- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Pemphigus
Pemphigus is a rare, IgG-mediated autoimmune blistering disorder of the skin and mucous membranes characterized by loss of keratinocyte cell-to-cell adhesion (acantholysis). The term is derived from the Greek word for “bubble” or blister. It most commonly affects older adults, with a median age of 71 years, and has a slight female predominance. Although rare, it can occur in neonates, children, and adolescents. If untreated, mortality historically reached 60–90%, but with modern therapy this has decreased to approximately 5%. Mortality is highest in patients with extensive mucocutaneous involvement.
There are three major subtypes. Pemphigus vulgaris accounts for 70–80% of cases and is the most serious form, with deeper mucocutaneous involvement. Up to 70% of patients initially present with painful oral lesions before cutaneous involvement develops. Autoantibodies are directed against desmoglein (Dsg) 1 and 3. Pemphigus foliaceus is more superficial, limited primarily to the skin, and associated with antibodies to Dsg1 only; oral lesions are uncommon and prognosis is generally better. Paraneoplastic pemphigus is often severe and associated with lymphoreticular malignancies. Endemic pemphigus foliaceus (fogo selvagem) is reported most commonly in South America and may be associated with environmental triggers such as insect bites.
The pathogenesis involves IgG autoantibodies targeting desmosomal cadherins (desmoglein 1 and 3) on keratinocytes. This immune attack results in acantholysis, cytoskeletal disruption, and apoptosis, leading to intraepidermal blister formation. Genetic predisposition is associated with certain HLA haplotypes, including DR4 and DRw6. Drug-induced pemphigus-like reactions have been reported with agents such as penicillamine, captopril, rifampin, piroxicam, and phenobarbital.
Clinically, patients present with flaccid bullae that rupture easily, leaving painful erosions with shreds of detached epithelium. Mucosal involvement, especially painful oral erosions, is common in pemphigus vulgaris and may precede skin findings. Lesions may spread to the scalp, chest, axillae, and groin. Crusted erosions, exfoliative plaques, and postinflammatory hyperpigmentation are common. The Nikolsky sign—epidermal separation with lateral pressure—is characteristic but not highly sensitive or specific. Without treatment, lesions persist and may lead to dehydration, malnutrition, infection, or sepsis.
Diagnosis is suspected clinically but requires confirmation with skin biopsy and direct immunofluorescence testing, which demonstrate intraepidermal blistering and intercellular IgG deposition. Serum antibody titers (indirect immunofluorescence or ELISA) may correlate with disease activity but are not typically obtained in the emergency setting. The differential diagnosis includes bullous pemphigoid, toxic epidermal necrolysis, dermatitis herpetiformis, erythema multiforme, lupus erythematosus, herpes simplex infection, and other blistering or erosive dermatoses.
Emergency management depends on severity. Mild-to-moderate disease may be managed with oral prednisone and urgent dermatology follow-up. Systemic corticosteroids remain the cornerstone of therapy. Severe disease may require high-dose corticosteroids, pulse intravenous methylprednisolone, or admission for plasmapheresis. Adjuvant immunosuppressive therapies such as azathioprine, mycophenolate, cyclophosphamide, cyclosporine, IV immunoglobulin, or rituximab may be added in refractory cases. Patients presenting with hypotension or sepsis require aggressive fluid resuscitation, broad-spectrum antibiotics if infection is suspected, and stress-dose steroids in those on chronic corticosteroids.
Admission is indicated for first-time presentations requiring biopsy and diagnostic confirmation, extensive mucocutaneous involvement, intractable pain, secondary infection, or signs of systemic compromise. ICU or burn unit admission may be necessary in cases of shock, sepsis, or large body surface involvement requiring intensive wound care. Patients with mild disease who are stable may be discharged with prompt dermatology follow-up.
Key clinical principles include recognizing early mucosal involvement, understanding that long-term immunosuppression is often required, and maintaining vigilance for complications such as adrenal crisis, severe infection, or steroid-induced metabolic derangements. Early diagnosis and coordinated dermatologic management significantly improve outcomes.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Penile Shaft Fracture
Penile shaft fracture is a traumatic rupture of the corpus cavernosum and its surrounding tunica albuginea, most often occurring during erection. The injury may also involve the corpus spongiosum and urethra, with urethral injury present in approximately 25–30% of cases. Hematoma formation occurs at the site of rupture, and the injury is typically unilateral and transverse, most commonly affecting the proximal shaft.
During erection, intracavernosal pressure rises to near arterial levels, expanding the corpora cavernosa and thinning the tunica albuginea, making it highly susceptible to rupture with blunt trauma. Because erection limits vertical movement while allowing lateral motion, forceful bending can create a vulnerable hinge point at the penile base. Penile fracture most commonly occurs during sexual intercourse, but can also result from manipulation, falls onto an erect penis, entanglement in clothing, or forceful detumescence practices such as “Taghaandan.” Predisposing factors include prior trauma, surgical procedures, Peyronie disease, urethritis, or scar tissue weakening the tunica.
Clinically, patients often report a loud “pop” or “crack” at the time of injury, followed by immediate detumescence and severe penile pain. Rapid swelling, ecchymosis, and deformity develop, often producing the classic “eggplant deformity” due to extensive hematoma. The penis deviates away from the side of the tear. Physical examination reveals a flaccid, swollen, ecchymotic penis with possible palpable defect along the shaft. Blood at the urethral meatus, hematuria, dysuria, urinary retention, or weak urinary stream suggests associated urethral injury. Late complications of untreated injury include erectile dysfunction, penile curvature, urethral stricture, and fistula formation.
Diagnosis is primarily clinical. Urinalysis should be performed to evaluate for urethral trauma. If urethral injury is suspected, retrograde urethrography should be performed before urethral catheterization and with low-pressure contrast injection. Ultrasound, cavernosography, or MRI may help confirm the tear or localize injury in equivocal cases, but imaging should not delay definitive management. Surgical exploration is recommended if clinical suspicion remains high, even when imaging is negative.
Emergency management prioritizes pain control and stabilization. Ice packs and elevation may help reduce swelling. In cases of urethral injury with urinary retention, suprapubic cystostomy may be required. Prophylactic antibiotics are generally unnecessary unless indicated for associated injuries. Urethral catheterization should only occur after urethral trauma has been excluded.
All patients with suspected penile fracture require urgent urologic consultation and hospital admission for prompt surgical repair. Early operative intervention significantly reduces complications such as erectile dysfunction, penile deformity, and urethral stricture. Delay in treatment is the primary cause of long-term morbidity. Follow-up with a urologist is essential to ensure restoration of normal urinary and sexual function.
Early recognition and timely surgical management are critical, as penile fracture is a urologic emergency with excellent outcomes when treated promptly.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Peptic Ulcer Disease
Peptic ulcer disease (PUD) results from a breakdown in the protective mucosal defenses of the stomach or duodenum, leading to ulceration from acid and pepsin injury. The condition develops when there is an imbalance between gastric acid production and the mucosa’s ability to protect itself. The two most common causes are infection with Helicobacter pylori and nonsteroidal anti-inflammatory drug (NSAID) use.
Helicobacter pylori is a gram-negative spiral bacterium that colonizes the gastric mucous layer. It is responsible for approximately 90–95% of duodenal ulcers and 80% of gastric ulcers. The organism increases antral gastrin production and impairs mucosal integrity. NSAIDs, including aspirin, interfere with prostaglandin synthesis, weakening mucosal defenses and predisposing to ulcer formation. Additional risk factors include cigarette smoking, alcohol use, severe physiologic stress, hypersecretory states (such as Zollinger–Ellison syndrome), and genetic predisposition, with more than 20% of patients reporting a family history.
Patients commonly present with epigastric pain described as burning, gnawing, or aching. The pain is typically midline and may be localized to the xiphoid or umbilical region. Duodenal ulcer pain usually occurs 90 minutes to 3 hours after meals, may awaken the patient at night, and is often relieved by food or antacids. In contrast, gastric ulcer pain typically worsens after meals and may be associated with nausea and anorexia. Clinical differentiation between gastric and duodenal ulcers can be difficult. Relief with antacids is common. Some patients present with heme-positive stools.
Complications are critical to recognize in the emergency setting. Acute perforation presents with sudden severe pain, rigid boardlike abdomen, generalized rebound tenderness, and possible radiation to the back or shoulder. Gastric outlet obstruction manifests with vomiting, abdominal distention, and a succussion splash. Hemorrhage may present with hematemesis, melena, hypotension, tachycardia, pallor, and orthostatic changes. NSAID-induced ulcers may be clinically silent until complications occur.
Initial evaluation includes a careful abdominal examination, Hemoccult testing, and assessment of vital signs including orthostatics. Laboratory findings are often normal in uncomplicated disease. A low hematocrit suggests bleeding, while leukocytosis may indicate perforation or penetration. Amylase and lipase may be elevated with penetration or when pancreatitis is in the differential. Type and cross-match should be performed in significant blood loss. Testing for H. pylori may include urea breath test, serology, or stool antigen testing. Chest or abdominal radiographs are useful when perforation or obstruction is suspected. Endoscopy is the diagnostic procedure of choice, allowing direct visualization, biopsy, and evaluation for malignancy.
Emergency management begins with ABC stabilization. Hypotensive patients require IV fluid resuscitation with large-bore IV access and early type and cross-match. Nasogastric decompression may be indicated in obstruction or significant hemorrhage. Pain may be treated with antacids or IV H2-receptor antagonists. Narcotics should be used cautiously to avoid masking serious pathology.
Ulcer healing is promoted with acid suppression therapy. Proton pump inhibitors (PPIs) such as omeprazole, pantoprazole, or lansoprazole are highly effective. H2-receptor antagonists (e.g., famotidine) may also be used. Sucralfate and misoprostol are additional options. Combined use of sucralfate with H2 blockers or PPIs is generally not recommended due to lack of additional benefit. NSAIDs should be discontinued whenever possible.
Eradication of H. pylori is essential in infected patients. Standard triple therapy includes a PPI plus clarithromycin and amoxicillin for 14 days. In penicillin-allergic patients, clarithromycin and metronidazole are substituted. Quadruple therapy with bismuth, tetracycline, metronidazole, and a PPI is used in resistant cases or as second-line therapy.
Complications require urgent consultation. Active upper GI bleeding necessitates fluid resuscitation, possible transfusion, and gastroenterology consultation for endoscopic therapy. Perforation requires emergency surgical consultation and broad-spectrum antibiotics. Gastric outlet obstruction requires decompression and supportive care.
Patients with uncomplicated disease, stable vital signs, normal hematocrit, and heme-negative stools may be discharged with acid suppression therapy and close outpatient follow-up. Admission is required for obstruction, perforation, active bleeding, significant anemia, or uncontrolled pain. All patients should have follow-up within 2–6 weeks to assess response to therapy. Patients older than 55 years or those with alarm symptoms should undergo endoscopic evaluation to exclude malignancy.
Early recognition and appropriate eradication of H. pylori, along with acid suppression and avoidance of NSAIDs, are the cornerstones of therapy. Failure to ensure follow-up may result in missed complications, including gastric cancer.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Perforated Viscus
A perforated viscus is a full-thickness disruption of a hollow abdominal organ that allows gastrointestinal contents to spill into the peritoneal cavity. This results in chemical and bacterial peritonitis, leading rapidly to systemic inflammatory response and potential septic shock. Perforation may occur from ulceration, inflammation, obstruction, ischemia, trauma, or iatrogenic injury. It is a surgical emergency requiring rapid recognition and intervention.
The most common cause is perforated peptic ulcer disease, frequently associated with NSAID use or Helicobacter pylori infection. Other causes include small bowel ischemia, inflammatory bowel disease, neoplasms, foreign bodies, diverticular disease, appendicitis, penetrating or blunt abdominal trauma, endoscopic procedures, and radiation enteritis or proctitis. In pediatric patients, trauma is the most common cause, particularly in neonates after difficult delivery, nonaccidental trauma, motor vehicle collisions, or falls. The jejunum is a common rupture site in children.
Patients typically present with sudden, severe abdominal pain that is initially localized but rapidly becomes diffuse as peritonitis develops. Examination reveals rigidity, guarding, rebound tenderness, and absent bowel sounds. Systemic findings may include fever, tachycardia, tachypnea, and hypotension. In advanced cases, patients may present in hypovolemic or septic shock. Elderly patients often have atypical presentations with less pronounced pain, minimal guarding, absence of leukocytosis, altered mental status, hypothermia, or blunted tachycardia due to medications or comorbidities.
The essential initial study is an upright chest radiograph to detect pneumoperitoneum. After the patient has been upright for 5–10 minutes, as little as 1–2 mL of free air may be visualized under the diaphragm. Sensitivity ranges from 50% to 85%. A left lateral decubitus abdominal radiograph may be more sensitive than a supine film. The double wall (Rigler) sign, in which both the mucosal and serosal surfaces of bowel are visible, suggests free intraperitoneal air. Abdominal CT is highly sensitive for detecting small amounts of free air and is indicated when clinical suspicion remains high despite normal plain films.
Laboratory evaluation includes CBC, electrolytes, renal function, glucose, liver function tests, coagulation profile, urinalysis, lipase, arterial blood gas, and lactate. Leukocytosis and elevated lactate support the diagnosis but are not required. Type and cross-match should be performed in unstable patients. ECG may be necessary to exclude cardiac causes of abdominal pain. In pregnant patients, ectopic pregnancy must be excluded.
Management begins with aggressive resuscitation following trauma and sepsis principles. Hypotension and tachycardia are treated with rapid infusion of 0.9% normal saline, typically 500 mL to 1 L boluses in adults, repeated as needed. Pediatric patients receive 20 mL/kg boluses. Vasopressors may be required if fluids are insufficient. Nasogastric decompression and Foley catheter placement are recommended. Broad-spectrum intravenous antibiotics must be administered promptly to cover enteric gram-negative bacilli, gram-positive cocci, and anaerobes. Appropriate regimens include a carbapenem, piperacillin–tazobactam, or a third- or fourth-generation cephalosporin combined with metronidazole. Analgesia should be provided without delaying surgical consultation.
Immediate surgical consultation is mandatory for all suspected or confirmed cases. Imaging should not delay operative intervention in unstable patients. Discharge is not appropriate, as perforated viscus is a surgical emergency requiring admission and definitive management. Early recognition, prompt antibiotic therapy, aggressive resuscitation, and urgent surgical intervention are critical to reducing morbidity and mortality.
- Published on
Emergency and Acute Medicine – Peritonsillar Abscess
Peritonsillar abscess is a suppurative complication of tonsillitis in which infection spreads beyond the tonsillar capsule into the space between the palatine tonsil and the pharyngeal muscles. It is the most common deep infection of the head and neck, with an incidence of approximately 30 per 100,000 people per year and about 45,000 cases annually in the United States. It occurs at any age but is most common in young adults between 20 and 40 years. Incidence peaks during November to December and April to May, corresponding with higher rates of streptococcal pharyngitis. Although uncommon, complications can include airway compromise, sepsis, recurrence in 12–15% of patients, spread to the lateral neck or mediastinum, spontaneous rupture with aspiration pneumonitis, internal jugular vein thrombosis (Lemierre syndrome), poststreptococcal glomerulonephritis or rheumatic fever, carotid sheath erosion with hemorrhage, severe dehydration, and intracranial extension such as meningitis, cavernous sinus thrombosis, cerebral abscess, or dural sinus thrombosis.
Two primary mechanisms are proposed for its development. One theory involves direct bacterial invasion into deeper tissues during acute pharyngitis. The other suggests obstruction and infection of the Weber glands located in the superior tonsillar pole. Smoking may increase risk. Infection is typically polymicrobial. Common pathogens include Group A Streptococcus, Staphylococcus species including MRSA, and anaerobes such as Prevotella, Peptostreptococcus, and Fusobacterium.
Patients commonly present with unilateral sore throat, fever, voice change, odynophagia, drooling, headache, referred ear pain, decreased oral intake, and malaise. Physical examination often reveals fever, trismus, a muffled “hot potato” voice, erythematous tonsils and soft palate, medial and inferior displacement of the superior pole of the affected tonsil, uvular deviation away from the affected side, halitosis, cervical lymphadenitis, and tenderness along the ipsilateral angle of the jaw. Airway assessment is critical, with attention to stridor, tripod positioning, or inability to handle secretions. Clinicians must also consider possible extension into deeper neck spaces when systemic toxicity or atypical findings are present.
Diagnosis is usually clinical based on careful oropharyngeal examination, although severe trismus may limit visualization. Throat culture and monospot testing may be considered, as infectious mononucleosis is present in up to 20% of cases. A complete blood count and abscess culture may be useful in selected patients. A basic metabolic panel may help assess dehydration. Bedside intraoral ultrasound can assist in identifying and localizing the abscess, particularly in cooperative patients, while transcutaneous ultrasound may be useful if trismus prevents intraoral imaging. CT of the neck with contrast is indicated when deep neck infection is suspected, after failed needle aspiration, or when examination is limited. MRI may help detect complications such as internal jugular vein thrombosis or carotid sheath involvement. Needle aspiration is both diagnostic and frequently therapeutic, and incision and drainage is also effective.
Management begins with airway evaluation and stabilization, IV access, cardiac and pulse oximetry monitoring, and supplemental oxygen as needed. Children account for 25–30% of cases and may require sedation or general anesthesia for drainage procedures. In young children with signs of upper airway obstruction, a lateral neck radiograph may be obtained before oral examination. Antibiotics should be started promptly, along with IV fluids for dehydration and appropriate analgesia. A single dose of corticosteroid such as dexamethasone may improve symptoms. Adequate local anesthesia using benzocaine spray and lidocaine with epinephrine is essential before drainage. Needle aspiration has a success rate of 87–94% and should be performed by clinicians experienced in airway management. The internal carotid artery lies approximately 2.5 cm posterolateral to the tonsil, so limiting needle depth to less than 0.5 cm is recommended. The superior pole is the most common site of maximal fluctuance. Incision and drainage has a success rate of 90–92% and should be performed using a guarded blade with no more than 1 cm exposed, avoiding incisions deeper than 0.5 cm. Packing is generally not required. Tonsillectomy may be indicated in cases of airway obstruction, recurrent severe pharyngitis, recurrent abscess, or failure of drainage.
Antibiotic therapy should continue for 14 days, as shorter courses may increase recurrence risk. Intravenous options include ampicillin/sulbactam or penicillin G combined with metronidazole. Clindamycin is appropriate for penicillin-allergic patients. Oral regimens include amoxicillin/clavulanate, penicillin VK with metronidazole, or clindamycin. A single dose of dexamethasone 10 mg (0.6 mg/kg in children, maximum 10 mg) may be administered.
Admission is indicated for airway compromise, sepsis, altered mental status, significant dehydration, or extension beyond the peritonsillar space. Most patients can be discharged after successful drainage if they tolerate oral intake and medications. Referral to otolaryngology is recommended, and interval tonsillectomy is often considered 6–8 weeks after resolution. Close follow-up within 24–48 hours is essential because treatment failure and recurrence are relatively common.
Peritonsillar abscess is a suppurative complication of tonsillitis in which infection spreads beyond the tonsillar capsule into the space between the palatine tonsil and the pharyngeal muscles. It is the most common deep infection of the head and neck, with an incidence of approximately 30 per 100,000 people per year and about 45,000 cases annually in the United States. It occurs at any age but is most common in young adults between 20 and 40 years. Incidence peaks during November to December and April to May, corresponding with higher rates of streptococcal pharyngitis. Although uncommon, complications can include airway compromise, sepsis, recurrence in 12–15% of patients, spread to the lateral neck or mediastinum, spontaneous rupture with aspiration pneumonitis, internal jugular vein thrombosis (Lemierre syndrome), poststreptococcal glomerulonephritis or rheumatic fever, carotid sheath erosion with hemorrhage, severe dehydration, and intracranial extension such as meningitis, cavernous sinus thrombosis, cerebral abscess, or dural sinus thrombosis.
Two primary mechanisms are proposed for its development. One theory involves direct bacterial invasion into deeper tissues during acute pharyngitis. The other suggests obstruction and infection of the Weber glands located in the superior tonsillar pole. Smoking may increase risk. Infection is typically polymicrobial. Common pathogens include Group A Streptococcus, Staphylococcus species including MRSA, and anaerobes such as Prevotella, Peptostreptococcus, and Fusobacterium.
Patients commonly present with unilateral sore throat, fever, voice change, odynophagia, drooling, headache, referred ear pain, decreased oral intake, and malaise. Physical examination often reveals fever, trismus, a muffled “hot potato” voice, erythematous tonsils and soft palate, medial and inferior displacement of the superior pole of the affected tonsil, uvular deviation away from the affected side, halitosis, cervical lymphadenitis, and tenderness along the ipsilateral angle of the jaw. Airway assessment is critical, with attention to stridor, tripod positioning, or inability to handle secretions. Clinicians must also consider possible extension into deeper neck spaces when systemic toxicity or atypical findings are present.
Diagnosis is usually clinical based on careful oropharyngeal examination, although severe trismus may limit visualization. Throat culture and monospot testing may be considered, as infectious mononucleosis is present in up to 20% of cases. A complete blood count and abscess culture may be useful in selected patients. A basic metabolic panel may help assess dehydration. Bedside intraoral ultrasound can assist in identifying and localizing the abscess, particularly in cooperative patients, while transcutaneous ultrasound may be useful if trismus prevents intraoral imaging. CT of the neck with contrast is indicated when deep neck infection is suspected, after failed needle aspiration, or when examination is limited. MRI may help detect complications such as internal jugular vein thrombosis or carotid sheath involvement. Needle aspiration is both diagnostic and frequently therapeutic, and incision and drainage is also effective.
Management begins with airway evaluation and stabilization, IV access, cardiac and pulse oximetry monitoring, and supplemental oxygen as needed. Children account for 25–30% of cases and may require sedation or general anesthesia for drainage procedures. In young children with signs of upper airway obstruction, a lateral neck radiograph may be obtained before oral examination. Antibiotics should be started promptly, along with IV fluids for dehydration and appropriate analgesia. A single dose of corticosteroid such as dexamethasone may improve symptoms. Adequate local anesthesia using benzocaine spray and lidocaine with epinephrine is essential before drainage. Needle aspiration has a success rate of 87–94% and should be performed by clinicians experienced in airway management. The internal carotid artery lies approximately 2.5 cm posterolateral to the tonsil, so limiting needle depth to less than 0.5 cm is recommended. The superior pole is the most common site of maximal fluctuance. Incision and drainage has a success rate of 90–92% and should be performed using a guarded blade with no more than 1 cm exposed, avoiding incisions deeper than 0.5 cm. Packing is generally not required. Tonsillectomy may be indicated in cases of airway obstruction, recurrent severe pharyngitis, recurrent abscess, or failure of drainage.
Antibiotic therapy should continue for 14 days, as shorter courses may increase recurrence risk. Intravenous options include ampicillin/sulbactam or penicillin G combined with metronidazole. Clindamycin is appropriate for penicillin-allergic patients. Oral regimens include amoxicillin/clavulanate, penicillin VK with metronidazole, or clindamycin. A single dose of dexamethasone 10 mg (0.6 mg/kg in children, maximum 10 mg) may be administered.
Admission is indicated for airway compromise, sepsis, altered mental status, significant dehydration, or extension beyond the peritonsillar space. Most patients can be discharged after successful drainage if they tolerate oral intake and medications. Referral to otolaryngology is recommended, and interval tonsillectomy is often considered 6–8 weeks after resolution. Close follow-up within 24–48 hours is essential because treatment failure and recurrence are relatively common.
- Published on
KembaraXtra – Emergency & Acute Medicine – Peripheral Vascular Disease
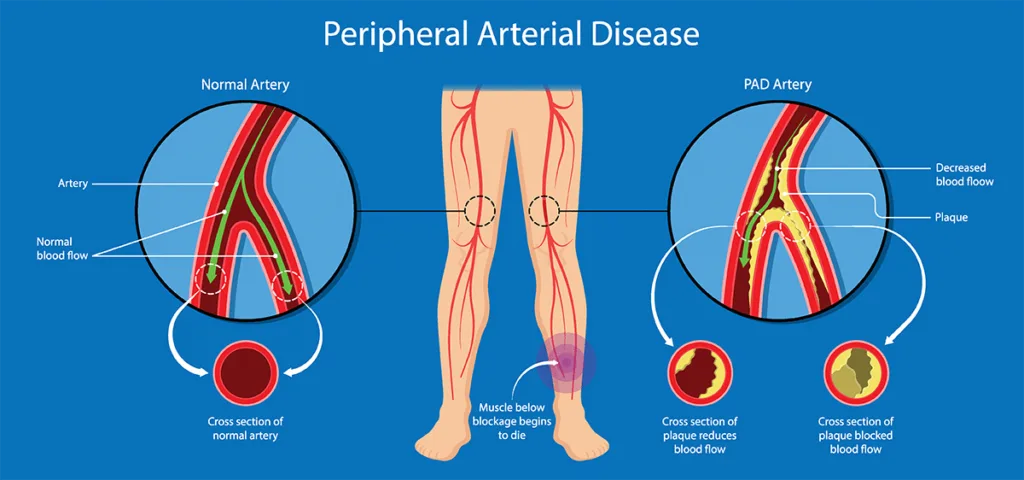
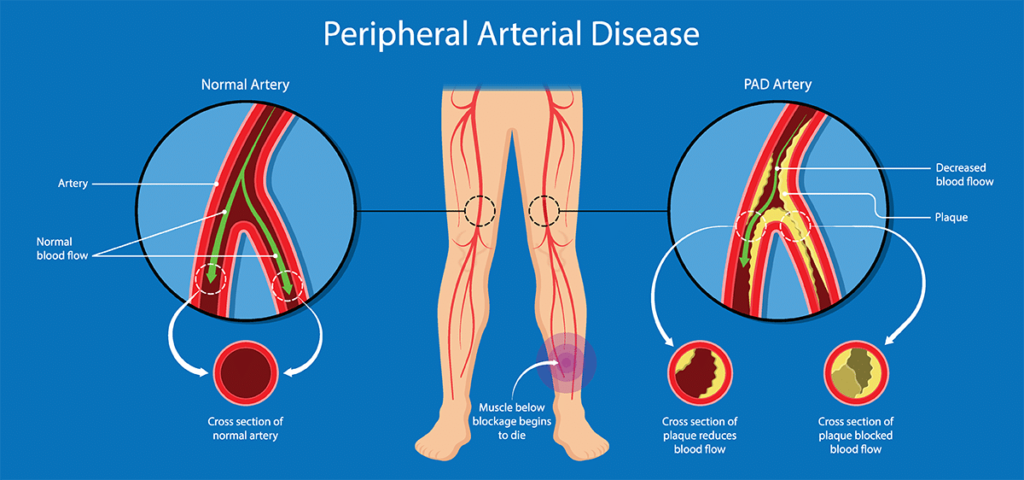
Peripheral vascular disease (PVD), also known as peripheral artery disease (PAD), refers to obstruction of one or more peripheral arteries due to atherosclerosis, thrombosis, or embolism. Many patients also have coexisting coronary artery disease and cerebrovascular disease. Major risk factors include age, smoking, diabetes mellitus, hyperlipidemia, and hypertension. PVD is associated with significant morbidity and mortality related to systemic atherosclerosis. Complications include aneurysm formation, thrombosis, ulceration, limb loss, and progression to critical limb ischemia.
Chronic arterial insufficiency (CAI) results from progressive atherosclerotic narrowing that produces subacute ischemia and claudication. About 10% of patients progress to critical limb ischemia. Acute arterial insufficiency (AAI) is caused by arterial thrombosis (approximately 50%) or embolism and produces acute limb ischemia characterized by the “6 Ps.” Atheroembolism occurs when rupture or disruption of an atherosclerotic plaque in the aorta, iliac, or femoral arteries releases cholesterol emboli that obstruct small vessels. It is often precipitated by invasive arterial procedures such as cardiac catheterization.
Etiologies include atherosclerotic plaque obstruction, arterial thrombosis, cardiac emboli (commonly from atrial fibrillation, valvular disease, or cardiomyopathy), aneurysm, infection, tumor, vasculitis, foreign body, thrombosis superimposed on chronic disease, and atheroembolism.
Patients with CAI typically report claudication—aching calf pain in femoropopliteal disease or buttock and thigh pain in aortoiliac disease—brought on by exertion and relieved with rest or dependent positioning. Severe disease presents with rest pain, usually beginning in the foot, or rapidly progressive claudication and ulceration. Acute arterial insufficiency presents with sudden extremity pain that increases in severity, often beginning distally and progressing proximally. Pain may decrease once sensory loss occurs. Atheroembolism presents with cold, painful digits and may involve multiple organs including kidneys, mesentery, and skin, especially following recent vascular procedures.
On examination, sudden onset of pain and pallor in an extremity is limb- and life-threatening. In CAI, findings include diminished or absent peripheral pulses, delayed capillary refill, cool skin, prolonged venous filling time, bruits, pallor with elevation and dependent rubor, muscle and skin atrophy, thickened nails, hair loss, and toe or heel ulcerations. Acute arterial insufficiency presents with the 6 Ps: pain, pallor, pulselessness, poikilothermia, paresthesias, and paralysis. Identifying a potential embolic source such as atrial fibrillation is essential. Atheroembolism may show painful ischemic digits, “blue toe syndrome,” and livedo reticularis.
The ankle–brachial index (ABI) is an important bedside test in chronic disease. An ABI <0.9 is abnormal and <0.4-0.5 indicates severe disease. in patients with diabetes, calcified vessels may produce falsely elevated values (>1.3). Acute arterial insufficiency is primarily a clinical diagnosis based on the 6 Ps. Patients with acute-on-chronic disease may tolerate ischemia better due to collateral circulation. Atheroembolism is diagnosed clinically, with further evaluation to identify the embolic source.
Laboratory evaluation includes CBC, platelets, electrolytes, renal function, glucose, coagulation studies, and creatine phosphokinase to assess muscle ischemia. Additional studies may include inflammatory markers for vasculitis, blood cultures for suspected endocarditis, and hypercoagulable testing when indicated.
Doppler ultrasound is commonly used to identify the level of arterial occlusion and detect thrombosis or aneurysm. CT angiography is widely used as a first-line diagnostic tool and guides decisions for operative or endovascular intervention. Angiography allows simultaneous diagnosis and treatment with angioplasty, atherectomy, or thrombolysis. MRI is sensitive but less practical in emergency settings.
Differential diagnoses include acute thrombosis or embolism, arterial dissection, deep venous thrombosis, venous insufficiency, compartment syndrome, Buerger disease, spinal stenosis, neuropathy, bursitis, arthritis, and reflex sympathetic dystrophy.
Prehospital care includes maintaining hemodynamic stability, placing the limb at rest in a dependent position, providing oxygen when needed, and cardiac monitoring. In the emergency department, management includes IV fluids for hypotension, cardiac monitoring, supplemental oxygen, adequate analgesia, and avoidance of temperature extremes.
Management of chronic arterial insufficiency includes antiplatelet therapy with aspirin (75–325 mg daily) or clopidogrel (75 mg daily). Cilostazol, pentoxifylline, or dipyridamole may be used in selected patients. Risk-factor modification is essential and includes smoking cessation, lipid and blood pressure control, diabetes management, and structured exercise therapy. Revascularization options include balloon angioplasty, atherectomy, or bypass grafting depending on anatomy and severity.
Acute arterial insufficiency requires immediate IV heparin (80 U/kg bolus followed by infusion at 18 U/kg/hr), unless aortic dissection or aneurysm is suspected. Emergent consultation with vascular surgery or interventional radiology is mandatory. Revascularization must occur within 4–6 hours of symptom onset to prevent irreversible ischemia. Treatment options include thrombectomy, embolectomy, angioplasty, thrombolysis, or bypass grafting. Complications include compartment syndrome, irreversible limb ischemia requiring amputation, rhabdomyolysis, renal failure, and electrolyte disturbances.
Atheroembolism is managed conservatively when tissue involvement is limited and renal function preserved. Treatment is supportive with wound care and analgesia. Vascular surgery referral within 12–24 hours is recommended, and evaluation to prevent further embolic events is essential. Amputation may be required for irreversibly necrotic tissue.
All patients with acute arterial insufficiency require hospital admission for evaluation and revascularization. Patients with chronic disease should be admitted if they develop rapidly progressive claudication or ischemic rest pain. Atheroembolism warrants admission if there is significant tissue involvement, infection, pain, or renal compromise. Stable patients with mild chronic disease or limited atheroembolism may be discharged with close follow-up.
Early recognition of acute limb ischemia is critical, as time to reperfusion determines limb salvage and survival.
- Published on
Emergency And Acute Medicine – Pertussis
Pertussis is an acute respiratory tract infection transmitted by small respiratory droplets. The organism attaches to respiratory epithelial cells via fimbriae and produces toxins that cause ciliary dysfunction, accumulation of debris, increased mucus production, and inflammatory infiltration. Bronchiolar congestion, obstruction, and necrosis may develop. Airway obstruction from mucus plugging can lead to hypoxia, hypoventilation, and increased intrathoracic or intracranial pressure. Secondary bacterial pneumonia may worsen respiratory failure. Central nervous system injury may result from encephalitis, hypoxia, or elevated intracranial pressure. Uncomplicated illness typically lasts 6–10 weeks, although about half resolve in under 6 weeks. Mortality is highest in infants under 1 year, especially those younger than 1 month. Most deaths are due to secondary bacterial pneumonia. The incubation period is usually 7–10 days. Disease is most common in young children, but incidence is increasing among adolescents. Adults serve as the primary reservoir. Peak incidence occurs in late summer and fall. Vaccination with Tdap provides prevention. The causative organism is Bordetella pertussis, a fastidious gram-negative pleomorphic bacillus.
The illness classically progresses through three phases, although infants may not follow distinct stages. The catarrhal stage lasts 1–2 weeks and resembles a mild upper respiratory infection with rhinorrhea, low-grade fever, malaise, sore throat, lacrimation, and mild cough. The paroxysmal stage lasts 1–6 weeks and is characterized by severe coughing spells that end with a sudden inspiratory “whoop.” Paroxysms may be associated with cyanosis, apnea (especially in infants under 6 months), post-tussive emesis, and altered mental status due to hypoxia. The convalescent stage lasts 2–12 weeks with gradual improvement and decreasing frequency of cough. Adults and partially immunized children often have milder or atypical presentations, sometimes limited to persistent cough without a classic whoop.
Diagnosis in the emergency setting is primarily clinical, especially when a characteristic paroxysmal cough is observed or there is a known exposure. Laboratory confirmation may support the diagnosis. PCR testing from a posterior nasopharyngeal swab or aspirate has high sensitivity and specificity but may produce false positives and false negatives depending on timing and prior antibiotic use. Culture on Bordet–Gengou medium remains the gold standard due to high specificity but has low sensitivity and requires 7–12 days for results. Serology is useful later in the course. Leukocytosis with marked lymphocytosis is common and correlates with disease severity. Chest radiographs are often normal but may show perihilar infiltrates, atelectasis, or secondary pneumonia.
Differential diagnoses include other causes of prolonged or paroxysmal cough such as infections with Bordetella parapertussis, Chlamydia species, adenovirus, pneumonia, bronchiolitis, influenza, reactive airway disease, foreign body aspiration, and cystic fibrosis.
Initial management focuses on airway and respiratory support. Oxygen supplementation and suctioning of mucus plugs are important, particularly in infants. Droplet precautions are required for 5 days after initiation of effective antimicrobial therapy. Adequate hydration must be maintained. Continuous monitoring is recommended during severe paroxysms, especially in infants. Antibiotics are most effective during the catarrhal phase but are still indicated during the paroxysmal phase to reduce transmission. Azithromycin is the first-line agent. Alternatives include clarithromycin, erythromycin, or trimethoprim–sulfamethoxazole, although erythromycin carries a risk of pyloric stenosis in neonates. Bronchodilators and corticosteroids are generally not recommended. Tdap vaccination should be offered when appropriate, including during each pregnancy between 27 and 36 weeks gestation to protect newborns.
Admission is indicated for patients under 1 year of age, those with apnea, cyanosis, pneumonia, encephalitis, or significant respiratory distress. Children without respiratory compromise may be discharged with close follow-up, hydration guidance, and avoidance of cough triggers such as smoke and pollutants. Postexposure prophylaxis with antibiotics is recommended for all close contacts regardless of age or immunization status. Patients may return to school or work after 5 days of appropriate antibiotic therapy.
Complications include epistaxis, subconjunctival hemorrhage, pneumonia, pneumothorax, subcutaneous or mediastinal emphysema, bronchiectasis, hernias, rectal prolapse, seizures, encephalitis, intracranial hemorrhage, and spinal epidural hemorrhage. Infants require particular vigilance due to high risk of apnea and severe respiratory compromise. Cases must be reported to public health authorities, and strict droplet precautions are essential to prevent spread.
Pertussis is an acute respiratory tract infection transmitted by small respiratory droplets. The organism attaches to respiratory epithelial cells via fimbriae and produces toxins that cause ciliary dysfunction, accumulation of debris, increased mucus production, and inflammatory infiltration. Bronchiolar congestion, obstruction, and necrosis may develop. Airway obstruction from mucus plugging can lead to hypoxia, hypoventilation, and increased intrathoracic or intracranial pressure. Secondary bacterial pneumonia may worsen respiratory failure. Central nervous system injury may result from encephalitis, hypoxia, or elevated intracranial pressure. Uncomplicated illness typically lasts 6–10 weeks, although about half resolve in under 6 weeks. Mortality is highest in infants under 1 year, especially those younger than 1 month. Most deaths are due to secondary bacterial pneumonia. The incubation period is usually 7–10 days. Disease is most common in young children, but incidence is increasing among adolescents. Adults serve as the primary reservoir. Peak incidence occurs in late summer and fall. Vaccination with Tdap provides prevention. The causative organism is Bordetella pertussis, a fastidious gram-negative pleomorphic bacillus.
The illness classically progresses through three phases, although infants may not follow distinct stages. The catarrhal stage lasts 1–2 weeks and resembles a mild upper respiratory infection with rhinorrhea, low-grade fever, malaise, sore throat, lacrimation, and mild cough. The paroxysmal stage lasts 1–6 weeks and is characterized by severe coughing spells that end with a sudden inspiratory “whoop.” Paroxysms may be associated with cyanosis, apnea (especially in infants under 6 months), post-tussive emesis, and altered mental status due to hypoxia. The convalescent stage lasts 2–12 weeks with gradual improvement and decreasing frequency of cough. Adults and partially immunized children often have milder or atypical presentations, sometimes limited to persistent cough without a classic whoop.
Diagnosis in the emergency setting is primarily clinical, especially when a characteristic paroxysmal cough is observed or there is a known exposure. Laboratory confirmation may support the diagnosis. PCR testing from a posterior nasopharyngeal swab or aspirate has high sensitivity and specificity but may produce false positives and false negatives depending on timing and prior antibiotic use. Culture on Bordet–Gengou medium remains the gold standard due to high specificity but has low sensitivity and requires 7–12 days for results. Serology is useful later in the course. Leukocytosis with marked lymphocytosis is common and correlates with disease severity. Chest radiographs are often normal but may show perihilar infiltrates, atelectasis, or secondary pneumonia.
Differential diagnoses include other causes of prolonged or paroxysmal cough such as infections with Bordetella parapertussis, Chlamydia species, adenovirus, pneumonia, bronchiolitis, influenza, reactive airway disease, foreign body aspiration, and cystic fibrosis.
Initial management focuses on airway and respiratory support. Oxygen supplementation and suctioning of mucus plugs are important, particularly in infants. Droplet precautions are required for 5 days after initiation of effective antimicrobial therapy. Adequate hydration must be maintained. Continuous monitoring is recommended during severe paroxysms, especially in infants. Antibiotics are most effective during the catarrhal phase but are still indicated during the paroxysmal phase to reduce transmission. Azithromycin is the first-line agent. Alternatives include clarithromycin, erythromycin, or trimethoprim–sulfamethoxazole, although erythromycin carries a risk of pyloric stenosis in neonates. Bronchodilators and corticosteroids are generally not recommended. Tdap vaccination should be offered when appropriate, including during each pregnancy between 27 and 36 weeks gestation to protect newborns.
Admission is indicated for patients under 1 year of age, those with apnea, cyanosis, pneumonia, encephalitis, or significant respiratory distress. Children without respiratory compromise may be discharged with close follow-up, hydration guidance, and avoidance of cough triggers such as smoke and pollutants. Postexposure prophylaxis with antibiotics is recommended for all close contacts regardless of age or immunization status. Patients may return to school or work after 5 days of appropriate antibiotic therapy.
Complications include epistaxis, subconjunctival hemorrhage, pneumonia, pneumothorax, subcutaneous or mediastinal emphysema, bronchiectasis, hernias, rectal prolapse, seizures, encephalitis, intracranial hemorrhage, and spinal epidural hemorrhage. Infants require particular vigilance due to high risk of apnea and severe respiratory compromise. Cases must be reported to public health authorities, and strict droplet precautions are essential to prevent spread.
- Published on
KembaraXtra – Emergency & Acute Medicine – Perirectal Abscess
Perirectal abscess is a localized infection with accumulation of purulent material adjacent to the anus or rectum. It most commonly results from infection of the anal crypt glands with spread into adjacent potential spaces separated by muscle and fascia. Perianal abscesses are the most common and typically present with a visible, tender red bulge near the anus. Ischiorectal abscesses occur in a large potential space and may grow significantly before diagnosis; they can communicate posteriorly to form a horseshoe abscess. Intersphincteric abscesses remain confined between the internal and external sphincters. Supralevator abscesses are deep, located above the levator ani, often present with systemic symptoms, and usually require operative drainage under general anesthesia. Infections are typically polymicrobial with mixed enteric organisms. Associated conditions include diabetes, inflammatory bowel disease, malignancy, and immunocompromised states.
Patients commonly present with constant perianal, rectal, or pelvic pain. Pain is often worsened by defecation, sitting, or coughing. Deeper abscesses such as ischiorectal or supralevator may produce dull pelvic or rectal pain and may be less painful if located above the dentate line. Fever, chills, constipation, and drainage may occur. On examination, findings include perianal swelling, erythema, induration, fluctuance, and marked tenderness. An abscess in the inner buttock cleft is a red flag, as rectal abscesses can track outward. Digital rectal examination is essential and may reveal rectal wall swelling or focal tenderness. A fistulous tract may be palpable as a cord-like structure or identified with gentle probing.
Diagnosis is primarily clinical and based on careful history and thorough rectal examination. A high index of suspicion is required in patients with persistent perirectal pain. Routine laboratory testing and imaging are not required for simple perianal abscesses. Leukocytosis with left shift may be present. Blood cultures are reserved for patients with signs of sepsis. CT scan with IV contrast or MRI is helpful when a deeper abscess is suspected or when the diagnosis is unclear. MRI is particularly useful for identifying fistulous tracts. Endoanal ultrasound may also assist in selected cases.
The differential diagnosis includes anal fissure, thrombosed or inflamed hemorrhoids, sentinel pile, anal ulcer, proctitis, and anorectal carcinoma.
Prompt incision and drainage are the definitive treatments. Delay in drainage may worsen outcomes. Bedside drainage is appropriate only for localized perianal abscesses. A radial incision should be made close to the anal verge, the cavity explored to break loculations, and copious irrigation performed. Loose packing may be placed and removed after 48 hours. Operative drainage under general anesthesia is indicated for deeper abscesses or when adequate drainage cannot be achieved with local anesthesia.
Antibiotics are not routinely required after adequate drainage but are indicated in patients with extensive cellulitis, systemic infection, immunosuppression, valvular heart disease, prosthetic devices, or diabetes. Oral options include amoxicillin-clavulanate or a fluoroquinolone with consideration for MRSA coverage when indicated. Intravenous regimens may include cefoxitin, ampicillin-sulbactam, or combination therapy with ampicillin, gentamicin, and either clindamycin or metronidazole.
Postprocedural care includes sitz baths three times daily beginning 24 hours after drainage, high-fiber diet or bulking agents, and adequate analgesia.
Patients requiring operative drainage or those with systemic toxicity or sepsis should be admitted. Patients with adequate bedside drainage and no systemic illness may be discharged with close follow-up. All patients should be referred to a surgeon within 24–48 hours to evaluate for fistula formation, which occurs in approximately 25–50% of anorectal abscesses.
Careful assessment of the extent of infection is critical. Thorough rectal examination and probing are mandatory, and imaging should be obtained when deeper extension is suspected. Deep abscesses above the dentate line may present with minimal pain and isolated fever, increasing the risk of delayed diagnosis.
- Published on
Infectious Diseases and Microbiology: Postoperative Fever
Basics
Description
Postoperative fever is defined as a body temperature above 38°C (100.4°F) occurring after an invasive procedure. It is classified by timing: immediate (during surgery or within hours), acute (within the first postoperative week), subacute (1–4 weeks after surgery), and delayed (more than one month postoperatively). Most cases result from the inflammatory response to surgery and resolve spontaneously, but fever may signal a serious complication. Evaluation requires careful history, physical examination, and appropriate laboratory and imaging studies, including cultures and Gram stains when indicated. Early postoperative fever is frequently noninfectious; however, fever persisting beyond 96 hours is more likely infectious. Consider that patients may have been incubating community-acquired infection preoperatively. New or persistent fever beyond four days strongly suggests ongoing pathology or a new complication. Surgical wounds, catheter insertion sites, and all dressings must be inspected, and recent interventions such as blood transfusions reviewed.
Epidemiology
Drug fever is the most common noninfectious cause of postoperative fever, most often linked to antimicrobials and heparin. Pneumonia is a common cause after cardiac surgery and occurs in more than 5% of such patients. Sternal wound infections after cardiothoracic surgery occur in up to 5%, typically around postoperative day seven. Postoperative aspergillosis after cardiothoracic procedures carries very high mortality. Fever alone is a poor predictor of infection, with low sensitivity. Postsurgical mediastinitis has high mortality. In obstetrics and gynecology, bacterial vaginosis may increase postoperative infection risk.
General Prevention
Aggressive pulmonary hygiene, including incentive spirometry and mobilization, reduces pulmonary complications such as atelectasis.
Etiology
Common infectious causes include urinary tract infection, pneumonia, sinusitis, suppurative thrombophlebitis, catheter-related infections, and Clostridioides difficile–associated diarrhea. Noninfectious causes include deep venous thrombosis, pulmonary embolism, subarachnoid hemorrhage, gout, and fat embolism. Surgical site infections are uncommon within the first 1–3 days except for aggressive pathogens such as group A streptococci or clostridia, which can present early. Atelectasis is frequently blamed but likely coincidental rather than causal. Other serious causes include transplant rejection. Drug-induced fever is most often associated with beta-lactams, antiepileptics, and heparin. Inflammatory states such as acute myocardial infarction, pancreatitis, or acute respiratory distress syndrome may produce fever without infection. Endocrine emergencies such as adrenal insufficiency or thyrotoxicosis may also present with fever.
Diagnosis
Physical Examination
Drug fever lacks specific features and usually develops days after medication exposure; rash and eosinophilia are uncommon. Malignant hyperthermia typically occurs intraoperatively but may be delayed up to 24 hours and is associated with agents such as succinylcholine or volatile anesthetics. Neuroleptic malignant syndrome is associated with antipsychotics, particularly haloperidol. Withdrawal syndromes from alcohol, opioids, barbiturates, or benzodiazepines may cause fever hours to days after admission, and prior substance use history may not be readily available.
Diagnostic Tests and Interpretation
Laboratory Studies
Urinalysis and urine culture are recommended in patients with indwelling catheters longer than 72 hours. Procalcitonin has uncertain value in distinguishing bacterial causes of postoperative fever.
Imaging
Duplex ultrasonography with Doppler should be considered for new extremity swelling suggestive of deep venous thrombosis. Routine chest radiography is not required within the first 72 postoperative hours if fever is the only indication.
Diagnostic Procedures/Other
Wound swab cultures are rarely useful unless there is clear clinical evidence of infection. Suspected deep intraabdominal abscess may require imaging and, if inconclusive, surgical exploration.
Treatment
Medications
Antibiotics are generally not indicated for early postoperative fever without evidence of infection. Critically ill patients or those with hemodynamic instability should receive empiric broad-spectrum antibiotics after thorough evaluation, but therapy should be discontinued after 48 hours if no infectious source is identified. Atelectasis management includes coughing exercises, incentive spirometry, chest physiotherapy, beta-2 agonists, intermittent positive-pressure breathing, and nebulization. Empiric antifungal therapy is not recommended initially.
Ongoing Care and Follow-Up
Drug fever is diagnosed by exclusion when other causes are ruled out. Surgical wounds and invasive device sites must be repeatedly examined for signs of infection.
Complications
Postoperative infections increase morbidity and mortality, may lead to sepsis, impair wound healing, and cause respiratory failure and other serious outcomes.
Basics
Description
Postoperative fever is defined as a body temperature above 38°C (100.4°F) occurring after an invasive procedure. It is classified by timing: immediate (during surgery or within hours), acute (within the first postoperative week), subacute (1–4 weeks after surgery), and delayed (more than one month postoperatively). Most cases result from the inflammatory response to surgery and resolve spontaneously, but fever may signal a serious complication. Evaluation requires careful history, physical examination, and appropriate laboratory and imaging studies, including cultures and Gram stains when indicated. Early postoperative fever is frequently noninfectious; however, fever persisting beyond 96 hours is more likely infectious. Consider that patients may have been incubating community-acquired infection preoperatively. New or persistent fever beyond four days strongly suggests ongoing pathology or a new complication. Surgical wounds, catheter insertion sites, and all dressings must be inspected, and recent interventions such as blood transfusions reviewed.
Epidemiology
Drug fever is the most common noninfectious cause of postoperative fever, most often linked to antimicrobials and heparin. Pneumonia is a common cause after cardiac surgery and occurs in more than 5% of such patients. Sternal wound infections after cardiothoracic surgery occur in up to 5%, typically around postoperative day seven. Postoperative aspergillosis after cardiothoracic procedures carries very high mortality. Fever alone is a poor predictor of infection, with low sensitivity. Postsurgical mediastinitis has high mortality. In obstetrics and gynecology, bacterial vaginosis may increase postoperative infection risk.
General Prevention
Aggressive pulmonary hygiene, including incentive spirometry and mobilization, reduces pulmonary complications such as atelectasis.
Etiology
Common infectious causes include urinary tract infection, pneumonia, sinusitis, suppurative thrombophlebitis, catheter-related infections, and Clostridioides difficile–associated diarrhea. Noninfectious causes include deep venous thrombosis, pulmonary embolism, subarachnoid hemorrhage, gout, and fat embolism. Surgical site infections are uncommon within the first 1–3 days except for aggressive pathogens such as group A streptococci or clostridia, which can present early. Atelectasis is frequently blamed but likely coincidental rather than causal. Other serious causes include transplant rejection. Drug-induced fever is most often associated with beta-lactams, antiepileptics, and heparin. Inflammatory states such as acute myocardial infarction, pancreatitis, or acute respiratory distress syndrome may produce fever without infection. Endocrine emergencies such as adrenal insufficiency or thyrotoxicosis may also present with fever.
Diagnosis
Physical Examination
Drug fever lacks specific features and usually develops days after medication exposure; rash and eosinophilia are uncommon. Malignant hyperthermia typically occurs intraoperatively but may be delayed up to 24 hours and is associated with agents such as succinylcholine or volatile anesthetics. Neuroleptic malignant syndrome is associated with antipsychotics, particularly haloperidol. Withdrawal syndromes from alcohol, opioids, barbiturates, or benzodiazepines may cause fever hours to days after admission, and prior substance use history may not be readily available.
Diagnostic Tests and Interpretation
Laboratory Studies
Urinalysis and urine culture are recommended in patients with indwelling catheters longer than 72 hours. Procalcitonin has uncertain value in distinguishing bacterial causes of postoperative fever.
Imaging
Duplex ultrasonography with Doppler should be considered for new extremity swelling suggestive of deep venous thrombosis. Routine chest radiography is not required within the first 72 postoperative hours if fever is the only indication.
Diagnostic Procedures/Other
Wound swab cultures are rarely useful unless there is clear clinical evidence of infection. Suspected deep intraabdominal abscess may require imaging and, if inconclusive, surgical exploration.
Treatment
Medications
Antibiotics are generally not indicated for early postoperative fever without evidence of infection. Critically ill patients or those with hemodynamic instability should receive empiric broad-spectrum antibiotics after thorough evaluation, but therapy should be discontinued after 48 hours if no infectious source is identified. Atelectasis management includes coughing exercises, incentive spirometry, chest physiotherapy, beta-2 agonists, intermittent positive-pressure breathing, and nebulization. Empiric antifungal therapy is not recommended initially.
Ongoing Care and Follow-Up
Drug fever is diagnosed by exclusion when other causes are ruled out. Surgical wounds and invasive device sites must be repeatedly examined for signs of infection.
Complications
Postoperative infections increase morbidity and mortality, may lead to sepsis, impair wound healing, and cause respiratory failure and other serious outcomes.

- Published on
Infectious Diseases and Microbiology: Red Eye
Basics
Description
Red eye may result from sight-threatening conditions such as uveitis, endophthalmitis, acute angle-closure glaucoma, or scleritis, which typically produce ciliary injection. More commonly, redness is due to conjunctival hyperemia associated with conjunctivitis, keratitis, dry eye disease, foreign body irritation (including contact lenses), blepharitis, or environmental irritants. Ocular trauma may cause subconjunctival hemorrhage. Not all causes are infectious. Uveitis involves intraocular inflammation and may be anterior, posterior, or pan-uveitis. Endophthalmitis is a severe intraocular infection involving the vitreous cavity. Acute angle-closure glaucoma is an ophthalmic emergency caused by obstruction of aqueous outflow and elevated intraocular pressure. Episcleritis affects superficial scleral tissues, while scleritis is a deeper, more severe inflammatory process that may occur with keratitis or uveitis. Conjunctivitis is the most common cause of red eye and usually includes discharge. Keratitis primarily affects the cornea.
Epidemiology
Primary acute angle closure occurs more frequently in Asian populations than in Caucasians. Incidence rates for conjunctivitis, keratitis, and uveitis vary and are addressed in their respective discussions.
Risk Factors
Risk factors for angle-closure glaucoma include advanced age, hyperopia, cataract, female sex, prior angle closure in the fellow eye, and Asian ethnicity; prophylactic laser iridotomy is often performed in the unaffected eye. Contact lens use increases the risk of bacterial keratitis. Subconjunctival hemorrhage may occur spontaneously or with bleeding disorders, minor trauma, or increased venous pressure from coughing or sneezing. Autoimmune connective tissue disorders are associated with ocular inflammation, and uveitis may be an initial manifestation.
General Prevention
Proper contact lens hygiene reduces infectious and inflammatory complications. Screening with gonioscopy and preventive laser iridotomy can prevent acute angle closure in high-risk individuals.
Pathophysiology
Ciliary injection involves deeper vascular branches and indicates inflammation of the cornea, iris, ciliary body, or sclera. Conjunctival injection is superficial, mobile with the conjunctiva, and improves with topical vasoconstrictors. Acute angle closure usually results from pupillary block, causing pressure differential between the posterior and anterior chambers, forward bowing of the iris, and obstruction of aqueous outflow through the trabecular meshwork.
Etiology
Conjunctivitis, keratitis, uveitis, and endophthalmitis have infectious and noninfectious causes. Acute angle-closure glaucoma and subconjunctival hemorrhage are noninfectious. Episcleritis is usually idiopathic, though immunologic reactions to herpes simplex or varicella zoster may occur. Scleritis is rarely infectious but may result from systemic infections or extension from keratitis; reported pathogens include fungi (Aspergillus, Fusarium), herpes viruses, mycobacteria, Nocardia, Pseudomonas, Proteus (after scleral buckle procedures), syphilis, leprosy, Lyme disease, and tuberculosis.
Commonly Associated Conditions
Endophthalmitis most commonly follows intraocular surgery. Contact lens wear strongly predisposes to bacterial keratitis.
Diagnosis
History
Subconjunctival hemorrhage is unilateral, painless, and vision is unaffected. Conjunctivitis often begins in one eye but is commonly bilateral and features discharge with minimal visual change. Keratitis is usually unilateral and associated with redness, foreign body sensation, tearing, and decreased vision. Uveitis presents with reduced vision, photophobia, and ocular pain. Acute angle-closure glaucoma presents with severe unilateral pain, decreased vision, nausea, and vomiting. Anterior scleritis causes severe pain and tenderness; posterior scleritis may cause significant visual impairment with less obvious redness. Episcleritis resembles conjunctivitis but has mild discomfort and no discharge. Endophthalmitis presents with pain and significant vision loss.
Physical Examination
Slit-lamp examination is essential. Subconjunctival hemorrhage appears as a sharply demarcated red patch under the conjunctiva. Conjunctivitis shows hyperemia, discharge, membranes or pseudomembranes, papillary or follicular reaction, and possibly preauricular lymphadenopathy. Keratitis reveals epithelial defects, stromal opacities, discharge, and anterior chamber inflammation. Anterior uveitis is diagnosed by inflammatory cells in the anterior chamber and keratic precipitates. Acute angle closure presents with a mid-dilated poorly reactive pupil, corneal edema, and elevated intraocular pressure.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine cultures are unnecessary in typical conjunctivitis except in hyperacute cases suggestive of Neisseria gonorrhoeae. Keratitis lesions are sampled for Gram stain and culture.
Imaging
Confocal microscopy assists in diagnosing Acanthamoeba keratitis. Neuroimaging may identify vascular abnormalities such as carotid-cavernous fistulas or arteriovenous malformations associated with red eye.
Diagnostic Procedures/Other
Corneal biopsy may be needed for refractory keratitis. Vitreous sampling during vitrectomy can assist in diagnosing uveitis or endophthalmitis via cytology, culture, and PCR.
Differential Diagnosis
Key distinguishing features include:
Visual acuity is typically preserved in conjunctivitis and subconjunctival hemorrhage but reduced in uveitis, keratitis, and acute angle closure. Discharge is common in conjunctivitis and keratitis but absent in subconjunctival hemorrhage, uveitis, and acute angle closure. Pain is absent in conjunctivitis and subconjunctival hemorrhage but present in uveitis, keratitis, and acute angle closure. Photophobia is typical of uveitis and sometimes keratitis. Pruritus suggests allergic conjunctivitis.
Treatment
Medications
Viral conjunctivitis is managed supportively with artificial tears and cold compresses; topical steroids are rarely required. Mild bacterial conjunctivitis is treated with topical antibiotics such as trimethoprim-polymyxin B or a fluoroquinolone for several days. Bacterial keratitis requires intensive fortified topical antibiotics administered hourly. Acute bacterial endophthalmitis is treated with intravitreal antibiotics targeting gram-positive and gram-negative organisms. Anterior uveitis is treated with topical corticosteroids and cycloplegic agents; infectious causes require specific antimicrobial therapy. Acute angle-closure glaucoma requires urgent reduction of intraocular pressure with systemic acetazolamide, intravenous mannitol, topical beta-blockers, and pilocarpine, followed by laser iridotomy. Episcleritis is treated with artificial tears, topical steroids, and oral NSAIDs. Scleritis often requires systemic corticosteroids and may necessitate immunomodulatory therapy depending on associated systemic disease.
Additional Treatment / Surgery
Laser iridotomy is definitive for angle closure after stabilization. Severe infectious keratitis or scleritis causing tissue thinning may require surgical grafting.
Prognosis
Outcome depends on etiology, ranging from benign in subconjunctival hemorrhage to guarded in endophthalmitis.
Complications
Chronic inflammation may lead to cataract formation, secondary glaucoma, and cystoid macular edema.
Basics
Description
Red eye may result from sight-threatening conditions such as uveitis, endophthalmitis, acute angle-closure glaucoma, or scleritis, which typically produce ciliary injection. More commonly, redness is due to conjunctival hyperemia associated with conjunctivitis, keratitis, dry eye disease, foreign body irritation (including contact lenses), blepharitis, or environmental irritants. Ocular trauma may cause subconjunctival hemorrhage. Not all causes are infectious. Uveitis involves intraocular inflammation and may be anterior, posterior, or pan-uveitis. Endophthalmitis is a severe intraocular infection involving the vitreous cavity. Acute angle-closure glaucoma is an ophthalmic emergency caused by obstruction of aqueous outflow and elevated intraocular pressure. Episcleritis affects superficial scleral tissues, while scleritis is a deeper, more severe inflammatory process that may occur with keratitis or uveitis. Conjunctivitis is the most common cause of red eye and usually includes discharge. Keratitis primarily affects the cornea.
Epidemiology
Primary acute angle closure occurs more frequently in Asian populations than in Caucasians. Incidence rates for conjunctivitis, keratitis, and uveitis vary and are addressed in their respective discussions.
Risk Factors
Risk factors for angle-closure glaucoma include advanced age, hyperopia, cataract, female sex, prior angle closure in the fellow eye, and Asian ethnicity; prophylactic laser iridotomy is often performed in the unaffected eye. Contact lens use increases the risk of bacterial keratitis. Subconjunctival hemorrhage may occur spontaneously or with bleeding disorders, minor trauma, or increased venous pressure from coughing or sneezing. Autoimmune connective tissue disorders are associated with ocular inflammation, and uveitis may be an initial manifestation.
General Prevention
Proper contact lens hygiene reduces infectious and inflammatory complications. Screening with gonioscopy and preventive laser iridotomy can prevent acute angle closure in high-risk individuals.
Pathophysiology
Ciliary injection involves deeper vascular branches and indicates inflammation of the cornea, iris, ciliary body, or sclera. Conjunctival injection is superficial, mobile with the conjunctiva, and improves with topical vasoconstrictors. Acute angle closure usually results from pupillary block, causing pressure differential between the posterior and anterior chambers, forward bowing of the iris, and obstruction of aqueous outflow through the trabecular meshwork.
Etiology
Conjunctivitis, keratitis, uveitis, and endophthalmitis have infectious and noninfectious causes. Acute angle-closure glaucoma and subconjunctival hemorrhage are noninfectious. Episcleritis is usually idiopathic, though immunologic reactions to herpes simplex or varicella zoster may occur. Scleritis is rarely infectious but may result from systemic infections or extension from keratitis; reported pathogens include fungi (Aspergillus, Fusarium), herpes viruses, mycobacteria, Nocardia, Pseudomonas, Proteus (after scleral buckle procedures), syphilis, leprosy, Lyme disease, and tuberculosis.
Commonly Associated Conditions
Endophthalmitis most commonly follows intraocular surgery. Contact lens wear strongly predisposes to bacterial keratitis.
Diagnosis
History
Subconjunctival hemorrhage is unilateral, painless, and vision is unaffected. Conjunctivitis often begins in one eye but is commonly bilateral and features discharge with minimal visual change. Keratitis is usually unilateral and associated with redness, foreign body sensation, tearing, and decreased vision. Uveitis presents with reduced vision, photophobia, and ocular pain. Acute angle-closure glaucoma presents with severe unilateral pain, decreased vision, nausea, and vomiting. Anterior scleritis causes severe pain and tenderness; posterior scleritis may cause significant visual impairment with less obvious redness. Episcleritis resembles conjunctivitis but has mild discomfort and no discharge. Endophthalmitis presents with pain and significant vision loss.
Physical Examination
Slit-lamp examination is essential. Subconjunctival hemorrhage appears as a sharply demarcated red patch under the conjunctiva. Conjunctivitis shows hyperemia, discharge, membranes or pseudomembranes, papillary or follicular reaction, and possibly preauricular lymphadenopathy. Keratitis reveals epithelial defects, stromal opacities, discharge, and anterior chamber inflammation. Anterior uveitis is diagnosed by inflammatory cells in the anterior chamber and keratic precipitates. Acute angle closure presents with a mid-dilated poorly reactive pupil, corneal edema, and elevated intraocular pressure.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine cultures are unnecessary in typical conjunctivitis except in hyperacute cases suggestive of Neisseria gonorrhoeae. Keratitis lesions are sampled for Gram stain and culture.
Imaging
Confocal microscopy assists in diagnosing Acanthamoeba keratitis. Neuroimaging may identify vascular abnormalities such as carotid-cavernous fistulas or arteriovenous malformations associated with red eye.
Diagnostic Procedures/Other
Corneal biopsy may be needed for refractory keratitis. Vitreous sampling during vitrectomy can assist in diagnosing uveitis or endophthalmitis via cytology, culture, and PCR.
Differential Diagnosis
Key distinguishing features include:
Visual acuity is typically preserved in conjunctivitis and subconjunctival hemorrhage but reduced in uveitis, keratitis, and acute angle closure. Discharge is common in conjunctivitis and keratitis but absent in subconjunctival hemorrhage, uveitis, and acute angle closure. Pain is absent in conjunctivitis and subconjunctival hemorrhage but present in uveitis, keratitis, and acute angle closure. Photophobia is typical of uveitis and sometimes keratitis. Pruritus suggests allergic conjunctivitis.
Treatment
Medications
Viral conjunctivitis is managed supportively with artificial tears and cold compresses; topical steroids are rarely required. Mild bacterial conjunctivitis is treated with topical antibiotics such as trimethoprim-polymyxin B or a fluoroquinolone for several days. Bacterial keratitis requires intensive fortified topical antibiotics administered hourly. Acute bacterial endophthalmitis is treated with intravitreal antibiotics targeting gram-positive and gram-negative organisms. Anterior uveitis is treated with topical corticosteroids and cycloplegic agents; infectious causes require specific antimicrobial therapy. Acute angle-closure glaucoma requires urgent reduction of intraocular pressure with systemic acetazolamide, intravenous mannitol, topical beta-blockers, and pilocarpine, followed by laser iridotomy. Episcleritis is treated with artificial tears, topical steroids, and oral NSAIDs. Scleritis often requires systemic corticosteroids and may necessitate immunomodulatory therapy depending on associated systemic disease.
Additional Treatment / Surgery
Laser iridotomy is definitive for angle closure after stabilization. Severe infectious keratitis or scleritis causing tissue thinning may require surgical grafting.
Prognosis
Outcome depends on etiology, ranging from benign in subconjunctival hemorrhage to guarded in endophthalmitis.
Complications
Chronic inflammation may lead to cataract formation, secondary glaucoma, and cystoid macular edema.

