- Published on
Symptoms and Signs – Differential Diagnosis of Jaundice
Jaundice is a condition characterised by a yellow colouring of the skin, mucous membranes, or sclera of the eyes. It specifically indicates the presence of high quantities of conjugated or unconjugated bilirubin in the bloodstream. Fair-skinned patients exhibit the most prominent manifestations on their face, trunk, and sclera, while dark-skinned patients experience them on their hard palate, sclera, and conjunctiva.
The manifestation of jaundice is more evident under natural sunlight. Indeed, it can be imperceptible under artificial or low-quality illumination. Frequently, it is accompanied by itching (due to the adverse effects of bile pigment on sensory neurons), dark urine, and feces of clay hue.
Jaundice can arise from three different pathophysiologic mechanisms. Refer to Jaundice: The Impaired Metabolism of Bilirubin. It could serve as the sole indicator of specific diseases, such as pancreatic cancer.
Historical Background and Physical Assessment
Accurately recording a patient's jaundice history is crucial for identifying its underlying etiology. Ask the patient to indicate the initial onset of jaundice. Is he additionally experiencing pruritus, feces of clay tone, or urine of dark color? Indicate any previous occurrences or a familial predisposition to jaundice. Does he have nonspecific manifestations, such as weariness, fever, or chills; gastrointestinal manifestations, such anorexia, stomach pain, nausea, weight loss, or vomiting; or cardiovascular manifestations, such as dyspnea or rapid heartbeats? Discuss alcohol consumption and any medical history of cancer, liver illness, or gallbladder problems. Has the patient experienced recent weight loss? Obtain a drug history as well. Request information regarding any prior occurrences of hepatitis, gallstones, or liver or pancreatic disorders.
Undertake the physical examination in a well-lit room. Ensure that the orange-yellow color is in fact jaundice and not caused by hypercarotenemia, which is more noticeable on the palms and soles and does not impact the sclera. Evaluate the patient's skin for its texture, dryness, hyperpigmentation, and presence of xanthomas. Look for spider angiomas or petechiae, clubbed fingers, and gynecomastia. To diagnose heart failure in the patient, use auscultation to detect arrhythmias, murmurs, gallops, crackles, and irregular bowel sounds. Conduct palpation of the lymph nodes.
edema and abdominal soreness, pain, and embolism. Conduct palpation and percussing of the liver and spleen to assess for enlargement, and do ascites testing using the shifting dullness and fluid wave procedures. Acquire initial measurements of the patient's cognitive condition: Delicate alterations in the sensorium can serve as an initial indication of declining liver function.
Jaundice: Impaired Bilirubin Metabolism
It manifests in three distinct forms: prehepatic, hepatic, and posthepatic jaundice. All three conditions result in elevated bilirubin levels in the bloodstream caused by compromised metabolism.
In cases of prehepatic jaundice, specific medical diseases and disorders, such as transfusion responses and sickle cell anemia, lead to significant hemolysis. Rapid lysis of red blood cells surpasses the liver's ability to conjugate bilirubin, resulting in the release of significant quantities of unconjugated bilirubin into the bloodstream. This leads to heightened intestinal conversion of bilirubin into water-soluble urobilinogen, which can be eliminated by urine and feces. The insolubility of unconjugated bilirubin in water prevents its direct excretion in urine.
The condition known as hepatic jaundice arises when the liver is unable to modify or eliminate bilirubin, resulting in elevated concentrations of both conjugated and unconjugated bilirubin in the bloodstream. This phenomenon manifests in conditions such as hepatitis, cirrhosis, metastatic cancer, and during the extended use of medications that are processed by the liver.
The condition known as posthepatic jaundice arises in individuals with a biliary or pancreatic disease when the normal rate of bilirubin formation is obstructed by inflammation, scar tissue, a tumor, or gallstones, therefore impeding the passage of bile into the gut. This results in the accrual of conjugated bilirubin in the bloodstream. Renal excretion of water-soluble, conjugated bilirubin occurs.
Medical Causes Carcinoma
Pancreatic cancer of the ampulla of Vater first presents with variable jaundice, slight stomach discomfort, a recurring fever, and chills. First indication of the condition may be occult bleeding. Additional symptoms reported are weight loss, itching, and back discomfort.
Hepatic cancer, whether it is primary liver cancer or carcinoma that has spread to the liver, can lead to jaundice by blocking the bile duct. Even advanced malignancy yields vague indications and symptoms, including pain and sensitivity in the right upper quadrant, nausea, loss of weight, and a mild temperature. Upon examination, one may observe irregular, nodular, hard hepatomegaly, ascites, peripheral edema, a bruit noted over the liver, and a mass in the right upper quadrant.
Progression of jaundice, perhaps accompanied by pruritus, may be the sole indication of pancreatic cancer. Common initial observations include nonspecific symptoms such as weight loss and discomfort in the back or abdomen. The other indications and manifestations encompass anorexia, nausea and vomiting, pyrexia, steatorrhea, exhaustion, debility, diarrhea, itching, and cutaneous lesions (often on the legs).
Cholangitis
Charcot’s triad is caused by blockage and infection in the common bile duct, resulting in jaundice, right upper quadrant pain, and a high temperature accompanied by chills.
Cholecystitis
25% of patients with cholecystitis develop nonobstructive jaundice. Biliary colic usually reaches its highest point suddenly and lasts for 2 to 4 hours. The discomfort thereafter focuses in the right upper quadrant and remains continuous. Jaundice is caused by local inflammation or the migration of kidney stones to the common bile duct. Additional symptoms include nausea, vomiting (often hinting the existence of a stone), fever, excessive sweating, chills, sensitivity upon touch, a positive Murphy's sign, and maybe abdominal distension and rigidity.
Cholelithiasis
Cholelithiasis invariably results in jaundice and biliary colic. The condition is defined by intense and persistent pain in the upper right quadrant or epigastrium of the right side, which extends to the right scapula or shoulder and worsens over a period of several hours. Presenting indications and manifestations include emesis, tachycardia, and agitation. An obstruction of the common bile duct results in pyrexia, chills, jaundice, feces with a clay-colored appearance, and stomach pain. Following the ingestion of a high-fat meal, the patient may encounter a sensation of nonspecific epigastric fullness and dyspepsia.
Cirrhosis
Mild to severe jaundice accompanied by pruritus in conditions of Laënnec's cirrhosis sometimes indicates hepatocellular necrosis or increasing hepatic insufficiency. Common initial symptoms include ascites, weakness, leg edema, nausea and vomiting, diarrhea or constipation, loss of appetite, weight loss, and pain in the right upper quadrant. Profound hematemesis and other propensities for bleeding may also manifest. Additional abnormalities include hepatomegaly and parotid gland enlargement, digits with clubbing, Dupuytren's contracture, cognitive impairment, asterixis, fetor hepaticus, spider angiomas, and palmar erythema. Males may have gynecomastia, sparse hair in the chest and axilla, and testicular atrophy; females may encounter anomalies in their menstrual cycles.
Fluctuating jaundice in primary biliary cirrhosis may manifest years after the initial occurrence of other symptoms, including nausea that worsens at sleep (often the first indicator), weakness, exhaustion, weight loss, and diffuse abdominal pain. Prolonged itching can result in skin excoriation. Complicating symptoms include excessive pigmentation; signs of impaired absorption, such as nighttime diarrhea, steatorrhea, purpura, and osteomalacia; hematemesis caused by varices in the esophagus; ascites; swelling; xanthelasmas; xanthomas on the palms, soles, and elbows; and enlarged liver.
Dubin-Johnson syndrome
Fluctuating jaundice that worsens with stress is the primary symptom of Dubin-Johnson syndrome, a rare, chronic hereditary disorder that often manifests as late as age 40. Possible findings include modest hepatic enlargement and discomfort, pain in the upper abdomen, feelings of nausea, and episodes of vomiting.
Heart failure
Hepatic dysfunction leading to jaundice is observed in patients with profound right-sided heart failure. Additional consequences encompass jugular vein dilatation, cyanosis, remittent swelling of the legs and sacrum, consistent weight increase, cognitive impairment, enlarged liver, nausea and vomiting, stomach pain, and loss of appetite caused by visceral edema. Manifestations of ascites occur late. Also present may be oliguria, significant weakness, and anxiety. In the event that left-sided heart failure occurs initially, additional symptoms may encompass weariness, difficulty breathing, constriction of breathing, repeated episodes of shortness of breath, rapid breathing, irregular heartbeats, and increased heart rate.
Hepatic abscess
Recurrent abscesses can lead to jaundice, although the main symptoms are a chronic fever accompanied by chills and perspiration. Additional observations include persistent, intense pain in the upper right quadrant or midepigastrium, which may be directed to the shoulder; feelings of nausea and vomiting; loss of appetite; enlargement of the liver; an increased size of the right hemidiaphragm; and fluid accumulation in the abdomen.
Hepatitis
Dark urine and clay-colored stools usually develop before jaundice in the late stages of acute viral hepatitis. The initial systemic manifestations are somewhat diverse and encompass tiredness, nausea, vomiting, malaise, arthralgia, myalgia, headache, anorexia, photophobia, pharyngitis, cough, diarrhea or constipation, and a low-grade fever accompanied with enlargement of the liver and lymph nodes. During the icteric phase, which passes within 2 to 3 weeks unless there are problems, systemic symptoms decrease, but there may be an enlarged, palpable liver, weight loss, anorexia, and discomfort and tenderness in the right upper quadrant.
Pancreatitis (acute). Acute edema of the pancreatic head and subsequent blockage Although jaundice can be caused by the common bile duct, the main symptom of acute pancreatitis is typically intense epigastric pain that often spreads to the trunk. Assuming a supine position with the knees flexed toward the chest or assuming an upright seated orientation provides relief. Initial manifestations include episodes of nausea, chronic vomiting, abdominal distension, and the presence of Turner's or Cullen's sign. Additional observations include pyrexia, increased heart rate, abdominal stiffness and sensitivity, reduced colonic noises, and crackling sounds.
Severe pancreatitis produces extreme restlessness; mottled skin; cold, diaphoretic extremities; paresthesia; and tetany — the last two being symptoms of hypocalcemia. Fulminant pancreatitis results in extensive hemorrhage.
Sickle cell anemia
In the patient with sickle cell anemia, hemolysis results in the development of jaundice. Additional observations encompass hindered growth and development, heightened vulnerability to infection, potentially fatal thrombotic consequences, and, frequently, the presence of leg ulcers, necrotic joints, pyrexia, and chills. Additional symptoms may include arthralgia and angina. The manifestations of severe hemolysis include hematuria and pallor, persistent weariness, weakness, dyspnea (or dyspnea during exertion), and tachycardia. Alternatively, the patient may exhibit splenomegaly. A sickle cell crisis is characterized by intense bone, abdominal, thoracic, and muscle pain, a low-grade fever, and heightened weakness, jaundice, and dyspnea.
Secondary Factors
Drugs
Many medications might induce liver damage and consequent jaundice. Sulfonamides, mercaptopurine, erythromycin estolate, niacin, troleandomycin, androgenic steroids, 3-hydroxy-3-methylglutaryl reductase inhibitors, phenothiazines, ethanol, methyldopa, rifampin, and Dilantin are among the examples of medications.
Therapeutic interventions. Acute jaundice following upper abdominal surgery can be caused by hepatocellular injury resulting from organ manipulation, edema, and blocked bile flow; by the injection of halothane; or by protracted surgery leading to shock, blood loss, or blood transfusion.
A surgical shunt commonly employed to mitigate portal hypertension, such as a portacaval shunt, can potentially result in the development of jaundice.
Points of Special Consideration
In order to reduce itching, do regular bathing of the patient; use an antipruritic cream, such as calamine; and give diphenhydramine or hydroxyzine. Readied the patient for diagnostic examinations aimed at assessing biliary and hepatic function. Additional laboratory tests include urobilinogen levels in urine and feces, serum bilirubin, liver enzyme, and cholesterol levels; prothrombin time; and a complete blood count. Additional diagnostic procedures available are ultrasonography, cholangiography, liver biopsy, and exploratory laparotomy.
Therapeutic Counseling for Patients
The patient should be instructed on suitable dietary modifications and strategies to alleviate pruritus should be explored.
Guidelines for Pediatric Populations
Neonatal populations often experience physiological jaundice, which typically manifests 3 to 5 days postpartum. Neonatal obstructive jaundice often arises as a consequence of congenital biliary atresia. Choledochal cysts, which are congenital cystic dilations of the common bile duct, can also lead to jaundice in children, especially those of Japanese ancestry.
An exhaustive list of additional causes of jaundice encompasses Crigler-Najjar syndrome, Gilbert's disease, Rotor's syndrome, thalassemia major, hereditary spherocytosis, erythroblastosis fetalis, Hodgkin's disease, infectious mononucleosis, Wilson's disease, amyloidosis, and Reye's syndrome.
Jaundice is a condition characterised by a yellow colouring of the skin, mucous membranes, or sclera of the eyes. It specifically indicates the presence of high quantities of conjugated or unconjugated bilirubin in the bloodstream. Fair-skinned patients exhibit the most prominent manifestations on their face, trunk, and sclera, while dark-skinned patients experience them on their hard palate, sclera, and conjunctiva.
The manifestation of jaundice is more evident under natural sunlight. Indeed, it can be imperceptible under artificial or low-quality illumination. Frequently, it is accompanied by itching (due to the adverse effects of bile pigment on sensory neurons), dark urine, and feces of clay hue.
Jaundice can arise from three different pathophysiologic mechanisms. Refer to Jaundice: The Impaired Metabolism of Bilirubin. It could serve as the sole indicator of specific diseases, such as pancreatic cancer.
Historical Background and Physical Assessment
Accurately recording a patient's jaundice history is crucial for identifying its underlying etiology. Ask the patient to indicate the initial onset of jaundice. Is he additionally experiencing pruritus, feces of clay tone, or urine of dark color? Indicate any previous occurrences or a familial predisposition to jaundice. Does he have nonspecific manifestations, such as weariness, fever, or chills; gastrointestinal manifestations, such anorexia, stomach pain, nausea, weight loss, or vomiting; or cardiovascular manifestations, such as dyspnea or rapid heartbeats? Discuss alcohol consumption and any medical history of cancer, liver illness, or gallbladder problems. Has the patient experienced recent weight loss? Obtain a drug history as well. Request information regarding any prior occurrences of hepatitis, gallstones, or liver or pancreatic disorders.
Undertake the physical examination in a well-lit room. Ensure that the orange-yellow color is in fact jaundice and not caused by hypercarotenemia, which is more noticeable on the palms and soles and does not impact the sclera. Evaluate the patient's skin for its texture, dryness, hyperpigmentation, and presence of xanthomas. Look for spider angiomas or petechiae, clubbed fingers, and gynecomastia. To diagnose heart failure in the patient, use auscultation to detect arrhythmias, murmurs, gallops, crackles, and irregular bowel sounds. Conduct palpation of the lymph nodes.
edema and abdominal soreness, pain, and embolism. Conduct palpation and percussing of the liver and spleen to assess for enlargement, and do ascites testing using the shifting dullness and fluid wave procedures. Acquire initial measurements of the patient's cognitive condition: Delicate alterations in the sensorium can serve as an initial indication of declining liver function.
Jaundice: Impaired Bilirubin Metabolism
It manifests in three distinct forms: prehepatic, hepatic, and posthepatic jaundice. All three conditions result in elevated bilirubin levels in the bloodstream caused by compromised metabolism.
In cases of prehepatic jaundice, specific medical diseases and disorders, such as transfusion responses and sickle cell anemia, lead to significant hemolysis. Rapid lysis of red blood cells surpasses the liver's ability to conjugate bilirubin, resulting in the release of significant quantities of unconjugated bilirubin into the bloodstream. This leads to heightened intestinal conversion of bilirubin into water-soluble urobilinogen, which can be eliminated by urine and feces. The insolubility of unconjugated bilirubin in water prevents its direct excretion in urine.
The condition known as hepatic jaundice arises when the liver is unable to modify or eliminate bilirubin, resulting in elevated concentrations of both conjugated and unconjugated bilirubin in the bloodstream. This phenomenon manifests in conditions such as hepatitis, cirrhosis, metastatic cancer, and during the extended use of medications that are processed by the liver.
The condition known as posthepatic jaundice arises in individuals with a biliary or pancreatic disease when the normal rate of bilirubin formation is obstructed by inflammation, scar tissue, a tumor, or gallstones, therefore impeding the passage of bile into the gut. This results in the accrual of conjugated bilirubin in the bloodstream. Renal excretion of water-soluble, conjugated bilirubin occurs.
Medical Causes Carcinoma
Pancreatic cancer of the ampulla of Vater first presents with variable jaundice, slight stomach discomfort, a recurring fever, and chills. First indication of the condition may be occult bleeding. Additional symptoms reported are weight loss, itching, and back discomfort.
Hepatic cancer, whether it is primary liver cancer or carcinoma that has spread to the liver, can lead to jaundice by blocking the bile duct. Even advanced malignancy yields vague indications and symptoms, including pain and sensitivity in the right upper quadrant, nausea, loss of weight, and a mild temperature. Upon examination, one may observe irregular, nodular, hard hepatomegaly, ascites, peripheral edema, a bruit noted over the liver, and a mass in the right upper quadrant.
Progression of jaundice, perhaps accompanied by pruritus, may be the sole indication of pancreatic cancer. Common initial observations include nonspecific symptoms such as weight loss and discomfort in the back or abdomen. The other indications and manifestations encompass anorexia, nausea and vomiting, pyrexia, steatorrhea, exhaustion, debility, diarrhea, itching, and cutaneous lesions (often on the legs).
Cholangitis
Charcot’s triad is caused by blockage and infection in the common bile duct, resulting in jaundice, right upper quadrant pain, and a high temperature accompanied by chills.
Cholecystitis
25% of patients with cholecystitis develop nonobstructive jaundice. Biliary colic usually reaches its highest point suddenly and lasts for 2 to 4 hours. The discomfort thereafter focuses in the right upper quadrant and remains continuous. Jaundice is caused by local inflammation or the migration of kidney stones to the common bile duct. Additional symptoms include nausea, vomiting (often hinting the existence of a stone), fever, excessive sweating, chills, sensitivity upon touch, a positive Murphy's sign, and maybe abdominal distension and rigidity.
Cholelithiasis
Cholelithiasis invariably results in jaundice and biliary colic. The condition is defined by intense and persistent pain in the upper right quadrant or epigastrium of the right side, which extends to the right scapula or shoulder and worsens over a period of several hours. Presenting indications and manifestations include emesis, tachycardia, and agitation. An obstruction of the common bile duct results in pyrexia, chills, jaundice, feces with a clay-colored appearance, and stomach pain. Following the ingestion of a high-fat meal, the patient may encounter a sensation of nonspecific epigastric fullness and dyspepsia.
Cirrhosis
Mild to severe jaundice accompanied by pruritus in conditions of Laënnec's cirrhosis sometimes indicates hepatocellular necrosis or increasing hepatic insufficiency. Common initial symptoms include ascites, weakness, leg edema, nausea and vomiting, diarrhea or constipation, loss of appetite, weight loss, and pain in the right upper quadrant. Profound hematemesis and other propensities for bleeding may also manifest. Additional abnormalities include hepatomegaly and parotid gland enlargement, digits with clubbing, Dupuytren's contracture, cognitive impairment, asterixis, fetor hepaticus, spider angiomas, and palmar erythema. Males may have gynecomastia, sparse hair in the chest and axilla, and testicular atrophy; females may encounter anomalies in their menstrual cycles.
Fluctuating jaundice in primary biliary cirrhosis may manifest years after the initial occurrence of other symptoms, including nausea that worsens at sleep (often the first indicator), weakness, exhaustion, weight loss, and diffuse abdominal pain. Prolonged itching can result in skin excoriation. Complicating symptoms include excessive pigmentation; signs of impaired absorption, such as nighttime diarrhea, steatorrhea, purpura, and osteomalacia; hematemesis caused by varices in the esophagus; ascites; swelling; xanthelasmas; xanthomas on the palms, soles, and elbows; and enlarged liver.
Dubin-Johnson syndrome
Fluctuating jaundice that worsens with stress is the primary symptom of Dubin-Johnson syndrome, a rare, chronic hereditary disorder that often manifests as late as age 40. Possible findings include modest hepatic enlargement and discomfort, pain in the upper abdomen, feelings of nausea, and episodes of vomiting.
Heart failure
Hepatic dysfunction leading to jaundice is observed in patients with profound right-sided heart failure. Additional consequences encompass jugular vein dilatation, cyanosis, remittent swelling of the legs and sacrum, consistent weight increase, cognitive impairment, enlarged liver, nausea and vomiting, stomach pain, and loss of appetite caused by visceral edema. Manifestations of ascites occur late. Also present may be oliguria, significant weakness, and anxiety. In the event that left-sided heart failure occurs initially, additional symptoms may encompass weariness, difficulty breathing, constriction of breathing, repeated episodes of shortness of breath, rapid breathing, irregular heartbeats, and increased heart rate.
Hepatic abscess
Recurrent abscesses can lead to jaundice, although the main symptoms are a chronic fever accompanied by chills and perspiration. Additional observations include persistent, intense pain in the upper right quadrant or midepigastrium, which may be directed to the shoulder; feelings of nausea and vomiting; loss of appetite; enlargement of the liver; an increased size of the right hemidiaphragm; and fluid accumulation in the abdomen.
Hepatitis
Dark urine and clay-colored stools usually develop before jaundice in the late stages of acute viral hepatitis. The initial systemic manifestations are somewhat diverse and encompass tiredness, nausea, vomiting, malaise, arthralgia, myalgia, headache, anorexia, photophobia, pharyngitis, cough, diarrhea or constipation, and a low-grade fever accompanied with enlargement of the liver and lymph nodes. During the icteric phase, which passes within 2 to 3 weeks unless there are problems, systemic symptoms decrease, but there may be an enlarged, palpable liver, weight loss, anorexia, and discomfort and tenderness in the right upper quadrant.
Pancreatitis (acute). Acute edema of the pancreatic head and subsequent blockage Although jaundice can be caused by the common bile duct, the main symptom of acute pancreatitis is typically intense epigastric pain that often spreads to the trunk. Assuming a supine position with the knees flexed toward the chest or assuming an upright seated orientation provides relief. Initial manifestations include episodes of nausea, chronic vomiting, abdominal distension, and the presence of Turner's or Cullen's sign. Additional observations include pyrexia, increased heart rate, abdominal stiffness and sensitivity, reduced colonic noises, and crackling sounds.
Severe pancreatitis produces extreme restlessness; mottled skin; cold, diaphoretic extremities; paresthesia; and tetany — the last two being symptoms of hypocalcemia. Fulminant pancreatitis results in extensive hemorrhage.
Sickle cell anemia
In the patient with sickle cell anemia, hemolysis results in the development of jaundice. Additional observations encompass hindered growth and development, heightened vulnerability to infection, potentially fatal thrombotic consequences, and, frequently, the presence of leg ulcers, necrotic joints, pyrexia, and chills. Additional symptoms may include arthralgia and angina. The manifestations of severe hemolysis include hematuria and pallor, persistent weariness, weakness, dyspnea (or dyspnea during exertion), and tachycardia. Alternatively, the patient may exhibit splenomegaly. A sickle cell crisis is characterized by intense bone, abdominal, thoracic, and muscle pain, a low-grade fever, and heightened weakness, jaundice, and dyspnea.
Secondary Factors
Drugs
Many medications might induce liver damage and consequent jaundice. Sulfonamides, mercaptopurine, erythromycin estolate, niacin, troleandomycin, androgenic steroids, 3-hydroxy-3-methylglutaryl reductase inhibitors, phenothiazines, ethanol, methyldopa, rifampin, and Dilantin are among the examples of medications.
Therapeutic interventions. Acute jaundice following upper abdominal surgery can be caused by hepatocellular injury resulting from organ manipulation, edema, and blocked bile flow; by the injection of halothane; or by protracted surgery leading to shock, blood loss, or blood transfusion.
A surgical shunt commonly employed to mitigate portal hypertension, such as a portacaval shunt, can potentially result in the development of jaundice.
Points of Special Consideration
In order to reduce itching, do regular bathing of the patient; use an antipruritic cream, such as calamine; and give diphenhydramine or hydroxyzine. Readied the patient for diagnostic examinations aimed at assessing biliary and hepatic function. Additional laboratory tests include urobilinogen levels in urine and feces, serum bilirubin, liver enzyme, and cholesterol levels; prothrombin time; and a complete blood count. Additional diagnostic procedures available are ultrasonography, cholangiography, liver biopsy, and exploratory laparotomy.
Therapeutic Counseling for Patients
The patient should be instructed on suitable dietary modifications and strategies to alleviate pruritus should be explored.
Guidelines for Pediatric Populations
Neonatal populations often experience physiological jaundice, which typically manifests 3 to 5 days postpartum. Neonatal obstructive jaundice often arises as a consequence of congenital biliary atresia. Choledochal cysts, which are congenital cystic dilations of the common bile duct, can also lead to jaundice in children, especially those of Japanese ancestry.
An exhaustive list of additional causes of jaundice encompasses Crigler-Najjar syndrome, Gilbert's disease, Rotor's syndrome, thalassemia major, hereditary spherocytosis, erythroblastosis fetalis, Hodgkin's disease, infectious mononucleosis, Wilson's disease, amyloidosis, and Reye's syndrome.


- Published on
Symptoms and Signs – Differential Diagnosis of Intermittent claudication
Typically occurring in the lower extremities, intermittent claudication refers to the sensation of cramping limb pain triggered by physical activity and alleviated by a brief period of rest lasting 1 to 2 minutes. The pain may be either acute or chronic; in the case of acute pain, it may indicate acute artery blockage. The prevalence of intermittent claudication is highest in males aged 50 to 60 who have a medical history of diabetes mellitus, hyperlipidemia, hypertension, or tobacco use. In the absence of therapy, it can advance to discomfort experienced while at rest. As collateral circulation typically develops, limb loss is rare in cases of persistent arterial blockage.
Intermittent claudication in occlusive artery disease is caused by insufficient blood flow distribution. Pain in the calf or foot is indicative of femoral or popliteal artery disease, while pain in the buttocks and upper thigh suggests injury to the aortoiliac arteries. Exercise-induced discomfort usually arises from the liberation of lactic acid caused by anaerobic metabolism in the ischemic area, resulting from blockage. Discontinuation of exercise results in the clearance of lactic acid and subsequent reduction of discomfort.
Neurological etiology of intermittent claudication may include constriction of the spinal column at the level of the cauda equina. This phenomenon generates pressure.
located on the nerve roots leading to the lower limbs. Walking enhances blood flow to the cauda equina, leading to heightened pressure on those nerves and consequent excruciating pain.
Physical manifestations include pallor upon standing, rubor upon bending (particularly on the toes and soles), alopecia on the toes, and reduced arterial perfusions.
Urgent medical interventions
To evaluate a patient experiencing abrupt sporadic claudication accompanied by intense or throbbing leg pain when at rest, assess the leg's temperature and color, and examine the pulses of the femoral, popliteal, posterior tibial, and dorsalis pedis. Query concerning the presence of numbness and tingling. Probable acute artery blockage is indicated by the absence of pulses, coldness, pallor, cyanosis, or mottled appearance of the leg, and the presence of paresthesia and pain. Note the region of pallor, cyanosis, or mottling and regularly reevaluate it, observing any expansion in the region.
Exclude the leg from elevation. Safeguard it, preventing any object from exerting pressure on it. Enrol the patient for preoperative diagnostic procedures including blood testing, urinalysis, electrocardiography, chest X-rays, lower-extremity Doppler examinations, and angiography. Establish an intravenous (I.V.) line and provide an anticoagulant in combination with analgesics.
Histories and Physical Assessment
For patients with persistent intermittent claudication, it is important to collect historical data initially. Request information on the distance he can walk before experiencing pain and the duration of rest required for it to diminish. Does he need to rest for a longer duration or can he walk a shorter distance now compared to before? Does the pattern of pain-rest exhibit variation? To what extent has this ailment impacted his lifestyle?
Collect a medical history of predisposing factors for atherosclerosis, including tobacco use, diabetes, high blood pressure, and high levels of lipids in the blood. Subsequently, inquire about any accompanying indications and manifestations, such as paresthesia in the afflicted limb and identifiable alterations in the hue of the fingers (from white to blue to pink) in response to smoking, exposure to cold, or stress. Does the male patient exhibit impotence?
Direct the physical examination towards the study of the cardiovascular system. Assess the femoral, popliteal, dorsalis pedis, and posterior tibial pulses by palpation. Draw attention to character, amplitude, and bilateral equality. Atherosclerotic disease of the femoral artery may be indicated by diminished or nonexistent popliteal and pedal pulses, while the femoral pulse remains detectable. Diminished femoral and distal pulses may suggest the presence of pathology in the terminal aorta or iliac branches. The absence of pedal pulses, together with normal femoral and popliteal pulses, may suggest the presence of Buerger's disease.
Conduct auscultation to detect bruits over the main arteries. Observe variations in color and warmth between his legs and arms, and identify the specific locations on his leg where these deviations occur. Elevate the afflicted limb for a duration of 2 minutes; if it turns pale or white, there is a significant reduction in blood circulation. Upon lowering the leg, what is the duration required for the restoration of color? A duration of thirty seconds or more suggests the presence of severe illness. If feasible, assess the patient's deep tendon reflexes (DTRs) during physical activity; determine if they are reduced in his lower limbs.
Ascertain the presence of ulceration on the patient's feet, toes, and fingers, and examine his hands and lower legs for small, sensitive lumps and redness along blood vessels. Observe the caliber of his nails and the amount of hair present on his fingers and toes.
Should the patient experience arm pain, examine his arms for a noticeable alteration in color (to white) when raised. Furthermore, examine the subclavian region for alterations in temperature, muscular atrophy, and a pulsing mass by palpation. Use palpation to assess and contrast the radial, ulnar, brachial, axillary, and subclavian pulses in order to detect zones of obstruction.
Medical etiology
Arterial occlusion (acute)
Intermittent severe claudication is caused by acute arterial occlusion. A saddle embolus might include bilateral limb involvement. Presenting symptoms include paresthesia, paresis, and a perception of coldness in the afflicted limb. The limb is cooled, pallid, and marked with cyanosis (mottled) and lacks pulses below the socket. Time required for capillary refill is extended.
Arteriosclerosis obliterans
Typically, arteriosclerosis obliterans impacts the femoral and popliteal arteries, resulting in sporadic claudication, which is the most prevalent sign, in the calf. Common concomitant observations include reduced or nonexistent popliteal and pedal pulses, chilliness in the afflicted limb, pallor upon elevation, and significant limb weakness during ongoing physical activity. Additional potential symptoms include numbness, paresthesia, and, in an advanced stage of the condition, resting discomfort in the toes or foot, ulceration, and gangrene.
Buerger's disease. Typically, Buerger's disease causes sporadic claudication of the instep. Men are disproportionately impacted compared to women; the majority of afflicted men are smokers and fall within the age range of 20 to 40. Although prevalent in the Orient, Southeast Asia, India, and the Middle East, it is uncommon among Blacks. Preliminary indications include the presence of migratory superficial nodules and redness along the blood vessels in the extremities (known as nodular phlebitis), together with migratory venous pruritus. The feet initially exhibit cold, cyanotic, and numb sensations upon exposure to cold.
Subsequently, they grow redder, heat up, and tickle. Occasionally, Buerger's disease may also manifest in the hands, resulting in painful ulcerations on the fingertips. Additional distinctive features include decreased peripheral pulses, nerve weakness in the hands and feet, and migrating superficial thrombophlebitis.
Neurogenic claudication. Neurospinal disease causes pain from neurogenic intermittent claudication that requires a longer rest time than the 2 to 3 minutes needed in vascular claudication. Associated findings include paresthesia, weakness and clumsiness when walking, and hypoactive DTRs after walking. Pulses are unaffected.
Special Considerations
Encourage the patient to exercise to improve collateral circulation and increase venous return and advise him to avoid prolonged sitting or standing as well as crossing his legs at the knees. If intermittent claudication interferes with the patient’s lifestyle, he may require diagnostic tests (Doppler flow studies, arteriography, and digital subtraction angiography) to determine the location and degree of occlusion.
Patient Counseling
Discuss the risk factors for intermittent claudication. Stress the importance of inspecting legs and feet for ulcers. Explain ways the patient can protect his extremities from injury and the elements. Teach him which signs and symptoms to report.
Pediatric Pointers
Intermittent claudication rarely occurs in children. Although it sometimes develops in patients with coarctation of the aorta, extensive compensatory collateral circulation typically prevents manifestation of this sign. Muscle cramps from exercise and growing pains may be mistaken for intermittent claudication in children.
Typically occurring in the lower extremities, intermittent claudication refers to the sensation of cramping limb pain triggered by physical activity and alleviated by a brief period of rest lasting 1 to 2 minutes. The pain may be either acute or chronic; in the case of acute pain, it may indicate acute artery blockage. The prevalence of intermittent claudication is highest in males aged 50 to 60 who have a medical history of diabetes mellitus, hyperlipidemia, hypertension, or tobacco use. In the absence of therapy, it can advance to discomfort experienced while at rest. As collateral circulation typically develops, limb loss is rare in cases of persistent arterial blockage.
Intermittent claudication in occlusive artery disease is caused by insufficient blood flow distribution. Pain in the calf or foot is indicative of femoral or popliteal artery disease, while pain in the buttocks and upper thigh suggests injury to the aortoiliac arteries. Exercise-induced discomfort usually arises from the liberation of lactic acid caused by anaerobic metabolism in the ischemic area, resulting from blockage. Discontinuation of exercise results in the clearance of lactic acid and subsequent reduction of discomfort.
Neurological etiology of intermittent claudication may include constriction of the spinal column at the level of the cauda equina. This phenomenon generates pressure.
located on the nerve roots leading to the lower limbs. Walking enhances blood flow to the cauda equina, leading to heightened pressure on those nerves and consequent excruciating pain.
Physical manifestations include pallor upon standing, rubor upon bending (particularly on the toes and soles), alopecia on the toes, and reduced arterial perfusions.
Urgent medical interventions
To evaluate a patient experiencing abrupt sporadic claudication accompanied by intense or throbbing leg pain when at rest, assess the leg's temperature and color, and examine the pulses of the femoral, popliteal, posterior tibial, and dorsalis pedis. Query concerning the presence of numbness and tingling. Probable acute artery blockage is indicated by the absence of pulses, coldness, pallor, cyanosis, or mottled appearance of the leg, and the presence of paresthesia and pain. Note the region of pallor, cyanosis, or mottling and regularly reevaluate it, observing any expansion in the region.
Exclude the leg from elevation. Safeguard it, preventing any object from exerting pressure on it. Enrol the patient for preoperative diagnostic procedures including blood testing, urinalysis, electrocardiography, chest X-rays, lower-extremity Doppler examinations, and angiography. Establish an intravenous (I.V.) line and provide an anticoagulant in combination with analgesics.
Histories and Physical Assessment
For patients with persistent intermittent claudication, it is important to collect historical data initially. Request information on the distance he can walk before experiencing pain and the duration of rest required for it to diminish. Does he need to rest for a longer duration or can he walk a shorter distance now compared to before? Does the pattern of pain-rest exhibit variation? To what extent has this ailment impacted his lifestyle?
Collect a medical history of predisposing factors for atherosclerosis, including tobacco use, diabetes, high blood pressure, and high levels of lipids in the blood. Subsequently, inquire about any accompanying indications and manifestations, such as paresthesia in the afflicted limb and identifiable alterations in the hue of the fingers (from white to blue to pink) in response to smoking, exposure to cold, or stress. Does the male patient exhibit impotence?
Direct the physical examination towards the study of the cardiovascular system. Assess the femoral, popliteal, dorsalis pedis, and posterior tibial pulses by palpation. Draw attention to character, amplitude, and bilateral equality. Atherosclerotic disease of the femoral artery may be indicated by diminished or nonexistent popliteal and pedal pulses, while the femoral pulse remains detectable. Diminished femoral and distal pulses may suggest the presence of pathology in the terminal aorta or iliac branches. The absence of pedal pulses, together with normal femoral and popliteal pulses, may suggest the presence of Buerger's disease.
Conduct auscultation to detect bruits over the main arteries. Observe variations in color and warmth between his legs and arms, and identify the specific locations on his leg where these deviations occur. Elevate the afflicted limb for a duration of 2 minutes; if it turns pale or white, there is a significant reduction in blood circulation. Upon lowering the leg, what is the duration required for the restoration of color? A duration of thirty seconds or more suggests the presence of severe illness. If feasible, assess the patient's deep tendon reflexes (DTRs) during physical activity; determine if they are reduced in his lower limbs.
Ascertain the presence of ulceration on the patient's feet, toes, and fingers, and examine his hands and lower legs for small, sensitive lumps and redness along blood vessels. Observe the caliber of his nails and the amount of hair present on his fingers and toes.
Should the patient experience arm pain, examine his arms for a noticeable alteration in color (to white) when raised. Furthermore, examine the subclavian region for alterations in temperature, muscular atrophy, and a pulsing mass by palpation. Use palpation to assess and contrast the radial, ulnar, brachial, axillary, and subclavian pulses in order to detect zones of obstruction.
Medical etiology
Arterial occlusion (acute)
Intermittent severe claudication is caused by acute arterial occlusion. A saddle embolus might include bilateral limb involvement. Presenting symptoms include paresthesia, paresis, and a perception of coldness in the afflicted limb. The limb is cooled, pallid, and marked with cyanosis (mottled) and lacks pulses below the socket. Time required for capillary refill is extended.
Arteriosclerosis obliterans
Typically, arteriosclerosis obliterans impacts the femoral and popliteal arteries, resulting in sporadic claudication, which is the most prevalent sign, in the calf. Common concomitant observations include reduced or nonexistent popliteal and pedal pulses, chilliness in the afflicted limb, pallor upon elevation, and significant limb weakness during ongoing physical activity. Additional potential symptoms include numbness, paresthesia, and, in an advanced stage of the condition, resting discomfort in the toes or foot, ulceration, and gangrene.
Buerger's disease. Typically, Buerger's disease causes sporadic claudication of the instep. Men are disproportionately impacted compared to women; the majority of afflicted men are smokers and fall within the age range of 20 to 40. Although prevalent in the Orient, Southeast Asia, India, and the Middle East, it is uncommon among Blacks. Preliminary indications include the presence of migratory superficial nodules and redness along the blood vessels in the extremities (known as nodular phlebitis), together with migratory venous pruritus. The feet initially exhibit cold, cyanotic, and numb sensations upon exposure to cold.
Subsequently, they grow redder, heat up, and tickle. Occasionally, Buerger's disease may also manifest in the hands, resulting in painful ulcerations on the fingertips. Additional distinctive features include decreased peripheral pulses, nerve weakness in the hands and feet, and migrating superficial thrombophlebitis.
Neurogenic claudication. Neurospinal disease causes pain from neurogenic intermittent claudication that requires a longer rest time than the 2 to 3 minutes needed in vascular claudication. Associated findings include paresthesia, weakness and clumsiness when walking, and hypoactive DTRs after walking. Pulses are unaffected.
Special Considerations
Encourage the patient to exercise to improve collateral circulation and increase venous return and advise him to avoid prolonged sitting or standing as well as crossing his legs at the knees. If intermittent claudication interferes with the patient’s lifestyle, he may require diagnostic tests (Doppler flow studies, arteriography, and digital subtraction angiography) to determine the location and degree of occlusion.
Patient Counseling
Discuss the risk factors for intermittent claudication. Stress the importance of inspecting legs and feet for ulcers. Explain ways the patient can protect his extremities from injury and the elements. Teach him which signs and symptoms to report.
Pediatric Pointers
Intermittent claudication rarely occurs in children. Although it sometimes develops in patients with coarctation of the aorta, extensive compensatory collateral circulation typically prevents manifestation of this sign. Muscle cramps from exercise and growing pains may be mistaken for intermittent claudication in children.

- Published on
Symptoms and Signs – Differential Diagnosis of Homans’ Sign
A positive Homans' sign is indicated by deep calf pain caused by forceful and sudden dorsiflexion of the ankle. The pain arises from venous thrombosis or inflammation of the muscles of the calf. Nevertheless, the reliability of a positive Homans' sign as a signal is questionable due to its occurrence in only 35% of patients with these disorders. A positive Homans' sign, even when correct, does not serve as an indicator of the severity of the venous disease.
This triggered indication may be mistaken for persisting calf pain, which can arise from strains, contusions, cellulitis, or arterial blockage, or with pain in the posterior ankle or Achilles tendon (for instance, in a woman with shortened Achilles tendons due to wearing high heels).
EXAMINING GUIDELINE Invoking Homans' Sign
To elicit Homans' sign, initially provide support to the patient's thigh with one hand and position their foot with the other hand. His leg is flexed slightly at the knee, followed by a forceful and sudden dorsiflexion of the ankle. A positive Homans' sign is indicated by the presence of severe calf pain. (If Homans' sign is positive, the patient may exert resistance to ankle dorsiflexion or automatically flex the knee.)
Historical Background and Physical Assessment
When a positive Homans' sign is detected, direct the patient's medical history towards the signs and symptoms that may manifest in conjunction with deep vein thrombosis (DVT) or thrombophlebitis. These symptoms include pulsating, irritating, weighty, or constricted sensations in the calf and leg pain experienced during or after physical exercise or regular activities. Furthermore, inquire about dyspnea or angina, symptoms that could suggest pulmonary embolism. Ensure to inquire about predisposing factors, such as a leg injury, recent surgical procedures, childbirth, usage of hormonal contraceptives, concurrent medical conditions (for example, cancer, nephrosis, hypercoagulable disorders), and extended periods of inactivity or bed rest.
Proceed to examine and palpate the patient's calf for signs of warmth, pain, redness, swelling, and the existence of a detectable vein. When you have a high suspicion of deep vein thrombosis (DVT), carefully elicit Homans' sign to prevent dislodging the clot, as this could lead to pulmonary embolism, a potentially fatal condition.
Furthermore, take measurements of the circumferences of both calves belonging to the patient. A calf exhibiting the positive Homans' sign may have increased size due to associated edema and swelling.
Medical etiology
Deep vein thrombophlebitis.
The sole clinical manifestations of deep vein thrombophlebitis may include a positive Homans' sign and calf soreness. In addition, the patient may have intense pain, weight, warmth, and swelling in the afflicted leg; obviously enlarged superficial veins or detectable, cord-like veins; and a fever, chills, and malaise.
DVT
Deep vein thrombosis (DVT) results in a positive Homans' sign, as well as tenderness to the deep calf veins, mild swelling of the calves and thighs, a low-grade temperature, and increased heart rate. Signs of deep vein thrombosis (DVT) in the femoral and iliac veins include significant localised swelling and pain. If deep vein thrombosis (DVT) leads to venous blockage, you will observe cyanosis and potentially indurated skin in the afflicted leg.
Popliteal cyst (ruptured)
Spontaneous rupture of this synovial cyst may result in a positive Homans' sign, together with an abrupt emergence of calf discomfort, swelling, and redness.
Cellulitis (superficial)
In general, superficial cellulitis mostly impacts the lower extremities, however it can also manifest in the upper extremities, resulting in discomfort, redness, soreness, and swelling. Furthermore, certain people may also manifest symptoms such as fever, chills, tachycardia, headache, and hypotension.
Points of Special Consideration
Ensure that the patient is placed on bed rest, with the afflicted leg raised directly above the level of the heart. Topically apply warm and damp compresses to the afflicted region, and provide gentle oral analgesics. Furthermore, make proper preparations for the patient to undergo additional diagnostic testing, such as Doppler investigations and venograms.
After the patient becomes ambulatory, recommend that he wear elastic support stockings once his discomfort subsides (often within 5 to 10 days) and to maintain their use for a minimum of 3 months. Furthermore, advise the patient to maintain an elevated position of the affected leg while sitting and to refrain from crossing their legs at the knees in order to avoid compromising blood flow to the popliteal region. Crossing at the ankles is permissible.
Therapeutic Counseling for Patients
Illustrate the specific indications of extended clotting time that the patient should promptly disclose when prescribed an anticoagulant. Elaborate on the advantages and applications of elastic support stockings. Place significant emphasis on essential dietary limitations (such as consuming green leafy vegetables), abstaining from alcohol, and the need of seeing the practitioner before to initiating any new medications. Emphasize the need of maintaining scheduled follow-up appointments.
Paediatric Guidelines
Homans' sign is seldom evaluated in children, who seldom experience deep vein thrombosis (DVT) or Thrombophlebitis.
A positive Homans' sign is indicated by deep calf pain caused by forceful and sudden dorsiflexion of the ankle. The pain arises from venous thrombosis or inflammation of the muscles of the calf. Nevertheless, the reliability of a positive Homans' sign as a signal is questionable due to its occurrence in only 35% of patients with these disorders. A positive Homans' sign, even when correct, does not serve as an indicator of the severity of the venous disease.
This triggered indication may be mistaken for persisting calf pain, which can arise from strains, contusions, cellulitis, or arterial blockage, or with pain in the posterior ankle or Achilles tendon (for instance, in a woman with shortened Achilles tendons due to wearing high heels).
EXAMINING GUIDELINE Invoking Homans' Sign
To elicit Homans' sign, initially provide support to the patient's thigh with one hand and position their foot with the other hand. His leg is flexed slightly at the knee, followed by a forceful and sudden dorsiflexion of the ankle. A positive Homans' sign is indicated by the presence of severe calf pain. (If Homans' sign is positive, the patient may exert resistance to ankle dorsiflexion or automatically flex the knee.)
Historical Background and Physical Assessment
When a positive Homans' sign is detected, direct the patient's medical history towards the signs and symptoms that may manifest in conjunction with deep vein thrombosis (DVT) or thrombophlebitis. These symptoms include pulsating, irritating, weighty, or constricted sensations in the calf and leg pain experienced during or after physical exercise or regular activities. Furthermore, inquire about dyspnea or angina, symptoms that could suggest pulmonary embolism. Ensure to inquire about predisposing factors, such as a leg injury, recent surgical procedures, childbirth, usage of hormonal contraceptives, concurrent medical conditions (for example, cancer, nephrosis, hypercoagulable disorders), and extended periods of inactivity or bed rest.
Proceed to examine and palpate the patient's calf for signs of warmth, pain, redness, swelling, and the existence of a detectable vein. When you have a high suspicion of deep vein thrombosis (DVT), carefully elicit Homans' sign to prevent dislodging the clot, as this could lead to pulmonary embolism, a potentially fatal condition.
Furthermore, take measurements of the circumferences of both calves belonging to the patient. A calf exhibiting the positive Homans' sign may have increased size due to associated edema and swelling.
Medical etiology
Deep vein thrombophlebitis.
The sole clinical manifestations of deep vein thrombophlebitis may include a positive Homans' sign and calf soreness. In addition, the patient may have intense pain, weight, warmth, and swelling in the afflicted leg; obviously enlarged superficial veins or detectable, cord-like veins; and a fever, chills, and malaise.
DVT
Deep vein thrombosis (DVT) results in a positive Homans' sign, as well as tenderness to the deep calf veins, mild swelling of the calves and thighs, a low-grade temperature, and increased heart rate. Signs of deep vein thrombosis (DVT) in the femoral and iliac veins include significant localised swelling and pain. If deep vein thrombosis (DVT) leads to venous blockage, you will observe cyanosis and potentially indurated skin in the afflicted leg.
Popliteal cyst (ruptured)
Spontaneous rupture of this synovial cyst may result in a positive Homans' sign, together with an abrupt emergence of calf discomfort, swelling, and redness.
Cellulitis (superficial)
In general, superficial cellulitis mostly impacts the lower extremities, however it can also manifest in the upper extremities, resulting in discomfort, redness, soreness, and swelling. Furthermore, certain people may also manifest symptoms such as fever, chills, tachycardia, headache, and hypotension.
Points of Special Consideration
Ensure that the patient is placed on bed rest, with the afflicted leg raised directly above the level of the heart. Topically apply warm and damp compresses to the afflicted region, and provide gentle oral analgesics. Furthermore, make proper preparations for the patient to undergo additional diagnostic testing, such as Doppler investigations and venograms.
After the patient becomes ambulatory, recommend that he wear elastic support stockings once his discomfort subsides (often within 5 to 10 days) and to maintain their use for a minimum of 3 months. Furthermore, advise the patient to maintain an elevated position of the affected leg while sitting and to refrain from crossing their legs at the knees in order to avoid compromising blood flow to the popliteal region. Crossing at the ankles is permissible.
Therapeutic Counseling for Patients
Illustrate the specific indications of extended clotting time that the patient should promptly disclose when prescribed an anticoagulant. Elaborate on the advantages and applications of elastic support stockings. Place significant emphasis on essential dietary limitations (such as consuming green leafy vegetables), abstaining from alcohol, and the need of seeing the practitioner before to initiating any new medications. Emphasize the need of maintaining scheduled follow-up appointments.
Paediatric Guidelines
Homans' sign is seldom evaluated in children, who seldom experience deep vein thrombosis (DVT) or Thrombophlebitis.

- Published on
Symptoms and Signs – Differential Diagnosis of Hoarseness
Hoarseness, characterized by a coarse or abrasive voice produced by infections, inflammatory lesions, or exudates of the larynx; laryngeal edema; and compression or rupture of the vocal cords or recurrent laryngeal nerve. Additionally, this prevalent symptom can arise from a thoracic aortic aneurysm, vocal cord paralysis, and systemic diseases such rheumatoid arthritis. It is notably exacerbated by excessive use of alcohol, smoking, inhalation of harmful vapors, excessive verbal communication, and screaming.
Hoarseness may manifest as either acute or chronic. Specifically, the development of irritating polyps or nodules on the vocal cords leads to chronic hoarseness and laryngitis. Consideration should be given to gastroesophageal reflux into the larynx as a potential etiology of chronic hoarseness. Hoarseness can also occur as a consequence of gradual deterioration of the laryngeal muscles and mucosa caused by the course of age, resulting in less regulation of the voice cords.
Historical Background and Physical Assessment
Gather a comprehensive medical history. Firstly, it is important to take into account his age and gender; laryngeal cancer is predominantly frequent among males aged 50 to 70. Be sure to inquire about the initiation of hoarseness. Has the patient exhibited excessive vocal exertion? Has he encountered dyspnea, pharyngitis, xerostomia, borborrhea, or dysphagia? Furthermore, inquire whether he has been in close proximity to or inside a fire during the last 48 hours. Note that an inhalation injury might lead to abrupt blockage of the airways.
Explore related symptoms next. Is there a medical history of cancer, rheumatoid arthritis, or aortic aneurysm in the patient? Is he habitually heavy on drinks or a smoker?
Inspect the mouth and pharynx for erythema or exudate, which may suggest an upper respiratory infection. To detect lumps, palpate the neck and examine the cervical lymph nodes and thyroid for enlargement. Can the trachea be palpated and is it located midline? Instruct the patient to extend his tongue; if he is unable to do so, he may have
Paralysis resulting from involvement of cranial nerves. Assess the eyes for corneal ulcers and swollen lacrimal ducts, which are indicative of Sjögren's syndrome. Vasodilation of the jugular and chest veins may suggest compression caused by an aortic aneurysm.
Ascertain the patient's vital signs, particularly observing a temperature and bradycardia. Examine the chest for any asymmetrical expansion or indications of respiratory difficulty such as nasal flaring, stridor, and intercostal retractions. Perform auscultation to detect crackles, rhonchi, wheezing, and tubular sounds, and use percussive techniques to inspect for dullness.
Medical etiology
Gastroesophageal reflux
Gastroesophageal reflux is the backward movement of stomach fluids into the esophagus, which can then flow into the hypopharynx. Subsequently, this causes irritation to the larynx, leading to hoarseness, throat pain, cough, throat clearing, and a feeling of a lump in the throat. Both the arytenoids and the vocal cords may exhibit erythema and edema.
Hypothyroidism
Hoarseness sometimes serves as an early indication of hypothyroidism. Additional symptoms include excessive tiredness, susceptibility to cold, weight increase despite anorexia, and menorrhagia.
Laryngeal cancer
Hoarseness is an initial indication of vocal cord cancer, although it may manifest at a later stage in cancer affecting other parts of the larynx. Typically, the patient has an extensive smoking history. Additional typical observations include a slight, non-productive cough; slight soreness in the throat; pain in the vocal cords; and occasionally, coughing up blood.
Laryngeal leukoplakia
Leukoplakia is a prevalent etiology of hoarseness, particularly among patients who smoke. On direct laryngoscopy, histologic analysis often shows dysphagia of mild, moderate, or severe severity.
Laryngitis
Hoarseness that persists may be the sole indication of persistent laryngitis. Acute laryngitis is characterized by the abrupt development of hoarseness or a total loss of voice. Associated symptoms include dyspnea (particularly during mastication or articulation), a cough, pyrexia, excessive sweating, pharyngitis, and rhinorrhea.
Rheumatoid arthritis (RA)
Vocal hoarseness may indicate involvement of the larynx. Additional observations encompass soreness, difficulty swallowing, a feeling of satiety or strain in the throat, difficulty breathing during physical activity, and involuntary breathing.
Thoracic aortic aneurysm (TAA)
A thoracic aortic aneurysm usually leads to asymptomatic presentation but can result in hoarseness. The predominant symptom is radiating pain that is particularly intense when the patient is lying on their back. Additional clinical manifestations include a cough with a brassy tone, difficulty breathing, wheezing, a pain in the lower back, shoulders, or belly, a torsion in the trachea, swelling in the face and neck, distension of the jugular vein, difficulty swallowing, noticeable chest veins, difficulty breathing, and perhaps, paresthesia or nerve pain.
Tracheal trauma
A torn tracheal mucosa can result in hoarseness, hemoptysis, dysphagia, neck pain, airway blockage, and breathing difficulty.
Vocal cord paralysis
Unilateral vocal cord paralysis results in the development of hoarseness and voice weakness. Paralysis may coexist with indications of injury, such as cranial and cervical discomfort and edema.
Vocal cord polyps or nodules
The main major complaint is raspy hoarseness, which is accompanied by a persistent cough and a crackling voice.
Traumatic inhalation injury
A fire or explosion-induced inhalation injury results in hoarseness, coughing, singed nose hairs, orofacial burns, and sputum tinged with soot. Later indications and manifestations include crackles, rhonchi, and wheezing, which quickly worsen to respiratory impairment.
Therapeutic interventions. Temporary or permanent unilateral vocal cord paralysis, resulting in hoarseness, can occur as a consequence of surgical trauma to the recurrent laryngeal nerve. Extended usage of intubation can result in transient hoarseness.
Points of Special Consideration
Vigilantly monitor the patient for stridor, a potential sign of bilateral vocal cord paralysis. Extended duration of hoarseness beyond 2 weeks necessitates the use of indirect or fiber-optic laryngoscopy to examine the larynx both at rest and during phonation.
Therapeutic Counseling for Patients
Elucidate the significance of vocal rest and instruct the patient in alternate methods of effective communication. Emphasise the need of abstaining from alcohol, smoking, and exposure to secondhand smoke.
Key Pediatric Resources
Congenital abnormalities, such as laryngocele and dysphonia plicae ventricularis, can lead to hoarseness symptoms in youngsters. It may arise in prepubescent boys as a result of juvenile papillomatosis affecting the upper respiratory system.
Hoarseness in newborns and young children sometimes arises from acute laryngotracheobronchitis, also known as croup. Pulmonary discomfort may be caused by acute laryngitis in children under the age of 5 due to the tiny size of the larynx, which is prone to spasms when irritated or infected. This may result in either partial or complete blockage of the
Larynx. Transient hoarseness often arises from laryngeal irritation caused by the aspiration of liquids, foreign objects, or stomach contents. Although immunization has rendered this disease uncommon, hoarseness can also result from diphtheria.
Assist the youngster experiencing hoarseness in modulating his voice. To reduce crying in an infant, provide comfort, engage in peaceful activities, and humidify the surroundings.
Hoarseness, characterized by a coarse or abrasive voice produced by infections, inflammatory lesions, or exudates of the larynx; laryngeal edema; and compression or rupture of the vocal cords or recurrent laryngeal nerve. Additionally, this prevalent symptom can arise from a thoracic aortic aneurysm, vocal cord paralysis, and systemic diseases such rheumatoid arthritis. It is notably exacerbated by excessive use of alcohol, smoking, inhalation of harmful vapors, excessive verbal communication, and screaming.
Hoarseness may manifest as either acute or chronic. Specifically, the development of irritating polyps or nodules on the vocal cords leads to chronic hoarseness and laryngitis. Consideration should be given to gastroesophageal reflux into the larynx as a potential etiology of chronic hoarseness. Hoarseness can also occur as a consequence of gradual deterioration of the laryngeal muscles and mucosa caused by the course of age, resulting in less regulation of the voice cords.
Historical Background and Physical Assessment
Gather a comprehensive medical history. Firstly, it is important to take into account his age and gender; laryngeal cancer is predominantly frequent among males aged 50 to 70. Be sure to inquire about the initiation of hoarseness. Has the patient exhibited excessive vocal exertion? Has he encountered dyspnea, pharyngitis, xerostomia, borborrhea, or dysphagia? Furthermore, inquire whether he has been in close proximity to or inside a fire during the last 48 hours. Note that an inhalation injury might lead to abrupt blockage of the airways.
Explore related symptoms next. Is there a medical history of cancer, rheumatoid arthritis, or aortic aneurysm in the patient? Is he habitually heavy on drinks or a smoker?
Inspect the mouth and pharynx for erythema or exudate, which may suggest an upper respiratory infection. To detect lumps, palpate the neck and examine the cervical lymph nodes and thyroid for enlargement. Can the trachea be palpated and is it located midline? Instruct the patient to extend his tongue; if he is unable to do so, he may have
Paralysis resulting from involvement of cranial nerves. Assess the eyes for corneal ulcers and swollen lacrimal ducts, which are indicative of Sjögren's syndrome. Vasodilation of the jugular and chest veins may suggest compression caused by an aortic aneurysm.
Ascertain the patient's vital signs, particularly observing a temperature and bradycardia. Examine the chest for any asymmetrical expansion or indications of respiratory difficulty such as nasal flaring, stridor, and intercostal retractions. Perform auscultation to detect crackles, rhonchi, wheezing, and tubular sounds, and use percussive techniques to inspect for dullness.
Medical etiology
Gastroesophageal reflux
Gastroesophageal reflux is the backward movement of stomach fluids into the esophagus, which can then flow into the hypopharynx. Subsequently, this causes irritation to the larynx, leading to hoarseness, throat pain, cough, throat clearing, and a feeling of a lump in the throat. Both the arytenoids and the vocal cords may exhibit erythema and edema.
Hypothyroidism
Hoarseness sometimes serves as an early indication of hypothyroidism. Additional symptoms include excessive tiredness, susceptibility to cold, weight increase despite anorexia, and menorrhagia.
Laryngeal cancer
Hoarseness is an initial indication of vocal cord cancer, although it may manifest at a later stage in cancer affecting other parts of the larynx. Typically, the patient has an extensive smoking history. Additional typical observations include a slight, non-productive cough; slight soreness in the throat; pain in the vocal cords; and occasionally, coughing up blood.
Laryngeal leukoplakia
Leukoplakia is a prevalent etiology of hoarseness, particularly among patients who smoke. On direct laryngoscopy, histologic analysis often shows dysphagia of mild, moderate, or severe severity.
Laryngitis
Hoarseness that persists may be the sole indication of persistent laryngitis. Acute laryngitis is characterized by the abrupt development of hoarseness or a total loss of voice. Associated symptoms include dyspnea (particularly during mastication or articulation), a cough, pyrexia, excessive sweating, pharyngitis, and rhinorrhea.
Rheumatoid arthritis (RA)
Vocal hoarseness may indicate involvement of the larynx. Additional observations encompass soreness, difficulty swallowing, a feeling of satiety or strain in the throat, difficulty breathing during physical activity, and involuntary breathing.
Thoracic aortic aneurysm (TAA)
A thoracic aortic aneurysm usually leads to asymptomatic presentation but can result in hoarseness. The predominant symptom is radiating pain that is particularly intense when the patient is lying on their back. Additional clinical manifestations include a cough with a brassy tone, difficulty breathing, wheezing, a pain in the lower back, shoulders, or belly, a torsion in the trachea, swelling in the face and neck, distension of the jugular vein, difficulty swallowing, noticeable chest veins, difficulty breathing, and perhaps, paresthesia or nerve pain.
Tracheal trauma
A torn tracheal mucosa can result in hoarseness, hemoptysis, dysphagia, neck pain, airway blockage, and breathing difficulty.
Vocal cord paralysis
Unilateral vocal cord paralysis results in the development of hoarseness and voice weakness. Paralysis may coexist with indications of injury, such as cranial and cervical discomfort and edema.
Vocal cord polyps or nodules
The main major complaint is raspy hoarseness, which is accompanied by a persistent cough and a crackling voice.
Traumatic inhalation injury
A fire or explosion-induced inhalation injury results in hoarseness, coughing, singed nose hairs, orofacial burns, and sputum tinged with soot. Later indications and manifestations include crackles, rhonchi, and wheezing, which quickly worsen to respiratory impairment.
Therapeutic interventions. Temporary or permanent unilateral vocal cord paralysis, resulting in hoarseness, can occur as a consequence of surgical trauma to the recurrent laryngeal nerve. Extended usage of intubation can result in transient hoarseness.
Points of Special Consideration
Vigilantly monitor the patient for stridor, a potential sign of bilateral vocal cord paralysis. Extended duration of hoarseness beyond 2 weeks necessitates the use of indirect or fiber-optic laryngoscopy to examine the larynx both at rest and during phonation.
Therapeutic Counseling for Patients
Elucidate the significance of vocal rest and instruct the patient in alternate methods of effective communication. Emphasise the need of abstaining from alcohol, smoking, and exposure to secondhand smoke.
Key Pediatric Resources
Congenital abnormalities, such as laryngocele and dysphonia plicae ventricularis, can lead to hoarseness symptoms in youngsters. It may arise in prepubescent boys as a result of juvenile papillomatosis affecting the upper respiratory system.
Hoarseness in newborns and young children sometimes arises from acute laryngotracheobronchitis, also known as croup. Pulmonary discomfort may be caused by acute laryngitis in children under the age of 5 due to the tiny size of the larynx, which is prone to spasms when irritated or infected. This may result in either partial or complete blockage of the
Larynx. Transient hoarseness often arises from laryngeal irritation caused by the aspiration of liquids, foreign objects, or stomach contents. Although immunization has rendered this disease uncommon, hoarseness can also result from diphtheria.
Assist the youngster experiencing hoarseness in modulating his voice. To reduce crying in an infant, provide comfort, engage in peaceful activities, and humidify the surroundings.
- Published on
Symptoms and Signs – Differential Diagnosis of Hepatomegaly
Hepatomegaly, an enlarged liver, indicates potentially reversible primary or secondary liver disease. This sign may stem from diverse pathophysiologic mechanisms, including dilated hepatic sinusoids (in heart failure), persistently high venous pressure leading to liver congestion (in chronic constrictive pericarditis), dysfunction and engorgement of hepatocytes (in hepatitis), fatty infiltration of parenchymal cells causing fibrous tissue (in cirrhosis), distention of liver cells with glycogen (in diabetes), and infiltration of amyloid (in amyloidosis).
Hepatomegaly may be confirmed by palpation, percussion, or radiologic tests. It may be mistaken for displacement of the liver by the diaphragm, in a
respiratory disorder; by an abdominal tumor; by a spinal deformity, such as kyphosis; by the gallbladder; or by fecal material or a tumor in the colon.
History and Physical Examination
Hepatomegaly is seldom a patient’s chief complaint. It usually comes to light during palpation and percussion of the abdomen.
If you suspect hepatomegaly, ask the patient about his use of alcohol and exposure to hepatitis. Also ask if he’s currently ill or taking any prescribed drugs. If he complains of abdominal pain, ask him to locate and describe it.
Inspect the patient’s skin and sclera for jaundice, dilated veins (suggesting generalized congestion), scars from previous surgery, and spider angiomas (commonly occurring in cirrhosis). Next, inspect the contour of his abdomen. Is it protuberant over the liver or distended (possibly from ascites)? Measure his abdominal girth.
Percuss the liver, but be careful to identify structures and conditions that can obscure dull percussion notes, such as the sternum, ribs, breast tissue, pleural effusions, and gas in the colon. (See Percussing for Liver Size and Position, page 400.) Next, during deep inspiration, palpate the liver’s edge; it’s tender and rounded in hepatitis and cardiac decompensation, rocklike in carcinoma, and firm in cirrhosis.
Record the patient's initial vital signs and evaluate his nutritional condition. The presence of a dysfunctional enlarged liver leads to muscle atrophy, pronounced skeletal prominences, weight loss, thinning of hair, and swelling.
Assess the degree of awareness exhibited by the patient. Accumulation of metabolic chemicals harmful to brain cells occurs when an enlarged liver loses its capacity to detoxify waste materials. Consequently, be vigilant for alterations in personality, irritability, restlessness, amnesia, difficulty focusing and impaired mental function, and, in a very sick patient, a state of unconsciousness.
Guidelines for Examination Analysis of Liver Size and Position via Percussion
Commence percussing up the right midclavicular line (MCL) from the right iliac crest while the patient is lying on their back, as depicted below. In patients with liver illness, the percussion note gets dull as one approaches the inferior edge of the liver, typically around the costal margin, but occasionally at a lower position. Delineate this location and thereafter strike downwards from the right clavicle, once more along the right medial collateral ligament (MCL). The superior border of the liver typically extends from the fifth to the seventh intercostal spaces. Mark the upper boundary.
The distance between the two indicated spots signifies the approximate extent of the liver's right lobe, which typically measures between 2¼ inches and 4¾ inches (6 to 12 cm).
Proceed to evaluate the left lobe of the liver in a similar manner, by percussing along the sternal midline. Once more, indicate the locations where you perceive less pronounced percussion sounds. In addition,
Measure the longitudinal extent of the left lobe, often falling within the range of 11⁄2" to 31⁄8" (4 to 8 cm). Document your observations to serve as a reference point.
Medical etiology
Amyloidosis
Amyloidosis is an uncommon condition marked by hepatomegaly, moderate jaundice, and various renal, cardiac, and gastrointestinal (GI) consequences.
Cirrhosis
In advanced stages of cirrhosis, the liver has an enlarged, nodular, and hardened appearance. Other late indications and symptoms impact all physiological systems of the body. The respiratory examination reveals restricted expansion of the thoracic region caused by abdominal ascites, resulting in hypoxia. The central nervous system findings encompass indications and manifestations of hepatic encephalopathy, including lethargy, slurred speech, asterixis, peripheral neuritis, paranoia, hallucinations, severe debility, and coma. Hematologic manifestations encompass epistaxis, facile bruising, and gingival bleeding. Possible endocrine manifestations include testicular atrophy, gynecomastia, alopecia, and menstrual abnormalities. Integumentary effects include abnormal pigmentation, jaundice, severe pruritus, extreme dryness,
Inadequate tissue turgor, hypertrophic spider angiomas, and palmar erythema.
Furthermore, the patient may experience fetor hepaticus, swollen superficial abdominal veins, muscle atrophy, exacerbation of right upper quadrant pain upon sitting up or leaning forward, and palpable spleen. Portal hypertension, which refers to increased pressure in the portal vein, leads to bleeding associated with esophageal varices.
Diabetes mellitus
Inadequately managed diabetes in obese individuals often leads to hepatic fatty infiltration, hepatomegaly, right upper quadrant pain, as well as excessive thirst, excessive appetite, and excessive urination. Type 2 diabetes exhibits a higher prevalence of these characteristics compared to type 1 diabetes. A chronically enlarged fatty liver usually presents with no symptoms other than mild discomfort.
Granulomatous disorders.
Sarcoidosis, histoplasmosis, and similar diseases invariably result in a somewhat enlarged and hard liver.
Hepatic abscess
Primary symptoms of hepatomegaly include fever, nausea, vomiting, chills, weakness, diarrhea, anorexia, an elevated right hemidiaphragm, and right upper quadrant discomfort and tenderness.
Hepatitis
Primary manifestations of viral hepatitis include nausea, anorexia, vomiting, lethargy, malaise, photophobia, pharyngitis, cough, and headache. Hepatomegaly manifests during the icteric phase and persists during the recovery phase. During the icteric phase, the initial indications and symptoms decrease as new ones manifest: liver soreness, modest weight loss, dark urine, clay-colored feces, jaundice, persistent itching, pain in the right upper quadrant, and enlarged spleen.
Hematologic malignancies and lymphomas
Leukemia and lymphomas are hematological malignancies characterised by abundant production of red blood cells, often resulting in significant enlargement of the liver and spleen, sometimes with abdominal pain. Common manifestations include malaise, a mild temperature, exhaustion, debility, rapid heart rate, loss of body weight, bleeding abnormalities, and loss of appetite.
Hepatocellular carcinoma
Typically, primary tumors result in uneven, nodular, firm enlargement of the liver, accompanied by discomfort or sensitivity in the right upper quadrant and a friction rub or bruit over the liver. Prominent associated symptoms include weight loss, anorexia, cachexia, nausea, and vomiting. Potential complications include peripheral edema, ascites, jaundice, and the presence of a palpable mass in the right upper quadrant. When hepatomegaly is caused by metastatic liver tumors, the patient's concomitant signs and symptoms are indicative of his initial malignancy.
Mononucleosis is an infectious disease.
Rarely, infectious mononucleosis leads to the development of hepatomegaly. Initial symptoms include a headache, general malaise, and exhaustion. Following a period of 3 to 5 days, the patient commonly experiences a sore throat. The patient presents with cervical lymphadenopathy and fever variations. Additional symptoms he may have include stomatitis, palate petechiae, periorbital edema, splenomegaly, exudative tonsillitis, pharyngitis, and even a maculopapular rash.
Obesity
Infiltration of the liver by fatty substances can lead to hepatomegaly. Significant weight loss leads to a reduction in liver size.
Cancer of the pancreas
Hepatomegaly is a characteristic feature of pancreatic cancer, often together with conventional signs and symptoms such as anorexia, weight loss, abdomen or back discomfort, and jaundice. Additional symptoms include emesis, pyrexia, exhaustion, debility, itching, and cutaneous lesions (often on the lower extremities).
Pericarditis
Congestive hepatomegaly is a significant manifestation of elevated systemic venous pressure in cases of chronic constrictive pericarditis. Commonly observed are enlarged jugular veins, which become more noticeable during inhalation. Aside from the standard symptoms of heart illness, further manifestations include peripheral edema, ascites, tiredness, and reduced muscle mass.
Special Considerations
Prepare the patient for liver enzyme, alkaline phosphatase, bilirubin, albumin, and globulin studies to evaluate liver function and for X-rays, a liver scan, celiac arteriography, a computed tomography scan, and ultrasonography to confirm hepatomegaly.
Bed rest, relief from stress, and adequate nutrition are important for the patient with hepatomegaly to help protect liver cells from further damage and to allow the liver to regenerate functioning cells. Dietary protein may need to be monitored and possibly restricted. Ammonia, a major cause of hepatic encephalopathy, is a by-product of protein metabolism. Hepatotoxic drugs or drugs metabolized by the liver should be given in very small doses, if at all. These treatment measures should be explained to the patient.
Patient Counseling
Explain the treatment plan for the underlying disorder. Stress the need to avoid alcohol and exposure to people with infections. Discuss the importance of pacing activities and rest.
Pediatric Pointers
Assess hepatomegaly in children the same way you do in adults. Childhood hepatomegaly may stem from Reye’s syndrome; biliary atresia; rare disorders, such as Wilson’s, Gaucher’s, and Niemann-Pick diseases; or poorly controlled type 1 diabetes mellitus.
Hepatomegaly, an enlarged liver, indicates potentially reversible primary or secondary liver disease. This sign may stem from diverse pathophysiologic mechanisms, including dilated hepatic sinusoids (in heart failure), persistently high venous pressure leading to liver congestion (in chronic constrictive pericarditis), dysfunction and engorgement of hepatocytes (in hepatitis), fatty infiltration of parenchymal cells causing fibrous tissue (in cirrhosis), distention of liver cells with glycogen (in diabetes), and infiltration of amyloid (in amyloidosis).
Hepatomegaly may be confirmed by palpation, percussion, or radiologic tests. It may be mistaken for displacement of the liver by the diaphragm, in a
respiratory disorder; by an abdominal tumor; by a spinal deformity, such as kyphosis; by the gallbladder; or by fecal material or a tumor in the colon.
History and Physical Examination
Hepatomegaly is seldom a patient’s chief complaint. It usually comes to light during palpation and percussion of the abdomen.
If you suspect hepatomegaly, ask the patient about his use of alcohol and exposure to hepatitis. Also ask if he’s currently ill or taking any prescribed drugs. If he complains of abdominal pain, ask him to locate and describe it.
Inspect the patient’s skin and sclera for jaundice, dilated veins (suggesting generalized congestion), scars from previous surgery, and spider angiomas (commonly occurring in cirrhosis). Next, inspect the contour of his abdomen. Is it protuberant over the liver or distended (possibly from ascites)? Measure his abdominal girth.
Percuss the liver, but be careful to identify structures and conditions that can obscure dull percussion notes, such as the sternum, ribs, breast tissue, pleural effusions, and gas in the colon. (See Percussing for Liver Size and Position, page 400.) Next, during deep inspiration, palpate the liver’s edge; it’s tender and rounded in hepatitis and cardiac decompensation, rocklike in carcinoma, and firm in cirrhosis.
Record the patient's initial vital signs and evaluate his nutritional condition. The presence of a dysfunctional enlarged liver leads to muscle atrophy, pronounced skeletal prominences, weight loss, thinning of hair, and swelling.
Assess the degree of awareness exhibited by the patient. Accumulation of metabolic chemicals harmful to brain cells occurs when an enlarged liver loses its capacity to detoxify waste materials. Consequently, be vigilant for alterations in personality, irritability, restlessness, amnesia, difficulty focusing and impaired mental function, and, in a very sick patient, a state of unconsciousness.
Guidelines for Examination Analysis of Liver Size and Position via Percussion
Commence percussing up the right midclavicular line (MCL) from the right iliac crest while the patient is lying on their back, as depicted below. In patients with liver illness, the percussion note gets dull as one approaches the inferior edge of the liver, typically around the costal margin, but occasionally at a lower position. Delineate this location and thereafter strike downwards from the right clavicle, once more along the right medial collateral ligament (MCL). The superior border of the liver typically extends from the fifth to the seventh intercostal spaces. Mark the upper boundary.
The distance between the two indicated spots signifies the approximate extent of the liver's right lobe, which typically measures between 2¼ inches and 4¾ inches (6 to 12 cm).
Proceed to evaluate the left lobe of the liver in a similar manner, by percussing along the sternal midline. Once more, indicate the locations where you perceive less pronounced percussion sounds. In addition,
Measure the longitudinal extent of the left lobe, often falling within the range of 11⁄2" to 31⁄8" (4 to 8 cm). Document your observations to serve as a reference point.
Medical etiology
Amyloidosis
Amyloidosis is an uncommon condition marked by hepatomegaly, moderate jaundice, and various renal, cardiac, and gastrointestinal (GI) consequences.
Cirrhosis
In advanced stages of cirrhosis, the liver has an enlarged, nodular, and hardened appearance. Other late indications and symptoms impact all physiological systems of the body. The respiratory examination reveals restricted expansion of the thoracic region caused by abdominal ascites, resulting in hypoxia. The central nervous system findings encompass indications and manifestations of hepatic encephalopathy, including lethargy, slurred speech, asterixis, peripheral neuritis, paranoia, hallucinations, severe debility, and coma. Hematologic manifestations encompass epistaxis, facile bruising, and gingival bleeding. Possible endocrine manifestations include testicular atrophy, gynecomastia, alopecia, and menstrual abnormalities. Integumentary effects include abnormal pigmentation, jaundice, severe pruritus, extreme dryness,
Inadequate tissue turgor, hypertrophic spider angiomas, and palmar erythema.
Furthermore, the patient may experience fetor hepaticus, swollen superficial abdominal veins, muscle atrophy, exacerbation of right upper quadrant pain upon sitting up or leaning forward, and palpable spleen. Portal hypertension, which refers to increased pressure in the portal vein, leads to bleeding associated with esophageal varices.
Diabetes mellitus
Inadequately managed diabetes in obese individuals often leads to hepatic fatty infiltration, hepatomegaly, right upper quadrant pain, as well as excessive thirst, excessive appetite, and excessive urination. Type 2 diabetes exhibits a higher prevalence of these characteristics compared to type 1 diabetes. A chronically enlarged fatty liver usually presents with no symptoms other than mild discomfort.
Granulomatous disorders.
Sarcoidosis, histoplasmosis, and similar diseases invariably result in a somewhat enlarged and hard liver.
Hepatic abscess
Primary symptoms of hepatomegaly include fever, nausea, vomiting, chills, weakness, diarrhea, anorexia, an elevated right hemidiaphragm, and right upper quadrant discomfort and tenderness.
Hepatitis
Primary manifestations of viral hepatitis include nausea, anorexia, vomiting, lethargy, malaise, photophobia, pharyngitis, cough, and headache. Hepatomegaly manifests during the icteric phase and persists during the recovery phase. During the icteric phase, the initial indications and symptoms decrease as new ones manifest: liver soreness, modest weight loss, dark urine, clay-colored feces, jaundice, persistent itching, pain in the right upper quadrant, and enlarged spleen.
Hematologic malignancies and lymphomas
Leukemia and lymphomas are hematological malignancies characterised by abundant production of red blood cells, often resulting in significant enlargement of the liver and spleen, sometimes with abdominal pain. Common manifestations include malaise, a mild temperature, exhaustion, debility, rapid heart rate, loss of body weight, bleeding abnormalities, and loss of appetite.
Hepatocellular carcinoma
Typically, primary tumors result in uneven, nodular, firm enlargement of the liver, accompanied by discomfort or sensitivity in the right upper quadrant and a friction rub or bruit over the liver. Prominent associated symptoms include weight loss, anorexia, cachexia, nausea, and vomiting. Potential complications include peripheral edema, ascites, jaundice, and the presence of a palpable mass in the right upper quadrant. When hepatomegaly is caused by metastatic liver tumors, the patient's concomitant signs and symptoms are indicative of his initial malignancy.
Mononucleosis is an infectious disease.
Rarely, infectious mononucleosis leads to the development of hepatomegaly. Initial symptoms include a headache, general malaise, and exhaustion. Following a period of 3 to 5 days, the patient commonly experiences a sore throat. The patient presents with cervical lymphadenopathy and fever variations. Additional symptoms he may have include stomatitis, palate petechiae, periorbital edema, splenomegaly, exudative tonsillitis, pharyngitis, and even a maculopapular rash.
Obesity
Infiltration of the liver by fatty substances can lead to hepatomegaly. Significant weight loss leads to a reduction in liver size.
Cancer of the pancreas
Hepatomegaly is a characteristic feature of pancreatic cancer, often together with conventional signs and symptoms such as anorexia, weight loss, abdomen or back discomfort, and jaundice. Additional symptoms include emesis, pyrexia, exhaustion, debility, itching, and cutaneous lesions (often on the lower extremities).
Pericarditis
Congestive hepatomegaly is a significant manifestation of elevated systemic venous pressure in cases of chronic constrictive pericarditis. Commonly observed are enlarged jugular veins, which become more noticeable during inhalation. Aside from the standard symptoms of heart illness, further manifestations include peripheral edema, ascites, tiredness, and reduced muscle mass.
Special Considerations
Prepare the patient for liver enzyme, alkaline phosphatase, bilirubin, albumin, and globulin studies to evaluate liver function and for X-rays, a liver scan, celiac arteriography, a computed tomography scan, and ultrasonography to confirm hepatomegaly.
Bed rest, relief from stress, and adequate nutrition are important for the patient with hepatomegaly to help protect liver cells from further damage and to allow the liver to regenerate functioning cells. Dietary protein may need to be monitored and possibly restricted. Ammonia, a major cause of hepatic encephalopathy, is a by-product of protein metabolism. Hepatotoxic drugs or drugs metabolized by the liver should be given in very small doses, if at all. These treatment measures should be explained to the patient.
Patient Counseling
Explain the treatment plan for the underlying disorder. Stress the need to avoid alcohol and exposure to people with infections. Discuss the importance of pacing activities and rest.
Pediatric Pointers
Assess hepatomegaly in children the same way you do in adults. Childhood hepatomegaly may stem from Reye’s syndrome; biliary atresia; rare disorders, such as Wilson’s, Gaucher’s, and Niemann-Pick diseases; or poorly controlled type 1 diabetes mellitus.
- Published on
Symptoms and Signs – Differential Diagnosis of Hemoptysis
Frightening to the patient and commonly ominous, hemoptysis is the expectoration of blood or bloody sputum from the lungs or tracheobronchial tree. It’s sometimes confused with bleeding from the mouth, throat, nasopharynx, or GI tract. (See Identifying Hemoptysis.) Expectoration of 200 mL of blood in a single episode suggests severe bleeding, whereas expectoration of 400 mL in 3 hours or more than 600 mL in 16 hours signals a life-threatening crisis.
Hemoptysis usually results from chronic bronchitis, lung cancer, or bronchiectasis. However, it may also result from inflammatory, infectious, cardiovascular, or coagulation disorders and, rarely, from a ruptured aortic aneurysm. In up to 15% of patients, the cause is unknown. The most common causes of massive hemoptysis are lung cancer, bronchiectasis, active tuberculosis (TB), and cavitary pulmonary disease from necrotic infections or TB.
EXAMINATION TIP Identifying Hemoptysis
These guidelines will help you distinguish hemoptysis from epistaxis, hematemesis, and brown, red, or pink sputum.
HEMOPTYSIS
Typically frothy because it's mixed with air, hemoptysis is typically bright red with an alkaline pH (tested with nitrazine paper). It's strongly suggested by the presence of respiratory signs and symptoms, including a cough, a tickling sensation in the throat, and blood produced from repeated coughing episodes. (You can rule out epistaxis because the patient's nasal passages and posterior pharynx are usually clear.)
HEMATEMESIS
The usual site of hematemesis is the GI tract; the patient vomits or regurgitates coffee-ground material that contains food particles, tests positive for occult blood, and has an acid pH. However, he may vomit bright red blood or swallowed blood from the oral cavity and nasopharynx. After an episode of hematemesis, the patient may have stools with traces of blood and may also complain of dyspepsia.
BROWN, RED, OR PINK SPUTUM
Brown, red, or pink sputum can result from oxidation of inhaled bronchodilators. Sputum that looks like old blood may result from rupture of an amebic abscess into the bronchus. Red or brown sputum may occur in a patient with pneumonia caused by the enterobacterium Serratia marcescens.
Several pathophysiologic processes can cause hemoptysis. (See What Happens in Hemoptysis.)
EMERGENCY INTERVENTIONS
If the patient coughs up copious amounts of blood, endotracheal intubation may be required. Suction frequently to remove blood. Lavage may be necessary to loosen tenacious secretions or clots. Massive hemoptysis can
cause airway obstruction and asphyxiation. Insert an I.V. line to allow fluid replacement, drug administration, and blood transfusions, if needed. An emergency bronchoscopy should be performed to identify the bleeding site. Monitor the patient's blood pressure and pulse to detect hypotension and tachycardia, and draw an arterial blood sample for laboratory analysis to monitor respiratory status.
What Happens in Hemoptysis
Hemoptysis results from bleeding into the respiratory tract by bronchial or pulmonary vessels. Bleeding reflects alterations in the vascular walls and in blood-clotting mechanisms. It can result from any of these pathophysiologic processes:
Hemorrhage and diapedesis of red blood cells from the pulmonary microvasculature into the alveoli
Necrosis of lung tissue that causes inflammation and rupture of blood vessels or hemorrhage into the alveolar spaces
Rupture of an aortic aneurysm into the tracheobronchial tree
Rupture of distended endobronchial blood vessels from pulmonary hypertension due to mitral stenosis
Rupture of a pulmonary arteriovenous fistula or of bronchial or pulmonary artery or pulmonary venous collateral channels
Sloughing of a caseous lesion into the tracheobronchial tree
Ulceration and erosion of the bronchial epithelium
History and Physical Examination
If the hemoptysis is mild, ask the patient when it began. Has he ever coughed up blood before? About how much blood is he coughing up now and about how often? Ask about a history of cardiac, pulmonary, or bleeding disorders. If he’s receiving anticoagulant therapy, find out the drug, its dosage and schedule, and the duration of therapy. Is he taking other prescription drugs? Does he smoke? Ask the patient if he has had a recent infection. Has he been exposed to TB? When was his last tine test and what were the results?
Take the patient’s vital signs and examine his nose, mouth, and pharynx for sources of bleeding. Inspect the configuration of his chest and look for abnormal
movement during breathing, the use of accessory muscles, and retractions. Observe his respiratory rate, depth, and rhythm. Finally, examine his skin for lesions.
Next, palpate the patient’s chest for diaphragm level and for tenderness, respiratory excursion, fremitus, and abnormal pulsations; then percuss for flatness, dullness, resonance, hyperresonance, and tympany. Finally, auscultate the lungs, noting especially the quality and intensity of breath sounds. Also auscultate for heart murmurs, bruits, and pleural friction rubs.
Obtain a sputum sample and examine it for overall quantity, for the amount of blood it contains, and for its color, odor, and consistency.
Medical etiology
Bronchial adenoma. In up to 30% of patients, bronchial adenoma is a nasty condition characterized by recurrent hemoptysis, a persistent cough, and local wheezing.
Bronchiectasis
Hemoptysis, attributed to inflamed bronchial surfaces and corroded bronchial blood vessels, can manifest as blood-tinged sputum or, in around 20% of cases, blood. The patient's sputum may also demonstrate copiousness, malodor, and purulent consistency. Indications of a late stage of the disease include a persistent cough, coarse crackles, clubbing, fever, weight loss, weariness, weakness, malaise, and dyspnea during physical activity.
Bronchitis (chronic).
Primarily, chronic bronchitis manifests as an initial productive cough that persists for a minimum duration of 3 months. In due course, this results in the generation of sputum containing blood; significant bleeding is quite rare. Additional respiratory manifestations include dyspnea, extended expiration, wheezing, dispersed rhonchi, auxiliary muscle activity, barrel chest, tachypnea, and clubbing (a late diagnosis).
Coagulation disorders.
Thrombocytopenia and disseminated intravascular coagulation are conditions that can lead to hemoptysis. In addition to their particular associated symptoms, many diseases may exhibit common general signs such as multisystem hemorrhaging (e.g., gastrointestinal bleeding or epistaxis) and purpuric lesions.
Pulmonary abscess
Approximately half of the patients with lung abscess experience the production of blood-stained sputum due to bronchial ulceration, necrosis, and granulation tissue. Typical presenting symptoms include a cough with copious quantities of purulent, malodorous sputum; a fever accompanied by chills; excessive sweating; lack of appetite; weight loss; a headache; weakness; difficulty breathing; chest discomfort that is either pleuritic or dull; and clubbing. Auscultation indicates both tubular and cavernous respiration. Ambient sounds and sonications. Affected side exhibits dullness upon percussion.
Lung cancer
Recurrent hemoptysis, an early indication, is often caused by bronchial ulceration and can range from blood-streaked sputum to untreated blood. Associated symptoms include a productive cough, difficulty breathing, elevated body temperature, loss of appetite, loss of body weight, wheezing, and chest discomfort (a delayed symptom).
Plague (Yersinia pestis).
This acute bacterial infection can manifest in its pneumonic form as hemoptysis, a productive cough, chest pain, tachypnea, dyspnea, increased respiratory distress, cardiopulmonary insufficiency, as well as the abrupt onset of chills, a fever, a headache, and myalgia.
Pneumonia
In as many as 50% of instances, Klebsiella pneumonia generates a viscous dark brown or crimson (currant jelly) sputum, which is so persistent that the patient experiences difficulties in clearing it from their mouth. The onset of this form of pneumonia is sudden and characterized by chills, a fever, difficulty breathing, a strong cough, and intense chest pain located in the pleura. Possible secondary manifestations may encompass cyanosis, prostration, tachycardia, reduced breath sounds, and crackles.
The mucoid sputum produced by pneumococcal pneumonia is pinkish or reddish in color. The presentation starts with abrupt, trembling shivers; a swiftly increasing body temperature; and, in more than 80% of instances, increased heart rate and fast breathing. Within a few hours, the patient usually develops a productive cough accompanied by intense, stabbing, pleuritic discomfort. With splinting, the excruciating chest pain causes quick, shallow, grunting respirations. An examination shows respiratory distress characterized by dyspnea and the utilization of auxiliary muscles, as well as crackles and dullness when percussion is applied to the afflicted lung. Pallor, debility, muscle soreness, and hunching posture are symptoms that accompany a high temperature.
Pulmonary edema
. The presence of severe dyspnea, orthopnea, gasping, anxiety, cyanosis, diffuse crackles, a ventricular gallop, and cold, clammy skin is often accompanied with the production of frothy, blood-tinged pink sputum in cases of severe cardiogenic or noncardiogenic pulmonary edema. Furthermore, this potentially fatal disorder can result in tachycardia, lethargy, cardiac arrhythmias, tachypnea, hypotension, and a thready pulse.
Pulmonary embolism with infarction.
In pulmonary embolism with infarction, a life-threatening condition, hemoptysis is a frequent observation, although major hemoptysis is rare. Typical early symptoms include shortness of breath and chest pain characterized by angiopathy or pleuritis. Additional typical clinical manifestations include rapid heart rate, rapid breathing, a mild low-grade fever, and excessive sweating. Less frequently, the patient may have chest splinting, leg swelling, and, in cases of a significant embolism, cyanosis, syncope, and distension of the jugular vein. Examination indicates reduced breath sounds, a pleural friction rub, crackles, and widespread wheezing. The patient presents with dullness upon percussion, as well as indications of circulatory collapse (a weak and rapid pulse; hypotension), cerebral ischemia (transient loss of consciousness, convulsions), and hypoxemia (restlessness and, especially in older patients, hemiplegia and other localized neurological weakness).
Pulmonary hypertension (primary)
Features typically manifest rather late. Common symptoms include haemoptysis, exertional dyspnea, and weariness. Exertion often triggers angina-like pain that may radiate to the neck but not to the arms. Additional characteristics observed are arrhythmias, syncope, cough, and hoarseness.
Pulmonary tuberculosis
Pulmonary tuberculosis often presents with blood-streaked or blood-tinged sputum, while advanced cavitary tuberculosis may result in profuse hemoptysis. The respiratory symptoms include a persistent productive cough, presence of fine crackles after coughing, difficulty breathing, dullness when percussioned, heightened tactile sensitivity, and potential amphoric breath noises. In addition, the patient may experience nocturnal perspiration night sweats, malaise, fatigue, a fever, anorexia, weight loss, and pleuritic chest pain.
Systemic lupus erythematosus (SLE). In 50% of patients with SLE, pleuritis and pneumonitis cause hemoptysis, a cough, dyspnea, pleuritic chest pain, and crackles. Related findings are a butterfly rash in the acute phase, nondeforming joint pain and stiffness, photosensitivity, Raynaud’s phenomenon, seizures or psychoses, anorexia with weight loss, and lymphadenopathy.
Tracheal trauma
Torn tracheal mucosa may cause hemoptysis, hoarseness, dysphagia, neck pain, airway occlusion, and respiratory distress.
Quantitative diagnostic testing. Surgical procedures such as bronchoscopy, laryngoscopy, mediastinoscopy, or lung biopsy might result in lung or airway damage, leading to bleeding and hemoptysis.
Key Factors to Consider
Console and comfort the patient, who may respond to this concerning indication with unease and fear. If deemed essential, put him in the lateral decubitus posture, with the suspected bleeding lung pointing downwards, in order to safeguard the nonleaking lung. Execute this procedure with prudence as hypoxemia may exacerbate when the healthy lung is oriented upwards.
Administer diagnostic tests to the patient in order to ascertain the underlying cause of the bleeding. Potential diagnostic tests may include a complete blood count, a sputum culture and smear, and a chest X-ray.
Radiography, coagulation tests, bronchoscopy, pulmonary biopsy, pulmonary arteriography, and a pulmonary computed tomography scan.
Therapeutic Counseling for Patients
Clarify the significance of reporting recurring incidents. Provide the patient with written guidelines for submitting sputum samples.
Guidelines for Pediatric Populations
Pediatric hemoptysis can result from Goodpasture's syndrome, cystic fibrosis, or, in rare cases, idiopathic primary pulmonary hemosiderosis. Sometimes, pulmonary bleeding occurring within the first 2 weeks of life cannot be attributed to any specific cause; in such instances, the prognosis is adverse.
Guidelines for Geriatrics
If the patient is prescribed anticoagulants, ascertain any necessary modifications in his diet or other drugs (including over-the-counter and natural supplements) as these elements can impact the process of clotting.
Frightening to the patient and commonly ominous, hemoptysis is the expectoration of blood or bloody sputum from the lungs or tracheobronchial tree. It’s sometimes confused with bleeding from the mouth, throat, nasopharynx, or GI tract. (See Identifying Hemoptysis.) Expectoration of 200 mL of blood in a single episode suggests severe bleeding, whereas expectoration of 400 mL in 3 hours or more than 600 mL in 16 hours signals a life-threatening crisis.
Hemoptysis usually results from chronic bronchitis, lung cancer, or bronchiectasis. However, it may also result from inflammatory, infectious, cardiovascular, or coagulation disorders and, rarely, from a ruptured aortic aneurysm. In up to 15% of patients, the cause is unknown. The most common causes of massive hemoptysis are lung cancer, bronchiectasis, active tuberculosis (TB), and cavitary pulmonary disease from necrotic infections or TB.
EXAMINATION TIP Identifying Hemoptysis
These guidelines will help you distinguish hemoptysis from epistaxis, hematemesis, and brown, red, or pink sputum.
HEMOPTYSIS
Typically frothy because it's mixed with air, hemoptysis is typically bright red with an alkaline pH (tested with nitrazine paper). It's strongly suggested by the presence of respiratory signs and symptoms, including a cough, a tickling sensation in the throat, and blood produced from repeated coughing episodes. (You can rule out epistaxis because the patient's nasal passages and posterior pharynx are usually clear.)
HEMATEMESIS
The usual site of hematemesis is the GI tract; the patient vomits or regurgitates coffee-ground material that contains food particles, tests positive for occult blood, and has an acid pH. However, he may vomit bright red blood or swallowed blood from the oral cavity and nasopharynx. After an episode of hematemesis, the patient may have stools with traces of blood and may also complain of dyspepsia.
BROWN, RED, OR PINK SPUTUM
Brown, red, or pink sputum can result from oxidation of inhaled bronchodilators. Sputum that looks like old blood may result from rupture of an amebic abscess into the bronchus. Red or brown sputum may occur in a patient with pneumonia caused by the enterobacterium Serratia marcescens.
Several pathophysiologic processes can cause hemoptysis. (See What Happens in Hemoptysis.)
EMERGENCY INTERVENTIONS
If the patient coughs up copious amounts of blood, endotracheal intubation may be required. Suction frequently to remove blood. Lavage may be necessary to loosen tenacious secretions or clots. Massive hemoptysis can
cause airway obstruction and asphyxiation. Insert an I.V. line to allow fluid replacement, drug administration, and blood transfusions, if needed. An emergency bronchoscopy should be performed to identify the bleeding site. Monitor the patient's blood pressure and pulse to detect hypotension and tachycardia, and draw an arterial blood sample for laboratory analysis to monitor respiratory status.
What Happens in Hemoptysis
Hemoptysis results from bleeding into the respiratory tract by bronchial or pulmonary vessels. Bleeding reflects alterations in the vascular walls and in blood-clotting mechanisms. It can result from any of these pathophysiologic processes:
Hemorrhage and diapedesis of red blood cells from the pulmonary microvasculature into the alveoli
Necrosis of lung tissue that causes inflammation and rupture of blood vessels or hemorrhage into the alveolar spaces
Rupture of an aortic aneurysm into the tracheobronchial tree
Rupture of distended endobronchial blood vessels from pulmonary hypertension due to mitral stenosis
Rupture of a pulmonary arteriovenous fistula or of bronchial or pulmonary artery or pulmonary venous collateral channels
Sloughing of a caseous lesion into the tracheobronchial tree
Ulceration and erosion of the bronchial epithelium
History and Physical Examination
If the hemoptysis is mild, ask the patient when it began. Has he ever coughed up blood before? About how much blood is he coughing up now and about how often? Ask about a history of cardiac, pulmonary, or bleeding disorders. If he’s receiving anticoagulant therapy, find out the drug, its dosage and schedule, and the duration of therapy. Is he taking other prescription drugs? Does he smoke? Ask the patient if he has had a recent infection. Has he been exposed to TB? When was his last tine test and what were the results?
Take the patient’s vital signs and examine his nose, mouth, and pharynx for sources of bleeding. Inspect the configuration of his chest and look for abnormal
movement during breathing, the use of accessory muscles, and retractions. Observe his respiratory rate, depth, and rhythm. Finally, examine his skin for lesions.
Next, palpate the patient’s chest for diaphragm level and for tenderness, respiratory excursion, fremitus, and abnormal pulsations; then percuss for flatness, dullness, resonance, hyperresonance, and tympany. Finally, auscultate the lungs, noting especially the quality and intensity of breath sounds. Also auscultate for heart murmurs, bruits, and pleural friction rubs.
Obtain a sputum sample and examine it for overall quantity, for the amount of blood it contains, and for its color, odor, and consistency.
Medical etiology
Bronchial adenoma. In up to 30% of patients, bronchial adenoma is a nasty condition characterized by recurrent hemoptysis, a persistent cough, and local wheezing.
Bronchiectasis
Hemoptysis, attributed to inflamed bronchial surfaces and corroded bronchial blood vessels, can manifest as blood-tinged sputum or, in around 20% of cases, blood. The patient's sputum may also demonstrate copiousness, malodor, and purulent consistency. Indications of a late stage of the disease include a persistent cough, coarse crackles, clubbing, fever, weight loss, weariness, weakness, malaise, and dyspnea during physical activity.
Bronchitis (chronic).
Primarily, chronic bronchitis manifests as an initial productive cough that persists for a minimum duration of 3 months. In due course, this results in the generation of sputum containing blood; significant bleeding is quite rare. Additional respiratory manifestations include dyspnea, extended expiration, wheezing, dispersed rhonchi, auxiliary muscle activity, barrel chest, tachypnea, and clubbing (a late diagnosis).
Coagulation disorders.
Thrombocytopenia and disseminated intravascular coagulation are conditions that can lead to hemoptysis. In addition to their particular associated symptoms, many diseases may exhibit common general signs such as multisystem hemorrhaging (e.g., gastrointestinal bleeding or epistaxis) and purpuric lesions.
Pulmonary abscess
Approximately half of the patients with lung abscess experience the production of blood-stained sputum due to bronchial ulceration, necrosis, and granulation tissue. Typical presenting symptoms include a cough with copious quantities of purulent, malodorous sputum; a fever accompanied by chills; excessive sweating; lack of appetite; weight loss; a headache; weakness; difficulty breathing; chest discomfort that is either pleuritic or dull; and clubbing. Auscultation indicates both tubular and cavernous respiration. Ambient sounds and sonications. Affected side exhibits dullness upon percussion.
Lung cancer
Recurrent hemoptysis, an early indication, is often caused by bronchial ulceration and can range from blood-streaked sputum to untreated blood. Associated symptoms include a productive cough, difficulty breathing, elevated body temperature, loss of appetite, loss of body weight, wheezing, and chest discomfort (a delayed symptom).
Plague (Yersinia pestis).
This acute bacterial infection can manifest in its pneumonic form as hemoptysis, a productive cough, chest pain, tachypnea, dyspnea, increased respiratory distress, cardiopulmonary insufficiency, as well as the abrupt onset of chills, a fever, a headache, and myalgia.
Pneumonia
In as many as 50% of instances, Klebsiella pneumonia generates a viscous dark brown or crimson (currant jelly) sputum, which is so persistent that the patient experiences difficulties in clearing it from their mouth. The onset of this form of pneumonia is sudden and characterized by chills, a fever, difficulty breathing, a strong cough, and intense chest pain located in the pleura. Possible secondary manifestations may encompass cyanosis, prostration, tachycardia, reduced breath sounds, and crackles.
The mucoid sputum produced by pneumococcal pneumonia is pinkish or reddish in color. The presentation starts with abrupt, trembling shivers; a swiftly increasing body temperature; and, in more than 80% of instances, increased heart rate and fast breathing. Within a few hours, the patient usually develops a productive cough accompanied by intense, stabbing, pleuritic discomfort. With splinting, the excruciating chest pain causes quick, shallow, grunting respirations. An examination shows respiratory distress characterized by dyspnea and the utilization of auxiliary muscles, as well as crackles and dullness when percussion is applied to the afflicted lung. Pallor, debility, muscle soreness, and hunching posture are symptoms that accompany a high temperature.
Pulmonary edema
. The presence of severe dyspnea, orthopnea, gasping, anxiety, cyanosis, diffuse crackles, a ventricular gallop, and cold, clammy skin is often accompanied with the production of frothy, blood-tinged pink sputum in cases of severe cardiogenic or noncardiogenic pulmonary edema. Furthermore, this potentially fatal disorder can result in tachycardia, lethargy, cardiac arrhythmias, tachypnea, hypotension, and a thready pulse.
Pulmonary embolism with infarction.
In pulmonary embolism with infarction, a life-threatening condition, hemoptysis is a frequent observation, although major hemoptysis is rare. Typical early symptoms include shortness of breath and chest pain characterized by angiopathy or pleuritis. Additional typical clinical manifestations include rapid heart rate, rapid breathing, a mild low-grade fever, and excessive sweating. Less frequently, the patient may have chest splinting, leg swelling, and, in cases of a significant embolism, cyanosis, syncope, and distension of the jugular vein. Examination indicates reduced breath sounds, a pleural friction rub, crackles, and widespread wheezing. The patient presents with dullness upon percussion, as well as indications of circulatory collapse (a weak and rapid pulse; hypotension), cerebral ischemia (transient loss of consciousness, convulsions), and hypoxemia (restlessness and, especially in older patients, hemiplegia and other localized neurological weakness).
Pulmonary hypertension (primary)
Features typically manifest rather late. Common symptoms include haemoptysis, exertional dyspnea, and weariness. Exertion often triggers angina-like pain that may radiate to the neck but not to the arms. Additional characteristics observed are arrhythmias, syncope, cough, and hoarseness.
Pulmonary tuberculosis
Pulmonary tuberculosis often presents with blood-streaked or blood-tinged sputum, while advanced cavitary tuberculosis may result in profuse hemoptysis. The respiratory symptoms include a persistent productive cough, presence of fine crackles after coughing, difficulty breathing, dullness when percussioned, heightened tactile sensitivity, and potential amphoric breath noises. In addition, the patient may experience nocturnal perspiration night sweats, malaise, fatigue, a fever, anorexia, weight loss, and pleuritic chest pain.
Systemic lupus erythematosus (SLE). In 50% of patients with SLE, pleuritis and pneumonitis cause hemoptysis, a cough, dyspnea, pleuritic chest pain, and crackles. Related findings are a butterfly rash in the acute phase, nondeforming joint pain and stiffness, photosensitivity, Raynaud’s phenomenon, seizures or psychoses, anorexia with weight loss, and lymphadenopathy.
Tracheal trauma
Torn tracheal mucosa may cause hemoptysis, hoarseness, dysphagia, neck pain, airway occlusion, and respiratory distress.
Quantitative diagnostic testing. Surgical procedures such as bronchoscopy, laryngoscopy, mediastinoscopy, or lung biopsy might result in lung or airway damage, leading to bleeding and hemoptysis.
Key Factors to Consider
Console and comfort the patient, who may respond to this concerning indication with unease and fear. If deemed essential, put him in the lateral decubitus posture, with the suspected bleeding lung pointing downwards, in order to safeguard the nonleaking lung. Execute this procedure with prudence as hypoxemia may exacerbate when the healthy lung is oriented upwards.
Administer diagnostic tests to the patient in order to ascertain the underlying cause of the bleeding. Potential diagnostic tests may include a complete blood count, a sputum culture and smear, and a chest X-ray.
Radiography, coagulation tests, bronchoscopy, pulmonary biopsy, pulmonary arteriography, and a pulmonary computed tomography scan.
Therapeutic Counseling for Patients
Clarify the significance of reporting recurring incidents. Provide the patient with written guidelines for submitting sputum samples.
Guidelines for Pediatric Populations
Pediatric hemoptysis can result from Goodpasture's syndrome, cystic fibrosis, or, in rare cases, idiopathic primary pulmonary hemosiderosis. Sometimes, pulmonary bleeding occurring within the first 2 weeks of life cannot be attributed to any specific cause; in such instances, the prognosis is adverse.
Guidelines for Geriatrics
If the patient is prescribed anticoagulants, ascertain any necessary modifications in his diet or other drugs (including over-the-counter and natural supplements) as these elements can impact the process of clotting.

- Published on
Symptoms and Signs – Differential Diagnosis of Hemianopsia
Hemianopsia is the condition characterized by the partial loss of vision in one half of the typical visual field, predominantly affecting either the right or left side of one or both eyes. In cases when the visual field abnormalities are the same in both eyes but impact less than half of the field of vision in each eye (known as incomplete homonymous hemianopsia), the lesion is likely located in the occipital lobe. Otherwise, it is more likely to affect the parietal or temporal lobe. Consult the section on Identifying Types of Hemianopsia.
Hemianopsia is the result of a damage to the optic chiasm, or a radiation exposure. Cognitive impairments resulting from cerebral lesions often manifest as deficiencies in color perception.
Historical Background and Physical Assessment
Indicate a potential visual field impairment if the patient appears surprised when approached from one side or if he is unable to perceive items positioned immediately in front of him. To ascertain the nature of the abnormality, compare the visual fields of the patient with your own, assuming that your own values are within the normal range. Initially, instruct the patient to shield his right eye while you shield your left eye. Next, position a pen or a handwriting instrument of comparable shape from the outer edge of his (and your) unprotected eye into his visual field. Request the patient to specify the initial time at which he perceives the thing. Does he perceive it simultaneously with your perception? Upon completion? Proceed to replicate this test in every quadrant of both eyes. Next, for each eye, graph the defect by delineating the region of visual loss by shading the corresponding area of a circle.
Differentiating Categories of Hemianopsia
Visual field abnormalities are caused by lesions of the optic pathways. The location of the lesion dictates the precise nature of the defect. For instance, if a lesion of the optic chiasm affects only the fibers that cross over to the opposite side, it results in bitemporal hemianopsia, which is the loss of vision in the temporal half of each field.
In contrast, a damage to the optic tract or a total damage to the optic radiation results in vision loss in both the left and right halves of the visual field, known as homonymous hemianopsia.
Next, assess the patient's state of awareness (LOC), measure his vital signs, and examine his pupillary response and motor function. Query whether he possesses
Reported recent occurrences of headache, dysarthria, or seizures. Does he have ptosis or weakening in his face or extremities? Experience hallucinations or have impaired color vision? With what onset did neurological problems manifest? Record a comprehensive medical history, specifically focusing on eye diseases, hypertension, diabetes mellitus, and recent head injuries.
Medical etiology
Carotid artery aneurysm
An internal carotid artery aneurysm might result in contralateral or bilateral impairments in the visual fields. Furthermore, it can induce hemiplegia, a reduced level of consciousness, a headache, aphasia, behavioral abnormalities, and unilateral hypoesthesia.
Occipital lobe lesion
Typical symptoms resulting from a lesion in one occipital lobe include incomplete homonymous hemianopsia, scotomas, and reduced color vision. Moreover, the patient may have visual hallucinations characterized by sudden bursts of light or color, as well as visions of objects, individuals, animals, or geometric shapes. These entities might manifest either within the faulty field or migrate towards it from the undamaged field.
Parietal lobe lesion
An injury to the parietal lobe results in homonymous hemianopsia and sensory impairments, including difficulty to detect body position or passive movement, as well as to localize tactile, thermal, or vibratory inputs. Furthermore, it can induce apraxia and visual or tactile agnosia.
Pituitary tumor
The compression of nerve fibers that supply the nasal half of both retinas by a tumor leads to full or partial bitemporal hemianopsia, initially affecting the upper visual fields and potentially advancing to blindness. Correlating symptoms include visual impairment, double vision, a headache, and, in rare cases, drowsiness, low body temperature, and convulsions.
Stroke
Hemianopsia can result when a hemorrhagic, thrombotic, or embolic stroke affects part of the optic pathway. Variations in associated signs and symptoms are contingent upon the site and magnitude of the stroke, but may encompass a reduced level of consciousness (LOC), cognitive impairments such as memory loss and impaired judgment, alterations in personality, emotional instability, headaches, and seizures. Additional symptoms that the patient may have include contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory loss, apraxia, agnosia, aphasia, impaired vision, reduced visual acuity, and diplopia. Furthermore, he may have urinary retention or incontinence, constipation, and vomiting.
Points of Special Consideration
Should the patient exhibit a substantial visual field impairment, additional diagnostic procedures such as perimetry or a tangent screen evaluation may be recommended.
To minimize the risk of surprising the patient, approach him from the side that is not affected and situate his bed in such a way that his unaffected side is facing the entrance. If he is capable of walking, eliminate any items that may lead to falls and caution him about other potential dangers. Strategically position his clock and other personal items within his visual range, but refraining from concealing hazardous items (such as hot meals) from his line of sight.
Therapeutic Counseling for Patients
Elaborate on compensation strategies and stress safety protocols.
Key Pediatric Resources
The most prevalent etiology of hemianopsia in children is a brain tumor. To facilitate the identification of this sign, search for nonverbal cues such as the youngster attempting to grasp a toy but failing to do so. To address his hemianopsia, position things within his visual area and advise his parents to learn this technique as well.
Hemianopsia is the condition characterized by the partial loss of vision in one half of the typical visual field, predominantly affecting either the right or left side of one or both eyes. In cases when the visual field abnormalities are the same in both eyes but impact less than half of the field of vision in each eye (known as incomplete homonymous hemianopsia), the lesion is likely located in the occipital lobe. Otherwise, it is more likely to affect the parietal or temporal lobe. Consult the section on Identifying Types of Hemianopsia.
Hemianopsia is the result of a damage to the optic chiasm, or a radiation exposure. Cognitive impairments resulting from cerebral lesions often manifest as deficiencies in color perception.
Historical Background and Physical Assessment
Indicate a potential visual field impairment if the patient appears surprised when approached from one side or if he is unable to perceive items positioned immediately in front of him. To ascertain the nature of the abnormality, compare the visual fields of the patient with your own, assuming that your own values are within the normal range. Initially, instruct the patient to shield his right eye while you shield your left eye. Next, position a pen or a handwriting instrument of comparable shape from the outer edge of his (and your) unprotected eye into his visual field. Request the patient to specify the initial time at which he perceives the thing. Does he perceive it simultaneously with your perception? Upon completion? Proceed to replicate this test in every quadrant of both eyes. Next, for each eye, graph the defect by delineating the region of visual loss by shading the corresponding area of a circle.
Differentiating Categories of Hemianopsia
Visual field abnormalities are caused by lesions of the optic pathways. The location of the lesion dictates the precise nature of the defect. For instance, if a lesion of the optic chiasm affects only the fibers that cross over to the opposite side, it results in bitemporal hemianopsia, which is the loss of vision in the temporal half of each field.
In contrast, a damage to the optic tract or a total damage to the optic radiation results in vision loss in both the left and right halves of the visual field, known as homonymous hemianopsia.
Next, assess the patient's state of awareness (LOC), measure his vital signs, and examine his pupillary response and motor function. Query whether he possesses
Reported recent occurrences of headache, dysarthria, or seizures. Does he have ptosis or weakening in his face or extremities? Experience hallucinations or have impaired color vision? With what onset did neurological problems manifest? Record a comprehensive medical history, specifically focusing on eye diseases, hypertension, diabetes mellitus, and recent head injuries.
Medical etiology
Carotid artery aneurysm
An internal carotid artery aneurysm might result in contralateral or bilateral impairments in the visual fields. Furthermore, it can induce hemiplegia, a reduced level of consciousness, a headache, aphasia, behavioral abnormalities, and unilateral hypoesthesia.
Occipital lobe lesion
Typical symptoms resulting from a lesion in one occipital lobe include incomplete homonymous hemianopsia, scotomas, and reduced color vision. Moreover, the patient may have visual hallucinations characterized by sudden bursts of light or color, as well as visions of objects, individuals, animals, or geometric shapes. These entities might manifest either within the faulty field or migrate towards it from the undamaged field.
Parietal lobe lesion
An injury to the parietal lobe results in homonymous hemianopsia and sensory impairments, including difficulty to detect body position or passive movement, as well as to localize tactile, thermal, or vibratory inputs. Furthermore, it can induce apraxia and visual or tactile agnosia.
Pituitary tumor
The compression of nerve fibers that supply the nasal half of both retinas by a tumor leads to full or partial bitemporal hemianopsia, initially affecting the upper visual fields and potentially advancing to blindness. Correlating symptoms include visual impairment, double vision, a headache, and, in rare cases, drowsiness, low body temperature, and convulsions.
Stroke
Hemianopsia can result when a hemorrhagic, thrombotic, or embolic stroke affects part of the optic pathway. Variations in associated signs and symptoms are contingent upon the site and magnitude of the stroke, but may encompass a reduced level of consciousness (LOC), cognitive impairments such as memory loss and impaired judgment, alterations in personality, emotional instability, headaches, and seizures. Additional symptoms that the patient may have include contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory loss, apraxia, agnosia, aphasia, impaired vision, reduced visual acuity, and diplopia. Furthermore, he may have urinary retention or incontinence, constipation, and vomiting.
Points of Special Consideration
Should the patient exhibit a substantial visual field impairment, additional diagnostic procedures such as perimetry or a tangent screen evaluation may be recommended.
To minimize the risk of surprising the patient, approach him from the side that is not affected and situate his bed in such a way that his unaffected side is facing the entrance. If he is capable of walking, eliminate any items that may lead to falls and caution him about other potential dangers. Strategically position his clock and other personal items within his visual range, but refraining from concealing hazardous items (such as hot meals) from his line of sight.
Therapeutic Counseling for Patients
Elaborate on compensation strategies and stress safety protocols.
Key Pediatric Resources
The most prevalent etiology of hemianopsia in children is a brain tumor. To facilitate the identification of this sign, search for nonverbal cues such as the youngster attempting to grasp a toy but failing to do so. To address his hemianopsia, position things within his visual area and advise his parents to learn this technique as well.
- Published on
Symptoms and Signs – Differential Diagnosis of Hematuria
Hematuria is an essential indicator of renal and urinary tract diseases, characterized by the undesired occurrence of blood in urine. More precisely, it refers to the presence of three or more red blood cells (RBCs) per high-power microscopic field in urine. A confirmation of microscopic hematuria is obtained by an occult blood test, although macroscopic hematuria is readily apparent. However, it is important to differentiate macroscopic hematuria from pseudohematuria. See Confirming Hematuria. Hematuria by macroscopic examination
May manifest as either continuous or intermittent, is often accompanied by pain, and can be worsened by extended periods of standing or walking.
Verification of Hematuria
To diagnose the patient with blood-tinged urine, ensure to exclude pseudohematuria, which is the presence of red or pink urine resulting from urinary pigments. Prioritise meticulous examination of the urine sample. The presence of crimson sediment almost certainly indicates real hematuria.
Furthermore, verify the patient's medical records for the administration of medications linked to pseudohematuria, such as rifampin, chlorzoxazone, phenazopyridine, phenothiazines, doxorubicin, phensuximide, phenytoin, daunomycin, and laxatives containing phenolphthalein.
Inquire about the patient's consumption of beets, berries, or foods containing red colored pigments that could potentially cause the urine to appear red. Notably, pseudohematuria can also be caused by porphyrinuria and excessive urate excretion.
Lastly, analyze the urine by means of a chemical reagent strip. This assay can definitively detect even minute hematuria and can also approximate the quantity of blood in the urine.
Hematuria can be categorized dependent on the specific stage of urination that it mostly impacts. Initial hematuria refers to bleeding at the beginning of urination, which often suggests urethral disease. Terminal hematuria refers to bleeding at the end of urination, which typically indicates disease of the bladder neck, posterior urethra, or prostate. Total hematuria refers to bleeding throughout urination, which typically indicates an underlying disease above the bladder neck.
Hematuria can occur due to two mechanisms: either the rupture or perforation of blood vessels in the renal system or urinary tract, or the decreased filtration of ROBCs into the urine caused by impaired glomerular function. The hue of the hematuric urine offers insight into the origin of the hemorrhage. In general, dark or brownish blood signifies bleeding in the kidneys or upper urinary tract, while bright red blood denotes bleeding in the lower urinary tract.
While hematuria is commonly associated with renal and urinary tract diseases, it can also arise from specific gastrointestinal, prostate, vaginal, or coagulation illnesses, as well as from the effects of certain medications. Hematuria can also be caused by invasive interventions and diagnostic investigations that require manipulative instrumentation of the renal and urologic systems. Fever and associated nonpathologic hematuria may occur.
States of hypercatabolism. After intense physical activity, transient hematuria may occur.
History and Physical Examination
Following the identification of hematuria, obtain a relevant medical history. In cases of macroscopic hematuria, inquire about the patient's initial observation of blood in their urine. Does its harshness differ between voidings? Does it exhibit more severity during the onset, middle, or conclusion of urination? Has this happened previously? Has the patient exhibited thrombotic events? Request information regarding bleeding hemorrhoids or the initiation of menstruation, if relevant, to exclude the possibility of artifactitious hematuria. Ask if there is any sensation of pain or burning during episodes of hematuria.
Inquire about any incidence of recent abdominal or flank trauma. Has the patient engaged in intense physical activity? Document any previous occurrences of renal, urinary, prostatic, or coagulation abnormalities. Then get a medication history, specifically mentioning anticoagulants or aspirin.
The physical examination should commence with the application of pressure and percussion to the abdomen and flanks. Next, apply pressure to the costovertebral angle (CVA) to evoke tenderness. Conduct a thorough examination of the urinary meatus for any signs of blood or irregularities. Utilise a chemical reagent strip to analyse a urine sample for protein content. Either a vaginal or digital rectal examination may be required.
Medical Causes
Bladder cancer
Bladder cancer, a leading cause of gross hematuria in males, can also bring about pain in the bladder, rectum, pelvis, flank, back, or leg. Additional typical symptoms include nocturia, dysuria, increased frequency and urgency of urination, vomiting, intestinal distress, and sleeplessness.
Bladder trauma
A distinctive feature of traumatic bladder rupture or perforation is the presence of gross hematuria. Commonly, hematuria is accompanied with lower abdomen pain and, in rare cases, anuria despite a strong urge to urinate. In addition, the patient may experience edema in the scrotum, buttocks, or perineum, as well as the manifestation of shock symptoms like rapid heart rate and low blood pressure.
Calculi
Hematuria produces by bladder and renal calculi may be accompanied by symptoms of a urinary tract infection (UTI), including dysuria and increased frequency and urgency of urination. Typically, bladder calculi result in gross hematuria, pain that radiates to the lower back, penile, or vulvar region, and, in certain cases, bladder distension.
Renal calculi can cause either microscopic or extensive hematuria. The primary indication, however, is the abrupt and intense pain that radiates from the central venous artery to the flank, suprapubic area, and external genitalia upon the passage of a calculus. The Pain can be absolutely agonizing at its maximum intensity. Additional indications and manifestations may encompass emesis, agitation, pyrexia, rigor, excessive abdominal distension, and, potentially, diminished gastrointestinal noises.
Cortical necrosis (acute)
In acute cortical necrosis, the presence of gross hematuria is accompanied with severe flank pain, urinary retention, increased white blood cell count, and fever.
Cystitis
Hematuria is a characteristic feature in all forms of cystitis. The typical presentation of bacterial cystitis is macroscopic hematuria accompanied by urine urgency and frequency, dysuria, nocturia, and tenesmus. The patient presents with perineal and lumbar pain, suprapubic discomfort, exhaustion, and intermittent episodes of low-grade fever.
Most prevalent in women, persistent interstitial cystitis sometimes results in visibly bloody hematuria. Characteristics commonly associated with this condition are increased frequency of urination, dysuria, nocturia, and tenesmus. In tubercular cystitis, microscopic and macroscopic hematuria might manifest, along with symptoms such as urine urgency and frequency, dysuria, tenesmus, flank discomfort, weariness, and anorexia. A typical presentation of viral cystitis is hematuria, urine urgency and frequency, dysuria, nocturia, tenesmus, and fever.
Diverticulitis
Should diverticulitis affect the bladder, it often results in microscopic hematuria, increased frequency and urgency of urination, dysuria, and Nocturia. Characteristic observations include pain in the lower left quadrant, tenderness in the abdomen, constipation or diarrhea, and occasionally a palpable, firm, fixed, and tender mass in the abdomen. In addition, the patient may experience slight nausea, flatulence, and a low-grade temperature.
Glomerulonephritis
Initial symptoms of acute glomerulonephritis often include gross hematuria, which gradually progresses to microscopic hematuria and red cell casts, and can last for several months. In addition, it can cause oliguria or anuria, proteinuria, a slight temperature, weariness, inflammation of the flank and abdomen, widespread swelling, elevated blood pressure, nausea, vomiting, and indications of lung congestion, such as crackles and a productive cough.
Primary manifestations of chronic glomerulonephritis can include microscopic hematuria, proteinuria, widespread edema, and elevated blood pressure. In severe stages of renal illness, signs and symptoms of uremia may also manifest.
Chronic interstitial nephritis
The usual manifestation of nephritis is microscopic hematuria. The patient suffering from acute interstitial nephritis may, however, experience gross hematuria. Additional features include pyrexia, a maculopapular eruption, and reduced urine output or absence of urine. In chronic interstitial nephritis, the patient presents with urine that is dilute, nearly colorless, and may be accompanied by excessive urination and elevated blood pressure.
Nephropathy (obstructive). Although microscopic or macroscopic hematuria may be caused by obstructive nephropathy, urine is seldom visibly colored with blood. The patient presents with colicky flank and abdominal pain, tenderness in the cerebrovascular accident (CVA), and alternating episodes of anuria or oliguria as well as polyuria.
Polycystic kidney disease
The inherited condition known as polycystic kidney disease can result in recurring microscopic or large hematuria. Predominantly asymptomatic until the age of 40, this condition can lead to elevated blood pressure, excessive urination, dull flank discomfort, and indications of a urinary tract infection, such as dysuria and urine frequency and urgency. In due course, the patient experiences an enlarged and sensitive belly, as well as lumbar discomfort that is worsened by physical activity and alleviated by reclining. Additionally, he may experience proteinuria and colicky abdominal pain caused by the presence of clots or stones in the ureteral canal.
Prostatitis
Prostatitis, whether acute or chronic, can result in visible blood in the urine, often detected at the end of urination. The condition may also cause increased frequency and urgency of urination, as well as dysuria accompanied by noticeable distension of the bladder. The clinical manifestations of acute prostatitis include fatigue, malaise, myalgia, polyarthralgia, fever accompanied by chills, nausea, vomiting, perineal and low back discomfort, and a reduced libido. Upon rectal probing, a painful, bloated, swampy, firm
prostate.
Typically, chronic prostatitis occurs after an acute inflammation. It can result in chronic urethral discharge, dull perineal soreness, ejaculatory symptoms, and reduced sexual desire.
Pyelonephritis (acute). One common manifestation of acute pyelonephritis is the development of microscopic or macroscopic hematuria, which then advances to severely bloody hematuria. Following the resolution of the illness, microscopic hematuria may continue for a few months. Associated indications and manifestations include a chronic elevated body temperature, pain in one or both flanks, sensitivity to cerebrovascular accidents (CVAs), tremors, debility, exhaustion, urinary retention, increased frequency and urgency of urination, night sweats, and heightened pulse rate. Furthermore, the patient may present with symptoms of nausea, anorexia, vomiting, and indications of paralytic ileus, such as reduced or nonexistent bowel sounds and abdominal distension.
Renal cancer
Typical symptoms include visibly crimson urine, chronic side pain, and a palpable lump or tumor in the either the side or abdomen. Passage of clots may be accompanied by colicky pain. Additional observations include pyrexia, constriction of the cerebral arteries, and elevated blood pressure. With severe disease, the patient may experience weight loss as well as nausea and vomiting.
Renal infarction
As a general rule, renal infarction results in gross hematuria. The patient may present with persistent, intense flank and upper abdomen discomfort accompanied by tenderness in the central venous artery, loss of appetite, and feelings of nausea and vomiting. Further observations include the presence of oliguria or anuria, proteinuria, hypoactive bowel sounds, and, within one to two days following the infarction, a fever and elevated blood pressure.
Renal papillary necrosis (acute)
An acute renal papillary necrosis often results in visibly bloody hematuria, followed by severe flank pain, discomfort in the carotid artery, abdominal stiffness and colicky pain, oliguria or anuria, pyuria, fever, chills, vomiting, and hypoactive bowel sounds. Prevalence of arthritis and hypertension is high.
Renal trauma
Approximately 80% of those who have experienced renal trauma have either microscopic or gross hematuria. Potential accompanying manifestations may encompass flank pain, a detectable mass on the flank, reduced urine output, hematoma or ecchymoses on the upper abdomen or flank, nausea and vomiting, and reduced bowel noises. Serious injury can trigger symptoms of shock, including rapid heart rate and low blood pressure.
Renal tuberculosis
First indication of renal TB is often gross hematuria. Concomitant symptoms include increased frequency of urination, difficulty urinating, excessive urination, muscle tension, painful abdomen, back discomfort, and presence of protein in the urine.
Renal vein thrombosis
Hematuria with gross bloodstained appearance often arises in cases of renal vein thrombosis. An abrupt venous blockage is characterized by the patient experiencing Persistent flank and lumbar pain, together with tenderness in the epigastric and CVA regions. Additional characteristics include pyrexia, pallor, proteinuria, peripheral edema, and, in cases of bilateral blockage, oliguria or anuria along with other uremic complications. The kidneys can be readily palpated. Progressing blockage of the veins leads to symptoms of nephrotic syndrome, proteinuria, and, in rare cases, peripheral edema.
Schistosomiasis
Schistosomiasis often results in sporadic hematuria occurring with urine. Complicating symptoms may include dysuria, colicky renal and bladder pain, and palpable lumps in the lower abdomen.
Sickle cell anemia
Sickle cell anemia is an inherited condition characterized by the presence of extensive hematuria occurring due to the congestion of the renal papillae. Common concomitant manifestations may encompass pallor, dehydration, persistent fatigue, polyarthralgia, leg ulcers, dyspnea, chest pain, hindered growth and development, hepatomegaly, and perhaps, jaundice. Auscultation detects rapid heart rate and murmurs of both systolic and diastolic contractions.
Systemic lupus erythematosus (SLE)
Gross hematuria and proteinuria may occur when SLE attacks the kidneys. The primary characteristics commonly linked with this condition are nondeforming joint pain and stiffness, a butterfly rash, sensitivity to light, Raynaud's phenomena, seizures or psychoses, a recurring fever, lymphadenopathy, oral or nasopharyngeal ulcers, anorexia, and weight loss.
Urethral trauma. Primary hematuria may manifest as blood in the urine meatus, accompanied by localised discomfort and ecchymoses in the penis or vulva.
Vasculitis often presents with microscopic hematuria. Common manifestations include fatigue, muscle soreness, pain in many joints, elevated body temperature, elevated blood pressure, paleness, and, sometimes, abnormal urine output. Additional symptoms, such as urticaria and purpura, probably indicate the cause of vasculitis.
Medical diagnostic testing. A renal biopsy is the diagnostic procedure most often linked to hematuria. A biopsy or manipulative instrumentation of the urinary system, such as in cystoscopy, may also cause this indication. Substance abuse. Pharmacological substances that frequently induce hematuria include anticoagulants, aspirin (with potential toxicity), analgesics, cyclophosphamide, metyrosine, phenylbutazone, oxyphenbutazone, penicillin, rifampin, and thiabendazole.
When used in conjunction with an anticoagulant, herbal treatments, such as garlic and
Administration of Ginkgo biloba may result in unfavourable responses, such as profuse bleeding and hematuria.
Therapeutic interventions. Therapeutic procedures that include the use of manipulative instruments to manipulate the urinary system, such as transurethral prostatectomy, have the potential to induce either microscopic or macroscopic hematuria. Following a kidney transplant, a patient may develop hematuria, with or without clots, necessitating the use of an indwelling urinary catheter for irrigation.
Points of Special Consideration
As hematuria might generate fear and distress in the patient, ensure to offer emotional support. Assess his vital signs at minimum every four hours and monitor fluid intake and output, including the volume and pattern of hematuria. Verify the patency of the indwelling urinary catheter in the patient and, if needed, irrigate it to eliminate any clots and tissue that could hinder urine outflow. Administer prescription analgesics and compel confinement to bed as necessary. Schedule the patient for diagnostic examinations, including blood and urine testing, cystoscopy, and renal X-rays or biopsies.
Therapeutic Counseling for Patients
Provide the patient with instructions on the three-glass approach for collecting sequence urine samples. Highlight the necessity of augmenting his consumption of fluids.
Guidelines for Pediatric Populations
A significant number of the factors outlined in this section also result in hematuria in children. Cyclophosphamide is somewhat more prone to induce hematuria in children than to adults.
Primary etiologies of hematuria in children include congenital abnormalities, such as obstructive uropathy and renal dysplasia; birth trauma; hematologic diseases, including vitamin K deficiency, hemophilia, and hemolytic-uremic syndrome; specific malignancies, such as Wilms tumor, bladder cancer, and rhabdomyosarcoma; allergies; and the presence of foreign agents in the urinary tract. Artifactual hematuria can occur as a consequence of surgical circumcision.
Geriatric Guidelines
Thorough assessment of hematuria in older people should involve a urine culture, excretory urography or sonography, and seeking advice from a urologist.
Hematuria is an essential indicator of renal and urinary tract diseases, characterized by the undesired occurrence of blood in urine. More precisely, it refers to the presence of three or more red blood cells (RBCs) per high-power microscopic field in urine. A confirmation of microscopic hematuria is obtained by an occult blood test, although macroscopic hematuria is readily apparent. However, it is important to differentiate macroscopic hematuria from pseudohematuria. See Confirming Hematuria. Hematuria by macroscopic examination
May manifest as either continuous or intermittent, is often accompanied by pain, and can be worsened by extended periods of standing or walking.
Verification of Hematuria
To diagnose the patient with blood-tinged urine, ensure to exclude pseudohematuria, which is the presence of red or pink urine resulting from urinary pigments. Prioritise meticulous examination of the urine sample. The presence of crimson sediment almost certainly indicates real hematuria.
Furthermore, verify the patient's medical records for the administration of medications linked to pseudohematuria, such as rifampin, chlorzoxazone, phenazopyridine, phenothiazines, doxorubicin, phensuximide, phenytoin, daunomycin, and laxatives containing phenolphthalein.
Inquire about the patient's consumption of beets, berries, or foods containing red colored pigments that could potentially cause the urine to appear red. Notably, pseudohematuria can also be caused by porphyrinuria and excessive urate excretion.
Lastly, analyze the urine by means of a chemical reagent strip. This assay can definitively detect even minute hematuria and can also approximate the quantity of blood in the urine.
Hematuria can be categorized dependent on the specific stage of urination that it mostly impacts. Initial hematuria refers to bleeding at the beginning of urination, which often suggests urethral disease. Terminal hematuria refers to bleeding at the end of urination, which typically indicates disease of the bladder neck, posterior urethra, or prostate. Total hematuria refers to bleeding throughout urination, which typically indicates an underlying disease above the bladder neck.
Hematuria can occur due to two mechanisms: either the rupture or perforation of blood vessels in the renal system or urinary tract, or the decreased filtration of ROBCs into the urine caused by impaired glomerular function. The hue of the hematuric urine offers insight into the origin of the hemorrhage. In general, dark or brownish blood signifies bleeding in the kidneys or upper urinary tract, while bright red blood denotes bleeding in the lower urinary tract.
While hematuria is commonly associated with renal and urinary tract diseases, it can also arise from specific gastrointestinal, prostate, vaginal, or coagulation illnesses, as well as from the effects of certain medications. Hematuria can also be caused by invasive interventions and diagnostic investigations that require manipulative instrumentation of the renal and urologic systems. Fever and associated nonpathologic hematuria may occur.
States of hypercatabolism. After intense physical activity, transient hematuria may occur.
History and Physical Examination
Following the identification of hematuria, obtain a relevant medical history. In cases of macroscopic hematuria, inquire about the patient's initial observation of blood in their urine. Does its harshness differ between voidings? Does it exhibit more severity during the onset, middle, or conclusion of urination? Has this happened previously? Has the patient exhibited thrombotic events? Request information regarding bleeding hemorrhoids or the initiation of menstruation, if relevant, to exclude the possibility of artifactitious hematuria. Ask if there is any sensation of pain or burning during episodes of hematuria.
Inquire about any incidence of recent abdominal or flank trauma. Has the patient engaged in intense physical activity? Document any previous occurrences of renal, urinary, prostatic, or coagulation abnormalities. Then get a medication history, specifically mentioning anticoagulants or aspirin.
The physical examination should commence with the application of pressure and percussion to the abdomen and flanks. Next, apply pressure to the costovertebral angle (CVA) to evoke tenderness. Conduct a thorough examination of the urinary meatus for any signs of blood or irregularities. Utilise a chemical reagent strip to analyse a urine sample for protein content. Either a vaginal or digital rectal examination may be required.
Medical Causes
Bladder cancer
Bladder cancer, a leading cause of gross hematuria in males, can also bring about pain in the bladder, rectum, pelvis, flank, back, or leg. Additional typical symptoms include nocturia, dysuria, increased frequency and urgency of urination, vomiting, intestinal distress, and sleeplessness.
Bladder trauma
A distinctive feature of traumatic bladder rupture or perforation is the presence of gross hematuria. Commonly, hematuria is accompanied with lower abdomen pain and, in rare cases, anuria despite a strong urge to urinate. In addition, the patient may experience edema in the scrotum, buttocks, or perineum, as well as the manifestation of shock symptoms like rapid heart rate and low blood pressure.
Calculi
Hematuria produces by bladder and renal calculi may be accompanied by symptoms of a urinary tract infection (UTI), including dysuria and increased frequency and urgency of urination. Typically, bladder calculi result in gross hematuria, pain that radiates to the lower back, penile, or vulvar region, and, in certain cases, bladder distension.
Renal calculi can cause either microscopic or extensive hematuria. The primary indication, however, is the abrupt and intense pain that radiates from the central venous artery to the flank, suprapubic area, and external genitalia upon the passage of a calculus. The Pain can be absolutely agonizing at its maximum intensity. Additional indications and manifestations may encompass emesis, agitation, pyrexia, rigor, excessive abdominal distension, and, potentially, diminished gastrointestinal noises.
Cortical necrosis (acute)
In acute cortical necrosis, the presence of gross hematuria is accompanied with severe flank pain, urinary retention, increased white blood cell count, and fever.
Cystitis
Hematuria is a characteristic feature in all forms of cystitis. The typical presentation of bacterial cystitis is macroscopic hematuria accompanied by urine urgency and frequency, dysuria, nocturia, and tenesmus. The patient presents with perineal and lumbar pain, suprapubic discomfort, exhaustion, and intermittent episodes of low-grade fever.
Most prevalent in women, persistent interstitial cystitis sometimes results in visibly bloody hematuria. Characteristics commonly associated with this condition are increased frequency of urination, dysuria, nocturia, and tenesmus. In tubercular cystitis, microscopic and macroscopic hematuria might manifest, along with symptoms such as urine urgency and frequency, dysuria, tenesmus, flank discomfort, weariness, and anorexia. A typical presentation of viral cystitis is hematuria, urine urgency and frequency, dysuria, nocturia, tenesmus, and fever.
Diverticulitis
Should diverticulitis affect the bladder, it often results in microscopic hematuria, increased frequency and urgency of urination, dysuria, and Nocturia. Characteristic observations include pain in the lower left quadrant, tenderness in the abdomen, constipation or diarrhea, and occasionally a palpable, firm, fixed, and tender mass in the abdomen. In addition, the patient may experience slight nausea, flatulence, and a low-grade temperature.
Glomerulonephritis
Initial symptoms of acute glomerulonephritis often include gross hematuria, which gradually progresses to microscopic hematuria and red cell casts, and can last for several months. In addition, it can cause oliguria or anuria, proteinuria, a slight temperature, weariness, inflammation of the flank and abdomen, widespread swelling, elevated blood pressure, nausea, vomiting, and indications of lung congestion, such as crackles and a productive cough.
Primary manifestations of chronic glomerulonephritis can include microscopic hematuria, proteinuria, widespread edema, and elevated blood pressure. In severe stages of renal illness, signs and symptoms of uremia may also manifest.
Chronic interstitial nephritis
The usual manifestation of nephritis is microscopic hematuria. The patient suffering from acute interstitial nephritis may, however, experience gross hematuria. Additional features include pyrexia, a maculopapular eruption, and reduced urine output or absence of urine. In chronic interstitial nephritis, the patient presents with urine that is dilute, nearly colorless, and may be accompanied by excessive urination and elevated blood pressure.
Nephropathy (obstructive). Although microscopic or macroscopic hematuria may be caused by obstructive nephropathy, urine is seldom visibly colored with blood. The patient presents with colicky flank and abdominal pain, tenderness in the cerebrovascular accident (CVA), and alternating episodes of anuria or oliguria as well as polyuria.
Polycystic kidney disease
The inherited condition known as polycystic kidney disease can result in recurring microscopic or large hematuria. Predominantly asymptomatic until the age of 40, this condition can lead to elevated blood pressure, excessive urination, dull flank discomfort, and indications of a urinary tract infection, such as dysuria and urine frequency and urgency. In due course, the patient experiences an enlarged and sensitive belly, as well as lumbar discomfort that is worsened by physical activity and alleviated by reclining. Additionally, he may experience proteinuria and colicky abdominal pain caused by the presence of clots or stones in the ureteral canal.
Prostatitis
Prostatitis, whether acute or chronic, can result in visible blood in the urine, often detected at the end of urination. The condition may also cause increased frequency and urgency of urination, as well as dysuria accompanied by noticeable distension of the bladder. The clinical manifestations of acute prostatitis include fatigue, malaise, myalgia, polyarthralgia, fever accompanied by chills, nausea, vomiting, perineal and low back discomfort, and a reduced libido. Upon rectal probing, a painful, bloated, swampy, firm
prostate.
Typically, chronic prostatitis occurs after an acute inflammation. It can result in chronic urethral discharge, dull perineal soreness, ejaculatory symptoms, and reduced sexual desire.
Pyelonephritis (acute). One common manifestation of acute pyelonephritis is the development of microscopic or macroscopic hematuria, which then advances to severely bloody hematuria. Following the resolution of the illness, microscopic hematuria may continue for a few months. Associated indications and manifestations include a chronic elevated body temperature, pain in one or both flanks, sensitivity to cerebrovascular accidents (CVAs), tremors, debility, exhaustion, urinary retention, increased frequency and urgency of urination, night sweats, and heightened pulse rate. Furthermore, the patient may present with symptoms of nausea, anorexia, vomiting, and indications of paralytic ileus, such as reduced or nonexistent bowel sounds and abdominal distension.
Renal cancer
Typical symptoms include visibly crimson urine, chronic side pain, and a palpable lump or tumor in the either the side or abdomen. Passage of clots may be accompanied by colicky pain. Additional observations include pyrexia, constriction of the cerebral arteries, and elevated blood pressure. With severe disease, the patient may experience weight loss as well as nausea and vomiting.
Renal infarction
As a general rule, renal infarction results in gross hematuria. The patient may present with persistent, intense flank and upper abdomen discomfort accompanied by tenderness in the central venous artery, loss of appetite, and feelings of nausea and vomiting. Further observations include the presence of oliguria or anuria, proteinuria, hypoactive bowel sounds, and, within one to two days following the infarction, a fever and elevated blood pressure.
Renal papillary necrosis (acute)
An acute renal papillary necrosis often results in visibly bloody hematuria, followed by severe flank pain, discomfort in the carotid artery, abdominal stiffness and colicky pain, oliguria or anuria, pyuria, fever, chills, vomiting, and hypoactive bowel sounds. Prevalence of arthritis and hypertension is high.
Renal trauma
Approximately 80% of those who have experienced renal trauma have either microscopic or gross hematuria. Potential accompanying manifestations may encompass flank pain, a detectable mass on the flank, reduced urine output, hematoma or ecchymoses on the upper abdomen or flank, nausea and vomiting, and reduced bowel noises. Serious injury can trigger symptoms of shock, including rapid heart rate and low blood pressure.
Renal tuberculosis
First indication of renal TB is often gross hematuria. Concomitant symptoms include increased frequency of urination, difficulty urinating, excessive urination, muscle tension, painful abdomen, back discomfort, and presence of protein in the urine.
Renal vein thrombosis
Hematuria with gross bloodstained appearance often arises in cases of renal vein thrombosis. An abrupt venous blockage is characterized by the patient experiencing Persistent flank and lumbar pain, together with tenderness in the epigastric and CVA regions. Additional characteristics include pyrexia, pallor, proteinuria, peripheral edema, and, in cases of bilateral blockage, oliguria or anuria along with other uremic complications. The kidneys can be readily palpated. Progressing blockage of the veins leads to symptoms of nephrotic syndrome, proteinuria, and, in rare cases, peripheral edema.
Schistosomiasis
Schistosomiasis often results in sporadic hematuria occurring with urine. Complicating symptoms may include dysuria, colicky renal and bladder pain, and palpable lumps in the lower abdomen.
Sickle cell anemia
Sickle cell anemia is an inherited condition characterized by the presence of extensive hematuria occurring due to the congestion of the renal papillae. Common concomitant manifestations may encompass pallor, dehydration, persistent fatigue, polyarthralgia, leg ulcers, dyspnea, chest pain, hindered growth and development, hepatomegaly, and perhaps, jaundice. Auscultation detects rapid heart rate and murmurs of both systolic and diastolic contractions.
Systemic lupus erythematosus (SLE)
Gross hematuria and proteinuria may occur when SLE attacks the kidneys. The primary characteristics commonly linked with this condition are nondeforming joint pain and stiffness, a butterfly rash, sensitivity to light, Raynaud's phenomena, seizures or psychoses, a recurring fever, lymphadenopathy, oral or nasopharyngeal ulcers, anorexia, and weight loss.
Urethral trauma. Primary hematuria may manifest as blood in the urine meatus, accompanied by localised discomfort and ecchymoses in the penis or vulva.
Vasculitis often presents with microscopic hematuria. Common manifestations include fatigue, muscle soreness, pain in many joints, elevated body temperature, elevated blood pressure, paleness, and, sometimes, abnormal urine output. Additional symptoms, such as urticaria and purpura, probably indicate the cause of vasculitis.
Medical diagnostic testing. A renal biopsy is the diagnostic procedure most often linked to hematuria. A biopsy or manipulative instrumentation of the urinary system, such as in cystoscopy, may also cause this indication. Substance abuse. Pharmacological substances that frequently induce hematuria include anticoagulants, aspirin (with potential toxicity), analgesics, cyclophosphamide, metyrosine, phenylbutazone, oxyphenbutazone, penicillin, rifampin, and thiabendazole.
When used in conjunction with an anticoagulant, herbal treatments, such as garlic and
Administration of Ginkgo biloba may result in unfavourable responses, such as profuse bleeding and hematuria.
Therapeutic interventions. Therapeutic procedures that include the use of manipulative instruments to manipulate the urinary system, such as transurethral prostatectomy, have the potential to induce either microscopic or macroscopic hematuria. Following a kidney transplant, a patient may develop hematuria, with or without clots, necessitating the use of an indwelling urinary catheter for irrigation.
Points of Special Consideration
As hematuria might generate fear and distress in the patient, ensure to offer emotional support. Assess his vital signs at minimum every four hours and monitor fluid intake and output, including the volume and pattern of hematuria. Verify the patency of the indwelling urinary catheter in the patient and, if needed, irrigate it to eliminate any clots and tissue that could hinder urine outflow. Administer prescription analgesics and compel confinement to bed as necessary. Schedule the patient for diagnostic examinations, including blood and urine testing, cystoscopy, and renal X-rays or biopsies.
Therapeutic Counseling for Patients
Provide the patient with instructions on the three-glass approach for collecting sequence urine samples. Highlight the necessity of augmenting his consumption of fluids.
Guidelines for Pediatric Populations
A significant number of the factors outlined in this section also result in hematuria in children. Cyclophosphamide is somewhat more prone to induce hematuria in children than to adults.
Primary etiologies of hematuria in children include congenital abnormalities, such as obstructive uropathy and renal dysplasia; birth trauma; hematologic diseases, including vitamin K deficiency, hemophilia, and hemolytic-uremic syndrome; specific malignancies, such as Wilms tumor, bladder cancer, and rhabdomyosarcoma; allergies; and the presence of foreign agents in the urinary tract. Artifactual hematuria can occur as a consequence of surgical circumcision.
Geriatric Guidelines
Thorough assessment of hematuria in older people should involve a urine culture, excretory urography or sonography, and seeking advice from a urologist.
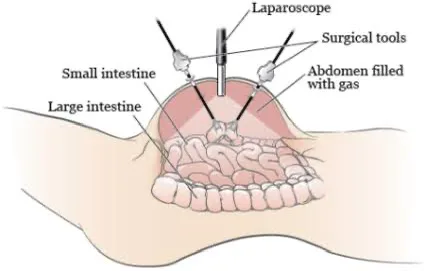
- Published on
Symptoms and Signs – Differential Diagnosis of Haematochezia, sometimes known as rectal hemorrhage,
Hematochezia, the passing of bloody stools, often presents as an early indication of gastrointestinal bleeding below the ligament of Treitz. Although typically preceded by hematemesis, this symptom may also occur with a fast bleeding of 1 L or more from the upper gastrointestinal tract.
The spectrum of hematochezia includes both solid, blood-streaked feces and liquid, bloody stools that might be deep crimson, dark mahogany, or maroon in hue. Typically, this indication manifests suddenly and is preceded by stomach pain.
While hematochezia is often linked to gastrointestinal complications, it can also arise from a coagulation abnormality, exposure to chemicals, or specific diagnostic procedures. Always an important indication, hematochezia can trigger potentially fatal hypovolemia.
Urgent medical interventions
If the patient presents with grave hematochezia, assess his vital signs. Upon observing indications of shock, such as low blood pressure and rapid heart rate, arrange the patient in a supine posture and raise his feet by 20 to 30 degrees. Make necessary arrangements to provide oxygen therapy and initiate a large-bore intravenous line for immediate fluid replenishment. The next step is to collect a blood sample for typing and crossmatching, measuring the hemoglobin level and hematocrit. Introduce a nasogastric tube. Administering iced lavage may be recommended to manage bleeding. Urgent endoscopy may be required to identify the origin of the bleeding.
Historical Background and Physical Assessment
If hematochezia is not immediately life-threatening, get the patient to provide a detailed account of the quantity, hue, and texture of his bloody feces. (If feasible, personally examine and describe the stools as well.) For how long have the stools exhibited hematochezia? Do their appearances generally remain consistent, or does the quantity of blood appear to fluctuate? Enquire about any related indications and manifestations.
Proceed to examine the patient's medical history, with particular attention to gastrointestinal and coagulation status.
Pathologies. Request information regarding the use of gastrointestinal irritants, including alcohol, aspirin, and other nonsteroidal anti-inflammatory medications (NSAIDs).
Initiate the physical survey by assessing for orthostatic hypotension, a first indication of shock. Measure the patient's blood pressure and pulse in supine, seated, and standing positions. Should the systolic pressure drop by 10 mm Hg or more or the pulse rate rise by 10 beats/minute or more upon changing position, it is advisable to consider the possibility of volume depletion and an imminent shock.
Assess the skin for the presence of petechiae or spider angiomas. Evaluate the abdomen by palpating for any signs of tenderness, pain, or lumps. Furthermore, observe lymphadenopathy. Finally, a digital rectal examination is necessary to exclude the presence of rectal tumors or hemorrhoids.
Medical etiology
Anal fissure. Minor hematochezia is a defining feature of anal fissure; blood may streak the feces or be seen on toilet tissue. Hematochezia is accompanied by intense rectal pain, which can lead to constipation by leading the patient to be reluctant to defecate.
Angiodysplastic lesions
Typically seen in older individuals, these arteriovenous lesions of the ascending colon often result in persistent, vivid red rectal bleeding. On rare occasions, this painless hematochezia can lead to potentially fatal blood loss and symptoms of shock, such as rapid heart rate and low arterial pressure.
Coagulation disorders
Individuals diagnosed with a coagulation condition, such as thrombocytopenia and disseminated intravascular coagulation, may have gastrointestinal bleeding characterized by mild to severe hematochezia. Bleeding can also manifest in other bodies systems, resulting in symptoms such as epistaxis and purpura. The associated findings differ depending on the particular coagulation problem.
Colitis
Especially in older people, ischemic colitis often results in bloody diarrhea. Haematochezia can manifest as either mild or significant and is often accompanied by intense, cramping lower abdomen discomfort and low blood pressure. Additional symptoms include gastric pain, distension, and lack of intestinal noises. Profound colitis can lead to potentially fatal hypovolemic shock and peritonitis.
In general, ulcerative colitis is characterized by the presence of bloody diarrhea that may also include mucus. Hematochezia is preceded by a range of abdominal pains, from mild to severe, and can result in very little to significant blood loss. Compound manifestations include pyrexia, anorexia, emesis, dyspepsia, tachycardia, and, on rare occasions, atrial fibrillation. Weight loss and weakness manifest in the later stages.
Colorectal carcinoma
Conspicuous crimson rectal bleeding, with or without pain, is a diagnostic indicator, particularly in cases of left colon cancer.
In most cases, a left colon tumor presents with initial indications of blockage, including rectal pressure, hemorrhage, and sporadic feelings of fullness or cramping. As the condition advances, the patient also has constipation, diarrhea characterized by ribbon-shaped feces, and chronic pain, which is usually alleviated by the passage of stools or flatus. The stool is visibly hematochezic.
Neoplasm development in the right colon at an early stage can result in melena, abdominal pain, pressure, and dull cramps. With advancing disease, the patient experiences a decline in physical strength and persistent tiredness. Further symptoms he may encounter include diarrhea, anorexia, weight loss, anemia, vomiting, an abdominal mass, and indications of blockage, such as abdominal distension and irregular bowel sounds.
Colorectal polyps.
Intermittent hematochezia in individuals under the age of 60 is mostly caused by colorectal polyps, although in certain cases these lesions may provide no symptoms. Polyps positioned high in the colon can result in the presence of blood-streaked feces. The feces exhibit a positive reaction when subjected to guaiac testing. Should the polyps be situated in greater proximity to the rectum, they may exhibit unrestricted bleeding.
Diverticulitis
In the elderly, diverticulitis often presents as a rapid onset of mild to severe rectal bleeding following the patient's urge to defecate. The bleeding may cease suddenly or may advance to life-threatening hemorrhage accompanied by symptoms of shock. Common indications and manifestations may include pain in the lower left quadrant that is alleviated by defecation, alternating bouts of constipation and diarrhea, loss of appetite, feelings of nausea and vomiting, irritation and tenderness in the abdomen, and a swollen belly.
Dysentery
Infection with Shigella, Amoeba, and Campylobacter often results in bloody diarrhea, although it is far less prevalent with Salmonella. May also manifest as abdominal pain or cramps, tenesmus, fever, and nausea.
Ruptured esophageal varices
For esophageal varices, a potentially fatal condition, hematochezia can vary from little rectal leakage to visibly bloody feces and may be followed by moderate to severe hematemesis or melena. Although painless, this substantial bleeding can trigger symptoms of shock, including rapid heart rate and low blood pressure. Indeed, symptoms of shock sometimes occur before obvious indications of bleeding. Most commonly, the patient has a documented medical record of persistent liver illness.
Foodborne illness caused by Staphylococcalism
Ingestion of food toxins may result in the patient experiencing bloody diarrhea within a timeframe of 1 to 6 hours. Common manifestations include intense, cramping stomach pain; nausea and vomiting; and prostration, all of which persist for a few hours.
Haemorrhoids
Hematochezia can concomitantly occur with external hemorrhoids, which usually lead to painful feces and consequent constipation. Less painful internal hemorrhoids often result in increased intermittent bleeding during bowel movements, which can ultimately cause symptoms of anemia, such as tiredness and exhaustion.
Bacterial leptospirosis
Hematochezia or melena, together with additional bleeding symptoms including epistaxis and hemoptysis, characterizes the severe type of leptospirosis known as Weil's syndrome. An abrupt frontal headache and intense thigh and lumbar myalgia, sometimes accompanied by cutaneous hyperesthesia, usually precede the bleeding. Presence of conjunctival suffusion is suggestive. The occurrence of bleeding is thereafter accompanied by chills, a swiftly increasing fever, and potentially, nausea and vomiting. The symptoms of fever, headache, and myalgia often worsen and continue for several weeks. Additional findings may encompass discomfort in the right upper quadrant, hepatomegaly, and jaundice.
Peptic ulcer
Embolism of the upper gastrointestinal tract is a frequent complication of peptic ulcer. The patient may exhibit hematochezia, hematemesis, or melena, contingent upon the speed and volume of hemorrhage. Should the peptic ulcer infiltrate an artery or vein, the occurrence of extensive bleeding might trigger indications of shock, including low blood pressure and rapid heart rate. Other symptoms may include chills, fever, nausea and vomiting, and indications of dehydration, such as parched mucous membranes, diminished skin elasticity, and excessive thirst. The patient commonly presents with a clinical background of epigastric pain that is alleviated by dietary intake or antacids. Additionally, there is a documented record of chronic tobacco, alcohol, or NSAID use.
Ulcerative proctitis
Ulcerative proctitis usually is characterized by a strong urge to defecate, yet the patient only excretes bright red blood, pus, or mucus. Additional typical indications and manifestations include sudden onset of constipation and tenicles.
Exams. Specific surgical interventions, including colonoscopy, polypectomy, and proctosigmoidoscopy, have the potential to induce rectal bleeding. Incidence of bowel perforation minimal.
Key Factors to Consider
After placing the patient on bed rest, regularly monitor his vital signs for indications of shock, including low blood pressure, rapid heart rate, a feeble pulse, and rapid breathing. Conduct hourly monitoring of his intake and outflow. Ensure to offer emotional assistance since hematochezia can create profound fear in the patient.
Prepare the patient for hematological tests and gastrointestinal procedures, including endoscopy and
Diagnostic gastrointestinal X-rays. Conduct a visual inspection of the patient's feces and analyse them for hidden blood. Should it be required, submit a stool sample to the laboratory for parasite testing.
Therapeutic Counseling for Patients
Detail the indications and manifestations that the patient should promptly disclose. Instruct the patient on ostomy self-care and address appropriate bowel eliminating practices. Articulate dietary guidelines and limitations.
Guidelines for Pediatric Populations
The prevalence of haematochezia is substantially lower in children compared to adults. The condition may arise due to structural abnormalities, including intussusception and Meckel’s diverticulum, as well as inflammatory illnesses, such peptic ulcer disease and ulcerative colitis.
In pediatric patients, ulcerative colitis usually manifests as chronic, rather than acute, manifestations and may also result in delayed growth and maturation associated with malnutrition. Incidents of rectal bleeding in children are always indicative of suspected sexual abuse.
Guidelines for Geriatrics
Given the heightened susceptibility of elderly individuals to colon cancer, it is advisable to assess hematochezia by colonoscopy once perirectal lesions have been eliminated as the contributing factor to bleeding.
Hematochezia, the passing of bloody stools, often presents as an early indication of gastrointestinal bleeding below the ligament of Treitz. Although typically preceded by hematemesis, this symptom may also occur with a fast bleeding of 1 L or more from the upper gastrointestinal tract.
The spectrum of hematochezia includes both solid, blood-streaked feces and liquid, bloody stools that might be deep crimson, dark mahogany, or maroon in hue. Typically, this indication manifests suddenly and is preceded by stomach pain.
While hematochezia is often linked to gastrointestinal complications, it can also arise from a coagulation abnormality, exposure to chemicals, or specific diagnostic procedures. Always an important indication, hematochezia can trigger potentially fatal hypovolemia.
Urgent medical interventions
If the patient presents with grave hematochezia, assess his vital signs. Upon observing indications of shock, such as low blood pressure and rapid heart rate, arrange the patient in a supine posture and raise his feet by 20 to 30 degrees. Make necessary arrangements to provide oxygen therapy and initiate a large-bore intravenous line for immediate fluid replenishment. The next step is to collect a blood sample for typing and crossmatching, measuring the hemoglobin level and hematocrit. Introduce a nasogastric tube. Administering iced lavage may be recommended to manage bleeding. Urgent endoscopy may be required to identify the origin of the bleeding.
Historical Background and Physical Assessment
If hematochezia is not immediately life-threatening, get the patient to provide a detailed account of the quantity, hue, and texture of his bloody feces. (If feasible, personally examine and describe the stools as well.) For how long have the stools exhibited hematochezia? Do their appearances generally remain consistent, or does the quantity of blood appear to fluctuate? Enquire about any related indications and manifestations.
Proceed to examine the patient's medical history, with particular attention to gastrointestinal and coagulation status.
Pathologies. Request information regarding the use of gastrointestinal irritants, including alcohol, aspirin, and other nonsteroidal anti-inflammatory medications (NSAIDs).
Initiate the physical survey by assessing for orthostatic hypotension, a first indication of shock. Measure the patient's blood pressure and pulse in supine, seated, and standing positions. Should the systolic pressure drop by 10 mm Hg or more or the pulse rate rise by 10 beats/minute or more upon changing position, it is advisable to consider the possibility of volume depletion and an imminent shock.
Assess the skin for the presence of petechiae or spider angiomas. Evaluate the abdomen by palpating for any signs of tenderness, pain, or lumps. Furthermore, observe lymphadenopathy. Finally, a digital rectal examination is necessary to exclude the presence of rectal tumors or hemorrhoids.
Medical etiology
Anal fissure. Minor hematochezia is a defining feature of anal fissure; blood may streak the feces or be seen on toilet tissue. Hematochezia is accompanied by intense rectal pain, which can lead to constipation by leading the patient to be reluctant to defecate.
Angiodysplastic lesions
Typically seen in older individuals, these arteriovenous lesions of the ascending colon often result in persistent, vivid red rectal bleeding. On rare occasions, this painless hematochezia can lead to potentially fatal blood loss and symptoms of shock, such as rapid heart rate and low arterial pressure.
Coagulation disorders
Individuals diagnosed with a coagulation condition, such as thrombocytopenia and disseminated intravascular coagulation, may have gastrointestinal bleeding characterized by mild to severe hematochezia. Bleeding can also manifest in other bodies systems, resulting in symptoms such as epistaxis and purpura. The associated findings differ depending on the particular coagulation problem.
Colitis
Especially in older people, ischemic colitis often results in bloody diarrhea. Haematochezia can manifest as either mild or significant and is often accompanied by intense, cramping lower abdomen discomfort and low blood pressure. Additional symptoms include gastric pain, distension, and lack of intestinal noises. Profound colitis can lead to potentially fatal hypovolemic shock and peritonitis.
In general, ulcerative colitis is characterized by the presence of bloody diarrhea that may also include mucus. Hematochezia is preceded by a range of abdominal pains, from mild to severe, and can result in very little to significant blood loss. Compound manifestations include pyrexia, anorexia, emesis, dyspepsia, tachycardia, and, on rare occasions, atrial fibrillation. Weight loss and weakness manifest in the later stages.
Colorectal carcinoma
Conspicuous crimson rectal bleeding, with or without pain, is a diagnostic indicator, particularly in cases of left colon cancer.
In most cases, a left colon tumor presents with initial indications of blockage, including rectal pressure, hemorrhage, and sporadic feelings of fullness or cramping. As the condition advances, the patient also has constipation, diarrhea characterized by ribbon-shaped feces, and chronic pain, which is usually alleviated by the passage of stools or flatus. The stool is visibly hematochezic.
Neoplasm development in the right colon at an early stage can result in melena, abdominal pain, pressure, and dull cramps. With advancing disease, the patient experiences a decline in physical strength and persistent tiredness. Further symptoms he may encounter include diarrhea, anorexia, weight loss, anemia, vomiting, an abdominal mass, and indications of blockage, such as abdominal distension and irregular bowel sounds.
Colorectal polyps.
Intermittent hematochezia in individuals under the age of 60 is mostly caused by colorectal polyps, although in certain cases these lesions may provide no symptoms. Polyps positioned high in the colon can result in the presence of blood-streaked feces. The feces exhibit a positive reaction when subjected to guaiac testing. Should the polyps be situated in greater proximity to the rectum, they may exhibit unrestricted bleeding.
Diverticulitis
In the elderly, diverticulitis often presents as a rapid onset of mild to severe rectal bleeding following the patient's urge to defecate. The bleeding may cease suddenly or may advance to life-threatening hemorrhage accompanied by symptoms of shock. Common indications and manifestations may include pain in the lower left quadrant that is alleviated by defecation, alternating bouts of constipation and diarrhea, loss of appetite, feelings of nausea and vomiting, irritation and tenderness in the abdomen, and a swollen belly.
Dysentery
Infection with Shigella, Amoeba, and Campylobacter often results in bloody diarrhea, although it is far less prevalent with Salmonella. May also manifest as abdominal pain or cramps, tenesmus, fever, and nausea.
Ruptured esophageal varices
For esophageal varices, a potentially fatal condition, hematochezia can vary from little rectal leakage to visibly bloody feces and may be followed by moderate to severe hematemesis or melena. Although painless, this substantial bleeding can trigger symptoms of shock, including rapid heart rate and low blood pressure. Indeed, symptoms of shock sometimes occur before obvious indications of bleeding. Most commonly, the patient has a documented medical record of persistent liver illness.
Foodborne illness caused by Staphylococcalism
Ingestion of food toxins may result in the patient experiencing bloody diarrhea within a timeframe of 1 to 6 hours. Common manifestations include intense, cramping stomach pain; nausea and vomiting; and prostration, all of which persist for a few hours.
Haemorrhoids
Hematochezia can concomitantly occur with external hemorrhoids, which usually lead to painful feces and consequent constipation. Less painful internal hemorrhoids often result in increased intermittent bleeding during bowel movements, which can ultimately cause symptoms of anemia, such as tiredness and exhaustion.
Bacterial leptospirosis
Hematochezia or melena, together with additional bleeding symptoms including epistaxis and hemoptysis, characterizes the severe type of leptospirosis known as Weil's syndrome. An abrupt frontal headache and intense thigh and lumbar myalgia, sometimes accompanied by cutaneous hyperesthesia, usually precede the bleeding. Presence of conjunctival suffusion is suggestive. The occurrence of bleeding is thereafter accompanied by chills, a swiftly increasing fever, and potentially, nausea and vomiting. The symptoms of fever, headache, and myalgia often worsen and continue for several weeks. Additional findings may encompass discomfort in the right upper quadrant, hepatomegaly, and jaundice.
Peptic ulcer
Embolism of the upper gastrointestinal tract is a frequent complication of peptic ulcer. The patient may exhibit hematochezia, hematemesis, or melena, contingent upon the speed and volume of hemorrhage. Should the peptic ulcer infiltrate an artery or vein, the occurrence of extensive bleeding might trigger indications of shock, including low blood pressure and rapid heart rate. Other symptoms may include chills, fever, nausea and vomiting, and indications of dehydration, such as parched mucous membranes, diminished skin elasticity, and excessive thirst. The patient commonly presents with a clinical background of epigastric pain that is alleviated by dietary intake or antacids. Additionally, there is a documented record of chronic tobacco, alcohol, or NSAID use.
Ulcerative proctitis
Ulcerative proctitis usually is characterized by a strong urge to defecate, yet the patient only excretes bright red blood, pus, or mucus. Additional typical indications and manifestations include sudden onset of constipation and tenicles.
Exams. Specific surgical interventions, including colonoscopy, polypectomy, and proctosigmoidoscopy, have the potential to induce rectal bleeding. Incidence of bowel perforation minimal.
Key Factors to Consider
After placing the patient on bed rest, regularly monitor his vital signs for indications of shock, including low blood pressure, rapid heart rate, a feeble pulse, and rapid breathing. Conduct hourly monitoring of his intake and outflow. Ensure to offer emotional assistance since hematochezia can create profound fear in the patient.
Prepare the patient for hematological tests and gastrointestinal procedures, including endoscopy and
Diagnostic gastrointestinal X-rays. Conduct a visual inspection of the patient's feces and analyse them for hidden blood. Should it be required, submit a stool sample to the laboratory for parasite testing.
Therapeutic Counseling for Patients
Detail the indications and manifestations that the patient should promptly disclose. Instruct the patient on ostomy self-care and address appropriate bowel eliminating practices. Articulate dietary guidelines and limitations.
Guidelines for Pediatric Populations
The prevalence of haematochezia is substantially lower in children compared to adults. The condition may arise due to structural abnormalities, including intussusception and Meckel’s diverticulum, as well as inflammatory illnesses, such peptic ulcer disease and ulcerative colitis.
In pediatric patients, ulcerative colitis usually manifests as chronic, rather than acute, manifestations and may also result in delayed growth and maturation associated with malnutrition. Incidents of rectal bleeding in children are always indicative of suspected sexual abuse.
Guidelines for Geriatrics
Given the heightened susceptibility of elderly individuals to colon cancer, it is advisable to assess hematochezia by colonoscopy once perirectal lesions have been eliminated as the contributing factor to bleeding.

- Published on
Symptoms and Signs – Differential Diagnosis of Hematemesis
Hematemesis, the act of vomiting blood, often denotes gastrointestinal bleeding occurring above the ligament of Treitz, which serves to suspend the duodenum at its point of connection with the jejunum. Fresh or recent bleeding is indicated by bright crimson or blood-streaked vomitus. Emesis of dark red, brown, or black hue (resembling the color and texture of coffee grounds) suggests the presence of blood that has been retained in the stomach and has undergone partial digestion.
Typically caused by a gastrointestinal illness, hematemesis can also arise from a coagulation disorder or a therapy that causes irritation to the gastrointestinal tract. Gastroesophageal varices Possible cause of hematemesis. The ingestion of blood from epistaxis or oropharyngeal erosion can also result in the occurrence of bloody vomitus. Acute hematemesis can be triggered by physical exertion, psychological pressure, and the consumption of an anti-inflammatory medication or alcohol. Hematemesis in a patient with esophageal varices might occur due to trauma caused by an ingestion of hard or partially chewed food. (Refer to Limited Causes of Hematemesis.)
Although the severity of hematemesis depends on the quantity, origin, and speed of the bleeding, it is always a reliable indicator. Profound hematemesis, characterized by the vomiting of 500 to 1,000 mL of blood, can be potentially fatal.
Urgent medical interventions
Should the patient exhibit severe hematemesis, assess his vital signs. If indications of shock are observed, such as constricted breathing, low blood pressure, and rapid heart rate, arrange the patient in a supine posture and raise his feet by 20 to 30 degrees. Initiate a large-bore intravenous line for urgent fluid replenishment. Submit a blood sample for typing and cross-matching, measure hemoglobin level and hematocrit, and provide oxygen therapy. An emergency endoscopy may be required to identify the origin of the bleeding. Make necessary arrangements to introduce a nasogastric (NG) tube for the purpose of suction or cooled lavage. One may use a Sengstaken-Blakemore tube to compress esophageal varices.
Historical Background and Physical Assessment
When the patient's hematemesis is not immediately life-threatening, start by obtaining a comprehensive medical history. First, ask the patient to provide a description of the quantity, hue, and texture of the vomit. When did he initially become aware of this sign? Has the patient previously had hematemesis? Determine whether he also experiences profuse or dark, tarry feces. Record whether hematemesis is typically preceded by symptoms such as nausea, flatulence, diarrhea, or weakness. Has he experienced recent episodes of retching accompanied by or without vomiting?
Then, inquire if any prior occurrence of ulcers or liver or coagulation abnormalities. Ascertain the extent of alcohol consumption by the patient, if any. Is he a habitual user of aspirin or more nonsteroidal anti-inflammatory drugs (NSAIDs), such as phenylbutazone or indomethacin? These medications can induce erosive gastritis or ulcers. Has he been prescribed warfarin or any other medications with anticoagulant properties? These medications heighten the patient's susceptibility to hemorrhaging.
The physical examination should commence by assessing for orthostatic hypotension, which serves as an early indicator of hypovolemia. Obtain blood pressure and pulse measurements while the patient is lying on their back, seated, and standing. Volume depletion is indicated by a significant reduction of 10 mm Hg or more in systolic pressure or an increase of 10 beats/minute or more in pulse rate. Once further vital signs have been obtained, examine the mucous membranes, nasopharynx, and skin for any indications of bleeding or other irregularities. Ultimately, examine the abdomen by means of palpation to detect any soreness, pain, or lumps. Note lymph node involvement.
Managing Hematemesis with Intubation
A patient diagnosed with hematemesis will require the insertion of a gastrointestinal tube to enable blood drainage, aspirate gastric contents, or to promote gastric lavage, if required. The following are the prevailing tubes and their respective applications.
Nasogastric tubes
The Salem-Sump tube, a double-lumen nasogastric (NG) tube, is utilized for the purpose of extracting stomach fluid and gas or aspirating gastric contents during medical procedures. Further applications include gastrointestinal lavage, medication delivery, and feeding. A primary benefit of this tube compared to the Levin tube, which is a single-lumen NG tube, is its ability to let atmospheric air to enter the patient's stomach, enabling the tube to float freely instead of being at risk of adhering to and damaging the gastric mucosa.
Wide-bore gastric tubes
The Edlich tube, shown on the right, houses a single wide-bore lumen with four apertures located close to the closed distal end. A syringe or funnel can be attached at the proximal end. As with other tubes, the Edlich tube is suitable for gastric lavage and rapid aspiration of a substantial amount of stomach contents.
The Ewald tube, a wide-bore tube designed for rapid passage of a substantial volume of fluid and clots, is particularly beneficial for gastric lavage in patients experiencing excessive intragastrointestinal bleeding and those who have consumed non-acidic or alkaline poison. The double-lumen Levacuator is a wide-bore tube having a big lumen for evacuating stomach contents and a smaller one for lavage.
Esophageal tubes
At right, the Sengstaken-Blakemore tube is a triple-lumen double-balloon esophageal tube equipped with a stomach aspiration port that enables drainage from beneath the gastric balloon. It can also be utilized for the administration of medicine. Because it lacks an esophageal balloon, the Linton-Nachlas tube can aspirate esophageal and stomach contents without the risk of necrosis. The Minnesota esophagogastric mucosal tamponade tube, It consists of four lumina and two balloons, and includes pressure-monitoring ports for both balloons without requiring Y-connectors.
Medical etiology
Anthrax (GI) Initial indications and symptoms following the consumption of contaminated meat from an animal afflicted with the gram-positive, spore-forming causative agent Bacillus anthracis encompass reduced appetite, nausea, vomiting, and pyrexia. The signs and symptoms may advance to hematemesis, stomach discomfort, and serious hemorrhagic ulceration.
Coagulation disorders
Disruption of normal clotting by any disease can lead to gastrointestinal bleeding and moderate to severe hematemesis. Hemorrhage can also manifest in other bodily systems, leading to symptoms such as epistaxis and ecchymosis. Variations in other related effects are contingent upon the particular coagulation condition, such as thrombocytopenia or hemophilia.
Esophageal cancer
Indicative of advanced esophageal cancer, hematemesis might be accompanied by persistent chest pain that extends to the back. Other symptoms include substernal engorgement, intense difficulty swallowing, nausea, vomiting with regurgitation and aspiration during the night, coughing up blood, a fever, hiccups, a sore throat, melena, and excessive salivation.
Esophageal rupture
Incidence of hematemesis is determined by the underlying cause of the rupture. When a medical device causes injury to the esophagus, hematemesis is often rather mild. But rupture caused by Boerhaave's syndrome (increased pressure in the esophagus from vomiting or retching) or other esophageal diseases usually results in more severe hematemesis. Furthermore, this potentially fatal condition can cause intense retrosternal, epigastric, neck, or scapular pain along with swelling in the chest and neck. Clinical examination shows the presence of subcutaneous crepitation in the chest wall, supraclavicular fossa, and neck. In addition, the patient may exhibit indications of respiratory distress, such as decreased breathing and the appearance of cyanosis.
Esophageal varices (ruptured)
The rupture of esophageal varices can result in life-threatening vomiting that is either coffee-ground or large, brilliant crimson in character. Following or even preceding hematemesis, signs of shock such as hypotension or tachycardia may manifest if the stomach becomes filled with blood before vomiting takes place. Other symptoms may include stomach distension and melena, or painless hematochezia, which can range from little leaking to significant rectal bleeding.
Gastrointestinal carcinoma
Vomitus that is painless, brilliant red, or dark brown in color is a delayed indication of stomach cancer, sometimes originating gradually alongside upper abdominal pain. The patient then experiences anorexia, low-grade nausea, and persistent dyspepsia that is not alleviated by antacids and worsened by meals. Subsequent symptoms may encompass exhaustion, debility, reduction in body weight, sensations of satiety, melena, changes in bowel patterns, and indications of malnutrition, such as breakdown of muscles and dry skin.
Gastritis (acute)
Haematemesis and melena are the predominant manifestations of acute gastritis. While these symptoms may be the sole indications, modest epigastric discomfort, nausea, fever, and malaise may also manifest. Profound blood loss triggers symptoms of shock. Usually, the patient has a documented record of alcohol misuse or has prior usage of aspirin or another nonsteroidal anti-inflammatory drug (NSAID). Malignant gastritis can also result from infection with Helicobacter pylori.
Mallory-Weiss syndrome
Marked by a rupture of the mucosal lining at the point where the esophagus and stomach meet, this condition can result in hematemesis and melena. Gastroesophageal reflux is often precipitated by intense vomiting, retching, or straining (such as from coughing), often in individuals with alcoholism or pyrexia. Intensive hemorrhaging can trigger symptoms of shock, including rapid heart rate, low blood pressure, difficulty breathing, and cold, damp skin.
Peptic ulcer
When a peptic ulcer infiltrates an artery, vein, or highly vascular tissue, hematemesis may result. Hematemesis of significant magnitude, and potentially life-threatening, is characteristic when an artery is breached. Other characteristics include melena or hematochezia, chills, a fever, and indications of shock and dehydration, such as rapid heart rate, low blood pressure, dry skin, and excessive thirst. The patient may have a clinical record of experiencing nausea, vomiting, discomfort in the epigastric region, and pain that is alleviated by dietary intake or antacids. Moreover, he may have a documented record of regularly consuming tobacco, alcohol, or NSAIDs.
Treatments
Hematemesis could be caused by traumatic NG or endotracheal intubation resulting in the ingestion of blood. The manifestation of this symptom may also be induced by nose or throat surgery in a similar manner.
Points of Special Consideration
Rigorously observe the patient's vital signs and be vigilant for indications of shock. Routinely examine the patient's feces for hidden blood, and maintain precise records of their food consumption and stool production. In order to avoid aspiration of vomitus, put the patient in a low or semi-Fowler's position when on bed rest. Retain suctioning equipment in close proximity and utilize it as necessary. The provision of regular dental hygiene and mental support is crucial, since the sight of bloody vomitus can evoke significant fear. Dispense an intravenous histamine-2 receptor antagonist; vasopressin may be necessary for variceal bleeding. Monitor the pH of gastrointestinal contents when the bleeding subsides, and administer hourly doses of antacids via NG tube, as needed.
Educational Instruction for Patients
Detail the specific meals and fluids that the patient should refrain from consuming, and emphasize the need of abstaining from alcohol.
Guidelines for Pediatric Populations
Hematemesis is less prevalent in children compared to adults and may be associated with the consumption of foreign bodies. At times, newborns may experience hematemesis when they ingest maternal blood during delivery or when they breastfeed from a prolapsed nipple. Infants with hemorrhagic illness of the newborn and esophageal erosion may experience hematemesis, necessitating prompt intervention with fluid replacement.
Guidelines for Geriatrics
Hematemesis in an older population can result from a vascular abnormality, an aortoenteric fistula, or upper gastrointestinal malignancy. Furthermore, the presence of chronic obstructive lung disease, chronic liver or renal failure, and chronic NSAID usage all increase the risk of bleeding in older individuals due to the simultaneous occurrence of ulcerative diseases.
Hematemesis, the act of vomiting blood, often denotes gastrointestinal bleeding occurring above the ligament of Treitz, which serves to suspend the duodenum at its point of connection with the jejunum. Fresh or recent bleeding is indicated by bright crimson or blood-streaked vomitus. Emesis of dark red, brown, or black hue (resembling the color and texture of coffee grounds) suggests the presence of blood that has been retained in the stomach and has undergone partial digestion.
Typically caused by a gastrointestinal illness, hematemesis can also arise from a coagulation disorder or a therapy that causes irritation to the gastrointestinal tract. Gastroesophageal varices Possible cause of hematemesis. The ingestion of blood from epistaxis or oropharyngeal erosion can also result in the occurrence of bloody vomitus. Acute hematemesis can be triggered by physical exertion, psychological pressure, and the consumption of an anti-inflammatory medication or alcohol. Hematemesis in a patient with esophageal varices might occur due to trauma caused by an ingestion of hard or partially chewed food. (Refer to Limited Causes of Hematemesis.)
Although the severity of hematemesis depends on the quantity, origin, and speed of the bleeding, it is always a reliable indicator. Profound hematemesis, characterized by the vomiting of 500 to 1,000 mL of blood, can be potentially fatal.
Urgent medical interventions
Should the patient exhibit severe hematemesis, assess his vital signs. If indications of shock are observed, such as constricted breathing, low blood pressure, and rapid heart rate, arrange the patient in a supine posture and raise his feet by 20 to 30 degrees. Initiate a large-bore intravenous line for urgent fluid replenishment. Submit a blood sample for typing and cross-matching, measure hemoglobin level and hematocrit, and provide oxygen therapy. An emergency endoscopy may be required to identify the origin of the bleeding. Make necessary arrangements to introduce a nasogastric (NG) tube for the purpose of suction or cooled lavage. One may use a Sengstaken-Blakemore tube to compress esophageal varices.
Historical Background and Physical Assessment
When the patient's hematemesis is not immediately life-threatening, start by obtaining a comprehensive medical history. First, ask the patient to provide a description of the quantity, hue, and texture of the vomit. When did he initially become aware of this sign? Has the patient previously had hematemesis? Determine whether he also experiences profuse or dark, tarry feces. Record whether hematemesis is typically preceded by symptoms such as nausea, flatulence, diarrhea, or weakness. Has he experienced recent episodes of retching accompanied by or without vomiting?
Then, inquire if any prior occurrence of ulcers or liver or coagulation abnormalities. Ascertain the extent of alcohol consumption by the patient, if any. Is he a habitual user of aspirin or more nonsteroidal anti-inflammatory drugs (NSAIDs), such as phenylbutazone or indomethacin? These medications can induce erosive gastritis or ulcers. Has he been prescribed warfarin or any other medications with anticoagulant properties? These medications heighten the patient's susceptibility to hemorrhaging.
The physical examination should commence by assessing for orthostatic hypotension, which serves as an early indicator of hypovolemia. Obtain blood pressure and pulse measurements while the patient is lying on their back, seated, and standing. Volume depletion is indicated by a significant reduction of 10 mm Hg or more in systolic pressure or an increase of 10 beats/minute or more in pulse rate. Once further vital signs have been obtained, examine the mucous membranes, nasopharynx, and skin for any indications of bleeding or other irregularities. Ultimately, examine the abdomen by means of palpation to detect any soreness, pain, or lumps. Note lymph node involvement.
Managing Hematemesis with Intubation
A patient diagnosed with hematemesis will require the insertion of a gastrointestinal tube to enable blood drainage, aspirate gastric contents, or to promote gastric lavage, if required. The following are the prevailing tubes and their respective applications.
Nasogastric tubes
The Salem-Sump tube, a double-lumen nasogastric (NG) tube, is utilized for the purpose of extracting stomach fluid and gas or aspirating gastric contents during medical procedures. Further applications include gastrointestinal lavage, medication delivery, and feeding. A primary benefit of this tube compared to the Levin tube, which is a single-lumen NG tube, is its ability to let atmospheric air to enter the patient's stomach, enabling the tube to float freely instead of being at risk of adhering to and damaging the gastric mucosa.
Wide-bore gastric tubes
The Edlich tube, shown on the right, houses a single wide-bore lumen with four apertures located close to the closed distal end. A syringe or funnel can be attached at the proximal end. As with other tubes, the Edlich tube is suitable for gastric lavage and rapid aspiration of a substantial amount of stomach contents.
The Ewald tube, a wide-bore tube designed for rapid passage of a substantial volume of fluid and clots, is particularly beneficial for gastric lavage in patients experiencing excessive intragastrointestinal bleeding and those who have consumed non-acidic or alkaline poison. The double-lumen Levacuator is a wide-bore tube having a big lumen for evacuating stomach contents and a smaller one for lavage.
Esophageal tubes
At right, the Sengstaken-Blakemore tube is a triple-lumen double-balloon esophageal tube equipped with a stomach aspiration port that enables drainage from beneath the gastric balloon. It can also be utilized for the administration of medicine. Because it lacks an esophageal balloon, the Linton-Nachlas tube can aspirate esophageal and stomach contents without the risk of necrosis. The Minnesota esophagogastric mucosal tamponade tube, It consists of four lumina and two balloons, and includes pressure-monitoring ports for both balloons without requiring Y-connectors.
Medical etiology
Anthrax (GI) Initial indications and symptoms following the consumption of contaminated meat from an animal afflicted with the gram-positive, spore-forming causative agent Bacillus anthracis encompass reduced appetite, nausea, vomiting, and pyrexia. The signs and symptoms may advance to hematemesis, stomach discomfort, and serious hemorrhagic ulceration.
Coagulation disorders
Disruption of normal clotting by any disease can lead to gastrointestinal bleeding and moderate to severe hematemesis. Hemorrhage can also manifest in other bodily systems, leading to symptoms such as epistaxis and ecchymosis. Variations in other related effects are contingent upon the particular coagulation condition, such as thrombocytopenia or hemophilia.
Esophageal cancer
Indicative of advanced esophageal cancer, hematemesis might be accompanied by persistent chest pain that extends to the back. Other symptoms include substernal engorgement, intense difficulty swallowing, nausea, vomiting with regurgitation and aspiration during the night, coughing up blood, a fever, hiccups, a sore throat, melena, and excessive salivation.
Esophageal rupture
Incidence of hematemesis is determined by the underlying cause of the rupture. When a medical device causes injury to the esophagus, hematemesis is often rather mild. But rupture caused by Boerhaave's syndrome (increased pressure in the esophagus from vomiting or retching) or other esophageal diseases usually results in more severe hematemesis. Furthermore, this potentially fatal condition can cause intense retrosternal, epigastric, neck, or scapular pain along with swelling in the chest and neck. Clinical examination shows the presence of subcutaneous crepitation in the chest wall, supraclavicular fossa, and neck. In addition, the patient may exhibit indications of respiratory distress, such as decreased breathing and the appearance of cyanosis.
Esophageal varices (ruptured)
The rupture of esophageal varices can result in life-threatening vomiting that is either coffee-ground or large, brilliant crimson in character. Following or even preceding hematemesis, signs of shock such as hypotension or tachycardia may manifest if the stomach becomes filled with blood before vomiting takes place. Other symptoms may include stomach distension and melena, or painless hematochezia, which can range from little leaking to significant rectal bleeding.
Gastrointestinal carcinoma
Vomitus that is painless, brilliant red, or dark brown in color is a delayed indication of stomach cancer, sometimes originating gradually alongside upper abdominal pain. The patient then experiences anorexia, low-grade nausea, and persistent dyspepsia that is not alleviated by antacids and worsened by meals. Subsequent symptoms may encompass exhaustion, debility, reduction in body weight, sensations of satiety, melena, changes in bowel patterns, and indications of malnutrition, such as breakdown of muscles and dry skin.
Gastritis (acute)
Haematemesis and melena are the predominant manifestations of acute gastritis. While these symptoms may be the sole indications, modest epigastric discomfort, nausea, fever, and malaise may also manifest. Profound blood loss triggers symptoms of shock. Usually, the patient has a documented record of alcohol misuse or has prior usage of aspirin or another nonsteroidal anti-inflammatory drug (NSAID). Malignant gastritis can also result from infection with Helicobacter pylori.
Mallory-Weiss syndrome
Marked by a rupture of the mucosal lining at the point where the esophagus and stomach meet, this condition can result in hematemesis and melena. Gastroesophageal reflux is often precipitated by intense vomiting, retching, or straining (such as from coughing), often in individuals with alcoholism or pyrexia. Intensive hemorrhaging can trigger symptoms of shock, including rapid heart rate, low blood pressure, difficulty breathing, and cold, damp skin.
Peptic ulcer
When a peptic ulcer infiltrates an artery, vein, or highly vascular tissue, hematemesis may result. Hematemesis of significant magnitude, and potentially life-threatening, is characteristic when an artery is breached. Other characteristics include melena or hematochezia, chills, a fever, and indications of shock and dehydration, such as rapid heart rate, low blood pressure, dry skin, and excessive thirst. The patient may have a clinical record of experiencing nausea, vomiting, discomfort in the epigastric region, and pain that is alleviated by dietary intake or antacids. Moreover, he may have a documented record of regularly consuming tobacco, alcohol, or NSAIDs.
Treatments
Hematemesis could be caused by traumatic NG or endotracheal intubation resulting in the ingestion of blood. The manifestation of this symptom may also be induced by nose or throat surgery in a similar manner.
Points of Special Consideration
Rigorously observe the patient's vital signs and be vigilant for indications of shock. Routinely examine the patient's feces for hidden blood, and maintain precise records of their food consumption and stool production. In order to avoid aspiration of vomitus, put the patient in a low or semi-Fowler's position when on bed rest. Retain suctioning equipment in close proximity and utilize it as necessary. The provision of regular dental hygiene and mental support is crucial, since the sight of bloody vomitus can evoke significant fear. Dispense an intravenous histamine-2 receptor antagonist; vasopressin may be necessary for variceal bleeding. Monitor the pH of gastrointestinal contents when the bleeding subsides, and administer hourly doses of antacids via NG tube, as needed.
Educational Instruction for Patients
Detail the specific meals and fluids that the patient should refrain from consuming, and emphasize the need of abstaining from alcohol.
Guidelines for Pediatric Populations
Hematemesis is less prevalent in children compared to adults and may be associated with the consumption of foreign bodies. At times, newborns may experience hematemesis when they ingest maternal blood during delivery or when they breastfeed from a prolapsed nipple. Infants with hemorrhagic illness of the newborn and esophageal erosion may experience hematemesis, necessitating prompt intervention with fluid replacement.
Guidelines for Geriatrics
Hematemesis in an older population can result from a vascular abnormality, an aortoenteric fistula, or upper gastrointestinal malignancy. Furthermore, the presence of chronic obstructive lung disease, chronic liver or renal failure, and chronic NSAID usage all increase the risk of bleeding in older individuals due to the simultaneous occurrence of ulcerative diseases.

