- Published on
Diagnostic Tests – Coronary Angiography (Cardiac Catheterization)
What Is Coronary Angiography / Cardiac Catheterization?
Coronary angiography—often performed as part of cardiac catheterization—is an invasive procedure in which a catheter is threaded through a large artery, typically the femoral or brachial artery, and advanced into the coronary vessels. Once in place, iodinated contrast dye is injected directly into the coronary arteries. X-ray fluoroscopy then captures dynamic images of blood flow, allowing clinicians to visualize the coronary anatomy in real time.
It is considered the gold standard for assessing coronary artery disease because it provides the most precise and direct evaluation of coronary lumen narrowing.
When Is Coronary Angiography the Correct Answer?
Angiography is indicated when a definitive understanding of coronary anatomy is needed, especially when noninvasive tests are abnormal or insufficient. It is the correct choice in the following scenarios:
What Does Coronary Angiography Show?
Coronary angiography provides direct visualization of the coronary arteries, allowing clinicians to determine:
What Is Coronary Angiography / Cardiac Catheterization?
Coronary angiography—often performed as part of cardiac catheterization—is an invasive procedure in which a catheter is threaded through a large artery, typically the femoral or brachial artery, and advanced into the coronary vessels. Once in place, iodinated contrast dye is injected directly into the coronary arteries. X-ray fluoroscopy then captures dynamic images of blood flow, allowing clinicians to visualize the coronary anatomy in real time.
It is considered the gold standard for assessing coronary artery disease because it provides the most precise and direct evaluation of coronary lumen narrowing.
When Is Coronary Angiography the Correct Answer?
Angiography is indicated when a definitive understanding of coronary anatomy is needed, especially when noninvasive tests are abnormal or insufficient. It is the correct choice in the following scenarios:
- After an abnormal cardiac stress test, to confirm the presence, severity, and location of coronary stenosis.
- Before coronary revascularization procedures, such as coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI)/angioplasty.
- In the setting of acute coronary syndromes, particularly unstable angina, where urgent diagnostic clarification is needed to guide management and potential intervention.
What Does Coronary Angiography Show?
Coronary angiography provides direct visualization of the coronary arteries, allowing clinicians to determine:
- The degree of stenosis (narrowing) of each coronary vessel
- The number of vessels involved
- The precise anatomic location of blockages
- Whether stenoses are severe enough to be considered clinically significant

- Published on
Diagnostic Tests – CK-MB
What Is CK-MB?
CK-MB (Creatine Kinase–Myocardial Band) is a cardiac enzyme released into the bloodstream when myocardial cells are damaged. It serves as a marker of acute myocardial injury, most commonly used in the evaluation of suspected myocardial infarction (MI). CK-MB levels begin to rise approximately 4–6 hours after the onset of chest pain, reach their peak at around 12–24 hours, and then decline relatively quickly because CK-MB has a shorter half-life than troponin.
Because of this rapid return to baseline, CK-MB is particularly useful for detecting reinfarction, where a second rise in enzyme levels may occur after an earlier MI.
When Is CK-MB the Correct Answer?
CK-MB should be selected when evaluating a patient with possible ischemic chest pain, especially if risk factors for coronary disease are present. Importantly, CK-MB can be elevated even when the EKG is nondiagnostic or lacks ST-segment elevation.
It is also the correct choice when chest pain recurs shortly after a recent myocardial infarction—usually within the previous few days. Because CK-MB falls faster than troponin, a new rise in CK-MB can reliably indicate re-infarction, making it uniquely valuable in this scenario.

- Published on
Diagnostic Tests – BNP (Brain Natriuretic Peptide)
What Is BNP?
Brain natriuretic peptide (BNP) is a hormone released primarily from the ventricles—and to a lesser extent the atria—in response to increased wall stretch and pressure overload. When the heart experiences volume expansion or elevated filling pressures, BNP is secreted to counteract these stresses by promoting diuresis, natriuresis, and vasodilation. It also inhibits the renin–angiotensin–aldosterone system (RAAS), helping the body reduce fluid overload.
BNP levels rise significantly in congestive heart failure (CHF) and other states of hypervolemia, making it a useful biomarker for assessing cardiac vs. non-cardiac causes of dyspnea.
When Is BNP the Correct Answer?
BNP testing is especially valuable when evaluating a patient with shortness of breath whose clinical presentation is not clearly diagnostic. If the history and physical exam are ambiguous—for example, when it is unclear whether symptoms are due to:
BNP becomes the correct test to help rule out CHF.
A normal or low BNP makes heart failure unlikely, while an elevated BNP supports—but does not definitively prove—the diagnosis of CHF. The key exam point: BNP is sensitive but not specific.
What Is the Most Accurate Test?
Although BNP is a useful screening tool, the most accurate diagnostic test for confirming heart failure is echocardiography. Echo provides direct visualization of cardiac structure and function, allowing assessment of ventricular size, wall motion, and ejection fraction.
What Is BNP?
Brain natriuretic peptide (BNP) is a hormone released primarily from the ventricles—and to a lesser extent the atria—in response to increased wall stretch and pressure overload. When the heart experiences volume expansion or elevated filling pressures, BNP is secreted to counteract these stresses by promoting diuresis, natriuresis, and vasodilation. It also inhibits the renin–angiotensin–aldosterone system (RAAS), helping the body reduce fluid overload.
BNP levels rise significantly in congestive heart failure (CHF) and other states of hypervolemia, making it a useful biomarker for assessing cardiac vs. non-cardiac causes of dyspnea.
When Is BNP the Correct Answer?
BNP testing is especially valuable when evaluating a patient with shortness of breath whose clinical presentation is not clearly diagnostic. If the history and physical exam are ambiguous—for example, when it is unclear whether symptoms are due to:
- Congestive heart failure
- Pneumonia
- COPD
- Pulmonary embolism
BNP becomes the correct test to help rule out CHF.
A normal or low BNP makes heart failure unlikely, while an elevated BNP supports—but does not definitively prove—the diagnosis of CHF. The key exam point: BNP is sensitive but not specific.
What Is the Most Accurate Test?
Although BNP is a useful screening tool, the most accurate diagnostic test for confirming heart failure is echocardiography. Echo provides direct visualization of cardiac structure and function, allowing assessment of ventricular size, wall motion, and ejection fraction.

- Published on
Diagnostic Tests – Ventricular Tachycardia (VT)
What Is the Diagnosis?
The EKG demonstrates ventricular tachycardia (VT), a dangerous arrhythmia characterized by a wide-complex tachycardia, with QRS complexes greater than 120 milliseconds. VT originates from the ventricles rather than the atria, which results in broad, abnormal QRS complexes that appear uniform or slightly varied depending on the underlying mechanism. By board exam convention, any regular wide-complex tachycardia should be assumed to be VT unless proven otherwise, making this an essential recognition pattern in cardiology.
What Case Will Go Along With This EKG?
Ventricular tachycardia can present with a wide range of symptoms, from mild palpitations to life-threatening instability. A typical case might involve a patient who develops syncope, lightheadedness, shortness of breath, or symptoms of congestive heart failure. In severe situations, VT may cause sudden cardiac death, emphasizing the need for rapid diagnosis and treatment. VT commonly occurs in patients with underlying structural heart disease, such as prior myocardial infarction, cardiomyopathy, severe electrolyte disturbances, or antiarrhythmic drug toxicity. Because symptoms alone cannot reliably identify VT, the EKG is essential for diagnosis.
How Do You Treat It?
Treatment of ventricular tachycardia depends entirely on patient stability. When the patient is unstable—with hypotension, chest pain, altered mental status, or signs of shock—the correct and immediate treatment is synchronized electrical cardioversion, which is lifesaving. For stable patients who are maintaining blood pressure and mentation, pharmacologic therapy is appropriate. Intravenous amiodarone is typically first-line, while lidocaine (especially in post–MI patients) and procainamide are effective alternatives. Regardless of the initial approach, VT is a serious arrhythmia that demands prompt intervention and frequently leads to further diagnostic evaluation, such as electrophysiology studies, to determine its etiology.
What Is the Diagnosis?
The EKG demonstrates ventricular tachycardia (VT), a dangerous arrhythmia characterized by a wide-complex tachycardia, with QRS complexes greater than 120 milliseconds. VT originates from the ventricles rather than the atria, which results in broad, abnormal QRS complexes that appear uniform or slightly varied depending on the underlying mechanism. By board exam convention, any regular wide-complex tachycardia should be assumed to be VT unless proven otherwise, making this an essential recognition pattern in cardiology.
What Case Will Go Along With This EKG?
Ventricular tachycardia can present with a wide range of symptoms, from mild palpitations to life-threatening instability. A typical case might involve a patient who develops syncope, lightheadedness, shortness of breath, or symptoms of congestive heart failure. In severe situations, VT may cause sudden cardiac death, emphasizing the need for rapid diagnosis and treatment. VT commonly occurs in patients with underlying structural heart disease, such as prior myocardial infarction, cardiomyopathy, severe electrolyte disturbances, or antiarrhythmic drug toxicity. Because symptoms alone cannot reliably identify VT, the EKG is essential for diagnosis.
How Do You Treat It?
Treatment of ventricular tachycardia depends entirely on patient stability. When the patient is unstable—with hypotension, chest pain, altered mental status, or signs of shock—the correct and immediate treatment is synchronized electrical cardioversion, which is lifesaving. For stable patients who are maintaining blood pressure and mentation, pharmacologic therapy is appropriate. Intravenous amiodarone is typically first-line, while lidocaine (especially in post–MI patients) and procainamide are effective alternatives. Regardless of the initial approach, VT is a serious arrhythmia that demands prompt intervention and frequently leads to further diagnostic evaluation, such as electrophysiology studies, to determine its etiology.

- Published on
Diagnostic Tests – Tilt-Table Testing
What Is Tilt-Table Testing?
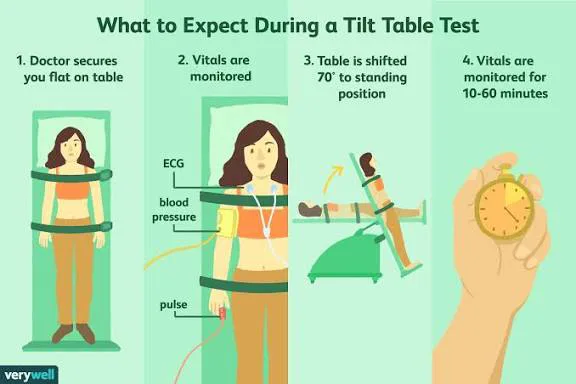
Tilt-table testing is a diagnostic procedure used to evaluate unexplained syncope, particularly when fainting episodes may be related to autonomic dysfunction or abnormal cardiovascular reflexes. The test involves monitoring blood pressure and heart rate while the patient is gradually tilted from a lying to an upright position. By changing the angle of the patient’s body, clinicians can observe how the cardiovascular system responds to positional changes that mimic everyday standing.
How Is Tilt-Table Testing Performed?
The patient is secured on a motorized table that can be tilted to various angles. Blood pressure and heart rate are recorded at baseline and during each positional shift. The test attempts to reproduce symptoms such as dizziness, lightheadedness, or syncope.
An abnormal result occurs when tilting produces:
- Syncope or near-syncope
- Significant dizziness
- An inappropriate or exaggerated drop in blood pressure
- Inadequate compensatory heart rate response (e.g., inappropriate bradycardia)
To enhance sensitivity, medications such as isoproterenol or nitroglycerin may be used as provocative agents, increasing the likelihood of triggering symptoms in susceptible patients.
When Is Tilt-Table Testing the Correct Answer?
Tilt-table testing is appropriate in cases of unexplained syncope, particularly when initial evaluation (history, physical exam, EKG, and routine labs) does not reveal a clear cause. It is especially valuable when syncope appears related to orthostatic changes, such as:
- Episodes of fainting when standing
- Symptoms consistent with neurocardiogenic (vasovagal) syncope
- A paradoxical or inappropriate bradycardia upon standing
- Suspected autonomic dysfunction
In these situations, a tilt-table test helps confirm whether syncope is due to abnormal autonomic reflexes rather than cardiac arrhythmias, structural disease, or neurologic disorders.
- Published on
Diagnostic Tests – Transesophageal Echocardiography (TEE)
What Is Transesophageal Echocardiography (TEE)?
Transesophageal echocardiography is a highly sensitive and detailed form of cardiac ultrasound in which images of the heart are obtained from within the esophagus rather than across the chest wall. Because the esophagus sits directly behind the heart, TEE provides superior visualization of posterior cardiac structures and is far more sensitive than transthoracic echocardiography (TTE) for detecting abnormalities of the left atrium, atrial appendage, mitral valve, and thoracic aorta.
TEE is especially useful for identifying conditions such as aortic dissection, thoracic aortic aneurysm, atrial thrombi, patent foramen ovale, and infective endocarditis vegetations.
How Is TEE Performed?
TEE is conducted by passing a flexible endoscopic probe with an ultrasound transducer at its tip through the patient’s mouth and into the esophagus. After mild sedation and local throat anesthesia, the probe is positioned behind the heart, where it emits ultrasound waves and captures high-resolution images unobstructed by the chest wall, lungs, or ribs.
This proximity allows for exceptionally clear visualization of cardiac chambers, valves, and the proximal aorta.
When Should You Choose or Answer TEE?
TEE is indicated when:
What Is the Most Accurate Diagnostic Test?
Although TEE is the most sensitive noninvasive method for visualizing many cardiac structures, the most accurate diagnostic test overall for coronary anatomy is left-heart cardiac catheterization (coronary angiography).
Catheterization provides direct measurement of coronary stenosis and remains the gold standard for diagnosing obstructive coronary artery disease.
What Is Transesophageal Echocardiography (TEE)?
Transesophageal echocardiography is a highly sensitive and detailed form of cardiac ultrasound in which images of the heart are obtained from within the esophagus rather than across the chest wall. Because the esophagus sits directly behind the heart, TEE provides superior visualization of posterior cardiac structures and is far more sensitive than transthoracic echocardiography (TTE) for detecting abnormalities of the left atrium, atrial appendage, mitral valve, and thoracic aorta.
TEE is especially useful for identifying conditions such as aortic dissection, thoracic aortic aneurysm, atrial thrombi, patent foramen ovale, and infective endocarditis vegetations.
How Is TEE Performed?
TEE is conducted by passing a flexible endoscopic probe with an ultrasound transducer at its tip through the patient’s mouth and into the esophagus. After mild sedation and local throat anesthesia, the probe is positioned behind the heart, where it emits ultrasound waves and captures high-resolution images unobstructed by the chest wall, lungs, or ribs.
This proximity allows for exceptionally clear visualization of cardiac chambers, valves, and the proximal aorta.
When Should You Choose or Answer TEE?
TEE is indicated when:
- Transthoracic echo is inadequate due to poor acoustic windows (obesity, COPD, chest wall deformities).
- There is a need to evaluate posterior cardiac structures, including:
- Left atrial or left atrial appendage thrombus
- Endocarditis with suspected valvular vegetations
- Suspected PFO or intracardiac shunts
- Suspected aortic dissection or aneurysm
What Is the Most Accurate Diagnostic Test?
Although TEE is the most sensitive noninvasive method for visualizing many cardiac structures, the most accurate diagnostic test overall for coronary anatomy is left-heart cardiac catheterization (coronary angiography).
Catheterization provides direct measurement of coronary stenosis and remains the gold standard for diagnosing obstructive coronary artery disease.

- Published on
Diagnostic Tests– Transthoracic or 2D Echocardiogram (TTE)
What Is a Transthoracic Echocardiogram (TTE)?
A transthoracic echocardiogram (TTE) is the standard, noninvasive ultrasound study of the heart. It provides detailed information about cardiac chamber size, ventricular function, valvular structure and motion, intracardiac masses, pericardial effusion, and aspects of aortic disease. Because it is safe, painless, and widely available, TTE is one of the most commonly used imaging tests in cardiology and serves as a cornerstone of cardiac evaluation.
How Is a TTE Performed?
The test is done by placing a sonographic transducer on the anterior chest wall (usually in the parasternal, apical, and subcostal windows). The transducer emits ultrasound waves that bounce off cardiac structures and return as high-resolution images. TTE provides real-time visualization of heart motion, wall thickening, valve opening and closing, and blood flow patterns when combined with Doppler imaging.
When Should You Choose or Answer TTE?
TTE is appropriate in a wide range of clinical situations, including:
TTE is the second most commonly performed cardiac test after the EKG.
What Is the Most Accurate Diagnostic Test?
Although TTE provides extensive structural and functional information, other tests are more accurate for specific purposes:
Thus, while TTE is an excellent first-line imaging study, it is not the single most accurate test for many specific conditions.
What Is a Transthoracic Echocardiogram (TTE)?
A transthoracic echocardiogram (TTE) is the standard, noninvasive ultrasound study of the heart. It provides detailed information about cardiac chamber size, ventricular function, valvular structure and motion, intracardiac masses, pericardial effusion, and aspects of aortic disease. Because it is safe, painless, and widely available, TTE is one of the most commonly used imaging tests in cardiology and serves as a cornerstone of cardiac evaluation.
How Is a TTE Performed?
The test is done by placing a sonographic transducer on the anterior chest wall (usually in the parasternal, apical, and subcostal windows). The transducer emits ultrasound waves that bounce off cardiac structures and return as high-resolution images. TTE provides real-time visualization of heart motion, wall thickening, valve opening and closing, and blood flow patterns when combined with Doppler imaging.
When Should You Choose or Answer TTE?
TTE is appropriate in a wide range of clinical situations, including:
- Any patient with an auscultated murmur or valvular abnormality to assess severity and structural impact.
- All patients with suspected or known congestive heart failure (CHF) to measure ejection fraction, which helps distinguish systolic vs. diastolic dysfunction—a crucial step because treatment differs significantly between the two.
- Evaluation of intracardiac masses, suspected tumors, thrombi, or vegetations when TEE is not yet indicated.
- Initial evaluation of pericardial effusion or suspected tamponade.
- General assessment of structural heart disease and ventricular function.
TTE is the second most commonly performed cardiac test after the EKG.
What Is the Most Accurate Diagnostic Test?
Although TTE provides extensive structural and functional information, other tests are more accurate for specific purposes:
- Transesophageal echocardiography (TEE) is more sensitive for evaluating the posterior cardiac structures, left atrial appendage, valves, and thoracic aorta.
- Coronary angiography remains the gold standard for identifying coronary artery stenosis and is more accurate for diagnosing obstructive coronary disease.
Thus, while TTE is an excellent first-line imaging study, it is not the single most accurate test for many specific conditions.

- Published on
Diagnostic Tests – Cardiac Electrophysiological (EP) Studies
What Is an EP Study?
A cardiac electrophysiological (EP) study is an invasive diagnostic procedure in which specialized catheters equipped with electrical sensing and stimulating electrodes are inserted into the heart via peripheral veins. These catheters record electrical activity directly from within the cardiac chambers and can deliver controlled electrical impulses.
This allows clinicians to identify abnormal rhythm disturbances, test the heart’s conduction pathways, and provoke arrhythmias under controlled conditions. The technique provides precise information about the site of origin, mechanism, and severity of cardiac arrhythmias.
When Is an EP Study the Correct Answer?
EP studies are used when definitive diagnosis or direct treatment of cardiac arrhythmias is required. They are typically chosen in the following situations:
In short, EP studies provide both definitive diagnosis and therapeutic options for complex rhythm disorders.
What Is an EP Study?
A cardiac electrophysiological (EP) study is an invasive diagnostic procedure in which specialized catheters equipped with electrical sensing and stimulating electrodes are inserted into the heart via peripheral veins. These catheters record electrical activity directly from within the cardiac chambers and can deliver controlled electrical impulses.
This allows clinicians to identify abnormal rhythm disturbances, test the heart’s conduction pathways, and provoke arrhythmias under controlled conditions. The technique provides precise information about the site of origin, mechanism, and severity of cardiac arrhythmias.
When Is an EP Study the Correct Answer?
EP studies are used when definitive diagnosis or direct treatment of cardiac arrhythmias is required. They are typically chosen in the following situations:
- Unexplained syncope, especially when arrhythmia is suspected and noninvasive testing is inconclusive.
- Detailed mapping of the cardiac conduction system, useful for complex arrhythmias or pre-ablation planning.
- Ablation therapy for arrhythmias such as supraventricular tachycardia (SVT) or Wolff-Parkinson-White (WPW) syndrome, where identifying and destroying the aberrant pathway cures the condition.
- Evaluation and placement of implantable cardioverter-defibrillators (ICDs) in patients at risk for malignant arrhythmias.
- Localization of the origin of sustained ventricular tachycardia, which is essential for targeted ablation or device therapy.
In short, EP studies provide both definitive diagnosis and therapeutic options for complex rhythm disorders.

- Published on
Diagnostic Tests – Holter Monitoring (24-Hour Ambulatory Cardiac Monitoring)
What Is Holter Monitoring?
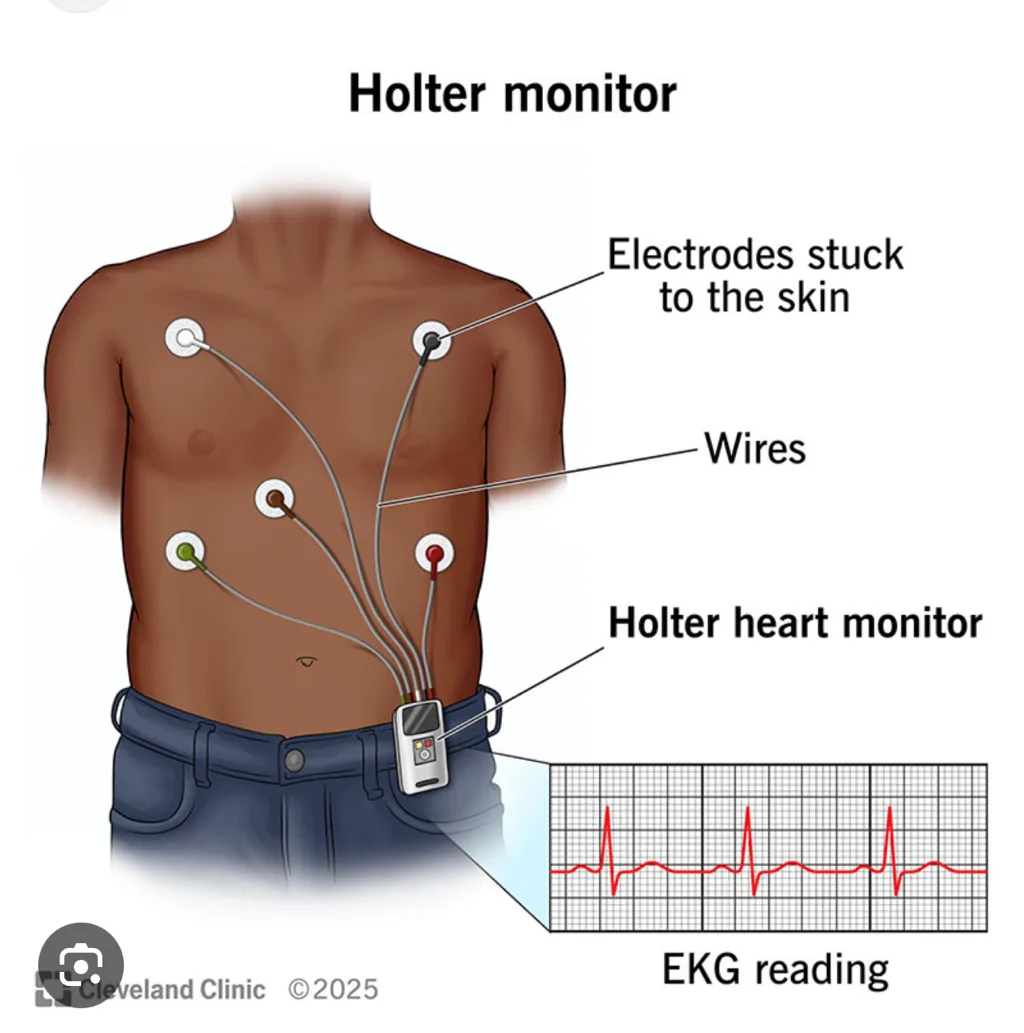
Holter monitoring is a form of continuous ambulatory EKG recording that captures a patient’s cardiac rhythm over a full 24-hour period (or sometimes longer). Unlike a single snapshot EKG performed in the clinic, a Holter monitor records every heartbeat over an extended time, making it possible to detect intermittent arrhythmias that may not be present during a brief office visit.
How Does It Work?
The patient wears several adhesive EKG leads on the chest, which are connected to a small portable recorder worn on a strap around the neck or clipped to the belt. The device continuously records a single-lead or multi-lead EKG while the patient goes about normal daily activities.
After 24 hours, the recording is reviewed—often at high speed—to identify brief rhythm disturbances such as premature beats, paroxysmal atrial fibrillation, supraventricular tachycardia, pauses, or transient conduction blocks. In this way, Holter monitoring captures arrhythmias that a standard EKG might easily miss.
What Is the Most Accurate Test?
Abnormalities detected on Holter monitoring can be evaluated further with:
Thus, while Holter monitors are excellent for detection, EP studies are more accurate for definitive diagnosis and treatment planning.
When Do You Answer Holter Monitoring?
Holter monitoring is the correct diagnostic choice when a patient has symptoms suggestive of an arrhythmia, but an in-office EKG is normal or nondiagnostic. Common indications include:
If the symptom is brief, infrequent, and unpredictable—and especially if the resting EKG is normal—Holter monitoring is the best initial test to capture the electrical event.
What Is Holter Monitoring?
Holter monitoring is a form of continuous ambulatory EKG recording that captures a patient’s cardiac rhythm over a full 24-hour period (or sometimes longer). Unlike a single snapshot EKG performed in the clinic, a Holter monitor records every heartbeat over an extended time, making it possible to detect intermittent arrhythmias that may not be present during a brief office visit.
How Does It Work?
The patient wears several adhesive EKG leads on the chest, which are connected to a small portable recorder worn on a strap around the neck or clipped to the belt. The device continuously records a single-lead or multi-lead EKG while the patient goes about normal daily activities.
After 24 hours, the recording is reviewed—often at high speed—to identify brief rhythm disturbances such as premature beats, paroxysmal atrial fibrillation, supraventricular tachycardia, pauses, or transient conduction blocks. In this way, Holter monitoring captures arrhythmias that a standard EKG might easily miss.
What Is the Most Accurate Test?
Abnormalities detected on Holter monitoring can be evaluated further with:
- Electrophysiologic (EP) studies, which provide the most accurate mapping and diagnosis of rhythm disorders
- Echocardiography, to assess structural causes of arrhythmias
Thus, while Holter monitors are excellent for detection, EP studies are more accurate for definitive diagnosis and treatment planning.
When Do You Answer Holter Monitoring?
Holter monitoring is the correct diagnostic choice when a patient has symptoms suggestive of an arrhythmia, but an in-office EKG is normal or nondiagnostic. Common indications include:
- Palpitations
- Syncope or near-syncope
- Intermittent dizziness
- Suspected paroxysmal arrhythmias not captured on a standard EKG
If the symptom is brief, infrequent, and unpredictable—and especially if the resting EKG is normal—Holter monitoring is the best initial test to capture the electrical event.
- Published on
Diagnostic Tests – Estrogen and Progesterone Receptors (ER/PR)
1. What Are These Tests?
Estrogen and progesterone receptor (ER/PR) testing is performed on all newly diagnosed breast cancer specimens to determine whether the tumor expresses hormone receptors. These receptors, when present on cancer cells, indicate that the tumor’s growth is influenced by estrogen or progesterone signaling. Identifying ER/PR positivity is crucial because it predicts whether the cancer is likely to respond to hormone-blocking therapy. In practice, a tissue sample from the breast tumor is analyzed using immunohistochemistry (IHC) to detect receptor presence. A tumor may be positive for estrogen receptors alone, progesterone receptors alone, or both.
2. What Is the Therapy?
Patients whose tumors express either estrogen receptors, progesterone receptors, or both are candidates for hormone (endocrine) therapy. The standard treatments include medications such as tamoxifen or raloxifene, which block estrogen’s action on breast tissue. Tamoxifen is most commonly used and is particularly effective when both estrogen and progesterone receptors are positive, as dual positivity predicts a stronger therapeutic response. These agents help reduce recurrence risk, shrink residual disease, and improve long-term outcomes by preventing estrogen-driven tumor growth. In some cases—especially in postmenopausal women—aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) may also be used, although the classic board-style answer based on your content focuses on tamoxifen or raloxifene.
1. What Are These Tests?
Estrogen and progesterone receptor (ER/PR) testing is performed on all newly diagnosed breast cancer specimens to determine whether the tumor expresses hormone receptors. These receptors, when present on cancer cells, indicate that the tumor’s growth is influenced by estrogen or progesterone signaling. Identifying ER/PR positivity is crucial because it predicts whether the cancer is likely to respond to hormone-blocking therapy. In practice, a tissue sample from the breast tumor is analyzed using immunohistochemistry (IHC) to detect receptor presence. A tumor may be positive for estrogen receptors alone, progesterone receptors alone, or both.
2. What Is the Therapy?
Patients whose tumors express either estrogen receptors, progesterone receptors, or both are candidates for hormone (endocrine) therapy. The standard treatments include medications such as tamoxifen or raloxifene, which block estrogen’s action on breast tissue. Tamoxifen is most commonly used and is particularly effective when both estrogen and progesterone receptors are positive, as dual positivity predicts a stronger therapeutic response. These agents help reduce recurrence risk, shrink residual disease, and improve long-term outcomes by preventing estrogen-driven tumor growth. In some cases—especially in postmenopausal women—aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) may also be used, although the classic board-style answer based on your content focuses on tamoxifen or raloxifene.

