- Published on
Emergency And Acute Medicine – Uncomplicated Pregnancy
Pregnancy is a normal physiologic state rather than a disease process, yet it imposes significant metabolic and anatomic changes on the mother to support fetal growth and development. In emergency care, all women of reproductive age presenting with abdominal pain are considered pregnant until proven otherwise—even with a history of sterilization. Hormonal changes driven primarily by placental progesterone and estrogen account for most physiologic adaptations. In adolescents, menarche typically occurs between ages 11 and 15. Pregnant adolescents may be unaware of or reluctant to disclose pregnancy; therefore, pregnancy must always be considered. Adolescent pregnancies also carry a higher risk of obstructive labor.
The physiologic changes of pregnancy are largely mediated by placental hormones. Human chorionic gonadotropin (hCG) prevents involution of the corpus luteum and stimulates continued production of estrogen and progesterone. Elevated hCG levels contribute to nausea and vomiting. Progesterone promotes development of decidual cells to nourish the early embryo, decreases uterine contractility to reduce the risk of spontaneous abortion, and helps prepare breast tissue for lactation. Estrogen stimulates enlargement of the uterus and breasts, growth of mammary ducts, enlargement of the external genitalia, and relaxation of pelvic ligaments and joints.
Diagnosis of pregnancy relies on history and physical examination, hormonal assays, and ultrasonography. The most common presenting symptom is amenorrhea in a sexually active woman, often accompanied by nausea, vomiting, breast tenderness, urinary frequency, fatigue, low back pain, constipation, heartburn, pica, weight gain, edema of the lower extremities, and progressive abdominal enlargement. Determining the first day of the last menstrual period (FDLMP) is essential, though up to 40% of women cannot accurately recall it. After 16 weeks’ gestation, fundal height in centimeters from the pubic symphysis approximates gestational age in weeks. Pelvic examination may identify uterine enlargement or abnormal masses.
Pregnancy testing measures the β-subunit of hCG. Urine tests typically detect levels ≥25 mIU/mL but may yield false negatives with dilute urine or high vitamin C intake. Home tests can detect pregnancy 9–12 days after conception but should be confirmed with serum hCG. Serum hCG becomes detectable 8–11 days post-conception and normally doubles approximately every 48 hours until 6–7 weeks’ gestation. hCG may remain detectable for up to 60 days following abortion. Serum progesterone levels help assess viability; levels <5 ng />L suggest a nonviable pregnancy, while levels ≥25 ng/mL are consistent with viability.
Ultrasonography is essential when evaluating abdominal pain, vaginal bleeding, or suspected complications. It confirms intrauterine versus ectopic pregnancy, estimates gestational age, assesses fetal viability, and identifies abnormalities. Transvaginal ultrasound is more sensitive and can detect intrauterine pregnancy at 4–5 weeks, whereas transabdominal ultrasound visualizes the gestational sac at approximately 5.5–6 weeks. Transvaginal ultrasound is contraindicated in cases of premature rupture of membranes or third-trimester bleeding. MRI is considered safe in pregnancy and is often preferred for evaluating appendicitis. Radiation exposure from plain radiography or CT is dose-dependent; efforts should be made to keep fetal exposure below 5,000 mrad. Shielding should be used whenever possible.
In the emergency setting, assume pregnancy until excluded. Prehospital and ED management prioritize maternal stabilization, as optimizing maternal condition improves fetal outcome. Advanced cardiac life support or trauma protocols should be followed when indicated. If gestational age exceeds 24 weeks, the patient should be positioned in the left lateral recumbent position to reduce inferior vena cava compression and improve cardiac output. Oxygen, cardiac monitoring, intravenous access, and fluids should be administered as needed.
Medication use in pregnancy requires careful consideration, especially during the first trimester when organogenesis occurs. Clinicians should review medication safety classifications before prescribing. Acetaminophen is the preferred over-the-counter analgesic, with dosing up to 500 mg every 6 hours (maximum 4 g/day). Short-term use of opioids such as morphine, codeine, oxycodone, hydrocodone, or meperidine may be considered for severe pain. Ondansetron 4 mg IM or IV every 8 hours may be used for nausea, and vitamin B6 (25 mg three times daily) or ginger may also provide relief. Antibiotic selection depends on maternal allergies, gestational age, and likely pathogens. Prenatal vitamins should be encouraged.
Admission is indicated for obstetric complications such as hyperemesis gravidarum with dehydration, complicated urinary tract infection, ectopic or molar pregnancy, septic abortion, preterm labor, premature rupture of membranes, preeclampsia or eclampsia, and severe pregnancy-induced hypertension. Pregnant patients with serious medical conditions warranting admission in nonpregnant patients should also be admitted. Patients without complications may be discharged with instructions for obstetric follow-up by 6–8 weeks’ gestation.
Key principles include assuming pregnancy in all reproductive-age women until ruled out, reviewing medication safety before administration, and minimizing fetal radiation exposure. The primary goal in emergency care is always maternal stabilization to ensure the best possible fetal outcome.
Pregnancy is a normal physiologic state rather than a disease process, yet it imposes significant metabolic and anatomic changes on the mother to support fetal growth and development. In emergency care, all women of reproductive age presenting with abdominal pain are considered pregnant until proven otherwise—even with a history of sterilization. Hormonal changes driven primarily by placental progesterone and estrogen account for most physiologic adaptations. In adolescents, menarche typically occurs between ages 11 and 15. Pregnant adolescents may be unaware of or reluctant to disclose pregnancy; therefore, pregnancy must always be considered. Adolescent pregnancies also carry a higher risk of obstructive labor.
The physiologic changes of pregnancy are largely mediated by placental hormones. Human chorionic gonadotropin (hCG) prevents involution of the corpus luteum and stimulates continued production of estrogen and progesterone. Elevated hCG levels contribute to nausea and vomiting. Progesterone promotes development of decidual cells to nourish the early embryo, decreases uterine contractility to reduce the risk of spontaneous abortion, and helps prepare breast tissue for lactation. Estrogen stimulates enlargement of the uterus and breasts, growth of mammary ducts, enlargement of the external genitalia, and relaxation of pelvic ligaments and joints.
Diagnosis of pregnancy relies on history and physical examination, hormonal assays, and ultrasonography. The most common presenting symptom is amenorrhea in a sexually active woman, often accompanied by nausea, vomiting, breast tenderness, urinary frequency, fatigue, low back pain, constipation, heartburn, pica, weight gain, edema of the lower extremities, and progressive abdominal enlargement. Determining the first day of the last menstrual period (FDLMP) is essential, though up to 40% of women cannot accurately recall it. After 16 weeks’ gestation, fundal height in centimeters from the pubic symphysis approximates gestational age in weeks. Pelvic examination may identify uterine enlargement or abnormal masses.
Pregnancy testing measures the β-subunit of hCG. Urine tests typically detect levels ≥25 mIU/mL but may yield false negatives with dilute urine or high vitamin C intake. Home tests can detect pregnancy 9–12 days after conception but should be confirmed with serum hCG. Serum hCG becomes detectable 8–11 days post-conception and normally doubles approximately every 48 hours until 6–7 weeks’ gestation. hCG may remain detectable for up to 60 days following abortion. Serum progesterone levels help assess viability; levels <5 ng />L suggest a nonviable pregnancy, while levels ≥25 ng/mL are consistent with viability.
Ultrasonography is essential when evaluating abdominal pain, vaginal bleeding, or suspected complications. It confirms intrauterine versus ectopic pregnancy, estimates gestational age, assesses fetal viability, and identifies abnormalities. Transvaginal ultrasound is more sensitive and can detect intrauterine pregnancy at 4–5 weeks, whereas transabdominal ultrasound visualizes the gestational sac at approximately 5.5–6 weeks. Transvaginal ultrasound is contraindicated in cases of premature rupture of membranes or third-trimester bleeding. MRI is considered safe in pregnancy and is often preferred for evaluating appendicitis. Radiation exposure from plain radiography or CT is dose-dependent; efforts should be made to keep fetal exposure below 5,000 mrad. Shielding should be used whenever possible.
In the emergency setting, assume pregnancy until excluded. Prehospital and ED management prioritize maternal stabilization, as optimizing maternal condition improves fetal outcome. Advanced cardiac life support or trauma protocols should be followed when indicated. If gestational age exceeds 24 weeks, the patient should be positioned in the left lateral recumbent position to reduce inferior vena cava compression and improve cardiac output. Oxygen, cardiac monitoring, intravenous access, and fluids should be administered as needed.
Medication use in pregnancy requires careful consideration, especially during the first trimester when organogenesis occurs. Clinicians should review medication safety classifications before prescribing. Acetaminophen is the preferred over-the-counter analgesic, with dosing up to 500 mg every 6 hours (maximum 4 g/day). Short-term use of opioids such as morphine, codeine, oxycodone, hydrocodone, or meperidine may be considered for severe pain. Ondansetron 4 mg IM or IV every 8 hours may be used for nausea, and vitamin B6 (25 mg three times daily) or ginger may also provide relief. Antibiotic selection depends on maternal allergies, gestational age, and likely pathogens. Prenatal vitamins should be encouraged.
Admission is indicated for obstetric complications such as hyperemesis gravidarum with dehydration, complicated urinary tract infection, ectopic or molar pregnancy, septic abortion, preterm labor, premature rupture of membranes, preeclampsia or eclampsia, and severe pregnancy-induced hypertension. Pregnant patients with serious medical conditions warranting admission in nonpregnant patients should also be admitted. Patients without complications may be discharged with instructions for obstetric follow-up by 6–8 weeks’ gestation.
Key principles include assuming pregnancy in all reproductive-age women until ruled out, reviewing medication safety before administration, and minimizing fetal radiation exposure. The primary goal in emergency care is always maternal stabilization to ensure the best possible fetal outcome.

- Published on
Emergency And Acute Medicine – Phalangeal Injuries, Hand
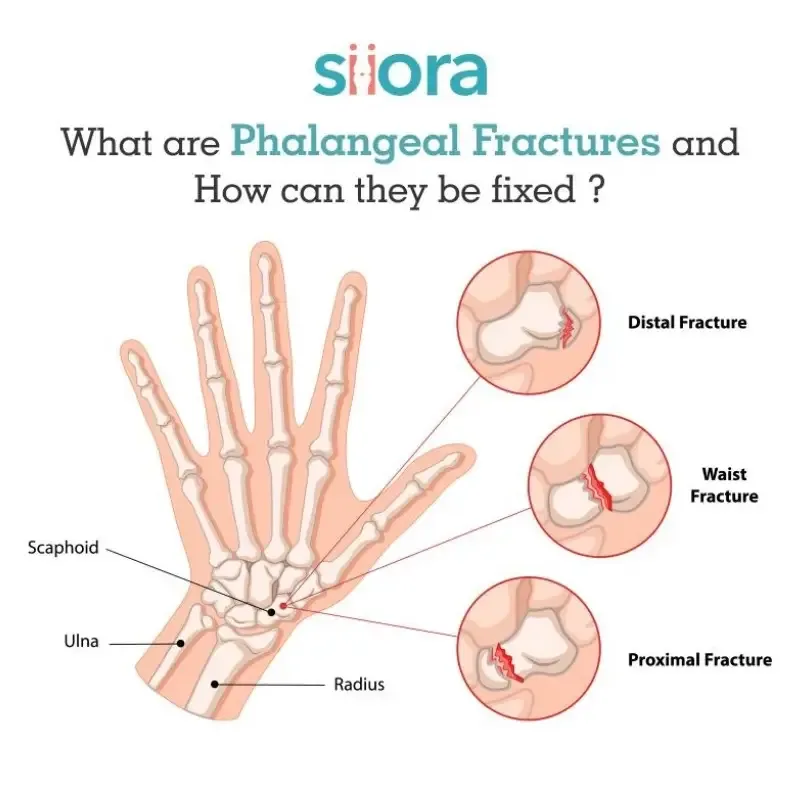
Phalangeal injuries account for a significant proportion of traumatic hand injuries, with the distal phalanx being the most frequently fractured bone in the hand. Dorsal dislocation of the proximal interphalangeal (PIP) joint is the most common finger dislocation. These injuries are typically related to sports, occupational trauma, crush mechanisms, or hyperextension and hyperflexion forces. Infections may complicate puncture wounds, bites, or aquatic exposures, with pathogens varying by mechanism. In children, diagnosis may be more difficult due to limited cooperation, and growth plate injuries are common.
Mechanism of injury provides critical diagnostic clues. Hyperextension injuries often result in ligamentous injury, chip fractures, or “Jersey finger,” which is rupture of the flexor digitorum profundus tendon from its distal insertion. Hyperflexion at the fingertip may cause “Mallet finger,” typically involving an avulsion fracture at the extensor tendon insertion. Crush injuries frequently produce fractures with associated soft-tissue damage. History should include handedness, occupation, comorbidities affecting healing, and tetanus status.
Examination must be systematic. Assess for swelling, deformity, angulation, rotation, shortening, lacerations, burns, nail injury, and neurovascular compromise. Evaluate each joint individually (MCP, PIP, DIP) with active and passive range of motion and resistance testing. Two-point discrimination should normally be 4–5 mm. Rotational deformity is best assessed by flexing the MCP joints while extending the PIP and DIP joints; all fingers should point toward the radius without overlap. Kanavel signs suggest infectious flexor tenosynovitis and include pain with passive extension, fusiform swelling, flexed posture at rest, and tenderness along the flexor sheath. In infants, consider hair tourniquet syndrome when swelling is unexplained.
Radiographs with anteroposterior, true lateral, and oblique views are essential. Ultrasound may assist in diagnosing tendon rupture. In children, open physes make interpretation more challenging, and Salter–Harris fractures may accompany apparent dislocations. Differential diagnosis includes fractures, tendon lacerations or ruptures, fight bites over dorsal MCP joints, and complex open injuries.
Prehospital reduction of finger dislocations is generally discouraged unless transport is prolonged or neurovascular compromise is present, as premature reduction may obscure associated ligamentous injury. Amputated digits should be wrapped in moist saline gauze, placed in a plastic bag, and then placed in a second bag containing ice without direct contact. Reimplantation is particularly considered for thumb injuries, multiple digits, amputations between the PIP and DIP joints, or amputations in children.
Initial management includes removal of rings, immobilization, elevation, and ice. Neurovascular compromise requires immediate reduction to neutral alignment. Interphalangeal dislocations are reduced with longitudinal traction and direction-specific maneuvers depending on dorsal, volar, or lateral displacement. Immobilization depends on the joint involved and direction of injury. MCP dislocations are reduced gently with traction and volar pressure and splinted appropriately. Postreduction stability must be assessed clinically and radiographically.
Closed distal phalanx fractures are typically splinted with DIP immobilization while allowing PIP motion. Middle and proximal phalanx fractures may be managed with buddy taping if stable, or reduced and immobilized in appropriate gutter splints when displaced. Acceptable alignment includes minimal shortening (1–2 mm), up to 10° of angulation, and absolutely no rotational deformity. Mallet finger requires strict DIP extension splinting while preserving PIP mobility. Jersey finger requires urgent specialist referral, with splinting in slight flexion and avoidance of forced DIP extension. Gamekeeper’s thumb is treated with thumb spica immobilization. Subungual hematomas are treated with nail trephination unless associated with significant tuft fracture. Open fractures require urgent surgical consultation and early intravenous antibiotics.
Tetanus status must be addressed. Digital nerve blocks should use anesthetic without epinephrine. Antibiotics are not required for clean uncomplicated wounds but should be tailored to contaminated injuries, bites, or suspected infectious tenosynovitis.
Stable injuries in appropriate splints may be discharged with orthopedic follow-up within one week. Emergent consultation is required for amputations, open fractures or joints, neurovascular compromise, infectious tenosynovitis, high-pressure injection injuries, or irreducible dislocations. Urgent consultation is necessary for unstable fractures, rotational deformity, joint involvement, epiphyseal injuries, tendon rupture, or persistent instability after reduction. Careful assessment of rotational alignment and tendon function is essential, as missed tendon injuries such as Jersey finger may lead to significant long-term dysfunction if not promptly managed.
Phalangeal injuries account for a significant proportion of traumatic hand injuries, with the distal phalanx being the most frequently fractured bone in the hand. Dorsal dislocation of the proximal interphalangeal (PIP) joint is the most common finger dislocation. These injuries are typically related to sports, occupational trauma, crush mechanisms, or hyperextension and hyperflexion forces. Infections may complicate puncture wounds, bites, or aquatic exposures, with pathogens varying by mechanism. In children, diagnosis may be more difficult due to limited cooperation, and growth plate injuries are common.
Mechanism of injury provides critical diagnostic clues. Hyperextension injuries often result in ligamentous injury, chip fractures, or “Jersey finger,” which is rupture of the flexor digitorum profundus tendon from its distal insertion. Hyperflexion at the fingertip may cause “Mallet finger,” typically involving an avulsion fracture at the extensor tendon insertion. Crush injuries frequently produce fractures with associated soft-tissue damage. History should include handedness, occupation, comorbidities affecting healing, and tetanus status.
Examination must be systematic. Assess for swelling, deformity, angulation, rotation, shortening, lacerations, burns, nail injury, and neurovascular compromise. Evaluate each joint individually (MCP, PIP, DIP) with active and passive range of motion and resistance testing. Two-point discrimination should normally be 4–5 mm. Rotational deformity is best assessed by flexing the MCP joints while extending the PIP and DIP joints; all fingers should point toward the radius without overlap. Kanavel signs suggest infectious flexor tenosynovitis and include pain with passive extension, fusiform swelling, flexed posture at rest, and tenderness along the flexor sheath. In infants, consider hair tourniquet syndrome when swelling is unexplained.
Radiographs with anteroposterior, true lateral, and oblique views are essential. Ultrasound may assist in diagnosing tendon rupture. In children, open physes make interpretation more challenging, and Salter–Harris fractures may accompany apparent dislocations. Differential diagnosis includes fractures, tendon lacerations or ruptures, fight bites over dorsal MCP joints, and complex open injuries.
Prehospital reduction of finger dislocations is generally discouraged unless transport is prolonged or neurovascular compromise is present, as premature reduction may obscure associated ligamentous injury. Amputated digits should be wrapped in moist saline gauze, placed in a plastic bag, and then placed in a second bag containing ice without direct contact. Reimplantation is particularly considered for thumb injuries, multiple digits, amputations between the PIP and DIP joints, or amputations in children.
Initial management includes removal of rings, immobilization, elevation, and ice. Neurovascular compromise requires immediate reduction to neutral alignment. Interphalangeal dislocations are reduced with longitudinal traction and direction-specific maneuvers depending on dorsal, volar, or lateral displacement. Immobilization depends on the joint involved and direction of injury. MCP dislocations are reduced gently with traction and volar pressure and splinted appropriately. Postreduction stability must be assessed clinically and radiographically.
Closed distal phalanx fractures are typically splinted with DIP immobilization while allowing PIP motion. Middle and proximal phalanx fractures may be managed with buddy taping if stable, or reduced and immobilized in appropriate gutter splints when displaced. Acceptable alignment includes minimal shortening (1–2 mm), up to 10° of angulation, and absolutely no rotational deformity. Mallet finger requires strict DIP extension splinting while preserving PIP mobility. Jersey finger requires urgent specialist referral, with splinting in slight flexion and avoidance of forced DIP extension. Gamekeeper’s thumb is treated with thumb spica immobilization. Subungual hematomas are treated with nail trephination unless associated with significant tuft fracture. Open fractures require urgent surgical consultation and early intravenous antibiotics.
Tetanus status must be addressed. Digital nerve blocks should use anesthetic without epinephrine. Antibiotics are not required for clean uncomplicated wounds but should be tailored to contaminated injuries, bites, or suspected infectious tenosynovitis.
Stable injuries in appropriate splints may be discharged with orthopedic follow-up within one week. Emergent consultation is required for amputations, open fractures or joints, neurovascular compromise, infectious tenosynovitis, high-pressure injection injuries, or irreducible dislocations. Urgent consultation is necessary for unstable fractures, rotational deformity, joint involvement, epiphyseal injuries, tendon rupture, or persistent instability after reduction. Careful assessment of rotational alignment and tendon function is essential, as missed tendon injuries such as Jersey finger may lead to significant long-term dysfunction if not promptly managed.
- Published on
Infectious Diseases and Microbiology: Trauma-Related Infections
Basics
Description
Trauma-related infections broadly include infections that arise directly or indirectly from wounds or injuries. A recently recognized high-risk group is patients needing emergency operations for non-trauma causes such as gastrointestinal perforation, obstruction, bleeding, or acute inflammation, which is associated with increased infection-related mortality.
Epidemiology
Incidence
Millions of wounds are treated annually in U.S. emergency departments, including large numbers of burns and lacerations, and cutting or piercing injuries generate substantial outpatient visits. Reported infection rates among trauma patients vary widely across studies. Sepsis contributes to a significant proportion of deaths in hospitalized trauma patients.
Risk Factors
Higher risk is linked to heavily contaminated wounds, impaired blood supply from injury, emergent splenectomy, glucocorticoid exposure, delayed treatment, obesity, and greater injury severity.
General Prevention
Thorough cleaning and irrigation with water or normal saline is essential. Topical antibiotics and occlusive dressings reduce infection rates in traumatic lacerations. Confirm tetanus immunization status and vaccinate patients who are overdue or uncertain. Highly contaminated wounds may require secondary intention healing or delayed primary closure. In open limb fractures, prophylactic antibiotics lower early infection risk. Although high-quality placebo-controlled trials are limited for severely injured contaminated patients, empiric antibiotics are commonly used for penetrating chest or abdominal injuries and severe head wounds. Short prophylactic courses are generally as effective as longer courses, supported by evidence in penetrating abdominal trauma showing no major outcome difference between 24-hour and 5-day regimens. Antibiotic levels can be altered by fluid shifts and hyperdynamic physiology, and data support higher doses for shorter durations, especially in trauma laparotomy patients. Short prophylaxis reduces infection in compound mandibular fractures. After traumatic splenectomy, the risk of early serious infection is low in isolated splenic injury but rises with greater injury and associated trauma; encapsulated organisms are key pathogens early and late. Administer pneumococcal and meningococcal vaccines once clinically stable after splenectomy. Strict infection control practices reduce hospital-acquired infections in severely injured patients.
Etiology
Trauma increases infection risk through vascular disruption and microcirculatory damage causing ischemia, edema, compartment syndromes, and necrosis; contamination of wounds and sterile spaces by soil or water exposure; post-shock immune dysfunction; reduced IgM responses after splenectomy compared with nonsplenectomized infected posttrauma patients; and additional immune suppression from corticosteroids used for head injury. Common infections in multiply injured patients include pneumonia and empyema, bacteremia or fungemia (including catheter-related), surgical site infection, intraabdominal infection, meningitis, urinary tract infection, sinus infection, wound infection, and Clostridioides difficile colitis after prior antibiotic exposure. Acinetobacter baumannii infections have been reported in injured military personnel from conflict regions, with some isolates susceptible only to carbapenems such as imipenem.
Diagnosis
History
Diagnosis is challenging because fever may be noninfectious after trauma, patients may be unable to provide history, examinations may be limited, and usual infection signs are less reliable in critically ill, multiply traumatized patients.
Physical Examination
Fever, tachycardia, and hypotension can occur after severe injury without infection. In critically ill patients, track ventilator requirements, sputum volume and character, and urine and stool output. In hospitalized trauma patients, perform a complete exam emphasizing indwelling devices, skin, operative wounds, abdomen, and respiratory findings. Inspect injured sites for local infection signs including pain, foul odor, erythema, swelling, purulent drainage, and delayed healing.
Diagnostic Tests and Interpretation
Laboratory Studies
Obtain CBC with differential, electrolytes, and kidney and liver function tests, recognizing leukocytosis may reflect trauma alone. Whenever possible, collect cultures from suspected sites before antibiotics, including blood, sputum, urine, cerebrospinal fluid studies and culture when penetrating head injury or CNS drains are present, wound cultures, and abscess cultures. With watery diarrhea and prior antibiotic exposure, test stool for C. difficile.
Imaging
Use chest radiography to assess pneumonia, especially in mechanically ventilated patients. Chest CT is more sensitive for thoracic infection in septic trauma patients and can guide correction of malpositioned or blocked thoracostomy tubes, though concurrent thoracic injuries can reduce test accuracy. Abdominal CT can identify intraabdominal infection such as perforation, colitis, cholecystitis, or abscess. For suspected extremity infection, ultrasound, CT, or MRI can help exclude abscess.
Diagnostic Procedures/Other
Image-guided or operative drainage of abscesses is diagnostic and therapeutic; send fluid for Gram stain, aerobic and anaerobic cultures, add fungal studies for abdominal or pelvic collections, and consider acid-fast bacilli smear and mycobacterial culture based on epidemiologic risk.
Differential Diagnosis
In severely injured patients, infection mimics include atelectasis, deep vein thrombosis, drug fever, allergic reactions or anaphylaxis, hypovolemia, large hematoma, sterile inflammation, pulmonary contusion, transfusion reactions, and central fever from brain injury.
Treatment
Medications
Correcting local anatomic problems such as open fractures or perforated abdominal organs is often more important than antibiotics alone. In trauma patients, unexplained hemodynamic instability not due to hypovolemia should prompt empiric antibiotics even if other infection signs are absent. Choose antibiotics based on suspected source, local resistance, trauma context (bites, water exposure, soil contamination), hospitalization duration and risk of resistant organisms, local MRSA prevalence, and allergies. If no source is identified, start broad-spectrum therapy including antistaphylococcal coverage plus broad gram-negative and anaerobic activity
.
Additional Treatment
Monitor clinical response and narrow therapy to culture and susceptibility results. If diagnostic evaluation is negative and the patient is stable, consider stopping antibiotics. Duration depends on infection site and clinical course. Remove central venous and urinary catheters as soon as they are no longer needed.
Issues for Referral
Severe injuries require urgent evaluation at experienced trauma centers with surgical and critical care capability. Infectious diseases consultation is useful when the patient is critically ill, not improving on therapy, or diagnosis remains uncertain.
Surgery/Other Procedures
Drain collections, debride necrotic tissue, and repair fractures or perforations promptly, and implement measures to mobilize respiratory secretions.
In-Patient Considerations
Initial Stabilization
Stabilize airway and circulation, provide rapid fluid resuscitation, and document all injuries.
Admission Criteria
Admit patients with penetrating injuries, fractures needing urgent repair, abnormal vital signs, impaired mental status, uncontrolled pain, or severe injuries. Burns meeting moderate to major thresholds require admission to specialized burn care centers.
Discharge Criteria
Discharge when fever has been absent for more than 24 hours, vital signs are stable, and follow-up for antibiotics and wound care is arranged.
Ongoing Care and Follow-Up
Patient Monitoring
Monitor closely for wound infection and healthcare-associated infections, which occur in a meaningful minority of hospitalized trauma patients.
Diet
Provide adequate nutritional support and consider nutrition consultation in severely injured hospitalized patients.
Patient Education
Teach warning signs of wound infection and provide clear instructions for wound care, including packing and dressing-change schedules.
Prognosis
Trauma-related infection increases mortality risk and is associated with worse functional outcomes during the year after injury compared with trauma patients without infection.
Complications
Serious outcomes include septic shock, respiratory failure, peritonitis and abdominal abscess, osteomyelitis, brain abscess, and acute acalculous cholecystitis.
Basics
Description
Trauma-related infections broadly include infections that arise directly or indirectly from wounds or injuries. A recently recognized high-risk group is patients needing emergency operations for non-trauma causes such as gastrointestinal perforation, obstruction, bleeding, or acute inflammation, which is associated with increased infection-related mortality.
Epidemiology
Incidence
Millions of wounds are treated annually in U.S. emergency departments, including large numbers of burns and lacerations, and cutting or piercing injuries generate substantial outpatient visits. Reported infection rates among trauma patients vary widely across studies. Sepsis contributes to a significant proportion of deaths in hospitalized trauma patients.
Risk Factors
Higher risk is linked to heavily contaminated wounds, impaired blood supply from injury, emergent splenectomy, glucocorticoid exposure, delayed treatment, obesity, and greater injury severity.
General Prevention
Thorough cleaning and irrigation with water or normal saline is essential. Topical antibiotics and occlusive dressings reduce infection rates in traumatic lacerations. Confirm tetanus immunization status and vaccinate patients who are overdue or uncertain. Highly contaminated wounds may require secondary intention healing or delayed primary closure. In open limb fractures, prophylactic antibiotics lower early infection risk. Although high-quality placebo-controlled trials are limited for severely injured contaminated patients, empiric antibiotics are commonly used for penetrating chest or abdominal injuries and severe head wounds. Short prophylactic courses are generally as effective as longer courses, supported by evidence in penetrating abdominal trauma showing no major outcome difference between 24-hour and 5-day regimens. Antibiotic levels can be altered by fluid shifts and hyperdynamic physiology, and data support higher doses for shorter durations, especially in trauma laparotomy patients. Short prophylaxis reduces infection in compound mandibular fractures. After traumatic splenectomy, the risk of early serious infection is low in isolated splenic injury but rises with greater injury and associated trauma; encapsulated organisms are key pathogens early and late. Administer pneumococcal and meningococcal vaccines once clinically stable after splenectomy. Strict infection control practices reduce hospital-acquired infections in severely injured patients.
Etiology
Trauma increases infection risk through vascular disruption and microcirculatory damage causing ischemia, edema, compartment syndromes, and necrosis; contamination of wounds and sterile spaces by soil or water exposure; post-shock immune dysfunction; reduced IgM responses after splenectomy compared with nonsplenectomized infected posttrauma patients; and additional immune suppression from corticosteroids used for head injury. Common infections in multiply injured patients include pneumonia and empyema, bacteremia or fungemia (including catheter-related), surgical site infection, intraabdominal infection, meningitis, urinary tract infection, sinus infection, wound infection, and Clostridioides difficile colitis after prior antibiotic exposure. Acinetobacter baumannii infections have been reported in injured military personnel from conflict regions, with some isolates susceptible only to carbapenems such as imipenem.
Diagnosis
History
Diagnosis is challenging because fever may be noninfectious after trauma, patients may be unable to provide history, examinations may be limited, and usual infection signs are less reliable in critically ill, multiply traumatized patients.
Physical Examination
Fever, tachycardia, and hypotension can occur after severe injury without infection. In critically ill patients, track ventilator requirements, sputum volume and character, and urine and stool output. In hospitalized trauma patients, perform a complete exam emphasizing indwelling devices, skin, operative wounds, abdomen, and respiratory findings. Inspect injured sites for local infection signs including pain, foul odor, erythema, swelling, purulent drainage, and delayed healing.
Diagnostic Tests and Interpretation
Laboratory Studies
Obtain CBC with differential, electrolytes, and kidney and liver function tests, recognizing leukocytosis may reflect trauma alone. Whenever possible, collect cultures from suspected sites before antibiotics, including blood, sputum, urine, cerebrospinal fluid studies and culture when penetrating head injury or CNS drains are present, wound cultures, and abscess cultures. With watery diarrhea and prior antibiotic exposure, test stool for C. difficile.
Imaging
Use chest radiography to assess pneumonia, especially in mechanically ventilated patients. Chest CT is more sensitive for thoracic infection in septic trauma patients and can guide correction of malpositioned or blocked thoracostomy tubes, though concurrent thoracic injuries can reduce test accuracy. Abdominal CT can identify intraabdominal infection such as perforation, colitis, cholecystitis, or abscess. For suspected extremity infection, ultrasound, CT, or MRI can help exclude abscess.
Diagnostic Procedures/Other
Image-guided or operative drainage of abscesses is diagnostic and therapeutic; send fluid for Gram stain, aerobic and anaerobic cultures, add fungal studies for abdominal or pelvic collections, and consider acid-fast bacilli smear and mycobacterial culture based on epidemiologic risk.
Differential Diagnosis
In severely injured patients, infection mimics include atelectasis, deep vein thrombosis, drug fever, allergic reactions or anaphylaxis, hypovolemia, large hematoma, sterile inflammation, pulmonary contusion, transfusion reactions, and central fever from brain injury.
Treatment
Medications
Correcting local anatomic problems such as open fractures or perforated abdominal organs is often more important than antibiotics alone. In trauma patients, unexplained hemodynamic instability not due to hypovolemia should prompt empiric antibiotics even if other infection signs are absent. Choose antibiotics based on suspected source, local resistance, trauma context (bites, water exposure, soil contamination), hospitalization duration and risk of resistant organisms, local MRSA prevalence, and allergies. If no source is identified, start broad-spectrum therapy including antistaphylococcal coverage plus broad gram-negative and anaerobic activity
.
Additional Treatment
Monitor clinical response and narrow therapy to culture and susceptibility results. If diagnostic evaluation is negative and the patient is stable, consider stopping antibiotics. Duration depends on infection site and clinical course. Remove central venous and urinary catheters as soon as they are no longer needed.
Issues for Referral
Severe injuries require urgent evaluation at experienced trauma centers with surgical and critical care capability. Infectious diseases consultation is useful when the patient is critically ill, not improving on therapy, or diagnosis remains uncertain.
Surgery/Other Procedures
Drain collections, debride necrotic tissue, and repair fractures or perforations promptly, and implement measures to mobilize respiratory secretions.
In-Patient Considerations
Initial Stabilization
Stabilize airway and circulation, provide rapid fluid resuscitation, and document all injuries.
Admission Criteria
Admit patients with penetrating injuries, fractures needing urgent repair, abnormal vital signs, impaired mental status, uncontrolled pain, or severe injuries. Burns meeting moderate to major thresholds require admission to specialized burn care centers.
Discharge Criteria
Discharge when fever has been absent for more than 24 hours, vital signs are stable, and follow-up for antibiotics and wound care is arranged.
Ongoing Care and Follow-Up
Patient Monitoring
Monitor closely for wound infection and healthcare-associated infections, which occur in a meaningful minority of hospitalized trauma patients.
Diet
Provide adequate nutritional support and consider nutrition consultation in severely injured hospitalized patients.
Patient Education
Teach warning signs of wound infection and provide clear instructions for wound care, including packing and dressing-change schedules.
Prognosis
Trauma-related infection increases mortality risk and is associated with worse functional outcomes during the year after injury compared with trauma patients without infection.
Complications
Serious outcomes include septic shock, respiratory failure, peritonitis and abdominal abscess, osteomyelitis, brain abscess, and acute acalculous cholecystitis.
- Published on
Infectious Diseases and Microbiology: Urethritis and Urethral Discharge
Basics
Description
Urethritis is inflammation of the urethra, often presenting with purulent or mucopurulent urethral discharge. In women, urethral syndrome or dysuria with sterile pyuria describes dysuria and urinary frequency with few or no bacteria detected in urine.
Approach to the Patient
Symptoms range from mild intermittent discomfort to persistent pain. History should include onset and duration of dysuria, associated symptoms, characteristics of discharge, and prior sexually transmitted infections. A complete genital examination is required. In men, palpate testes and spermatic cord to exclude epididymitis and evaluate for prostatitis; assess for cystitis in both sexes. To obtain discharge for examination, the urethra should be gently milked after the patient has avoided urination for several hours, ideally overnight.
Epidemiology
Urethritis is more common in men and represents one of the most frequently recognized sexually transmitted infections. Nongonococcal urethritis remains prevalent. Gonorrhea continues to affect adolescents and young adults disproportionately, particularly women aged 15–24 years. A substantial proportion of nongonococcal urethritis is caused by Chlamydia trachomatis. Antimicrobial resistance patterns, including quinolone-resistant Neisseria gonorrhoeae, have influenced treatment recommendations. Endourethral syphilitic chancre should also be considered in appropriate settings.
Risk Factors
Transmission risk depends on sexual exposure type. A high proportion of women exposed to men with urethral gonorrhea develop cervicitis, whereas fewer exposed men acquire infection from infected women. Incidence is highest among young, single individuals of lower socioeconomic and educational status.
General Prevention
Condom use reduces transmission of most sexually transmitted infections. Sexual partners of individuals with gonococcal or nongonococcal urethritis require evaluation and treatment to prevent reinfection and complications. Women with urinary symptoms without bacteriuria should be tested for N. gonorrhoeae. Patients diagnosed with urethritis should undergo screening for other sexually transmitted infections.
Etiology
Infectious causes include N. gonorrhoeae, C. trachomatis, Ureaplasma urealyticum, Mycoplasma genitalium, Trichomonas vaginalis, herpes simplex virus, and adenovirus. Noninfectious causes include Stevens–Johnson syndrome, granulomatosis with polyangiitis, chemical or mechanical irritation, and reactive arthritis (Reiter syndrome).
Diagnosis
Most men with urethral gonorrhea develop symptoms within days to two weeks after exposure, whereas nongonococcal urethritis typically has a 7–14 day incubation period. Dysuria is common in both conditions. Gonococcal discharge is usually purulent; nongonococcal discharge is less often purulent. Acute urethral syndrome presents with dysuria, urgency, and frequency.
Diagnostic Tests and Interpretation
Laboratory Studies
Gram-stained urethral smear showing five or more neutrophils per high-power field supports urethritis. Intracellular gram-negative diplococci confirm gonorrhea. Absence of diplococci suggests nongonococcal urethritis. Gram stain has high sensitivity for gonococcal infection in symptomatic men. First-void urine sediment may also demonstrate inflammatory cells. Nucleic acid amplification testing for N. gonorrhoeae and C. trachomatis is highly sensitive and specific and is recommended to guide patient and partner management. Candida has occasionally been implicated in urethritis when no other pathogen is identified.
Differential Diagnosis
Exclude systemic complications such as disseminated gonococcal infection or reactive arthritis. Consider bacterial prostatitis, cystitis, and in women, pyelonephritis if fever or flank pain is present. In sterile pyuria, evaluate for sexually transmitted pathogens such as C. trachomatis and N. gonorrhoeae, as well as other causes including tuberculosis or prostatitis.
Treatment
Medications
Gonococcal urethritis requires ceftriaxone in a single intramuscular dose, and most patients should also receive therapy targeting chlamydia. Nongonococcal urethritis is treated with doxycycline for seven days or a single dose of azithromycin. Alternative regimens include oral cephalosporins or spectinomycin where available. Fluoroquinolones are no longer recommended for gonorrhea due to resistance. Persistent or recurrent symptoms warrant reassessment for reinfection, treatment nonadherence, resistant strains, or coinfection such as T. vaginalis, which may require metronidazole. Recurrent nongonococcal urethritis may need prolonged therapy and evaluation for prostatic or structural abnormalities.
Ongoing Care and Follow-Up
Persistent hematuria after treatment requires urologic evaluation. Recurrence may reflect reinfection, coinfection, or treatment failure.
Complications
Chlamydia can cause salpingitis or bartholinitis and may result in neonatal conjunctivitis or pneumonia. Ureaplasma carriage has been associated with infertility. Both N. gonorrhoeae and C. trachomatis can cause acute epididymitis.
Basics
Description
Urethritis is inflammation of the urethra, often presenting with purulent or mucopurulent urethral discharge. In women, urethral syndrome or dysuria with sterile pyuria describes dysuria and urinary frequency with few or no bacteria detected in urine.
Approach to the Patient
Symptoms range from mild intermittent discomfort to persistent pain. History should include onset and duration of dysuria, associated symptoms, characteristics of discharge, and prior sexually transmitted infections. A complete genital examination is required. In men, palpate testes and spermatic cord to exclude epididymitis and evaluate for prostatitis; assess for cystitis in both sexes. To obtain discharge for examination, the urethra should be gently milked after the patient has avoided urination for several hours, ideally overnight.
Epidemiology
Urethritis is more common in men and represents one of the most frequently recognized sexually transmitted infections. Nongonococcal urethritis remains prevalent. Gonorrhea continues to affect adolescents and young adults disproportionately, particularly women aged 15–24 years. A substantial proportion of nongonococcal urethritis is caused by Chlamydia trachomatis. Antimicrobial resistance patterns, including quinolone-resistant Neisseria gonorrhoeae, have influenced treatment recommendations. Endourethral syphilitic chancre should also be considered in appropriate settings.
Risk Factors
Transmission risk depends on sexual exposure type. A high proportion of women exposed to men with urethral gonorrhea develop cervicitis, whereas fewer exposed men acquire infection from infected women. Incidence is highest among young, single individuals of lower socioeconomic and educational status.
General Prevention
Condom use reduces transmission of most sexually transmitted infections. Sexual partners of individuals with gonococcal or nongonococcal urethritis require evaluation and treatment to prevent reinfection and complications. Women with urinary symptoms without bacteriuria should be tested for N. gonorrhoeae. Patients diagnosed with urethritis should undergo screening for other sexually transmitted infections.
Etiology
Infectious causes include N. gonorrhoeae, C. trachomatis, Ureaplasma urealyticum, Mycoplasma genitalium, Trichomonas vaginalis, herpes simplex virus, and adenovirus. Noninfectious causes include Stevens–Johnson syndrome, granulomatosis with polyangiitis, chemical or mechanical irritation, and reactive arthritis (Reiter syndrome).
Diagnosis
Most men with urethral gonorrhea develop symptoms within days to two weeks after exposure, whereas nongonococcal urethritis typically has a 7–14 day incubation period. Dysuria is common in both conditions. Gonococcal discharge is usually purulent; nongonococcal discharge is less often purulent. Acute urethral syndrome presents with dysuria, urgency, and frequency.
Diagnostic Tests and Interpretation
Laboratory Studies
Gram-stained urethral smear showing five or more neutrophils per high-power field supports urethritis. Intracellular gram-negative diplococci confirm gonorrhea. Absence of diplococci suggests nongonococcal urethritis. Gram stain has high sensitivity for gonococcal infection in symptomatic men. First-void urine sediment may also demonstrate inflammatory cells. Nucleic acid amplification testing for N. gonorrhoeae and C. trachomatis is highly sensitive and specific and is recommended to guide patient and partner management. Candida has occasionally been implicated in urethritis when no other pathogen is identified.
Differential Diagnosis
Exclude systemic complications such as disseminated gonococcal infection or reactive arthritis. Consider bacterial prostatitis, cystitis, and in women, pyelonephritis if fever or flank pain is present. In sterile pyuria, evaluate for sexually transmitted pathogens such as C. trachomatis and N. gonorrhoeae, as well as other causes including tuberculosis or prostatitis.
Treatment
Medications
Gonococcal urethritis requires ceftriaxone in a single intramuscular dose, and most patients should also receive therapy targeting chlamydia. Nongonococcal urethritis is treated with doxycycline for seven days or a single dose of azithromycin. Alternative regimens include oral cephalosporins or spectinomycin where available. Fluoroquinolones are no longer recommended for gonorrhea due to resistance. Persistent or recurrent symptoms warrant reassessment for reinfection, treatment nonadherence, resistant strains, or coinfection such as T. vaginalis, which may require metronidazole. Recurrent nongonococcal urethritis may need prolonged therapy and evaluation for prostatic or structural abnormalities.
Ongoing Care and Follow-Up
Persistent hematuria after treatment requires urologic evaluation. Recurrence may reflect reinfection, coinfection, or treatment failure.
Complications
Chlamydia can cause salpingitis or bartholinitis and may result in neonatal conjunctivitis or pneumonia. Ureaplasma carriage has been associated with infertility. Both N. gonorrhoeae and C. trachomatis can cause acute epididymitis.
- Published on
Infectious Disease and Microbiology – Adenovirus Infections
Adenovirus infections are caused by nonenveloped, double-stranded DNA viruses measuring approximately 70–80 nm in diameter. Human adenoviruses belong to the genus Mastadenovirus and include more than 50 serotypes. These viruses possess an icosahedral capsid composed of 20 triangular faces and 12 vertices. The genome consists of linear double-stranded DNA encoding structural and nonstructural proteins. Infection may result in either lytic replication or latent persistence, and certain serotypes have demonstrated oncogenic potential in animal models.
Adenoviruses contribute to a proportion of viral respiratory illnesses. Although rhinoviruses are the most common cause of acute respiratory infections, adenoviruses account for up to 5% of respiratory infections in children and fewer than 2% in adults. Infections occur most frequently from fall through spring. Transmission occurs via inhalation of aerosolized particles, direct inoculation of conjunctival mucosa, and possibly via the fecal–oral route. Outbreaks of acute respiratory disease due to specific serotypes are well documented among military recruits, particularly in winter and spring. Following infection, type-specific antibodies develop and provide protection against reinfection with the same serotype. Severe or disseminated disease may occur in immunocompromised individuals, including patients with AIDS, solid-organ or bone marrow transplant recipients, and children with congenital immunodeficiencies.
In children, adenovirus commonly causes acute upper respiratory tract infection characterized by prominent rhinitis. Lower respiratory involvement, including bronchiolitis and pneumonia, may occur. Pharyngoconjunctival fever is a distinctive syndrome seen in outbreaks, particularly in summer camps, presenting with low-grade fever for 3–5 days followed by rhinitis, sore throat, cervical lymphadenopathy, and conjunctivitis, typically resolving within 1–2 weeks. Adenovirus also causes pharyngitis and, in young children, acute diarrheal illness. Other manifestations include hemorrhagic cystitis and epidemic keratoconjunctivitis. In adults, acute respiratory disease presents with sore throat, gradual onset of fever that may reach 39°C, cough, coryza, and lymphadenopathy. In immunocompromised patients, adenovirus pneumonia may present abruptly with fever, rigors, malaise, nonproductive cough, gastrointestinal symptoms, headache, and arthralgia.
Physical examination may reveal pharyngeal edema, injection, and tonsillar enlargement with minimal exudate. Ocular involvement presents with conjunctival injection and discharge. In immunocompromised hosts, localizing findings may be minimal despite severe disease.
Definitive diagnosis is established by viral culture or detection of adenovirus from conjunctival, oropharyngeal, sputum, urine, or stool specimens. Viral cytopathic effects in tissue culture can be confirmed by immunofluorescence or other immunologic assays. Certain enteric adenovirus types require specialized cell lines or direct ELISA testing of stool. Serologic diagnosis may demonstrate rising antibody titers using complement fixation, neutralization assays, ELISA, or radioimmunoassay. In adenovirus pneumonia, chest radiography often shows bilateral diffuse interstitial infiltrates and occasionally pleural effusions. The clinical presentation is frequently indistinguishable from other viral respiratory infections or Mycoplasma pneumoniae.
Management is primarily supportive, as no specific antiviral therapy is routinely indicated for immunocompetent patients. Live oral vaccines targeting adenovirus types 4 and 7 are used in military settings to prevent outbreaks. In immunocompromised individuals with severe infection, treatment with cidofovir and intravenous immunoglobulin has shown benefit in some cases. Intravenous gamma globulin and type-specific antibodies may also be helpful. Ribavirin and ganciclovir have been used in selected cases, although evidence remains limited.
In transplant recipients and other immunocompromised patients, adenovirus pneumonia carries significant morbidity and mortality, which may exceed 60%, underscoring the importance of early recognition and supportive management.
Adenovirus infections are caused by nonenveloped, double-stranded DNA viruses measuring approximately 70–80 nm in diameter. Human adenoviruses belong to the genus Mastadenovirus and include more than 50 serotypes. These viruses possess an icosahedral capsid composed of 20 triangular faces and 12 vertices. The genome consists of linear double-stranded DNA encoding structural and nonstructural proteins. Infection may result in either lytic replication or latent persistence, and certain serotypes have demonstrated oncogenic potential in animal models.
Adenoviruses contribute to a proportion of viral respiratory illnesses. Although rhinoviruses are the most common cause of acute respiratory infections, adenoviruses account for up to 5% of respiratory infections in children and fewer than 2% in adults. Infections occur most frequently from fall through spring. Transmission occurs via inhalation of aerosolized particles, direct inoculation of conjunctival mucosa, and possibly via the fecal–oral route. Outbreaks of acute respiratory disease due to specific serotypes are well documented among military recruits, particularly in winter and spring. Following infection, type-specific antibodies develop and provide protection against reinfection with the same serotype. Severe or disseminated disease may occur in immunocompromised individuals, including patients with AIDS, solid-organ or bone marrow transplant recipients, and children with congenital immunodeficiencies.
In children, adenovirus commonly causes acute upper respiratory tract infection characterized by prominent rhinitis. Lower respiratory involvement, including bronchiolitis and pneumonia, may occur. Pharyngoconjunctival fever is a distinctive syndrome seen in outbreaks, particularly in summer camps, presenting with low-grade fever for 3–5 days followed by rhinitis, sore throat, cervical lymphadenopathy, and conjunctivitis, typically resolving within 1–2 weeks. Adenovirus also causes pharyngitis and, in young children, acute diarrheal illness. Other manifestations include hemorrhagic cystitis and epidemic keratoconjunctivitis. In adults, acute respiratory disease presents with sore throat, gradual onset of fever that may reach 39°C, cough, coryza, and lymphadenopathy. In immunocompromised patients, adenovirus pneumonia may present abruptly with fever, rigors, malaise, nonproductive cough, gastrointestinal symptoms, headache, and arthralgia.
Physical examination may reveal pharyngeal edema, injection, and tonsillar enlargement with minimal exudate. Ocular involvement presents with conjunctival injection and discharge. In immunocompromised hosts, localizing findings may be minimal despite severe disease.
Definitive diagnosis is established by viral culture or detection of adenovirus from conjunctival, oropharyngeal, sputum, urine, or stool specimens. Viral cytopathic effects in tissue culture can be confirmed by immunofluorescence or other immunologic assays. Certain enteric adenovirus types require specialized cell lines or direct ELISA testing of stool. Serologic diagnosis may demonstrate rising antibody titers using complement fixation, neutralization assays, ELISA, or radioimmunoassay. In adenovirus pneumonia, chest radiography often shows bilateral diffuse interstitial infiltrates and occasionally pleural effusions. The clinical presentation is frequently indistinguishable from other viral respiratory infections or Mycoplasma pneumoniae.
Management is primarily supportive, as no specific antiviral therapy is routinely indicated for immunocompetent patients. Live oral vaccines targeting adenovirus types 4 and 7 are used in military settings to prevent outbreaks. In immunocompromised individuals with severe infection, treatment with cidofovir and intravenous immunoglobulin has shown benefit in some cases. Intravenous gamma globulin and type-specific antibodies may also be helpful. Ribavirin and ganciclovir have been used in selected cases, although evidence remains limited.
In transplant recipients and other immunocompromised patients, adenovirus pneumonia carries significant morbidity and mortality, which may exceed 60%, underscoring the importance of early recognition and supportive management.
- Published on
Infectious Diseases and Microbiology: Vaginal Discharge / Vaginitis
Vaginal discharge may be physiologic or pathologic. Normal vaginal discharge, also referred to as leukorrhea, consists of cervical mucus and desquamated epithelial cells and is not associated with irritation, odor, or discomfort. In contrast, pathologic discharge is usually associated with infection and may present with abnormal color due to increased polymorphonuclear leukocytes, increased volume, malodor, vulvar pruritus, burning, dysuria, or dyspareunia. The three most common infectious causes of vaginitis are bacterial vaginosis, trichomoniasis, and candidiasis. Bacterial vaginosis represents a disruption of normal vaginal flora in which hydrogen-peroxide–producing lactobacilli are replaced by anaerobic organisms, mycoplasmas, and Gardnerella vaginalis.
Evaluation begins with a detailed history focusing on the characteristics of the discharge, associated symptoms, prior similar episodes, and a complete sexual history. Office-based diagnostic evaluation includes measurement of vaginal pH, performance of the amine (“whiff”) test by adding 10% potassium hydroxide to vaginal secretions, and microscopic examination of saline wet mount preparations to identify clue cells, motile trichomonads, and white blood cells. A potassium hydroxide preparation may reveal Candida pseudohyphae. In sexually active women, both endocervical and high vaginal swabs should be obtained. Chlamydial testing requires sampling of the squamocolumnar junction for culture or nucleic acid amplification testing. Screening cultures may include selective media for Neisseria gonorrhoeae, Candida species, and beta-hemolytic streptococci.
Bacterial vaginosis is the most common cause of vulvovaginal symptoms, followed by vulvovaginal candidiasis. Trichomoniasis is less common in developed countries. Risk factors for vaginal infections include unprotected sexual contact, multiple sexual partners, young age, and certain socioeconomic factors. Bacterial vaginosis is particularly associated with new or multiple sexual partners.
Clinically, vulvovaginal candidiasis often presents with vulvar pruritus and burning, dysuria at the urethral orifice, vaginal erythema, and occasionally thick, white, curd-like discharge. However, only a minority of patients exhibit the classic discharge. Trichomoniasis commonly presents with malodorous yellow discharge, vulvar erythema, itching, dysuria, urinary frequency, and dyspareunia, although symptoms are nonspecific. Bacterial vaginosis typically produces a thin, homogeneous discharge with a characteristic fishy odor that may be more noticeable after intercourse. In the absence of identifiable pathogens, vulvar inflammation may reflect noninfectious irritation or allergic reactions.
Diagnosis of trichomoniasis is commonly made by identifying motile organisms on saline wet mount, although sensitivity is moderate. Direct immunofluorescent testing and culture are more sensitive when available. Candidiasis is diagnosed by microscopic identification of budding yeast or pseudohyphae on saline or potassium hydroxide preparation. Vaginal pH in candidiasis is typically normal (≤4.5), and the amine test is negative. The presence of white blood cells without yeast or trichomonads suggests cervicitis. Absence of organisms on microscopy does not exclude infection, as culture or PCR may be required.
Treatment depends on the identified etiology. Trichomoniasis is treated with a single 2 g oral dose of metronidazole. Bacterial vaginosis is treated with oral metronidazole 500 mg twice daily for seven days or clindamycin 300 mg twice daily for seven days. Intravaginal metronidazole gel or clindamycin cream are effective alternatives. Symptomatic candidiasis is treated primarily with intravaginal azole antifungals such as clotrimazole, miconazole, butoconazole, or terconazole. Oral fluconazole as a single dose is an alternative but is more costly. In pregnancy, intravaginal azoles may be used after the first trimester.
Recurrent vulvovaginal candidiasis, defined as four or more episodes per year, may occur more frequently in women with diabetes mellitus or HIV infection. Vaginal trichomoniasis and bacterial vaginosis during pregnancy are associated with increased risk of preterm labor. Bacterial vaginosis is also associated with pelvic infections, postoperative endometritis, neonatal sepsis, increased risk of HIV acquisition and transmission, and increased susceptibility to other sexually transmitted infections.
Vaginal discharge may be physiologic or pathologic. Normal vaginal discharge, also referred to as leukorrhea, consists of cervical mucus and desquamated epithelial cells and is not associated with irritation, odor, or discomfort. In contrast, pathologic discharge is usually associated with infection and may present with abnormal color due to increased polymorphonuclear leukocytes, increased volume, malodor, vulvar pruritus, burning, dysuria, or dyspareunia. The three most common infectious causes of vaginitis are bacterial vaginosis, trichomoniasis, and candidiasis. Bacterial vaginosis represents a disruption of normal vaginal flora in which hydrogen-peroxide–producing lactobacilli are replaced by anaerobic organisms, mycoplasmas, and Gardnerella vaginalis.
Evaluation begins with a detailed history focusing on the characteristics of the discharge, associated symptoms, prior similar episodes, and a complete sexual history. Office-based diagnostic evaluation includes measurement of vaginal pH, performance of the amine (“whiff”) test by adding 10% potassium hydroxide to vaginal secretions, and microscopic examination of saline wet mount preparations to identify clue cells, motile trichomonads, and white blood cells. A potassium hydroxide preparation may reveal Candida pseudohyphae. In sexually active women, both endocervical and high vaginal swabs should be obtained. Chlamydial testing requires sampling of the squamocolumnar junction for culture or nucleic acid amplification testing. Screening cultures may include selective media for Neisseria gonorrhoeae, Candida species, and beta-hemolytic streptococci.
Bacterial vaginosis is the most common cause of vulvovaginal symptoms, followed by vulvovaginal candidiasis. Trichomoniasis is less common in developed countries. Risk factors for vaginal infections include unprotected sexual contact, multiple sexual partners, young age, and certain socioeconomic factors. Bacterial vaginosis is particularly associated with new or multiple sexual partners.
Clinically, vulvovaginal candidiasis often presents with vulvar pruritus and burning, dysuria at the urethral orifice, vaginal erythema, and occasionally thick, white, curd-like discharge. However, only a minority of patients exhibit the classic discharge. Trichomoniasis commonly presents with malodorous yellow discharge, vulvar erythema, itching, dysuria, urinary frequency, and dyspareunia, although symptoms are nonspecific. Bacterial vaginosis typically produces a thin, homogeneous discharge with a characteristic fishy odor that may be more noticeable after intercourse. In the absence of identifiable pathogens, vulvar inflammation may reflect noninfectious irritation or allergic reactions.
Diagnosis of trichomoniasis is commonly made by identifying motile organisms on saline wet mount, although sensitivity is moderate. Direct immunofluorescent testing and culture are more sensitive when available. Candidiasis is diagnosed by microscopic identification of budding yeast or pseudohyphae on saline or potassium hydroxide preparation. Vaginal pH in candidiasis is typically normal (≤4.5), and the amine test is negative. The presence of white blood cells without yeast or trichomonads suggests cervicitis. Absence of organisms on microscopy does not exclude infection, as culture or PCR may be required.
Treatment depends on the identified etiology. Trichomoniasis is treated with a single 2 g oral dose of metronidazole. Bacterial vaginosis is treated with oral metronidazole 500 mg twice daily for seven days or clindamycin 300 mg twice daily for seven days. Intravaginal metronidazole gel or clindamycin cream are effective alternatives. Symptomatic candidiasis is treated primarily with intravaginal azole antifungals such as clotrimazole, miconazole, butoconazole, or terconazole. Oral fluconazole as a single dose is an alternative but is more costly. In pregnancy, intravaginal azoles may be used after the first trimester.
Recurrent vulvovaginal candidiasis, defined as four or more episodes per year, may occur more frequently in women with diabetes mellitus or HIV infection. Vaginal trichomoniasis and bacterial vaginosis during pregnancy are associated with increased risk of preterm labor. Bacterial vaginosis is also associated with pelvic infections, postoperative endometritis, neonatal sepsis, increased risk of HIV acquisition and transmission, and increased susceptibility to other sexually transmitted infections.
- Published on
Infectious Disease and Microbiology – Actinomycosis
Actinomycosis is a chronic, slowly progressive, suppurative, and tissue-destructive infection characterized by mass-like lesions and sinus tract formation. It most commonly affects the head and neck region but may also involve the thorax, abdomen, pelvis, central nervous system, bones, and soft tissues. The disease is indolent and often mimics malignancy or other chronic infections.
The reported incidence is approximately 1 per 300,000 population in the United States and about 1 per 100,000 in Europe. It occurs at all ages, with peak frequency in middle-aged adults, and has a male-to-female ratio of about 3:1. Risk factors include poor oral hygiene, dental manipulation, oral trauma, intrauterine contraceptive device (especially when used for more than 2 years), abdominal surgery, appendicitis, diverticulitis, foreign bodies, malnutrition, and immunodeficiency such as HIV infection, chronic granulomatous disease, or prolonged corticosteroid therapy. Cases have also been described in osteoradionecrosis and bisphosphonate-related mandibular osteonecrosis. Prevention includes maintaining good oral hygiene and, in women with long-term intrauterine devices and suspicious symptoms, device removal with short-term antibiotic therapy. Patient isolation is not required.
Humans are the natural reservoir. The organisms colonize the oral cavity, particularly dental plaque and tonsillar crypts, as commensals. Infection typically follows disruption of the mucosal barrier due to trauma or surgery, allowing invasion into deeper tissues. The disease spreads contiguously and occasionally hematogenously. Aspiration may lead to thoracic involvement, while abdominal and pelvic disease often follows bowel perforation, appendicitis, or diverticulitis. Although incubation is unclear, diagnosis is usually delayed because of the chronic course. Clinical forms include cervicofacial, thoracic, abdominal, pelvic, central nervous system, and disseminated disease.
Actinomyces species are microaerophilic or anaerobic, filamentous, branched, Gram-positive, non–acid-fast rods. Actinomyces israelii is the most frequently identified species, although A. naeslundii, A. meyeri, A. odontolyticus, and Propionibacterium propionica have also been implicated. These organisms are normal flora of the oral cavity and female genital tract. Most infections are polymicrobial, often involving anaerobic oral flora that may act as copathogens.
Clinical presentation varies by site. Patients may have low-grade fever, weight loss, and pain. Cervicofacial disease often presents with perimandibular swelling, trismus, and purplish discoloration of overlying skin, with sinus tract formation draining characteristic yellow “sulfur granules.” Thoracic disease presents with cough, chest pain, dyspnea, mass-like lesions, pleural thickening, empyema, chest wall invasion, and possible mediastinal or spinal involvement. Abdominal disease typically manifests as a firm mass, often in the right iliac fossa following appendicitis, or in the left lower quadrant after diverticulitis, sometimes with chronic perianal abscesses and fistulae. Pelvic disease may present as abscesses or a “frozen pelvis.” Central nervous system involvement causes focal neurologic deficits or chronic meningitis.
Diagnosis requires high suspicion, especially when mass lesions coexist with draining sinuses and sulfur granules. Specimens should be obtained before antibiotic therapy. Gram stain of pus or tissue from sterile sites demonstrating filamentous, Gram-positive, non–acid-fast organisms is more sensitive than culture. Swab cultures are not recommended, and specimens must be processed anaerobically. Direct immunofluorescence may assist in specific cases. Imaging with CT or MRI helps determine disease extent. Lung disease may show the “open bronchus sign.” Bone involvement may demonstrate a saw-toothed appearance, and CNS disease often appears as single or multiloculated lesions with surrounding edema. Differential diagnosis includes malignancy, nocardiosis, tuberculosis, botryomycosis, and endemic fungal infections.
Treatment consists of prolonged high-dose penicillin therapy. Recommended first-line therapy includes intravenous penicillin G (10–24 million units daily in divided doses) for 2–6 weeks, followed by oral penicillin V for 6–12 months, or intravenous ampicillin followed by oral amoxicillin for similar duration. Mild cervicofacial disease may be treated with oral therapy alone. Alternatives for penicillin-allergic patients include tetracyclines, erythromycin, or clindamycin. Surgical intervention, including abscess drainage or excision of fibrotic tissue, is often necessary.
Prognosis is generally excellent with appropriate prolonged therapy, as resistance among Actinomyces species is rare. Treatment failure usually suggests an undrained abscess or presence of resistant copathogens. Potential complications include disseminated disease and bowel obstruction in extensive abdominal or pelvic involvement.
Actinomycosis is a chronic, slowly progressive, suppurative, and tissue-destructive infection characterized by mass-like lesions and sinus tract formation. It most commonly affects the head and neck region but may also involve the thorax, abdomen, pelvis, central nervous system, bones, and soft tissues. The disease is indolent and often mimics malignancy or other chronic infections.
The reported incidence is approximately 1 per 300,000 population in the United States and about 1 per 100,000 in Europe. It occurs at all ages, with peak frequency in middle-aged adults, and has a male-to-female ratio of about 3:1. Risk factors include poor oral hygiene, dental manipulation, oral trauma, intrauterine contraceptive device (especially when used for more than 2 years), abdominal surgery, appendicitis, diverticulitis, foreign bodies, malnutrition, and immunodeficiency such as HIV infection, chronic granulomatous disease, or prolonged corticosteroid therapy. Cases have also been described in osteoradionecrosis and bisphosphonate-related mandibular osteonecrosis. Prevention includes maintaining good oral hygiene and, in women with long-term intrauterine devices and suspicious symptoms, device removal with short-term antibiotic therapy. Patient isolation is not required.
Humans are the natural reservoir. The organisms colonize the oral cavity, particularly dental plaque and tonsillar crypts, as commensals. Infection typically follows disruption of the mucosal barrier due to trauma or surgery, allowing invasion into deeper tissues. The disease spreads contiguously and occasionally hematogenously. Aspiration may lead to thoracic involvement, while abdominal and pelvic disease often follows bowel perforation, appendicitis, or diverticulitis. Although incubation is unclear, diagnosis is usually delayed because of the chronic course. Clinical forms include cervicofacial, thoracic, abdominal, pelvic, central nervous system, and disseminated disease.
Actinomyces species are microaerophilic or anaerobic, filamentous, branched, Gram-positive, non–acid-fast rods. Actinomyces israelii is the most frequently identified species, although A. naeslundii, A. meyeri, A. odontolyticus, and Propionibacterium propionica have also been implicated. These organisms are normal flora of the oral cavity and female genital tract. Most infections are polymicrobial, often involving anaerobic oral flora that may act as copathogens.
Clinical presentation varies by site. Patients may have low-grade fever, weight loss, and pain. Cervicofacial disease often presents with perimandibular swelling, trismus, and purplish discoloration of overlying skin, with sinus tract formation draining characteristic yellow “sulfur granules.” Thoracic disease presents with cough, chest pain, dyspnea, mass-like lesions, pleural thickening, empyema, chest wall invasion, and possible mediastinal or spinal involvement. Abdominal disease typically manifests as a firm mass, often in the right iliac fossa following appendicitis, or in the left lower quadrant after diverticulitis, sometimes with chronic perianal abscesses and fistulae. Pelvic disease may present as abscesses or a “frozen pelvis.” Central nervous system involvement causes focal neurologic deficits or chronic meningitis.
Diagnosis requires high suspicion, especially when mass lesions coexist with draining sinuses and sulfur granules. Specimens should be obtained before antibiotic therapy. Gram stain of pus or tissue from sterile sites demonstrating filamentous, Gram-positive, non–acid-fast organisms is more sensitive than culture. Swab cultures are not recommended, and specimens must be processed anaerobically. Direct immunofluorescence may assist in specific cases. Imaging with CT or MRI helps determine disease extent. Lung disease may show the “open bronchus sign.” Bone involvement may demonstrate a saw-toothed appearance, and CNS disease often appears as single or multiloculated lesions with surrounding edema. Differential diagnosis includes malignancy, nocardiosis, tuberculosis, botryomycosis, and endemic fungal infections.
Treatment consists of prolonged high-dose penicillin therapy. Recommended first-line therapy includes intravenous penicillin G (10–24 million units daily in divided doses) for 2–6 weeks, followed by oral penicillin V for 6–12 months, or intravenous ampicillin followed by oral amoxicillin for similar duration. Mild cervicofacial disease may be treated with oral therapy alone. Alternatives for penicillin-allergic patients include tetracyclines, erythromycin, or clindamycin. Surgical intervention, including abscess drainage or excision of fibrotic tissue, is often necessary.
Prognosis is generally excellent with appropriate prolonged therapy, as resistance among Actinomyces species is rare. Treatment failure usually suggests an undrained abscess or presence of resistant copathogens. Potential complications include disseminated disease and bowel obstruction in extensive abdominal or pelvic involvement.
- Published on
Infectious Disease and Microbiology – Acne Vulgaris
Acne vulgaris (common acne) is a chronic inflammatory disorder of the pilosebaceous unit, particularly the sebaceous follicles. It is characterized by comedones, papules, pustules, nodules, and in more severe cases, scarring. The condition primarily affects areas rich in sebaceous glands, including the face, neck, chest, upper back, and upper arms.
Acne is one of the most common skin diseases, affecting more than 85% of individuals at some point between adolescence and early adulthood, with a mean age of approximately 24 years. It accounts for up to 2 million office visits annually among adolescents aged 15–19 years. A major risk factor is increased responsiveness of sebaceous glands and keratinocytes to androgenic hormones, particularly during puberty. Elevated androgen levels such as testosterone, dehydroepiandrosterone sulfate (DHEAS), or androstenedione may worsen acne severity, especially in women.
The pathophysiology involves inflammatory changes within sebaceous follicles, leading to accumulation of lipid-rich sebum and proliferation of Cutibacterium acnes (formerly Propionibacterium acnes), a Gram-positive anaerobic bacterium that normally exists in low numbers on the skin. Overgrowth of this organism within the follicle triggers inflammation, follicular rupture, and extension of inflammation into the surrounding dermis. This process results in the formation of papules, pustules, and nodules.
Clinically, patients present with open comedones (blackheads) or closed comedones (whiteheads). As inflammation progresses, lesions may become painful and form pustules or nodules. Scarring suggests more aggressive disease. Acne is classified as mild when primarily noninflammatory comedones are present, moderate when inflammatory papules and pustules affect larger skin areas, and severe when large painful nodules with potential scarring are present.
Treatment depends on severity. Mild to moderate acne often responds to topical therapy, including retinoids, benzoyl peroxide, and topical antimicrobials. Retinoids reduce sebaceous gland activity and normalize follicular keratinization. Benzoyl peroxide acts as a bactericidal agent and is often combined with topical antibiotics to reduce resistance. More severe cases may require oral antibiotics such as doxycycline, minocycline, tetracycline, trimethoprim-sulfamethoxazole, erythromycin, or clindamycin, although resistance has become increasingly common.
For severe nodulocystic acne or cases associated with scarring, oral isotretinoin is indicated. It reduces sebaceous gland size and sebum production, inhibits bacterial growth, and has anti-inflammatory properties. However, isotretinoin is highly teratogenic and may cause hypertriglyceridemia. Women of childbearing age must use two forms of contraception during treatment. Reports have also suggested possible associations with mood changes.
Additional therapies may include spironolactone or oral contraceptives in patients with hyperandrogenism. Intralesional corticosteroids can be used for severe inflammatory nodules. With appropriate treatment and adherence, most patients experience significant improvement, and early management helps reduce the risk of permanent scarring.
Acne vulgaris (common acne) is a chronic inflammatory disorder of the pilosebaceous unit, particularly the sebaceous follicles. It is characterized by comedones, papules, pustules, nodules, and in more severe cases, scarring. The condition primarily affects areas rich in sebaceous glands, including the face, neck, chest, upper back, and upper arms.
Acne is one of the most common skin diseases, affecting more than 85% of individuals at some point between adolescence and early adulthood, with a mean age of approximately 24 years. It accounts for up to 2 million office visits annually among adolescents aged 15–19 years. A major risk factor is increased responsiveness of sebaceous glands and keratinocytes to androgenic hormones, particularly during puberty. Elevated androgen levels such as testosterone, dehydroepiandrosterone sulfate (DHEAS), or androstenedione may worsen acne severity, especially in women.
The pathophysiology involves inflammatory changes within sebaceous follicles, leading to accumulation of lipid-rich sebum and proliferation of Cutibacterium acnes (formerly Propionibacterium acnes), a Gram-positive anaerobic bacterium that normally exists in low numbers on the skin. Overgrowth of this organism within the follicle triggers inflammation, follicular rupture, and extension of inflammation into the surrounding dermis. This process results in the formation of papules, pustules, and nodules.
Clinically, patients present with open comedones (blackheads) or closed comedones (whiteheads). As inflammation progresses, lesions may become painful and form pustules or nodules. Scarring suggests more aggressive disease. Acne is classified as mild when primarily noninflammatory comedones are present, moderate when inflammatory papules and pustules affect larger skin areas, and severe when large painful nodules with potential scarring are present.
Treatment depends on severity. Mild to moderate acne often responds to topical therapy, including retinoids, benzoyl peroxide, and topical antimicrobials. Retinoids reduce sebaceous gland activity and normalize follicular keratinization. Benzoyl peroxide acts as a bactericidal agent and is often combined with topical antibiotics to reduce resistance. More severe cases may require oral antibiotics such as doxycycline, minocycline, tetracycline, trimethoprim-sulfamethoxazole, erythromycin, or clindamycin, although resistance has become increasingly common.
For severe nodulocystic acne or cases associated with scarring, oral isotretinoin is indicated. It reduces sebaceous gland size and sebum production, inhibits bacterial growth, and has anti-inflammatory properties. However, isotretinoin is highly teratogenic and may cause hypertriglyceridemia. Women of childbearing age must use two forms of contraception during treatment. Reports have also suggested possible associations with mood changes.
Additional therapies may include spironolactone or oral contraceptives in patients with hyperandrogenism. Intralesional corticosteroids can be used for severe inflammatory nodules. With appropriate treatment and adherence, most patients experience significant improvement, and early management helps reduce the risk of permanent scarring.
- Published on
Infectious Disease and Microbiology – Aspergillosis
Aspergillosis describes a spectrum of illnesses caused by species of Aspergillus, ranging from simple colonization or allergic reactions to localized or disseminated invasive disease. Although virtually any organ may be involved, the lungs are most commonly affected, followed by the paranasal sinuses and, less frequently, the central nervous system.
The number of Aspergillus species implicated in human disease continues to expand. Aspergillus fumigatus remains the most common cause of invasive infection, but A. flavus, A. terreus, A. niger, and A. versicolor are increasingly recognized. Invasive aspergillosis is second only to candidiasis among invasive fungal infections in immunocompromised patients. Major risk factors include granulocytopenia (the most significant), hematopoietic stem cell transplantation, solid-organ transplantation, acute leukemia, prolonged corticosteroid or cytotoxic therapy, chronic obstructive pulmonary disease treated with steroids, prolonged antibiotic use, liver failure, diabetes mellitus, chronic granulomatous disease, and advanced AIDS (CD4 count ≤50 cells/mm³). Genetic polymorphisms in Toll-like receptors 4 and 9 may influence susceptibility to invasive aspergillosis and allergic bronchopulmonary aspergillosis (ABPA), respectively.
Preventive strategies focus on environmental control, particularly during hospital construction activities, to reduce exposure to airborne conidia. High-efficiency particulate air (HEPA) filtration systems are recommended for high-risk patients. In selected individuals with prior invasive disease who may become neutropenic, antifungal prophylaxis with agents such as voriconazole or amphotericin B may be considered.
Pathophysiologically, inhaled conidia are small enough to reach the alveoli. In immunocompetent hosts, alveolar macrophages clear the spores. In immunocompromised individuals, impaired macrophage function allows germination into hyphae, triggering inflammatory cytokine release, vascular invasion, tissue necrosis, and possible hematogenous dissemination. In ABPA, colonization in atopic individuals activates TH2 CD4+ T cells, driving IgE production and eosinophilia, exacerbating asthma and potentially leading to bronchiectasis. Chronic pulmonary aspergillosis, including aspergilloma formation, often develops in patients with prior lung disease such as tuberculosis, lung cancer resection, ABPA, or bullous disease.
Clinical manifestations vary by syndrome. ABPA occurs in patients with asthma or cystic fibrosis and presents with worsening respiratory symptoms, malaise, and occasionally hemoptysis. Chronic pulmonary aspergillosis typically presents with weight loss, chronic cough, hemoptysis, dyspnea, and constitutional symptoms. Invasive aspergillosis commonly presents with fever, pleuritic chest pain, cough, dyspnea, and hemoptysis, especially in neutropenic or otherwise immunocompromised hosts.
Diagnosis depends on clinical suspicion and supportive laboratory and imaging findings. In ABPA, chest imaging may show upper-lobe infiltrates, bronchial wall thickening, bronchiectasis, or ground-glass opacities. Peripheral eosinophilia, elevated total serum IgE, positive immediate skin test to Aspergillus, and elevated serum IgG to A. fumigatus support the diagnosis. Chronic pulmonary aspergillosis is characterized radiographically by one or more lung cavities, sometimes containing a mobile aspergilloma with an air-crescent sign. Invasive aspergillosis requires demonstration of fungal invasion on tissue biopsy for definitive diagnosis. Serum galactomannan and β-glucan assays are useful adjunctive tests, particularly in high-risk patients.
Treatment depends on disease type. ABPA is managed with systemic glucocorticoids combined with itraconazole, with steroids tapered over several months when possible. Chronic pulmonary aspergillosis often requires long-term antifungal therapy, commonly with voriconazole, and in selected cases surgical resection of aspergilloma. Embolization may be used to control hemoptysis. Invasive aspergillosis is treated with voriconazole as first-line therapy. Alternatives include amphotericin B, itraconazole, or echinocandins, although combination therapy remains of uncertain benefit. Surgical debridement is recommended when feasible.
Patients with invasive disease require prompt initiation of antifungal therapy and stabilization of hemodynamic parameters. Hospital admission is warranted for unstable patients, those with significant hemoptysis, or immunocompromised individuals with fever. Long-term monitoring is essential to detect relapse, progression, or drug toxicity. Therapeutic drug monitoring of voriconazole trough levels is recommended during prolonged therapy.
Prognosis depends largely on the degree of immunosuppression and fungal burden. Complications include massive hemoptysis in chronic disease, pulmonary fibrosis and bronchiectasis in ABPA, pneumothorax, empyema, and disseminated infection in invasive disease. Central nervous system involvement may result in vascular occlusion and severe neurologic sequelae. Early recognition and aggressive management are critical to improving outcomes.
Aspergillosis describes a spectrum of illnesses caused by species of Aspergillus, ranging from simple colonization or allergic reactions to localized or disseminated invasive disease. Although virtually any organ may be involved, the lungs are most commonly affected, followed by the paranasal sinuses and, less frequently, the central nervous system.
The number of Aspergillus species implicated in human disease continues to expand. Aspergillus fumigatus remains the most common cause of invasive infection, but A. flavus, A. terreus, A. niger, and A. versicolor are increasingly recognized. Invasive aspergillosis is second only to candidiasis among invasive fungal infections in immunocompromised patients. Major risk factors include granulocytopenia (the most significant), hematopoietic stem cell transplantation, solid-organ transplantation, acute leukemia, prolonged corticosteroid or cytotoxic therapy, chronic obstructive pulmonary disease treated with steroids, prolonged antibiotic use, liver failure, diabetes mellitus, chronic granulomatous disease, and advanced AIDS (CD4 count ≤50 cells/mm³). Genetic polymorphisms in Toll-like receptors 4 and 9 may influence susceptibility to invasive aspergillosis and allergic bronchopulmonary aspergillosis (ABPA), respectively.
Preventive strategies focus on environmental control, particularly during hospital construction activities, to reduce exposure to airborne conidia. High-efficiency particulate air (HEPA) filtration systems are recommended for high-risk patients. In selected individuals with prior invasive disease who may become neutropenic, antifungal prophylaxis with agents such as voriconazole or amphotericin B may be considered.
Pathophysiologically, inhaled conidia are small enough to reach the alveoli. In immunocompetent hosts, alveolar macrophages clear the spores. In immunocompromised individuals, impaired macrophage function allows germination into hyphae, triggering inflammatory cytokine release, vascular invasion, tissue necrosis, and possible hematogenous dissemination. In ABPA, colonization in atopic individuals activates TH2 CD4+ T cells, driving IgE production and eosinophilia, exacerbating asthma and potentially leading to bronchiectasis. Chronic pulmonary aspergillosis, including aspergilloma formation, often develops in patients with prior lung disease such as tuberculosis, lung cancer resection, ABPA, or bullous disease.
Clinical manifestations vary by syndrome. ABPA occurs in patients with asthma or cystic fibrosis and presents with worsening respiratory symptoms, malaise, and occasionally hemoptysis. Chronic pulmonary aspergillosis typically presents with weight loss, chronic cough, hemoptysis, dyspnea, and constitutional symptoms. Invasive aspergillosis commonly presents with fever, pleuritic chest pain, cough, dyspnea, and hemoptysis, especially in neutropenic or otherwise immunocompromised hosts.
Diagnosis depends on clinical suspicion and supportive laboratory and imaging findings. In ABPA, chest imaging may show upper-lobe infiltrates, bronchial wall thickening, bronchiectasis, or ground-glass opacities. Peripheral eosinophilia, elevated total serum IgE, positive immediate skin test to Aspergillus, and elevated serum IgG to A. fumigatus support the diagnosis. Chronic pulmonary aspergillosis is characterized radiographically by one or more lung cavities, sometimes containing a mobile aspergilloma with an air-crescent sign. Invasive aspergillosis requires demonstration of fungal invasion on tissue biopsy for definitive diagnosis. Serum galactomannan and β-glucan assays are useful adjunctive tests, particularly in high-risk patients.
Treatment depends on disease type. ABPA is managed with systemic glucocorticoids combined with itraconazole, with steroids tapered over several months when possible. Chronic pulmonary aspergillosis often requires long-term antifungal therapy, commonly with voriconazole, and in selected cases surgical resection of aspergilloma. Embolization may be used to control hemoptysis. Invasive aspergillosis is treated with voriconazole as first-line therapy. Alternatives include amphotericin B, itraconazole, or echinocandins, although combination therapy remains of uncertain benefit. Surgical debridement is recommended when feasible.
Patients with invasive disease require prompt initiation of antifungal therapy and stabilization of hemodynamic parameters. Hospital admission is warranted for unstable patients, those with significant hemoptysis, or immunocompromised individuals with fever. Long-term monitoring is essential to detect relapse, progression, or drug toxicity. Therapeutic drug monitoring of voriconazole trough levels is recommended during prolonged therapy.
Prognosis depends largely on the degree of immunosuppression and fungal burden. Complications include massive hemoptysis in chronic disease, pulmonary fibrosis and bronchiectasis in ABPA, pneumothorax, empyema, and disseminated infection in invasive disease. Central nervous system involvement may result in vascular occlusion and severe neurologic sequelae. Early recognition and aggressive management are critical to improving outcomes.

- Published on
Infectious Disease and Microbiology – Atypical Mycobacteria (Nontuberculous Mycobacteria)
Atypical mycobacteria refer to infections caused by nontuberculous mycobacteria (NTM), a diverse group of environmental mycobacterial species distinct from Mycobacterium tuberculosis. In children, atypical mycobacteria should be considered in cases of unilateral cervical lymphadenitis, particularly in those aged 1–5 years. The swelling typically involves the anterior cervical chain, enlarges gradually, and may form fistulas through the skin. Enlarged lymph nodes are often painless, and systemic symptoms are uncommon. Most pediatric cases are caused by Mycobacterium avium complex (MAC), while M. scrofulaceum and M. tuberculosis are less frequent causes. Approximately 300 cases of MAC lymphadenitis occur annually in the United States. Overall prevalence ranges from 1 to 7.2 cases per 100,000 persons in the US, varying by region, and about half of NTM isolates represent true pathogens.
Risk factors for NTM infection include advanced age, immunosuppression, HIV infection with low CD4 counts, interferon-gamma deficiencies, and underlying structural lung disease such as bronchiectasis or chronic obstructive pulmonary disease. Genetic defects such as IFN-γ receptor 1 (IFNγR1) or interleukin-12 receptor β1 (IL-12βR1) deficiency predispose individuals to disseminated disease. In patients with AIDS and CD4 counts below 100 cells/mm³, primary prophylaxis with weekly azithromycin 1200 mg is recommended; alternatives include clarithromycin or rifabutin.
NTM are widely found in soil and water, including hot tubs and tap water. Human-to-human transmission has not been documented. Infection occurs primarily through ingestion or inhalation rather than reactivation of latent disease. Granuloma formation results from interactions between macrophages, lymphocytes, and natural killer cells. Disseminated infection arises from uncontrolled localized disease, especially in immunocompromised hosts. These organisms are aerobic, non–spore-forming bacilli with mycolic acid–containing cell walls. They are categorized by growth rate into rapid-growing mycobacteria (e.g., M. fortuitum, M. chelonae/abscessus, M. smegmatis), intermediate growers (e.g., M. marinum, M. gordonae), and slow-growing organisms (e.g., MAC, M. kansasii, M. xenopi, M. scrofulaceum, M. haemophilum, M. ulcerans).
Clinical syndromes include pulmonary disease, lymphadenitis, skin and soft tissue infection, osteoarticular disease, catheter-related infection, and disseminated disease. Pulmonary infection typically presents with chronic productive cough and may progress to weight loss, fatigue, dyspnea, hemoptysis, and chest pain. Soft tissue infections often follow trauma, surgery, or aquatic exposure and appear as papular or ulcerative lesions that may spread along lymphatics. Lymphadenitis usually manifests as painless or mildly tender enlargement of submandibular or jugular lymph nodes. Disseminated disease, most commonly seen in advanced HIV infection, presents with fever, fatigue, anorexia, and laboratory abnormalities such as pancytopenia or elevated alkaline phosphatase.
Diagnosis requires correlation of clinical, radiographic, and microbiologic findings because NTM may represent colonization rather than true infection. In pulmonary disease, chest imaging may show upper-lobe cavitary lesions, nodular or reticulonodular infiltrates, or adenopathy. Cavitary disease is common in MAC pulmonary infections and typically involves thin-walled cavities measuring 2–4 cm. At least three sputum samples (or bronchoalveolar lavage specimens) should be obtained for acid-fast bacillus smear and culture. Mycobacterial blood cultures are positive in approximately 90% of disseminated MAC cases. Tissue biopsy demonstrating granulomas with giant cells and acid-fast bacilli supports localized infection, whereas well-formed granulomas may be absent in disseminated disease. Definitive identification and susceptibility testing should be performed at specialized laboratories.
Treatment depends on the species and site of infection and often requires prolonged multidrug therapy. Pulmonary MAC is treated with rifampin, ethambutol, and a macrolide (azithromycin or clarithromycin), sometimes with an aminoglycoside for severe disease. Therapy continues for at least 12 months after cultures become negative. Pulmonary infection with M. kansasii is treated with isoniazid, rifampin, and ethambutol. Rapid-growing mycobacteria causing soft tissue infections are treated with two active agents based on susceptibility testing, such as trimethoprim–sulfamethoxazole, doxycycline, levofloxacin, or clarithromycin. Severe M. abscessus infections may require amikacin combined with clarithromycin and cefoxitin or imipenem. Disseminated MAC in HIV patients is treated with a macrolide plus ethambutol, with consideration of adding rifampin.
Surgical management may be necessary in selected cases. Resection of affected lymph nodes in MAC lymphadenitis achieves cure in approximately 90% of pediatric cases without antimicrobials. Lung resection may be considered in localized refractory pulmonary disease. Incision and drainage are often required for soft tissue infections.
Long-term follow-up is essential because therapy may last months to years and drug toxicities are common. Patients require regular laboratory monitoring, evaluation for drug–drug interactions, and sometimes therapeutic drug monitoring. Prognosis depends on the infecting species, the site of disease, and the host’s immune status. Complications include ulceration and fistula formation in lymphadenitis and, rarely, gastrointestinal complications such as intussusception or obstruction in disseminated MAC.
Atypical mycobacteria refer to infections caused by nontuberculous mycobacteria (NTM), a diverse group of environmental mycobacterial species distinct from Mycobacterium tuberculosis. In children, atypical mycobacteria should be considered in cases of unilateral cervical lymphadenitis, particularly in those aged 1–5 years. The swelling typically involves the anterior cervical chain, enlarges gradually, and may form fistulas through the skin. Enlarged lymph nodes are often painless, and systemic symptoms are uncommon. Most pediatric cases are caused by Mycobacterium avium complex (MAC), while M. scrofulaceum and M. tuberculosis are less frequent causes. Approximately 300 cases of MAC lymphadenitis occur annually in the United States. Overall prevalence ranges from 1 to 7.2 cases per 100,000 persons in the US, varying by region, and about half of NTM isolates represent true pathogens.
Risk factors for NTM infection include advanced age, immunosuppression, HIV infection with low CD4 counts, interferon-gamma deficiencies, and underlying structural lung disease such as bronchiectasis or chronic obstructive pulmonary disease. Genetic defects such as IFN-γ receptor 1 (IFNγR1) or interleukin-12 receptor β1 (IL-12βR1) deficiency predispose individuals to disseminated disease. In patients with AIDS and CD4 counts below 100 cells/mm³, primary prophylaxis with weekly azithromycin 1200 mg is recommended; alternatives include clarithromycin or rifabutin.
NTM are widely found in soil and water, including hot tubs and tap water. Human-to-human transmission has not been documented. Infection occurs primarily through ingestion or inhalation rather than reactivation of latent disease. Granuloma formation results from interactions between macrophages, lymphocytes, and natural killer cells. Disseminated infection arises from uncontrolled localized disease, especially in immunocompromised hosts. These organisms are aerobic, non–spore-forming bacilli with mycolic acid–containing cell walls. They are categorized by growth rate into rapid-growing mycobacteria (e.g., M. fortuitum, M. chelonae/abscessus, M. smegmatis), intermediate growers (e.g., M. marinum, M. gordonae), and slow-growing organisms (e.g., MAC, M. kansasii, M. xenopi, M. scrofulaceum, M. haemophilum, M. ulcerans).
Clinical syndromes include pulmonary disease, lymphadenitis, skin and soft tissue infection, osteoarticular disease, catheter-related infection, and disseminated disease. Pulmonary infection typically presents with chronic productive cough and may progress to weight loss, fatigue, dyspnea, hemoptysis, and chest pain. Soft tissue infections often follow trauma, surgery, or aquatic exposure and appear as papular or ulcerative lesions that may spread along lymphatics. Lymphadenitis usually manifests as painless or mildly tender enlargement of submandibular or jugular lymph nodes. Disseminated disease, most commonly seen in advanced HIV infection, presents with fever, fatigue, anorexia, and laboratory abnormalities such as pancytopenia or elevated alkaline phosphatase.
Diagnosis requires correlation of clinical, radiographic, and microbiologic findings because NTM may represent colonization rather than true infection. In pulmonary disease, chest imaging may show upper-lobe cavitary lesions, nodular or reticulonodular infiltrates, or adenopathy. Cavitary disease is common in MAC pulmonary infections and typically involves thin-walled cavities measuring 2–4 cm. At least three sputum samples (or bronchoalveolar lavage specimens) should be obtained for acid-fast bacillus smear and culture. Mycobacterial blood cultures are positive in approximately 90% of disseminated MAC cases. Tissue biopsy demonstrating granulomas with giant cells and acid-fast bacilli supports localized infection, whereas well-formed granulomas may be absent in disseminated disease. Definitive identification and susceptibility testing should be performed at specialized laboratories.
Treatment depends on the species and site of infection and often requires prolonged multidrug therapy. Pulmonary MAC is treated with rifampin, ethambutol, and a macrolide (azithromycin or clarithromycin), sometimes with an aminoglycoside for severe disease. Therapy continues for at least 12 months after cultures become negative. Pulmonary infection with M. kansasii is treated with isoniazid, rifampin, and ethambutol. Rapid-growing mycobacteria causing soft tissue infections are treated with two active agents based on susceptibility testing, such as trimethoprim–sulfamethoxazole, doxycycline, levofloxacin, or clarithromycin. Severe M. abscessus infections may require amikacin combined with clarithromycin and cefoxitin or imipenem. Disseminated MAC in HIV patients is treated with a macrolide plus ethambutol, with consideration of adding rifampin.
Surgical management may be necessary in selected cases. Resection of affected lymph nodes in MAC lymphadenitis achieves cure in approximately 90% of pediatric cases without antimicrobials. Lung resection may be considered in localized refractory pulmonary disease. Incision and drainage are often required for soft tissue infections.
Long-term follow-up is essential because therapy may last months to years and drug toxicities are common. Patients require regular laboratory monitoring, evaluation for drug–drug interactions, and sometimes therapeutic drug monitoring. Prognosis depends on the infecting species, the site of disease, and the host’s immune status. Complications include ulceration and fistula formation in lymphadenitis and, rarely, gastrointestinal complications such as intussusception or obstruction in disseminated MAC.

