- Published on
Symptoms and Signs – Differential Diagnosis of Pulsus Paradoxus
Pulsus paradoxus, also known as paradoxical pulse, refers to a significant decrease in blood pressure during inhalation. Systolic pressure typically decreases by less than 10 mm Hg during inspiration. Pulsus paradoxus is characterized by a decrease exceeding 10 mm Hg.
When systolic pressure decreases by more than 20 mm Hg, peripheral pulses may become faintly perceptible or may vanish during inspiration. Pulsus paradoxus is believed to arise from an amplified inspiratory increase in negative intrathoracic pressure. Systolic pressure typically decreases after inhalation due to blood accumulation in the pulmonary system. This thus diminishes left ventricular filling and stroke volume while transmitting negative intrathoracic pressure to the aorta. Conditions that cause significant intrapleural pressure fluctuations, such asthma, or those that diminish left-sided cardiac filling, such as pericardial tamponade, result in pulsus paradoxus.
Utilize a sphygmomanometer or an intra-arterial monitoring device to precisely detect and quantify pulsus paradoxus. Inflate the blood pressure cuff 10 to 20 mm Hg above the maximum systolic pressure. Subsequently, deflate the cuff at a rate of 2 mm Hg per second until the initial Korotkoff sound is audible during expiration. Record the systolic pressure. As you gradually deflate the cuff, monitor the patient's breathing rhythm. In the presence of pulsus paradoxus, Korotkoff noises will cease during inspiration and reemerge during expiration. Proceed to deflate the cuff until Korotkoff noises are audible during both inspiration and expiration, and thereafter, record the systolic pressure. Deduct this measurement from the initial one to ascertain the extent of pulsus paradoxus. An abnormality is indicated by a differential over 10 mm Hg.
Pulsus paradoxus can also be identified by palpating the radial pulse during multiple cycles of sluggish inspiration and expiration. Pulsus paradoxus is indicated by a marked reduction in pulse during inspiration. When assessing for pulsus paradoxus, it is essential to exclude irregular cardiac rhythms and tachycardia, since these conditions can lead to fluctuations in pulse amplitude, hence complicating the accurate identification of actual pulsus paradoxus.
CRITICAL INTERVENTIONS
Pulsus paradoxus may indicate cardiac tamponade, a critical complication of pericardial effusion that arises when an excessive accumulation of blood or fluid compresses the heart. Upon detecting pulsus paradoxus, promptly assess the patient's other vital signs. Assess for further indicators of cardiac tamponade, including dyspnea, tachypnea, diaphoresis, jugular vein distention, tachycardia, constricted pulse pressure, and hypotension. Emergency pericardiocentesis may be required to aspirate blood or fluid from the pericardial sac. Subsequently, assess the efficacy of pericardiocentesis by quantifying the extent of pulsus paradoxus; it should diminish following aspiration.
Medical History and Physical Assessment
Determine whether the patient has a history of persistent cardiac or pulmonary disease if cardiac tamponade is absent. Inquire about the progression of related signs and symptoms, including cough or chest pain. Subsequently, auscultate for atypical respiratory sounds.
Cardiac tamponade.
Pulsus paradoxus frequently manifests in cardiac tamponade; nevertheless, it may be challenging to identify if intrapericardial pressure escalates suddenly and severe hypotension ensues. In cases of severe tamponade, the assessment typically uncovers the following hallmark findings: hypotension, attenuated or muffled heart sounds, and distended jugular veins. Associated findings encompass chest pain, a pericardial friction rub, diminished pulse pressure, anxiety, restlessness, clammy skin, and hepatomegaly. Notable respiratory signs and symptoms encompass dyspnea, tachypnea, and cyanosis; the patient generally adopts an upright position and leans forward to enhance breathing. In cases of progressive cardiac tamponade, pulsus paradoxus may present alongside weakness, anorexia, and weight loss. The patient may claim chest pain; yet, he will not exhibit muffled heart sounds or significant hypotension.
Chronic obstructive pulmonary disease (COPD)
The significant variations in intrathoracic pressure associated with COPD result in pulsus paradoxus and maybe tachycardia. Additional findings may include dyspnea, tachypnea, wheezing, a productive or nonproductive cough, activation of accessory muscles, barrel chest, and clubbing. The patient may exhibit laborious, pursed-lip breathing following effort or even while at rest. He generally assumes an upright position and leans forward to enhance respiration. Auscultation indicates diminished breath sounds, rhonchi, and crackles. Weight reduction, cyanosis, and edema may manifest.
Chronic constrictive pericarditis
Pulsus paradoxus may manifest in as many as 50% of individuals with pericarditis. Additional findings encompass a pericardial friction rub, thoracic discomfort, exertional dyspnea, orthopnea, hepatomegaly, and ascites. Patients also demonstrate peripheral edema and Kussmaul's sign - jugular vein distention that intensifies after inhalation.
Massive pulmonary embolism
Reduced left ventricular filling and stroke volume in major pulmonary embolism result in pulsus paradoxus, syncope, severe anxiety, dyspnea, tachypnea, and pleuritic chest pain. The patient exhibits cyanosis and jugular vein distension. He may experience circulatory collapse, characterized by hypotension and a weak, fast pulse. Pulmonary infarction can result in hemoptysis, diminished breath sounds, and a pleural friction rub in the affected region.
Prepare the patient for an echocardiography to assess heart motion and identify the underlying issue. Additionally, observe his vital signs and regularly assess the extent of contradiction. An escalation in the level of paradox may signify the recurrence or exacerbation of cardiac tamponade or the imminent onset of respiratory arrest in severe COPD. Intensive respiratory therapy, including chest physiotherapy, may prevent the necessity for endotracheal intubation.
Instruct the patient with COPD on self-care practices, including pursed-lip and diaphragmatic breathing, coughing, and deep breathing exercises, along with the correct utilization of home oxygen equipment. Highlight the significance of prescribed medications and their potential side effects.
Pulsus paradoxus frequently manifests in pediatric patients with chronic respiratory conditions, particularly after an acute asthma exacerbation. Children with pericarditis may develop pulsus paradoxus as a result of cardiac tamponade, but this condition is more prevalent in adults. Pulsus paradoxus above 20 mm Hg is a dependable sign of cardiac tamponade in pediatric patients; a variation of 10 to 20 mm Hg is ambiguous.
Pulsus paradoxus, also known as paradoxical pulse, refers to a significant decrease in blood pressure during inhalation. Systolic pressure typically decreases by less than 10 mm Hg during inspiration. Pulsus paradoxus is characterized by a decrease exceeding 10 mm Hg.
When systolic pressure decreases by more than 20 mm Hg, peripheral pulses may become faintly perceptible or may vanish during inspiration. Pulsus paradoxus is believed to arise from an amplified inspiratory increase in negative intrathoracic pressure. Systolic pressure typically decreases after inhalation due to blood accumulation in the pulmonary system. This thus diminishes left ventricular filling and stroke volume while transmitting negative intrathoracic pressure to the aorta. Conditions that cause significant intrapleural pressure fluctuations, such asthma, or those that diminish left-sided cardiac filling, such as pericardial tamponade, result in pulsus paradoxus.
Utilize a sphygmomanometer or an intra-arterial monitoring device to precisely detect and quantify pulsus paradoxus. Inflate the blood pressure cuff 10 to 20 mm Hg above the maximum systolic pressure. Subsequently, deflate the cuff at a rate of 2 mm Hg per second until the initial Korotkoff sound is audible during expiration. Record the systolic pressure. As you gradually deflate the cuff, monitor the patient's breathing rhythm. In the presence of pulsus paradoxus, Korotkoff noises will cease during inspiration and reemerge during expiration. Proceed to deflate the cuff until Korotkoff noises are audible during both inspiration and expiration, and thereafter, record the systolic pressure. Deduct this measurement from the initial one to ascertain the extent of pulsus paradoxus. An abnormality is indicated by a differential over 10 mm Hg.
Pulsus paradoxus can also be identified by palpating the radial pulse during multiple cycles of sluggish inspiration and expiration. Pulsus paradoxus is indicated by a marked reduction in pulse during inspiration. When assessing for pulsus paradoxus, it is essential to exclude irregular cardiac rhythms and tachycardia, since these conditions can lead to fluctuations in pulse amplitude, hence complicating the accurate identification of actual pulsus paradoxus.
CRITICAL INTERVENTIONS
Pulsus paradoxus may indicate cardiac tamponade, a critical complication of pericardial effusion that arises when an excessive accumulation of blood or fluid compresses the heart. Upon detecting pulsus paradoxus, promptly assess the patient's other vital signs. Assess for further indicators of cardiac tamponade, including dyspnea, tachypnea, diaphoresis, jugular vein distention, tachycardia, constricted pulse pressure, and hypotension. Emergency pericardiocentesis may be required to aspirate blood or fluid from the pericardial sac. Subsequently, assess the efficacy of pericardiocentesis by quantifying the extent of pulsus paradoxus; it should diminish following aspiration.
Medical History and Physical Assessment
Determine whether the patient has a history of persistent cardiac or pulmonary disease if cardiac tamponade is absent. Inquire about the progression of related signs and symptoms, including cough or chest pain. Subsequently, auscultate for atypical respiratory sounds.
Cardiac tamponade.
Pulsus paradoxus frequently manifests in cardiac tamponade; nevertheless, it may be challenging to identify if intrapericardial pressure escalates suddenly and severe hypotension ensues. In cases of severe tamponade, the assessment typically uncovers the following hallmark findings: hypotension, attenuated or muffled heart sounds, and distended jugular veins. Associated findings encompass chest pain, a pericardial friction rub, diminished pulse pressure, anxiety, restlessness, clammy skin, and hepatomegaly. Notable respiratory signs and symptoms encompass dyspnea, tachypnea, and cyanosis; the patient generally adopts an upright position and leans forward to enhance breathing. In cases of progressive cardiac tamponade, pulsus paradoxus may present alongside weakness, anorexia, and weight loss. The patient may claim chest pain; yet, he will not exhibit muffled heart sounds or significant hypotension.
Chronic obstructive pulmonary disease (COPD)
The significant variations in intrathoracic pressure associated with COPD result in pulsus paradoxus and maybe tachycardia. Additional findings may include dyspnea, tachypnea, wheezing, a productive or nonproductive cough, activation of accessory muscles, barrel chest, and clubbing. The patient may exhibit laborious, pursed-lip breathing following effort or even while at rest. He generally assumes an upright position and leans forward to enhance respiration. Auscultation indicates diminished breath sounds, rhonchi, and crackles. Weight reduction, cyanosis, and edema may manifest.
Chronic constrictive pericarditis
Pulsus paradoxus may manifest in as many as 50% of individuals with pericarditis. Additional findings encompass a pericardial friction rub, thoracic discomfort, exertional dyspnea, orthopnea, hepatomegaly, and ascites. Patients also demonstrate peripheral edema and Kussmaul's sign - jugular vein distention that intensifies after inhalation.
Massive pulmonary embolism
Reduced left ventricular filling and stroke volume in major pulmonary embolism result in pulsus paradoxus, syncope, severe anxiety, dyspnea, tachypnea, and pleuritic chest pain. The patient exhibits cyanosis and jugular vein distension. He may experience circulatory collapse, characterized by hypotension and a weak, fast pulse. Pulmonary infarction can result in hemoptysis, diminished breath sounds, and a pleural friction rub in the affected region.
Prepare the patient for an echocardiography to assess heart motion and identify the underlying issue. Additionally, observe his vital signs and regularly assess the extent of contradiction. An escalation in the level of paradox may signify the recurrence or exacerbation of cardiac tamponade or the imminent onset of respiratory arrest in severe COPD. Intensive respiratory therapy, including chest physiotherapy, may prevent the necessity for endotracheal intubation.
Instruct the patient with COPD on self-care practices, including pursed-lip and diaphragmatic breathing, coughing, and deep breathing exercises, along with the correct utilization of home oxygen equipment. Highlight the significance of prescribed medications and their potential side effects.
Pulsus paradoxus frequently manifests in pediatric patients with chronic respiratory conditions, particularly after an acute asthma exacerbation. Children with pericarditis may develop pulsus paradoxus as a result of cardiac tamponade, but this condition is more prevalent in adults. Pulsus paradoxus above 20 mm Hg is a dependable sign of cardiac tamponade in pediatric patients; a variation of 10 to 20 mm Hg is ambiguous.

- Published on
Symptoms and Signs – Differential Diagnosis of Pustular Rash
A pustular rash consists of clusters of pustules, which are visible accumulations of pus located inside or beneath the epidermis, typically seen in hair follicles or sweat pores. These lesions exhibit significant variability in size and morphology and may be either generalized or restricted to the hair follicles or sweat glands. .
Pustules may arise from a dermatological or systemic condition, the administration of specific medications, or contact with a skin irritant. Individuals who have swum in salt water frequently exhibit a papulopustular rash beneath the bathing suit or on other areas of the body due to irritation from marine organisms. While some pustular lesions are sterile, a pustular rash typically signifies an infection. A vesicular eruption, or acute contact dermatitis, may develop pustules if a subsequent infection arises.
Medical History and Physical Assessment
Request the patient to detail the characteristics, site, and onset of the initial pustular lesion. Did a different form of skin lesion occur prior to the pustule? Investigate the dissemination of the lesions. Inquire about the patient's current medications and whether he has utilized topical treatment for his rash. If so, what type did he apply, and when was the latest application? Ascertain whether he has a familial predisposition to a dermatological condition. Assess the complete skin surface, seeing whether it is dry, oily, moist, or greasy. Document the precise position and distribution of the skin lesions, including their color, shape, and dimensions.
Etiological Factors
Acne vulgaris
Pustules characterize the inflammatory lesions of acne vulgaris, which are accompanied by papules, nodules, cysts, open comedones (blackheads), and closed comedones (whiteheads). Lesions frequently manifest on the face, shoulders, back, and chest. Additional observations encompass tenderness upon palpation, pruritus, and a burning sensation. Chronic recurring lesions result in scarring.
Blastomycosis
Blastomycosis is a fungal illness characterized by tiny, painless, nonpruritic macules or papules that may grow into well-defined, verrucous, crusty, or ulcerated lesions surrounded by pustules. A localized infection may result in a singular lesion, whereas a systemic infection may produce several lesions on the hands, feet, face, and wrists. Blastomycosis manifests symptoms of pulmonary infection, including pleuritic chest discomfort and a dry, hacking or productive cough, occasionally accompanied by hemoptysis.
Folliculitis
Folliculitis is a bacterial infection of hair follicles characterized by individual pustules, each containing a hair and perhaps accompanied by itching. “Hot tub” folliculitis results in pustules on regions obscured by a bathing suit.
Furunculosis
A furuncle is an acute, deep-seated, erythematous, warm, and painful abscess that develops from staphylococcal folliculitis. Furuncles typically commence as tiny, sensitive red pustules at the follicular base. They are likely to manifest on the face, neck, forearm, groin, axillae, buttocks, and legs, or in regions susceptible to recurrent friction. The pustules typically remain tense for 2 to 4 days before becoming fluctuant. The rupture releases pus and necrotic tissue. Subsequently, pain diminishes; however, erythema and edema may endure.
Contagious impetigo
Impetigo contagiosa, a vesiculopustular eruptive condition manifesting in nonbullous and bullous variants, is typically induced by streptococci or staphylococci. Vesicles develop and rupture, leading to the formation of a crust from the exudate: a dense, yellow crust in streptococcal impetigo and a thin, transparent crust in staphylococcal impetigo. Both kinds typically result in painless pruritus.
Monkeypox.
A pustular rash including elevated, fluid-filled vesicles that subsequently crust, scab, and detach is indicative of a monkeypox viral infection. Macular, papular, and vesicular lesions may also manifest with a monkeypox rash. Furthermore, symptoms may encompass fever, headache, backache, lymphadenopathy, sore throat, cough, and weariness.
Pustular miliaria
Pustular miliaria is an anhidrotic condition characterized by pustular lesions that originate as small erythematous papulovesicles at the sweat pores. Diffuse erythema may emanate from the lesion. The rash, along with the accompanying burning and itching, exacerbates with perspiration.
Pustular psoriasis
Small vesicles develop and ultimately transform into pustules in pustular psoriasis. The patient may have itchiness, burning sensations, and pain. Localized pustular psoriasis typically impacts the hands and feet. Generalized pustular psoriasis can abruptly manifest in individuals with psoriasis, psoriatic arthritis, or exfoliative psoriasis; while uncommon, this variant of psoriasis has the potential to be lethal.
Rosacea
Rosacea is a persistent hyperemic condition that frequently manifests as telangiectasia, accompanied by acute episodes of pustules, papules, and edema. Rosacea, marked by chronic erythema, may initially present as a flush affecting the forehead, cheeks, nose, and chin. Intermittent bouts progressively grow more chronic, and the skin — rather than reverting to its natural hue — exhibits different degrees of erythema.
Scabies
Scabies is characterized by threadlike channels or burrows beneath the skin, and may also result in pustules, vesicles, and excoriations. The lesions are a few millimeters in length, with a swollen nodule or red papule that harbors the itch mite.
GENDER INDICATOR
In males, crusted lesions frequently manifest on the glans, shaft, and scrotum. Lesions may develop on the nipples in women. These lesions exhibit a preference for skin creases in both genders. Crusty excoriated lesions also manifest on the wrists, elbows, axillae, waistline, posterior knees, and ankles. Associated pruritus exacerbates with inactivity and elevated temperatures.
Variola major (smallpox)
Preliminary indications encompass elevated temperature, general discomfort, extreme fatigue, intense cephalalgia, lumbar pain, and gastrointestinal distress. A maculopapular rash emerges on the mucosal surfaces of the mouth, throat, face, and forearms, subsequently disseminating to the trunk and legs. Within two days, the rash evolves into vesicular and subsequently pustular lesions. The lesions manifest concurrently, exhibit uniform characteristics, and are more pronounced on the facial and extremity regions. The pustules are round, solid, and deeply entrenched in the dermis. After 8 to 9 days, the pustules develop a crust, which subsequently detaches from the skin, resulting in a pitted scar. In lethal instances, mortality occurs due to encephalitis, significant hemorrhaging, or subsequent infection
Varicella zoster
As immunity against varicella wanes, the virus reactivates along a dermatome, resulting in intensely painful and itchy vesicles and pustules (herpes zoster, or shingles). Despite the elimination of the rash, individuals may have chronic pain (postherpetic neuralgia) that can last for months. Alternative Causes Pharmaceutical substances. Bromides and iodides frequently induce a pustular rash.
Additional pharmacological causes encompass corticotropin, corticosteroids, dactinomycin, trimethadione, lithium, phenytoin, phenobarbital, isoniazid, hormonal contraceptives, androgens, and anabolic steroids.
Monitor wound and skin isolation protocols until infection is excluded by a Gram stain or culture and sensitivity analysis of the pustule's contents. If the organism is contagious, prevent drainage from contacting unaffected skin. Instruct the patient to maintain the segregation of his bathroom items and linens from those of other family members. Pain and itching, changes in body image, and the stress of solitude may lead to sleep disturbances, anxiety, and depression. Administer analgesics and antipruritics, and prompt the patient to articulate his emotions.
Elucidate the etiology of the condition, available therapeutic modalities, and strategies to mitigate the transmission of infection. Offer emotional assistance and knowledge on pain and itching alleviation. Disorders that cause a pustular rash in infants include varicella, erythema toxicum neonatorum, candidiasis, impetigo, infantile acropustulosis, and acrodermatitis enteropathica.
A pustular rash consists of clusters of pustules, which are visible accumulations of pus located inside or beneath the epidermis, typically seen in hair follicles or sweat pores. These lesions exhibit significant variability in size and morphology and may be either generalized or restricted to the hair follicles or sweat glands. .
Pustules may arise from a dermatological or systemic condition, the administration of specific medications, or contact with a skin irritant. Individuals who have swum in salt water frequently exhibit a papulopustular rash beneath the bathing suit or on other areas of the body due to irritation from marine organisms. While some pustular lesions are sterile, a pustular rash typically signifies an infection. A vesicular eruption, or acute contact dermatitis, may develop pustules if a subsequent infection arises.
Medical History and Physical Assessment
Request the patient to detail the characteristics, site, and onset of the initial pustular lesion. Did a different form of skin lesion occur prior to the pustule? Investigate the dissemination of the lesions. Inquire about the patient's current medications and whether he has utilized topical treatment for his rash. If so, what type did he apply, and when was the latest application? Ascertain whether he has a familial predisposition to a dermatological condition. Assess the complete skin surface, seeing whether it is dry, oily, moist, or greasy. Document the precise position and distribution of the skin lesions, including their color, shape, and dimensions.
Etiological Factors
Acne vulgaris
Pustules characterize the inflammatory lesions of acne vulgaris, which are accompanied by papules, nodules, cysts, open comedones (blackheads), and closed comedones (whiteheads). Lesions frequently manifest on the face, shoulders, back, and chest. Additional observations encompass tenderness upon palpation, pruritus, and a burning sensation. Chronic recurring lesions result in scarring.
Blastomycosis
Blastomycosis is a fungal illness characterized by tiny, painless, nonpruritic macules or papules that may grow into well-defined, verrucous, crusty, or ulcerated lesions surrounded by pustules. A localized infection may result in a singular lesion, whereas a systemic infection may produce several lesions on the hands, feet, face, and wrists. Blastomycosis manifests symptoms of pulmonary infection, including pleuritic chest discomfort and a dry, hacking or productive cough, occasionally accompanied by hemoptysis.
Folliculitis
Folliculitis is a bacterial infection of hair follicles characterized by individual pustules, each containing a hair and perhaps accompanied by itching. “Hot tub” folliculitis results in pustules on regions obscured by a bathing suit.
Furunculosis
A furuncle is an acute, deep-seated, erythematous, warm, and painful abscess that develops from staphylococcal folliculitis. Furuncles typically commence as tiny, sensitive red pustules at the follicular base. They are likely to manifest on the face, neck, forearm, groin, axillae, buttocks, and legs, or in regions susceptible to recurrent friction. The pustules typically remain tense for 2 to 4 days before becoming fluctuant. The rupture releases pus and necrotic tissue. Subsequently, pain diminishes; however, erythema and edema may endure.
Contagious impetigo
Impetigo contagiosa, a vesiculopustular eruptive condition manifesting in nonbullous and bullous variants, is typically induced by streptococci or staphylococci. Vesicles develop and rupture, leading to the formation of a crust from the exudate: a dense, yellow crust in streptococcal impetigo and a thin, transparent crust in staphylococcal impetigo. Both kinds typically result in painless pruritus.
Monkeypox.
A pustular rash including elevated, fluid-filled vesicles that subsequently crust, scab, and detach is indicative of a monkeypox viral infection. Macular, papular, and vesicular lesions may also manifest with a monkeypox rash. Furthermore, symptoms may encompass fever, headache, backache, lymphadenopathy, sore throat, cough, and weariness.
Pustular miliaria
Pustular miliaria is an anhidrotic condition characterized by pustular lesions that originate as small erythematous papulovesicles at the sweat pores. Diffuse erythema may emanate from the lesion. The rash, along with the accompanying burning and itching, exacerbates with perspiration.
Pustular psoriasis
Small vesicles develop and ultimately transform into pustules in pustular psoriasis. The patient may have itchiness, burning sensations, and pain. Localized pustular psoriasis typically impacts the hands and feet. Generalized pustular psoriasis can abruptly manifest in individuals with psoriasis, psoriatic arthritis, or exfoliative psoriasis; while uncommon, this variant of psoriasis has the potential to be lethal.
Rosacea
Rosacea is a persistent hyperemic condition that frequently manifests as telangiectasia, accompanied by acute episodes of pustules, papules, and edema. Rosacea, marked by chronic erythema, may initially present as a flush affecting the forehead, cheeks, nose, and chin. Intermittent bouts progressively grow more chronic, and the skin — rather than reverting to its natural hue — exhibits different degrees of erythema.
Scabies
Scabies is characterized by threadlike channels or burrows beneath the skin, and may also result in pustules, vesicles, and excoriations. The lesions are a few millimeters in length, with a swollen nodule or red papule that harbors the itch mite.
GENDER INDICATOR
In males, crusted lesions frequently manifest on the glans, shaft, and scrotum. Lesions may develop on the nipples in women. These lesions exhibit a preference for skin creases in both genders. Crusty excoriated lesions also manifest on the wrists, elbows, axillae, waistline, posterior knees, and ankles. Associated pruritus exacerbates with inactivity and elevated temperatures.
Variola major (smallpox)
Preliminary indications encompass elevated temperature, general discomfort, extreme fatigue, intense cephalalgia, lumbar pain, and gastrointestinal distress. A maculopapular rash emerges on the mucosal surfaces of the mouth, throat, face, and forearms, subsequently disseminating to the trunk and legs. Within two days, the rash evolves into vesicular and subsequently pustular lesions. The lesions manifest concurrently, exhibit uniform characteristics, and are more pronounced on the facial and extremity regions. The pustules are round, solid, and deeply entrenched in the dermis. After 8 to 9 days, the pustules develop a crust, which subsequently detaches from the skin, resulting in a pitted scar. In lethal instances, mortality occurs due to encephalitis, significant hemorrhaging, or subsequent infection
Varicella zoster
As immunity against varicella wanes, the virus reactivates along a dermatome, resulting in intensely painful and itchy vesicles and pustules (herpes zoster, or shingles). Despite the elimination of the rash, individuals may have chronic pain (postherpetic neuralgia) that can last for months. Alternative Causes Pharmaceutical substances. Bromides and iodides frequently induce a pustular rash.
Additional pharmacological causes encompass corticotropin, corticosteroids, dactinomycin, trimethadione, lithium, phenytoin, phenobarbital, isoniazid, hormonal contraceptives, androgens, and anabolic steroids.
Monitor wound and skin isolation protocols until infection is excluded by a Gram stain or culture and sensitivity analysis of the pustule's contents. If the organism is contagious, prevent drainage from contacting unaffected skin. Instruct the patient to maintain the segregation of his bathroom items and linens from those of other family members. Pain and itching, changes in body image, and the stress of solitude may lead to sleep disturbances, anxiety, and depression. Administer analgesics and antipruritics, and prompt the patient to articulate his emotions.
Elucidate the etiology of the condition, available therapeutic modalities, and strategies to mitigate the transmission of infection. Offer emotional assistance and knowledge on pain and itching alleviation. Disorders that cause a pustular rash in infants include varicella, erythema toxicum neonatorum, candidiasis, impetigo, infantile acropustulosis, and acrodermatitis enteropathica.

- Published on
Symptoms and Signs - Widened Pulse Pressure
Pulse pressure is the differential between systolic and diastolic blood pressures. Systolic pressure typically exceeds diastolic pressure by around 40 mm Hg. Widened pulse pressure - a disparity above 50 mm Hg — frequently arises as a physiological reaction to fever, elevated temperatures, physical exertion, anxiety, anemia, or pregnancy. Nonetheless, it may also stem from specific neurological disorders—particularly life-threatening elevated intracranial pressure (ICP)—or from cardiovascular conditions that induce retrograde blood flow into the heart with each contraction, such as aortic insufficiency. Widened pulse pressure can be readily determined by monitoring arterial blood pressure and is frequently observed during standard sphygmomanometric measurements.
URGENT INTERVENTIONS
If the patient's level of consciousness (LOC) is diminished and you suspect that the widening pulse pressure is due to increased intracranial pressure (ICP), assess his vital signs. Ensure a patent airway and prepare to hyperventilate the patient using a handheld resuscitation bag to decrease the partial pressure of carbon dioxide and, therefore, intracranial pressure. Conduct a comprehensive neurologic examination to establish a baseline for evaluating future alterations. Utilize the Glasgow Coma Scale to assess the patient's level of consciousness.
Additionally, evaluate cranial nerve function, particularly cranial nerves III, IV, and VI, and examine pupillary responses, reflexes, and muscular tone. The insertion of an intracranial pressure monitor may be required. If increasing intracranial pressure is not suspected, inquire about accompanying symptoms, including chest pain, dyspnea, weakness, exhaustion, or syncope. Examine for edema and auscultate for murmurs.
Etiological Factors
Aortic regurgitation
In acute aortic insufficiency, the pulse pressure steadily spreads as the valve deteriorates, leading to a bounding pulse and the emergence of an atrial or ventricular gallop. These symptoms may include chest pain, palpitations, pallor, pronounced carotid pulsations, pulsus bisferiens, and indicators of heart failure, such as crackles, dyspnea, and jugular vein distention. Auscultation may disclose several murmurs, including a prevalent early diastolic murmur and an apical diastolic rumble known as the Austin Flint murmur.
Arteriosclerosis
Arteriosclerosis leads to diminished arterial compliance, resulting in a progressive and permanent widening of pulse pressure if the underlying condition remains untreated. This symptom is preceded by mild hypertension and is accompanied by indications of vascular insufficiency, including claudication, angina, and abnormalities in speech and vision.
Febrile condition
A fever may result in an increased pulse pressure. Associated symptoms differ based on the particular condition.
Elevated intracranial pressure
Widening pulse pressure is an intermediate to late indicator of elevated intracranial pressure. A diminished level of consciousness is the initial and most sensitive sign of this critical state, while the emergence and advancement of widening pulse pressure correspond with increasing intracranial pressure. A disparity of 50 mm Hg may indicate a fast decline in the patient's health.
Evaluation indicates Cushing's triad: bradycardia, hypertension, and alterations in breathing patterns. Additional findings encompass cephalalgia, emesis, and compromised or asymmetrical motor function. The patient may also demonstrate visual abnormalities, including blurriness or photophobia, as well as alterations in pupil size.
Should the patient exhibit elevated intracranial pressure, consistently reassess their neurological condition and meticulously match your observations with prior exams. Remain vigilant for signs of restlessness, disorientation, unresponsiveness, or diminished level of consciousness. It is important to note that elevated intracranial pressure (ICP) is typically indicated by nuanced alterations in the patient's state rather than the sudden onset of a singular sign or symptom.
Elucidate necessary dietary adjustments, including the limitation of sodium and saturated fats. Emphasize the significance of scheduling rest intervals. In the event of a diminished level of consciousness in the patient, deliberate on certain safety protocols to enact.
Elevated intracranial pressure results in an expanded pulse pressure in a pediatric patient. Patent ductus arteriosus (PDA) may also contribute to this condition, however this indication might not be apparent at birth. The older child with PDA exhibits exertional dyspnea, accompanied by a further widening of pulse pressure during physical activity. Guidelines for Geriatric Care Recent studies indicate that widening pulse pressure serves as a more potent predictor of cardiovascular events in elderly people compared to elevated systolic or diastolic blood pressure.
Pulse pressure is the differential between systolic and diastolic blood pressures. Systolic pressure typically exceeds diastolic pressure by around 40 mm Hg. Widened pulse pressure - a disparity above 50 mm Hg — frequently arises as a physiological reaction to fever, elevated temperatures, physical exertion, anxiety, anemia, or pregnancy. Nonetheless, it may also stem from specific neurological disorders—particularly life-threatening elevated intracranial pressure (ICP)—or from cardiovascular conditions that induce retrograde blood flow into the heart with each contraction, such as aortic insufficiency. Widened pulse pressure can be readily determined by monitoring arterial blood pressure and is frequently observed during standard sphygmomanometric measurements.
URGENT INTERVENTIONS
If the patient's level of consciousness (LOC) is diminished and you suspect that the widening pulse pressure is due to increased intracranial pressure (ICP), assess his vital signs. Ensure a patent airway and prepare to hyperventilate the patient using a handheld resuscitation bag to decrease the partial pressure of carbon dioxide and, therefore, intracranial pressure. Conduct a comprehensive neurologic examination to establish a baseline for evaluating future alterations. Utilize the Glasgow Coma Scale to assess the patient's level of consciousness.
Additionally, evaluate cranial nerve function, particularly cranial nerves III, IV, and VI, and examine pupillary responses, reflexes, and muscular tone. The insertion of an intracranial pressure monitor may be required. If increasing intracranial pressure is not suspected, inquire about accompanying symptoms, including chest pain, dyspnea, weakness, exhaustion, or syncope. Examine for edema and auscultate for murmurs.
Etiological Factors
Aortic regurgitation
In acute aortic insufficiency, the pulse pressure steadily spreads as the valve deteriorates, leading to a bounding pulse and the emergence of an atrial or ventricular gallop. These symptoms may include chest pain, palpitations, pallor, pronounced carotid pulsations, pulsus bisferiens, and indicators of heart failure, such as crackles, dyspnea, and jugular vein distention. Auscultation may disclose several murmurs, including a prevalent early diastolic murmur and an apical diastolic rumble known as the Austin Flint murmur.
Arteriosclerosis
Arteriosclerosis leads to diminished arterial compliance, resulting in a progressive and permanent widening of pulse pressure if the underlying condition remains untreated. This symptom is preceded by mild hypertension and is accompanied by indications of vascular insufficiency, including claudication, angina, and abnormalities in speech and vision.
Febrile condition
A fever may result in an increased pulse pressure. Associated symptoms differ based on the particular condition.
Elevated intracranial pressure
Widening pulse pressure is an intermediate to late indicator of elevated intracranial pressure. A diminished level of consciousness is the initial and most sensitive sign of this critical state, while the emergence and advancement of widening pulse pressure correspond with increasing intracranial pressure. A disparity of 50 mm Hg may indicate a fast decline in the patient's health.
Evaluation indicates Cushing's triad: bradycardia, hypertension, and alterations in breathing patterns. Additional findings encompass cephalalgia, emesis, and compromised or asymmetrical motor function. The patient may also demonstrate visual abnormalities, including blurriness or photophobia, as well as alterations in pupil size.
Should the patient exhibit elevated intracranial pressure, consistently reassess their neurological condition and meticulously match your observations with prior exams. Remain vigilant for signs of restlessness, disorientation, unresponsiveness, or diminished level of consciousness. It is important to note that elevated intracranial pressure (ICP) is typically indicated by nuanced alterations in the patient's state rather than the sudden onset of a singular sign or symptom.
Elucidate necessary dietary adjustments, including the limitation of sodium and saturated fats. Emphasize the significance of scheduling rest intervals. In the event of a diminished level of consciousness in the patient, deliberate on certain safety protocols to enact.
Elevated intracranial pressure results in an expanded pulse pressure in a pediatric patient. Patent ductus arteriosus (PDA) may also contribute to this condition, however this indication might not be apparent at birth. The older child with PDA exhibits exertional dyspnea, accompanied by a further widening of pulse pressure during physical activity. Guidelines for Geriatric Care Recent studies indicate that widening pulse pressure serves as a more potent predictor of cardiovascular events in elderly people compared to elevated systolic or diastolic blood pressure.
- Published on
Symptoms and Signs – Differential Diagnosis of Pulsus Alternans
Pulsus alternans, characterized by a beat-to-beat variation in the magnitude and strength of a peripheral pulse, is indicative of severe left-sided heart failure. Despite the regularity of the pulse rhythm, contractions fluctuate between powerful and feeble. Refer to Comparing Arterial Pressure Waves, page 608. A change in the intensity of heart sounds and existing heart murmurs may accompany this symptom. Pulsus alternans is believed to arise from variations in stroke volume associated with beat-to-beat fluctuations in the contractility of the left ventricle. Recumbency or physical activity enhances venous return and mitigates the irregular pulse, which often resolves with heart failure medication. Infrequently, a patient exhibiting normal left ventricular function may present with pulsus alternans; nonetheless, this aberrant pulse typically does not endure beyond 10 to 12 beats.
Pulsus alternans, while most readily seen using sphygmomanometry, can also be discerned by palpating the brachial, radial, or femoral artery when systolic pressure fluctuates by greater than 20 mm Hg between beats. Due to the minor fluctuations in arterial pressure that transpire during regular respiration, which may conceal this aberrant pulse, it is necessary for the patient to hold their breath during palpation. Exert gentle pressure to prevent extinguishing the feebler pulse.
To identify pulsus alternans with a sphygmomanometer, inflate the cuff 10 to 20 mm Hg above the systolic pressure assessed by palpation, then gradually deflate it. Initially, only the prominent beats will be audible. As deflation progresses, all beats will become discernible and tangible, subsequently achieving uniform intensity. The disparity between this point and the peak systolic level is frequently utilized to assess the extent of pulsus alternans. Upon the removal of the cuff, pulsus alternans reemerges. At times, the faint beat is so diminished that no discernible pulse is felt at the periphery. This results in complete pulsus alternans, an apparent reduction of the pulse rate by half.
URGENT INTERVENTIONS
Pulsus alternans signifies a significant alteration in the patient's condition. Upon detection, promptly assess his additional vital signs. Thoroughly assess the patient's heart rate, breathing pattern, and blood pressure. Auscultate for a ventricular gallop and heightened crackles.
Etiological Factors in Medicine
Left ventricular heart failure.
Pulsus alternans in left-sided heart failure is typically triggered by a premature contraction and is virtually invariably accompanied by a ventricular gallop. Additional observations encompass hypotension and cyanosis. Potential respiratory manifestations encompass exertional and paroxysmal nocturnal dyspnea, orthopnea, tachypnea, Cheyne-Stokes respirations, hemoptysis, and crackles. Fatigue and debilitation are prevalent.
In the event of acute left-sided heart failure, prepare the patient for pulmonary artery catheter insertion and transport to an intensive or cardiac care unit. Simultaneously, raise the head of his bed to enhance respiratory expansion and augment oxygenation. Modify the patient's existing treatment regimen to enhance cardiac output, alleviate the heart's workload, and facilitate diuresis.
Instruct the patient regarding left-sided heart failure, the prescribed pharmacological treatments and their potential side effects, as well as suggested lifestyle modifications. Emphasize the significance of subsequent care with a healthcare provider. Pulsus alternans, which can also manifest in a child with heart failure, may be challenging to evaluate if the youngster is crying or agitated. Attempt to soothe the infant by holding him, if his condition allows. Pulsus Bisferiens A biferious pulse is a hyperdynamic, double-peaked pulse distinguished by two systolic peaks separated by a midsystolic trough. The two peaks may be equivalent or one may exceed the other; often, however, the initial peak is more pronounced or vigorous than the subsequent one. The initial peak (percussion wave) is thought to represent the pulse pressure, whereas the subsequent peak (tidal wave) is attributed to reverberation from the periphery.
Pulsus bisferiens occurs in instances where a substantial blood volume is swiftly expelled from the left ventricle, such as in aortic insufficiency. The pulse may be detected in peripheral arteries or shown on an arterial pressure wave recording.
To identify pulsus bisferiens, gently palpate the carotid, brachial, radial, or femoral artery. The pulse is most readily palpable in the carotid artery. Simultaneously, auscultate the patient's heart sounds to ascertain whether the two perceptible peaks occur during systole. Should they do so, you will perceive the dual pulse between S1 and S2.
Medical History and Physical Assessment
Upon detecting a biferiant pulse, examine the patient's medical history for heart conditions. Subsequently, ascertain the medications he is now prescribed, if any, and inquire about any further medical conditions he may have. Additionally, inquire about the progression of related signs and symptoms, like dyspnea, chest pain, or exhaustion. Determine the duration of his symptoms and whether they fluctuate with exercise or rest. Subsequently, assess his vital signs and auscultate for any abnormal cardiac or respiratory sounds.
Etiological Factors
Aortic regurgitation.
Aortic insufficiency is characterized by a bifid pulse in the heart. Most patients with chronic aortic insufficiency, the most prevalent organic cardiac abnormality, remain asymptomatic until the ages of 40 to 50. Nonetheless, exertional dyspnea, exacerbated tiredness, orthopnea, and ultimately, paroxysmal nocturnal dyspnea may manifest. Acute aortic insufficiency can manifest as signs and symptoms of left-sided heart failure and circulatory collapse, including weakness, acute dyspnea, hypotension, a ventricular gallop, and tachycardia. Supplementary findings encompass chest discomfort, palpitations, pallor, and pronounced, sudden carotid pulsations. The patient may present with expanded pulse pressure and one or more murmurs, particularly an apical diastolic rumble (Austin Flint murmur). Elevated cardiac output conditions. Pulsus bisferiens typically manifests in high-output conditions, including anemia, thyrotoxicosis, fever, and physical exertion. Accompanying signs differ based on the underlying etiology and may encompass mild tachycardia, a cervical venous hum, and an increased pulse pressure.
Hypertrophic obstructive cardiomyopathy
Approximately 40% of individuals with hypertrophic obstructive cardiomyopathy exhibit pulsus bisferiens due to a pressure gradient in the left ventricular outflow tract. The pulse is documented more frequently than it is palpated; it ascends swiftly, with the initial wave being the most vigorous. Accompanying observations include of a systolic murmur, dyspnea, angina, tiredness, and syncope.
Analysis of Arterial Pressure Waves
The depicted waveforms assist in distinguishing a normal arterial pulse from pulsus alternans and pulsus paradoxus.
STANDARD ARTERIAL PULSE
The percussion wave in a typical arterial pulse signifies the ejection of blood into the aorta during early systole. The tidal wave represents the apex of the pulse wave (subsequently systole), whereas the dicrotic notch signifies the commencement of diastole.
Pulsus alternans
Pulsus alternans refers to a rhythmic variation in pulse amplitude and strength from one beat to the next. Despite the regularity of the pulsus alternans rhythm, the volume fluctuates. Upon measuring the blood pressure of a patient exhibiting this anomaly, one will initially detect a pronounced Korotkoff sound, followed by a softer sound, with the two alternating continuously. Pulsus alternans frequently occurs in conditions of diminished contractility associated with left-sided heart failure.
Pulsus Bisferiens
Pulsus bisferiens is characterized by a double-beating pulse exhibiting two systolic peaks. The initial beat indicates pulse pressure, whereas the subsequent one represents reverberation from the periphery. Pulsus bisferiens is typically associated with aortic insufficiency (including aortic stenosis and aortic regurgitation), hypertrophic cardiomyopathy, or elevated cardiac output conditions.
Pulsus Paradoxus
Pulsus paradoxus is an abnormal decrease in blood pressure during inspiration, caused by an elevation in negative intrathoracic pressure. Pulsus paradoxus more than 10 mm Hg is deemed abnormal and may arise from cardiac tamponade, constrictive pericarditis, or severe pulmonary illness.
Prepare the patient for diagnostic evaluations, such an electrocardiogram, chest X-ray, cardiac catheterization, or angiography, to ascertain the underlying reason of the irregular pulse.
Identify the signs and symptoms of heart failure that necessitate reporting, as well as the significance of scheduling rest times. Pulsus bisferiens can be detected in children with a significant patent ductus arteriosus, as well as in those with congenital aortic stenosis and insufficiency.
Pulsus alternans, characterized by a beat-to-beat variation in the magnitude and strength of a peripheral pulse, is indicative of severe left-sided heart failure. Despite the regularity of the pulse rhythm, contractions fluctuate between powerful and feeble. Refer to Comparing Arterial Pressure Waves, page 608. A change in the intensity of heart sounds and existing heart murmurs may accompany this symptom. Pulsus alternans is believed to arise from variations in stroke volume associated with beat-to-beat fluctuations in the contractility of the left ventricle. Recumbency or physical activity enhances venous return and mitigates the irregular pulse, which often resolves with heart failure medication. Infrequently, a patient exhibiting normal left ventricular function may present with pulsus alternans; nonetheless, this aberrant pulse typically does not endure beyond 10 to 12 beats.
Pulsus alternans, while most readily seen using sphygmomanometry, can also be discerned by palpating the brachial, radial, or femoral artery when systolic pressure fluctuates by greater than 20 mm Hg between beats. Due to the minor fluctuations in arterial pressure that transpire during regular respiration, which may conceal this aberrant pulse, it is necessary for the patient to hold their breath during palpation. Exert gentle pressure to prevent extinguishing the feebler pulse.
To identify pulsus alternans with a sphygmomanometer, inflate the cuff 10 to 20 mm Hg above the systolic pressure assessed by palpation, then gradually deflate it. Initially, only the prominent beats will be audible. As deflation progresses, all beats will become discernible and tangible, subsequently achieving uniform intensity. The disparity between this point and the peak systolic level is frequently utilized to assess the extent of pulsus alternans. Upon the removal of the cuff, pulsus alternans reemerges. At times, the faint beat is so diminished that no discernible pulse is felt at the periphery. This results in complete pulsus alternans, an apparent reduction of the pulse rate by half.
URGENT INTERVENTIONS
Pulsus alternans signifies a significant alteration in the patient's condition. Upon detection, promptly assess his additional vital signs. Thoroughly assess the patient's heart rate, breathing pattern, and blood pressure. Auscultate for a ventricular gallop and heightened crackles.
Etiological Factors in Medicine
Left ventricular heart failure.
Pulsus alternans in left-sided heart failure is typically triggered by a premature contraction and is virtually invariably accompanied by a ventricular gallop. Additional observations encompass hypotension and cyanosis. Potential respiratory manifestations encompass exertional and paroxysmal nocturnal dyspnea, orthopnea, tachypnea, Cheyne-Stokes respirations, hemoptysis, and crackles. Fatigue and debilitation are prevalent.
In the event of acute left-sided heart failure, prepare the patient for pulmonary artery catheter insertion and transport to an intensive or cardiac care unit. Simultaneously, raise the head of his bed to enhance respiratory expansion and augment oxygenation. Modify the patient's existing treatment regimen to enhance cardiac output, alleviate the heart's workload, and facilitate diuresis.
Instruct the patient regarding left-sided heart failure, the prescribed pharmacological treatments and their potential side effects, as well as suggested lifestyle modifications. Emphasize the significance of subsequent care with a healthcare provider. Pulsus alternans, which can also manifest in a child with heart failure, may be challenging to evaluate if the youngster is crying or agitated. Attempt to soothe the infant by holding him, if his condition allows. Pulsus Bisferiens A biferious pulse is a hyperdynamic, double-peaked pulse distinguished by two systolic peaks separated by a midsystolic trough. The two peaks may be equivalent or one may exceed the other; often, however, the initial peak is more pronounced or vigorous than the subsequent one. The initial peak (percussion wave) is thought to represent the pulse pressure, whereas the subsequent peak (tidal wave) is attributed to reverberation from the periphery.
Pulsus bisferiens occurs in instances where a substantial blood volume is swiftly expelled from the left ventricle, such as in aortic insufficiency. The pulse may be detected in peripheral arteries or shown on an arterial pressure wave recording.
To identify pulsus bisferiens, gently palpate the carotid, brachial, radial, or femoral artery. The pulse is most readily palpable in the carotid artery. Simultaneously, auscultate the patient's heart sounds to ascertain whether the two perceptible peaks occur during systole. Should they do so, you will perceive the dual pulse between S1 and S2.
Medical History and Physical Assessment
Upon detecting a biferiant pulse, examine the patient's medical history for heart conditions. Subsequently, ascertain the medications he is now prescribed, if any, and inquire about any further medical conditions he may have. Additionally, inquire about the progression of related signs and symptoms, like dyspnea, chest pain, or exhaustion. Determine the duration of his symptoms and whether they fluctuate with exercise or rest. Subsequently, assess his vital signs and auscultate for any abnormal cardiac or respiratory sounds.
Etiological Factors
Aortic regurgitation.
Aortic insufficiency is characterized by a bifid pulse in the heart. Most patients with chronic aortic insufficiency, the most prevalent organic cardiac abnormality, remain asymptomatic until the ages of 40 to 50. Nonetheless, exertional dyspnea, exacerbated tiredness, orthopnea, and ultimately, paroxysmal nocturnal dyspnea may manifest. Acute aortic insufficiency can manifest as signs and symptoms of left-sided heart failure and circulatory collapse, including weakness, acute dyspnea, hypotension, a ventricular gallop, and tachycardia. Supplementary findings encompass chest discomfort, palpitations, pallor, and pronounced, sudden carotid pulsations. The patient may present with expanded pulse pressure and one or more murmurs, particularly an apical diastolic rumble (Austin Flint murmur). Elevated cardiac output conditions. Pulsus bisferiens typically manifests in high-output conditions, including anemia, thyrotoxicosis, fever, and physical exertion. Accompanying signs differ based on the underlying etiology and may encompass mild tachycardia, a cervical venous hum, and an increased pulse pressure.
Hypertrophic obstructive cardiomyopathy
Approximately 40% of individuals with hypertrophic obstructive cardiomyopathy exhibit pulsus bisferiens due to a pressure gradient in the left ventricular outflow tract. The pulse is documented more frequently than it is palpated; it ascends swiftly, with the initial wave being the most vigorous. Accompanying observations include of a systolic murmur, dyspnea, angina, tiredness, and syncope.
Analysis of Arterial Pressure Waves
The depicted waveforms assist in distinguishing a normal arterial pulse from pulsus alternans and pulsus paradoxus.
STANDARD ARTERIAL PULSE
The percussion wave in a typical arterial pulse signifies the ejection of blood into the aorta during early systole. The tidal wave represents the apex of the pulse wave (subsequently systole), whereas the dicrotic notch signifies the commencement of diastole.
Pulsus alternans
Pulsus alternans refers to a rhythmic variation in pulse amplitude and strength from one beat to the next. Despite the regularity of the pulsus alternans rhythm, the volume fluctuates. Upon measuring the blood pressure of a patient exhibiting this anomaly, one will initially detect a pronounced Korotkoff sound, followed by a softer sound, with the two alternating continuously. Pulsus alternans frequently occurs in conditions of diminished contractility associated with left-sided heart failure.
Pulsus Bisferiens
Pulsus bisferiens is characterized by a double-beating pulse exhibiting two systolic peaks. The initial beat indicates pulse pressure, whereas the subsequent one represents reverberation from the periphery. Pulsus bisferiens is typically associated with aortic insufficiency (including aortic stenosis and aortic regurgitation), hypertrophic cardiomyopathy, or elevated cardiac output conditions.
Pulsus Paradoxus
Pulsus paradoxus is an abnormal decrease in blood pressure during inspiration, caused by an elevation in negative intrathoracic pressure. Pulsus paradoxus more than 10 mm Hg is deemed abnormal and may arise from cardiac tamponade, constrictive pericarditis, or severe pulmonary illness.
Prepare the patient for diagnostic evaluations, such an electrocardiogram, chest X-ray, cardiac catheterization, or angiography, to ascertain the underlying reason of the irregular pulse.
Identify the signs and symptoms of heart failure that necessitate reporting, as well as the significance of scheduling rest times. Pulsus bisferiens can be detected in children with a significant patent ductus arteriosus, as well as in those with congenital aortic stenosis and insufficiency.
- Published on
Symptoms and Signs – Differential Diagnosis of Ptosis
Ptosis refers to the abnormal sagging of one or both upper eyelids. This sign may be persistent, progressing, or intermittent, and it can be unilateral or bilateral. Unilateral conditions are easily identifiable by assessing the relative locations of the eyelids. In cases of bilateral or moderate conditions, detection is challenging; the eyelids may be positioned unusually low, obscuring the upper portion of the iris or even partially concealing the pupil, rather than merely overlapping the iris. Additional indicators consist of a furrowed brow or a tilted head—both facilitate the patient's ability to view under their sagging eyelids. In cases of severe ptosis, the patient may be unable to elevate his eyelids spontaneously. Due to the potential similarity between ptosis and enophthalmos, exophthalmometry may be necessary. Ptosis may be categorized as either congenital or acquired.
Classification is essential for appropriate treatment.
Congenital ptosis arises from the underdevelopment of the levator muscle or dysfunction of the third cranial (oculomotor) nerve. Acquired ptosis may arise from trauma to or inflammation of the associated muscles and nerves, some pharmaceuticals, systemic diseases, intracranial lesions, or life-threatening aneurysms.
The predominant cause is elderly age, which diminishes muscle flexibility and results in senile ptosis.
Medical History and Physical Assessment
Inquire when the patient first observed the onset of his ptosis. Additionally, inquire whether it has deteriorated or improved since he first observed it. Ascertain whether he has lately experienced a catastrophic eye injury. If he has, refrain from manipulating the eye to avert additional harm. Inquire about ocular discomfort or cephalalgia, and ascertain its locus and intensity. Has the patient undergone alterations in vision? If so, request that he elucidate them. Acquire a comprehensive medication history, with particular emphasis on the administration of a chemotherapeutic agent. Evaluate the extent of ptosis and examine for eyelid edema, exophthalmos, deviation, and conjunctival injection. Assess extraocular muscle function by examining the six cardinal fields of sight. Meticulously assess the pupils' dimensions, hue, morphology, and responsiveness to illumination, and evaluate visual acuity. Be aware that ptosis may sometimes signify a life-threatening condition. Sudden unilateral ptosis may indicate a brain aneurysm.
Etiological Factors
Botulism
Acute cranial nerve damage resulting from botulism infection manifests with characteristic symptoms of ptosis, dysarthria, dysphagia, and diplopia. Additional findings encompass xerostomia, pharyngitis, asthenia, emesis, diarrhea, hyporeflexia, and dyspnea.
Cerebral aneurysm
An aneurysm compressing the oculomotor nerve may result in abrupt ptosis, diplopia, a dilated pupil, and an inability to swivel the eye. These could be the initial indications of this life-threatening condition. A ruptured aneurysm generally results in an abrupt, intense headache, accompanied by nausea, vomiting, and a diminished state of awareness (LOC). Additional findings comprise nuchal rigidity, back and leg discomfort, fever, restlessness, irritability, intermittent seizures, blurred vision, hemiparesis, sensory abnormalities, dysphagia, and visual impairments.
Neoplasm of the lacrimal gland
A tumor of the lacrimal gland typically results in mild to severe ptosis, contingent upon the tumor's size and location. It may also induce brow elevation, exophthalmos, ocular deviation, and potentially, ocular discomfort.
Myasthenia gravis
The initial indication of myasthenia gravis is often gradual bilateral ptosis, which can range from mild to severe and is associated with diminished eye closure and diplopia. Additional characteristics encompass muscular weakness and exhaustion, which may ultimately result in paralysis. Depending on the afflicted muscles, other observations may encompass masklike facies, difficulty in mastication or deglutition, dyspnea, and cyanosis.
Ocular muscular dystrophy
In ocular muscular dystrophy, bilateral ptosis gradually advances to total eyelid occlusion. Associated signs and symptoms encompass progressive external ophthalmoplegia, as well as muscular weakness and atrophy affecting the upper face, neck, trunk, and limbs.
Ocular injury
Injury to the nerves or muscles governing the eyelids may result in mild to severe ptosis. Depending on the extent of the injury, symptoms may include ocular pain, eyelid edema, ecchymosis, and diminished visual acuity.
Parry-Romberg syndrome
Parry-Romberg syndrome is characterized by unilateral ptosis and facial hemiatrophy. Additional indicators comprise miosis, diminished pupillary response to light, enophthalmos, heterochromia, ocular muscle paralysis, nystagmus, and atrophy of the neck, shoulder, trunk, and extremities.
Alternative Causes Pharmaceuticals
Vinca alkaloids may induce ptosis. Plumbism. In cases of lead poisoning, ptosis typically manifests during a period of 3 to 6 months. Additional findings encompass anorexia, nausea, vomiting, diarrhea, colicky abdominal discomfort, a lead line on the gums, diminished level of consciousness, tachycardia, hypotension, and potentially irritability and peripheral nerve weakness.
Orient the patient to his surroundings if he has diminished visual acuity. Offer specialized spectacle frames that elevate the eyelid through traction via a wire support. These frames are typically utilized to assist patients with transient paresis or those who are not suitable candidates for surgery. Prepare the patient for diagnostic assessments, including the Tensilon test and slit-lamp examination. Should he require surgical intervention to rectify levator muscle dysfunction, elucidate the method to him.
Elucidate the fundamental etiology of the condition, any necessary diagnostic assessments, and the therapeutic alternatives available for the patient. Additionally, address self-esteem concerns.
Astigmatism and myopia may be linked to childhood ptosis. Parents generally identify congenital ptosis during infancy. Typically, ptosis is unilateral, persistent, and associated with lagophthalmos, resulting in the newborn sleeping with eyes partially open. In the event of this occurrence, instruct on appropriate ocular care to avert desiccation.
Ptosis refers to the abnormal sagging of one or both upper eyelids. This sign may be persistent, progressing, or intermittent, and it can be unilateral or bilateral. Unilateral conditions are easily identifiable by assessing the relative locations of the eyelids. In cases of bilateral or moderate conditions, detection is challenging; the eyelids may be positioned unusually low, obscuring the upper portion of the iris or even partially concealing the pupil, rather than merely overlapping the iris. Additional indicators consist of a furrowed brow or a tilted head—both facilitate the patient's ability to view under their sagging eyelids. In cases of severe ptosis, the patient may be unable to elevate his eyelids spontaneously. Due to the potential similarity between ptosis and enophthalmos, exophthalmometry may be necessary. Ptosis may be categorized as either congenital or acquired.
Classification is essential for appropriate treatment.
Congenital ptosis arises from the underdevelopment of the levator muscle or dysfunction of the third cranial (oculomotor) nerve. Acquired ptosis may arise from trauma to or inflammation of the associated muscles and nerves, some pharmaceuticals, systemic diseases, intracranial lesions, or life-threatening aneurysms.
The predominant cause is elderly age, which diminishes muscle flexibility and results in senile ptosis.
Medical History and Physical Assessment
Inquire when the patient first observed the onset of his ptosis. Additionally, inquire whether it has deteriorated or improved since he first observed it. Ascertain whether he has lately experienced a catastrophic eye injury. If he has, refrain from manipulating the eye to avert additional harm. Inquire about ocular discomfort or cephalalgia, and ascertain its locus and intensity. Has the patient undergone alterations in vision? If so, request that he elucidate them. Acquire a comprehensive medication history, with particular emphasis on the administration of a chemotherapeutic agent. Evaluate the extent of ptosis and examine for eyelid edema, exophthalmos, deviation, and conjunctival injection. Assess extraocular muscle function by examining the six cardinal fields of sight. Meticulously assess the pupils' dimensions, hue, morphology, and responsiveness to illumination, and evaluate visual acuity. Be aware that ptosis may sometimes signify a life-threatening condition. Sudden unilateral ptosis may indicate a brain aneurysm.
Etiological Factors
Botulism
Acute cranial nerve damage resulting from botulism infection manifests with characteristic symptoms of ptosis, dysarthria, dysphagia, and diplopia. Additional findings encompass xerostomia, pharyngitis, asthenia, emesis, diarrhea, hyporeflexia, and dyspnea.
Cerebral aneurysm
An aneurysm compressing the oculomotor nerve may result in abrupt ptosis, diplopia, a dilated pupil, and an inability to swivel the eye. These could be the initial indications of this life-threatening condition. A ruptured aneurysm generally results in an abrupt, intense headache, accompanied by nausea, vomiting, and a diminished state of awareness (LOC). Additional findings comprise nuchal rigidity, back and leg discomfort, fever, restlessness, irritability, intermittent seizures, blurred vision, hemiparesis, sensory abnormalities, dysphagia, and visual impairments.
Neoplasm of the lacrimal gland
A tumor of the lacrimal gland typically results in mild to severe ptosis, contingent upon the tumor's size and location. It may also induce brow elevation, exophthalmos, ocular deviation, and potentially, ocular discomfort.
Myasthenia gravis
The initial indication of myasthenia gravis is often gradual bilateral ptosis, which can range from mild to severe and is associated with diminished eye closure and diplopia. Additional characteristics encompass muscular weakness and exhaustion, which may ultimately result in paralysis. Depending on the afflicted muscles, other observations may encompass masklike facies, difficulty in mastication or deglutition, dyspnea, and cyanosis.
Ocular muscular dystrophy
In ocular muscular dystrophy, bilateral ptosis gradually advances to total eyelid occlusion. Associated signs and symptoms encompass progressive external ophthalmoplegia, as well as muscular weakness and atrophy affecting the upper face, neck, trunk, and limbs.
Ocular injury
Injury to the nerves or muscles governing the eyelids may result in mild to severe ptosis. Depending on the extent of the injury, symptoms may include ocular pain, eyelid edema, ecchymosis, and diminished visual acuity.
Parry-Romberg syndrome
Parry-Romberg syndrome is characterized by unilateral ptosis and facial hemiatrophy. Additional indicators comprise miosis, diminished pupillary response to light, enophthalmos, heterochromia, ocular muscle paralysis, nystagmus, and atrophy of the neck, shoulder, trunk, and extremities.
Alternative Causes Pharmaceuticals
Vinca alkaloids may induce ptosis. Plumbism. In cases of lead poisoning, ptosis typically manifests during a period of 3 to 6 months. Additional findings encompass anorexia, nausea, vomiting, diarrhea, colicky abdominal discomfort, a lead line on the gums, diminished level of consciousness, tachycardia, hypotension, and potentially irritability and peripheral nerve weakness.
Orient the patient to his surroundings if he has diminished visual acuity. Offer specialized spectacle frames that elevate the eyelid through traction via a wire support. These frames are typically utilized to assist patients with transient paresis or those who are not suitable candidates for surgery. Prepare the patient for diagnostic assessments, including the Tensilon test and slit-lamp examination. Should he require surgical intervention to rectify levator muscle dysfunction, elucidate the method to him.
Elucidate the fundamental etiology of the condition, any necessary diagnostic assessments, and the therapeutic alternatives available for the patient. Additionally, address self-esteem concerns.
Astigmatism and myopia may be linked to childhood ptosis. Parents generally identify congenital ptosis during infancy. Typically, ptosis is unilateral, persistent, and associated with lagophthalmos, resulting in the newborn sleeping with eyes partially open. In the event of this occurrence, instruct on appropriate ocular care to avert desiccation.

- Published on
Symptoms and Signs – Differential Diagnosis of Narrowed Pulse Pressure
Pulse pressure, defined as the differential between systolic and diastolic blood pressures, is assessed using sphygmomanometry or intra-arterial monitoring. Systolic pressure typically surpasses diastolic by around 40 mm Hg. Narrowed pressure – a disparity of less than 30 mm Hg — arises when peripheral vascular resistance escalates, cardiac output diminishes, or intravascular volume significantly reduces. In conditions that induce mechanical blockage, such as aortic stenosis, pulse pressure correlates directly with the severity of the underlying problem. Narrowed pulse pressure, typically a late indicator, does not in itself denote an emergency, despite its frequent association with shock and other critical conditions. Medical History and Physical Assessment Upon identifying a constricted pulse pressure, assess for additional indicators of heart failure, including hypotension, tachycardia, dyspnea, jugular vein distention, pulmonary crackles, and diminished urine output. Additionally, assess alterations in skin temperature or pigmentation, the intensity of peripheral pulses, and the patient's level of awareness (LOC). Perform auscultation of the heart to detect murmurs. Inquire about a history of chest discomfort, dizziness, or syncope.
Etiological Factors
Cardiac tamponade
In cardiac tamponade, a life-threatening condition, pulse pressure decreases by 10 to 20 mm Hg. Classic signs include paradoxical pulse, jugular vein distention, hypotension, and muffled heart sounds. The patient may exhibit anxiety, restlessness, cyanosis, diaphoresis, and chest pain. He may demonstrate dyspnea, tachypnea, diminished level of consciousness, and a weak, fast pulse. A pericardial friction rub and hepatomegaly may additionally manifest.
Cardiac insufficiency
Narrowed pulse pressure manifests relatively late and may be associated with tachypnea, palpitations, dependent edema, consistent weight gain despite nausea and anorexia, chest tightness, diminished cognitive responsiveness, hypotension, diaphoresis, pallor, and oliguria. Evaluation indicates a ventricular gallop, inspiratory crackles, and potentially a sore, palpable liver. Subsequently, dullness arises at the lung bases, and hemoptysis, cyanosis, pronounced hepatomegaly, and significant pitting edema may manifest.
Shock
Anaphylactic shock results in restricted pulse pressure occurring late, following a fast, weak pulse that then becomes uniformly nonexistent. Shortly after exposure to an allergen, the patient exhibits hypotension, anxiety, restlessness, and a sense of impending doom, accompanied by severe pruritus, a throbbing headache, and potentially urticaria. Additional findings encompass dyspnea, stridor, and hoarseness; chest or throat constriction; skin flushing; nausea, stomach cramps, urine incontinence; and seizures. Narrowed pulse pressure manifests rather late in cardiogenic shock. Peripheral pulses are generally absent, whereas central pulses are feeble. A decrease in systolic pressure to 30 mm Hg below baseline, or a prolonged reading below 80 mm Hg not due to medication, results in inadequate tissue perfusion. Inadequate perfusion results in tachycardia, tachypnea, chilly, pale, clammy skin, cyanosis, oliguria, restlessness, disorientation, and obtundation. Narrowed pulse pressure manifests as a late symptom in hypovolemic shock. All peripheral pulses initially weaken and thereafter become universally missing. Prolonged shock results in hypotension, urine output below 25 mL/hour, disorientation, diminished level of consciousness, and potentially, hypothermia. Narrowed pulse pressure is a rather late indicator of septic shock. All peripheral pulses initially weaken and thereafter become universally missing. As shock advances, the patient has oliguria, polydipsia, anxiety, agitation, disorientation, and hypotension. The extremities exhibit coolness and cyanosis; the skin becomes chilly and clammy. Eventually, he experiences significant hypotension, ongoing oliguria or anuria, respiratory failure, and coma.
Closely observe the patient for alterations in pulse rate or quality, as well as for hypotension or a reduced level of consciousness. Prepare him for diagnostic testing, including echocardiogram, to identify valvular heart disease or cardiac tamponade resulting from a pericardial effusion.
Elucidate the disorder, its remedies, and the specific foods and fluids the patient should refrain from consuming. Emphasize the significance of rest intervals to mitigate weariness.Narrowed pulse pressure in children may arise from congenital aortic stenosis and conditions that also impact adults.
Pulse pressure, defined as the differential between systolic and diastolic blood pressures, is assessed using sphygmomanometry or intra-arterial monitoring. Systolic pressure typically surpasses diastolic by around 40 mm Hg. Narrowed pressure – a disparity of less than 30 mm Hg — arises when peripheral vascular resistance escalates, cardiac output diminishes, or intravascular volume significantly reduces. In conditions that induce mechanical blockage, such as aortic stenosis, pulse pressure correlates directly with the severity of the underlying problem. Narrowed pulse pressure, typically a late indicator, does not in itself denote an emergency, despite its frequent association with shock and other critical conditions. Medical History and Physical Assessment Upon identifying a constricted pulse pressure, assess for additional indicators of heart failure, including hypotension, tachycardia, dyspnea, jugular vein distention, pulmonary crackles, and diminished urine output. Additionally, assess alterations in skin temperature or pigmentation, the intensity of peripheral pulses, and the patient's level of awareness (LOC). Perform auscultation of the heart to detect murmurs. Inquire about a history of chest discomfort, dizziness, or syncope.
Etiological Factors
Cardiac tamponade
In cardiac tamponade, a life-threatening condition, pulse pressure decreases by 10 to 20 mm Hg. Classic signs include paradoxical pulse, jugular vein distention, hypotension, and muffled heart sounds. The patient may exhibit anxiety, restlessness, cyanosis, diaphoresis, and chest pain. He may demonstrate dyspnea, tachypnea, diminished level of consciousness, and a weak, fast pulse. A pericardial friction rub and hepatomegaly may additionally manifest.
Cardiac insufficiency
Narrowed pulse pressure manifests relatively late and may be associated with tachypnea, palpitations, dependent edema, consistent weight gain despite nausea and anorexia, chest tightness, diminished cognitive responsiveness, hypotension, diaphoresis, pallor, and oliguria. Evaluation indicates a ventricular gallop, inspiratory crackles, and potentially a sore, palpable liver. Subsequently, dullness arises at the lung bases, and hemoptysis, cyanosis, pronounced hepatomegaly, and significant pitting edema may manifest.
Shock
Anaphylactic shock results in restricted pulse pressure occurring late, following a fast, weak pulse that then becomes uniformly nonexistent. Shortly after exposure to an allergen, the patient exhibits hypotension, anxiety, restlessness, and a sense of impending doom, accompanied by severe pruritus, a throbbing headache, and potentially urticaria. Additional findings encompass dyspnea, stridor, and hoarseness; chest or throat constriction; skin flushing; nausea, stomach cramps, urine incontinence; and seizures. Narrowed pulse pressure manifests rather late in cardiogenic shock. Peripheral pulses are generally absent, whereas central pulses are feeble. A decrease in systolic pressure to 30 mm Hg below baseline, or a prolonged reading below 80 mm Hg not due to medication, results in inadequate tissue perfusion. Inadequate perfusion results in tachycardia, tachypnea, chilly, pale, clammy skin, cyanosis, oliguria, restlessness, disorientation, and obtundation. Narrowed pulse pressure manifests as a late symptom in hypovolemic shock. All peripheral pulses initially weaken and thereafter become universally missing. Prolonged shock results in hypotension, urine output below 25 mL/hour, disorientation, diminished level of consciousness, and potentially, hypothermia. Narrowed pulse pressure is a rather late indicator of septic shock. All peripheral pulses initially weaken and thereafter become universally missing. As shock advances, the patient has oliguria, polydipsia, anxiety, agitation, disorientation, and hypotension. The extremities exhibit coolness and cyanosis; the skin becomes chilly and clammy. Eventually, he experiences significant hypotension, ongoing oliguria or anuria, respiratory failure, and coma.
Closely observe the patient for alterations in pulse rate or quality, as well as for hypotension or a reduced level of consciousness. Prepare him for diagnostic testing, including echocardiogram, to identify valvular heart disease or cardiac tamponade resulting from a pericardial effusion.
Elucidate the disorder, its remedies, and the specific foods and fluids the patient should refrain from consuming. Emphasize the significance of rest intervals to mitigate weariness.Narrowed pulse pressure in children may arise from congenital aortic stenosis and conditions that also impact adults.

- Published on
Symptoms and Signs – Bounding Pulse
A bounding pulse, characterized by its strength and palpable nature, is generated by significant pressure waves resulting from blood ejection from the left ventricle during each contraction, and may be observable over superficial peripheral arteries. It is marked by consistent, periodic dilation and constriction of the artery walls and is not diminished by palpation pressure. An individual in good health exhibits a bounding pulse during physical exertion, gestation, and episodes of anxiety. This symptom may also arise from fever and specific endocrine, hematologic, and cardiovascular diseases that elevate the basal metabolic rate.
Medical History and Physical Assessment
Upon detecting a palpable pulse, assess the patient's further vital signs, followed by auscultation of the heart and lungs for any aberrant noises, rates, or rhythms. Inquire whether the patient has observed any weakness, weariness, dyspnea, or other alterations in health. Examine his medical history for hyperthyroidism, anemia, or a cardiovascular condition, and inquire about his alcohol consumption.
Etiological Factors
Acute alcoholism
Vasodilation results in a rapid, pulsating heartbeat and a reddened visage. An alcoholic breath odor and an ataxic gait are prevalent. Additional findings encompass hypothermia, bradypnea, laborious and noisy respirations, nausea, vomiting, diuresis, diminished consciousness, and seizures.
Aortic regurgitation
The bounding pulse linked to aortic insufficiency, often referred to as a water-hammer pulse, is marked by a swift, vigorous expansion of the arterial pulse, succeeded by a quick contraction. Widened pulse pressure is also observed. This condition may result in manifestations linked to left-sided heart failure and cardiovascular collapse, including weakness, severe dyspnea, hypotension, an S3 heart sound, and tachycardia. Supplementary findings encompass pallor, chest discomfort, palpitations, ness pronounced, sudden carotid pulsations. The patient may suffer pulsus bisferiens, an early systolic murmur, a murmur audible over the femoral artery during both systole and diastole, and a high-pitched diastolic murmur commencing with the second heart sound. An apical diastolic rumbling, known as the Austin Flint murmur, may manifest, particularly in cases of heart failure. The majority of individuals with chronic aortic insufficiency remain asymptomatic until their 40s or 50s, at which point they may have exertional dyspnea, heightened tiredness, orthopnea, and ultimately, paroxysmal nocturnal dyspnea, angina, and syncope
Febrile condition
A fever may induce a bounding pulse. The accompanying findings indicate the particular condition.
Thyrotoxicosis
Thyrotoxicosis results in a fast, robust, and pulsatile heartbeat. Accompanying symptoms include of tachycardia, palpitations, an S3 or S4 gallop, weight loss despite heightened appetite, and heat intolerance. The patient may also experience diarrhea, thyroid enlargement, dyspnea, tremors, anxiety, chest pain, exophthalmos, and indications of cardiovascular collapse. His skin will exhibit warmth, moisture, and diaphoresis, and he may demonstrate hypersensitivity to heat.
Prepare the patient for diagnostic laboratory and radiographic examinations. Should a bounding pulse be accompanied with a rapid or irregular heartbeat, it may be necessary to link the patient to a cardiac monitor for further assessment.
Examine the necessary dietary alterations and fluid limitations for the patient. Highlight the significance of abstaining from alcohol and, if necessary, direct the patient to Alcoholics Anonymous. Emphasize the significance of rest intervals and delineate the signs and symptoms that should be reported.
A bounding pulse may be normal in newborns or children due to the proximity of arteries to the skin surface. It may also arise from patent ductus arteriosus if the left-to-right shunt is substantial.
A bounding pulse, characterized by its strength and palpable nature, is generated by significant pressure waves resulting from blood ejection from the left ventricle during each contraction, and may be observable over superficial peripheral arteries. It is marked by consistent, periodic dilation and constriction of the artery walls and is not diminished by palpation pressure. An individual in good health exhibits a bounding pulse during physical exertion, gestation, and episodes of anxiety. This symptom may also arise from fever and specific endocrine, hematologic, and cardiovascular diseases that elevate the basal metabolic rate.
Medical History and Physical Assessment
Upon detecting a palpable pulse, assess the patient's further vital signs, followed by auscultation of the heart and lungs for any aberrant noises, rates, or rhythms. Inquire whether the patient has observed any weakness, weariness, dyspnea, or other alterations in health. Examine his medical history for hyperthyroidism, anemia, or a cardiovascular condition, and inquire about his alcohol consumption.
Etiological Factors
Acute alcoholism
Vasodilation results in a rapid, pulsating heartbeat and a reddened visage. An alcoholic breath odor and an ataxic gait are prevalent. Additional findings encompass hypothermia, bradypnea, laborious and noisy respirations, nausea, vomiting, diuresis, diminished consciousness, and seizures.
Aortic regurgitation
The bounding pulse linked to aortic insufficiency, often referred to as a water-hammer pulse, is marked by a swift, vigorous expansion of the arterial pulse, succeeded by a quick contraction. Widened pulse pressure is also observed. This condition may result in manifestations linked to left-sided heart failure and cardiovascular collapse, including weakness, severe dyspnea, hypotension, an S3 heart sound, and tachycardia. Supplementary findings encompass pallor, chest discomfort, palpitations, ness pronounced, sudden carotid pulsations. The patient may suffer pulsus bisferiens, an early systolic murmur, a murmur audible over the femoral artery during both systole and diastole, and a high-pitched diastolic murmur commencing with the second heart sound. An apical diastolic rumbling, known as the Austin Flint murmur, may manifest, particularly in cases of heart failure. The majority of individuals with chronic aortic insufficiency remain asymptomatic until their 40s or 50s, at which point they may have exertional dyspnea, heightened tiredness, orthopnea, and ultimately, paroxysmal nocturnal dyspnea, angina, and syncope
Febrile condition
A fever may induce a bounding pulse. The accompanying findings indicate the particular condition.
Thyrotoxicosis
Thyrotoxicosis results in a fast, robust, and pulsatile heartbeat. Accompanying symptoms include of tachycardia, palpitations, an S3 or S4 gallop, weight loss despite heightened appetite, and heat intolerance. The patient may also experience diarrhea, thyroid enlargement, dyspnea, tremors, anxiety, chest pain, exophthalmos, and indications of cardiovascular collapse. His skin will exhibit warmth, moisture, and diaphoresis, and he may demonstrate hypersensitivity to heat.
Prepare the patient for diagnostic laboratory and radiographic examinations. Should a bounding pulse be accompanied with a rapid or irregular heartbeat, it may be necessary to link the patient to a cardiac monitor for further assessment.
Examine the necessary dietary alterations and fluid limitations for the patient. Highlight the significance of abstaining from alcohol and, if necessary, direct the patient to Alcoholics Anonymous. Emphasize the significance of rest intervals and delineate the signs and symptoms that should be reported.
A bounding pulse may be normal in newborns or children due to the proximity of arteries to the skin surface. It may also arise from patent ductus arteriosus if the left-to-right shunt is substantial.
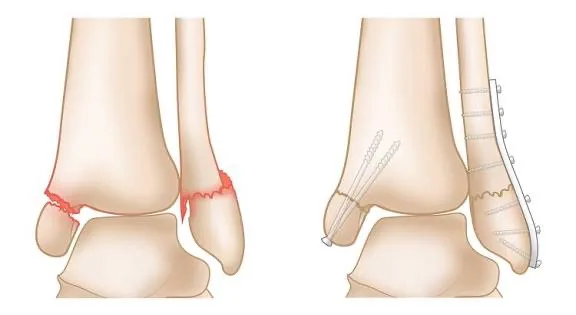
- Published on
Symptoms and Signs -Differential Diagnosis of Psychotic Behavior
Psychotic behavior signifies a failure or refusal to perceive and accept reality and to engage with others. The onset may be abrupt or gradual, evolving from ambiguous symptoms of weariness, insomnia, or headaches to withdrawal, social isolation, and fixation on specific concerns, culminating in significant functional impairment. Multiple behaviors, alone or collectively, may signify psychotic activity. These include delusions, illusions, hallucinations, odd language, and perseveration. Delusions are persistent beliefs that have no basis in reality or in the patient’s knowledge or experience such as delusions of grandeur. Illusions are erroneous interpretations of external sensory stimuli, exemplified by a mirage in the desert.
Conversely, hallucinations are sensory experiences that occur without external stimulation. Unusual language indicates a breakdown in communication. The spectrum includes echolalia (the meaningless repetition of words or phrases), clang association (the repetition of phonetically related words or phrases), and neologisms (the invention and utilization of terms understood solely by the patient). Perseveration, a continual verbal or muscular response, may signify organic brain pathology. Motor alterations encompass inactivity, excessive activity, and repetitive motions.
Medical History and Physical Assessment
Due to the patient's behavior potentially complicating or endangering the acquisition of relevant information, conduct the interview in a tranquil, secure, and adequately illuminated environment. Ensure sufficient personal space to prevent threatening or distressing the patient. Request that he elucidate his issue and the conditions that may have contributed to its emergence. Gather a comprehensive drug history, with particular emphasis on antipsychotic usage, and investigate his consumption of alcohol and other substances, including cocaine, specifying the length and quantity of use. Inquire about recent ailments or incidents. While the patient speaks, observe for cognitive, linguistic, or perceptual anomalies, including delusions. Do ideas and actions appear to align? Observe atypical gestures, posture, walk, vocal tone, and mannerisms. Does the patient appear to be responding to stimuli? For example, is he glancing around the room? Conduct an interview with the patient's family. Which family members does he appear closest to? What is the family's characterization of the patient's relationships, communication dynamics, and role? Has a relative ever been admitted to a hospital for psychiatric or emotional disorders? Ask about the patient’s compliance with his drug schedule. Ultimately, assess the patient's surroundings, educational background, employment history, and socioeconomic situation. Are community services accessible? How does the patient spend his leisure time? Does he possess friends? Has he ever experienced a profound emotional relationship?
Etiological Factors in Medicine
Organic diseases
Multiple biological illnesses, including alcohol withdrawal syndrome, cocaine or amphetamine abuse, brain hypoxia, and nutritional deficiencies, can elicit psychotic behavior.
Endocrine problems, including adrenal failure, and severe infections, such as encephalitis, may also induce psychotic behavior.
Neurologic reasons include Alzheimer’s disease and other dementias. Psychiatric disorders. Psychotic behavior typically manifests in bipolar disorder, personality disorders, schizophrenia, and certain pervasive developmental problems.
Regulating Psychotic Behavior
A patient exhibiting psychotic behavior may experience intense fear and struggle to distinguish between themselves and surroundings. Adhere to these instructions to regulate his conduct and avert harm to the patient, personnel, and others. Remove potentially dangerous things, such as belts or metal utensils, from the patient’s environment. Assist the patient in distinguishing between reality and illusion in a sincere and authentic manner. Be direct, concise, and nonthreatening when communicating to the patient. Engage in straightforward, tangible topics and refrain from theoretical or philosophical discussions. Affirm the patient's accurate impressions of reality while rectifying any misperceptions in a straightforward manner. Never dispute with the patient, but also don’t reinforce his misperceptions. If the patient is apprehensive, remain with him. Only touch the patient to offer reassurance if you have prior experience and are certain it is safe. Relocate the patient to a more secure and less stimulating setting. Deliver individualized care if the patient's conduct is exceedingly peculiar, disruptive to other patients, or poses a danger to himself. Administer suitable medication to the patient. Alternative Causes Pharmaceuticals. Some pharmaceuticals may induce psychotic behavior.
Nevertheless, virtually every medication can elicit psychotic behavior as an uncommon, severe adverse or idiosyncratic response. Surgery. Postoperative delirium and melancholy can induce psychotic behavior. Particular Considerations Consistently assess the patient's awareness of reality. Assist him in forming a perception of reality by addressing him by his chosen name, introducing yourself, elucidating his location, and utilizing timekeeping devices and calendars.
Urge the patient to participate in organized activities. Nonetheless, if he is nonverbal or incoherent, ensure to dedicate attention to him. For example, sit or stroll with him or talk about the day, the season, the weather, or other concrete issues. Refrain from creating time obligations that you cannot fulfill, since this will only distress the patient and lead to further withdrawal. Refer the patient for a mental assessment. Administer an antipsychotic or other medications as required, and prepare him for transfer to a mental health facility if deemed necessary. Do not neglect the patient's physiological requirements. Assess his dietary practices to prevent dehydration and malnutrition, and observe his elimination patterns, particularly if he is on an antipsychotic, which may induce constipation.
Elucidate the significance of organized activities and examine the patient's medications, including proper administration techniques.
In children, psychotic behavior may stem from early infantile autism, symbiotic infantile psychosis, or childhood schizophrenia, all of which can impede language development, abstract reasoning, and sociability. An teenage patient displaying psychotic behavior may have a history of several days of substance use or deprivation of sleep or nutrition, which must be assessed and rectified prior to the initiation of therapy.
Psychotic behavior signifies a failure or refusal to perceive and accept reality and to engage with others. The onset may be abrupt or gradual, evolving from ambiguous symptoms of weariness, insomnia, or headaches to withdrawal, social isolation, and fixation on specific concerns, culminating in significant functional impairment. Multiple behaviors, alone or collectively, may signify psychotic activity. These include delusions, illusions, hallucinations, odd language, and perseveration. Delusions are persistent beliefs that have no basis in reality or in the patient’s knowledge or experience such as delusions of grandeur. Illusions are erroneous interpretations of external sensory stimuli, exemplified by a mirage in the desert.
Conversely, hallucinations are sensory experiences that occur without external stimulation. Unusual language indicates a breakdown in communication. The spectrum includes echolalia (the meaningless repetition of words or phrases), clang association (the repetition of phonetically related words or phrases), and neologisms (the invention and utilization of terms understood solely by the patient). Perseveration, a continual verbal or muscular response, may signify organic brain pathology. Motor alterations encompass inactivity, excessive activity, and repetitive motions.
Medical History and Physical Assessment
Due to the patient's behavior potentially complicating or endangering the acquisition of relevant information, conduct the interview in a tranquil, secure, and adequately illuminated environment. Ensure sufficient personal space to prevent threatening or distressing the patient. Request that he elucidate his issue and the conditions that may have contributed to its emergence. Gather a comprehensive drug history, with particular emphasis on antipsychotic usage, and investigate his consumption of alcohol and other substances, including cocaine, specifying the length and quantity of use. Inquire about recent ailments or incidents. While the patient speaks, observe for cognitive, linguistic, or perceptual anomalies, including delusions. Do ideas and actions appear to align? Observe atypical gestures, posture, walk, vocal tone, and mannerisms. Does the patient appear to be responding to stimuli? For example, is he glancing around the room? Conduct an interview with the patient's family. Which family members does he appear closest to? What is the family's characterization of the patient's relationships, communication dynamics, and role? Has a relative ever been admitted to a hospital for psychiatric or emotional disorders? Ask about the patient’s compliance with his drug schedule. Ultimately, assess the patient's surroundings, educational background, employment history, and socioeconomic situation. Are community services accessible? How does the patient spend his leisure time? Does he possess friends? Has he ever experienced a profound emotional relationship?
Etiological Factors in Medicine
Organic diseases
Multiple biological illnesses, including alcohol withdrawal syndrome, cocaine or amphetamine abuse, brain hypoxia, and nutritional deficiencies, can elicit psychotic behavior.
Endocrine problems, including adrenal failure, and severe infections, such as encephalitis, may also induce psychotic behavior.
Neurologic reasons include Alzheimer’s disease and other dementias. Psychiatric disorders. Psychotic behavior typically manifests in bipolar disorder, personality disorders, schizophrenia, and certain pervasive developmental problems.
Regulating Psychotic Behavior
A patient exhibiting psychotic behavior may experience intense fear and struggle to distinguish between themselves and surroundings. Adhere to these instructions to regulate his conduct and avert harm to the patient, personnel, and others. Remove potentially dangerous things, such as belts or metal utensils, from the patient’s environment. Assist the patient in distinguishing between reality and illusion in a sincere and authentic manner. Be direct, concise, and nonthreatening when communicating to the patient. Engage in straightforward, tangible topics and refrain from theoretical or philosophical discussions. Affirm the patient's accurate impressions of reality while rectifying any misperceptions in a straightforward manner. Never dispute with the patient, but also don’t reinforce his misperceptions. If the patient is apprehensive, remain with him. Only touch the patient to offer reassurance if you have prior experience and are certain it is safe. Relocate the patient to a more secure and less stimulating setting. Deliver individualized care if the patient's conduct is exceedingly peculiar, disruptive to other patients, or poses a danger to himself. Administer suitable medication to the patient. Alternative Causes Pharmaceuticals. Some pharmaceuticals may induce psychotic behavior.
Nevertheless, virtually every medication can elicit psychotic behavior as an uncommon, severe adverse or idiosyncratic response. Surgery. Postoperative delirium and melancholy can induce psychotic behavior. Particular Considerations Consistently assess the patient's awareness of reality. Assist him in forming a perception of reality by addressing him by his chosen name, introducing yourself, elucidating his location, and utilizing timekeeping devices and calendars.
Urge the patient to participate in organized activities. Nonetheless, if he is nonverbal or incoherent, ensure to dedicate attention to him. For example, sit or stroll with him or talk about the day, the season, the weather, or other concrete issues. Refrain from creating time obligations that you cannot fulfill, since this will only distress the patient and lead to further withdrawal. Refer the patient for a mental assessment. Administer an antipsychotic or other medications as required, and prepare him for transfer to a mental health facility if deemed necessary. Do not neglect the patient's physiological requirements. Assess his dietary practices to prevent dehydration and malnutrition, and observe his elimination patterns, particularly if he is on an antipsychotic, which may induce constipation.
Elucidate the significance of organized activities and examine the patient's medications, including proper administration techniques.
In children, psychotic behavior may stem from early infantile autism, symbiotic infantile psychosis, or childhood schizophrenia, all of which can impede language development, abstract reasoning, and sociability. An teenage patient displaying psychotic behavior may have a history of several days of substance use or deprivation of sleep or nutrition, which must be assessed and rectified prior to the initiation of therapy.

- Published on
Symptoms and Signs – Differential Diagnosis of Pruritus
This distressing itching sensation, often eliciting scratching for comfort, impacts the skin, specific mucous membranes, and the eyes. Pruritus is most intense at night and may be aggravated by elevated skin temperature, diminished skin turgor, local vasodilation, dermatoses, and stress. Pruritus, the most prevalent symptom of dermatologic illnesses, may also arise from a local or systemic condition or as a consequence of pharmacological agents. Physiologic pruritus, including pruritic urticarial papules and plaques of pregnancy, may manifest in primigravidas throughout the late third trimester. Pruritus may also arise from emotional distress or exposure to skin irritants.
Medical History and Physical Assessment
Should the patient indicate pruritus, request a detailed account of its start, frequency, and intensity. If pruritus manifests at night, inquire whether it hinders his ability to initiate sleep or disrupts his sleep after he has fallen asleep. Pruritus associated with dermatoses typically inhibits sleep without disrupting it. Is the pruritus localized or generalized? When does it reach its peak severity? What is the duration? Is there a correlation between activities such as physical exercise, bathing, wearing makeup, or the usage of perfumes? Inquire about the patient's skin cleansing regimen.
Specifically, monitor for excessive bathing, abrasive soaps, contact allergies, and extremely hot water. Does he have occupational exposure to recognized skin irritants, such as fiberglass insulation or chemicals? Inquire about the patient's overall health and the medications he is currently taking, as new prescriptions may be questionable. Has he traveled internationally recently? Does he possess any pets? Do any other individuals in the household mention experiencing itching? Do activity, stress, fear, melancholy, or disease appear to exacerbate the itching? Inquire about exposure to skin irritants, prior dermatological conditions, and associated symptoms. Subsequently, acquire a comprehensive drug history. Assess the patient for indicators of scratching, including excoriation, purpura, scabs, scars, or lichenification. Examine initial lesions to assist in confirming dermatoses.
Etiological Factors
Anemia due to iron deficiency
. Iron deficiency anemia may rarely cause pruritus. Anemia, initially asymptomatic, may subsequently lead to exertional dyspnea, tiredness, lethargy, pallor, irritability, headache, tachycardia, diminished muscle tone, and perhaps, murmurs. Chronic anemia results in spoon-shaped nails (koilonychia), brittle nails (cheilosis), fissured corners of the mouth, a smooth tongue (glossitis), and difficulty swallowing (dysphagia).
Cutaneous anthrax.
Anthrax is an acute infectious disease caused by the gram-positive, spore-forming bacteria Bacillus anthracis. It may arise in humans exposed to contaminated animals, infected animal tissue, or biological warfare. Cutaneous anthrax arises when the bacterium infiltrates a cut or abrasion on the skin. The infection initiates as a tiny, painless, or pruritic macular or papular lesion that resembles an insect bite. Within 1 to 2 days, it progresses to a vesicle and subsequently becomes a painless ulcer with a distinctive black, necrotic center. Lymphadenopathy, malaise, headache, or fever may occur.
Conjunctivitis
All types of conjunctivitis induce ocular itching, burning, and discomfort, accompanied by photophobia, conjunctival hyperemia, a sensation of foreign body presence, excessive lacrimation, and a sensation of fullness around the eye. Allergic conjunctivitis can result in a milky redness and a viscous ocular discharge. Bacterial conjunctivitis generally results in intense redness and a mucopurulent discharge that can cause the eyelids to adhere. Fungal conjunctivitis results in a viscous, purulent discharge along with crusting and adhesion of the eyelid. Viral conjunctivitis may result in excessive tearing, minimal discharge, and swelling of the preauricular lymph nodes.
Dermatitis
Various forms of dermatitis may induce pruritus alongside a cutaneous lesion. Atopic dermatitis commences with acute, severe itching and an erythematous rash on dry skin at flexural regions (antecubital fossa, popliteal area, and neck). During a flare-up, scratching may induce edema, scaling, and pustules. Chronic atopic dermatitis can lead to the development of dry, scaly skin characterized by white dermatographia, blanching, and lichenification. Minor irritants and allergens can induce contact dermatitis, characterized by pruritic tiny vesicles that may exude and scale, accompanied by erythema. A severe reaction may result in significant localized edema.
Dermatitis herpetiformis, predominantly observed in males aged 20 to 50, initially manifests as severe pruritus and a stinging sensation. Lesions, symmetrically distributed, develop on the buttocks, shoulders, elbows, and knees between 8 and 12 hours later. Occasionally, they can develop on the neck, face, and scalp. The lesions are characterized as erythematous and may be papular, bullous, or pustular.
Hepatobiliary disorder
Pruritus, a significant diagnostic indicator of liver and gallbladder disease, is frequently associated with jaundice and may be either universal or limited to the palms and soles. Additional characteristics encompass right upper quadrant pain, clay-colored feces, chills, fever, flatulence, belching, a sensation of bloating, epigastric burning, and regurgitation of bitter fluid. Subsequently, liver disease may result in cognitive alterations, ascites, hemorrhagic predispositions, spider angiomas, palmar erythema, xerosis, fetor hepaticus, distended superficial abdominal veins, bilateral gynecomastia, testicular atrophy or menstruation abnormalities, and hepatomegaly.
Herpes zoster
Within 2 to 4 days of experiencing fever and malaise, symptoms such as pruritus, paresthesia or hyperesthesia, and intense, deep pain due to cutaneous nerve involvement manifest on the trunk or extremities in a dermatomal distribution. Within two weeks following the onset of first symptoms, erythematous, nodular cutaneous eruptions manifest in the painful regions and progress to a vesicular stage. Approximately ten days later, the vesicles burst and develop scabs.
Chronic lymphocytic leukemia
Pruritus is a rare manifestation in leukemia. Additional distinctive signs and symptoms encompass fatigue, malaise, widespread lymphadenopathy, fever, hepatomegaly, splenomegaly, weight loss, pallor, hemorrhage, and palpitations.
Lichen simplex chronicus
Continuous friction and abrasion result in localized itching and a defined scaling lesion with distinct borders. Subsequently, the skin becomes thickened and papules develop.
Chronic myringitis
Myringitis causes itching in the afflicted ear, accompanied with purulent discharge and progressive hearing loss. Infestation by lice. Pruritus, a notable symptom, manifests in the region of infestation.
Pediculosis capitis (head lice) can lead to scalp excoriation due to scratching, as well as matted, malodorous, dull hair; occipital and cervical lymphadenopathy; and oval, gray-white nits on hair shafts. Pediculosis corporis (body lice) first results in little red papules, typically located on the shoulders, torso, or buttocks, which may develop into urticarial lesions due to scratching. Subsequently, rashes or wheals may manifest. If left untreated, pediculosis corporis results in dry, discolored, heavily encrusted, scaly skin accompanied by bacterial infection and scars. In extreme instances, it results in cephalalgia, pyrexia, and general discomfort. In cases of pediculosis pubis (pubic lice), scratching frequently results in skin irritation. Nits or adult lice, along with erythematous, pruritic papules, may manifest in pubic hair or in the hair surrounding the anus, abdomen, or thighs.
Pityriasis rosea
Pityriasis rosea may induce mild itching that is exacerbated by hot baths or showers. It typically commences with an erythematous herald patch – a slightly elevated, oval lesion measuring around 2 to 6 cm in diameter. After many days or weeks, scaly yellow-tan or erythematous lesions appear on the trunk and extremities, lasting for 2 to 6 weeks. Sometimes, these lesions are macular, vesicular, or urticarial.
Psoriasis
Pruritus and discomfort are prevalent in psoriasis. This dermatological condition usually initiates with diminutive erythematous papules that expand or merge to create raised red plaques adorned with silvery scales on the scalp, chest, elbows, knees, back, buttocks, and genitalia. Nail pitting may manifest.
Scabies
Scabies generally induces localized pruritus that disrupts the patient's sleep. It may become generalized and endure for up to two weeks post-treatment. Threadlike lesions, many millimeters in length, appear beside a large nodule or red papule.
GENDER INDICATOR
In males, desiccated lesions may develop on the glans penis, penile shaft, and scrotum. In females, lesions may also occur on or near the nipples. In both genders, the lesions have a preference for skin creases. Crusty excoriated lesions develop on the wrists, elbows, axillae, waistline, posterior knees, and ankles. Excoriation due to scratching is prevalent.
Athlete's foot
Tinea pedis is a fungal infection characterized by intense foot pruritus, pain during ambulation, scaling and blistering between the toes, and a dry, scaly squamous inflammation affecting the entire sole. Hives. Severe itching and stinging manifest as temporary, erythematous or pale wheals on the skin or mucous membranes. Prickly feelings usually precede the wheals, which can occur on any body region and may vary in size from pinpoint to palm-sized or greater. Vaginitis. Vaginitis typically results in localized itching and a malodorous vaginal discharge that may be purulent, white or gray, and curd-like. Perineal discomfort and urine impairment may also manifest.
Alternative Causes
HERB NOTIFICATION
Consumption of ginkgo tree fruit pulp may lead to the rapid development of vesicles, causing intense pruritus. Bedbug infestations. Bedbug bites generally elicit itching and burning sensations on the ankles and lower legs, accompanied by clusters of purpuric patches.
Pharmacological hypersensitivity
A minor and localized allergic reaction to medications such as penicillin and sulfonamides may result in itching, erythema, urticarial rash, and edema. Nonetheless, a strong medication reaction may precipitate anaphylaxis.
Administer a topical or oral corticosteroid, an antihistamine, or a sedative, if prescribed. In the absence of localized illness or skin lesions, consider a systemic disease and prepare the patient for a complete blood count and differential, erythrocyte sedimentation rate, protein electrophoresis, and radiologic examinations.
Instruct the patient on methods to manage pruritus. Emphasize the significance of refraining from scratching. Numerous adult illnesses can induce pruritus in children, albeit impacting distinct regions of the body. For example, scabies may impact the scalp in newborns, but not in adults. Pityriasis rosea can impact the facial region, hands, and feet of teenagers. Certain pediatric illnesses, including measles and chickenpox, may induce pruritus.
This distressing itching sensation, often eliciting scratching for comfort, impacts the skin, specific mucous membranes, and the eyes. Pruritus is most intense at night and may be aggravated by elevated skin temperature, diminished skin turgor, local vasodilation, dermatoses, and stress. Pruritus, the most prevalent symptom of dermatologic illnesses, may also arise from a local or systemic condition or as a consequence of pharmacological agents. Physiologic pruritus, including pruritic urticarial papules and plaques of pregnancy, may manifest in primigravidas throughout the late third trimester. Pruritus may also arise from emotional distress or exposure to skin irritants.
Medical History and Physical Assessment
Should the patient indicate pruritus, request a detailed account of its start, frequency, and intensity. If pruritus manifests at night, inquire whether it hinders his ability to initiate sleep or disrupts his sleep after he has fallen asleep. Pruritus associated with dermatoses typically inhibits sleep without disrupting it. Is the pruritus localized or generalized? When does it reach its peak severity? What is the duration? Is there a correlation between activities such as physical exercise, bathing, wearing makeup, or the usage of perfumes? Inquire about the patient's skin cleansing regimen.
Specifically, monitor for excessive bathing, abrasive soaps, contact allergies, and extremely hot water. Does he have occupational exposure to recognized skin irritants, such as fiberglass insulation or chemicals? Inquire about the patient's overall health and the medications he is currently taking, as new prescriptions may be questionable. Has he traveled internationally recently? Does he possess any pets? Do any other individuals in the household mention experiencing itching? Do activity, stress, fear, melancholy, or disease appear to exacerbate the itching? Inquire about exposure to skin irritants, prior dermatological conditions, and associated symptoms. Subsequently, acquire a comprehensive drug history. Assess the patient for indicators of scratching, including excoriation, purpura, scabs, scars, or lichenification. Examine initial lesions to assist in confirming dermatoses.
Etiological Factors
Anemia due to iron deficiency
. Iron deficiency anemia may rarely cause pruritus. Anemia, initially asymptomatic, may subsequently lead to exertional dyspnea, tiredness, lethargy, pallor, irritability, headache, tachycardia, diminished muscle tone, and perhaps, murmurs. Chronic anemia results in spoon-shaped nails (koilonychia), brittle nails (cheilosis), fissured corners of the mouth, a smooth tongue (glossitis), and difficulty swallowing (dysphagia).
Cutaneous anthrax.
Anthrax is an acute infectious disease caused by the gram-positive, spore-forming bacteria Bacillus anthracis. It may arise in humans exposed to contaminated animals, infected animal tissue, or biological warfare. Cutaneous anthrax arises when the bacterium infiltrates a cut or abrasion on the skin. The infection initiates as a tiny, painless, or pruritic macular or papular lesion that resembles an insect bite. Within 1 to 2 days, it progresses to a vesicle and subsequently becomes a painless ulcer with a distinctive black, necrotic center. Lymphadenopathy, malaise, headache, or fever may occur.
Conjunctivitis
All types of conjunctivitis induce ocular itching, burning, and discomfort, accompanied by photophobia, conjunctival hyperemia, a sensation of foreign body presence, excessive lacrimation, and a sensation of fullness around the eye. Allergic conjunctivitis can result in a milky redness and a viscous ocular discharge. Bacterial conjunctivitis generally results in intense redness and a mucopurulent discharge that can cause the eyelids to adhere. Fungal conjunctivitis results in a viscous, purulent discharge along with crusting and adhesion of the eyelid. Viral conjunctivitis may result in excessive tearing, minimal discharge, and swelling of the preauricular lymph nodes.
Dermatitis
Various forms of dermatitis may induce pruritus alongside a cutaneous lesion. Atopic dermatitis commences with acute, severe itching and an erythematous rash on dry skin at flexural regions (antecubital fossa, popliteal area, and neck). During a flare-up, scratching may induce edema, scaling, and pustules. Chronic atopic dermatitis can lead to the development of dry, scaly skin characterized by white dermatographia, blanching, and lichenification. Minor irritants and allergens can induce contact dermatitis, characterized by pruritic tiny vesicles that may exude and scale, accompanied by erythema. A severe reaction may result in significant localized edema.
Dermatitis herpetiformis, predominantly observed in males aged 20 to 50, initially manifests as severe pruritus and a stinging sensation. Lesions, symmetrically distributed, develop on the buttocks, shoulders, elbows, and knees between 8 and 12 hours later. Occasionally, they can develop on the neck, face, and scalp. The lesions are characterized as erythematous and may be papular, bullous, or pustular.
Hepatobiliary disorder
Pruritus, a significant diagnostic indicator of liver and gallbladder disease, is frequently associated with jaundice and may be either universal or limited to the palms and soles. Additional characteristics encompass right upper quadrant pain, clay-colored feces, chills, fever, flatulence, belching, a sensation of bloating, epigastric burning, and regurgitation of bitter fluid. Subsequently, liver disease may result in cognitive alterations, ascites, hemorrhagic predispositions, spider angiomas, palmar erythema, xerosis, fetor hepaticus, distended superficial abdominal veins, bilateral gynecomastia, testicular atrophy or menstruation abnormalities, and hepatomegaly.
Herpes zoster
Within 2 to 4 days of experiencing fever and malaise, symptoms such as pruritus, paresthesia or hyperesthesia, and intense, deep pain due to cutaneous nerve involvement manifest on the trunk or extremities in a dermatomal distribution. Within two weeks following the onset of first symptoms, erythematous, nodular cutaneous eruptions manifest in the painful regions and progress to a vesicular stage. Approximately ten days later, the vesicles burst and develop scabs.
Chronic lymphocytic leukemia
Pruritus is a rare manifestation in leukemia. Additional distinctive signs and symptoms encompass fatigue, malaise, widespread lymphadenopathy, fever, hepatomegaly, splenomegaly, weight loss, pallor, hemorrhage, and palpitations.
Lichen simplex chronicus
Continuous friction and abrasion result in localized itching and a defined scaling lesion with distinct borders. Subsequently, the skin becomes thickened and papules develop.
Chronic myringitis
Myringitis causes itching in the afflicted ear, accompanied with purulent discharge and progressive hearing loss. Infestation by lice. Pruritus, a notable symptom, manifests in the region of infestation.
Pediculosis capitis (head lice) can lead to scalp excoriation due to scratching, as well as matted, malodorous, dull hair; occipital and cervical lymphadenopathy; and oval, gray-white nits on hair shafts. Pediculosis corporis (body lice) first results in little red papules, typically located on the shoulders, torso, or buttocks, which may develop into urticarial lesions due to scratching. Subsequently, rashes or wheals may manifest. If left untreated, pediculosis corporis results in dry, discolored, heavily encrusted, scaly skin accompanied by bacterial infection and scars. In extreme instances, it results in cephalalgia, pyrexia, and general discomfort. In cases of pediculosis pubis (pubic lice), scratching frequently results in skin irritation. Nits or adult lice, along with erythematous, pruritic papules, may manifest in pubic hair or in the hair surrounding the anus, abdomen, or thighs.
Pityriasis rosea
Pityriasis rosea may induce mild itching that is exacerbated by hot baths or showers. It typically commences with an erythematous herald patch – a slightly elevated, oval lesion measuring around 2 to 6 cm in diameter. After many days or weeks, scaly yellow-tan or erythematous lesions appear on the trunk and extremities, lasting for 2 to 6 weeks. Sometimes, these lesions are macular, vesicular, or urticarial.
Psoriasis
Pruritus and discomfort are prevalent in psoriasis. This dermatological condition usually initiates with diminutive erythematous papules that expand or merge to create raised red plaques adorned with silvery scales on the scalp, chest, elbows, knees, back, buttocks, and genitalia. Nail pitting may manifest.
Scabies
Scabies generally induces localized pruritus that disrupts the patient's sleep. It may become generalized and endure for up to two weeks post-treatment. Threadlike lesions, many millimeters in length, appear beside a large nodule or red papule.
GENDER INDICATOR
In males, desiccated lesions may develop on the glans penis, penile shaft, and scrotum. In females, lesions may also occur on or near the nipples. In both genders, the lesions have a preference for skin creases. Crusty excoriated lesions develop on the wrists, elbows, axillae, waistline, posterior knees, and ankles. Excoriation due to scratching is prevalent.
Athlete's foot
Tinea pedis is a fungal infection characterized by intense foot pruritus, pain during ambulation, scaling and blistering between the toes, and a dry, scaly squamous inflammation affecting the entire sole. Hives. Severe itching and stinging manifest as temporary, erythematous or pale wheals on the skin or mucous membranes. Prickly feelings usually precede the wheals, which can occur on any body region and may vary in size from pinpoint to palm-sized or greater. Vaginitis. Vaginitis typically results in localized itching and a malodorous vaginal discharge that may be purulent, white or gray, and curd-like. Perineal discomfort and urine impairment may also manifest.
Alternative Causes
HERB NOTIFICATION
Consumption of ginkgo tree fruit pulp may lead to the rapid development of vesicles, causing intense pruritus. Bedbug infestations. Bedbug bites generally elicit itching and burning sensations on the ankles and lower legs, accompanied by clusters of purpuric patches.
Pharmacological hypersensitivity
A minor and localized allergic reaction to medications such as penicillin and sulfonamides may result in itching, erythema, urticarial rash, and edema. Nonetheless, a strong medication reaction may precipitate anaphylaxis.
Administer a topical or oral corticosteroid, an antihistamine, or a sedative, if prescribed. In the absence of localized illness or skin lesions, consider a systemic disease and prepare the patient for a complete blood count and differential, erythrocyte sedimentation rate, protein electrophoresis, and radiologic examinations.
Instruct the patient on methods to manage pruritus. Emphasize the significance of refraining from scratching. Numerous adult illnesses can induce pruritus in children, albeit impacting distinct regions of the body. For example, scabies may impact the scalp in newborns, but not in adults. Pityriasis rosea can impact the facial region, hands, and feet of teenagers. Certain pediatric illnesses, including measles and chickenpox, may induce pruritus.

- Published on
Symptoms and Signs- Differential Diagnosis of Pericardial Friction Rub
A pericardial friction rub, typically brief, is a scratching, grating, or crunching sound produced when two inflamed layers of the pericardium move against each other. This odd sound, varying from weak to loud, is most audible around the lower left sternal boundary during deep inspiration. This suggests pericarditis, which may arise from an acute infection, a cardiac or renal condition, postpericardiotomy syndrome, or the administration of specific medications. At times, a pericardial friction rub may mimic a murmur or a pleural friction rub. The basic pericardial friction rub comprises three components.
Medical History and Physical Assessment Acquire a comprehensive medical history, with particular emphasis on heart problems. Has the patient recently experienced a myocardial infarction or undergone heart surgery? Has he ever experienced pericarditis or a rheumatic condition, such as rheumatoid arthritis or systemic lupus erythematosus? Does he have chronic kidney disease or an infection? Should the patient report chest pain, inquire about its characteristics and location. What alleviates the discomfort? What exacerbates it? Assess the patient's vital signs, with particular attention to hypotension, tachycardia, an irregular pulse, tachypnea, and fever. Examine for jugular vein distention, edema, ascites, and hepatomegaly. Perform auscultation of the lungs to detect crackles.
EXAMINATION TIP: Pericardial Friction Rub vs Murmur Is the auditory phenomenon a pericardial friction rub or a murmur? This is how to determine. The traditional pericardial friction rub comprises three auditory components, according to the periods of the heart cycle. In certain cases, the presystolic and early diastolic sounds of the rub may be imperceptible, leading to a resemblance to the murmurs associated with mitral insufficiency or aortic stenosis and insufficiency. To differentiate a pericardial friction rub from a murmur in the absence of the traditional three-component sound, re-auscultate and consider the following questions:
WHAT IS THE DEPTH OF THE SOUND?
A pericardial friction rub typically has a surface sound, but a murmur has a deeper resonance in the chest. Does the sound propagate? A pericardial friction rub typically does not radiate, although a murmur may radiate extensively. Does the sound fluctuate with inspiration or alterations in patient position? A pericardial friction rub is typically most pronounced during inhalation and is optimally detected when the patient assumes a forward-leaning position. A murmur fluctuates in timing and duration with both variables.
Etiological Factors
Pericarditis
A pericardial friction rub is the defining characteristic of acute pericarditis. This condition induces acute precordial or retrosternal discomfort that typically radiates to the left shoulder, neck, and back. The pain intensifies when heavy breathing, coughing, lying flat, and potentially while swallowing. It diminishes as he assumes an upright position and leans forward. The patient may additionally have fever, dyspnea, tachycardia, and arrhythmias.
Contrasting Auscultation Results During auscultation, one may identify a pleural friction rub, a pericardial friction rub, or crackles—three aberrant noises frequently conflated. Utilize these pictures to elucidate auscultation findings.
EXAMINATION TIP: Comprehending Pericardial Friction Rubs The basic pericardial friction rub is characterized by three distinct phases. The three auditory components are associated with periods of the cardiac cycle. The presystolic component (A) signifies atrial systole and occurs before to the first heart sound (S1). The systolic component (B), typically the most pronounced, signifies ventricular systole and transpires between the first heart sound (S1) and the second heart sound (S2). The early diastolic component (C) signifies ventricular diastole and occurs subsequent to S2. Occasionally, the early diastolic component coalesces with the presystolic component, resulting in a diphasic to-and-fro sound during auscultation. Auscultation in some patients may reveal only a single component—a monophasic rub, usually occurring during ventricular systole.
Chronic constrictive pericarditis leads to the gradual development of a pericardial friction rub, accompanied by manifestations of reduced cardiac filling and output, including peripheral edema, ascites, Kussmaul's sign (jugular vein distention on inspiration), and hepatomegaly. Dyspnea, orthopnea, paradoxical pulse, and thoracic discomfort may also manifest.
Additional Factors: Substances. Procainamide and chemotherapy agents may induce pericarditis.
Persist in observing the patient's cardiovascular condition. Should the pericardial friction rub cease, remain vigilant for indications of cardiac tamponade: pallor; cool, clammy skin; hypotension; tachycardia; tachypnea; paradoxical pulse; and heightened jugular vein distention. Should these indications manifest, prepare the patient for pericardiocentesis to avert cardiovascular collapse. Ensure the patient receives sufficient rest.
Administer an anti-inflammatory, antiarrhythmic, diuretic, or antibiotic to address the underlying etiology. If required, ready him for a pericardiectomy to facilitate optimal heart filling and contraction.
Elucidate the fundamental problem, its therapeutic interventions, and the measures the patient might undertake to alleviate his symptoms. Pediatric Guidelines Bacterial pericarditis can manifest within the initial two decades of life, typically prior to the age of 6. A pericardial friction rub may manifest, although additional signs and symptoms—such as fever, tachycardia, dyspnea, chest discomfort, jugular vein distention, and hepatomegaly—more consistently signify this life-threatening condition. A pericardial friction rub may also manifest following surgery to rectify congenital heart abnormalities. Nevertheless, it typically dissipates without the onset of pericarditis.
A pericardial friction rub, typically brief, is a scratching, grating, or crunching sound produced when two inflamed layers of the pericardium move against each other. This odd sound, varying from weak to loud, is most audible around the lower left sternal boundary during deep inspiration. This suggests pericarditis, which may arise from an acute infection, a cardiac or renal condition, postpericardiotomy syndrome, or the administration of specific medications. At times, a pericardial friction rub may mimic a murmur or a pleural friction rub. The basic pericardial friction rub comprises three components.
Medical History and Physical Assessment Acquire a comprehensive medical history, with particular emphasis on heart problems. Has the patient recently experienced a myocardial infarction or undergone heart surgery? Has he ever experienced pericarditis or a rheumatic condition, such as rheumatoid arthritis or systemic lupus erythematosus? Does he have chronic kidney disease or an infection? Should the patient report chest pain, inquire about its characteristics and location. What alleviates the discomfort? What exacerbates it? Assess the patient's vital signs, with particular attention to hypotension, tachycardia, an irregular pulse, tachypnea, and fever. Examine for jugular vein distention, edema, ascites, and hepatomegaly. Perform auscultation of the lungs to detect crackles.
EXAMINATION TIP: Pericardial Friction Rub vs Murmur Is the auditory phenomenon a pericardial friction rub or a murmur? This is how to determine. The traditional pericardial friction rub comprises three auditory components, according to the periods of the heart cycle. In certain cases, the presystolic and early diastolic sounds of the rub may be imperceptible, leading to a resemblance to the murmurs associated with mitral insufficiency or aortic stenosis and insufficiency. To differentiate a pericardial friction rub from a murmur in the absence of the traditional three-component sound, re-auscultate and consider the following questions:
WHAT IS THE DEPTH OF THE SOUND?
A pericardial friction rub typically has a surface sound, but a murmur has a deeper resonance in the chest. Does the sound propagate? A pericardial friction rub typically does not radiate, although a murmur may radiate extensively. Does the sound fluctuate with inspiration or alterations in patient position? A pericardial friction rub is typically most pronounced during inhalation and is optimally detected when the patient assumes a forward-leaning position. A murmur fluctuates in timing and duration with both variables.
Etiological Factors
Pericarditis
A pericardial friction rub is the defining characteristic of acute pericarditis. This condition induces acute precordial or retrosternal discomfort that typically radiates to the left shoulder, neck, and back. The pain intensifies when heavy breathing, coughing, lying flat, and potentially while swallowing. It diminishes as he assumes an upright position and leans forward. The patient may additionally have fever, dyspnea, tachycardia, and arrhythmias.
Contrasting Auscultation Results During auscultation, one may identify a pleural friction rub, a pericardial friction rub, or crackles—three aberrant noises frequently conflated. Utilize these pictures to elucidate auscultation findings.
EXAMINATION TIP: Comprehending Pericardial Friction Rubs The basic pericardial friction rub is characterized by three distinct phases. The three auditory components are associated with periods of the cardiac cycle. The presystolic component (A) signifies atrial systole and occurs before to the first heart sound (S1). The systolic component (B), typically the most pronounced, signifies ventricular systole and transpires between the first heart sound (S1) and the second heart sound (S2). The early diastolic component (C) signifies ventricular diastole and occurs subsequent to S2. Occasionally, the early diastolic component coalesces with the presystolic component, resulting in a diphasic to-and-fro sound during auscultation. Auscultation in some patients may reveal only a single component—a monophasic rub, usually occurring during ventricular systole.
Chronic constrictive pericarditis leads to the gradual development of a pericardial friction rub, accompanied by manifestations of reduced cardiac filling and output, including peripheral edema, ascites, Kussmaul's sign (jugular vein distention on inspiration), and hepatomegaly. Dyspnea, orthopnea, paradoxical pulse, and thoracic discomfort may also manifest.
Additional Factors: Substances. Procainamide and chemotherapy agents may induce pericarditis.
Persist in observing the patient's cardiovascular condition. Should the pericardial friction rub cease, remain vigilant for indications of cardiac tamponade: pallor; cool, clammy skin; hypotension; tachycardia; tachypnea; paradoxical pulse; and heightened jugular vein distention. Should these indications manifest, prepare the patient for pericardiocentesis to avert cardiovascular collapse. Ensure the patient receives sufficient rest.
Administer an anti-inflammatory, antiarrhythmic, diuretic, or antibiotic to address the underlying etiology. If required, ready him for a pericardiectomy to facilitate optimal heart filling and contraction.
Elucidate the fundamental problem, its therapeutic interventions, and the measures the patient might undertake to alleviate his symptoms. Pediatric Guidelines Bacterial pericarditis can manifest within the initial two decades of life, typically prior to the age of 6. A pericardial friction rub may manifest, although additional signs and symptoms—such as fever, tachycardia, dyspnea, chest discomfort, jugular vein distention, and hepatomegaly—more consistently signify this life-threatening condition. A pericardial friction rub may also manifest following surgery to rectify congenital heart abnormalities. Nevertheless, it typically dissipates without the onset of pericarditis.

