- Published on
Emergency and Acute Medicine – Acidosis
Overview and Definitions
Acidosis refers to physiologic processes that reduce blood pH and is broadly classified into respiratory acidosis and metabolic acidosis. Respiratory acidosis results from alveolar hypoventilation with retention of carbon dioxide, defined by a PaCO₂ greater than 45 mm Hg or higher than expected for appropriate respiratory compensation. Metabolic acidosis occurs when serum pH decreases due to a reduction in plasma bicarbonate, either from accumulation of acids or loss of bicarbonate from the body. Correct identification of the primary disorder and any mixed acid–base disturbances is essential in emergency care.
Respiratory Acidosis: Pathophysiology and Causes
Respiratory acidosis develops when ventilation is inadequate to eliminate carbon dioxide. Causes fall into three broad categories. The first is central nervous system depression, including sleep apnea, anesthesia, sedative or opioid overdose, CNS infections, or structural brain lesions. The second category involves impaired gas exchange at the alveolar level, such as in COPD, asthma, pneumonia, pulmonary edema, interstitial lung disease, obesity hypoventilation, or pulmonary contusion. The third category reflects failure of carbon dioxide transport from tissues to alveoli, as seen in severe heart failure or pulmonary edema. Neuromuscular disorders—including Guillain–Barré syndrome, myasthenia gravis, muscular dystrophy, spinal cord injury, or electrolyte abnormalities—may also impair ventilation. Upper airway obstruction, whether congenital, infectious, or foreign body–related, must also be considered.
Metabolic Acidosis: Classification and Mechanisms
Metabolic acidosis is classified based on the anion gap. In elevated anion gap metabolic acidosis, bicarbonate is consumed buffering excess strong acids, leaving unmeasured anions in circulation. Common causes are recalled with the mnemonic A CATPILES MUD, including lactic acidosis, ketoacidosis, renal failure (uremia), and toxic ingestions. Some causes are associated with an elevated osmolar gap, remembered by ME DIE, which suggests toxic alcohol exposure.
In normal anion gap (hyperchloremic) metabolic acidosis, bicarbonate is lost or not regenerated, without accumulation of unmeasured anions. This occurs with gastrointestinal bicarbonate losses (such as diarrhea or fistulas), renal tubular acidosis, or ingestion of substances that generate hydrochloric acid. Renal tubular acidosis is subdivided into distal (type I), proximal (type II), and type IV forms, each with characteristic bicarbonate and potassium abnormalities.
Clinical Presentation
Symptoms of acidosis are often nonspecific. Patients may present with tachypnea or deep, labored (Kussmaul) respirations in metabolic acidosis, or hypoventilation in respiratory acidosis. Additional findings include tachycardia, somnolence, confusion, altered mental status from hypercapnia, and cardiac conduction abnormalities or dysrhythmias, particularly with severe electrolyte derangements.
Essential Evaluation
Initial evaluation includes serum electrolytes, renal function, glucose, and arterial blood gases. Metabolic acidosis is suggested by a low bicarbonate level, while respiratory acidosis is characterized by carbon dioxide retention. Hyperkalemia and hypercalcemia may accompany severe metabolic acidosis. Carbon monoxide levels should be measured when exposure is suspected.
Calculation of the anion gap (Na⁺ − [Cl⁻ + HCO₃⁻]) is critical, with correction for hypoalbuminemia. The degree of compensation must be assessed by comparing expected versus observed PaCO₂ or bicarbonate levels. Failure of appropriate compensation suggests a mixed acid–base disorder.
Advanced Acid–Base Interpretation
In metabolic acidosis, expected PaCO₂ can be estimated using standard formulas. If measured PaCO₂ is higher than expected, concomitant respiratory acidosis or inadequate compensation is present. The delta gap helps identify mixed metabolic disorders by comparing changes in the anion gap with changes in bicarbonate concentration. Disproportionate changes indicate additional metabolic alkalosis or non–anion gap acidosis.
Diagnostic Testing
Arterial blood gas analysis remains the reference standard, though venous blood gas sampling may be useful in stable patients for screening. Urinalysis for glucose and ketones, serum lactate, ketone levels, and toxicology screening are obtained as indicated. Measurement of serum osmolality and calculation of the osmolar gap can suggest toxic alcohol ingestion, though a normal gap does not exclude this diagnosis. Imaging and ECG may help identify underlying cardiopulmonary or ischemic causes.
Management and Stabilization
Initial management focuses on airway, breathing, and circulation. Early intubation should be considered in severe metabolic acidosis when respiratory compensation is failing. Empiric administration of naloxone, dextrose, and thiamine is appropriate in patients with altered mental status.
Respiratory acidosis is managed by treating the underlying cause and providing ventilatory support when hypercapnia worsens. Metabolic acidosis requires identification and correction of the underlying etiology, such as diabetic ketoacidosis, lactic acidosis, or toxic ingestion, along with correction of electrolyte abnormalities and volume resuscitation. Hemodialysis may be necessary in select cases.
Disposition and Follow-Up
Patients with severe acidosis, altered mental status, respiratory failure, hemodynamic instability, significant electrolyte disturbances, or dysrhythmias generally require hospital admission, often to an intensive care setting. Discharge may be considered only when acidosis is resolving, the underlying cause is addressed, and close follow-up is ensured.
Clinical Pearls and Pitfalls
Mixed acid–base disorders are common and frequently missed. Normal pH does not exclude significant pathology if PaCO₂ and bicarbonate are both abnormal. Failure to recognize inadequate respiratory compensation in metabolic acidosis can delay lifesaving ventilatory support. Careful, systematic acid–base analysis is essential in emergency and acute care settings.
Overview and Definitions
Acidosis refers to physiologic processes that reduce blood pH and is broadly classified into respiratory acidosis and metabolic acidosis. Respiratory acidosis results from alveolar hypoventilation with retention of carbon dioxide, defined by a PaCO₂ greater than 45 mm Hg or higher than expected for appropriate respiratory compensation. Metabolic acidosis occurs when serum pH decreases due to a reduction in plasma bicarbonate, either from accumulation of acids or loss of bicarbonate from the body. Correct identification of the primary disorder and any mixed acid–base disturbances is essential in emergency care.
Respiratory Acidosis: Pathophysiology and Causes
Respiratory acidosis develops when ventilation is inadequate to eliminate carbon dioxide. Causes fall into three broad categories. The first is central nervous system depression, including sleep apnea, anesthesia, sedative or opioid overdose, CNS infections, or structural brain lesions. The second category involves impaired gas exchange at the alveolar level, such as in COPD, asthma, pneumonia, pulmonary edema, interstitial lung disease, obesity hypoventilation, or pulmonary contusion. The third category reflects failure of carbon dioxide transport from tissues to alveoli, as seen in severe heart failure or pulmonary edema. Neuromuscular disorders—including Guillain–Barré syndrome, myasthenia gravis, muscular dystrophy, spinal cord injury, or electrolyte abnormalities—may also impair ventilation. Upper airway obstruction, whether congenital, infectious, or foreign body–related, must also be considered.
Metabolic Acidosis: Classification and Mechanisms
Metabolic acidosis is classified based on the anion gap. In elevated anion gap metabolic acidosis, bicarbonate is consumed buffering excess strong acids, leaving unmeasured anions in circulation. Common causes are recalled with the mnemonic A CATPILES MUD, including lactic acidosis, ketoacidosis, renal failure (uremia), and toxic ingestions. Some causes are associated with an elevated osmolar gap, remembered by ME DIE, which suggests toxic alcohol exposure.
In normal anion gap (hyperchloremic) metabolic acidosis, bicarbonate is lost or not regenerated, without accumulation of unmeasured anions. This occurs with gastrointestinal bicarbonate losses (such as diarrhea or fistulas), renal tubular acidosis, or ingestion of substances that generate hydrochloric acid. Renal tubular acidosis is subdivided into distal (type I), proximal (type II), and type IV forms, each with characteristic bicarbonate and potassium abnormalities.
Clinical Presentation
Symptoms of acidosis are often nonspecific. Patients may present with tachypnea or deep, labored (Kussmaul) respirations in metabolic acidosis, or hypoventilation in respiratory acidosis. Additional findings include tachycardia, somnolence, confusion, altered mental status from hypercapnia, and cardiac conduction abnormalities or dysrhythmias, particularly with severe electrolyte derangements.
Essential Evaluation
Initial evaluation includes serum electrolytes, renal function, glucose, and arterial blood gases. Metabolic acidosis is suggested by a low bicarbonate level, while respiratory acidosis is characterized by carbon dioxide retention. Hyperkalemia and hypercalcemia may accompany severe metabolic acidosis. Carbon monoxide levels should be measured when exposure is suspected.
Calculation of the anion gap (Na⁺ − [Cl⁻ + HCO₃⁻]) is critical, with correction for hypoalbuminemia. The degree of compensation must be assessed by comparing expected versus observed PaCO₂ or bicarbonate levels. Failure of appropriate compensation suggests a mixed acid–base disorder.
Advanced Acid–Base Interpretation
In metabolic acidosis, expected PaCO₂ can be estimated using standard formulas. If measured PaCO₂ is higher than expected, concomitant respiratory acidosis or inadequate compensation is present. The delta gap helps identify mixed metabolic disorders by comparing changes in the anion gap with changes in bicarbonate concentration. Disproportionate changes indicate additional metabolic alkalosis or non–anion gap acidosis.
Diagnostic Testing
Arterial blood gas analysis remains the reference standard, though venous blood gas sampling may be useful in stable patients for screening. Urinalysis for glucose and ketones, serum lactate, ketone levels, and toxicology screening are obtained as indicated. Measurement of serum osmolality and calculation of the osmolar gap can suggest toxic alcohol ingestion, though a normal gap does not exclude this diagnosis. Imaging and ECG may help identify underlying cardiopulmonary or ischemic causes.
Management and Stabilization
Initial management focuses on airway, breathing, and circulation. Early intubation should be considered in severe metabolic acidosis when respiratory compensation is failing. Empiric administration of naloxone, dextrose, and thiamine is appropriate in patients with altered mental status.
Respiratory acidosis is managed by treating the underlying cause and providing ventilatory support when hypercapnia worsens. Metabolic acidosis requires identification and correction of the underlying etiology, such as diabetic ketoacidosis, lactic acidosis, or toxic ingestion, along with correction of electrolyte abnormalities and volume resuscitation. Hemodialysis may be necessary in select cases.
Disposition and Follow-Up
Patients with severe acidosis, altered mental status, respiratory failure, hemodynamic instability, significant electrolyte disturbances, or dysrhythmias generally require hospital admission, often to an intensive care setting. Discharge may be considered only when acidosis is resolving, the underlying cause is addressed, and close follow-up is ensured.
Clinical Pearls and Pitfalls
Mixed acid–base disorders are common and frequently missed. Normal pH does not exclude significant pathology if PaCO₂ and bicarbonate are both abnormal. Failure to recognize inadequate respiratory compensation in metabolic acidosis can delay lifesaving ventilatory support. Careful, systematic acid–base analysis is essential in emergency and acute care settings.
- Published on
Emergency and Acute Medicine – Acetaminophen (APAP) Poisoning
Overview and Pathophysiology
Acetaminophen is widely available as a single-agent analgesic, in combination with opioid medications, and as an ingredient in more than 200 over-the-counter cold and flu products. It is among the most common causes of both intentional and accidental poisoning and is the leading cause of acute liver failure requiring transplantation in the United States.
After ingestion, most acetaminophen is safely metabolized, but a small fraction is converted by the cytochrome P-450 system into N-acetyl-p-benzoquinoneimine (NAPQI), a highly toxic metabolite. Under normal conditions, NAPQI is neutralized by glutathione. In overdose, glutathione stores are rapidly depleted, allowing NAPQI to accumulate and cause hepatocellular injury. N-acetylcysteine (NAC) restores glutathione levels and prevents or limits liver damage. Patients with malnutrition are at higher risk because of reduced baseline glutathione reserves.
Pharmacokinetics and Toxic Thresholds
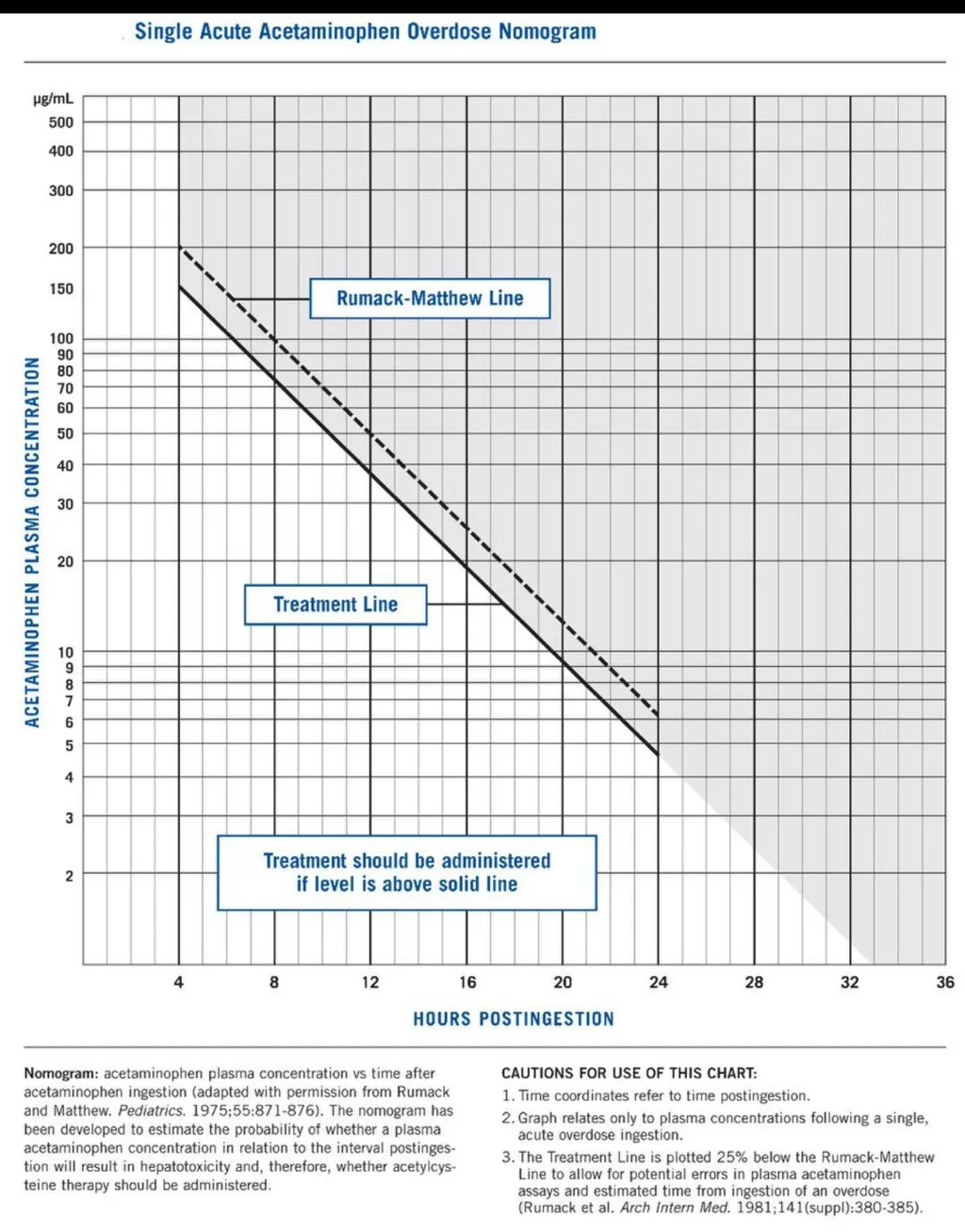
The normal acetaminophen half-life is approximately 2.5–4 hours but becomes prolonged in overdose, often exceeding 4 hours and indicating hepatic dysfunction. An acute ingestion greater than 150 mg/kg is potentially toxic. At 4 hours after ingestion, a serum acetaminophen level of 140 μg/mL or higher suggests toxicity, while therapeutic levels range from 5–20 μg/mL. The Rumack–Matthew nomogram is used to guide treatment decisions following a single, acute ingestion.
Clinical Course and Symptoms
Toxicity typically progresses through four stages.
Phase I (0.5–24 hours): Nausea, vomiting, and malaise may occur, particularly with large ingestions, though symptoms can be mild or absent early.
Phase II (24–72 hours): Gastrointestinal symptoms may improve, but liver injury evolves. Patients develop right upper quadrant pain, rising transaminases, prolonged PT/INR, elevated bilirubin, and sometimes oliguria.
Phase III (72–96 hours): This is the most critical period. Liver enzyme abnormalities peak, hepatic encephalopathy may appear, and worsening coagulopathy or renal failure signals a high likelihood of requiring liver transplantation.
Phase IV (96 hours to 10 days): Patients either recover with gradual hepatic regeneration or progress to fulminant liver failure.
Essential Evaluation
A careful history must identify all acetaminophen-containing products ingested and the timing of ingestion. A serum acetaminophen level should be obtained at 4 hours post-ingestion or immediately upon presentation if more than 4 hours have elapsed. The Rumack–Matthew nomogram applies only to single, acute ingestions and should not be used for chronic or delayed presentations. Early consultation with a poison center or toxicologist is strongly recommended.
Diagnostic Testing
Laboratory evaluation includes serum acetaminophen concentration, electrolytes, blood urea nitrogen, creatinine, glucose, liver enzymes (AST typically rises first), bilirubin, and PT/INR. Severe toxicity may result in AST/ALT levels exceeding 10,000 IU/L. A pregnancy test and toxicology screen should be obtained when appropriate.
Differential Diagnosis
Acetaminophen toxicity should always be considered as a co-ingestant in overdose. Other causes of acute liver injury include viral hepatitis, Reye syndrome, Amanita mushroom poisoning, herbal or dietary supplement toxicity, and other hepatotoxic drugs.
Initial Stabilization
Management begins with airway, breathing, and circulation assessment. Supplemental oxygen should be provided as needed. In patients with altered mental status, empiric administration of naloxone, thiamine, and dextrose (or bedside glucose testing) is appropriate.
Emergency Department Management
Supportive care includes intravenous fluids and antiemetics. A single dose of activated charcoal should be administered if the patient presents soon after ingestion.
N-acetylcysteine (NAC) is the cornerstone of therapy and is nearly 100% effective at preventing hepatotoxicity if started within 8 hours of acute overdose.
NAC Administration Options
Oral NAC has an unpleasant taste and odor and should be diluted to improve tolerability; antiemetics are often required. Vomited doses within one hour should be repeated, and persistent vomiting necessitates nasogastric or intravenous administration.
Intravenous NAC is given as a 21-hour infusion protocol. Oral NAC may be administered intravenously if the IV formulation is unavailable, with toxicology guidance.
Pregnancy Considerations
NAC is not teratogenic and crosses the placenta. Treating the mother effectively protects the fetus, particularly after 14 weeks’ gestation when fetal metabolism can produce toxic metabolites.
Disposition and Follow-Up
Admission is required for patients with hepatotoxic acetaminophen levels, abnormal liver tests, chronic ingestion with liver injury, or suicide attempts requiring psychiatric care.
Asymptomatic patients with non-toxic ingestions who do not require NAC may be discharged with counseling. Early hepatology or transplant consultation is warranted when significant liver injury is present. Patients with intentional overdose require psychiatric evaluation, while those with accidental poisoning need poison-prevention counseling.
Clinical Pearls and Pitfalls
Always consider occult acetaminophen exposure in patients presenting after opioid overdose or with unexplained liver injury. The Rumack–Matthew nomogram should not be used for chronic ingestion or late presentation. NAC should not be stopped until acetaminophen levels are undetectable and clinical and laboratory evidence of hepatotoxicity has improved or resolved.
Overview and Pathophysiology
Acetaminophen is widely available as a single-agent analgesic, in combination with opioid medications, and as an ingredient in more than 200 over-the-counter cold and flu products. It is among the most common causes of both intentional and accidental poisoning and is the leading cause of acute liver failure requiring transplantation in the United States.
After ingestion, most acetaminophen is safely metabolized, but a small fraction is converted by the cytochrome P-450 system into N-acetyl-p-benzoquinoneimine (NAPQI), a highly toxic metabolite. Under normal conditions, NAPQI is neutralized by glutathione. In overdose, glutathione stores are rapidly depleted, allowing NAPQI to accumulate and cause hepatocellular injury. N-acetylcysteine (NAC) restores glutathione levels and prevents or limits liver damage. Patients with malnutrition are at higher risk because of reduced baseline glutathione reserves.
Pharmacokinetics and Toxic Thresholds
The normal acetaminophen half-life is approximately 2.5–4 hours but becomes prolonged in overdose, often exceeding 4 hours and indicating hepatic dysfunction. An acute ingestion greater than 150 mg/kg is potentially toxic. At 4 hours after ingestion, a serum acetaminophen level of 140 μg/mL or higher suggests toxicity, while therapeutic levels range from 5–20 μg/mL. The Rumack–Matthew nomogram is used to guide treatment decisions following a single, acute ingestion.
Clinical Course and Symptoms
Toxicity typically progresses through four stages.
Phase I (0.5–24 hours): Nausea, vomiting, and malaise may occur, particularly with large ingestions, though symptoms can be mild or absent early.
Phase II (24–72 hours): Gastrointestinal symptoms may improve, but liver injury evolves. Patients develop right upper quadrant pain, rising transaminases, prolonged PT/INR, elevated bilirubin, and sometimes oliguria.
Phase III (72–96 hours): This is the most critical period. Liver enzyme abnormalities peak, hepatic encephalopathy may appear, and worsening coagulopathy or renal failure signals a high likelihood of requiring liver transplantation.
Phase IV (96 hours to 10 days): Patients either recover with gradual hepatic regeneration or progress to fulminant liver failure.
Essential Evaluation
A careful history must identify all acetaminophen-containing products ingested and the timing of ingestion. A serum acetaminophen level should be obtained at 4 hours post-ingestion or immediately upon presentation if more than 4 hours have elapsed. The Rumack–Matthew nomogram applies only to single, acute ingestions and should not be used for chronic or delayed presentations. Early consultation with a poison center or toxicologist is strongly recommended.
Diagnostic Testing
Laboratory evaluation includes serum acetaminophen concentration, electrolytes, blood urea nitrogen, creatinine, glucose, liver enzymes (AST typically rises first), bilirubin, and PT/INR. Severe toxicity may result in AST/ALT levels exceeding 10,000 IU/L. A pregnancy test and toxicology screen should be obtained when appropriate.
Differential Diagnosis
Acetaminophen toxicity should always be considered as a co-ingestant in overdose. Other causes of acute liver injury include viral hepatitis, Reye syndrome, Amanita mushroom poisoning, herbal or dietary supplement toxicity, and other hepatotoxic drugs.
Initial Stabilization
Management begins with airway, breathing, and circulation assessment. Supplemental oxygen should be provided as needed. In patients with altered mental status, empiric administration of naloxone, thiamine, and dextrose (or bedside glucose testing) is appropriate.
Emergency Department Management
Supportive care includes intravenous fluids and antiemetics. A single dose of activated charcoal should be administered if the patient presents soon after ingestion.
N-acetylcysteine (NAC) is the cornerstone of therapy and is nearly 100% effective at preventing hepatotoxicity if started within 8 hours of acute overdose.
- If the acetaminophen level cannot be obtained within 8 hours and toxicity is suspected, NAC should be started empirically and stopped if levels prove non-toxic.
- For presentations ≥8 hours after ingestion, NAC should be started immediately while awaiting laboratory confirmation.
- For late (>24 hours) or chronic ingestions, NAC is indicated if ingestion exceeds 150 mg/kg, symptoms are present, or liver tests are abnormal. Therapy may be discontinued once acetaminophen is undetectable and liver enzymes remain normal.
NAC Administration Options
Oral NAC has an unpleasant taste and odor and should be diluted to improve tolerability; antiemetics are often required. Vomited doses within one hour should be repeated, and persistent vomiting necessitates nasogastric or intravenous administration.
Intravenous NAC is given as a 21-hour infusion protocol. Oral NAC may be administered intravenously if the IV formulation is unavailable, with toxicology guidance.
Pregnancy Considerations
NAC is not teratogenic and crosses the placenta. Treating the mother effectively protects the fetus, particularly after 14 weeks’ gestation when fetal metabolism can produce toxic metabolites.
Disposition and Follow-Up
Admission is required for patients with hepatotoxic acetaminophen levels, abnormal liver tests, chronic ingestion with liver injury, or suicide attempts requiring psychiatric care.
Asymptomatic patients with non-toxic ingestions who do not require NAC may be discharged with counseling. Early hepatology or transplant consultation is warranted when significant liver injury is present. Patients with intentional overdose require psychiatric evaluation, while those with accidental poisoning need poison-prevention counseling.
Clinical Pearls and Pitfalls
Always consider occult acetaminophen exposure in patients presenting after opioid overdose or with unexplained liver injury. The Rumack–Matthew nomogram should not be used for chronic ingestion or late presentation. NAC should not be stopped until acetaminophen levels are undetectable and clinical and laboratory evidence of hepatotoxicity has improved or resolved.
- Published on
Emergency and Acute Medicine – Pediatric Abuse (Nonaccidental Trauma, NAT)
Overview and Scope
Pediatric abuse, also referred to as nonaccidental trauma (NAT), represents a major public health concern in the United States. It affects an estimated 2–3% of children annually, with millions impacted each year. Mortality from child maltreatment remains significant, with the majority of deaths occurring in children younger than five years, and infants accounting for a large proportion. All health care professionals are legally mandated reporters of suspected child abuse or neglect. Importantly, abuse occurs across all socioeconomic, cultural, and religious groups.
Risk Factors
Risk factors span the child, caregiver, and family environment. Children at highest risk are typically younger than four years, particularly infants, premature babies, multiples, and those with physical, developmental, or special health care needs.
Caregiver-related risk factors include a history of being abused, poor impulse control, violent behavior, mental illness, substance use, rigid or unrealistic expectations of the child, low self-esteem, and young parental age.
Family-level risk factors include financial stress, social isolation, frequent relocation, marital instability, unwanted pregnancy, and poor parent–child bonding.
Clinical Presentation and History
A hallmark of NAT is a history that is inconsistent with the reported injury or illness. Red flags include unexplained injury, apnea, ingestion, recurrent trauma, or death. Caregivers may be reluctant to provide information, deny knowledge of the injury, or offer changing or implausible explanations. Discrepancies between different caregivers are common.
In some cases, the described mechanism is developmentally impossible for the child. Delays in seeking medical care and inappropriate caregiver responses to the child’s condition are particularly concerning.
Failure to thrive may signal neglect, often related to inadequate caloric intake or impaired caregiver bonding. Munchausen syndrome by proxy should be considered in children with recurrent unexplained illness or suspicious metabolic abnormalities. Reviewing prior emergency department visits and communication with the primary care provider can reveal concerning patterns.
Physical Examination Findings
Physical findings often do not match the provided history. Cutaneous injuries are common and may include bruises with regular patterns, sharp demarcations, finger marks, slap marks, bite marks, burns from cigarettes or immersion (“stocking,” “glove,” or doughnut-shaped buttock burns), and injuries in unusual locations such as the buttocks, hips, face (excluding the forehead), back, thighs, genitalia, or pinna.
Bruises may be present at different stages of healing. While color alone is unreliable for precise dating, the presence of multiple injuries of varying age is suspicious.
Skeletal injuries are frequently multiple and unexplained, often in different stages of healing. Highly concerning findings include classic metaphyseal lesions, posterior rib fractures, fractures crossing suture lines, spiral fractures of long bones, subperiosteal new bone formation, and fractures of uncommon sites such as the scapula, sternum, vertebrae, or spinous processes without adequate mechanism.
Central Nervous System and Ocular Findings
Head injury is the leading cause of death in abused children. Findings may include altered mental status, seizures, skull fractures (particularly in children younger than one year), subdural or subarachnoid hemorrhage, and features consistent with shaken infant injury involving rotational and shearing forces.
Ocular findings are critical clues. Retinal hemorrhages—often bilateral—are present in the majority of abusive head injuries and are rare in accidental trauma without significant head injury. Additional findings may include hyphema, corneal abrasions, or conjunctival hemorrhage.
Abdominal, Genitourinary, and Sexual Abuse Findings
Abusive abdominal trauma may involve lacerations of solid organs, intramural bowel hematomas (especially duodenal), or retroperitoneal hemorrhage.
Anogenital findings such as contusions, erythema, lacerations, scarring, foreign material, sexually transmitted infections, or pregnancy in a child younger than twelve years strongly suggest sexual abuse. Unexplained death must always raise concern for NAT.
Essential Evaluation and Legal Responsibilities
When abuse is suspected, clinicians are legally required to make a formal oral and written report to the appropriate child protection agency. Certainty is not required—reasonable suspicion is sufficient.
Evaluation should include a thorough medical assessment, detailed documentation of findings, and photographic or diagrammatic recording of injuries when appropriate. Family, social, and environmental assessments are typically conducted in coordination with child welfare services.
Diagnostic Testing and Imaging
Laboratory studies are guided by presentation. A bleeding disorder screen is appropriate when bruising is prominent or recurrent. In cases of significant trauma, laboratory evaluation may include complete blood count, liver enzymes, pancreatic enzymes, and urinalysis. Toxicology and metabolic testing are indicated in children with altered mental status.
Imaging plays a central role. A full skeletal survey is recommended for children younger than two years and selectively for older children when abuse is strongly suspected. Additional imaging is obtained based on clinical findings, including abdominal CT for suspected visceral injury and neuroimaging for suspected head trauma. MRI serves as a valuable adjunct for detecting shear injury, evolving hemorrhage, and hypoxic-ischemic changes.
Differential Diagnosis
Conditions that may mimic abuse must be carefully considered, including accidental trauma, birth-related injuries, infections, dermatologic conditions, hematologic or oncologic disorders, bleeding diatheses, nutritional deficiencies, metabolic or genetic bone disease, cultural healing practices, intoxications, metabolic derangements, epilepsy, and sudden infant death syndromes. Differentiation relies on correlation of clinical findings with history, development, and investigative results.
Emergency Department Management
Medical stabilization and trauma care take priority. Clinicians must maintain a nonjudgmental approach while ensuring mandatory reporting and rapid involvement of child protection services. Communication with caregivers should emphasize concern for the child’s safety and well-being. Security may be required in some situations. All siblings and other children in the household must also be evaluated within an appropriate timeframe.
Disposition and Follow-Up
Admission is indicated for traumatic injuries requiring observation or intervention, or when safe disposition cannot be assured. Discharge is considered only after a complete evaluation, confirmation of a safe environment, and coordination with child welfare authorities. Many children require protective placement, including foster care, to prevent further harm.
Clinical Pearls and Pitfalls
A history that does not align with physical findings should immediately raise concern for nonaccidental trauma. When child abuse is suspected, reporting is mandatory and time-sensitive. The primary goal in all cases is ensuring the safety of the child and any siblings.
Overview and Scope
Pediatric abuse, also referred to as nonaccidental trauma (NAT), represents a major public health concern in the United States. It affects an estimated 2–3% of children annually, with millions impacted each year. Mortality from child maltreatment remains significant, with the majority of deaths occurring in children younger than five years, and infants accounting for a large proportion. All health care professionals are legally mandated reporters of suspected child abuse or neglect. Importantly, abuse occurs across all socioeconomic, cultural, and religious groups.
Risk Factors
Risk factors span the child, caregiver, and family environment. Children at highest risk are typically younger than four years, particularly infants, premature babies, multiples, and those with physical, developmental, or special health care needs.
Caregiver-related risk factors include a history of being abused, poor impulse control, violent behavior, mental illness, substance use, rigid or unrealistic expectations of the child, low self-esteem, and young parental age.
Family-level risk factors include financial stress, social isolation, frequent relocation, marital instability, unwanted pregnancy, and poor parent–child bonding.
Clinical Presentation and History
A hallmark of NAT is a history that is inconsistent with the reported injury or illness. Red flags include unexplained injury, apnea, ingestion, recurrent trauma, or death. Caregivers may be reluctant to provide information, deny knowledge of the injury, or offer changing or implausible explanations. Discrepancies between different caregivers are common.
In some cases, the described mechanism is developmentally impossible for the child. Delays in seeking medical care and inappropriate caregiver responses to the child’s condition are particularly concerning.
Failure to thrive may signal neglect, often related to inadequate caloric intake or impaired caregiver bonding. Munchausen syndrome by proxy should be considered in children with recurrent unexplained illness or suspicious metabolic abnormalities. Reviewing prior emergency department visits and communication with the primary care provider can reveal concerning patterns.
Physical Examination Findings
Physical findings often do not match the provided history. Cutaneous injuries are common and may include bruises with regular patterns, sharp demarcations, finger marks, slap marks, bite marks, burns from cigarettes or immersion (“stocking,” “glove,” or doughnut-shaped buttock burns), and injuries in unusual locations such as the buttocks, hips, face (excluding the forehead), back, thighs, genitalia, or pinna.
Bruises may be present at different stages of healing. While color alone is unreliable for precise dating, the presence of multiple injuries of varying age is suspicious.
Skeletal injuries are frequently multiple and unexplained, often in different stages of healing. Highly concerning findings include classic metaphyseal lesions, posterior rib fractures, fractures crossing suture lines, spiral fractures of long bones, subperiosteal new bone formation, and fractures of uncommon sites such as the scapula, sternum, vertebrae, or spinous processes without adequate mechanism.
Central Nervous System and Ocular Findings
Head injury is the leading cause of death in abused children. Findings may include altered mental status, seizures, skull fractures (particularly in children younger than one year), subdural or subarachnoid hemorrhage, and features consistent with shaken infant injury involving rotational and shearing forces.
Ocular findings are critical clues. Retinal hemorrhages—often bilateral—are present in the majority of abusive head injuries and are rare in accidental trauma without significant head injury. Additional findings may include hyphema, corneal abrasions, or conjunctival hemorrhage.
Abdominal, Genitourinary, and Sexual Abuse Findings
Abusive abdominal trauma may involve lacerations of solid organs, intramural bowel hematomas (especially duodenal), or retroperitoneal hemorrhage.
Anogenital findings such as contusions, erythema, lacerations, scarring, foreign material, sexually transmitted infections, or pregnancy in a child younger than twelve years strongly suggest sexual abuse. Unexplained death must always raise concern for NAT.
Essential Evaluation and Legal Responsibilities
When abuse is suspected, clinicians are legally required to make a formal oral and written report to the appropriate child protection agency. Certainty is not required—reasonable suspicion is sufficient.
Evaluation should include a thorough medical assessment, detailed documentation of findings, and photographic or diagrammatic recording of injuries when appropriate. Family, social, and environmental assessments are typically conducted in coordination with child welfare services.
Diagnostic Testing and Imaging
Laboratory studies are guided by presentation. A bleeding disorder screen is appropriate when bruising is prominent or recurrent. In cases of significant trauma, laboratory evaluation may include complete blood count, liver enzymes, pancreatic enzymes, and urinalysis. Toxicology and metabolic testing are indicated in children with altered mental status.
Imaging plays a central role. A full skeletal survey is recommended for children younger than two years and selectively for older children when abuse is strongly suspected. Additional imaging is obtained based on clinical findings, including abdominal CT for suspected visceral injury and neuroimaging for suspected head trauma. MRI serves as a valuable adjunct for detecting shear injury, evolving hemorrhage, and hypoxic-ischemic changes.
Differential Diagnosis
Conditions that may mimic abuse must be carefully considered, including accidental trauma, birth-related injuries, infections, dermatologic conditions, hematologic or oncologic disorders, bleeding diatheses, nutritional deficiencies, metabolic or genetic bone disease, cultural healing practices, intoxications, metabolic derangements, epilepsy, and sudden infant death syndromes. Differentiation relies on correlation of clinical findings with history, development, and investigative results.
Emergency Department Management
Medical stabilization and trauma care take priority. Clinicians must maintain a nonjudgmental approach while ensuring mandatory reporting and rapid involvement of child protection services. Communication with caregivers should emphasize concern for the child’s safety and well-being. Security may be required in some situations. All siblings and other children in the household must also be evaluated within an appropriate timeframe.
Disposition and Follow-Up
Admission is indicated for traumatic injuries requiring observation or intervention, or when safe disposition cannot be assured. Discharge is considered only after a complete evaluation, confirmation of a safe environment, and coordination with child welfare authorities. Many children require protective placement, including foster care, to prevent further harm.
Clinical Pearls and Pitfalls
A history that does not align with physical findings should immediately raise concern for nonaccidental trauma. When child abuse is suspected, reporting is mandatory and time-sensitive. The primary goal in all cases is ensuring the safety of the child and any siblings.
- Published on
Emergency and Acute Medicine – Elder Abuse
Overview and Definition
Elder abuse encompasses a spectrum of harmful behaviors directed toward older adults, typically by individuals on whom they depend for care or support. Abuse may be emotional, including insults, humiliation, threats of abandonment, or institutionalization. Physical and sexual abuse involves acts such as hitting, slapping, pushing, burning, inappropriate restraint, or forced sexual activity. Material or financial exploitation includes theft, coercion, or misuse of an elder’s money or property. Neglect refers to acts or omissions by a caregiver or the patient that compromise health or safety, including failure to provide adequate nutrition, shelter, hygiene, or medical care.
Epidemiology and Impact
In the United States, an estimated 1–2 million adults aged 65 years or older are mistreated annually, a figure expected to rise as the population ages. Neglect accounts for the majority of cases, followed by physical mistreatment, financial exploitation, and emotional abuse; sexual abuse is reported less frequently. Family members—most often spouses or adult children—are responsible in approximately 90% of cases. Financial exploitation is particularly underreported, with many cases never reaching authorities. Even mild forms of abuse are associated with a markedly increased risk of mortality and higher rates of chronic pain, musculoskeletal, gastrointestinal, and psychological disorders.
Etiology and Risk Factors
Abuse often arises from caregiver stress, dependency, mental illness, substance use, or financial reliance on the elder. Victim-related factors include physical or cognitive impairment, dependence for activities of daily living, and social isolation, all of which increase vulnerability.
Clinical Presentation
Presentations are highly variable and may be subtle. Histories may be inconsistent, vague, or implausible, and discrepancies may exist between accounts provided by the patient and caregiver. Red flags include delays in seeking medical care, previously untreated conditions, inability or unwillingness to meet basic needs, and medication mismanagement such as incorrect dosing, missing prescriptions, or unfilled medications. Behavioral changes in the elder—withdrawal, fearfulness, demoralization, or substance use—may be evident. Concerning caregiver behaviors include controlling interactions, refusal to leave the patient alone with clinicians, poor knowledge of the patient’s condition, or evidence of significant psychosocial stressors.
Physical Examination Findings
Examination may reveal injuries inconsistent with the reported mechanism or injuries at different stages of healing. Suspicious findings include bruises, burns, lacerations, or abrasions in unusual locations such as the inner arms, torso, buttocks, scalp, or genital and rectal areas. Lesions on wrists or ankles may suggest restraint use. Signs of neglect include poor hygiene, dehydration, weight loss, malnutrition, and pressure ulcers.
Essential Evaluation
Assessment should prioritize patient safety and confidentiality. History should be obtained without caregivers present, as many abused elders fear retaliation, institutionalization, or feel shame or responsibility for the abuse. Clinicians should ask directly but sensitively about mistreatment or neglect. Information from caregivers, relatives, friends, or neighbors may provide important context.
Detailed documentation is critical and should include verbatim patient statements, psychosocial history, caregiver dynamics, substance use, prior involvement of adult protective services, and thorough descriptions of physical findings. Photographic documentation of injuries, when appropriate, can be invaluable. A structured safety assessment is essential.
Diagnostic Testing
Laboratory studies, imaging, and procedures should be guided by the patient’s medical condition and suspected injuries. There are no specific tests that diagnose abuse; rather, diagnosis relies on correlation of clinical findings, risk factors, and patient disclosure.
Differential Diagnosis
Elder abuse can present with any chief complaint. Clinicians must distinguish abuse or neglect from medical conditions that may mimic it, such as dehydration, poorly fitting dentures, burns from accidents, ecchymoses related to anticoagulation, insomnia, medication nonadherence, dementia, or depression.
Prehospital Considerations
Emergency medical personnel may observe critical environmental and interpersonal details, including unsafe living conditions, evidence of neglect, or fearful interactions between the elder and caregiver, which should be communicated to the receiving team.
Emergency Department Management
Initial care follows standard priorities, addressing airway, breathing, circulation, and any life-threatening medical or traumatic conditions. Separation of the patient from caregivers may be necessary to allow safe evaluation. Early involvement of social work is essential for safety planning, caregiver respite, and coordination with community resources. Adult protective services should be notified when abuse or neglect is suspected, in accordance with local laws.
Competent elders retain the right to accept or decline treatment or disposition, even when risks remain, underscoring the importance of clear communication and documentation.
Disposition and Follow-Up
Admission is indicated when medical conditions require inpatient care, when the home environment is unsafe, or when additional time is needed to clarify concerns and coordinate protection. Discharge may be considered only after medical issues are addressed and a safe environment is assured through social services or legal intervention.
Many jurisdictions mandate reporting of suspected elder abuse; clinicians must comply with local regulations. Referral for substance use treatment, mental health services, or caregiver support may be appropriate.
Clinical Pearls and Pitfalls
Elder abuse is common, underrecognized, and associated with high morbidity and mortality. Diagnosis often depends on asking directly in a private setting and recognizing subtle patterns rather than relying on a single finding. Failure to separate the patient from caregivers or to document thoroughly can result in missed opportunities for protection and intervention.
Overview and Definition
Elder abuse encompasses a spectrum of harmful behaviors directed toward older adults, typically by individuals on whom they depend for care or support. Abuse may be emotional, including insults, humiliation, threats of abandonment, or institutionalization. Physical and sexual abuse involves acts such as hitting, slapping, pushing, burning, inappropriate restraint, or forced sexual activity. Material or financial exploitation includes theft, coercion, or misuse of an elder’s money or property. Neglect refers to acts or omissions by a caregiver or the patient that compromise health or safety, including failure to provide adequate nutrition, shelter, hygiene, or medical care.
Epidemiology and Impact
In the United States, an estimated 1–2 million adults aged 65 years or older are mistreated annually, a figure expected to rise as the population ages. Neglect accounts for the majority of cases, followed by physical mistreatment, financial exploitation, and emotional abuse; sexual abuse is reported less frequently. Family members—most often spouses or adult children—are responsible in approximately 90% of cases. Financial exploitation is particularly underreported, with many cases never reaching authorities. Even mild forms of abuse are associated with a markedly increased risk of mortality and higher rates of chronic pain, musculoskeletal, gastrointestinal, and psychological disorders.
Etiology and Risk Factors
Abuse often arises from caregiver stress, dependency, mental illness, substance use, or financial reliance on the elder. Victim-related factors include physical or cognitive impairment, dependence for activities of daily living, and social isolation, all of which increase vulnerability.
Clinical Presentation
Presentations are highly variable and may be subtle. Histories may be inconsistent, vague, or implausible, and discrepancies may exist between accounts provided by the patient and caregiver. Red flags include delays in seeking medical care, previously untreated conditions, inability or unwillingness to meet basic needs, and medication mismanagement such as incorrect dosing, missing prescriptions, or unfilled medications. Behavioral changes in the elder—withdrawal, fearfulness, demoralization, or substance use—may be evident. Concerning caregiver behaviors include controlling interactions, refusal to leave the patient alone with clinicians, poor knowledge of the patient’s condition, or evidence of significant psychosocial stressors.
Physical Examination Findings
Examination may reveal injuries inconsistent with the reported mechanism or injuries at different stages of healing. Suspicious findings include bruises, burns, lacerations, or abrasions in unusual locations such as the inner arms, torso, buttocks, scalp, or genital and rectal areas. Lesions on wrists or ankles may suggest restraint use. Signs of neglect include poor hygiene, dehydration, weight loss, malnutrition, and pressure ulcers.
Essential Evaluation
Assessment should prioritize patient safety and confidentiality. History should be obtained without caregivers present, as many abused elders fear retaliation, institutionalization, or feel shame or responsibility for the abuse. Clinicians should ask directly but sensitively about mistreatment or neglect. Information from caregivers, relatives, friends, or neighbors may provide important context.
Detailed documentation is critical and should include verbatim patient statements, psychosocial history, caregiver dynamics, substance use, prior involvement of adult protective services, and thorough descriptions of physical findings. Photographic documentation of injuries, when appropriate, can be invaluable. A structured safety assessment is essential.
Diagnostic Testing
Laboratory studies, imaging, and procedures should be guided by the patient’s medical condition and suspected injuries. There are no specific tests that diagnose abuse; rather, diagnosis relies on correlation of clinical findings, risk factors, and patient disclosure.
Differential Diagnosis
Elder abuse can present with any chief complaint. Clinicians must distinguish abuse or neglect from medical conditions that may mimic it, such as dehydration, poorly fitting dentures, burns from accidents, ecchymoses related to anticoagulation, insomnia, medication nonadherence, dementia, or depression.
Prehospital Considerations
Emergency medical personnel may observe critical environmental and interpersonal details, including unsafe living conditions, evidence of neglect, or fearful interactions between the elder and caregiver, which should be communicated to the receiving team.
Emergency Department Management
Initial care follows standard priorities, addressing airway, breathing, circulation, and any life-threatening medical or traumatic conditions. Separation of the patient from caregivers may be necessary to allow safe evaluation. Early involvement of social work is essential for safety planning, caregiver respite, and coordination with community resources. Adult protective services should be notified when abuse or neglect is suspected, in accordance with local laws.
Competent elders retain the right to accept or decline treatment or disposition, even when risks remain, underscoring the importance of clear communication and documentation.
Disposition and Follow-Up
Admission is indicated when medical conditions require inpatient care, when the home environment is unsafe, or when additional time is needed to clarify concerns and coordinate protection. Discharge may be considered only after medical issues are addressed and a safe environment is assured through social services or legal intervention.
Many jurisdictions mandate reporting of suspected elder abuse; clinicians must comply with local regulations. Referral for substance use treatment, mental health services, or caregiver support may be appropriate.
Clinical Pearls and Pitfalls
Elder abuse is common, underrecognized, and associated with high morbidity and mortality. Diagnosis often depends on asking directly in a private setting and recognizing subtle patterns rather than relying on a single finding. Failure to separate the patient from caregivers or to document thoroughly can result in missed opportunities for protection and intervention.

- Published on
Emergency and Acute Medicine – Skin and Soft Tissue Abscess
Overview and Definition
A skin or soft tissue abscess is a localized collection of pus that is encapsulated by inflamed tissue. Abscesses may develop anywhere on the body and vary widely in size, depth, and microbiology depending on location and patient risk factors. Variants include furuncles, which originate from infected hair follicles and commonly affect the back, axillae, and lower extremities, and carbuncles, which are larger, deeper, and more extensive infections.
Special anatomic locations have distinct considerations. Mammalian bites are typically polymicrobial. Breast abscesses may occur during lactation (puerperal) or due to duct ectasia, with differing microbial patterns. Hidradenitis suppurativa involves chronic abscess formation in apocrine gland–bearing areas such as the groin and scalp. Pilonidal abscesses arise from epithelial disruption in the gluteal cleft, while Bartholin abscesses result from duct obstruction. Perirectal abscesses originate from anal crypts and frequently require operative management. Other important entities include pyomyositis, abscesses related to IV drug use, paronychia, and felons of the distal finger pulp.
Etiology and Risk Factors
Abscess formation usually follows a break in the skin, obstruction of sebaceous or sweat glands, or inflammation of hair follicles. Most abscesses are bacterial, with microbiology reflecting local skin flora. Staphylococcus aureus is the most common pathogen, and community-acquired MRSA is frequently implicated.
Some abscesses may be sterile, particularly in individuals who inject chemical irritants intravenously. Risk factors include immunosuppression, soft tissue trauma, mammalian or human bites, tissue ischemia, IV drug use, and inflammatory bowel disease, particularly in perirectal infections.
Clinical Presentation
Local findings typically include erythema, warmth, swelling, tenderness, and fluctuance. Surrounding cellulitis is common, and regional lymphadenopathy or lymphangitis may occur. Systemic symptoms are often absent in uncomplicated cases. However, patients with extensive infection, necrotizing soft tissue involvement, or bacteremia may present with fever, rigors, hypotension, or altered mental status, indicating sepsis.
History and Physical Examination
History should address prior abscesses, which raise suspicion for MRSA, as well as immunosuppression, medication use (such as chronic steroids or chemotherapy), IV drug use, and recent animal or human bites.
Physical examination focuses on defining the location, size, and depth of infection and identifying associated cellulitis, subcutaneous air, or involvement of deep structures. Abscesses involving high-risk areas—such as the face, neck, hands, feet, perirectal region, or genitalia—require heightened caution and often specialty consultation.
Essential Workup
Diagnosis is primarily clinical. Gram stain and routine cultures are not necessary for simple abscesses in otherwise healthy individuals. Wound cultures may be useful when systemic antibiotics are planned, in recurrent infections to document MRSA, in immunocompromised hosts, in abscesses involving the face or hand, or when initial therapy fails.
Diagnostic Testing
Routine laboratory testing is generally unnecessary. Blood glucose measurement may be helpful when undiagnosed diabetes or diabetic ketoacidosis is suspected. In febrile or systemically ill patients, or those with recent IV drug use, blood cultures, lactate, renal function tests, and creatine kinase (if myositis is suspected) are appropriate.
Bedside ultrasound is valuable for differentiating cellulitis from abscess. CT or MRI may be needed to assess deep tissue involvement, while plain radiographs can detect gas in tissue planes.
Differential Diagnosis
Conditions that may mimic abscess include cellulitis, necrotizing fasciitis, hematoma, cysts, and aneurysm, particularly in IV drug users.
Initial Stabilization
Patients with signs of sepsis require prompt IV access, oxygen, crystalloid resuscitation, blood cultures, lactate measurement, and early broad-spectrum antibiotics with MRSA coverage. Rapid source control through drainage is essential.
Definitive Management
Incision and drainage is the cornerstone of abscess treatment. The incision must be sufficiently deep to allow complete evacuation, and elliptical incisions help prevent premature closure. Loculations should be gently broken up, and the cavity irrigated thoroughly.
Loose packing is recommended for abscesses larger than 5 cm, in patients with significant comorbidities, or when abscesses involve high-risk locations. For small, uncomplicated abscesses, routine packing is not always necessary.
Routine antibiotics are not required after drainage of uncomplicated abscesses. Antibiotic therapy is indicated in cases of systemic illness, significant cellulitis, facial abscesses with risk of cavernous sinus drainage, mammalian bites, immunocompromised patients, and perirectal abscesses, which generally require operative management.
The loop drainage technique offers a less invasive alternative that facilitates ongoing drainage, simplifies wound care, and often avoids repeat emergency department visits.
Pediatric Considerations
Incision and drainage are painful procedures in children and frequently require procedural sedation and adequate analgesia.
Antibiotic Therapy
Antibiotic selection should be guided by local resistance patterns. Oral agents are used for moderate associated cellulitis, while intravenous antibiotics are reserved for systemic illness or extensive infection. MRSA-active agents are commonly required, and broader coverage is necessary for bites or facial infections.
Disposition and Follow-Up
Admission is indicated for patients with sepsis, immunocompromised status with significant cellulitis, perirectal involvement, or abscesses requiring operative debridement.
Most patients with uncomplicated abscesses can be discharged after incision and drainage with close outpatient follow-up.
Follow-Up Care
Patients should return in 24–48 hours for wound reassessment and packing removal if used. Warm soaks are recommended for several days after packing removal to promote continued drainage.
Clinical Pearls and Pitfalls
Recurrent abscesses should prompt consideration of community-acquired MRSA. Adequate pain control is essential during drainage procedures. Always assess for deeper infections such as tenosynovitis or deep fascial space involvement, particularly in hand infections.
Overview and Definition
A skin or soft tissue abscess is a localized collection of pus that is encapsulated by inflamed tissue. Abscesses may develop anywhere on the body and vary widely in size, depth, and microbiology depending on location and patient risk factors. Variants include furuncles, which originate from infected hair follicles and commonly affect the back, axillae, and lower extremities, and carbuncles, which are larger, deeper, and more extensive infections.
Special anatomic locations have distinct considerations. Mammalian bites are typically polymicrobial. Breast abscesses may occur during lactation (puerperal) or due to duct ectasia, with differing microbial patterns. Hidradenitis suppurativa involves chronic abscess formation in apocrine gland–bearing areas such as the groin and scalp. Pilonidal abscesses arise from epithelial disruption in the gluteal cleft, while Bartholin abscesses result from duct obstruction. Perirectal abscesses originate from anal crypts and frequently require operative management. Other important entities include pyomyositis, abscesses related to IV drug use, paronychia, and felons of the distal finger pulp.
Etiology and Risk Factors
Abscess formation usually follows a break in the skin, obstruction of sebaceous or sweat glands, or inflammation of hair follicles. Most abscesses are bacterial, with microbiology reflecting local skin flora. Staphylococcus aureus is the most common pathogen, and community-acquired MRSA is frequently implicated.
Some abscesses may be sterile, particularly in individuals who inject chemical irritants intravenously. Risk factors include immunosuppression, soft tissue trauma, mammalian or human bites, tissue ischemia, IV drug use, and inflammatory bowel disease, particularly in perirectal infections.
Clinical Presentation
Local findings typically include erythema, warmth, swelling, tenderness, and fluctuance. Surrounding cellulitis is common, and regional lymphadenopathy or lymphangitis may occur. Systemic symptoms are often absent in uncomplicated cases. However, patients with extensive infection, necrotizing soft tissue involvement, or bacteremia may present with fever, rigors, hypotension, or altered mental status, indicating sepsis.
History and Physical Examination
History should address prior abscesses, which raise suspicion for MRSA, as well as immunosuppression, medication use (such as chronic steroids or chemotherapy), IV drug use, and recent animal or human bites.
Physical examination focuses on defining the location, size, and depth of infection and identifying associated cellulitis, subcutaneous air, or involvement of deep structures. Abscesses involving high-risk areas—such as the face, neck, hands, feet, perirectal region, or genitalia—require heightened caution and often specialty consultation.
Essential Workup
Diagnosis is primarily clinical. Gram stain and routine cultures are not necessary for simple abscesses in otherwise healthy individuals. Wound cultures may be useful when systemic antibiotics are planned, in recurrent infections to document MRSA, in immunocompromised hosts, in abscesses involving the face or hand, or when initial therapy fails.
Diagnostic Testing
Routine laboratory testing is generally unnecessary. Blood glucose measurement may be helpful when undiagnosed diabetes or diabetic ketoacidosis is suspected. In febrile or systemically ill patients, or those with recent IV drug use, blood cultures, lactate, renal function tests, and creatine kinase (if myositis is suspected) are appropriate.
Bedside ultrasound is valuable for differentiating cellulitis from abscess. CT or MRI may be needed to assess deep tissue involvement, while plain radiographs can detect gas in tissue planes.
Differential Diagnosis
Conditions that may mimic abscess include cellulitis, necrotizing fasciitis, hematoma, cysts, and aneurysm, particularly in IV drug users.
Initial Stabilization
Patients with signs of sepsis require prompt IV access, oxygen, crystalloid resuscitation, blood cultures, lactate measurement, and early broad-spectrum antibiotics with MRSA coverage. Rapid source control through drainage is essential.
Definitive Management
Incision and drainage is the cornerstone of abscess treatment. The incision must be sufficiently deep to allow complete evacuation, and elliptical incisions help prevent premature closure. Loculations should be gently broken up, and the cavity irrigated thoroughly.
Loose packing is recommended for abscesses larger than 5 cm, in patients with significant comorbidities, or when abscesses involve high-risk locations. For small, uncomplicated abscesses, routine packing is not always necessary.
Routine antibiotics are not required after drainage of uncomplicated abscesses. Antibiotic therapy is indicated in cases of systemic illness, significant cellulitis, facial abscesses with risk of cavernous sinus drainage, mammalian bites, immunocompromised patients, and perirectal abscesses, which generally require operative management.
The loop drainage technique offers a less invasive alternative that facilitates ongoing drainage, simplifies wound care, and often avoids repeat emergency department visits.
Pediatric Considerations
Incision and drainage are painful procedures in children and frequently require procedural sedation and adequate analgesia.
Antibiotic Therapy
Antibiotic selection should be guided by local resistance patterns. Oral agents are used for moderate associated cellulitis, while intravenous antibiotics are reserved for systemic illness or extensive infection. MRSA-active agents are commonly required, and broader coverage is necessary for bites or facial infections.
Disposition and Follow-Up
Admission is indicated for patients with sepsis, immunocompromised status with significant cellulitis, perirectal involvement, or abscesses requiring operative debridement.
Most patients with uncomplicated abscesses can be discharged after incision and drainage with close outpatient follow-up.
Follow-Up Care
Patients should return in 24–48 hours for wound reassessment and packing removal if used. Warm soaks are recommended for several days after packing removal to promote continued drainage.
Clinical Pearls and Pitfalls
Recurrent abscesses should prompt consideration of community-acquired MRSA. Adequate pain control is essential during drainage procedures. Always assess for deeper infections such as tenosynovitis or deep fascial space involvement, particularly in hand infections.
- Published on
Emergency and Acute Medicine – Imaging in Abdominal Trauma
Overview
Imaging plays a central role in the evaluation of abdominal trauma and must be guided by the patient’s history, physical examination, and—most importantly—hemodynamic status. Abdominal trauma occurs across a broad spectrum, ranging from isolated abdominal injury to severe multisystem trauma. Injuries are categorized as blunt or penetrating, with penetrating trauma further subdivided into stab wounds and gunshot wounds. Hemodynamic stability is the key determinant in selecting appropriate imaging and procedural strategies. Unstable patients generally require rapid surgical decision-making, whereas many stable patients can be managed nonoperatively with careful imaging and observation.
Clinical Assessment
History should focus on the mechanism of injury, use of restraints, airbags or helmets, prehospital vital signs, mental status at the scene, and any change in mental status. A complete AMPLE history is essential, including allergies (especially to medications or contrast), current medications, past medical and surgical history, last oral intake, and events leading up to the injury.
Physical examination begins with an ABCDE survey (Airway, Breathing, Circulation, Disability, Exposure), followed by full exposure of the patient and careful palpation of all abdominal quadrants. Abdominal injury is identified in only about half of trauma patients, and the physical exam may be unreliable in intoxicated, uncooperative, or multisystem trauma patients.
General Imaging Strategy
All trauma patients are initially managed using the ABCDE approach. Imaging decisions are then tailored according to stability.
Unstable Trauma Patients
Hemodynamically unstable patients should undergo immediate bedside ultrasonography as part of the primary survey. A positive FAST examination strongly suggests intra-abdominal bleeding as the cause of hypotension. A negative FAST raises concern for alternative bleeding sources, including retroperitoneal hemorrhage, pelvic fractures, thoracic bleeding, or significant blood loss prior to arrival. Surgical consultation should be obtained immediately to prepare for definitive operative management.
Stable Trauma Patients
In stable patients, three principal diagnostic modalities are used to define the extent of abdominal injury.
Ultrasound is often the initial screening test. A positive study in a stable patient raises concern for potential deterioration and should prompt rapid CT imaging and surgical consultation.
CT scanning is the definitive diagnostic tool in stable abdominal trauma. It provides superior detection of solid organ and retroperitoneal injuries compared with ultrasound and helps determine whether nonoperative management or interventional radiology techniques, such as embolization, are appropriate. CT is indicated in all stable patients with stab wounds and in patients with gross hematuria to evaluate for renal injury.
Diagnostic peritoneal lavage is now infrequently used, having largely been replaced by ultrasound and CT.
Laboratory Evaluation
Initial laboratory studies include blood type and screen, complete blood count, electrolytes, creatinine, lipase, urinalysis, and electrocardiography when indicated. These tests support imaging findings and assist in identifying associated injuries or complications.
Ultrasound (FAST Examination)
The FAST exam evaluates dependent intraperitoneal spaces where free fluid accumulates, including the hepatorenal recess (Morison pouch), splenorenal space, suprapubic region, and pericardium.
Advantages include rapid bedside performance, noninvasiveness, lack of radiation or contrast, and repeatability during resuscitation.
Limitations include operator dependence and poor sensitivity for solid organ parenchymal injuries, retroperitoneal bleeding, bowel injury, and hemorrhage associated with pelvic fractures.
A positive study is defined by visualization of free fluid or obvious organ injury. Adequate evaluation requires views of the right upper quadrant, left upper quadrant, pelvis, and heart.
Computed Tomography (CT)
CT scanning has a sensitivity of approximately 85–98% for abdominal trauma and provides detailed anatomic information about organ injury. It supports nonoperative management strategies and allows evaluation of the spine and adjacent structures.
Disadvantages include cost, radiation exposure, and the need for intravenous contrast, which carries a risk of allergic reaction and nephrotoxicity. Certain injuries—such as isolated diaphragmatic, pancreatic, or bowel injuries—may be missed early after trauma.
CT is indicated in hemodynamically stable patients and is contraindicated in unstable patients or those who already require emergent laparotomy. Many centers now use a “pan-scan” approach in multisystem trauma, though this increases cumulative radiation exposure.
Angiography
Angiography is useful for identifying and embolizing bleeding vessels, particularly in patients with pelvic fractures or solid organ hemorrhage. It may be used in selected unstable patients when surgical control is not immediately feasible.
Diagnostic Peritoneal Lavage (DPL)
DPL is invasive but highly sensitive for detecting intra-abdominal bleeding, mesenteric injury, and hollow viscus injury. It is now reserved for select situations, such as unstable patients with equivocal ultrasound findings or those requiring emergent surgery for another indication.
A positive test includes aspiration of blood, bile, bowel contents, or urine, or elevated red blood cell counts depending on the mechanism of injury. Contraindications include clear indications for laparotomy, and relative contraindications include prior abdominal surgery, pregnancy, and pediatric patients.
Disposition and Follow-Up
All unstable trauma patients require admission and frequently operative management. Most patients with multisystem trauma and abdominal involvement should be admitted. Pregnant patients beyond 24 weeks’ gestation require hospital admission for fetal–maternal monitoring.
Stable patients may be discharged only after a negative evaluation, sustained hemodynamic stability, and assurance of reliable follow-up and access to emergency care.
Discharge Advice and Safety Netting
Patients discharged after abdominal trauma must be instructed to return immediately for worsening abdominal pain, distention, vomiting, rectal bleeding, or any new concerning symptoms, as intestinal and pancreatic injuries may present late.
Clinical Pearls and Pitfalls
Bedside ultrasound can be performed immediately during resuscitation and repeated if clinical status changes. Increasing reliance on CT has reduced missed injuries but also increased radiation exposure and lifetime cancer risk. Diagnostic peritoneal lavage and local wound exploration are now less commonly used. Common pitfalls include failure to obtain early blood typing and pregnancy testing, and discharging pregnant patients beyond 24 weeks without appropriate monitoring.
Overview
Imaging plays a central role in the evaluation of abdominal trauma and must be guided by the patient’s history, physical examination, and—most importantly—hemodynamic status. Abdominal trauma occurs across a broad spectrum, ranging from isolated abdominal injury to severe multisystem trauma. Injuries are categorized as blunt or penetrating, with penetrating trauma further subdivided into stab wounds and gunshot wounds. Hemodynamic stability is the key determinant in selecting appropriate imaging and procedural strategies. Unstable patients generally require rapid surgical decision-making, whereas many stable patients can be managed nonoperatively with careful imaging and observation.
Clinical Assessment
History should focus on the mechanism of injury, use of restraints, airbags or helmets, prehospital vital signs, mental status at the scene, and any change in mental status. A complete AMPLE history is essential, including allergies (especially to medications or contrast), current medications, past medical and surgical history, last oral intake, and events leading up to the injury.
Physical examination begins with an ABCDE survey (Airway, Breathing, Circulation, Disability, Exposure), followed by full exposure of the patient and careful palpation of all abdominal quadrants. Abdominal injury is identified in only about half of trauma patients, and the physical exam may be unreliable in intoxicated, uncooperative, or multisystem trauma patients.
General Imaging Strategy
All trauma patients are initially managed using the ABCDE approach. Imaging decisions are then tailored according to stability.
Unstable Trauma Patients
Hemodynamically unstable patients should undergo immediate bedside ultrasonography as part of the primary survey. A positive FAST examination strongly suggests intra-abdominal bleeding as the cause of hypotension. A negative FAST raises concern for alternative bleeding sources, including retroperitoneal hemorrhage, pelvic fractures, thoracic bleeding, or significant blood loss prior to arrival. Surgical consultation should be obtained immediately to prepare for definitive operative management.
Stable Trauma Patients
In stable patients, three principal diagnostic modalities are used to define the extent of abdominal injury.
Ultrasound is often the initial screening test. A positive study in a stable patient raises concern for potential deterioration and should prompt rapid CT imaging and surgical consultation.
CT scanning is the definitive diagnostic tool in stable abdominal trauma. It provides superior detection of solid organ and retroperitoneal injuries compared with ultrasound and helps determine whether nonoperative management or interventional radiology techniques, such as embolization, are appropriate. CT is indicated in all stable patients with stab wounds and in patients with gross hematuria to evaluate for renal injury.
Diagnostic peritoneal lavage is now infrequently used, having largely been replaced by ultrasound and CT.
Laboratory Evaluation
Initial laboratory studies include blood type and screen, complete blood count, electrolytes, creatinine, lipase, urinalysis, and electrocardiography when indicated. These tests support imaging findings and assist in identifying associated injuries or complications.
Ultrasound (FAST Examination)
The FAST exam evaluates dependent intraperitoneal spaces where free fluid accumulates, including the hepatorenal recess (Morison pouch), splenorenal space, suprapubic region, and pericardium.
Advantages include rapid bedside performance, noninvasiveness, lack of radiation or contrast, and repeatability during resuscitation.
Limitations include operator dependence and poor sensitivity for solid organ parenchymal injuries, retroperitoneal bleeding, bowel injury, and hemorrhage associated with pelvic fractures.
A positive study is defined by visualization of free fluid or obvious organ injury. Adequate evaluation requires views of the right upper quadrant, left upper quadrant, pelvis, and heart.
Computed Tomography (CT)
CT scanning has a sensitivity of approximately 85–98% for abdominal trauma and provides detailed anatomic information about organ injury. It supports nonoperative management strategies and allows evaluation of the spine and adjacent structures.
Disadvantages include cost, radiation exposure, and the need for intravenous contrast, which carries a risk of allergic reaction and nephrotoxicity. Certain injuries—such as isolated diaphragmatic, pancreatic, or bowel injuries—may be missed early after trauma.
CT is indicated in hemodynamically stable patients and is contraindicated in unstable patients or those who already require emergent laparotomy. Many centers now use a “pan-scan” approach in multisystem trauma, though this increases cumulative radiation exposure.
Angiography
Angiography is useful for identifying and embolizing bleeding vessels, particularly in patients with pelvic fractures or solid organ hemorrhage. It may be used in selected unstable patients when surgical control is not immediately feasible.
Diagnostic Peritoneal Lavage (DPL)
DPL is invasive but highly sensitive for detecting intra-abdominal bleeding, mesenteric injury, and hollow viscus injury. It is now reserved for select situations, such as unstable patients with equivocal ultrasound findings or those requiring emergent surgery for another indication.
A positive test includes aspiration of blood, bile, bowel contents, or urine, or elevated red blood cell counts depending on the mechanism of injury. Contraindications include clear indications for laparotomy, and relative contraindications include prior abdominal surgery, pregnancy, and pediatric patients.
Disposition and Follow-Up
All unstable trauma patients require admission and frequently operative management. Most patients with multisystem trauma and abdominal involvement should be admitted. Pregnant patients beyond 24 weeks’ gestation require hospital admission for fetal–maternal monitoring.
Stable patients may be discharged only after a negative evaluation, sustained hemodynamic stability, and assurance of reliable follow-up and access to emergency care.
Discharge Advice and Safety Netting
Patients discharged after abdominal trauma must be instructed to return immediately for worsening abdominal pain, distention, vomiting, rectal bleeding, or any new concerning symptoms, as intestinal and pancreatic injuries may present late.
Clinical Pearls and Pitfalls
Bedside ultrasound can be performed immediately during resuscitation and repeated if clinical status changes. Increasing reliance on CT has reduced missed injuries but also increased radiation exposure and lifetime cancer risk. Diagnostic peritoneal lavage and local wound exploration are now less commonly used. Common pitfalls include failure to obtain early blood typing and pregnancy testing, and discharging pregnant patients beyond 24 weeks without appropriate monitoring.
- Published on
Emergency and Acute Medicine – Spontaneous Abortion (Early Pregnancy Loss)
Overview and Definitions
Spontaneous abortion refers to the unintentional termination of an intrauterine pregnancy before 20 weeks of gestation. It is also commonly termed early pregnancy loss or miscarriage. This condition occurs in approximately 15–20% of clinically recognized pregnancies, making it the most frequent complication of early pregnancy. Vaginal bleeding during the first trimester is reported in nearly one-quarter of pregnant patients, and about half of these cases ultimately result in pregnancy loss.
Several clinical subtypes are recognized. Threatened abortion presents with vaginal bleeding and a closed cervical os in the presence of a viable intrauterine pregnancy; approximately half of these patients will go on to miscarry. Inevitable abortion is characterized by bleeding with an open cervical os before expulsion of products of conception (POC). Incomplete abortion involves partial expulsion of POC with retained tissue and ongoing bleeding, while complete abortion describes full expulsion of all POC with subsequent closure of the cervical os. Missed abortion occurs when fetal demise is present without uterine activity or expulsion. Septic abortion is complicated by intrauterine infection, and recurrent spontaneous abortion is defined as three or more consecutive pregnancy losses.
Etiology and Risk Factors
The most common cause of spontaneous abortion is fetal chromosomal abnormality. Other contributing factors include uterine structural abnormalities and a variety of maternal risk factors. These include advanced maternal or paternal age, increased parity, smoking, alcohol or cocaine use, conception within a short interval after delivery, and chronic maternal illnesses such as poorly controlled diabetes, autoimmune disease, or celiac disease. Extremes of maternal body mass index, intrauterine devices, multiple prior elective abortions, and prior pregnancy losses also increase risk.
Maternal infections—including bacterial vaginosis, sexually transmitted infections, viral illnesses, parasitic infections, and TORCH pathogens—are important contributors. Certain medications, toxins, and uterine abnormalities such as fibroids, adhesions, or congenital malformations further predispose to pregnancy loss.
Clinical Presentation
Patients commonly present with vaginal bleeding and may report abdominal pain or cramping. Important historical details include last menstrual period, gestational age, obstetric history, prenatal care, and known risk factors. Bleeding should be quantified by duration and number of pads used, and patients should be asked about passage of clots or tissue. Symptoms such as dizziness or syncope may suggest significant blood loss.
Physical Examination
Assessment begins with evaluation of hemodynamic stability. Because blood volume is increased during pregnancy, particularly toward the end of the first trimester, patients may lose a substantial amount of blood before abnormal vital signs appear. Pelvic examination is essential to assess cervical dilation, amount of bleeding, and presence of POC. Adnexal tenderness or signs of peritoneal irritation raise concern for ectopic pregnancy. A bimanual examination helps estimate uterine size, which correlates with gestational age.
Essential Workup
Confirmation of pregnancy and assessment of gestational age and viability are central to evaluation. Imaging and laboratory studies are guided by clinical stability and suspected diagnosis.
Diagnostic Tests and Interpretation
Pregnancy is confirmed with urine or serum testing; most urine tests become positive at low β-hCG levels early in gestation and may remain positive for weeks after pregnancy loss. Laboratory evaluation includes complete blood count, rapid hemoglobin assessment, blood type and Rh status, and quantitative β-hCG levels. Type and cross-match are required for patients with active bleeding or anemia. Any expelled tissue should be sent for pathologic confirmation.
Transvaginal ultrasound is the preferred imaging modality in early pregnancy and can identify a gestational sac by approximately five weeks and cardiac activity by about six and a half weeks. Transabdominal ultrasound detects findings later. The discriminatory β-hCG zone defines the level at which a normal intrauterine pregnancy should be visualized and helps differentiate early pregnancy loss from ectopic pregnancy.
Differential Diagnosis
In patients with a positive pregnancy test and vaginal bleeding, alternative diagnoses include ectopic pregnancy, molar pregnancy, pregnancy of unknown location, cervicitis, subchorionic hemorrhage, septic abortion, and trauma. In later pregnancy, placental abruption and placenta previa must be considered.
Initial Stabilization and Emergency Management
Prehospital and early emergency department care focuses on monitoring vital signs, providing oxygen, establishing intravenous access, and treating hypovolemia. Unstable patients require aggressive resuscitation with large-bore IV access, crystalloid infusion, and transfusion of packed red blood cells if they fail to stabilize. Gynecologic consultation is urgent in unstable patients, as ruptured ectopic pregnancy must always be excluded.
Definitive Management by Clinical Type
Threatened abortion is managed conservatively with pelvic rest and close obstetric follow-up. Patients without documented cardiac activity early in pregnancy require serial β-hCG testing to assess viability and exclude ectopic pregnancy.
Inevitable and incomplete abortions may be managed expectantly, medically with misoprostol, or surgically with dilation and curettage. Surgical management reduces the risk of unplanned admissions and transfusion and allows pathologic confirmation of POC.
Complete abortion typically requires no intervention beyond observation, although uterotonic agents may be used if bleeding persists.
Missed abortion carries a risk of disseminated intravascular coagulation when fetal tissue is retained for several weeks, necessitating laboratory monitoring and specialist follow-up. Management options include expectant, medical, or surgical approaches based on patient preference and clinical stability.
Medications
Rh-negative patients require Rho(D) immunoglobulin to prevent alloimmunization, with dosing based on gestational age. Misoprostol is used for medical management of pregnancy loss under obstetric guidance. Uterotonic agents such as oxytocin or methylergonovine may be required to control heavy bleeding.
Disposition and Follow-Up
Admission is required for suspected ectopic pregnancy, hemodynamic instability, significant anemia, septic abortion, disseminated intravascular coagulation, or suspected gestational trophoblastic disease.
Stable patients may be discharged after appropriate treatment or observation, with pain control and close obstetric follow-up. Clear return precautions are essential.
Discharge Counseling and Support
Patients should be advised to return immediately for worsening bleeding, dizziness, fever, or increasing pain. Pelvic rest is recommended during active bleeding. Emotional support and reassurance are crucial, emphasizing that early pregnancy loss is common and not the result of patient actions.
Clinical Pearls and Pitfalls
Always maintain a high index of suspicion for ectopic pregnancy in early pregnancy bleeding. Significant blood loss can occur despite initially normal vital signs, and careful reassessment is essential.
Overview and Definitions
Spontaneous abortion refers to the unintentional termination of an intrauterine pregnancy before 20 weeks of gestation. It is also commonly termed early pregnancy loss or miscarriage. This condition occurs in approximately 15–20% of clinically recognized pregnancies, making it the most frequent complication of early pregnancy. Vaginal bleeding during the first trimester is reported in nearly one-quarter of pregnant patients, and about half of these cases ultimately result in pregnancy loss.
Several clinical subtypes are recognized. Threatened abortion presents with vaginal bleeding and a closed cervical os in the presence of a viable intrauterine pregnancy; approximately half of these patients will go on to miscarry. Inevitable abortion is characterized by bleeding with an open cervical os before expulsion of products of conception (POC). Incomplete abortion involves partial expulsion of POC with retained tissue and ongoing bleeding, while complete abortion describes full expulsion of all POC with subsequent closure of the cervical os. Missed abortion occurs when fetal demise is present without uterine activity or expulsion. Septic abortion is complicated by intrauterine infection, and recurrent spontaneous abortion is defined as three or more consecutive pregnancy losses.
Etiology and Risk Factors
The most common cause of spontaneous abortion is fetal chromosomal abnormality. Other contributing factors include uterine structural abnormalities and a variety of maternal risk factors. These include advanced maternal or paternal age, increased parity, smoking, alcohol or cocaine use, conception within a short interval after delivery, and chronic maternal illnesses such as poorly controlled diabetes, autoimmune disease, or celiac disease. Extremes of maternal body mass index, intrauterine devices, multiple prior elective abortions, and prior pregnancy losses also increase risk.
Maternal infections—including bacterial vaginosis, sexually transmitted infections, viral illnesses, parasitic infections, and TORCH pathogens—are important contributors. Certain medications, toxins, and uterine abnormalities such as fibroids, adhesions, or congenital malformations further predispose to pregnancy loss.
Clinical Presentation
Patients commonly present with vaginal bleeding and may report abdominal pain or cramping. Important historical details include last menstrual period, gestational age, obstetric history, prenatal care, and known risk factors. Bleeding should be quantified by duration and number of pads used, and patients should be asked about passage of clots or tissue. Symptoms such as dizziness or syncope may suggest significant blood loss.
Physical Examination
Assessment begins with evaluation of hemodynamic stability. Because blood volume is increased during pregnancy, particularly toward the end of the first trimester, patients may lose a substantial amount of blood before abnormal vital signs appear. Pelvic examination is essential to assess cervical dilation, amount of bleeding, and presence of POC. Adnexal tenderness or signs of peritoneal irritation raise concern for ectopic pregnancy. A bimanual examination helps estimate uterine size, which correlates with gestational age.
Essential Workup
Confirmation of pregnancy and assessment of gestational age and viability are central to evaluation. Imaging and laboratory studies are guided by clinical stability and suspected diagnosis.
Diagnostic Tests and Interpretation
Pregnancy is confirmed with urine or serum testing; most urine tests become positive at low β-hCG levels early in gestation and may remain positive for weeks after pregnancy loss. Laboratory evaluation includes complete blood count, rapid hemoglobin assessment, blood type and Rh status, and quantitative β-hCG levels. Type and cross-match are required for patients with active bleeding or anemia. Any expelled tissue should be sent for pathologic confirmation.
Transvaginal ultrasound is the preferred imaging modality in early pregnancy and can identify a gestational sac by approximately five weeks and cardiac activity by about six and a half weeks. Transabdominal ultrasound detects findings later. The discriminatory β-hCG zone defines the level at which a normal intrauterine pregnancy should be visualized and helps differentiate early pregnancy loss from ectopic pregnancy.
Differential Diagnosis
In patients with a positive pregnancy test and vaginal bleeding, alternative diagnoses include ectopic pregnancy, molar pregnancy, pregnancy of unknown location, cervicitis, subchorionic hemorrhage, septic abortion, and trauma. In later pregnancy, placental abruption and placenta previa must be considered.
Initial Stabilization and Emergency Management
Prehospital and early emergency department care focuses on monitoring vital signs, providing oxygen, establishing intravenous access, and treating hypovolemia. Unstable patients require aggressive resuscitation with large-bore IV access, crystalloid infusion, and transfusion of packed red blood cells if they fail to stabilize. Gynecologic consultation is urgent in unstable patients, as ruptured ectopic pregnancy must always be excluded.
Definitive Management by Clinical Type
Threatened abortion is managed conservatively with pelvic rest and close obstetric follow-up. Patients without documented cardiac activity early in pregnancy require serial β-hCG testing to assess viability and exclude ectopic pregnancy.
Inevitable and incomplete abortions may be managed expectantly, medically with misoprostol, or surgically with dilation and curettage. Surgical management reduces the risk of unplanned admissions and transfusion and allows pathologic confirmation of POC.
Complete abortion typically requires no intervention beyond observation, although uterotonic agents may be used if bleeding persists.
Missed abortion carries a risk of disseminated intravascular coagulation when fetal tissue is retained for several weeks, necessitating laboratory monitoring and specialist follow-up. Management options include expectant, medical, or surgical approaches based on patient preference and clinical stability.
Medications
Rh-negative patients require Rho(D) immunoglobulin to prevent alloimmunization, with dosing based on gestational age. Misoprostol is used for medical management of pregnancy loss under obstetric guidance. Uterotonic agents such as oxytocin or methylergonovine may be required to control heavy bleeding.
Disposition and Follow-Up
Admission is required for suspected ectopic pregnancy, hemodynamic instability, significant anemia, septic abortion, disseminated intravascular coagulation, or suspected gestational trophoblastic disease.
Stable patients may be discharged after appropriate treatment or observation, with pain control and close obstetric follow-up. Clear return precautions are essential.
Discharge Counseling and Support
Patients should be advised to return immediately for worsening bleeding, dizziness, fever, or increasing pain. Pelvic rest is recommended during active bleeding. Emotional support and reassurance are crucial, emphasizing that early pregnancy loss is common and not the result of patient actions.
Clinical Pearls and Pitfalls
Always maintain a high index of suspicion for ectopic pregnancy in early pregnancy bleeding. Significant blood loss can occur despite initially normal vital signs, and careful reassessment is essential.
- Published on
Click here to start customizing
