceeds 32°C or return of spontaneous circulation occurs. Corticosteroids have no proven benefit. Poor prognostic indicators include prolonged submersion, severe acidosis, need for cardiopulmonary resuscitation, low oxygen saturation, and low Glasgow Coma Scale score.
Medication
Epinephrine, vasopressin, lidocaine, and sodium bicarbonate may be administered when clinically indicated.
Follow-Up And Disposition
Patients with respiratory symptoms, neurologic abnormalities, abnormal imaging or laboratory findings, or those requiring ventilatory support should be admitted, often to intensive care. Symptomatic patients or those with significant submersion history require observation. Patients may be discharged only after at least eight hours of observation with no respiratory distress, no neurologic impairment, and reliable caregivers.
Pearls And Pitfalls
All drowning patients require observation for delayed complications. Hypothermia may be protective. Prevention through supervision and water safety education is essential.

- Published on
Emergency and Acute Medicine – Domestic Violence
Basics
Description
Intimate partner violence (IPV) is physical, sexual, or psychological abuse by a current or former partner. It occurs in adult and adolescent intimate relationships across all socioeconomic groups.
Etiology
Most victims are women injured by male perpetrators, but men and individuals in same-sex relationships may also be victims. Risk factors include female sex, young age (20–24 years), and separation from a partner or spouse.
Diagnosis
Directly asking about IPV increases identification of victims.
Signs and symptoms
Traumatic injuries include a wide range of presentations. Unwitnessed head, neck, and facial injuries are common. Forearm bruises or fractures may suggest defensive posture. Injuries may be in various stages of healing.
Psychiatric and medical associations include chronic pain syndromes, depression, somatization, anxiety, suicidality, and substance abuse.
Alert
Clinical clues include discrepancies between history and physical findings, a partner refusing to leave the patient alone with the provider, delay in seeking care, any injury during pregnancy, concerning patient–partner interactions, and multiple symptoms without clear physical findings.
History
Screening questions can identify IPV. Evidence is mixed regarding improved outcomes, but IPV screening is required by the Joint Commission and supported by some professional organizations. Screening should be direct, nonjudgmental, supportive, and private. Computer-based ED screening may be effective. Consider IPV in patients with substance abuse or intoxication, who may be at higher risk and under-identified.
Physical examination
Perform a careful examination for traumatic injuries and a mental status assessment.
Essential workup
After IPV identification, perform a directed evaluation for traumatic injuries and acute medical or behavioral health conditions. Assess risk for future injury or victimization.
Differential diagnosis
Maintain a high index of suspicion for IPV in patients with traumatic injuries, behavioral health complaints, and medical presentations such as genitourinary or gynecologic complaints and multiple somatic symptoms.
Treatment
Prehospital
Provide standard trauma evaluation and treatment. Incorporate accurate EMS descriptions into the medical record.
Initial stabilization and therapy
Provide timely medical care and ongoing emotional support throughout evaluation and treatment.
Emergency department treatment and procedures
Interview the patient privately without family members present. Use a professional medical interpreter when needed. Document thoroughly using the patient’s exact words; careful documentation is admissible in court. Record extent and location of injuries; diagrams or photographs are helpful.
If stable for discharge, assess lethality risk, including escalating violence, threats of homicide or suicide, and access to lethal weapons. Collaborate with the patient to create a discharge plan aligned with their wishes. Arrange referrals for victim services, emergency shelter information, hotlines, restraining order information, and legal services.
Mandatory reporting varies by state and may increase risk or pose ethical challenges. Inform patients of reporting requirements and potential outcomes.
Medication
Acetaminophen 650–975 mg PO.
Morphine sulfate 0.1 mg/kg/dose IV or IM.
Follow-up and disposition
Admission criteria
Use standard admission guidelines based on injury severity. Medically stable patients with imminent safety risk may require hospitalization until a safe plan is established.
Discharge criteria
Patients whose safety is ensured and whose injuries are manageable as an outpatient may be discharged.
Issues for referral
Advocacy services availability varies by region.
Follow-up recommendations
Provide information on outpatient services and emergency shelter options.
Pearls and pitfalls
Failure to consider IPV in the differential diagnosis. Inadequate, nonobjective documentation of assault details and exam findings. Failure to assess discharge safety and arrange appropriate referrals. Mandatory reporting laws remain controversial and may have unintended consequences.
Basics
Description
Intimate partner violence (IPV) is physical, sexual, or psychological abuse by a current or former partner. It occurs in adult and adolescent intimate relationships across all socioeconomic groups.
Etiology
Most victims are women injured by male perpetrators, but men and individuals in same-sex relationships may also be victims. Risk factors include female sex, young age (20–24 years), and separation from a partner or spouse.
Diagnosis
Directly asking about IPV increases identification of victims.
Signs and symptoms
Traumatic injuries include a wide range of presentations. Unwitnessed head, neck, and facial injuries are common. Forearm bruises or fractures may suggest defensive posture. Injuries may be in various stages of healing.
Psychiatric and medical associations include chronic pain syndromes, depression, somatization, anxiety, suicidality, and substance abuse.
Alert
Clinical clues include discrepancies between history and physical findings, a partner refusing to leave the patient alone with the provider, delay in seeking care, any injury during pregnancy, concerning patient–partner interactions, and multiple symptoms without clear physical findings.
History
Screening questions can identify IPV. Evidence is mixed regarding improved outcomes, but IPV screening is required by the Joint Commission and supported by some professional organizations. Screening should be direct, nonjudgmental, supportive, and private. Computer-based ED screening may be effective. Consider IPV in patients with substance abuse or intoxication, who may be at higher risk and under-identified.
Physical examination
Perform a careful examination for traumatic injuries and a mental status assessment.
Essential workup
After IPV identification, perform a directed evaluation for traumatic injuries and acute medical or behavioral health conditions. Assess risk for future injury or victimization.
Differential diagnosis
Maintain a high index of suspicion for IPV in patients with traumatic injuries, behavioral health complaints, and medical presentations such as genitourinary or gynecologic complaints and multiple somatic symptoms.
Treatment
Prehospital
Provide standard trauma evaluation and treatment. Incorporate accurate EMS descriptions into the medical record.
Initial stabilization and therapy
Provide timely medical care and ongoing emotional support throughout evaluation and treatment.
Emergency department treatment and procedures
Interview the patient privately without family members present. Use a professional medical interpreter when needed. Document thoroughly using the patient’s exact words; careful documentation is admissible in court. Record extent and location of injuries; diagrams or photographs are helpful.
If stable for discharge, assess lethality risk, including escalating violence, threats of homicide or suicide, and access to lethal weapons. Collaborate with the patient to create a discharge plan aligned with their wishes. Arrange referrals for victim services, emergency shelter information, hotlines, restraining order information, and legal services.
Mandatory reporting varies by state and may increase risk or pose ethical challenges. Inform patients of reporting requirements and potential outcomes.
Medication
Acetaminophen 650–975 mg PO.
Morphine sulfate 0.1 mg/kg/dose IV or IM.
Follow-up and disposition
Admission criteria
Use standard admission guidelines based on injury severity. Medically stable patients with imminent safety risk may require hospitalization until a safe plan is established.
Discharge criteria
Patients whose safety is ensured and whose injuries are manageable as an outpatient may be discharged.
Issues for referral
Advocacy services availability varies by region.
Follow-up recommendations
Provide information on outpatient services and emergency shelter options.
Pearls and pitfalls
Failure to consider IPV in the differential diagnosis. Inadequate, nonobjective documentation of assault details and exam findings. Failure to assess discharge safety and arrange appropriate referrals. Mandatory reporting laws remain controversial and may have unintended consequences.
- Published on
Emergency and Acute Medicine – Dizziness
Basics
Description
Patient descriptions of dizziness (vertigo, lightheadedness, disequilibrium, or nonspecific terms) are often unreliable and should not guide decision making. A safer approach emphasizes associated symptoms, timing, and triggers, followed by a focused physical examination for diagnostic clues. Dizziness is categorized using a “timing and triggers” framework. Acute vestibular syndrome presents with abrupt onset of persistent dizziness. Episodic vestibular syndrome consists of spontaneous episodes lasting minutes to hours. Positional vestibular syndrome causes very brief episodes, typically 20–50 seconds, triggered by head or body position changes. Chronic vestibular syndrome has a gradual onset and persists for weeks to months or longer.
Etiology
General medical causes account for nearly half of cases and include arrhythmias, hypoglycemia and other metabolic disturbances, hypovolemia, sepsis, infections, and low cardiac output states. Otologic or vestibular causes represent about one third and include benign paroxysmal positional vertigo, labyrinthitis, and vestibular neuritis. Neurologic causes include stroke, transient ischemic attack, and vestibular migraine. Psychiatric causes such as anxiety and depression account for a smaller proportion.
Diagnosis
Signs and symptoms
History should define the timing and trigger pattern and assess for red flags. Key questions address onset, persistence versus intermittence, duration of episodes, positional triggers, associated hearing or neurologic symptoms, recent head injury, and new medications. Review of systems should focus on clues to serious disease, including headache suggesting stroke or dissection, ear pain suggesting otitis or mastoiditis, hearing changes suggesting Ménière disease or labyrinthitis, neck pain suggesting vertebral dissection, fever suggesting infection, dyspnea suggesting pulmonary embolism or anemia, chest pain suggesting acute coronary syndrome, fluid losses suggesting hypovolemia, and pregnancy-related complications.
Exacerbation with head motion occurs in both central and peripheral causes; however, dizziness only with head motion in an otherwise asymptomatic patient suggests a peripheral etiology.
Physical examination
Vital signs are assessed, including orthostatic testing. Otoscopic examination, cardiac examination, and a complete neurologic examination are essential. Cranial nerves II–XII should be evaluated with special attention to nystagmus. Gait observation and cerebellar testing are performed. The Dix–Hallpike maneuver is reserved for intermittent symptoms.
The HINTS examination is used only in patients with acute vestibular syndrome and consists of head impulse testing, nystagmus assessment, and testing for skew deviation. In the first 48 hours of symptoms, this exam can be more sensitive than MRI for detecting stroke. A normal head impulse test without corrective saccade suggests a central cause, whereas a corrective saccade suggests a peripheral cause. Direction-changing, vertical, or torsional nystagmus suggests a central etiology, while direction-fixed nystagmus suggests a peripheral cause. A vertical corrective saccade on alternate cover testing indicates a central process. Any concerning component should prompt concern for stroke.
Essential workup
History and physical examination are mandatory and often sufficient. Triage focuses on abnormal vital signs, altered mentation, or focal deficits. The evaluation is guided by timing, triggers, and telltale signs such as HINTS findings in acute dizziness.
Diagnosis tests and interpretation
Laboratory testing may include serum glucose, hematocrit if anemia is suspected, electrolytes, renal function tests, venous blood gas when carbon monoxide or hypercapnia is considered, urinalysis for infection, and toxicology screening when exposure is suspected.
Imaging includes noncontrast head CT when acute hemorrhage is suspected, recognizing limited sensitivity for posterior circulation ischemia. MRI is indicated when no alternative etiology is found and the HINTS exam is concerning.
Diagnostic procedures may include Dix–Hallpike testing, head thrust testing, and skew deviation assessment. Electrocardiography is used to detect arrhythmia or myocardial ischemia. Lumbar puncture is considered for unexplained headache or infectious signs.
Differential diagnosis
Acute vestibular syndrome includes benign causes such as vestibular neuritis and labyrinthitis and dangerous causes such as cerebellar or brainstem stroke. Episodic vestibular syndrome includes vestibular migraine and transient ischemic attack. Positional vestibular syndrome includes benign paroxysmal positional vertigo and, rarely, central paroxysmal positional vertigo from posterior fossa mass. Chronic vestibular syndrome includes psychiatric causes, medication effects, and rarely posterior fossa tumors.
Treatment
Initial stabilization and therapy
Stabilization is directed by abnormal vital signs or associated systemic illness. Management depends on classification of dizziness and suspected etiology.
Emergency department treatment and procedures
Symptomatic control is provided while evaluation proceeds. If benign paroxysmal positional vertigo is suspected, the Epley maneuver should be performed.
Medication
Symptomatic medications include ondansetron, diazepam, diphenhydramine, meclizine for short-term use only, and promethazine. Response to these agents does not establish etiology.
Follow-up and disposition
Admission criteria
Admission decisions depend on the underlying cause and associated symptoms, particularly concern for stroke, cardiac disease, or systemic illness.
Discharge criteria
Patients with isolated dizziness, normal neurologic and oculomotor examinations, and ability to function safely at home may be discharged with instructions.
Issues for referral
Outpatient referral may be to primary care, otolaryngology, or neurology depending on the suspected cause.
Follow-up recommendations
Patients should avoid driving or operating machinery while symptomatic and rise slowly from sitting or lying positions. They should seek immediate care for new neurologic deficits, signs of infection, acute cardiopulmonary symptoms, or significant fluid losses.
Pearls and pitfalls
The timing-and-triggers approach improves diagnostic accuracy. Advanced age and vascular risk factors increase stroke likelihood. Noncontrast CT is insensitive for acute cerebellar stroke, and cerebellar infarction may present with isolated dizziness. A negative head impulse test is concerning for central pathology. The treatment for benign paroxysmal positional vertigo is the Epley maneuver, not vestibular suppressants.
Basics
Description
Patient descriptions of dizziness (vertigo, lightheadedness, disequilibrium, or nonspecific terms) are often unreliable and should not guide decision making. A safer approach emphasizes associated symptoms, timing, and triggers, followed by a focused physical examination for diagnostic clues. Dizziness is categorized using a “timing and triggers” framework. Acute vestibular syndrome presents with abrupt onset of persistent dizziness. Episodic vestibular syndrome consists of spontaneous episodes lasting minutes to hours. Positional vestibular syndrome causes very brief episodes, typically 20–50 seconds, triggered by head or body position changes. Chronic vestibular syndrome has a gradual onset and persists for weeks to months or longer.
Etiology
General medical causes account for nearly half of cases and include arrhythmias, hypoglycemia and other metabolic disturbances, hypovolemia, sepsis, infections, and low cardiac output states. Otologic or vestibular causes represent about one third and include benign paroxysmal positional vertigo, labyrinthitis, and vestibular neuritis. Neurologic causes include stroke, transient ischemic attack, and vestibular migraine. Psychiatric causes such as anxiety and depression account for a smaller proportion.
Diagnosis
Signs and symptoms
History should define the timing and trigger pattern and assess for red flags. Key questions address onset, persistence versus intermittence, duration of episodes, positional triggers, associated hearing or neurologic symptoms, recent head injury, and new medications. Review of systems should focus on clues to serious disease, including headache suggesting stroke or dissection, ear pain suggesting otitis or mastoiditis, hearing changes suggesting Ménière disease or labyrinthitis, neck pain suggesting vertebral dissection, fever suggesting infection, dyspnea suggesting pulmonary embolism or anemia, chest pain suggesting acute coronary syndrome, fluid losses suggesting hypovolemia, and pregnancy-related complications.
Exacerbation with head motion occurs in both central and peripheral causes; however, dizziness only with head motion in an otherwise asymptomatic patient suggests a peripheral etiology.
Physical examination
Vital signs are assessed, including orthostatic testing. Otoscopic examination, cardiac examination, and a complete neurologic examination are essential. Cranial nerves II–XII should be evaluated with special attention to nystagmus. Gait observation and cerebellar testing are performed. The Dix–Hallpike maneuver is reserved for intermittent symptoms.
The HINTS examination is used only in patients with acute vestibular syndrome and consists of head impulse testing, nystagmus assessment, and testing for skew deviation. In the first 48 hours of symptoms, this exam can be more sensitive than MRI for detecting stroke. A normal head impulse test without corrective saccade suggests a central cause, whereas a corrective saccade suggests a peripheral cause. Direction-changing, vertical, or torsional nystagmus suggests a central etiology, while direction-fixed nystagmus suggests a peripheral cause. A vertical corrective saccade on alternate cover testing indicates a central process. Any concerning component should prompt concern for stroke.
Essential workup
History and physical examination are mandatory and often sufficient. Triage focuses on abnormal vital signs, altered mentation, or focal deficits. The evaluation is guided by timing, triggers, and telltale signs such as HINTS findings in acute dizziness.
Diagnosis tests and interpretation
Laboratory testing may include serum glucose, hematocrit if anemia is suspected, electrolytes, renal function tests, venous blood gas when carbon monoxide or hypercapnia is considered, urinalysis for infection, and toxicology screening when exposure is suspected.
Imaging includes noncontrast head CT when acute hemorrhage is suspected, recognizing limited sensitivity for posterior circulation ischemia. MRI is indicated when no alternative etiology is found and the HINTS exam is concerning.
Diagnostic procedures may include Dix–Hallpike testing, head thrust testing, and skew deviation assessment. Electrocardiography is used to detect arrhythmia or myocardial ischemia. Lumbar puncture is considered for unexplained headache or infectious signs.
Differential diagnosis
Acute vestibular syndrome includes benign causes such as vestibular neuritis and labyrinthitis and dangerous causes such as cerebellar or brainstem stroke. Episodic vestibular syndrome includes vestibular migraine and transient ischemic attack. Positional vestibular syndrome includes benign paroxysmal positional vertigo and, rarely, central paroxysmal positional vertigo from posterior fossa mass. Chronic vestibular syndrome includes psychiatric causes, medication effects, and rarely posterior fossa tumors.
Treatment
Initial stabilization and therapy
Stabilization is directed by abnormal vital signs or associated systemic illness. Management depends on classification of dizziness and suspected etiology.
Emergency department treatment and procedures
Symptomatic control is provided while evaluation proceeds. If benign paroxysmal positional vertigo is suspected, the Epley maneuver should be performed.
Medication
Symptomatic medications include ondansetron, diazepam, diphenhydramine, meclizine for short-term use only, and promethazine. Response to these agents does not establish etiology.
Follow-up and disposition
Admission criteria
Admission decisions depend on the underlying cause and associated symptoms, particularly concern for stroke, cardiac disease, or systemic illness.
Discharge criteria
Patients with isolated dizziness, normal neurologic and oculomotor examinations, and ability to function safely at home may be discharged with instructions.
Issues for referral
Outpatient referral may be to primary care, otolaryngology, or neurology depending on the suspected cause.
Follow-up recommendations
Patients should avoid driving or operating machinery while symptomatic and rise slowly from sitting or lying positions. They should seek immediate care for new neurologic deficits, signs of infection, acute cardiopulmonary symptoms, or significant fluid losses.
Pearls and pitfalls
The timing-and-triggers approach improves diagnostic accuracy. Advanced age and vascular risk factors increase stroke likelihood. Noncontrast CT is insensitive for acute cerebellar stroke, and cerebellar infarction may present with isolated dizziness. A negative head impulse test is concerning for central pathology. The treatment for benign paroxysmal positional vertigo is the Epley maneuver, not vestibular suppressants.

- Published on
Emergency And Acute Medicine - Ehrlichiosis
Foundational overview
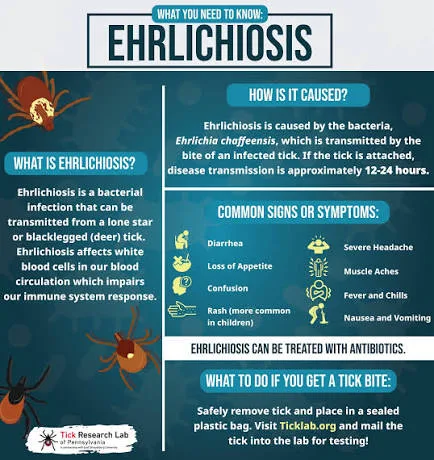
Ehrlichiosis is a tick-transmitted human infection that typically presents as a nonspecific febrile illness. Multiple forms exist, but two predominate in North America. Human monocytic ehrlichiosis was first recognized in 1987 and is transmitted by the lone star tick, Amblyomma americanum, with distribution primarily in the central, southern, and mid-Atlantic United States and expansion into parts of New England. Human granulocytic ehrlichiosis, also known as human granulocytic anaplasmosis, was described in 1994 and is transmitted by Ixodes scapularis, the same vector responsible for Lyme disease. Although all forms are tick borne, they differ in vectors and geographic distribution, with HME and HGE/HGA representing the clinically most relevant pathogens.
Causative organisms and pathogenesis
Ehrlichiosis is caused by obligate intracellular bacteria. Human monocytic ehrlichiosis results from infection with Ehrlichia chaffeensis, whereas human granulocytic ehrlichiosis/anaplasmosis is caused by Anaplasma phagocytophila. Taxonomic classification has evolved with advances in molecular diagnostics. Unlike Rocky Mountain spotted fever, vasculitis is typically absent. A third clinically similar infection caused by Ehrlichia ewingii may occur, also transmitted by the lone star tick. Compared with RMSF, ehrlichiosis more commonly affects adults over 40 years of age.
Clinical manifestations and symptom patterns
The clinical features of HME and HGE/HGA are largely overlapping. Many infected individuals experience asymptomatic seroconversion, and reported cases often represent more severe illness. Coinfection with other tick-borne pathogens from a single bite may complicate the presentation. Approximately one-quarter of pediatric patients develop severe disease.
Historical features
Epidemiologic context is critical. Most cases occur between April and October, with seasonal variability related to climate and geography. Symptoms typically begin 1–2 weeks after a tick bite, with a median onset of 9–10 days. Patients may recall a lone star tick bite more readily than a deer tick bite. Onset is often abrupt and includes fever, chills, headache, myalgias, and malaise. Rash is common in HME but infrequent in HGE/HGA and is often delayed. Severe illness may involve complications such as acute respiratory distress syndrome, renal failure, shock, rhabdomyolysis, gastrointestinal symptoms, central or peripheral nervous system involvement, seizures, or disseminated intravascular coagulation. Immunocompromised patients are at higher risk for severe outcomes.
Physical examination findings
Patients are typically febrile. Rash, when present, may be macular, maculopapular, or petechial and usually involves the trunk while sparing the palms and soles. Lymphadenopathy and hepatosplenomegaly may occur. Neurologic abnormalities can include altered mental status or meningismus, and pulmonary findings such as rales or rhonchi may be evident in patients with respiratory complications. In children, fever, headache, and rash are common, with lymphadenopathy frequently noted.
Essential diagnostic approach
Ehrlichiosis is primarily a clinical diagnosis and should be considered in patients with undifferentiated febrile illness during warm months, particularly with possible tick exposure. The CDC defines the illness as fever accompanied by symptoms such as headache, myalgia, cytopenias, or elevated transaminases, along with confirmatory laboratory evidence.
Laboratory evaluation and interpretation
Common laboratory abnormalities include leukopenia, thrombocytopenia, anemia, and elevated hepatic transaminases, often two to six times normal. Indirect immunofluorescence antibody testing is widely available and highly sensitive when paired acute and convalescent samples are obtained. Peripheral blood smear may reveal morulae, more commonly in HGE/HGA than HME, though sensitivity varies. PCR and culture testing are not routinely available. Lumbar puncture may show lymphocytic pleocytosis and elevated protein. Imaging is guided by complications, including head CT for encephalopathy and chest radiography for respiratory symptoms.
Conditions to distinguish from ehrlichiosis
The differential diagnosis includes other tick-borne illnesses such as Rocky Mountain spotted fever, Lyme disease, and babesiosis, as well as viral syndromes, mononucleosis, thrombotic thrombocytopenic purpura, hematologic malignancies, cholangitis, and pneumonia.
Initial stabilization principles
Standard airway, breathing, and circulation assessment should be performed in all patients.
Emergency department management
Empiric antimicrobial therapy should be initiated promptly when ehrlichiosis is suspected. Doxycycline is the treatment of choice for adults and children, including those under 9 years of age, as short courses have not been shown to cause clinically significant tooth discoloration. Therapy should continue for at least three days after fever resolution, with a minimum total course of seven days; longer treatment is required for severe disease. Rifampin may be used in pregnant patients, those with doxycycline allergy, or mildly affected young children. Coverage for other potential coinfections should be considered.
Medication considerations
Doxycycline is administered at 100 mg IV or orally every 12 hours in adults. Pediatric dosing is weight based, up to adult maximums. Despite typical age-related contraindications, doxycycline remains the drug of choice for severe pediatric disease. Rifampin is an alternative in selected populations. In pregnancy, rifampin is preferred, though doxycycline may be considered in life-threatening illness.
Disposition and follow-up planning
Hospital admission is recommended for patients with severe disease, significant comorbidities, immunosuppression, or inability to tolerate oral therapy. The case fatality rate for HME may reach 3%. Patients with mild illness who appear clinically stable may be discharged with close follow-up, as symptoms usually resolve within one to two weeks, though rare long-term neurologic sequelae have been reported.
Referral considerations
Specialty consultation is indicated for patients with severe or complicated disease.
Key clinical insights and common errors
Ehrlichiosis is a potentially fatal but treatable tick-borne illness that is frequently diagnosed clinically. Failure to consider it in patients with nonspecific febrile illness during tick season is a common error. Early initiation of doxycycline significantly improves outcomes and should not be delayed pending confirmatory testing. Coinfection with other tick-borne pathogens should always be considered, particularly in endemic regions.
Foundational overview
Ehrlichiosis is a tick-transmitted human infection that typically presents as a nonspecific febrile illness. Multiple forms exist, but two predominate in North America. Human monocytic ehrlichiosis was first recognized in 1987 and is transmitted by the lone star tick, Amblyomma americanum, with distribution primarily in the central, southern, and mid-Atlantic United States and expansion into parts of New England. Human granulocytic ehrlichiosis, also known as human granulocytic anaplasmosis, was described in 1994 and is transmitted by Ixodes scapularis, the same vector responsible for Lyme disease. Although all forms are tick borne, they differ in vectors and geographic distribution, with HME and HGE/HGA representing the clinically most relevant pathogens.
Causative organisms and pathogenesis
Ehrlichiosis is caused by obligate intracellular bacteria. Human monocytic ehrlichiosis results from infection with Ehrlichia chaffeensis, whereas human granulocytic ehrlichiosis/anaplasmosis is caused by Anaplasma phagocytophila. Taxonomic classification has evolved with advances in molecular diagnostics. Unlike Rocky Mountain spotted fever, vasculitis is typically absent. A third clinically similar infection caused by Ehrlichia ewingii may occur, also transmitted by the lone star tick. Compared with RMSF, ehrlichiosis more commonly affects adults over 40 years of age.
Clinical manifestations and symptom patterns
The clinical features of HME and HGE/HGA are largely overlapping. Many infected individuals experience asymptomatic seroconversion, and reported cases often represent more severe illness. Coinfection with other tick-borne pathogens from a single bite may complicate the presentation. Approximately one-quarter of pediatric patients develop severe disease.
Historical features
Epidemiologic context is critical. Most cases occur between April and October, with seasonal variability related to climate and geography. Symptoms typically begin 1–2 weeks after a tick bite, with a median onset of 9–10 days. Patients may recall a lone star tick bite more readily than a deer tick bite. Onset is often abrupt and includes fever, chills, headache, myalgias, and malaise. Rash is common in HME but infrequent in HGE/HGA and is often delayed. Severe illness may involve complications such as acute respiratory distress syndrome, renal failure, shock, rhabdomyolysis, gastrointestinal symptoms, central or peripheral nervous system involvement, seizures, or disseminated intravascular coagulation. Immunocompromised patients are at higher risk for severe outcomes.
Physical examination findings
Patients are typically febrile. Rash, when present, may be macular, maculopapular, or petechial and usually involves the trunk while sparing the palms and soles. Lymphadenopathy and hepatosplenomegaly may occur. Neurologic abnormalities can include altered mental status or meningismus, and pulmonary findings such as rales or rhonchi may be evident in patients with respiratory complications. In children, fever, headache, and rash are common, with lymphadenopathy frequently noted.
Essential diagnostic approach
Ehrlichiosis is primarily a clinical diagnosis and should be considered in patients with undifferentiated febrile illness during warm months, particularly with possible tick exposure. The CDC defines the illness as fever accompanied by symptoms such as headache, myalgia, cytopenias, or elevated transaminases, along with confirmatory laboratory evidence.
Laboratory evaluation and interpretation
Common laboratory abnormalities include leukopenia, thrombocytopenia, anemia, and elevated hepatic transaminases, often two to six times normal. Indirect immunofluorescence antibody testing is widely available and highly sensitive when paired acute and convalescent samples are obtained. Peripheral blood smear may reveal morulae, more commonly in HGE/HGA than HME, though sensitivity varies. PCR and culture testing are not routinely available. Lumbar puncture may show lymphocytic pleocytosis and elevated protein. Imaging is guided by complications, including head CT for encephalopathy and chest radiography for respiratory symptoms.
Conditions to distinguish from ehrlichiosis
The differential diagnosis includes other tick-borne illnesses such as Rocky Mountain spotted fever, Lyme disease, and babesiosis, as well as viral syndromes, mononucleosis, thrombotic thrombocytopenic purpura, hematologic malignancies, cholangitis, and pneumonia.
Initial stabilization principles
Standard airway, breathing, and circulation assessment should be performed in all patients.
Emergency department management
Empiric antimicrobial therapy should be initiated promptly when ehrlichiosis is suspected. Doxycycline is the treatment of choice for adults and children, including those under 9 years of age, as short courses have not been shown to cause clinically significant tooth discoloration. Therapy should continue for at least three days after fever resolution, with a minimum total course of seven days; longer treatment is required for severe disease. Rifampin may be used in pregnant patients, those with doxycycline allergy, or mildly affected young children. Coverage for other potential coinfections should be considered.
Medication considerations
Doxycycline is administered at 100 mg IV or orally every 12 hours in adults. Pediatric dosing is weight based, up to adult maximums. Despite typical age-related contraindications, doxycycline remains the drug of choice for severe pediatric disease. Rifampin is an alternative in selected populations. In pregnancy, rifampin is preferred, though doxycycline may be considered in life-threatening illness.
Disposition and follow-up planning
Hospital admission is recommended for patients with severe disease, significant comorbidities, immunosuppression, or inability to tolerate oral therapy. The case fatality rate for HME may reach 3%. Patients with mild illness who appear clinically stable may be discharged with close follow-up, as symptoms usually resolve within one to two weeks, though rare long-term neurologic sequelae have been reported.
Referral considerations
Specialty consultation is indicated for patients with severe or complicated disease.
Key clinical insights and common errors
Ehrlichiosis is a potentially fatal but treatable tick-borne illness that is frequently diagnosed clinically. Failure to consider it in patients with nonspecific febrile illness during tick season is a common error. Early initiation of doxycycline significantly improves outcomes and should not be delayed pending confirmatory testing. Coinfection with other tick-borne pathogens should always be considered, particularly in endemic regions.
- Published on
Emergency And Acute Medicine - Electrical Injury
Basics Description
Electricity represents the movement of electrons through a conductor down a gradient from higher to lower concentration. The severity and pattern of electrical injury depend on multiple factors, including voltage, current strength and type, tissue resistance, and duration of contact. According to Ohm’s law, voltage equals current multiplied by resistance, meaning that current increases with higher voltage and decreases with greater resistance. Electrical sources are broadly divided into low- and high-voltage exposures. Household outlets typically supply 110 V, dryers and ranges about 220 V, subway third rails approximately 600 V, residential trunk lines around 7,620 V, and industrial power lines may reach 100,000 V. Some household devices contain internal transformers that increase voltage despite being plugged into low-voltage outlets.
Tissue resistance influences injury patterns. Nerves, muscles, and blood vessels have low resistance and conduct electricity efficiently, while bone, fat, and tendon have higher resistance. Moist skin lowers resistance, whereas calloused skin increases it. Higher resistance generates more heat at the tissue level. Current strength, measured in amperes, determines physiologic effects. Very small currents produce tingling, slightly higher levels cause pain, and increasing currents lead to muscle tetany, respiratory muscle paralysis, ventricular fibrillation, or asystole. Alternating current, used in homes and offices, reverses direction rhythmically and is more dangerous than direct current because it can cause sustained muscle contraction and prolonged contact, increasing the risk of ventricular fibrillation. Direct current, used in defibrillators and industrial sources, tends to cause a single powerful muscle contraction that may throw the victim away from the source, shortening exposure but increasing traumatic injury risk.
Electrical injuries follow a trimodal age distribution, affecting toddlers exposed to outlets and cords, adolescents engaging in risk-taking behaviors, and adults with occupational exposures.
Etiology
Electrical injuries occur through several mechanisms. Direct contact can cause electrothermal burns with coagulation necrosis of skin and deep tissues, often underestimating the true extent of injury. Flame injuries may result from ignition of clothing or surrounding materials. Electrical arcs can produce flash burns when high-voltage current passes through air, usually causing superficial partial-thickness burns. Primary electrical effects include cardiac dysrhythmias and sustained muscle contraction, while secondary injuries result from falls or being thrown due to intense muscle tetany.
Diagnosis Signs And Symptoms
Clinical manifestations vary by organ system. Head and neck involvement is common in high-voltage injuries and may include facial or corneal burns, tympanic membrane perforation, and delayed ocular complications such as cataracts or optic nerve damage. Cardiovascular effects are a leading cause of mortality and include cardiac arrest, ventricular fibrillation, asystole, and transient dysrhythmias. Respiratory compromise may occur from central respiratory inhibition, chest wall tetany, or traumatic lung injury. Neurologic findings range from transient confusion and amnesia to seizures, coma, spinal cord injury, and long-term neuropsychiatric sequelae. Vascular injury can lead to thrombosis, compartment syndrome, and renal failure from myoglobinuria. Musculoskeletal injuries may result from powerful muscle contractions, classically causing vertebral fractures, posterior shoulder dislocations, or femoral neck fractures. Dermatologic findings include entry and exit wounds, commonly on the hands, feet, or head, as well as characteristic “kissing” burns at flexor surfaces.
Essential Workup
Evaluation should include urinalysis to assess for myoglobin, electrocardiography, and cardiac enzymes in patients with high-voltage exposure or cardiorespiratory symptoms. Cardiac monitoring is indicated for patients with loss of consciousness, dysrhythmias, abnormal ECGs, hypoxia, chest pain, known heart disease, or significant associated trauma. Asymptomatic patients with normal ECGs and low-voltage exposure generally do not require prolonged monitoring.
Diagnosis Tests And Interpretation
Laboratory testing is often unnecessary for minor household exposures but should be considered when myoglobinuria or high-voltage injury is suspected. Creatine kinase, electrolytes, renal function tests, and cardiac biomarkers provide baseline assessment and help identify complications such as rhabdomyolysis, metabolic derangements, or myocardial injury. Imaging studies are guided by clinical findings and concern for associated trauma.
Differential Diagnosis
Important considerations include distinguishing deep electrothermal injury from superficial flash burns and separating electrical injury effects from trauma-related instability.
Treatment Prehospital
Scene safety is paramount, with immediate disconnection of the power source. Victims should be assumed to have traumatic injuries if unstable or unconscious, with spinal immobilization as indicated. Early cardiopulmonary resuscitation may be lifesaving in electrical arrest. Burns should be covered with clean, dry dressings, and fractures or dislocations splinted.
Initial Stabilization And Therapy
Management follows standard airway, breathing, and circulation principles. Local wound care, fracture reduction, and immobilization are addressed early.
Emergency Department Treatment And Procedures
Aggressive intravenous fluid resuscitation is often required due to extensive third spacing within injured muscle, targeting urine output of at least 1 mL/kg/hr. Foley catheter placement assists in monitoring. Prevention of renal failure includes maintaining urine flow and alkalinization with sodium bicarbonate to reduce myoglobin toxicity. Diuretics such as furosemide or mannitol may be used selectively. Tetanus prophylaxis and adequate analgesia are essential.
Medication
Therapeutic options include intravenous sodium bicarbonate to alkalinize urine, loop diuretics, and osmotic diuretics when indicated to maintain urine output and prevent renal complications.
Follow-Up Disposition
Admission is required for patients with loss of consciousness, dysrhythmias, abnormal ECGs, suspected deep tissue injury, myoglobinuria, significant burns, major trauma, or pregnancy beyond 20 weeks’ gestation. Patients with minor low-voltage injuries, normal examinations, and no symptoms after observation may be discharged with appropriate instructions.
Follow-Up Recommendations
Patients should receive specialty referral as indicated, including burn care, neurology for delayed neurologic symptoms, obstetrics for pregnant patients, dentistry or reconstructive surgery for pediatric oral burns, and ophthalmology to screen for delayed cataract formation.
Clinical Insights And Common Errors
Routine prolonged cardiac monitoring is unnecessary in asymptomatic patients with normal ECGs after low-voltage exposure. In significant electrical injuries, adequate fluid resuscitation is critical to counteract extensive third spacing and prevent renal failure.
Basics Description
Electricity represents the movement of electrons through a conductor down a gradient from higher to lower concentration. The severity and pattern of electrical injury depend on multiple factors, including voltage, current strength and type, tissue resistance, and duration of contact. According to Ohm’s law, voltage equals current multiplied by resistance, meaning that current increases with higher voltage and decreases with greater resistance. Electrical sources are broadly divided into low- and high-voltage exposures. Household outlets typically supply 110 V, dryers and ranges about 220 V, subway third rails approximately 600 V, residential trunk lines around 7,620 V, and industrial power lines may reach 100,000 V. Some household devices contain internal transformers that increase voltage despite being plugged into low-voltage outlets.
Tissue resistance influences injury patterns. Nerves, muscles, and blood vessels have low resistance and conduct electricity efficiently, while bone, fat, and tendon have higher resistance. Moist skin lowers resistance, whereas calloused skin increases it. Higher resistance generates more heat at the tissue level. Current strength, measured in amperes, determines physiologic effects. Very small currents produce tingling, slightly higher levels cause pain, and increasing currents lead to muscle tetany, respiratory muscle paralysis, ventricular fibrillation, or asystole. Alternating current, used in homes and offices, reverses direction rhythmically and is more dangerous than direct current because it can cause sustained muscle contraction and prolonged contact, increasing the risk of ventricular fibrillation. Direct current, used in defibrillators and industrial sources, tends to cause a single powerful muscle contraction that may throw the victim away from the source, shortening exposure but increasing traumatic injury risk.
Electrical injuries follow a trimodal age distribution, affecting toddlers exposed to outlets and cords, adolescents engaging in risk-taking behaviors, and adults with occupational exposures.
Etiology
Electrical injuries occur through several mechanisms. Direct contact can cause electrothermal burns with coagulation necrosis of skin and deep tissues, often underestimating the true extent of injury. Flame injuries may result from ignition of clothing or surrounding materials. Electrical arcs can produce flash burns when high-voltage current passes through air, usually causing superficial partial-thickness burns. Primary electrical effects include cardiac dysrhythmias and sustained muscle contraction, while secondary injuries result from falls or being thrown due to intense muscle tetany.
Diagnosis Signs And Symptoms
Clinical manifestations vary by organ system. Head and neck involvement is common in high-voltage injuries and may include facial or corneal burns, tympanic membrane perforation, and delayed ocular complications such as cataracts or optic nerve damage. Cardiovascular effects are a leading cause of mortality and include cardiac arrest, ventricular fibrillation, asystole, and transient dysrhythmias. Respiratory compromise may occur from central respiratory inhibition, chest wall tetany, or traumatic lung injury. Neurologic findings range from transient confusion and amnesia to seizures, coma, spinal cord injury, and long-term neuropsychiatric sequelae. Vascular injury can lead to thrombosis, compartment syndrome, and renal failure from myoglobinuria. Musculoskeletal injuries may result from powerful muscle contractions, classically causing vertebral fractures, posterior shoulder dislocations, or femoral neck fractures. Dermatologic findings include entry and exit wounds, commonly on the hands, feet, or head, as well as characteristic “kissing” burns at flexor surfaces.
Essential Workup
Evaluation should include urinalysis to assess for myoglobin, electrocardiography, and cardiac enzymes in patients with high-voltage exposure or cardiorespiratory symptoms. Cardiac monitoring is indicated for patients with loss of consciousness, dysrhythmias, abnormal ECGs, hypoxia, chest pain, known heart disease, or significant associated trauma. Asymptomatic patients with normal ECGs and low-voltage exposure generally do not require prolonged monitoring.
Diagnosis Tests And Interpretation
Laboratory testing is often unnecessary for minor household exposures but should be considered when myoglobinuria or high-voltage injury is suspected. Creatine kinase, electrolytes, renal function tests, and cardiac biomarkers provide baseline assessment and help identify complications such as rhabdomyolysis, metabolic derangements, or myocardial injury. Imaging studies are guided by clinical findings and concern for associated trauma.
Differential Diagnosis
Important considerations include distinguishing deep electrothermal injury from superficial flash burns and separating electrical injury effects from trauma-related instability.
Treatment Prehospital
Scene safety is paramount, with immediate disconnection of the power source. Victims should be assumed to have traumatic injuries if unstable or unconscious, with spinal immobilization as indicated. Early cardiopulmonary resuscitation may be lifesaving in electrical arrest. Burns should be covered with clean, dry dressings, and fractures or dislocations splinted.
Initial Stabilization And Therapy
Management follows standard airway, breathing, and circulation principles. Local wound care, fracture reduction, and immobilization are addressed early.
Emergency Department Treatment And Procedures
Aggressive intravenous fluid resuscitation is often required due to extensive third spacing within injured muscle, targeting urine output of at least 1 mL/kg/hr. Foley catheter placement assists in monitoring. Prevention of renal failure includes maintaining urine flow and alkalinization with sodium bicarbonate to reduce myoglobin toxicity. Diuretics such as furosemide or mannitol may be used selectively. Tetanus prophylaxis and adequate analgesia are essential.
Medication
Therapeutic options include intravenous sodium bicarbonate to alkalinize urine, loop diuretics, and osmotic diuretics when indicated to maintain urine output and prevent renal complications.
Follow-Up Disposition
Admission is required for patients with loss of consciousness, dysrhythmias, abnormal ECGs, suspected deep tissue injury, myoglobinuria, significant burns, major trauma, or pregnancy beyond 20 weeks’ gestation. Patients with minor low-voltage injuries, normal examinations, and no symptoms after observation may be discharged with appropriate instructions.
Follow-Up Recommendations
Patients should receive specialty referral as indicated, including burn care, neurology for delayed neurologic symptoms, obstetrics for pregnant patients, dentistry or reconstructive surgery for pediatric oral burns, and ophthalmology to screen for delayed cataract formation.
Clinical Insights And Common Errors
Routine prolonged cardiac monitoring is unnecessary in asymptomatic patients with normal ECGs after low-voltage exposure. In significant electrical injuries, adequate fluid resuscitation is critical to counteract extensive third spacing and prevent renal failure.

- Published on
Emergency And Acute Medicine - Elbow Injuries
Overview and injury patterns
Elbow trauma includes both bony and soft tissue injuries and varies by age and mechanism. In children, supracondylar fractures are the most frequent elbow fractures, most often occurring between 5 and 10 years of age and rarely after adolescence. These fractures are commonly extension type injuries caused by a fall on an outstretched hand with the elbow extended or hyperextended. Extension injuries are classified by displacement, ranging from nondisplaced to completely displaced fractures. Flexion type supracondylar fractures are less common and result from a direct blow to a flexed elbow. Radial head fractures typically occur through indirect mechanisms such as a fall on an outstretched hand, where force is transmitted up the forearm into the capitellum.
Soft tissue injuries are also common. Elbow dislocation is the second most frequent large-joint dislocation after the shoulder, with posterior dislocations accounting for the majority. Overuse injuries such as medial and lateral epicondylitis involve repetitive stress at the flexor or extensor tendon insertions and are often seen in individuals whose occupations or sports require repetitive wrist rotation and gripping.
Age specific considerations
In young children, radial head subluxation, commonly referred to as nursemaid’s elbow, accounts for a significant proportion of upper extremity injuries. It most often affects children aged 1 to 4 years and results from sudden longitudinal traction on the pronated forearm. Pediatric patients are also at risk for nonaccidental trauma, which should be considered when the history does not align with the injury pattern.
Mechanisms and causes
Understanding the mechanism of injury is essential, as most elbow injuries are caused by indirect trauma transmitted through the forearm bones, such as falls on an outstretched hand. Direct blows to the elbow are a less common cause of fractures or dislocations.
Clinical presentation and examination features
The manner in which a patient holds the injured arm often provides diagnostic clues. In flexion type supracondylar fractures, patients typically support the forearm with the opposite hand and hold the elbow flexed at 90 degrees. Extension type fractures may present with the arm held at the side in an abnormal configuration. Posterior elbow dislocations produce a prominent olecranon, whereas anterior dislocations cause loss of the normal olecranon contour. Radial head subluxation presents with the elbow slightly flexed and the forearm pronated, with resistance to movement. Epicondylitis develops gradually, with aching pain over the medial or lateral elbow that worsens with grasping or twisting activities.
Essential evaluation steps
Plain radiographs are the cornerstone of evaluation and should include assessment of the wrist and shoulder for associated injuries. A thorough neurovascular examination is mandatory, along with inspection of the skin and assessment for compartment syndrome, which is particularly associated with supracondylar fractures.
Diagnostic studies and interpretation
Routine anteroposterior and lateral radiographs are usually sufficient, with oblique views added when subtle fractures are suspected. The presence of a fat pad sign is an important indicator of intra-articular injury. An elevated anterior fat pad or any visible posterior fat pad suggests joint effusion. In adults, an isolated posterior fat pad sign often indicates a radial head fracture, while in children it is more suggestive of a supracondylar fracture. Pediatric radiographs can be challenging due to unossified cartilage, so alignment lines and comparison views of the unaffected elbow may be helpful.
Conditions to distinguish from elbow trauma
Alternative diagnoses include sprains, strains, effusions, contusions, bursitis, and inflammatory arthritis.
Prehospital and early management principles
Initial care focuses on appropriate splinting and immobilization to prevent further injury during transport and evaluation.
Emergency department management strategies
Immobilization prior to imaging is essential. Orthopedic consultation is recommended for all but stable, nondisplaced fractures. Nondisplaced supracondylar fractures may be managed with posterior splinting and close follow-up, while displaced fractures require urgent orthopedic involvement, especially if vascular compromise is present. Elbow dislocations should be reduced promptly when neurovascular compromise exists, followed by splinting at 90 degrees of flexion. Minimally displaced radial head fractures may be managed with aspiration and immobilization, whereas more complex injuries warrant specialist evaluation. Radial head subluxation can often be reduced with a single supination-flexion maneuver or hyperpronation technique. Overuse injuries are treated conservatively with rest, splinting in severe cases, and anti-inflammatory therapy.
Medication and analgesia considerations
Adequate pain control is important and may include nonsteroidal anti-inflammatory drugs, acetaminophen-opioid combinations, or intravenous opioids for severe pain. Conscious sedation is often required to facilitate reduction of dislocations or displaced fractures.
Disposition and follow-up planning
Admission is indicated for open fractures, vascular injuries, fractures requiring surgical intervention, or significant swelling that raises concern for compartment syndrome. Stable fractures and successfully reduced dislocations may be discharged with splinting and orthopedic follow-up within 24 to 48 hours.
Clinical insights and frequent errors
A posterior fat pad sign should never be dismissed as normal. Neurovascular status must be assessed and documented before and after reduction of any elbow injury. Caregivers of children with supracondylar fractures should be educated on warning signs of compartment syndrome, as delayed recognition can result in serious morbidity.
Overview and injury patterns
Elbow trauma includes both bony and soft tissue injuries and varies by age and mechanism. In children, supracondylar fractures are the most frequent elbow fractures, most often occurring between 5 and 10 years of age and rarely after adolescence. These fractures are commonly extension type injuries caused by a fall on an outstretched hand with the elbow extended or hyperextended. Extension injuries are classified by displacement, ranging from nondisplaced to completely displaced fractures. Flexion type supracondylar fractures are less common and result from a direct blow to a flexed elbow. Radial head fractures typically occur through indirect mechanisms such as a fall on an outstretched hand, where force is transmitted up the forearm into the capitellum.
Soft tissue injuries are also common. Elbow dislocation is the second most frequent large-joint dislocation after the shoulder, with posterior dislocations accounting for the majority. Overuse injuries such as medial and lateral epicondylitis involve repetitive stress at the flexor or extensor tendon insertions and are often seen in individuals whose occupations or sports require repetitive wrist rotation and gripping.
Age specific considerations
In young children, radial head subluxation, commonly referred to as nursemaid’s elbow, accounts for a significant proportion of upper extremity injuries. It most often affects children aged 1 to 4 years and results from sudden longitudinal traction on the pronated forearm. Pediatric patients are also at risk for nonaccidental trauma, which should be considered when the history does not align with the injury pattern.
Mechanisms and causes
Understanding the mechanism of injury is essential, as most elbow injuries are caused by indirect trauma transmitted through the forearm bones, such as falls on an outstretched hand. Direct blows to the elbow are a less common cause of fractures or dislocations.
Clinical presentation and examination features
The manner in which a patient holds the injured arm often provides diagnostic clues. In flexion type supracondylar fractures, patients typically support the forearm with the opposite hand and hold the elbow flexed at 90 degrees. Extension type fractures may present with the arm held at the side in an abnormal configuration. Posterior elbow dislocations produce a prominent olecranon, whereas anterior dislocations cause loss of the normal olecranon contour. Radial head subluxation presents with the elbow slightly flexed and the forearm pronated, with resistance to movement. Epicondylitis develops gradually, with aching pain over the medial or lateral elbow that worsens with grasping or twisting activities.
Essential evaluation steps
Plain radiographs are the cornerstone of evaluation and should include assessment of the wrist and shoulder for associated injuries. A thorough neurovascular examination is mandatory, along with inspection of the skin and assessment for compartment syndrome, which is particularly associated with supracondylar fractures.
Diagnostic studies and interpretation
Routine anteroposterior and lateral radiographs are usually sufficient, with oblique views added when subtle fractures are suspected. The presence of a fat pad sign is an important indicator of intra-articular injury. An elevated anterior fat pad or any visible posterior fat pad suggests joint effusion. In adults, an isolated posterior fat pad sign often indicates a radial head fracture, while in children it is more suggestive of a supracondylar fracture. Pediatric radiographs can be challenging due to unossified cartilage, so alignment lines and comparison views of the unaffected elbow may be helpful.
Conditions to distinguish from elbow trauma
Alternative diagnoses include sprains, strains, effusions, contusions, bursitis, and inflammatory arthritis.
Prehospital and early management principles
Initial care focuses on appropriate splinting and immobilization to prevent further injury during transport and evaluation.
Emergency department management strategies
Immobilization prior to imaging is essential. Orthopedic consultation is recommended for all but stable, nondisplaced fractures. Nondisplaced supracondylar fractures may be managed with posterior splinting and close follow-up, while displaced fractures require urgent orthopedic involvement, especially if vascular compromise is present. Elbow dislocations should be reduced promptly when neurovascular compromise exists, followed by splinting at 90 degrees of flexion. Minimally displaced radial head fractures may be managed with aspiration and immobilization, whereas more complex injuries warrant specialist evaluation. Radial head subluxation can often be reduced with a single supination-flexion maneuver or hyperpronation technique. Overuse injuries are treated conservatively with rest, splinting in severe cases, and anti-inflammatory therapy.
Medication and analgesia considerations
Adequate pain control is important and may include nonsteroidal anti-inflammatory drugs, acetaminophen-opioid combinations, or intravenous opioids for severe pain. Conscious sedation is often required to facilitate reduction of dislocations or displaced fractures.
Disposition and follow-up planning
Admission is indicated for open fractures, vascular injuries, fractures requiring surgical intervention, or significant swelling that raises concern for compartment syndrome. Stable fractures and successfully reduced dislocations may be discharged with splinting and orthopedic follow-up within 24 to 48 hours.
Clinical insights and frequent errors
A posterior fat pad sign should never be dismissed as normal. Neurovascular status must be assessed and documented before and after reduction of any elbow injury. Caregivers of children with supracondylar fractures should be educated on warning signs of compartment syndrome, as delayed recognition can result in serious morbidity.

- Published on
Emergency And Acute Medicine - Endometriosis
Basic Overview
Endometriosis is defined by the presence of endometrial glands and stroma located outside the uterine cavity. It is an estrogen-dependent, chronic inflammatory condition. The disorder affects approximately 6–10% of women of reproductive age and up to 50–60% of women and adolescents presenting with chronic pelvic pain. Ectopic endometrial tissue is most commonly found within the pelvic cavity, particularly on the ovaries and uterosacral ligaments, likely related to retrograde menstruation. Less commonly, implants may occur at distant sites, including the bowel, diaphragm, and lungs.
Underlying Mechanisms
The exact cause of endometriosis remains unknown.
Risk Factors And Special Populations
Risk factors include early menarche, short menstrual cycles, anatomic obstruction to menstrual outflow, and a suspected genetic predisposition supported by family and twin studies.
In pediatric patients, endometriosis does not occur before menarche.
Clinical Presentation
Symptoms vary widely and are often chronic and cyclical. Dysmenorrhea is the most common complaint, occurring in the majority of patients. Other frequent symptoms include deep pelvic pain, dyspareunia, abnormal uterine bleeding, lower abdominal pain, nausea, abdominal bloating, and infertility, which affects up to half of patients.
Physical Examination Findings
Pelvic examination may reveal focal tenderness, particularly along the uterosacral ligaments, a retroverted uterus, rectovaginal nodularity, or a palpable pelvic mass. Findings depend on the location and extent of ectopic endometrial tissue and may be subtle or absent. Rarely, thoracic involvement may cause catamenial pneumothorax, characterized by recurrent pneumothorax coinciding with menses.
Initial Evaluation Priorities
A pregnancy test is mandatory in all patients of reproductive age. Testing for gonorrhea and chlamydia should be considered. Additional diagnostic studies are guided by the history and physical examination. Endometriosis is rarely definitively diagnosed in the emergency department.
Diagnostic Studies And Interpretation
Laboratory evaluation typically includes pregnancy testing and sexually transmitted infection screening. Hematocrit and type-and-screen testing are indicated if bleeding is significant.
Imaging has limited sensitivity in the acute setting. Ultrasound and CT have low diagnostic yield, while MRI offers higher sensitivity and specificity but is not routinely used emergently. Definitive diagnosis generally requires laparoscopy.
Conditions To Consider
The differential diagnosis includes appendicitis, ectopic pregnancy, pelvic inflammatory disease, tubo-ovarian abscess, ovarian cyst or torsion, inflammatory bowel disease, irritable bowel syndrome, dysfunctional uterine bleeding, and physiologic menstrual pain such as mittelschmerz.
Emergency Management Principles
Prehospital care focuses on stabilization and analgesia as needed.
Initial Stabilization Measures
Patients with hypotension or tachycardia due to blood loss should receive isotonic intravenous fluids. Transfusion with packed red blood cells may be necessary in cases of significant hemorrhage.
Emergency Department Interventions
Management is largely symptomatic and includes pain control. Hormonal therapy, such as oral progestins or gonadotropin-releasing hormone agonists, should be initiated only in consultation with gynecology or the patient’s primary care clinician. Gynecology consultation is indicated for severe pain, heavy bleeding, or suspected complications.
Medication Options
First-line analgesia includes nonsteroidal anti-inflammatory drugs and acetaminophen. Ketorolac may be used for moderate to severe pain, and opioids are reserved for refractory cases.
Disposition And Follow-Up
Hospital admission is warranted for patients with intractable pain, significant bleeding, peritoneal signs, diagnostic uncertainty, or need for further evaluation. Most patients with suspected endometriosis who are clinically stable can be discharged with adequate pain control and outpatient gynecology referral.
Follow-Up Guidance
All suspected cases require referral to a gynecologist for definitive diagnosis and long-term management.
Clinical Insights And Common Errors
Endometriosis affects a substantial proportion of women of reproductive age and commonly presents with cyclical pelvic pain. It is rarely diagnosed during an initial emergency department visit, and delays in diagnosis often span years. Emergency clinicians must exclude other acute and life-threatening conditions, manage symptoms appropriately, and ensure reliable outpatient follow-up. Endometriosis is a chronic disease that requires ongoing care by gynecology or primary care providers.
Basic Overview
Endometriosis is defined by the presence of endometrial glands and stroma located outside the uterine cavity. It is an estrogen-dependent, chronic inflammatory condition. The disorder affects approximately 6–10% of women of reproductive age and up to 50–60% of women and adolescents presenting with chronic pelvic pain. Ectopic endometrial tissue is most commonly found within the pelvic cavity, particularly on the ovaries and uterosacral ligaments, likely related to retrograde menstruation. Less commonly, implants may occur at distant sites, including the bowel, diaphragm, and lungs.
Underlying Mechanisms
The exact cause of endometriosis remains unknown.
Risk Factors And Special Populations
Risk factors include early menarche, short menstrual cycles, anatomic obstruction to menstrual outflow, and a suspected genetic predisposition supported by family and twin studies.
In pediatric patients, endometriosis does not occur before menarche.
Clinical Presentation
Symptoms vary widely and are often chronic and cyclical. Dysmenorrhea is the most common complaint, occurring in the majority of patients. Other frequent symptoms include deep pelvic pain, dyspareunia, abnormal uterine bleeding, lower abdominal pain, nausea, abdominal bloating, and infertility, which affects up to half of patients.
Physical Examination Findings
Pelvic examination may reveal focal tenderness, particularly along the uterosacral ligaments, a retroverted uterus, rectovaginal nodularity, or a palpable pelvic mass. Findings depend on the location and extent of ectopic endometrial tissue and may be subtle or absent. Rarely, thoracic involvement may cause catamenial pneumothorax, characterized by recurrent pneumothorax coinciding with menses.
Initial Evaluation Priorities
A pregnancy test is mandatory in all patients of reproductive age. Testing for gonorrhea and chlamydia should be considered. Additional diagnostic studies are guided by the history and physical examination. Endometriosis is rarely definitively diagnosed in the emergency department.
Diagnostic Studies And Interpretation
Laboratory evaluation typically includes pregnancy testing and sexually transmitted infection screening. Hematocrit and type-and-screen testing are indicated if bleeding is significant.
Imaging has limited sensitivity in the acute setting. Ultrasound and CT have low diagnostic yield, while MRI offers higher sensitivity and specificity but is not routinely used emergently. Definitive diagnosis generally requires laparoscopy.
Conditions To Consider
The differential diagnosis includes appendicitis, ectopic pregnancy, pelvic inflammatory disease, tubo-ovarian abscess, ovarian cyst or torsion, inflammatory bowel disease, irritable bowel syndrome, dysfunctional uterine bleeding, and physiologic menstrual pain such as mittelschmerz.
Emergency Management Principles
Prehospital care focuses on stabilization and analgesia as needed.
Initial Stabilization Measures
Patients with hypotension or tachycardia due to blood loss should receive isotonic intravenous fluids. Transfusion with packed red blood cells may be necessary in cases of significant hemorrhage.
Emergency Department Interventions
Management is largely symptomatic and includes pain control. Hormonal therapy, such as oral progestins or gonadotropin-releasing hormone agonists, should be initiated only in consultation with gynecology or the patient’s primary care clinician. Gynecology consultation is indicated for severe pain, heavy bleeding, or suspected complications.
Medication Options
First-line analgesia includes nonsteroidal anti-inflammatory drugs and acetaminophen. Ketorolac may be used for moderate to severe pain, and opioids are reserved for refractory cases.
Disposition And Follow-Up
Hospital admission is warranted for patients with intractable pain, significant bleeding, peritoneal signs, diagnostic uncertainty, or need for further evaluation. Most patients with suspected endometriosis who are clinically stable can be discharged with adequate pain control and outpatient gynecology referral.
Follow-Up Guidance
All suspected cases require referral to a gynecologist for definitive diagnosis and long-term management.
Clinical Insights And Common Errors
Endometriosis affects a substantial proportion of women of reproductive age and commonly presents with cyclical pelvic pain. It is rarely diagnosed during an initial emergency department visit, and delays in diagnosis often span years. Emergency clinicians must exclude other acute and life-threatening conditions, manage symptoms appropriately, and ensure reliable outpatient follow-up. Endometriosis is a chronic disease that requires ongoing care by gynecology or primary care providers.

- Published on
Emergency And Acute Medicine - Encephalitis
Basics Overview
Encephalitis is an acute inflammatory process involving the brain parenchyma and accounts for approximately 20,000 cases annually in the United States, with an overall mortality near 10%. The inflammatory response leads to neuronal destruction, cerebral edema, and petechial hemorrhages. Central nervous system infection most commonly occurs via hematogenous spread from respiratory or gastrointestinal sources, blood transfusion, or organ transplantation. Certain pathogens, including rabies virus, herpes simplex virus (HSV), and varicella zoster virus (VZV), may reach the CNS through neural migration.
Etiologic Factors
Viral infections represent the most frequent cause, although noninfectious etiologies such as autoimmune, paraneoplastic, and collagen vascular diseases are increasingly recognized. In nearly half of cases, no specific cause is identified. HSV accounts for approximately 10–20% of all encephalitis cases, and early antiviral therapy significantly improves outcomes. Arboviruses cause 10–15% of cases and are transmitted by mosquitoes or ticks during warmer months. Eastern equine encephalitis is notable for its fulminant course and hippocampal involvement, while Western equine encephalitis tends to follow a nonspecific prodrome. Japanese encephalitis, the most common arboviral encephalitis worldwide, often progresses from mild systemic symptoms to severe neurologic dysfunction.
Flaviviruses such as West Nile virus have increased in incidence in North America and are associated with higher morbidity and mortality in elderly patients, with possible flaccid paralysis and respiratory failure. Enteroviruses primarily affect children and usually follow a benign course. Measles-related encephalitis may occur acutely or years after infection and often involves seizures and rapid neurologic decline. HIV-associated encephalitis is linked to low CD4 counts and presents with white matter degeneration, motor spasticity, and dementia. Rabies causes isolated CNS infection without systemic illness.
Nonviral infectious causes include Mycoplasma pneumoniae, Toxoplasma gondii, Rickettsia rickettsii, Mycobacterium tuberculosis, Borrelia burgdorferi, and Bartonella henselae. In immunocompromised patients, pathogens such as Cryptococcus neoformans, CMV, HHV-6, Listeria monocytogenes, and VZV are common. Autoimmune etiologies include anti-LGI1 and anti–NMDA receptor encephalitis.
Clinical Features And Symptoms
Encephalitis often begins after a brief flulike prodrome characterized by fever, headache, myalgias, sore throat, and reduced appetite. Progressive neurologic involvement includes altered mental status ranging from confusion to coma, personality changes, hallucinations, psychosis, agitation, or delirium. Seizures are common, as are focal neurologic deficits such as tremor, ataxia, cranial nerve palsies, and autonomic instability. Rash may accompany certain infectious causes. Papilledema may be present, and the disease course may be indolent or rapidly progressive, potentially resulting in permanent neurologic injury or death.
Diagnostic Evaluation
A lumbar puncture is essential and typically reveals lymphocytic pleocytosis, elevated protein, and normal glucose in viral etiologies. CSF should undergo Gram stain, culture, and targeted antigen or antibody testing based on clinical suspicion. PCR testing of CSF is critical for confirming viral causes, particularly HSV, VZV, enteroviruses, and West Nile virus. Blood studies include CBC, metabolic panel, liver function tests, and blood cultures. Imaging begins with CT to exclude mass lesions or hemorrhage, while MRI is more sensitive for detecting temporal lobe abnormalities typical of HSV encephalitis. EEG is useful in patients with seizures or unexplained altered mental status.
Differential Considerations
Conditions that may mimic encephalitis include meningitis, brain abscess, sepsis, ischemic or hemorrhagic stroke, head trauma, subarachnoid hemorrhage, metabolic encephalopathies, epilepsy, acute disseminated encephalomyelitis, neoplasms, and toxic exposures such as carbon monoxide.
Initial Management And Stabilization
Immediate priorities include airway protection, seizure control, and stabilization of vital functions. Patients with depressed consciousness or absent protective reflexes require intubation. Empiric treatment for altered mental status includes glucose, thiamine, and naloxone when indicated. Signs of increased intracranial pressure warrant hyperventilation and osmotic therapy with mannitol, along with neurosurgical consultation. Intravenous fluids should be administered cautiously to avoid worsening cerebral edema.
Emergency Department Care
Seizures are treated promptly with benzodiazepines, followed by longer-acting antiepileptic agents if recurrent. Although no specific therapy exists for most viral encephalitides, intravenous acyclovir must be initiated immediately when HSV encephalitis is suspected, based on clinical presentation and preliminary CSF or imaging findings. In immunocompromised patients, ganciclovir or foscarnet should be considered for CMV or HHV-6. Broad-spectrum antibiotics should be administered when meningitis cannot be excluded, especially in the presence of rash or systemic toxicity.
Pharmacologic Therapy
Recommended agents include intravenous acyclovir for suspected HSV, benzodiazepines for acute seizure control, fosphenytoin or phenobarbital for seizure prophylaxis, and mannitol for elevated intracranial pressure. Antiviral therapy should not be delayed while awaiting confirmatory testing.
Disposition And Follow-Up
All patients with suspected or confirmed encephalitis require hospital admission for close neurologic monitoring and definitive management.
Clinical Insights And Common Errors
Empiric treatment with acyclovir should be started immediately in any patient with unexplained encephalitis, as delays significantly increase morbidity and mortality. Failure to initiate early antiviral therapy remains one of the most critical and preventable errors in management.
Basics Overview
Encephalitis is an acute inflammatory process involving the brain parenchyma and accounts for approximately 20,000 cases annually in the United States, with an overall mortality near 10%. The inflammatory response leads to neuronal destruction, cerebral edema, and petechial hemorrhages. Central nervous system infection most commonly occurs via hematogenous spread from respiratory or gastrointestinal sources, blood transfusion, or organ transplantation. Certain pathogens, including rabies virus, herpes simplex virus (HSV), and varicella zoster virus (VZV), may reach the CNS through neural migration.
Etiologic Factors
Viral infections represent the most frequent cause, although noninfectious etiologies such as autoimmune, paraneoplastic, and collagen vascular diseases are increasingly recognized. In nearly half of cases, no specific cause is identified. HSV accounts for approximately 10–20% of all encephalitis cases, and early antiviral therapy significantly improves outcomes. Arboviruses cause 10–15% of cases and are transmitted by mosquitoes or ticks during warmer months. Eastern equine encephalitis is notable for its fulminant course and hippocampal involvement, while Western equine encephalitis tends to follow a nonspecific prodrome. Japanese encephalitis, the most common arboviral encephalitis worldwide, often progresses from mild systemic symptoms to severe neurologic dysfunction.
Flaviviruses such as West Nile virus have increased in incidence in North America and are associated with higher morbidity and mortality in elderly patients, with possible flaccid paralysis and respiratory failure. Enteroviruses primarily affect children and usually follow a benign course. Measles-related encephalitis may occur acutely or years after infection and often involves seizures and rapid neurologic decline. HIV-associated encephalitis is linked to low CD4 counts and presents with white matter degeneration, motor spasticity, and dementia. Rabies causes isolated CNS infection without systemic illness.
Nonviral infectious causes include Mycoplasma pneumoniae, Toxoplasma gondii, Rickettsia rickettsii, Mycobacterium tuberculosis, Borrelia burgdorferi, and Bartonella henselae. In immunocompromised patients, pathogens such as Cryptococcus neoformans, CMV, HHV-6, Listeria monocytogenes, and VZV are common. Autoimmune etiologies include anti-LGI1 and anti–NMDA receptor encephalitis.
Clinical Features And Symptoms
Encephalitis often begins after a brief flulike prodrome characterized by fever, headache, myalgias, sore throat, and reduced appetite. Progressive neurologic involvement includes altered mental status ranging from confusion to coma, personality changes, hallucinations, psychosis, agitation, or delirium. Seizures are common, as are focal neurologic deficits such as tremor, ataxia, cranial nerve palsies, and autonomic instability. Rash may accompany certain infectious causes. Papilledema may be present, and the disease course may be indolent or rapidly progressive, potentially resulting in permanent neurologic injury or death.
Diagnostic Evaluation
A lumbar puncture is essential and typically reveals lymphocytic pleocytosis, elevated protein, and normal glucose in viral etiologies. CSF should undergo Gram stain, culture, and targeted antigen or antibody testing based on clinical suspicion. PCR testing of CSF is critical for confirming viral causes, particularly HSV, VZV, enteroviruses, and West Nile virus. Blood studies include CBC, metabolic panel, liver function tests, and blood cultures. Imaging begins with CT to exclude mass lesions or hemorrhage, while MRI is more sensitive for detecting temporal lobe abnormalities typical of HSV encephalitis. EEG is useful in patients with seizures or unexplained altered mental status.
Differential Considerations
Conditions that may mimic encephalitis include meningitis, brain abscess, sepsis, ischemic or hemorrhagic stroke, head trauma, subarachnoid hemorrhage, metabolic encephalopathies, epilepsy, acute disseminated encephalomyelitis, neoplasms, and toxic exposures such as carbon monoxide.
Initial Management And Stabilization
Immediate priorities include airway protection, seizure control, and stabilization of vital functions. Patients with depressed consciousness or absent protective reflexes require intubation. Empiric treatment for altered mental status includes glucose, thiamine, and naloxone when indicated. Signs of increased intracranial pressure warrant hyperventilation and osmotic therapy with mannitol, along with neurosurgical consultation. Intravenous fluids should be administered cautiously to avoid worsening cerebral edema.
Emergency Department Care
Seizures are treated promptly with benzodiazepines, followed by longer-acting antiepileptic agents if recurrent. Although no specific therapy exists for most viral encephalitides, intravenous acyclovir must be initiated immediately when HSV encephalitis is suspected, based on clinical presentation and preliminary CSF or imaging findings. In immunocompromised patients, ganciclovir or foscarnet should be considered for CMV or HHV-6. Broad-spectrum antibiotics should be administered when meningitis cannot be excluded, especially in the presence of rash or systemic toxicity.
Pharmacologic Therapy
Recommended agents include intravenous acyclovir for suspected HSV, benzodiazepines for acute seizure control, fosphenytoin or phenobarbital for seizure prophylaxis, and mannitol for elevated intracranial pressure. Antiviral therapy should not be delayed while awaiting confirmatory testing.
Disposition And Follow-Up
All patients with suspected or confirmed encephalitis require hospital admission for close neurologic monitoring and definitive management.
Clinical Insights And Common Errors
Empiric treatment with acyclovir should be started immediately in any patient with unexplained encephalitis, as delays significantly increase morbidity and mortality. Failure to initiate early antiviral therapy remains one of the most critical and preventable errors in management.
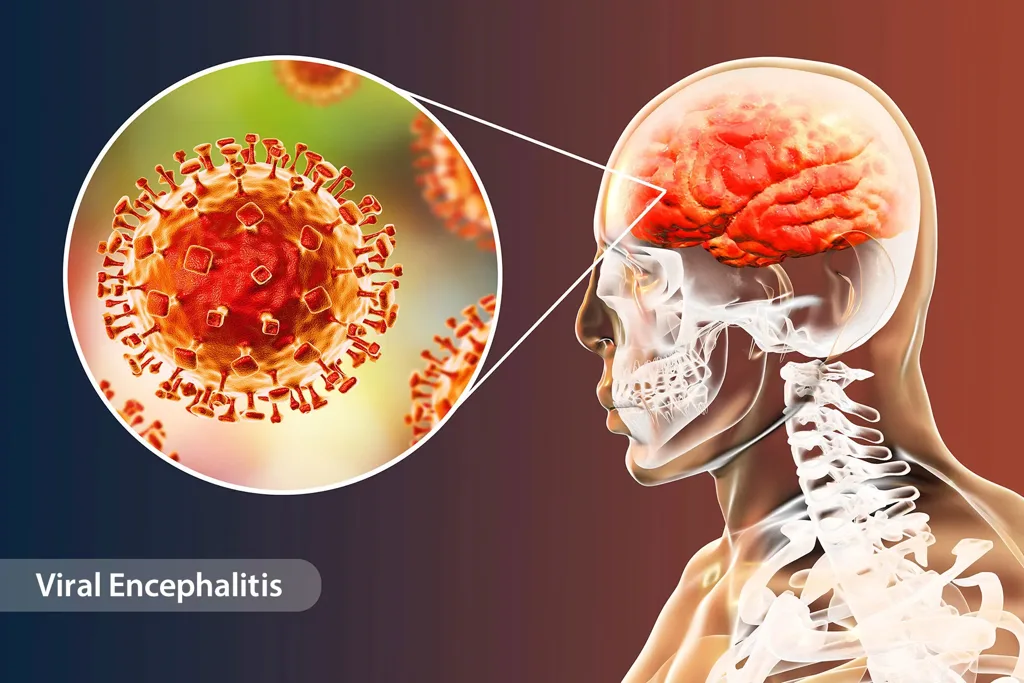
- Published on
Emergency And Acute Medicine - Endocarditis
Basic Overview
Endocarditis is an inflammatory condition involving the endothelial lining of the heart. It most commonly affects native cardiac valves but may also involve prosthetic valves, the interventricular septum, chordae tendineae, mural endocardium, or intracardiac devices. The disease is defined by the formation of vegetations, which are thrombotic aggregates of fibrin and platelets that become colonized by microorganisms. Progressive bacterial growth enlarges these vegetations, disrupts normal blood flow, provokes inflammation, and may result in systemic embolization. The condition is almost always infectious in origin, typically bacterial. Rare noninfectious forms include nonbacterial thrombotic (marantic) endocarditis associated with hypercoagulable states and Libman–Sacks endocarditis related to systemic lupus erythematosus, both characterized by small sterile vegetations.
Epidemiologic Features
Endocarditis occurs more frequently in men, with incidence rates significantly higher than in women. Risk increases with advanced age, poor dental hygiene, and comorbid medical conditions. Structural heart disease, including rheumatic heart disease, mitral valve prolapse, aortic valve dysfunction, congenital heart defects, and prosthetic valves, predisposes patients due to altered intracardiac flow. Hemodialysis, diabetes, and indwelling intravascular catheters further increase risk. Intravenous drug use confers a particularly high risk and commonly involves right-sided valves. Septic embolization may lead to neurologic, pulmonary, splenic, renal, hepatic, or coronary complications, as well as mycotic aneurysm formation.
Causative Mechanisms
Most cases are due to bacterial infection. Common pathogens include Staphylococcus aureus, the most frequent cause across all populations and especially prevalent among intravenous drug users. Streptococcus viridans is a typical cause of native valve disease and originates from the oropharynx. Streptococcus bovis is associated with colonic polyps or gastrointestinal malignancy. Streptococcus pneumoniae may cause aggressive valvular destruction and heart failure. Staphylococcus epidermidis is frequently implicated in prosthetic valve infections. Enterococci are often linked to genitourinary or gastrointestinal instrumentation. Fungal causes, such as Candida or Aspergillus, occur primarily in immunocompromised patients or those with prosthetic valves. Culture-negative endocarditis may result from organisms such as Coxiella burnetii, Bartonella, or Brucella.
Clinical Presentation
Fever is the most common symptom, present in the majority of patients, though it may be absent in the elderly, those with chronic renal failure, heart failure, or severe debility. Constitutional symptoms include chills, sweats, rigors, malaise, and flulike illness. Cardiac findings often include a new or changing murmur and signs of heart failure. Embolic phenomena may cause neurologic deficits, stroke, or mycotic aneurysms. Cutaneous manifestations include petechiae, splinter hemorrhages, Osler nodes, and Janeway lesions. Splenomegaly, abdominal or back pain, arthralgias, and myalgias may also be present.
Diagnostic Assessment
Evaluation should focus on identifying risk factors in patients with unexplained fever. Multiple sets of blood cultures obtained before antibiotic administration are essential. Laboratory studies commonly show anemia, leukocytosis, elevated inflammatory markers, and microscopic hematuria. Electrocardiography may reveal arrhythmias or new conduction abnormalities. Chest radiography can demonstrate signs of heart failure or septic pulmonary emboli. Echocardiography is critical for diagnosis, with transesophageal echocardiography offering superior sensitivity for detecting vegetations, abscesses, and valvular dysfunction. Computed tomography may aid in identifying complications.
Differential Considerations
Conditions that may mimic endocarditis include rheumatic fever, atrial myxoma, acute pericarditis, myocardial infarction, aortic dissection with valvular involvement, thrombotic thrombocytopenic purpura, systemic lupus erythematosus, metastatic malignancy, septicemia, and cotton fever.
Initial Management Principles
Patients should be closely monitored for signs of heart failure or embolic complications. Early consultation with cardiology and cardiothoracic surgery is required for patients with severe valvular dysfunction, intracardiac abscess, prosthetic valve instability, persistent infection despite therapy, or large or fungal vegetations. Empiric intravenous bactericidal antibiotics should be initiated after blood cultures are obtained, with regimens tailored based on valve type, risk factors, and local resistance patterns.
Antimicrobial Therapy
Empiric treatment commonly includes combinations of penicillin, nafcillin, gentamicin, or vancomycin, adjusted once culture data are available. Prosthetic valve infections and intravenous drug use often require broader coverage, including rifampin. Resistant organisms may necessitate agents such as daptomycin or quinupristin–dalfopristin. Fungal endocarditis is treated with amphotericin B, and HACEK organisms respond well to ceftriaxone.
Disposition And Follow-Up
All patients with suspected or confirmed endocarditis require hospital admission. Individuals with hemodynamic instability, neurologic complications, or heart failure should be managed in a monitored or intensive care setting. There are no criteria for emergency department discharge.
Clinical Insights And Common Errors
Endocarditis should be strongly considered in any patient with fever and a new or changing murmur, even in the absence of known valvular disease. Health care exposure and indwelling devices are important risk factors. Failure to obtain adequate blood cultures before antibiotics or to recognize embolic and heart failure complications can delay diagnosis and worsen outcomes. All intravenous drug users presenting with fever should be admitted and evaluated for endocarditis.
Basic Overview
Endocarditis is an inflammatory condition involving the endothelial lining of the heart. It most commonly affects native cardiac valves but may also involve prosthetic valves, the interventricular septum, chordae tendineae, mural endocardium, or intracardiac devices. The disease is defined by the formation of vegetations, which are thrombotic aggregates of fibrin and platelets that become colonized by microorganisms. Progressive bacterial growth enlarges these vegetations, disrupts normal blood flow, provokes inflammation, and may result in systemic embolization. The condition is almost always infectious in origin, typically bacterial. Rare noninfectious forms include nonbacterial thrombotic (marantic) endocarditis associated with hypercoagulable states and Libman–Sacks endocarditis related to systemic lupus erythematosus, both characterized by small sterile vegetations.
Epidemiologic Features
Endocarditis occurs more frequently in men, with incidence rates significantly higher than in women. Risk increases with advanced age, poor dental hygiene, and comorbid medical conditions. Structural heart disease, including rheumatic heart disease, mitral valve prolapse, aortic valve dysfunction, congenital heart defects, and prosthetic valves, predisposes patients due to altered intracardiac flow. Hemodialysis, diabetes, and indwelling intravascular catheters further increase risk. Intravenous drug use confers a particularly high risk and commonly involves right-sided valves. Septic embolization may lead to neurologic, pulmonary, splenic, renal, hepatic, or coronary complications, as well as mycotic aneurysm formation.
Causative Mechanisms
Most cases are due to bacterial infection. Common pathogens include Staphylococcus aureus, the most frequent cause across all populations and especially prevalent among intravenous drug users. Streptococcus viridans is a typical cause of native valve disease and originates from the oropharynx. Streptococcus bovis is associated with colonic polyps or gastrointestinal malignancy. Streptococcus pneumoniae may cause aggressive valvular destruction and heart failure. Staphylococcus epidermidis is frequently implicated in prosthetic valve infections. Enterococci are often linked to genitourinary or gastrointestinal instrumentation. Fungal causes, such as Candida or Aspergillus, occur primarily in immunocompromised patients or those with prosthetic valves. Culture-negative endocarditis may result from organisms such as Coxiella burnetii, Bartonella, or Brucella.
Clinical Presentation
Fever is the most common symptom, present in the majority of patients, though it may be absent in the elderly, those with chronic renal failure, heart failure, or severe debility. Constitutional symptoms include chills, sweats, rigors, malaise, and flulike illness. Cardiac findings often include a new or changing murmur and signs of heart failure. Embolic phenomena may cause neurologic deficits, stroke, or mycotic aneurysms. Cutaneous manifestations include petechiae, splinter hemorrhages, Osler nodes, and Janeway lesions. Splenomegaly, abdominal or back pain, arthralgias, and myalgias may also be present.
Diagnostic Assessment
Evaluation should focus on identifying risk factors in patients with unexplained fever. Multiple sets of blood cultures obtained before antibiotic administration are essential. Laboratory studies commonly show anemia, leukocytosis, elevated inflammatory markers, and microscopic hematuria. Electrocardiography may reveal arrhythmias or new conduction abnormalities. Chest radiography can demonstrate signs of heart failure or septic pulmonary emboli. Echocardiography is critical for diagnosis, with transesophageal echocardiography offering superior sensitivity for detecting vegetations, abscesses, and valvular dysfunction. Computed tomography may aid in identifying complications.
Differential Considerations
Conditions that may mimic endocarditis include rheumatic fever, atrial myxoma, acute pericarditis, myocardial infarction, aortic dissection with valvular involvement, thrombotic thrombocytopenic purpura, systemic lupus erythematosus, metastatic malignancy, septicemia, and cotton fever.
Initial Management Principles
Patients should be closely monitored for signs of heart failure or embolic complications. Early consultation with cardiology and cardiothoracic surgery is required for patients with severe valvular dysfunction, intracardiac abscess, prosthetic valve instability, persistent infection despite therapy, or large or fungal vegetations. Empiric intravenous bactericidal antibiotics should be initiated after blood cultures are obtained, with regimens tailored based on valve type, risk factors, and local resistance patterns.
Antimicrobial Therapy
Empiric treatment commonly includes combinations of penicillin, nafcillin, gentamicin, or vancomycin, adjusted once culture data are available. Prosthetic valve infections and intravenous drug use often require broader coverage, including rifampin. Resistant organisms may necessitate agents such as daptomycin or quinupristin–dalfopristin. Fungal endocarditis is treated with amphotericin B, and HACEK organisms respond well to ceftriaxone.
Disposition And Follow-Up
All patients with suspected or confirmed endocarditis require hospital admission. Individuals with hemodynamic instability, neurologic complications, or heart failure should be managed in a monitored or intensive care setting. There are no criteria for emergency department discharge.
Clinical Insights And Common Errors
Endocarditis should be strongly considered in any patient with fever and a new or changing murmur, even in the absence of known valvular disease. Health care exposure and indwelling devices are important risk factors. Failure to obtain adequate blood cultures before antibiotics or to recognize embolic and heart failure complications can delay diagnosis and worsen outcomes. All intravenous drug users presenting with fever should be admitted and evaluated for endocarditis.