- Published on
Medical Terms - Barlow's sign
A sign of congenital hip dislocation identified within the initial 6 weeks of life. To elicit this sign, position the newborn supine with the hips flexed at 90 degrees and the knees fully flexed. Position your palm over the infant's knee, placing your thumb in the femoral triangle adjacent to the lesser trochanter and your index finger over the larger trochanter. Position the hip in midabduction while applying gentle posterior and lateral pressure with your thumb and posterior and medial pressure with your palm. Upon detecting a click of the femoral head as it dislocates along the posterior rim of the acetabular socket, you have elicited this indication.
A sign of congenital hip dislocation identified within the initial 6 weeks of life. To elicit this sign, position the newborn supine with the hips flexed at 90 degrees and the knees fully flexed. Position your palm over the infant's knee, placing your thumb in the femoral triangle adjacent to the lesser trochanter and your index finger over the larger trochanter. Position the hip in midabduction while applying gentle posterior and lateral pressure with your thumb and posterior and medial pressure with your palm. Upon detecting a click of the femoral head as it dislocates along the posterior rim of the acetabular socket, you have elicited this indication.

- Published on
Surgery -Analgesia
Effectively managing a patient's pain during the perioperative period is a fundamental obligation of a surgical student. The advantages of managing acute pain encompass: • Wound healing. • Mobility. • Patient contentment. • Premature hospital discharge. • Decrease in the likelihood of thromboembolic occurrences. In instances of acute pain resulting from trauma, surgery, delivery, or a medical condition, it is crucial to ascertain the location, temporal characteristics, and intensity of the pain. Various approaches are available for evaluating the patient's pain
Techniques for Evaluating Acute Pain
Visual analogue scale (VAS)
-Scored between ‘no pain’ and ‘pain as bad as it can be’
Verbal response score (VRS)
Pain scored as a number, e.g. 4 out of 10, or verbally, e.g.
mild, severe, excruciating
Autonomic response
Sweating, tachycardia, hypertension (HTN)
Dynamic pain scores
Pain on movement; ability to take a deep breath; ability
to cough
The objective of postoperative analgesia is to reduce the dosage of analgesic drugs, hence avoiding side effects, while ensuring sufficient and efficient pain relief. The World Health Organization analgesic ladder This was initially devised for the management of persistent pain associated with cancer. The ladder is being employed to address multiple forms of pain. The technique involves the immediate prescription of analgesics upon the onset of pain and the adjustment of the regimen until the patient achieves pain relief, utilizing the ladder system
Postoperatively, patients will necessitate potent and effective analgesia. The oral route is favored whenever feasible. In the acute postoperative phase or in cases of vomiting, intravenous administration may be necessary.
The intramuscular (IM) method is unpleasant and has inconsistent absorption; it should be avoided when feasible. The analgesic regimen can be titrated down utilizing the World Health Organization (WHO) ladder as the patient convalesces in the days subsequent to the procedure. To guarantee that patients receive consistent and extended analgesia, these should be supplied routinely rather than on an as-needed basis. Adjuvant medicines are agents that augment the efficacy of analgesics, such as anticonvulsants like gabapentin utilized for neuropathic pain.
WHO Pain Relief Ladder
Mild pain
Non-opioid (e.g. aspirin, paracetamol or NSAID) +/− adjuvant
Mild to moderate pain
Weak opioid (e.g. codeine)
+/− non-opioid
+/− adjuvant
Moderate to severe pain
Strong opioid
(e.g. morphine)
+/− non-opioid
+/− adjuvant
Effectively managing a patient's pain during the perioperative period is a fundamental obligation of a surgical student. The advantages of managing acute pain encompass: • Wound healing. • Mobility. • Patient contentment. • Premature hospital discharge. • Decrease in the likelihood of thromboembolic occurrences. In instances of acute pain resulting from trauma, surgery, delivery, or a medical condition, it is crucial to ascertain the location, temporal characteristics, and intensity of the pain. Various approaches are available for evaluating the patient's pain
Techniques for Evaluating Acute Pain
Visual analogue scale (VAS)
-Scored between ‘no pain’ and ‘pain as bad as it can be’
Verbal response score (VRS)
Pain scored as a number, e.g. 4 out of 10, or verbally, e.g.
mild, severe, excruciating
Autonomic response
Sweating, tachycardia, hypertension (HTN)
Dynamic pain scores
Pain on movement; ability to take a deep breath; ability
to cough
The objective of postoperative analgesia is to reduce the dosage of analgesic drugs, hence avoiding side effects, while ensuring sufficient and efficient pain relief. The World Health Organization analgesic ladder This was initially devised for the management of persistent pain associated with cancer. The ladder is being employed to address multiple forms of pain. The technique involves the immediate prescription of analgesics upon the onset of pain and the adjustment of the regimen until the patient achieves pain relief, utilizing the ladder system
Postoperatively, patients will necessitate potent and effective analgesia. The oral route is favored whenever feasible. In the acute postoperative phase or in cases of vomiting, intravenous administration may be necessary.
The intramuscular (IM) method is unpleasant and has inconsistent absorption; it should be avoided when feasible. The analgesic regimen can be titrated down utilizing the World Health Organization (WHO) ladder as the patient convalesces in the days subsequent to the procedure. To guarantee that patients receive consistent and extended analgesia, these should be supplied routinely rather than on an as-needed basis. Adjuvant medicines are agents that augment the efficacy of analgesics, such as anticonvulsants like gabapentin utilized for neuropathic pain.
WHO Pain Relief Ladder
Mild pain
Non-opioid (e.g. aspirin, paracetamol or NSAID) +/− adjuvant
Mild to moderate pain
Weak opioid (e.g. codeine)
+/− non-opioid
+/− adjuvant
Moderate to severe pain
Strong opioid
(e.g. morphine)
+/− non-opioid
+/− adjuvant

- Published on
Medical Terms – Abadie’s Sign
Abadie's sign -Spasm of the levator palpebrae superioris muscle. This indication may be subtle or pronounced and may impact one eye or both eyes. It indicates an exophthalmic goiter associated with Graves' disease.
Abadie's sign -Spasm of the levator palpebrae superioris muscle. This indication may be subtle or pronounced and may impact one eye or both eyes. It indicates an exophthalmic goiter associated with Graves' disease.

- Published on
Symptoms and Signs – Differential Diagnosis of Excessive Weight Loss
Weight loss may indicate reduced food consumption, diminished nutrient absorption, heightened metabolic demands, or a combination thereof. The reasons encompass endocrine, neoplastic, gastrointestinal, and psychiatric illnesses; nutritional inadequacies; infections; and neurological lesions that result in paralysis and dysphagia. Weight loss may occur due to factors that inhibit adequate food consumption, including painful oral lesions, poorly fitting dentures, and tooth loss. The cause may be the metabolic impact of poverty, restrictive diets, excessive physical activity, or specific medications. Weight loss may manifest as a delayed symptom in chronic conditions such as heart failure and renal illness. In certain disorders, however, it is a consequence of anorexia.
Medical History and Physical Assessment
Commence with a comprehensive dietary history, as weight loss is typically attributable to insufficient caloric consumption. Investigate the reasons for the patient's inadequate dietary intake. Inquire about his prior weight and whether the recent reduction was deliberate. Remain vigilant for lifestyle or occupational alterations that could contribute to anxiety or despair. Has he become separated or divorced? Has a relative or acquaintance lately passed away? Has he lately transitioned to a new position? Investigate recent alterations in bowel habits, including diarrhea or voluminous, buoyant feces. Has the patient had nausea, vomiting, or abdominal pain, which may suggest a gastrointestinal disorder? Has he experienced polydipsia, polyuria, or heat intolerance, which may indicate an endocrine disorder? Conduct a meticulous drug history, paying particular attention to the usage of diet medications and laxatives. Meticulously assess the patient's height and weight, and inquire about his prior weight. Assess his vital signs and document his overall appearance: Is he adequately nourished? Do his garments fit properly? Is muscular atrophy apparent? Inquire about specific weight fluctuations, including approximate dates. Subsequently, assess the patient's skin for turgor and irregular pigmentation, particularly in the vicinity of the joints. Does he exhibit pallor or jaundice? Inspect his oral cavity, assessing the state of his teeth or dentures. Examine for indications of infection or irritation on the palatal surface, and observe any hyperpigmentation of the buccal mucosa.
Additionally, examine the patient’s eyes for exophthalmos and inspect the neck for edema; assess the lungs for abnormal sounds. Examine the abdomen for indications of wasting, and palpate for lumps, discomfort, and hepatomegaly. Standard laboratory and radiologic assessments, including complete blood count, serum albumin levels, urinalysis, chest X-ray, and upper gastrointestinal series, typically elucidate the etiology. Nearly all physical etiologies are clinically apparent during the initial assessment. Cancer, gastrointestinal problems, and depression are the predominant pathological reasons.
Etiological Factors
Adrenal insufficiency. Adrenal insufficiency results in weight loss, accompanied by anorexia, weakness, exhaustion, irritability, syncope, nausea, vomiting, stomach discomfort, and either diarrhea or constipation. Hyperpigmentation may manifest at the joints, belt line, palmar wrinkles, lips, gums, tongue, and buccal mucosa.
Anorexia nervosa
Anorexia nervosa is a psychogenic condition predominantly affecting young women, defined by significant self-induced weight loss of 10% to 50% of premorbid weight, which is generally within the normal range or no more than 5 lb (2.3 kg) above optimal weight. Associated observations encompass skeletal muscle atrophy, reduction of adipose tissue, hypotension, constipation, dental cavities, increased vulnerability to infections, mottled or pallid skin, cold sensitivity, hirsutism on the face and body, alopecia or scalp hair loss, and amenorrhea. The patient typically exhibits hyperactivity and energy, along with an intense dread of weight gain. Self-induced vomiting or the use of laxatives or diuretics may result in dehydration or metabolic alkalosis or acidosis.
Oncology
Weight loss frequently indicates the presence of cancer. Additional results indicate the nature, location, and stage of the tumor, which may encompass fatigue, pain, nausea, vomiting, anorexia, irregular bleeding, and a palpable lump.
Crohn's disease
Weight loss is associated with persistent cramping, stomach discomfort, and anorexia. Additional signs and symptoms encompass diarrhea, nausea, fever, tachycardia, abdominal soreness and guarding, hyperactive bowel noises, abdominal distension, and pain. Perianal lesions and a discernible lump in the right or left lower quadrant may also be evident.
Cryptosporidiosis
Weight loss may ensue from cryptosporidiosis, an opportunistic protozoan infection. Additional results encompass abundant watery diarrhea, stomach cramping, flatulence, anorexia, lethargy, fever, nausea, vomiting, and myalgia.
Depression
Severe depression may result in weight loss or weight gain, accompanied by insomnia or hypersomnia, anorexia, apathy, exhaustion, and feelings of worthlessness. Indecision, lack of coherence, and suicidal ideation or actions may also manifest.
Diabetes mellitus
Weight loss can occur in diabetes mellitus, even with heightened hunger. Additional findings encompass polydipsia, asthenia, tiredness, and polyuria accompanied by nocturia.
Esophagitis
Inflammation of the esophagus causes discomfort, resulting in a temporary cessation of eating and consequent weight reduction. Severe oral and anterior chest discomfort is accompanied by hypersalivation, dysphagia, tachypnea, and hematemesis. Should a stricture occur, dysphagia and weight loss will reemerge.
Gastroenteritis
Weight loss in gastroenteritis is attributed to malabsorption and dehydration. Loss may occur abruptly in acute viral infections or responses, or progressively in parasite illnesses. Additional findings encompass diminished skin turgor, desiccated mucous membranes, tachycardia, hypotension, diarrhea, stomach discomfort and soreness, hyperactive bowel noises, nausea, vomiting, fever, and malaise.
Leukemia
Acute leukemia results in progressive weight loss, intense fatigue, elevated fever, swollen and bleeding gums, and a propensity for bleeding. Dyspnea, tachycardia, palpitations, and abdominal or osseous pain may manifest. As the condition advances, neurological symptoms may ultimately manifest. Chronic leukemia, which develops gradually in adults, results in progressive weight loss accompanied by malaise, weariness, pallor, splenomegaly, bleeding tendencies, anemia, dermatological eruptions, anorexia, and fever.
Lymphoma
Hodgkin's disease and non-Hodgkin's lymphoma result in progressive weight loss. Accompanying symptoms include of fever, tiredness, night sweats, malaise, hepatosplenomegaly, and lymphadenopathy. Scaly rashes and itching may occur. Pulmonary tuberculosis. Pulmonary tuberculosis results in progressive weight loss, accompanied by weariness, weakness, anorexia, nocturnal diaphoresis, and low-grade fever. Additional clinical manifestations encompass a cough accompanied by hemoptysis or mucopurulent sputum, dyspnea, and pleuritic chest discomfort. Examination may indicate dullness on percussion, crackles post-coughing, heightened tactile fremitus, and amphoric breath noises. Stomatitis. Stomatitis, characterized by inflammation of the oral mucosa (often red, puffy, and ulcerated), leads to weight loss due to reduced food intake. Related symptoms encompass fever, heightened salivation, lethargy, oral pain, anorexia, and swollen, hemorrhaging gums.
Thyrotoxicosis
Thyrotoxicosis results in heightened metabolism, leading to weight loss. Additional distinctive signs and symptoms encompass anxiety, heat intolerance, diarrhea, heightened appetite, palpitations, tachycardia, diaphoresis, fine tremors, and potentially an enlarged thyroid and exophthalmos. A gallop rhythm may be audible in the ventricles or atria. Alternative Causes Pharmaceuticals. Amphetamines and improper dosages of thyroid medications can result in weight reduction. Abuse of laxatives can induce a malabsorptive condition resulting in weight loss. Chemotherapeutic drugs induce stomatitis or nausea and vomiting, which, when pronounced, results in weight loss.
Refer your patient for psychological treatment if weight loss adversely impacts his body image. In cases of chronic disease, provide hyperalimentation or tube feedings to sustain nutrition and avert edema, impaired healing, and muscular atrophy. Monitor daily caloric intake and conduct weekly weigh-ins. Seek the expertise of a nutritionist to establish a suitable diet and nutritional supplements that provide sufficient caloric intake.
Offer advice on an appropriate diet and maintaining a food journal. Educate the patient on proper oral hygiene practices. Facilitate a referral to psychological counseling, if deemed suitable.
In babies, weight loss may result from failure-to-thrive syndrome. In pediatric patients, significant weight loss may serve as the initial manifestation of diabetes mellitus. Chronic, progressive weight loss occurs in children with marasmus, a kind of non-edematous protein-calorie malnutrition. Weight loss may also arise from child abuse or neglect, an infection leading to high fevers, hand-foot-and-mouth disease which induces painful oral lesions, a gastrointestinal disorder producing vomiting and diarrhea, or celiac disease.
Certain older people undergo slow, modest weight loss attributed to alterations in body composition, including reductions in height and lean body mass, as well as a diminished basal metabolic rate, resulting in lowered energy needs. Unintentional rapid weight loss is a strong predictor of morbidity and mortality in the elderly. Additional non-disease factors contributing to weight loss in this demographic encompass dental loss, challenges in mastication, and social seclusion. Alcoholism can also result in weight loss.
Weight loss may indicate reduced food consumption, diminished nutrient absorption, heightened metabolic demands, or a combination thereof. The reasons encompass endocrine, neoplastic, gastrointestinal, and psychiatric illnesses; nutritional inadequacies; infections; and neurological lesions that result in paralysis and dysphagia. Weight loss may occur due to factors that inhibit adequate food consumption, including painful oral lesions, poorly fitting dentures, and tooth loss. The cause may be the metabolic impact of poverty, restrictive diets, excessive physical activity, or specific medications. Weight loss may manifest as a delayed symptom in chronic conditions such as heart failure and renal illness. In certain disorders, however, it is a consequence of anorexia.
Medical History and Physical Assessment
Commence with a comprehensive dietary history, as weight loss is typically attributable to insufficient caloric consumption. Investigate the reasons for the patient's inadequate dietary intake. Inquire about his prior weight and whether the recent reduction was deliberate. Remain vigilant for lifestyle or occupational alterations that could contribute to anxiety or despair. Has he become separated or divorced? Has a relative or acquaintance lately passed away? Has he lately transitioned to a new position? Investigate recent alterations in bowel habits, including diarrhea or voluminous, buoyant feces. Has the patient had nausea, vomiting, or abdominal pain, which may suggest a gastrointestinal disorder? Has he experienced polydipsia, polyuria, or heat intolerance, which may indicate an endocrine disorder? Conduct a meticulous drug history, paying particular attention to the usage of diet medications and laxatives. Meticulously assess the patient's height and weight, and inquire about his prior weight. Assess his vital signs and document his overall appearance: Is he adequately nourished? Do his garments fit properly? Is muscular atrophy apparent? Inquire about specific weight fluctuations, including approximate dates. Subsequently, assess the patient's skin for turgor and irregular pigmentation, particularly in the vicinity of the joints. Does he exhibit pallor or jaundice? Inspect his oral cavity, assessing the state of his teeth or dentures. Examine for indications of infection or irritation on the palatal surface, and observe any hyperpigmentation of the buccal mucosa.
Additionally, examine the patient’s eyes for exophthalmos and inspect the neck for edema; assess the lungs for abnormal sounds. Examine the abdomen for indications of wasting, and palpate for lumps, discomfort, and hepatomegaly. Standard laboratory and radiologic assessments, including complete blood count, serum albumin levels, urinalysis, chest X-ray, and upper gastrointestinal series, typically elucidate the etiology. Nearly all physical etiologies are clinically apparent during the initial assessment. Cancer, gastrointestinal problems, and depression are the predominant pathological reasons.
Etiological Factors
Adrenal insufficiency. Adrenal insufficiency results in weight loss, accompanied by anorexia, weakness, exhaustion, irritability, syncope, nausea, vomiting, stomach discomfort, and either diarrhea or constipation. Hyperpigmentation may manifest at the joints, belt line, palmar wrinkles, lips, gums, tongue, and buccal mucosa.
Anorexia nervosa
Anorexia nervosa is a psychogenic condition predominantly affecting young women, defined by significant self-induced weight loss of 10% to 50% of premorbid weight, which is generally within the normal range or no more than 5 lb (2.3 kg) above optimal weight. Associated observations encompass skeletal muscle atrophy, reduction of adipose tissue, hypotension, constipation, dental cavities, increased vulnerability to infections, mottled or pallid skin, cold sensitivity, hirsutism on the face and body, alopecia or scalp hair loss, and amenorrhea. The patient typically exhibits hyperactivity and energy, along with an intense dread of weight gain. Self-induced vomiting or the use of laxatives or diuretics may result in dehydration or metabolic alkalosis or acidosis.
Oncology
Weight loss frequently indicates the presence of cancer. Additional results indicate the nature, location, and stage of the tumor, which may encompass fatigue, pain, nausea, vomiting, anorexia, irregular bleeding, and a palpable lump.
Crohn's disease
Weight loss is associated with persistent cramping, stomach discomfort, and anorexia. Additional signs and symptoms encompass diarrhea, nausea, fever, tachycardia, abdominal soreness and guarding, hyperactive bowel noises, abdominal distension, and pain. Perianal lesions and a discernible lump in the right or left lower quadrant may also be evident.
Cryptosporidiosis
Weight loss may ensue from cryptosporidiosis, an opportunistic protozoan infection. Additional results encompass abundant watery diarrhea, stomach cramping, flatulence, anorexia, lethargy, fever, nausea, vomiting, and myalgia.
Depression
Severe depression may result in weight loss or weight gain, accompanied by insomnia or hypersomnia, anorexia, apathy, exhaustion, and feelings of worthlessness. Indecision, lack of coherence, and suicidal ideation or actions may also manifest.
Diabetes mellitus
Weight loss can occur in diabetes mellitus, even with heightened hunger. Additional findings encompass polydipsia, asthenia, tiredness, and polyuria accompanied by nocturia.
Esophagitis
Inflammation of the esophagus causes discomfort, resulting in a temporary cessation of eating and consequent weight reduction. Severe oral and anterior chest discomfort is accompanied by hypersalivation, dysphagia, tachypnea, and hematemesis. Should a stricture occur, dysphagia and weight loss will reemerge.
Gastroenteritis
Weight loss in gastroenteritis is attributed to malabsorption and dehydration. Loss may occur abruptly in acute viral infections or responses, or progressively in parasite illnesses. Additional findings encompass diminished skin turgor, desiccated mucous membranes, tachycardia, hypotension, diarrhea, stomach discomfort and soreness, hyperactive bowel noises, nausea, vomiting, fever, and malaise.
Leukemia
Acute leukemia results in progressive weight loss, intense fatigue, elevated fever, swollen and bleeding gums, and a propensity for bleeding. Dyspnea, tachycardia, palpitations, and abdominal or osseous pain may manifest. As the condition advances, neurological symptoms may ultimately manifest. Chronic leukemia, which develops gradually in adults, results in progressive weight loss accompanied by malaise, weariness, pallor, splenomegaly, bleeding tendencies, anemia, dermatological eruptions, anorexia, and fever.
Lymphoma
Hodgkin's disease and non-Hodgkin's lymphoma result in progressive weight loss. Accompanying symptoms include of fever, tiredness, night sweats, malaise, hepatosplenomegaly, and lymphadenopathy. Scaly rashes and itching may occur. Pulmonary tuberculosis. Pulmonary tuberculosis results in progressive weight loss, accompanied by weariness, weakness, anorexia, nocturnal diaphoresis, and low-grade fever. Additional clinical manifestations encompass a cough accompanied by hemoptysis or mucopurulent sputum, dyspnea, and pleuritic chest discomfort. Examination may indicate dullness on percussion, crackles post-coughing, heightened tactile fremitus, and amphoric breath noises. Stomatitis. Stomatitis, characterized by inflammation of the oral mucosa (often red, puffy, and ulcerated), leads to weight loss due to reduced food intake. Related symptoms encompass fever, heightened salivation, lethargy, oral pain, anorexia, and swollen, hemorrhaging gums.
Thyrotoxicosis
Thyrotoxicosis results in heightened metabolism, leading to weight loss. Additional distinctive signs and symptoms encompass anxiety, heat intolerance, diarrhea, heightened appetite, palpitations, tachycardia, diaphoresis, fine tremors, and potentially an enlarged thyroid and exophthalmos. A gallop rhythm may be audible in the ventricles or atria. Alternative Causes Pharmaceuticals. Amphetamines and improper dosages of thyroid medications can result in weight reduction. Abuse of laxatives can induce a malabsorptive condition resulting in weight loss. Chemotherapeutic drugs induce stomatitis or nausea and vomiting, which, when pronounced, results in weight loss.
Refer your patient for psychological treatment if weight loss adversely impacts his body image. In cases of chronic disease, provide hyperalimentation or tube feedings to sustain nutrition and avert edema, impaired healing, and muscular atrophy. Monitor daily caloric intake and conduct weekly weigh-ins. Seek the expertise of a nutritionist to establish a suitable diet and nutritional supplements that provide sufficient caloric intake.
Offer advice on an appropriate diet and maintaining a food journal. Educate the patient on proper oral hygiene practices. Facilitate a referral to psychological counseling, if deemed suitable.
In babies, weight loss may result from failure-to-thrive syndrome. In pediatric patients, significant weight loss may serve as the initial manifestation of diabetes mellitus. Chronic, progressive weight loss occurs in children with marasmus, a kind of non-edematous protein-calorie malnutrition. Weight loss may also arise from child abuse or neglect, an infection leading to high fevers, hand-foot-and-mouth disease which induces painful oral lesions, a gastrointestinal disorder producing vomiting and diarrhea, or celiac disease.
Certain older people undergo slow, modest weight loss attributed to alterations in body composition, including reductions in height and lean body mass, as well as a diminished basal metabolic rate, resulting in lowered energy needs. Unintentional rapid weight loss is a strong predictor of morbidity and mortality in the elderly. Additional non-disease factors contributing to weight loss in this demographic encompass dental loss, challenges in mastication, and social seclusion. Alcoholism can also result in weight loss.

- Published on
Medical Terms – Aaron’s Sign
Aaron's Sign- Chest or abdominal pain (precordial or epigastric) provoked by the application of moderate yet progressively increasing pressure on McBurney’s point. A positive indicator signifies appendicitis.
Aaron's Sign- Chest or abdominal pain (precordial or epigastric) provoked by the application of moderate yet progressively increasing pressure on McBurney’s point. A positive indicator signifies appendicitis.

- Published on
Symptoms and Signs – Differential Diagnosis of wheezing /Sibilant rhonchi Wheezes are abnormal respiratory noises characterized by a high-pitched, melodic, squealing, creaking, or moaning nature. They result from air moving at high velocity via a constricted airway. When originating in the major airways, they can be detected by pressing an unassisted ear against the chest wall or at the mouth. When originating in smaller airways, they can be detected by placing a stethoscope on the anterior or posterior chest. In contrast to crackles and rhonchi, wheezes cannot be alleviated by coughing. Prolonged wheezing typically occurs on expiration when the bronchi are constricted and narrowed.
Factors contributing to airway constriction encompass bronchospasm; mucosal hypertrophy or edema; partial obstruction due to a neoplasm, foreign object, or secretions; and external compression, as shown in tension pneumothorax or goiter. Wheezing occurs upon inspiration due to airway blockage.
URGENT INTERVENTIONS
Assess the severity of the patient's respiratory distress. Is he attentive? Is he agitated, perplexed, apprehensive, or fearful? Are his respirations excessively rapid, sluggish, superficial, or profound? Are they anomalous? Is wheezing audible through his mouth? Does he demonstrate heightened utilization of accessory muscles; augmented chest wall movement; intercostal, suprasternal, or supraclavicular retractions; stridor; or nasal flaring?
Assess his other vital signs, observing for hypotension or hypertension, as well as diminished oxygen saturation or an irregular, weak, fast, or bradycardic pulse. Assist the patient in achieving relaxation, provide humidified oxygen via face mask, and promote slow, deep breathing. Ensure that endotracheal intubation and emergency resuscitation equipment are readily accessible. Contact the respiratory therapy department to provide intermittent positive pressure ventilation and nebulization treatments with bronchodilators. Establish an intravenous line for the administration of medications, including diuretics, steroids, bronchodilators, and sedatives. Execute the abdominal thrust procedure as indicated for airway blockage.
Medical History and Physical Assessment
In the absence of respiratory distress, gather the patient's history. What triggers his wheezing? Does he suffer from asthma or allergies? Does he smoke or possess a history of pulmonary, cardiac, or circulatory disorders? Is he diagnosed with cancer? Inquire about recent surgical procedures, illnesses, traumas, or alterations in appetite, weight, exercise tolerance, or sleep patterns. Acquire a pharmacological history. Inquire regarding exposure to toxic vapors or any respiratory irritants. Inquire about the characteristics of the cough, including its sound, onset, and frequency. Does he experience bouts of coughing? Is his cough dry, productive of sputum, or hemorrhagic? Inquire with the patient regarding any chest pain experienced. If he experiences pain, evaluate its quality, onset, duration, intensity, and radiation. Does it intensify with breathing, coughing, or specific positions? Examine the patient’s nose and mouth for congestion, discharge, or signs of infection, such as halitosis. If he produces sputum, collect a sample for examination. Check for cyanosis, pallor, clamminess, lumps, tenderness, swelling, distended jugular veins, and swollen lymph nodes. Inspect his chest for aberrant structure and asymmetrical motion, and determine if the trachea is midline.
Percuss for dullness or hyperresonance, and auscultate for crackles, rhonchi, or pleural friction rubs. Note absent or hypoactive breath sounds, aberrant heart sounds, gallops, or murmurs. Also, note arrhythmias, bradycardia, or tachycardia.
Medical Causes
Anaphylaxis
Anaphylaxis is an allergic reaction that can produce tracheal edema or bronchospasm, resulting in severe wheezing and stridor. Initial signs and symptoms include panic, weakness, sneezing, dyspnea, nasal pruritus, urticaria, erythema, and angioedema. Respiratory distress manifests with nasal flaring, utilization of accessory muscles, and intercostal retractions. Additional findings encompass nasal edema and congestion; abundant, watery rhinorrhea; chest or throat constriction; and dysphagia.
Cardiac consequences encompass arrhythmias and hypotension.
Inhalation of a foreign object. Partial obstruction due to a foreign body results in abrupt wheezing and perhaps stridor; a dry, intermittent cough; choking; and hoarseness. Additional findings encompass tachycardia, dyspnea, diminished breath sounds, and even cyanosis. A retained foreign body can induce inflammation, resulting in fever, discomfort, and edema.
Aspiration pneumonitis
Aspiration pneumonitis may present with wheezing, tachypnea, pronounced dyspnea, cyanosis, tachycardia, fever, a productive (finally purulent) cough, and pink, frothy sputum.
Asthma
Wheezing is a primary and fundamental indicator of asthma. It is audible at the orifice during exhalation. A dry cough initially progresses to a productive cough with thick mucus. Additional findings encompass apprehension, extended expiration, intercostal and supraclavicular retractions, rhonchi, utilization of accessory muscles, nasal flaring, and tachypnea. Asthma also induces tachycardia, diaphoresis, and flushing or cyanosis.
Blast lung damage
An acute development of wheezing is a common symptom of respiratory distress after blast lung injury. Associated respiratory findings include dyspnea, hemoptysis, cough, tachypnea, hypoxia, apnea, cyanosis, decreased breath sounds, and hemodynamic instability. Treatment is based on the nature of the explosion, the environment in which it occurred, and any chemical or biological substances involved.
EXAMINATION TIP
Evaluating Breath Sounds Diminished or missing breath sounds suggest some interference with airflow. If pus, fluid, or air fills the pleural space, breath sounds will be quieter than normal. In the event that a foreign object or secretions obstruct a bronchus, breath sounds will be reduced or nonexistent in the distal lung tissue. Enhanced chest wall thickness, as observed in obese or highly muscular patients, may result in diminished, distant, or inaudible breath sounds. Absent breath sounds generally signify a lack of ventilatory capacity. Adventitious breath sounds will be audible when air traverses constricted airways, encounters moisture, or when the membranes lining the thoracic cavity become irritated. These consist of crackles, rhonchi, wheezes, and pleural friction rubs. Typically, these noises signify pulmonary illness. Adhere to the auscultation sequences demonstrated to evaluate the patient's respiratory sounds. Instruct the patient to take full, deep breaths and assess the sound variances between each side. Document the location, time, and nature of any atypical respiratory sounds. Bronchial adenoma. Bronchial adenoma, a covert condition, results in unilateral, potentially severe wheeze. Chronic cough and recurrent hemoptysis are prevalent characteristics. Symptoms of airway blockage may manifest subsequently.
Bronchiectasis
Excessive mucus frequently results in intermittent and localized or diffuse wheeze. A profuse, malodorous, mucopurulent cough is characteristic. It is accompanied by hemoptysis, rhonchi, and gritty crackles. Weight reduction, weariness, debilitation, exertional dyspnea, pyrexia, malaise, halitosis, and advanced clubbing may also manifest.
Chronic bronchitis
Bronchitis induces wheezing that fluctuates in degree, location, and intensity. Accompanying observations consist of extended expiration, coarse crackles, dispersed rhonchi, and a dry cough that subsequently turns productive. Additional consequences encompass dyspnea, utilization of accessory muscles, barrel chest, tachypnea, clubbing, edema, weight gain, and cyanosis.
Bronchogenic carcinoma
Obstruction may result in localized wheezing. Common manifestations encompass a productive cough, dyspnea, hemoptysis (first blood-streaked sputum, potentially progressing to significant bleeding), anorexia, and weight reduction. Edema of the upper extremities and thoracic discomfort may also manifest.
Emphysema
Emphysema, a kind of chronic obstructive lung disease, may result in mild to moderate wheezing. Associated findings encompass dyspnea, malaise, tachypnea, reduced breath sounds, peripheral cyanosis, pursed-lip breathing, anorexia, and malaise. Accessory muscle utilization, barrel chest, a persistent productive cough, and digital clubbing may also manifest.
Coccidioidomycosis of the lungs
Pulmonary coccidioidomycosis can induce wheezing and rhonchi, accompanied by cough, fever, chills, pleuritic chest discomfort, headache, weakness, malaise, anorexia, and macular rash.
Pulmonary edema
Wheezing may manifest in pulmonary edema, a critical condition. Additional signs and symptoms encompass coughing, exertional dyspnea, paroxysmal nocturnal dyspnea, and subsequently, orthopnea. The examination indicates tachycardia, tachypnea, dependent crackles, and a diastolic gallop. Severe pulmonary edema results in rapid, laborious breathing; widespread crackles; a productive cough with frothy, bloody sputum; arrhythmias; cold, clammy, cyanotic skin; hypotension; and a thready pulse.
Respiratory syncytial virus (RSV)
Wheezing commonly accompanies RSV bronchiolitis, an illness of the lower respiratory tract frequently observed in children under one year of age. Additional acute respiratory symptoms encompass apnea, coughing, tachypnea, nasal flaring, fever, and chest retractions. The majority of youngsters recuperate from RSV infection within 8 to 15 days without complications. Premature newborns and those with preexisting respiratory, cardiac, neuromuscular, and immunological disorders necessitate special attention.
Tracheobronchitis
Auscultation may reveal wheezing, rhonchi, and crackles. The patient presents with a cough, mild fever, abrupt chills, myalgia, and substernal discomfort.
Wegener's granulomatosis
Wegener’s granulomatosis can induce mild to moderate wheeze if it compresses the principal airways. Additional findings encompass a cough (potentially sanguineous), dyspnea, pleuritic thoracic discomfort, hemorrhagic cutaneous lesions, and advancing renal insufficiency. Epistaxis and acute sinusitis are prevalent.
Prepare the patient for diagnostic evaluations, including chest X-rays, arterial blood gas analysis, pulmonary function assessments, and sputum cultures. Facilitate the patient's respiration by situating him in a semi-Fowler's stance and constantly adjusting his position. Administer pulmonary physiotherapy as required. Administer an antibiotic to address infection, a bronchodilator to alleviate bronchospasm and ensure airway patency, a steroid to diminish inflammation, and a mucolytic or expectorant to enhance secretion flow. Administer humidification to facilitate the thinning of secretions.
Furnish the patient with information regarding his prescribed medications, and elucidate methods to enhance drainage and avert the accumulation of secretions, if necessary. Additionally, elucidate deep breathing and coughing procedures, as well as the need of augmenting fluid consumption.
Children are particularly vulnerable to wheezing due to their narrow airways, which facilitate fast occlusion. The principal causes of wheezing include bronchospasm, mucosal edema, and secretion buildup. These may manifest in conditions such as cystic fibrosis, foreign body aspiration, acute bronchiolitis, and pulmonary hemosiderosis.
Factors contributing to airway constriction encompass bronchospasm; mucosal hypertrophy or edema; partial obstruction due to a neoplasm, foreign object, or secretions; and external compression, as shown in tension pneumothorax or goiter. Wheezing occurs upon inspiration due to airway blockage.
URGENT INTERVENTIONS
Assess the severity of the patient's respiratory distress. Is he attentive? Is he agitated, perplexed, apprehensive, or fearful? Are his respirations excessively rapid, sluggish, superficial, or profound? Are they anomalous? Is wheezing audible through his mouth? Does he demonstrate heightened utilization of accessory muscles; augmented chest wall movement; intercostal, suprasternal, or supraclavicular retractions; stridor; or nasal flaring?
Assess his other vital signs, observing for hypotension or hypertension, as well as diminished oxygen saturation or an irregular, weak, fast, or bradycardic pulse. Assist the patient in achieving relaxation, provide humidified oxygen via face mask, and promote slow, deep breathing. Ensure that endotracheal intubation and emergency resuscitation equipment are readily accessible. Contact the respiratory therapy department to provide intermittent positive pressure ventilation and nebulization treatments with bronchodilators. Establish an intravenous line for the administration of medications, including diuretics, steroids, bronchodilators, and sedatives. Execute the abdominal thrust procedure as indicated for airway blockage.
Medical History and Physical Assessment
In the absence of respiratory distress, gather the patient's history. What triggers his wheezing? Does he suffer from asthma or allergies? Does he smoke or possess a history of pulmonary, cardiac, or circulatory disorders? Is he diagnosed with cancer? Inquire about recent surgical procedures, illnesses, traumas, or alterations in appetite, weight, exercise tolerance, or sleep patterns. Acquire a pharmacological history. Inquire regarding exposure to toxic vapors or any respiratory irritants. Inquire about the characteristics of the cough, including its sound, onset, and frequency. Does he experience bouts of coughing? Is his cough dry, productive of sputum, or hemorrhagic? Inquire with the patient regarding any chest pain experienced. If he experiences pain, evaluate its quality, onset, duration, intensity, and radiation. Does it intensify with breathing, coughing, or specific positions? Examine the patient’s nose and mouth for congestion, discharge, or signs of infection, such as halitosis. If he produces sputum, collect a sample for examination. Check for cyanosis, pallor, clamminess, lumps, tenderness, swelling, distended jugular veins, and swollen lymph nodes. Inspect his chest for aberrant structure and asymmetrical motion, and determine if the trachea is midline.
Percuss for dullness or hyperresonance, and auscultate for crackles, rhonchi, or pleural friction rubs. Note absent or hypoactive breath sounds, aberrant heart sounds, gallops, or murmurs. Also, note arrhythmias, bradycardia, or tachycardia.
Medical Causes
Anaphylaxis
Anaphylaxis is an allergic reaction that can produce tracheal edema or bronchospasm, resulting in severe wheezing and stridor. Initial signs and symptoms include panic, weakness, sneezing, dyspnea, nasal pruritus, urticaria, erythema, and angioedema. Respiratory distress manifests with nasal flaring, utilization of accessory muscles, and intercostal retractions. Additional findings encompass nasal edema and congestion; abundant, watery rhinorrhea; chest or throat constriction; and dysphagia.
Cardiac consequences encompass arrhythmias and hypotension.
Inhalation of a foreign object. Partial obstruction due to a foreign body results in abrupt wheezing and perhaps stridor; a dry, intermittent cough; choking; and hoarseness. Additional findings encompass tachycardia, dyspnea, diminished breath sounds, and even cyanosis. A retained foreign body can induce inflammation, resulting in fever, discomfort, and edema.
Aspiration pneumonitis
Aspiration pneumonitis may present with wheezing, tachypnea, pronounced dyspnea, cyanosis, tachycardia, fever, a productive (finally purulent) cough, and pink, frothy sputum.
Asthma
Wheezing is a primary and fundamental indicator of asthma. It is audible at the orifice during exhalation. A dry cough initially progresses to a productive cough with thick mucus. Additional findings encompass apprehension, extended expiration, intercostal and supraclavicular retractions, rhonchi, utilization of accessory muscles, nasal flaring, and tachypnea. Asthma also induces tachycardia, diaphoresis, and flushing or cyanosis.
Blast lung damage
An acute development of wheezing is a common symptom of respiratory distress after blast lung injury. Associated respiratory findings include dyspnea, hemoptysis, cough, tachypnea, hypoxia, apnea, cyanosis, decreased breath sounds, and hemodynamic instability. Treatment is based on the nature of the explosion, the environment in which it occurred, and any chemical or biological substances involved.
EXAMINATION TIP
Evaluating Breath Sounds Diminished or missing breath sounds suggest some interference with airflow. If pus, fluid, or air fills the pleural space, breath sounds will be quieter than normal. In the event that a foreign object or secretions obstruct a bronchus, breath sounds will be reduced or nonexistent in the distal lung tissue. Enhanced chest wall thickness, as observed in obese or highly muscular patients, may result in diminished, distant, or inaudible breath sounds. Absent breath sounds generally signify a lack of ventilatory capacity. Adventitious breath sounds will be audible when air traverses constricted airways, encounters moisture, or when the membranes lining the thoracic cavity become irritated. These consist of crackles, rhonchi, wheezes, and pleural friction rubs. Typically, these noises signify pulmonary illness. Adhere to the auscultation sequences demonstrated to evaluate the patient's respiratory sounds. Instruct the patient to take full, deep breaths and assess the sound variances between each side. Document the location, time, and nature of any atypical respiratory sounds. Bronchial adenoma. Bronchial adenoma, a covert condition, results in unilateral, potentially severe wheeze. Chronic cough and recurrent hemoptysis are prevalent characteristics. Symptoms of airway blockage may manifest subsequently.
Bronchiectasis
Excessive mucus frequently results in intermittent and localized or diffuse wheeze. A profuse, malodorous, mucopurulent cough is characteristic. It is accompanied by hemoptysis, rhonchi, and gritty crackles. Weight reduction, weariness, debilitation, exertional dyspnea, pyrexia, malaise, halitosis, and advanced clubbing may also manifest.
Chronic bronchitis
Bronchitis induces wheezing that fluctuates in degree, location, and intensity. Accompanying observations consist of extended expiration, coarse crackles, dispersed rhonchi, and a dry cough that subsequently turns productive. Additional consequences encompass dyspnea, utilization of accessory muscles, barrel chest, tachypnea, clubbing, edema, weight gain, and cyanosis.
Bronchogenic carcinoma
Obstruction may result in localized wheezing. Common manifestations encompass a productive cough, dyspnea, hemoptysis (first blood-streaked sputum, potentially progressing to significant bleeding), anorexia, and weight reduction. Edema of the upper extremities and thoracic discomfort may also manifest.
Emphysema
Emphysema, a kind of chronic obstructive lung disease, may result in mild to moderate wheezing. Associated findings encompass dyspnea, malaise, tachypnea, reduced breath sounds, peripheral cyanosis, pursed-lip breathing, anorexia, and malaise. Accessory muscle utilization, barrel chest, a persistent productive cough, and digital clubbing may also manifest.
Coccidioidomycosis of the lungs
Pulmonary coccidioidomycosis can induce wheezing and rhonchi, accompanied by cough, fever, chills, pleuritic chest discomfort, headache, weakness, malaise, anorexia, and macular rash.
Pulmonary edema
Wheezing may manifest in pulmonary edema, a critical condition. Additional signs and symptoms encompass coughing, exertional dyspnea, paroxysmal nocturnal dyspnea, and subsequently, orthopnea. The examination indicates tachycardia, tachypnea, dependent crackles, and a diastolic gallop. Severe pulmonary edema results in rapid, laborious breathing; widespread crackles; a productive cough with frothy, bloody sputum; arrhythmias; cold, clammy, cyanotic skin; hypotension; and a thready pulse.
Respiratory syncytial virus (RSV)
Wheezing commonly accompanies RSV bronchiolitis, an illness of the lower respiratory tract frequently observed in children under one year of age. Additional acute respiratory symptoms encompass apnea, coughing, tachypnea, nasal flaring, fever, and chest retractions. The majority of youngsters recuperate from RSV infection within 8 to 15 days without complications. Premature newborns and those with preexisting respiratory, cardiac, neuromuscular, and immunological disorders necessitate special attention.
Tracheobronchitis
Auscultation may reveal wheezing, rhonchi, and crackles. The patient presents with a cough, mild fever, abrupt chills, myalgia, and substernal discomfort.
Wegener's granulomatosis
Wegener’s granulomatosis can induce mild to moderate wheeze if it compresses the principal airways. Additional findings encompass a cough (potentially sanguineous), dyspnea, pleuritic thoracic discomfort, hemorrhagic cutaneous lesions, and advancing renal insufficiency. Epistaxis and acute sinusitis are prevalent.
Prepare the patient for diagnostic evaluations, including chest X-rays, arterial blood gas analysis, pulmonary function assessments, and sputum cultures. Facilitate the patient's respiration by situating him in a semi-Fowler's stance and constantly adjusting his position. Administer pulmonary physiotherapy as required. Administer an antibiotic to address infection, a bronchodilator to alleviate bronchospasm and ensure airway patency, a steroid to diminish inflammation, and a mucolytic or expectorant to enhance secretion flow. Administer humidification to facilitate the thinning of secretions.
Furnish the patient with information regarding his prescribed medications, and elucidate methods to enhance drainage and avert the accumulation of secretions, if necessary. Additionally, elucidate deep breathing and coughing procedures, as well as the need of augmenting fluid consumption.
Children are particularly vulnerable to wheezing due to their narrow airways, which facilitate fast occlusion. The principal causes of wheezing include bronchospasm, mucosal edema, and secretion buildup. These may manifest in conditions such as cystic fibrosis, foreign body aspiration, acute bronchiolitis, and pulmonary hemosiderosis.

- Published on
Symptoms and Signs – Differential Diagnosis of Excessive Weight Gain
Weight gain transpires when caloric intake surpasses the body's energy needs, resulting in augmented adipose tissue accumulation. It may also arise when fluid retention leads to edema. Weight gain due to overeating may primarily stem from emotional issues, particularly worry, guilt, and despair, as well as social influences. In the elderly, weight gain typically indicates a prolonged caloric intake despite the normal, gradual decline in basal metabolic rate. Women experience steady weight growth during pregnancy, while periodic weight gain typically happens during menstruation. Weight gain, a primary indicator of numerous endocrine illnesses, also manifests in conditions that restrict activity, particularly cardiovascular and pulmonary disorders. This may also arise from pharmacological treatments that enhance hunger or induce fluid retention, as well as from cardiovascular, hepatic, and renal conditions that lead to edema.
Medical History and Physical Assessment
Ascertain your patient's historical tendencies of weight fluctuation. Is there a familial history of obesity, thyroid disorders, or diabetes mellitus? Evaluate his dietary and exercise habits. Has his appetite augmented? Does he engage in regular exercise or any exercise at all? Subsequently, inquire about concomitant symptoms. Has he encountered visual abnormalities, dysphonia, paresthesia, or heightened urination and thirst? Has he developed impotence? If the patient is female, has she encountered menstrual irregularities or experienced weight gain during her monthly cycle? Assess the patient's mental condition. Is he experiencing anxiety or depression? Does he exhibit a delayed response? Is his recollection deficient? Which drugs is he now utilizing? During the physical examination, assess skinfold thickness to estimate adipose reserves.
Observe fat distribution, the existence of localized or generalized edema, and overall nutritional status. Examine for further anomalies, including irregular body hair distribution, alopecia, and xerosis. Obtain and document the patient's vital signs.
Etiological Factors
Acromegaly
Acromegaly induces considerable weight gain. Additional findings encompass coarse facial characteristics, prognathism, swollen extremities, hyperhidrosis, seborrheic skin, deepened voice, back and joint discomfort, lethargy, somnolence, and heat sensitivity. Hirsutism may occasionally manifest.
Diabetes mellitus
The heightened appetite linked to diabetes mellitus may result in weight gain, although weight loss may occasionally occur instead. Additional findings encompass weariness, polydipsia, polyuria, nocturia, weakness, polyphagia, and somnolence. Hypercortisolism. Significant weight accumulation, typically localized to the torso and the nape of the neck (buffalo hump), is a hallmark of this condition. Additional cushingoid characteristics encompass slender extremities, a rounded moon face, muscular weakness, purple striae, emotional lability, and heightened vulnerability to infections. Gynecomastia can manifest in males; hirsutism, acne, and monthly irregularities may manifest in females.
Hyperinsulinemia
Hyperinsulinism elevates appetite, resulting in weight gain. Emotional lability, dyspepsia, asthenia, diaphoresis, tachycardia, visual abnormalities, and syncope are also present.
Hypogonadism
Weight gain is prevalent with hypogonadism. Prepubertal hypogonadism results in eunuchoid body proportions, characterized by comparatively sparse face and body hair, as well as a high-pitched voice. Postpubertal hypogonadism results in diminished libido, erectile dysfunction, and infertility.
Dysfunction of the hypothalamus
Conditions like Laurence-Moon-Bardet-Biedl syndrome induce an insatiable appetite leading to weight gain, as well as modifications in body temperature and sleep patterns. Hypothyroidism. In hypothyroidism, weight gain transpires despite starvation. Associated signs and symptoms encompass weariness, cold intolerance, constipation, menorrhagia, diminished intellectual and motor activity, dry, pale, cool skin, dry, thin hair, and thick, brittle nails. Myalgia, dysphonia, diminished deep tendon reflexes, bradycardia, and abdominal distension may manifest. Ultimately, the visage adopts a lackluster demeanor accompanied by periorbital edema.
Assessment of Nutritional Status To evaluate a patient's nutritional condition in cases of significant weight loss or growth, measure skinfold thickness, midarm circumference, and calculate midarm muscle circumference. Skinfold measurements indicate adipose tissue mass, with subcutaneous fat comprising around 50% of the body's total adipose tissue. Midarm measures indicate the mass of both skeletal muscle and fat tissue. Utilize the outlined procedures to obtain these measurements.
Standard anthropometric measurements differ based on the patient's age and sex, as detailed in a chart of normative anthropometric values.
A triceps or subscapular skinfold measurement below 60% of the standard value signifies severe fat reserve depletion, a range between 60% and 90% suggests moderate to mild depletion, and above 90% denotes large fat reserves. A midarm circumference below 90% of the usual value signifies caloric deficiency, whereas a measurement beyond 90% denotes sufficient or abundant muscle and fat. A midarm muscular circumference below 90% signifies protein depletion, while a measurement above 90% denotes sufficient or abundant protein reserves. To assess the triceps skin fold, identify the midway of the patient's upper arm utilizing a non-elastic tape measure. Indicate the middle using a felt-tip pen. Subsequently, pinch the skin with your thumb and forefinger approximately 1 cm above the midpoint. Position the calipers at the middle and apply pressure for approximately 3 seconds. Document the measurement indicated on the handle gauge to the closest 0.5 mm. Obtain two additional readings and calculate the average of all three to mitigate any measurement inaccuracies. To assess the subscapular skin fold, utilize your thumb and forefinger to pinch the skin directly beneath the scapular angle, aligning with the skin's natural cleavage. Utilize the calipers and continue as you would while assessing the triceps skin fold. Subscapular and triceps skinfold measurements are reliable indicators of fat loss or growth during hospitalization. To assess midarm circumference, return to the midpoint previously indicated on the patient's upper arm. Subsequently, employ a tape measure to ascertain the arm circumference at this location. This measurement encompasses both skeletal muscle and adipose tissue mass, aiding in the assessment of protein and caloric reserves. To get midarm muscle circumference, multiply the triceps skinfold thickness (in centimeters) by 3.143, then remove this value from the midarm circumference. Midarm muscular circumference exclusively indicates muscle mass, serving as a more sensitive measure of protein stores.
Metabolic syndrome
Excessive weight gain, especially the accumulation of adipose tissue in the abdominal region or an imbalanced waist-hip ratio (apple shape), constitutes a risk factor for this condition. Additional risk factors encompass hypertension, heightened glucose and insulin concentrations, and irregular cholesterol, triglyceride, and high-density lipoprotein levels. It is estimated that about 50 million individuals in the United States possess metabolic syndrome. Adopting a healthy lifestyle, enhancing dietary habits, reducing weight, and augmenting physical activity are methods to mitigate or postpone the dangers linked to metabolic syndrome.
Nephrotic syndrome
In nephrotic syndrome, weight increase is attributable to edema. In extreme instances, anasarca manifests, resulting in a body weight increase of up to 50%. Associated effects encompass abdominal distension, orthostatic hypotension, and tiredness.
Pancreatic islet cell neoplasm
Pancreatic islet cell tumors induce hyperphagia, resulting in weight gain. Additional observations encompass emotional lability, weakness, malaise, weariness, restlessness, diaphoresis, palpitations, tachycardia, visual abnormalities, and syncope. Preeclampsia. Preeclampsia may present with rapid weight increase (surpassing the typical weight growth during pregnancy), nausea and vomiting, epigastric discomfort, hypertension, and visual disturbances such as blurring or diplopia. Sheehan's syndrome. Sheehan’s syndrome, prevalent in women who have significant obstetric hemorrhage, may result in weight gain.
Additional Causes: Substances
Corticosteroids, phenothiazines, and tricyclic antidepressants induce weight gain due to fluid retention and heightened appetite. Additional medications that may contribute to weight gain encompass hormonal contraceptives, which promote fluid retention; cyproheptadine, which stimulates hunger; and lithium, which can precipitate hypothyroidism.
Psychological treatment may be essential for those experiencing weight gain, especially when it stems from emotional issues or when disproportionate weight distribution affects body image. Exercises for obese patients or those with cardiopulmonary disorders should be strictly monitored. Additional investigation to exclude potential secondary causes should encompass serum thyroid-stimulating hormone assessment and dexamethasone suppression tests. Laboratory test findings for all patients should ideally encompass cardiac risk variables, including serum cholesterol, triglyceride, and glucose levels. Examine the significance of weight management and offer recommendations for suitable physical activity. Furthermore, elucidate the significance of behavior adjustment and adherence to dietary guidelines.
Weight gain in children may be attributed to an endocrine disease, such as hypercortisolism. Additional causes encompass inactivity resulting from Prader-Willi syndrome, Down syndrome, Werdnig-Hoffmann illness, advanced stages of muscular dystrophy, and severe cerebral palsy. Nonpathological factors encompass inadequate dietary practices, inactive leisure activities, and psychological issues, particularly in teens. Irrespective of the reason, dissuade fad diets and offer a comprehensive weight loss regimen. The prevalence of obesity is rising among children. Optimal weights, correlated with minimal mortality rates, rise with age.
Weight gain transpires when caloric intake surpasses the body's energy needs, resulting in augmented adipose tissue accumulation. It may also arise when fluid retention leads to edema. Weight gain due to overeating may primarily stem from emotional issues, particularly worry, guilt, and despair, as well as social influences. In the elderly, weight gain typically indicates a prolonged caloric intake despite the normal, gradual decline in basal metabolic rate. Women experience steady weight growth during pregnancy, while periodic weight gain typically happens during menstruation. Weight gain, a primary indicator of numerous endocrine illnesses, also manifests in conditions that restrict activity, particularly cardiovascular and pulmonary disorders. This may also arise from pharmacological treatments that enhance hunger or induce fluid retention, as well as from cardiovascular, hepatic, and renal conditions that lead to edema.
Medical History and Physical Assessment
Ascertain your patient's historical tendencies of weight fluctuation. Is there a familial history of obesity, thyroid disorders, or diabetes mellitus? Evaluate his dietary and exercise habits. Has his appetite augmented? Does he engage in regular exercise or any exercise at all? Subsequently, inquire about concomitant symptoms. Has he encountered visual abnormalities, dysphonia, paresthesia, or heightened urination and thirst? Has he developed impotence? If the patient is female, has she encountered menstrual irregularities or experienced weight gain during her monthly cycle? Assess the patient's mental condition. Is he experiencing anxiety or depression? Does he exhibit a delayed response? Is his recollection deficient? Which drugs is he now utilizing? During the physical examination, assess skinfold thickness to estimate adipose reserves.
Observe fat distribution, the existence of localized or generalized edema, and overall nutritional status. Examine for further anomalies, including irregular body hair distribution, alopecia, and xerosis. Obtain and document the patient's vital signs.
Etiological Factors
Acromegaly
Acromegaly induces considerable weight gain. Additional findings encompass coarse facial characteristics, prognathism, swollen extremities, hyperhidrosis, seborrheic skin, deepened voice, back and joint discomfort, lethargy, somnolence, and heat sensitivity. Hirsutism may occasionally manifest.
Diabetes mellitus
The heightened appetite linked to diabetes mellitus may result in weight gain, although weight loss may occasionally occur instead. Additional findings encompass weariness, polydipsia, polyuria, nocturia, weakness, polyphagia, and somnolence. Hypercortisolism. Significant weight accumulation, typically localized to the torso and the nape of the neck (buffalo hump), is a hallmark of this condition. Additional cushingoid characteristics encompass slender extremities, a rounded moon face, muscular weakness, purple striae, emotional lability, and heightened vulnerability to infections. Gynecomastia can manifest in males; hirsutism, acne, and monthly irregularities may manifest in females.
Hyperinsulinemia
Hyperinsulinism elevates appetite, resulting in weight gain. Emotional lability, dyspepsia, asthenia, diaphoresis, tachycardia, visual abnormalities, and syncope are also present.
Hypogonadism
Weight gain is prevalent with hypogonadism. Prepubertal hypogonadism results in eunuchoid body proportions, characterized by comparatively sparse face and body hair, as well as a high-pitched voice. Postpubertal hypogonadism results in diminished libido, erectile dysfunction, and infertility.
Dysfunction of the hypothalamus
Conditions like Laurence-Moon-Bardet-Biedl syndrome induce an insatiable appetite leading to weight gain, as well as modifications in body temperature and sleep patterns. Hypothyroidism. In hypothyroidism, weight gain transpires despite starvation. Associated signs and symptoms encompass weariness, cold intolerance, constipation, menorrhagia, diminished intellectual and motor activity, dry, pale, cool skin, dry, thin hair, and thick, brittle nails. Myalgia, dysphonia, diminished deep tendon reflexes, bradycardia, and abdominal distension may manifest. Ultimately, the visage adopts a lackluster demeanor accompanied by periorbital edema.
Assessment of Nutritional Status To evaluate a patient's nutritional condition in cases of significant weight loss or growth, measure skinfold thickness, midarm circumference, and calculate midarm muscle circumference. Skinfold measurements indicate adipose tissue mass, with subcutaneous fat comprising around 50% of the body's total adipose tissue. Midarm measures indicate the mass of both skeletal muscle and fat tissue. Utilize the outlined procedures to obtain these measurements.
Standard anthropometric measurements differ based on the patient's age and sex, as detailed in a chart of normative anthropometric values.
A triceps or subscapular skinfold measurement below 60% of the standard value signifies severe fat reserve depletion, a range between 60% and 90% suggests moderate to mild depletion, and above 90% denotes large fat reserves. A midarm circumference below 90% of the usual value signifies caloric deficiency, whereas a measurement beyond 90% denotes sufficient or abundant muscle and fat. A midarm muscular circumference below 90% signifies protein depletion, while a measurement above 90% denotes sufficient or abundant protein reserves. To assess the triceps skin fold, identify the midway of the patient's upper arm utilizing a non-elastic tape measure. Indicate the middle using a felt-tip pen. Subsequently, pinch the skin with your thumb and forefinger approximately 1 cm above the midpoint. Position the calipers at the middle and apply pressure for approximately 3 seconds. Document the measurement indicated on the handle gauge to the closest 0.5 mm. Obtain two additional readings and calculate the average of all three to mitigate any measurement inaccuracies. To assess the subscapular skin fold, utilize your thumb and forefinger to pinch the skin directly beneath the scapular angle, aligning with the skin's natural cleavage. Utilize the calipers and continue as you would while assessing the triceps skin fold. Subscapular and triceps skinfold measurements are reliable indicators of fat loss or growth during hospitalization. To assess midarm circumference, return to the midpoint previously indicated on the patient's upper arm. Subsequently, employ a tape measure to ascertain the arm circumference at this location. This measurement encompasses both skeletal muscle and adipose tissue mass, aiding in the assessment of protein and caloric reserves. To get midarm muscle circumference, multiply the triceps skinfold thickness (in centimeters) by 3.143, then remove this value from the midarm circumference. Midarm muscular circumference exclusively indicates muscle mass, serving as a more sensitive measure of protein stores.
Metabolic syndrome
Excessive weight gain, especially the accumulation of adipose tissue in the abdominal region or an imbalanced waist-hip ratio (apple shape), constitutes a risk factor for this condition. Additional risk factors encompass hypertension, heightened glucose and insulin concentrations, and irregular cholesterol, triglyceride, and high-density lipoprotein levels. It is estimated that about 50 million individuals in the United States possess metabolic syndrome. Adopting a healthy lifestyle, enhancing dietary habits, reducing weight, and augmenting physical activity are methods to mitigate or postpone the dangers linked to metabolic syndrome.
Nephrotic syndrome
In nephrotic syndrome, weight increase is attributable to edema. In extreme instances, anasarca manifests, resulting in a body weight increase of up to 50%. Associated effects encompass abdominal distension, orthostatic hypotension, and tiredness.
Pancreatic islet cell neoplasm
Pancreatic islet cell tumors induce hyperphagia, resulting in weight gain. Additional observations encompass emotional lability, weakness, malaise, weariness, restlessness, diaphoresis, palpitations, tachycardia, visual abnormalities, and syncope. Preeclampsia. Preeclampsia may present with rapid weight increase (surpassing the typical weight growth during pregnancy), nausea and vomiting, epigastric discomfort, hypertension, and visual disturbances such as blurring or diplopia. Sheehan's syndrome. Sheehan’s syndrome, prevalent in women who have significant obstetric hemorrhage, may result in weight gain.
Additional Causes: Substances
Corticosteroids, phenothiazines, and tricyclic antidepressants induce weight gain due to fluid retention and heightened appetite. Additional medications that may contribute to weight gain encompass hormonal contraceptives, which promote fluid retention; cyproheptadine, which stimulates hunger; and lithium, which can precipitate hypothyroidism.
Psychological treatment may be essential for those experiencing weight gain, especially when it stems from emotional issues or when disproportionate weight distribution affects body image. Exercises for obese patients or those with cardiopulmonary disorders should be strictly monitored. Additional investigation to exclude potential secondary causes should encompass serum thyroid-stimulating hormone assessment and dexamethasone suppression tests. Laboratory test findings for all patients should ideally encompass cardiac risk variables, including serum cholesterol, triglyceride, and glucose levels. Examine the significance of weight management and offer recommendations for suitable physical activity. Furthermore, elucidate the significance of behavior adjustment and adherence to dietary guidelines.
Weight gain in children may be attributed to an endocrine disease, such as hypercortisolism. Additional causes encompass inactivity resulting from Prader-Willi syndrome, Down syndrome, Werdnig-Hoffmann illness, advanced stages of muscular dystrophy, and severe cerebral palsy. Nonpathological factors encompass inadequate dietary practices, inactive leisure activities, and psychological issues, particularly in teens. Irrespective of the reason, dissuade fad diets and offer a comprehensive weight loss regimen. The prevalence of obesity is rising among children. Optimal weights, correlated with minimal mortality rates, rise with age.

- Published on
Symptoms and Signs – Differential Diagnosis of Vulvar Lesions
Vulvar lesions are cutaneous masses, nodules, papules, vesicles, or ulcers arising from benign or malignant tumors, dystrophies, dermatoses, or infections. They may emerge anywhere on the vulva and could remain unnoticed until a gynecological examination. Typically, the patient observes lesions due to accompanying symptoms, like pruritus, dysuria, or dyspareunia.
Medical History and Physical Assessment
Inquire when the patient first observed a vulvar lesion and ascertain any accompanying characteristics, including swelling, pain, tenderness, itching, or discharge. Does she exhibit lesions in other areas of her body? Inquire about the signs and symptoms of systemic illness, including malaise, fever, or rash in other regions of the body. Is the patient engaged in sexual activity? Could she have been exposed to a sexually transmitted infection? Additionally, assess the lesion, conduct a pelvic examination, and get cultures.
Etiological Factors
Basal cell carcinoma
This nodular tumor, prevalent in postmenopausal women, features a central ulcer and a raised, poorly defined border. The tumor is usually asymptomatic but may sometimes induce itching, hemorrhage, discharge, and a burning feeling.
Nonmalignant cysts
Epidermal inclusion cysts, the predominant vulvar cysts, typically manifest on the labia majora and are generally spherical and asymptomatic. They occasionally exhibit erythema and tenderness. Bartholin's duct cysts are often unilateral, tense, nontender, and palpable; they manifest on the posterior labia minora and may induce minor discomfort during intercourse or, when sizable, impede intercourse or even ambulation. Bartholin's abscess, an infection of a Bartholin's duct cyst, results in progressive pain and tenderness, along with potential vulvar enlargement, erythema, and deformity.
Sexually transmitted illnesses are the predominant cause of vulvar lesions in premenopausal women, while vulvar tumors and cysts are the primary lesions in women aged 50 to 70.
Benign tumors of the vulva
Benign vulvar tumors, whether cystic or solid, are typically asymptomatic.
Chancroid
Chancroid, an uncommon sexually transmitted infection, results in painful vulvar sores. Headache, malaise, and a temperature of 102.2°F (39°C) may manifest, accompanied by swollen, painful inguinal lymph nodes.
Genital warts
Genital warts, a sexually transmitted infection, manifest as painless lesions on the vulva, vagina, and cervix. Warts commence as little red or pink protuberances that develop into pedunculated formations. Numerous swellings exhibiting a cauliflower-like morphology are prevalent. Additional findings including pruritus, erythema, and a copious, mucopurulent vaginal discharge. Patients often report experiencing burning or paresthesia in the vaginal introitus.
Gonorrhea
Vulvar lesions, typically localized to Bartholin’s glands, may manifest with pruritus, a burning feeling, discomfort, and a green-yellow vaginal discharge; nevertheless, the majority of patients remain asymptomatic. Additional findings encompass dysuria and urine incontinence; vaginal erythema, edema, hemorrhage, and engorgement; as well as intense pelvic and lower abdominal pain.
Granuloma inguinale
Initially, a solitary painless macule or papule emerges on the vulva, progressing to an ulcerated, elevated, beefy-red lesion with a granular, friable margin. Additional painless and sometimes malodorous lesions may appear on the labia, vagina, or cervix. Infection and pain ensue, leading to the enlargement and potential tenderness of regional lymph nodes. Systemic consequences encompass fever, weight reduction, and malaise.
Genital herpes simplex
Herpes simplex manifests as fluid-filled vesicles on the cervix and perhaps on the vulva, labia, perianal area, vagina, or oral cavity. The vesicles, initially asymptomatic, may rupture and progress into widespread, superficial, painful ulcers, accompanied by erythema, significant edema, and tender inguinal lymphadenopathy. Additional results encompass pyrexia, malaise, and dysuria.
Lymphogranuloma venereum
Individuals with lymphogranuloma venereum, a bacterial infection, typically have a solitary, painless papule or ulcer on the posterior vulva that resolves within a few days. Unilateral, painful, and swollen lymph nodes typically manifest 2 to 6 weeks later. Additional findings including fever, chills, headache, anorexia, myalgias, arthralgias, weight loss, and perineal edema.
Squamous cell carcinoma
Invasive carcinoma predominantly affects postmenopausal women and may manifest as vulvar pruritus, discomfort, and a vulvar mass. As the tumor expands, it may invade the vagina, anus, and urethra, resulting in hemorrhage, discharge, or dysuria. Carcinoma in situ predominantly occurs in premenopausal women, manifesting as a vulvar lesion that may seem white or red, elevated, well-defined, wet, crusty, and solitary.
Hyperplasia of squamous cells
Previously referred to as hyperplastic dystrophy, these vulvar lesions may be distinctly outlined or indistinct; localized or widespread; and exhibit red, brown, white, or a combination of red and white hues. Intense pruritus, maybe accompanied by vulvar pain, severe burning, and dyspareunia, is the primary symptom.
Lichen sclerosus, a kind of vulvar dystrophy, results in vulvar skin exhibiting a parchment-like texture. Fissures may arise between the clitoris and urethra or other vulvar regions.
Syphilis
Chancres, the principal vulvar lesions of syphilis, may manifest on the vulva, vagina, or cervix 10 to 90 days following initial exposure. Typically painless, they commence as papules that subsequently dissolve, exhibiting indurated, elevated margins and transparent bases. Condylomata lata, extremely infectious secondary vulvar lesions, are elevated, gray, flat-topped, and frequently ulcerated. Additional findings encompass a maculopapular, pustular, or nodular rash; cephalalgia; malaise; anorexia; weight reduction; pyrexia; nausea; emesis; widespread lymphadenopathy; and pharyngitis. Systemic viral infection. Varicella, measles, and other systemic viral infections may result in vulvar lesions.
Anticipate the administration of a systemic antibiotic, antiviral, topical corticosteroid, topical testosterone, or an antipruritic.
Sitz baths may enhance the patient's comfort. Deliver guidance about safer sex behaviors.Vulvar lesions in children may arise from congenital syphilis or gonorrhea. Assess for sexual abuse. Vulvar dystrophies and neoplasms have an increased prevalence with advancing age. All vulvar lesions should be presumed malignant until demonstrated otherwise. Additionally, numerous women maintain sexual activity into their later years and may originate from an era when sexually transmitted infections were not openly addressed. These patients should be interrogated regarding sexual activity and instructed on safer sex practices.
Vulvar lesions are cutaneous masses, nodules, papules, vesicles, or ulcers arising from benign or malignant tumors, dystrophies, dermatoses, or infections. They may emerge anywhere on the vulva and could remain unnoticed until a gynecological examination. Typically, the patient observes lesions due to accompanying symptoms, like pruritus, dysuria, or dyspareunia.
Medical History and Physical Assessment
Inquire when the patient first observed a vulvar lesion and ascertain any accompanying characteristics, including swelling, pain, tenderness, itching, or discharge. Does she exhibit lesions in other areas of her body? Inquire about the signs and symptoms of systemic illness, including malaise, fever, or rash in other regions of the body. Is the patient engaged in sexual activity? Could she have been exposed to a sexually transmitted infection? Additionally, assess the lesion, conduct a pelvic examination, and get cultures.
Etiological Factors
Basal cell carcinoma
This nodular tumor, prevalent in postmenopausal women, features a central ulcer and a raised, poorly defined border. The tumor is usually asymptomatic but may sometimes induce itching, hemorrhage, discharge, and a burning feeling.
Nonmalignant cysts
Epidermal inclusion cysts, the predominant vulvar cysts, typically manifest on the labia majora and are generally spherical and asymptomatic. They occasionally exhibit erythema and tenderness. Bartholin's duct cysts are often unilateral, tense, nontender, and palpable; they manifest on the posterior labia minora and may induce minor discomfort during intercourse or, when sizable, impede intercourse or even ambulation. Bartholin's abscess, an infection of a Bartholin's duct cyst, results in progressive pain and tenderness, along with potential vulvar enlargement, erythema, and deformity.
Sexually transmitted illnesses are the predominant cause of vulvar lesions in premenopausal women, while vulvar tumors and cysts are the primary lesions in women aged 50 to 70.
Benign tumors of the vulva
Benign vulvar tumors, whether cystic or solid, are typically asymptomatic.
Chancroid
Chancroid, an uncommon sexually transmitted infection, results in painful vulvar sores. Headache, malaise, and a temperature of 102.2°F (39°C) may manifest, accompanied by swollen, painful inguinal lymph nodes.
Genital warts
Genital warts, a sexually transmitted infection, manifest as painless lesions on the vulva, vagina, and cervix. Warts commence as little red or pink protuberances that develop into pedunculated formations. Numerous swellings exhibiting a cauliflower-like morphology are prevalent. Additional findings including pruritus, erythema, and a copious, mucopurulent vaginal discharge. Patients often report experiencing burning or paresthesia in the vaginal introitus.
Gonorrhea
Vulvar lesions, typically localized to Bartholin’s glands, may manifest with pruritus, a burning feeling, discomfort, and a green-yellow vaginal discharge; nevertheless, the majority of patients remain asymptomatic. Additional findings encompass dysuria and urine incontinence; vaginal erythema, edema, hemorrhage, and engorgement; as well as intense pelvic and lower abdominal pain.
Granuloma inguinale
Initially, a solitary painless macule or papule emerges on the vulva, progressing to an ulcerated, elevated, beefy-red lesion with a granular, friable margin. Additional painless and sometimes malodorous lesions may appear on the labia, vagina, or cervix. Infection and pain ensue, leading to the enlargement and potential tenderness of regional lymph nodes. Systemic consequences encompass fever, weight reduction, and malaise.
Genital herpes simplex
Herpes simplex manifests as fluid-filled vesicles on the cervix and perhaps on the vulva, labia, perianal area, vagina, or oral cavity. The vesicles, initially asymptomatic, may rupture and progress into widespread, superficial, painful ulcers, accompanied by erythema, significant edema, and tender inguinal lymphadenopathy. Additional results encompass pyrexia, malaise, and dysuria.
Lymphogranuloma venereum
Individuals with lymphogranuloma venereum, a bacterial infection, typically have a solitary, painless papule or ulcer on the posterior vulva that resolves within a few days. Unilateral, painful, and swollen lymph nodes typically manifest 2 to 6 weeks later. Additional findings including fever, chills, headache, anorexia, myalgias, arthralgias, weight loss, and perineal edema.
Squamous cell carcinoma
Invasive carcinoma predominantly affects postmenopausal women and may manifest as vulvar pruritus, discomfort, and a vulvar mass. As the tumor expands, it may invade the vagina, anus, and urethra, resulting in hemorrhage, discharge, or dysuria. Carcinoma in situ predominantly occurs in premenopausal women, manifesting as a vulvar lesion that may seem white or red, elevated, well-defined, wet, crusty, and solitary.
Hyperplasia of squamous cells
Previously referred to as hyperplastic dystrophy, these vulvar lesions may be distinctly outlined or indistinct; localized or widespread; and exhibit red, brown, white, or a combination of red and white hues. Intense pruritus, maybe accompanied by vulvar pain, severe burning, and dyspareunia, is the primary symptom.
Lichen sclerosus, a kind of vulvar dystrophy, results in vulvar skin exhibiting a parchment-like texture. Fissures may arise between the clitoris and urethra or other vulvar regions.
Syphilis
Chancres, the principal vulvar lesions of syphilis, may manifest on the vulva, vagina, or cervix 10 to 90 days following initial exposure. Typically painless, they commence as papules that subsequently dissolve, exhibiting indurated, elevated margins and transparent bases. Condylomata lata, extremely infectious secondary vulvar lesions, are elevated, gray, flat-topped, and frequently ulcerated. Additional findings encompass a maculopapular, pustular, or nodular rash; cephalalgia; malaise; anorexia; weight reduction; pyrexia; nausea; emesis; widespread lymphadenopathy; and pharyngitis. Systemic viral infection. Varicella, measles, and other systemic viral infections may result in vulvar lesions.
Anticipate the administration of a systemic antibiotic, antiviral, topical corticosteroid, topical testosterone, or an antipruritic.
Sitz baths may enhance the patient's comfort. Deliver guidance about safer sex behaviors.Vulvar lesions in children may arise from congenital syphilis or gonorrhea. Assess for sexual abuse. Vulvar dystrophies and neoplasms have an increased prevalence with advancing age. All vulvar lesions should be presumed malignant until demonstrated otherwise. Additionally, numerous women maintain sexual activity into their later years and may originate from an era when sexually transmitted infections were not openly addressed. These patients should be interrogated regarding sexual activity and instructed on safer sex practices.
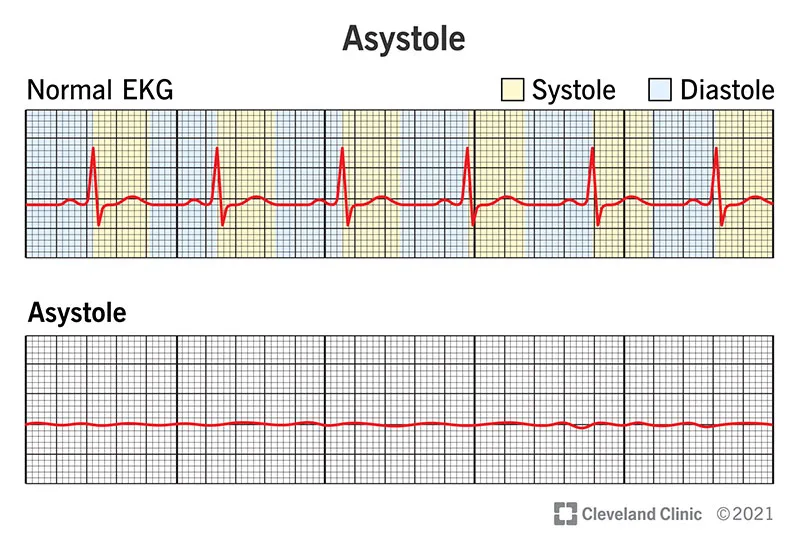
- Published on
Symptoms and Signs – Differential Diagnosis of Visual Blurring
Visual blurring is a prevalent symptom characterized by diminished visual acuity and fuzzy visual features. This may stem from ocular trauma, a neurological or ocular condition, or a disorder with vascular implications, such as diabetes mellitus. Visual blurring may also arise from mucus traversing the cornea, a refractive defect, ill-fitting contact lenses, or specific medications.
Medical History and Physical Assessment
In cases of visual blurring followed by acute, intense ocular pain, a history of trauma, or abrupt vision loss, initiate an ophthalmologic evaluation. Refer to Managing Sudden Vision Loss, page 738. In the event of a penetrating or perforating ocular injury, refrain from contacting the eye. In the absence of patient concern, inquire about the duration of the visual blurring. Does it happen exclusively at specific intervals? Inquire about concomitant signs and symptoms, including discomfort or discharge. If visual blurring occurred post-injury, gather facts of the incident and inquire whether vision was compromised shortly following the damage. Acquire a medical and pharmacological history. Examine the patient's eye, observing for lid edema, discharge, or conjunctival or scleral erythema. Additionally, observe an unevenly shaped iris, potentially indicative of prior trauma, and frequent blinking, which may suggest corneal injury. Evaluate the patient for alterations in pupil size and assess visual acuity in each eye.
Etiological Factors
Cerebral neoplasm
Visual distortion may manifest in the presence of a brain tumor. Related results encompass diminished level of consciousness (LOC), cephalalgia, apathy, alterations in behavior, amnesia, reduced attention span, vertigo, and disorientation. A tumor may also induce aphasia, convulsions, ataxia, and indications of hormonal imbalance. The subsequent effects include papilledema, vomiting, elevated systolic blood pressure, widening pulse pressure, and decorticate posture.
Cataract
Cataract is an asymptomatic condition that results in progressive visual impairment. Additional effects encompass halo vision (an initial indicator), visual glare in intense light, gradual vision deterioration, and a gray pupil that subsequently becomes milky white.
Concussion
Following blunt head trauma, vision may become hazy, double, or temporarily impaired. Additional findings encompass alterations in level of consciousness and behavior.
Corneal abrasions
Visual distortion may manifest alongside intense ocular discomfort, light sensitivity, erythema, and profuse lacrimation. Foreign bodies in the cornea. Visual distortion may be accompanied by a sensation of a foreign body, increased lacrimation, light sensitivity, severe ocular pain, miosis, conjunctival hyperemia, and a dark speck on the cornea.
Diabetic retinopathy
Retinal edema and hemorrhage result in progressive blurring, perhaps leading to blindness.
Dislocated lens.
Dislocation of the lens, particularly beyond the visual axis, results in visual blurring and, in cases of trauma, erythema.
Ocular neoplasm
Should the tumor affect the macula, visual blurring may manifest as the initial symptom. Associated findings encompass diverse visual field deficits.
Glaucoma
Acute angle-closure glaucoma, an eye emergency, manifests abruptly with unilateral visual impairment and intense pain. Additional findings encompass halo vision, a moderately dilated and nonreactive pupil, conjunctival injection, a clouded cornea, and diminished visual acuity. Significantly increased intraocular pressure may induce nausea and emesis. In chronic angle-closure glaucoma, transitory visual blurring and halo vision may occur prior to discomfort and blindness.
Genetic corneal dystrophies
Visual blurring may either remain constant or progressively deteriorate over time. Certain dystrophies induce concomitant discomfort, visual impairment, photophobia, lacrimation, and corneal opacities.
Elevated blood pressure
Hypertension can induce vision impairment and a persistent morning headache that diminishes in intensity during the day. If diastolic blood pressure surpasses 120 mm Hg, the patient may experience an intense, pulsating headache. Accompanying symptoms encompass restlessness, confusion, nausea, vomiting, seizures, and diminished level of consciousness.
Hyphema
Blunt ocular injuries with bleeding in the anterior chamber results in vision impairment. Additional consequences encompass considerable pain, diffuse conjunctival injection, apparent hemorrhage in the anterior chamber, ecchymosis, eyelid edema, and a firm eye.
Iritis
Acute iritis results in abrupt visual impairment, moderate to intense ocular discomfort, photophobia, conjunctival hyperemia, and miosis.
Optic neuritis
Inflammation, degeneration, or demyelination of the optic nerve typically results in an acute episode of visual blurring and vision impairment. Associated findings encompass scotomas and ocular discomfort. The ophthalmoscopic examination demonstrates optic disk hyperemia, significant venous distension, indistinct disk boundaries, and engorgement of the physiological cup.
Retinal detachment
Acute visual blurring may be the preliminary indication of retinal detachment. Visual blurring intensifies, followed by floaters and intermittent flashes of light. Progressive detachment exacerbates visual impairment.
Central retinal vein blockage
Retinal vein blockage results in progressive unilateral visual blurring and various levels of vision impairment.
Age-related macular degeneration
Senile macular degeneration can lead to visual blurring (initially more pronounced at night) and gradual or fast deterioration of vision.
Cerebrovascular accident
Transient episodes of bilateral vision blurring may precede or coincide with a stroke. Accompanying findings consist of diminished level of consciousness, contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory deficit, and apraxia. Stroke may result in agnosia, aphasia, homonymous hemianopia, diplopia, disorientation, amnesia, and impaired judgment. Additional features encompass urinary retention or incontinence, constipation, alterations in behavior, emotional lability, cephalalgia, emesis, and seizures.
Temporal arteritis
This condition, prevalent in women over 60, results in abrupt blurred vision, visual loss, and a pulsating unilateral headache in the temporal or frontotemporal area. Prodromal signs and symptoms encompass malaise, anorexia, weight reduction, weakness, low-grade fever, and widespread myalgia. Additional findings encompass bewilderment, disorientation, enlarged, nodular, sensitive temporal arteries, and erythema of the surrounding skin. Hemorrhage in the vitreous body. This syndrome is characterized by abrupt unilateral visual blurring and fluctuating vision loss. Visual floaters or black streaks may also manifest.
Additional Factors: Substances
Visual blurring may result from the influence of cycloplegics, reserpine, clomiphene, phenylbutazone, thiazide diuretics, antihistamines, anticholinergics, or phenothiazines.
Prepare the patient for diagnostic evaluations, including tonometry, slit-lamp examination, skull and orbital X-rays, and, if a neurological lesion is suspected, a computed tomography scan. Instruct him on the administration of ophthalmic medication as required. If visual impairment results in irreversible vision loss, offer emotional support, orient him to his environment, and ensure his safety. Prepare him for surgery if required.
Instruct the patient on the proper technique for administering eye drops. Instruct him on safety protocols and underscore the significance of maintaining awareness of his surroundings.
Visual blurring in children may result from congenital syphilis, congenital cataracts, refractive problems, ocular traumas or infections, and elevated intracranial pressure. Refer the youngster to an ophthalmologist if warranted. Assess vision in school-age children similarly to adults; evaluate children aged 3 to 6 using the Snellen symbol chart. Refer to Testing Visual Acuity.. Assess children using Allen cards, each depicting a recognizable object, such as an animal. Instruct the youngster to cover one eye and recognize the objects as you present them. Subsequently, request that he identify them while you slowly retreat. Document the maximum distance at which he can recognize a minimum of three images.
Older individuals may develop heightened myopia due to alterations in the lens. Furthermore, the minimum distance for clear vision gradually diminishes with age.
Visual blurring is a prevalent symptom characterized by diminished visual acuity and fuzzy visual features. This may stem from ocular trauma, a neurological or ocular condition, or a disorder with vascular implications, such as diabetes mellitus. Visual blurring may also arise from mucus traversing the cornea, a refractive defect, ill-fitting contact lenses, or specific medications.
Medical History and Physical Assessment
In cases of visual blurring followed by acute, intense ocular pain, a history of trauma, or abrupt vision loss, initiate an ophthalmologic evaluation. Refer to Managing Sudden Vision Loss, page 738. In the event of a penetrating or perforating ocular injury, refrain from contacting the eye. In the absence of patient concern, inquire about the duration of the visual blurring. Does it happen exclusively at specific intervals? Inquire about concomitant signs and symptoms, including discomfort or discharge. If visual blurring occurred post-injury, gather facts of the incident and inquire whether vision was compromised shortly following the damage. Acquire a medical and pharmacological history. Examine the patient's eye, observing for lid edema, discharge, or conjunctival or scleral erythema. Additionally, observe an unevenly shaped iris, potentially indicative of prior trauma, and frequent blinking, which may suggest corneal injury. Evaluate the patient for alterations in pupil size and assess visual acuity in each eye.
Etiological Factors
Cerebral neoplasm
Visual distortion may manifest in the presence of a brain tumor. Related results encompass diminished level of consciousness (LOC), cephalalgia, apathy, alterations in behavior, amnesia, reduced attention span, vertigo, and disorientation. A tumor may also induce aphasia, convulsions, ataxia, and indications of hormonal imbalance. The subsequent effects include papilledema, vomiting, elevated systolic blood pressure, widening pulse pressure, and decorticate posture.
Cataract
Cataract is an asymptomatic condition that results in progressive visual impairment. Additional effects encompass halo vision (an initial indicator), visual glare in intense light, gradual vision deterioration, and a gray pupil that subsequently becomes milky white.
Concussion
Following blunt head trauma, vision may become hazy, double, or temporarily impaired. Additional findings encompass alterations in level of consciousness and behavior.
Corneal abrasions
Visual distortion may manifest alongside intense ocular discomfort, light sensitivity, erythema, and profuse lacrimation. Foreign bodies in the cornea. Visual distortion may be accompanied by a sensation of a foreign body, increased lacrimation, light sensitivity, severe ocular pain, miosis, conjunctival hyperemia, and a dark speck on the cornea.
Diabetic retinopathy
Retinal edema and hemorrhage result in progressive blurring, perhaps leading to blindness.
Dislocated lens.
Dislocation of the lens, particularly beyond the visual axis, results in visual blurring and, in cases of trauma, erythema.
Ocular neoplasm
Should the tumor affect the macula, visual blurring may manifest as the initial symptom. Associated findings encompass diverse visual field deficits.
Glaucoma
Acute angle-closure glaucoma, an eye emergency, manifests abruptly with unilateral visual impairment and intense pain. Additional findings encompass halo vision, a moderately dilated and nonreactive pupil, conjunctival injection, a clouded cornea, and diminished visual acuity. Significantly increased intraocular pressure may induce nausea and emesis. In chronic angle-closure glaucoma, transitory visual blurring and halo vision may occur prior to discomfort and blindness.
Genetic corneal dystrophies
Visual blurring may either remain constant or progressively deteriorate over time. Certain dystrophies induce concomitant discomfort, visual impairment, photophobia, lacrimation, and corneal opacities.
Elevated blood pressure
Hypertension can induce vision impairment and a persistent morning headache that diminishes in intensity during the day. If diastolic blood pressure surpasses 120 mm Hg, the patient may experience an intense, pulsating headache. Accompanying symptoms encompass restlessness, confusion, nausea, vomiting, seizures, and diminished level of consciousness.
Hyphema
Blunt ocular injuries with bleeding in the anterior chamber results in vision impairment. Additional consequences encompass considerable pain, diffuse conjunctival injection, apparent hemorrhage in the anterior chamber, ecchymosis, eyelid edema, and a firm eye.
Iritis
Acute iritis results in abrupt visual impairment, moderate to intense ocular discomfort, photophobia, conjunctival hyperemia, and miosis.
Optic neuritis
Inflammation, degeneration, or demyelination of the optic nerve typically results in an acute episode of visual blurring and vision impairment. Associated findings encompass scotomas and ocular discomfort. The ophthalmoscopic examination demonstrates optic disk hyperemia, significant venous distension, indistinct disk boundaries, and engorgement of the physiological cup.
Retinal detachment
Acute visual blurring may be the preliminary indication of retinal detachment. Visual blurring intensifies, followed by floaters and intermittent flashes of light. Progressive detachment exacerbates visual impairment.
Central retinal vein blockage
Retinal vein blockage results in progressive unilateral visual blurring and various levels of vision impairment.
Age-related macular degeneration
Senile macular degeneration can lead to visual blurring (initially more pronounced at night) and gradual or fast deterioration of vision.
Cerebrovascular accident
Transient episodes of bilateral vision blurring may precede or coincide with a stroke. Accompanying findings consist of diminished level of consciousness, contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory deficit, and apraxia. Stroke may result in agnosia, aphasia, homonymous hemianopia, diplopia, disorientation, amnesia, and impaired judgment. Additional features encompass urinary retention or incontinence, constipation, alterations in behavior, emotional lability, cephalalgia, emesis, and seizures.
Temporal arteritis
This condition, prevalent in women over 60, results in abrupt blurred vision, visual loss, and a pulsating unilateral headache in the temporal or frontotemporal area. Prodromal signs and symptoms encompass malaise, anorexia, weight reduction, weakness, low-grade fever, and widespread myalgia. Additional findings encompass bewilderment, disorientation, enlarged, nodular, sensitive temporal arteries, and erythema of the surrounding skin. Hemorrhage in the vitreous body. This syndrome is characterized by abrupt unilateral visual blurring and fluctuating vision loss. Visual floaters or black streaks may also manifest.
Additional Factors: Substances
Visual blurring may result from the influence of cycloplegics, reserpine, clomiphene, phenylbutazone, thiazide diuretics, antihistamines, anticholinergics, or phenothiazines.
Prepare the patient for diagnostic evaluations, including tonometry, slit-lamp examination, skull and orbital X-rays, and, if a neurological lesion is suspected, a computed tomography scan. Instruct him on the administration of ophthalmic medication as required. If visual impairment results in irreversible vision loss, offer emotional support, orient him to his environment, and ensure his safety. Prepare him for surgery if required.
Instruct the patient on the proper technique for administering eye drops. Instruct him on safety protocols and underscore the significance of maintaining awareness of his surroundings.
Visual blurring in children may result from congenital syphilis, congenital cataracts, refractive problems, ocular traumas or infections, and elevated intracranial pressure. Refer the youngster to an ophthalmologist if warranted. Assess vision in school-age children similarly to adults; evaluate children aged 3 to 6 using the Snellen symbol chart. Refer to Testing Visual Acuity.. Assess children using Allen cards, each depicting a recognizable object, such as an animal. Instruct the youngster to cover one eye and recognize the objects as you present them. Subsequently, request that he identify them while you slowly retreat. Document the maximum distance at which he can recognize a minimum of three images.
Older individuals may develop heightened myopia due to alterations in the lens. Furthermore, the minimum distance for clear vision gradually diminishes with age.

- Published on
Symptoms and Signs – Differential Diagnosis of Acts of Violence
Violent behavior, which is characterized by an abrupt loss of self-control, is the use of physical force to harm, violate, or mistreat a person or object. It's also possible that this conduct is self-directed. It could be brought on by the use of specific medications or by a biological or mental illness. Physical examination and history Find out if the patient has a history of violent behavior during your evaluation. Is he drunk or experiencing withdrawal symptoms from drugs or alcohol? Does he have a history of domestic violence, such as assault of his spouse or children or physical punishment?
Keep an eye out for signs that the patient is losing control and might start acting aggressively. Has he changed his behavior suddenly? Can't he just sit still? An attempt to release aggressiveness may be indicated by increased activity. Does he abruptly stop doing anything, implying that things will be fine soon? Does he gesture angrily or threaten others verbally? Is he laughing, jittery, or tense? An increase in feeling like this could signal a loss of control. Your patient might have an organic disorder if his aggressive behavior is a recent occurrence. Conduct a physical examination and get a medical history. Keep an eye out for a sharp shift in his consciousness. An organic disorder is suggested by disorientation, a failure to remember recent events, and the manifestation of tics, jerks, tremors, and asterixis.
Medical Reasons
organic illnesses
Violent behavior can be a symptom of disorders brought on by metabolic or neurological malfunction. Epilepsy, brain tumors, encephalitis, head trauma, endocrine problems, metabolic diseases (including calcium imbalance and uremia), and severe physical trauma are among the common causes
mental health conditions
In psychotic diseases like schizophrenia, violent behavior is a defensive technique used in reaction to a perceived threat. Personality disorders like borderline or antisocial personality may elicit a similar reaction.
Understanding the causes of the aggressive patient's conduct is essential to manage him effectively. For instance, a family history of physical punishment or abuse of a spouse or child may be the root cause of his behavior. Drug or alcohol misuse, as well as rigid family roles that inhibit personal development and uniqueness, may potentially be linked to his aggressive conduct.
FAMILY VIOLENCE CAUSES
According to social scientists, cultural attitudes that encourage violence as well as the stress and annoyance brought on by cramped living quarters and poverty are the main causes of family violence. According to social learning theorist Albert Bandura, people pick up violent conduct by watching and copying family members who use physical force and verbal abuse to express their hostile emotions. (They also pick up knowledge from movies and television, particularly when the violent hero becomes well-known and powerful.) Families with these traits may have members who are more likely to act violently, which could start a cycle of violence that continues from one generation to the next.
Other Reasons alcohol and drug
Some medications, such lidocaine and penicillin G, can cause violent behavior. Violent behavior can also result from amphetamines, alcohol misuse or withdrawal, hallucinogens, and barbiturates.
The most common settings for violent behavior are emergency rooms, critical care units, and acute and crisis mental health facilities. Be alert in these circumstances because accidents and natural calamities also raise the risk of aggressive conduct. Your objective is to maintain composure and establish environmental control in the event that your patient becomes aggressive or possibly violent.
Protect yourself first. Avoid overreacting, stay away from the patient, and seek for help. Keep your cool and make sure you have enough staff on hand to restrain or subdue the patient if needed. To prevent alarming or upsetting the patient further, encourage him to relocate to a peaceful area away from people, activity, and noise. Tell him he's secure, reassure him, and explain what's going on. Take the patient's violent threats seriously and let the people they are directed at know.
Administer a psychotropic drug if directed. Keep in mind that how you treat a violent patient may be influenced by your own attitudes. Ask for assistance from another staff member if you're feeling anxious or critical.
Counseling for Patients
Tell the patient that he is secure, reassure him, and explain what is happening. Explain the cause of the patient's violent behavior, if any, once he has calmed down. Tips for Pediatrics Threats from adolescents and younger children are frequently the result of violent imaginations, desires, or unfulfilled wants. Extremely violent adolescents may come from homes where there has been a history of physical or psychological abuse. These kids might act violently toward their siblings, friends, and pets.
Violent behavior, which is characterized by an abrupt loss of self-control, is the use of physical force to harm, violate, or mistreat a person or object. It's also possible that this conduct is self-directed. It could be brought on by the use of specific medications or by a biological or mental illness. Physical examination and history Find out if the patient has a history of violent behavior during your evaluation. Is he drunk or experiencing withdrawal symptoms from drugs or alcohol? Does he have a history of domestic violence, such as assault of his spouse or children or physical punishment?
Keep an eye out for signs that the patient is losing control and might start acting aggressively. Has he changed his behavior suddenly? Can't he just sit still? An attempt to release aggressiveness may be indicated by increased activity. Does he abruptly stop doing anything, implying that things will be fine soon? Does he gesture angrily or threaten others verbally? Is he laughing, jittery, or tense? An increase in feeling like this could signal a loss of control. Your patient might have an organic disorder if his aggressive behavior is a recent occurrence. Conduct a physical examination and get a medical history. Keep an eye out for a sharp shift in his consciousness. An organic disorder is suggested by disorientation, a failure to remember recent events, and the manifestation of tics, jerks, tremors, and asterixis.
Medical Reasons
organic illnesses
Violent behavior can be a symptom of disorders brought on by metabolic or neurological malfunction. Epilepsy, brain tumors, encephalitis, head trauma, endocrine problems, metabolic diseases (including calcium imbalance and uremia), and severe physical trauma are among the common causes
mental health conditions
In psychotic diseases like schizophrenia, violent behavior is a defensive technique used in reaction to a perceived threat. Personality disorders like borderline or antisocial personality may elicit a similar reaction.
Understanding the causes of the aggressive patient's conduct is essential to manage him effectively. For instance, a family history of physical punishment or abuse of a spouse or child may be the root cause of his behavior. Drug or alcohol misuse, as well as rigid family roles that inhibit personal development and uniqueness, may potentially be linked to his aggressive conduct.
FAMILY VIOLENCE CAUSES
According to social scientists, cultural attitudes that encourage violence as well as the stress and annoyance brought on by cramped living quarters and poverty are the main causes of family violence. According to social learning theorist Albert Bandura, people pick up violent conduct by watching and copying family members who use physical force and verbal abuse to express their hostile emotions. (They also pick up knowledge from movies and television, particularly when the violent hero becomes well-known and powerful.) Families with these traits may have members who are more likely to act violently, which could start a cycle of violence that continues from one generation to the next.
Other Reasons alcohol and drug
Some medications, such lidocaine and penicillin G, can cause violent behavior. Violent behavior can also result from amphetamines, alcohol misuse or withdrawal, hallucinogens, and barbiturates.
The most common settings for violent behavior are emergency rooms, critical care units, and acute and crisis mental health facilities. Be alert in these circumstances because accidents and natural calamities also raise the risk of aggressive conduct. Your objective is to maintain composure and establish environmental control in the event that your patient becomes aggressive or possibly violent.
Protect yourself first. Avoid overreacting, stay away from the patient, and seek for help. Keep your cool and make sure you have enough staff on hand to restrain or subdue the patient if needed. To prevent alarming or upsetting the patient further, encourage him to relocate to a peaceful area away from people, activity, and noise. Tell him he's secure, reassure him, and explain what's going on. Take the patient's violent threats seriously and let the people they are directed at know.
Administer a psychotropic drug if directed. Keep in mind that how you treat a violent patient may be influenced by your own attitudes. Ask for assistance from another staff member if you're feeling anxious or critical.
Counseling for Patients
Tell the patient that he is secure, reassure him, and explain what is happening. Explain the cause of the patient's violent behavior, if any, once he has calmed down. Tips for Pediatrics Threats from adolescents and younger children are frequently the result of violent imaginations, desires, or unfulfilled wants. Extremely violent adolescents may come from homes where there has been a history of physical or psychological abuse. These kids might act violently toward their siblings, friends, and pets.

