- Published on
Emergency and Acute Medicine – Patent Ductus Arteriosus
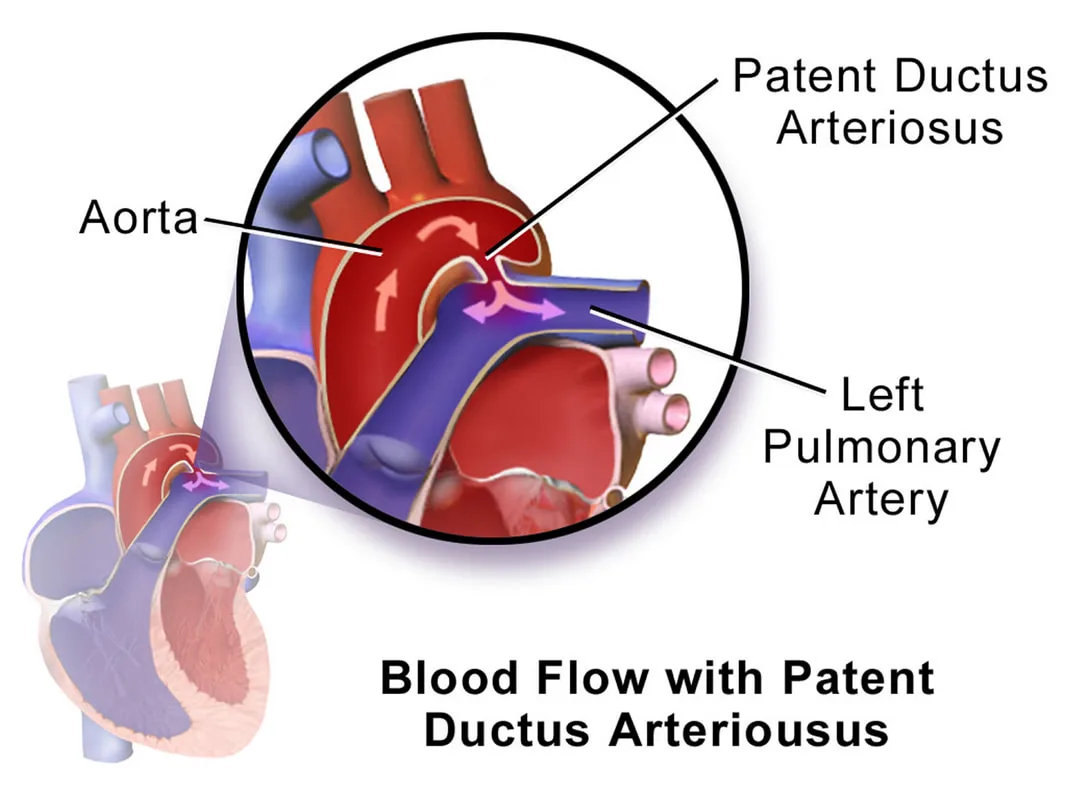
Patent ductus arteriosus (PDA) is a condition in which the fetal vessel connecting the pulmonary trunk to the descending aorta fails to close after birth. Normally, shortly after delivery, increased oxygen tension and changes in prostaglandin metabolism lead to ductal constriction, closure, and eventual fibrosis. In preterm infants, persistent patency may represent a physiologic and sometimes life-saving response related to hypoxia and immaturity. In contrast, persistence of the ductus in full-term infants represents a true congenital malformation due to structural deficiencies of the ductal wall.
As pulmonary vascular resistance falls after birth, blood is shunted from the aorta into the pulmonary artery, producing a left-to-right shunt. The magnitude of shunting depends on ductal size and the relative pulmonary and systemic vascular resistances, and in severe cases up to 70% of left ventricular output may pass through the ductus. Risk factors include prematurity, hypoxic conditions, high altitude, maternal rubella infection, and coexisting congenital heart disease, with a female predominance.
Clinical presentation varies with ductal size. Small PDAs may be asymptomatic, whereas larger shunts can lead to congestive heart failure, often within the first days of life. Typical findings include wide pulse pressure, a prominent apical impulse, a palpable thrill, and a characteristic continuous “machinery” murmur best heard at the second left intercostal space and radiating along the left sternal border. Additional features may include recurrent pulmonary infections and failure to thrive.
Diagnosis is primarily established through imaging. Chest radiography may be normal in infants but can show increased pulmonary vascular markings, cardiac chamber enlargement, and dilated great vessels in older patients. Electrocardiography may reveal left ventricular hypertrophy, with right ventricular hypertrophy indicating more severe disease. Echocardiography with Doppler is the diagnostic modality of choice, allowing visualization of ductal size, left atrial enlargement, and continuous aortic-to-pulmonary flow. Cardiac catheterization confirms shunting when needed and may be used therapeutically.
Management depends on patient age, symptoms, and ductal significance. Small, asymptomatic PDAs may be observed. In preterm infants, pharmacologic closure with prostaglandin synthesis inhibitors such as indomethacin is often effective during the first week of life. Full-term infants and children generally require definitive closure, as spontaneous resolution is rare; options include surgical ligation or transcatheter occlusion techniques. Supportive care includes oxygen for heart failure, fluid and sodium restriction, correction of anemia, and endocarditis prophylaxis when indicated.
Admission is required for patients with heart failure, pulmonary hypertension, or suspected endocarditis. Asymptomatic patients may be discharged with close cardiology follow-up and plans for elective closure. Key clinical points include recognition that heart failure may reduce renal perfusion and urine output, and that indomethacin therapy carries risks such as gastrointestinal bleeding.
Patent ductus arteriosus (PDA) is a condition in which the fetal vessel connecting the pulmonary trunk to the descending aorta fails to close after birth. Normally, shortly after delivery, increased oxygen tension and changes in prostaglandin metabolism lead to ductal constriction, closure, and eventual fibrosis. In preterm infants, persistent patency may represent a physiologic and sometimes life-saving response related to hypoxia and immaturity. In contrast, persistence of the ductus in full-term infants represents a true congenital malformation due to structural deficiencies of the ductal wall.
As pulmonary vascular resistance falls after birth, blood is shunted from the aorta into the pulmonary artery, producing a left-to-right shunt. The magnitude of shunting depends on ductal size and the relative pulmonary and systemic vascular resistances, and in severe cases up to 70% of left ventricular output may pass through the ductus. Risk factors include prematurity, hypoxic conditions, high altitude, maternal rubella infection, and coexisting congenital heart disease, with a female predominance.
Clinical presentation varies with ductal size. Small PDAs may be asymptomatic, whereas larger shunts can lead to congestive heart failure, often within the first days of life. Typical findings include wide pulse pressure, a prominent apical impulse, a palpable thrill, and a characteristic continuous “machinery” murmur best heard at the second left intercostal space and radiating along the left sternal border. Additional features may include recurrent pulmonary infections and failure to thrive.
Diagnosis is primarily established through imaging. Chest radiography may be normal in infants but can show increased pulmonary vascular markings, cardiac chamber enlargement, and dilated great vessels in older patients. Electrocardiography may reveal left ventricular hypertrophy, with right ventricular hypertrophy indicating more severe disease. Echocardiography with Doppler is the diagnostic modality of choice, allowing visualization of ductal size, left atrial enlargement, and continuous aortic-to-pulmonary flow. Cardiac catheterization confirms shunting when needed and may be used therapeutically.
Management depends on patient age, symptoms, and ductal significance. Small, asymptomatic PDAs may be observed. In preterm infants, pharmacologic closure with prostaglandin synthesis inhibitors such as indomethacin is often effective during the first week of life. Full-term infants and children generally require definitive closure, as spontaneous resolution is rare; options include surgical ligation or transcatheter occlusion techniques. Supportive care includes oxygen for heart failure, fluid and sodium restriction, correction of anemia, and endocarditis prophylaxis when indicated.
Admission is required for patients with heart failure, pulmonary hypertension, or suspected endocarditis. Asymptomatic patients may be discharged with close cardiology follow-up and plans for elective closure. Key clinical points include recognition that heart failure may reduce renal perfusion and urine output, and that indomethacin therapy carries risks such as gastrointestinal bleeding.
- Published on
Emergency and Acute Medicine – Patellar Injuries
Patellar injuries encompass a spectrum of conditions involving the patella and its associated extensor mechanism, including patellar dislocation, patellar fracture, patellar tendon rupture, and patellar tendinitis. These injuries commonly result from traumatic forces, sudden deceleration, or repetitive overuse and are frequently encountered in athletic and emergency settings. Accurate recognition is essential, as management ranges from conservative treatment to urgent surgical intervention.
Patellar dislocation most often occurs due to sudden knee flexion combined with external rotation of the tibia on the femur, accompanied by a strong contraction of the quadriceps muscle. Lateral dislocation is by far the most common type, with the patella displaced over the lateral femoral condyle. Direct trauma to the patella is a less frequent cause. Risk factors include genu valgum, patella alta, shallow femoral trochlea, weak vastus medialis, pes planus, and structural abnormalities of the patella. Dislocations are particularly common in adolescent athletes, especially females, and younger age at first dislocation is associated with higher recurrence rates.
Patients with patellar dislocation typically report a sensation of the knee “giving way,” often accompanied by a popping or tearing feeling, immediate pain, swelling, and difficulty bearing weight. On examination, there may be an obvious lateral deformity of the patella, although spontaneous reduction frequently occurs before ED evaluation. Tenderness along the patella and a positive apprehension test (Fairbanks sign) are characteristic findings.
Patellar fractures are most commonly caused by direct trauma such as a fall or direct blow to the knee, often resulting in comminuted or minimally displaced fractures. Indirect mechanisms involve excessive tension through the extensor mechanism, leading to transverse or displaced fractures. Transverse fractures account for the majority of cases, followed by comminuted, longitudinal, and osteochondral fractures. Patients present with anterior knee pain, swelling, hemarthrosis, difficulty ambulating, and impaired knee extension. Palpable defects or crepitus may be present.
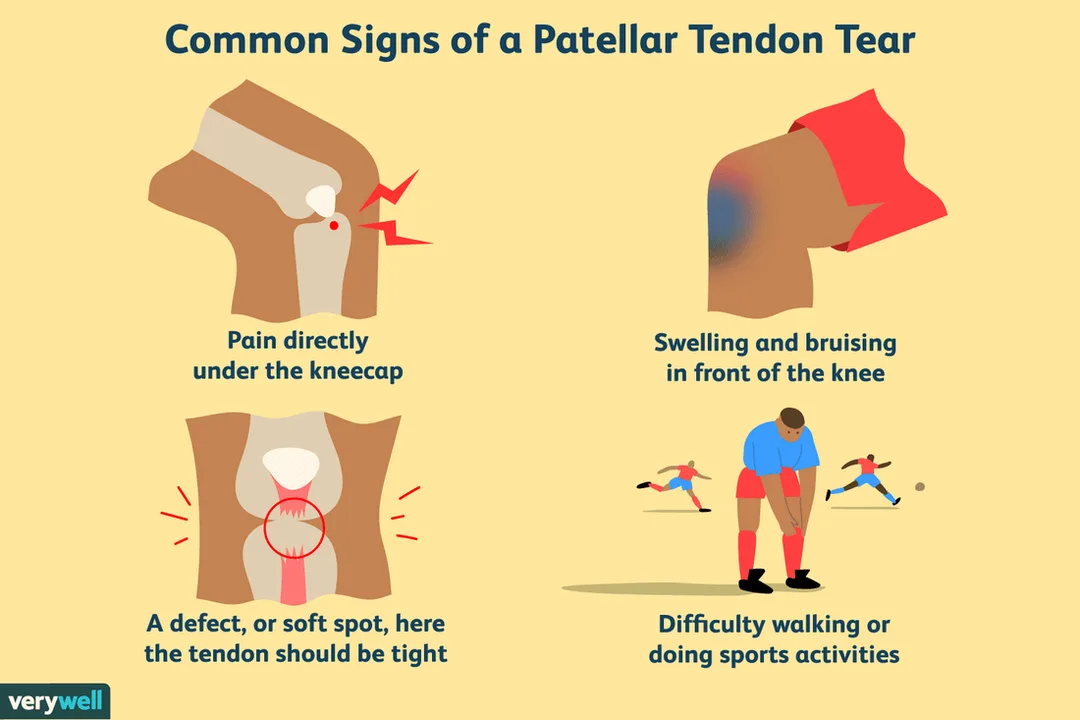
Patellar tendon rupture usually results from a forceful eccentric contraction of the quadriceps on a flexed knee, such as during landing from a jump or heavy lifting. It occurs more often in older athletes and in patients with predisposing conditions such as chronic patellar tendinitis, diabetes mellitus, inflammatory arthropathies, prior steroid injections, or previous knee surgery. Clinically, patients experience abrupt severe pain, inability to maintain knee extension, and a high-riding patella on examination or imaging.
Patellar tendinitis, also known as “jumper’s knee,” is an overuse injury caused by repetitive microtrauma from activities involving frequent jumping or rapid acceleration and deceleration. It is common in volleyball players, basketball players, runners, and high jumpers. Patients typically report localized pain at the inferior pole of the patella or proximal patellar tendon that worsens with stair climbing or rising from a seated position.
Radiographic evaluation is essential in suspected patellar injuries. Standard anteroposterior, lateral, and sunrise (axial) views of the knee should be obtained. In patellar dislocations, postreduction radiographs are important to exclude associated osteochondral fractures. A bipartite patella may mimic fracture and should be distinguished with comparison views if needed. In patellar tendon rupture, imaging may reveal a superiorly displaced patella. Radiographs are often normal in early patellar tendinitis.
Management depends on the specific injury. Simple lateral patellar dislocations are typically reduced by gentle knee extension, sometimes with medial pressure on the patella. Procedural analgesia or sedation may be required. Other dislocation types (superior, medial, or intra-articular) should not be reduced in the ED and require orthopedic consultation. Patellar fractures warrant orthopedic evaluation; nondisplaced fractures with intact extensor function may be treated nonoperatively with immobilization, while displaced or open fractures require surgical management. Patellar tendon rupture requires early orthopedic consultation and surgical repair, typically within two to six weeks. Patellar tendinitis is managed conservatively with rest, activity modification, NSAIDs, and physical therapy.
Patients with successfully reduced lateral patellar dislocations and normal postreduction imaging may be discharged with a knee immobilizer, crutches, and close orthopedic follow-up. Admission is indicated for irreducible dislocations, associated fractures, open injuries, or compromised extensor mechanism. Important clinical pearls include recognizing that patellar dislocations may spontaneously reduce prior to evaluation and that swelling may obscure a palpable defect in patellar tendon rupture.
Patellar injuries encompass a spectrum of conditions involving the patella and its associated extensor mechanism, including patellar dislocation, patellar fracture, patellar tendon rupture, and patellar tendinitis. These injuries commonly result from traumatic forces, sudden deceleration, or repetitive overuse and are frequently encountered in athletic and emergency settings. Accurate recognition is essential, as management ranges from conservative treatment to urgent surgical intervention.
Patellar dislocation most often occurs due to sudden knee flexion combined with external rotation of the tibia on the femur, accompanied by a strong contraction of the quadriceps muscle. Lateral dislocation is by far the most common type, with the patella displaced over the lateral femoral condyle. Direct trauma to the patella is a less frequent cause. Risk factors include genu valgum, patella alta, shallow femoral trochlea, weak vastus medialis, pes planus, and structural abnormalities of the patella. Dislocations are particularly common in adolescent athletes, especially females, and younger age at first dislocation is associated with higher recurrence rates.
Patients with patellar dislocation typically report a sensation of the knee “giving way,” often accompanied by a popping or tearing feeling, immediate pain, swelling, and difficulty bearing weight. On examination, there may be an obvious lateral deformity of the patella, although spontaneous reduction frequently occurs before ED evaluation. Tenderness along the patella and a positive apprehension test (Fairbanks sign) are characteristic findings.
Patellar fractures are most commonly caused by direct trauma such as a fall or direct blow to the knee, often resulting in comminuted or minimally displaced fractures. Indirect mechanisms involve excessive tension through the extensor mechanism, leading to transverse or displaced fractures. Transverse fractures account for the majority of cases, followed by comminuted, longitudinal, and osteochondral fractures. Patients present with anterior knee pain, swelling, hemarthrosis, difficulty ambulating, and impaired knee extension. Palpable defects or crepitus may be present.
Patellar tendon rupture usually results from a forceful eccentric contraction of the quadriceps on a flexed knee, such as during landing from a jump or heavy lifting. It occurs more often in older athletes and in patients with predisposing conditions such as chronic patellar tendinitis, diabetes mellitus, inflammatory arthropathies, prior steroid injections, or previous knee surgery. Clinically, patients experience abrupt severe pain, inability to maintain knee extension, and a high-riding patella on examination or imaging.
Patellar tendinitis, also known as “jumper’s knee,” is an overuse injury caused by repetitive microtrauma from activities involving frequent jumping or rapid acceleration and deceleration. It is common in volleyball players, basketball players, runners, and high jumpers. Patients typically report localized pain at the inferior pole of the patella or proximal patellar tendon that worsens with stair climbing or rising from a seated position.
Radiographic evaluation is essential in suspected patellar injuries. Standard anteroposterior, lateral, and sunrise (axial) views of the knee should be obtained. In patellar dislocations, postreduction radiographs are important to exclude associated osteochondral fractures. A bipartite patella may mimic fracture and should be distinguished with comparison views if needed. In patellar tendon rupture, imaging may reveal a superiorly displaced patella. Radiographs are often normal in early patellar tendinitis.
Management depends on the specific injury. Simple lateral patellar dislocations are typically reduced by gentle knee extension, sometimes with medial pressure on the patella. Procedural analgesia or sedation may be required. Other dislocation types (superior, medial, or intra-articular) should not be reduced in the ED and require orthopedic consultation. Patellar fractures warrant orthopedic evaluation; nondisplaced fractures with intact extensor function may be treated nonoperatively with immobilization, while displaced or open fractures require surgical management. Patellar tendon rupture requires early orthopedic consultation and surgical repair, typically within two to six weeks. Patellar tendinitis is managed conservatively with rest, activity modification, NSAIDs, and physical therapy.
Patients with successfully reduced lateral patellar dislocations and normal postreduction imaging may be discharged with a knee immobilizer, crutches, and close orthopedic follow-up. Admission is indicated for irreducible dislocations, associated fractures, open injuries, or compromised extensor mechanism. Important clinical pearls include recognizing that patellar dislocations may spontaneously reduce prior to evaluation and that swelling may obscure a palpable defect in patellar tendon rupture.
- Published on
Emergency and Acute Medicine – Paronychia
Paronychia is an inflammatory condition of the nail folds surrounding the nail plate that occurs when disruption of the protective seal between the nail plate and nail fold allows microorganisms to enter the eponychial space. This disruption commonly follows minor trauma and leads to localized infection and inflammation.
The etiology differs between acute and chronic paronychia. Acute paronychia is most commonly caused by *Staphylococcus aureus*, although streptococci, *Pseudomonas*, and anaerobic organisms may also be involved. Chronic paronychia is multifactorial and results from repeated exposure to allergens and irritants, with fungal organisms—most commonly *Candida albicans*—frequently coexisting alongside *Staphylococcus* species.
Clinically, paronychia presents with pain, warmth, swelling, and erythema of the proximal or lateral nail folds, usually developing two to five days after trauma. For symptoms to meet criteria for chronic paronychia, they must persist for more than six weeks. A careful history is important. Acute paronychia is often associated with nail biting, finger sucking, aggressive manicuring, or direct trauma. Chronic paronychia is commonly seen in individuals with occupations involving persistent moisture exposure, such as dishwashers or bartenders, and occurs more frequently in patients with diabetes or peripheral vascular disease. In children, infections often involve anaerobic oral flora due to nail biting.
On physical examination, early paronychia begins as localized erythema, swelling, and tenderness at the dorsolateral nail fold, which may bulge over the nail plate. As the condition progresses, a subcuticular or subungual abscess may form. Green discoloration of the nail suggests *Pseudomonas* infection, while nail plate hypertrophy raises concern for a fungal etiology.
The diagnosis of paronychia is primarily clinical and based on history and physical examination. Evaluation should include assessment for associated infections such as felon or cellulitis and confirmation of tetanus immunization status. Laboratory testing is generally not helpful, and cultures are not routinely indicated. If herpetic whitlow is suspected, a Tzanck smear or viral culture may be considered. Imaging with soft tissue radiographs is reserved for suspected foreign bodies or possible osteomyelitis. A digital pressure test, using opposing pressure between the thumb and affected finger, may help identify early subungual abscess formation.
Management depends on the stage and type of paronychia. Early acute paronychia without purulence can often be treated with warm-water soaks four times daily, with or without topical antibiotics or corticosteroids. If a superficial abscess is present, elevation of the eponychial fold using a small blade or needle may allow adequate drainage; local anesthesia or a digital nerve block may be required. When infection extends beneath the nail plate, partial nail removal may be necessary, while extensive subungual abscesses may require complete nail removal. Runaround abscesses involving both sides of the nail fold require partial proximal nail removal with packing to prevent re-adhesion.
Antibiotic therapy is recommended when there is cellulitis, abscess formation, or systemic signs of infection. Appropriate first-line oral agents include trimethoprim–sulfamethoxazole, dicloxacillin, or amoxicillin–clavulanate, typically for five to ten days depending on severity. Clindamycin or amoxicillin–clavulanate is preferred when infection is associated with nail biting or oral exposure. Chronic paronychia management focuses on avoidance of irritants and moisture, with topical corticosteroids considered first-line therapy, often combined with a broad-spectrum topical antifungal. Refractory cases may require surgical eponychial marsupialization or oral antifungal therapy.
Admission is rarely required for paronychia alone. Patients with uncomplicated infections may be discharged with appropriate wound care instructions and follow-up. Those with packing in place should be re-evaluated within 24 hours. Referral is indicated for chronic or recurrent paronychia that does not respond to standard therapy.
Key clinical pearls include recognizing that acute paronychia generally responds well to timely drainage with or without antibiotics, while chronic paronychia is usually driven by repeated exposure to irritants rather than infection alone. Conditions such as psoriasis, Reiter syndrome, and herpetic whitlow can mimic paronychia and should be considered in recurrent or atypical cases.
Paronychia is an inflammatory condition of the nail folds surrounding the nail plate that occurs when disruption of the protective seal between the nail plate and nail fold allows microorganisms to enter the eponychial space. This disruption commonly follows minor trauma and leads to localized infection and inflammation.
The etiology differs between acute and chronic paronychia. Acute paronychia is most commonly caused by *Staphylococcus aureus*, although streptococci, *Pseudomonas*, and anaerobic organisms may also be involved. Chronic paronychia is multifactorial and results from repeated exposure to allergens and irritants, with fungal organisms—most commonly *Candida albicans*—frequently coexisting alongside *Staphylococcus* species.
Clinically, paronychia presents with pain, warmth, swelling, and erythema of the proximal or lateral nail folds, usually developing two to five days after trauma. For symptoms to meet criteria for chronic paronychia, they must persist for more than six weeks. A careful history is important. Acute paronychia is often associated with nail biting, finger sucking, aggressive manicuring, or direct trauma. Chronic paronychia is commonly seen in individuals with occupations involving persistent moisture exposure, such as dishwashers or bartenders, and occurs more frequently in patients with diabetes or peripheral vascular disease. In children, infections often involve anaerobic oral flora due to nail biting.
On physical examination, early paronychia begins as localized erythema, swelling, and tenderness at the dorsolateral nail fold, which may bulge over the nail plate. As the condition progresses, a subcuticular or subungual abscess may form. Green discoloration of the nail suggests *Pseudomonas* infection, while nail plate hypertrophy raises concern for a fungal etiology.
The diagnosis of paronychia is primarily clinical and based on history and physical examination. Evaluation should include assessment for associated infections such as felon or cellulitis and confirmation of tetanus immunization status. Laboratory testing is generally not helpful, and cultures are not routinely indicated. If herpetic whitlow is suspected, a Tzanck smear or viral culture may be considered. Imaging with soft tissue radiographs is reserved for suspected foreign bodies or possible osteomyelitis. A digital pressure test, using opposing pressure between the thumb and affected finger, may help identify early subungual abscess formation.
Management depends on the stage and type of paronychia. Early acute paronychia without purulence can often be treated with warm-water soaks four times daily, with or without topical antibiotics or corticosteroids. If a superficial abscess is present, elevation of the eponychial fold using a small blade or needle may allow adequate drainage; local anesthesia or a digital nerve block may be required. When infection extends beneath the nail plate, partial nail removal may be necessary, while extensive subungual abscesses may require complete nail removal. Runaround abscesses involving both sides of the nail fold require partial proximal nail removal with packing to prevent re-adhesion.
Antibiotic therapy is recommended when there is cellulitis, abscess formation, or systemic signs of infection. Appropriate first-line oral agents include trimethoprim–sulfamethoxazole, dicloxacillin, or amoxicillin–clavulanate, typically for five to ten days depending on severity. Clindamycin or amoxicillin–clavulanate is preferred when infection is associated with nail biting or oral exposure. Chronic paronychia management focuses on avoidance of irritants and moisture, with topical corticosteroids considered first-line therapy, often combined with a broad-spectrum topical antifungal. Refractory cases may require surgical eponychial marsupialization or oral antifungal therapy.
Admission is rarely required for paronychia alone. Patients with uncomplicated infections may be discharged with appropriate wound care instructions and follow-up. Those with packing in place should be re-evaluated within 24 hours. Referral is indicated for chronic or recurrent paronychia that does not respond to standard therapy.
Key clinical pearls include recognizing that acute paronychia generally responds well to timely drainage with or without antibiotics, while chronic paronychia is usually driven by repeated exposure to irritants rather than infection alone. Conditions such as psoriasis, Reiter syndrome, and herpetic whitlow can mimic paronychia and should be considered in recurrent or atypical cases.

- Published on
Emergency and Acute Medicine – Parkinson Disease
Parkinson disease (PD) is a gradually progressive neurodegenerative disorder that typically affects individuals in middle or late life. It is characterized by degeneration of dopaminergic neurons in the substantia nigra, formation of Lewy bodies in remaining neurons, and accelerated cortical atrophy. Although symptoms often begin unilaterally, the disease usually progresses to symmetric involvement. Parkinson disease affects approximately 1% of people over 60 years of age and up to 4% of those over 80. Importantly, nonspecific symptoms such as fatigue, constipation, and hyposmia may precede the diagnosis by many years, sometimes up to two decades.
The etiology of Parkinson disease is most often sporadic or idiopathic. However, several other conditions can present with parkinsonism and must be considered, especially in the emergency setting. These include drug-induced causes such as neuroleptics and sudden withdrawal of dopaminergic medications leading to parkinsonism–hyperpyrexia syndrome, as well as exposure to toxins like carbon monoxide, methanol, cyanide, organophosphates, and MPTP. Structural brain lesions involving the basal ganglia or midbrain, hydrocephalus, infections such as viral encephalitis or Mycoplasma, and other neurologic conditions like central pontine myelinolysis and encephalitis lethargica can also produce parkinsonian features.
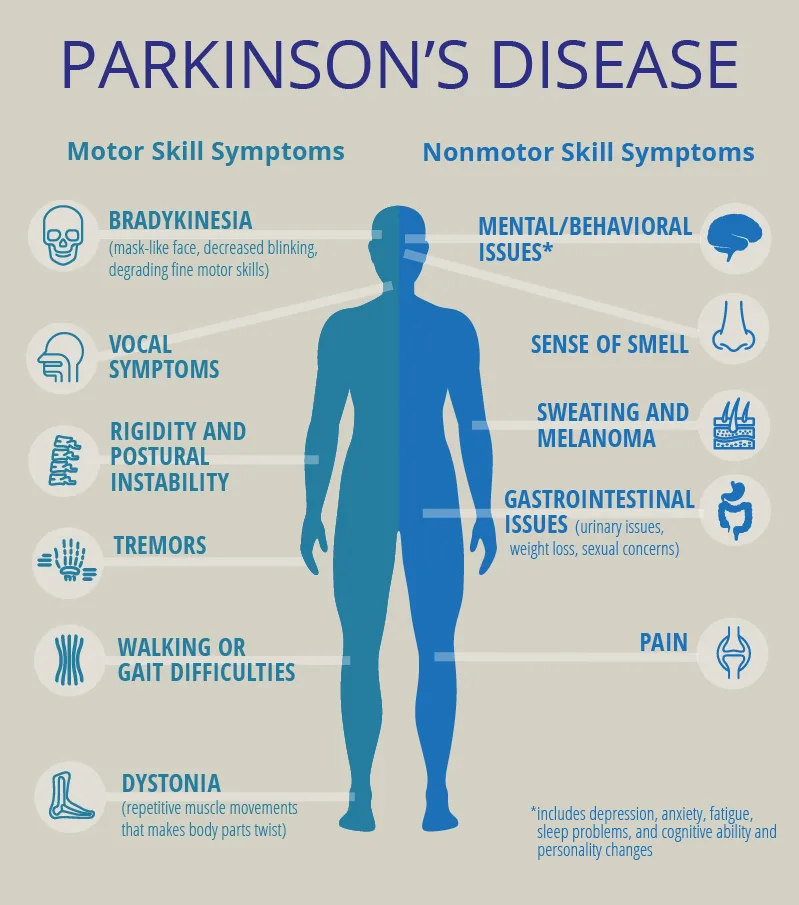
Clinical manifestations of Parkinson disease are divided into nonmotor and motor symptoms. Nonmotor symptoms include orthostatic hypotension, constipation, delayed gastric emptying, dysphagia, pain and sensory disturbances, depression, hallucinations, dementia, and sleep disorders. Motor symptoms are classically defined by resting “pill-rolling” tremor, cogwheel rigidity due to increased muscle tone, bradykinesia with marked slowness of movement, postural instability, stooped posture, and a reduced facial expression often described as a “masked face.” A sudden change in baseline motor function or mental status in a patient with known PD may be the only sign of an underlying systemic illness such as infection.
History is the cornerstone of diagnosis and emergency assessment. Important elements include the onset and progression of symptoms, whether the presentation was gradual or sudden, medication adherence, and exposure to drugs or toxins that may cause parkinsonism. Sudden withdrawal or noncompliance with dopaminergic therapy can precipitate parkinsonism–hyperpyrexia syndrome, a life-threatening condition marked by rigidity, hyperthermia, reduced consciousness, autonomic instability, and complications such as acute renal failure, rhabdomyolysis, venous thrombosis, and disseminated intravascular coagulation.
Physical examination typically reveals cogwheel rigidity, resting tremor, bradykinesia, and postural abnormalities. Diagnosis of Parkinson disease is primarily clinical, and no specific laboratory test is required to confirm it. In the emergency department, investigations are directed toward identifying alternative diagnoses, complications, or precipitants of deterioration. Laboratory studies may be indicated if parkinsonism–hyperpyrexia syndrome or infection is suspected. Neuroimaging with CT or MRI is not required to diagnose PD but may be performed to evaluate dementia or exclude other neurologic conditions. Chest radiography may be useful when respiratory infection is suspected.
The differential diagnosis of Parkinson disease is broad and includes essential tremor, benign familial tremor, major depression, Wilson disease, Huntington disease, Alzheimer disease, dementia with Lewy bodies, Creutzfeldt–Jakob disease, vitamin B12 deficiency, hypothyroidism, hydrocephalus, multi-infarct dementia, and toxic exposures such as carbon monoxide poisoning. Careful clinical assessment is essential to avoid misdiagnosis.
Management in the emergency department focuses on symptom control, identification and treatment of triggers, and prevention of complications. Antiparkinsonian medications may be initiated or adjusted in consultation with neurology. Patients with mild disease may not require immediate pharmacologic therapy, while those with moderate disease often benefit from dopaminergic or anticholinergic agents. Underlying infections or metabolic disturbances should be treated promptly. Parkinsonism–hyperpyrexia syndrome requires urgent replacement of dopaminergic therapy, supportive care, and management of associated complications.
Common medications used in Parkinson disease include carbidopa/levodopa as first-line therapy, dopamine agonists such as pramipexole and ropinirole, MAO-B inhibitors like selegiline and rasagiline, anticholinergics such as benztropine for tremor-dominant disease, and amantadine to stimulate dopamine release. Adjunctive agents like entacapone may be used to enhance levodopa bioavailability. In parkinsonism–hyperpyrexia syndrome, intravenous or enteral levodopa and bromocriptine are essential.
Admission is indicated for patients with Parkinson disease who present with serious medical conditions such as infection, trauma, cardiovascular or cerebrovascular emergencies, electrolyte disturbances, altered mental status, medication complications, failure to thrive, or suspected abuse. Patients with depression and suicidal intent or complications related to deep brain stimulation devices also require inpatient care. Stable patients with mild to moderate disease may be discharged with medications and urgent outpatient neurology follow-up.
Key clinical pearls include recognizing that Parkinson disease can be difficult to diagnose and is frequently confused with other neurologic conditions. Sudden withdrawal of dopaminergic medications is a medical emergency and must be avoided. In the emergency setting, vigilance for systemic illness, medication noncompliance, and life-threatening complications is critical to optimal patient outcomes.
Parkinson disease (PD) is a gradually progressive neurodegenerative disorder that typically affects individuals in middle or late life. It is characterized by degeneration of dopaminergic neurons in the substantia nigra, formation of Lewy bodies in remaining neurons, and accelerated cortical atrophy. Although symptoms often begin unilaterally, the disease usually progresses to symmetric involvement. Parkinson disease affects approximately 1% of people over 60 years of age and up to 4% of those over 80. Importantly, nonspecific symptoms such as fatigue, constipation, and hyposmia may precede the diagnosis by many years, sometimes up to two decades.
The etiology of Parkinson disease is most often sporadic or idiopathic. However, several other conditions can present with parkinsonism and must be considered, especially in the emergency setting. These include drug-induced causes such as neuroleptics and sudden withdrawal of dopaminergic medications leading to parkinsonism–hyperpyrexia syndrome, as well as exposure to toxins like carbon monoxide, methanol, cyanide, organophosphates, and MPTP. Structural brain lesions involving the basal ganglia or midbrain, hydrocephalus, infections such as viral encephalitis or Mycoplasma, and other neurologic conditions like central pontine myelinolysis and encephalitis lethargica can also produce parkinsonian features.
Clinical manifestations of Parkinson disease are divided into nonmotor and motor symptoms. Nonmotor symptoms include orthostatic hypotension, constipation, delayed gastric emptying, dysphagia, pain and sensory disturbances, depression, hallucinations, dementia, and sleep disorders. Motor symptoms are classically defined by resting “pill-rolling” tremor, cogwheel rigidity due to increased muscle tone, bradykinesia with marked slowness of movement, postural instability, stooped posture, and a reduced facial expression often described as a “masked face.” A sudden change in baseline motor function or mental status in a patient with known PD may be the only sign of an underlying systemic illness such as infection.
History is the cornerstone of diagnosis and emergency assessment. Important elements include the onset and progression of symptoms, whether the presentation was gradual or sudden, medication adherence, and exposure to drugs or toxins that may cause parkinsonism. Sudden withdrawal or noncompliance with dopaminergic therapy can precipitate parkinsonism–hyperpyrexia syndrome, a life-threatening condition marked by rigidity, hyperthermia, reduced consciousness, autonomic instability, and complications such as acute renal failure, rhabdomyolysis, venous thrombosis, and disseminated intravascular coagulation.
Physical examination typically reveals cogwheel rigidity, resting tremor, bradykinesia, and postural abnormalities. Diagnosis of Parkinson disease is primarily clinical, and no specific laboratory test is required to confirm it. In the emergency department, investigations are directed toward identifying alternative diagnoses, complications, or precipitants of deterioration. Laboratory studies may be indicated if parkinsonism–hyperpyrexia syndrome or infection is suspected. Neuroimaging with CT or MRI is not required to diagnose PD but may be performed to evaluate dementia or exclude other neurologic conditions. Chest radiography may be useful when respiratory infection is suspected.
The differential diagnosis of Parkinson disease is broad and includes essential tremor, benign familial tremor, major depression, Wilson disease, Huntington disease, Alzheimer disease, dementia with Lewy bodies, Creutzfeldt–Jakob disease, vitamin B12 deficiency, hypothyroidism, hydrocephalus, multi-infarct dementia, and toxic exposures such as carbon monoxide poisoning. Careful clinical assessment is essential to avoid misdiagnosis.
Management in the emergency department focuses on symptom control, identification and treatment of triggers, and prevention of complications. Antiparkinsonian medications may be initiated or adjusted in consultation with neurology. Patients with mild disease may not require immediate pharmacologic therapy, while those with moderate disease often benefit from dopaminergic or anticholinergic agents. Underlying infections or metabolic disturbances should be treated promptly. Parkinsonism–hyperpyrexia syndrome requires urgent replacement of dopaminergic therapy, supportive care, and management of associated complications.
Common medications used in Parkinson disease include carbidopa/levodopa as first-line therapy, dopamine agonists such as pramipexole and ropinirole, MAO-B inhibitors like selegiline and rasagiline, anticholinergics such as benztropine for tremor-dominant disease, and amantadine to stimulate dopamine release. Adjunctive agents like entacapone may be used to enhance levodopa bioavailability. In parkinsonism–hyperpyrexia syndrome, intravenous or enteral levodopa and bromocriptine are essential.
Admission is indicated for patients with Parkinson disease who present with serious medical conditions such as infection, trauma, cardiovascular or cerebrovascular emergencies, electrolyte disturbances, altered mental status, medication complications, failure to thrive, or suspected abuse. Patients with depression and suicidal intent or complications related to deep brain stimulation devices also require inpatient care. Stable patients with mild to moderate disease may be discharged with medications and urgent outpatient neurology follow-up.
Key clinical pearls include recognizing that Parkinson disease can be difficult to diagnose and is frequently confused with other neurologic conditions. Sudden withdrawal of dopaminergic medications is a medical emergency and must be avoided. In the emergency setting, vigilance for systemic illness, medication noncompliance, and life-threatening complications is critical to optimal patient outcomes.
- Published on
Emergency and Acute Medicine – Paraphimosis
Paraphimosis is a urologic emergency defined by entrapment of the retracted foreskin proximal to the glans penis. This entrapment leads to progressive lymphatic congestion and venous obstruction, which can ultimately compromise arterial blood flow to the glans. If not promptly recognized and treated, paraphimosis may result in ischemia, necrosis, and permanent penile injury.
The condition most commonly occurs when the foreskin is retracted and not returned to its normal position. Predisposing factors include phimosis, inflammation, trauma, and sexual inexperience, particularly in individuals unaware of the need to reduce the foreskin after intercourse. Paraphimosis is frequently iatrogenic, occurring after physical examination, urinary catheterization, cystoscopy, or genital hygiene when the foreskin is left retracted.
Patients typically present with penile pain, a visibly retracted foreskin, and a swollen, edematous glans. The glans may appear erythematous, dusky, or cyanotic as venous congestion progresses. Local cellulitis may be present, and in advanced or untreated cases, necrosis of the glans can develop. Physical examination should include careful inspection of the entire penis to exclude constricting foreign bodies or bands, such as hair tourniquets, wire, or string, which can mimic paraphimosis.
The diagnosis of paraphimosis is clinical and should be made based on history and physical examination alone. Treatment must not be delayed for laboratory or imaging studies. Imaging is generally unnecessary unless a foreign body is suspected, in which case radiographs may be obtained after restoration of adequate perfusion.
Initial management focuses on rapid reduction of edema and prompt return of the foreskin to its normal position to restore blood flow. Pain control is essential and may require local anesthesia, a penile nerve block, systemic analgesia, or conscious sedation, especially in children. Ice packs may be applied to the glans to reduce swelling while preparations for reduction are made. Manual reduction is the first-line treatment and involves circumferential compression of the edematous glans while simultaneously applying traction to advance the foreskin distally over the glans.
If manual reduction is unsuccessful, additional techniques may be employed to reduce edema. These include the multiple puncture technique, in which small-gauge needle punctures are made in the swollen foreskin to allow expression of edema fluid, followed by another attempt at manual reduction. Osmotic methods, such as application of gauze soaked in 50% dextrose, may also help decrease edema if immediate reduction is delayed. When noninvasive methods fail, a dorsal slit of the foreskin may be required to release the constricting ring. In some cases, suturing may be necessary after reduction if the incision is extensive.
Antibiotics are generally not required unless there is associated cellulitis or balanoposthitis. Once reduction is successful and symptoms resolve, most patients can be discharged with close urologic follow-up. Admission is indicated for patients with penile necrosis, severe infection, or inability to achieve reduction. Urologic consultation is recommended in all cases, and circumcision may be considered to prevent recurrence, although this remains a topic of clinical debate.
Patient education is essential to prevent recurrence. Patients should be instructed on proper foreskin hygiene and the importance of returning the foreskin to its normal position after retraction for cleaning, sexual activity, or medical procedures. Early recognition and prompt management are key to preventing serious complications of paraphimosis.
Paraphimosis is a urologic emergency defined by entrapment of the retracted foreskin proximal to the glans penis. This entrapment leads to progressive lymphatic congestion and venous obstruction, which can ultimately compromise arterial blood flow to the glans. If not promptly recognized and treated, paraphimosis may result in ischemia, necrosis, and permanent penile injury.
The condition most commonly occurs when the foreskin is retracted and not returned to its normal position. Predisposing factors include phimosis, inflammation, trauma, and sexual inexperience, particularly in individuals unaware of the need to reduce the foreskin after intercourse. Paraphimosis is frequently iatrogenic, occurring after physical examination, urinary catheterization, cystoscopy, or genital hygiene when the foreskin is left retracted.
Patients typically present with penile pain, a visibly retracted foreskin, and a swollen, edematous glans. The glans may appear erythematous, dusky, or cyanotic as venous congestion progresses. Local cellulitis may be present, and in advanced or untreated cases, necrosis of the glans can develop. Physical examination should include careful inspection of the entire penis to exclude constricting foreign bodies or bands, such as hair tourniquets, wire, or string, which can mimic paraphimosis.
The diagnosis of paraphimosis is clinical and should be made based on history and physical examination alone. Treatment must not be delayed for laboratory or imaging studies. Imaging is generally unnecessary unless a foreign body is suspected, in which case radiographs may be obtained after restoration of adequate perfusion.
Initial management focuses on rapid reduction of edema and prompt return of the foreskin to its normal position to restore blood flow. Pain control is essential and may require local anesthesia, a penile nerve block, systemic analgesia, or conscious sedation, especially in children. Ice packs may be applied to the glans to reduce swelling while preparations for reduction are made. Manual reduction is the first-line treatment and involves circumferential compression of the edematous glans while simultaneously applying traction to advance the foreskin distally over the glans.
If manual reduction is unsuccessful, additional techniques may be employed to reduce edema. These include the multiple puncture technique, in which small-gauge needle punctures are made in the swollen foreskin to allow expression of edema fluid, followed by another attempt at manual reduction. Osmotic methods, such as application of gauze soaked in 50% dextrose, may also help decrease edema if immediate reduction is delayed. When noninvasive methods fail, a dorsal slit of the foreskin may be required to release the constricting ring. In some cases, suturing may be necessary after reduction if the incision is extensive.
Antibiotics are generally not required unless there is associated cellulitis or balanoposthitis. Once reduction is successful and symptoms resolve, most patients can be discharged with close urologic follow-up. Admission is indicated for patients with penile necrosis, severe infection, or inability to achieve reduction. Urologic consultation is recommended in all cases, and circumcision may be considered to prevent recurrence, although this remains a topic of clinical debate.
Patient education is essential to prevent recurrence. Patients should be instructed on proper foreskin hygiene and the importance of returning the foreskin to its normal position after retraction for cleaning, sexual activity, or medical procedures. Early recognition and prompt management are key to preventing serious complications of paraphimosis.

- Published on
Emergency and Acute Medicine – Panic Attack
Panic attacks are characterized by sudden episodes of intense fear accompanied by prominent physical symptoms that peak rapidly, usually within 10 minutes, and resolve within approximately 20–30 minutes. Some patients, particularly those with medical illness, may experience a nonfearful variant dominated by somatic symptoms. Panic disorder is defined by recurrent, unexpected panic attacks followed by at least one month of persistent concern about additional attacks, worry about their implications, or maladaptive behavioral changes such as avoidance. Panic disorder may occur with or without agoraphobia, which reflects anxiety related to fear of being unable to escape or obtain help. The condition is often episodic or chronic and is frequently comorbid with depression, substance use disorders, functional disability, and increased suicidal risk.
The underlying mechanism involves dysregulation of the limbic system with excessive norepinephrine release and altered serotonergic and benzodiazepine receptor function, triggering a maladaptive “fight-or-flight” response. Genetic factors play an important role, with family history of panic or anxiety disorders commonly reported. Risk factors include major life stressors in the year preceding onset, childhood shyness or separation anxiety, female sex, and stimulant use such as cocaine. Panic attacks may initially arise in the context of physical illness or substance use and persist even after the precipitating condition has resolved.
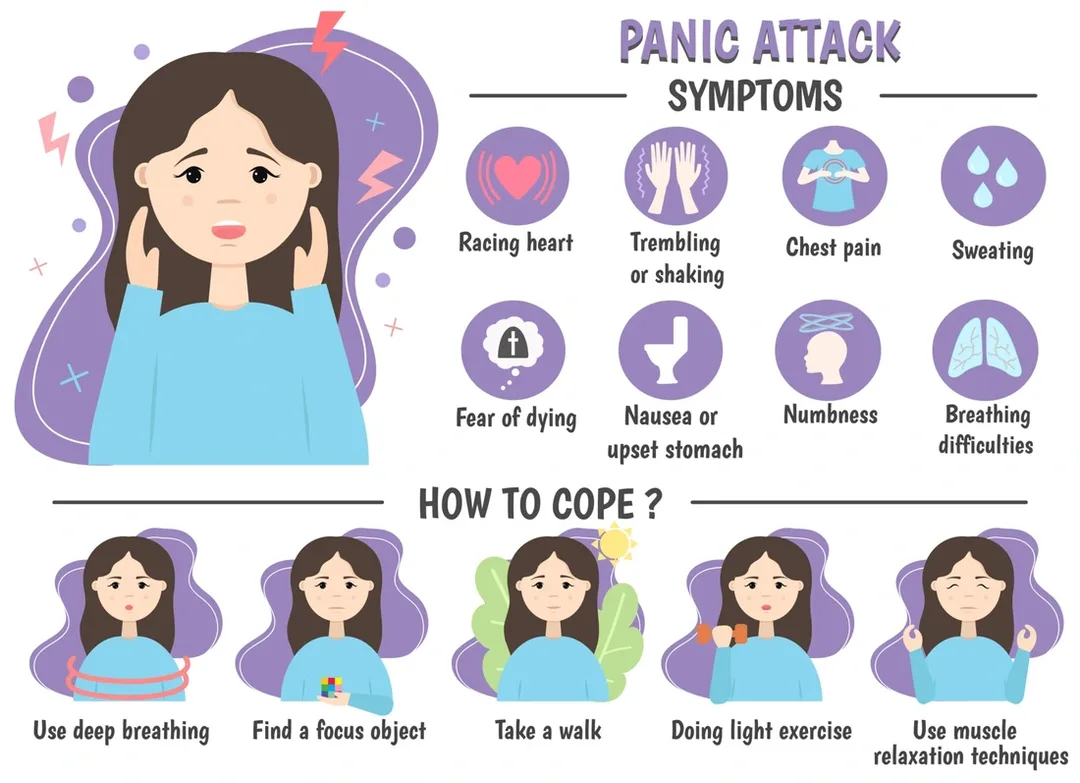
Clinical presentation reflects widespread autonomic activation. Cardiac symptoms include palpitations, tachycardia, and chest discomfort. Respiratory complaints such as shortness of breath, choking sensations, or smothering feelings are common. Neurologic and systemic symptoms include tremor, dizziness, lightheadedness, paresthesias, sweating, chills, flushing, and feelings of unreality or depersonalization. Gastrointestinal symptoms such as nausea, cramping, and abdominal pain may occur. Intense, stereotyped fears often center on imminent death, having a heart attack, losing control, or “going crazy.” A thorough history should explore medical conditions, medications (including over-the-counter and herbal products), substance and caffeine use, age at onset, triggering stressors, avoidance behaviors, prior treatment response, and family history of anxiety or substance use.
Physical examination should be complete and focused on cardiopulmonary and neurologic systems, guided by presenting symptoms. The essential workup is individualized and often minimal, aimed at excluding organic causes suggested by the history or exam. Laboratory evaluation may include basic metabolic studies, glucose, thyroid-stimulating hormone, and toxicology screening. Electrocardiography is appropriate for patients over 40 years of age, those with cardiac symptoms, or those taking tricyclic antidepressants. Additional testing such as Holter monitoring, arterial blood gases, or EEG is reserved for specific indications.
The differential diagnosis is broad and must be carefully considered, particularly in first presentations, late-onset cases, or atypical features. Cardiopulmonary causes include myocardial ischemia, arrhythmias, pulmonary embolism, asthma, and pneumonia. Metabolic and endocrine disorders include hypoglycemia, hyperthyroidism, electrolyte abnormalities, and pheochromocytoma. Neurologic conditions such as seizures or transient ischemic attack, medication effects, substance intoxication or withdrawal, and other psychiatric disorders including PTSD, obsessive-compulsive disorder, and somatoform disorders must also be considered.
Initial management focuses on calm reassurance and patient education. Most panic attacks resolve spontaneously, and excessive medical intervention may reinforce fear. Explaining the physiologic basis of symptoms can reduce distress and interrupt the cycle of escalating anxiety. In the emergency department, short-acting, high-potency benzodiazepines may be used for severe or persistent symptoms. Lorazepam is often preferred due to its rapid onset and smoother offset. Clonazepam is effective but has a slower onset and is better suited for maintenance therapy rather than acute control. Alprazolam should generally be avoided due to rapid offset and risk of rebound anxiety. Long-term management of recurrent panic attacks or panic disorder relies on cognitive–behavioral therapy and selective serotonin reuptake inhibitors, which should be initiated in the outpatient setting when follow-up is assured.
Admission is rarely required unless needed to exclude a serious medical condition or for psychiatric indications such as suicidality. Most patients can be safely discharged once symptoms resolve, with reassurance and clear follow-up plans. Referral to primary care or mental health services is recommended for recurrent attacks, interepisode anxiety, or avoidance behaviors. Patients should be counseled to avoid triggers such as caffeine, stimulants, and alcohol. Key pearls include recognizing that panic attacks are self-limited, maintaining a calm clinical approach, using medications judiciously, and emphasizing nonpharmacologic strategies such as cognitive–behavioral therapy to achieve durable symptom control.
Panic attacks are characterized by sudden episodes of intense fear accompanied by prominent physical symptoms that peak rapidly, usually within 10 minutes, and resolve within approximately 20–30 minutes. Some patients, particularly those with medical illness, may experience a nonfearful variant dominated by somatic symptoms. Panic disorder is defined by recurrent, unexpected panic attacks followed by at least one month of persistent concern about additional attacks, worry about their implications, or maladaptive behavioral changes such as avoidance. Panic disorder may occur with or without agoraphobia, which reflects anxiety related to fear of being unable to escape or obtain help. The condition is often episodic or chronic and is frequently comorbid with depression, substance use disorders, functional disability, and increased suicidal risk.
The underlying mechanism involves dysregulation of the limbic system with excessive norepinephrine release and altered serotonergic and benzodiazepine receptor function, triggering a maladaptive “fight-or-flight” response. Genetic factors play an important role, with family history of panic or anxiety disorders commonly reported. Risk factors include major life stressors in the year preceding onset, childhood shyness or separation anxiety, female sex, and stimulant use such as cocaine. Panic attacks may initially arise in the context of physical illness or substance use and persist even after the precipitating condition has resolved.
Clinical presentation reflects widespread autonomic activation. Cardiac symptoms include palpitations, tachycardia, and chest discomfort. Respiratory complaints such as shortness of breath, choking sensations, or smothering feelings are common. Neurologic and systemic symptoms include tremor, dizziness, lightheadedness, paresthesias, sweating, chills, flushing, and feelings of unreality or depersonalization. Gastrointestinal symptoms such as nausea, cramping, and abdominal pain may occur. Intense, stereotyped fears often center on imminent death, having a heart attack, losing control, or “going crazy.” A thorough history should explore medical conditions, medications (including over-the-counter and herbal products), substance and caffeine use, age at onset, triggering stressors, avoidance behaviors, prior treatment response, and family history of anxiety or substance use.
Physical examination should be complete and focused on cardiopulmonary and neurologic systems, guided by presenting symptoms. The essential workup is individualized and often minimal, aimed at excluding organic causes suggested by the history or exam. Laboratory evaluation may include basic metabolic studies, glucose, thyroid-stimulating hormone, and toxicology screening. Electrocardiography is appropriate for patients over 40 years of age, those with cardiac symptoms, or those taking tricyclic antidepressants. Additional testing such as Holter monitoring, arterial blood gases, or EEG is reserved for specific indications.
The differential diagnosis is broad and must be carefully considered, particularly in first presentations, late-onset cases, or atypical features. Cardiopulmonary causes include myocardial ischemia, arrhythmias, pulmonary embolism, asthma, and pneumonia. Metabolic and endocrine disorders include hypoglycemia, hyperthyroidism, electrolyte abnormalities, and pheochromocytoma. Neurologic conditions such as seizures or transient ischemic attack, medication effects, substance intoxication or withdrawal, and other psychiatric disorders including PTSD, obsessive-compulsive disorder, and somatoform disorders must also be considered.
Initial management focuses on calm reassurance and patient education. Most panic attacks resolve spontaneously, and excessive medical intervention may reinforce fear. Explaining the physiologic basis of symptoms can reduce distress and interrupt the cycle of escalating anxiety. In the emergency department, short-acting, high-potency benzodiazepines may be used for severe or persistent symptoms. Lorazepam is often preferred due to its rapid onset and smoother offset. Clonazepam is effective but has a slower onset and is better suited for maintenance therapy rather than acute control. Alprazolam should generally be avoided due to rapid offset and risk of rebound anxiety. Long-term management of recurrent panic attacks or panic disorder relies on cognitive–behavioral therapy and selective serotonin reuptake inhibitors, which should be initiated in the outpatient setting when follow-up is assured.
Admission is rarely required unless needed to exclude a serious medical condition or for psychiatric indications such as suicidality. Most patients can be safely discharged once symptoms resolve, with reassurance and clear follow-up plans. Referral to primary care or mental health services is recommended for recurrent attacks, interepisode anxiety, or avoidance behaviors. Patients should be counseled to avoid triggers such as caffeine, stimulants, and alcohol. Key pearls include recognizing that panic attacks are self-limited, maintaining a calm clinical approach, using medications judiciously, and emphasizing nonpharmacologic strategies such as cognitive–behavioral therapy to achieve durable symptom control.
- Published on
Emergency and Acute Medicine – Nursemaid’s Elbow
Nursemaid’s elbow is the most common elbow injury in children younger than five years of age. It occurs when sudden longitudinal traction is applied to the distal radius, causing the annular ligament to slip over the radial head and become interposed between the radius and the capitellum. Typical mechanisms include lifting or pulling a child by the hands or arms, swinging the child during play, wrestling, or abrupt traction during a fall. In infants younger than six months, the injury may occur when the child rolls onto the arm. By approximately five years of age, the annular ligament becomes thicker and more resistant to displacement, making this injury uncommon in older children.
Children with nursemaid’s elbow classically refuse to use the affected arm. The elbow is usually held slightly flexed, with the forearm pronated and close to the trunk. Pain is noted with elbow flexion and particularly with forearm supination or pronation. There is typically minimal or no swelling and no obvious deformity. Point tenderness is absent or limited to mild tenderness over the anterolateral radial head. Passive range of motion is usually painless, but the child avoids active use of the arm. Although a history of pulling on the arm is characteristic, it is reported in only about half of cases, and alternative mechanisms such as minor trauma or twisting injuries should be considered.
The diagnosis of nursemaid’s elbow is clinical and relies on a classic history and physical examination findings. Routine imaging is not required. Radiographs should be obtained if there is focal bony tenderness, soft tissue swelling, deformity, ecchymosis, an atypical history, failed reduction attempts, or persistent refusal to use the arm after reduction. The differential diagnosis includes fractures of the humerus, radius, or ulna, elbow dislocation, septic arthritis, osteomyelitis, and rarely neoplasm.
Prehospital care consists of placing ice on the elbow to reduce discomfort, immobilizing the arm in a sling or splint for transport, and assessing distal neurovascular status. In the emergency department, initial stabilization includes confirmation of intact distal motor, sensory, and vascular function before attempting reduction.
Definitive treatment is reduction of the radial head subluxation. Two reduction techniques are commonly used. The supination–flexion technique involves gentle axial traction while supinating the forearm, followed by smooth flexion of the elbow, with the examiner’s thumb applying pressure over the radial head. The hyperpronation technique involves gentle axial traction with forceful hyperpronation of the forearm, with extension if the arm is not already extended, again stabilizing the radial head. Hyperpronation is generally more successful and is often perceived as less painful by caregivers. A subtle click may be palpated during successful reduction. The child may cry briefly during the maneuver but often resumes normal use of the arm within minutes. If the child does not use the arm within 15 minutes, a second reduction attempt should be performed, preferably using the alternate technique. Failure after two attempts warrants radiographic evaluation.
Medications are usually unnecessary, as pain resolves rapidly after successful reduction. If needed, acetaminophen or ibuprofen may be given for comfort. There are no admission criteria for uncomplicated nursemaid’s elbow. Children may be discharged once they regain full, unrestricted use of the arm. Parents should be counseled to avoid lifting or pulling the child by the hands, wrists, or forearms. Recurrence is common, with rates of approximately 27–39%, until the child reaches five years of age.
Follow-up is not required after successful reduction. If reduction is unsuccessful and imaging is negative for fracture, orthopedic referral is recommended, and the arm should be placed in a sling or posterior splint for outpatient evaluation. Key pearls include maintaining suspicion with a classic presentation, avoiding unnecessary radiographs, ensuring that at least one reduction attempt uses the hyperpronation technique, and recognizing that short delays in reduction do not result in long-term sequelae.
Nursemaid’s elbow is the most common elbow injury in children younger than five years of age. It occurs when sudden longitudinal traction is applied to the distal radius, causing the annular ligament to slip over the radial head and become interposed between the radius and the capitellum. Typical mechanisms include lifting or pulling a child by the hands or arms, swinging the child during play, wrestling, or abrupt traction during a fall. In infants younger than six months, the injury may occur when the child rolls onto the arm. By approximately five years of age, the annular ligament becomes thicker and more resistant to displacement, making this injury uncommon in older children.
Children with nursemaid’s elbow classically refuse to use the affected arm. The elbow is usually held slightly flexed, with the forearm pronated and close to the trunk. Pain is noted with elbow flexion and particularly with forearm supination or pronation. There is typically minimal or no swelling and no obvious deformity. Point tenderness is absent or limited to mild tenderness over the anterolateral radial head. Passive range of motion is usually painless, but the child avoids active use of the arm. Although a history of pulling on the arm is characteristic, it is reported in only about half of cases, and alternative mechanisms such as minor trauma or twisting injuries should be considered.
The diagnosis of nursemaid’s elbow is clinical and relies on a classic history and physical examination findings. Routine imaging is not required. Radiographs should be obtained if there is focal bony tenderness, soft tissue swelling, deformity, ecchymosis, an atypical history, failed reduction attempts, or persistent refusal to use the arm after reduction. The differential diagnosis includes fractures of the humerus, radius, or ulna, elbow dislocation, septic arthritis, osteomyelitis, and rarely neoplasm.
Prehospital care consists of placing ice on the elbow to reduce discomfort, immobilizing the arm in a sling or splint for transport, and assessing distal neurovascular status. In the emergency department, initial stabilization includes confirmation of intact distal motor, sensory, and vascular function before attempting reduction.
Definitive treatment is reduction of the radial head subluxation. Two reduction techniques are commonly used. The supination–flexion technique involves gentle axial traction while supinating the forearm, followed by smooth flexion of the elbow, with the examiner’s thumb applying pressure over the radial head. The hyperpronation technique involves gentle axial traction with forceful hyperpronation of the forearm, with extension if the arm is not already extended, again stabilizing the radial head. Hyperpronation is generally more successful and is often perceived as less painful by caregivers. A subtle click may be palpated during successful reduction. The child may cry briefly during the maneuver but often resumes normal use of the arm within minutes. If the child does not use the arm within 15 minutes, a second reduction attempt should be performed, preferably using the alternate technique. Failure after two attempts warrants radiographic evaluation.
Medications are usually unnecessary, as pain resolves rapidly after successful reduction. If needed, acetaminophen or ibuprofen may be given for comfort. There are no admission criteria for uncomplicated nursemaid’s elbow. Children may be discharged once they regain full, unrestricted use of the arm. Parents should be counseled to avoid lifting or pulling the child by the hands, wrists, or forearms. Recurrence is common, with rates of approximately 27–39%, until the child reaches five years of age.
Follow-up is not required after successful reduction. If reduction is unsuccessful and imaging is negative for fracture, orthopedic referral is recommended, and the arm should be placed in a sling or posterior splint for outpatient evaluation. Key pearls include maintaining suspicion with a classic presentation, avoiding unnecessary radiographs, ensuring that at least one reduction attempt uses the hyperpronation technique, and recognizing that short delays in reduction do not result in long-term sequelae.

- Published on
Emergency and Acute Medicine – Nonsteroidal Anti-Inflammatory Poisoning
Nonsteroidal anti-inflammatory drugs (NSAIDs) exert their effects by inhibiting cyclooxygenase (COX), thereby blocking the conversion of arachidonic acid to prostaglandins. In most cases, NSAID ingestion results in low morbidity, and toxicity is usually mild. Much of the published toxicity data involves ibuprofen, largely because of its widespread over-the-counter availability. Fatal outcomes are rare but have been reported with massive ingestions. Patients with underlying congestive heart failure or renal insufficiency are at increased risk of toxicity because NSAIDs promote sodium and water retention and reduce renal blood flow. Experience with COX-2 inhibitors such as celecoxib in overdose is limited, but management is similar to that of traditional NSAIDs. Patients may still ingest rofecoxib or valdecoxib from stored supplies despite their withdrawal from the US market.
NSAIDs are available both by prescription and over the counter and include agents such as ibuprofen, naproxen, diclofenac, ketorolac, indomethacin, meloxicam, sulindac, piroxicam, and others. Toxic effects vary slightly among agents, but the overall clinical approach remains similar.
Clinical manifestations primarily involve the gastrointestinal and central nervous systems. Gastrointestinal symptoms include nausea, vomiting, and epigastric pain. Neurologic findings range from drowsiness, dizziness, and lethargy to aseptic meningitis and seizures in severe cases. Cardiovascular effects may include hypotension and tachycardia. Pulmonary complications such as eosinophilic pneumonia, apnea, or hyperventilation are uncommon but reported. Renal effects include acute renal failure, hyperkalemia, acute tubular necrosis, and acute interstitial nephritis. Hepatic injury may present as hepatocellular damage or cholestatic jaundice, particularly with diclofenac or sulindac. Metabolic effects are usually limited to a mild, transient metabolic acidosis. Hypersensitivity reactions can occur and include asthma exacerbations, angioedema, urticaria, and aseptic meningitis.
Evaluation begins with a focused history and assessment of the specific NSAID ingested, as subtle toxicologic differences exist between agents. Most cases result in mild toxicity, but identification of the drug is helpful because aseptic meningitis is more commonly associated with ibuprofen, while liver toxicity is more frequently seen with diclofenac and sulindac.
Laboratory evaluation should include electrolytes, blood urea nitrogen, creatinine, and glucose to assess baseline renal function and metabolic status. A complete blood count and arterial blood gas are indicated in large overdoses or if metabolic acidosis is suspected. Coagulation studies may be obtained, noting that etodolac can cause false-positive bilirubin or ketone dipstick results. Acetaminophen and salicylate levels should be obtained in all suspected NSAID ingestions, as patients often confuse these medications. Toxicology screens are not useful because NSAIDs are difficult to detect and results do not alter management.
The differential diagnosis includes other causes of metabolic acidosis, gastrointestinal irritation, and altered mental status, such as salicylate poisoning, isoniazid toxicity, ethylene glycol, methanol, and isopropanol ingestion.
Management is largely supportive. Prehospital care should focus on bringing all medication containers for identification. Initial stabilization follows standard airway, breathing, and circulation principles, with administration of naloxone, thiamine, and dextrose for altered mental status when indicated. In the emergency department, activated charcoal may be administered if the patient presents early after ingestion. Enhanced elimination techniques such as hemodialysis are not effective due to the high degree of plasma protein binding of NSAIDs.
Admission is indicated for patients with persistent vomiting, hematemesis, central nervous system depression, seizures, metabolic acidosis, hypotension or hypertension, congestive heart failure, or renal failure. Asymptomatic patients with nontoxic ingestions who remain well after 6–8 hours of observation may be safely discharged. Intentional ingestions warrant psychiatric evaluation and follow-up.
Key clinical points include the generally benign nature of NSAID poisoning, the importance of evaluating for coingestions, and the routine measurement of acetaminophen and salicylate levels. Massive overdoses and patients with underlying cardiac or renal disease carry a higher risk of significant toxicity and require closer monitoring.
Nonsteroidal anti-inflammatory drugs (NSAIDs) exert their effects by inhibiting cyclooxygenase (COX), thereby blocking the conversion of arachidonic acid to prostaglandins. In most cases, NSAID ingestion results in low morbidity, and toxicity is usually mild. Much of the published toxicity data involves ibuprofen, largely because of its widespread over-the-counter availability. Fatal outcomes are rare but have been reported with massive ingestions. Patients with underlying congestive heart failure or renal insufficiency are at increased risk of toxicity because NSAIDs promote sodium and water retention and reduce renal blood flow. Experience with COX-2 inhibitors such as celecoxib in overdose is limited, but management is similar to that of traditional NSAIDs. Patients may still ingest rofecoxib or valdecoxib from stored supplies despite their withdrawal from the US market.
NSAIDs are available both by prescription and over the counter and include agents such as ibuprofen, naproxen, diclofenac, ketorolac, indomethacin, meloxicam, sulindac, piroxicam, and others. Toxic effects vary slightly among agents, but the overall clinical approach remains similar.
Clinical manifestations primarily involve the gastrointestinal and central nervous systems. Gastrointestinal symptoms include nausea, vomiting, and epigastric pain. Neurologic findings range from drowsiness, dizziness, and lethargy to aseptic meningitis and seizures in severe cases. Cardiovascular effects may include hypotension and tachycardia. Pulmonary complications such as eosinophilic pneumonia, apnea, or hyperventilation are uncommon but reported. Renal effects include acute renal failure, hyperkalemia, acute tubular necrosis, and acute interstitial nephritis. Hepatic injury may present as hepatocellular damage or cholestatic jaundice, particularly with diclofenac or sulindac. Metabolic effects are usually limited to a mild, transient metabolic acidosis. Hypersensitivity reactions can occur and include asthma exacerbations, angioedema, urticaria, and aseptic meningitis.
Evaluation begins with a focused history and assessment of the specific NSAID ingested, as subtle toxicologic differences exist between agents. Most cases result in mild toxicity, but identification of the drug is helpful because aseptic meningitis is more commonly associated with ibuprofen, while liver toxicity is more frequently seen with diclofenac and sulindac.
Laboratory evaluation should include electrolytes, blood urea nitrogen, creatinine, and glucose to assess baseline renal function and metabolic status. A complete blood count and arterial blood gas are indicated in large overdoses or if metabolic acidosis is suspected. Coagulation studies may be obtained, noting that etodolac can cause false-positive bilirubin or ketone dipstick results. Acetaminophen and salicylate levels should be obtained in all suspected NSAID ingestions, as patients often confuse these medications. Toxicology screens are not useful because NSAIDs are difficult to detect and results do not alter management.
The differential diagnosis includes other causes of metabolic acidosis, gastrointestinal irritation, and altered mental status, such as salicylate poisoning, isoniazid toxicity, ethylene glycol, methanol, and isopropanol ingestion.
Management is largely supportive. Prehospital care should focus on bringing all medication containers for identification. Initial stabilization follows standard airway, breathing, and circulation principles, with administration of naloxone, thiamine, and dextrose for altered mental status when indicated. In the emergency department, activated charcoal may be administered if the patient presents early after ingestion. Enhanced elimination techniques such as hemodialysis are not effective due to the high degree of plasma protein binding of NSAIDs.
Admission is indicated for patients with persistent vomiting, hematemesis, central nervous system depression, seizures, metabolic acidosis, hypotension or hypertension, congestive heart failure, or renal failure. Asymptomatic patients with nontoxic ingestions who remain well after 6–8 hours of observation may be safely discharged. Intentional ingestions warrant psychiatric evaluation and follow-up.
Key clinical points include the generally benign nature of NSAID poisoning, the importance of evaluating for coingestions, and the routine measurement of acetaminophen and salicylate levels. Massive overdoses and patients with underlying cardiac or renal disease carry a higher risk of significant toxicity and require closer monitoring.
- Published on
Emergency and Acute Medicine – Pancreatitis (Don’t-Miss Points Included)
Pancreatitis is inflammation of the pancreas caused by premature activation, liberation, and autodigestion of the gland by pancreatic enzymes. Acute pancreatitis results in temporary impairment of exocrine and endocrine function that usually resolves over weeks to months, whereas chronic pancreatitis leads to progressive and irreversible glandular destruction with steatorrhea, malabsorption, diabetes, and chronic pain. A pancreatic pseudocyst is a common complication, defined as a pancreatic enzyme–rich fluid collection surrounded by fibrous tissue without epithelial lining, typically forming 4–6 weeks after acute pancreatitis.
The two most common causes of acute pancreatitis—gallstones and alcohol abuse—account for 75–80% of cases and must always be considered first. Chronic pancreatitis is most commonly due to long-term alcohol abuse (70–80%). Other important etiologies include pancreatic duct obstruction, ischemia, medications, infections, metabolic disorders (hypercalcemia, hyperlipidemia), trauma, post-ERCP injury, penetrating peptic ulcer disease, hereditary causes, and rare toxins (e.g., scorpion venom). In children, pancreatitis is most often caused by viral illness, trauma, or medications. Pancreatic pseudocysts occur in 5–16% of acute pancreatitis and up to 40% of chronic pancreatitis, and rupture or hemorrhage is life-threatening.
Severe epigastric pain radiating to the back is the hallmark symptom and is present in nearly all patients. Pain is often worse when supine and may improve with leaning forward. Nausea and vomiting occur in most cases, with low-grade fever, hypotension, and jaundice being common associated findings. Decreased or absent bowel sounds are typical. Cullen sign (periumbilical ecchymosis) and Grey Turner sign (flank ecchymosis) are rare but ominous indicators of hemorrhagic pancreatitis. Respiratory complications are common and include pleural effusions (especially left-sided), atelectasis, pulmonary edema, and hypoxemia. Cardiovascular instability may progress to shock, while neurologic findings range from irritability to confusion and coma. Significant GI bleeding is uncommon and suggests an alternative diagnosis.
Diagnosis relies on clinical presentation supported by laboratory testing. Serum lipase is the most reliable diagnostic test, rising within 4-8 hours of symptom onset and remaining elevated longer than amylase. Amylase may be elevated earlier but is less specific and may be normal in severe disease. Additional lab abnormalities include leukocytosis, hemoconcentration (hematocrit >47% suggests risk of necrosis), electrolyte abnormalities, hyperglycemia, hypocalcemia (marker of severe disease), hypomagnesemia (especially in alcohol use), and abnormal liver enzymes suggesting biliary pancreatitis. Ranson criteria must be assessed, as a score ≥3 indicates severe disease with increased mortality. Arterial blood gases are required in hypoxic or toxic patients.
Imaging is guided by clinical severity. Ultrasound is essential when gallstones are suspected. CT abdomen with contrast is indicated for severe pancreatitis, diagnostic uncertainty, suspected necrosis, hemorrhage, or pseudocyst, and should not be performed routinely in mild cases. Chest radiographs may reveal pleural effusions or atelectasis. ERCP is indicated urgently only in severe pancreatitis with cholangitis or persistent biliary obstruction.
Initial management must not be delayed. Aggressive IV fluid resuscitation is critical and lifesaving, often requiring 5–6 liters in the first 24 hours, with close monitoring of vitals, urine output, and electrolytes. Supplemental oxygen and cardiac monitoring are mandatory. Early and adequate opioid analgesia is essential; morphine or hydromorphone are appropriate. Antiemetics should be administered promptly. Nasogastric suction is not routinely indicated but may help in severe disease or intractable vomiting. Antibiotics are NOT indicated unless infected pancreatic necrosis is confirmed—routine prophylaxis increases resistance without benefit. Correct electrolyte abnormalities promptly, especially hypocalcemia, hypokalemia, and hypomagnesemia.
Patients with significant pain, vomiting, hypoxia, systemic instability, or laboratory evidence of severe disease require hospital admission. ICU admission is mandatory for necrotizing or hemorrhagic pancreatitis. Discharge is appropriate only for mild acute pancreatitis when the patient tolerates oral intake, has controlled pain, and no biliary obstruction. Chronic pancreatitis patients may be discharged if pain is minimal and oral intake is adequate. All discharged patients require close follow-up within 24–48 hours.
Critical Don’t-Miss Pearls
- Gallstones and alcohol cause 75–80% of acute pancreatitis—always rule them out first
- Lipase > amylase for diagnosis; normal amylase does NOT exclude pancreatitis
- Early aggressive IV fluids reduce necrosis and mortality
- Ranson score ≥3 = severe disease
- Do NOT give antibiotics unless infected necrosis is proven
- NG tubes are not routine
- CT early only if diagnosis is unclear or disease is severe
- Ruptured or hemorrhagic pseudocyst = surgical emergency
- Hypocalcemia and rising hematocrit are markers of severe disease
Pancreatitis is common, potentially lethal, and time-sensitive—early recognition, aggressive resuscitation, and avoidance of common pitfalls are critical to survival.
- Published on
Emergency and Acute Medicine – Pancreatic Trauma
Pancreatic trauma most commonly results from a direct epigastric blow that compresses the pancreas against the vertebral column in blunt trauma or from penetrating injury by a sharp object. Because of the retroperitoneal location of the pancreas, significant force is usually required to cause injury. In children, pancreatic trauma often reflects proportionately greater force to a smaller body mass, leading to multisystem injuries, and clinicians must consider nonaccidental trauma, malpositioned seat belts, and child abuse. Pediatric patients may present without hypotension despite serious injury.
Penetrating trauma is the most common mechanism overall, while blunt trauma typically involves steering wheels, seat belts, or bicycle handlebars impacting the upper abdomen. Pancreatic injury is rarely isolated, with approximately 90% of cases associated with injuries to adjacent structures including the liver, stomach, spleen, kidneys, duodenum, colon, small bowel, common bile duct, gallbladder, major vascular structures, and the spine, particularly Chance fractures.
Clinical presentation is often subtle and nonspecific, and the extent of pancreatic injury may not be apparent on initial evaluation. Patients typically report diffuse or epigastric abdominal pain that may be out of proportion to physical findings and vital signs. Associated findings include upper abdominal soft-tissue contusions, lower rib or costal cartilage injuries, hypotension, and signs of retroperitoneal hemorrhage such as Grey Turner or Cullen signs. Vascular injury is the leading cause of mortality and mandates immediate evaluation and surgical consideration when suspected.
Physical examination should be thorough and repeated serially, with inspection for abrasions, contusions, and penetrating wounds, including a complete log roll. Clinicians should assess bowel sounds, abdominal tenderness, guarding, rebound, and evaluate for occult bleeding with rectal or genital examinations as appropriate. Serial vital signs and examinations are essential, as early findings may be minimal despite significant injury.
Diagnostic evaluation is dictated by patient stability and associated injuries. Contrast-enhanced abdominal CT is the cornerstone of evaluation for pancreatic trauma, although imaging may still miss injuries, particularly ductal disruptions. MRCP is increasingly used in trauma centers to better assess pancreatic duct involvement. Laboratory testing includes hematocrit, complete metabolic profile, coagulation studies, and type and screen. Serum amylase and lipase are unreliable for ruling out pancreatic injury; normal levels do not exclude injury, while elevations are nonspecific but may raise suspicion. FAST ultrasound may identify associated injuries but is insensitive for pancreatic damage.
Initial management follows standard trauma principles with airway protection, hemodynamic resuscitation using crystalloids or blood products, and early surgical consultation. Nasogastric decompression may be beneficial. Broad-spectrum antibiotics are indicated for penetrating injuries or when operative intervention is required, with coverage for both aerobic and anaerobic enteric organisms. Early identification of ductal injury significantly reduces morbidity and mortality.
Definitive management depends on injury grade and patient stability. Minor pancreatic injuries are often managed with drainage, while higher-grade injuries involving ductal disruption may require resection and drainage, pancreaticoduodenectomy, or selective endoscopic interventions. There is insufficient evidence to support routine use of octreotide. All patients with suspected pancreatic injury require hospital admission, observation, and serial examinations, with unstable patients proceeding directly to operative exploration.
Complications may present in a delayed fashion and include pancreatitis, pseudocyst formation, fistulas, and vascular aneurysms. Long-term endocrine or exocrine dysfunction is uncommon unless extensive pancreatic tissue is destroyed or resected. A high index of suspicion, careful imaging selection, and early surgical involvement are essential to optimize outcomes in pancreatic trauma.

