- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Peptic Ulcer Disease
Peptic ulcer disease (PUD) results from a breakdown in the protective mucosal defenses of the stomach or duodenum, leading to ulceration from acid and pepsin injury. The condition develops when there is an imbalance between gastric acid production and the mucosa’s ability to protect itself. The two most common causes are infection with Helicobacter pylori and nonsteroidal anti-inflammatory drug (NSAID) use.
Helicobacter pylori is a gram-negative spiral bacterium that colonizes the gastric mucous layer. It is responsible for approximately 90–95% of duodenal ulcers and 80% of gastric ulcers. The organism increases antral gastrin production and impairs mucosal integrity. NSAIDs, including aspirin, interfere with prostaglandin synthesis, weakening mucosal defenses and predisposing to ulcer formation. Additional risk factors include cigarette smoking, alcohol use, severe physiologic stress, hypersecretory states (such as Zollinger–Ellison syndrome), and genetic predisposition, with more than 20% of patients reporting a family history.
Patients commonly present with epigastric pain described as burning, gnawing, or aching. The pain is typically midline and may be localized to the xiphoid or umbilical region. Duodenal ulcer pain usually occurs 90 minutes to 3 hours after meals, may awaken the patient at night, and is often relieved by food or antacids. In contrast, gastric ulcer pain typically worsens after meals and may be associated with nausea and anorexia. Clinical differentiation between gastric and duodenal ulcers can be difficult. Relief with antacids is common. Some patients present with heme-positive stools.
Complications are critical to recognize in the emergency setting. Acute perforation presents with sudden severe pain, rigid boardlike abdomen, generalized rebound tenderness, and possible radiation to the back or shoulder. Gastric outlet obstruction manifests with vomiting, abdominal distention, and a succussion splash. Hemorrhage may present with hematemesis, melena, hypotension, tachycardia, pallor, and orthostatic changes. NSAID-induced ulcers may be clinically silent until complications occur.
Initial evaluation includes a careful abdominal examination, Hemoccult testing, and assessment of vital signs including orthostatics. Laboratory findings are often normal in uncomplicated disease. A low hematocrit suggests bleeding, while leukocytosis may indicate perforation or penetration. Amylase and lipase may be elevated with penetration or when pancreatitis is in the differential. Type and cross-match should be performed in significant blood loss. Testing for H. pylori may include urea breath test, serology, or stool antigen testing. Chest or abdominal radiographs are useful when perforation or obstruction is suspected. Endoscopy is the diagnostic procedure of choice, allowing direct visualization, biopsy, and evaluation for malignancy.
Emergency management begins with ABC stabilization. Hypotensive patients require IV fluid resuscitation with large-bore IV access and early type and cross-match. Nasogastric decompression may be indicated in obstruction or significant hemorrhage. Pain may be treated with antacids or IV H2-receptor antagonists. Narcotics should be used cautiously to avoid masking serious pathology.
Ulcer healing is promoted with acid suppression therapy. Proton pump inhibitors (PPIs) such as omeprazole, pantoprazole, or lansoprazole are highly effective. H2-receptor antagonists (e.g., famotidine) may also be used. Sucralfate and misoprostol are additional options. Combined use of sucralfate with H2 blockers or PPIs is generally not recommended due to lack of additional benefit. NSAIDs should be discontinued whenever possible.
Eradication of H. pylori is essential in infected patients. Standard triple therapy includes a PPI plus clarithromycin and amoxicillin for 14 days. In penicillin-allergic patients, clarithromycin and metronidazole are substituted. Quadruple therapy with bismuth, tetracycline, metronidazole, and a PPI is used in resistant cases or as second-line therapy.
Complications require urgent consultation. Active upper GI bleeding necessitates fluid resuscitation, possible transfusion, and gastroenterology consultation for endoscopic therapy. Perforation requires emergency surgical consultation and broad-spectrum antibiotics. Gastric outlet obstruction requires decompression and supportive care.
Patients with uncomplicated disease, stable vital signs, normal hematocrit, and heme-negative stools may be discharged with acid suppression therapy and close outpatient follow-up. Admission is required for obstruction, perforation, active bleeding, significant anemia, or uncontrolled pain. All patients should have follow-up within 2–6 weeks to assess response to therapy. Patients older than 55 years or those with alarm symptoms should undergo endoscopic evaluation to exclude malignancy.
Early recognition and appropriate eradication of H. pylori, along with acid suppression and avoidance of NSAIDs, are the cornerstones of therapy. Failure to ensure follow-up may result in missed complications, including gastric cancer.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Perforated Viscus
A perforated viscus is a full-thickness disruption of a hollow abdominal organ that allows gastrointestinal contents to spill into the peritoneal cavity. This results in chemical and bacterial peritonitis, leading rapidly to systemic inflammatory response and potential septic shock. Perforation may occur from ulceration, inflammation, obstruction, ischemia, trauma, or iatrogenic injury. It is a surgical emergency requiring rapid recognition and intervention.
The most common cause is perforated peptic ulcer disease, frequently associated with NSAID use or Helicobacter pylori infection. Other causes include small bowel ischemia, inflammatory bowel disease, neoplasms, foreign bodies, diverticular disease, appendicitis, penetrating or blunt abdominal trauma, endoscopic procedures, and radiation enteritis or proctitis. In pediatric patients, trauma is the most common cause, particularly in neonates after difficult delivery, nonaccidental trauma, motor vehicle collisions, or falls. The jejunum is a common rupture site in children.
Patients typically present with sudden, severe abdominal pain that is initially localized but rapidly becomes diffuse as peritonitis develops. Examination reveals rigidity, guarding, rebound tenderness, and absent bowel sounds. Systemic findings may include fever, tachycardia, tachypnea, and hypotension. In advanced cases, patients may present in hypovolemic or septic shock. Elderly patients often have atypical presentations with less pronounced pain, minimal guarding, absence of leukocytosis, altered mental status, hypothermia, or blunted tachycardia due to medications or comorbidities.
The essential initial study is an upright chest radiograph to detect pneumoperitoneum. After the patient has been upright for 5–10 minutes, as little as 1–2 mL of free air may be visualized under the diaphragm. Sensitivity ranges from 50% to 85%. A left lateral decubitus abdominal radiograph may be more sensitive than a supine film. The double wall (Rigler) sign, in which both the mucosal and serosal surfaces of bowel are visible, suggests free intraperitoneal air. Abdominal CT is highly sensitive for detecting small amounts of free air and is indicated when clinical suspicion remains high despite normal plain films.
Laboratory evaluation includes CBC, electrolytes, renal function, glucose, liver function tests, coagulation profile, urinalysis, lipase, arterial blood gas, and lactate. Leukocytosis and elevated lactate support the diagnosis but are not required. Type and cross-match should be performed in unstable patients. ECG may be necessary to exclude cardiac causes of abdominal pain. In pregnant patients, ectopic pregnancy must be excluded.
Management begins with aggressive resuscitation following trauma and sepsis principles. Hypotension and tachycardia are treated with rapid infusion of 0.9% normal saline, typically 500 mL to 1 L boluses in adults, repeated as needed. Pediatric patients receive 20 mL/kg boluses. Vasopressors may be required if fluids are insufficient. Nasogastric decompression and Foley catheter placement are recommended. Broad-spectrum intravenous antibiotics must be administered promptly to cover enteric gram-negative bacilli, gram-positive cocci, and anaerobes. Appropriate regimens include a carbapenem, piperacillin–tazobactam, or a third- or fourth-generation cephalosporin combined with metronidazole. Analgesia should be provided without delaying surgical consultation.
Immediate surgical consultation is mandatory for all suspected or confirmed cases. Imaging should not delay operative intervention in unstable patients. Discharge is not appropriate, as perforated viscus is a surgical emergency requiring admission and definitive management. Early recognition, prompt antibiotic therapy, aggressive resuscitation, and urgent surgical intervention are critical to reducing morbidity and mortality.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Pericarditis
Pericarditis is inflammation, infection, or infiltration of the pericardial sac surrounding the heart. A pericardial effusion may or may not be present. Acute pericarditis has a rapid onset and may be complicated by cardiac tamponade if significant fluid accumulates. Constrictive pericarditis results from chronic inflammation leading to thickening, fibrosis, and adherence of the pericardium to the myocardium, impairing diastolic filling.
The most common cause is idiopathic, presumed viral in many cases. Viral etiologies include coxsackievirus, echovirus, adenovirus, Epstein–Barr virus, cytomegalovirus, hepatitis B, HIV, and others. Bacterial causes include tuberculosis, staphylococcal and streptococcal species, Haemophilus, Salmonella, and Legionella. Fungal, parasitic, neoplastic, uremic, autoimmune, post–myocardial infarction (Dressler syndrome), radiation, trauma, postpericardiotomy, aortic dissection, myxedema, pancreatitis, inflammatory bowel disease, amyloidosis, and drug-induced causes are also recognized.
Chest pain is the hallmark symptom. It is typically sharp, pleuritic, and substernal, worsened by lying supine or coughing, and improved by sitting up or leaning forward. Pain may radiate to the trapezius ridge due to phrenic nerve irritation. Associated symptoms include fever, mild dyspnea, cough, hoarseness, nausea, and anorexia. A history of recent viral illness, autoimmune disease, malignancy, or prior pericarditis episodes is common.
On examination, tachycardia and tachypnea may be present. A pericardial friction rub is highly specific and best heard at the lower left sternal border, often accentuated when the patient leans forward. The classic rub is triphasic, with presystolic, systolic, and early diastolic components, though any combination may be heard. If a significant effusion develops, features of cardiac tamponade may appear, including hypotension, jugular venous distention, and muffled heart sounds. Pulsus paradoxus may be present. Constrictive pericarditis produces signs of right- and left-sided heart failure such as peripheral edema, ascites, hepatic congestion, and pulmonary edema.
Electrocardiography typically demonstrates four classic stages. Stage 1 shows diffuse concave ST elevation with PR depression, except in aVR and V1. Stage 2 reveals normalization of ST and PR segments with T-wave flattening. Stage 3 shows diffuse T-wave inversion. Stage 4 reflects normalization of T waves. Electrical alternans suggests a significant effusion. Cardiac enzymes may be mildly elevated in myopericarditis but are useful to distinguish from acute myocardial infarction.
Laboratory studies may show leukocytosis and elevated inflammatory markers such as ESR and C-reactive protein. Chest radiograph is usually normal unless more than 250 mL of fluid has accumulated, in which case cardiomegaly may be visible. Echocardiography is the diagnostic modality of choice for detecting pericardial effusion and can identify even small fluid collections. CT scanning can detect pericardial thickening or calcifications, particularly in constrictive pericarditis. Pericardiocentesis is reserved for diagnostic clarification or therapeutic relief in tamponade.
Initial management follows standard airway, breathing, and circulation principles. Emergent pericardiocentesis is indicated in hemodynamically unstable patients with tamponade. Most cases of idiopathic or viral pericarditis are treated with nonsteroidal anti-inflammatory drugs. Ibuprofen or aspirin are commonly used and may be tapered gradually to reduce recurrence. Colchicine is recommended in combination with NSAIDs to decrease recurrence rates and may be continued for approximately three months. Corticosteroids are reserved for refractory cases, autoimmune causes, or when NSAIDs are contraindicated, as they are associated with higher recurrence rates. Bacterial pericarditis requires urgent IV antibiotics and drainage. Uremic pericarditis requires intensified dialysis. Neoplastic pericarditis is managed in conjunction with oncology.
Patients with hemodynamic instability, cardiac tamponade, malignant arrhythmias, large effusions, anticoagulation use, high fever, immunosuppression, trauma, malignancy, or suspected bacterial etiology require hospital admission, often to a monitored or intensive care setting. Stable patients with mild symptoms and no high-risk features may be managed as outpatients with close follow-up.
The classic presentation includes a recent viral illness followed by sharp, positional chest pain and a friction rub. Distinguishing pericarditis from acute myocardial infarction and other causes of chest pain is critical. NSAIDs remain the cornerstone of therapy, and most patients improve within two weeks with appropriate treatment.
- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Perilunate Dislocation
Perilunate dislocation is a serious high-energy wrist injury in which the lunate remains aligned with the distal radius, while the distal carpal bones—most notably the capitate—are displaced dorsally in approximately 95% of cases and volarly in about 5%. It is an unstable injury that requires early surgical treatment because it carries a high risk of long-term complications, particularly post-traumatic arthritis. The scaphoid is frequently fractured in association with perilunate dislocations.
The usual mechanism of injury is wrist hyperextension combined with ulnar deviation. These injuries typically result from significant trauma such as falls from height, motor vehicle accidents, industrial accidents, or sporting injuries. Because of the force involved, concomitant upper extremity injuries are common and must always be assessed.
Patients typically present with severe wrist pain, marked swelling, and diffuse tenderness. There may be decreased range of motion and sometimes visible deformity. Paresthesias in the median nerve distribution are common due to swelling and compression within the carpal tunnel. A careful history often reveals a high-energy injury. On examination, the wrist is swollen and painful with limited motion. Sensory changes in the median nerve distribution may be present, and neurovascular status—including capillary refill and 2-point discrimination—must be carefully assessed and documented. Skin integrity should be evaluated, as open injuries can occur. Importantly, this diagnosis is frequently missed on initial evaluation.
Radiographs of the wrist are essential and must include AP, lateral, and oblique views. The true lateral view is most diagnostic. Normally, the radius, lunate, and capitate should align in a straight line on the lateral film. In perilunate dislocation, the lunate remains aligned with the radius, but the capitate is displaced dorsally (most commonly) or volarly. CT or MRI is generally not required in the emergency department but may be used for preoperative planning.
The differential diagnosis includes lunate dislocation, lunate fracture, scapholunate dissociation, distal radius fracture, and other ligamentous wrist injuries. In pediatric patients, nonaccidental trauma should be considered.
Management begins with assessment for more serious associated injuries, followed by immobilization, elevation, ice application, and adequate pain control. Closed reduction should be attempted emergently. Traction is applied for approximately 10 minutes using finger traps with counterweights, followed by manual traction. The injury is briefly recreated with wrist extension while volar pressure is applied over the lunate, and then slow wrist flexion is performed to relocate the distal carpal bones. After reduction, the wrist should be immobilized in a sugar-tong splint in neutral position, post-reduction radiographs obtained, and neurovascular status reassessed. Procedural sedation is often required.
Definitive treatment requires operative fixation with ligament repair to restore stability and minimize long-term complications. All patients should have urgent hand surgery consultation.
Patients should be admitted if the injury is open, irreducible, associated with neurovascular compromise, or part of multiple trauma. Closed injuries with successful reduction and intact neurovascular status may be discharged with reliable orthopedic follow-up within 2–3 days, though all cases ultimately require surgical evaluation.
Complications are common even with appropriate treatment and include median nerve injury, tendon problems, wrist instability, complex regional pain syndrome, decreased grip strength, and post-traumatic arthritis. Up to 25% of these injuries are missed at initial presentation. Delayed diagnosis significantly worsens outcomes and may necessitate salvage procedures.
- Published on
Emergency and Acute Medicine – Periodontal Abscess
A periodontal abscess is a localized collection of pus within the supporting structures of the teeth, including the periodontal ligament and alveolar bone. It typically develops as a complication of progressive periodontal disease, where bone loss leads to the formation of periodontal pockets. Food particles and debris accumulate within these pockets. Coronal epithelial tissues may reattach to the tooth surface while bacteria and debris remain trapped, impairing drainage. This environment promotes secondary infection and abscess formation.
Although primarily localized, periodontal abscesses can lead to serious complications if untreated. These include osteomyelitis, dentocutaneous fistula, cavernous sinus thrombosis, Ludwig angina, maxillary sinusitis, mediastinitis, tooth loss, and sepsis. In children, periodontal abscesses are rare; periapical abscesses are more common and typically originate in the pulp, often associated with dental caries.
The infection is usually polymicrobial. Common pathogens include anaerobic gram-negative rods, Peptostreptococci, viridans group streptococci, and Neisseria species.
Diagnosis is clinical. Patients typically present with localized dental pain, facial swelling, malaise, and sometimes fever. On examination, there may be focal gingival swelling or fluctuance, tenderness to palpation, increased tooth mobility, and possible lymphadenopathy. A parulis—a pimple-like lesion on the gingiva—may be present in chronic abscesses, representing the end of a draining sinus tract. Pus may be expressed from the sinus tract. Heat sensitivity may occur. Trismus is generally absent unless infection has spread to the muscles of mastication.
Imaging and laboratory studies are not routinely required for diagnosis. However, panoramic, periapical, or occlusal radiographs may help confirm the diagnosis and determine the extent of disease. Bedside ultrasound can assist in identifying fluid collections. CT imaging may be indicated if there is concern for extension into adjacent structures. Anaerobic cultures may be considered in complicated cases or in immunocompromised patients. Electric pulp testing, performed by a dental specialist during follow-up, helps assess tooth viability.
The differential diagnosis includes periapical abscess, maxillary sinusitis, aphthous ulcers, oral herpes, salivary gland tumors, mumps, sialadenitis, localized adenopathy, facial cellulitis, acute otitis media, and peritonsillar abscess. In children, periapical abscess is more likely. For asymptomatic parulis, fibroma, pyogenic granuloma, peripheral ossifying granuloma, or Kaposi sarcoma should be considered.
Prehospital management rarely involves airway emergencies. However, if signs of airway compromise are present, airway equipment should be available, the patient transported upright, and supplemental oxygen provided. Initial stabilization in the emergency setting includes assessment of airway patency and securing the airway if there is respiratory distress, inability to manage secretions, or significant oropharyngeal swelling.
Emergency department management focuses on analgesia and drainage. NSAIDs or opioids may be used for pain control. Incision and drainage are performed under local anesthesia, typically using 2% lidocaine with epinephrine. A small stab incision is made toward the alveolar bone, followed by blunt dissection and irrigation with saline. If the cavity is large, a small iodoform gauze or Penrose drain may be placed for 24–48 hours and secured to prevent aspiration.
Antibiotics are indicated when the abscess is extensive or when systemic signs are present. Penicillin VK is considered first-line therapy. For penicillin-allergic patients, azithromycin, erythromycin, or clindamycin may be used. Clindamycin is also appropriate for patients who fail penicillin therapy. Ampicillin/sulbactam may be required for severe infections. Warm salt water rinses are recommended hourly while awake for 24–48 hours.
Admission is required for severe infections, complications such as cavernous sinus thrombosis or osteomyelitis, airway compromise, Ludwig angina, systemic toxicity, immunocompromised patients, treatment failure, or inability to manage the condition at home. Uncomplicated cases may be discharged with close dental follow-up within 24–48 hours.
Dental follow-up is essential for definitive care, including assessment of tooth viability, possible extraction, root canal therapy, and removal of drains. Without proper dental evaluation, symptoms may recur and long-term tooth preservation may be compromised. Maxillary sinusitis may be misdiagnosed if a thorough oral examination is not performed, underscoring the importance of careful assessment and timely referral.
A periodontal abscess is a localized collection of pus within the supporting structures of the teeth, including the periodontal ligament and alveolar bone. It typically develops as a complication of progressive periodontal disease, where bone loss leads to the formation of periodontal pockets. Food particles and debris accumulate within these pockets. Coronal epithelial tissues may reattach to the tooth surface while bacteria and debris remain trapped, impairing drainage. This environment promotes secondary infection and abscess formation.
Although primarily localized, periodontal abscesses can lead to serious complications if untreated. These include osteomyelitis, dentocutaneous fistula, cavernous sinus thrombosis, Ludwig angina, maxillary sinusitis, mediastinitis, tooth loss, and sepsis. In children, periodontal abscesses are rare; periapical abscesses are more common and typically originate in the pulp, often associated with dental caries.
The infection is usually polymicrobial. Common pathogens include anaerobic gram-negative rods, Peptostreptococci, viridans group streptococci, and Neisseria species.
Diagnosis is clinical. Patients typically present with localized dental pain, facial swelling, malaise, and sometimes fever. On examination, there may be focal gingival swelling or fluctuance, tenderness to palpation, increased tooth mobility, and possible lymphadenopathy. A parulis—a pimple-like lesion on the gingiva—may be present in chronic abscesses, representing the end of a draining sinus tract. Pus may be expressed from the sinus tract. Heat sensitivity may occur. Trismus is generally absent unless infection has spread to the muscles of mastication.
Imaging and laboratory studies are not routinely required for diagnosis. However, panoramic, periapical, or occlusal radiographs may help confirm the diagnosis and determine the extent of disease. Bedside ultrasound can assist in identifying fluid collections. CT imaging may be indicated if there is concern for extension into adjacent structures. Anaerobic cultures may be considered in complicated cases or in immunocompromised patients. Electric pulp testing, performed by a dental specialist during follow-up, helps assess tooth viability.
The differential diagnosis includes periapical abscess, maxillary sinusitis, aphthous ulcers, oral herpes, salivary gland tumors, mumps, sialadenitis, localized adenopathy, facial cellulitis, acute otitis media, and peritonsillar abscess. In children, periapical abscess is more likely. For asymptomatic parulis, fibroma, pyogenic granuloma, peripheral ossifying granuloma, or Kaposi sarcoma should be considered.
Prehospital management rarely involves airway emergencies. However, if signs of airway compromise are present, airway equipment should be available, the patient transported upright, and supplemental oxygen provided. Initial stabilization in the emergency setting includes assessment of airway patency and securing the airway if there is respiratory distress, inability to manage secretions, or significant oropharyngeal swelling.
Emergency department management focuses on analgesia and drainage. NSAIDs or opioids may be used for pain control. Incision and drainage are performed under local anesthesia, typically using 2% lidocaine with epinephrine. A small stab incision is made toward the alveolar bone, followed by blunt dissection and irrigation with saline. If the cavity is large, a small iodoform gauze or Penrose drain may be placed for 24–48 hours and secured to prevent aspiration.
Antibiotics are indicated when the abscess is extensive or when systemic signs are present. Penicillin VK is considered first-line therapy. For penicillin-allergic patients, azithromycin, erythromycin, or clindamycin may be used. Clindamycin is also appropriate for patients who fail penicillin therapy. Ampicillin/sulbactam may be required for severe infections. Warm salt water rinses are recommended hourly while awake for 24–48 hours.
Admission is required for severe infections, complications such as cavernous sinus thrombosis or osteomyelitis, airway compromise, Ludwig angina, systemic toxicity, immunocompromised patients, treatment failure, or inability to manage the condition at home. Uncomplicated cases may be discharged with close dental follow-up within 24–48 hours.
Dental follow-up is essential for definitive care, including assessment of tooth viability, possible extraction, root canal therapy, and removal of drains. Without proper dental evaluation, symptoms may recur and long-term tooth preservation may be compromised. Maxillary sinusitis may be misdiagnosed if a thorough oral examination is not performed, underscoring the importance of careful assessment and timely referral.

- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Periorbital and Orbital Cellulitis
Periorbital (preseptal) cellulitis and orbital cellulitis are infections involving the tissues around the eye, distinguished by their anatomic relationship to the orbital septum. The orbital septum is a connective tissue extension of the orbital periosteum that separates superficial eyelid structures from the deeper orbital contents. Periorbital cellulitis is confined to tissues anterior to this septum, whereas orbital cellulitis involves structures deep to it. This distinction is critical because orbital cellulitis is a true medical emergency with risk of permanent vision loss and life-threatening complications.
Periorbital cellulitis most commonly occurs as a complication of upper respiratory tract infection or sinusitis, where inflammatory edema leads to vascular and lymphatic congestion. It may also arise from local eyelid infections such as blepharitis, hordeolum, or dacryocystitis, or from surrounding skin disruptions including insect bites, minor trauma, impetigo, or dermatologic conditions. The septum typically acts as a barrier to deeper spread, although it may be incomplete.
Orbital cellulitis usually results from extension of infection from adjacent structures, most commonly ethmoid sinusitis penetrating the thin lamina papyracea. Other causes include dental abscess, retained orbital foreign body, puncture wounds, orbital fractures, postoperative infections, and hematogenous spread through valveless orbital veins. Rarely, it results from direct progression of periorbital cellulitis. Common pathogens include Streptococcus pneumoniae, Streptococcus viridans, Streptococcus pyogenes, Streptococcus anginosus, and Staphylococcus aureus. Anaerobes, Bacteroides species, and gram-negative organisms may also be involved.
All forms of orbital cellulitis carry significant morbidity and mortality risk. Complications include permanent visual loss, subperiosteal abscess, cavernous sinus thrombosis, and central nervous system infections. Fungal orbital cellulitis, particularly cerebrorhino-orbital phycomycosis (CROP), is rare but highly lethal, especially in immunocompromised patients and those with diabetic ketoacidosis. It often begins in the paranasal sinuses and invades blood vessels, causing thrombosis and tissue necrosis. Bloody nasal discharge and necrosis of the palate or nasal mucosa may be present.
In children, routine Hib and pneumococcal vaccinations have reduced incidence, but infection still occurs. Periorbital cellulitis is approximately five times more common and usually affects children younger than five years, whereas orbital cellulitis is more common in children older than five.
Both conditions present with unilateral red, swollen eyelids, and swelling may be severe in either. The key differences lie in systemic toxicity and ocular involvement. Orbital cellulitis is often preceded by sinusitis (60–90% of cases), dental infection, trauma, or recent surgery. Patients may report eye pain, visual changes, decreased color vision, diplopia, restricted or painful extraocular movements, and headache. Fever above 39°C and a toxic appearance are common. On examination, findings may include proptosis, conjunctival injection, chemosis, afferent pupillary defect, decreased visual acuity, ophthalmoplegia, and signs of meningismus.
Periorbital cellulitis typically follows local skin injury or superficial infection and presents more subacutely with low-grade fever and minimal systemic symptoms. Visual acuity and extraocular movements remain normal, and there are no signs of deep orbital involvement.
A complete eye examination is essential in all cases. This includes assessment of visual acuity, extraocular movements, pupillary response, fundoscopic examination, intraocular pressure measurement, and a thorough neurologic exam.
Laboratory studies are supportive but not diagnostic. A white blood cell count below 15,000 is more typical of periorbital cellulitis, whereas higher counts may suggest orbital involvement. Blood cultures and cultures of purulent material may be obtained, particularly if bacteremia is suspected. When gonorrhea is considered, appropriate culture media should be used.
Contrast-enhanced CT of the orbits is indicated when there are central nervous system signs, visual disturbances, proptosis, painful or restricted extraocular movements, ophthalmoplegia, bilateral edema, lack of improvement within 24 hours, or clinical deterioration. CT helps define the extent of infection, detect sinusitis, orbital emphysema, subperiosteal abscess, foreign bodies, and cavernous sinus thrombosis. Lumbar puncture may be necessary in toxic patients with meningismus to exclude CNS involvement.
Treatment depends on severity and depth of infection. Periorbital cellulitis in stable patients typically responds to oral antibiotics such as amoxicillin-clavulanate, cephalexin, clindamycin, or dicloxacillin. Parenteral antibiotics are indicated for toxic appearance, suspected bacteremia, or inability to tolerate oral therapy. Close follow-up within 24–48 hours is essential.
Orbital cellulitis requires hospital admission and immediate intravenous antibiotics. Early ophthalmology consultation is mandatory, and ENT consultation should be considered when sinusitis is the source. Empiric therapy commonly includes IV ceftriaxone or other broad-spectrum coverage, with vancomycin added if MRSA is suspected. Metronidazole may be included when anaerobic infection is likely. Surgical intervention may be required for abscess drainage, sinus decompression, or optic nerve decompression. In suspected fungal infection, high-dose IV amphotericin B and urgent surgical debridement are required.
Patients with periorbital cellulitis may be discharged if they have no systemic toxicity, no orbital findings, can tolerate oral antibiotics, and have reliable follow-up. Admission is required for orbital cellulitis, systemic toxicity, visual impairment, inability to arrange follow-up, progression on oral therapy, or high-risk conditions.
Any patient presenting with a red, swollen eye must be carefully evaluated for orbital cellulitis. A detailed history should include recent sinusitis, trauma, dental infection, surgery, immunocompromised state, or recent diabetic ketoacidosis. Clinicians must carefully assess for systemic toxicity, visual changes, pain with eye movement, and neurologic symptoms to avoid missing this potentially vision- and life-threatening condition.

- Published on
KembaraXtra -Medicine- Emergency and Acute Medicine – Peripheral Neuropathy
Peripheral neuropathy is a broad term describing disorders of peripheral nerves that may involve motor, sensory, or autonomic fibers. Patients commonly present with muscle weakness, atrophy, pain, numbness, or a combination of these symptoms. The condition may be acute or chronic, symmetric or asymmetric, and distal or proximal in distribution.
Etiology varies widely and depends on the clinical presentation. Causes include metabolic disorders, endocrine disease, nutritional deficiencies, toxins, medications, autoimmune conditions, infections, hereditary disorders, trauma, and neoplastic processes. Diabetes mellitus is the most common cause of symmetric peripheral neuropathy. Acute demyelinating processes such as Guillain–Barré syndrome must be considered in rapidly progressive cases.
Sensory nerve dysfunction presents with numbness, tingling, paresthesias, dysesthesias, or burning pain. Large-fiber neuropathy leads to decreased vibration and position sense, whereas small-fiber neuropathy affects pain and temperature sensation. Deep tendon reflexes are often reduced due to impairment of the sensory afferent limb. Symptoms typically follow a stocking-glove distribution in symmetric polyneuropathy.
Motor nerve involvement causes weakness, usually distal greater than proximal. Fasciculations may occur, and chronic disease can lead to muscle atrophy and diminished tone. Reflexes may be reduced or absent due to impaired motor efferent conduction.
Autonomic dysfunction may manifest as orthostatic hypotension, constipation, urinary retention, erectile dysfunction, or other signs of impaired autonomic regulation.
History should focus on duration of symptoms, pattern of involvement (symmetric versus asymmetric), distribution (distal versus proximal), and whether symptoms are sensory, motor, or mixed. Medication exposure, toxin exposure, systemic disease, recent infections, and family history should be reviewed.
Physical examination requires a thorough neurologic assessment, including strength testing, reflex evaluation, and detailed sensory examination. Sensory loss in a stocking-glove pattern supports a length-dependent polyneuropathy. Early absence of reflexes, particularly in an acute presentation, should raise concern for demyelinating neuropathy such as Guillain–Barré syndrome, which can progress to respiratory failure.
Essential evaluation depends on acuity and severity. In acute or rapidly progressive weakness, early neurology consultation is critical. Laboratory studies may include a basic metabolic panel, complete blood count, liver function tests, urinalysis, thyroid-stimulating hormone, and targeted testing such as HIV or vitamin B12 levels based on clinical suspicion. Electrocardiogram and imaging such as chest radiograph or head CT may be obtained when indicated by associated symptoms.
Electromyography and nerve conduction studies are typically arranged by neurology to characterize axonal versus demyelinating patterns. Lumbar puncture may be required when Guillain–Barré syndrome is suspected.
Differential diagnosis depends on distribution. Focal neuropathies are often due to entrapment syndromes such as carpal tunnel, ulnar tunnel, tarsal tunnel, or peroneal nerve compression. Multifocal neuropathy (mononeuropathy multiplex) may result from diabetes, vasculitis, connective tissue disease, sarcoidosis, leprosy, malignancy, or HIV infection. Symmetric polyneuropathy commonly results from diabetes, hypothyroidism, nutritional deficiency, alcohol use, medication toxicity, critical illness, electrolyte disturbances, toxins, or Guillain–Barré syndrome. Myelopathy may mimic peripheral neuropathy and should be suspected in patients with back pain, saddle anesthesia, or lower extremity weakness.
Initial management in the emergency setting focuses on airway protection in severe cases, especially when Guillain–Barré syndrome is suspected. Monitoring for respiratory compromise is essential. Offending toxins or medications should be discontinued, and underlying systemic conditions should be treated.
Pain control may include opioids when necessary. Neuropathic pain can be managed with agents such as gabapentin, titrated gradually to effect. Carbamazepine may be used for specific neuropathic syndromes such as trigeminal neuralgia. Intravenous immunoglobulin is indicated for Guillain–Barré syndrome.
Admission is required for patients with respiratory distress, acute gait disturbance, rapidly progressive weakness, or intractable pain. Stable patients without respiratory compromise or significant functional impairment may be discharged with appropriate outpatient follow-up.
Failure to recognize Guillain–Barré syndrome is a critical pitfall, as delayed diagnosis can lead to respiratory failure and significant morbidity. Early identification and appropriate monitoring are essential in patients with acute, progressive peripheral neuropathy.

- Published on
Emergency And Acute Medicine – Pertussis
Pertussis is an acute respiratory tract infection transmitted by small respiratory droplets. The organism attaches to respiratory epithelial cells via fimbriae and produces toxins that cause ciliary dysfunction, accumulation of debris, increased mucus production, and inflammatory infiltration. Bronchiolar congestion, obstruction, and necrosis may develop. Airway obstruction from mucus plugging can lead to hypoxia, hypoventilation, and increased intrathoracic or intracranial pressure. Secondary bacterial pneumonia may worsen respiratory failure. Central nervous system injury may result from encephalitis, hypoxia, or elevated intracranial pressure. Uncomplicated illness typically lasts 6–10 weeks, although about half resolve in under 6 weeks. Mortality is highest in infants under 1 year, especially those younger than 1 month. Most deaths are due to secondary bacterial pneumonia. The incubation period is usually 7–10 days. Disease is most common in young children, but incidence is increasing among adolescents. Adults serve as the primary reservoir. Peak incidence occurs in late summer and fall. Vaccination with Tdap provides prevention. The causative organism is Bordetella pertussis, a fastidious gram-negative pleomorphic bacillus.
The illness classically progresses through three phases, although infants may not follow distinct stages. The catarrhal stage lasts 1–2 weeks and resembles a mild upper respiratory infection with rhinorrhea, low-grade fever, malaise, sore throat, lacrimation, and mild cough. The paroxysmal stage lasts 1–6 weeks and is characterized by severe coughing spells that end with a sudden inspiratory “whoop.” Paroxysms may be associated with cyanosis, apnea (especially in infants under 6 months), post-tussive emesis, and altered mental status due to hypoxia. The convalescent stage lasts 2–12 weeks with gradual improvement and decreasing frequency of cough. Adults and partially immunized children often have milder or atypical presentations, sometimes limited to persistent cough without a classic whoop.
Diagnosis in the emergency setting is primarily clinical, especially when a characteristic paroxysmal cough is observed or there is a known exposure. Laboratory confirmation may support the diagnosis. PCR testing from a posterior nasopharyngeal swab or aspirate has high sensitivity and specificity but may produce false positives and false negatives depending on timing and prior antibiotic use. Culture on Bordet–Gengou medium remains the gold standard due to high specificity but has low sensitivity and requires 7–12 days for results. Serology is useful later in the course. Leukocytosis with marked lymphocytosis is common and correlates with disease severity. Chest radiographs are often normal but may show perihilar infiltrates, atelectasis, or secondary pneumonia.
Differential diagnoses include other causes of prolonged or paroxysmal cough such as infections with Bordetella parapertussis, Chlamydia species, adenovirus, pneumonia, bronchiolitis, influenza, reactive airway disease, foreign body aspiration, and cystic fibrosis.
Initial management focuses on airway and respiratory support. Oxygen supplementation and suctioning of mucus plugs are important, particularly in infants. Droplet precautions are required for 5 days after initiation of effective antimicrobial therapy. Adequate hydration must be maintained. Continuous monitoring is recommended during severe paroxysms, especially in infants. Antibiotics are most effective during the catarrhal phase but are still indicated during the paroxysmal phase to reduce transmission. Azithromycin is the first-line agent. Alternatives include clarithromycin, erythromycin, or trimethoprim–sulfamethoxazole, although erythromycin carries a risk of pyloric stenosis in neonates. Bronchodilators and corticosteroids are generally not recommended. Tdap vaccination should be offered when appropriate, including during each pregnancy between 27 and 36 weeks gestation to protect newborns.
Admission is indicated for patients under 1 year of age, those with apnea, cyanosis, pneumonia, encephalitis, or significant respiratory distress. Children without respiratory compromise may be discharged with close follow-up, hydration guidance, and avoidance of cough triggers such as smoke and pollutants. Postexposure prophylaxis with antibiotics is recommended for all close contacts regardless of age or immunization status. Patients may return to school or work after 5 days of appropriate antibiotic therapy.
Complications include epistaxis, subconjunctival hemorrhage, pneumonia, pneumothorax, subcutaneous or mediastinal emphysema, bronchiectasis, hernias, rectal prolapse, seizures, encephalitis, intracranial hemorrhage, and spinal epidural hemorrhage. Infants require particular vigilance due to high risk of apnea and severe respiratory compromise. Cases must be reported to public health authorities, and strict droplet precautions are essential to prevent spread.
Pertussis is an acute respiratory tract infection transmitted by small respiratory droplets. The organism attaches to respiratory epithelial cells via fimbriae and produces toxins that cause ciliary dysfunction, accumulation of debris, increased mucus production, and inflammatory infiltration. Bronchiolar congestion, obstruction, and necrosis may develop. Airway obstruction from mucus plugging can lead to hypoxia, hypoventilation, and increased intrathoracic or intracranial pressure. Secondary bacterial pneumonia may worsen respiratory failure. Central nervous system injury may result from encephalitis, hypoxia, or elevated intracranial pressure. Uncomplicated illness typically lasts 6–10 weeks, although about half resolve in under 6 weeks. Mortality is highest in infants under 1 year, especially those younger than 1 month. Most deaths are due to secondary bacterial pneumonia. The incubation period is usually 7–10 days. Disease is most common in young children, but incidence is increasing among adolescents. Adults serve as the primary reservoir. Peak incidence occurs in late summer and fall. Vaccination with Tdap provides prevention. The causative organism is Bordetella pertussis, a fastidious gram-negative pleomorphic bacillus.
The illness classically progresses through three phases, although infants may not follow distinct stages. The catarrhal stage lasts 1–2 weeks and resembles a mild upper respiratory infection with rhinorrhea, low-grade fever, malaise, sore throat, lacrimation, and mild cough. The paroxysmal stage lasts 1–6 weeks and is characterized by severe coughing spells that end with a sudden inspiratory “whoop.” Paroxysms may be associated with cyanosis, apnea (especially in infants under 6 months), post-tussive emesis, and altered mental status due to hypoxia. The convalescent stage lasts 2–12 weeks with gradual improvement and decreasing frequency of cough. Adults and partially immunized children often have milder or atypical presentations, sometimes limited to persistent cough without a classic whoop.
Diagnosis in the emergency setting is primarily clinical, especially when a characteristic paroxysmal cough is observed or there is a known exposure. Laboratory confirmation may support the diagnosis. PCR testing from a posterior nasopharyngeal swab or aspirate has high sensitivity and specificity but may produce false positives and false negatives depending on timing and prior antibiotic use. Culture on Bordet–Gengou medium remains the gold standard due to high specificity but has low sensitivity and requires 7–12 days for results. Serology is useful later in the course. Leukocytosis with marked lymphocytosis is common and correlates with disease severity. Chest radiographs are often normal but may show perihilar infiltrates, atelectasis, or secondary pneumonia.
Differential diagnoses include other causes of prolonged or paroxysmal cough such as infections with Bordetella parapertussis, Chlamydia species, adenovirus, pneumonia, bronchiolitis, influenza, reactive airway disease, foreign body aspiration, and cystic fibrosis.
Initial management focuses on airway and respiratory support. Oxygen supplementation and suctioning of mucus plugs are important, particularly in infants. Droplet precautions are required for 5 days after initiation of effective antimicrobial therapy. Adequate hydration must be maintained. Continuous monitoring is recommended during severe paroxysms, especially in infants. Antibiotics are most effective during the catarrhal phase but are still indicated during the paroxysmal phase to reduce transmission. Azithromycin is the first-line agent. Alternatives include clarithromycin, erythromycin, or trimethoprim–sulfamethoxazole, although erythromycin carries a risk of pyloric stenosis in neonates. Bronchodilators and corticosteroids are generally not recommended. Tdap vaccination should be offered when appropriate, including during each pregnancy between 27 and 36 weeks gestation to protect newborns.
Admission is indicated for patients under 1 year of age, those with apnea, cyanosis, pneumonia, encephalitis, or significant respiratory distress. Children without respiratory compromise may be discharged with close follow-up, hydration guidance, and avoidance of cough triggers such as smoke and pollutants. Postexposure prophylaxis with antibiotics is recommended for all close contacts regardless of age or immunization status. Patients may return to school or work after 5 days of appropriate antibiotic therapy.
Complications include epistaxis, subconjunctival hemorrhage, pneumonia, pneumothorax, subcutaneous or mediastinal emphysema, bronchiectasis, hernias, rectal prolapse, seizures, encephalitis, intracranial hemorrhage, and spinal epidural hemorrhage. Infants require particular vigilance due to high risk of apnea and severe respiratory compromise. Cases must be reported to public health authorities, and strict droplet precautions are essential to prevent spread.
- Published on
Emergency and Acute Medicine – Peritonsillar Abscess
Peritonsillar abscess is a suppurative complication of tonsillitis in which infection spreads beyond the tonsillar capsule into the space between the palatine tonsil and the pharyngeal muscles. It is the most common deep infection of the head and neck, with an incidence of approximately 30 per 100,000 people per year and about 45,000 cases annually in the United States. It occurs at any age but is most common in young adults between 20 and 40 years. Incidence peaks during November to December and April to May, corresponding with higher rates of streptococcal pharyngitis. Although uncommon, complications can include airway compromise, sepsis, recurrence in 12–15% of patients, spread to the lateral neck or mediastinum, spontaneous rupture with aspiration pneumonitis, internal jugular vein thrombosis (Lemierre syndrome), poststreptococcal glomerulonephritis or rheumatic fever, carotid sheath erosion with hemorrhage, severe dehydration, and intracranial extension such as meningitis, cavernous sinus thrombosis, cerebral abscess, or dural sinus thrombosis.
Two primary mechanisms are proposed for its development. One theory involves direct bacterial invasion into deeper tissues during acute pharyngitis. The other suggests obstruction and infection of the Weber glands located in the superior tonsillar pole. Smoking may increase risk. Infection is typically polymicrobial. Common pathogens include Group A Streptococcus, Staphylococcus species including MRSA, and anaerobes such as Prevotella, Peptostreptococcus, and Fusobacterium.
Patients commonly present with unilateral sore throat, fever, voice change, odynophagia, drooling, headache, referred ear pain, decreased oral intake, and malaise. Physical examination often reveals fever, trismus, a muffled “hot potato” voice, erythematous tonsils and soft palate, medial and inferior displacement of the superior pole of the affected tonsil, uvular deviation away from the affected side, halitosis, cervical lymphadenitis, and tenderness along the ipsilateral angle of the jaw. Airway assessment is critical, with attention to stridor, tripod positioning, or inability to handle secretions. Clinicians must also consider possible extension into deeper neck spaces when systemic toxicity or atypical findings are present.
Diagnosis is usually clinical based on careful oropharyngeal examination, although severe trismus may limit visualization. Throat culture and monospot testing may be considered, as infectious mononucleosis is present in up to 20% of cases. A complete blood count and abscess culture may be useful in selected patients. A basic metabolic panel may help assess dehydration. Bedside intraoral ultrasound can assist in identifying and localizing the abscess, particularly in cooperative patients, while transcutaneous ultrasound may be useful if trismus prevents intraoral imaging. CT of the neck with contrast is indicated when deep neck infection is suspected, after failed needle aspiration, or when examination is limited. MRI may help detect complications such as internal jugular vein thrombosis or carotid sheath involvement. Needle aspiration is both diagnostic and frequently therapeutic, and incision and drainage is also effective.
Management begins with airway evaluation and stabilization, IV access, cardiac and pulse oximetry monitoring, and supplemental oxygen as needed. Children account for 25–30% of cases and may require sedation or general anesthesia for drainage procedures. In young children with signs of upper airway obstruction, a lateral neck radiograph may be obtained before oral examination. Antibiotics should be started promptly, along with IV fluids for dehydration and appropriate analgesia. A single dose of corticosteroid such as dexamethasone may improve symptoms. Adequate local anesthesia using benzocaine spray and lidocaine with epinephrine is essential before drainage. Needle aspiration has a success rate of 87–94% and should be performed by clinicians experienced in airway management. The internal carotid artery lies approximately 2.5 cm posterolateral to the tonsil, so limiting needle depth to less than 0.5 cm is recommended. The superior pole is the most common site of maximal fluctuance. Incision and drainage has a success rate of 90–92% and should be performed using a guarded blade with no more than 1 cm exposed, avoiding incisions deeper than 0.5 cm. Packing is generally not required. Tonsillectomy may be indicated in cases of airway obstruction, recurrent severe pharyngitis, recurrent abscess, or failure of drainage.
Antibiotic therapy should continue for 14 days, as shorter courses may increase recurrence risk. Intravenous options include ampicillin/sulbactam or penicillin G combined with metronidazole. Clindamycin is appropriate for penicillin-allergic patients. Oral regimens include amoxicillin/clavulanate, penicillin VK with metronidazole, or clindamycin. A single dose of dexamethasone 10 mg (0.6 mg/kg in children, maximum 10 mg) may be administered.
Admission is indicated for airway compromise, sepsis, altered mental status, significant dehydration, or extension beyond the peritonsillar space. Most patients can be discharged after successful drainage if they tolerate oral intake and medications. Referral to otolaryngology is recommended, and interval tonsillectomy is often considered 6–8 weeks after resolution. Close follow-up within 24–48 hours is essential because treatment failure and recurrence are relatively common.
Peritonsillar abscess is a suppurative complication of tonsillitis in which infection spreads beyond the tonsillar capsule into the space between the palatine tonsil and the pharyngeal muscles. It is the most common deep infection of the head and neck, with an incidence of approximately 30 per 100,000 people per year and about 45,000 cases annually in the United States. It occurs at any age but is most common in young adults between 20 and 40 years. Incidence peaks during November to December and April to May, corresponding with higher rates of streptococcal pharyngitis. Although uncommon, complications can include airway compromise, sepsis, recurrence in 12–15% of patients, spread to the lateral neck or mediastinum, spontaneous rupture with aspiration pneumonitis, internal jugular vein thrombosis (Lemierre syndrome), poststreptococcal glomerulonephritis or rheumatic fever, carotid sheath erosion with hemorrhage, severe dehydration, and intracranial extension such as meningitis, cavernous sinus thrombosis, cerebral abscess, or dural sinus thrombosis.
Two primary mechanisms are proposed for its development. One theory involves direct bacterial invasion into deeper tissues during acute pharyngitis. The other suggests obstruction and infection of the Weber glands located in the superior tonsillar pole. Smoking may increase risk. Infection is typically polymicrobial. Common pathogens include Group A Streptococcus, Staphylococcus species including MRSA, and anaerobes such as Prevotella, Peptostreptococcus, and Fusobacterium.
Patients commonly present with unilateral sore throat, fever, voice change, odynophagia, drooling, headache, referred ear pain, decreased oral intake, and malaise. Physical examination often reveals fever, trismus, a muffled “hot potato” voice, erythematous tonsils and soft palate, medial and inferior displacement of the superior pole of the affected tonsil, uvular deviation away from the affected side, halitosis, cervical lymphadenitis, and tenderness along the ipsilateral angle of the jaw. Airway assessment is critical, with attention to stridor, tripod positioning, or inability to handle secretions. Clinicians must also consider possible extension into deeper neck spaces when systemic toxicity or atypical findings are present.
Diagnosis is usually clinical based on careful oropharyngeal examination, although severe trismus may limit visualization. Throat culture and monospot testing may be considered, as infectious mononucleosis is present in up to 20% of cases. A complete blood count and abscess culture may be useful in selected patients. A basic metabolic panel may help assess dehydration. Bedside intraoral ultrasound can assist in identifying and localizing the abscess, particularly in cooperative patients, while transcutaneous ultrasound may be useful if trismus prevents intraoral imaging. CT of the neck with contrast is indicated when deep neck infection is suspected, after failed needle aspiration, or when examination is limited. MRI may help detect complications such as internal jugular vein thrombosis or carotid sheath involvement. Needle aspiration is both diagnostic and frequently therapeutic, and incision and drainage is also effective.
Management begins with airway evaluation and stabilization, IV access, cardiac and pulse oximetry monitoring, and supplemental oxygen as needed. Children account for 25–30% of cases and may require sedation or general anesthesia for drainage procedures. In young children with signs of upper airway obstruction, a lateral neck radiograph may be obtained before oral examination. Antibiotics should be started promptly, along with IV fluids for dehydration and appropriate analgesia. A single dose of corticosteroid such as dexamethasone may improve symptoms. Adequate local anesthesia using benzocaine spray and lidocaine with epinephrine is essential before drainage. Needle aspiration has a success rate of 87–94% and should be performed by clinicians experienced in airway management. The internal carotid artery lies approximately 2.5 cm posterolateral to the tonsil, so limiting needle depth to less than 0.5 cm is recommended. The superior pole is the most common site of maximal fluctuance. Incision and drainage has a success rate of 90–92% and should be performed using a guarded blade with no more than 1 cm exposed, avoiding incisions deeper than 0.5 cm. Packing is generally not required. Tonsillectomy may be indicated in cases of airway obstruction, recurrent severe pharyngitis, recurrent abscess, or failure of drainage.
Antibiotic therapy should continue for 14 days, as shorter courses may increase recurrence risk. Intravenous options include ampicillin/sulbactam or penicillin G combined with metronidazole. Clindamycin is appropriate for penicillin-allergic patients. Oral regimens include amoxicillin/clavulanate, penicillin VK with metronidazole, or clindamycin. A single dose of dexamethasone 10 mg (0.6 mg/kg in children, maximum 10 mg) may be administered.
Admission is indicated for airway compromise, sepsis, altered mental status, significant dehydration, or extension beyond the peritonsillar space. Most patients can be discharged after successful drainage if they tolerate oral intake and medications. Referral to otolaryngology is recommended, and interval tonsillectomy is often considered 6–8 weeks after resolution. Close follow-up within 24–48 hours is essential because treatment failure and recurrence are relatively common.
- Published on
KembaraXtra – Emergency & Acute Medicine – Peripheral Vascular Disease
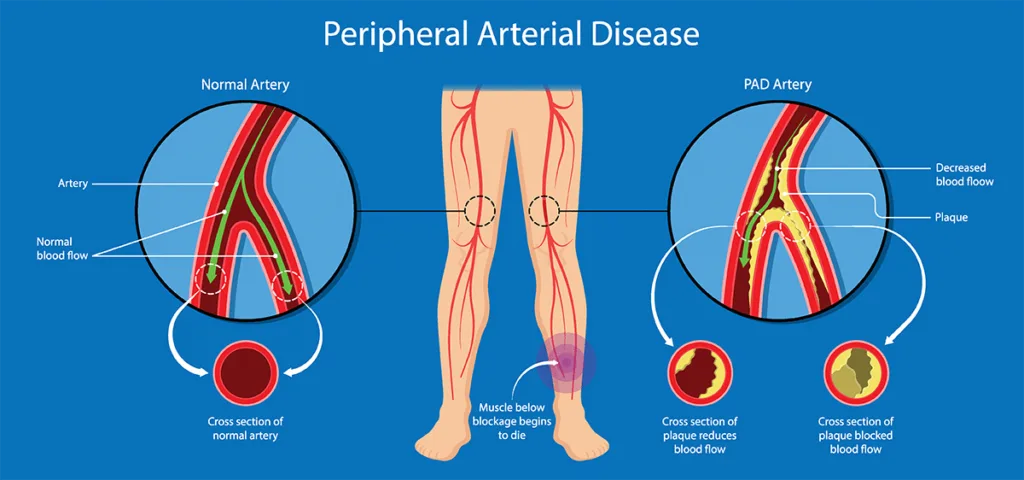
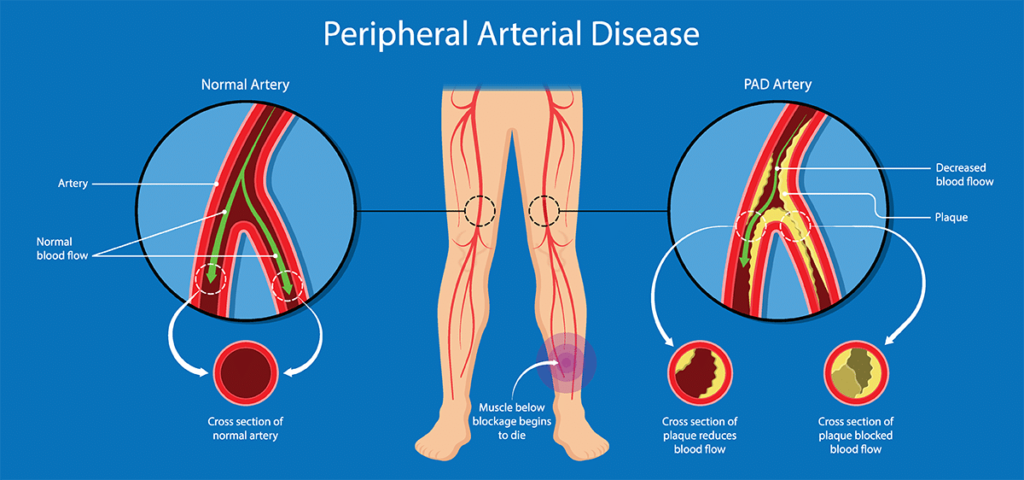
Peripheral vascular disease (PVD), also known as peripheral artery disease (PAD), refers to obstruction of one or more peripheral arteries due to atherosclerosis, thrombosis, or embolism. Many patients also have coexisting coronary artery disease and cerebrovascular disease. Major risk factors include age, smoking, diabetes mellitus, hyperlipidemia, and hypertension. PVD is associated with significant morbidity and mortality related to systemic atherosclerosis. Complications include aneurysm formation, thrombosis, ulceration, limb loss, and progression to critical limb ischemia.
Chronic arterial insufficiency (CAI) results from progressive atherosclerotic narrowing that produces subacute ischemia and claudication. About 10% of patients progress to critical limb ischemia. Acute arterial insufficiency (AAI) is caused by arterial thrombosis (approximately 50%) or embolism and produces acute limb ischemia characterized by the “6 Ps.” Atheroembolism occurs when rupture or disruption of an atherosclerotic plaque in the aorta, iliac, or femoral arteries releases cholesterol emboli that obstruct small vessels. It is often precipitated by invasive arterial procedures such as cardiac catheterization.
Etiologies include atherosclerotic plaque obstruction, arterial thrombosis, cardiac emboli (commonly from atrial fibrillation, valvular disease, or cardiomyopathy), aneurysm, infection, tumor, vasculitis, foreign body, thrombosis superimposed on chronic disease, and atheroembolism.
Patients with CAI typically report claudication—aching calf pain in femoropopliteal disease or buttock and thigh pain in aortoiliac disease—brought on by exertion and relieved with rest or dependent positioning. Severe disease presents with rest pain, usually beginning in the foot, or rapidly progressive claudication and ulceration. Acute arterial insufficiency presents with sudden extremity pain that increases in severity, often beginning distally and progressing proximally. Pain may decrease once sensory loss occurs. Atheroembolism presents with cold, painful digits and may involve multiple organs including kidneys, mesentery, and skin, especially following recent vascular procedures.
On examination, sudden onset of pain and pallor in an extremity is limb- and life-threatening. In CAI, findings include diminished or absent peripheral pulses, delayed capillary refill, cool skin, prolonged venous filling time, bruits, pallor with elevation and dependent rubor, muscle and skin atrophy, thickened nails, hair loss, and toe or heel ulcerations. Acute arterial insufficiency presents with the 6 Ps: pain, pallor, pulselessness, poikilothermia, paresthesias, and paralysis. Identifying a potential embolic source such as atrial fibrillation is essential. Atheroembolism may show painful ischemic digits, “blue toe syndrome,” and livedo reticularis.
The ankle–brachial index (ABI) is an important bedside test in chronic disease. An ABI <0.9 is abnormal and <0.4-0.5 indicates severe disease. in patients with diabetes, calcified vessels may produce falsely elevated values (>1.3). Acute arterial insufficiency is primarily a clinical diagnosis based on the 6 Ps. Patients with acute-on-chronic disease may tolerate ischemia better due to collateral circulation. Atheroembolism is diagnosed clinically, with further evaluation to identify the embolic source.
Laboratory evaluation includes CBC, platelets, electrolytes, renal function, glucose, coagulation studies, and creatine phosphokinase to assess muscle ischemia. Additional studies may include inflammatory markers for vasculitis, blood cultures for suspected endocarditis, and hypercoagulable testing when indicated.
Doppler ultrasound is commonly used to identify the level of arterial occlusion and detect thrombosis or aneurysm. CT angiography is widely used as a first-line diagnostic tool and guides decisions for operative or endovascular intervention. Angiography allows simultaneous diagnosis and treatment with angioplasty, atherectomy, or thrombolysis. MRI is sensitive but less practical in emergency settings.
Differential diagnoses include acute thrombosis or embolism, arterial dissection, deep venous thrombosis, venous insufficiency, compartment syndrome, Buerger disease, spinal stenosis, neuropathy, bursitis, arthritis, and reflex sympathetic dystrophy.
Prehospital care includes maintaining hemodynamic stability, placing the limb at rest in a dependent position, providing oxygen when needed, and cardiac monitoring. In the emergency department, management includes IV fluids for hypotension, cardiac monitoring, supplemental oxygen, adequate analgesia, and avoidance of temperature extremes.
Management of chronic arterial insufficiency includes antiplatelet therapy with aspirin (75–325 mg daily) or clopidogrel (75 mg daily). Cilostazol, pentoxifylline, or dipyridamole may be used in selected patients. Risk-factor modification is essential and includes smoking cessation, lipid and blood pressure control, diabetes management, and structured exercise therapy. Revascularization options include balloon angioplasty, atherectomy, or bypass grafting depending on anatomy and severity.
Acute arterial insufficiency requires immediate IV heparin (80 U/kg bolus followed by infusion at 18 U/kg/hr), unless aortic dissection or aneurysm is suspected. Emergent consultation with vascular surgery or interventional radiology is mandatory. Revascularization must occur within 4–6 hours of symptom onset to prevent irreversible ischemia. Treatment options include thrombectomy, embolectomy, angioplasty, thrombolysis, or bypass grafting. Complications include compartment syndrome, irreversible limb ischemia requiring amputation, rhabdomyolysis, renal failure, and electrolyte disturbances.
Atheroembolism is managed conservatively when tissue involvement is limited and renal function preserved. Treatment is supportive with wound care and analgesia. Vascular surgery referral within 12–24 hours is recommended, and evaluation to prevent further embolic events is essential. Amputation may be required for irreversibly necrotic tissue.
All patients with acute arterial insufficiency require hospital admission for evaluation and revascularization. Patients with chronic disease should be admitted if they develop rapidly progressive claudication or ischemic rest pain. Atheroembolism warrants admission if there is significant tissue involvement, infection, pain, or renal compromise. Stable patients with mild chronic disease or limited atheroembolism may be discharged with close follow-up.
Early recognition of acute limb ischemia is critical, as time to reperfusion determines limb salvage and survival.