- Published on
Diagnostic Tests: C-Peptide
Overview — What This Test Is
The C-peptide test measures the serum level of C-peptide, a byproduct released when proinsulin is cleaved into insulin within pancreatic β-cells. Because C-peptide is secreted only with endogenous insulin and is absent in injected (exogenous) insulin, it is the best test for distinguishing endogenous from exogenous hyperinsulinemia in patients presenting with hypoglycemia.
Interpretation of Low C-Peptide Levels
Low C-peptide levels in the setting of hypoglycemia indicate exogenous insulin administration. In this situation, insulin levels are elevated, but C-peptide is suppressed because the insulin is being injected rather than produced by the pancreas. This finding is classic for factitious hypoglycemia, often due to insulin abuse, and may be seen in patients with psychiatric disease or repeated unexplained hospital visits.
Interpretation of High C-Peptide Levels
High C-peptide levels reflect endogenous insulin production. This occurs when the pancreas is actively secreting insulin, such as in:
In these cases, both insulin and C-peptide levels are elevated during episodes of hypoglycemia.
When to Choose a C-Peptide Level
You should answer C-peptide level when a patient presents with:
In exam questions, C-peptide is the next best diagnostic step to determine the cause of hyperinsulinemic hypoglycemia and to differentiate insulin abuse from endogenous insulin excess.
Overview — What This Test Is
The C-peptide test measures the serum level of C-peptide, a byproduct released when proinsulin is cleaved into insulin within pancreatic β-cells. Because C-peptide is secreted only with endogenous insulin and is absent in injected (exogenous) insulin, it is the best test for distinguishing endogenous from exogenous hyperinsulinemia in patients presenting with hypoglycemia.
Interpretation of Low C-Peptide Levels
Low C-peptide levels in the setting of hypoglycemia indicate exogenous insulin administration. In this situation, insulin levels are elevated, but C-peptide is suppressed because the insulin is being injected rather than produced by the pancreas. This finding is classic for factitious hypoglycemia, often due to insulin abuse, and may be seen in patients with psychiatric disease or repeated unexplained hospital visits.
Interpretation of High C-Peptide Levels
High C-peptide levels reflect endogenous insulin production. This occurs when the pancreas is actively secreting insulin, such as in:
- Insulinoma
- Sulfonylurea use, which stimulates pancreatic insulin release
In these cases, both insulin and C-peptide levels are elevated during episodes of hypoglycemia.
When to Choose a C-Peptide Level
You should answer C-peptide level when a patient presents with:
- Unexplained hypoglycemia
- Elevated insulin levels
- Recurrent or unexplained hospital admissions
- Suspicion of factitious disorder or insulin-secreting tumor
In exam questions, C-peptide is the next best diagnostic step to determine the cause of hyperinsulinemic hypoglycemia and to differentiate insulin abuse from endogenous insulin excess.
- Published on
Diagnostic Tests: Prenatal Screening
Routine Prenatal Screening Tests
Basic prenatal screening is recommended for all pregnancies to assess maternal health, identify infectious risks, and evaluate fetal development. These tests are part of standard obstetric care and are not dependent on maternal age or risk status. Routine prenatal screening includes cervical cytology, a complete blood count (CBC), and urinalysis to detect anemia, infection, or renal abnormalities. Maternal blood testing also includes blood group, Rh factor, and antibody screening to prevent hemolytic disease of the newborn, along with serologic testing for syphilis and assessment of rubella immunity.
Additional routine evaluations include glucose screening for gestational diabetes and fetal ultrasound for pregnancy dating, growth monitoring, and anatomic assessment. Cervical cultures are obtained to screen for Neisseria gonorrhoeae, Chlamydia trachomatis, and Group B Streptococcus, which are important causes of maternal and neonatal infection.
High-Risk Pregnancies and Mothers Over Age 35
In high-risk pregnancies, particularly in women 35 years of age or older, additional testing is required because of the increased risk of chromosomal abnormalities. In these cases, the appropriate diagnostic approach is chromosomal screening for fetal abnormalities.
On exams, when the clinical stem emphasizes advanced maternal age or otherwise labels the pregnancy as high risk, the correct answer is chromosomal screening, rather than repeating routine prenatal laboratory tests.
.
Routine Prenatal Screening Tests
Basic prenatal screening is recommended for all pregnancies to assess maternal health, identify infectious risks, and evaluate fetal development. These tests are part of standard obstetric care and are not dependent on maternal age or risk status. Routine prenatal screening includes cervical cytology, a complete blood count (CBC), and urinalysis to detect anemia, infection, or renal abnormalities. Maternal blood testing also includes blood group, Rh factor, and antibody screening to prevent hemolytic disease of the newborn, along with serologic testing for syphilis and assessment of rubella immunity.
Additional routine evaluations include glucose screening for gestational diabetes and fetal ultrasound for pregnancy dating, growth monitoring, and anatomic assessment. Cervical cultures are obtained to screen for Neisseria gonorrhoeae, Chlamydia trachomatis, and Group B Streptococcus, which are important causes of maternal and neonatal infection.
High-Risk Pregnancies and Mothers Over Age 35
In high-risk pregnancies, particularly in women 35 years of age or older, additional testing is required because of the increased risk of chromosomal abnormalities. In these cases, the appropriate diagnostic approach is chromosomal screening for fetal abnormalities.
On exams, when the clinical stem emphasizes advanced maternal age or otherwise labels the pregnancy as high risk, the correct answer is chromosomal screening, rather than repeating routine prenatal laboratory tests.
.

- Published on
Diagnostic Tests: Diagnostic Peritoneal Lavage (DPL)
When to Answer DPL
Diagnostic peritoneal lavage is indicated in the setting of blunt abdominal trauma when the patient is hemodynamically unstable or unconscious and the abdomen cannot be reliably examined. The classic scenario is a comatose or intoxicated trauma patient with multiple injuries and unexplained shock, where rapid determination of intra-abdominal bleeding is required. In this procedure, a catheter is placed into the peritoneal cavity, saline is infused, then aspirated and analyzed for evidence of injury.
Patients in Whom DPL Should NOT Be Used
DPL is not appropriate in several important clinical situations:
Findings That Make DPL Positive
A DPL is considered positive when any of the following are found in the aspirated fluid:
Any of these findings indicates significant intra-abdominal injury requiring surgical intervention.
What DPL Misses
A major limitation of DPL is that it is inadequate for detecting retroperitoneal injuries. Injuries to retroperitoneal structures such as the pancreas, kidneys, duodenum, or great vessels may be missed, making CT imaging superior in stable patients.
When to Answer DPL
Diagnostic peritoneal lavage is indicated in the setting of blunt abdominal trauma when the patient is hemodynamically unstable or unconscious and the abdomen cannot be reliably examined. The classic scenario is a comatose or intoxicated trauma patient with multiple injuries and unexplained shock, where rapid determination of intra-abdominal bleeding is required. In this procedure, a catheter is placed into the peritoneal cavity, saline is infused, then aspirated and analyzed for evidence of injury.
Patients in Whom DPL Should NOT Be Used
DPL is not appropriate in several important clinical situations:
- Patients with signs of an acute abdomen
Any evidence of a perforated viscus or clear intra-abdominal bleeding mandates immediate surgical exploration, not DPL. - Patients with gunshot wounds to the abdomen
Penetrating abdominal trauma from firearms is an indication for direct surgical exploration. - Hemodynamically stable patients with abdominal trauma
If the patient is stable and there are no definitive signs of perforation on physical exam, the correct study is an abdominal CT scan, not DPL.
Findings That Make DPL Positive
A DPL is considered positive when any of the following are found in the aspirated fluid:
- Red blood cells >100,000/mm³
- White blood cells >500/mm³
- Presence of bile
- Presence of feces
Any of these findings indicates significant intra-abdominal injury requiring surgical intervention.
What DPL Misses
A major limitation of DPL is that it is inadequate for detecting retroperitoneal injuries. Injuries to retroperitoneal structures such as the pancreas, kidneys, duodenum, or great vessels may be missed, making CT imaging superior in stable patients.

- Published on
Diagnostic Tests: Diagnostic Abdominal Laparoscopy (DAL)
Overview — What This Test Is
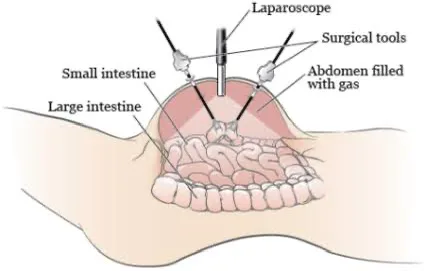
Diagnostic abdominal laparoscopy (DAL) is a minimally invasive surgical procedure that allows direct visualization of intra-abdominal structures using a laparoscope inserted through small abdominal incisions. Because it permits real-time inspection of organs, DAL is highly accurate when noninvasive tests fail to provide a clear diagnosis. It can also guide immediate management decisions and, in some cases, allow therapeutic intervention.
DAL is particularly useful in evaluating conditions where imaging or biopsy results are inconclusive and where a full exploratory laparotomy may be unnecessarily invasive.
Non-Trauma Indications for DAL
Diagnostic abdominal laparoscopy is used for direct evaluation in several non-trauma scenarios, including:
In these cases, DAL provides superior anatomic detail compared with imaging alone.
When to Answer DAL in Trauma Patients
In trauma settings, DAL is indicated in hemodynamically stable patients as a less invasive alternative to exploratory laparotomy. It is especially valuable when:
DAL is particularly useful for detecting diaphragmatic injuries, which are often difficult to identify on CT imaging alone.
A classic scenario is a motor vehicle accident victim with persistent concern for abdominal injury despite inconclusive imaging studies.
Overview — What This Test Is
Diagnostic abdominal laparoscopy (DAL) is a minimally invasive surgical procedure that allows direct visualization of intra-abdominal structures using a laparoscope inserted through small abdominal incisions. Because it permits real-time inspection of organs, DAL is highly accurate when noninvasive tests fail to provide a clear diagnosis. It can also guide immediate management decisions and, in some cases, allow therapeutic intervention.
DAL is particularly useful in evaluating conditions where imaging or biopsy results are inconclusive and where a full exploratory laparotomy may be unnecessarily invasive.
Non-Trauma Indications for DAL
Diagnostic abdominal laparoscopy is used for direct evaluation in several non-trauma scenarios, including:
- Ascites of unclear etiology, when fluid analysis and imaging are nondiagnostic
- Liver disease with an inconclusive biopsy, allowing direct inspection and targeted sampling
- Staging of abdominal malignancies, to assess tumor spread and operability
In these cases, DAL provides superior anatomic detail compared with imaging alone.
When to Answer DAL in Trauma Patients
In trauma settings, DAL is indicated in hemodynamically stable patients as a less invasive alternative to exploratory laparotomy. It is especially valuable when:
- The patient has suffered blunt or penetrating trauma
- Abdominal CT scan is nondiagnostic or equivocal
- There is ongoing suspicion of intra-abdominal organ injury
DAL is particularly useful for detecting diaphragmatic injuries, which are often difficult to identify on CT imaging alone.
A classic scenario is a motor vehicle accident victim with persistent concern for abdominal injury despite inconclusive imaging studies.
- Published on
Diagnostic Tests: Pelvic Laparoscopy
Overview — What This Test Is
Pelvic laparoscopy is a minimally invasive surgical procedure that allows direct visualization of pelvic structures through small abdominal incisions using a laparoscope. Because it provides real-time, direct inspection, pelvic laparoscopy is considered the most accurate diagnostic test for several gynecologic conditions, particularly when noninvasive imaging is inconclusive.
It can also be diagnostic and therapeutic, allowing for immediate intervention during the same procedure.
Conditions Best Diagnosed With Pelvic Laparoscopy
Pelvic laparoscopy is the most accurate test for diagnosing:
When Pelvic Laparoscopy Is the Correct Answer
Choose pelvic laparoscopy in high-risk or unclear cases where rapid, definitive diagnosis is required:
In these scenarios, laparoscopy allows immediate confirmation and management of potentially life-threatening or refractory pelvic conditions.
Overview — What This Test Is
Pelvic laparoscopy is a minimally invasive surgical procedure that allows direct visualization of pelvic structures through small abdominal incisions using a laparoscope. Because it provides real-time, direct inspection, pelvic laparoscopy is considered the most accurate diagnostic test for several gynecologic conditions, particularly when noninvasive imaging is inconclusive.
It can also be diagnostic and therapeutic, allowing for immediate intervention during the same procedure.
Conditions Best Diagnosed With Pelvic Laparoscopy
Pelvic laparoscopy is the most accurate test for diagnosing:
- Ectopic pregnancy
- Pelvic inflammatory disease (PID), especially complicated or refractory cases
- Endometriosis
- Ovarian or pelvic cysts
- Chronic pelvic pain of unclear etiology
When Pelvic Laparoscopy Is the Correct Answer
Choose pelvic laparoscopy in high-risk or unclear cases where rapid, definitive diagnosis is required:
- Pelvic pain with vaginal bleeding and a positive β-hCG, particularly when:
- The β-hCG level is lower than expected for the estimated gestational age
- There is concern for ectopic pregnancy
- Persistent lower abdominal pain in a woman treated for PID who shows an incomplete response to antibiotics, and pregnancy has been excluded
In these scenarios, laparoscopy allows immediate confirmation and management of potentially life-threatening or refractory pelvic conditions.

- Published on
Diagnostic Tests: Urine Microalbumin
Overview — What This Test Is
Urine microalbumin testing detects small amounts of albumin in the urine that are not identified by standard urine dipstick testing. It is a highly sensitive screening test for early diabetic nephropathy, identifying kidney damage before overt proteinuria or decline in renal function occurs.
When to Answer Urine Microalbumin
You should choose urine microalbumin in a clinical scenario involving:
If a standard urine dipstick is already positive for protein, microalbumin testing is not necessary, as the disease has progressed beyond the microalbumin stage. In clinical practice, yearly screening with urine microalbumin is recommended for diabetic patients.
Treatment When the Test Is Positive
If microalbuminuria is detected, the treatment is aimed at preventing progression of diabetic kidney disease. The primary therapy is:
These medications reduce intraglomerular pressure and slow the progression of nephropathy, even in patients who are not hypertensive.
What Constitutes a Positive Test
Urine albumin excretion is interpreted as follows:
Overview — What This Test Is
Urine microalbumin testing detects small amounts of albumin in the urine that are not identified by standard urine dipstick testing. It is a highly sensitive screening test for early diabetic nephropathy, identifying kidney damage before overt proteinuria or decline in renal function occurs.
When to Answer Urine Microalbumin
You should choose urine microalbumin in a clinical scenario involving:
- Diabetes mellitus for more than 5 years
- Normal serum creatinine and normal GFR
- Negative routine urinalysis for protein
If a standard urine dipstick is already positive for protein, microalbumin testing is not necessary, as the disease has progressed beyond the microalbumin stage. In clinical practice, yearly screening with urine microalbumin is recommended for diabetic patients.
Treatment When the Test Is Positive
If microalbuminuria is detected, the treatment is aimed at preventing progression of diabetic kidney disease. The primary therapy is:
- ACE inhibitors or
- Angiotensin receptor blockers (ARBs)
These medications reduce intraglomerular pressure and slow the progression of nephropathy, even in patients who are not hypertensive.
What Constitutes a Positive Test
Urine albumin excretion is interpreted as follows:
- Published on
Diagnostic Tests: Intravenous Pyelogram (IVP)
Overview — Clinical Context for IVP
An intravenous pyelogram (IVP) is a historical imaging test that involved injecting intravenous contrast followed by a series of X-rays to visualize the renal collecting system, including the calyces, renal pelvis, and ureters. Although it was once used to evaluate renal colic, especially when no stones were visible on plain radiographs, IVP has little to no role in modern clinical practice and is almost always an incorrect answer on exams.
Because the test is slow, requires contrast, and provides limited information compared with modern imaging, it has largely been abandoned.
Most Accurate and Preferred Tests Today
IVP has been replaced by safer and more effective imaging modalities:
Because IVP uses contrast, it carries risks of contrast-induced nephropathy and allergic reactions, making it inferior to CT and ultrasound.
Key Exam Pearl
If ultrasound or CT scan appears as an answer choice, IVP is never the correct answer. On exams, IVP is typically included as a distractor rather than the best diagnostic option.
Overview — Clinical Context for IVP
An intravenous pyelogram (IVP) is a historical imaging test that involved injecting intravenous contrast followed by a series of X-rays to visualize the renal collecting system, including the calyces, renal pelvis, and ureters. Although it was once used to evaluate renal colic, especially when no stones were visible on plain radiographs, IVP has little to no role in modern clinical practice and is almost always an incorrect answer on exams.
Because the test is slow, requires contrast, and provides limited information compared with modern imaging, it has largely been abandoned.
Most Accurate and Preferred Tests Today
IVP has been replaced by safer and more effective imaging modalities:
- Renal ultrasound
- Best initial test for suspected renal colic
- No radiation or contrast
- Especially useful in pregnancy or patients with renal insufficiency
- Non-contrast CT scan of the abdomen and pelvis
- Most accurate test for detecting kidney stones
- Fast, highly sensitive and specific
- Does not require contrast when evaluating for stones
Because IVP uses contrast, it carries risks of contrast-induced nephropathy and allergic reactions, making it inferior to CT and ultrasound.
Key Exam Pearl
If ultrasound or CT scan appears as an answer choice, IVP is never the correct answer. On exams, IVP is typically included as a distractor rather than the best diagnostic option.

- Published on
Diagnostic Tests: Right Upper Quadrant (RUQ) Ultrasound
Clinical Scenarios Where RUQ Ultrasound Is the Correct Answer
A right upper quadrant ultrasound is the first-line imaging test when a patient presents with right upper quadrant abdominal pain, with or without fever. It is specifically designed to evaluate the hepatobiliary system and is highly effective for identifying both liver and biliary tract pathology. RUQ ultrasound is appropriate when assessing:
Most Accurate Diagnostic Tests
While RUQ ultrasound is the best initial test, the most accurate diagnostic tests depend on the suspected pathology:
Significance of Pain During RUQ Ultrasound
If the patient experiences marked tenderness when the ultrasound transducer presses over the gallbladder, this finding is known as a positive Murphy’s sign. A sonographic Murphy’s sign is highly suggestive of acute cholecystitis, especially when accompanied by gallstones, gallbladder wall thickening, or pericholecystic fluid on ultrasound.
Clinical Scenarios Where RUQ Ultrasound Is the Correct Answer
A right upper quadrant ultrasound is the first-line imaging test when a patient presents with right upper quadrant abdominal pain, with or without fever. It is specifically designed to evaluate the hepatobiliary system and is highly effective for identifying both liver and biliary tract pathology. RUQ ultrasound is appropriate when assessing:
- Liver pathology, including:
- Hepatic masses (tumors, abscesses, cysts)
- Evidence of portal hypertension
- Gallbladder and biliary tree disorders, such as:
- Cholelithiasis
- Acute or chronic cholecystitis
- Choledocholithiasis
- Cholangitis
Most Accurate Diagnostic Tests
While RUQ ultrasound is the best initial test, the most accurate diagnostic tests depend on the suspected pathology:
- Biliary pathology (stones, obstruction, cholangitis):
- ERCP (Endoscopic Retrograde Cholangiopancreatography)
- MRCP (Magnetic Resonance Cholangiopancreatography)
- Liver pathology (tumors, diffuse liver disease):
- Liver biopsy is the most accurate test
Significance of Pain During RUQ Ultrasound
If the patient experiences marked tenderness when the ultrasound transducer presses over the gallbladder, this finding is known as a positive Murphy’s sign. A sonographic Murphy’s sign is highly suggestive of acute cholecystitis, especially when accompanied by gallstones, gallbladder wall thickening, or pericholecystic fluid on ultrasound.

- Published on
Diagnostic Tests: Renal Ultrasound
Overview — Clinical Conditions Commonly Evaluate
Renal ultrasound is a noninvasive imaging study that uses sound waves to visualize the kidneys and surrounding structures. It does not require contrast and exposes the patient to no radiation, making it especially useful as a first-line test in many renal and urinary conditions. Renal ultrasound is commonly used in the evaluation of:
Because it is safe, quick, and widely available, renal ultrasound is often preferred as the initial imaging modality.
When Renal Ultrasound Is the Correct Answer
You should answer renal ultrasound in clinical scenarios involving unexplained urinary or flank symptoms, particularly when structural disease or obstruction is suspected. Typical situations include:
Overview — Clinical Conditions Commonly Evaluate
Renal ultrasound is a noninvasive imaging study that uses sound waves to visualize the kidneys and surrounding structures. It does not require contrast and exposes the patient to no radiation, making it especially useful as a first-line test in many renal and urinary conditions. Renal ultrasound is commonly used in the evaluation of:
- Kidney stones (to detect hydronephrosis from obstruction)
- Congenital renal malformations
- Pediatric renal tumors
- Recurrent urinary tract infections
- Chronic renal failure (to assess kidney size and chronicity)
- Renal artery stenosis (with Doppler studies)
- Polycystic kidney disease
Because it is safe, quick, and widely available, renal ultrasound is often preferred as the initial imaging modality.
When Renal Ultrasound Is the Correct Answer
You should answer renal ultrasound in clinical scenarios involving unexplained urinary or flank symptoms, particularly when structural disease or obstruction is suspected. Typical situations include:
- Unexplained hematuria, especially when associated with flank pain or tenderness
- Flank pain suggestive of renal obstruction or infection
- Dysuric symptoms (frequency, burning with urination) accompanied by:
- White blood cells on urinalysis
- Flank pain, raising concern for upper urinary tract involvement (e.g., pyelonephritis or obstruction)

- Published on
Diagnostic Tests: Cystography (Voiding Cystography / Voiding Cystourethrography)
Overview — What This Test Is
Cystography, also known as voiding cystography or voiding cystourethrography (VCUG), is a radiographic imaging study used to visualize the bladder and urethra during filling and emptying. Contrast material is instilled into the bladder through a catheter, and X-ray images are obtained as the bladder fills and during voiding. This test evaluates the anatomy and integrity of the lower urinary tract, particularly the bladder and urethra.
It is important not to confuse cystography with cystometrics, which measures bladder pressures and is used primarily to evaluate urinary incontinence. Cystography assesses structure and reflux, not pressure.
When to Choose Cystography
Cystography is the correct diagnostic study in several clinical scenarios where structural abnormalities or reflux are suspected. These include:
Bladder Trauma
- Suspected bladder rupture following pelvic or abdominal trauma
Neoplasia
- Evaluation of tumors in or around the bladder
Urinary Tract Infections in Children
Cystography is particularly important in pediatric UTI evaluation to detect vesicoureteral reflux (VUR). Indications include:
- All children younger than 5 years old with a UTI
- Children of any age with febrile UTI
- All boys, regardless of age, with a UTI
These populations have a higher risk of underlying anatomic abnormalities that predispose them to recurrent infections and renal damage.

