- Published on
Emergency And Acute Medicine – Cystic Fibrosis
Foundational Overview
Cystic fibrosis is caused by a defect in the cystic fibrosis transmembrane conductance regulator (CFTR). CFTR functions as an ATP-regulated chloride channel that modulates chloride and sodium transport across epithelial cell surfaces. Dysfunction leads to abnormal electrolyte movement in exocrine glands and secretory epithelia. The result is thick, viscous secretions, impaired mucociliary clearance, recurrent pulmonary infections, and progressive obstructive lung disease. Exocrine pancreatic insufficiency causes malabsorption, while chronic sinus disease is common.
Cystic fibrosis occurs in approximately 1 in 3,600 live births in the White population, 1 in 29,000 in African American individuals, and 1 in 6,500 in Hispanic individuals. About 30% of cases are detected through newborn screening, and 75% are diagnosed within the first two years of life. Approximately 30,000 children and young adults in the United States live with cystic fibrosis. Median life expectancy in the U.S. is about 40 years, with 40% of patients older than 18 years. Roughly 10 million Americans are asymptomatic carriers. Sixteen percent of lung transplants in the U.S. are performed for cystic fibrosis–related lung disease.
Predisposing Factors
Cystic fibrosis is an autosomal recessive genetic disorder involving the CFTR gene on the long arm of chromosome 7. Numerous mutations exist, resulting in variable phenotypes. Classic disease is most commonly associated with homozygous ΔF508 mutations. Cystic fibrosis remains the most common lethal genetic disease in the United States.
Infectious Contributors And Pathogenesis
Patients are predisposed to chronic and recurrent pulmonary infections, often involving multidrug-resistant organisms. Common pathogens include methicillin-sensitive and methicillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa (with prevalence increasing with age and chronic infection in more than 70% of adults), Haemophilus influenzae, Stenotrophomonas maltophilia, and Achromobacter xylosoxidans.
Burkholderia cepacia occurs in approximately 3% of patients and is associated with rapid clinical deterioration. Nontuberculous mycobacteria, including Mycobacterium avium complex and Mycobacterium abscessus, and fungal pathogens such as Aspergillus are also encountered.
Clinical Manifestations
General findings include failure to thrive, recurrent respiratory infections, anasarca in infancy, and a characteristic salty taste of the skin.
Head and neck involvement includes nasal polyps, severe headaches from sinusitis, and recurrent otitis media.
Pulmonary features include persistent cough that progresses from dry to productive, recurrent bronchiolitis or pneumonitis in the first year of life, wheezing, hemoptysis, pneumonia, chronic bronchitis, bronchiectasis, respiratory distress, pneumothorax, and pneumomediastinum. Pulmonary complications are the most common cause of hospitalization.
Cardiac complications include congestive heart failure, cor pulmonale, and pulmonary hypertension.
Gastrointestinal manifestations include abdominal pain, meconium ileus, distal intestinal obstructive syndrome (DIOS, also called meconium ileus equivalent), gastroesophageal reflux, cholelithiasis, pancreatitis, pancreatic insufficiency, ileocecal intussusception, foul-smelling fatty stools, jaundice or cirrhosis, rectal prolapse, hematemesis, and small-intestinal bacterial overgrowth.
Musculoskeletal and systemic findings include bone pain, edema or joint effusions, decreased cortical bone thickness, and recurrent venous thrombosis. Cardiorespiratory failure is the leading cause of death.
Essential Diagnostic Evaluation
Initial confirmation relies on sweat chloride testing. DNA analysis is indicated if sweat testing is equivocal. Nasal potential difference testing is reserved for cases where DNA analysis is inconclusive.
Diagnostic Studies And Interpretation
The sweat chloride test is diagnostic when chloride concentration exceeds 60 mEq/L in the presence of classic symptoms. Stool studies may demonstrate decreased elastase, trypsin, or chymotrypsin, and increased fat on 72-hour fecal fat testing. Immunoreactive trypsin (IRT) screening identifies increased risk but may yield false positives or negatives.
DNA analysis detects approximately 90% of cystic fibrosis chromosomes and is positive when two abnormal CFTR genes are present. Genotyping alone cannot establish the diagnosis, as more than 1,300 CFTR mutations exist and modifying mutations may attenuate disease severity.
Laboratory evaluation may reveal thrombocytopenia, hyponatremic hypochloremic metabolic alkalosis, hyperglycemia or new-onset diabetes in adolescents and adults (with ketoacidosis being rare), and abnormal liver function tests or prolonged prothrombin time in the setting of liver disease or bleeding. Arterial blood gases may show hypoxemia and metabolic alkalosis. Sputum cultures often reveal chronic pseudomonal colonization.
Specialized studies include nasal potential difference testing, which is complex and time-consuming, and semen analysis demonstrating azoospermia in affected males.
Imaging findings on chest radiography include hyperaeration, peribronchial thickening, atelectasis, hilar lymphadenopathy, pneumothorax, pneumomediastinum, bronchiectasis, and blebs. Chest CT better defines bronchiectasis and bleb disease. Abdominal imaging is indicated for pain, vomiting, or distention to evaluate for DIOS or intussusception. Barium enema is used when intussusception is suspected. Routine sinus radiographs are of limited value, as they are almost always abnormal; CT imaging is required for operative planning.
Bronchoalveolar lavage may demonstrate neutrophilic inflammation but is unnecessary when pulmonary disease is clinically evident.
Conditions To Exclude
Respiratory alternatives include asthma, recurrent pneumonia, bronchiectasis from other causes, pertussis, immunodeficiency, foreign body aspiration, alpha-1 antitrypsin deficiency, and ciliary dyskinesia.
Gastrointestinal mimics include chronic diarrhea, gastroenteritis, and milk allergy.
Other causes of elevated sweat electrolytes include fucosidosis, glycogen storage disease type I, mucopolysaccharidoses, hypothyroidism, vasopressin-resistant diabetes insipidus, adrenal insufficiency, familial cholestasis or hypoparathyroidism, malnutrition, ectodermal dysplasia, atopic dermatitis, and prostaglandin E1 infusion.
Emergency And Acute Care Management
Prehospital considerations include transcutaneous pacing for unstable type II second-degree or third-degree heart block. Atropine should be avoided in type II second-degree block due to risk of progression to complete heart block.
Emergency department priorities focus on stabilization of airway, breathing, and circulation, with correction of fluid, electrolyte, glucose, and respiratory abnormalities. Bronchodilators and steroids are used for wheezing. Small pneumothoraces under 5–10% may be observed, while larger ones require thoracostomy. Early consultation with the patient’s cystic fibrosis specialist is essential.
Right-sided heart failure is treated with diuretics. Hemoptysis requires evaluation of coagulation status and transfusion as indicated. Ventilatory support may be necessary in severe respiratory failure.
DIOS often requires surgical intervention. Hematemesis is managed with packed red blood cells, correction of coagulopathy, and early endoscopic consultation. Intussusception is treated with air or barium enema, with surgery if unsuccessful. Rectal prolapse is manually reduced, with surgical consultation as needed.
Respiratory care includes aggressive pulmonary toilet, chest physiotherapy, mucus-thinning inhaled agents, and antibiotics tailored to culture and sensitivity results. Treatment regimens vary based on organism profile, including coverage for MSSA, MRSA, Pseudomonas aeruginosa, Burkholderia cepacia, and Haemophilus influenzae. Ciprofloxacin may replace aminoglycosides when organisms are sensitive.
Disease-specific therapies include CFTR modulators such as ivacaftor to improve protein function, nebulized hypertonic saline to restore airway surface liquid, and dornase alfa to reduce mucus viscosity. Adjunctive strategies include high-dose ibuprofen for anti-inflammatory effects, inhaled antibiotics, nutritional optimization, exercise programs, and consideration of lung transplantation in advanced disease.
Pharmacologic Therapy
Antibiotic regimens include aminoglycosides, antipseudomonal penicillins, cephalosporins, carbapenems, vancomycin, and trimethoprim–sulfamethoxazole, dosed carefully due to altered pharmacokinetics in undernourished patients. Close monitoring of drug levels, particularly with aminoglycosides, is essential.
Disposition And Follow-Up
Hospital admission is required for pulmonary exacerbations with significant decline from baseline, hypoxemia, resistant organisms, or failure of outpatient therapy, as well as pneumothorax, hemoptysis, hematemesis, intussusception, unexplained abdominal pain, bowel obstruction, or hyperglycemia.
Discharge requires close follow-up to review culture sensitivities and adjust therapy. Patients should avoid excessive heat exposure and may require oral salt supplementation during periods of heavy sweating.
Care Coordination And Long-Term Planning
All patients should be followed by a specialized cystic fibrosis pulmonary center. Acute exacerbations warrant early consultation. Long-term care requires a multidisciplinary team approach incorporating airway clearance, antibiotics, nutritional support, pancreatic enzyme replacement, and exercise programs.
Key Clinical Insights And Common Pitfalls
In cystic fibrosis patients with acute respiratory distress, pneumothorax must always be considered and promptly evaluated with chest imaging. In those presenting with abdominal pain or vomiting, distal intestinal obstructive syndrome and intussusception should remain high on the differential.
Foundational Overview
Cystic fibrosis is caused by a defect in the cystic fibrosis transmembrane conductance regulator (CFTR). CFTR functions as an ATP-regulated chloride channel that modulates chloride and sodium transport across epithelial cell surfaces. Dysfunction leads to abnormal electrolyte movement in exocrine glands and secretory epithelia. The result is thick, viscous secretions, impaired mucociliary clearance, recurrent pulmonary infections, and progressive obstructive lung disease. Exocrine pancreatic insufficiency causes malabsorption, while chronic sinus disease is common.
Cystic fibrosis occurs in approximately 1 in 3,600 live births in the White population, 1 in 29,000 in African American individuals, and 1 in 6,500 in Hispanic individuals. About 30% of cases are detected through newborn screening, and 75% are diagnosed within the first two years of life. Approximately 30,000 children and young adults in the United States live with cystic fibrosis. Median life expectancy in the U.S. is about 40 years, with 40% of patients older than 18 years. Roughly 10 million Americans are asymptomatic carriers. Sixteen percent of lung transplants in the U.S. are performed for cystic fibrosis–related lung disease.
Predisposing Factors
Cystic fibrosis is an autosomal recessive genetic disorder involving the CFTR gene on the long arm of chromosome 7. Numerous mutations exist, resulting in variable phenotypes. Classic disease is most commonly associated with homozygous ΔF508 mutations. Cystic fibrosis remains the most common lethal genetic disease in the United States.
Infectious Contributors And Pathogenesis
Patients are predisposed to chronic and recurrent pulmonary infections, often involving multidrug-resistant organisms. Common pathogens include methicillin-sensitive and methicillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa (with prevalence increasing with age and chronic infection in more than 70% of adults), Haemophilus influenzae, Stenotrophomonas maltophilia, and Achromobacter xylosoxidans.
Burkholderia cepacia occurs in approximately 3% of patients and is associated with rapid clinical deterioration. Nontuberculous mycobacteria, including Mycobacterium avium complex and Mycobacterium abscessus, and fungal pathogens such as Aspergillus are also encountered.
Clinical Manifestations
General findings include failure to thrive, recurrent respiratory infections, anasarca in infancy, and a characteristic salty taste of the skin.
Head and neck involvement includes nasal polyps, severe headaches from sinusitis, and recurrent otitis media.
Pulmonary features include persistent cough that progresses from dry to productive, recurrent bronchiolitis or pneumonitis in the first year of life, wheezing, hemoptysis, pneumonia, chronic bronchitis, bronchiectasis, respiratory distress, pneumothorax, and pneumomediastinum. Pulmonary complications are the most common cause of hospitalization.
Cardiac complications include congestive heart failure, cor pulmonale, and pulmonary hypertension.
Gastrointestinal manifestations include abdominal pain, meconium ileus, distal intestinal obstructive syndrome (DIOS, also called meconium ileus equivalent), gastroesophageal reflux, cholelithiasis, pancreatitis, pancreatic insufficiency, ileocecal intussusception, foul-smelling fatty stools, jaundice or cirrhosis, rectal prolapse, hematemesis, and small-intestinal bacterial overgrowth.
Musculoskeletal and systemic findings include bone pain, edema or joint effusions, decreased cortical bone thickness, and recurrent venous thrombosis. Cardiorespiratory failure is the leading cause of death.
Essential Diagnostic Evaluation
Initial confirmation relies on sweat chloride testing. DNA analysis is indicated if sweat testing is equivocal. Nasal potential difference testing is reserved for cases where DNA analysis is inconclusive.
Diagnostic Studies And Interpretation
The sweat chloride test is diagnostic when chloride concentration exceeds 60 mEq/L in the presence of classic symptoms. Stool studies may demonstrate decreased elastase, trypsin, or chymotrypsin, and increased fat on 72-hour fecal fat testing. Immunoreactive trypsin (IRT) screening identifies increased risk but may yield false positives or negatives.
DNA analysis detects approximately 90% of cystic fibrosis chromosomes and is positive when two abnormal CFTR genes are present. Genotyping alone cannot establish the diagnosis, as more than 1,300 CFTR mutations exist and modifying mutations may attenuate disease severity.
Laboratory evaluation may reveal thrombocytopenia, hyponatremic hypochloremic metabolic alkalosis, hyperglycemia or new-onset diabetes in adolescents and adults (with ketoacidosis being rare), and abnormal liver function tests or prolonged prothrombin time in the setting of liver disease or bleeding. Arterial blood gases may show hypoxemia and metabolic alkalosis. Sputum cultures often reveal chronic pseudomonal colonization.
Specialized studies include nasal potential difference testing, which is complex and time-consuming, and semen analysis demonstrating azoospermia in affected males.
Imaging findings on chest radiography include hyperaeration, peribronchial thickening, atelectasis, hilar lymphadenopathy, pneumothorax, pneumomediastinum, bronchiectasis, and blebs. Chest CT better defines bronchiectasis and bleb disease. Abdominal imaging is indicated for pain, vomiting, or distention to evaluate for DIOS or intussusception. Barium enema is used when intussusception is suspected. Routine sinus radiographs are of limited value, as they are almost always abnormal; CT imaging is required for operative planning.
Bronchoalveolar lavage may demonstrate neutrophilic inflammation but is unnecessary when pulmonary disease is clinically evident.
Conditions To Exclude
Respiratory alternatives include asthma, recurrent pneumonia, bronchiectasis from other causes, pertussis, immunodeficiency, foreign body aspiration, alpha-1 antitrypsin deficiency, and ciliary dyskinesia.
Gastrointestinal mimics include chronic diarrhea, gastroenteritis, and milk allergy.
Other causes of elevated sweat electrolytes include fucosidosis, glycogen storage disease type I, mucopolysaccharidoses, hypothyroidism, vasopressin-resistant diabetes insipidus, adrenal insufficiency, familial cholestasis or hypoparathyroidism, malnutrition, ectodermal dysplasia, atopic dermatitis, and prostaglandin E1 infusion.
Emergency And Acute Care Management
Prehospital considerations include transcutaneous pacing for unstable type II second-degree or third-degree heart block. Atropine should be avoided in type II second-degree block due to risk of progression to complete heart block.
Emergency department priorities focus on stabilization of airway, breathing, and circulation, with correction of fluid, electrolyte, glucose, and respiratory abnormalities. Bronchodilators and steroids are used for wheezing. Small pneumothoraces under 5–10% may be observed, while larger ones require thoracostomy. Early consultation with the patient’s cystic fibrosis specialist is essential.
Right-sided heart failure is treated with diuretics. Hemoptysis requires evaluation of coagulation status and transfusion as indicated. Ventilatory support may be necessary in severe respiratory failure.
DIOS often requires surgical intervention. Hematemesis is managed with packed red blood cells, correction of coagulopathy, and early endoscopic consultation. Intussusception is treated with air or barium enema, with surgery if unsuccessful. Rectal prolapse is manually reduced, with surgical consultation as needed.
Respiratory care includes aggressive pulmonary toilet, chest physiotherapy, mucus-thinning inhaled agents, and antibiotics tailored to culture and sensitivity results. Treatment regimens vary based on organism profile, including coverage for MSSA, MRSA, Pseudomonas aeruginosa, Burkholderia cepacia, and Haemophilus influenzae. Ciprofloxacin may replace aminoglycosides when organisms are sensitive.
Disease-specific therapies include CFTR modulators such as ivacaftor to improve protein function, nebulized hypertonic saline to restore airway surface liquid, and dornase alfa to reduce mucus viscosity. Adjunctive strategies include high-dose ibuprofen for anti-inflammatory effects, inhaled antibiotics, nutritional optimization, exercise programs, and consideration of lung transplantation in advanced disease.
Pharmacologic Therapy
Antibiotic regimens include aminoglycosides, antipseudomonal penicillins, cephalosporins, carbapenems, vancomycin, and trimethoprim–sulfamethoxazole, dosed carefully due to altered pharmacokinetics in undernourished patients. Close monitoring of drug levels, particularly with aminoglycosides, is essential.
Disposition And Follow-Up
Hospital admission is required for pulmonary exacerbations with significant decline from baseline, hypoxemia, resistant organisms, or failure of outpatient therapy, as well as pneumothorax, hemoptysis, hematemesis, intussusception, unexplained abdominal pain, bowel obstruction, or hyperglycemia.
Discharge requires close follow-up to review culture sensitivities and adjust therapy. Patients should avoid excessive heat exposure and may require oral salt supplementation during periods of heavy sweating.
Care Coordination And Long-Term Planning
All patients should be followed by a specialized cystic fibrosis pulmonary center. Acute exacerbations warrant early consultation. Long-term care requires a multidisciplinary team approach incorporating airway clearance, antibiotics, nutritional support, pancreatic enzyme replacement, and exercise programs.
Key Clinical Insights And Common Pitfalls
In cystic fibrosis patients with acute respiratory distress, pneumothorax must always be considered and promptly evaluated with chest imaging. In those presenting with abdominal pain or vomiting, distal intestinal obstructive syndrome and intussusception should remain high on the differential.

- Published on
Emergency And Acute Medicine – Cyanosis
Overview
Cyanosis is an abnormal bluish discoloration of the skin or mucous membranes caused by increased concentrations of deoxygenated hemoglobin or abnormal hemoglobin derivatives within capillary blood. Clinically significant levels include deoxygenated hemoglobin greater than 5 g/dL, methemoglobin greater than 1.5 g/dL, or sulfhemoglobin greater than 0.5 g/dL. The absolute amount of deoxygenated hemoglobin determines the blue coloration, not the oxyhemoglobin concentration. Cyanosis is more apparent in patients with polycythemia and may be difficult to detect in anemic patients. Skin thickness and pigmentation influence visibility. Cyanosis may be central, reflecting systemic hypoxemia or abnormal hemoglobin, or peripheral, reflecting increased oxygen extraction or impaired blood flow.
Pathophysiologic Types
Central cyanosis results from hypoxemia, right-to-left cardiac shunting, or abnormal hemoglobin species. Peripheral cyanosis occurs when tissues extract excessive oxygen due to hypoperfusion, vasoconstriction from cold exposure, or arterial or venous insufficiency. Acrocyanosis is a painless, symmetric bluish discoloration of distal extremities with an unclear underlying mechanism.
Causes
Central causes include impaired pulmonary function from hypoventilation, ventilation–perfusion mismatch, or diffusion defects; intracardiac or intrapulmonary shunts; high-altitude exposure; and abnormal hemoglobins. Peripheral causes include shock, cold exposure, arterial insufficiency, venous insufficiency, Raynaud phenomenon, and acrocyanosis. Abnormal hemoglobin states include congenital or acquired methemoglobinemia and sulfhemoglobinemia, often related to medications, chemicals, or genetic enzyme deficiencies.
Pediatric Considerations
In children, cyanosis may reflect cyanotic congenital heart disease such as tetralogy of Fallot, transposition of the great vessels, truncus arteriosus, pulmonary or tricuspid atresia, Ebstein anomaly, total anomalous pulmonary venous return, or duct-dependent lesions. Respiratory causes include upper and lower airway obstruction, bronchiolitis, pneumonia, pulmonary edema, or foreign body aspiration. Neurologic causes such as breath-holding spells should also be considered.
Clinical Presentation
Patients exhibit a bluish discoloration of skin or mucous membranes that typically blanches with pressure. Methemoglobinemia may produce chocolate-brown blood or slate-gray discoloration. History should establish onset, progression, associated symptoms such as dyspnea or altered mental status, medication use, and possible occupational or chemical exposures. Physical examination focuses on respiratory distress, hemodynamic stability, distribution of discoloration, cardiac and pulmonary findings, presence of clubbing, and peripheral perfusion.
Initial Assessment
Airway and ventilation assessment is the first priority. Hypoxemia from cardiac or pulmonary causes is most common and should be addressed immediately. Abnormal hemoglobin states should be considered when cyanosis persists despite adequate oxygenation.
Diagnostic Evaluation
Pulse oximetry may be misleading in abnormal hemoglobin states, hypoperfusion, or pigmented skin. Arterial blood gas analysis assesses oxygen tension and saturation; cyanosis with a normal PaO₂ suggests methemoglobinemia. Chocolate-colored blood supports this diagnosis, which should be confirmed by measuring methemoglobin levels. Laboratory studies include complete blood count and basic chemistries. Imaging such as chest radiography and targeted neck films helps evaluate pulmonary, cardiac, or airway pathology. Echocardiography is useful when shunt or structural heart disease is suspected.
Conditions To Differentiate
Noncyanotic causes of skin discoloration that do not blanch include drug-induced pigmentation, heavy metal deposition, metabolic disorders, tattoos, and rare conditions such as chromhidrosis.
Emergency Management
Prehospital and emergency care focuses on securing the airway, providing 100% oxygen via a nonrebreather mask, correcting ventilation problems, and supporting circulation. Bronchodilators, racemic epinephrine, diuretics, or prostaglandin E1 may be required depending on the underlying cause. Methylene blue is indicated for symptomatic methemoglobinemia with levels above 30%, except in patients with glucose-6-phosphate dehydrogenase deficiency.
Disposition
Most patients with cyanosis require hospital admission, and any instability mandates intensive care. Discharge may be considered only when a reversible cause has been identified, treated, and resolved, with stable oxygenation and close follow-up arranged.
Practical Insights And Common Diagnostic Errors
Always presume hypoxemia first and rapidly evaluate airway and breathing. Cyanosis that does not improve with high-flow oxygen or is associated with chocolate-colored blood should prompt evaluation for methemoglobinemia. Failure to recognize abnormal hemoglobin states is a frequent cause of delayed diagnosis.
Overview
Cyanosis is an abnormal bluish discoloration of the skin or mucous membranes caused by increased concentrations of deoxygenated hemoglobin or abnormal hemoglobin derivatives within capillary blood. Clinically significant levels include deoxygenated hemoglobin greater than 5 g/dL, methemoglobin greater than 1.5 g/dL, or sulfhemoglobin greater than 0.5 g/dL. The absolute amount of deoxygenated hemoglobin determines the blue coloration, not the oxyhemoglobin concentration. Cyanosis is more apparent in patients with polycythemia and may be difficult to detect in anemic patients. Skin thickness and pigmentation influence visibility. Cyanosis may be central, reflecting systemic hypoxemia or abnormal hemoglobin, or peripheral, reflecting increased oxygen extraction or impaired blood flow.
Pathophysiologic Types
Central cyanosis results from hypoxemia, right-to-left cardiac shunting, or abnormal hemoglobin species. Peripheral cyanosis occurs when tissues extract excessive oxygen due to hypoperfusion, vasoconstriction from cold exposure, or arterial or venous insufficiency. Acrocyanosis is a painless, symmetric bluish discoloration of distal extremities with an unclear underlying mechanism.
Causes
Central causes include impaired pulmonary function from hypoventilation, ventilation–perfusion mismatch, or diffusion defects; intracardiac or intrapulmonary shunts; high-altitude exposure; and abnormal hemoglobins. Peripheral causes include shock, cold exposure, arterial insufficiency, venous insufficiency, Raynaud phenomenon, and acrocyanosis. Abnormal hemoglobin states include congenital or acquired methemoglobinemia and sulfhemoglobinemia, often related to medications, chemicals, or genetic enzyme deficiencies.
Pediatric Considerations
In children, cyanosis may reflect cyanotic congenital heart disease such as tetralogy of Fallot, transposition of the great vessels, truncus arteriosus, pulmonary or tricuspid atresia, Ebstein anomaly, total anomalous pulmonary venous return, or duct-dependent lesions. Respiratory causes include upper and lower airway obstruction, bronchiolitis, pneumonia, pulmonary edema, or foreign body aspiration. Neurologic causes such as breath-holding spells should also be considered.
Clinical Presentation
Patients exhibit a bluish discoloration of skin or mucous membranes that typically blanches with pressure. Methemoglobinemia may produce chocolate-brown blood or slate-gray discoloration. History should establish onset, progression, associated symptoms such as dyspnea or altered mental status, medication use, and possible occupational or chemical exposures. Physical examination focuses on respiratory distress, hemodynamic stability, distribution of discoloration, cardiac and pulmonary findings, presence of clubbing, and peripheral perfusion.
Initial Assessment
Airway and ventilation assessment is the first priority. Hypoxemia from cardiac or pulmonary causes is most common and should be addressed immediately. Abnormal hemoglobin states should be considered when cyanosis persists despite adequate oxygenation.
Diagnostic Evaluation
Pulse oximetry may be misleading in abnormal hemoglobin states, hypoperfusion, or pigmented skin. Arterial blood gas analysis assesses oxygen tension and saturation; cyanosis with a normal PaO₂ suggests methemoglobinemia. Chocolate-colored blood supports this diagnosis, which should be confirmed by measuring methemoglobin levels. Laboratory studies include complete blood count and basic chemistries. Imaging such as chest radiography and targeted neck films helps evaluate pulmonary, cardiac, or airway pathology. Echocardiography is useful when shunt or structural heart disease is suspected.
Conditions To Differentiate
Noncyanotic causes of skin discoloration that do not blanch include drug-induced pigmentation, heavy metal deposition, metabolic disorders, tattoos, and rare conditions such as chromhidrosis.
Emergency Management
Prehospital and emergency care focuses on securing the airway, providing 100% oxygen via a nonrebreather mask, correcting ventilation problems, and supporting circulation. Bronchodilators, racemic epinephrine, diuretics, or prostaglandin E1 may be required depending on the underlying cause. Methylene blue is indicated for symptomatic methemoglobinemia with levels above 30%, except in patients with glucose-6-phosphate dehydrogenase deficiency.
Disposition
Most patients with cyanosis require hospital admission, and any instability mandates intensive care. Discharge may be considered only when a reversible cause has been identified, treated, and resolved, with stable oxygenation and close follow-up arranged.
Practical Insights And Common Diagnostic Errors
Always presume hypoxemia first and rapidly evaluate airway and breathing. Cyanosis that does not improve with high-flow oxygen or is associated with chocolate-colored blood should prompt evaluation for methemoglobinemia. Failure to recognize abnormal hemoglobin states is a frequent cause of delayed diagnosis.


- Published on
Emergency And Acute Medicine – Cyanide Poisoning
Overview
Cyanide toxicity occurs through inhalation or gastrointestinal absorption. Cyanide is an intracellular toxin that disrupts aerobic metabolism by inhibiting oxidative phosphorylation, resulting in impaired oxygen utilization and reduced ATP production. Detoxification primarily occurs via the hepatic mitochondrial enzyme rhodanese, which combines cyanide with sulfur in an irreversible reaction to form the less toxic, water-soluble thiocyanate. Cyanide can also bind hemoglobin to form reversible cyanhemoglobin or bind hydroxocobalamin to form nontoxic cyanocobalamin. Effective detoxification depends on adequate sulfur availability, particularly thiosulfate.
Causes And Sources
Cyanide exposure most commonly occurs during fires as a combustion by-product of natural and synthetic materials. Industrial sources include metal plating, microchip and plastic manufacturing, chemical synthesis, pesticides, and solvents such as artificial nail remover and metal polishes. Cyanide may also be produced during nitroprusside metabolism and by certain bacterial infections. Dietary sources include amygdalin-containing plants such as apricot pits, peach pits, apple seeds, pear seeds, and cassava. Jewelry making is another recognized exposure risk.
Clinical Features
The heart and brain are the most sensitive organs and are typically affected first. Neurologic manifestations include headache, confusion, syncope, seizures, and coma. Cardiovascular findings include dyspnea, chest pain, rapid progression to cardiorespiratory collapse, and death. Gastrointestinal symptoms such as nausea and vomiting may occur. Oral exposure can be caustic, with as little as 50 mg causing death. Inhalational exposure to 50 ppm may cause anxiety, palpitations, dyspnea, and headache, while concentrations of 100–135 ppm can be lethal in less than one hour.
Initial Evaluation
A history suggestive of smoke inhalation, industrial exposure, or intentional ingestion should raise suspicion. Classic findings such as the odor of bitter almonds or bright red retinal vessels are often absent. Key clinical clues include abrupt onset or rapid deterioration, severe lactic acidosis, and elevated venous oxygen saturation due to impaired cellular oxygen utilization, resulting in arterialized venous blood gases.
Diagnostic Studies
Laboratory evaluation typically includes complete blood count, metabolic panel, liver profile, creatine phosphokinase, carboxyhemoglobin, and methemoglobin levels. Cyanide levels are usually send-out tests and not available in real time; levels above 0.5–1 mg/L are toxic, and levels of 2.5–3 mg/L are often fatal. Blood gas analysis may show elevated mixed venous oxygen saturation, reduced arteriovenous oxygen difference, and markedly elevated lactate levels greater than 8 mmol/L, which serve as a useful surrogate marker when exposure history is consistent. Chest radiography may assist in evaluating concurrent inhalation injury.
Conditions To Differentiate
The differential diagnosis includes carbon monoxide poisoning, hydrogen sulfide exposure, methemoglobinemia, sulfhemoglobinemia, inert gas asphyxiation, and other causes of high anion gap metabolic acidosis.
Prehospital Management
Immediate removal from the source of exposure is critical, while preventing secondary contamination of rescuers. Contaminated clothing should be removed and bagged, and liquid exposures require thorough washing with soap and water. Vapor exposures may resolve with simple removal from the environment.
Emergency Stabilization
Initial management follows standard airway, breathing, and circulation principles. Administer 100% oxygen regardless of measured oxygen tension, as it acts synergistically with antidotes. Gastric lavage and activated charcoal may be considered for recent oral ingestion if no contraindications exist. Dermal exposures require standard decontamination measures.
Definitive Treatment
Hydroxocobalamin is the preferred first-line antidote for patients with significant toxicity, including persistent high anion gap metabolic acidosis, hyperlactatemia, seizures, syncope, dysrhythmias, or hypotension. It binds cyanide to form cyanocobalamin, which is renally excreted. Advantages include the absence of methemoglobinemia and hypotension. Limitations include cost, drug incompatibilities within IV lines, and interference with certain laboratory assays.
An alternative is the traditional cyanide antidote kit, which includes amyl nitrite, sodium nitrite, and sodium thiosulfate. Nitrites induce methemoglobinemia to sequester cyanide away from mitochondria, while sodium thiosulfate enhances enzymatic detoxification via rhodanese. Nitrites should not be used empirically and require caution due to the risk of excessive methemoglobinemia and hypotension. Hyperbaric oxygen therapy may be considered as adjunctive treatment to maximize tissue oxygenation.
Medication Summary
First-line therapy is hydroxocobalamin administered intravenously at weight-based dosing, with repeat dosing if necessary. Activated charcoal may be used for recent ingestions. Second-line therapy involves the cyanide antidote kit, including carefully dosed nitrites and sodium thiosulfate. Special dosing considerations apply in pediatric patients, pregnancy, and those with hepatic or renal impairment.
Disposition And Follow-Up
All symptomatic patients require intensive care unit admission. Asymptomatic patients may be discharged after at least four hours of observation if no symptoms develop, as survival beyond this period is usually associated with full recovery. Psychiatric evaluation is indicated for intentional exposures.
Key Clinical Insights And Common Errors
In patients presenting with hypotension, seizures, altered mental status, severe lactic acidosis, and high anion gap metabolic acidosis, cyanide poisoning should be strongly considered and treated empirically. Serum lactate is a valuable surrogate marker when exposure history is suggestive. Victims of smoke inhalation may have combined cyanide toxicity, carbon monoxide poisoning, and methemoglobinemia. When carbon monoxide levels are markedly elevated, concomitant cyanide exposure should be suspected. To avoid worsening oxygen delivery, initial treatment should prioritize hydroxocobalamin or sodium thiosulfate without nitrites when methemoglobinemia would be harmful.
Overview
Cyanide toxicity occurs through inhalation or gastrointestinal absorption. Cyanide is an intracellular toxin that disrupts aerobic metabolism by inhibiting oxidative phosphorylation, resulting in impaired oxygen utilization and reduced ATP production. Detoxification primarily occurs via the hepatic mitochondrial enzyme rhodanese, which combines cyanide with sulfur in an irreversible reaction to form the less toxic, water-soluble thiocyanate. Cyanide can also bind hemoglobin to form reversible cyanhemoglobin or bind hydroxocobalamin to form nontoxic cyanocobalamin. Effective detoxification depends on adequate sulfur availability, particularly thiosulfate.
Causes And Sources
Cyanide exposure most commonly occurs during fires as a combustion by-product of natural and synthetic materials. Industrial sources include metal plating, microchip and plastic manufacturing, chemical synthesis, pesticides, and solvents such as artificial nail remover and metal polishes. Cyanide may also be produced during nitroprusside metabolism and by certain bacterial infections. Dietary sources include amygdalin-containing plants such as apricot pits, peach pits, apple seeds, pear seeds, and cassava. Jewelry making is another recognized exposure risk.
Clinical Features
The heart and brain are the most sensitive organs and are typically affected first. Neurologic manifestations include headache, confusion, syncope, seizures, and coma. Cardiovascular findings include dyspnea, chest pain, rapid progression to cardiorespiratory collapse, and death. Gastrointestinal symptoms such as nausea and vomiting may occur. Oral exposure can be caustic, with as little as 50 mg causing death. Inhalational exposure to 50 ppm may cause anxiety, palpitations, dyspnea, and headache, while concentrations of 100–135 ppm can be lethal in less than one hour.
Initial Evaluation
A history suggestive of smoke inhalation, industrial exposure, or intentional ingestion should raise suspicion. Classic findings such as the odor of bitter almonds or bright red retinal vessels are often absent. Key clinical clues include abrupt onset or rapid deterioration, severe lactic acidosis, and elevated venous oxygen saturation due to impaired cellular oxygen utilization, resulting in arterialized venous blood gases.
Diagnostic Studies
Laboratory evaluation typically includes complete blood count, metabolic panel, liver profile, creatine phosphokinase, carboxyhemoglobin, and methemoglobin levels. Cyanide levels are usually send-out tests and not available in real time; levels above 0.5–1 mg/L are toxic, and levels of 2.5–3 mg/L are often fatal. Blood gas analysis may show elevated mixed venous oxygen saturation, reduced arteriovenous oxygen difference, and markedly elevated lactate levels greater than 8 mmol/L, which serve as a useful surrogate marker when exposure history is consistent. Chest radiography may assist in evaluating concurrent inhalation injury.
Conditions To Differentiate
The differential diagnosis includes carbon monoxide poisoning, hydrogen sulfide exposure, methemoglobinemia, sulfhemoglobinemia, inert gas asphyxiation, and other causes of high anion gap metabolic acidosis.
Prehospital Management
Immediate removal from the source of exposure is critical, while preventing secondary contamination of rescuers. Contaminated clothing should be removed and bagged, and liquid exposures require thorough washing with soap and water. Vapor exposures may resolve with simple removal from the environment.
Emergency Stabilization
Initial management follows standard airway, breathing, and circulation principles. Administer 100% oxygen regardless of measured oxygen tension, as it acts synergistically with antidotes. Gastric lavage and activated charcoal may be considered for recent oral ingestion if no contraindications exist. Dermal exposures require standard decontamination measures.
Definitive Treatment
Hydroxocobalamin is the preferred first-line antidote for patients with significant toxicity, including persistent high anion gap metabolic acidosis, hyperlactatemia, seizures, syncope, dysrhythmias, or hypotension. It binds cyanide to form cyanocobalamin, which is renally excreted. Advantages include the absence of methemoglobinemia and hypotension. Limitations include cost, drug incompatibilities within IV lines, and interference with certain laboratory assays.
An alternative is the traditional cyanide antidote kit, which includes amyl nitrite, sodium nitrite, and sodium thiosulfate. Nitrites induce methemoglobinemia to sequester cyanide away from mitochondria, while sodium thiosulfate enhances enzymatic detoxification via rhodanese. Nitrites should not be used empirically and require caution due to the risk of excessive methemoglobinemia and hypotension. Hyperbaric oxygen therapy may be considered as adjunctive treatment to maximize tissue oxygenation.
Medication Summary
First-line therapy is hydroxocobalamin administered intravenously at weight-based dosing, with repeat dosing if necessary. Activated charcoal may be used for recent ingestions. Second-line therapy involves the cyanide antidote kit, including carefully dosed nitrites and sodium thiosulfate. Special dosing considerations apply in pediatric patients, pregnancy, and those with hepatic or renal impairment.
Disposition And Follow-Up
All symptomatic patients require intensive care unit admission. Asymptomatic patients may be discharged after at least four hours of observation if no symptoms develop, as survival beyond this period is usually associated with full recovery. Psychiatric evaluation is indicated for intentional exposures.
Key Clinical Insights And Common Errors
In patients presenting with hypotension, seizures, altered mental status, severe lactic acidosis, and high anion gap metabolic acidosis, cyanide poisoning should be strongly considered and treated empirically. Serum lactate is a valuable surrogate marker when exposure history is suggestive. Victims of smoke inhalation may have combined cyanide toxicity, carbon monoxide poisoning, and methemoglobinemia. When carbon monoxide levels are markedly elevated, concomitant cyanide exposure should be suspected. To avoid worsening oxygen delivery, initial treatment should prioritize hydroxocobalamin or sodium thiosulfate without nitrites when methemoglobinemia would be harmful.

- Published on
Emergency And Acute Medicine – Cushing Syndrome
Overview
Cushing disease refers specifically to excess adrenocorticotropic hormone (ACTH) production from a pituitary adenoma. Cushing syndrome describes the clinical state resulting from prolonged exposure to excessive glucocorticoids, regardless of the source.
Predisposing Factors
Genetic associations include multiple endocrine neoplasia type I and Carney complex, which is characterized by pigmented lentigines, atrial myxomas, and germ-cell tumors associated with Cushing disease.
Underlying Causes
The most common cause is exogenous glucocorticoid administration, whether therapeutic or surreptitious. Endogenous causes include ACTH-secreting pituitary adenomas, adrenal cortisol overproduction from adenoma, carcinoma, or micronodular disease, and ectopic ACTH production. Tumors associated with ectopic ACTH secretion include small cell lung carcinoma (most common), uterine cervical carcinoma, pancreatic islet cell tumors associated with MEN I, medullary thyroid carcinoma, pheochromocytoma, ganglioneuroma, melanoma, prostate carcinoma, and carcinoid tumors arising from the lung, pancreas, gastrointestinal tract, thymus, or ovary.
Clinical Recognition
The most critical emergency consideration is recognizing the risk of addisonian (adrenal) crisis during periods of physiologic stress. While Cushing syndrome itself is not usually an emergency diagnosis, early identification in the emergency setting may prevent significant morbidity and mortality.
In children, suspicion should be raised when obesity progresses in the absence of normal linear growth. During pregnancy, Cushing syndrome is rare but has been associated with severe preeclampsia and HELLP syndrome.
History And Physical Findings
Patients may have a prior diagnosis of Cushing disease or a history of corticosteroid use. Changes in weight, facial appearance, hirsutism, or psychiatric symptoms are important historical clues.
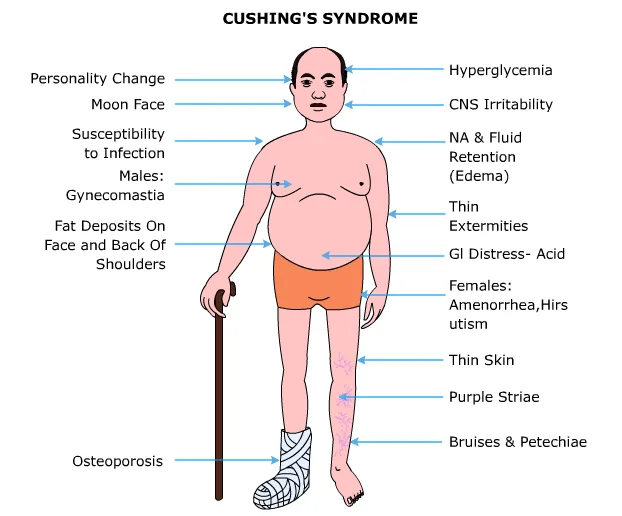
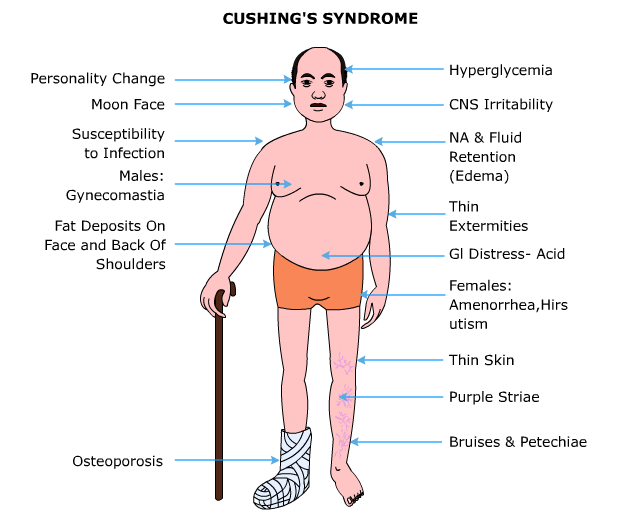
On examination, characteristic findings include moon facies, a dorsocervical fat pad (buffalo hump), central obesity with thin extremities, and supraclavicular fat deposition. These features are particularly concerning in stressed patients because of the risk of adrenal crisis.
Cardiovascular manifestations include uncontrolled hypertension. Neurologic findings may include stroke, pseudotumor cerebri (especially with exogenous steroid use), or spinal lipomatosis causing cord or nerve root compression. Gastrointestinal complications include peptic ulcer disease, gastrointestinal hemorrhage, pancreatitis, and fatty liver. Psychiatric manifestations are common and include mood disorders, depression, memory impairment, euphoria, and toxic psychosis.
Musculoskeletal findings include proximal muscle weakness, pathologic fractures, osteoporosis, and avascular necrosis of the humeral or femoral heads. Endocrine effects include glucose intolerance, hyperlipidemia, amenorrhea, hirsutism, or male-pattern balding in females. Hematologic changes include neutrophilia with lymphopenia and eosinopenia, increasing susceptibility to opportunistic infections. Ophthalmologic complications include cataracts and glaucoma, particularly with exogenous steroid use. Dermatologic features include wide purple striae, hyperpigmentation of the buccal mucosa due to excess ACTH, facial plethora, thin skin, poor wound healing, easy bruising, acne, and hyperhidrosis.
Essential Emergency Evaluation
Definitive diagnosis cannot be established in the emergency department. The priority is identifying patients at risk for addisonian crisis and managing concurrent life-threatening conditions such as myocardial infarction, stroke, sepsis, pathologic fractures, uncontrolled diabetes, or psychiatric emergencies requiring admission.
Diagnostic Studies
Laboratory evaluation may reveal hypokalemia with metabolic alkalosis, diminished glucose tolerance, overt diabetes, glycosuria, leukocytosis, and eosinopenia. Electrocardiography is useful to evaluate for myocardial ischemia, and chest radiography may identify tumors producing ectopic ACTH. Plain radiographs may be indicated if pathologic fractures are suspected and may show delayed bone age.
Definitive outpatient testing includes pituitary MRI, adrenal CT imaging, and dexamethasone suppression testing. Low-dose dexamethasone testing is used as a screening tool, though false positives are common. High-dose dexamethasone suppression testing may be required to confirm endogenous Cushing syndrome.
Alternative Diagnoses To Consider
Conditions that may mimic Cushing syndrome include alcohol-induced pseudo-Cushing syndrome, obesity, psychiatric disorders such as depression or panic disorder, and physiologic states including chronic stress, late pregnancy, and chronic strenuous exercise.
Emergency Management
Patients with iatrogenic Cushing syndrome may develop acute addisonian crisis during stress. These patients can also exhibit severe behavioral disturbances. The leading causes of death in untreated Cushing syndrome are infection, stroke, and myocardial infarction.
Initial management focuses on preventing adrenal crisis and treating associated complications. This includes intravenous fluids, glucose control, blood pressure management, appropriate cultures and antibiotics for suspected infection, and prompt treatment of cardiovascular or neurologic emergencies. Stress-dose steroids with hydrocortisone should be administered in patients with suspected adrenal crisis.
Medications that reduce cortisol production are rarely initiated in the emergency setting and should only be started under endocrinology guidance in patients with severe symptoms awaiting definitive therapy.
Definitive Therapy
Management depends on etiology. Exogenous steroid exposure requires gradual tapering when feasible, along with calcium, vitamin D, and estrogen supplementation if appropriate. Pituitary-dependent disease is treated with transsphenoidal surgery, with radiation reserved for refractory cases. Adrenal tumors require surgical resection, with medical therapy for unresectable metastatic disease. Ectopic ACTH-producing tumors are treated with surgical resection when possible and medical therapy otherwise.
Medications
Hydrocortisone is indicated only in adrenal crisis and is given intravenously. Additional agents such as ketoconazole, metyrapone, aminoglutethimide, mifepristone, mitotane, cyproheptadine, bromocriptine, pasireotide, or spironolactone may be used for symptomatic control under specialist supervision.
Disposition And Follow-Up
Hospital admission is required for patients with complications such as myocardial infarction, stroke, sepsis, pathologic fracture, uncontrolled diabetes, psychiatric emergencies, or impending adrenal crisis. Stable patients without these features may be discharged with close follow-up.
Referral And Long-Term Care
All patients with suspected Cushing syndrome require referral for definitive evaluation. Conditions secondary to hypercortisolism should be addressed concurrently.
Practical Insights And Common Pitfalls
Maintain a high index of suspicion in physiologically stressed patients with characteristic body habitus, especially those with supraclavicular fat pads. Early recognition is essential to prevent addisonian crisis and associated morbidity.
Overview
Cushing disease refers specifically to excess adrenocorticotropic hormone (ACTH) production from a pituitary adenoma. Cushing syndrome describes the clinical state resulting from prolonged exposure to excessive glucocorticoids, regardless of the source.
Predisposing Factors
Genetic associations include multiple endocrine neoplasia type I and Carney complex, which is characterized by pigmented lentigines, atrial myxomas, and germ-cell tumors associated with Cushing disease.
Underlying Causes
The most common cause is exogenous glucocorticoid administration, whether therapeutic or surreptitious. Endogenous causes include ACTH-secreting pituitary adenomas, adrenal cortisol overproduction from adenoma, carcinoma, or micronodular disease, and ectopic ACTH production. Tumors associated with ectopic ACTH secretion include small cell lung carcinoma (most common), uterine cervical carcinoma, pancreatic islet cell tumors associated with MEN I, medullary thyroid carcinoma, pheochromocytoma, ganglioneuroma, melanoma, prostate carcinoma, and carcinoid tumors arising from the lung, pancreas, gastrointestinal tract, thymus, or ovary.
Clinical Recognition
The most critical emergency consideration is recognizing the risk of addisonian (adrenal) crisis during periods of physiologic stress. While Cushing syndrome itself is not usually an emergency diagnosis, early identification in the emergency setting may prevent significant morbidity and mortality.
In children, suspicion should be raised when obesity progresses in the absence of normal linear growth. During pregnancy, Cushing syndrome is rare but has been associated with severe preeclampsia and HELLP syndrome.
History And Physical Findings
Patients may have a prior diagnosis of Cushing disease or a history of corticosteroid use. Changes in weight, facial appearance, hirsutism, or psychiatric symptoms are important historical clues.
On examination, characteristic findings include moon facies, a dorsocervical fat pad (buffalo hump), central obesity with thin extremities, and supraclavicular fat deposition. These features are particularly concerning in stressed patients because of the risk of adrenal crisis.
Cardiovascular manifestations include uncontrolled hypertension. Neurologic findings may include stroke, pseudotumor cerebri (especially with exogenous steroid use), or spinal lipomatosis causing cord or nerve root compression. Gastrointestinal complications include peptic ulcer disease, gastrointestinal hemorrhage, pancreatitis, and fatty liver. Psychiatric manifestations are common and include mood disorders, depression, memory impairment, euphoria, and toxic psychosis.
Musculoskeletal findings include proximal muscle weakness, pathologic fractures, osteoporosis, and avascular necrosis of the humeral or femoral heads. Endocrine effects include glucose intolerance, hyperlipidemia, amenorrhea, hirsutism, or male-pattern balding in females. Hematologic changes include neutrophilia with lymphopenia and eosinopenia, increasing susceptibility to opportunistic infections. Ophthalmologic complications include cataracts and glaucoma, particularly with exogenous steroid use. Dermatologic features include wide purple striae, hyperpigmentation of the buccal mucosa due to excess ACTH, facial plethora, thin skin, poor wound healing, easy bruising, acne, and hyperhidrosis.
Essential Emergency Evaluation
Definitive diagnosis cannot be established in the emergency department. The priority is identifying patients at risk for addisonian crisis and managing concurrent life-threatening conditions such as myocardial infarction, stroke, sepsis, pathologic fractures, uncontrolled diabetes, or psychiatric emergencies requiring admission.
Diagnostic Studies
Laboratory evaluation may reveal hypokalemia with metabolic alkalosis, diminished glucose tolerance, overt diabetes, glycosuria, leukocytosis, and eosinopenia. Electrocardiography is useful to evaluate for myocardial ischemia, and chest radiography may identify tumors producing ectopic ACTH. Plain radiographs may be indicated if pathologic fractures are suspected and may show delayed bone age.
Definitive outpatient testing includes pituitary MRI, adrenal CT imaging, and dexamethasone suppression testing. Low-dose dexamethasone testing is used as a screening tool, though false positives are common. High-dose dexamethasone suppression testing may be required to confirm endogenous Cushing syndrome.
Alternative Diagnoses To Consider
Conditions that may mimic Cushing syndrome include alcohol-induced pseudo-Cushing syndrome, obesity, psychiatric disorders such as depression or panic disorder, and physiologic states including chronic stress, late pregnancy, and chronic strenuous exercise.
Emergency Management
Patients with iatrogenic Cushing syndrome may develop acute addisonian crisis during stress. These patients can also exhibit severe behavioral disturbances. The leading causes of death in untreated Cushing syndrome are infection, stroke, and myocardial infarction.
Initial management focuses on preventing adrenal crisis and treating associated complications. This includes intravenous fluids, glucose control, blood pressure management, appropriate cultures and antibiotics for suspected infection, and prompt treatment of cardiovascular or neurologic emergencies. Stress-dose steroids with hydrocortisone should be administered in patients with suspected adrenal crisis.
Medications that reduce cortisol production are rarely initiated in the emergency setting and should only be started under endocrinology guidance in patients with severe symptoms awaiting definitive therapy.
Definitive Therapy
Management depends on etiology. Exogenous steroid exposure requires gradual tapering when feasible, along with calcium, vitamin D, and estrogen supplementation if appropriate. Pituitary-dependent disease is treated with transsphenoidal surgery, with radiation reserved for refractory cases. Adrenal tumors require surgical resection, with medical therapy for unresectable metastatic disease. Ectopic ACTH-producing tumors are treated with surgical resection when possible and medical therapy otherwise.
Medications
Hydrocortisone is indicated only in adrenal crisis and is given intravenously. Additional agents such as ketoconazole, metyrapone, aminoglutethimide, mifepristone, mitotane, cyproheptadine, bromocriptine, pasireotide, or spironolactone may be used for symptomatic control under specialist supervision.
Disposition And Follow-Up
Hospital admission is required for patients with complications such as myocardial infarction, stroke, sepsis, pathologic fracture, uncontrolled diabetes, psychiatric emergencies, or impending adrenal crisis. Stable patients without these features may be discharged with close follow-up.
Referral And Long-Term Care
All patients with suspected Cushing syndrome require referral for definitive evaluation. Conditions secondary to hypercortisolism should be addressed concurrently.
Practical Insights And Common Pitfalls
Maintain a high index of suspicion in physiologically stressed patients with characteristic body habitus, especially those with supraclavicular fat pads. Early recognition is essential to prevent addisonian crisis and associated morbidity.
- Published on
Emergency And Acute Medicine – Croup
Description
Croup is a viral infection of the upper respiratory tract that most commonly affects children between 6 months and 3 years of age. It typically presents as laryngotracheitis or laryngotracheobronchitis with inspiratory stridor caused by extrathoracic airway obstruction. Expiratory wheezing suggests lower airway involvement. The disease results from inflammatory edema of the subglottic region, the narrowest portion of the pediatric airway, and may progress to respiratory failure in severe cases.
Etiology
The most common causative organisms are parainfluenza virus types 1, 2, and 3. Other causes include human coronavirus NL63, influenza A and B, adenovirus, respiratory syncytial virus, measles, Mycoplasma pneumoniae, and herpes simplex virus.
Clinical Presentation
Children usually develop a nonspecific upper respiratory prodrome with or without fever. Important historical features include duration of illness, prior tracheal intubation, risk of foreign body aspiration, previous episodes of croup, history of wheezing, and immunization status, particularly against Haemophilus influenzae type b, diphtheria, pertussis, tetanus, and influenza.
On examination, children are often not toxic appearing and typically prefer to sit upright. Cyanosis is uncommon and suggests severe disease when present. Clinicians should assess the quality of cry or voice, mental status, hydration, presence of drooling or trismus, neck mobility, stridor at rest, and work of breathing.
Severity can be graded using the Westley croup score, which incorporates stridor, retractions, air entry, cyanosis, and level of consciousness.
Diagnostic Evaluation
Continuous pulse oximetry is recommended. Routine laboratory testing is not indicated. Imaging is generally unnecessary but, when obtained for atypical presentations, anteroposterior and lateral neck radiographs may show the classic “steeple sign” reflecting subglottic narrowing. Imaging should never delay airway management in patients with suspected epiglottitis or bacterial tracheitis, and children must be closely monitored if imaging is performed.
Differential Diagnosis
Infectious causes include bacterial tracheitis, epiglottitis, retropharyngeal or parapharyngeal abscess, peritonsillar abscess, and diphtheria. Noninfectious causes include foreign body aspiration, angioedema, congenital airway abnormalities such as laryngomalacia or tracheomalacia, acquired subglottic stenosis, vocal cord paralysis, airway burns, hemangioma, laryngeal papillomatosis, and vocal cord dysfunction in adolescents.
Initial Management
Children should be allowed to maintain their position of comfort, and interventions that may increase distress, such as IV access or intramuscular injections, should be deferred when possible. In cases of severe respiratory distress, immediate nebulized epinephrine should be administered.
Emergency Department Management
Nebulized racemic epinephrine or L-epinephrine is indicated for stridor at rest or significant respiratory distress and is effective in reducing airway edema. Supplemental oxygen may be provided via blow-by if hypoxia is suspected. Dexamethasone significantly improves outcomes by reducing the need for intubation, hospital admission, and return visits, and is effective even in mild cases. If there is an incomplete response to epinephrine, heliox may be considered to reduce work of breathing.
For patients with impending or established respiratory failure, tracheal intubation should be performed by the most experienced provider available using an uncuffed endotracheal tube 0.5–1 mm smaller than standard size. If epiglottitis or foreign body aspiration is suspected, airway management should ideally occur in the operating room with surgical backup available.
Medications
Racemic epinephrine 2.25% is administered as 0.25–0.5 mL nebulized in normal saline. L-epinephrine 1:1,000 may be given as 5 mL nebulized. Dexamethasone is given as a single dose of 0.6 mg/kg, up to a maximum of 10 mg, via oral, intravenous, or intramuscular routes. Heliox may be administered as a 70:30 helium–oxygen mixture. Antibiotics are not indicated.
Disposition And Follow-Up
Hospital admission is recommended for young infants, children with pre-existing airway disease, persistent or recurrent stridor at rest despite treatment, or those requiring repeated epinephrine treatments. Pediatric intensive care admission is indicated for severe obstruction, frequent need for epinephrine or heliox, or need for intubation.
Children may be discharged if they have normal oxygenation on room air, no stridor at rest after observation for at least 2–3 hours, and reliable caregivers with access to follow-up care.
Referral Considerations
Evaluation by specialists is warranted for children with suspected anatomic airway abnormalities, recurrent episodes, prior intubation, or infants younger than one year with unexplained stridor.
Follow-Up Guidance
Most children with uncomplicated croup do not require routine follow-up. Caregivers should be instructed to seek medical attention if stridor persists, worsens, or recurs.
Key Teaching Points And Common Errors
Stridor in young infants warrants careful evaluation due to a higher likelihood of congenital airway abnormalities. Early epiglottitis or bacterial tracheitis may closely mimic croup and should be considered when symptoms are atypical or severe.
Description
Croup is a viral infection of the upper respiratory tract that most commonly affects children between 6 months and 3 years of age. It typically presents as laryngotracheitis or laryngotracheobronchitis with inspiratory stridor caused by extrathoracic airway obstruction. Expiratory wheezing suggests lower airway involvement. The disease results from inflammatory edema of the subglottic region, the narrowest portion of the pediatric airway, and may progress to respiratory failure in severe cases.
Etiology
The most common causative organisms are parainfluenza virus types 1, 2, and 3. Other causes include human coronavirus NL63, influenza A and B, adenovirus, respiratory syncytial virus, measles, Mycoplasma pneumoniae, and herpes simplex virus.
Clinical Presentation
Children usually develop a nonspecific upper respiratory prodrome with or without fever. Important historical features include duration of illness, prior tracheal intubation, risk of foreign body aspiration, previous episodes of croup, history of wheezing, and immunization status, particularly against Haemophilus influenzae type b, diphtheria, pertussis, tetanus, and influenza.
On examination, children are often not toxic appearing and typically prefer to sit upright. Cyanosis is uncommon and suggests severe disease when present. Clinicians should assess the quality of cry or voice, mental status, hydration, presence of drooling or trismus, neck mobility, stridor at rest, and work of breathing.
Severity can be graded using the Westley croup score, which incorporates stridor, retractions, air entry, cyanosis, and level of consciousness.
Diagnostic Evaluation
Continuous pulse oximetry is recommended. Routine laboratory testing is not indicated. Imaging is generally unnecessary but, when obtained for atypical presentations, anteroposterior and lateral neck radiographs may show the classic “steeple sign” reflecting subglottic narrowing. Imaging should never delay airway management in patients with suspected epiglottitis or bacterial tracheitis, and children must be closely monitored if imaging is performed.
Differential Diagnosis
Infectious causes include bacterial tracheitis, epiglottitis, retropharyngeal or parapharyngeal abscess, peritonsillar abscess, and diphtheria. Noninfectious causes include foreign body aspiration, angioedema, congenital airway abnormalities such as laryngomalacia or tracheomalacia, acquired subglottic stenosis, vocal cord paralysis, airway burns, hemangioma, laryngeal papillomatosis, and vocal cord dysfunction in adolescents.
Initial Management
Children should be allowed to maintain their position of comfort, and interventions that may increase distress, such as IV access or intramuscular injections, should be deferred when possible. In cases of severe respiratory distress, immediate nebulized epinephrine should be administered.
Emergency Department Management
Nebulized racemic epinephrine or L-epinephrine is indicated for stridor at rest or significant respiratory distress and is effective in reducing airway edema. Supplemental oxygen may be provided via blow-by if hypoxia is suspected. Dexamethasone significantly improves outcomes by reducing the need for intubation, hospital admission, and return visits, and is effective even in mild cases. If there is an incomplete response to epinephrine, heliox may be considered to reduce work of breathing.
For patients with impending or established respiratory failure, tracheal intubation should be performed by the most experienced provider available using an uncuffed endotracheal tube 0.5–1 mm smaller than standard size. If epiglottitis or foreign body aspiration is suspected, airway management should ideally occur in the operating room with surgical backup available.
Medications
Racemic epinephrine 2.25% is administered as 0.25–0.5 mL nebulized in normal saline. L-epinephrine 1:1,000 may be given as 5 mL nebulized. Dexamethasone is given as a single dose of 0.6 mg/kg, up to a maximum of 10 mg, via oral, intravenous, or intramuscular routes. Heliox may be administered as a 70:30 helium–oxygen mixture. Antibiotics are not indicated.
Disposition And Follow-Up
Hospital admission is recommended for young infants, children with pre-existing airway disease, persistent or recurrent stridor at rest despite treatment, or those requiring repeated epinephrine treatments. Pediatric intensive care admission is indicated for severe obstruction, frequent need for epinephrine or heliox, or need for intubation.
Children may be discharged if they have normal oxygenation on room air, no stridor at rest after observation for at least 2–3 hours, and reliable caregivers with access to follow-up care.
Referral Considerations
Evaluation by specialists is warranted for children with suspected anatomic airway abnormalities, recurrent episodes, prior intubation, or infants younger than one year with unexplained stridor.
Follow-Up Guidance
Most children with uncomplicated croup do not require routine follow-up. Caregivers should be instructed to seek medical attention if stridor persists, worsens, or recurs.
Key Teaching Points And Common Errors
Stridor in young infants warrants careful evaluation due to a higher likelihood of congenital airway abnormalities. Early epiglottitis or bacterial tracheitis may closely mimic croup and should be considered when symptoms are atypical or severe.

- Published on
Emergency and Acute Medicine – Cough
Physiologic Basis and Clinical Overview
Cough is a sudden, forceful, spasmodic contraction of the thoracic cavity that results in the rapid expulsion of air from the lungs, typically producing a characteristic sound. The cough mechanism begins with a deep inspiration followed by closure of the glottis, contraction of expiratory muscles, and a marked rise in intrapulmonary pressure. When the glottis opens, air is expelled at high velocity, facilitating the clearance of secretions and foreign material. Vibration of the vocal cords in conjunction with the tracheobronchial walls, lung parenchyma, and airway secretions produces the audible cough.
Cough serves as a vital protective defense mechanism for clearing the airway and may occur voluntarily or involuntarily. Involuntary coughing is mediated through vagal afferent nerves, while voluntary coughing is under cortical control, allowing suppression or intentional initiation. Because of this cortical influence, placebo effects can significantly impact cough frequency and severity. The reflex arc involves activation of respiratory tissue receptors, transmission through afferent neurons to the central cough center, and efferent signaling to the respiratory muscles. Mechanical receptors located in the larynx, trachea, and carina respond to touch and displacement, whereas chemical receptors in the larynx and bronchi respond to gases, fumes, mucus, edema, pus, and thermal stimuli.
Severe or persistent coughing may result in complications including epistaxis, subconjunctival hemorrhage, syncope, pneumothorax, pneumomediastinum, emesis, hernia formation, rectal prolapse, urinary or fecal incontinence, seizures, encephalitis, intracranial hemorrhage, spinal epidural hemorrhage, digital clubbing, and pruriginous rash.
Etiology and Duration-Based Classification
Acute cough, defined as lasting less than three weeks, is most commonly caused by pneumonia, acute bronchitis, sinusitis, pertussis, tuberculosis, upper respiratory tract infections, cough-variant asthma, COPD exacerbations, bronchiectasis, pulmonary embolism, left ventricular failure, airway obstruction from food or pills, gastroesophageal reflux disease, allergies, and bronchospasm.
Subacute cough, lasting three to eight weeks, is often postinfectious in origin and may be associated with pertussis, bronchitis, bacterial sinusitis, asthma, GERD, or pulmonary embolism.
Chronic cough, persisting for more than eight weeks, is commonly due to postnasal drip, asthma, GERD, chronic bronchitis, tuberculosis, bronchiectasis, eosinophilic bronchitis, ACE inhibitor use, bronchogenic carcinoma, carcinomatosis, sarcoidosis, left ventricular failure, aspiration syndromes, or psychogenic and habitual causes.
Pediatric Considerations
In children, the most frequent causes of cough include asthma, viral respiratory illness, acute bronchitis, pneumonia, sinusitis, and GERD. Less common causes include tracheobronchomalacia, mediastinal tumors, acyanotic congenital heart disease such as ventricular septal defect or patent ductus arteriosus, pulmonary stenosis, tetralogy of Fallot, retained airway foreign bodies, chronic milk aspiration, and environmental exposures. Evaluation should incorporate neonatal history, feeding patterns, growth and developmental milestones, allergy history, eczema, and sleep disorders. Chest radiography is indicated when foreign body ingestion or aspiration is suspected.
Clinical Features
Cough may be productive or nonproductive. Frothy sputum suggests pulmonary edema, while mucopurulent sputum is often associated with bacterial pneumonia or bronchitis but may also occur in viral infections. Rust-colored sputum suggests pneumococcal pneumonia, and “currant jelly” sputum is characteristic of Klebsiella pneumoniae. Hemoptysis may occur in a variety of conditions. Post-tussive syncope or emesis and paroxysmal coughing are suggestive of pertussis. Associated symptoms include shortness of breath, chest pain, fever, chills, night sweats, and wheezing. GERD-related cough may be accompanied by heartburn, dysphagia, regurgitation, belching, or early satiety. Weight loss, poor appetite, and fatigue raise concern for malignancy.
History should focus on cough duration to classify it as acute, subacute, or chronic, sputum characteristics including hemoptysis, and the presence of post-tussive emesis or syncope. Gastrointestinal symptoms may suggest GERD, while weight loss and night sweats in chronic cough raise suspicion for tuberculosis.
Physical Examination
Vital signs should be carefully assessed. Lung examination may reveal absent or decreased breath sounds suggesting reduced airflow or hyperinflation, crackles indicating alveolar opening, rhonchi from large airway obstruction, wheezes from narrowed airways, or stridor indicating upper airway obstruction. Signs of respiratory distress include use of accessory muscles and abdominal breathing.
Essential Diagnostic Approach
A comprehensive medical history should include cough duration, associated symptoms, exposure to sick contacts, smoking history, ACE inhibitor use, immunocompromised status including HIV, and potential tuberculosis exposure. Electrocardiography is indicated in patients with cardiac disease, chest pain, abnormal vital signs, or absence of infectious symptoms.
Laboratory studies should be guided by clinical presentation and may include a complete blood count with differential, sputum Gram stain and culture, acid-fast bacilli testing, CD4 count, pertussis serology, D-dimer testing, and influenza testing in high-risk or hospitalized patients.
Chest radiography is indicated for immunocompromised patients and in otherwise healthy patients with acute cough and sputum production when accompanied by tachycardia, tachypnea, fever above 38°C, focal lung findings, ill appearance, change in chronic cough pattern, or persistence of cough after discontinuation of an ACE inhibitor. Chest CT is reserved for abnormal radiographs or evaluation for pulmonary embolism. Peak flow testing may assist in asthma evaluation, while bronchoscopy is indicated for unexplained masses on imaging, hemoptysis, or suspected malignancy.
Differential Diagnosis
The differential diagnosis mirrors the etiologic categories described above and should be guided by duration, associated symptoms, and patient risk factors.
Emergency Department Management
Initial evaluation requires assessment of airway, breathing, and circulation. Treatment is directed at the underlying cause. Respiratory infections may require antibiotics, antivirals for influenza, decongestants, or antitussives. Asthma exacerbations are treated with inhaled beta-agonists and corticosteroids. GERD-related cough is managed with H2 blockers, proton pump inhibitors, and antacids. Suspected pertussis requires macrolide therapy and five days of isolation. Exacerbations of chronic bronchitis are treated with inhaled beta-agonists and steroids. Malignancy-related cough is managed with supportive care.
Pharmacologic Therapy
Antibiotic selection should target the suspected pathogen. Antiviral therapy includes oseltamivir at standard adult and pediatric dosing. Antitussives such as codeine, dextromethorphan, and hydrocodone may be used judiciously. Bronchodilators include inhaled albuterol and ipratropium. Decongestants such as chlorpheniramine and phenylpropanolamine may be used when indicated. Mucolytics such as guaifenesin aid secretion clearance. Corticosteroids may include intranasal dexamethasone or systemic methylprednisolone or prednisone, depending on severity and etiology.
Disposition and Follow-Up
Hospital admission is warranted for patients with hypoxemia, critical illness, suspected tuberculosis with radiographic findings, immunocompromised patients with fever, or those at risk for sepsis or bacteremia. Patients may be discharged if oxygenation is at baseline, oral medications are tolerated, and a safe home environment is assured. Close outpatient follow-up with a primary care physician is recommended.
Patient Guidance and Preventive Measures
Patients should be advised to stop smoking and avoid exposure to tobacco smoke, asbestos, and other respiratory irritants. Dietary modifications for GERD include avoiding caffeine-containing beverages, refraining from eating at least four hours before bedtime, and elevating the head during sleep. Immediate medical attention is required for chest pain, hemoptysis, shortness of breath, or syncope.
Key Clinical Insights and Common Errors
For patients whose clinical presentation is consistent with GERD-related cough, empiric treatment is recommended before pursuing diagnostic testing. In cases of presumed acute bronchitis, routine antibiotic therapy is not supported by evidence and should be avoided.
Physiologic Basis and Clinical Overview
Cough is a sudden, forceful, spasmodic contraction of the thoracic cavity that results in the rapid expulsion of air from the lungs, typically producing a characteristic sound. The cough mechanism begins with a deep inspiration followed by closure of the glottis, contraction of expiratory muscles, and a marked rise in intrapulmonary pressure. When the glottis opens, air is expelled at high velocity, facilitating the clearance of secretions and foreign material. Vibration of the vocal cords in conjunction with the tracheobronchial walls, lung parenchyma, and airway secretions produces the audible cough.
Cough serves as a vital protective defense mechanism for clearing the airway and may occur voluntarily or involuntarily. Involuntary coughing is mediated through vagal afferent nerves, while voluntary coughing is under cortical control, allowing suppression or intentional initiation. Because of this cortical influence, placebo effects can significantly impact cough frequency and severity. The reflex arc involves activation of respiratory tissue receptors, transmission through afferent neurons to the central cough center, and efferent signaling to the respiratory muscles. Mechanical receptors located in the larynx, trachea, and carina respond to touch and displacement, whereas chemical receptors in the larynx and bronchi respond to gases, fumes, mucus, edema, pus, and thermal stimuli.
Severe or persistent coughing may result in complications including epistaxis, subconjunctival hemorrhage, syncope, pneumothorax, pneumomediastinum, emesis, hernia formation, rectal prolapse, urinary or fecal incontinence, seizures, encephalitis, intracranial hemorrhage, spinal epidural hemorrhage, digital clubbing, and pruriginous rash.
Etiology and Duration-Based Classification
Acute cough, defined as lasting less than three weeks, is most commonly caused by pneumonia, acute bronchitis, sinusitis, pertussis, tuberculosis, upper respiratory tract infections, cough-variant asthma, COPD exacerbations, bronchiectasis, pulmonary embolism, left ventricular failure, airway obstruction from food or pills, gastroesophageal reflux disease, allergies, and bronchospasm.
Subacute cough, lasting three to eight weeks, is often postinfectious in origin and may be associated with pertussis, bronchitis, bacterial sinusitis, asthma, GERD, or pulmonary embolism.
Chronic cough, persisting for more than eight weeks, is commonly due to postnasal drip, asthma, GERD, chronic bronchitis, tuberculosis, bronchiectasis, eosinophilic bronchitis, ACE inhibitor use, bronchogenic carcinoma, carcinomatosis, sarcoidosis, left ventricular failure, aspiration syndromes, or psychogenic and habitual causes.
Pediatric Considerations
In children, the most frequent causes of cough include asthma, viral respiratory illness, acute bronchitis, pneumonia, sinusitis, and GERD. Less common causes include tracheobronchomalacia, mediastinal tumors, acyanotic congenital heart disease such as ventricular septal defect or patent ductus arteriosus, pulmonary stenosis, tetralogy of Fallot, retained airway foreign bodies, chronic milk aspiration, and environmental exposures. Evaluation should incorporate neonatal history, feeding patterns, growth and developmental milestones, allergy history, eczema, and sleep disorders. Chest radiography is indicated when foreign body ingestion or aspiration is suspected.
Clinical Features
Cough may be productive or nonproductive. Frothy sputum suggests pulmonary edema, while mucopurulent sputum is often associated with bacterial pneumonia or bronchitis but may also occur in viral infections. Rust-colored sputum suggests pneumococcal pneumonia, and “currant jelly” sputum is characteristic of Klebsiella pneumoniae. Hemoptysis may occur in a variety of conditions. Post-tussive syncope or emesis and paroxysmal coughing are suggestive of pertussis. Associated symptoms include shortness of breath, chest pain, fever, chills, night sweats, and wheezing. GERD-related cough may be accompanied by heartburn, dysphagia, regurgitation, belching, or early satiety. Weight loss, poor appetite, and fatigue raise concern for malignancy.
History should focus on cough duration to classify it as acute, subacute, or chronic, sputum characteristics including hemoptysis, and the presence of post-tussive emesis or syncope. Gastrointestinal symptoms may suggest GERD, while weight loss and night sweats in chronic cough raise suspicion for tuberculosis.
Physical Examination
Vital signs should be carefully assessed. Lung examination may reveal absent or decreased breath sounds suggesting reduced airflow or hyperinflation, crackles indicating alveolar opening, rhonchi from large airway obstruction, wheezes from narrowed airways, or stridor indicating upper airway obstruction. Signs of respiratory distress include use of accessory muscles and abdominal breathing.
Essential Diagnostic Approach
A comprehensive medical history should include cough duration, associated symptoms, exposure to sick contacts, smoking history, ACE inhibitor use, immunocompromised status including HIV, and potential tuberculosis exposure. Electrocardiography is indicated in patients with cardiac disease, chest pain, abnormal vital signs, or absence of infectious symptoms.
Laboratory studies should be guided by clinical presentation and may include a complete blood count with differential, sputum Gram stain and culture, acid-fast bacilli testing, CD4 count, pertussis serology, D-dimer testing, and influenza testing in high-risk or hospitalized patients.
Chest radiography is indicated for immunocompromised patients and in otherwise healthy patients with acute cough and sputum production when accompanied by tachycardia, tachypnea, fever above 38°C, focal lung findings, ill appearance, change in chronic cough pattern, or persistence of cough after discontinuation of an ACE inhibitor. Chest CT is reserved for abnormal radiographs or evaluation for pulmonary embolism. Peak flow testing may assist in asthma evaluation, while bronchoscopy is indicated for unexplained masses on imaging, hemoptysis, or suspected malignancy.
Differential Diagnosis
The differential diagnosis mirrors the etiologic categories described above and should be guided by duration, associated symptoms, and patient risk factors.
Emergency Department Management
Initial evaluation requires assessment of airway, breathing, and circulation. Treatment is directed at the underlying cause. Respiratory infections may require antibiotics, antivirals for influenza, decongestants, or antitussives. Asthma exacerbations are treated with inhaled beta-agonists and corticosteroids. GERD-related cough is managed with H2 blockers, proton pump inhibitors, and antacids. Suspected pertussis requires macrolide therapy and five days of isolation. Exacerbations of chronic bronchitis are treated with inhaled beta-agonists and steroids. Malignancy-related cough is managed with supportive care.
Pharmacologic Therapy
Antibiotic selection should target the suspected pathogen. Antiviral therapy includes oseltamivir at standard adult and pediatric dosing. Antitussives such as codeine, dextromethorphan, and hydrocodone may be used judiciously. Bronchodilators include inhaled albuterol and ipratropium. Decongestants such as chlorpheniramine and phenylpropanolamine may be used when indicated. Mucolytics such as guaifenesin aid secretion clearance. Corticosteroids may include intranasal dexamethasone or systemic methylprednisolone or prednisone, depending on severity and etiology.
Disposition and Follow-Up
Hospital admission is warranted for patients with hypoxemia, critical illness, suspected tuberculosis with radiographic findings, immunocompromised patients with fever, or those at risk for sepsis or bacteremia. Patients may be discharged if oxygenation is at baseline, oral medications are tolerated, and a safe home environment is assured. Close outpatient follow-up with a primary care physician is recommended.
Patient Guidance and Preventive Measures
Patients should be advised to stop smoking and avoid exposure to tobacco smoke, asbestos, and other respiratory irritants. Dietary modifications for GERD include avoiding caffeine-containing beverages, refraining from eating at least four hours before bedtime, and elevating the head during sleep. Immediate medical attention is required for chest pain, hemoptysis, shortness of breath, or syncope.
Key Clinical Insights and Common Errors
For patients whose clinical presentation is consistent with GERD-related cough, empiric treatment is recommended before pursuing diagnostic testing. In cases of presumed acute bronchitis, routine antibiotic therapy is not supported by evidence and should be avoided.
- Published on
Emergency and Acute Medicine – Corneal Foreign Body
Definition and Pathologic Considerations
A corneal foreign body refers to any foreign material lodged on or embedded within the corneal epithelium. When only the epithelial layer is disrupted, the injury results in a corneal abrasion; however, involvement of deeper corneal layers may lead to permanent scarring. The presence of a foreign body often provokes an inflammatory response that can extend beyond the cornea to involve surrounding ocular structures.
Etiology and Material Characteristics
Foreign material on the cornea induces inflammation and may lead to conjunctivitis, corneal edema, iritis, or tissue necrosis. Organic materials such as plant matter or insect fragments are poorly tolerated and carry a higher risk of infection. Inorganic materials that oxidize, including iron and copper, are also poorly tolerated because oxidation products act as persistent irritants. In contrast, inert materials such as paint, glass, plastic, fiberglass, and nonoxidizing metals are generally better tolerated by the cornea.
Clinical Presentation
Patients typically report a foreign body sensation accompanied by eye pain, tearing, conjunctival and scleral injection, blurred or decreased vision, and photophobia. A visible foreign body or rust ring may be noted, and some patients develop signs of traumatic iritis. A common history is that something fell, flew, or otherwise entered the eye. It is important to note that hot, high-speed projectiles may not cause immediate pain, increasing the risk of delayed presentation and more serious injury.
History and Physical Examination
A thorough history should assess the mechanism of injury, type of material involved, likelihood of high-velocity impact, and timing of symptom onset. Physical examination requires a complete ocular assessment, including evaluation of visual acuity, visual fields, extraocular movements, eyelids and lashes, pupils, sclera, conjunctiva, anterior chamber, and fundi. Slit-lamp examination is essential, and fluorescein staining should be performed to assess for epithelial defects. A Seidel test is required to identify aqueous leakage suggestive of corneal perforation. Intraocular pressure may be measured only if there is no evidence of globe perforation.
Essential Diagnostic Workup
Determining the nature of the injury is critical to assess the likelihood of globe penetration. An intraocular foreign body should be suspected with high-speed mechanisms such as hammering metal on metal, use of industrial machinery, or a positive Seidel test. Imaging is required when intraocular involvement is suspected. Orbital computed tomography or B-mode ultrasonography may be used to evaluate for intraocular foreign bodies, while plain orbital radiographs may screen for metallic foreign bodies. Magnetic resonance imaging must be avoided if a metallic foreign body is possible.
Differential Diagnosis
The differential diagnosis includes conjunctival foreign body, corneal abrasion, corneal perforation with or without intraocular foreign body, corneal ulcer, and infectious or inflammatory keratitis.
Initial and Prehospital Management
In the prehospital setting, a Fox shield should be placed, and the patient positioned upright to minimize further injury. In the emergency department, topical anesthetic drops are applied to alleviate discomfort and facilitate examination and treatment.
Emergency Department Management
Foreign bodies penetrating beyond the corneal epithelium into or past the Bowman membrane should be referred to an ophthalmologist due to the risk of permanent scarring. Superficial foreign bodies may be removed in the emergency department. Initial attempts include irrigation with normal saline directed obliquely across the corneal surface. If unsuccessful, removal may be performed using a 25-gauge needle or foreign body spud under slit-lamp visualization. The needle should be held bevel up and kept parallel to the corneal surface, with the examiner’s hand stabilized against the patient’s cheek to ensure control.
Iron-containing foreign bodies may leave a rust ring within three hours due to oxidation. Rust rings delay healing and perpetuate inflammation and should be removed either at the time of foreign body extraction or after a short delay of approximately 24 hours, using a needle or burr.
After removal, the Seidel test should be repeated to exclude perforation. The resultant corneal abrasion should be treated with topical antibiotic drops or ointment. Cycloplegic agents may be initiated if keratitis or traumatic iritis is suspected. Tetanus immunization should be updated as indicated, and analgesia provided using NSAIDs or acetaminophen with or without opioids. Pediatric patients may require sedation to allow adequate examination and foreign body removal.
Medications
Cycloplegic agents commonly used include cyclopentolate 1–2%, one drop three times daily, and homatropine 2% or 5%, one drop daily. Topical antibiotics are often prescribed for three to five days despite limited evidence of benefit and include erythromycin ointment, sulfacetamide drops, ciprofloxacin drops, ofloxacin drops, or polymyxin–trimethoprim drops. Topical NSAIDs such as ketorolac or diclofenac drops may be used for pain control.
Disposition and Follow-Up
Admission is required for patients with globe penetration. All other corneal foreign bodies may be discharged after appropriate treatment. Ophthalmology consultation is recommended for removal of vegetative material due to the high risk of ulceration, any evidence of infection or corneal ulcer, multiple foreign bodies, or incomplete removal. Ophthalmology follow-up within 24 hours is indicated for abrasions involving the visual axis, large abrasions, worsening or persistent symptoms, or rust ring removal. Patients should be instructed to return for reevaluation if symptoms persist or worsen within one to two days.
Key Clinical Insights and Common Errors
An intraocular foreign body must always be considered, particularly in patients with high-velocity mechanisms or industrial tool use. Eye patching does not improve pain or healing and is not recommended. After removal, most corneal foreign bodies can be managed as simple corneal abrasions and typically heal without complication. Topical anesthetics should never be prescribed for home use due to corneal toxicity and delayed healing.
Definition and Pathologic Considerations
A corneal foreign body refers to any foreign material lodged on or embedded within the corneal epithelium. When only the epithelial layer is disrupted, the injury results in a corneal abrasion; however, involvement of deeper corneal layers may lead to permanent scarring. The presence of a foreign body often provokes an inflammatory response that can extend beyond the cornea to involve surrounding ocular structures.
Etiology and Material Characteristics
Foreign material on the cornea induces inflammation and may lead to conjunctivitis, corneal edema, iritis, or tissue necrosis. Organic materials such as plant matter or insect fragments are poorly tolerated and carry a higher risk of infection. Inorganic materials that oxidize, including iron and copper, are also poorly tolerated because oxidation products act as persistent irritants. In contrast, inert materials such as paint, glass, plastic, fiberglass, and nonoxidizing metals are generally better tolerated by the cornea.
Clinical Presentation
Patients typically report a foreign body sensation accompanied by eye pain, tearing, conjunctival and scleral injection, blurred or decreased vision, and photophobia. A visible foreign body or rust ring may be noted, and some patients develop signs of traumatic iritis. A common history is that something fell, flew, or otherwise entered the eye. It is important to note that hot, high-speed projectiles may not cause immediate pain, increasing the risk of delayed presentation and more serious injury.
History and Physical Examination
A thorough history should assess the mechanism of injury, type of material involved, likelihood of high-velocity impact, and timing of symptom onset. Physical examination requires a complete ocular assessment, including evaluation of visual acuity, visual fields, extraocular movements, eyelids and lashes, pupils, sclera, conjunctiva, anterior chamber, and fundi. Slit-lamp examination is essential, and fluorescein staining should be performed to assess for epithelial defects. A Seidel test is required to identify aqueous leakage suggestive of corneal perforation. Intraocular pressure may be measured only if there is no evidence of globe perforation.
Essential Diagnostic Workup
Determining the nature of the injury is critical to assess the likelihood of globe penetration. An intraocular foreign body should be suspected with high-speed mechanisms such as hammering metal on metal, use of industrial machinery, or a positive Seidel test. Imaging is required when intraocular involvement is suspected. Orbital computed tomography or B-mode ultrasonography may be used to evaluate for intraocular foreign bodies, while plain orbital radiographs may screen for metallic foreign bodies. Magnetic resonance imaging must be avoided if a metallic foreign body is possible.
Differential Diagnosis
The differential diagnosis includes conjunctival foreign body, corneal abrasion, corneal perforation with or without intraocular foreign body, corneal ulcer, and infectious or inflammatory keratitis.
Initial and Prehospital Management
In the prehospital setting, a Fox shield should be placed, and the patient positioned upright to minimize further injury. In the emergency department, topical anesthetic drops are applied to alleviate discomfort and facilitate examination and treatment.
Emergency Department Management
Foreign bodies penetrating beyond the corneal epithelium into or past the Bowman membrane should be referred to an ophthalmologist due to the risk of permanent scarring. Superficial foreign bodies may be removed in the emergency department. Initial attempts include irrigation with normal saline directed obliquely across the corneal surface. If unsuccessful, removal may be performed using a 25-gauge needle or foreign body spud under slit-lamp visualization. The needle should be held bevel up and kept parallel to the corneal surface, with the examiner’s hand stabilized against the patient’s cheek to ensure control.
Iron-containing foreign bodies may leave a rust ring within three hours due to oxidation. Rust rings delay healing and perpetuate inflammation and should be removed either at the time of foreign body extraction or after a short delay of approximately 24 hours, using a needle or burr.
After removal, the Seidel test should be repeated to exclude perforation. The resultant corneal abrasion should be treated with topical antibiotic drops or ointment. Cycloplegic agents may be initiated if keratitis or traumatic iritis is suspected. Tetanus immunization should be updated as indicated, and analgesia provided using NSAIDs or acetaminophen with or without opioids. Pediatric patients may require sedation to allow adequate examination and foreign body removal.
Medications
Cycloplegic agents commonly used include cyclopentolate 1–2%, one drop three times daily, and homatropine 2% or 5%, one drop daily. Topical antibiotics are often prescribed for three to five days despite limited evidence of benefit and include erythromycin ointment, sulfacetamide drops, ciprofloxacin drops, ofloxacin drops, or polymyxin–trimethoprim drops. Topical NSAIDs such as ketorolac or diclofenac drops may be used for pain control.
Disposition and Follow-Up
Admission is required for patients with globe penetration. All other corneal foreign bodies may be discharged after appropriate treatment. Ophthalmology consultation is recommended for removal of vegetative material due to the high risk of ulceration, any evidence of infection or corneal ulcer, multiple foreign bodies, or incomplete removal. Ophthalmology follow-up within 24 hours is indicated for abrasions involving the visual axis, large abrasions, worsening or persistent symptoms, or rust ring removal. Patients should be instructed to return for reevaluation if symptoms persist or worsen within one to two days.
Key Clinical Insights and Common Errors
An intraocular foreign body must always be considered, particularly in patients with high-velocity mechanisms or industrial tool use. Eye patching does not improve pain or healing and is not recommended. After removal, most corneal foreign bodies can be managed as simple corneal abrasions and typically heal without complication. Topical anesthetics should never be prescribed for home use due to corneal toxicity and delayed healing.
- Published on
Emergency and Acute Medicine – Corneal Burn
Definition and Mechanisms of Injury
A corneal burn results from inappropriate exposure of the cornea to chemical agents, extreme heat or cold, electrical current, or radiant energy, leading to injury of the corneal tissue and frequently extending to adjacent ocular structures. The severity of injury is determined by the duration of exposure, the nature of the offending agent, its concentration, and in chemical injuries, the pH and ionic properties of the solution.
Alkali burns are particularly dangerous because they cause an immediate rise in ocular pH and are highly lipid soluble, allowing rapid penetration through ocular tissues. Without prompt intervention, alkalis continue to penetrate deeper layers, with significant injury occurring in less than one minute. Calcium-based alkalis are a notable exception, as they penetrate less effectively due to soap formation; although they may cause marked corneal opacification, their overall prognosis is often better than that of other alkali burns. Acid burns cause rapid coagulation of corneal epithelial proteins, leading to opacification. This coagulation creates a barrier that limits deeper penetration, except in the case of hydrofluoric acid, which is lipophilic and behaves more like an alkali, penetrating rapidly and causing severe injury.
Thermal burns generally affect the eyelids more than the globe because of reflex blinking and the Bell phenomenon, in which the eyes roll upward and outward. When the cornea is involved, injury severity depends on the duration and intensity of heat exposure. Electrical injuries occur when current passes through the head with an entry point at or near the eye. Radiation injuries result from ultraviolet light exposure to the cornea.
Etiology and Sources of Exposure
Common alkali agents include ammonia found in fertilizers, refrigerants, household ammonia, and cleaning agents; potassium hydroxide; magnesium hydroxide from sparklers, flares, and fireworks; sodium hydroxide in drain cleaners; and lime compounds used in cement, plaster, mortar, and whitewash. Motor vehicle airbag deployment can also release nonspecific alkali during inflation.
Acid exposures include sulfuric acid from car batteries and toilet cleaners, sulfurous acid used as food preservatives, acetic acid in vinegar, bleach, and hydrofluoric acid used in glass etching, brick cleaning, metal electropolishing, brewery fermentation control, and rust removal. Thermal injuries may result from hot liquids, molten metal, flames, hot smoke or gases, flash burns, steam, or cigarette burns. Radiation injuries are associated with sun lamps, tanning booths, high-altitude sunlight, reflected ultraviolet light from snow or water, and arc welding. In pediatric cases, the possibility of abuse or neglect must always be considered.
Clinical Presentation
Patients often present with severe eye pain, photophobia, excessive tearing, and a foreign body sensation. Conjunctival injection, corneal edema, corneal opacification, and reduced visual acuity are common. More severe findings include limbal blanching, lens opacification, vesicle formation with clear or hemorrhagic fluid in hypothermal injuries, and necrosis of the iris or ciliary body.
The history should focus on identifying the type of exposure and, when possible, inspection of any containers brought by the patient to determine active and inactive ingredients. The vehicle of exposure should be clarified, as aerosols are common and propellants may cause intraocular foreign bodies or perforation. Duration of exposure, time to irrigation, symptom onset, pre-existing visual impairment, protective eyewear use, contact lens use, and treatments initiated prior to arrival should be documented.
Physical Examination and Diagnostic Evaluation
A complete ocular examination should be performed after adequate irrigation. Visual acuity should be assessed first, followed by inspection of the cornea, conjunctivae, and limbus under bright white light. Slit-lamp examination is essential to evaluate anterior segment inflammation. Fluorescein staining helps identify corneal epithelial defects, including punctate lesions with a discrete inferior border typical of ultraviolet radiation burns, and can be used to detect perforation with the Seidel test. Lens clarity and fundus appearance should be assessed when possible, and intraocular pressure should be measured, particularly in delayed presentations. Examination of the eyelids and eyelashes is important to identify retained particulate matter. In acid or alkali burns, ocular pH should be measured using litmus paper or pH indicator strips placed in the inferior conjunctival fornix.
In children, handheld slit lamps and Wood lamps are particularly useful to facilitate examination.
Differential Diagnosis
Conditions that may resemble corneal burns include viral keratitis, corneal ulcer, corneal erosion syndrome, corneal foreign body, corneal abrasion, and hypothermal injury.
Prehospital and Initial Management
At the scene, immediate irrigation for 15–30 minutes is critical unless other life-threatening conditions require urgent transport. Whenever possible, the offending substance container should be brought to the hospital. Continuous irrigation with water or normal saline should be maintained during transport.
Initial stabilization depends on the type of exposure. For unknown chemical exposures, acid or alkali injury should be assumed, and irrigation initiated with any available diluting fluid, preferably water or normal saline. Thermal injuries should be managed with cool, moist dressings and overlying ice packs.
Emergency Department Treatment
For chemical exposures, including alkalis, acids, and mace, continuous irrigation is performed until a target pH of 7.3–7.5 is achieved, typically requiring 1–2 liters of fluid over 30–60 minutes using a Morgan lens. Ocular pH should be checked every 30 minutes, with pH paper placed in the inferior conjunctival fornix, and rechecked at 5 and 30 minutes after irrigation to confirm normalization. Topical anesthetics such as proparacaine may be required to facilitate irrigation. The fornices must be carefully inspected with the eye moved through full range of motion to ensure complete removal of particulate material.
Prophylactic topical antibiotics targeting Staphylococcus and Pseudomonas species are recommended until epithelial healing is complete, commonly using gentamicin ointment in combination with erythromycin or bacitracin. Cycloplegic agents such as cyclopentolate or atropine are used to reduce pain and prevent posterior synechiae. Oral analgesics are often required. If intraocular pressure is elevated, immediate ophthalmologic consultation is necessary, and treatment may include acetazolamide and topical timolol. Topical corticosteroids may be used to control anterior uveitis only after consultation with ophthalmology. Eye patching and surgical intervention may be required in cases of corneal penetration. Mild injuries warrant ophthalmology consultation by phone, while all moderate to severe injuries require immediate ophthalmologic evaluation or transfer to a specialized eye center. Hydrofluoric acid burns require standard treatment plus 1% calcium gluconate eye drops and admission for systemic analgesia.
Thermal injuries are managed with frequent moist dressing changes, topical antibiotics four times daily, generous lubrication, and moisture chambers when eyelid injury is extensive. Steroids may be used for short durations under ophthalmologic guidance. Any second- or third-degree eyelid burn requires ophthalmology consultation. Cigarette ash or hot liquid splashes usually cause superficial epithelial injury and are treated similarly to corneal abrasions. Electrical injuries require irrigation, wound care, antibiotic ointment, cycloplegics if uveitis is present, and adequate analgesia. Radiation injuries are treated with topical anesthetics for examination, short-acting cycloplegics, antibiotic ointment, and oral opioids if pain is severe.
Medications
Common treatments include artificial tears, cycloplegics such as atropine, cyclopentolate, homatropine, or tropicamide, topical antibiotics including bacitracin, erythromycin, gentamicin, sulfacetamide, ciprofloxacin, and tobramycin, and short-term topical anesthetics for in-hospital use only.
Disposition and Follow-Up
Admission is indicated for patients with intractable pain, elevated intraocular pressure, corneal penetration requiring surgical intervention, hydrofluoric acid burns requiring observation, or suspected child abuse. All mild corneal burns may be discharged once stabilized. Mandatory ophthalmology follow-up within 12–24 hours is required for all patients and should be arranged prior to discharge.
Key Management Principles and Safety Considerations
In chemical exposures, ocular examination should be delayed until adequate irrigation has been completed. Any patient with a corneal epithelial defect requires ophthalmologic follow-up within 12–24 hours. Topical anesthetics should never be prescribed for outpatient use, as they delay epithelial healing and increase the risk of serious complications.
Definition and Mechanisms of Injury
A corneal burn results from inappropriate exposure of the cornea to chemical agents, extreme heat or cold, electrical current, or radiant energy, leading to injury of the corneal tissue and frequently extending to adjacent ocular structures. The severity of injury is determined by the duration of exposure, the nature of the offending agent, its concentration, and in chemical injuries, the pH and ionic properties of the solution.
Alkali burns are particularly dangerous because they cause an immediate rise in ocular pH and are highly lipid soluble, allowing rapid penetration through ocular tissues. Without prompt intervention, alkalis continue to penetrate deeper layers, with significant injury occurring in less than one minute. Calcium-based alkalis are a notable exception, as they penetrate less effectively due to soap formation; although they may cause marked corneal opacification, their overall prognosis is often better than that of other alkali burns. Acid burns cause rapid coagulation of corneal epithelial proteins, leading to opacification. This coagulation creates a barrier that limits deeper penetration, except in the case of hydrofluoric acid, which is lipophilic and behaves more like an alkali, penetrating rapidly and causing severe injury.
Thermal burns generally affect the eyelids more than the globe because of reflex blinking and the Bell phenomenon, in which the eyes roll upward and outward. When the cornea is involved, injury severity depends on the duration and intensity of heat exposure. Electrical injuries occur when current passes through the head with an entry point at or near the eye. Radiation injuries result from ultraviolet light exposure to the cornea.
Etiology and Sources of Exposure
Common alkali agents include ammonia found in fertilizers, refrigerants, household ammonia, and cleaning agents; potassium hydroxide; magnesium hydroxide from sparklers, flares, and fireworks; sodium hydroxide in drain cleaners; and lime compounds used in cement, plaster, mortar, and whitewash. Motor vehicle airbag deployment can also release nonspecific alkali during inflation.
Acid exposures include sulfuric acid from car batteries and toilet cleaners, sulfurous acid used as food preservatives, acetic acid in vinegar, bleach, and hydrofluoric acid used in glass etching, brick cleaning, metal electropolishing, brewery fermentation control, and rust removal. Thermal injuries may result from hot liquids, molten metal, flames, hot smoke or gases, flash burns, steam, or cigarette burns. Radiation injuries are associated with sun lamps, tanning booths, high-altitude sunlight, reflected ultraviolet light from snow or water, and arc welding. In pediatric cases, the possibility of abuse or neglect must always be considered.
Clinical Presentation
Patients often present with severe eye pain, photophobia, excessive tearing, and a foreign body sensation. Conjunctival injection, corneal edema, corneal opacification, and reduced visual acuity are common. More severe findings include limbal blanching, lens opacification, vesicle formation with clear or hemorrhagic fluid in hypothermal injuries, and necrosis of the iris or ciliary body.
The history should focus on identifying the type of exposure and, when possible, inspection of any containers brought by the patient to determine active and inactive ingredients. The vehicle of exposure should be clarified, as aerosols are common and propellants may cause intraocular foreign bodies or perforation. Duration of exposure, time to irrigation, symptom onset, pre-existing visual impairment, protective eyewear use, contact lens use, and treatments initiated prior to arrival should be documented.
Physical Examination and Diagnostic Evaluation
A complete ocular examination should be performed after adequate irrigation. Visual acuity should be assessed first, followed by inspection of the cornea, conjunctivae, and limbus under bright white light. Slit-lamp examination is essential to evaluate anterior segment inflammation. Fluorescein staining helps identify corneal epithelial defects, including punctate lesions with a discrete inferior border typical of ultraviolet radiation burns, and can be used to detect perforation with the Seidel test. Lens clarity and fundus appearance should be assessed when possible, and intraocular pressure should be measured, particularly in delayed presentations. Examination of the eyelids and eyelashes is important to identify retained particulate matter. In acid or alkali burns, ocular pH should be measured using litmus paper or pH indicator strips placed in the inferior conjunctival fornix.
In children, handheld slit lamps and Wood lamps are particularly useful to facilitate examination.
Differential Diagnosis
Conditions that may resemble corneal burns include viral keratitis, corneal ulcer, corneal erosion syndrome, corneal foreign body, corneal abrasion, and hypothermal injury.
Prehospital and Initial Management
At the scene, immediate irrigation for 15–30 minutes is critical unless other life-threatening conditions require urgent transport. Whenever possible, the offending substance container should be brought to the hospital. Continuous irrigation with water or normal saline should be maintained during transport.
Initial stabilization depends on the type of exposure. For unknown chemical exposures, acid or alkali injury should be assumed, and irrigation initiated with any available diluting fluid, preferably water or normal saline. Thermal injuries should be managed with cool, moist dressings and overlying ice packs.
Emergency Department Treatment
For chemical exposures, including alkalis, acids, and mace, continuous irrigation is performed until a target pH of 7.3–7.5 is achieved, typically requiring 1–2 liters of fluid over 30–60 minutes using a Morgan lens. Ocular pH should be checked every 30 minutes, with pH paper placed in the inferior conjunctival fornix, and rechecked at 5 and 30 minutes after irrigation to confirm normalization. Topical anesthetics such as proparacaine may be required to facilitate irrigation. The fornices must be carefully inspected with the eye moved through full range of motion to ensure complete removal of particulate material.
Prophylactic topical antibiotics targeting Staphylococcus and Pseudomonas species are recommended until epithelial healing is complete, commonly using gentamicin ointment in combination with erythromycin or bacitracin. Cycloplegic agents such as cyclopentolate or atropine are used to reduce pain and prevent posterior synechiae. Oral analgesics are often required. If intraocular pressure is elevated, immediate ophthalmologic consultation is necessary, and treatment may include acetazolamide and topical timolol. Topical corticosteroids may be used to control anterior uveitis only after consultation with ophthalmology. Eye patching and surgical intervention may be required in cases of corneal penetration. Mild injuries warrant ophthalmology consultation by phone, while all moderate to severe injuries require immediate ophthalmologic evaluation or transfer to a specialized eye center. Hydrofluoric acid burns require standard treatment plus 1% calcium gluconate eye drops and admission for systemic analgesia.
Thermal injuries are managed with frequent moist dressing changes, topical antibiotics four times daily, generous lubrication, and moisture chambers when eyelid injury is extensive. Steroids may be used for short durations under ophthalmologic guidance. Any second- or third-degree eyelid burn requires ophthalmology consultation. Cigarette ash or hot liquid splashes usually cause superficial epithelial injury and are treated similarly to corneal abrasions. Electrical injuries require irrigation, wound care, antibiotic ointment, cycloplegics if uveitis is present, and adequate analgesia. Radiation injuries are treated with topical anesthetics for examination, short-acting cycloplegics, antibiotic ointment, and oral opioids if pain is severe.
Medications
Common treatments include artificial tears, cycloplegics such as atropine, cyclopentolate, homatropine, or tropicamide, topical antibiotics including bacitracin, erythromycin, gentamicin, sulfacetamide, ciprofloxacin, and tobramycin, and short-term topical anesthetics for in-hospital use only.
Disposition and Follow-Up
Admission is indicated for patients with intractable pain, elevated intraocular pressure, corneal penetration requiring surgical intervention, hydrofluoric acid burns requiring observation, or suspected child abuse. All mild corneal burns may be discharged once stabilized. Mandatory ophthalmology follow-up within 12–24 hours is required for all patients and should be arranged prior to discharge.
Key Management Principles and Safety Considerations
In chemical exposures, ocular examination should be delayed until adequate irrigation has been completed. Any patient with a corneal epithelial defect requires ophthalmologic follow-up within 12–24 hours. Topical anesthetics should never be prescribed for outpatient use, as they delay epithelial healing and increase the risk of serious complications.


- Published on
Emergency and Acute Medicine – Corneal Abrasion
Definition and General Description
A corneal abrasion is defined as any tear, defect, or disruption of the corneal epithelium. It is a common ocular injury that may result from direct trauma, spontaneous epithelial breakdown, foreign body exposure, or contact lens use. Because the cornea is densely innervated, even small epithelial defects can cause significant pain and visual disturbance.
Etiology and Mechanisms of Injury
Traumatic corneal abrasions are most frequently caused by fingernails, tree branches, hairbrushes or combs, sand or small stones, snow, pens or pencils, toys, chemical exposures, airbag deployment, pepper spray, paper or cardboard, makeup applicators, and animal paws. Foreign body–related abrasions may occur from materials such as wood, glass, metal, rust, plastic, fiberglass, or vegetable matter, including foreign bodies trapped beneath the eyelid. Contact lens–related abrasions are associated with overwear, improper lens fit, or inadequate lens hygiene. Spontaneous corneal abrasions usually occur in patients with a history of prior corneal trauma or those with an underlying defect of the corneal epithelium, such as recurrent corneal erosion syndrome.
Clinical Presentation
Patients typically present with severe ocular pain accompanied by a gritty or scratchy sensation, excessive tearing, blepharospasm, and a persistent foreign body sensation. Photophobia is common and may be pronounced if traumatic iritis is present. Additional symptoms include conjunctival injection, blurred or diminished vision, and headache.
The history should specifically address any direct trauma to the eye, known or suspected foreign body exposure, contact lens use, previous corneal abrasions, prior ocular or periocular surgery, pre-existing visual impairment, and the timing of symptom onset. Associated injuries or symptoms should be assessed, as well as any treatment attempted before presentation. Inquiry about occupational or recreational eye protection, systemic diseases such as diabetes or autoimmune disorders, and tetanus immunization status is also important.
Pediatric Considerations
In children, the presentation may differ significantly from adults. Excessive crying may be the primary manifestation. In infants younger than 12 months, there is often no clear history of eye trauma, and corneal abrasion may present as an inconsolable crying infant. In neonates and infants aged 1–12 weeks, corneal abrasions may be incidental findings and not the cause of irritability. Children older than 12 months are more likely to have a history of minor eye trauma and demonstrate more obvious ocular signs.
Physical Examination and Diagnostic Evaluation
If clinically indicated, the initial evaluation should include assessment for other life-threatening injuries following standard primary survey principles. A focused but complete eye examination is essential and should aim to exclude penetrating injury or infection. This includes gross inspection of the eye, assessment of visual acuity, and a penlight examination to evaluate conjunctival injection, pupil shape and reactivity, and the presence of corneal opacity or infiltrate. The upper eyelids should be everted to assess for retained foreign bodies. Slit-lamp examination allows evaluation of the anterior chamber for inflammation, detection of corneal laceration or penetrating trauma, and identification of infiltrates. Fluorescein staining is used to confirm the diagnosis and determine the size and location of the epithelial defect.
In pediatric patients, handheld slit lamps and Wood lamps can be particularly helpful in facilitating examination.
Differential Diagnosis
The differential diagnosis includes viral or bacterial conjunctivitis, corneal ulcer, acute glaucoma, herpes zoster ophthalmicus, infectious or ultraviolet keratitis, recurrent corneal erosion syndrome, and uveitis. More serious ocular injuries must also be considered, including corneal laceration or perforation, hyphema, iris prolapse, and lens disruption.
Initial Management and Emergency Department Care
Initial therapy includes instillation of a topical anesthetic, such as proparacaine or tetracaine, to facilitate examination. In the emergency department, superficial foreign bodies should be removed when present. A residual rust ring does not require emergent removal and can be addressed within 24–48 hours. Pain control may be achieved with oral NSAIDs, acetaminophen, or oral opioids when necessary.
Topical NSAIDs such as diclofenac or ketorolac have demonstrated effectiveness for pain control, although there are rare reports of adverse effects; these agents should be avoided in patients with pre-existing ocular surface disease or those who have recently undergone eye surgery. Cycloplegic agents may be used selectively to relieve ciliary spasm, including cyclopentolate, tropicamide, or homatropine.
Topical antibiotics are commonly prescribed despite limited evidence, primarily to prevent secondary infection. Ointments are preferred over drops due to their lubricating properties. Antibiotics should be discontinued once the patient has been symptom free for 24 hours. Contact lens wearers require antipseudomonal coverage, such as ciprofloxacin. Eye patching does not improve healing or pain control, particularly within the first 24 hours, and is not recommended for small abrasions. Patching should never be used in contact lens wearers or in injuries with high infection risk, such as those involving organic matter. The role of patching in large abrasions greater than 10 mm remains unclear.
Contact lenses should not be worn until the abrasion has fully healed and the eye has felt normal for at least one week without medication. In cases of severe pain, a bandage contact lens may be considered, provided there is no evidence of infection and close daily follow-up is ensured. Routine tetanus prophylaxis is not required, but immunization should be updated if the abrasion is caused by or contaminated with dirt or organic material. Emergent ophthalmology consultation is required for suspected intraocular foreign bodies, penetrating globe injuries, or the presence of corneal infiltrates, white spots, or opacities.
Medications
Commonly used medications include topical ciprofloxacin 0.35% drops four times daily, erythromycin 0.5% ointment four times daily, gentamicin drops or ointment, sulfacetamide drops or ointment, and tobramycin drops or ointment. Cycloplegics such as cyclopentolate, tropicamide, or homatropine may be used as indicated. Topical NSAIDs include diclofenac 0.1% or ketorolac 0.5% drops four times daily. Proparacaine should be used only once in the emergency department and not prescribed for outpatient use.
Disposition and Follow-Up
Hospital admission is reserved for patients with associated injuries requiring inpatient care. All uncomplicated corneal abrasions may be discharged from the emergency department. Although no definitive studies define optimal follow-up, standard practice recommends follow-up for all corneal abrasions to ensure complete healing without infection or scarring. Contact lens wearers, patients with patched eyes, or those with bandage contact lenses should be re-evaluated by ophthalmology within 24 hours. Central or large abrasions also warrant ophthalmologic follow-up within 24 hours, while smaller peripheral abrasions may be rechecked within 48–72 hours.
Essential Clinical Cautions and Common Errors
Clinicians must always carefully evaluate for penetrating globe injuries and signs of infection. Patients should never be discharged with topical anesthetics, as these agents are toxic to the corneal epithelium and delay healing, despite limited evidence suggesting dilute formulations may be safe. Mydriatic agents should not be used in patients with a history of glaucoma. Contact lens use should not be resumed until the patient has been evaluated and cleared by ophthalmology.
Definition and General Description
A corneal abrasion is defined as any tear, defect, or disruption of the corneal epithelium. It is a common ocular injury that may result from direct trauma, spontaneous epithelial breakdown, foreign body exposure, or contact lens use. Because the cornea is densely innervated, even small epithelial defects can cause significant pain and visual disturbance.
Etiology and Mechanisms of Injury
Traumatic corneal abrasions are most frequently caused by fingernails, tree branches, hairbrushes or combs, sand or small stones, snow, pens or pencils, toys, chemical exposures, airbag deployment, pepper spray, paper or cardboard, makeup applicators, and animal paws. Foreign body–related abrasions may occur from materials such as wood, glass, metal, rust, plastic, fiberglass, or vegetable matter, including foreign bodies trapped beneath the eyelid. Contact lens–related abrasions are associated with overwear, improper lens fit, or inadequate lens hygiene. Spontaneous corneal abrasions usually occur in patients with a history of prior corneal trauma or those with an underlying defect of the corneal epithelium, such as recurrent corneal erosion syndrome.
Clinical Presentation
Patients typically present with severe ocular pain accompanied by a gritty or scratchy sensation, excessive tearing, blepharospasm, and a persistent foreign body sensation. Photophobia is common and may be pronounced if traumatic iritis is present. Additional symptoms include conjunctival injection, blurred or diminished vision, and headache.
The history should specifically address any direct trauma to the eye, known or suspected foreign body exposure, contact lens use, previous corneal abrasions, prior ocular or periocular surgery, pre-existing visual impairment, and the timing of symptom onset. Associated injuries or symptoms should be assessed, as well as any treatment attempted before presentation. Inquiry about occupational or recreational eye protection, systemic diseases such as diabetes or autoimmune disorders, and tetanus immunization status is also important.
Pediatric Considerations
In children, the presentation may differ significantly from adults. Excessive crying may be the primary manifestation. In infants younger than 12 months, there is often no clear history of eye trauma, and corneal abrasion may present as an inconsolable crying infant. In neonates and infants aged 1–12 weeks, corneal abrasions may be incidental findings and not the cause of irritability. Children older than 12 months are more likely to have a history of minor eye trauma and demonstrate more obvious ocular signs.
Physical Examination and Diagnostic Evaluation
If clinically indicated, the initial evaluation should include assessment for other life-threatening injuries following standard primary survey principles. A focused but complete eye examination is essential and should aim to exclude penetrating injury or infection. This includes gross inspection of the eye, assessment of visual acuity, and a penlight examination to evaluate conjunctival injection, pupil shape and reactivity, and the presence of corneal opacity or infiltrate. The upper eyelids should be everted to assess for retained foreign bodies. Slit-lamp examination allows evaluation of the anterior chamber for inflammation, detection of corneal laceration or penetrating trauma, and identification of infiltrates. Fluorescein staining is used to confirm the diagnosis and determine the size and location of the epithelial defect.
In pediatric patients, handheld slit lamps and Wood lamps can be particularly helpful in facilitating examination.
Differential Diagnosis
The differential diagnosis includes viral or bacterial conjunctivitis, corneal ulcer, acute glaucoma, herpes zoster ophthalmicus, infectious or ultraviolet keratitis, recurrent corneal erosion syndrome, and uveitis. More serious ocular injuries must also be considered, including corneal laceration or perforation, hyphema, iris prolapse, and lens disruption.
Initial Management and Emergency Department Care
Initial therapy includes instillation of a topical anesthetic, such as proparacaine or tetracaine, to facilitate examination. In the emergency department, superficial foreign bodies should be removed when present. A residual rust ring does not require emergent removal and can be addressed within 24–48 hours. Pain control may be achieved with oral NSAIDs, acetaminophen, or oral opioids when necessary.
Topical NSAIDs such as diclofenac or ketorolac have demonstrated effectiveness for pain control, although there are rare reports of adverse effects; these agents should be avoided in patients with pre-existing ocular surface disease or those who have recently undergone eye surgery. Cycloplegic agents may be used selectively to relieve ciliary spasm, including cyclopentolate, tropicamide, or homatropine.
Topical antibiotics are commonly prescribed despite limited evidence, primarily to prevent secondary infection. Ointments are preferred over drops due to their lubricating properties. Antibiotics should be discontinued once the patient has been symptom free for 24 hours. Contact lens wearers require antipseudomonal coverage, such as ciprofloxacin. Eye patching does not improve healing or pain control, particularly within the first 24 hours, and is not recommended for small abrasions. Patching should never be used in contact lens wearers or in injuries with high infection risk, such as those involving organic matter. The role of patching in large abrasions greater than 10 mm remains unclear.
Contact lenses should not be worn until the abrasion has fully healed and the eye has felt normal for at least one week without medication. In cases of severe pain, a bandage contact lens may be considered, provided there is no evidence of infection and close daily follow-up is ensured. Routine tetanus prophylaxis is not required, but immunization should be updated if the abrasion is caused by or contaminated with dirt or organic material. Emergent ophthalmology consultation is required for suspected intraocular foreign bodies, penetrating globe injuries, or the presence of corneal infiltrates, white spots, or opacities.
Medications
Commonly used medications include topical ciprofloxacin 0.35% drops four times daily, erythromycin 0.5% ointment four times daily, gentamicin drops or ointment, sulfacetamide drops or ointment, and tobramycin drops or ointment. Cycloplegics such as cyclopentolate, tropicamide, or homatropine may be used as indicated. Topical NSAIDs include diclofenac 0.1% or ketorolac 0.5% drops four times daily. Proparacaine should be used only once in the emergency department and not prescribed for outpatient use.
Disposition and Follow-Up
Hospital admission is reserved for patients with associated injuries requiring inpatient care. All uncomplicated corneal abrasions may be discharged from the emergency department. Although no definitive studies define optimal follow-up, standard practice recommends follow-up for all corneal abrasions to ensure complete healing without infection or scarring. Contact lens wearers, patients with patched eyes, or those with bandage contact lenses should be re-evaluated by ophthalmology within 24 hours. Central or large abrasions also warrant ophthalmologic follow-up within 24 hours, while smaller peripheral abrasions may be rechecked within 48–72 hours.
Essential Clinical Cautions and Common Errors
Clinicians must always carefully evaluate for penetrating globe injuries and signs of infection. Patients should never be discharged with topical anesthetics, as these agents are toxic to the corneal epithelium and delay healing, despite limited evidence suggesting dilute formulations may be safe. Mydriatic agents should not be used in patients with a history of glaucoma. Contact lens use should not be resumed until the patient has been evaluated and cleared by ophthalmology.
- Published on
Emergency and Acute Medicine – Cor Pulmonale
Definition and Pathophysiologic Overview
Cor pulmonale refers to right ventricular hypertrophy or dilation caused by elevated pulmonary artery pressure. Right ventricular hypertrophy resulting from primary left-sided heart disease or congenital cardiac abnormalities is not classified as cor pulmonale. The disorder may be acute or chronic, depending on the rapidity and duration of pulmonary hypertension and the adaptive capacity of the right ventricle.
Acute cor pulmonale is marked by sudden right ventricular dilation with thinning and stretching of the ventricular wall, caused by an abrupt increase in right ventricular afterload due to acute pulmonary hypertension. The most common cause is a massive pulmonary embolism. Chronic cor pulmonale develops from long-standing pulmonary hypertension and is characterized initially by right ventricular hypertrophy, followed by dilation and eventual right-sided heart failure. This chronic form most often results from persistent alveolar hypoxia and represents an adaptive response to sustained elevation in pulmonary vascular resistance.
The pulmonary circulation is normally a low-pressure, low-resistance system with thin-walled, distensible arteries. Mean pulmonary arterial pressure typically ranges from 12 to 15 mm Hg, while normal left atrial pressure is approximately 6 to 10 mm Hg, resulting in a small pressure gradient of 6 to 9 mm Hg to drive pulmonary blood flow. Pulmonary arterial pressure is determined by cardiac output, pulmonary venous pressure, and pulmonary vascular resistance. Pulmonary hypertension may arise from markedly increased cardiac output, left-to-right shunts due to congenital heart disease, or most commonly hypoxia. Hypoxic pulmonary vasoconstriction is an adaptive response to alveolar hypoxia that preserves ventilation–perfusion matching by increasing pulmonary arterial pressure to maintain flow through the pulmonary vascular bed. Pulmonary embolism produces a similar effect by increasing resistance to pulmonary blood flow, while increased blood viscosity or elevated intrathoracic pressure can further impair pulmonary circulation.
Pulmonary hypertension is categorized into five groups. Group 1 includes pulmonary arterial hypertension. Group 2 consists of pulmonary hypertension due to left-sided heart disease, in which associated right ventricular dysfunction is not considered cor pulmonale. Group 3 includes pulmonary hypertension due to lung disease and/or hypoxia. Group 4 encompasses chronic thromboembolic pulmonary hypertension. Group 5 includes pulmonary hypertension with unclear or multifactorial mechanisms.
Epidemiology
Approximately 86,000 deaths occur annually from chronic obstructive pulmonary disease, with associated right ventricular failure contributing significantly in many cases. Cor pulmonale accounts for 10–30% of heart failure admissions in the United States. Among patients older than 50 years with COPD, about half develop pulmonary hypertension and are therefore at risk for cor pulmonale. Disease progression is closely tied to the severity of the underlying pulmonary disorder, and once cor pulmonale develops, the estimated five-year survival rate is approximately 30%.
Etiology
Chronic hypoxia is the most frequent cause of cor pulmonale and may result from COPD, residence at high altitude, obstructive sleep apnea, or chest wall deformities such as kyphoscoliosis. Other causes include pulmonary embolism and interstitial lung diseases such as scleroderma, systemic lupus erythematosus, mixed connective tissue disease, sarcoidosis, pulmonary Langerhans cell histiocytosis, neurofibromatosis, lymphangioleiomyomatosis, and cystic fibrosis. Additional contributing factors include severe anemia, obesity, pulmonary veno-occlusive disease, pulmonary vascular obstruction from tumors or lymphadenopathy, increased blood viscosity as seen in polycythemia vera or leukemia, and elevated intrathoracic pressure due to mechanical ventilation with positive end-expiratory pressure. Idiopathic primary pulmonary hypertension is a less common cause.
Clinical Manifestations
Patients frequently present with exertional dyspnea, easy fatigability, weakness, and reduced exercise tolerance. Additional symptoms include exertional syncope, cough, hemoptysis, and exertional angina even in the absence of coronary artery disease. Anorexia, right upper quadrant discomfort, wheezing, hoarseness, and weight gain may occur as right-sided heart failure progresses. Signs of volume overload include hepatomegaly, ascites, and peripheral edema. In advanced disease, cardiogenic shock may develop, manifested by oliguria, cool extremities, and pulmonary edema resulting from interventricular septal displacement that impairs left ventricular diastolic filling.
History commonly reveals exercise intolerance, palpitations, chest pain, lightheadedness, syncope, and lower extremity swelling. Physical examination may show jugular venous distention with prominent A and V waves, increased chest diameter, crackles or wheezes on lung auscultation, and a left parasternal heave. Splitting of the second heart sound or murmurs related to pulmonary vasculature abnormalities may be present. A hepatojugular reflex, pulsatile liver, and pitting edema of the lower extremities are typical findings in advanced cases.
Diagnostic Evaluation
Pulse oximetry or arterial blood gas analysis typically demonstrates resting hypoxemia with arterial oxygen tensions of 40–60 mm Hg and resting carbon dioxide levels often between 40 and 70 mm Hg. Hematocrit is frequently elevated due to secondary polycythemia. Elevated B-type natriuretic peptide levels are sensitive for moderate to severe pulmonary hypertension and may independently predict mortality, although elevation alone is insufficient to establish the diagnosis of cor pulmonale. Other laboratory tests are generally of limited diagnostic value.
Chest radiography often reveals signs of pulmonary hypertension, including enlarged pulmonary arteries greater than 16–18 mm and an enlarged right ventricular silhouette. Although abnormalities are seen in more than 90% of patients, chest radiographs do not reliably indicate disease severity. Pleural effusions are not a feature of isolated cor pulmonale. Electrocardiography may demonstrate right-axis deviation, right bundle branch block, right ventricular hypertrophy with dominant R waves in leads V1 and V2, prominent S waves in leads V5 and V6, small R waves with deep S waves across the precordium, and right atrial enlargement with tall, peaked P waves consistent with P pulmonale. Acute cor pulmonale may show an S1Q3 pattern, transient hypoxia-related changes, and right precordial T-wave flattening.
Echocardiography is the preferred noninvasive diagnostic modality and may demonstrate right ventricular hypertrophy or dilation, tricuspid regurgitation, and Doppler-based estimation of pulmonary artery pressure and right ventricular ejection fraction. Chest computed tomography, ventilation–perfusion scanning, or pulmonary angiography are useful when acute cor pulmonale is suspected, particularly in cases of pulmonary embolism. Magnetic resonance imaging offers superior assessment of right ventricular size and function compared with echocardiography. Pulmonary function testing may reveal reduced diffusion capacity associated with pulmonary hypertension. Right-heart catheterization remains the most accurate method for assessing pulmonary vascular hemodynamics and provides precise measurements of pulmonary arterial and pulmonary capillary wedge pressures.
Differential Diagnosis
The differential diagnosis includes primary left-sided heart disease such as mitral stenosis, congenital heart disease including Eisenmenger syndrome with left-to-right shunting, hypothyroidism, and cirrhosis.
Management and Prehospital Care
Prehospital treatment is supportive and includes supplemental oxygen titrated to achieve arterial oxygen saturation of approximately 90%, establishment of intravenous access, continuous cardiac monitoring, and pulse oximetry. Bronchospasm related to underlying respiratory disease should be treated with beta-agonist nebulizers. Vasodilators and diuretics have no role in the prehospital setting. Patients with severe hypoxia may require endotracheal intubation.
Emergency Department Treatment
Management in the emergency department is directed at treating the underlying disease process and reducing pulmonary hypertension. Supplemental oxygen should be administered to raise arterial oxygen saturation to 90%, thereby reducing pulmonary vasoconstriction and right ventricular afterload while improving cardiac output and promoting diuresis. Careful monitoring of ventilation and carbon dioxide levels is essential, as hypercapnia may suppress respiratory drive and worsen acidosis. Diuretics such as furosemide may be used cautiously to reduce circulating blood volume and pulmonary artery pressure, with close attention to avoiding hypovolemia and electrolyte disturbances. Patients should be maintained on salt and fluid restriction. Digoxin has no role in the treatment of cor pulmonale.
Bronchodilator therapy is particularly beneficial in patients with COPD, as it reduces ventricular afterload and improves airflow. Selective beta-adrenergic agents such as subcutaneous terbutaline may be administered, and theophylline may be considered to enhance diaphragmatic contractility and reduce muscle fatigue. Anticoagulation should be considered in patients at high risk for thromboembolic disease. In acutely decompensated COPD, early initiation of corticosteroids and antibiotics is indicated. Improvement of the underlying respiratory disorder typically results in improved right ventricular function.
Medications
Furosemide may be administered at doses of 20–60 mg intravenously in adults, with pediatric dosing starting at 1 mg/kg and titrated as needed to a maximum of 6 mg/kg. Terbutaline may be administered at a dose of 0.25 mg subcutaneously.
Disposition and Follow-Up
Hospital admission is indicated for patients with new-onset hypoxia, anasarca, severe respiratory failure, or when required by the severity of the underlying disease. Patients without hypoxia or with stable oxygen requirements may be considered for discharge. Close outpatient follow-up is essential once the underlying etiology has responded to acute management, and evaluation for sleep apnea with a sleep study should be coordinated by the patient’s physician when indicated. Home oxygen therapy should be ensured for patients with chronic hypoxia.
Key Clinical Insights and Common Management Errors
Physical examination findings may be unreliable in patients with COPD because chest hyperinflation often obscures classic signs of cor pulmonale. Vasodilator therapy should be reserved for cases in which conventional management and adequate oxygenation have failed and should be used with caution.
Definition and Pathophysiologic Overview
Cor pulmonale refers to right ventricular hypertrophy or dilation caused by elevated pulmonary artery pressure. Right ventricular hypertrophy resulting from primary left-sided heart disease or congenital cardiac abnormalities is not classified as cor pulmonale. The disorder may be acute or chronic, depending on the rapidity and duration of pulmonary hypertension and the adaptive capacity of the right ventricle.
Acute cor pulmonale is marked by sudden right ventricular dilation with thinning and stretching of the ventricular wall, caused by an abrupt increase in right ventricular afterload due to acute pulmonary hypertension. The most common cause is a massive pulmonary embolism. Chronic cor pulmonale develops from long-standing pulmonary hypertension and is characterized initially by right ventricular hypertrophy, followed by dilation and eventual right-sided heart failure. This chronic form most often results from persistent alveolar hypoxia and represents an adaptive response to sustained elevation in pulmonary vascular resistance.
The pulmonary circulation is normally a low-pressure, low-resistance system with thin-walled, distensible arteries. Mean pulmonary arterial pressure typically ranges from 12 to 15 mm Hg, while normal left atrial pressure is approximately 6 to 10 mm Hg, resulting in a small pressure gradient of 6 to 9 mm Hg to drive pulmonary blood flow. Pulmonary arterial pressure is determined by cardiac output, pulmonary venous pressure, and pulmonary vascular resistance. Pulmonary hypertension may arise from markedly increased cardiac output, left-to-right shunts due to congenital heart disease, or most commonly hypoxia. Hypoxic pulmonary vasoconstriction is an adaptive response to alveolar hypoxia that preserves ventilation–perfusion matching by increasing pulmonary arterial pressure to maintain flow through the pulmonary vascular bed. Pulmonary embolism produces a similar effect by increasing resistance to pulmonary blood flow, while increased blood viscosity or elevated intrathoracic pressure can further impair pulmonary circulation.
Pulmonary hypertension is categorized into five groups. Group 1 includes pulmonary arterial hypertension. Group 2 consists of pulmonary hypertension due to left-sided heart disease, in which associated right ventricular dysfunction is not considered cor pulmonale. Group 3 includes pulmonary hypertension due to lung disease and/or hypoxia. Group 4 encompasses chronic thromboembolic pulmonary hypertension. Group 5 includes pulmonary hypertension with unclear or multifactorial mechanisms.
Epidemiology
Approximately 86,000 deaths occur annually from chronic obstructive pulmonary disease, with associated right ventricular failure contributing significantly in many cases. Cor pulmonale accounts for 10–30% of heart failure admissions in the United States. Among patients older than 50 years with COPD, about half develop pulmonary hypertension and are therefore at risk for cor pulmonale. Disease progression is closely tied to the severity of the underlying pulmonary disorder, and once cor pulmonale develops, the estimated five-year survival rate is approximately 30%.
Etiology
Chronic hypoxia is the most frequent cause of cor pulmonale and may result from COPD, residence at high altitude, obstructive sleep apnea, or chest wall deformities such as kyphoscoliosis. Other causes include pulmonary embolism and interstitial lung diseases such as scleroderma, systemic lupus erythematosus, mixed connective tissue disease, sarcoidosis, pulmonary Langerhans cell histiocytosis, neurofibromatosis, lymphangioleiomyomatosis, and cystic fibrosis. Additional contributing factors include severe anemia, obesity, pulmonary veno-occlusive disease, pulmonary vascular obstruction from tumors or lymphadenopathy, increased blood viscosity as seen in polycythemia vera or leukemia, and elevated intrathoracic pressure due to mechanical ventilation with positive end-expiratory pressure. Idiopathic primary pulmonary hypertension is a less common cause.
Clinical Manifestations
Patients frequently present with exertional dyspnea, easy fatigability, weakness, and reduced exercise tolerance. Additional symptoms include exertional syncope, cough, hemoptysis, and exertional angina even in the absence of coronary artery disease. Anorexia, right upper quadrant discomfort, wheezing, hoarseness, and weight gain may occur as right-sided heart failure progresses. Signs of volume overload include hepatomegaly, ascites, and peripheral edema. In advanced disease, cardiogenic shock may develop, manifested by oliguria, cool extremities, and pulmonary edema resulting from interventricular septal displacement that impairs left ventricular diastolic filling.
History commonly reveals exercise intolerance, palpitations, chest pain, lightheadedness, syncope, and lower extremity swelling. Physical examination may show jugular venous distention with prominent A and V waves, increased chest diameter, crackles or wheezes on lung auscultation, and a left parasternal heave. Splitting of the second heart sound or murmurs related to pulmonary vasculature abnormalities may be present. A hepatojugular reflex, pulsatile liver, and pitting edema of the lower extremities are typical findings in advanced cases.
Diagnostic Evaluation
Pulse oximetry or arterial blood gas analysis typically demonstrates resting hypoxemia with arterial oxygen tensions of 40–60 mm Hg and resting carbon dioxide levels often between 40 and 70 mm Hg. Hematocrit is frequently elevated due to secondary polycythemia. Elevated B-type natriuretic peptide levels are sensitive for moderate to severe pulmonary hypertension and may independently predict mortality, although elevation alone is insufficient to establish the diagnosis of cor pulmonale. Other laboratory tests are generally of limited diagnostic value.
Chest radiography often reveals signs of pulmonary hypertension, including enlarged pulmonary arteries greater than 16–18 mm and an enlarged right ventricular silhouette. Although abnormalities are seen in more than 90% of patients, chest radiographs do not reliably indicate disease severity. Pleural effusions are not a feature of isolated cor pulmonale. Electrocardiography may demonstrate right-axis deviation, right bundle branch block, right ventricular hypertrophy with dominant R waves in leads V1 and V2, prominent S waves in leads V5 and V6, small R waves with deep S waves across the precordium, and right atrial enlargement with tall, peaked P waves consistent with P pulmonale. Acute cor pulmonale may show an S1Q3 pattern, transient hypoxia-related changes, and right precordial T-wave flattening.
Echocardiography is the preferred noninvasive diagnostic modality and may demonstrate right ventricular hypertrophy or dilation, tricuspid regurgitation, and Doppler-based estimation of pulmonary artery pressure and right ventricular ejection fraction. Chest computed tomography, ventilation–perfusion scanning, or pulmonary angiography are useful when acute cor pulmonale is suspected, particularly in cases of pulmonary embolism. Magnetic resonance imaging offers superior assessment of right ventricular size and function compared with echocardiography. Pulmonary function testing may reveal reduced diffusion capacity associated with pulmonary hypertension. Right-heart catheterization remains the most accurate method for assessing pulmonary vascular hemodynamics and provides precise measurements of pulmonary arterial and pulmonary capillary wedge pressures.
Differential Diagnosis
The differential diagnosis includes primary left-sided heart disease such as mitral stenosis, congenital heart disease including Eisenmenger syndrome with left-to-right shunting, hypothyroidism, and cirrhosis.
Management and Prehospital Care
Prehospital treatment is supportive and includes supplemental oxygen titrated to achieve arterial oxygen saturation of approximately 90%, establishment of intravenous access, continuous cardiac monitoring, and pulse oximetry. Bronchospasm related to underlying respiratory disease should be treated with beta-agonist nebulizers. Vasodilators and diuretics have no role in the prehospital setting. Patients with severe hypoxia may require endotracheal intubation.
Emergency Department Treatment
Management in the emergency department is directed at treating the underlying disease process and reducing pulmonary hypertension. Supplemental oxygen should be administered to raise arterial oxygen saturation to 90%, thereby reducing pulmonary vasoconstriction and right ventricular afterload while improving cardiac output and promoting diuresis. Careful monitoring of ventilation and carbon dioxide levels is essential, as hypercapnia may suppress respiratory drive and worsen acidosis. Diuretics such as furosemide may be used cautiously to reduce circulating blood volume and pulmonary artery pressure, with close attention to avoiding hypovolemia and electrolyte disturbances. Patients should be maintained on salt and fluid restriction. Digoxin has no role in the treatment of cor pulmonale.
Bronchodilator therapy is particularly beneficial in patients with COPD, as it reduces ventricular afterload and improves airflow. Selective beta-adrenergic agents such as subcutaneous terbutaline may be administered, and theophylline may be considered to enhance diaphragmatic contractility and reduce muscle fatigue. Anticoagulation should be considered in patients at high risk for thromboembolic disease. In acutely decompensated COPD, early initiation of corticosteroids and antibiotics is indicated. Improvement of the underlying respiratory disorder typically results in improved right ventricular function.
Medications
Furosemide may be administered at doses of 20–60 mg intravenously in adults, with pediatric dosing starting at 1 mg/kg and titrated as needed to a maximum of 6 mg/kg. Terbutaline may be administered at a dose of 0.25 mg subcutaneously.
Disposition and Follow-Up
Hospital admission is indicated for patients with new-onset hypoxia, anasarca, severe respiratory failure, or when required by the severity of the underlying disease. Patients without hypoxia or with stable oxygen requirements may be considered for discharge. Close outpatient follow-up is essential once the underlying etiology has responded to acute management, and evaluation for sleep apnea with a sleep study should be coordinated by the patient’s physician when indicated. Home oxygen therapy should be ensured for patients with chronic hypoxia.
Key Clinical Insights and Common Management Errors
Physical examination findings may be unreliable in patients with COPD because chest hyperinflation often obscures classic signs of cor pulmonale. Vasodilator therapy should be reserved for cases in which conventional management and adequate oxygenation have failed and should be used with caution.

