- Published on
Emergency and Acute Medicine – Central Retinal Artery Occlusion
Overview
Central retinal artery occlusion (CRAO) is an obstruction of the central retinal artery resulting in sudden, painless, monocular vision loss. It typically affects adults aged 50–70 years and is often described as a “stroke of the eye.” The ophthalmic artery is the first branch of the carotid artery. Risk factors include hypertension, atherosclerosis, carotid artery disease, valvular heart disease, coronary artery disease, vasculitis, lupus, sickle cell disease, and trauma. Incidence is approximately 1–10 per 100,000. Irreversible retinal injury can occur within 90 minutes.
Causative Mechanisms
Embolic causes are most common and include cholesterol or platelet emboli from carotid atherosclerosis, carotid stenosis, valvular heart disease, atrial myxoma, or arterial dissection. Thrombotic causes result from rupture of an atherosclerotic plaque or hypercoagulable states such as sickle cell disease. Inflammatory causes include giant cell arteritis, lupus, and systemic vasculitis. Arterial spasm may be migraine-related. Reduced ocular perfusion may occur with severe hypotension, acute angle-closure glaucoma, or retrobulbar hemorrhage.
Clinical Presentation
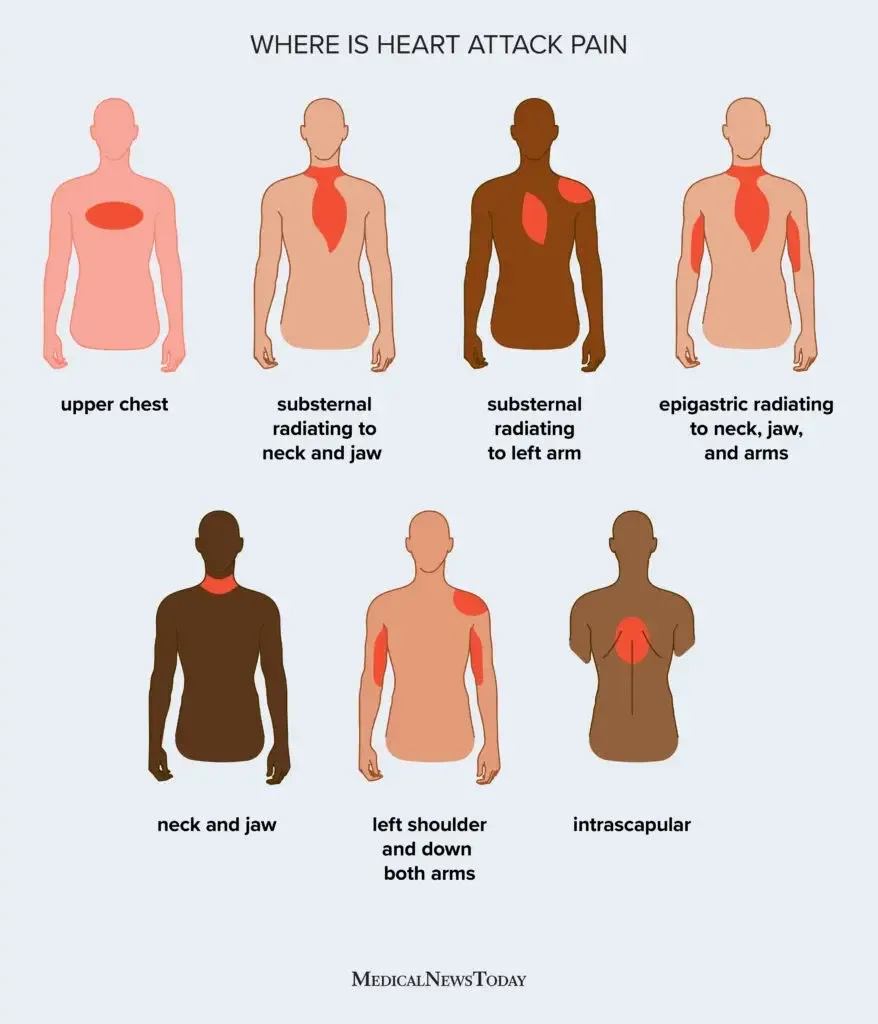
Patients present with sudden, painless, unilateral vision loss. Some report prior transient episodes of visual loss lasting seconds to minutes (amaurosis fugax). Visual acuity is markedly reduced. An afferent pupillary defect is usually present. Fundoscopy may reveal emboli within retinal vessels appearing as yellow-white glistening plaques, ischemic retinal edema within 15–20 minutes, and a classic cherry-red spot at the fovea. Retinal arteries may appear empty or show segmented “box-carring.” Within 1–2 hours, the infarcted retina becomes opaque. Partial visual field deficits suggest branch retinal artery involvement.
Essential Evaluation
Immediate assessment includes visual acuity, visual fields, fundoscopic examination, intraocular pressure measurement, and urgent ophthalmology consultation.
Diagnostic Studies
Laboratory evaluation targets underlying causes and includes CBC with platelets, PT/PTT, electrolytes, renal function, glucose, ESR and CRP (especially in patients >55 years for giant cell arteritis), ANA, RF, RPR, hemoglobin electrophoresis, and serum protein electrophoresis. Imaging focuses on embolic sources and includes carotid Doppler ultrasound and echocardiography. Fluorescein angiography or electroretinography may confirm diagnosis.
Differential Considerations
Acute angle-closure glaucoma, central retinal vein occlusion, giant cell arteritis, optic neuritis, and retinal detachment.
Emergency Management Principles
This is a true ophthalmologic emergency. Treatment must begin immediately to attempt retinal salvage. Goals include embolus displacement or dissolution, vasodilation to improve retinal perfusion, and reduction of intraocular pressure to enhance the perfusion gradient.
Emergency Department Interventions
Initiate immediate ocular (global) massage with the patient supine: apply firm pressure on the closed eyelid for 15 seconds, release for 15 seconds, and repeat for five cycles. Administer 100% oxygen via nonrebreather mask and consider hyperbaric oxygen if within 24 hours of onset. Carbogen inhalation may be used if available. Reduce intraocular pressure with IV acetazolamide and topical timolol. Administer aspirin and IV heparin to prevent clot propagation. Obtain emergent ophthalmology consultation for possible anterior chamber paracentesis and consideration of intra-arterial fibrinolysis. If inflammatory arteritis is suspected, begin high-dose systemic corticosteroids immediately.
Medications
First-line options include acetazolamide 500 mg IV or PO, timolol maleate 0.5% ophthalmic drops, IV heparin (80 U/kg bolus then 18 U/kg/hr infusion), and carbogen inhalation. Second-line or adjunctive therapies include aspirin 325 mg PO, methylprednisolone 250 mg IV for suspected arteritis, mannitol, and sublingual nitroglycerin.
Disposition and Follow-Up
Most acute cases require admission for urgent evaluation of embolic, thrombotic, or inflammatory sources. Chronic or remote occlusions without active disease may be evaluated outpatient. All suspected cases require immediate ophthalmology involvement. Carotid imaging is recommended in most patients.
Clinical Insights and Pitfalls
Transient monocular vision loss (amaurosis fugax) is a warning sign for CRAO and systemic stroke and requires urgent evaluation. CRAO is a medical and ophthalmologic emergency with a very narrow therapeutic window. Thorough documentation of visual acuity and fundoscopic findings is essential.
Overview
Central retinal artery occlusion (CRAO) is an obstruction of the central retinal artery resulting in sudden, painless, monocular vision loss. It typically affects adults aged 50–70 years and is often described as a “stroke of the eye.” The ophthalmic artery is the first branch of the carotid artery. Risk factors include hypertension, atherosclerosis, carotid artery disease, valvular heart disease, coronary artery disease, vasculitis, lupus, sickle cell disease, and trauma. Incidence is approximately 1–10 per 100,000. Irreversible retinal injury can occur within 90 minutes.
Causative Mechanisms
Embolic causes are most common and include cholesterol or platelet emboli from carotid atherosclerosis, carotid stenosis, valvular heart disease, atrial myxoma, or arterial dissection. Thrombotic causes result from rupture of an atherosclerotic plaque or hypercoagulable states such as sickle cell disease. Inflammatory causes include giant cell arteritis, lupus, and systemic vasculitis. Arterial spasm may be migraine-related. Reduced ocular perfusion may occur with severe hypotension, acute angle-closure glaucoma, or retrobulbar hemorrhage.
Clinical Presentation
Patients present with sudden, painless, unilateral vision loss. Some report prior transient episodes of visual loss lasting seconds to minutes (amaurosis fugax). Visual acuity is markedly reduced. An afferent pupillary defect is usually present. Fundoscopy may reveal emboli within retinal vessels appearing as yellow-white glistening plaques, ischemic retinal edema within 15–20 minutes, and a classic cherry-red spot at the fovea. Retinal arteries may appear empty or show segmented “box-carring.” Within 1–2 hours, the infarcted retina becomes opaque. Partial visual field deficits suggest branch retinal artery involvement.
Essential Evaluation
Immediate assessment includes visual acuity, visual fields, fundoscopic examination, intraocular pressure measurement, and urgent ophthalmology consultation.
Diagnostic Studies
Laboratory evaluation targets underlying causes and includes CBC with platelets, PT/PTT, electrolytes, renal function, glucose, ESR and CRP (especially in patients >55 years for giant cell arteritis), ANA, RF, RPR, hemoglobin electrophoresis, and serum protein electrophoresis. Imaging focuses on embolic sources and includes carotid Doppler ultrasound and echocardiography. Fluorescein angiography or electroretinography may confirm diagnosis.
Differential Considerations
Acute angle-closure glaucoma, central retinal vein occlusion, giant cell arteritis, optic neuritis, and retinal detachment.
Emergency Management Principles
This is a true ophthalmologic emergency. Treatment must begin immediately to attempt retinal salvage. Goals include embolus displacement or dissolution, vasodilation to improve retinal perfusion, and reduction of intraocular pressure to enhance the perfusion gradient.
Emergency Department Interventions
Initiate immediate ocular (global) massage with the patient supine: apply firm pressure on the closed eyelid for 15 seconds, release for 15 seconds, and repeat for five cycles. Administer 100% oxygen via nonrebreather mask and consider hyperbaric oxygen if within 24 hours of onset. Carbogen inhalation may be used if available. Reduce intraocular pressure with IV acetazolamide and topical timolol. Administer aspirin and IV heparin to prevent clot propagation. Obtain emergent ophthalmology consultation for possible anterior chamber paracentesis and consideration of intra-arterial fibrinolysis. If inflammatory arteritis is suspected, begin high-dose systemic corticosteroids immediately.
Medications
First-line options include acetazolamide 500 mg IV or PO, timolol maleate 0.5% ophthalmic drops, IV heparin (80 U/kg bolus then 18 U/kg/hr infusion), and carbogen inhalation. Second-line or adjunctive therapies include aspirin 325 mg PO, methylprednisolone 250 mg IV for suspected arteritis, mannitol, and sublingual nitroglycerin.
Disposition and Follow-Up
Most acute cases require admission for urgent evaluation of embolic, thrombotic, or inflammatory sources. Chronic or remote occlusions without active disease may be evaluated outpatient. All suspected cases require immediate ophthalmology involvement. Carotid imaging is recommended in most patients.
Clinical Insights and Pitfalls
Transient monocular vision loss (amaurosis fugax) is a warning sign for CRAO and systemic stroke and requires urgent evaluation. CRAO is a medical and ophthalmologic emergency with a very narrow therapeutic window. Thorough documentation of visual acuity and fundoscopic findings is essential.

- Published on
Emergency and Acute Medicine – Cervical Adenitis
Overview
Cervical adenitis is an acute bacterial infection of a cervical lymph node, most often arising after a preceding bacterial infection of the head or neck. It is primarily a pediatric condition but is increasingly recognized in adults, particularly those who are immunocompromised (HIV, malignancy, transplant recipients). Any cervical node may be involved, though more than 80% of pediatric cases affect the submandibular or deep cervical nodes, commonly the jugulodigastric node just below the mandibular angle. Cervical lymph nodes serve as the final common drainage pathway for the head and neck. Initial lymphadenopathy reflects hyperplasia and lymphocytic infiltration; progression to lymphadenitis occurs when bacteria proliferate within the lymphatic system, leading to neutrophil activation, pus formation, abscess development, and a clinically warm, tender, erythematous, swollen node.
Causative Factors
Approximately 70% of cases are due to group A β-hemolytic Streptococcus, 20% to Staphylococcus aureus, and about 10% to viral or other bacterial causes. Community-acquired MRSA infections are increasingly common, particularly in children, who have high colonization and invasive disease rates. Mycobacterial causes include tuberculosis (scrofula), typically a chronic posterior cervical lymphadenitis with strongly positive PPD and nonsurgical management, and atypical mycobacteria such as Mycobacterium avium complex, which usually presents as chronic submandibular or anterior cervical lymphadenitis and is treated surgically. Bartonella henselae causes catscratch disease, a subacute lymphadenitis with minimal systemic symptoms that usually resolves spontaneously over 4–6 weeks. Anaerobes should be considered with dental or gingival infections. Rare pathogens include gram-negative bacilli, Yersinia pestis, group B Streptococcus, Francisella tularensis, alpha-streptococcus, and Bacillus anthracis.
In neonates, group B Streptococcus and S. aureus predominate. Group B streptococcal cellulitis–adenitis syndrome presents in infants 3–7 weeks old with fever, submandibular or facial cellulitis, ipsilateral otitis media, and a high rate of bacteremia. Viral infections often cause bilateral adenopathy. In older adults, malignancy should be considered, particularly with hard, fixed, nontender nodes and absence of systemic infection signs.
Clinical Presentation
Patients typically present with a unilateral, enlarged, tender cervical lymph node with overlying warmth and erythema. The node is initially firm and may become fluctuant as suppuration develops. Fever may be present, along with malaise, and irritability in infants and children. A concurrent head or neck infection is common, including pharyngitis, tonsillitis, peritonsillar abscess, otitis media or externa, dental infection, impetigo, or scalp infection.
History and Examination
Key history includes timing of onset, associated fever, weight loss or rash, exposure or travel history, and comorbidities or birth history in infants. Physical examination requires a complete head and neck assessment with attention to airway patency and overall clinical appearance.
Evaluation Strategy
Cervical adenitis is primarily a clinical diagnosis. Identification of a primary head or neck infection source is essential. If no local source is found, tuberculosis exposure should be considered and systemic or viral illness evaluated. Laboratory studies are unnecessary when a clear, treatable source is identified. Blood cultures are reserved for toxic-appearing patients, and full sepsis evaluation is required in neonates. When etiology is unclear, adjunct testing such as CBC with differential, Monospot, throat cultures, and targeted serologies (EBV, CMV, toxoplasmosis) may be useful. Imaging with chest radiograph, lateral neck film, or Panorex can help identify occult sources or deep space infection; chest radiograph may screen for tuberculosis. Ultrasound can distinguish cystic from solid lesions and detect deep abscesses, while CT or MRI helps delineate deep space infections or congenital masses. Fluctuant nodes should undergo needle aspiration for Gram stain, acid-fast stain, and aerobic, anaerobic, mycobacterial, and fungal cultures, except when tuberculosis is suspected, due to risk of sinus tract formation.
Alternative Diagnoses
Consider reactive lymphadenopathy from viral infections (adenovirus, rhinovirus, enterovirus, EBV, HSV, VZV, CMV), mumps, rubella, rubeola, Kawasaki disease, Kikuchi disease, PFAPA syndrome, toxoplasmosis, congenital cysts (branchial cleft, thyroglossal duct cyst, cystic hygroma), malignancy (leukemia, lymphoma, rhabdomyosarcoma, thyroid carcinoma), and systemic inflammatory diseases such as lupus or sarcoidosis.
Management Principles
Airway monitoring is essential if significant neck swelling is present. Treatment targets the underlying source of infection, with empiric coverage for group A Streptococcus and S. aureus; MRSA coverage should be considered if there is poor response to standard therapy. All fluctuant nodes require aspiration. Oral agents such as cephalexin, cefadroxil, or amoxicillin–clavulanate are commonly effective. Clindamycin or amoxicillin–clavulanate is preferred when dental or anaerobic sources are suspected. CA-MRSA may be treated with clindamycin or TMP-SMX, recognizing increasing resistance; toxic patients may require IV vancomycin or linezolid. Antibiotic therapy should continue for at least 10 days. Adjunctive measures include warm compresses and analgesia.
Disposition and Follow-Up
Admission is indicated for neonates, airway compromise, toxic appearance, immunocompromised patients, inability to tolerate oral intake, or failure of outpatient therapy. Most patients can be discharged on oral antibiotics with mandatory re-evaluation in 48–72 hours. Patients should return immediately for worsening symptoms, abscess formation, voice changes, dyspnea, or systemic illness. Referral to ENT or dentistry is based on the infection source, and concerning features for malignancy or congenital anomalies warrant specialist evaluation.
Clinical Insights
Cervical adenitis is a clinical diagnosis most often caused by group A Streptococcus or Staphylococcus aureus. Unilateral, warm, tender, erythematous lymphadenopathy is characteristic. Consider group B Streptococcus in young infants and MRSA in cases not improving with standard therapy. Disposition decisions should be guided by overall clinical status rather than node size alone.
Overview
Cervical adenitis is an acute bacterial infection of a cervical lymph node, most often arising after a preceding bacterial infection of the head or neck. It is primarily a pediatric condition but is increasingly recognized in adults, particularly those who are immunocompromised (HIV, malignancy, transplant recipients). Any cervical node may be involved, though more than 80% of pediatric cases affect the submandibular or deep cervical nodes, commonly the jugulodigastric node just below the mandibular angle. Cervical lymph nodes serve as the final common drainage pathway for the head and neck. Initial lymphadenopathy reflects hyperplasia and lymphocytic infiltration; progression to lymphadenitis occurs when bacteria proliferate within the lymphatic system, leading to neutrophil activation, pus formation, abscess development, and a clinically warm, tender, erythematous, swollen node.
Causative Factors
Approximately 70% of cases are due to group A β-hemolytic Streptococcus, 20% to Staphylococcus aureus, and about 10% to viral or other bacterial causes. Community-acquired MRSA infections are increasingly common, particularly in children, who have high colonization and invasive disease rates. Mycobacterial causes include tuberculosis (scrofula), typically a chronic posterior cervical lymphadenitis with strongly positive PPD and nonsurgical management, and atypical mycobacteria such as Mycobacterium avium complex, which usually presents as chronic submandibular or anterior cervical lymphadenitis and is treated surgically. Bartonella henselae causes catscratch disease, a subacute lymphadenitis with minimal systemic symptoms that usually resolves spontaneously over 4–6 weeks. Anaerobes should be considered with dental or gingival infections. Rare pathogens include gram-negative bacilli, Yersinia pestis, group B Streptococcus, Francisella tularensis, alpha-streptococcus, and Bacillus anthracis.
In neonates, group B Streptococcus and S. aureus predominate. Group B streptococcal cellulitis–adenitis syndrome presents in infants 3–7 weeks old with fever, submandibular or facial cellulitis, ipsilateral otitis media, and a high rate of bacteremia. Viral infections often cause bilateral adenopathy. In older adults, malignancy should be considered, particularly with hard, fixed, nontender nodes and absence of systemic infection signs.
Clinical Presentation
Patients typically present with a unilateral, enlarged, tender cervical lymph node with overlying warmth and erythema. The node is initially firm and may become fluctuant as suppuration develops. Fever may be present, along with malaise, and irritability in infants and children. A concurrent head or neck infection is common, including pharyngitis, tonsillitis, peritonsillar abscess, otitis media or externa, dental infection, impetigo, or scalp infection.
History and Examination
Key history includes timing of onset, associated fever, weight loss or rash, exposure or travel history, and comorbidities or birth history in infants. Physical examination requires a complete head and neck assessment with attention to airway patency and overall clinical appearance.
Evaluation Strategy
Cervical adenitis is primarily a clinical diagnosis. Identification of a primary head or neck infection source is essential. If no local source is found, tuberculosis exposure should be considered and systemic or viral illness evaluated. Laboratory studies are unnecessary when a clear, treatable source is identified. Blood cultures are reserved for toxic-appearing patients, and full sepsis evaluation is required in neonates. When etiology is unclear, adjunct testing such as CBC with differential, Monospot, throat cultures, and targeted serologies (EBV, CMV, toxoplasmosis) may be useful. Imaging with chest radiograph, lateral neck film, or Panorex can help identify occult sources or deep space infection; chest radiograph may screen for tuberculosis. Ultrasound can distinguish cystic from solid lesions and detect deep abscesses, while CT or MRI helps delineate deep space infections or congenital masses. Fluctuant nodes should undergo needle aspiration for Gram stain, acid-fast stain, and aerobic, anaerobic, mycobacterial, and fungal cultures, except when tuberculosis is suspected, due to risk of sinus tract formation.
Alternative Diagnoses
Consider reactive lymphadenopathy from viral infections (adenovirus, rhinovirus, enterovirus, EBV, HSV, VZV, CMV), mumps, rubella, rubeola, Kawasaki disease, Kikuchi disease, PFAPA syndrome, toxoplasmosis, congenital cysts (branchial cleft, thyroglossal duct cyst, cystic hygroma), malignancy (leukemia, lymphoma, rhabdomyosarcoma, thyroid carcinoma), and systemic inflammatory diseases such as lupus or sarcoidosis.
Management Principles
Airway monitoring is essential if significant neck swelling is present. Treatment targets the underlying source of infection, with empiric coverage for group A Streptococcus and S. aureus; MRSA coverage should be considered if there is poor response to standard therapy. All fluctuant nodes require aspiration. Oral agents such as cephalexin, cefadroxil, or amoxicillin–clavulanate are commonly effective. Clindamycin or amoxicillin–clavulanate is preferred when dental or anaerobic sources are suspected. CA-MRSA may be treated with clindamycin or TMP-SMX, recognizing increasing resistance; toxic patients may require IV vancomycin or linezolid. Antibiotic therapy should continue for at least 10 days. Adjunctive measures include warm compresses and analgesia.
Disposition and Follow-Up
Admission is indicated for neonates, airway compromise, toxic appearance, immunocompromised patients, inability to tolerate oral intake, or failure of outpatient therapy. Most patients can be discharged on oral antibiotics with mandatory re-evaluation in 48–72 hours. Patients should return immediately for worsening symptoms, abscess formation, voice changes, dyspnea, or systemic illness. Referral to ENT or dentistry is based on the infection source, and concerning features for malignancy or congenital anomalies warrant specialist evaluation.
Clinical Insights
Cervical adenitis is a clinical diagnosis most often caused by group A Streptococcus or Staphylococcus aureus. Unilateral, warm, tender, erythematous lymphadenopathy is characteristic. Consider group B Streptococcus in young infants and MRSA in cases not improving with standard therapy. Disposition decisions should be guided by overall clinical status rather than node size alone.
- Published on
Emergency and Acute Medicine - Cerebrovascular Accident (Stroke)
Overview
A cerebrovascular accident (CVA) results from interruption of blood flow to a specific brain region. Clinical deficits correspond to the vascular territory involved. Onset may be abrupt and complete or stepwise and fluctuating. Stroke accounts for ~1 in 18 deaths in the United States, with ~610,000 new cases annually.
Predisposing Factors
Hypertension, diabetes mellitus, smoking, coronary artery disease, cardiac dysrhythmias, peripheral vascular disease, oral contraceptive use, polycythemia vera, sickle cell disease, antithrombin III deficiency, protein C or S deficiency.
Pathologic Mechanisms
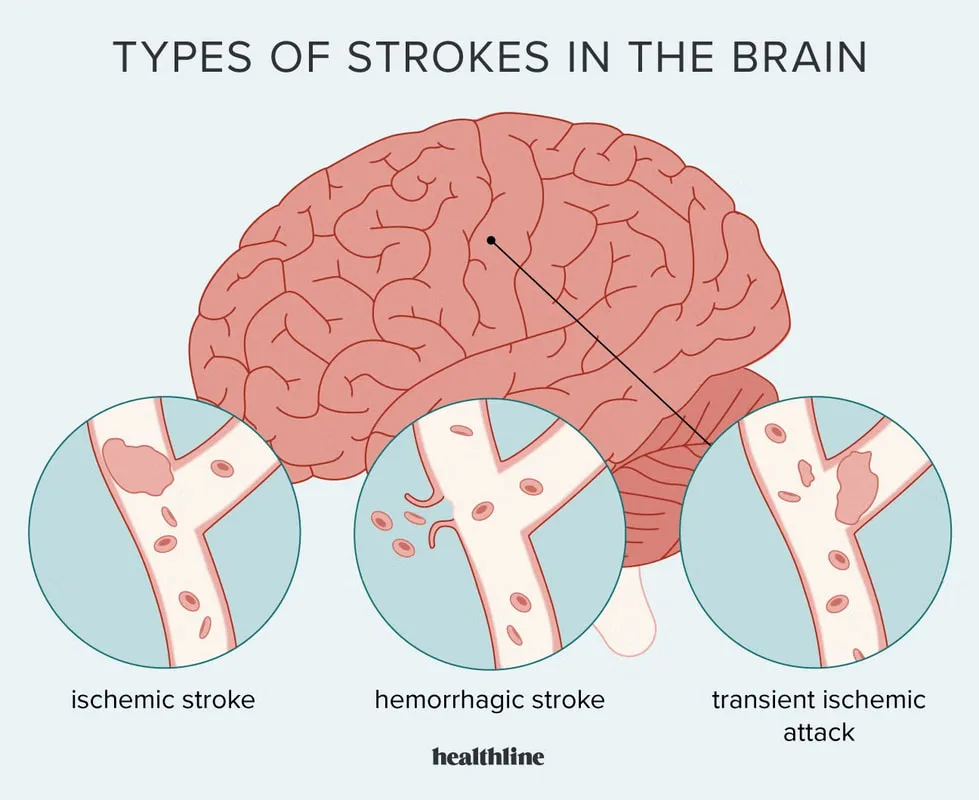
Ischemic stroke includes thrombotic, embolic, dissection-related, or hypoperfusion etiologies. Thrombotic stroke most often results from clot formation at an ulcerated atherosclerotic plaque or from sludging states (sickle cell disease, polycythemia vera, protein C deficiency). Embolic stroke arises from cardiac mural thrombi (atrial fibrillation, mitral stenosis, cardiomyopathy, CHF, MI), prosthetic or abnormal valves, carotid or aortic arch plaques, atrial myxoma, or ventricular aneurysm thrombi. Arterial dissection may involve carotid arteries or be associated with arteritis (giant cell, Takayasu) or fibromuscular dysplasia. Global ischemic stroke results from systemic hypotension due to sepsis, hemorrhage, or shock. Hemorrhagic stroke includes intracerebral and subarachnoid hemorrhage.
Pediatrics: Usually secondary to underlying disease (sickle cell disease, leukemia, infection, blood dyscrasia); younger children often present with seizures or altered mental status.
Clinical Features
History focuses on exact time of onset or last known normal, trauma or surgery, medications, confusion, headache, vertigo, and focal neurologic deficits.
General exam may show Cheyne–Stokes respirations, apnea, hypertension, dysrhythmias, or murmurs.
Anterior cerebral artery involvement causes contralateral leg-predominant weakness and sensory loss, apraxia, confusion, and impaired judgment.
Middle cerebral artery involvement causes contralateral face and arm weakness, hemisensory loss, homonymous hemianopsia, aphasia or dysarthria, and agnosia.
Posterior cerebral artery involvement causes cortical blindness, visual agnosia, memory impairment, altered mental status, third-nerve palsy, or hemiballismus.
Vertebrobasilar strokes cause vertigo, diplopia, nystagmus, visual field defects, and crossed cranial nerve and motor deficits; basilar artery occlusion may lead to quadriplegia, locked-in syndrome, or coma.
Watershed infarcts produce proximal limb weakness with sparing of face, hands, and feet.
Initial Evaluation Priorities
Perform a focused neurologic examination and calculate the NIH Stroke Scale when possible. Obtain emergent noncontrast head CT to differentiate ischemic from hemorrhagic stroke; early CT may be normal within 24–48 hours. Goals include CT completion within 25 minutes, interpretation within 45 minutes, and thrombolytic administration within 60 minutes if indicated. If CT is negative but subarachnoid hemorrhage is suspected, perform lumbar puncture. Obtain ECG, oxygen saturation, and rapid blood glucose.
Diagnostic Studies
Laboratory tests include CBC, electrolytes, renal and liver function, PT/PTT, urinalysis, and ESR when indicated. Additional studies may include cardiac enzymes, pregnancy test, toxicology screen, alcohol level, ABG, and blood cultures. Imaging may include MRI for early ischemia, chest radiograph, and carotid ultrasound. ECG evaluates for arrhythmia; lumbar puncture is required if CT is nondiagnostic and SAH remains suspected.
Key Differentials
Intracranial hemorrhage, hypoglycemia, seizure with Todd paralysis, conversion disorder, transient global amnesia, encephalitis or meningitis, peripheral neuropathy, intracranial abscess, migraine, air embolism, TIA, metabolic encephalopathy, neoplasm, vasculitis, multiple sclerosis, compressive myelopathy, vestibulitis, medication or toxin effects.
Prehospital Considerations
Patients may have impaired movement or communication. Field neurologic assessment should include level of consciousness, GCS, speech, facial symmetry, gait, and motor deficits. Fingerstick glucose is essential.
Stabilization Measures
Ensure airway protection; provide supplemental oxygen at 2–4 L/min. Intubation may be required for airway control or ICP management. For altered mental status, administer naloxone and thiamine and correct hypoglycemia.
Emergency Department Management
Treat severe hypertension only if SBP >220 mm Hg or DBP >120 mm Hg, or if required for comorbid conditions; initial target is <180 />10 mm Hg. Control seizures with benzodiazepines followed by fosphenytoin or phenytoin. Maintain euvolemia and normothermia.
Thrombolysis: For ischemic stroke only, administer IV alteplase within 4.5 hours of symptom onset if criteria are met. Avoid antiplatelet and anticoagulant therapy for 24 hours post-tPA.
Contraindications: Prior intracranial hemorrhage, recent stroke or head trauma (<3 months), major surgery (<14 days), uncontrolled hypertension, bleeding diathesis, recent mi, inr>1.7, platelets <100,000, intracranial neoplasm, seizure at onset, rapidly improving symptoms, pregnancy, recent internal bleeding, glucose <50 mg />L, age <18 years.< />pan>
3-4.5 hour exclusions: Age >80, oral anticoagulant use, NIHSS >25 or >1/3 MCA involvement, prior stroke plus diabetes.
Manage cerebral edema with head elevation, controlled ventilation (PaCO₂ 35–40 mm Hg), mannitol, and neurosurgical consultation when indicated. Selected patients may undergo intra-arterial thrombolysis or mechanical thrombectomy.
Medications
First line: Alteplase 0.9 mg/kg IV (max 90 mg), aspirin 81–325 mg PO/PR, labetalol IV bolus and infusion.
Second line: Clopidogrel, diazepam, enalapril, hydralazine, mannitol, nicardipine, nitroprusside, trimethaphan.
Pediatrics: Heparin or LMWH often used; pediatric stroke consultation available via 1-800-NOCLOTS.
Disposition
All acute strokes require hospital admission. ICU admission is indicated for depressed consciousness, hemodynamic instability, serious arrhythmias, elevated ICP, or tPA administration.
Discharge may be considered for completed strokes days to weeks old in patients who are functionally independent or have reliable support.
Follow-Up Care
Neurology consultation, primary care follow-up, and rehabilitation services including speech and occupational therapy.
Clinical Pearls
Document prehospital observations carefully. Accurate symptom onset time is critical for thrombolysis eligibility. Avoid rapid BP reduction to prevent cerebral hypoperfusion. Door-to-needle time goal is under 60 minutes.
Overview
A cerebrovascular accident (CVA) results from interruption of blood flow to a specific brain region. Clinical deficits correspond to the vascular territory involved. Onset may be abrupt and complete or stepwise and fluctuating. Stroke accounts for ~1 in 18 deaths in the United States, with ~610,000 new cases annually.
Predisposing Factors
Hypertension, diabetes mellitus, smoking, coronary artery disease, cardiac dysrhythmias, peripheral vascular disease, oral contraceptive use, polycythemia vera, sickle cell disease, antithrombin III deficiency, protein C or S deficiency.
Pathologic Mechanisms
Ischemic stroke includes thrombotic, embolic, dissection-related, or hypoperfusion etiologies. Thrombotic stroke most often results from clot formation at an ulcerated atherosclerotic plaque or from sludging states (sickle cell disease, polycythemia vera, protein C deficiency). Embolic stroke arises from cardiac mural thrombi (atrial fibrillation, mitral stenosis, cardiomyopathy, CHF, MI), prosthetic or abnormal valves, carotid or aortic arch plaques, atrial myxoma, or ventricular aneurysm thrombi. Arterial dissection may involve carotid arteries or be associated with arteritis (giant cell, Takayasu) or fibromuscular dysplasia. Global ischemic stroke results from systemic hypotension due to sepsis, hemorrhage, or shock. Hemorrhagic stroke includes intracerebral and subarachnoid hemorrhage.
Pediatrics: Usually secondary to underlying disease (sickle cell disease, leukemia, infection, blood dyscrasia); younger children often present with seizures or altered mental status.
Clinical Features
History focuses on exact time of onset or last known normal, trauma or surgery, medications, confusion, headache, vertigo, and focal neurologic deficits.
General exam may show Cheyne–Stokes respirations, apnea, hypertension, dysrhythmias, or murmurs.
Anterior cerebral artery involvement causes contralateral leg-predominant weakness and sensory loss, apraxia, confusion, and impaired judgment.
Middle cerebral artery involvement causes contralateral face and arm weakness, hemisensory loss, homonymous hemianopsia, aphasia or dysarthria, and agnosia.
Posterior cerebral artery involvement causes cortical blindness, visual agnosia, memory impairment, altered mental status, third-nerve palsy, or hemiballismus.
Vertebrobasilar strokes cause vertigo, diplopia, nystagmus, visual field defects, and crossed cranial nerve and motor deficits; basilar artery occlusion may lead to quadriplegia, locked-in syndrome, or coma.
Watershed infarcts produce proximal limb weakness with sparing of face, hands, and feet.
Initial Evaluation Priorities
Perform a focused neurologic examination and calculate the NIH Stroke Scale when possible. Obtain emergent noncontrast head CT to differentiate ischemic from hemorrhagic stroke; early CT may be normal within 24–48 hours. Goals include CT completion within 25 minutes, interpretation within 45 minutes, and thrombolytic administration within 60 minutes if indicated. If CT is negative but subarachnoid hemorrhage is suspected, perform lumbar puncture. Obtain ECG, oxygen saturation, and rapid blood glucose.
Diagnostic Studies
Laboratory tests include CBC, electrolytes, renal and liver function, PT/PTT, urinalysis, and ESR when indicated. Additional studies may include cardiac enzymes, pregnancy test, toxicology screen, alcohol level, ABG, and blood cultures. Imaging may include MRI for early ischemia, chest radiograph, and carotid ultrasound. ECG evaluates for arrhythmia; lumbar puncture is required if CT is nondiagnostic and SAH remains suspected.
Key Differentials
Intracranial hemorrhage, hypoglycemia, seizure with Todd paralysis, conversion disorder, transient global amnesia, encephalitis or meningitis, peripheral neuropathy, intracranial abscess, migraine, air embolism, TIA, metabolic encephalopathy, neoplasm, vasculitis, multiple sclerosis, compressive myelopathy, vestibulitis, medication or toxin effects.
Prehospital Considerations
Patients may have impaired movement or communication. Field neurologic assessment should include level of consciousness, GCS, speech, facial symmetry, gait, and motor deficits. Fingerstick glucose is essential.
Stabilization Measures
Ensure airway protection; provide supplemental oxygen at 2–4 L/min. Intubation may be required for airway control or ICP management. For altered mental status, administer naloxone and thiamine and correct hypoglycemia.
Emergency Department Management
Treat severe hypertension only if SBP >220 mm Hg or DBP >120 mm Hg, or if required for comorbid conditions; initial target is <180 />10 mm Hg. Control seizures with benzodiazepines followed by fosphenytoin or phenytoin. Maintain euvolemia and normothermia.
Thrombolysis: For ischemic stroke only, administer IV alteplase within 4.5 hours of symptom onset if criteria are met. Avoid antiplatelet and anticoagulant therapy for 24 hours post-tPA.
Contraindications: Prior intracranial hemorrhage, recent stroke or head trauma (<3 months), major surgery (<14 days), uncontrolled hypertension, bleeding diathesis, recent mi, inr>1.7, platelets <100,000, intracranial neoplasm, seizure at onset, rapidly improving symptoms, pregnancy, recent internal bleeding, glucose <50 mg />L, age <18 years.< />pan>
3-4.5 hour exclusions: Age >80, oral anticoagulant use, NIHSS >25 or >1/3 MCA involvement, prior stroke plus diabetes.
Manage cerebral edema with head elevation, controlled ventilation (PaCO₂ 35–40 mm Hg), mannitol, and neurosurgical consultation when indicated. Selected patients may undergo intra-arterial thrombolysis or mechanical thrombectomy.
Medications
First line: Alteplase 0.9 mg/kg IV (max 90 mg), aspirin 81–325 mg PO/PR, labetalol IV bolus and infusion.
Second line: Clopidogrel, diazepam, enalapril, hydralazine, mannitol, nicardipine, nitroprusside, trimethaphan.
Pediatrics: Heparin or LMWH often used; pediatric stroke consultation available via 1-800-NOCLOTS.
Disposition
All acute strokes require hospital admission. ICU admission is indicated for depressed consciousness, hemodynamic instability, serious arrhythmias, elevated ICP, or tPA administration.
Discharge may be considered for completed strokes days to weeks old in patients who are functionally independent or have reliable support.
Follow-Up Care
Neurology consultation, primary care follow-up, and rehabilitation services including speech and occupational therapy.
Clinical Pearls
Document prehospital observations carefully. Accurate symptom onset time is critical for thrombolysis eligibility. Avoid rapid BP reduction to prevent cerebral hypoperfusion. Door-to-needle time goal is under 60 minutes.
- Published on
Emergency and Acute Medicine – Central Retinal Vein Occlusion
Overview
Central retinal vein occlusion (CRVO) is characterized by decreased visual acuity due to venous outflow obstruction of the retina. Vision loss is typically acute, unilateral, and painless. The condition results from impaired venous drainage leading to retinal hemorrhage, edema, and ischemia.
Pathophysiologic Types
Ischemic CRVO accounts for approximately 20–25% of cases and represents complete venous obstruction. Blocked venous return causes capillary backflow, extensive hemorrhage, macular edema, and retinal ischemia. Thrombosis is promoted by limited space at the lamina cribrosa, slow blood flow, vessel wall changes, adjacent arteriosclerotic arterial compression, and increased blood viscosity.
Nonischemic CRVO represents partial or incomplete occlusion and is generally milder with better visual prognosis.
Clinical Features
Patients present with acute, painless, unilateral loss of vision. In nonischemic CRVO, vision loss may be intermittent or incomplete. Visual acuity is often severely reduced, commonly worse than 20/200. An afferent pupillary defect may be present. Fundoscopic examination reveals dilated and tortuous retinal veins, widespread retinal hemorrhages involving all four quadrants in central involvement, optic disc edema, and cotton wool spots. Extensive hemorrhage produces the classic “blood and thunder” appearance.
Essential Assessment
Measure blood pressure. Perform visual acuity testing, visual field assessment, fundoscopy, and tonometry. Normal intraocular pressure ranges from 10–21 mm Hg.
Diagnostic Evaluation
Laboratory studies include CBC, PT/PTT, ESR, ANA, and serum protein electrophoresis to assess for systemic or hyperviscosity conditions. Fluorescein angiography, performed by ophthalmology, differentiates ischemic from nonischemic CRVO by identifying areas of capillary nonperfusion. Gonioscopy is used to evaluate for iris or angle neovascularization.
Differential Considerations
Amaurosis fugax or TIA, cavernous sinus thrombosis, diabetic or hypertensive retinopathy, hyperviscosity syndromes (sickle cell disease, polycythemia, leukemia, multiple myeloma), ocular ischemia syndrome, papilledema, retinal artery occlusion, retinal detachment, temporal arteritis, vitreous hemorrhage, severe anemia with thrombocytopenia, and functional vision loss.
Initial Management Principles
There are no prehospital eye-specific interventions. In the ED, address elevated intraocular pressure if present and manage underlying systemic conditions. The cornerstone of management is early recognition and urgent ophthalmologic referral.
Emergency Department Management
No therapy has proven definitive benefit in the ED setting. In consultation with ophthalmology, attempted therapies may include aspirin, anti-inflammatory agents, systemic corticosteroids, systemic anticoagulation, fibrinolytics (controversial), or laser chorioretinal anastomosis.
Definitive and Ophthalmologic Therapies
Ophthalmologists may use intravitreal corticosteroids such as triamcinolone or antivascular endothelial growth factor agents such as bevacizumab. Panretinal photocoagulation is often performed if neovascularization develops.
Disposition and Follow-Up
Admission depends on ophthalmologic assessment and need for intervention. Patients may be discharged if immediate ophthalmology follow-up is ensured. If ophthalmologic care is unavailable, initiate management of associated conditions and transfer to a facility with specialty services. Long-term follow-up is essential, particularly for ischemic CRVO, to detect neovascularization and secondary glaucoma. Patients require full medical evaluation for underlying vascular disease and comorbidity management.
Clinical Insights and Pitfalls
Elevated intraocular pressure from edema or neovascularization can worsen ischemia and lead to permanent vision loss if untreated. Bilateral CRVO or CRVO in young patients should prompt evaluation for hyperviscosity syndromes and systemic disease.
Overview
Central retinal vein occlusion (CRVO) is characterized by decreased visual acuity due to venous outflow obstruction of the retina. Vision loss is typically acute, unilateral, and painless. The condition results from impaired venous drainage leading to retinal hemorrhage, edema, and ischemia.
Pathophysiologic Types
Ischemic CRVO accounts for approximately 20–25% of cases and represents complete venous obstruction. Blocked venous return causes capillary backflow, extensive hemorrhage, macular edema, and retinal ischemia. Thrombosis is promoted by limited space at the lamina cribrosa, slow blood flow, vessel wall changes, adjacent arteriosclerotic arterial compression, and increased blood viscosity.
Nonischemic CRVO represents partial or incomplete occlusion and is generally milder with better visual prognosis.
Clinical Features
Patients present with acute, painless, unilateral loss of vision. In nonischemic CRVO, vision loss may be intermittent or incomplete. Visual acuity is often severely reduced, commonly worse than 20/200. An afferent pupillary defect may be present. Fundoscopic examination reveals dilated and tortuous retinal veins, widespread retinal hemorrhages involving all four quadrants in central involvement, optic disc edema, and cotton wool spots. Extensive hemorrhage produces the classic “blood and thunder” appearance.
Essential Assessment
Measure blood pressure. Perform visual acuity testing, visual field assessment, fundoscopy, and tonometry. Normal intraocular pressure ranges from 10–21 mm Hg.
Diagnostic Evaluation
Laboratory studies include CBC, PT/PTT, ESR, ANA, and serum protein electrophoresis to assess for systemic or hyperviscosity conditions. Fluorescein angiography, performed by ophthalmology, differentiates ischemic from nonischemic CRVO by identifying areas of capillary nonperfusion. Gonioscopy is used to evaluate for iris or angle neovascularization.
Differential Considerations
Amaurosis fugax or TIA, cavernous sinus thrombosis, diabetic or hypertensive retinopathy, hyperviscosity syndromes (sickle cell disease, polycythemia, leukemia, multiple myeloma), ocular ischemia syndrome, papilledema, retinal artery occlusion, retinal detachment, temporal arteritis, vitreous hemorrhage, severe anemia with thrombocytopenia, and functional vision loss.
Initial Management Principles
There are no prehospital eye-specific interventions. In the ED, address elevated intraocular pressure if present and manage underlying systemic conditions. The cornerstone of management is early recognition and urgent ophthalmologic referral.
Emergency Department Management
No therapy has proven definitive benefit in the ED setting. In consultation with ophthalmology, attempted therapies may include aspirin, anti-inflammatory agents, systemic corticosteroids, systemic anticoagulation, fibrinolytics (controversial), or laser chorioretinal anastomosis.
Definitive and Ophthalmologic Therapies
Ophthalmologists may use intravitreal corticosteroids such as triamcinolone or antivascular endothelial growth factor agents such as bevacizumab. Panretinal photocoagulation is often performed if neovascularization develops.
Disposition and Follow-Up
Admission depends on ophthalmologic assessment and need for intervention. Patients may be discharged if immediate ophthalmology follow-up is ensured. If ophthalmologic care is unavailable, initiate management of associated conditions and transfer to a facility with specialty services. Long-term follow-up is essential, particularly for ischemic CRVO, to detect neovascularization and secondary glaucoma. Patients require full medical evaluation for underlying vascular disease and comorbidity management.
Clinical Insights and Pitfalls
Elevated intraocular pressure from edema or neovascularization can worsen ischemia and lead to permanent vision loss if untreated. Bilateral CRVO or CRVO in young patients should prompt evaluation for hyperviscosity syndromes and systemic disease.
- Published on
Emergency and Acute Medicine – Cerebral Aneurysm
Core Overview
A cerebral aneurysm is a focal dilation or outpouching of a cerebral artery wall. It occurs in approximately 5–10% of the population. Rupture of saccular aneurysms accounts for 5–15% of all strokes. Distribution of ruptured aneurysms includes the anterior communicating artery (≈40%), internal carotid artery (≈30%), middle cerebral artery (≈20%), and vertebrobasilar system (≈5–10%).
Underlying Causes and Associations
Most cerebral aneurysms are saccular (berry) aneurysms, representing about 90% of cases. They develop at arterial bifurcations and weak points in vessel walls and increase in incidence with age. Multiple aneurysms occur in 20–30% of patients. Higher prevalence is seen with polycystic kidney disease, cerebral AVMs, connective tissue disorders (Ehlers–Danlos, Marfan), fibromuscular dysplasia, moyamoya syndrome, coarctation of the aorta, sickle cell disease, neurofibromatosis, and inflammatory or genetic disorders. Fusiform or dolichoectatic aneurysms account for about 7% and are more common in peripheral vessels. Mycotic aneurysms occur in roughly 10% of patients with bacterial endocarditis. Traumatic and neoplastic aneurysms are less common. A first-degree relative with an aneurysm nearly doubles lifetime risk. In children, aneurysms are rare but often large and located in the posterior circulation.
Clinical Presentation
Most aneurysms are asymptomatic until rupture. Sentinel headaches occur in 30–60% of patients and may precede rupture. Rupture leads to subarachnoid hemorrhage, typically presenting with a sudden, severe “thunderclap” headache described as the worst headache of life, often without focal deficits. Nuchal rigidity is common due to blood in the CSF. Seizures, syncope, or altered mental status may occur. Compression of adjacent structures can cause focal neurologic signs. ACA aneurysms may affect optic pathways, causing visual field deficits. Internal carotid–posterior communicating artery aneurysms often compress the oculomotor nerve, producing ptosis, diplopia, and a fixed dilated pupil. Cortical aneurysms may cause hemiparesis, aphasia, visual disturbances, or seizures.
Essential Evaluation
A complete neurologic examination is critical. Emergent noncontrast head CT detects 90–95% of subarachnoid hemorrhages. If CT is negative but suspicion remains high, lumbar puncture with CSF analysis is required.
Diagnostic Studies
Laboratory testing includes CBC, coagulation studies, electrolytes, renal and liver function tests, and arterial blood gas as indicated. Imaging includes chest radiography for pulmonary edema. Four-vessel cerebral angiography remains the diagnostic gold standard. CTA and MRA can identify aneurysms larger than 3 mm. Transcranial Doppler ultrasound is useful for monitoring vasospasm. Lumbar puncture is indicated when CT is normal but aneurysmal rupture is suspected.
Key Differentials
Consider arteriovenous malformation, intracranial hemorrhage (subdural, epidural, intracerebral), thromboembolic stroke, meningitis, encephalitis, migraine, optic neuritis, acute glaucoma, hypertensive encephalopathy, metabolic disturbances, sinusitis, and temporal arteritis.
Prehospital Priorities
Field neurologic assessment is valuable, including level of consciousness, speech, motor deficits, gait, and facial symmetry. Patients with suspected subarachnoid hemorrhage may require emergent airway protection and rapid transport to a facility with CT and ICU capabilities.
Initial Stabilization
Secure airway, breathing, and circulation. Provide supplemental oxygen and continuous cardiac and pulse oximetry monitoring. Rapid-sequence intubation may be necessary. Check blood glucose immediately in altered patients and correct hypoglycemia. Reverse anticoagulation when indicated. Control nausea and vomiting to prevent spikes in intracranial pressure. Treat seizures acutely with IV benzodiazepines and antiepileptics; routine seizure prophylaxis is not recommended.
Emergency Department Management
Early goals include prevention of rebleeding, vasospasm, and hydrocephalus. Management follows subarachnoid hemorrhage protocols. Early neurosurgical involvement is essential. Ventriculostomy may be required for intracranial pressure control and can reduce systemic hypertension.
Definitive Intervention
Timing of angiography and repair remains debated, though early intervention is favored to reduce rebleeding and vasospasm. Pediatric aneurysms carry a high hemorrhage risk and should be repaired early.
Pharmacologic Therapy
Blood pressure control is essential, commonly with labetalol or nicardipine. Nimodipine is used orally or via nasogastric tube to reduce vasospasm risk and should never be given intravenously. Antiemetics and stool softeners help prevent increases in intracranial pressure. Antiepileptics are used for active seizures.
Disposition and Follow-Up
All patients with aneurysmal subarachnoid hemorrhage require ICU admission. Symptomatic unruptured aneurysms warrant admission and urgent neurosurgical consultation due to high rupture risk. Incidentally discovered, asymptomatic aneurysms may be discharged with close neurosurgical follow-up. Annual rupture risk is approximately 1–2%, with treatment thresholds often considered in the 4–8 mm range.
Clinical Pearls and Pitfalls
A normal CT does not exclude subarachnoid hemorrhage—lumbar puncture is essential when suspicion persists. Vasospasm typically develops around day 3 after bleeding or surgery. Nimodipine reduces vasospasm-related morbidity but must never be administered intravenously. Avoid nitroprusside and nitroglycerin, as they can increase cerebral blood volume and intracranial pressure.
Core Overview
A cerebral aneurysm is a focal dilation or outpouching of a cerebral artery wall. It occurs in approximately 5–10% of the population. Rupture of saccular aneurysms accounts for 5–15% of all strokes. Distribution of ruptured aneurysms includes the anterior communicating artery (≈40%), internal carotid artery (≈30%), middle cerebral artery (≈20%), and vertebrobasilar system (≈5–10%).
Underlying Causes and Associations
Most cerebral aneurysms are saccular (berry) aneurysms, representing about 90% of cases. They develop at arterial bifurcations and weak points in vessel walls and increase in incidence with age. Multiple aneurysms occur in 20–30% of patients. Higher prevalence is seen with polycystic kidney disease, cerebral AVMs, connective tissue disorders (Ehlers–Danlos, Marfan), fibromuscular dysplasia, moyamoya syndrome, coarctation of the aorta, sickle cell disease, neurofibromatosis, and inflammatory or genetic disorders. Fusiform or dolichoectatic aneurysms account for about 7% and are more common in peripheral vessels. Mycotic aneurysms occur in roughly 10% of patients with bacterial endocarditis. Traumatic and neoplastic aneurysms are less common. A first-degree relative with an aneurysm nearly doubles lifetime risk. In children, aneurysms are rare but often large and located in the posterior circulation.
Clinical Presentation
Most aneurysms are asymptomatic until rupture. Sentinel headaches occur in 30–60% of patients and may precede rupture. Rupture leads to subarachnoid hemorrhage, typically presenting with a sudden, severe “thunderclap” headache described as the worst headache of life, often without focal deficits. Nuchal rigidity is common due to blood in the CSF. Seizures, syncope, or altered mental status may occur. Compression of adjacent structures can cause focal neurologic signs. ACA aneurysms may affect optic pathways, causing visual field deficits. Internal carotid–posterior communicating artery aneurysms often compress the oculomotor nerve, producing ptosis, diplopia, and a fixed dilated pupil. Cortical aneurysms may cause hemiparesis, aphasia, visual disturbances, or seizures.
Essential Evaluation
A complete neurologic examination is critical. Emergent noncontrast head CT detects 90–95% of subarachnoid hemorrhages. If CT is negative but suspicion remains high, lumbar puncture with CSF analysis is required.
Diagnostic Studies
Laboratory testing includes CBC, coagulation studies, electrolytes, renal and liver function tests, and arterial blood gas as indicated. Imaging includes chest radiography for pulmonary edema. Four-vessel cerebral angiography remains the diagnostic gold standard. CTA and MRA can identify aneurysms larger than 3 mm. Transcranial Doppler ultrasound is useful for monitoring vasospasm. Lumbar puncture is indicated when CT is normal but aneurysmal rupture is suspected.
Key Differentials
Consider arteriovenous malformation, intracranial hemorrhage (subdural, epidural, intracerebral), thromboembolic stroke, meningitis, encephalitis, migraine, optic neuritis, acute glaucoma, hypertensive encephalopathy, metabolic disturbances, sinusitis, and temporal arteritis.
Prehospital Priorities
Field neurologic assessment is valuable, including level of consciousness, speech, motor deficits, gait, and facial symmetry. Patients with suspected subarachnoid hemorrhage may require emergent airway protection and rapid transport to a facility with CT and ICU capabilities.
Initial Stabilization
Secure airway, breathing, and circulation. Provide supplemental oxygen and continuous cardiac and pulse oximetry monitoring. Rapid-sequence intubation may be necessary. Check blood glucose immediately in altered patients and correct hypoglycemia. Reverse anticoagulation when indicated. Control nausea and vomiting to prevent spikes in intracranial pressure. Treat seizures acutely with IV benzodiazepines and antiepileptics; routine seizure prophylaxis is not recommended.
Emergency Department Management
Early goals include prevention of rebleeding, vasospasm, and hydrocephalus. Management follows subarachnoid hemorrhage protocols. Early neurosurgical involvement is essential. Ventriculostomy may be required for intracranial pressure control and can reduce systemic hypertension.
Definitive Intervention
Timing of angiography and repair remains debated, though early intervention is favored to reduce rebleeding and vasospasm. Pediatric aneurysms carry a high hemorrhage risk and should be repaired early.
Pharmacologic Therapy
Blood pressure control is essential, commonly with labetalol or nicardipine. Nimodipine is used orally or via nasogastric tube to reduce vasospasm risk and should never be given intravenously. Antiemetics and stool softeners help prevent increases in intracranial pressure. Antiepileptics are used for active seizures.
Disposition and Follow-Up
All patients with aneurysmal subarachnoid hemorrhage require ICU admission. Symptomatic unruptured aneurysms warrant admission and urgent neurosurgical consultation due to high rupture risk. Incidentally discovered, asymptomatic aneurysms may be discharged with close neurosurgical follow-up. Annual rupture risk is approximately 1–2%, with treatment thresholds often considered in the 4–8 mm range.
Clinical Pearls and Pitfalls
A normal CT does not exclude subarachnoid hemorrhage—lumbar puncture is essential when suspicion persists. Vasospasm typically develops around day 3 after bleeding or surgery. Nimodipine reduces vasospasm-related morbidity but must never be administered intravenously. Avoid nitroprusside and nitroglycerin, as they can increase cerebral blood volume and intracranial pressure.

- Published on
Emergency And Acute Medicine – Cirrhosis
Overview And Pathophysiology
Cirrhosis is a progressive and chronic disease marked by ongoing inflammation, hepatocellular injury and necrosis, diffuse fibrosis, and the formation of regenerative nodules. These changes lead to distortion and eventual loss of normal hepatic lobular and vascular architecture. In advanced stages, cirrhosis is irreversible and results in intrahepatic portal hypertension due to increased sinusoidal resistance, compression of central veins, and abnormal arterial–portal venous shunting. Cirrhosis is a major public health concern and is among the leading causes of death in the United States.
Etiology And Risk Factors
Chronic alcohol abuse is the most common cause of cirrhosis in the United States, followed by chronic viral hepatitis B and C. Other causes include autoimmune hepatitis, primary biliary cirrhosis, secondary biliary cirrhosis from sclerosing cholangitis, and metabolic disorders such as hereditary hemochromatosis, Wilson disease, and porphyria. Drug-induced liver injury from agents such as acetaminophen, methotrexate, amiodarone, and methyldopa may contribute. Hepatic congestion from right-sided heart failure, constrictive pericarditis, or Budd–Chiari syndrome can lead to cirrhosis. Infiltrative diseases, nonalcoholic steatohepatitis, diffuse hepatocellular carcinoma, and chronic infections such as schistosomiasis or tertiary syphilis are less common causes. Pediatric causes include congenital biliary disorders, metabolic diseases, cystic fibrosis, and α1-antitrypsin deficiency.
Clinical Presentation
Cirrhosis may remain asymptomatic for years or present insidiously with nonspecific complaints such as fatigue, malaise, anorexia, nausea, weight loss, pruritus, and jaundice. Physical findings may include hepatomegaly, splenomegaly, abdominal discomfort, collateral venous circulation with caput medusae, palmar erythema, spider telangiectasias, parotid enlargement, clubbing, and nail changes. Endocrine manifestations include gynecomastia, testicular atrophy, impotence, amenorrhea, and loss of libido. Advanced disease may present with hypotension, fever, fetor hepaticus, asterixis, renal dysfunction, and signs of portal hypertension.
Complications And Decompensated Disease
The development of complications defines decompensated cirrhosis. These include ascites, spontaneous bacterial peritonitis, hepatic encephalopathy, and variceal hemorrhage. Hepatic encephalopathy may be precipitated by gastrointestinal bleeding, infection, excessive dietary protein, electrolyte abnormalities, sedatives, constipation, or renal failure. Variceal bleeding occurs in approximately one-third of patients and carries a high mortality rate with each episode. Other complications include portal hypertensive gastropathy, hepatorenal syndrome due to reduced renal perfusion, and hepatopulmonary syndrome characterized by intrapulmonary vascular dilation and hypoxemia.
Diagnostic Evaluation
Diagnosis relies on a thorough history and physical examination supported by laboratory and imaging studies. Laboratory findings may include anemia, macrocytosis, leukopenia, thrombocytopenia, hypoalbuminemia, hyperbilirubinemia, prolonged prothrombin time, and elevated globulins. Transaminase levels reflect ongoing injury, with an AST to ALT ratio greater than two suggesting alcoholic liver disease. Additional testing is directed at identifying the underlying cause and complications, including viral hepatitis serologies, autoimmune markers, iron studies, ceruloplasmin, α1-antitrypsin levels, and α-fetoprotein. Ultrasound is used to assess liver architecture, ascites, splenomegaly, and portal vein patency, while CT imaging further evaluates abnormal findings. Endoscopy is indicated for variceal surveillance or upper gastrointestinal bleeding, and paracentesis is essential for new or worsening ascites or suspected spontaneous bacterial peritonitis.
Emergency And Acute Management
Initial management focuses on stabilizing the patient and treating life-threatening complications. Altered mental status should prompt administration of dextrose, thiamine, and naloxone as indicated. Hypotension should be corrected with intravenous fluids to prevent ischemic liver injury. Suspected variceal bleeding requires proton pump inhibitors, octreotide infusion, correction of coagulopathy, and urgent endoscopic intervention. Broad-spectrum antibiotics are indicated for suspected sepsis or spontaneous bacterial peritonitis. Hepatic encephalopathy is treated with lactulose and correction of precipitating factors. Ascites management includes sodium restriction, diuretics, and therapeutic paracentesis when necessary.
Definitive And Specialized Therapy
Treatment of underlying etiologies includes phlebotomy or chelation for hemochromatosis, immunosuppressive therapy for autoimmune hepatitis, antiviral therapy for chronic viral hepatitis when appropriate, ursodeoxycholic acid for primary biliary cirrhosis, and chelation therapy for Wilson disease. Nonselective β-blockers reduce the risk of variceal bleeding. Nutritional support with adequate calories and protein is essential unless limited by encephalopathy. Liver transplantation remains the only curative option for advanced cirrhosis.
Disposition And Follow-Up
Patients with acute decompensation, gastrointestinal bleeding, sepsis, advanced hepatic encephalopathy, hepatorenal syndrome, or hepatopulmonary syndrome require hospital admission, often to an intensive care unit. Patients with compensated cirrhosis and no acute complications may be managed as outpatients with close gastroenterology follow-up. All newly diagnosed patients should be referred for specialist evaluation and long-term management.
Clinical Pearls And Pitfalls
Cirrhosis presents with a wide range of clinical manifestations, and prognosis varies significantly depending on disease severity and complications. Any complication signals transition to decompensated disease and worsens prognosis. Symptoms of spontaneous bacterial peritonitis may be subtle, requiring a low threshold for diagnostic paracentesis. Early recognition and aggressive management of complications are critical to improving outcomes.
Overview And Pathophysiology
Cirrhosis is a progressive and chronic disease marked by ongoing inflammation, hepatocellular injury and necrosis, diffuse fibrosis, and the formation of regenerative nodules. These changes lead to distortion and eventual loss of normal hepatic lobular and vascular architecture. In advanced stages, cirrhosis is irreversible and results in intrahepatic portal hypertension due to increased sinusoidal resistance, compression of central veins, and abnormal arterial–portal venous shunting. Cirrhosis is a major public health concern and is among the leading causes of death in the United States.
Etiology And Risk Factors
Chronic alcohol abuse is the most common cause of cirrhosis in the United States, followed by chronic viral hepatitis B and C. Other causes include autoimmune hepatitis, primary biliary cirrhosis, secondary biliary cirrhosis from sclerosing cholangitis, and metabolic disorders such as hereditary hemochromatosis, Wilson disease, and porphyria. Drug-induced liver injury from agents such as acetaminophen, methotrexate, amiodarone, and methyldopa may contribute. Hepatic congestion from right-sided heart failure, constrictive pericarditis, or Budd–Chiari syndrome can lead to cirrhosis. Infiltrative diseases, nonalcoholic steatohepatitis, diffuse hepatocellular carcinoma, and chronic infections such as schistosomiasis or tertiary syphilis are less common causes. Pediatric causes include congenital biliary disorders, metabolic diseases, cystic fibrosis, and α1-antitrypsin deficiency.
Clinical Presentation
Cirrhosis may remain asymptomatic for years or present insidiously with nonspecific complaints such as fatigue, malaise, anorexia, nausea, weight loss, pruritus, and jaundice. Physical findings may include hepatomegaly, splenomegaly, abdominal discomfort, collateral venous circulation with caput medusae, palmar erythema, spider telangiectasias, parotid enlargement, clubbing, and nail changes. Endocrine manifestations include gynecomastia, testicular atrophy, impotence, amenorrhea, and loss of libido. Advanced disease may present with hypotension, fever, fetor hepaticus, asterixis, renal dysfunction, and signs of portal hypertension.
Complications And Decompensated Disease
The development of complications defines decompensated cirrhosis. These include ascites, spontaneous bacterial peritonitis, hepatic encephalopathy, and variceal hemorrhage. Hepatic encephalopathy may be precipitated by gastrointestinal bleeding, infection, excessive dietary protein, electrolyte abnormalities, sedatives, constipation, or renal failure. Variceal bleeding occurs in approximately one-third of patients and carries a high mortality rate with each episode. Other complications include portal hypertensive gastropathy, hepatorenal syndrome due to reduced renal perfusion, and hepatopulmonary syndrome characterized by intrapulmonary vascular dilation and hypoxemia.
Diagnostic Evaluation
Diagnosis relies on a thorough history and physical examination supported by laboratory and imaging studies. Laboratory findings may include anemia, macrocytosis, leukopenia, thrombocytopenia, hypoalbuminemia, hyperbilirubinemia, prolonged prothrombin time, and elevated globulins. Transaminase levels reflect ongoing injury, with an AST to ALT ratio greater than two suggesting alcoholic liver disease. Additional testing is directed at identifying the underlying cause and complications, including viral hepatitis serologies, autoimmune markers, iron studies, ceruloplasmin, α1-antitrypsin levels, and α-fetoprotein. Ultrasound is used to assess liver architecture, ascites, splenomegaly, and portal vein patency, while CT imaging further evaluates abnormal findings. Endoscopy is indicated for variceal surveillance or upper gastrointestinal bleeding, and paracentesis is essential for new or worsening ascites or suspected spontaneous bacterial peritonitis.
Emergency And Acute Management
Initial management focuses on stabilizing the patient and treating life-threatening complications. Altered mental status should prompt administration of dextrose, thiamine, and naloxone as indicated. Hypotension should be corrected with intravenous fluids to prevent ischemic liver injury. Suspected variceal bleeding requires proton pump inhibitors, octreotide infusion, correction of coagulopathy, and urgent endoscopic intervention. Broad-spectrum antibiotics are indicated for suspected sepsis or spontaneous bacterial peritonitis. Hepatic encephalopathy is treated with lactulose and correction of precipitating factors. Ascites management includes sodium restriction, diuretics, and therapeutic paracentesis when necessary.
Definitive And Specialized Therapy
Treatment of underlying etiologies includes phlebotomy or chelation for hemochromatosis, immunosuppressive therapy for autoimmune hepatitis, antiviral therapy for chronic viral hepatitis when appropriate, ursodeoxycholic acid for primary biliary cirrhosis, and chelation therapy for Wilson disease. Nonselective β-blockers reduce the risk of variceal bleeding. Nutritional support with adequate calories and protein is essential unless limited by encephalopathy. Liver transplantation remains the only curative option for advanced cirrhosis.
Disposition And Follow-Up
Patients with acute decompensation, gastrointestinal bleeding, sepsis, advanced hepatic encephalopathy, hepatorenal syndrome, or hepatopulmonary syndrome require hospital admission, often to an intensive care unit. Patients with compensated cirrhosis and no acute complications may be managed as outpatients with close gastroenterology follow-up. All newly diagnosed patients should be referred for specialist evaluation and long-term management.
Clinical Pearls And Pitfalls
Cirrhosis presents with a wide range of clinical manifestations, and prognosis varies significantly depending on disease severity and complications. Any complication signals transition to decompensated disease and worsens prognosis. Symptoms of spontaneous bacterial peritonitis may be subtle, requiring a low threshold for diagnostic paracentesis. Early recognition and aggressive management of complications are critical to improving outcomes.
- Published on
Emergency And Acute Medicine – Chronic Obstructive Pulmonary Disease
Overview And Disease Process
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death in the United States and affects approximately 10% of the population, including nearly half of long-term smokers. It is characterized by persistent airflow limitation resulting from a combination of emphysema, chronic bronchitis, and components of reactive airway disease. Emphysema involves irreversible alveolar destruction with loss of elastic recoil, while chronic bronchitis is defined by airway inflammation without alveolar damage. Reactive airway disease contributes reversible bronchospasm, mucus plugging, and mucosal edema. Patients frequently have comorbid hypertension, diabetes, heart failure, and cardiovascular disease. Recurrent exacerbations are associated with increased mortality, faster decline in lung function, poorer quality of life, and higher rates of hospitalization.
Risk Factors And Causes
Cigarette smoking is the primary cause, with COPD developing in approximately 15% of smokers. Additional risk factors include air pollution, airway hyperresponsiveness, genetic conditions such as α1-antitrypsin deficiency, and possible autoimmune mechanisms. Acute exacerbations are most commonly triggered by infections. Viral infections account for more than half of exacerbations, particularly rhinovirus and respiratory syncytial virus. Bacterial pathogens are isolated in 40–60% of cases, most often Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumoniae. Exacerbations are more likely when dyspnea worsens, sputum volume increases, and sputum becomes purulent. Environmental pollutants, reduced immunity, and seasonal variation—especially winter months—also contribute.
Clinical Presentation
Patients commonly report progressive dyspnea on exertion, chronic cough, sputum production, wheezing, fatigue, and sometimes orthopnea. In advanced cases, altered mental status may occur due to carbon dioxide retention. Physical examination may reveal wheezing, prolonged expiratory phase, decreased air movement, use of accessory muscles, barrel chest, cyanosis, jugular venous distension, peripheral edema, and cardiac gallops. Severe disease may lead to carbon dioxide narcosis with confusion or somnolence.
Diagnostic Evaluation
Laboratory studies may show secondary polycythemia from chronic hypoxemia or leukocytosis during infectious exacerbations. Arterial blood gas analysis often demonstrates hypercapnia with or without acidosis and impaired oxygenation. β-natriuretic peptide testing may help differentiate COPD exacerbation from heart failure. Chest radiography is used to identify pneumonia, pneumothorax, heart failure, or lobar collapse, while computed tomography is reserved for suspected pulmonary embolism or further disease characterization. Pulse oximetry, electrocardiography, pulmonary function testing, and echocardiography are useful adjuncts depending on clinical context.
Differential Diagnosis
Conditions that may mimic or coexist with a COPD exacerbation include pneumothorax, pneumonia, congestive heart failure, pulmonary embolism, asthma, upper airway obstruction, restrictive lung disease, acute respiratory distress syndrome, pleural effusion, acute coronary syndrome, pericardial effusion, and metabolic derangements.
Early And Emergency Management
Initial prehospital and emergency care focuses on supplemental oxygen and rapid bronchodilation. Oxygen should not be withheld due to fear of carbon dioxide retention; instead, patients should be closely monitored. In the emergency department, oxygen therapy is titrated to maintain oxygen saturation above 90–92%, with careful observation for hypoventilation. Noninvasive positive pressure ventilation is the preferred method of ventilatory support for hypercapnic respiratory failure and can often prevent intubation. Endotracheal intubation is reserved for patients with clinical fatigue, worsening mental status, inability to tolerate therapy, or ineffective ventilation.
Definitive Treatment
Management includes continuous cardiac and oxygen monitoring, inhaled short-acting β-agonists and anticholinergics, and systemic corticosteroids to reduce airway inflammation and relapse risk. Antibiotics are indicated when fever, increased sputum production, or worsening dyspnea suggests bacterial infection, with macrolides offering potential additional anti-inflammatory benefit. Ventilator strategies should allow sufficient expiratory time to minimize air trapping, accepting permissive hypercapnia when necessary.
Disposition And Follow-Up
Intensive care admission is required for patients needing intubation, those with severe acidosis, refractory hypoxemia, carbon dioxide narcosis, or significant comorbid cardiac or pulmonary disease. Hospital admission is appropriate for patients with pneumonia, lobar collapse, increased work of breathing, or failure to improve with emergency treatment. Discharge may be considered for mild exacerbations that resolve in the emergency department with stable oxygen saturation above 92%. Long-term management includes smoking cessation, vaccination against influenza and pneumococcus, trigger avoidance, and consideration of specialist referral for advanced therapies such as lung volume reduction surgery.
Clinical Pearls And Pitfalls
Noninvasive positive pressure ventilation is the therapy of choice when optimal medical treatment is insufficient. Patients with COPD are at increased risk for cardiovascular disease, diabetes, and hypertension, emphasizing the importance of preventive care. Routine immunization and early recognition of exacerbations are essential to improving outcomes.
Overview And Disease Process
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death in the United States and affects approximately 10% of the population, including nearly half of long-term smokers. It is characterized by persistent airflow limitation resulting from a combination of emphysema, chronic bronchitis, and components of reactive airway disease. Emphysema involves irreversible alveolar destruction with loss of elastic recoil, while chronic bronchitis is defined by airway inflammation without alveolar damage. Reactive airway disease contributes reversible bronchospasm, mucus plugging, and mucosal edema. Patients frequently have comorbid hypertension, diabetes, heart failure, and cardiovascular disease. Recurrent exacerbations are associated with increased mortality, faster decline in lung function, poorer quality of life, and higher rates of hospitalization.
Risk Factors And Causes
Cigarette smoking is the primary cause, with COPD developing in approximately 15% of smokers. Additional risk factors include air pollution, airway hyperresponsiveness, genetic conditions such as α1-antitrypsin deficiency, and possible autoimmune mechanisms. Acute exacerbations are most commonly triggered by infections. Viral infections account for more than half of exacerbations, particularly rhinovirus and respiratory syncytial virus. Bacterial pathogens are isolated in 40–60% of cases, most often Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumoniae. Exacerbations are more likely when dyspnea worsens, sputum volume increases, and sputum becomes purulent. Environmental pollutants, reduced immunity, and seasonal variation—especially winter months—also contribute.
Clinical Presentation
Patients commonly report progressive dyspnea on exertion, chronic cough, sputum production, wheezing, fatigue, and sometimes orthopnea. In advanced cases, altered mental status may occur due to carbon dioxide retention. Physical examination may reveal wheezing, prolonged expiratory phase, decreased air movement, use of accessory muscles, barrel chest, cyanosis, jugular venous distension, peripheral edema, and cardiac gallops. Severe disease may lead to carbon dioxide narcosis with confusion or somnolence.
Diagnostic Evaluation
Laboratory studies may show secondary polycythemia from chronic hypoxemia or leukocytosis during infectious exacerbations. Arterial blood gas analysis often demonstrates hypercapnia with or without acidosis and impaired oxygenation. β-natriuretic peptide testing may help differentiate COPD exacerbation from heart failure. Chest radiography is used to identify pneumonia, pneumothorax, heart failure, or lobar collapse, while computed tomography is reserved for suspected pulmonary embolism or further disease characterization. Pulse oximetry, electrocardiography, pulmonary function testing, and echocardiography are useful adjuncts depending on clinical context.
Differential Diagnosis
Conditions that may mimic or coexist with a COPD exacerbation include pneumothorax, pneumonia, congestive heart failure, pulmonary embolism, asthma, upper airway obstruction, restrictive lung disease, acute respiratory distress syndrome, pleural effusion, acute coronary syndrome, pericardial effusion, and metabolic derangements.
Early And Emergency Management
Initial prehospital and emergency care focuses on supplemental oxygen and rapid bronchodilation. Oxygen should not be withheld due to fear of carbon dioxide retention; instead, patients should be closely monitored. In the emergency department, oxygen therapy is titrated to maintain oxygen saturation above 90–92%, with careful observation for hypoventilation. Noninvasive positive pressure ventilation is the preferred method of ventilatory support for hypercapnic respiratory failure and can often prevent intubation. Endotracheal intubation is reserved for patients with clinical fatigue, worsening mental status, inability to tolerate therapy, or ineffective ventilation.
Definitive Treatment
Management includes continuous cardiac and oxygen monitoring, inhaled short-acting β-agonists and anticholinergics, and systemic corticosteroids to reduce airway inflammation and relapse risk. Antibiotics are indicated when fever, increased sputum production, or worsening dyspnea suggests bacterial infection, with macrolides offering potential additional anti-inflammatory benefit. Ventilator strategies should allow sufficient expiratory time to minimize air trapping, accepting permissive hypercapnia when necessary.
Disposition And Follow-Up
Intensive care admission is required for patients needing intubation, those with severe acidosis, refractory hypoxemia, carbon dioxide narcosis, or significant comorbid cardiac or pulmonary disease. Hospital admission is appropriate for patients with pneumonia, lobar collapse, increased work of breathing, or failure to improve with emergency treatment. Discharge may be considered for mild exacerbations that resolve in the emergency department with stable oxygen saturation above 92%. Long-term management includes smoking cessation, vaccination against influenza and pneumococcus, trigger avoidance, and consideration of specialist referral for advanced therapies such as lung volume reduction surgery.
Clinical Pearls And Pitfalls
Noninvasive positive pressure ventilation is the therapy of choice when optimal medical treatment is insufficient. Patients with COPD are at increased risk for cardiovascular disease, diabetes, and hypertension, emphasizing the importance of preventive care. Routine immunization and early recognition of exacerbations are essential to improving outcomes.

- Published on
Emergency and acute medicine – penetrating chest trauma
Cause and mechanism
Penetrating chest trauma most commonly results from gunshot wounds or stab wounds. Less frequently, injury occurs from impalement on a sharp object following a fall or high-energy impact. These mechanisms place intrathoracic organs and major vessels at high risk for rapid deterioration.
Clinical features
Patients may present with an object impaled in the chest wall or an obvious penetrating wound with variable external bleeding. Common symptoms include chest pain, dyspnea, and respiratory distress. Altered mental status may occur secondary to hypoxemia or shock. Physical findings can include absent or asymmetric breath sounds, hypotension, and jugular venous distention, suggesting pneumothorax, hemothorax, or cardiac tamponade.
Initial evaluation
A rapid assessment of airway, breathing, and circulation is mandatory. The focused exam should evaluate respiratory effort, chest wall excursion, crepitus, subcutaneous emphysema, breath sounds, and heart sounds. An upright chest radiograph is preferred to identify pneumothorax, although a supine film should be obtained first if spinal precautions are required. Baseline hemoglobin, pulse oximetry, arterial blood gas, serum lactate, and type and screen should be obtained early.
Diagnostic studies
Echocardiography is indicated when tamponade is suspected or when a wound is near the heart. In penetrating precordial injuries, hemopericardium may decompress into the pleural space, so repeat pericardial ultrasound after chest tube placement is recommended. Electrocardiography assists in identifying myocardial injury. With gunshot wounds, imaging must account for all entry and exit sites, and additional studies of the abdomen or pelvis may be required. Arteriography is indicated if great vessel injury is suspected. Esophageal evaluation with contrast swallow or endoscopy and bronchoscopy should be considered when aerodigestive injury is possible.
Differential considerations
Life-threatening diagnoses include pneumothorax, tension or open pneumothorax, hemothorax, pulmonary contusion, myocardial contusion or rupture, pericardial tamponade, traumatic aortic injury, tracheobronchial or esophageal injury, diaphragmatic rupture, intra-abdominal injury, and spinal cord injury.
Prehospital priorities
All patients with signs of life should be transported rapidly to a trauma center. Full spinal immobilization is indicated when spinal injury is suspected. Impaled objects must never be removed in the field because they may be tamponading major bleeding. Suspected tension pneumothorax requires immediate needle decompression. Large open pneumothoraces should be covered with a three-sided occlusive dressing to prevent tension physiology. Transport should not be delayed for intravenous access.
Early resuscitation
Airway, breathing, and circulation management is the priority. Endotracheal intubation is indicated for respiratory distress, hypoxia, or hypotension. Supplemental oxygen should be provided to stable patients. Two large-bore peripheral IV lines should be established, with cautious fluid resuscitation. In penetrating aortic injury, permissive hypotension with a systolic pressure around 90 mm Hg is recommended until surgical control is achieved. Suspected tension pneumothorax requires immediate needle thoracostomy followed by chest tube placement without waiting for imaging. Pericardial tamponade with instability warrants emergency pericardiocentesis followed by rapid operative intervention.
Emergency department management
The trauma surgeon should be notified immediately. Tube thoracostomy is required for pneumothorax or hemothorax, using appropriately sized tubes. Aggressive crystalloid resuscitation should be avoided when pulmonary contusion is present. Wounds below the nipple line or posterior scapular tip raise concern for intra-abdominal injury and require further evaluation with ultrasound, CT, diagnostic peritoneal lavage, or operative exploration. Chest wounds should not be probed, and impaled objects should only be removed in the operating room. All foreign material should be preserved as forensic evidence. Tetanus prophylaxis should be updated as indicated.
Medications and supportive care
Analgesia and sedation should be provided using small, titrated doses of short-acting agents to avoid respiratory compromise. High-dose steroids for spinal cord injury remain controversial and should follow institutional protocols. Broad-spectrum intravenous antibiotics are indicated if wounds are grossly contaminated.
Disposition and outcomes
All patients with penetrating chest trauma require hospital admission. Hemodynamically unstable patients should proceed directly to the operating room. Emergency department thoracotomy may be lifesaving in selected patients with penetrating torso trauma who had signs of life in the field and short prehospital CPR duration. Large initial chest tube output or persistent bleeding mandates surgical intervention. Patients with isolated minor chest wall wounds and normal imaging may be observed briefly and discharged if repeat evaluation excludes intrathoracic injury and the patient remains stable.
Cause and mechanism
Penetrating chest trauma most commonly results from gunshot wounds or stab wounds. Less frequently, injury occurs from impalement on a sharp object following a fall or high-energy impact. These mechanisms place intrathoracic organs and major vessels at high risk for rapid deterioration.
Clinical features
Patients may present with an object impaled in the chest wall or an obvious penetrating wound with variable external bleeding. Common symptoms include chest pain, dyspnea, and respiratory distress. Altered mental status may occur secondary to hypoxemia or shock. Physical findings can include absent or asymmetric breath sounds, hypotension, and jugular venous distention, suggesting pneumothorax, hemothorax, or cardiac tamponade.
Initial evaluation
A rapid assessment of airway, breathing, and circulation is mandatory. The focused exam should evaluate respiratory effort, chest wall excursion, crepitus, subcutaneous emphysema, breath sounds, and heart sounds. An upright chest radiograph is preferred to identify pneumothorax, although a supine film should be obtained first if spinal precautions are required. Baseline hemoglobin, pulse oximetry, arterial blood gas, serum lactate, and type and screen should be obtained early.
Diagnostic studies
Echocardiography is indicated when tamponade is suspected or when a wound is near the heart. In penetrating precordial injuries, hemopericardium may decompress into the pleural space, so repeat pericardial ultrasound after chest tube placement is recommended. Electrocardiography assists in identifying myocardial injury. With gunshot wounds, imaging must account for all entry and exit sites, and additional studies of the abdomen or pelvis may be required. Arteriography is indicated if great vessel injury is suspected. Esophageal evaluation with contrast swallow or endoscopy and bronchoscopy should be considered when aerodigestive injury is possible.
Differential considerations
Life-threatening diagnoses include pneumothorax, tension or open pneumothorax, hemothorax, pulmonary contusion, myocardial contusion or rupture, pericardial tamponade, traumatic aortic injury, tracheobronchial or esophageal injury, diaphragmatic rupture, intra-abdominal injury, and spinal cord injury.
Prehospital priorities
All patients with signs of life should be transported rapidly to a trauma center. Full spinal immobilization is indicated when spinal injury is suspected. Impaled objects must never be removed in the field because they may be tamponading major bleeding. Suspected tension pneumothorax requires immediate needle decompression. Large open pneumothoraces should be covered with a three-sided occlusive dressing to prevent tension physiology. Transport should not be delayed for intravenous access.
Early resuscitation
Airway, breathing, and circulation management is the priority. Endotracheal intubation is indicated for respiratory distress, hypoxia, or hypotension. Supplemental oxygen should be provided to stable patients. Two large-bore peripheral IV lines should be established, with cautious fluid resuscitation. In penetrating aortic injury, permissive hypotension with a systolic pressure around 90 mm Hg is recommended until surgical control is achieved. Suspected tension pneumothorax requires immediate needle thoracostomy followed by chest tube placement without waiting for imaging. Pericardial tamponade with instability warrants emergency pericardiocentesis followed by rapid operative intervention.
Emergency department management
The trauma surgeon should be notified immediately. Tube thoracostomy is required for pneumothorax or hemothorax, using appropriately sized tubes. Aggressive crystalloid resuscitation should be avoided when pulmonary contusion is present. Wounds below the nipple line or posterior scapular tip raise concern for intra-abdominal injury and require further evaluation with ultrasound, CT, diagnostic peritoneal lavage, or operative exploration. Chest wounds should not be probed, and impaled objects should only be removed in the operating room. All foreign material should be preserved as forensic evidence. Tetanus prophylaxis should be updated as indicated.
Medications and supportive care
Analgesia and sedation should be provided using small, titrated doses of short-acting agents to avoid respiratory compromise. High-dose steroids for spinal cord injury remain controversial and should follow institutional protocols. Broad-spectrum intravenous antibiotics are indicated if wounds are grossly contaminated.
Disposition and outcomes
All patients with penetrating chest trauma require hospital admission. Hemodynamically unstable patients should proceed directly to the operating room. Emergency department thoracotomy may be lifesaving in selected patients with penetrating torso trauma who had signs of life in the field and short prehospital CPR duration. Large initial chest tube output or persistent bleeding mandates surgical intervention. Patients with isolated minor chest wall wounds and normal imaging may be observed briefly and discharged if repeat evaluation excludes intrathoracic injury and the patient remains stable.
- Published on
Emergency and Acute Medicine – Cholelithiasis
Overview and mechanism
Cholelithiasis refers to the presence of gallstones that become symptomatic when they obstruct the cystic duct or common bile duct, disrupting normal bile flow and triggering gallbladder spasm. This produces the characteristic pain of biliary colic. A related functional disorder, biliary dyskinesia, causes identical symptoms despite the absence of stones. When stones migrate into the common bile duct (choledocholithiasis), pain may be more prolonged and is often accompanied by abnormal liver function tests and bilirubin elevation, with risk of complications such as cholangitis or pancreatitis.
Causes and risk factors
Most gallstones are cholesterol stones, which develop when bile becomes supersaturated with cholesterol. Pigment stones account for about one fifth of cases and consist mainly of calcium bilirubinate; they are commonly associated with hemolytic disorders that increase unconjugated bilirubin levels. The incidence of gallstones rises with age and is higher in females, with additional risk factors including obesity, pregnancy, rapid weight loss, Hispanic ethnicity, and medications that promote biliary stasis such as oral contraceptives or ceftriaxone. In children, gallstones are rare and are usually linked to hemolytic anemias such as sickle cell disease or hereditary spherocytosis. Biliary sludge, a nonstone crystalline material, may also cause biliary colic and is associated with pregnancy, rapid weight loss, certain medications, and organ transplantation. Chronic obstruction with calcium deposition can lead to a porcelain gallbladder, a condition associated with an increased risk of gallbladder carcinoma.
Clinical presentation
Patients typically describe dull, aching epigastric or right upper quadrant pain that develops gradually over several minutes, persists for 30 minutes to several hours, and then resolves. The pain often radiates to the right scapula, shoulder, or thoracic spine and is frequently triggered by a large or fatty meal. Associated symptoms include anorexia, nausea, and vomiting. Patients are usually afebrile; the presence of fever or chills suggests a complication such as cholecystitis or cholangitis.
Examination findings
On examination, there is tenderness to deep palpation in the right upper quadrant without rebound or guarding. A Murphy sign may be present during an active episode of biliary colic but should resolve once the pain subsides.
Initial evaluation
Assessment includes exclusion of cardiac causes when appropriate, along with basic laboratory testing such as a complete blood count, liver function tests, pancreatic enzymes, urinalysis, and pregnancy testing when indicated. These tests help distinguish uncomplicated biliary colic from complications involving infection, obstruction, or pancreatitis.
Diagnostic studies
Laboratory studies are often normal in uncomplicated cholelithiasis. Leukocytosis or significant liver enzyme abnormalities suggest cholecystitis, cholangitis, or common bile duct obstruction. Ultrasound is the imaging modality of choice, with high sensitivity and specificity for gallstones and the ability to assess bile duct dilation and gallbladder wall changes. Hepatobiliary scintigraphy is useful when cholecystitis is suspected but ultrasound findings are equivocal, though it does not directly visualize stones. Computed tomography is less sensitive for gallstones but may identify complications or alternative diagnoses.
Differential considerations
Conditions that can mimic biliary colic include myocardial infarction, abdominal aortic aneurysm, acute cholecystitis, cholangitis, pancreatitis, renal colic, peptic ulcer disease, pneumonia involving the right lower lobe, hepatitis, and other intra-abdominal emergencies.
Early management
Initial treatment focuses on supportive care. Intravenous access and fluids are provided for patients with vomiting or dehydration, and oral intake is withheld during acute symptoms. Pain control is essential, often with parenteral nonsteroidal anti-inflammatory drugs or opioids combined with antiemetics once the diagnosis is reasonably secure.
Emergency department care
Hydration, analgesia, and antiemetics form the mainstay of treatment for uncomplicated biliary colic. Anticholinergic agents have not demonstrated benefit. Ongoing reassessment is required to ensure symptoms resolve and that no complications develop.
Disposition and follow-up
Patients should be admitted and receive surgical or gastroenterology consultation if there is evidence of cholecystitis, cholangitis, common bile duct obstruction, or gallstone pancreatitis. Discharge may be considered when pain has fully resolved, laboratory and imaging studies show no complications, and the patient can tolerate oral intake. All patients with symptomatic gallstones require referral for surgical evaluation, and those with choledocholithiasis need gastroenterology follow-up.
Clinical pearls
Gallstones detected incidentally on imaging may not be the cause of abdominal pain, so alternative diagnoses must always be considered. Ultrasound is the most accurate initial test for gallstones, while hepatobiliary scintigraphy is particularly useful for diagnosing cystic duct obstruction and acute cholecystitis. Computed tomography may miss non-radiopaque stones and should not be relied upon alone for diagnosis.
Overview and mechanism
Cholelithiasis refers to the presence of gallstones that become symptomatic when they obstruct the cystic duct or common bile duct, disrupting normal bile flow and triggering gallbladder spasm. This produces the characteristic pain of biliary colic. A related functional disorder, biliary dyskinesia, causes identical symptoms despite the absence of stones. When stones migrate into the common bile duct (choledocholithiasis), pain may be more prolonged and is often accompanied by abnormal liver function tests and bilirubin elevation, with risk of complications such as cholangitis or pancreatitis.
Causes and risk factors
Most gallstones are cholesterol stones, which develop when bile becomes supersaturated with cholesterol. Pigment stones account for about one fifth of cases and consist mainly of calcium bilirubinate; they are commonly associated with hemolytic disorders that increase unconjugated bilirubin levels. The incidence of gallstones rises with age and is higher in females, with additional risk factors including obesity, pregnancy, rapid weight loss, Hispanic ethnicity, and medications that promote biliary stasis such as oral contraceptives or ceftriaxone. In children, gallstones are rare and are usually linked to hemolytic anemias such as sickle cell disease or hereditary spherocytosis. Biliary sludge, a nonstone crystalline material, may also cause biliary colic and is associated with pregnancy, rapid weight loss, certain medications, and organ transplantation. Chronic obstruction with calcium deposition can lead to a porcelain gallbladder, a condition associated with an increased risk of gallbladder carcinoma.
Clinical presentation
Patients typically describe dull, aching epigastric or right upper quadrant pain that develops gradually over several minutes, persists for 30 minutes to several hours, and then resolves. The pain often radiates to the right scapula, shoulder, or thoracic spine and is frequently triggered by a large or fatty meal. Associated symptoms include anorexia, nausea, and vomiting. Patients are usually afebrile; the presence of fever or chills suggests a complication such as cholecystitis or cholangitis.
Examination findings
On examination, there is tenderness to deep palpation in the right upper quadrant without rebound or guarding. A Murphy sign may be present during an active episode of biliary colic but should resolve once the pain subsides.
Initial evaluation
Assessment includes exclusion of cardiac causes when appropriate, along with basic laboratory testing such as a complete blood count, liver function tests, pancreatic enzymes, urinalysis, and pregnancy testing when indicated. These tests help distinguish uncomplicated biliary colic from complications involving infection, obstruction, or pancreatitis.
Diagnostic studies
Laboratory studies are often normal in uncomplicated cholelithiasis. Leukocytosis or significant liver enzyme abnormalities suggest cholecystitis, cholangitis, or common bile duct obstruction. Ultrasound is the imaging modality of choice, with high sensitivity and specificity for gallstones and the ability to assess bile duct dilation and gallbladder wall changes. Hepatobiliary scintigraphy is useful when cholecystitis is suspected but ultrasound findings are equivocal, though it does not directly visualize stones. Computed tomography is less sensitive for gallstones but may identify complications or alternative diagnoses.
Differential considerations
Conditions that can mimic biliary colic include myocardial infarction, abdominal aortic aneurysm, acute cholecystitis, cholangitis, pancreatitis, renal colic, peptic ulcer disease, pneumonia involving the right lower lobe, hepatitis, and other intra-abdominal emergencies.
Early management
Initial treatment focuses on supportive care. Intravenous access and fluids are provided for patients with vomiting or dehydration, and oral intake is withheld during acute symptoms. Pain control is essential, often with parenteral nonsteroidal anti-inflammatory drugs or opioids combined with antiemetics once the diagnosis is reasonably secure.
Emergency department care
Hydration, analgesia, and antiemetics form the mainstay of treatment for uncomplicated biliary colic. Anticholinergic agents have not demonstrated benefit. Ongoing reassessment is required to ensure symptoms resolve and that no complications develop.
Disposition and follow-up
Patients should be admitted and receive surgical or gastroenterology consultation if there is evidence of cholecystitis, cholangitis, common bile duct obstruction, or gallstone pancreatitis. Discharge may be considered when pain has fully resolved, laboratory and imaging studies show no complications, and the patient can tolerate oral intake. All patients with symptomatic gallstones require referral for surgical evaluation, and those with choledocholithiasis need gastroenterology follow-up.
Clinical pearls
Gallstones detected incidentally on imaging may not be the cause of abdominal pain, so alternative diagnoses must always be considered. Ultrasound is the most accurate initial test for gallstones, while hepatobiliary scintigraphy is particularly useful for diagnosing cystic duct obstruction and acute cholecystitis. Computed tomography may miss non-radiopaque stones and should not be relied upon alone for diagnosis.
- Published on
Emergency and acute medicine – Chest Pain
Overview
Chest pain is one of the most common presenting complaints in the emergency department and frequently represents a potentially life-threatening condition such as acute coronary syndrome, pulmonary embolism, or aortic dissection. Until proven otherwise, chest pain should always be considered dangerous. Although categorization can suggest etiology, presentations are often variable, vague, and misleading.
Anatomic patterns of pain
Thoracic pain arises from structures such as the myocardium, pericardium, ascending aorta, pulmonary artery, mediastinum, or esophagus. It is typically deep, visceral, and poorly localized, ranging from crushing pressure to burning or indigestion-like discomfort.
Epigastric pain may originate from the descending aorta, diaphragm, gallbladder, pancreas, duodenum, or stomach and is often referred to the xiphoid area or back.
Pleuritic pain results from inflammation or trauma of ribs, muscles, pleura, or pericardium and worsens with breathing, coughing, laughing, or sneezing; tenderness to palpation may be present.
Diaphragmatic pleurisy causes sharp epigastric, lower retrosternal, or shoulder pain that intensifies with thoracic movement.
Chest wall pain involves skin and subcutaneous structures and is reproducible with palpation, arm movement, neck extension, or vertical pressure on the head.
Causes
Thoracic causes include acute coronary syndrome, myocarditis, pericarditis, stress-induced cardiomyopathy, stimulant use, thoracic aortic dissection, and esophageal disorders such as reflux, spasm, rupture, or mediastinitis.
Epigastric causes include descending aortic dissection, peptic ulcer disease, pancreatitis, cholecystitis, splenic or hepatic injury, and subdiaphragmatic abscess.
Pleuritic pain may result from pulmonary embolism, pneumothorax, pneumonia, costochondritis, or sickle cell acute chest syndrome.
Chest wall causes include musculoskeletal strain, rib fractures, herpes zoster, thrombophlebitis, xiphisternal arthritis, and breast pathology.
Clinical features
Coronary ischemia commonly presents with pressure-like or squeezing pain radiating to the arm or jaw, associated with dyspnea, diaphoresis, nausea, vomiting, weakness, or fatigue, especially in women and older adults.
Aortic dissection typically causes sudden, severe pain with maximal intensity at onset, often tearing and radiating to the back or flank, accompanied by hypertension, pulse deficits, murmurs, syncope, or neurologic symptoms.
Pulmonary embolism presents with pleuritic pain, dyspnea, anxiety, tachycardia, tachypnea, syncope, or low-grade fever.
Acute pericarditis causes substernal pain worsened by lying flat and relieved by leaning forward, often with fever and a friction rub.
Pneumothorax produces sudden pleuritic pain with dyspnea and unilateral decreased breath sounds.
History and examination
History is the most critical diagnostic tool and should focus on onset, duration, location, quality, radiation, provoking and relieving factors, associated symptoms, and prior cardiac risk factors. Physical examination should include careful cardiac, pulmonary, vascular, abdominal, and skin assessments, looking for murmurs, rubs, breath sound asymmetry, pulse deficits, abdominal tenderness, or zoster lesions.
Investigations
An electrocardiogram should be obtained and interpreted within 10 minutes of arrival, with serial tracings when suspicion for acute coronary syndrome persists. Laboratory testing is individualized based on risk and presentation and may include cardiac biomarkers and D-dimer in selected low-risk patients.
Chest radiography evaluates for pneumothorax, pneumonia, heart failure, mediastinal widening, or esophageal rupture. Computed tomography is useful for pulmonary embolism and aortic dissection. Ultrasound and echocardiography rapidly assess pericardial effusion, valvular disease, right ventricular strain, pneumothorax, and pleural effusion.
Management principles
Prehospital and early emergency care should be guided by risk assessment and may include intravenous access, cardiac monitoring, oxygen, aspirin, nitrates, and analgesia when a cardiac cause is suspected.
Initial stabilization focuses on airway, breathing, circulation, oxygenation, intravenous access, and continuous monitoring. Definitive treatment depends on the suspected underlying cause and should not be delayed in high-risk presentations.
Disposition and follow-up
Admission decisions depend on the likelihood of life-threatening cardiopulmonary disease. Patients deemed low risk after thorough evaluation may be discharged with close outpatient follow-up. Patients should receive clear return precautions for persistent, worsening, or recurrent chest pain, associated dyspnea, diaphoresis, syncope, or radiation of pain.
Clinical cautions
Avoid reliance on a single cardiac biomarker, response to medications, or a single electrocardiogram. Serial ECGs and reassessment are essential in patients with suspected acute coronary syndrome or recurrent symptoms.
Overview
Chest pain is one of the most common presenting complaints in the emergency department and frequently represents a potentially life-threatening condition such as acute coronary syndrome, pulmonary embolism, or aortic dissection. Until proven otherwise, chest pain should always be considered dangerous. Although categorization can suggest etiology, presentations are often variable, vague, and misleading.
Anatomic patterns of pain
Thoracic pain arises from structures such as the myocardium, pericardium, ascending aorta, pulmonary artery, mediastinum, or esophagus. It is typically deep, visceral, and poorly localized, ranging from crushing pressure to burning or indigestion-like discomfort.
Epigastric pain may originate from the descending aorta, diaphragm, gallbladder, pancreas, duodenum, or stomach and is often referred to the xiphoid area or back.
Pleuritic pain results from inflammation or trauma of ribs, muscles, pleura, or pericardium and worsens with breathing, coughing, laughing, or sneezing; tenderness to palpation may be present.
Diaphragmatic pleurisy causes sharp epigastric, lower retrosternal, or shoulder pain that intensifies with thoracic movement.
Chest wall pain involves skin and subcutaneous structures and is reproducible with palpation, arm movement, neck extension, or vertical pressure on the head.
Causes
Thoracic causes include acute coronary syndrome, myocarditis, pericarditis, stress-induced cardiomyopathy, stimulant use, thoracic aortic dissection, and esophageal disorders such as reflux, spasm, rupture, or mediastinitis.
Epigastric causes include descending aortic dissection, peptic ulcer disease, pancreatitis, cholecystitis, splenic or hepatic injury, and subdiaphragmatic abscess.
Pleuritic pain may result from pulmonary embolism, pneumothorax, pneumonia, costochondritis, or sickle cell acute chest syndrome.
Chest wall causes include musculoskeletal strain, rib fractures, herpes zoster, thrombophlebitis, xiphisternal arthritis, and breast pathology.
Clinical features
Coronary ischemia commonly presents with pressure-like or squeezing pain radiating to the arm or jaw, associated with dyspnea, diaphoresis, nausea, vomiting, weakness, or fatigue, especially in women and older adults.
Aortic dissection typically causes sudden, severe pain with maximal intensity at onset, often tearing and radiating to the back or flank, accompanied by hypertension, pulse deficits, murmurs, syncope, or neurologic symptoms.
Pulmonary embolism presents with pleuritic pain, dyspnea, anxiety, tachycardia, tachypnea, syncope, or low-grade fever.
Acute pericarditis causes substernal pain worsened by lying flat and relieved by leaning forward, often with fever and a friction rub.
Pneumothorax produces sudden pleuritic pain with dyspnea and unilateral decreased breath sounds.
History and examination
History is the most critical diagnostic tool and should focus on onset, duration, location, quality, radiation, provoking and relieving factors, associated symptoms, and prior cardiac risk factors. Physical examination should include careful cardiac, pulmonary, vascular, abdominal, and skin assessments, looking for murmurs, rubs, breath sound asymmetry, pulse deficits, abdominal tenderness, or zoster lesions.
Investigations
An electrocardiogram should be obtained and interpreted within 10 minutes of arrival, with serial tracings when suspicion for acute coronary syndrome persists. Laboratory testing is individualized based on risk and presentation and may include cardiac biomarkers and D-dimer in selected low-risk patients.
Chest radiography evaluates for pneumothorax, pneumonia, heart failure, mediastinal widening, or esophageal rupture. Computed tomography is useful for pulmonary embolism and aortic dissection. Ultrasound and echocardiography rapidly assess pericardial effusion, valvular disease, right ventricular strain, pneumothorax, and pleural effusion.
Management principles
Prehospital and early emergency care should be guided by risk assessment and may include intravenous access, cardiac monitoring, oxygen, aspirin, nitrates, and analgesia when a cardiac cause is suspected.
Initial stabilization focuses on airway, breathing, circulation, oxygenation, intravenous access, and continuous monitoring. Definitive treatment depends on the suspected underlying cause and should not be delayed in high-risk presentations.
Disposition and follow-up
Admission decisions depend on the likelihood of life-threatening cardiopulmonary disease. Patients deemed low risk after thorough evaluation may be discharged with close outpatient follow-up. Patients should receive clear return precautions for persistent, worsening, or recurrent chest pain, associated dyspnea, diaphoresis, syncope, or radiation of pain.
Clinical cautions
Avoid reliance on a single cardiac biomarker, response to medications, or a single electrocardiogram. Serial ECGs and reassessment are essential in patients with suspected acute coronary syndrome or recurrent symptoms.