- Published on
Emergency And Acute Medicine – Immunizations
Basics
Description Immunization enhances resistance to infectious diseases through passive or active mechanisms. Passive immunization involves administration of antibodies or maternal antibody transfer via placenta or breast milk. Active immunization stimulates the immune system, producing IgM antibodies within 7–10 days followed by IgG antibodies peaking at 2–6 weeks. Oral and nasal vaccines induce mucosal IgA, whereas parenteral vaccines primarily induce systemic immunity. Improper storage, dosing, or administration route can reduce effectiveness.
Etiology
Live attenuated vaccines (e.g., measles, mumps, rubella, varicella, rotavirus) replicate in the host and may cause severe disease in immunocompromised patients. Inactivated vaccines (e.g., IPV, hepatitis A, influenza, pertussis) are safe in immunocompromised patients. Toxoid, subunit, and conjugate vaccines (e.g., tetanus, diphtheria, Hib, pneumococcus, meningococcus, HPV) use antigenic components to stimulate immunity. Hepatitis B vaccines are produced using recombinant DNA technology. Combination vaccines reduce injection burden but increase cost.
Epidemiology
Widespread immunization has markedly reduced many life-threatening infections. Polio has been eliminated from the Western Hemisphere. Hib, diphtheria, and tetanus are now rare in North America. Measles, rubella, and varicella persist mainly in unimmunized populations and travelers. Conjugate pneumococcal vaccines have reduced invasive disease by more than 90% for vaccine serotypes. Rotavirus vaccines reduce severe gastroenteritis. Annual influenza vaccines are produced based on global surveillance. Immunization schedules are tailored by age, pregnancy status, comorbidities, travel, occupation, and immune status.
Diagnosis
Signs And Symptoms Adverse events are usually mild and self-limited. Common reactions include local pain, swelling, erythema, and low-grade fever. Fever is seen after rotavirus, pneumococcal, HPV, MMR/MMRV, meningococcal, and influenza vaccines. Rash may follow varicella or MMR vaccines. Neurologic adverse events are rare and include febrile seizures, hypotonic–hyporesponsive episodes, and very rarely encephalopathy or Guillain–Barré syndrome. Gastrointestinal symptoms may occur after rotavirus vaccine. Live attenuated intranasal influenza vaccine may cause mild respiratory symptoms.
Essential Workup
Review immunization status during ED visits. Determine reasons for incomplete vaccination. Identify true contraindications, including prior anaphylaxis to a vaccine or specific components (e.g., yeast for HepB, egg protein for influenza, neomycin or gelatin for MMR). Assess for conditions requiring deferral, such as moderate to severe acute illness, immunodeficiency, pregnancy (for live vaccines), or recent immune globulin administration.
Treatment
Prehospital And Initial Stabilization Focus on airway, breathing, and circulation.
Emergency Department Management Treat anaphylaxis with epinephrine, antihistamines, bronchodilators, and IV fluids. Manage local reactions with cold compresses and analgesics. Treat fever, myalgias, and arthralgias with acetaminophen or ibuprofen. Manage seizures with benzodiazepines. Provide active or passive immunization as indicated for wound management or exposure prophylaxis. Avoid salicylates for 6 weeks after varicella vaccination in children.
Medication
Acetaminophen 15 mg/kg/dose PO q4–6h.
Ibuprofen 10 mg/kg/dose PO q6–8h.
Follow-Up And Disposition
Admission Criteria Serious adverse reactions such as anaphylaxis, encephalopathy, or severe neurologic symptoms.
Discharge Criteria Routine postimmunization reactions without complications.
Follow-Up Recommendations Arrange primary care follow-up to complete immunization schedules. Report unexpected adverse events to the Vaccine Adverse Event Reporting System.
Key Points And Cautions
Most vaccine reactions are mild and self-limited. True contraindications are rare. Failure to recognize contraindications or to continue antihistamines after allergic reactions may lead to complications. Immunization remains one of the most effective preventive interventions in emergency and acute medicine.
Basics
Description Immunization enhances resistance to infectious diseases through passive or active mechanisms. Passive immunization involves administration of antibodies or maternal antibody transfer via placenta or breast milk. Active immunization stimulates the immune system, producing IgM antibodies within 7–10 days followed by IgG antibodies peaking at 2–6 weeks. Oral and nasal vaccines induce mucosal IgA, whereas parenteral vaccines primarily induce systemic immunity. Improper storage, dosing, or administration route can reduce effectiveness.
Etiology
Live attenuated vaccines (e.g., measles, mumps, rubella, varicella, rotavirus) replicate in the host and may cause severe disease in immunocompromised patients. Inactivated vaccines (e.g., IPV, hepatitis A, influenza, pertussis) are safe in immunocompromised patients. Toxoid, subunit, and conjugate vaccines (e.g., tetanus, diphtheria, Hib, pneumococcus, meningococcus, HPV) use antigenic components to stimulate immunity. Hepatitis B vaccines are produced using recombinant DNA technology. Combination vaccines reduce injection burden but increase cost.
Epidemiology
Widespread immunization has markedly reduced many life-threatening infections. Polio has been eliminated from the Western Hemisphere. Hib, diphtheria, and tetanus are now rare in North America. Measles, rubella, and varicella persist mainly in unimmunized populations and travelers. Conjugate pneumococcal vaccines have reduced invasive disease by more than 90% for vaccine serotypes. Rotavirus vaccines reduce severe gastroenteritis. Annual influenza vaccines are produced based on global surveillance. Immunization schedules are tailored by age, pregnancy status, comorbidities, travel, occupation, and immune status.
Diagnosis
Signs And Symptoms Adverse events are usually mild and self-limited. Common reactions include local pain, swelling, erythema, and low-grade fever. Fever is seen after rotavirus, pneumococcal, HPV, MMR/MMRV, meningococcal, and influenza vaccines. Rash may follow varicella or MMR vaccines. Neurologic adverse events are rare and include febrile seizures, hypotonic–hyporesponsive episodes, and very rarely encephalopathy or Guillain–Barré syndrome. Gastrointestinal symptoms may occur after rotavirus vaccine. Live attenuated intranasal influenza vaccine may cause mild respiratory symptoms.
Essential Workup
Review immunization status during ED visits. Determine reasons for incomplete vaccination. Identify true contraindications, including prior anaphylaxis to a vaccine or specific components (e.g., yeast for HepB, egg protein for influenza, neomycin or gelatin for MMR). Assess for conditions requiring deferral, such as moderate to severe acute illness, immunodeficiency, pregnancy (for live vaccines), or recent immune globulin administration.
Treatment
Prehospital And Initial Stabilization Focus on airway, breathing, and circulation.
Emergency Department Management Treat anaphylaxis with epinephrine, antihistamines, bronchodilators, and IV fluids. Manage local reactions with cold compresses and analgesics. Treat fever, myalgias, and arthralgias with acetaminophen or ibuprofen. Manage seizures with benzodiazepines. Provide active or passive immunization as indicated for wound management or exposure prophylaxis. Avoid salicylates for 6 weeks after varicella vaccination in children.
Medication
Acetaminophen 15 mg/kg/dose PO q4–6h.
Ibuprofen 10 mg/kg/dose PO q6–8h.
Follow-Up And Disposition
Admission Criteria Serious adverse reactions such as anaphylaxis, encephalopathy, or severe neurologic symptoms.
Discharge Criteria Routine postimmunization reactions without complications.
Follow-Up Recommendations Arrange primary care follow-up to complete immunization schedules. Report unexpected adverse events to the Vaccine Adverse Event Reporting System.
Key Points And Cautions
Most vaccine reactions are mild and self-limited. True contraindications are rare. Failure to recognize contraindications or to continue antihistamines after allergic reactions may lead to complications. Immunization remains one of the most effective preventive interventions in emergency and acute medicine.
- Published on
Emergency And Acute Medicine – Idiopathic Thrombocytopenic Purpura
Basics
Description Idiopathic thrombocytopenic purpura (ITP) is isolated thrombocytopenia without an identifiable cause and with normal other cell lines. Incidence is approximately 2–5 per 100,000 per year. Acute ITP commonly affects children, with about 80% recovering within 8 weeks with or without therapy. Chronic ITP occurs mainly in adults, particularly young women, and often requires treatment to achieve remission. Refractory chronic ITP is characterized by fluctuating platelet counts and poor response to therapy.
Etiology
Immune-mediated platelet destruction due to autoantibodies, primarily IgG, leading to splenic and hepatic macrophage clearance. Some patients lack detectable autoantibodies, suggesting T-cell–mediated cytotoxicity. Complement activation may contribute. Decreased platelet production may occur in chronic or refractory disease. Eradication of Helicobacter pylori has been associated with platelet recovery in some patients.
Diagnosis
Signs And Symptoms
History: Mucocutaneous bleeding is most common, including epistaxis, gingival bleeding, menorrhagia, and conjunctival hemorrhage. Gastrointestinal bleeding, hemarthrosis, hematuria, and hematomas are uncommon. Pediatric cases often follow viral illness by 2–3 weeks. Adults typically have insidious onset; up to one-quarter are asymptomatic.
Physical exam: Petechiae and nonpalpable purpura are common. Spleen size is normal; splenomegaly suggests an alternate diagnosis. Intracranial hemorrhage is the most serious complication and leading cause of death, with risk increasing with age.
Essential Workup
Diagnosis of exclusion. CBC with differential and peripheral smear. PT and PTT if bleeding. Renal and liver function tests. Type and screen if bleeding. Pregnancy test when appropriate. Consider HIV testing.
Diagnosis Tests And Interpretation
Labs: Isolated thrombocytopenia with increased mean platelet volume. Normal RBC and WBC morphology. Normal coagulation studies and liver function.
Imaging: Noncontrast CT head if headache, neurologic deficits, trauma, or concern for intracranial hemorrhage.
Procedures: Bone marrow biopsy in patients >60 years, atypical cases, refractory disease, or prior to splenectomy. Antibody testing is not clinically useful.
Differential Diagnosis
Bone marrow failure or infiltration, splenic sequestration, thrombotic microangiopathies, disseminated intravascular coagulation, HELLP syndrome, valvular disease, and drug-induced thrombocytopenia.
Treatment
Prehospital And Initial Stabilization ABCs with attention to airway in severe mucosal bleeding or CNS hemorrhage. Establish IV access. Control bleeding with direct pressure.
Emergency Department Management Management depends on platelet count, bleeding severity, duration, age, and comorbidities. Observation is appropriate for children without bleeding or profound thrombocytopenia. Life-threatening bleeding requires high-dose IV corticosteroids, IVIG, and platelet transfusions (given after steroids or IVIG). Platelet transfusions alone are often ineffective. Aminocaproic acid may be considered for mucosal bleeding.
Medication
First line: High-dose glucocorticoids (dexamethasone 40 mg daily or prednisone 1–2 mg/kg/day), IVIG 1–2 g/kg for critical bleeding or urgent platelet rise, Anti-D immunoglobulin in Rh-positive patients.
Second line: Immunosuppressive agents, rituximab, thrombopoietin receptor agonists, or splenectomy for refractory disease.
Pregnancy Considerations
Differentiate from gestational thrombocytopenia and HELLP syndrome. Maternal platelet count does not predict neonatal thrombocytopenia. Mode of delivery is based on obstetric indications. Neonates should be screened and treated if thrombocytopenic.
Follow-Up And Disposition
Admission Criteria Life-threatening bleeding, any bleeding with platelets <20,000 />micro;L, asymptomatic patients with platelets <20,000 />micro;L and unreliable follow-up.
Discharge Criteria Asymptomatic patients or minor bleeding with platelets >30,000/µL.
Follow-Up Recommendations Hematology follow-up is required in all cases.
Key Points And Cautions
Exclude pseudothrombocytopenia before diagnosis. Spontaneous bleeding is uncommon until platelets fall below 10,000/µL. Intracranial hemorrhage risk increases with age and mandates urgent evaluation.
Basics
Description Idiopathic thrombocytopenic purpura (ITP) is isolated thrombocytopenia without an identifiable cause and with normal other cell lines. Incidence is approximately 2–5 per 100,000 per year. Acute ITP commonly affects children, with about 80% recovering within 8 weeks with or without therapy. Chronic ITP occurs mainly in adults, particularly young women, and often requires treatment to achieve remission. Refractory chronic ITP is characterized by fluctuating platelet counts and poor response to therapy.
Etiology
Immune-mediated platelet destruction due to autoantibodies, primarily IgG, leading to splenic and hepatic macrophage clearance. Some patients lack detectable autoantibodies, suggesting T-cell–mediated cytotoxicity. Complement activation may contribute. Decreased platelet production may occur in chronic or refractory disease. Eradication of Helicobacter pylori has been associated with platelet recovery in some patients.
Diagnosis
Signs And Symptoms
History: Mucocutaneous bleeding is most common, including epistaxis, gingival bleeding, menorrhagia, and conjunctival hemorrhage. Gastrointestinal bleeding, hemarthrosis, hematuria, and hematomas are uncommon. Pediatric cases often follow viral illness by 2–3 weeks. Adults typically have insidious onset; up to one-quarter are asymptomatic.
Physical exam: Petechiae and nonpalpable purpura are common. Spleen size is normal; splenomegaly suggests an alternate diagnosis. Intracranial hemorrhage is the most serious complication and leading cause of death, with risk increasing with age.
Essential Workup
Diagnosis of exclusion. CBC with differential and peripheral smear. PT and PTT if bleeding. Renal and liver function tests. Type and screen if bleeding. Pregnancy test when appropriate. Consider HIV testing.
Diagnosis Tests And Interpretation
Labs: Isolated thrombocytopenia with increased mean platelet volume. Normal RBC and WBC morphology. Normal coagulation studies and liver function.
Imaging: Noncontrast CT head if headache, neurologic deficits, trauma, or concern for intracranial hemorrhage.
Procedures: Bone marrow biopsy in patients >60 years, atypical cases, refractory disease, or prior to splenectomy. Antibody testing is not clinically useful.
Differential Diagnosis
Bone marrow failure or infiltration, splenic sequestration, thrombotic microangiopathies, disseminated intravascular coagulation, HELLP syndrome, valvular disease, and drug-induced thrombocytopenia.
Treatment
Prehospital And Initial Stabilization ABCs with attention to airway in severe mucosal bleeding or CNS hemorrhage. Establish IV access. Control bleeding with direct pressure.
Emergency Department Management Management depends on platelet count, bleeding severity, duration, age, and comorbidities. Observation is appropriate for children without bleeding or profound thrombocytopenia. Life-threatening bleeding requires high-dose IV corticosteroids, IVIG, and platelet transfusions (given after steroids or IVIG). Platelet transfusions alone are often ineffective. Aminocaproic acid may be considered for mucosal bleeding.
Medication
First line: High-dose glucocorticoids (dexamethasone 40 mg daily or prednisone 1–2 mg/kg/day), IVIG 1–2 g/kg for critical bleeding or urgent platelet rise, Anti-D immunoglobulin in Rh-positive patients.
Second line: Immunosuppressive agents, rituximab, thrombopoietin receptor agonists, or splenectomy for refractory disease.
Pregnancy Considerations
Differentiate from gestational thrombocytopenia and HELLP syndrome. Maternal platelet count does not predict neonatal thrombocytopenia. Mode of delivery is based on obstetric indications. Neonates should be screened and treated if thrombocytopenic.
Follow-Up And Disposition
Admission Criteria Life-threatening bleeding, any bleeding with platelets <20,000 />micro;L, asymptomatic patients with platelets <20,000 />micro;L and unreliable follow-up.
Discharge Criteria Asymptomatic patients or minor bleeding with platelets >30,000/µL.
Follow-Up Recommendations Hematology follow-up is required in all cases.
Key Points And Cautions
Exclude pseudothrombocytopenia before diagnosis. Spontaneous bleeding is uncommon until platelets fall below 10,000/µL. Intracranial hemorrhage risk increases with age and mandates urgent evaluation.
- Published on
Emergency And Acute Medicine – Hypothyroidism
Basics
Description Decreased effective circulating thyroid hormone causes reduced metabolic rate and diminished catecholamine sensitivity. More common in women and the elderly. Myxedema coma is a rare, life-threatening decompensation marked by altered mental status and impaired thermoregulation precipitated by stress in a hypothyroid patient.
Etiology
Primary causes include idiopathic, congenital, autoimmune thyroiditis (Hashimoto disease), iodine deficiency (most common worldwide), neoplasm, infection, and iatrogenic causes (thyroid surgery, radioiodine, external radiation). Drug induced causes include iodides, lithium, amiodarone, sunitinib, bexarotene, interferons, narcotics, and sedatives. Central hypothyroidism is rare and due to pituitary or hypothalamic dysfunction, often with other hormone deficiencies.
Myxedema coma is triggered by infection, hypothermia, intoxication, drugs, stroke, heart failure, trauma, or pregnancy.
Diagnosis
Signs And Symptoms
History: Fatigue, cold intolerance, weight gain, constipation, depression, cognitive slowing, headaches, myalgias, muscle weakness, menorrhagia, infertility, carpal tunnel syndrome.
Physical exam: Periorbital edema, coarse sparse hair, brittle nails, loss of lateral third of eyebrows, hoarse voice, goiter, dry pale cool skin, nonpitting edema, prolonged relaxation of deep tendon reflexes.
Myxedema coma: Altered mental status, hypothermia, hypotension, bradycardia, respiratory failure.
Pediatric And Geriatric Considerations
Congenital hypothyroidism largely prevented by newborn screening. Childhood disease usually due to Hashimoto thyroiditis and may impair growth and development. Elderly patients may present atypically, mimicking normal aging.
Essential Workup
Laboratory confirmation may not be immediately available; treatment should be initiated based on clinical suspicion in severe cases.
Diagnosis Tests And Interpretation
Labs: Low total and free T4 and T3. TSH elevated in primary hypothyroidism, normal or low in central causes. Associated findings include anemia, hyponatremia, hypoglycemia, hypoxemia, hypercapnia, respiratory acidosis, elevated CK, LDH, cholesterol, and creatinine.
Imaging: Chest radiograph may show cardiomegaly from pericardial effusion.
ECG: Sinus bradycardia, low voltage, PR prolongation, bundle branch blocks, QT prolongation, nonspecific ST–T changes; Osborn waves if profoundly hypothermic.
Differential Diagnosis
Chronic kidney disease, heart failure, depression, hypoalbuminemia, pernicious anemia, nephrotic syndrome, sepsis.
Alert Euthyroid sick syndrome may cause abnormal thyroid tests during acute illness.
Treatment
Initial Stabilization/Therapy ABCs with airway protection and ventilation as needed. Cardiac monitoring, oxygen supplementation, cautious passive rewarming. Avoid aggressive rewarming.
Emergency Department Treatment/Procedures
Mild hypothyroidism: Outpatient oral thyroid hormone replacement.
Myxedema coma: Medical emergency. Initiate IV thyroid hormone replacement immediately on suspicion. Use lower doses and avoid aggressive T3 in elderly or cardiac patients. Administer hydrocortisone to prevent adrenal crisis. Treat hypoglycemia with dextrose, hypotension with IV fluids (pressors often ineffective until thyroid hormone given), severe hyponatremia with hypertonic saline if indicated. Identify and treat precipitating cause.
Medication
First line thyroid hormone therapy:
• T4 IV load ~2 μg/kg (ideal body weight) then 10–40 μg IV or PO daily
• Optional T3 IV 10 μg load then 10 μg IV q8–12h (avoid in elderly/cardiac patients)
Second line/supportive: Hydrocortisone 100 mg IV q6–8h, dextrose IV for hypoglycemia.
Follow-Up And Disposition
Admission Criteria All patients with myxedema coma require ICU admission.
Discharge Criteria Uncomplicated hypothyroidism suitable for outpatient management.
Follow-Up Recommendations Primary care or endocrinology follow-up for long-term thyroid hormone management. Pregnant, elderly, and cardiac patients require cautious dose titration.
Key Points And Cautions
Symptoms are nonspecific and easily overlooked. Myxedema coma has high mortality and requires prompt treatment. Do not delay therapy awaiting lab confirmation. Avoid aggressive T3 use in elderly or patients with ischemic heart disease.
Basics
Description Decreased effective circulating thyroid hormone causes reduced metabolic rate and diminished catecholamine sensitivity. More common in women and the elderly. Myxedema coma is a rare, life-threatening decompensation marked by altered mental status and impaired thermoregulation precipitated by stress in a hypothyroid patient.
Etiology
Primary causes include idiopathic, congenital, autoimmune thyroiditis (Hashimoto disease), iodine deficiency (most common worldwide), neoplasm, infection, and iatrogenic causes (thyroid surgery, radioiodine, external radiation). Drug induced causes include iodides, lithium, amiodarone, sunitinib, bexarotene, interferons, narcotics, and sedatives. Central hypothyroidism is rare and due to pituitary or hypothalamic dysfunction, often with other hormone deficiencies.
Myxedema coma is triggered by infection, hypothermia, intoxication, drugs, stroke, heart failure, trauma, or pregnancy.
Diagnosis
Signs And Symptoms
History: Fatigue, cold intolerance, weight gain, constipation, depression, cognitive slowing, headaches, myalgias, muscle weakness, menorrhagia, infertility, carpal tunnel syndrome.
Physical exam: Periorbital edema, coarse sparse hair, brittle nails, loss of lateral third of eyebrows, hoarse voice, goiter, dry pale cool skin, nonpitting edema, prolonged relaxation of deep tendon reflexes.
Myxedema coma: Altered mental status, hypothermia, hypotension, bradycardia, respiratory failure.
Pediatric And Geriatric Considerations
Congenital hypothyroidism largely prevented by newborn screening. Childhood disease usually due to Hashimoto thyroiditis and may impair growth and development. Elderly patients may present atypically, mimicking normal aging.
Essential Workup
Laboratory confirmation may not be immediately available; treatment should be initiated based on clinical suspicion in severe cases.
Diagnosis Tests And Interpretation
Labs: Low total and free T4 and T3. TSH elevated in primary hypothyroidism, normal or low in central causes. Associated findings include anemia, hyponatremia, hypoglycemia, hypoxemia, hypercapnia, respiratory acidosis, elevated CK, LDH, cholesterol, and creatinine.
Imaging: Chest radiograph may show cardiomegaly from pericardial effusion.
ECG: Sinus bradycardia, low voltage, PR prolongation, bundle branch blocks, QT prolongation, nonspecific ST–T changes; Osborn waves if profoundly hypothermic.
Differential Diagnosis
Chronic kidney disease, heart failure, depression, hypoalbuminemia, pernicious anemia, nephrotic syndrome, sepsis.
Alert Euthyroid sick syndrome may cause abnormal thyroid tests during acute illness.
Treatment
Initial Stabilization/Therapy ABCs with airway protection and ventilation as needed. Cardiac monitoring, oxygen supplementation, cautious passive rewarming. Avoid aggressive rewarming.
Emergency Department Treatment/Procedures
Mild hypothyroidism: Outpatient oral thyroid hormone replacement.
Myxedema coma: Medical emergency. Initiate IV thyroid hormone replacement immediately on suspicion. Use lower doses and avoid aggressive T3 in elderly or cardiac patients. Administer hydrocortisone to prevent adrenal crisis. Treat hypoglycemia with dextrose, hypotension with IV fluids (pressors often ineffective until thyroid hormone given), severe hyponatremia with hypertonic saline if indicated. Identify and treat precipitating cause.
Medication
First line thyroid hormone therapy:
• T4 IV load ~2 μg/kg (ideal body weight) then 10–40 μg IV or PO daily
• Optional T3 IV 10 μg load then 10 μg IV q8–12h (avoid in elderly/cardiac patients)
Second line/supportive: Hydrocortisone 100 mg IV q6–8h, dextrose IV for hypoglycemia.
Follow-Up And Disposition
Admission Criteria All patients with myxedema coma require ICU admission.
Discharge Criteria Uncomplicated hypothyroidism suitable for outpatient management.
Follow-Up Recommendations Primary care or endocrinology follow-up for long-term thyroid hormone management. Pregnant, elderly, and cardiac patients require cautious dose titration.
Key Points And Cautions
Symptoms are nonspecific and easily overlooked. Myxedema coma has high mortality and requires prompt treatment. Do not delay therapy awaiting lab confirmation. Avoid aggressive T3 use in elderly or patients with ischemic heart disease.

- Published on
Emergency And Acute Medicine – Hypothermia
Basics
Description Core body temperature <35°c. risk factors include impaired thermoregulation (infants, elderly), comorbid illness, intoxication, and environmental exposure. heat loss occurs via radiation (most significant), conduction, convection, evaporation, respiration. production relies on shivering, nonshivering thermogenesis, increased thyroxine epinephrine.< />pan>
Etiology
Dermal disease (burns, exfoliative dermatitis, severe psoriasis). Drug induced (ethanol, phenothiazines, sedative–hypnotics). Environmental exposure (immersion, nonimmersion). Iatrogenic causes (aggressive fluid resuscitation, heat stroke treatment). Metabolic disorders (hypothyroidism, hypopituitarism, hypoadrenalism). Neurologic conditions (spinal cord injury, head trauma, stroke, tumor, Wernicke disease). Neuromuscular inefficiency (extremes of age, impaired shivering, lack of acclimatization). Sepsis. Pediatric patients are at higher risk because of increased surface area to mass ratio; consider nonaccidental trauma.
Diagnosis
Signs And Symptoms
Mild (35–32.2°C): Hypertension, shivering, tachycardia progressing to bradycardia, tachypnea, vasoconstriction, apathy, ataxia, cold diuresis, impaired judgment.
Moderate (32.2–28°C): Atrial dysrhythmias, bradycardia refractory to atropine, decreased level of consciousness, hypoventilation with CO₂ retention, dilated pupils, diminished gag reflex, cessation of shivering, hyporeflexia, hypotension, J (Osborn) waves.
Severe (<28°c): apnea, coma, minimal eeg activity, nonreactive pupils, oliguria, pulmonary edema, ventricular dysrhythmias or asystole.< />pan>
History Duration and circumstances of cold exposure or submersion.
Physical Exam Pulse and blood pressure may be difficult to detect; pupils often dilated at very low temperatures.
Essential Workup Accurate core temperature measurement.
Diagnosis Tests And Interpretation
Lab Fingerstick glucose, ABG (no temperature correction), CBC (hemoconcentration), electrolytes, BUN/creatinine, potassium, CPK, lactate, coagulation studies, toxicology screen.
Imaging CXR for pneumonia.
ECG Bradyarrhythmias, atrial fibrillation, ventricular fibrillation, prolonged PR/QRS/QT, Osborn waves.
Differential Diagnosis Environmental exposure, sepsis, CNS pathology, metabolic disorders, drug toxicity.
Treatment
Prehospital Patient is not dead until “warm and dead.” Prolonged pulse checks (30–45 s). CPR during transport if indicated.
Initial Stabilization/Therapy ABCs, supplemental oxygen, safe intubation if needed, cardiac monitoring, warmed IV fluids (D5NS preferred), remove wet clothing, passive rewarming, naloxone, dextrose, and thiamine for altered mental status, stress-dose steroids if adrenal insufficiency suspected.
Emergency Department Treatment/Procedures Handle gently to avoid precipitating ventricular fibrillation. Most dysrhythmias resolve with rewarming alone. Defibrillate up to 1–3 times below 28–30°C, then defer until rewarmed. Active rewarming is required for core temperature <32°c. use passive external rewarming for mild cases, active (forced warm air, trunk first) moderate and core (humidified oxygen, warmed iv fluids, peritoneal or pleural lavage, extracorporeal including hemodialysis cardiopulmonary bypass) severe hypothermia cardiac arrest. faster rates (1–2°c />r) are associated with better outcomes.
Medication Amiodarone for persistent ventricular dysrhythmias after rewarming, dextrose for hypoglycemia, hydrocortisone or methylprednisolone if adrenal insufficiency suspected, levothyroxine only for myxedema coma, naloxone, thiamine.
Follow-Up And Disposition
Admission Criteria Moderate to severe hypothermia (<32°c).< />pan>
Discharge Criteria Young, healthy patients with very mild hypothermia who normalize and have a safe, warm environment.
Follow-Up Recommendations Social services involvement for patients at risk of recurrent cold exposure.
Key Points And Cautions Defibrillation is rarely effective below 28–30°C. Atrial fibrillation often resolves with rewarming alone. Beware afterdrop and rewarming shock. Gentle handling and adequate volume resuscitation are essential.
Basics
Description Core body temperature <35°c. risk factors include impaired thermoregulation (infants, elderly), comorbid illness, intoxication, and environmental exposure. heat loss occurs via radiation (most significant), conduction, convection, evaporation, respiration. production relies on shivering, nonshivering thermogenesis, increased thyroxine epinephrine.< />pan>
Etiology
Dermal disease (burns, exfoliative dermatitis, severe psoriasis). Drug induced (ethanol, phenothiazines, sedative–hypnotics). Environmental exposure (immersion, nonimmersion). Iatrogenic causes (aggressive fluid resuscitation, heat stroke treatment). Metabolic disorders (hypothyroidism, hypopituitarism, hypoadrenalism). Neurologic conditions (spinal cord injury, head trauma, stroke, tumor, Wernicke disease). Neuromuscular inefficiency (extremes of age, impaired shivering, lack of acclimatization). Sepsis. Pediatric patients are at higher risk because of increased surface area to mass ratio; consider nonaccidental trauma.
Diagnosis
Signs And Symptoms
Mild (35–32.2°C): Hypertension, shivering, tachycardia progressing to bradycardia, tachypnea, vasoconstriction, apathy, ataxia, cold diuresis, impaired judgment.
Moderate (32.2–28°C): Atrial dysrhythmias, bradycardia refractory to atropine, decreased level of consciousness, hypoventilation with CO₂ retention, dilated pupils, diminished gag reflex, cessation of shivering, hyporeflexia, hypotension, J (Osborn) waves.
Severe (<28°c): apnea, coma, minimal eeg activity, nonreactive pupils, oliguria, pulmonary edema, ventricular dysrhythmias or asystole.< />pan>
History Duration and circumstances of cold exposure or submersion.
Physical Exam Pulse and blood pressure may be difficult to detect; pupils often dilated at very low temperatures.
Essential Workup Accurate core temperature measurement.
Diagnosis Tests And Interpretation
Lab Fingerstick glucose, ABG (no temperature correction), CBC (hemoconcentration), electrolytes, BUN/creatinine, potassium, CPK, lactate, coagulation studies, toxicology screen.
Imaging CXR for pneumonia.
ECG Bradyarrhythmias, atrial fibrillation, ventricular fibrillation, prolonged PR/QRS/QT, Osborn waves.
Differential Diagnosis Environmental exposure, sepsis, CNS pathology, metabolic disorders, drug toxicity.
Treatment
Prehospital Patient is not dead until “warm and dead.” Prolonged pulse checks (30–45 s). CPR during transport if indicated.
Initial Stabilization/Therapy ABCs, supplemental oxygen, safe intubation if needed, cardiac monitoring, warmed IV fluids (D5NS preferred), remove wet clothing, passive rewarming, naloxone, dextrose, and thiamine for altered mental status, stress-dose steroids if adrenal insufficiency suspected.
Emergency Department Treatment/Procedures Handle gently to avoid precipitating ventricular fibrillation. Most dysrhythmias resolve with rewarming alone. Defibrillate up to 1–3 times below 28–30°C, then defer until rewarmed. Active rewarming is required for core temperature <32°c. use passive external rewarming for mild cases, active (forced warm air, trunk first) moderate and core (humidified oxygen, warmed iv fluids, peritoneal or pleural lavage, extracorporeal including hemodialysis cardiopulmonary bypass) severe hypothermia cardiac arrest. faster rates (1–2°c />r) are associated with better outcomes.
Medication Amiodarone for persistent ventricular dysrhythmias after rewarming, dextrose for hypoglycemia, hydrocortisone or methylprednisolone if adrenal insufficiency suspected, levothyroxine only for myxedema coma, naloxone, thiamine.
Follow-Up And Disposition
Admission Criteria Moderate to severe hypothermia (<32°c).< />pan>
Discharge Criteria Young, healthy patients with very mild hypothermia who normalize and have a safe, warm environment.
Follow-Up Recommendations Social services involvement for patients at risk of recurrent cold exposure.
Key Points And Cautions Defibrillation is rarely effective below 28–30°C. Atrial fibrillation often resolves with rewarming alone. Beware afterdrop and rewarming shock. Gentle handling and adequate volume resuscitation are essential.

- Published on
Emergency And Acute Medicine: Hyponatremia
Basics
Description Hyponatremia is defined as serum sodium <136 meq /> and is the most common electrolyte disturbance, occurring in 1–4% of hospitalized patients.
Etiology
Pseudohyponatremia Low measured sodium with normal serum osmolality due to displacement of sodium in the aqueous phase; seen with hyperlipidemia or hyperproteinemia (e.g., multiple myeloma).
Hyponatremia With Normal Osmolarity And Fluid Overload Inappropriate water retention seen in CHF, cirrhosis, renal failure, and nephrotic syndrome.
Hyponatremia With Normal Osmolarity And Euvolemia Dilutional hyponatremia with increased total body water and minimal edema. Causes include hypothyroidism, stress, SIADH (pulmonary disease, CNS disorders, malignancy, HIV), water intoxication, postoperative states, beer potomania, MDMA use, and mineralocorticoid abnormalities.
Hyponatremia With Normal Osmolarity And Hypovolemia Total body sodium and water loss with sodium loss predominating; causes include GI losses, sweating, burns, cerebral salt wasting, cystic fibrosis, salt-wasting nephropathies, and diuretics.
Drug Induced ADH stimulation (amiodarone, carbamazepine, cyclophosphamide, opiates, vincristine), increased ADH sensitivity (chlorpropamide, NSAIDs), or increased thirst (SSRIs, antipsychotics, MDMA).
Hyponatremia With Hyperosmolarity Due to osmotically active substances, most commonly hyperglycemia. Corrected Na = measured Na + 0.016 × (glucose − 100). Also seen with mannitol, maltose, or glycine.
Pediatric Considerations Higher risk of water intoxication and iatrogenic hyponatremia.
Pregnancy Considerations Vasopressin antagonists are pregnancy class C.
Geriatric Considerations Increased symptom burden due to impaired free water excretion and low sodium intake.
Diagnosis
Signs And Symptoms Mild (Na >120): headache, nausea, vomiting, weakness, anorexia, cramps. Moderate (110–120): confusion, hallucinations, bizarre behavior, incontinence, gait disturbance. Severe (<110): seizures, coma, herniation signs, respiratory arrest. chronic hyponatremia may be asymptomatic.< />pan>
History And Exam Review medications and assess volume status. Perform full neurologic examination.
Essential Workup Confirm serum sodium level with repeat testing.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose (correct sodium if hyperglycemic), serum and urine osmolality, urine sodium, thyroid and adrenal function, CPK if rhabdomyolysis suspected. Plasma osmolality = 2 × Na + glucose/18 + BUN/2.8.
Imaging CXR for CHF, infection, or malignancy. CT head if altered mental status.
Differential Diagnosis Pseudohyponatremia from hyperglycemia, hyperlipidemia, hyperproteinemia, or radiocontrast exposure.
Treatment
Prehospital Supportive care and IV access.
Initial Stabilization/Therapy ABCs, IV 0.9% NS, naloxone, thiamine, and D50W for altered mental status.
Emergency Department Treatment/Procedures Management depends on severity, chronicity, and cause. Chronic hyponatremia requires slow correction to prevent osmotic demyelination; limit correction to 10-12 mEq/L in 24 hr. Acute severe hyponatremia with seizures requires hypertonic saline to raise sodium 8-10 mEq/L over 4-6 hr or to >120–125 mEq/L, then slow or stop correction. Typical dose is 200–400 mL of 3% saline over 2 hr or 1–2 mL/kg/hr.
Hypovolemic Hyponatremia Restore volume with 0.9% NS.
Euvolemic Or Hypervolemic Hyponatremia Water restriction (<1 l />ay), high salt intake, or 0.9% NS with loop diuretics. Maximum correction rate 0.5 mEq/L/hr.
Medication
First Line 500 mL–1 L isotonic saline bolus.
Adjuncts Furosemide 20–40 mg IV.
Second Line Conivaptan IV or tolvaptan PO for euvolemic or hypervolemic hyponatremia only.
Follow-Up And Disposition
Admission Criteria Symptomatic hyponatremia, sodium <120 meq />, or comorbid risk factors.
Discharge Criteria Sodium >130 mEq/L and asymptomatic, or stable chronic mild hyponatremia with close follow-up.
Follow-Up Recommendations Repeat sodium within one week, especially if diuretic-related.
Pearls And Pitfalls Avoid rapid correction to prevent osmotic demyelination syndrome, especially in women, alcoholics, malnourished patients, those with hypokalemia, or liver transplant history. Perform serial neurologic exams. Beware of falsely low sodium from blood draws near hypotonic IV lines. Thiazide-induced hyponatremia may persist up to two weeks after discontinuation.
Basics
Description Hyponatremia is defined as serum sodium <136 meq /> and is the most common electrolyte disturbance, occurring in 1–4% of hospitalized patients.
Etiology
Pseudohyponatremia Low measured sodium with normal serum osmolality due to displacement of sodium in the aqueous phase; seen with hyperlipidemia or hyperproteinemia (e.g., multiple myeloma).
Hyponatremia With Normal Osmolarity And Fluid Overload Inappropriate water retention seen in CHF, cirrhosis, renal failure, and nephrotic syndrome.
Hyponatremia With Normal Osmolarity And Euvolemia Dilutional hyponatremia with increased total body water and minimal edema. Causes include hypothyroidism, stress, SIADH (pulmonary disease, CNS disorders, malignancy, HIV), water intoxication, postoperative states, beer potomania, MDMA use, and mineralocorticoid abnormalities.
Hyponatremia With Normal Osmolarity And Hypovolemia Total body sodium and water loss with sodium loss predominating; causes include GI losses, sweating, burns, cerebral salt wasting, cystic fibrosis, salt-wasting nephropathies, and diuretics.
Drug Induced ADH stimulation (amiodarone, carbamazepine, cyclophosphamide, opiates, vincristine), increased ADH sensitivity (chlorpropamide, NSAIDs), or increased thirst (SSRIs, antipsychotics, MDMA).
Hyponatremia With Hyperosmolarity Due to osmotically active substances, most commonly hyperglycemia. Corrected Na = measured Na + 0.016 × (glucose − 100). Also seen with mannitol, maltose, or glycine.
Pediatric Considerations Higher risk of water intoxication and iatrogenic hyponatremia.
Pregnancy Considerations Vasopressin antagonists are pregnancy class C.
Geriatric Considerations Increased symptom burden due to impaired free water excretion and low sodium intake.
Diagnosis
Signs And Symptoms Mild (Na >120): headache, nausea, vomiting, weakness, anorexia, cramps. Moderate (110–120): confusion, hallucinations, bizarre behavior, incontinence, gait disturbance. Severe (<110): seizures, coma, herniation signs, respiratory arrest. chronic hyponatremia may be asymptomatic.< />pan>
History And Exam Review medications and assess volume status. Perform full neurologic examination.
Essential Workup Confirm serum sodium level with repeat testing.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose (correct sodium if hyperglycemic), serum and urine osmolality, urine sodium, thyroid and adrenal function, CPK if rhabdomyolysis suspected. Plasma osmolality = 2 × Na + glucose/18 + BUN/2.8.
Imaging CXR for CHF, infection, or malignancy. CT head if altered mental status.
Differential Diagnosis Pseudohyponatremia from hyperglycemia, hyperlipidemia, hyperproteinemia, or radiocontrast exposure.
Treatment
Prehospital Supportive care and IV access.
Initial Stabilization/Therapy ABCs, IV 0.9% NS, naloxone, thiamine, and D50W for altered mental status.
Emergency Department Treatment/Procedures Management depends on severity, chronicity, and cause. Chronic hyponatremia requires slow correction to prevent osmotic demyelination; limit correction to 10-12 mEq/L in 24 hr. Acute severe hyponatremia with seizures requires hypertonic saline to raise sodium 8-10 mEq/L over 4-6 hr or to >120–125 mEq/L, then slow or stop correction. Typical dose is 200–400 mL of 3% saline over 2 hr or 1–2 mL/kg/hr.
Hypovolemic Hyponatremia Restore volume with 0.9% NS.
Euvolemic Or Hypervolemic Hyponatremia Water restriction (<1 l />ay), high salt intake, or 0.9% NS with loop diuretics. Maximum correction rate 0.5 mEq/L/hr.
Medication
First Line 500 mL–1 L isotonic saline bolus.
Adjuncts Furosemide 20–40 mg IV.
Second Line Conivaptan IV or tolvaptan PO for euvolemic or hypervolemic hyponatremia only.
Follow-Up And Disposition
Admission Criteria Symptomatic hyponatremia, sodium <120 meq />, or comorbid risk factors.
Discharge Criteria Sodium >130 mEq/L and asymptomatic, or stable chronic mild hyponatremia with close follow-up.
Follow-Up Recommendations Repeat sodium within one week, especially if diuretic-related.
Pearls And Pitfalls Avoid rapid correction to prevent osmotic demyelination syndrome, especially in women, alcoholics, malnourished patients, those with hypokalemia, or liver transplant history. Perform serial neurologic exams. Beware of falsely low sodium from blood draws near hypotonic IV lines. Thiazide-induced hyponatremia may persist up to two weeks after discontinuation.

- Published on
Emergency And Acute Medicine: Hypocalcemia
Basics
Description Hypocalcemia is defined as a total plasma calcium level <8.7 mg/dL. Ionized calcium may be normal and therefore asymptomatic. Normal total serum calcium is 8.7–10.5 mg/dL.
Etiology Incidence is ~0.6% in the general population. Mechanisms include increased calcium loss from or decreased entry into the circulation. Circulating calcium exists as protein bound (45–50%, mainly albumin), complexed to anions (5–10%), and ionized free calcium (45–50%, physiologically active). Calcium homeostasis is regulated by parathyroid hormone, vitamin D (1,25-dihydroxyvitamin D), and calcitonin. Hypoalbuminemia is the most common cause; for each 1 g/dL decrease in albumin, total calcium decreases by ~0.8 mg/dL while ionized calcium remains unchanged.
Pediatric considerations Children have higher normal calcium levels (9.2–11 mg/dL). Neonatal hypocalcemia is defined as total calcium <7.5 mg/dL or ionized calcium <4 mg/dL and may present with jitteriness, tachypnea, apnea with cyanosis, and vomiting.
Diagnosis
Signs And Symptoms Occur when ionized calcium <3.2 mg/dL and depend on severity and rate of decline. Neuromuscular findings include paresthesias, hyperreflexia, muscle spasms, tetany, Chvostek sign, Trousseau sign, laryngeal stridor, seizures, and choreoathetosis. Cardiovascular effects include torsades de pointes, heart block, hypotension, impaired contractility, bradycardia, QT and ST prolongation, and T-wave abnormalities. Psychiatric manifestations include anxiety, irritability, depression, psychosis, confusion, and movement disorders. Ocular findings include papilledema and cataracts in acute cases.
Essential Workup Confirm diagnosis with serum ionized calcium level.
Diagnosis Tests And Interpretation
Lab ABG (pH changes affect ionized calcium), serum albumin, electrolytes, BUN/creatinine, glucose, magnesium, phosphate, PTH, and vitamin D metabolites as indicated.
ECG Prolonged QT interval and possible heart block.
Differential Diagnosis Impaired PTH secretion or action (post-surgical hypoparathyroidism, autoimmune or congenital hypoparathyroidism, pseudohypoparathyroidism), impaired vitamin D synthesis or action (malabsorption, renal disease), calcium sequestration or complexing (hyperphosphatemia, transfusion citrate, pancreatitis, rhabdomyolysis, alkalosis), hypomagnesemia, medications (bisphosphonates, calcitonin, phenytoin, cisplatin, PPIs), malignancy, sepsis, burns, and hungry bone syndrome after parathyroidectomy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, and cardiac monitoring.
Emergency Department Treatment/Procedures Treat symptomatic hypocalcemia as an emergency. Give IV calcium gluconate 1–2 g in 50 mL D5W over 20 min. Faster infusion may cause dysrhythmias. Follow bolus with continuous infusion (0.5–1.5 mg/kg/hr elemental calcium). Do not mix calcium with bicarbonate or phosphate. Monitor calcium every 1–4 hr and titrate to symptoms or ECG changes. Correct hypomagnesemia if present (Mg 2 g IV). Use caution in patients on digoxin.
Chronic management Oral calcium 1.5–2 g/day (up to 4 g/day if malabsorption) plus vitamin D supplementation. Calcitriol is preferred for rapid onset.
Medications
IV calcium Calcium gluconate, calcium chloride, or calcium gluceptate (dose by elemental calcium).
Oral calcium Calcium carbonate, citrate, gluconate, lactate, or glubionate.
Vitamin D Calcitriol, ergocalciferol, or related preparations as indicated.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ionized calcium <3.2 mg/dL, or need for continuous IV calcium.
Discharge Criteria Asymptomatic patients with ionized calcium >3.2 mg/dL and no significant comorbidities.
Follow-Up Recommendations Endocrinology follow-up for disorders of PTH or vitamin D metabolism.
Pearls And Pitfalls Hypocalcemia has multiple causes; treatment depends on severity and etiology. Severe symptoms require IV calcium. Hypocalcemia will not correct if magnesium deficiency is not treated first.
Basics
Description Hypocalcemia is defined as a total plasma calcium level <8.7 mg/dL. Ionized calcium may be normal and therefore asymptomatic. Normal total serum calcium is 8.7–10.5 mg/dL.
Etiology Incidence is ~0.6% in the general population. Mechanisms include increased calcium loss from or decreased entry into the circulation. Circulating calcium exists as protein bound (45–50%, mainly albumin), complexed to anions (5–10%), and ionized free calcium (45–50%, physiologically active). Calcium homeostasis is regulated by parathyroid hormone, vitamin D (1,25-dihydroxyvitamin D), and calcitonin. Hypoalbuminemia is the most common cause; for each 1 g/dL decrease in albumin, total calcium decreases by ~0.8 mg/dL while ionized calcium remains unchanged.
Pediatric considerations Children have higher normal calcium levels (9.2–11 mg/dL). Neonatal hypocalcemia is defined as total calcium <7.5 mg/dL or ionized calcium <4 mg/dL and may present with jitteriness, tachypnea, apnea with cyanosis, and vomiting.
Diagnosis
Signs And Symptoms Occur when ionized calcium <3.2 mg/dL and depend on severity and rate of decline. Neuromuscular findings include paresthesias, hyperreflexia, muscle spasms, tetany, Chvostek sign, Trousseau sign, laryngeal stridor, seizures, and choreoathetosis. Cardiovascular effects include torsades de pointes, heart block, hypotension, impaired contractility, bradycardia, QT and ST prolongation, and T-wave abnormalities. Psychiatric manifestations include anxiety, irritability, depression, psychosis, confusion, and movement disorders. Ocular findings include papilledema and cataracts in acute cases.
Essential Workup Confirm diagnosis with serum ionized calcium level.
Diagnosis Tests And Interpretation
Lab ABG (pH changes affect ionized calcium), serum albumin, electrolytes, BUN/creatinine, glucose, magnesium, phosphate, PTH, and vitamin D metabolites as indicated.
ECG Prolonged QT interval and possible heart block.
Differential Diagnosis Impaired PTH secretion or action (post-surgical hypoparathyroidism, autoimmune or congenital hypoparathyroidism, pseudohypoparathyroidism), impaired vitamin D synthesis or action (malabsorption, renal disease), calcium sequestration or complexing (hyperphosphatemia, transfusion citrate, pancreatitis, rhabdomyolysis, alkalosis), hypomagnesemia, medications (bisphosphonates, calcitonin, phenytoin, cisplatin, PPIs), malignancy, sepsis, burns, and hungry bone syndrome after parathyroidectomy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, and cardiac monitoring.
Emergency Department Treatment/Procedures Treat symptomatic hypocalcemia as an emergency. Give IV calcium gluconate 1–2 g in 50 mL D5W over 20 min. Faster infusion may cause dysrhythmias. Follow bolus with continuous infusion (0.5–1.5 mg/kg/hr elemental calcium). Do not mix calcium with bicarbonate or phosphate. Monitor calcium every 1–4 hr and titrate to symptoms or ECG changes. Correct hypomagnesemia if present (Mg 2 g IV). Use caution in patients on digoxin.
Chronic management Oral calcium 1.5–2 g/day (up to 4 g/day if malabsorption) plus vitamin D supplementation. Calcitriol is preferred for rapid onset.
Medications
IV calcium Calcium gluconate, calcium chloride, or calcium gluceptate (dose by elemental calcium).
Oral calcium Calcium carbonate, citrate, gluconate, lactate, or glubionate.
Vitamin D Calcitriol, ergocalciferol, or related preparations as indicated.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ionized calcium <3.2 mg/dL, or need for continuous IV calcium.
Discharge Criteria Asymptomatic patients with ionized calcium >3.2 mg/dL and no significant comorbidities.
Follow-Up Recommendations Endocrinology follow-up for disorders of PTH or vitamin D metabolism.
Pearls And Pitfalls Hypocalcemia has multiple causes; treatment depends on severity and etiology. Severe symptoms require IV calcium. Hypocalcemia will not correct if magnesium deficiency is not treated first.

- Published on
Emergency And Acute Medicine: Hypoglycemic Agent Poisoning
Basics
Description Hypoglycemic agent poisoning results from oral or parenteral agents that cause hypoglycemia or metabolic derangements. Poisoning may be intentional or accidental.
Etiology
Insulin Enhances cellular glucose uptake, limits cerebral glucose availability, and shifts potassium intracellularly causing hypokalemia.
Sulfonylureas And Meglitinides Increase pancreatic insulin release, reduce hepatic glucose production, and increase peripheral insulin sensitivity. Effects are potentiated by polypharmacy, alcohol use, hepatic dysfunction, and renal insufficiency.
GLP-1 Modulators Exenatide and DPP-4 inhibitors (e.g., sitagliptin, saxagliptin) enhance insulin secretion and delay gastric emptying. Effects in overdose are unclear.
Biguanides (Metformin) Rarely cause hypoglycemia alone but, with insulin, increase cellular glucose uptake, inhibit gluconeogenesis, reduce GI glucose absorption, and promote lactate accumulation leading to lactic acidosis.
Thiazolidinediones Increase insulin sensitivity and glucose uptake in the presence of insulin.
α-Glucosidase Inhibitors Reduce carbohydrate absorption and systemic glucose.
Diagnosis
Signs And Symptoms
Insulin Or Sulfonylureas Hypoglycemia often when glucose <40–60 mg />L. Symptoms include diaphoresis, pallor, tremor, hunger, nausea, headache, blurred vision, paresthesias, weakness, anxiety, confusion, seizures, coma, tachycardia or late bradycardia, hypertension, and hypothermia. β-blockers may blunt adrenergic signs.
Biguanides Lactic acidosis with nausea, vomiting, abdominal pain, agitation, lethargy, coma, Kussmaul respirations, hypotension, and tachycardia.
Pediatric Considerations Neonatal hypoglycemia may occur after maternal sulfonylurea use. Ingestion of a single sulfonylurea tablet can cause severe hypoglycemia or death. Onset may be delayed up to 8 hr.
History
Diabetes diagnosis, access to medications, dosing errors, renal or hepatic disease, alcohol use, and possible malicious or intentional ingestion.
Physical Exam Tachycardia (may be blunted), altered mental status, ataxia, seizures, or coma.
Essential Workup
Frequent glucose monitoring, vital signs, and neurologic assessment. Check electrolytes and lactate for biguanides and liver function tests for thiazolidinediones.
Diagnosis Tests And Interpretation
Lab Serum glucose pre- and post-treatment, electrolytes (hypokalemia, anion gap acidosis), BUN/creatinine, CBC, ethanol level, lactate, LFTs, ABG. Insulin and C-peptide levels may confirm exogenous insulin use.
Imaging/Other ECG for dysrhythmias, EEG for persistent coma, CT head for prolonged hypoglycemia, CXR for aspiration or pulmonary edema.
Differential Diagnosis Adrenal insufficiency, panhypopituitarism, sepsis, insulinoma, neuroendocrine tumors, cirrhosis, ethanol or salicylate ingestion, β-blocker overdose, Ackee fruit poisoning.
Treatment
Prehospital Transport medications and pill bottles with patient.
Initial Stabilization/Therapy ABCs, oxygen, IV access, cardiac monitoring, pulse oximetry. Give naloxone, thiamine, and dextrose if altered mental status.
Emergency Department Treatment/Procedures Treat hypoglycemia with IV dextrose bolus followed by D5W or D10W infusion. Allow oral intake when mental status improves. Persistent neuroglycopenia requires repeat dextrose. Consider activated charcoal for recent oral ingestions. Treat hypotension with IV fluids and cautious vasopressors. Give bicarbonate for severe metformin-associated acidosis (pH <7). use benzodiazepines for seizures. sulfonylurea-induced recurrent hypoglycemia, inhibit insulin secretion with octreotide or diazoxide. consider early hemodialysis severe biguanide-associated lactic acidosis.< />pan>
Medications
Activated charcoal 1 g/kg PO. Dextrose 50–100 mL D50 IV (peds: D25 2 mL/kg). Octreotide 50–100 μg SC/IV q8–12h. Diazoxide 200 mg PO or 1–3 mg/kg IV. Glucagon 1–2 mg IM/SC/IV. Benzodiazepines for seizures. Thiamine 100 mg IV/IM.
Follow-Up And Disposition
Admission Criteria
Sulfonylurea or long-acting insulin exposure, recurrent or refractory hypoglycemia, need for continuous dextrose infusion, intentional overdose, all pediatric sulfonylurea ingestions, or metabolic complications from biguanides.
Discharge Criteria
Short-acting insulin error with dietary insufficiency, normal mental status, stable glucose after ≥4 hr observation, and tolerating oral intake.
Issues For Referral Poison prevention counseling for accidental exposure; psychiatric evaluation for intentional poisoning.
Follow-Up Recommendations
Close outpatient follow-up for glucose monitoring and medication adjustment.
Pearls And Pitfalls Sulfonylureas have prolonged effects with delayed or recurrent hypoglycemia—observe carefully. Metformin must be withheld 48 hr after IV contrast due to lactic acidosis risk. Persistent hypoglycemia requires octreotide, not repeated dextrose alone.
Basics
Description Hypoglycemic agent poisoning results from oral or parenteral agents that cause hypoglycemia or metabolic derangements. Poisoning may be intentional or accidental.
Etiology
Insulin Enhances cellular glucose uptake, limits cerebral glucose availability, and shifts potassium intracellularly causing hypokalemia.
Sulfonylureas And Meglitinides Increase pancreatic insulin release, reduce hepatic glucose production, and increase peripheral insulin sensitivity. Effects are potentiated by polypharmacy, alcohol use, hepatic dysfunction, and renal insufficiency.
GLP-1 Modulators Exenatide and DPP-4 inhibitors (e.g., sitagliptin, saxagliptin) enhance insulin secretion and delay gastric emptying. Effects in overdose are unclear.
Biguanides (Metformin) Rarely cause hypoglycemia alone but, with insulin, increase cellular glucose uptake, inhibit gluconeogenesis, reduce GI glucose absorption, and promote lactate accumulation leading to lactic acidosis.
Thiazolidinediones Increase insulin sensitivity and glucose uptake in the presence of insulin.
α-Glucosidase Inhibitors Reduce carbohydrate absorption and systemic glucose.
Diagnosis
Signs And Symptoms
Insulin Or Sulfonylureas Hypoglycemia often when glucose <40–60 mg />L. Symptoms include diaphoresis, pallor, tremor, hunger, nausea, headache, blurred vision, paresthesias, weakness, anxiety, confusion, seizures, coma, tachycardia or late bradycardia, hypertension, and hypothermia. β-blockers may blunt adrenergic signs.
Biguanides Lactic acidosis with nausea, vomiting, abdominal pain, agitation, lethargy, coma, Kussmaul respirations, hypotension, and tachycardia.
Pediatric Considerations Neonatal hypoglycemia may occur after maternal sulfonylurea use. Ingestion of a single sulfonylurea tablet can cause severe hypoglycemia or death. Onset may be delayed up to 8 hr.
History
Diabetes diagnosis, access to medications, dosing errors, renal or hepatic disease, alcohol use, and possible malicious or intentional ingestion.
Physical Exam Tachycardia (may be blunted), altered mental status, ataxia, seizures, or coma.
Essential Workup
Frequent glucose monitoring, vital signs, and neurologic assessment. Check electrolytes and lactate for biguanides and liver function tests for thiazolidinediones.
Diagnosis Tests And Interpretation
Lab Serum glucose pre- and post-treatment, electrolytes (hypokalemia, anion gap acidosis), BUN/creatinine, CBC, ethanol level, lactate, LFTs, ABG. Insulin and C-peptide levels may confirm exogenous insulin use.
Imaging/Other ECG for dysrhythmias, EEG for persistent coma, CT head for prolonged hypoglycemia, CXR for aspiration or pulmonary edema.
Differential Diagnosis Adrenal insufficiency, panhypopituitarism, sepsis, insulinoma, neuroendocrine tumors, cirrhosis, ethanol or salicylate ingestion, β-blocker overdose, Ackee fruit poisoning.
Treatment
Prehospital Transport medications and pill bottles with patient.
Initial Stabilization/Therapy ABCs, oxygen, IV access, cardiac monitoring, pulse oximetry. Give naloxone, thiamine, and dextrose if altered mental status.
Emergency Department Treatment/Procedures Treat hypoglycemia with IV dextrose bolus followed by D5W or D10W infusion. Allow oral intake when mental status improves. Persistent neuroglycopenia requires repeat dextrose. Consider activated charcoal for recent oral ingestions. Treat hypotension with IV fluids and cautious vasopressors. Give bicarbonate for severe metformin-associated acidosis (pH <7). use benzodiazepines for seizures. sulfonylurea-induced recurrent hypoglycemia, inhibit insulin secretion with octreotide or diazoxide. consider early hemodialysis severe biguanide-associated lactic acidosis.< />pan>
Medications
Activated charcoal 1 g/kg PO. Dextrose 50–100 mL D50 IV (peds: D25 2 mL/kg). Octreotide 50–100 μg SC/IV q8–12h. Diazoxide 200 mg PO or 1–3 mg/kg IV. Glucagon 1–2 mg IM/SC/IV. Benzodiazepines for seizures. Thiamine 100 mg IV/IM.
Follow-Up And Disposition
Admission Criteria
Sulfonylurea or long-acting insulin exposure, recurrent or refractory hypoglycemia, need for continuous dextrose infusion, intentional overdose, all pediatric sulfonylurea ingestions, or metabolic complications from biguanides.
Discharge Criteria
Short-acting insulin error with dietary insufficiency, normal mental status, stable glucose after ≥4 hr observation, and tolerating oral intake.
Issues For Referral Poison prevention counseling for accidental exposure; psychiatric evaluation for intentional poisoning.
Follow-Up Recommendations
Close outpatient follow-up for glucose monitoring and medication adjustment.
Pearls And Pitfalls Sulfonylureas have prolonged effects with delayed or recurrent hypoglycemia—observe carefully. Metformin must be withheld 48 hr after IV contrast due to lactic acidosis risk. Persistent hypoglycemia requires octreotide, not repeated dextrose alone.
- Published on
Emergency And Acute Medicine: Hypoparathyroidism
Basics
Description Hypoparathyroidism results from deficiency of parathyroid hormone (PTH), whereas pseudohypoparathyroidism is due to end-organ resistance to PTH. PTH reduces urinary calcium loss, increases urinary phosphate loss, stimulates renal conversion of vitamin D to its active form, and mobilizes calcium and phosphate from bone. Hypocalcemia is the primary metabolic abnormality. Calcitonin promotes deposition of calcium and phosphate into bone. Magnesium is required for both PTH production and peripheral PTH action. Primary hypoparathyroidism reflects intrinsic gland failure, while pseudohypoparathyroidism features elevated PTH with tissue resistance and is often associated with hypothyroidism and hypogonadism. Genetic associations include congenital absence (DiGeorge syndrome), autoimmune polyglandular syndrome type I, Wilson disease, and Albright hereditary osteodystrophy.
Etiology
Failure of parathyroid function due to autoimmune destruction, surgical removal or vascular disruption, radiation injury, or severe hypomagnesemia. Pseudohypoparathyroidism is caused by end-organ resistance to PTH.
Diagnosis
Signs And Symptoms The most common symptomatic presentation occurs postoperatively after parathyroid or thyroid surgery. Neonates may have transient disease with neurodevelopmental consequences proportional to hypocalcemia duration. Symptoms relate to hypocalcemia severity and acuity. Neuromuscular findings include circumoral and distal paresthesias, carpopedal spasm, tetany, positive Chvostek and Trousseau signs, laryngospasm, bronchospasm, muscle cramps, and seizures. Cardiovascular manifestations include prolonged QT interval, heart block, heart failure, ventricular arrhythmias, and vasoconstriction. Neuropsychiatric features include confusion, hallucinations, memory impairment, dementia, extrapyramidal symptoms, and raised intracranial pressure with papilledema. Dermatologic findings include brittle hair and nails, psoriasis, hyperpigmentation, and lenticular cataracts.
Essential Workup
In asymptomatic hypocalcemia, check albumin and correct total calcium. If symptomatic with normal total calcium, evaluate for alkalosis and obtain ionized calcium. Symptomatic low ionized calcium warrants PTH measurement.
Diagnosis Tests And Interpretation
Lab Corrected calcium = measured calcium + 0.8(4 − albumin). Obtain ionized calcium if symptomatic. Check electrolytes, BUN, creatinine, glucose, magnesium, phosphorus, and ABG if alkalosis suspected. Ionized calcium decreases by 3–8% for every 0.1 pH unit increase. Phosphate is typically elevated except in vitamin D deficiency.
Diagnostic Procedures ECG shows QT prolongation due to ST-segment lengthening.
Differential Diagnosis
Pseudohypocalcemia from hypoalbuminemia, alkalosis-related reduction in ionized calcium, hypomagnesemia, congenital PTH resistance, vitamin D deficiency, renal failure, sepsis, pancreatitis, rhabdomyolysis, acute hyperphosphatemia, and chelation from citrate or toxins.
Treatment
Prehospital Consider calcium administration for refractory ventricular fibrillation or status epilepticus in known or suspected hypocalcemia.
Initial Stabilization/Therapy Secure airway if laryngospasm is present. Initiate cardiac monitoring and seizure precautions. Administer IV calcium for unstable rhythms or tetany.
Emergency Department Treatment/Procedures Life-threatening hypocalcemia requires IV calcium chloride or calcium gluconate. Non–life-threatening cases should receive slow calcium infusion with frequent monitoring. Avoid rapid correction unless unstable. Replace magnesium if deficient. Maintain calcium at the lowest asymptomatic level, then transition to oral therapy. Bind phosphate when elevated and supplement vitamin D, preferably with calcitriol. Avoid high-phosphate beverages and evaluate for associated endocrinopathies.
Medication
First Line Calcium gluconate IV for most cases; calcium chloride reserved for life-threatening instability. Magnesium sulfate IV if deficient.
Second Line Oral calcium salts (carbonate or acetate), phosphate binders (sevelamer), magnesium oxide, vitamin D or calcitriol, and thiazide diuretics to reduce urinary calcium loss.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ECG abnormalities, inability to tolerate oral therapy, or markedly low corrected calcium.
Discharge Criteria Asymptomatic patients without admission criteria.
Follow-Up Recommendations Repeat calcium, phosphorus, and magnesium levels within 1–2 days for patients requiring treatment.
Key Points And Cautions
Postoperative hypocalcemia is the most common symptomatic presentation. Symptoms are often mistaken for anxiety or hyperventilation. Exclude sepsis or rhabdomyolysis in nonoperative cases. Except in life-threatening situations, avoid rapid IV calcium administration to prevent complications.
Basics
Description Hypoparathyroidism results from deficiency of parathyroid hormone (PTH), whereas pseudohypoparathyroidism is due to end-organ resistance to PTH. PTH reduces urinary calcium loss, increases urinary phosphate loss, stimulates renal conversion of vitamin D to its active form, and mobilizes calcium and phosphate from bone. Hypocalcemia is the primary metabolic abnormality. Calcitonin promotes deposition of calcium and phosphate into bone. Magnesium is required for both PTH production and peripheral PTH action. Primary hypoparathyroidism reflects intrinsic gland failure, while pseudohypoparathyroidism features elevated PTH with tissue resistance and is often associated with hypothyroidism and hypogonadism. Genetic associations include congenital absence (DiGeorge syndrome), autoimmune polyglandular syndrome type I, Wilson disease, and Albright hereditary osteodystrophy.
Etiology
Failure of parathyroid function due to autoimmune destruction, surgical removal or vascular disruption, radiation injury, or severe hypomagnesemia. Pseudohypoparathyroidism is caused by end-organ resistance to PTH.
Diagnosis
Signs And Symptoms The most common symptomatic presentation occurs postoperatively after parathyroid or thyroid surgery. Neonates may have transient disease with neurodevelopmental consequences proportional to hypocalcemia duration. Symptoms relate to hypocalcemia severity and acuity. Neuromuscular findings include circumoral and distal paresthesias, carpopedal spasm, tetany, positive Chvostek and Trousseau signs, laryngospasm, bronchospasm, muscle cramps, and seizures. Cardiovascular manifestations include prolonged QT interval, heart block, heart failure, ventricular arrhythmias, and vasoconstriction. Neuropsychiatric features include confusion, hallucinations, memory impairment, dementia, extrapyramidal symptoms, and raised intracranial pressure with papilledema. Dermatologic findings include brittle hair and nails, psoriasis, hyperpigmentation, and lenticular cataracts.
Essential Workup
In asymptomatic hypocalcemia, check albumin and correct total calcium. If symptomatic with normal total calcium, evaluate for alkalosis and obtain ionized calcium. Symptomatic low ionized calcium warrants PTH measurement.
Diagnosis Tests And Interpretation
Lab Corrected calcium = measured calcium + 0.8(4 − albumin). Obtain ionized calcium if symptomatic. Check electrolytes, BUN, creatinine, glucose, magnesium, phosphorus, and ABG if alkalosis suspected. Ionized calcium decreases by 3–8% for every 0.1 pH unit increase. Phosphate is typically elevated except in vitamin D deficiency.
Diagnostic Procedures ECG shows QT prolongation due to ST-segment lengthening.
Differential Diagnosis
Pseudohypocalcemia from hypoalbuminemia, alkalosis-related reduction in ionized calcium, hypomagnesemia, congenital PTH resistance, vitamin D deficiency, renal failure, sepsis, pancreatitis, rhabdomyolysis, acute hyperphosphatemia, and chelation from citrate or toxins.
Treatment
Prehospital Consider calcium administration for refractory ventricular fibrillation or status epilepticus in known or suspected hypocalcemia.
Initial Stabilization/Therapy Secure airway if laryngospasm is present. Initiate cardiac monitoring and seizure precautions. Administer IV calcium for unstable rhythms or tetany.
Emergency Department Treatment/Procedures Life-threatening hypocalcemia requires IV calcium chloride or calcium gluconate. Non–life-threatening cases should receive slow calcium infusion with frequent monitoring. Avoid rapid correction unless unstable. Replace magnesium if deficient. Maintain calcium at the lowest asymptomatic level, then transition to oral therapy. Bind phosphate when elevated and supplement vitamin D, preferably with calcitriol. Avoid high-phosphate beverages and evaluate for associated endocrinopathies.
Medication
First Line Calcium gluconate IV for most cases; calcium chloride reserved for life-threatening instability. Magnesium sulfate IV if deficient.
Second Line Oral calcium salts (carbonate or acetate), phosphate binders (sevelamer), magnesium oxide, vitamin D or calcitriol, and thiazide diuretics to reduce urinary calcium loss.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ECG abnormalities, inability to tolerate oral therapy, or markedly low corrected calcium.
Discharge Criteria Asymptomatic patients without admission criteria.
Follow-Up Recommendations Repeat calcium, phosphorus, and magnesium levels within 1–2 days for patients requiring treatment.
Key Points And Cautions
Postoperative hypocalcemia is the most common symptomatic presentation. Symptoms are often mistaken for anxiety or hyperventilation. Exclude sepsis or rhabdomyolysis in nonoperative cases. Except in life-threatening situations, avoid rapid IV calcium administration to prevent complications.
- Published on
KembaraXtra-Emergency and Acute Medicine: Hydatidiform Mole
Basics
Description Hydatidiform mole is a noninvasive, localized tumor arising from trophoblastic tissue and may be associated with malignancy. Twinning with a normal pregnancy is possible but carries a higher risk of persistent maternal disease and metastasis, although a normal infant may occasionally result. Complete mole occurs in ~1/1,500 pregnancies, with no fetal tissue, diffuse chorionic villi swelling, and diffuse trophoblastic hyperplasia; malignancy develops in 15–20% (commonly lung). Genetics are typically 46,XX (90%) or 46,XY (10%) with paternal-only DNA due to fertilization of an enucleated ovum by two sperm or duplication of a haploid sperm. Partial mole occurs in ~1/750 pregnancies, often with fetal or embryonic tissue, focal villous swelling, and focal trophoblastic hyperplasia; malignancy risk is 4–12%. Genetics are usually triploid (69XXX, 69XXY, rarely 69XYY) with both maternal and paternal DNA.
Etiology Largely unknown. Risk factors include extremes of maternal age (>35 years with 5–10× risk; <20 years), prior molar pregnancy (1–2% recurrence), higher prevalence in Asian and Latin American regions, dietary deficiency of animal fat and vitamin A, smoking (>15 cigarettes/day), maternal blood types AB/A/B, infertility or nulliparity, and occurrence in ~1 of 600 therapeutic abortions.
Diagnosis
Signs and symptoms Usually exaggerated pregnancy symptoms. Complete mole commonly presents with painless vaginal bleeding (97%) described as “prune juice,” passage of grapelike vesicles, hyperemesis from high β-hCG, preeclampsia (27%), hyperthyroidism (7%), and acute respiratory distress (2%) from trophoblastic emboli or related cardiopulmonary effects. Partial mole often resembles threatened or spontaneous abortion with vaginal bleeding, possible fetal heart tones, and later presentation.
History Missed menses, positive pregnancy test, nausea, vomiting, vaginal bleeding.
Physical exam Uterine size–date discrepancy in 50–66% (larger in complete, smaller in partial). Ovarian enlargement with bilateral theca lutein cysts is common in complete moles.
Essential workup
Laboratory β-hCG (often >100,000 mIU/mL in complete moles; lower in partial; >40,000 mIU/mL indicates poorer prognosis), blood type/Rh and cross-match, CBC, coagulation profile, electrolytes with BUN/creatinine, LFTs, TSH/free T4 if hyperthyroidism suspected, urinalysis for proteinuria.
Imaging
Ultrasound shows a “snowstorm” pattern with absent fetus and no amniotic fluid in complete moles and a “Swiss-cheese” placental appearance with possible fetus in partial moles. Chest X-ray assesses pulmonary edema and metastatic disease.
Pathology
All products of conception require histology. Complete moles show edematous villi with diffuse trophoblastic hyperplasia; partial moles show fetal tissue, vessels, amnion, and edematous villi.
Differential diagnosis
Threatened, missed, or incomplete abortion; ectopic pregnancy; hyperthyroidism; hyperemesis gravidarum; hypertension and preeclampsia.
Treatment
Prehospital Secure airway, provide oxygen, establish IV access, treat seizures with benzodiazepines, and save passed tissue.
Initial stabilization IV access, cardiac monitoring, and blood preparation if evacuation is planned.
Emergency department management Intubate for respiratory distress; give β-blockers before evacuation for hyperthyroidism; manage preeclampsia/eclampsia with benzodiazepines and magnesium sulfate and control blood pressure with hydralazine or labetalol; transfuse blood products for coagulopathy; administer Rho(D) immune globulin; perform suction curettage (fertility-sparing and curative in ~80%) with oxytocin; consider chemoprophylaxis only in selected high-risk cases with reliable follow-up; consider hysterectomy for older patients, those not desiring fertility, or high-risk disease.
Follow-up and disposition
Admission criteria Uterine size >16 weeks, clinical preeclampsia/hyperthyroidism/respiratory distress, hemodynamic instability, partial mole, or hysterectomy.
Discharge criteria Uncomplicated curettage of a small, low-risk mole with reliable follow-up.
Follow-up recommendations Close OB-GYN follow-up with serial β-hCG weekly for ≥4 weeks then monthly until undetectable; any rise prompts evaluation for metastasis. Use contraception and avoid pregnancy for 12 months; perform early ultrasound in future pregnancies. Recurrence risk is 1–1.5% after one mole and up to 20% after two.
Pearls and pitfalls Diagnosis may be missed with apparent normal pregnancy, preeclampsia before 24 weeks, or severe hyperemesis. Strict β-hCG follow-up is essential; up to 20% may develop malignancy if not monitored.
Basics
Description Hydatidiform mole is a noninvasive, localized tumor arising from trophoblastic tissue and may be associated with malignancy. Twinning with a normal pregnancy is possible but carries a higher risk of persistent maternal disease and metastasis, although a normal infant may occasionally result. Complete mole occurs in ~1/1,500 pregnancies, with no fetal tissue, diffuse chorionic villi swelling, and diffuse trophoblastic hyperplasia; malignancy develops in 15–20% (commonly lung). Genetics are typically 46,XX (90%) or 46,XY (10%) with paternal-only DNA due to fertilization of an enucleated ovum by two sperm or duplication of a haploid sperm. Partial mole occurs in ~1/750 pregnancies, often with fetal or embryonic tissue, focal villous swelling, and focal trophoblastic hyperplasia; malignancy risk is 4–12%. Genetics are usually triploid (69XXX, 69XXY, rarely 69XYY) with both maternal and paternal DNA.
Etiology Largely unknown. Risk factors include extremes of maternal age (>35 years with 5–10× risk; <20 years), prior molar pregnancy (1–2% recurrence), higher prevalence in Asian and Latin American regions, dietary deficiency of animal fat and vitamin A, smoking (>15 cigarettes/day), maternal blood types AB/A/B, infertility or nulliparity, and occurrence in ~1 of 600 therapeutic abortions.
Diagnosis
Signs and symptoms Usually exaggerated pregnancy symptoms. Complete mole commonly presents with painless vaginal bleeding (97%) described as “prune juice,” passage of grapelike vesicles, hyperemesis from high β-hCG, preeclampsia (27%), hyperthyroidism (7%), and acute respiratory distress (2%) from trophoblastic emboli or related cardiopulmonary effects. Partial mole often resembles threatened or spontaneous abortion with vaginal bleeding, possible fetal heart tones, and later presentation.
History Missed menses, positive pregnancy test, nausea, vomiting, vaginal bleeding.
Physical exam Uterine size–date discrepancy in 50–66% (larger in complete, smaller in partial). Ovarian enlargement with bilateral theca lutein cysts is common in complete moles.
Essential workup
Laboratory β-hCG (often >100,000 mIU/mL in complete moles; lower in partial; >40,000 mIU/mL indicates poorer prognosis), blood type/Rh and cross-match, CBC, coagulation profile, electrolytes with BUN/creatinine, LFTs, TSH/free T4 if hyperthyroidism suspected, urinalysis for proteinuria.
Imaging
Ultrasound shows a “snowstorm” pattern with absent fetus and no amniotic fluid in complete moles and a “Swiss-cheese” placental appearance with possible fetus in partial moles. Chest X-ray assesses pulmonary edema and metastatic disease.
Pathology
All products of conception require histology. Complete moles show edematous villi with diffuse trophoblastic hyperplasia; partial moles show fetal tissue, vessels, amnion, and edematous villi.
Differential diagnosis
Threatened, missed, or incomplete abortion; ectopic pregnancy; hyperthyroidism; hyperemesis gravidarum; hypertension and preeclampsia.
Treatment
Prehospital Secure airway, provide oxygen, establish IV access, treat seizures with benzodiazepines, and save passed tissue.
Initial stabilization IV access, cardiac monitoring, and blood preparation if evacuation is planned.
Emergency department management Intubate for respiratory distress; give β-blockers before evacuation for hyperthyroidism; manage preeclampsia/eclampsia with benzodiazepines and magnesium sulfate and control blood pressure with hydralazine or labetalol; transfuse blood products for coagulopathy; administer Rho(D) immune globulin; perform suction curettage (fertility-sparing and curative in ~80%) with oxytocin; consider chemoprophylaxis only in selected high-risk cases with reliable follow-up; consider hysterectomy for older patients, those not desiring fertility, or high-risk disease.
Follow-up and disposition
Admission criteria Uterine size >16 weeks, clinical preeclampsia/hyperthyroidism/respiratory distress, hemodynamic instability, partial mole, or hysterectomy.
Discharge criteria Uncomplicated curettage of a small, low-risk mole with reliable follow-up.
Follow-up recommendations Close OB-GYN follow-up with serial β-hCG weekly for ≥4 weeks then monthly until undetectable; any rise prompts evaluation for metastasis. Use contraception and avoid pregnancy for 12 months; perform early ultrasound in future pregnancies. Recurrence risk is 1–1.5% after one mole and up to 20% after two.
Pearls and pitfalls Diagnosis may be missed with apparent normal pregnancy, preeclampsia before 24 weeks, or severe hyperemesis. Strict β-hCG follow-up is essential; up to 20% may develop malignancy if not monitored.
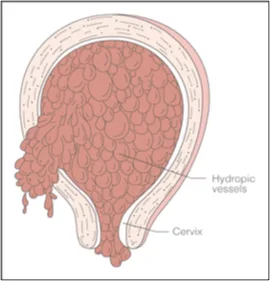
- Published on
Infectious Diseases and Microbiology: Dysuria and Fever
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.

