- Published on
Emergency And Acute Medicine – Fibromyalgia
Basics Description
Fibromyalgia is a nonarticular, noninflammatory syndrome characterized by chronic, widespread musculoskeletal pain and heightened pain sensitivity to normally nonpainful stimuli (allodynia). It is more common in females and is associated with diffuse tenderness at multiple sites, fatigue, sleep disturbance, muscle stiffness, and cognitive difficulties involving attention and memory. Physical examination findings are often limited. Fibromyalgia is not a diagnosis of exclusion and may coexist with other rheumatologic or medical conditions.
Etiology
The underlying mechanism is believed to involve central pain processing abnormalities, with increased activity of pronociceptive pathways and reduced activity of antinociceptive pathways in the brain and spinal cord. Identified contributors include elevated substance P levels and decreased biogenic amines such as norepinephrine, serotonin, and dopamine. Reduced gray matter volume in certain brain regions has also been described. A genetic predisposition is suggested, with approximately one third of patients having an affected first-degree relative; candidate genes include those related to serotonin and dopamine pathways. Psychological factors are common, and many patients have comorbid psychiatric conditions. In susceptible individuals, fibromyalgia may be triggered by physical trauma, illness, inflammation, or chronic stress, with hypothalamic–pituitary–adrenal axis dysfunction often preceding symptom onset.
Diagnosis Signs And Symptoms
Patients report widespread pain involving both sides of the body, above and below the waist, and the axial skeleton, persisting for more than three months. Common associated symptoms include morning stiffness, generalized weakness, persistent fatigue not relieved by rest, sleep disturbance, muscle spasms, paresthesias, impaired concentration or memory, headaches, gastrointestinal discomfort relieved by bowel movements, pelvic or bladder discomfort, jaw or facial pain, and mood disturbances. Physical examination is typically unremarkable aside from tenderness at characteristic sites.
Essential Workup
History is the most important diagnostic tool. In the emergency department, evaluation is primarily focused on distinguishing chronic fibromyalgia pain from acute pain due to trauma, injury, or new medical conditions. If diagnostic confirmation is required, American College of Rheumatology criteria may be applied, including widespread pain for at least three months with either tender point assessment or use of the Widespread Pain Index (WPI) and Symptom Severity (SS) scale. Tender points are classically located at bilateral sites including the occiput, low cervical region, trapezius, supraspinatus, second rib, lateral epicondyle, gluteal region, greater trochanter, and medial knee fat pad.
Diagnosis Tests And Interpretation
Laboratory testing is not diagnostic and should be reserved for exclusion of alternative or acute conditions. Studies may include CBC, basic chemistries, ESR, muscle enzymes, thyroid function tests, and urinalysis when clinically indicated. Imaging and invasive procedures are not routinely useful and should only be performed to evaluate suspected alternative diagnoses.
Differential Diagnosis
Conditions to consider include myofascial pain syndrome, chronic fatigue syndrome, major depression, polymyalgia rheumatica, Lyme disease, hypothyroidism, collagen vascular diseases, electrolyte abnormalities, metabolic or drug-induced myopathies, osteomalacia, spondyloarthropathies, interstitial cystitis, and urinary tract infection.
Treatment
Emergency department management focuses on patient education, reassurance, and exclusion of acute pathology. Patients should be informed that fibromyalgia is chronic but not life-threatening, deforming, or associated with reduced life expectancy. Long-term management aims to reduce pain and improve function and requires outpatient follow-up. Pharmacologic therapy with central nervous system–acting agents is most effective, including gabapentin, pregabalin, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors. Opioids are not recommended and may worsen long-term pain. NSAIDs and corticosteroids have not demonstrated benefit. Local injections into tender points remain controversial due to lack of strong evidence.
Medication
Acetaminophen 650 mg PO q4h. Amitriptyline 25–50 mg PO at bedtime. Cyclobenzaprine 5–10 mg PO TID. Duloxetine 60 mg PO daily or BID. Gabapentin starting at 300 mg PO TID with gradual titration. Milnacipran starting at 12.5 mg daily and titrated to 50–100 mg PO BID. Pregabalin starting at 50 mg PO TID, titrated to a maximum of 450 mg/day. Tramadol may be used as an adjunct in selected patients.
Follow Up Disposition
Patients with uncomplicated fibromyalgia can be discharged with outpatient follow-up. Admission is reserved for those with serious underlying disease, intractable pain, immunocompromised status, or suicidal ideation.
Follow Up Recommendations
Patients should be referred to a primary care provider, rheumatologist, or pain specialist for ongoing management. Gradual aerobic exercise programs are encouraged, along with sleep hygiene measures such as regular sleep schedules and avoidance of caffeine in the evening. Stress management strategies and cognitive-behavioral therapy can provide sustained benefit.
Practical Takeaways And Frequent Missteps
Careful distinction between chronic fibromyalgia symptoms and new or acute pain is essential, as patients may still develop unrelated emergent conditions. Avoid unnecessary diagnostic testing once acute pathology has been excluded, and avoid opioid prescribing, which may worsen long-term outcomes.
Basics Description
Fibromyalgia is a nonarticular, noninflammatory syndrome characterized by chronic, widespread musculoskeletal pain and heightened pain sensitivity to normally nonpainful stimuli (allodynia). It is more common in females and is associated with diffuse tenderness at multiple sites, fatigue, sleep disturbance, muscle stiffness, and cognitive difficulties involving attention and memory. Physical examination findings are often limited. Fibromyalgia is not a diagnosis of exclusion and may coexist with other rheumatologic or medical conditions.
Etiology
The underlying mechanism is believed to involve central pain processing abnormalities, with increased activity of pronociceptive pathways and reduced activity of antinociceptive pathways in the brain and spinal cord. Identified contributors include elevated substance P levels and decreased biogenic amines such as norepinephrine, serotonin, and dopamine. Reduced gray matter volume in certain brain regions has also been described. A genetic predisposition is suggested, with approximately one third of patients having an affected first-degree relative; candidate genes include those related to serotonin and dopamine pathways. Psychological factors are common, and many patients have comorbid psychiatric conditions. In susceptible individuals, fibromyalgia may be triggered by physical trauma, illness, inflammation, or chronic stress, with hypothalamic–pituitary–adrenal axis dysfunction often preceding symptom onset.
Diagnosis Signs And Symptoms
Patients report widespread pain involving both sides of the body, above and below the waist, and the axial skeleton, persisting for more than three months. Common associated symptoms include morning stiffness, generalized weakness, persistent fatigue not relieved by rest, sleep disturbance, muscle spasms, paresthesias, impaired concentration or memory, headaches, gastrointestinal discomfort relieved by bowel movements, pelvic or bladder discomfort, jaw or facial pain, and mood disturbances. Physical examination is typically unremarkable aside from tenderness at characteristic sites.
Essential Workup
History is the most important diagnostic tool. In the emergency department, evaluation is primarily focused on distinguishing chronic fibromyalgia pain from acute pain due to trauma, injury, or new medical conditions. If diagnostic confirmation is required, American College of Rheumatology criteria may be applied, including widespread pain for at least three months with either tender point assessment or use of the Widespread Pain Index (WPI) and Symptom Severity (SS) scale. Tender points are classically located at bilateral sites including the occiput, low cervical region, trapezius, supraspinatus, second rib, lateral epicondyle, gluteal region, greater trochanter, and medial knee fat pad.
Diagnosis Tests And Interpretation
Laboratory testing is not diagnostic and should be reserved for exclusion of alternative or acute conditions. Studies may include CBC, basic chemistries, ESR, muscle enzymes, thyroid function tests, and urinalysis when clinically indicated. Imaging and invasive procedures are not routinely useful and should only be performed to evaluate suspected alternative diagnoses.
Differential Diagnosis
Conditions to consider include myofascial pain syndrome, chronic fatigue syndrome, major depression, polymyalgia rheumatica, Lyme disease, hypothyroidism, collagen vascular diseases, electrolyte abnormalities, metabolic or drug-induced myopathies, osteomalacia, spondyloarthropathies, interstitial cystitis, and urinary tract infection.
Treatment
Emergency department management focuses on patient education, reassurance, and exclusion of acute pathology. Patients should be informed that fibromyalgia is chronic but not life-threatening, deforming, or associated with reduced life expectancy. Long-term management aims to reduce pain and improve function and requires outpatient follow-up. Pharmacologic therapy with central nervous system–acting agents is most effective, including gabapentin, pregabalin, tricyclic antidepressants, and serotonin–norepinephrine reuptake inhibitors. Opioids are not recommended and may worsen long-term pain. NSAIDs and corticosteroids have not demonstrated benefit. Local injections into tender points remain controversial due to lack of strong evidence.
Medication
Acetaminophen 650 mg PO q4h. Amitriptyline 25–50 mg PO at bedtime. Cyclobenzaprine 5–10 mg PO TID. Duloxetine 60 mg PO daily or BID. Gabapentin starting at 300 mg PO TID with gradual titration. Milnacipran starting at 12.5 mg daily and titrated to 50–100 mg PO BID. Pregabalin starting at 50 mg PO TID, titrated to a maximum of 450 mg/day. Tramadol may be used as an adjunct in selected patients.
Follow Up Disposition
Patients with uncomplicated fibromyalgia can be discharged with outpatient follow-up. Admission is reserved for those with serious underlying disease, intractable pain, immunocompromised status, or suicidal ideation.
Follow Up Recommendations
Patients should be referred to a primary care provider, rheumatologist, or pain specialist for ongoing management. Gradual aerobic exercise programs are encouraged, along with sleep hygiene measures such as regular sleep schedules and avoidance of caffeine in the evening. Stress management strategies and cognitive-behavioral therapy can provide sustained benefit.
Practical Takeaways And Frequent Missteps
Careful distinction between chronic fibromyalgia symptoms and new or acute pain is essential, as patients may still develop unrelated emergent conditions. Avoid unnecessary diagnostic testing once acute pathology has been excluded, and avoid opioid prescribing, which may worsen long-term outcomes.

- Published on
Emergency And Acute Medicine – Flail Chest
Basics Description
Flail chest is defined by a free-floating segment of the chest wall created when three or more adjacent ribs are fractured in two or more locations. It may also occur with rib fractures combined with sternal fractures or costochondral separations. The unstable segment characteristically moves inward during inspiration and outward during expiration (paradoxical motion). The primary clinical problem in flail chest is not the chest wall instability itself but the associated pulmonary contusion, which leads to impaired gas exchange rather than altered ventilatory mechanics.
Etiology
Flail chest results from high-energy blunt thoracic trauma, most commonly motor vehicle collisions, falls from height, assaults, or missile injuries. Rib fractures usually occur at the point of impact or at the posterior rib angle, with ribs 4–9 most frequently involved. Energy transfer to adjacent lung tissue disrupts the alveolocapillary membrane, producing pulmonary contusion, ventilation–perfusion mismatch, arteriovenous shunting, hypoxemia, and potential respiratory failure.
Pediatric considerations: Children have more elastic chest walls, making rib fractures less common; when present, they imply severe energy transfer.
Geriatric considerations: Older adults are more susceptible to rib fractures, often from low-energy mechanisms, and outcomes are worsened by osteoporosis.
Diagnosis Signs And Symptoms
History typically includes significant blunt chest trauma with localized chest wall pain that worsens with inspiration, coughing, or movement. Patients may report pleuritic chest pain, dyspnea, or hemoptysis.
Physical examination may reveal paradoxical chest wall motion, which can be subtle or absent early due to muscle spasm and splinting. Additional findings include multiple rib fractures with tenderness, crepitus, ecchymosis, edema, and bony step-offs. Respiratory findings range from tachypnea and splinting respirations to cyanosis, hypoxia, tachycardia, hypotension, and progressive crackles or diminished breath sounds as pulmonary contusion evolves.
Essential Workup
Diagnosis is primarily clinical and supported by imaging. Continuous monitoring of oxygenation and respiratory status is essential.
Diagnosis Tests And Interpretation
Laboratory studies may include arterial blood gas analysis demonstrating hypoxemia and an elevated alveolar–arterial gradient.
Chest radiography may show rib fractures and associated intrathoracic injuries such as pneumothorax, hemothorax, pneumomediastinum, or pulmonary contusion, which often becomes radiographically apparent within 6–12 hours.
Thoracic CT is more sensitive than plain radiographs and frequently identifies additional rib fractures and associated injuries not seen on initial chest X-ray.
Differential Diagnosis
Chest wall contusion, intercostal muscle strain, costochondral separation, sternal fracture or dislocation, and pulmonary conditions such as ARDS, pulmonary laceration, embolism, heart failure, pneumonia, or noncardiogenic pulmonary edema.
Treatment
Prehospital care includes positioning the patient with the injured side down to stabilize the chest wall and improve ventilation of the unaffected lung. Patients with significant thoracic trauma should be transported to a trauma center.
Initial stabilization follows airway, breathing, and circulation priorities with supplemental oxygen, IV access, cardiac monitoring, and pulse oximetry. Endotracheal intubation is indicated for severe hypoxemia, significant underlying lung disease, or impending respiratory failure.
Emergency department management focuses on maintaining adequate oxygenation and ventilation. High-flow oxygen is first-line in alert patients; noninvasive positive pressure ventilation may be used if oxygenation remains inadequate. Early invasive mechanical ventilation is indicated when noninvasive measures fail, providing physiologic internal stabilization of the flail segment. External fixation of the chest wall is not recommended.
Aggressive pain control is critical to prevent hypoventilation, atelectasis, and pneumonia. Intercostal nerve blocks with bupivacaine can provide effective temporary analgesia. Careful fluid management is essential to avoid worsening pulmonary edema in the presence of contusion. Prophylactic antibiotics are not indicated.
Medication
Analgesia may include acetaminophen–opioid combinations, IV or oral opioids such as morphine or hydromorphone, patient-controlled analgesia, and regional techniques. Bupivacaine 0.5% may be used for intercostal nerve blocks. Thoracic epidural analgesia should be considered in patients with severe pain or opioid-related hypoventilation. NSAIDs are generally discouraged due to bleeding risk. Acetaminophen dosing should not exceed recommended daily limits.
Follow Up Disposition
All patients with flail chest require admission to a critical care or closely monitored setting for respiratory observation and pain management. Discharge from the emergency department is not appropriate.
Clinical Takeaways And Common Pitfalls
Early and adequate pain control is essential to prevent respiratory complications. Always assess for associated injuries, particularly pulmonary contusion and pneumothorax. Elderly patients have markedly worse outcomes and require vigilant monitoring and aggressive supportive care.
Basics Description
Flail chest is defined by a free-floating segment of the chest wall created when three or more adjacent ribs are fractured in two or more locations. It may also occur with rib fractures combined with sternal fractures or costochondral separations. The unstable segment characteristically moves inward during inspiration and outward during expiration (paradoxical motion). The primary clinical problem in flail chest is not the chest wall instability itself but the associated pulmonary contusion, which leads to impaired gas exchange rather than altered ventilatory mechanics.
Etiology
Flail chest results from high-energy blunt thoracic trauma, most commonly motor vehicle collisions, falls from height, assaults, or missile injuries. Rib fractures usually occur at the point of impact or at the posterior rib angle, with ribs 4–9 most frequently involved. Energy transfer to adjacent lung tissue disrupts the alveolocapillary membrane, producing pulmonary contusion, ventilation–perfusion mismatch, arteriovenous shunting, hypoxemia, and potential respiratory failure.
Pediatric considerations: Children have more elastic chest walls, making rib fractures less common; when present, they imply severe energy transfer.
Geriatric considerations: Older adults are more susceptible to rib fractures, often from low-energy mechanisms, and outcomes are worsened by osteoporosis.
Diagnosis Signs And Symptoms
History typically includes significant blunt chest trauma with localized chest wall pain that worsens with inspiration, coughing, or movement. Patients may report pleuritic chest pain, dyspnea, or hemoptysis.
Physical examination may reveal paradoxical chest wall motion, which can be subtle or absent early due to muscle spasm and splinting. Additional findings include multiple rib fractures with tenderness, crepitus, ecchymosis, edema, and bony step-offs. Respiratory findings range from tachypnea and splinting respirations to cyanosis, hypoxia, tachycardia, hypotension, and progressive crackles or diminished breath sounds as pulmonary contusion evolves.
Essential Workup
Diagnosis is primarily clinical and supported by imaging. Continuous monitoring of oxygenation and respiratory status is essential.
Diagnosis Tests And Interpretation
Laboratory studies may include arterial blood gas analysis demonstrating hypoxemia and an elevated alveolar–arterial gradient.
Chest radiography may show rib fractures and associated intrathoracic injuries such as pneumothorax, hemothorax, pneumomediastinum, or pulmonary contusion, which often becomes radiographically apparent within 6–12 hours.
Thoracic CT is more sensitive than plain radiographs and frequently identifies additional rib fractures and associated injuries not seen on initial chest X-ray.
Differential Diagnosis
Chest wall contusion, intercostal muscle strain, costochondral separation, sternal fracture or dislocation, and pulmonary conditions such as ARDS, pulmonary laceration, embolism, heart failure, pneumonia, or noncardiogenic pulmonary edema.
Treatment
Prehospital care includes positioning the patient with the injured side down to stabilize the chest wall and improve ventilation of the unaffected lung. Patients with significant thoracic trauma should be transported to a trauma center.
Initial stabilization follows airway, breathing, and circulation priorities with supplemental oxygen, IV access, cardiac monitoring, and pulse oximetry. Endotracheal intubation is indicated for severe hypoxemia, significant underlying lung disease, or impending respiratory failure.
Emergency department management focuses on maintaining adequate oxygenation and ventilation. High-flow oxygen is first-line in alert patients; noninvasive positive pressure ventilation may be used if oxygenation remains inadequate. Early invasive mechanical ventilation is indicated when noninvasive measures fail, providing physiologic internal stabilization of the flail segment. External fixation of the chest wall is not recommended.
Aggressive pain control is critical to prevent hypoventilation, atelectasis, and pneumonia. Intercostal nerve blocks with bupivacaine can provide effective temporary analgesia. Careful fluid management is essential to avoid worsening pulmonary edema in the presence of contusion. Prophylactic antibiotics are not indicated.
Medication
Analgesia may include acetaminophen–opioid combinations, IV or oral opioids such as morphine or hydromorphone, patient-controlled analgesia, and regional techniques. Bupivacaine 0.5% may be used for intercostal nerve blocks. Thoracic epidural analgesia should be considered in patients with severe pain or opioid-related hypoventilation. NSAIDs are generally discouraged due to bleeding risk. Acetaminophen dosing should not exceed recommended daily limits.
Follow Up Disposition
All patients with flail chest require admission to a critical care or closely monitored setting for respiratory observation and pain management. Discharge from the emergency department is not appropriate.
Clinical Takeaways And Common Pitfalls
Early and adequate pain control is essential to prevent respiratory complications. Always assess for associated injuries, particularly pulmonary contusion and pneumothorax. Elderly patients have markedly worse outcomes and require vigilant monitoring and aggressive supportive care.


- Published on
Emergency And Acute Medicine – Foot Fracture
Basics Description
Foot fractures involve injury to the tarsal bones or metatarsals, including the calcaneus, talus, navicular, cuboid, cuneiforms, and metatarsals.
Etiology
The most common foot fractures involve the metatarsals and phalanges. The calcaneus is the most frequently fractured tarsal bone.
Calcaneus fractures usually result from high-velocity axial compression to the heel; approximately 75% are intra-articular and 50% are associated with other injuries, including spinal fractures, lower extremity trauma, bilateral involvement, or open wounds.
Metatarsal fractures may result from stress, twisting injuries, or direct trauma. The first metatarsal is often injured by direct force. The second and third metatarsals are most commonly affected by stress or twisting injuries. The fifth metatarsal commonly sustains avulsion fractures at the proximal apophysis (dancer’s fracture) or a Jones fracture at the metaphyseal–diaphyseal junction from inversion injury.
Talus fractures are typically caused by dorsiflexion with axial loading. Navicular fractures result from axial compression or stress. Cuboid and cuneiform fractures are rare and usually occur with associated injuries, particularly tarsometatarsal (Lisfranc) injuries. Lisfranc injuries are high-energy injuries caused by axial load on a plantar-flexed foot or forced eversion and are frequently missed on initial evaluation.
Pediatric considerations include a predominance of metatarsal fractures, often from direct trauma, with physeal injury possible. Calcaneal fractures in children are less commonly intra-articular and less often associated with spinal injury.
Diagnosis Signs And Symptoms
History usually reveals trauma; stress fractures may present with progressive pain related to repetitive activity.
Physical examination may show ecchymosis, swelling, deformity, localized tenderness, pain with weight bearing, or joint instability.
Essential Workup
A focused extremity examination is required to assess neurovascular status, skin integrity, swelling, deformity, and function. In suspected calcaneal fractures, evaluation of the spine is essential due to the risk of associated injury. Standard anteroposterior, lateral, and oblique foot radiographs are required.
Diagnosis Tests And Interpretation
Imaging may require special views depending on the suspected injury. Lisfranc injuries may require weight-bearing stress views, MRI for ligamentous assessment, or CT. Talar fractures may require oblique views or CT. Calcaneal fractures require axial views, with a Böhler angle less than 20° suggesting compression fracture, and often CT for further definition. Lumbar spine imaging is recommended in calcaneal fractures. Stress fractures may not be visible on initial radiographs and may require delayed imaging, bone scan, or CT.
Complications to assess include compartment syndrome, nonunion, avascular necrosis (especially with talar neck fractures), and sural nerve injury with calcaneal fractures.
Differential Diagnosis
Ankle sprain, foot contusion, talar dome injury, and Freiberg disease may mimic foot fractures.
Treatment
Prehospital care includes ice application, immobilization, and spinal precautions when calcaneal fracture is suspected.
Initial stabilization prioritizes management of associated injuries.
Emergency department management includes airway, breathing, and circulation assessment, neurovascular evaluation, prompt reduction of dislocations with reassessment, immobilization in a bulky splint, elevation, ice, and crutches. Circumferential casting should be delayed until swelling subsides. Pain control is essential. Compartment syndrome should be suspected with severe pain, swelling, or pain on passive toe movement. Early orthopedic consultation is required for displaced, open, or midfoot fractures.
Medication
Analgesics and sedatives may be used as indicated for pain control and procedural sedation. Antibiotics are indicated for open fractures.
Follow Up Disposition
Admission criteria include open fractures, compartment syndrome, neurovascular compromise, or need for immediate operative fixation.
Discharge criteria include stable patients with isolated, nondisplaced metatarsal fractures who can be managed with immobilization and close orthopedic follow-up.
Clinical Insights And Frequent Errors
Calcaneal fractures should prompt evaluation for spinal injury. Lisfranc injuries are commonly missed and require a high index of suspicion. Persistent pain or swelling despite normal initial imaging warrants reevaluation for occult or stress fractures.
Basics Description
Foot fractures involve injury to the tarsal bones or metatarsals, including the calcaneus, talus, navicular, cuboid, cuneiforms, and metatarsals.
Etiology
The most common foot fractures involve the metatarsals and phalanges. The calcaneus is the most frequently fractured tarsal bone.
Calcaneus fractures usually result from high-velocity axial compression to the heel; approximately 75% are intra-articular and 50% are associated with other injuries, including spinal fractures, lower extremity trauma, bilateral involvement, or open wounds.
Metatarsal fractures may result from stress, twisting injuries, or direct trauma. The first metatarsal is often injured by direct force. The second and third metatarsals are most commonly affected by stress or twisting injuries. The fifth metatarsal commonly sustains avulsion fractures at the proximal apophysis (dancer’s fracture) or a Jones fracture at the metaphyseal–diaphyseal junction from inversion injury.
Talus fractures are typically caused by dorsiflexion with axial loading. Navicular fractures result from axial compression or stress. Cuboid and cuneiform fractures are rare and usually occur with associated injuries, particularly tarsometatarsal (Lisfranc) injuries. Lisfranc injuries are high-energy injuries caused by axial load on a plantar-flexed foot or forced eversion and are frequently missed on initial evaluation.
Pediatric considerations include a predominance of metatarsal fractures, often from direct trauma, with physeal injury possible. Calcaneal fractures in children are less commonly intra-articular and less often associated with spinal injury.
Diagnosis Signs And Symptoms
History usually reveals trauma; stress fractures may present with progressive pain related to repetitive activity.
Physical examination may show ecchymosis, swelling, deformity, localized tenderness, pain with weight bearing, or joint instability.
Essential Workup
A focused extremity examination is required to assess neurovascular status, skin integrity, swelling, deformity, and function. In suspected calcaneal fractures, evaluation of the spine is essential due to the risk of associated injury. Standard anteroposterior, lateral, and oblique foot radiographs are required.
Diagnosis Tests And Interpretation
Imaging may require special views depending on the suspected injury. Lisfranc injuries may require weight-bearing stress views, MRI for ligamentous assessment, or CT. Talar fractures may require oblique views or CT. Calcaneal fractures require axial views, with a Böhler angle less than 20° suggesting compression fracture, and often CT for further definition. Lumbar spine imaging is recommended in calcaneal fractures. Stress fractures may not be visible on initial radiographs and may require delayed imaging, bone scan, or CT.
Complications to assess include compartment syndrome, nonunion, avascular necrosis (especially with talar neck fractures), and sural nerve injury with calcaneal fractures.
Differential Diagnosis
Ankle sprain, foot contusion, talar dome injury, and Freiberg disease may mimic foot fractures.
Treatment
Prehospital care includes ice application, immobilization, and spinal precautions when calcaneal fracture is suspected.
Initial stabilization prioritizes management of associated injuries.
Emergency department management includes airway, breathing, and circulation assessment, neurovascular evaluation, prompt reduction of dislocations with reassessment, immobilization in a bulky splint, elevation, ice, and crutches. Circumferential casting should be delayed until swelling subsides. Pain control is essential. Compartment syndrome should be suspected with severe pain, swelling, or pain on passive toe movement. Early orthopedic consultation is required for displaced, open, or midfoot fractures.
Medication
Analgesics and sedatives may be used as indicated for pain control and procedural sedation. Antibiotics are indicated for open fractures.
Follow Up Disposition
Admission criteria include open fractures, compartment syndrome, neurovascular compromise, or need for immediate operative fixation.
Discharge criteria include stable patients with isolated, nondisplaced metatarsal fractures who can be managed with immobilization and close orthopedic follow-up.
Clinical Insights And Frequent Errors
Calcaneal fractures should prompt evaluation for spinal injury. Lisfranc injuries are commonly missed and require a high index of suspicion. Persistent pain or swelling despite normal initial imaging warrants reevaluation for occult or stress fractures.


- Published on
Emergency And Acute Medicine - Extremity Trauma, Penetrating
Condition overview
Penetrating extremity trauma refers to injuries in which an object breaches the skin and underlying tissues of an arm or leg. These injuries range from minor puncture wounds to severe limb-threatening trauma involving vascular, neurologic, musculoskeletal, or compartment compromise.
Mechanisms of injury
Common mechanisms include stab or puncture wounds, gunshot wounds, lacerations, animal or human bites, and high-pressure injection injuries. High-muzzle-velocity gunshot wounds are particularly destructive, as the shock wave may cause extensive tissue damage beyond the visible wound tract, often with more damage at the exit wound than the entry site.
Clinical presentation
Findings may include entry and exit wounds, lacerations, or punctures. Vascular injury should be suspected with decreased or absent distal pulses, ischemic changes, expanding hematoma, or a bruit or thrill over the injury; the presence of a distal pulse does not exclude proximal vascular damage. Neurologic injury may present with paresthesias, weakness, or loss of sensation distal to the wound. Musculoskeletal injury may manifest as deformity, joint effusion, ligamentous laxity, or limited range of motion. Compartment syndrome is suggested by severe, constant pain, pain with passive stretch, compartment tenderness, weakness, and sensory deficits, with pallor and pulselessness being late findings.
History and examination priorities
Key historical elements include the mechanism and timing of injury, circumstances such as assault or self-harm, and comorbid conditions including diabetes, immunosuppression, peripheral vascular disease, valvular heart disease, or asplenia. Examination should document wound location, size, depth, and shape, and assess for exit wounds. Distal pulses should be compared bilaterally by palpation and Doppler. Capillary refill, motor and sensory function, joint stability, and signs of compartment syndrome must be evaluated. The wound should be carefully inspected for foreign bodies.
Diagnostic evaluation
The physical examination guides further testing. Acute wound cultures are not routinely indicated. Plain radiographs with at least anteroposterior and lateral views are used to detect fractures or radiopaque foreign bodies. Ultrasound, fluoroscopy, or CT may help identify radiolucent foreign bodies. When vascular injury is suspected and immediate surgery is not required, arteriography may be indicated.
Management principles
Prehospital care focuses on hemorrhage control with direct pressure, limb elevation, pain control, neurovascular assessment, and stabilization of impaled objects in place. In the emergency department, airway and hemodynamic stabilization take priority. The wound should be fully exposed, constricting items removed, and bleeding controlled with direct pressure; blind clamping and prolonged tourniquet use are discouraged. After a full neurologic exam, pain control is provided. Visible debris and devitalized tissue are removed, with copious high-pressure saline irrigation as the cornerstone of wound care. Tetanus prophylaxis is essential.
Stab and gunshot wounds should receive a single dose of cefazolin in the emergency department. Extremities should be immobilized when vascular injury, fracture, tendon injury, or joint violation is suspected. Loss of distal pulse or signs of ischemia mandate emergent surgical consultation without delay for imaging. Clean lacerations seen within 6–8 hours may be closed primarily; puncture wounds and gunshot wounds should not be closed primarily, with delayed primary closure considered for contaminated or older wounds.
Special considerations
Plantar puncture wounds require careful inspection and removal of foreign material; aggressive probing or irrigation may worsen contamination. Prophylactic antibiotics are generally not recommended unless the patient is diabetic, immunocompromised, or the wound is highly contaminated or delayed in presentation. High-pressure injection injuries of the hand require immediate orthopedic evaluation, as surface wounds may underestimate deep tissue involvement. Small inert foreign bodies, including bullets, may be left in place if not near vital structures, whereas organic material should always be removed.
Disposition and follow-up
Admission and emergent surgical consultation are required for suspected vascular injury, compartment syndrome, joint penetration, high-velocity gunshot wounds, or contaminated wounds in high-risk patients. Stable patients without indications for surgery may be discharged after appropriate wound care with instructions for elevation, wound hygiene, and close follow-up within 24–48 hours.
Key clinical lessons
A normal distal pulse does not exclude significant vascular injury. High-pressure hand injuries and plantar puncture wounds are commonly underestimated. Failure of a puncture wound infection to improve with antibiotics should prompt concern for a retained foreign body.
Condition overview
Penetrating extremity trauma refers to injuries in which an object breaches the skin and underlying tissues of an arm or leg. These injuries range from minor puncture wounds to severe limb-threatening trauma involving vascular, neurologic, musculoskeletal, or compartment compromise.
Mechanisms of injury
Common mechanisms include stab or puncture wounds, gunshot wounds, lacerations, animal or human bites, and high-pressure injection injuries. High-muzzle-velocity gunshot wounds are particularly destructive, as the shock wave may cause extensive tissue damage beyond the visible wound tract, often with more damage at the exit wound than the entry site.
Clinical presentation
Findings may include entry and exit wounds, lacerations, or punctures. Vascular injury should be suspected with decreased or absent distal pulses, ischemic changes, expanding hematoma, or a bruit or thrill over the injury; the presence of a distal pulse does not exclude proximal vascular damage. Neurologic injury may present with paresthesias, weakness, or loss of sensation distal to the wound. Musculoskeletal injury may manifest as deformity, joint effusion, ligamentous laxity, or limited range of motion. Compartment syndrome is suggested by severe, constant pain, pain with passive stretch, compartment tenderness, weakness, and sensory deficits, with pallor and pulselessness being late findings.
History and examination priorities
Key historical elements include the mechanism and timing of injury, circumstances such as assault or self-harm, and comorbid conditions including diabetes, immunosuppression, peripheral vascular disease, valvular heart disease, or asplenia. Examination should document wound location, size, depth, and shape, and assess for exit wounds. Distal pulses should be compared bilaterally by palpation and Doppler. Capillary refill, motor and sensory function, joint stability, and signs of compartment syndrome must be evaluated. The wound should be carefully inspected for foreign bodies.
Diagnostic evaluation
The physical examination guides further testing. Acute wound cultures are not routinely indicated. Plain radiographs with at least anteroposterior and lateral views are used to detect fractures or radiopaque foreign bodies. Ultrasound, fluoroscopy, or CT may help identify radiolucent foreign bodies. When vascular injury is suspected and immediate surgery is not required, arteriography may be indicated.
Management principles
Prehospital care focuses on hemorrhage control with direct pressure, limb elevation, pain control, neurovascular assessment, and stabilization of impaled objects in place. In the emergency department, airway and hemodynamic stabilization take priority. The wound should be fully exposed, constricting items removed, and bleeding controlled with direct pressure; blind clamping and prolonged tourniquet use are discouraged. After a full neurologic exam, pain control is provided. Visible debris and devitalized tissue are removed, with copious high-pressure saline irrigation as the cornerstone of wound care. Tetanus prophylaxis is essential.
Stab and gunshot wounds should receive a single dose of cefazolin in the emergency department. Extremities should be immobilized when vascular injury, fracture, tendon injury, or joint violation is suspected. Loss of distal pulse or signs of ischemia mandate emergent surgical consultation without delay for imaging. Clean lacerations seen within 6–8 hours may be closed primarily; puncture wounds and gunshot wounds should not be closed primarily, with delayed primary closure considered for contaminated or older wounds.
Special considerations
Plantar puncture wounds require careful inspection and removal of foreign material; aggressive probing or irrigation may worsen contamination. Prophylactic antibiotics are generally not recommended unless the patient is diabetic, immunocompromised, or the wound is highly contaminated or delayed in presentation. High-pressure injection injuries of the hand require immediate orthopedic evaluation, as surface wounds may underestimate deep tissue involvement. Small inert foreign bodies, including bullets, may be left in place if not near vital structures, whereas organic material should always be removed.
Disposition and follow-up
Admission and emergent surgical consultation are required for suspected vascular injury, compartment syndrome, joint penetration, high-velocity gunshot wounds, or contaminated wounds in high-risk patients. Stable patients without indications for surgery may be discharged after appropriate wound care with instructions for elevation, wound hygiene, and close follow-up within 24–48 hours.
Key clinical lessons
A normal distal pulse does not exclude significant vascular injury. High-pressure hand injuries and plantar puncture wounds are commonly underestimated. Failure of a puncture wound infection to improve with antibiotics should prompt concern for a retained foreign body.
- Published on
Emergency And Acute Medicine – Shaft and Distal Forearm Fractures
Basics Description
Forearm shaft fractures may involve one or both bones and are frequently displaced due to muscular contraction. These injuries may be associated with joint dislocations, including Galeazzi fractures, which involve a distal radius fracture with distal radioulnar joint dislocation, and Monteggia fractures, which involve a proximal ulna fracture with radial head dislocation.
Distal forearm fractures include several classic patterns. Colles fractures result from hyperextension with dorsal displacement of the distal radius fragment and are often associated with ulnar styloid injury. Smith fractures occur with hyperflexion and result in volar displacement. Barton fractures are intra-articular fractures of the dorsal rim of the distal radius and may involve carpal dislocation. Hutchinson fractures involve the radial styloid.
In children, shaft fractures commonly present as torus fractures, greenstick fractures, or plastic deformities. Distal fractures in pediatric patients frequently involve Salter–Harris growth plate injuries.
Etiology
Common mechanisms include direct blows to the forearm, longitudinal compression such as falls on an outstretched hand, horizontal force, and excessive pronation, supination, hyperextension, or hyperflexion.
Diagnosis Signs And Symptoms
Patients typically present with pain, deformity, swelling, and limited function. History should include mechanism of injury, hand dominance, occupational or repetitive stress factors, and prior bone disease or fractures.
Physical examination focuses on deformity, tenderness, crepitus, edema, ecchymosis, joint effusions at the elbow or wrist, abnormal mobility, and careful assessment of neurovascular status. Findings concerning for compartment syndrome require urgent attention.
Essential Workup
Suspected forearm fractures require anteroposterior and lateral radiographs that include the wrist, forearm, and elbow to evaluate joints above and below the injury.
Diagnosis Tests And Interpretation
Imaging may include CT for complex or intra-articular fractures. Compartment pressure measurement is indicated when compartment syndrome is suspected. Laboratory studies are generally reserved for preoperative evaluation.
Differential Diagnosis
Consider muscle or ligament injury, elbow or wrist dislocations, contusions or hematomas, infection, tumors, osteomyelitis, vascular or neurologic injury, arthritis, and in children, normal growth plates or nutrient vessels that may mimic fractures.
Treatment
Prehospital care includes elevation, splinting, and immobilization of the elbow and wrist. Open fractures should be covered with sterile dressings and not reduced in the field.
In the emergency department, nondisplaced shaft fractures are treated with long-arm splinting and orthopedic referral. Displaced shaft fractures often require orthopedic consultation and operative fixation.
Nondisplaced distal fractures are managed with sugar-tong or anteroposterior splints and referral. Simple Colles or Smith fractures may be reduced in the emergency department and splinted, while complicated patterns require orthopedic consultation. Barton and Hutchinson fractures are splinted and referred, with operative management as needed.
Open fractures require antibiotics, tetanus prophylaxis, splinting, and immediate orthopedic consultation. Any fracture associated with neurovascular compromise or compartment syndrome requires urgent specialist evaluation.
In pediatric patients, minimally angulated torus or greenstick fractures may be splinted and referred, while plastic deformities and Salter–Harris fractures require orthopedic consultation.
Medication
Pain control is achieved with acetaminophen, NSAIDs, or opioids as appropriate. Open fractures require parenteral antibiotics such as first-generation cephalosporins, with additional coverage for contaminated wounds. Tetanus prophylaxis should be updated as indicated.
Follow Up Disposition
Admission is required for open fractures, compartment syndrome, neurovascular compromise, fractures requiring immediate surgery, or suspected nonaccidental trauma.
Discharge is appropriate after adequate reduction and immobilization, confirmation of intact neurovascular status, effective pain control, and ensured orthopedic follow-up with clear splint and cast care instructions.
Clinical Insights And Common Pitfalls
Always evaluate for a second fracture or associated joint dislocation. Reassess neurovascular status frequently and maintain a high index of suspicion for evolving compartment syndrome.
Basics Description
Forearm shaft fractures may involve one or both bones and are frequently displaced due to muscular contraction. These injuries may be associated with joint dislocations, including Galeazzi fractures, which involve a distal radius fracture with distal radioulnar joint dislocation, and Monteggia fractures, which involve a proximal ulna fracture with radial head dislocation.
Distal forearm fractures include several classic patterns. Colles fractures result from hyperextension with dorsal displacement of the distal radius fragment and are often associated with ulnar styloid injury. Smith fractures occur with hyperflexion and result in volar displacement. Barton fractures are intra-articular fractures of the dorsal rim of the distal radius and may involve carpal dislocation. Hutchinson fractures involve the radial styloid.
In children, shaft fractures commonly present as torus fractures, greenstick fractures, or plastic deformities. Distal fractures in pediatric patients frequently involve Salter–Harris growth plate injuries.
Etiology
Common mechanisms include direct blows to the forearm, longitudinal compression such as falls on an outstretched hand, horizontal force, and excessive pronation, supination, hyperextension, or hyperflexion.
Diagnosis Signs And Symptoms
Patients typically present with pain, deformity, swelling, and limited function. History should include mechanism of injury, hand dominance, occupational or repetitive stress factors, and prior bone disease or fractures.
Physical examination focuses on deformity, tenderness, crepitus, edema, ecchymosis, joint effusions at the elbow or wrist, abnormal mobility, and careful assessment of neurovascular status. Findings concerning for compartment syndrome require urgent attention.
Essential Workup
Suspected forearm fractures require anteroposterior and lateral radiographs that include the wrist, forearm, and elbow to evaluate joints above and below the injury.
Diagnosis Tests And Interpretation
Imaging may include CT for complex or intra-articular fractures. Compartment pressure measurement is indicated when compartment syndrome is suspected. Laboratory studies are generally reserved for preoperative evaluation.
Differential Diagnosis
Consider muscle or ligament injury, elbow or wrist dislocations, contusions or hematomas, infection, tumors, osteomyelitis, vascular or neurologic injury, arthritis, and in children, normal growth plates or nutrient vessels that may mimic fractures.
Treatment
Prehospital care includes elevation, splinting, and immobilization of the elbow and wrist. Open fractures should be covered with sterile dressings and not reduced in the field.
In the emergency department, nondisplaced shaft fractures are treated with long-arm splinting and orthopedic referral. Displaced shaft fractures often require orthopedic consultation and operative fixation.
Nondisplaced distal fractures are managed with sugar-tong or anteroposterior splints and referral. Simple Colles or Smith fractures may be reduced in the emergency department and splinted, while complicated patterns require orthopedic consultation. Barton and Hutchinson fractures are splinted and referred, with operative management as needed.
Open fractures require antibiotics, tetanus prophylaxis, splinting, and immediate orthopedic consultation. Any fracture associated with neurovascular compromise or compartment syndrome requires urgent specialist evaluation.
In pediatric patients, minimally angulated torus or greenstick fractures may be splinted and referred, while plastic deformities and Salter–Harris fractures require orthopedic consultation.
Medication
Pain control is achieved with acetaminophen, NSAIDs, or opioids as appropriate. Open fractures require parenteral antibiotics such as first-generation cephalosporins, with additional coverage for contaminated wounds. Tetanus prophylaxis should be updated as indicated.
Follow Up Disposition
Admission is required for open fractures, compartment syndrome, neurovascular compromise, fractures requiring immediate surgery, or suspected nonaccidental trauma.
Discharge is appropriate after adequate reduction and immobilization, confirmation of intact neurovascular status, effective pain control, and ensured orthopedic follow-up with clear splint and cast care instructions.
Clinical Insights And Common Pitfalls
Always evaluate for a second fracture or associated joint dislocation. Reassess neurovascular status frequently and maintain a high index of suspicion for evolving compartment syndrome.


- Published on
Emergency And Acute Medicine – Foreign Body in the ear
Basics Description
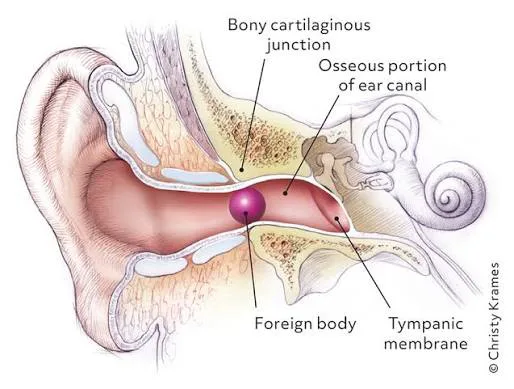
Foreign bodies lodged in the external auditory canal are common, particularly in children younger than 8 years. The canal is a cartilaginous and bony passage lined with highly sensitive periosteum, making removal painful; small children may require procedural sedation or general anesthesia. Foreign bodies often lodge at the junction of the cartilaginous and bony canal or at the isthmus. The canal is innervated by the facial, glossopharyngeal, and vagus nerves.
Inanimate objects often present late because children may delay reporting. The right ear is more commonly involved due to right-handedness. Predisposing factors include cerumen impaction, pica, and psychiatric illness.
Complications include canal laceration, tympanic membrane perforation (often iatrogenic), otitis externa, temporomandibular joint erosion, parapharyngeal abscess, mastoiditis, meningitis, and brain abscess. Button batteries are particularly dangerous due to electrical injury and pressure necrosis, often causing rapid tissue destruction.
Etiology
Children commonly insert beads, stones, paper, seeds, popcorn kernels, beans, toys, and button batteries. Adults more often present with cotton-swab tips, earplugs, insects (cockroaches most common in the US), or concealed illicit drugs.
Diagnosis Signs And Symptoms
Symptoms include unilateral ear pain, fullness, decreased hearing, crying in infants, buzzing or movement sensation with live insects, nausea, dizziness, ipsilateral tearing, itching, bleeding, or purulent discharge.
History should include prior removal attempts and possible trauma.
Physical examination requires careful otoscopy before and after removal to identify the object type, assess swelling risk, evaluate for otitis externa, retained fragments, or tympanic membrane perforation. A bilateral ear exam and inspection of nostrils are essential, especially in children and psychiatric patients. Concerning findings such as vertigo, nystagmus, hearing loss, facial nerve weakness, or severe pain warrant ENT consultation.
Essential Workup
A careful otoscopic examination is the cornerstone. Identify the foreign body and minimize patient discomfort before attempting removal.
Diagnosis Tests And Interpretation
Laboratory studies are not indicated. CT imaging is reserved for suspected infectious, erosive, or intracranial complications. Otomicroscopy may assist when standard techniques fail.
Differential Diagnosis
Cerumen impaction, otitis externa, canal hematoma, granuloma, trauma, tympanic membrane perforation, residual inflammation after self-removal, and tumors.
Treatment
Prehospital care for suspected live insects includes instillation of warm lidocaine or mineral oil to immobilize the insect; field removal attempts are discouraged.
In the emergency department, ensure adequate lighting, proper head immobilization, and analgesia. Lidocaine (1–2%) may be instilled topically or injected into the canal walls. Procedural sedation is recommended for children or uncooperative adults and should be used early to prevent traumatic repeated attempts.
Removal techniques depend on object type: irrigation for non–button battery objects; forceps, hooks, suction, Fogarty catheter, or cyanoacrylate glue for selected cases; acetone for Styrofoam or adhesive materials. Vegetable matter should not be irrigated. Button batteries must never be irrigated and require urgent removal. Live insects should be killed first with lidocaine, alcohol, or mineral oil before extraction. Sharp objects and complicated cases require ENT referral.
Medication
Analgesia or sedation may include fentanyl, ketamine, or midazolam. Topical antibiotic-steroid drops are indicated if canal abrasion or infection is suspected. Oral antibiotics are reserved for tympanic membrane perforation or secondary infection.
Follow Up Disposition
Admission is required for button batteries that cannot be removed.
Discharge is appropriate once the foreign body is removed or if a nonhazardous object cannot be safely removed in the ED.
ENT referral is indicated for failed removal, complications, immunocompromised patients, or significant trauma.
Follow Up Recommendations
Advise patients not to insert objects into the ear. Provide short-term analgesia after traumatic removal. Treat otitis externa with topical antimicrobials. Avoid water submersion if trauma or infection is present and arrange ENT follow-up when indicated.
Key Practice Insights And Avoidable Errors
Early use of procedural sedation improves success and reduces complications. Never irrigate an ear containing a button battery, as this can rapidly worsen tissue necrosis.
Basics Description
Foreign bodies lodged in the external auditory canal are common, particularly in children younger than 8 years. The canal is a cartilaginous and bony passage lined with highly sensitive periosteum, making removal painful; small children may require procedural sedation or general anesthesia. Foreign bodies often lodge at the junction of the cartilaginous and bony canal or at the isthmus. The canal is innervated by the facial, glossopharyngeal, and vagus nerves.
Inanimate objects often present late because children may delay reporting. The right ear is more commonly involved due to right-handedness. Predisposing factors include cerumen impaction, pica, and psychiatric illness.
Complications include canal laceration, tympanic membrane perforation (often iatrogenic), otitis externa, temporomandibular joint erosion, parapharyngeal abscess, mastoiditis, meningitis, and brain abscess. Button batteries are particularly dangerous due to electrical injury and pressure necrosis, often causing rapid tissue destruction.
Etiology
Children commonly insert beads, stones, paper, seeds, popcorn kernels, beans, toys, and button batteries. Adults more often present with cotton-swab tips, earplugs, insects (cockroaches most common in the US), or concealed illicit drugs.
Diagnosis Signs And Symptoms
Symptoms include unilateral ear pain, fullness, decreased hearing, crying in infants, buzzing or movement sensation with live insects, nausea, dizziness, ipsilateral tearing, itching, bleeding, or purulent discharge.
History should include prior removal attempts and possible trauma.
Physical examination requires careful otoscopy before and after removal to identify the object type, assess swelling risk, evaluate for otitis externa, retained fragments, or tympanic membrane perforation. A bilateral ear exam and inspection of nostrils are essential, especially in children and psychiatric patients. Concerning findings such as vertigo, nystagmus, hearing loss, facial nerve weakness, or severe pain warrant ENT consultation.
Essential Workup
A careful otoscopic examination is the cornerstone. Identify the foreign body and minimize patient discomfort before attempting removal.
Diagnosis Tests And Interpretation
Laboratory studies are not indicated. CT imaging is reserved for suspected infectious, erosive, or intracranial complications. Otomicroscopy may assist when standard techniques fail.
Differential Diagnosis
Cerumen impaction, otitis externa, canal hematoma, granuloma, trauma, tympanic membrane perforation, residual inflammation after self-removal, and tumors.
Treatment
Prehospital care for suspected live insects includes instillation of warm lidocaine or mineral oil to immobilize the insect; field removal attempts are discouraged.
In the emergency department, ensure adequate lighting, proper head immobilization, and analgesia. Lidocaine (1–2%) may be instilled topically or injected into the canal walls. Procedural sedation is recommended for children or uncooperative adults and should be used early to prevent traumatic repeated attempts.
Removal techniques depend on object type: irrigation for non–button battery objects; forceps, hooks, suction, Fogarty catheter, or cyanoacrylate glue for selected cases; acetone for Styrofoam or adhesive materials. Vegetable matter should not be irrigated. Button batteries must never be irrigated and require urgent removal. Live insects should be killed first with lidocaine, alcohol, or mineral oil before extraction. Sharp objects and complicated cases require ENT referral.
Medication
Analgesia or sedation may include fentanyl, ketamine, or midazolam. Topical antibiotic-steroid drops are indicated if canal abrasion or infection is suspected. Oral antibiotics are reserved for tympanic membrane perforation or secondary infection.
Follow Up Disposition
Admission is required for button batteries that cannot be removed.
Discharge is appropriate once the foreign body is removed or if a nonhazardous object cannot be safely removed in the ED.
ENT referral is indicated for failed removal, complications, immunocompromised patients, or significant trauma.
Follow Up Recommendations
Advise patients not to insert objects into the ear. Provide short-term analgesia after traumatic removal. Treat otitis externa with topical antimicrobials. Avoid water submersion if trauma or infection is present and arrange ENT follow-up when indicated.
Key Practice Insights And Avoidable Errors
Early use of procedural sedation improves success and reduces complications. Never irrigate an ear containing a button battery, as this can rapidly worsen tissue necrosis.
- Published on
Emergency And Acute Medicine – Dyspnea
Core Concept Overview
Dyspnea is the subjective sensation of uncomfortable or difficult breathing and represents a symptom rather than a diagnosis. It differs from objective signs of increased work of breathing and ranges from mild air hunger to a sensation of suffocation. Although breathing is usually an unconscious activity, dyspnea reflects a conscious perception arising from disruption of normal gas exchange, acid–base balance, metabolic demands, or central nervous system drive. It is a common emergency department complaint, accounting for approximately 3.5% of visits. The sensation results from impaired ventilation, perfusion, metabolic function, or neural control. Respiratory control depends on brainstem and cortical centers, chemoreceptors responsive to carbon dioxide and oxygen levels, mechanoreceptors within respiratory muscles and lung tissue, and intact neuromuscular pathways to the diaphragm and chest wall. Dysfunction at any point in this complex system can produce dyspnea.
Causes And Pathophysiologic Categories
Upper airway causes include epiglottitis, laryngeal obstruction, tracheitis or tracheobronchitis, and angioedema. Pulmonary etiologies encompass asthma, bronchitis, pneumonia, pneumothorax, pulmonary embolism, pulmonary hypertension, emphysema, restrictive lung disease, effusions, malignancy, chest wall trauma, and drug-induced lung injury. Cardiovascular causes include arrhythmias, coronary artery disease, intracardiac shunts, left ventricular failure, valvular disease, pericardial pathology, and cardiac tumors. Neuromuscular causes involve central nervous system disorders, peripheral neuropathies, myopathies, spinal cord disease, and diaphragmatic or phrenic nerve dysfunction. Metabolic acidosis from sepsis, diabetic or alcoholic ketoacidosis, renal failure, or severe thiamine deficiency may drive dyspnea. Toxic causes include methemoglobinemia, salicylate poisoning, and cellular asphyxiants such as carbon monoxide, cyanide, hydrogen sulfide, sodium azide, and toxic alcohols. Abdominal compression from ascites, pregnancy, or morbid obesity may impair ventilation. Psychogenic causes include anxiety and hyperventilation. Other contributors include anemia, altitude exposure, and anaphylaxis.
Special Population Considerations
In older adults, the most common causes of dyspnea are decompensated heart failure, pneumonia, chronic obstructive pulmonary disease, pulmonary embolism, and asthma. In children under two years of age, common causes include asthma, croup, congenital airway or cardiac anomalies, foreign-body aspiration, nasopharyngeal obstruction, and shock.
Clinical Manifestations
Patients may report difficult, labored, or uncomfortable breathing. Upper airway involvement may present with stridor. Pulmonary findings include tachypnea, accessory muscle use, wheezing, rales, asymmetric breath sounds, poor air movement, or prolonged expiration. Cardiovascular findings may include jugular venous distention, murmurs, or an S3 gallop. Neurologic involvement may cause altered mental status. General signs include diaphoresis, pallor, cyanosis, edema, clubbing, upright posture, or ketotic breath odor.
Focused History Assessment
Key elements include prior episodes of dyspnea, onset and time course, precipitating factors, severity, and progression. Elicit history of stridor or wheezing, exercise tolerance, medication use and compliance, allergen exposure, and past medical conditions. Associated symptoms such as chest pain, fever, cough, and hemoptysis should be explored.
Physical Examination Priorities
Assess for signs of acute distress including altered mental status, cyanosis, severe tachypnea, and retractions. Auscultate carefully for stridor, rales, wheezing, or diminished breath sounds and evaluate cardiovascular and neurologic status.
Essential Diagnostic Evaluation
Continuous pulse oximetry should be applied, recognizing that values may be misleading in hyperventilation or carbon monoxide exposure. End-tidal carbon dioxide monitoring provides rapid estimation of ventilation and waveform clues to etiology. Chest radiography evaluates pulmonary pathology and cardiac size. Arterial blood gas analysis assesses oxygenation and acid–base status and allows calculation of the alveolar–arterial gradient to identify gas exchange abnormalities.
Diagnostic Studies And Interpretation
Laboratory testing may include complete blood count for anemia or infection, metabolic panel for renal or metabolic derangements, B-type natriuretic peptide for heart failure, toxicology screening, methemoglobin or carboxyhemoglobin levels, thyroid studies, and D-dimer when pulmonary embolism is suspected. Imaging includes chest radiography, CT pulmonary angiography or ventilation–perfusion scanning for embolism, and soft tissue neck imaging or fiberoptic evaluation for upper airway obstruction. Electrocardiography assesses for ischemia, arrhythmias, or pericardial disease. Pulmonary function testing or peak flow may help evaluate reactive airway disease, and specialized testing may be considered for neuromuscular disorders.
Alternative Diagnoses To Consider
Less common considerations include anticholinergic or adrenergic toxidromes, thyroid storm, and factitious disorders.
Prehospital Management Principles
All patients should receive supplemental oxygen, continuous monitoring, and early intervention directed at the suspected cause, such as bronchodilators for asthma, diuretics for heart failure, or ventilatory support when indicated. Advanced airway management should be used for impending respiratory failure.
Initial Resuscitation Strategy
Follow airway, breathing, and circulation priorities. Immediate intubation is required for respiratory arrest, severe altered mental status, or unstable vital signs. Noninvasive ventilation may be used in alert patients but is contraindicated in hemodynamic instability, suspected upper airway obstruction, inability to protect the airway, active gastrointestinal bleeding, or ongoing seizures.
Emergency Department Management
Treatment is directed at the underlying etiology, including antibiotics and fluids for pneumonia, positive pressure ventilation and diuretics for heart failure, bronchodilators and corticosteroids for asthma, and antiplatelet or anticoagulant therapy for myocardial infarction when appropriate. Symptom-directed and palliative measures, including opioids, may be appropriate for refractory dyspnea in terminal illness.
Disposition Planning
Hospital admission is indicated for patients requiring assisted ventilation, persistent hypoxia, significantly elevated alveolar–arterial gradients, or conditions requiring inpatient therapy. Discharge may be considered for patients with stable disease, adequate oxygenation, and safe ambulatory pulse oximetry.
Referral And Follow-Up Needs
Specialty referral should be based on the identified or suspected etiology.
Discharge Instructions And Return Precautions
Patients should avoid smoking and be counseled on cessation. They should return for worsening symptoms, lack of improvement within 24 hours, new chest pain, high fever, worsening cough or wheeze, gastrointestinal symptoms, neurologic changes, or any significant new concern.
Clinical Pearls And Common Errors
Altered mental status in a dyspneic patient mandates immediate airway consideration. Dyspnea severity should be quantified and reassessed. Not all dyspnea is respiratory in origin; metabolic disturbances and catastrophic neurologic events must remain in the differential.
Core Concept Overview
Dyspnea is the subjective sensation of uncomfortable or difficult breathing and represents a symptom rather than a diagnosis. It differs from objective signs of increased work of breathing and ranges from mild air hunger to a sensation of suffocation. Although breathing is usually an unconscious activity, dyspnea reflects a conscious perception arising from disruption of normal gas exchange, acid–base balance, metabolic demands, or central nervous system drive. It is a common emergency department complaint, accounting for approximately 3.5% of visits. The sensation results from impaired ventilation, perfusion, metabolic function, or neural control. Respiratory control depends on brainstem and cortical centers, chemoreceptors responsive to carbon dioxide and oxygen levels, mechanoreceptors within respiratory muscles and lung tissue, and intact neuromuscular pathways to the diaphragm and chest wall. Dysfunction at any point in this complex system can produce dyspnea.
Causes And Pathophysiologic Categories
Upper airway causes include epiglottitis, laryngeal obstruction, tracheitis or tracheobronchitis, and angioedema. Pulmonary etiologies encompass asthma, bronchitis, pneumonia, pneumothorax, pulmonary embolism, pulmonary hypertension, emphysema, restrictive lung disease, effusions, malignancy, chest wall trauma, and drug-induced lung injury. Cardiovascular causes include arrhythmias, coronary artery disease, intracardiac shunts, left ventricular failure, valvular disease, pericardial pathology, and cardiac tumors. Neuromuscular causes involve central nervous system disorders, peripheral neuropathies, myopathies, spinal cord disease, and diaphragmatic or phrenic nerve dysfunction. Metabolic acidosis from sepsis, diabetic or alcoholic ketoacidosis, renal failure, or severe thiamine deficiency may drive dyspnea. Toxic causes include methemoglobinemia, salicylate poisoning, and cellular asphyxiants such as carbon monoxide, cyanide, hydrogen sulfide, sodium azide, and toxic alcohols. Abdominal compression from ascites, pregnancy, or morbid obesity may impair ventilation. Psychogenic causes include anxiety and hyperventilation. Other contributors include anemia, altitude exposure, and anaphylaxis.
Special Population Considerations
In older adults, the most common causes of dyspnea are decompensated heart failure, pneumonia, chronic obstructive pulmonary disease, pulmonary embolism, and asthma. In children under two years of age, common causes include asthma, croup, congenital airway or cardiac anomalies, foreign-body aspiration, nasopharyngeal obstruction, and shock.
Clinical Manifestations
Patients may report difficult, labored, or uncomfortable breathing. Upper airway involvement may present with stridor. Pulmonary findings include tachypnea, accessory muscle use, wheezing, rales, asymmetric breath sounds, poor air movement, or prolonged expiration. Cardiovascular findings may include jugular venous distention, murmurs, or an S3 gallop. Neurologic involvement may cause altered mental status. General signs include diaphoresis, pallor, cyanosis, edema, clubbing, upright posture, or ketotic breath odor.
Focused History Assessment
Key elements include prior episodes of dyspnea, onset and time course, precipitating factors, severity, and progression. Elicit history of stridor or wheezing, exercise tolerance, medication use and compliance, allergen exposure, and past medical conditions. Associated symptoms such as chest pain, fever, cough, and hemoptysis should be explored.
Physical Examination Priorities
Assess for signs of acute distress including altered mental status, cyanosis, severe tachypnea, and retractions. Auscultate carefully for stridor, rales, wheezing, or diminished breath sounds and evaluate cardiovascular and neurologic status.
Essential Diagnostic Evaluation
Continuous pulse oximetry should be applied, recognizing that values may be misleading in hyperventilation or carbon monoxide exposure. End-tidal carbon dioxide monitoring provides rapid estimation of ventilation and waveform clues to etiology. Chest radiography evaluates pulmonary pathology and cardiac size. Arterial blood gas analysis assesses oxygenation and acid–base status and allows calculation of the alveolar–arterial gradient to identify gas exchange abnormalities.
Diagnostic Studies And Interpretation
Laboratory testing may include complete blood count for anemia or infection, metabolic panel for renal or metabolic derangements, B-type natriuretic peptide for heart failure, toxicology screening, methemoglobin or carboxyhemoglobin levels, thyroid studies, and D-dimer when pulmonary embolism is suspected. Imaging includes chest radiography, CT pulmonary angiography or ventilation–perfusion scanning for embolism, and soft tissue neck imaging or fiberoptic evaluation for upper airway obstruction. Electrocardiography assesses for ischemia, arrhythmias, or pericardial disease. Pulmonary function testing or peak flow may help evaluate reactive airway disease, and specialized testing may be considered for neuromuscular disorders.
Alternative Diagnoses To Consider
Less common considerations include anticholinergic or adrenergic toxidromes, thyroid storm, and factitious disorders.
Prehospital Management Principles
All patients should receive supplemental oxygen, continuous monitoring, and early intervention directed at the suspected cause, such as bronchodilators for asthma, diuretics for heart failure, or ventilatory support when indicated. Advanced airway management should be used for impending respiratory failure.
Initial Resuscitation Strategy
Follow airway, breathing, and circulation priorities. Immediate intubation is required for respiratory arrest, severe altered mental status, or unstable vital signs. Noninvasive ventilation may be used in alert patients but is contraindicated in hemodynamic instability, suspected upper airway obstruction, inability to protect the airway, active gastrointestinal bleeding, or ongoing seizures.
Emergency Department Management
Treatment is directed at the underlying etiology, including antibiotics and fluids for pneumonia, positive pressure ventilation and diuretics for heart failure, bronchodilators and corticosteroids for asthma, and antiplatelet or anticoagulant therapy for myocardial infarction when appropriate. Symptom-directed and palliative measures, including opioids, may be appropriate for refractory dyspnea in terminal illness.
Disposition Planning
Hospital admission is indicated for patients requiring assisted ventilation, persistent hypoxia, significantly elevated alveolar–arterial gradients, or conditions requiring inpatient therapy. Discharge may be considered for patients with stable disease, adequate oxygenation, and safe ambulatory pulse oximetry.
Referral And Follow-Up Needs
Specialty referral should be based on the identified or suspected etiology.
Discharge Instructions And Return Precautions
Patients should avoid smoking and be counseled on cessation. They should return for worsening symptoms, lack of improvement within 24 hours, new chest pain, high fever, worsening cough or wheeze, gastrointestinal symptoms, neurologic changes, or any significant new concern.
Clinical Pearls And Common Errors
Altered mental status in a dyspneic patient mandates immediate airway consideration. Dyspnea severity should be quantified and reassessed. Not all dyspnea is respiratory in origin; metabolic disturbances and catastrophic neurologic events must remain in the differential.

- Published on
Emergency And Acute Medicine – Dysphagia
Basics Description
Dysphagia is defined as difficulty swallowing and may result from neuromuscular or mechanical causes. It can involve impairment at the oropharyngeal or esophageal level, and careful clinical distinction is essential because etiologies, workup, and urgency differ significantly.
Etiology
Oropharyngeal (transfer) dysphagia is characterized by difficulty initiating a swallow and impaired transfer of food from the mouth to the proximal esophagus. Patients often swallow solids more easily than liquids and develop symptoms immediately upon swallowing. Associated features include nasal or oral regurgitation, coughing, choking, drooling, and aspiration. This form is usually due to neuromuscular disorders causing bulbar muscle weakness or impaired coordination.
Esophageal (transport) dysphagia results from failure of normal transit through the esophagus and is associated with a retrosternal sticking sensation occurring seconds after swallowing. Patients may experience nocturnal regurgitation, aspiration, or regurgitation of undigested food, which is characteristic of esophageal obstruction. Causes include motility disorders and mechanical obstruction.
Functional dysphagia is a diagnosis of exclusion after a full evaluation shows no mechanical or neuromuscular pathology, with symptoms lasting longer than 12 weeks.
Odynophagia refers to pain with swallowing and is a separate but often related condition. Pain localization is generally poor; upper esophageal pain is better localized due to somatic innervation, while lower esophageal visceral pain is poorly localized and may mimic acute coronary syndrome.
Pediatric Considerations
In infants and newborns, common causes include prematurity, congenital malformations, neuromuscular disease, infection such as candidiasis, and inflammation. Foreign body aspiration must always be considered. Other pediatric causes include caustic ingestions, infections, neurologic disorders, and sequelae of head injury. Acquired tracheoesophageal fistula may occur after disk battery or caustic ingestion or prior surgery. Life-threatening pediatric causes include epiglottitis, retropharyngeal abscess, central nervous system infection, botulism, esophageal perforation, and diphtheria.
Diagnosis Signs And Symptoms
Symptoms include difficulty initiating swallowing, sensation of food sticking after swallowing, coughing or choking after eating, impaired gag reflex, dysphonia, drooling, dysarthria, and chest pain.
History
Determine whether dysphagia occurs with solids, liquids, or both. Difficulty with both solids and liquids suggests a neuromuscular disorder, whereas solids alone or progression from solids to liquids suggests mechanical obstruction. Immediate symptoms indicate oropharyngeal dysphagia, while delayed symptoms suggest esophageal involvement. Intermittent symptoms suggest rings or webs, whereas progressive symptoms raise concern for peptic or malignant strictures. Acute onset is concerning for life-threatening causes, with food impaction being the most common. Associated symptoms such as nasal regurgitation, choking, heartburn, or weight loss should be elicited.
Physical-Exam
Findings are often subtle or normal. Perform careful oropharyngeal inspection, pulmonary and cardiac auscultation, and a complete neurologic examination with emphasis on cranial nerves V, VII, IX, X, and XII.
Essential Workup
Ensure adequate airway evaluation and perform a thorough neurologic examination.
Diagnosis Tests And Interpretation
Electrocardiogram should be obtained when chest discomfort raises concern for cardiac etiology. No routine laboratory studies are indicated. Chest radiograph may show dilated esophagus in achalasia, aspiration pneumonitis, or extrinsic compression. Lateral neck radiograph may be helpful in selected cases. Modified barium swallow or videofluoroscopy assesses anatomy and function but should not be performed if endoscopy is anticipated. CT or MRI of the head is indicated for new-onset neuromuscular dysphagia. Upper endoscopy allows relief of obstruction, direct visualization, and biopsy when indicated. Esophageal manometry and fiberoptic nasopharyngeal laryngoscopy are usually performed in the outpatient setting.
Differential Diagnosis
Oropharyngeal causes include infections such as botulism and central nervous system infections, mechanical causes including congenital abnormalities and malignancy, medication-induced injury, and neuromuscular disorders such as stroke, amyotrophic lateral sclerosis, Guillain–Barré syndrome, myasthenia gravis, Parkinson disease, multiple sclerosis, and traumatic brain injury. Esophageal causes include mechanical obstruction from diverticula, webs, foreign bodies, neoplasms, strictures, rings, radiation injury, and postsurgical changes; motility disorders such as achalasia and diffuse esophageal spasm; inflammatory conditions including eosinophilic or pill esophagitis; and extrinsic compression from cardiovascular or mediastinal abnormalities.
Treatment Pre Hospital
Maintain vigilant airway monitoring and position the patient comfortably with suction readily available.
Initial Stabilization And Therapy
Maintain airway vigilance and keep the patient NPO. Administer intravenous fluids with 0.9% normal saline for dehydration. Evaluate urgently for life-threatening causes including retropharyngeal abscess or hematoma, epiglottitis, foreign body, upper airway obstruction, and cardiovascular etiologies.
Emergency Department Treatment And Procedures
Nitroglycerin may be used for esophageal spasm. Glucagon may be attempted for food impaction. Treat complications such as airway obstruction, aspiration pneumonia, dehydration, and malnutrition. Endoscopy is indicated when obstruction persists. Dietary modifications include thickened liquids for neuromuscular disorders and thin liquids for mechanical causes.
Medication
Glucagon 1 mg IV may be administered for food impaction, with a second 1 mg dose after 5 minutes if no improvement; pediatric dosing is 0.02–0.03 mg/kg, not exceeding 0.5 mg. Calcium channel blockers and nitrates may be considered for esophageal motility disorders such as achalasia.
Follow-Up And Disposition
Admission is required for persistent esophageal obstruction, inability to protect the airway, inability to tolerate secretions, or compromised hydration or nutrition. Patients who are stable and well hydrated may be discharged with urgent referral to neurology, otolaryngology, or gastroenterology.
Issues For Referral
Next-day follow-up with primary care, ENT, or gastroenterology is recommended.
Follow-Up Recommendations
Clear liquid diet until specialist evaluation. Return immediately for shortness of breath, chest pain, or inability to tolerate secretions.
Pearls And Pitfalls
Always consider foreign body aspiration in children. Dysphagia is a common presentation of stroke and should be considered in patients with recurrent pneumonia. Life-threatening causes must be excluded before deferring evaluation to the outpatient setting.
Basics Description
Dysphagia is defined as difficulty swallowing and may result from neuromuscular or mechanical causes. It can involve impairment at the oropharyngeal or esophageal level, and careful clinical distinction is essential because etiologies, workup, and urgency differ significantly.
Etiology
Oropharyngeal (transfer) dysphagia is characterized by difficulty initiating a swallow and impaired transfer of food from the mouth to the proximal esophagus. Patients often swallow solids more easily than liquids and develop symptoms immediately upon swallowing. Associated features include nasal or oral regurgitation, coughing, choking, drooling, and aspiration. This form is usually due to neuromuscular disorders causing bulbar muscle weakness or impaired coordination.
Esophageal (transport) dysphagia results from failure of normal transit through the esophagus and is associated with a retrosternal sticking sensation occurring seconds after swallowing. Patients may experience nocturnal regurgitation, aspiration, or regurgitation of undigested food, which is characteristic of esophageal obstruction. Causes include motility disorders and mechanical obstruction.
Functional dysphagia is a diagnosis of exclusion after a full evaluation shows no mechanical or neuromuscular pathology, with symptoms lasting longer than 12 weeks.
Odynophagia refers to pain with swallowing and is a separate but often related condition. Pain localization is generally poor; upper esophageal pain is better localized due to somatic innervation, while lower esophageal visceral pain is poorly localized and may mimic acute coronary syndrome.
Pediatric Considerations
In infants and newborns, common causes include prematurity, congenital malformations, neuromuscular disease, infection such as candidiasis, and inflammation. Foreign body aspiration must always be considered. Other pediatric causes include caustic ingestions, infections, neurologic disorders, and sequelae of head injury. Acquired tracheoesophageal fistula may occur after disk battery or caustic ingestion or prior surgery. Life-threatening pediatric causes include epiglottitis, retropharyngeal abscess, central nervous system infection, botulism, esophageal perforation, and diphtheria.
Diagnosis Signs And Symptoms
Symptoms include difficulty initiating swallowing, sensation of food sticking after swallowing, coughing or choking after eating, impaired gag reflex, dysphonia, drooling, dysarthria, and chest pain.
History
Determine whether dysphagia occurs with solids, liquids, or both. Difficulty with both solids and liquids suggests a neuromuscular disorder, whereas solids alone or progression from solids to liquids suggests mechanical obstruction. Immediate symptoms indicate oropharyngeal dysphagia, while delayed symptoms suggest esophageal involvement. Intermittent symptoms suggest rings or webs, whereas progressive symptoms raise concern for peptic or malignant strictures. Acute onset is concerning for life-threatening causes, with food impaction being the most common. Associated symptoms such as nasal regurgitation, choking, heartburn, or weight loss should be elicited.
Physical-Exam
Findings are often subtle or normal. Perform careful oropharyngeal inspection, pulmonary and cardiac auscultation, and a complete neurologic examination with emphasis on cranial nerves V, VII, IX, X, and XII.
Essential Workup
Ensure adequate airway evaluation and perform a thorough neurologic examination.
Diagnosis Tests And Interpretation
Electrocardiogram should be obtained when chest discomfort raises concern for cardiac etiology. No routine laboratory studies are indicated. Chest radiograph may show dilated esophagus in achalasia, aspiration pneumonitis, or extrinsic compression. Lateral neck radiograph may be helpful in selected cases. Modified barium swallow or videofluoroscopy assesses anatomy and function but should not be performed if endoscopy is anticipated. CT or MRI of the head is indicated for new-onset neuromuscular dysphagia. Upper endoscopy allows relief of obstruction, direct visualization, and biopsy when indicated. Esophageal manometry and fiberoptic nasopharyngeal laryngoscopy are usually performed in the outpatient setting.
Differential Diagnosis
Oropharyngeal causes include infections such as botulism and central nervous system infections, mechanical causes including congenital abnormalities and malignancy, medication-induced injury, and neuromuscular disorders such as stroke, amyotrophic lateral sclerosis, Guillain–Barré syndrome, myasthenia gravis, Parkinson disease, multiple sclerosis, and traumatic brain injury. Esophageal causes include mechanical obstruction from diverticula, webs, foreign bodies, neoplasms, strictures, rings, radiation injury, and postsurgical changes; motility disorders such as achalasia and diffuse esophageal spasm; inflammatory conditions including eosinophilic or pill esophagitis; and extrinsic compression from cardiovascular or mediastinal abnormalities.
Treatment Pre Hospital
Maintain vigilant airway monitoring and position the patient comfortably with suction readily available.
Initial Stabilization And Therapy
Maintain airway vigilance and keep the patient NPO. Administer intravenous fluids with 0.9% normal saline for dehydration. Evaluate urgently for life-threatening causes including retropharyngeal abscess or hematoma, epiglottitis, foreign body, upper airway obstruction, and cardiovascular etiologies.
Emergency Department Treatment And Procedures
Nitroglycerin may be used for esophageal spasm. Glucagon may be attempted for food impaction. Treat complications such as airway obstruction, aspiration pneumonia, dehydration, and malnutrition. Endoscopy is indicated when obstruction persists. Dietary modifications include thickened liquids for neuromuscular disorders and thin liquids for mechanical causes.
Medication
Glucagon 1 mg IV may be administered for food impaction, with a second 1 mg dose after 5 minutes if no improvement; pediatric dosing is 0.02–0.03 mg/kg, not exceeding 0.5 mg. Calcium channel blockers and nitrates may be considered for esophageal motility disorders such as achalasia.
Follow-Up And Disposition
Admission is required for persistent esophageal obstruction, inability to protect the airway, inability to tolerate secretions, or compromised hydration or nutrition. Patients who are stable and well hydrated may be discharged with urgent referral to neurology, otolaryngology, or gastroenterology.
Issues For Referral
Next-day follow-up with primary care, ENT, or gastroenterology is recommended.
Follow-Up Recommendations
Clear liquid diet until specialist evaluation. Return immediately for shortness of breath, chest pain, or inability to tolerate secretions.
Pearls And Pitfalls
Always consider foreign body aspiration in children. Dysphagia is a common presentation of stroke and should be considered in patients with recurrent pneumonia. Life-threatening causes must be excluded before deferring evaluation to the outpatient setting.

- Published on
Emergency And Acute Medicine – Dysfunctional Uterine Bleeding
Basics Description
Abnormal uterine bleeding refers to an alteration in the pattern or volume of normal menses. Typical menstrual blood loss is 30–80 mL, with a normal cycle interval of 28 ± 7 days. Abnormal uterine bleeding is classified into dysfunctional uterine bleeding (DUB) and organic uterine bleeding. Dysfunctional uterine bleeding is hormonally mediated, divided into anovulatory and ovulatory categories, is not due to organic or iatrogenic causes, and is therefore a diagnosis of exclusion. Organic uterine bleeding is related to systemic illness or disease of the reproductive tract.
Etiology
Anovulatory bleeding, the most common cause, results from unopposed estrogen stimulation of the proliferative endometrium. Neuroendocrine dysfunction may be associated with polycystic ovarian syndrome, very low-calorie diets, rapid weight changes, intense exercise, anorexia, psychological stress, obesity, medications, hypothyroidism, or primary hypothalamic dysfunction. Ovulatory bleeding is caused by inadequate uterine prostaglandin F2α, increased uterine contractility, or excessive prostacycline production, which diminishes platelet function and increases uterine vasodilation.
Pediatric Considerations
Anovulatory bleeding is common during adolescence due to immaturity of the hypothalamic–pituitary–ovarian axis.
Diagnosis Signs And Symptoms
Patients present with abnormal uterine bleeding in the absence of systemic or structural disease. It is most common in perimenarcheal and perimenopausal women and is typically painless. Anovulatory patterns include metrorrhagia with irregular bleeding between periods, menorrhagia with regular cycles and excessive flow greater than 80 mL or lasting more than 7 days, oligomenorrhea with cycles longer than 35 days, and menometrorrhagia with heavy and irregular bleeding.
History
History focuses on bleeding pattern, duration, volume, associated symptoms, medication use, and risk factors for pregnancy or systemic disease.
Physical-Exam
Acne, hirsutism, and obesity suggest polycystic ovarian syndrome. Pelvic examination typically reveals mild to moderate bleeding. Pallor, tachycardia, hypotension, and orthostasis indicate severe blood loss. Evaluate for trauma or foreign bodies.
Alert
Hemodynamic instability is rare in dysfunctional uterine bleeding; if present, consider ectopic pregnancy or another cause of acute hemorrhage.
Essential Workup
A pregnancy test is mandatory.
Diagnosis Tests And Interpretation
Laboratory evaluation includes pregnancy test, complete blood count, and coagulation studies. Iron studies, thyroid-stimulating hormone, luteinizing hormone, follicle-stimulating hormone, prolactin, and cervical cultures are typically deferred for outpatient follow-up. Pelvic ultrasound may identify uterine, tubal, or ovarian pathology and help exclude organic causes. Dilation and curettage may be required for heavy bleeding unresponsive to therapy. Endometrial biopsy is recommended for patients older than 35 years.
Differential Diagnosis
Pregnancy-related causes include threatened, incomplete, or spontaneous abortion, ectopic pregnancy, and molar pregnancy. Infectious causes include vaginitis, cervicitis, and pelvic inflammatory disease. Coagulopathies include von Willebrand disease, idiopathic thrombocytopenic purpura, platelet disorders, and thalassemia. Medication-related causes include warfarin, aspirin, oral contraceptives, tricyclic antidepressants, and antipsychotics. Systemic illnesses include adrenal, hepatic, renal, thyroid disease, diabetes, and other endocrinopathies. Anatomic causes include fibroids, endometriosis, polyps, endometrial hyperplasia, malignancy, intrauterine devices, and trauma.
Treatment Pre Hospital
Administer intravenous crystalloids as needed for hypotension or tachycardia secondary to heavy bleeding.
Initial Stabilization And Therapy
Follow ABCs. Transfuse packed red blood cells for significant bleeding unresponsive to crystalloid resuscitation.
Emergency Department Treatment And Procedures
Observation is usually sufficient for mild bleeding. Administer intravenous fluids or packed red blood cells for continued bleeding or hemodynamic instability. Obtain gynecology consultation for severe bleeding unresponsive to medical therapy. Dilation and curettage may be necessary for instability. Endometrial ablation or hysterectomy is reserved for refractory cases.
Medication
Conjugated estrogen is indicated for heavy bleeding with hemodynamic instability at 2.5 mg orally every 6 hours or 25 mg intravenously, repeatable after 3 hours if needed. Ibuprofen 400–800 mg orally every 8 hours reduces prostaglandin synthesis. Medroxyprogesterone acetate 5–10 mg orally daily is added once bleeding subsides. Combined oral contraceptives containing ethinyl estradiol 35 μg and norethindrone 1 mg may be given four times daily for one week. Tranexamic acid 1,300 mg orally three times daily for five days may be used, though limited by gastrointestinal side effects and allergy risk. Medications may be deferred in mild cases with outpatient gynecology referral.
Follow-Up And Disposition
Admission is required for significant blood loss, continued bleeding, or hemodynamic instability requiring aggressive resuscitation or operative intervention. Most patients may be discharged once bleeding is controlled and vital signs are stable, with gynecology follow-up arranged.
Issues For Referral
Endometrial biopsy is indicated for patients older than 35 years. Follow-up with gynecology or primary care is essential to evaluate for ongoing blood loss or malignancy.
Pearls And Pitfalls
Dysfunctional uterine bleeding is a diagnosis of exclusion. Only 2% of endometrial carcinomas occur before age 40. Hemodynamic instability makes DUB an unlikely primary diagnosis.

- Published on
Emergency And Acute Medicine - Dystonic Reaction
Foundational Overview
Normal CNS motor control depends on a balance between dopaminergic and cholinergic activity. Certain medications block dopamine receptors in the basal ganglia, creating relative cholinergic excess. This imbalance produces acute, involuntary muscle contractions, most often affecting the face and neck, though the trunk, pelvis, and extremities may also be involved. Symptoms are typically alarming but rarely life threatening, except in uncommon cases involving the laryngeal muscles. Onset usually occurs within hours of exposure and almost always within the first week. Children and young adults are at highest risk; males are affected more often. Prior dystonic reactions and recent cocaine use increase susceptibility, while occurrence after age 45 is rare.
Causes And Risk Factors
Most reactions follow exposure to dopamine antagonists, particularly antipsychotics, antiemetics, and some antidepressants. Incidence varies widely and correlates with drug potency—higher with agents such as haloperidol or fluphenazine, lower with chlorpromazine or thioridazine, and lowest with atypical antipsychotics. Common antiemetic triggers include metoclopramide, prochlorperazine, promethazine, and droperidol. Other implicated agents include cyclic antidepressants, H2 blockers, selected antimalarials, antihistamines, anticonvulsants, lithium, doxepin, and phencyclidine. Children are particularly vulnerable when febrile or dehydrated.
Clinical Recognition
History typically reveals recent ingestion or dose escalation of a neuroleptic or antiemetic, or reduction of prophylactic anticholinergic therapy. Patients remain alert and oriented, though speech may be impaired by facial or tongue involvement. Involuntary sustained muscle contractions are characteristic. Examination may reveal oculogyric crisis with painful eye deviation, blepharospasm, buccolingual involvement with facial grimacing, trismus, tongue protrusion, dysphagia, spasmodic torticollis, truncal arching (opisthotonos), abdominal wall spasm, or, rarely, laryngeal dystonia presenting with stridor or dysphonia.
Essential Evaluation
Diagnosis is clinical, supported by a compatible medication history and rapid resolution after treatment. Failure to improve should prompt reconsideration of the diagnosis.
Diagnostic Studies
Routine laboratory or imaging studies are unnecessary. If symptoms persist despite therapy, evaluate for alternative causes such as hypocalcemia.
Differential Considerations
Distinguish acute dystonia from tardive dyskinesia, akathisia, seizures, psychogenic events, tetanus, strychnine poisoning, chronic neurologic dystonias, scorpion envenomation, meningitis, encephalitis, mandibular dislocation, and metabolic disturbances such as hypocalcemia.
Prehospital Care
These reactions are rarely fatal. Attention should focus on airway protection, especially with tongue or laryngeal involvement. Obtain information on recent medication or substance exposure and transport medication containers when possible.
Initial Stabilization
Ensure airway patency and monitor for respiratory compromise related to oropharyngeal or laryngeal spasm.
Emergency Department Management
First-line therapy is intravenous anticholinergic medication, which rapidly restores neurotransmitter balance. Diphenhydramine or benztropine typically produces improvement within minutes, with complete resolution within 30 minutes. Intramuscular administration is an alternative when IV access is unavailable. Oral therapy should continue for several days to prevent recurrence. Benzodiazepines are reserved for refractory cases. Lack of response should prompt reevaluation for alternate diagnoses.
Pharmacologic Therapy
Diphenhydramine 1–2 mg/kg IV or IM (maximum 100 mg), followed by oral dosing for three days, is first line. Benztropine 1–2 mg IV or IM followed by oral dosing is an alternative, avoiding use in children under three years. Diazepam may be used for persistent symptoms.
Disposition And Follow-Up
Admission is rarely required unless symptoms fail to resolve, airway protection is a concern, or the diagnosis is uncertain. Patients with laryngeal involvement should be observed after symptom resolution. Discharge is appropriate once symptoms resolve; the offending agent should be discontinued, and patients cautioned about sedating medications. Follow-up with the prescribing clinician is recommended.
Key Clinical Insights And Common Errors
Acute dystonia is diagnosed by characteristic presentation and rapid response to anticholinergic therapy. Diphenhydramine is the preferred first-line treatment. Failure to improve should prompt reassessment for alternative or more serious conditions.
Foundational Overview
Normal CNS motor control depends on a balance between dopaminergic and cholinergic activity. Certain medications block dopamine receptors in the basal ganglia, creating relative cholinergic excess. This imbalance produces acute, involuntary muscle contractions, most often affecting the face and neck, though the trunk, pelvis, and extremities may also be involved. Symptoms are typically alarming but rarely life threatening, except in uncommon cases involving the laryngeal muscles. Onset usually occurs within hours of exposure and almost always within the first week. Children and young adults are at highest risk; males are affected more often. Prior dystonic reactions and recent cocaine use increase susceptibility, while occurrence after age 45 is rare.
Causes And Risk Factors
Most reactions follow exposure to dopamine antagonists, particularly antipsychotics, antiemetics, and some antidepressants. Incidence varies widely and correlates with drug potency—higher with agents such as haloperidol or fluphenazine, lower with chlorpromazine or thioridazine, and lowest with atypical antipsychotics. Common antiemetic triggers include metoclopramide, prochlorperazine, promethazine, and droperidol. Other implicated agents include cyclic antidepressants, H2 blockers, selected antimalarials, antihistamines, anticonvulsants, lithium, doxepin, and phencyclidine. Children are particularly vulnerable when febrile or dehydrated.
Clinical Recognition
History typically reveals recent ingestion or dose escalation of a neuroleptic or antiemetic, or reduction of prophylactic anticholinergic therapy. Patients remain alert and oriented, though speech may be impaired by facial or tongue involvement. Involuntary sustained muscle contractions are characteristic. Examination may reveal oculogyric crisis with painful eye deviation, blepharospasm, buccolingual involvement with facial grimacing, trismus, tongue protrusion, dysphagia, spasmodic torticollis, truncal arching (opisthotonos), abdominal wall spasm, or, rarely, laryngeal dystonia presenting with stridor or dysphonia.
Essential Evaluation
Diagnosis is clinical, supported by a compatible medication history and rapid resolution after treatment. Failure to improve should prompt reconsideration of the diagnosis.
Diagnostic Studies
Routine laboratory or imaging studies are unnecessary. If symptoms persist despite therapy, evaluate for alternative causes such as hypocalcemia.
Differential Considerations
Distinguish acute dystonia from tardive dyskinesia, akathisia, seizures, psychogenic events, tetanus, strychnine poisoning, chronic neurologic dystonias, scorpion envenomation, meningitis, encephalitis, mandibular dislocation, and metabolic disturbances such as hypocalcemia.
Prehospital Care
These reactions are rarely fatal. Attention should focus on airway protection, especially with tongue or laryngeal involvement. Obtain information on recent medication or substance exposure and transport medication containers when possible.
Initial Stabilization
Ensure airway patency and monitor for respiratory compromise related to oropharyngeal or laryngeal spasm.
Emergency Department Management
First-line therapy is intravenous anticholinergic medication, which rapidly restores neurotransmitter balance. Diphenhydramine or benztropine typically produces improvement within minutes, with complete resolution within 30 minutes. Intramuscular administration is an alternative when IV access is unavailable. Oral therapy should continue for several days to prevent recurrence. Benzodiazepines are reserved for refractory cases. Lack of response should prompt reevaluation for alternate diagnoses.
Pharmacologic Therapy
Diphenhydramine 1–2 mg/kg IV or IM (maximum 100 mg), followed by oral dosing for three days, is first line. Benztropine 1–2 mg IV or IM followed by oral dosing is an alternative, avoiding use in children under three years. Diazepam may be used for persistent symptoms.
Disposition And Follow-Up
Admission is rarely required unless symptoms fail to resolve, airway protection is a concern, or the diagnosis is uncertain. Patients with laryngeal involvement should be observed after symptom resolution. Discharge is appropriate once symptoms resolve; the offending agent should be discontinued, and patients cautioned about sedating medications. Follow-up with the prescribing clinician is recommended.
Key Clinical Insights And Common Errors
Acute dystonia is diagnosed by characteristic presentation and rapid response to anticholinergic therapy. Diphenhydramine is the preferred first-line treatment. Failure to improve should prompt reassessment for alternative or more serious conditions.

