- Published on
Emergency and Acute Medicine – Elder Abuse
Overview and Definition
Elder abuse encompasses a spectrum of harmful behaviors directed toward older adults, typically by individuals on whom they depend for care or support. Abuse may be emotional, including insults, humiliation, threats of abandonment, or institutionalization. Physical and sexual abuse involves acts such as hitting, slapping, pushing, burning, inappropriate restraint, or forced sexual activity. Material or financial exploitation includes theft, coercion, or misuse of an elder’s money or property. Neglect refers to acts or omissions by a caregiver or the patient that compromise health or safety, including failure to provide adequate nutrition, shelter, hygiene, or medical care.
Epidemiology and Impact
In the United States, an estimated 1–2 million adults aged 65 years or older are mistreated annually, a figure expected to rise as the population ages. Neglect accounts for the majority of cases, followed by physical mistreatment, financial exploitation, and emotional abuse; sexual abuse is reported less frequently. Family members—most often spouses or adult children—are responsible in approximately 90% of cases. Financial exploitation is particularly underreported, with many cases never reaching authorities. Even mild forms of abuse are associated with a markedly increased risk of mortality and higher rates of chronic pain, musculoskeletal, gastrointestinal, and psychological disorders.
Etiology and Risk Factors
Abuse often arises from caregiver stress, dependency, mental illness, substance use, or financial reliance on the elder. Victim-related factors include physical or cognitive impairment, dependence for activities of daily living, and social isolation, all of which increase vulnerability.
Clinical Presentation
Presentations are highly variable and may be subtle. Histories may be inconsistent, vague, or implausible, and discrepancies may exist between accounts provided by the patient and caregiver. Red flags include delays in seeking medical care, previously untreated conditions, inability or unwillingness to meet basic needs, and medication mismanagement such as incorrect dosing, missing prescriptions, or unfilled medications. Behavioral changes in the elder—withdrawal, fearfulness, demoralization, or substance use—may be evident. Concerning caregiver behaviors include controlling interactions, refusal to leave the patient alone with clinicians, poor knowledge of the patient’s condition, or evidence of significant psychosocial stressors.
Physical Examination Findings
Examination may reveal injuries inconsistent with the reported mechanism or injuries at different stages of healing. Suspicious findings include bruises, burns, lacerations, or abrasions in unusual locations such as the inner arms, torso, buttocks, scalp, or genital and rectal areas. Lesions on wrists or ankles may suggest restraint use. Signs of neglect include poor hygiene, dehydration, weight loss, malnutrition, and pressure ulcers.
Essential Evaluation
Assessment should prioritize patient safety and confidentiality. History should be obtained without caregivers present, as many abused elders fear retaliation, institutionalization, or feel shame or responsibility for the abuse. Clinicians should ask directly but sensitively about mistreatment or neglect. Information from caregivers, relatives, friends, or neighbors may provide important context.
Detailed documentation is critical and should include verbatim patient statements, psychosocial history, caregiver dynamics, substance use, prior involvement of adult protective services, and thorough descriptions of physical findings. Photographic documentation of injuries, when appropriate, can be invaluable. A structured safety assessment is essential.
Diagnostic Testing
Laboratory studies, imaging, and procedures should be guided by the patient’s medical condition and suspected injuries. There are no specific tests that diagnose abuse; rather, diagnosis relies on correlation of clinical findings, risk factors, and patient disclosure.
Differential Diagnosis
Elder abuse can present with any chief complaint. Clinicians must distinguish abuse or neglect from medical conditions that may mimic it, such as dehydration, poorly fitting dentures, burns from accidents, ecchymoses related to anticoagulation, insomnia, medication nonadherence, dementia, or depression.
Prehospital Considerations
Emergency medical personnel may observe critical environmental and interpersonal details, including unsafe living conditions, evidence of neglect, or fearful interactions between the elder and caregiver, which should be communicated to the receiving team.
Emergency Department Management
Initial care follows standard priorities, addressing airway, breathing, circulation, and any life-threatening medical or traumatic conditions. Separation of the patient from caregivers may be necessary to allow safe evaluation. Early involvement of social work is essential for safety planning, caregiver respite, and coordination with community resources. Adult protective services should be notified when abuse or neglect is suspected, in accordance with local laws.
Competent elders retain the right to accept or decline treatment or disposition, even when risks remain, underscoring the importance of clear communication and documentation.
Disposition and Follow-Up
Admission is indicated when medical conditions require inpatient care, when the home environment is unsafe, or when additional time is needed to clarify concerns and coordinate protection. Discharge may be considered only after medical issues are addressed and a safe environment is assured through social services or legal intervention.
Many jurisdictions mandate reporting of suspected elder abuse; clinicians must comply with local regulations. Referral for substance use treatment, mental health services, or caregiver support may be appropriate.
Clinical Pearls and Pitfalls
Elder abuse is common, underrecognized, and associated with high morbidity and mortality. Diagnosis often depends on asking directly in a private setting and recognizing subtle patterns rather than relying on a single finding. Failure to separate the patient from caregivers or to document thoroughly can result in missed opportunities for protection and intervention.
Overview and Definition
Elder abuse encompasses a spectrum of harmful behaviors directed toward older adults, typically by individuals on whom they depend for care or support. Abuse may be emotional, including insults, humiliation, threats of abandonment, or institutionalization. Physical and sexual abuse involves acts such as hitting, slapping, pushing, burning, inappropriate restraint, or forced sexual activity. Material or financial exploitation includes theft, coercion, or misuse of an elder’s money or property. Neglect refers to acts or omissions by a caregiver or the patient that compromise health or safety, including failure to provide adequate nutrition, shelter, hygiene, or medical care.
Epidemiology and Impact
In the United States, an estimated 1–2 million adults aged 65 years or older are mistreated annually, a figure expected to rise as the population ages. Neglect accounts for the majority of cases, followed by physical mistreatment, financial exploitation, and emotional abuse; sexual abuse is reported less frequently. Family members—most often spouses or adult children—are responsible in approximately 90% of cases. Financial exploitation is particularly underreported, with many cases never reaching authorities. Even mild forms of abuse are associated with a markedly increased risk of mortality and higher rates of chronic pain, musculoskeletal, gastrointestinal, and psychological disorders.
Etiology and Risk Factors
Abuse often arises from caregiver stress, dependency, mental illness, substance use, or financial reliance on the elder. Victim-related factors include physical or cognitive impairment, dependence for activities of daily living, and social isolation, all of which increase vulnerability.
Clinical Presentation
Presentations are highly variable and may be subtle. Histories may be inconsistent, vague, or implausible, and discrepancies may exist between accounts provided by the patient and caregiver. Red flags include delays in seeking medical care, previously untreated conditions, inability or unwillingness to meet basic needs, and medication mismanagement such as incorrect dosing, missing prescriptions, or unfilled medications. Behavioral changes in the elder—withdrawal, fearfulness, demoralization, or substance use—may be evident. Concerning caregiver behaviors include controlling interactions, refusal to leave the patient alone with clinicians, poor knowledge of the patient’s condition, or evidence of significant psychosocial stressors.
Physical Examination Findings
Examination may reveal injuries inconsistent with the reported mechanism or injuries at different stages of healing. Suspicious findings include bruises, burns, lacerations, or abrasions in unusual locations such as the inner arms, torso, buttocks, scalp, or genital and rectal areas. Lesions on wrists or ankles may suggest restraint use. Signs of neglect include poor hygiene, dehydration, weight loss, malnutrition, and pressure ulcers.
Essential Evaluation
Assessment should prioritize patient safety and confidentiality. History should be obtained without caregivers present, as many abused elders fear retaliation, institutionalization, or feel shame or responsibility for the abuse. Clinicians should ask directly but sensitively about mistreatment or neglect. Information from caregivers, relatives, friends, or neighbors may provide important context.
Detailed documentation is critical and should include verbatim patient statements, psychosocial history, caregiver dynamics, substance use, prior involvement of adult protective services, and thorough descriptions of physical findings. Photographic documentation of injuries, when appropriate, can be invaluable. A structured safety assessment is essential.
Diagnostic Testing
Laboratory studies, imaging, and procedures should be guided by the patient’s medical condition and suspected injuries. There are no specific tests that diagnose abuse; rather, diagnosis relies on correlation of clinical findings, risk factors, and patient disclosure.
Differential Diagnosis
Elder abuse can present with any chief complaint. Clinicians must distinguish abuse or neglect from medical conditions that may mimic it, such as dehydration, poorly fitting dentures, burns from accidents, ecchymoses related to anticoagulation, insomnia, medication nonadherence, dementia, or depression.
Prehospital Considerations
Emergency medical personnel may observe critical environmental and interpersonal details, including unsafe living conditions, evidence of neglect, or fearful interactions between the elder and caregiver, which should be communicated to the receiving team.
Emergency Department Management
Initial care follows standard priorities, addressing airway, breathing, circulation, and any life-threatening medical or traumatic conditions. Separation of the patient from caregivers may be necessary to allow safe evaluation. Early involvement of social work is essential for safety planning, caregiver respite, and coordination with community resources. Adult protective services should be notified when abuse or neglect is suspected, in accordance with local laws.
Competent elders retain the right to accept or decline treatment or disposition, even when risks remain, underscoring the importance of clear communication and documentation.
Disposition and Follow-Up
Admission is indicated when medical conditions require inpatient care, when the home environment is unsafe, or when additional time is needed to clarify concerns and coordinate protection. Discharge may be considered only after medical issues are addressed and a safe environment is assured through social services or legal intervention.
Many jurisdictions mandate reporting of suspected elder abuse; clinicians must comply with local regulations. Referral for substance use treatment, mental health services, or caregiver support may be appropriate.
Clinical Pearls and Pitfalls
Elder abuse is common, underrecognized, and associated with high morbidity and mortality. Diagnosis often depends on asking directly in a private setting and recognizing subtle patterns rather than relying on a single finding. Failure to separate the patient from caregivers or to document thoroughly can result in missed opportunities for protection and intervention.

- Published on
Emergency and Acute Medicine – Pediatric Abuse (Nonaccidental Trauma, NAT)
Overview and Scope
Pediatric abuse, also referred to as nonaccidental trauma (NAT), represents a major public health concern in the United States. It affects an estimated 2–3% of children annually, with millions impacted each year. Mortality from child maltreatment remains significant, with the majority of deaths occurring in children younger than five years, and infants accounting for a large proportion. All health care professionals are legally mandated reporters of suspected child abuse or neglect. Importantly, abuse occurs across all socioeconomic, cultural, and religious groups.
Risk Factors
Risk factors span the child, caregiver, and family environment. Children at highest risk are typically younger than four years, particularly infants, premature babies, multiples, and those with physical, developmental, or special health care needs.
Caregiver-related risk factors include a history of being abused, poor impulse control, violent behavior, mental illness, substance use, rigid or unrealistic expectations of the child, low self-esteem, and young parental age.
Family-level risk factors include financial stress, social isolation, frequent relocation, marital instability, unwanted pregnancy, and poor parent–child bonding.
Clinical Presentation and History
A hallmark of NAT is a history that is inconsistent with the reported injury or illness. Red flags include unexplained injury, apnea, ingestion, recurrent trauma, or death. Caregivers may be reluctant to provide information, deny knowledge of the injury, or offer changing or implausible explanations. Discrepancies between different caregivers are common.
In some cases, the described mechanism is developmentally impossible for the child. Delays in seeking medical care and inappropriate caregiver responses to the child’s condition are particularly concerning.
Failure to thrive may signal neglect, often related to inadequate caloric intake or impaired caregiver bonding. Munchausen syndrome by proxy should be considered in children with recurrent unexplained illness or suspicious metabolic abnormalities. Reviewing prior emergency department visits and communication with the primary care provider can reveal concerning patterns.
Physical Examination Findings
Physical findings often do not match the provided history. Cutaneous injuries are common and may include bruises with regular patterns, sharp demarcations, finger marks, slap marks, bite marks, burns from cigarettes or immersion (“stocking,” “glove,” or doughnut-shaped buttock burns), and injuries in unusual locations such as the buttocks, hips, face (excluding the forehead), back, thighs, genitalia, or pinna.
Bruises may be present at different stages of healing. While color alone is unreliable for precise dating, the presence of multiple injuries of varying age is suspicious.
Skeletal injuries are frequently multiple and unexplained, often in different stages of healing. Highly concerning findings include classic metaphyseal lesions, posterior rib fractures, fractures crossing suture lines, spiral fractures of long bones, subperiosteal new bone formation, and fractures of uncommon sites such as the scapula, sternum, vertebrae, or spinous processes without adequate mechanism.
Central Nervous System and Ocular Findings
Head injury is the leading cause of death in abused children. Findings may include altered mental status, seizures, skull fractures (particularly in children younger than one year), subdural or subarachnoid hemorrhage, and features consistent with shaken infant injury involving rotational and shearing forces.
Ocular findings are critical clues. Retinal hemorrhages—often bilateral—are present in the majority of abusive head injuries and are rare in accidental trauma without significant head injury. Additional findings may include hyphema, corneal abrasions, or conjunctival hemorrhage.
Abdominal, Genitourinary, and Sexual Abuse Findings
Abusive abdominal trauma may involve lacerations of solid organs, intramural bowel hematomas (especially duodenal), or retroperitoneal hemorrhage.
Anogenital findings such as contusions, erythema, lacerations, scarring, foreign material, sexually transmitted infections, or pregnancy in a child younger than twelve years strongly suggest sexual abuse. Unexplained death must always raise concern for NAT.
Essential Evaluation and Legal Responsibilities
When abuse is suspected, clinicians are legally required to make a formal oral and written report to the appropriate child protection agency. Certainty is not required—reasonable suspicion is sufficient.
Evaluation should include a thorough medical assessment, detailed documentation of findings, and photographic or diagrammatic recording of injuries when appropriate. Family, social, and environmental assessments are typically conducted in coordination with child welfare services.
Diagnostic Testing and Imaging
Laboratory studies are guided by presentation. A bleeding disorder screen is appropriate when bruising is prominent or recurrent. In cases of significant trauma, laboratory evaluation may include complete blood count, liver enzymes, pancreatic enzymes, and urinalysis. Toxicology and metabolic testing are indicated in children with altered mental status.
Imaging plays a central role. A full skeletal survey is recommended for children younger than two years and selectively for older children when abuse is strongly suspected. Additional imaging is obtained based on clinical findings, including abdominal CT for suspected visceral injury and neuroimaging for suspected head trauma. MRI serves as a valuable adjunct for detecting shear injury, evolving hemorrhage, and hypoxic-ischemic changes.
Differential Diagnosis
Conditions that may mimic abuse must be carefully considered, including accidental trauma, birth-related injuries, infections, dermatologic conditions, hematologic or oncologic disorders, bleeding diatheses, nutritional deficiencies, metabolic or genetic bone disease, cultural healing practices, intoxications, metabolic derangements, epilepsy, and sudden infant death syndromes. Differentiation relies on correlation of clinical findings with history, development, and investigative results.
Emergency Department Management
Medical stabilization and trauma care take priority. Clinicians must maintain a nonjudgmental approach while ensuring mandatory reporting and rapid involvement of child protection services. Communication with caregivers should emphasize concern for the child’s safety and well-being. Security may be required in some situations. All siblings and other children in the household must also be evaluated within an appropriate timeframe.
Disposition and Follow-Up
Admission is indicated for traumatic injuries requiring observation or intervention, or when safe disposition cannot be assured. Discharge is considered only after a complete evaluation, confirmation of a safe environment, and coordination with child welfare authorities. Many children require protective placement, including foster care, to prevent further harm.
Clinical Pearls and Pitfalls
A history that does not align with physical findings should immediately raise concern for nonaccidental trauma. When child abuse is suspected, reporting is mandatory and time-sensitive. The primary goal in all cases is ensuring the safety of the child and any siblings.
Overview and Scope
Pediatric abuse, also referred to as nonaccidental trauma (NAT), represents a major public health concern in the United States. It affects an estimated 2–3% of children annually, with millions impacted each year. Mortality from child maltreatment remains significant, with the majority of deaths occurring in children younger than five years, and infants accounting for a large proportion. All health care professionals are legally mandated reporters of suspected child abuse or neglect. Importantly, abuse occurs across all socioeconomic, cultural, and religious groups.
Risk Factors
Risk factors span the child, caregiver, and family environment. Children at highest risk are typically younger than four years, particularly infants, premature babies, multiples, and those with physical, developmental, or special health care needs.
Caregiver-related risk factors include a history of being abused, poor impulse control, violent behavior, mental illness, substance use, rigid or unrealistic expectations of the child, low self-esteem, and young parental age.
Family-level risk factors include financial stress, social isolation, frequent relocation, marital instability, unwanted pregnancy, and poor parent–child bonding.
Clinical Presentation and History
A hallmark of NAT is a history that is inconsistent with the reported injury or illness. Red flags include unexplained injury, apnea, ingestion, recurrent trauma, or death. Caregivers may be reluctant to provide information, deny knowledge of the injury, or offer changing or implausible explanations. Discrepancies between different caregivers are common.
In some cases, the described mechanism is developmentally impossible for the child. Delays in seeking medical care and inappropriate caregiver responses to the child’s condition are particularly concerning.
Failure to thrive may signal neglect, often related to inadequate caloric intake or impaired caregiver bonding. Munchausen syndrome by proxy should be considered in children with recurrent unexplained illness or suspicious metabolic abnormalities. Reviewing prior emergency department visits and communication with the primary care provider can reveal concerning patterns.
Physical Examination Findings
Physical findings often do not match the provided history. Cutaneous injuries are common and may include bruises with regular patterns, sharp demarcations, finger marks, slap marks, bite marks, burns from cigarettes or immersion (“stocking,” “glove,” or doughnut-shaped buttock burns), and injuries in unusual locations such as the buttocks, hips, face (excluding the forehead), back, thighs, genitalia, or pinna.
Bruises may be present at different stages of healing. While color alone is unreliable for precise dating, the presence of multiple injuries of varying age is suspicious.
Skeletal injuries are frequently multiple and unexplained, often in different stages of healing. Highly concerning findings include classic metaphyseal lesions, posterior rib fractures, fractures crossing suture lines, spiral fractures of long bones, subperiosteal new bone formation, and fractures of uncommon sites such as the scapula, sternum, vertebrae, or spinous processes without adequate mechanism.
Central Nervous System and Ocular Findings
Head injury is the leading cause of death in abused children. Findings may include altered mental status, seizures, skull fractures (particularly in children younger than one year), subdural or subarachnoid hemorrhage, and features consistent with shaken infant injury involving rotational and shearing forces.
Ocular findings are critical clues. Retinal hemorrhages—often bilateral—are present in the majority of abusive head injuries and are rare in accidental trauma without significant head injury. Additional findings may include hyphema, corneal abrasions, or conjunctival hemorrhage.
Abdominal, Genitourinary, and Sexual Abuse Findings
Abusive abdominal trauma may involve lacerations of solid organs, intramural bowel hematomas (especially duodenal), or retroperitoneal hemorrhage.
Anogenital findings such as contusions, erythema, lacerations, scarring, foreign material, sexually transmitted infections, or pregnancy in a child younger than twelve years strongly suggest sexual abuse. Unexplained death must always raise concern for NAT.
Essential Evaluation and Legal Responsibilities
When abuse is suspected, clinicians are legally required to make a formal oral and written report to the appropriate child protection agency. Certainty is not required—reasonable suspicion is sufficient.
Evaluation should include a thorough medical assessment, detailed documentation of findings, and photographic or diagrammatic recording of injuries when appropriate. Family, social, and environmental assessments are typically conducted in coordination with child welfare services.
Diagnostic Testing and Imaging
Laboratory studies are guided by presentation. A bleeding disorder screen is appropriate when bruising is prominent or recurrent. In cases of significant trauma, laboratory evaluation may include complete blood count, liver enzymes, pancreatic enzymes, and urinalysis. Toxicology and metabolic testing are indicated in children with altered mental status.
Imaging plays a central role. A full skeletal survey is recommended for children younger than two years and selectively for older children when abuse is strongly suspected. Additional imaging is obtained based on clinical findings, including abdominal CT for suspected visceral injury and neuroimaging for suspected head trauma. MRI serves as a valuable adjunct for detecting shear injury, evolving hemorrhage, and hypoxic-ischemic changes.
Differential Diagnosis
Conditions that may mimic abuse must be carefully considered, including accidental trauma, birth-related injuries, infections, dermatologic conditions, hematologic or oncologic disorders, bleeding diatheses, nutritional deficiencies, metabolic or genetic bone disease, cultural healing practices, intoxications, metabolic derangements, epilepsy, and sudden infant death syndromes. Differentiation relies on correlation of clinical findings with history, development, and investigative results.
Emergency Department Management
Medical stabilization and trauma care take priority. Clinicians must maintain a nonjudgmental approach while ensuring mandatory reporting and rapid involvement of child protection services. Communication with caregivers should emphasize concern for the child’s safety and well-being. Security may be required in some situations. All siblings and other children in the household must also be evaluated within an appropriate timeframe.
Disposition and Follow-Up
Admission is indicated for traumatic injuries requiring observation or intervention, or when safe disposition cannot be assured. Discharge is considered only after a complete evaluation, confirmation of a safe environment, and coordination with child welfare authorities. Many children require protective placement, including foster care, to prevent further harm.
Clinical Pearls and Pitfalls
A history that does not align with physical findings should immediately raise concern for nonaccidental trauma. When child abuse is suspected, reporting is mandatory and time-sensitive. The primary goal in all cases is ensuring the safety of the child and any siblings.
- Published on
Emergency and Acute Medicine – Acidosis
Overview and Definitions
Acidosis refers to physiologic processes that reduce blood pH and is broadly classified into respiratory acidosis and metabolic acidosis. Respiratory acidosis results from alveolar hypoventilation with retention of carbon dioxide, defined by a PaCO₂ greater than 45 mm Hg or higher than expected for appropriate respiratory compensation. Metabolic acidosis occurs when serum pH decreases due to a reduction in plasma bicarbonate, either from accumulation of acids or loss of bicarbonate from the body. Correct identification of the primary disorder and any mixed acid–base disturbances is essential in emergency care.
Respiratory Acidosis: Pathophysiology and Causes
Respiratory acidosis develops when ventilation is inadequate to eliminate carbon dioxide. Causes fall into three broad categories. The first is central nervous system depression, including sleep apnea, anesthesia, sedative or opioid overdose, CNS infections, or structural brain lesions. The second category involves impaired gas exchange at the alveolar level, such as in COPD, asthma, pneumonia, pulmonary edema, interstitial lung disease, obesity hypoventilation, or pulmonary contusion. The third category reflects failure of carbon dioxide transport from tissues to alveoli, as seen in severe heart failure or pulmonary edema. Neuromuscular disorders—including Guillain–Barré syndrome, myasthenia gravis, muscular dystrophy, spinal cord injury, or electrolyte abnormalities—may also impair ventilation. Upper airway obstruction, whether congenital, infectious, or foreign body–related, must also be considered.
Metabolic Acidosis: Classification and Mechanisms
Metabolic acidosis is classified based on the anion gap. In elevated anion gap metabolic acidosis, bicarbonate is consumed buffering excess strong acids, leaving unmeasured anions in circulation. Common causes are recalled with the mnemonic A CATPILES MUD, including lactic acidosis, ketoacidosis, renal failure (uremia), and toxic ingestions. Some causes are associated with an elevated osmolar gap, remembered by ME DIE, which suggests toxic alcohol exposure.
In normal anion gap (hyperchloremic) metabolic acidosis, bicarbonate is lost or not regenerated, without accumulation of unmeasured anions. This occurs with gastrointestinal bicarbonate losses (such as diarrhea or fistulas), renal tubular acidosis, or ingestion of substances that generate hydrochloric acid. Renal tubular acidosis is subdivided into distal (type I), proximal (type II), and type IV forms, each with characteristic bicarbonate and potassium abnormalities.
Clinical Presentation
Symptoms of acidosis are often nonspecific. Patients may present with tachypnea or deep, labored (Kussmaul) respirations in metabolic acidosis, or hypoventilation in respiratory acidosis. Additional findings include tachycardia, somnolence, confusion, altered mental status from hypercapnia, and cardiac conduction abnormalities or dysrhythmias, particularly with severe electrolyte derangements.
Essential Evaluation
Initial evaluation includes serum electrolytes, renal function, glucose, and arterial blood gases. Metabolic acidosis is suggested by a low bicarbonate level, while respiratory acidosis is characterized by carbon dioxide retention. Hyperkalemia and hypercalcemia may accompany severe metabolic acidosis. Carbon monoxide levels should be measured when exposure is suspected.
Calculation of the anion gap (Na⁺ − [Cl⁻ + HCO₃⁻]) is critical, with correction for hypoalbuminemia. The degree of compensation must be assessed by comparing expected versus observed PaCO₂ or bicarbonate levels. Failure of appropriate compensation suggests a mixed acid–base disorder.
Advanced Acid–Base Interpretation
In metabolic acidosis, expected PaCO₂ can be estimated using standard formulas. If measured PaCO₂ is higher than expected, concomitant respiratory acidosis or inadequate compensation is present. The delta gap helps identify mixed metabolic disorders by comparing changes in the anion gap with changes in bicarbonate concentration. Disproportionate changes indicate additional metabolic alkalosis or non–anion gap acidosis.
Diagnostic Testing
Arterial blood gas analysis remains the reference standard, though venous blood gas sampling may be useful in stable patients for screening. Urinalysis for glucose and ketones, serum lactate, ketone levels, and toxicology screening are obtained as indicated. Measurement of serum osmolality and calculation of the osmolar gap can suggest toxic alcohol ingestion, though a normal gap does not exclude this diagnosis. Imaging and ECG may help identify underlying cardiopulmonary or ischemic causes.
Management and Stabilization
Initial management focuses on airway, breathing, and circulation. Early intubation should be considered in severe metabolic acidosis when respiratory compensation is failing. Empiric administration of naloxone, dextrose, and thiamine is appropriate in patients with altered mental status.
Respiratory acidosis is managed by treating the underlying cause and providing ventilatory support when hypercapnia worsens. Metabolic acidosis requires identification and correction of the underlying etiology, such as diabetic ketoacidosis, lactic acidosis, or toxic ingestion, along with correction of electrolyte abnormalities and volume resuscitation. Hemodialysis may be necessary in select cases.
Disposition and Follow-Up
Patients with severe acidosis, altered mental status, respiratory failure, hemodynamic instability, significant electrolyte disturbances, or dysrhythmias generally require hospital admission, often to an intensive care setting. Discharge may be considered only when acidosis is resolving, the underlying cause is addressed, and close follow-up is ensured.
Clinical Pearls and Pitfalls
Mixed acid–base disorders are common and frequently missed. Normal pH does not exclude significant pathology if PaCO₂ and bicarbonate are both abnormal. Failure to recognize inadequate respiratory compensation in metabolic acidosis can delay lifesaving ventilatory support. Careful, systematic acid–base analysis is essential in emergency and acute care settings.
Overview and Definitions
Acidosis refers to physiologic processes that reduce blood pH and is broadly classified into respiratory acidosis and metabolic acidosis. Respiratory acidosis results from alveolar hypoventilation with retention of carbon dioxide, defined by a PaCO₂ greater than 45 mm Hg or higher than expected for appropriate respiratory compensation. Metabolic acidosis occurs when serum pH decreases due to a reduction in plasma bicarbonate, either from accumulation of acids or loss of bicarbonate from the body. Correct identification of the primary disorder and any mixed acid–base disturbances is essential in emergency care.
Respiratory Acidosis: Pathophysiology and Causes
Respiratory acidosis develops when ventilation is inadequate to eliminate carbon dioxide. Causes fall into three broad categories. The first is central nervous system depression, including sleep apnea, anesthesia, sedative or opioid overdose, CNS infections, or structural brain lesions. The second category involves impaired gas exchange at the alveolar level, such as in COPD, asthma, pneumonia, pulmonary edema, interstitial lung disease, obesity hypoventilation, or pulmonary contusion. The third category reflects failure of carbon dioxide transport from tissues to alveoli, as seen in severe heart failure or pulmonary edema. Neuromuscular disorders—including Guillain–Barré syndrome, myasthenia gravis, muscular dystrophy, spinal cord injury, or electrolyte abnormalities—may also impair ventilation. Upper airway obstruction, whether congenital, infectious, or foreign body–related, must also be considered.
Metabolic Acidosis: Classification and Mechanisms
Metabolic acidosis is classified based on the anion gap. In elevated anion gap metabolic acidosis, bicarbonate is consumed buffering excess strong acids, leaving unmeasured anions in circulation. Common causes are recalled with the mnemonic A CATPILES MUD, including lactic acidosis, ketoacidosis, renal failure (uremia), and toxic ingestions. Some causes are associated with an elevated osmolar gap, remembered by ME DIE, which suggests toxic alcohol exposure.
In normal anion gap (hyperchloremic) metabolic acidosis, bicarbonate is lost or not regenerated, without accumulation of unmeasured anions. This occurs with gastrointestinal bicarbonate losses (such as diarrhea or fistulas), renal tubular acidosis, or ingestion of substances that generate hydrochloric acid. Renal tubular acidosis is subdivided into distal (type I), proximal (type II), and type IV forms, each with characteristic bicarbonate and potassium abnormalities.
Clinical Presentation
Symptoms of acidosis are often nonspecific. Patients may present with tachypnea or deep, labored (Kussmaul) respirations in metabolic acidosis, or hypoventilation in respiratory acidosis. Additional findings include tachycardia, somnolence, confusion, altered mental status from hypercapnia, and cardiac conduction abnormalities or dysrhythmias, particularly with severe electrolyte derangements.
Essential Evaluation
Initial evaluation includes serum electrolytes, renal function, glucose, and arterial blood gases. Metabolic acidosis is suggested by a low bicarbonate level, while respiratory acidosis is characterized by carbon dioxide retention. Hyperkalemia and hypercalcemia may accompany severe metabolic acidosis. Carbon monoxide levels should be measured when exposure is suspected.
Calculation of the anion gap (Na⁺ − [Cl⁻ + HCO₃⁻]) is critical, with correction for hypoalbuminemia. The degree of compensation must be assessed by comparing expected versus observed PaCO₂ or bicarbonate levels. Failure of appropriate compensation suggests a mixed acid–base disorder.
Advanced Acid–Base Interpretation
In metabolic acidosis, expected PaCO₂ can be estimated using standard formulas. If measured PaCO₂ is higher than expected, concomitant respiratory acidosis or inadequate compensation is present. The delta gap helps identify mixed metabolic disorders by comparing changes in the anion gap with changes in bicarbonate concentration. Disproportionate changes indicate additional metabolic alkalosis or non–anion gap acidosis.
Diagnostic Testing
Arterial blood gas analysis remains the reference standard, though venous blood gas sampling may be useful in stable patients for screening. Urinalysis for glucose and ketones, serum lactate, ketone levels, and toxicology screening are obtained as indicated. Measurement of serum osmolality and calculation of the osmolar gap can suggest toxic alcohol ingestion, though a normal gap does not exclude this diagnosis. Imaging and ECG may help identify underlying cardiopulmonary or ischemic causes.
Management and Stabilization
Initial management focuses on airway, breathing, and circulation. Early intubation should be considered in severe metabolic acidosis when respiratory compensation is failing. Empiric administration of naloxone, dextrose, and thiamine is appropriate in patients with altered mental status.
Respiratory acidosis is managed by treating the underlying cause and providing ventilatory support when hypercapnia worsens. Metabolic acidosis requires identification and correction of the underlying etiology, such as diabetic ketoacidosis, lactic acidosis, or toxic ingestion, along with correction of electrolyte abnormalities and volume resuscitation. Hemodialysis may be necessary in select cases.
Disposition and Follow-Up
Patients with severe acidosis, altered mental status, respiratory failure, hemodynamic instability, significant electrolyte disturbances, or dysrhythmias generally require hospital admission, often to an intensive care setting. Discharge may be considered only when acidosis is resolving, the underlying cause is addressed, and close follow-up is ensured.
Clinical Pearls and Pitfalls
Mixed acid–base disorders are common and frequently missed. Normal pH does not exclude significant pathology if PaCO₂ and bicarbonate are both abnormal. Failure to recognize inadequate respiratory compensation in metabolic acidosis can delay lifesaving ventilatory support. Careful, systematic acid–base analysis is essential in emergency and acute care settings.
- Published on
Emergency and Acute Medicine – Acetaminophen (APAP) Poisoning
Overview and Pathophysiology
Acetaminophen is widely available as a single-agent analgesic, in combination with opioid medications, and as an ingredient in more than 200 over-the-counter cold and flu products. It is among the most common causes of both intentional and accidental poisoning and is the leading cause of acute liver failure requiring transplantation in the United States.
After ingestion, most acetaminophen is safely metabolized, but a small fraction is converted by the cytochrome P-450 system into N-acetyl-p-benzoquinoneimine (NAPQI), a highly toxic metabolite. Under normal conditions, NAPQI is neutralized by glutathione. In overdose, glutathione stores are rapidly depleted, allowing NAPQI to accumulate and cause hepatocellular injury. N-acetylcysteine (NAC) restores glutathione levels and prevents or limits liver damage. Patients with malnutrition are at higher risk because of reduced baseline glutathione reserves.
Pharmacokinetics and Toxic Thresholds
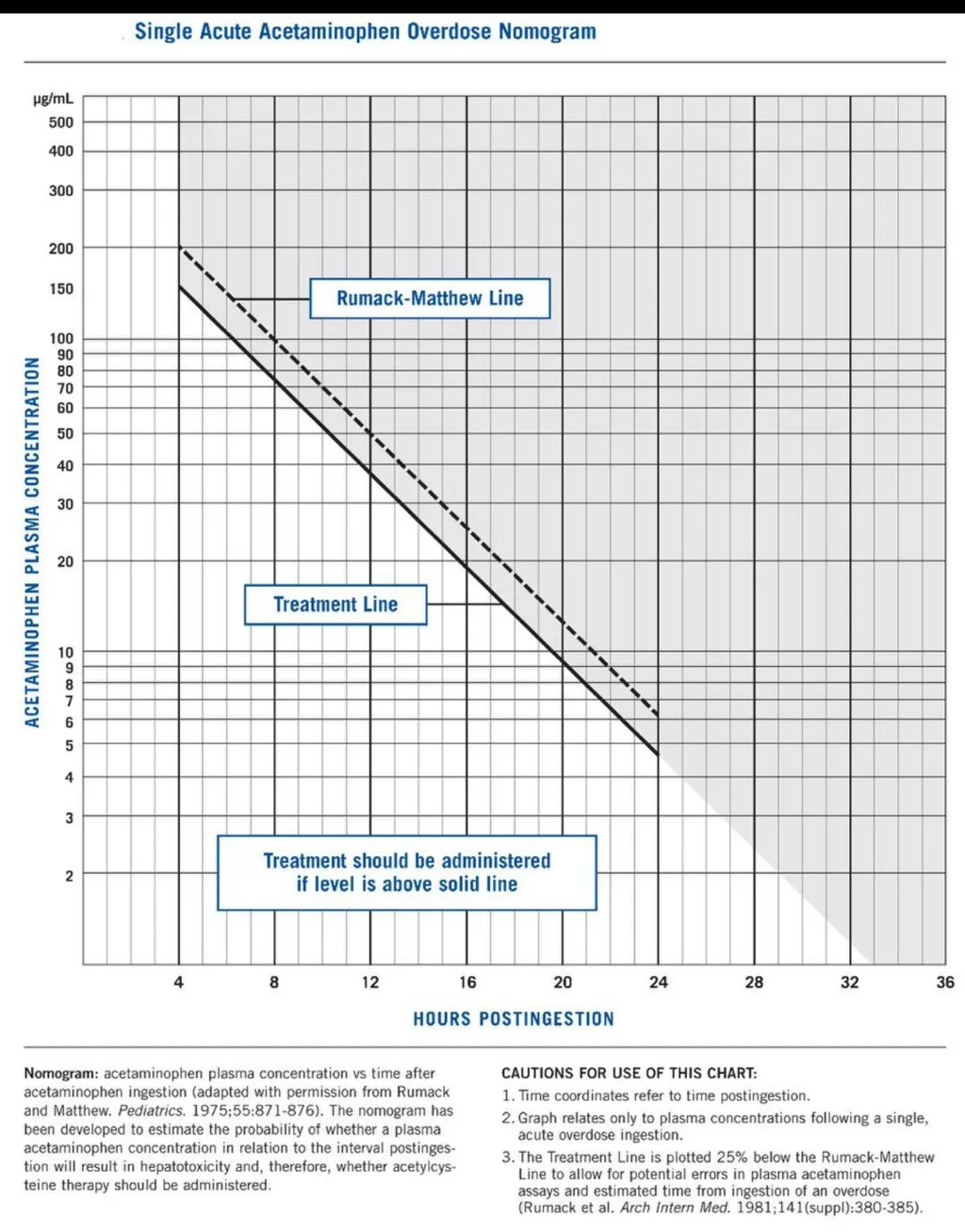
The normal acetaminophen half-life is approximately 2.5–4 hours but becomes prolonged in overdose, often exceeding 4 hours and indicating hepatic dysfunction. An acute ingestion greater than 150 mg/kg is potentially toxic. At 4 hours after ingestion, a serum acetaminophen level of 140 μg/mL or higher suggests toxicity, while therapeutic levels range from 5–20 μg/mL. The Rumack–Matthew nomogram is used to guide treatment decisions following a single, acute ingestion.
Clinical Course and Symptoms
Toxicity typically progresses through four stages.
Phase I (0.5–24 hours): Nausea, vomiting, and malaise may occur, particularly with large ingestions, though symptoms can be mild or absent early.
Phase II (24–72 hours): Gastrointestinal symptoms may improve, but liver injury evolves. Patients develop right upper quadrant pain, rising transaminases, prolonged PT/INR, elevated bilirubin, and sometimes oliguria.
Phase III (72–96 hours): This is the most critical period. Liver enzyme abnormalities peak, hepatic encephalopathy may appear, and worsening coagulopathy or renal failure signals a high likelihood of requiring liver transplantation.
Phase IV (96 hours to 10 days): Patients either recover with gradual hepatic regeneration or progress to fulminant liver failure.
Essential Evaluation
A careful history must identify all acetaminophen-containing products ingested and the timing of ingestion. A serum acetaminophen level should be obtained at 4 hours post-ingestion or immediately upon presentation if more than 4 hours have elapsed. The Rumack–Matthew nomogram applies only to single, acute ingestions and should not be used for chronic or delayed presentations. Early consultation with a poison center or toxicologist is strongly recommended.
Diagnostic Testing
Laboratory evaluation includes serum acetaminophen concentration, electrolytes, blood urea nitrogen, creatinine, glucose, liver enzymes (AST typically rises first), bilirubin, and PT/INR. Severe toxicity may result in AST/ALT levels exceeding 10,000 IU/L. A pregnancy test and toxicology screen should be obtained when appropriate.
Differential Diagnosis
Acetaminophen toxicity should always be considered as a co-ingestant in overdose. Other causes of acute liver injury include viral hepatitis, Reye syndrome, Amanita mushroom poisoning, herbal or dietary supplement toxicity, and other hepatotoxic drugs.
Initial Stabilization
Management begins with airway, breathing, and circulation assessment. Supplemental oxygen should be provided as needed. In patients with altered mental status, empiric administration of naloxone, thiamine, and dextrose (or bedside glucose testing) is appropriate.
Emergency Department Management
Supportive care includes intravenous fluids and antiemetics. A single dose of activated charcoal should be administered if the patient presents soon after ingestion.
N-acetylcysteine (NAC) is the cornerstone of therapy and is nearly 100% effective at preventing hepatotoxicity if started within 8 hours of acute overdose.
NAC Administration Options
Oral NAC has an unpleasant taste and odor and should be diluted to improve tolerability; antiemetics are often required. Vomited doses within one hour should be repeated, and persistent vomiting necessitates nasogastric or intravenous administration.
Intravenous NAC is given as a 21-hour infusion protocol. Oral NAC may be administered intravenously if the IV formulation is unavailable, with toxicology guidance.
Pregnancy Considerations
NAC is not teratogenic and crosses the placenta. Treating the mother effectively protects the fetus, particularly after 14 weeks’ gestation when fetal metabolism can produce toxic metabolites.
Disposition and Follow-Up
Admission is required for patients with hepatotoxic acetaminophen levels, abnormal liver tests, chronic ingestion with liver injury, or suicide attempts requiring psychiatric care.
Asymptomatic patients with non-toxic ingestions who do not require NAC may be discharged with counseling. Early hepatology or transplant consultation is warranted when significant liver injury is present. Patients with intentional overdose require psychiatric evaluation, while those with accidental poisoning need poison-prevention counseling.
Clinical Pearls and Pitfalls
Always consider occult acetaminophen exposure in patients presenting after opioid overdose or with unexplained liver injury. The Rumack–Matthew nomogram should not be used for chronic ingestion or late presentation. NAC should not be stopped until acetaminophen levels are undetectable and clinical and laboratory evidence of hepatotoxicity has improved or resolved.
Overview and Pathophysiology
Acetaminophen is widely available as a single-agent analgesic, in combination with opioid medications, and as an ingredient in more than 200 over-the-counter cold and flu products. It is among the most common causes of both intentional and accidental poisoning and is the leading cause of acute liver failure requiring transplantation in the United States.
After ingestion, most acetaminophen is safely metabolized, but a small fraction is converted by the cytochrome P-450 system into N-acetyl-p-benzoquinoneimine (NAPQI), a highly toxic metabolite. Under normal conditions, NAPQI is neutralized by glutathione. In overdose, glutathione stores are rapidly depleted, allowing NAPQI to accumulate and cause hepatocellular injury. N-acetylcysteine (NAC) restores glutathione levels and prevents or limits liver damage. Patients with malnutrition are at higher risk because of reduced baseline glutathione reserves.
Pharmacokinetics and Toxic Thresholds
The normal acetaminophen half-life is approximately 2.5–4 hours but becomes prolonged in overdose, often exceeding 4 hours and indicating hepatic dysfunction. An acute ingestion greater than 150 mg/kg is potentially toxic. At 4 hours after ingestion, a serum acetaminophen level of 140 μg/mL or higher suggests toxicity, while therapeutic levels range from 5–20 μg/mL. The Rumack–Matthew nomogram is used to guide treatment decisions following a single, acute ingestion.
Clinical Course and Symptoms
Toxicity typically progresses through four stages.
Phase I (0.5–24 hours): Nausea, vomiting, and malaise may occur, particularly with large ingestions, though symptoms can be mild or absent early.
Phase II (24–72 hours): Gastrointestinal symptoms may improve, but liver injury evolves. Patients develop right upper quadrant pain, rising transaminases, prolonged PT/INR, elevated bilirubin, and sometimes oliguria.
Phase III (72–96 hours): This is the most critical period. Liver enzyme abnormalities peak, hepatic encephalopathy may appear, and worsening coagulopathy or renal failure signals a high likelihood of requiring liver transplantation.
Phase IV (96 hours to 10 days): Patients either recover with gradual hepatic regeneration or progress to fulminant liver failure.
Essential Evaluation
A careful history must identify all acetaminophen-containing products ingested and the timing of ingestion. A serum acetaminophen level should be obtained at 4 hours post-ingestion or immediately upon presentation if more than 4 hours have elapsed. The Rumack–Matthew nomogram applies only to single, acute ingestions and should not be used for chronic or delayed presentations. Early consultation with a poison center or toxicologist is strongly recommended.
Diagnostic Testing
Laboratory evaluation includes serum acetaminophen concentration, electrolytes, blood urea nitrogen, creatinine, glucose, liver enzymes (AST typically rises first), bilirubin, and PT/INR. Severe toxicity may result in AST/ALT levels exceeding 10,000 IU/L. A pregnancy test and toxicology screen should be obtained when appropriate.
Differential Diagnosis
Acetaminophen toxicity should always be considered as a co-ingestant in overdose. Other causes of acute liver injury include viral hepatitis, Reye syndrome, Amanita mushroom poisoning, herbal or dietary supplement toxicity, and other hepatotoxic drugs.
Initial Stabilization
Management begins with airway, breathing, and circulation assessment. Supplemental oxygen should be provided as needed. In patients with altered mental status, empiric administration of naloxone, thiamine, and dextrose (or bedside glucose testing) is appropriate.
Emergency Department Management
Supportive care includes intravenous fluids and antiemetics. A single dose of activated charcoal should be administered if the patient presents soon after ingestion.
N-acetylcysteine (NAC) is the cornerstone of therapy and is nearly 100% effective at preventing hepatotoxicity if started within 8 hours of acute overdose.
- If the acetaminophen level cannot be obtained within 8 hours and toxicity is suspected, NAC should be started empirically and stopped if levels prove non-toxic.
- For presentations ≥8 hours after ingestion, NAC should be started immediately while awaiting laboratory confirmation.
- For late (>24 hours) or chronic ingestions, NAC is indicated if ingestion exceeds 150 mg/kg, symptoms are present, or liver tests are abnormal. Therapy may be discontinued once acetaminophen is undetectable and liver enzymes remain normal.
NAC Administration Options
Oral NAC has an unpleasant taste and odor and should be diluted to improve tolerability; antiemetics are often required. Vomited doses within one hour should be repeated, and persistent vomiting necessitates nasogastric or intravenous administration.
Intravenous NAC is given as a 21-hour infusion protocol. Oral NAC may be administered intravenously if the IV formulation is unavailable, with toxicology guidance.
Pregnancy Considerations
NAC is not teratogenic and crosses the placenta. Treating the mother effectively protects the fetus, particularly after 14 weeks’ gestation when fetal metabolism can produce toxic metabolites.
Disposition and Follow-Up
Admission is required for patients with hepatotoxic acetaminophen levels, abnormal liver tests, chronic ingestion with liver injury, or suicide attempts requiring psychiatric care.
Asymptomatic patients with non-toxic ingestions who do not require NAC may be discharged with counseling. Early hepatology or transplant consultation is warranted when significant liver injury is present. Patients with intentional overdose require psychiatric evaluation, while those with accidental poisoning need poison-prevention counseling.
Clinical Pearls and Pitfalls
Always consider occult acetaminophen exposure in patients presenting after opioid overdose or with unexplained liver injury. The Rumack–Matthew nomogram should not be used for chronic ingestion or late presentation. NAC should not be stopped until acetaminophen levels are undetectable and clinical and laboratory evidence of hepatotoxicity has improved or resolved.
- Published on
Emergency and Acute Medicine – Adrenal Insufficiency
Overview and Clinical Significance
Adrenal insufficiency occurs when cortisol production is inadequate to meet the body’s physiologic or stress-related demands. In emergency and acute care, the most critical presentation is acute adrenal insufficiency (Addisonian crisis), a life-threatening condition characterized by hypotension, electrolyte disturbances, and shock. Because laboratory confirmation is often delayed or unavailable in the emergency department, early recognition and empiric treatment are essential to prevent morbidity and mortality.
Etiology and Pathophysiology
Adrenal insufficiency is classified as primary, secondary, or tertiary. Primary adrenal insufficiency results from destruction or dysfunction of the adrenal glands and leads to deficiencies in cortisol and often aldosterone. Causes include autoimmune disease, congenital adrenal hyperplasia, infections (such as tuberculosis or fungal disease), metastatic cancer, infiltrative disorders, bilateral adrenal hemorrhage, and medication-related suppression (e.g., etomidate, ketoconazole). Secondary adrenal insufficiency arises from pituitary dysfunction or chronic suppression of ACTH, most commonly due to prolonged glucocorticoid therapy. Tertiary adrenal insufficiency results from hypothalamic dysfunction. An Addisonian crisis is often triggered by infection, trauma, surgery, dehydration, pregnancy, abrupt steroid withdrawal, or initiation of thyroid hormone in an undiagnosed patient.
Clinical Presentation
Symptoms are frequently nonspecific and may include fatigue, weakness, anorexia, nausea, vomiting, abdominal pain, salt craving, dizziness, and muscle or joint pain. Physical findings often include hypotension, tachycardia, fever or hypothermia, weight loss, and altered mental status. Findings more specific to primary adrenal insufficiency include hyperpigmentation, vitiligo, dehydration, hyperkalemia, and hyponatremia. In Addisonian crisis, patients may present in circulatory shock with severe hypotension, hypoglycemia, electrolyte abnormalities, and acute kidney injury.
Diagnostic Evaluation
Diagnosis in the emergency department is primarily clinical. Laboratory findings typically demonstrate hyponatremia, hyperkalemia, elevated BUN and creatinine from volume depletion, and low or inappropriately normal glucose levels. A random serum cortisol level below 20 μg/dL in a critically ill or hypotensive patient strongly suggests adrenal insufficiency, but treatment should not be delayed while awaiting results. Definitive confirmation with a cosyntropin (ACTH) stimulation test is usually performed after stabilization. If steroids must be administered before testing, dexamethasone is preferred because it does not interfere with cortisol assays.
Emergency Management
Initial management follows airway, breathing, and circulation principles. Aggressive volume resuscitation with isotonic saline is critical to correct hypovolemia and hypotension. Immediate glucocorticoid replacement is required, with intravenous hydrocortisone as first-line therapy; dexamethasone is an acceptable alternative. Hypoglycemia should be treated with intravenous dextrose, and life-threatening hyperkalemia managed using standard emergency protocols. Identification and treatment of precipitating factors, particularly infection or medication nonadherence, are essential components of care.
Disposition and Key Pitfalls
All patients with acute adrenal insufficiency require hospital admission, and those with hemodynamic instability should be managed in an intensive care setting. With timely therapy, blood pressure and clinical status typically improve within several hours. A major pitfall in emergency care is failure to recognize adrenal insufficiency in patients with unexplained hypotension or shock refractory to fluids and vasopressors. When suspected, steroid therapy should be administered immediately, as early treatment is lifesaving and should never be delayed for diagnostic confirmation.

- Published on
Emergency and Acute Medicine – Acute Coronary Syndrome: Myocardial Infarction
Overview and Definitions
Myocardial infarction (MI) results from an acute imbalance between myocardial oxygen supply and demand, leading to ischemia and irreversible myocardial injury. It is a core component of acute coronary syndrome (ACS), which includes unstable angina, non–ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). Differentiation among these entities is essential, as management strategies and urgency of reperfusion differ substantially.
Etiology and Pathophysiology
The most common cause of MI is atherosclerotic coronary artery disease with plaque rupture and superallowing thrombus formation, resulting in partial or complete coronary occlusion. Other mechanisms include coronary vasospasm (variant/Prinzmetal angina), microvascular dysfunction, coronary embolism, arteritis (e.g., lupus, Takayasu arteritis, Kawasaki disease), prolonged hypotension, severe anemia, carbon monoxide poisoning, thyroid storm, or structural abnormalities such as aneurysm or ectasia. Cocaine and amphetamine use may precipitate MI through intense vasospasm and thrombosis.
Major risk factors include hypercholesterolemia, diabetes mellitus, hypertension, smoking, male sex, postmenopausal status in women, and a family history of premature coronary artery disease.
Clinical Presentation
Chest pain is the most common presenting symptom. Patients typically describe substernal pressure, heaviness, squeezing, burning, or tightness. Pain may radiate to the arms, shoulders, back, neck, or jaw. Anginal equivalents, particularly common in older adults, women, and patients with diabetes, include dyspnea, diaphoresis, nausea or vomiting, abdominal pain, syncope, or unexplained weakness.
Symptoms often last longer than 30 minutes and may occur at rest or with exertion. Many patients report preceding crescendo angina. Pain is usually not positional or pleuritic and is often only partially relieved by rest or nitroglycerin. A clenched fist over the chest (Levine sign) is suggestive of ischemic pain.
Physical Examination
The physical exam may be normal, especially early. Possible findings include tachycardia, hypertension during pain, S3 or S4 gallop, a new murmur from papillary muscle dysfunction with mitral regurgitation, diminished peripheral pulses, or signs of acute decompensated heart failure.
Essential Emergency Evaluation
History remains the most critical element in differentiating MI from noncardiac causes of chest pain. Rapid assessment and early testing are required to avoid delays in reperfusion therapy.
Electrocardiography
A 12-lead ECG is the cornerstone of diagnosis and must be obtained immediately. ECG findings help distinguish STEMI from NSTEMI and nonischemic causes of ST elevation such as pericarditis, early repolarization, left ventricular hypertrophy with strain, prior infarction with aneurysm, or hyperkalemia.
Diagnostic criteria for STEMI include new ST-segment elevation at the J point in two contiguous leads (with sex- and lead-specific thresholds). ST depression in leads V1–V2 may indicate posterior infarction.
New or presumed new left bundle branch block alone is no longer considered diagnostic of STEMI; however, Sgarbossa criteria can identify MI in patients with LBBB. Echocardiography may reveal regional wall motion abnormalities or mechanical complications.
Laboratory and Imaging Studies
Cardiac biomarkers (troponin I or T, CK-MB) confirm myocardial necrosis and guide risk stratification. Additional testing includes electrolytes, calcium, magnesium, renal function, and digoxin level when relevant. Chest radiography may reveal pulmonary edema, cardiomegaly, or alternative diagnoses such as aortic dissection.
Differential Diagnosis
The differential for MI-like chest pain includes aortic dissection, pulmonary embolism, pericarditis, pneumonia, pneumothorax, esophageal disorders, biliary disease, peptic ulcer disease, anxiety or panic disorder, and musculoskeletal chest pain.
Prehospital and Initial ED Management
Early management includes IV access, cardiac monitoring, oxygen if hypoxic, aspirin administration, and sublingual nitroglycerin for symptom relief. When feasible, a prehospital ECG with advance notification to the receiving facility improves outcomes.
Definitive Emergency Treatment
STEMI is a time-critical emergency requiring immediate reperfusion. Primary percutaneous coronary intervention (PCI) is preferred and should occur within 90 minutes of first medical contact. If PCI is not available within 120 minutes, fibrinolytic therapy should be administered promptly.
All patients without contraindications should receive aspirin. Dual antiplatelet therapy with clopidogrel, prasugrel, or ticagrelor is used based on reperfusion strategy and patient factors. Nitrates are administered if systolic blood pressure is adequate and there is no evidence of right ventricular infarction.
β-blockers are recommended within the first 24 hours unless contraindicated. Anticoagulation with unfractionated heparin, bivalirudin, or low-molecular-weight heparin is used depending on whether PCI or thrombolysis is planned. Morphine may be used judiciously for pain control.
Life-threatening dysrhythmias and conduction disturbances must be managed promptly, with pacing or defibrillation as indicated. Patients in cardiogenic shock require urgent transfer to a catheterization laboratory for revascularization and mechanical circulatory support when necessary.
Disposition and Follow-Up
All patients with confirmed myocardial infarction require hospital admission, typically to a coronary care or intensive care unit. Patients with uncertain diagnoses often benefit from observation with serial ECGs, biomarkers, and advanced testing. No patient with MI should be discharged from the emergency department.
Clinical Pearls and Pitfalls
Rapid recognition and reperfusion save myocardium and lives—time is muscle. Door-to-needle time for thrombolysis should be within 30 minutes when PCI is unavailable. A single normal ECG or negative biomarker does not exclude MI early in the course. New LBBB alone should not be considered diagnostic without supportive findings. Maintain a high index of suspicion in patients with atypical presentations.
Overview and Definitions
Myocardial infarction (MI) results from an acute imbalance between myocardial oxygen supply and demand, leading to ischemia and irreversible myocardial injury. It is a core component of acute coronary syndrome (ACS), which includes unstable angina, non–ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). Differentiation among these entities is essential, as management strategies and urgency of reperfusion differ substantially.
Etiology and Pathophysiology
The most common cause of MI is atherosclerotic coronary artery disease with plaque rupture and superallowing thrombus formation, resulting in partial or complete coronary occlusion. Other mechanisms include coronary vasospasm (variant/Prinzmetal angina), microvascular dysfunction, coronary embolism, arteritis (e.g., lupus, Takayasu arteritis, Kawasaki disease), prolonged hypotension, severe anemia, carbon monoxide poisoning, thyroid storm, or structural abnormalities such as aneurysm or ectasia. Cocaine and amphetamine use may precipitate MI through intense vasospasm and thrombosis.
Major risk factors include hypercholesterolemia, diabetes mellitus, hypertension, smoking, male sex, postmenopausal status in women, and a family history of premature coronary artery disease.
Clinical Presentation
Chest pain is the most common presenting symptom. Patients typically describe substernal pressure, heaviness, squeezing, burning, or tightness. Pain may radiate to the arms, shoulders, back, neck, or jaw. Anginal equivalents, particularly common in older adults, women, and patients with diabetes, include dyspnea, diaphoresis, nausea or vomiting, abdominal pain, syncope, or unexplained weakness.
Symptoms often last longer than 30 minutes and may occur at rest or with exertion. Many patients report preceding crescendo angina. Pain is usually not positional or pleuritic and is often only partially relieved by rest or nitroglycerin. A clenched fist over the chest (Levine sign) is suggestive of ischemic pain.
Physical Examination
The physical exam may be normal, especially early. Possible findings include tachycardia, hypertension during pain, S3 or S4 gallop, a new murmur from papillary muscle dysfunction with mitral regurgitation, diminished peripheral pulses, or signs of acute decompensated heart failure.
Essential Emergency Evaluation
History remains the most critical element in differentiating MI from noncardiac causes of chest pain. Rapid assessment and early testing are required to avoid delays in reperfusion therapy.
Electrocardiography
A 12-lead ECG is the cornerstone of diagnosis and must be obtained immediately. ECG findings help distinguish STEMI from NSTEMI and nonischemic causes of ST elevation such as pericarditis, early repolarization, left ventricular hypertrophy with strain, prior infarction with aneurysm, or hyperkalemia.
Diagnostic criteria for STEMI include new ST-segment elevation at the J point in two contiguous leads (with sex- and lead-specific thresholds). ST depression in leads V1–V2 may indicate posterior infarction.
New or presumed new left bundle branch block alone is no longer considered diagnostic of STEMI; however, Sgarbossa criteria can identify MI in patients with LBBB. Echocardiography may reveal regional wall motion abnormalities or mechanical complications.
Laboratory and Imaging Studies
Cardiac biomarkers (troponin I or T, CK-MB) confirm myocardial necrosis and guide risk stratification. Additional testing includes electrolytes, calcium, magnesium, renal function, and digoxin level when relevant. Chest radiography may reveal pulmonary edema, cardiomegaly, or alternative diagnoses such as aortic dissection.
Differential Diagnosis
The differential for MI-like chest pain includes aortic dissection, pulmonary embolism, pericarditis, pneumonia, pneumothorax, esophageal disorders, biliary disease, peptic ulcer disease, anxiety or panic disorder, and musculoskeletal chest pain.
Prehospital and Initial ED Management
Early management includes IV access, cardiac monitoring, oxygen if hypoxic, aspirin administration, and sublingual nitroglycerin for symptom relief. When feasible, a prehospital ECG with advance notification to the receiving facility improves outcomes.
Definitive Emergency Treatment
STEMI is a time-critical emergency requiring immediate reperfusion. Primary percutaneous coronary intervention (PCI) is preferred and should occur within 90 minutes of first medical contact. If PCI is not available within 120 minutes, fibrinolytic therapy should be administered promptly.
All patients without contraindications should receive aspirin. Dual antiplatelet therapy with clopidogrel, prasugrel, or ticagrelor is used based on reperfusion strategy and patient factors. Nitrates are administered if systolic blood pressure is adequate and there is no evidence of right ventricular infarction.
β-blockers are recommended within the first 24 hours unless contraindicated. Anticoagulation with unfractionated heparin, bivalirudin, or low-molecular-weight heparin is used depending on whether PCI or thrombolysis is planned. Morphine may be used judiciously for pain control.
Life-threatening dysrhythmias and conduction disturbances must be managed promptly, with pacing or defibrillation as indicated. Patients in cardiogenic shock require urgent transfer to a catheterization laboratory for revascularization and mechanical circulatory support when necessary.
Disposition and Follow-Up
All patients with confirmed myocardial infarction require hospital admission, typically to a coronary care or intensive care unit. Patients with uncertain diagnoses often benefit from observation with serial ECGs, biomarkers, and advanced testing. No patient with MI should be discharged from the emergency department.
Clinical Pearls and Pitfalls
Rapid recognition and reperfusion save myocardium and lives—time is muscle. Door-to-needle time for thrombolysis should be within 30 minutes when PCI is unavailable. A single normal ECG or negative biomarker does not exclude MI early in the course. New LBBB alone should not be considered diagnostic without supportive findings. Maintain a high index of suspicion in patients with atypical presentations.

- Published on
Emergency and Acute Medicine – Acromioclavicular (AC) Joint Injury
Anatomy and Injury Overview
The acromioclavicular (AC) joint is formed by the distal clavicle articulating with the acromion of the scapula. Stability is provided by the acromioclavicular (AC) ligament, the coracoclavicular (CC) ligament, and dynamic support from the deltoid and trapezius muscles. The AC ligament primarily maintains horizontal stability, while the CC ligament provides vertical stability. Injury occurs along a predictable spectrum, classically described by the Rockwood classification, which reflects progressive disruption of these stabilizing structures.
Rockwood Classification
Type I injuries involve a sprain of the AC ligament without rupture. The CC ligament, deltoid, and trapezius remain intact, and radiographs are normal; diagnosis is clinical, with localized AC joint tenderness.
Type II injuries feature rupture of the AC ligament with horizontal instability of the distal clavicle and a sprained but intact CC ligament. Mild deltoid and trapezius injury may be present. Imaging shows slight widening of the AC joint (normally <5 mm) with a normal cc distance (11–13 mm).< />pan>
Type III injuries include rupture of both the AC and CC ligaments, producing horizontal and vertical instability. The deltoid and trapezius are detached, and radiographs demonstrate widening of the AC joint with superior displacement of the distal clavicle, typically about 100%.
Types IV, V, and VI represent severe injuries and are best appreciated on axillary or lateral views. All require operative management and carry a higher risk of prolonged disability. Type IV involves posterior displacement of the clavicle into the trapezius; Type V shows marked superior displacement with a 100–300% increase in CC distance and dramatic shoulder droop; Type VI, usually associated with high-energy trauma, features inferior displacement of the clavicle into a subacromial or subcoracoid position and is often accompanied by neurovascular injury.
Mechanism and Epidemiology
AC joint injuries are most common in young, active males, particularly during contact sports. The typical mechanism is a direct blow to the superior or lateral shoulder with the arm adducted, such as during a fall. Less commonly, injury occurs indirectly through a fall on an outstretched hand or elbow, transmitting force to the AC joint.
Clinical Presentation
Patients usually report pain over the superior or anterior shoulder following trauma, worsened by cross-body movement, reaching behind the back, or overhead activity. The severity of symptoms correlates with the degree of ligament disruption. Associated neurovascular complaints or cervical spine symptoms should heighten concern for severe injury.
Physical Examination
Examination is best performed with the patient seated or standing, as gravity accentuates instability. Inspection may reveal swelling, ecchymosis, deformity, asymmetry, or skin tenting. A prominent distal clavicle with a sagging acromion suggests at least a Type II injury.
Palpation should proceed systematically from the sternoclavicular joint along the clavicle to the AC joint, CC ligament, coracoid process, scapula, and proximal humerus. AC joint tenderness suggests AC ligament injury, while horizontal instability indicates rupture. Tenderness or vertical instability implicates CC ligament disruption.
Provocative maneuvers include the cross-body adduction test, which compresses the AC joint and reproduces pain, and the O’Brien test, which may elicit superior shoulder pain in AC pathology. A complete distal neurovascular examination, including assessment of the brachial plexus, and a careful cervical spine evaluation are essential.
Diagnostic Evaluation
Diagnosis relies on history, examination, and targeted imaging. Dedicated AC joint radiographs with bilateral comparison are recommended when injury is suspected, as standard shoulder views may obscure subtle findings. The Zanca view (10–15° cephalic tilt) improves visualization of the AC joint, while axillary views are critical for identifying posterior or inferior clavicular displacement. Stress views are no longer routinely recommended. Advanced imaging with CT or MRI is reserved for surgical planning or complex injuries, and angiography may be indicated if vascular compromise is suspected.
Differential Diagnosis
Conditions that may mimic AC joint injury include shoulder dislocation, clavicle or acromion fractures, rotator cuff pathology, tendinitis, adhesive capsulitis, cervical radiculopathy, osteoarthritis, osteomyelitis, and—in children—distal clavicle physeal fractures.
Management in the Emergency Setting
Initial care includes ice application, sling immobilization, analgesia, and cervical spine precautions when indicated.
Type I and II injuries are managed conservatively with rest, ice, NSAIDs, brief sling use (typically 3–7 days), and early range-of-motion exercises. Most patients return to normal activity within 2–4 weeks once painless strength and motion are restored.
Type III injuries require sling immobilization, analgesia, and early orthopedic referral (within 72 hours). Management is controversial, with treatment individualized based on patient age, activity level, occupation, hand dominance, and reinjury risk.
Types IV, V, and VI injuries necessitate immediate orthopedic consultation and operative repair.
A recognized long-term complication of AC joint injury is post-traumatic arthritis.
Pediatric Considerations
In children, the clavicle is encased in a periosteal sleeve, with the CC ligament contained within and the AC ligament external and more vulnerable. True AC joint dislocations are uncommon in pediatrics and are usually Type I or II. Distal clavicle physeal fractures are more frequent. Younger children with Type III injuries are typically managed conservatively, while adolescents may require more aggressive treatment. Types IV–VI generally require surgery.
Disposition and Follow-Up
Patients with Type I or II injuries may be discharged with orthopedic follow-up in 2–4 weeks. Type III injuries require urgent orthopedic evaluation, and Types IV–VI typically warrant admission for operative management. Open injuries and pediatric cases should receive prompt specialist assessment.
Clinical Pearls and Pitfalls
Normal CC spacing distinguishes Type I and II injuries and supports conservative management. Type III injuries demonstrate complete superior displacement and require early orthopedic input. Types IV–VI share ligamentous disruption with Type III injuries but differ by clavicular position and uniformly require surgical repair.
Anatomy and Injury Overview
The acromioclavicular (AC) joint is formed by the distal clavicle articulating with the acromion of the scapula. Stability is provided by the acromioclavicular (AC) ligament, the coracoclavicular (CC) ligament, and dynamic support from the deltoid and trapezius muscles. The AC ligament primarily maintains horizontal stability, while the CC ligament provides vertical stability. Injury occurs along a predictable spectrum, classically described by the Rockwood classification, which reflects progressive disruption of these stabilizing structures.
Rockwood Classification
Type I injuries involve a sprain of the AC ligament without rupture. The CC ligament, deltoid, and trapezius remain intact, and radiographs are normal; diagnosis is clinical, with localized AC joint tenderness.
Type II injuries feature rupture of the AC ligament with horizontal instability of the distal clavicle and a sprained but intact CC ligament. Mild deltoid and trapezius injury may be present. Imaging shows slight widening of the AC joint (normally <5 mm) with a normal cc distance (11–13 mm).< />pan>
Type III injuries include rupture of both the AC and CC ligaments, producing horizontal and vertical instability. The deltoid and trapezius are detached, and radiographs demonstrate widening of the AC joint with superior displacement of the distal clavicle, typically about 100%.
Types IV, V, and VI represent severe injuries and are best appreciated on axillary or lateral views. All require operative management and carry a higher risk of prolonged disability. Type IV involves posterior displacement of the clavicle into the trapezius; Type V shows marked superior displacement with a 100–300% increase in CC distance and dramatic shoulder droop; Type VI, usually associated with high-energy trauma, features inferior displacement of the clavicle into a subacromial or subcoracoid position and is often accompanied by neurovascular injury.
Mechanism and Epidemiology
AC joint injuries are most common in young, active males, particularly during contact sports. The typical mechanism is a direct blow to the superior or lateral shoulder with the arm adducted, such as during a fall. Less commonly, injury occurs indirectly through a fall on an outstretched hand or elbow, transmitting force to the AC joint.
Clinical Presentation
Patients usually report pain over the superior or anterior shoulder following trauma, worsened by cross-body movement, reaching behind the back, or overhead activity. The severity of symptoms correlates with the degree of ligament disruption. Associated neurovascular complaints or cervical spine symptoms should heighten concern for severe injury.
Physical Examination
Examination is best performed with the patient seated or standing, as gravity accentuates instability. Inspection may reveal swelling, ecchymosis, deformity, asymmetry, or skin tenting. A prominent distal clavicle with a sagging acromion suggests at least a Type II injury.
Palpation should proceed systematically from the sternoclavicular joint along the clavicle to the AC joint, CC ligament, coracoid process, scapula, and proximal humerus. AC joint tenderness suggests AC ligament injury, while horizontal instability indicates rupture. Tenderness or vertical instability implicates CC ligament disruption.
Provocative maneuvers include the cross-body adduction test, which compresses the AC joint and reproduces pain, and the O’Brien test, which may elicit superior shoulder pain in AC pathology. A complete distal neurovascular examination, including assessment of the brachial plexus, and a careful cervical spine evaluation are essential.
Diagnostic Evaluation
Diagnosis relies on history, examination, and targeted imaging. Dedicated AC joint radiographs with bilateral comparison are recommended when injury is suspected, as standard shoulder views may obscure subtle findings. The Zanca view (10–15° cephalic tilt) improves visualization of the AC joint, while axillary views are critical for identifying posterior or inferior clavicular displacement. Stress views are no longer routinely recommended. Advanced imaging with CT or MRI is reserved for surgical planning or complex injuries, and angiography may be indicated if vascular compromise is suspected.
Differential Diagnosis
Conditions that may mimic AC joint injury include shoulder dislocation, clavicle or acromion fractures, rotator cuff pathology, tendinitis, adhesive capsulitis, cervical radiculopathy, osteoarthritis, osteomyelitis, and—in children—distal clavicle physeal fractures.
Management in the Emergency Setting
Initial care includes ice application, sling immobilization, analgesia, and cervical spine precautions when indicated.
Type I and II injuries are managed conservatively with rest, ice, NSAIDs, brief sling use (typically 3–7 days), and early range-of-motion exercises. Most patients return to normal activity within 2–4 weeks once painless strength and motion are restored.
Type III injuries require sling immobilization, analgesia, and early orthopedic referral (within 72 hours). Management is controversial, with treatment individualized based on patient age, activity level, occupation, hand dominance, and reinjury risk.
Types IV, V, and VI injuries necessitate immediate orthopedic consultation and operative repair.
A recognized long-term complication of AC joint injury is post-traumatic arthritis.
Pediatric Considerations
In children, the clavicle is encased in a periosteal sleeve, with the CC ligament contained within and the AC ligament external and more vulnerable. True AC joint dislocations are uncommon in pediatrics and are usually Type I or II. Distal clavicle physeal fractures are more frequent. Younger children with Type III injuries are typically managed conservatively, while adolescents may require more aggressive treatment. Types IV–VI generally require surgery.
Disposition and Follow-Up
Patients with Type I or II injuries may be discharged with orthopedic follow-up in 2–4 weeks. Type III injuries require urgent orthopedic evaluation, and Types IV–VI typically warrant admission for operative management. Open injuries and pediatric cases should receive prompt specialist assessment.
Clinical Pearls and Pitfalls
Normal CC spacing distinguishes Type I and II injuries and supports conservative management. Type III injuries demonstrate complete superior displacement and require early orthopedic input. Types IV–VI share ligamentous disruption with Type III injuries but differ by clavicular position and uniformly require surgical repair.

- Published on
Emergency and Acute Medicine – Acute Coronary Syndrome: Myocardial Infarction
Overview and Definitions
Myocardial infarction (MI) results from an acute imbalance between myocardial oxygen supply and demand, leading to ischemia and irreversible myocardial injury. It is a core component of acute coronary syndrome (ACS), which includes unstable angina, non–ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). Differentiation among these entities is essential, as management strategies and urgency of reperfusion differ substantially.
Etiology and Pathophysiology
The most common cause of MI is atherosclerotic coronary artery disease with plaque rupture and superallowing thrombus formation, resulting in partial or complete coronary occlusion. Other mechanisms include coronary vasospasm (variant/Prinzmetal angina), microvascular dysfunction, coronary embolism, arteritis (e.g., lupus, Takayasu arteritis, Kawasaki disease), prolonged hypotension, severe anemia, carbon monoxide poisoning, thyroid storm, or structural abnormalities such as aneurysm or ectasia. Cocaine and amphetamine use may precipitate MI through intense vasospasm and thrombosis.
Major risk factors include hypercholesterolemia, diabetes mellitus, hypertension, smoking, male sex, postmenopausal status in women, and a family history of premature coronary artery disease.
Clinical Presentation
Chest pain is the most common presenting symptom. Patients typically describe substernal pressure, heaviness, squeezing, burning, or tightness. Pain may radiate to the arms, shoulders, back, neck, or jaw. Anginal equivalents, particularly common in older adults, women, and patients with diabetes, include dyspnea, diaphoresis, nausea or vomiting, abdominal pain, syncope, or unexplained weakness.
Symptoms often last longer than 30 minutes and may occur at rest or with exertion. Many patients report preceding crescendo angina. Pain is usually not positional or pleuritic and is often only partially relieved by rest or nitroglycerin. A clenched fist over the chest (Levine sign) is suggestive of ischemic pain.
Physical Examination
The physical exam may be normal, especially early. Possible findings include tachycardia, hypertension during pain, S3 or S4 gallop, a new murmur from papillary muscle dysfunction with mitral regurgitation, diminished peripheral pulses, or signs of acute decompensated heart failure.
Essential Emergency Evaluation
History remains the most critical element in differentiating MI from noncardiac causes of chest pain. Rapid assessment and early testing are required to avoid delays in reperfusion therapy.
Electrocardiography
A 12-lead ECG is the cornerstone of diagnosis and must be obtained immediately. ECG findings help distinguish STEMI from NSTEMI and nonischemic causes of ST elevation such as pericarditis, early repolarization, left ventricular hypertrophy with strain, prior infarction with aneurysm, or hyperkalemia.
Diagnostic criteria for STEMI include new ST-segment elevation at the J point in two contiguous leads (with sex- and lead-specific thresholds). ST depression in leads V1–V2 may indicate posterior infarction.
New or presumed new left bundle branch block alone is no longer considered diagnostic of STEMI; however, Sgarbossa criteria can identify MI in patients with LBBB. Echocardiography may reveal regional wall motion abnormalities or mechanical complications.
Laboratory and Imaging Studies
Cardiac biomarkers (troponin I or T, CK-MB) confirm myocardial necrosis and guide risk stratification. Additional testing includes electrolytes, calcium, magnesium, renal function, and digoxin level when relevant. Chest radiography may reveal pulmonary edema, cardiomegaly, or alternative diagnoses such as aortic dissection.
Differential Diagnosis
The differential for MI-like chest pain includes aortic dissection, pulmonary embolism, pericarditis, pneumonia, pneumothorax, esophageal disorders, biliary disease, peptic ulcer disease, anxiety or panic disorder, and musculoskeletal chest pain.
Prehospital and Initial ED Management
Early management includes IV access, cardiac monitoring, oxygen if hypoxic, aspirin administration, and sublingual nitroglycerin for symptom relief. When feasible, a prehospital ECG with advance notification to the receiving facility improves outcomes.
Definitive Emergency Treatment
STEMI is a time-critical emergency requiring immediate reperfusion. Primary percutaneous coronary intervention (PCI) is preferred and should occur within 90 minutes of first medical contact. If PCI is not available within 120 minutes, fibrinolytic therapy should be administered promptly.
All patients without contraindications should receive aspirin. Dual antiplatelet therapy with clopidogrel, prasugrel, or ticagrelor is used based on reperfusion strategy and patient factors. Nitrates are administered if systolic blood pressure is adequate and there is no evidence of right ventricular infarction.
β-blockers are recommended within the first 24 hours unless contraindicated. Anticoagulation with unfractionated heparin, bivalirudin, or low-molecular-weight heparin is used depending on whether PCI or thrombolysis is planned. Morphine may be used judiciously for pain control.
Life-threatening dysrhythmias and conduction disturbances must be managed promptly, with pacing or defibrillation as indicated. Patients in cardiogenic shock require urgent transfer to a catheterization laboratory for revascularization and mechanical circulatory support when necessary.
Disposition and Follow-Up
All patients with confirmed myocardial infarction require hospital admission, typically to a coronary care or intensive care unit. Patients with uncertain diagnoses often benefit from observation with serial ECGs, biomarkers, and advanced testing. No patient with MI should be discharged from the emergency department.
Clinical Pearls and Pitfalls
Rapid recognition and reperfusion save myocardium and lives—time is muscle. Door-to-needle time for thrombolysis should be within 30 minutes when PCI is unavailable. A single normal ECG or negative biomarker does not exclude MI early in the course. New LBBB alone should not be considered diagnostic without supportive findings. Maintain a high index of suspicion in patients with atypical presentations.
Overview and Definitions
Myocardial infarction (MI) results from an acute imbalance between myocardial oxygen supply and demand, leading to ischemia and irreversible myocardial injury. It is a core component of acute coronary syndrome (ACS), which includes unstable angina, non–ST-elevation myocardial infarction (NSTEMI), and ST-elevation myocardial infarction (STEMI). Differentiation among these entities is essential, as management strategies and urgency of reperfusion differ substantially.
Etiology and Pathophysiology
The most common cause of MI is atherosclerotic coronary artery disease with plaque rupture and superallowing thrombus formation, resulting in partial or complete coronary occlusion. Other mechanisms include coronary vasospasm (variant/Prinzmetal angina), microvascular dysfunction, coronary embolism, arteritis (e.g., lupus, Takayasu arteritis, Kawasaki disease), prolonged hypotension, severe anemia, carbon monoxide poisoning, thyroid storm, or structural abnormalities such as aneurysm or ectasia. Cocaine and amphetamine use may precipitate MI through intense vasospasm and thrombosis.
Major risk factors include hypercholesterolemia, diabetes mellitus, hypertension, smoking, male sex, postmenopausal status in women, and a family history of premature coronary artery disease.
Clinical Presentation
Chest pain is the most common presenting symptom. Patients typically describe substernal pressure, heaviness, squeezing, burning, or tightness. Pain may radiate to the arms, shoulders, back, neck, or jaw. Anginal equivalents, particularly common in older adults, women, and patients with diabetes, include dyspnea, diaphoresis, nausea or vomiting, abdominal pain, syncope, or unexplained weakness.
Symptoms often last longer than 30 minutes and may occur at rest or with exertion. Many patients report preceding crescendo angina. Pain is usually not positional or pleuritic and is often only partially relieved by rest or nitroglycerin. A clenched fist over the chest (Levine sign) is suggestive of ischemic pain.
Physical Examination
The physical exam may be normal, especially early. Possible findings include tachycardia, hypertension during pain, S3 or S4 gallop, a new murmur from papillary muscle dysfunction with mitral regurgitation, diminished peripheral pulses, or signs of acute decompensated heart failure.
Essential Emergency Evaluation
History remains the most critical element in differentiating MI from noncardiac causes of chest pain. Rapid assessment and early testing are required to avoid delays in reperfusion therapy.
Electrocardiography
A 12-lead ECG is the cornerstone of diagnosis and must be obtained immediately. ECG findings help distinguish STEMI from NSTEMI and nonischemic causes of ST elevation such as pericarditis, early repolarization, left ventricular hypertrophy with strain, prior infarction with aneurysm, or hyperkalemia.
Diagnostic criteria for STEMI include new ST-segment elevation at the J point in two contiguous leads (with sex- and lead-specific thresholds). ST depression in leads V1–V2 may indicate posterior infarction.
New or presumed new left bundle branch block alone is no longer considered diagnostic of STEMI; however, Sgarbossa criteria can identify MI in patients with LBBB. Echocardiography may reveal regional wall motion abnormalities or mechanical complications.
Laboratory and Imaging Studies
Cardiac biomarkers (troponin I or T, CK-MB) confirm myocardial necrosis and guide risk stratification. Additional testing includes electrolytes, calcium, magnesium, renal function, and digoxin level when relevant. Chest radiography may reveal pulmonary edema, cardiomegaly, or alternative diagnoses such as aortic dissection.
Differential Diagnosis
The differential for MI-like chest pain includes aortic dissection, pulmonary embolism, pericarditis, pneumonia, pneumothorax, esophageal disorders, biliary disease, peptic ulcer disease, anxiety or panic disorder, and musculoskeletal chest pain.
Prehospital and Initial ED Management
Early management includes IV access, cardiac monitoring, oxygen if hypoxic, aspirin administration, and sublingual nitroglycerin for symptom relief. When feasible, a prehospital ECG with advance notification to the receiving facility improves outcomes.
Definitive Emergency Treatment
STEMI is a time-critical emergency requiring immediate reperfusion. Primary percutaneous coronary intervention (PCI) is preferred and should occur within 90 minutes of first medical contact. If PCI is not available within 120 minutes, fibrinolytic therapy should be administered promptly.
All patients without contraindications should receive aspirin. Dual antiplatelet therapy with clopidogrel, prasugrel, or ticagrelor is used based on reperfusion strategy and patient factors. Nitrates are administered if systolic blood pressure is adequate and there is no evidence of right ventricular infarction.
β-blockers are recommended within the first 24 hours unless contraindicated. Anticoagulation with unfractionated heparin, bivalirudin, or low-molecular-weight heparin is used depending on whether PCI or thrombolysis is planned. Morphine may be used judiciously for pain control.
Life-threatening dysrhythmias and conduction disturbances must be managed promptly, with pacing or defibrillation as indicated. Patients in cardiogenic shock require urgent transfer to a catheterization laboratory for revascularization and mechanical circulatory support when necessary.
Disposition and Follow-Up
All patients with confirmed myocardial infarction require hospital admission, typically to a coronary care or intensive care unit. Patients with uncertain diagnoses often benefit from observation with serial ECGs, biomarkers, and advanced testing. No patient with MI should be discharged from the emergency department.
Clinical Pearls and Pitfalls
Rapid recognition and reperfusion save myocardium and lives—time is muscle. Door-to-needle time for thrombolysis should be within 30 minutes when PCI is unavailable. A single normal ECG or negative biomarker does not exclude MI early in the course. New LBBB alone should not be considered diagnostic without supportive findings. Maintain a high index of suspicion in patients with atypical presentations.
- Published on
Diagnostic Test – Gallium Scanning
1. How does this test work?
Gallium scanning is a nuclear medicine imaging study used to detect infection and certain malignancies.
Mechanism:
2. When is a gallium scan the appropriate choice?
Choose a gallium scan when the clinical picture includes:
1. How does this test work?
Gallium scanning is a nuclear medicine imaging study used to detect infection and certain malignancies.
Mechanism:
- Gallium localizes to areas with:
- Increased white blood cell activity
- Increased iron metabolism
- It is transported in the blood bound to transferrin
- Areas of inflammation, infection, or malignancy show increased gallium uptake
2. When is a gallium scan the appropriate choice?
Choose a gallium scan when the clinical picture includes:
- Persistent fever without localizing symptoms
- Negative initial evaluation, including:
- Blood cultures
- Chest X-ray
- Urinalysis
- Fever of unknown origin (FUO)
- Lymphoma
- Occult abscesses
- A biopsy is the most definitive test following an abnormal gallium scan
- Malignancy → requires histologic confirmation
- Infection → requires culture confirmation

- Published on
Diagnostic Test – Herpes Simplex PCR
1. What is this?
Herpes simplex PCR is a molecular diagnostic test performed on cerebrospinal fluid (CSF).
It detects HSV DNA and is the single most accurate diagnostic test for herpes simplex encephalitis.
2. When is this the correct choice?
Select HSV PCR of the CSF when the clinical scenario includes:
- Fever
- Headache
- Altered mental status or confusion
- Symptom duration less than 2 weeks
Key test-taking point:
- CSF HSV PCR is more accurate than:
- EEG
- Head CT
- Brain MRI
- Even brain biopsy