- Published on
Symptoms and Signs – Differential Diagnosis of Clay-colored stool
Hepatic, gallbladder, or pancreatic problems are typically the cause of pale, putty-colored feces. Bile pigments are typically responsible for the stool's distinctive brown hue. However, the production or release of these pigments into the colon may be impeded by hepatocellular degeneration or biliary blockage, leading to stools that are clay-colored. These stools are frequently linked to dark, "cola-colored" urine and jaundice.
Physical examination and history
Record the patient's initial observation of clay-colored feces, then look into related symptoms like exhaustion, anorexia, weight loss, nausea, vomiting, abdominal discomfort, and dark urine. Does the patient have issues breaking down large meals or fatty foods? Is he prone to bruises? Next, look over the patient's medical history for conditions related to the pancreas, liver, or gallbladder. Has he ever had surgery on his biliary system? Has he had barium studies recently? For a few days, barium lightens the color of stool. Inquire about the usage of an acid as well, as excessive use may brighten the color of the stool. Take note of any past alcohol use or exposure to other chemicals that can harm the liver. After evaluating the patient's overall appearance, examine his vital signs and look for jaundice in his eyes and skin. Next, look at the abdomen: Auscultate for hypoactive bowel sounds and check for ascites and distention. Check for masses and rebound soreness by percussion and palpation. Lastly, collect feces and urine samples for examination in a lab.
Medical Reasons
carcinoma of the bile duct
Clay-colored feces are frequently a first indication of bile duct cancer. Other symptoms include jaundice, pruritus, weight loss and anorexia, upper abdominal pain, bleeding tendencies, and a palpable tumor.
cirrhosis of the liver
Unknown pruritus that gets worse at night, weakness, exhaustion, weight loss, and nebulous stomach pain are often followed by clay-colored feces; these symptoms can last for years. Jaundice, hyperpigmentation, and malabsorption symptoms such nocturnal diarrhea, steatorrhea, purpura, and osteomalacia-related back and bone pain are related findings. Additionally, the patient may experience xanthomas on his elbows, palms, and soles, hematemesis, ascites, edema, and firm, nontender hepatomegaly.
cholerosing (cholangitis)
Cholangitis, a chronic inflammatory disease characterized by bile duct fibrosis, can result in fever, chills, right upper quadrant pain, pruritus, clay-colored feces, and intermittent or chronic jaundice.
Cholelithiasis
When stones in the biliary tract block the common bile duct, it can result in choledocholithiasis, which is characterized by clay-colored feces. On the other hand, regular and clay-colored feces may alternate if the obstruction is sporadic. Dyspepsia and the typical biliary colic that occurs with abrupt, acute blockage are associated symptoms. Antacids do not help this ache in the right upper quadrant, which worsens over several hours and may radiate to the shoulder blades or epigastrium. Tachycardia, restlessness, nausea, food intolerance, vomiting, soreness in the upper abdomen, fever, chills, and jaundice are all symptoms that accompany the pain. liver cancer. Weight loss, weakness, and anorexia are typically experienced by the patient prior to the development of clay-colored feces. He may subsequently experience fever, ascites, dependent edema, jaundice, right upper quadrant pain, and nodular, hard hepatomegaly. If a significant portion of the liver is affected by the cancer, auscultation may reveal a bruit, hum, or rubbing sound.
Hepatitis
The icteric phase of viral hepatitis begins with clay-colored feces, which are usually followed within 1 to 5 days by jaundice. Mild weight loss, dark urine, and the persistence of some preicteric symptoms like anorexia and painful hepatomegaly are associated symptoms. The patient may experience severe pruritus, splenomegaly, enlarged cervical lymph nodes, and right upper quadrant pain during the icteric phase. Even though the patient's appetite normally returns and his hepatomegaly lessens, he nevertheless experiences weariness, flatulence, abdominal pain or tenderness, and dyspepsia after the jaundice goes away. Full healing occurs six months after the posticteric phase, which typically lasts two to six weeks. Along with other symptoms of viral hepatitis, clay-colored feces are a symptom of cholestatic nonviral hepatitis.
carcinoma of the pancreas
Clay-colored stools are a common bile duct obstruction linked to pancreatic cancer. Back or abdominal discomfort, jaundice, pruritus, nausea, vomiting, anorexia, weight loss, weakness, exhaustion, and fever are classic symptoms. Additional potential side effects include splenomegaly, mental instability, diarrhea, skin rashes (particularly on the legs), and symptoms of gastrointestinal bleeding. A bruit in the left upper quadrant and periumbilical region may be detected by auscultation.
Acute pancreatitis
An inflammatory condition called pancreatitis can result in jaundice, dark urine, and clay-colored feces. Usually, it also results in excruciating epigastric pain that travels to the back and gets worse when you lie down. A fever, soreness and rigidity in the abdomen, hypoactive bowel sounds, crackles at the bases of the lungs, nausea, and vomiting are all related symptoms. Significant restlessness, tachycardia, mottled skin, and cold, sweaty extremities are symptoms of acute pancreatitis.
Other Reasons
surgery for the biliary system. Clay-colored feces may be the result of bile duct stricture brought on by biliary surgery.
Get the patient ready for diagnostic procedures such endoscopy, retrograde cholangiopancreatography, hepatitis panels, liver enzyme and serum bilirubin levels, sonograms, computed tomography scans, and stool analyses.
Counseling for Patients Describe dietary changes, the significance of abstaining from alcohol, the necessity of rest, and strategies to lessen stomach discomfort. Infants suffering from biliary atresia may have feces that are clay-colored. Surgery should be taken into consideration early on for the treatment of chronic systems since older people with cholelithiasis are more likely to experience consequences if the condition is left untreated.
Hepatic, gallbladder, or pancreatic problems are typically the cause of pale, putty-colored feces. Bile pigments are typically responsible for the stool's distinctive brown hue. However, the production or release of these pigments into the colon may be impeded by hepatocellular degeneration or biliary blockage, leading to stools that are clay-colored. These stools are frequently linked to dark, "cola-colored" urine and jaundice.
Physical examination and history
Record the patient's initial observation of clay-colored feces, then look into related symptoms like exhaustion, anorexia, weight loss, nausea, vomiting, abdominal discomfort, and dark urine. Does the patient have issues breaking down large meals or fatty foods? Is he prone to bruises? Next, look over the patient's medical history for conditions related to the pancreas, liver, or gallbladder. Has he ever had surgery on his biliary system? Has he had barium studies recently? For a few days, barium lightens the color of stool. Inquire about the usage of an acid as well, as excessive use may brighten the color of the stool. Take note of any past alcohol use or exposure to other chemicals that can harm the liver. After evaluating the patient's overall appearance, examine his vital signs and look for jaundice in his eyes and skin. Next, look at the abdomen: Auscultate for hypoactive bowel sounds and check for ascites and distention. Check for masses and rebound soreness by percussion and palpation. Lastly, collect feces and urine samples for examination in a lab.
Medical Reasons
carcinoma of the bile duct
Clay-colored feces are frequently a first indication of bile duct cancer. Other symptoms include jaundice, pruritus, weight loss and anorexia, upper abdominal pain, bleeding tendencies, and a palpable tumor.
cirrhosis of the liver
Unknown pruritus that gets worse at night, weakness, exhaustion, weight loss, and nebulous stomach pain are often followed by clay-colored feces; these symptoms can last for years. Jaundice, hyperpigmentation, and malabsorption symptoms such nocturnal diarrhea, steatorrhea, purpura, and osteomalacia-related back and bone pain are related findings. Additionally, the patient may experience xanthomas on his elbows, palms, and soles, hematemesis, ascites, edema, and firm, nontender hepatomegaly.
cholerosing (cholangitis)
Cholangitis, a chronic inflammatory disease characterized by bile duct fibrosis, can result in fever, chills, right upper quadrant pain, pruritus, clay-colored feces, and intermittent or chronic jaundice.
Cholelithiasis
When stones in the biliary tract block the common bile duct, it can result in choledocholithiasis, which is characterized by clay-colored feces. On the other hand, regular and clay-colored feces may alternate if the obstruction is sporadic. Dyspepsia and the typical biliary colic that occurs with abrupt, acute blockage are associated symptoms. Antacids do not help this ache in the right upper quadrant, which worsens over several hours and may radiate to the shoulder blades or epigastrium. Tachycardia, restlessness, nausea, food intolerance, vomiting, soreness in the upper abdomen, fever, chills, and jaundice are all symptoms that accompany the pain. liver cancer. Weight loss, weakness, and anorexia are typically experienced by the patient prior to the development of clay-colored feces. He may subsequently experience fever, ascites, dependent edema, jaundice, right upper quadrant pain, and nodular, hard hepatomegaly. If a significant portion of the liver is affected by the cancer, auscultation may reveal a bruit, hum, or rubbing sound.
Hepatitis
The icteric phase of viral hepatitis begins with clay-colored feces, which are usually followed within 1 to 5 days by jaundice. Mild weight loss, dark urine, and the persistence of some preicteric symptoms like anorexia and painful hepatomegaly are associated symptoms. The patient may experience severe pruritus, splenomegaly, enlarged cervical lymph nodes, and right upper quadrant pain during the icteric phase. Even though the patient's appetite normally returns and his hepatomegaly lessens, he nevertheless experiences weariness, flatulence, abdominal pain or tenderness, and dyspepsia after the jaundice goes away. Full healing occurs six months after the posticteric phase, which typically lasts two to six weeks. Along with other symptoms of viral hepatitis, clay-colored feces are a symptom of cholestatic nonviral hepatitis.
carcinoma of the pancreas
Clay-colored stools are a common bile duct obstruction linked to pancreatic cancer. Back or abdominal discomfort, jaundice, pruritus, nausea, vomiting, anorexia, weight loss, weakness, exhaustion, and fever are classic symptoms. Additional potential side effects include splenomegaly, mental instability, diarrhea, skin rashes (particularly on the legs), and symptoms of gastrointestinal bleeding. A bruit in the left upper quadrant and periumbilical region may be detected by auscultation.
Acute pancreatitis
An inflammatory condition called pancreatitis can result in jaundice, dark urine, and clay-colored feces. Usually, it also results in excruciating epigastric pain that travels to the back and gets worse when you lie down. A fever, soreness and rigidity in the abdomen, hypoactive bowel sounds, crackles at the bases of the lungs, nausea, and vomiting are all related symptoms. Significant restlessness, tachycardia, mottled skin, and cold, sweaty extremities are symptoms of acute pancreatitis.
Other Reasons
surgery for the biliary system. Clay-colored feces may be the result of bile duct stricture brought on by biliary surgery.
Get the patient ready for diagnostic procedures such endoscopy, retrograde cholangiopancreatography, hepatitis panels, liver enzyme and serum bilirubin levels, sonograms, computed tomography scans, and stool analyses.
Counseling for Patients Describe dietary changes, the significance of abstaining from alcohol, the necessity of rest, and strategies to lessen stomach discomfort. Infants suffering from biliary atresia may have feces that are clay-colored. Surgery should be taken into consideration early on for the treatment of chronic systems since older people with cholelithiasis are more likely to experience consequences if the condition is left untreated.

- Published on
Symptoms and Signs – Differential Diagnosis of Stridor
Stridor is a loud, harsh, musical respiratory sound that arises from a blockage in the trachea or larynx. This indication is often audible during inspiration but may also manifest during expiration in cases of severe upper airway blockage. It may commence as low-pitched "croaking" and advance to high-pitched "crowing" as respiration intensifies. Life-threatening upper airway obstruction may arise from foreign-body aspiration, excessive secretions, an intraluminal tumor, localized edema or muscular spasms, and external compression due to a tumor or aneurysm.
URGENT INTERVENTIONS
Upon hearing stridor, promptly assess the patient's vital signs, particularly oxygen saturation, and evaluate for additional indicators of partial airway obstruction—such as choking or gagging, tachypnea, dyspnea, shallow respirations, intercostal retractions, nasal flaring, tachycardia, cyanosis, and diaphoresis. Be mindful that a sudden cessation of stridor indicates total obstruction, wherein the patient exhibits inspiratory chest movement but lacks breath sounds. Incapable of speech, he rapidly becomes lethargic and loses consciousness.
Upon detecting indications of airway obstruction, attempt to alleviate the obstruction with back blows or abdominal thrusts (Heimlich maneuver). Subsequently, provide oxygen by nasal cannula or face mask, or ready the patient for emergency endotracheal intubation or tracheostomy and mechanical ventilation.
Refer to Emergency Endotracheal Intubation. Prepare equipment for the aspiration of vomitus or blood via the endotracheal or tracheostomy tube. Attach the patient to a cardiac monitor and arrange him in an upright posture to facilitate respiration.
Medical History and Physical Assessment
When the patient's condition allows, acquire a medical history from the patient or a family member. Initially, ascertain the onset of the stridor. Has he previously experienced it? Does he possess an upper respiratory tract infection? How long has he possessed it? Inquire about a history of allergies, neoplasms, and respiratory and vascular conditions. Document recent exposure to smoke or harmful vapors or gasses. Subsequently, investigate related indications and symptoms. Does stridor manifest with discomfort or cough? Subsequently, inspect the patient's oral cavity for excessive secretions, foreign substances, irritation, and edema. Examine his neck for edema, tumors, subcutaneous crepitus, and scars. Examine the patient's chest for delayed, diminished, or uneven expansion. Perform auscultation to detect wheezes, rhonchi, crackles, rubs, and other atypical respiratory sounds. Perform percussion to assess for dullness, tympany, or flatness. Finally, observe for burns or indications of trauma, like ecchymoses and lacerations.
URGENT INTERVENTIONS
Urgent Endotracheal Intubation In a patient exhibiting stridor, it may be necessary to execute emergency endotracheal intubation to secure a patent airway and facilitate mechanical ventilation. Simply adhere to these fundamental steps: Assemble the requisite apparatus. Elucidate the protocol to the patient. Position the patient supine with a small blanket or pillow beneath his head. This posture aligns the axes of the oropharynx, posterior pharynx, and trachea. Inspect the cuff of the endotracheal tube for any leakage. Post-intubation, inflate the cuff employing the minimal leak approach. Verify tube placement by auscultating for bilateral breath sounds or employing a capnometer; monitor the patient for chest expansion and assess for warm exhalations at the endotracheal tube's entrance. Insert an oral airway or occlusal block. Stabilize the endotracheal tube and airway with an ET tube holder or adhesive tape. Extract secretions from the patient's oral cavity and the endotracheal tube as necessary. Provide oxygen or commence mechanical ventilation (or both). Post-intubation, aspirate secretions as necessary and assess cuff pressure once every shift, rectifying any air leaks using the minimal leak approach. Administer oral hygiene every 2 to 3 hours and as required. Prepare the patient for chest X-rays to verify tube placement, and restrain and reassure him as necessary.
Etiological Factors
Trauma to the airway. Localized trauma to the upper airway frequently leads to acute blockage, resulting in the abrupt emergence of stridor. This symptom is accompanied by dysphonia, dysphagia, hemoptysis, cyanosis, use of accessory muscles, intercostal retractions, nasal flaring, tachypnea, increasing dyspnea, and shallow respirations. Palpation may disclose subcutaneous crepitus in the neck or upper thorax.
Anaphylaxis
A strong allergic reaction can lead to upper airway edema and laryngospasm, resulting in stridor and several indicators of respiratory distress, including nasal flaring, wheezing, use of accessory muscles, intercostal retractions, and dyspnea. The patient may also experience nasal congestion and abundant, watery rhinorrhea. Usually, these respiratory effects are preceded by sensations of impending doom or terror, weakness, diaphoresis, sneezing, nasal itching, hives, erythema, and angioedema. Common related symptoms include chest or throat constriction, dysphagia, and perhaps indicators of shock, such as hypotension, tachycardia, and chilly, clammy skin.
Inhalation anthrax
The initial signs and symptoms resemble influenza and encompass fever, chills, fatigue, cough, and thoracic pain. The condition often manifests in two phases, followed by a recovery interval after the onset of early symptoms. The second stage progresses rapidly, characterized by stridor, fever, dyspnea, and hypotension, typically resulting in death within 24 hours. Radiologic results reveal mediastinitis and symmetrical mediastinal enlargement. Inhalation of an extraneous object. Acute stridor is indicative of foreign-body aspiration, a critical medical emergency. Associated observations encompass a sudden onset of dry, paroxysmal cough; gagging or choking; hoarseness; tachycardia; wheezing; dyspnea; tachypnea; intercostal muscular retractions; reduced breath sounds; cyanosis; and shallow respirations. The patient generally exhibits anxiety and anguish.
Hypocalcemia
Hypocalcemia may lead to laryngospasm, resulting in stridor. Additional results encompass paresthesia, carpopedal spasm, and positive Chvostek's and Trousseau's symptoms. Inhalation trauma. Within 48 hours of inhaling smoke or toxic fumes, the patient may experience laryngeal edema and bronchospasms, leading to stridor. Accompanying signs and symptoms encompass singed nose hairs, orofacial burns, coughing, hoarseness, sooty sputum, crackles, rhonchi, wheezes, and additional indicators of respiratory distress, including dyspnea, utilization of accessory muscles, intercostal retractions, and nasal flaring.
Mediastinal neoplasm
A mediastinal tumor typically presents asymptomatically initially but may later exert pressure on the trachea and bronchi, leading to stridor. Additional consequences encompass hoarseness, a brassy cough, tracheal deviation or tugging, distended neck veins, facial and cervical edema, stertorous breathing, and suprasternal retractions during inhalation. The patient may additionally experience dyspnea, dysphagia, and pain in the chest, shoulder, or arm. Retrosternal thyroid gland. Retrosternal thyroid is an anatomical anomaly that results in stridor, dysphagia, cough, hoarseness, and tracheal deviation. It may also induce manifestations of thyrotoxicosis.
Alternative Etiologies
Diagnostic Assessments. Bronchoscopy or laryngoscopy may induce laryngospasm and stridor.
Therapies
Following extended intubation, the patient may display laryngeal edema and stridor upon extubation. Aerosol treatment utilizing epinephrine may diminish stridor. Reintubation may be required in some instances. Neck surgery, including thyroidectomy, may result in laryngeal paralysis and stridor. Persist in vigilant observation of the patient's vital signs. Prepare him for diagnostic assessments, including arterial blood gas analysis and chest radiographs.
Instruct on the fundamental condition and elucidate all protocols and therapies. Stridor is a significant indicator of airway obstruction in a pediatric patient. Upon hearing this signal, immediate intervention is necessary to avert complete airway obstruction. This emergency can occur more swiftly in a youngster due to a narrower airway compared to that of an adult. Stridor in children can be attributed to foreign-body aspiration, croup syndrome, laryngeal diphtheria, pertussis, retropharyngeal abscess, and congenital laryngeal anomalies. Management of partial airway obstruction generally includes the administration of hot or cold steam within a mist tent or hood, intravenous fluids and electrolytes, along with ample rest.
Stridor is a loud, harsh, musical respiratory sound that arises from a blockage in the trachea or larynx. This indication is often audible during inspiration but may also manifest during expiration in cases of severe upper airway blockage. It may commence as low-pitched "croaking" and advance to high-pitched "crowing" as respiration intensifies. Life-threatening upper airway obstruction may arise from foreign-body aspiration, excessive secretions, an intraluminal tumor, localized edema or muscular spasms, and external compression due to a tumor or aneurysm.
URGENT INTERVENTIONS
Upon hearing stridor, promptly assess the patient's vital signs, particularly oxygen saturation, and evaluate for additional indicators of partial airway obstruction—such as choking or gagging, tachypnea, dyspnea, shallow respirations, intercostal retractions, nasal flaring, tachycardia, cyanosis, and diaphoresis. Be mindful that a sudden cessation of stridor indicates total obstruction, wherein the patient exhibits inspiratory chest movement but lacks breath sounds. Incapable of speech, he rapidly becomes lethargic and loses consciousness.
Upon detecting indications of airway obstruction, attempt to alleviate the obstruction with back blows or abdominal thrusts (Heimlich maneuver). Subsequently, provide oxygen by nasal cannula or face mask, or ready the patient for emergency endotracheal intubation or tracheostomy and mechanical ventilation.
Refer to Emergency Endotracheal Intubation. Prepare equipment for the aspiration of vomitus or blood via the endotracheal or tracheostomy tube. Attach the patient to a cardiac monitor and arrange him in an upright posture to facilitate respiration.
Medical History and Physical Assessment
When the patient's condition allows, acquire a medical history from the patient or a family member. Initially, ascertain the onset of the stridor. Has he previously experienced it? Does he possess an upper respiratory tract infection? How long has he possessed it? Inquire about a history of allergies, neoplasms, and respiratory and vascular conditions. Document recent exposure to smoke or harmful vapors or gasses. Subsequently, investigate related indications and symptoms. Does stridor manifest with discomfort or cough? Subsequently, inspect the patient's oral cavity for excessive secretions, foreign substances, irritation, and edema. Examine his neck for edema, tumors, subcutaneous crepitus, and scars. Examine the patient's chest for delayed, diminished, or uneven expansion. Perform auscultation to detect wheezes, rhonchi, crackles, rubs, and other atypical respiratory sounds. Perform percussion to assess for dullness, tympany, or flatness. Finally, observe for burns or indications of trauma, like ecchymoses and lacerations.
URGENT INTERVENTIONS
Urgent Endotracheal Intubation In a patient exhibiting stridor, it may be necessary to execute emergency endotracheal intubation to secure a patent airway and facilitate mechanical ventilation. Simply adhere to these fundamental steps: Assemble the requisite apparatus. Elucidate the protocol to the patient. Position the patient supine with a small blanket or pillow beneath his head. This posture aligns the axes of the oropharynx, posterior pharynx, and trachea. Inspect the cuff of the endotracheal tube for any leakage. Post-intubation, inflate the cuff employing the minimal leak approach. Verify tube placement by auscultating for bilateral breath sounds or employing a capnometer; monitor the patient for chest expansion and assess for warm exhalations at the endotracheal tube's entrance. Insert an oral airway or occlusal block. Stabilize the endotracheal tube and airway with an ET tube holder or adhesive tape. Extract secretions from the patient's oral cavity and the endotracheal tube as necessary. Provide oxygen or commence mechanical ventilation (or both). Post-intubation, aspirate secretions as necessary and assess cuff pressure once every shift, rectifying any air leaks using the minimal leak approach. Administer oral hygiene every 2 to 3 hours and as required. Prepare the patient for chest X-rays to verify tube placement, and restrain and reassure him as necessary.
Etiological Factors
Trauma to the airway. Localized trauma to the upper airway frequently leads to acute blockage, resulting in the abrupt emergence of stridor. This symptom is accompanied by dysphonia, dysphagia, hemoptysis, cyanosis, use of accessory muscles, intercostal retractions, nasal flaring, tachypnea, increasing dyspnea, and shallow respirations. Palpation may disclose subcutaneous crepitus in the neck or upper thorax.
Anaphylaxis
A strong allergic reaction can lead to upper airway edema and laryngospasm, resulting in stridor and several indicators of respiratory distress, including nasal flaring, wheezing, use of accessory muscles, intercostal retractions, and dyspnea. The patient may also experience nasal congestion and abundant, watery rhinorrhea. Usually, these respiratory effects are preceded by sensations of impending doom or terror, weakness, diaphoresis, sneezing, nasal itching, hives, erythema, and angioedema. Common related symptoms include chest or throat constriction, dysphagia, and perhaps indicators of shock, such as hypotension, tachycardia, and chilly, clammy skin.
Inhalation anthrax
The initial signs and symptoms resemble influenza and encompass fever, chills, fatigue, cough, and thoracic pain. The condition often manifests in two phases, followed by a recovery interval after the onset of early symptoms. The second stage progresses rapidly, characterized by stridor, fever, dyspnea, and hypotension, typically resulting in death within 24 hours. Radiologic results reveal mediastinitis and symmetrical mediastinal enlargement. Inhalation of an extraneous object. Acute stridor is indicative of foreign-body aspiration, a critical medical emergency. Associated observations encompass a sudden onset of dry, paroxysmal cough; gagging or choking; hoarseness; tachycardia; wheezing; dyspnea; tachypnea; intercostal muscular retractions; reduced breath sounds; cyanosis; and shallow respirations. The patient generally exhibits anxiety and anguish.
Hypocalcemia
Hypocalcemia may lead to laryngospasm, resulting in stridor. Additional results encompass paresthesia, carpopedal spasm, and positive Chvostek's and Trousseau's symptoms. Inhalation trauma. Within 48 hours of inhaling smoke or toxic fumes, the patient may experience laryngeal edema and bronchospasms, leading to stridor. Accompanying signs and symptoms encompass singed nose hairs, orofacial burns, coughing, hoarseness, sooty sputum, crackles, rhonchi, wheezes, and additional indicators of respiratory distress, including dyspnea, utilization of accessory muscles, intercostal retractions, and nasal flaring.
Mediastinal neoplasm
A mediastinal tumor typically presents asymptomatically initially but may later exert pressure on the trachea and bronchi, leading to stridor. Additional consequences encompass hoarseness, a brassy cough, tracheal deviation or tugging, distended neck veins, facial and cervical edema, stertorous breathing, and suprasternal retractions during inhalation. The patient may additionally experience dyspnea, dysphagia, and pain in the chest, shoulder, or arm. Retrosternal thyroid gland. Retrosternal thyroid is an anatomical anomaly that results in stridor, dysphagia, cough, hoarseness, and tracheal deviation. It may also induce manifestations of thyrotoxicosis.
Alternative Etiologies
Diagnostic Assessments. Bronchoscopy or laryngoscopy may induce laryngospasm and stridor.
Therapies
Following extended intubation, the patient may display laryngeal edema and stridor upon extubation. Aerosol treatment utilizing epinephrine may diminish stridor. Reintubation may be required in some instances. Neck surgery, including thyroidectomy, may result in laryngeal paralysis and stridor. Persist in vigilant observation of the patient's vital signs. Prepare him for diagnostic assessments, including arterial blood gas analysis and chest radiographs.
Instruct on the fundamental condition and elucidate all protocols and therapies. Stridor is a significant indicator of airway obstruction in a pediatric patient. Upon hearing this signal, immediate intervention is necessary to avert complete airway obstruction. This emergency can occur more swiftly in a youngster due to a narrower airway compared to that of an adult. Stridor in children can be attributed to foreign-body aspiration, croup syndrome, laryngeal diphtheria, pertussis, retropharyngeal abscess, and congenital laryngeal anomalies. Management of partial airway obstruction generally includes the administration of hot or cold steam within a mist tent or hood, intravenous fluids and electrolytes, along with ample rest.

- Published on
Symptoms and Signs – Differential Diagnosis of Splenomegaly
Splenomegaly, or an enlarged spleen, is not a diagnostic indicator in and of itself because it can occur in up to 5% of healthy persons and with a variety of illnesses. However, it typically indicates a hematologic, autoimmune, neoplastic, or hepatic disease, infection, or trauma. Since the spleen is the largest lymph node in the body, any process that causes lymphadenopathy can lead to splenomegaly. It could be a sign of extramedullary hemopoiesis, phagocytic cell proliferation, vascular congestion linked to portal hypertension, reactive hyperplasia (a reaction to infection or inflammation), or neoplastic cell proliferation or infiltration.
TIP FOR EXAMINATION
How to Check for Splenomegaly via Palpating Careful and delicate probing is necessary to detect splenomegaly without rupturing the enlarged spleen. Pay close attention to these steps: Position yourself at the patient's right side while she is in the supine position. To move the spleen forward, place your left hand beneath the left costovertebral angle and provide a slight push. Next, lightly place your right hand beneath the front costal edge on the left. Ask the patient to inhale deeply and then release it. Feel for the edge of the spleen with your right hand when she exhales by moving it along the tissue contours beneath the rib border. When you touch the enlarged spleen, it should feel like a solid lump. Don't forget to start your abdominal palpation low enough to reach the edge of a large spleen. The splenomegaly can be categorized as moderate (1½ to 3″ [4 to 8 cm] below the costal margin), considerable (more than or equal to 3″ [8 cm] below the costal margin), or minor (½ to 1½″ [1 to 4 cm] below the costal margin). To shift the spleen forward, place the patient back on her right side with her hips and knees slightly bent. The palpation process should then be repeated. Light palpation beneath the left costal border can reveal splenomegaly.
However, as this method isn't always recommended or successful, a computed tomography or radionuclide scan would be required to confirm splenomegaly.
Interventions for Emergencies
Avoid palpating the abdomen if the patient has a history of thoracic or abdominal injuries since this could worsen internal bleeding. Instead, look for symptoms of shock, like tachypnea and tachycardia, as well as pain in the left upper quadrant. You should consider splenic rupture if you notice these symptoms. For emergency blood and fluid replacement, establish an intravenous line and give oxygen. Additionally, start cardiac monitoring and catheterize the patient to assess urine output. Get the patient ready for any upcoming procedure. Physical examination and history Start by looking into related symptoms and indicators if splenomegaly is discovered during a standard physical examination. Inquire as to whether the patient has been abnormally exhausted recently. Does he have sore throats, colds, or other diseases often? Is he prone to bruises? Inquire about early satiety, stomach fullness, and pain in the left upper quadrant. Lastly, check for pallor and ecchymoses on the patient's skin and feel for lymphadenopathy in his neck, groin, and axillae.
Medical Reasons
Brucellosis
Splenomegaly is a significant symptom of severe cases of brucellosis, an uncommon infection. Fatigue, headache, backache, anorexia, arthralgia, fever, chills, sweating, and malaise are the typical sneaky symptoms of brucellosis. Hepatomegaly, lymphadenopathy, weight loss, and pressure-induced spinal or peripheral nerve discomfort are possible later symptoms.
Cirrhosis
Moderate to significant splenomegaly develops in about one-third of people with severe cirrhosis. Jaundice, hepatomegaly, leg edema, hematemesis, and ascites are among additional late symptoms. Hepatic encephalopathy symptoms include slurred speech, asterixis, fetor hepaticus, and a lowered state of consciousness that could lead to a coma. Serious pruritus, poor tissue turgor, spider angiomas, palmar erythema, pallor, and indications of bleeding tendencies are possible cutaneous side effects in addition to jaundice. Menstrual abnormalities or testicular atrophy, gynecomastia, and axillary and chest hair loss are examples of endocrine consequences. Additionally, the patient may experience fever and right upper abdomen pain that gets worse when they sit up or lean forward.
Feely's syndrome
Felty's syndrome, which is associated with persistent rheumatoid arthritis, is characterized by splenomegaly. Rheumatoid nodules, palmar erythema, lymphadenopathy, leg ulcers, joint discomfort and deformity, and sensory or motor loss are all associated findings.
Histoplasmosis
Both hepatomegaly and splenomegaly are frequently caused by acute disseminated histoplasmosis. Additionally, it may result in lymphadenopathy, jaundice, fever, anorexia, emaciation, and anemia symptoms like malaise, weakness, exhaustion, and pallor. Pain, hoarseness, and dysphagia can occasionally be caused by ulceration of the patient's tongue, palate, epiglottis, and larynx.
Leukemia
An early indicator of both acute and chronic leukemia is moderate to severe splenomegaly. Splenomegaly in patients with chronic granulocytic leukemia can occasionally be unpleasant. Hepatomegaly, lymphadenopathy, exhaustion, malaise, pallor, fever, gum edema, bleeding disorders, anorexia, weight loss, and discomfort in the bones, joints, and abdomen may accompany it. Acute leukemia can also occasionally result in palpitations, tachycardia, and dyspnea. Confusion, headache, vomiting, seizures, papilledema, and nuchal rigidity are all possible symptoms of severe disease.
infectious mononucleosis
Splenomegaly, a frequent symptom of mononucleosis, is most noticeable in the second and third weeks of the illness. A sore throat, cervical lymphadenopathy, and a fluctuating fever with an evening peak of 101°F to 102°F (38.3°C to 38.9°C) are the three main symptoms that are typically present. Hepatomegaly, jaundice, and a maculopapular rash can also occasionally happen. carcinoma of the pancreas. If the splenic vein is compressed by tumor growth, pancreatic cancer may result in moderate to severe splenomegaly. Back or abdominal discomfort, anorexia, nausea, vomiting, weight loss, gastrointestinal hemorrhage, jaundice, pruritus, skin lesions, emotional instability, weakness, and exhaustion are further distinctive symptoms. Hepatomegaly and a painful abdominal mass may be palpable; auscultation indicates a bruit in the left upper quadrant and periumbilical region.
Vera polycythemia
The spleen may grow significantly in the latter stages of polycythemia vera, causing pleuritic chest discomfort, stomach fullness, and easy satiety. Splenomegaly has several different and common signs and symptoms. The patient may have headache, vertigo, weakness, exhaustion, disorientation, and deep, purplish-red oral mucous membranes. In addition, he might experience tinnitus, hazy or double vision, scotoma, elevated blood pressure, intermittent claudication, finger and toe paresthesia, and impaired mentation. Pruritus, urticaria, reddish cyanosis, epigastric pain, weight loss, hepatomegaly, and bleeding tendencies are other symptoms.
Sarcoidosis
Sarcoidosis is a granulomatous disease that can cause hepatomegaly and splenomegaly, as well as possibly some nebulous stomach pain. A nonproductive cough, dyspnea, malaise, exhaustion, arthralgia, myalgia, weight loss, lymphadenopathy, skin lesions, an irregular pulse, blurred vision, dysphagia, and seizures are some of its further symptoms, which differ depending on the body system that is impacted. rupture of the spleen. Splenomegaly can be caused by a ruptured spleen and significant bleeding. Additionally, the patient may have Kehr's sign, abdominal rigidity, and pain in the left upper quadrant.
Purpura caused by thrombotic thrombocytopenia
Along with fever, pallor, jaundice, vaginal bleeding, hematuria, and splenomegaly and hepatomegaly, thrombotic thrombocytopenic purpura can also cause these symptoms. Additional side effects include arthralgia, headache, pallor, weakness, exhaustion, and abdominal pain. The patient eventually exhibits symptoms of renal failure and neurologic decline.
Get the patient ready for diagnostic procedures such a full blood count, blood cultures, and splenic computed tomography and radionuclide scans. Counseling for Patients Emphasize the value of adhering to medication therapy and teach the patient how to prevent infection.
In addition to the previously mentioned causes, children may develop splenomegaly as a result of sickle cell disease, Gaucher's disease, Niemann-Pick disease, congenital hemolytic anemia, hereditary spherocytosis, sickle cell disease, or beta-thalassemia (Cooley's anemia). The most frequent cause of splenomegaly in children with impaired immune systems is a splenic abscess.
Splenomegaly, or an enlarged spleen, is not a diagnostic indicator in and of itself because it can occur in up to 5% of healthy persons and with a variety of illnesses. However, it typically indicates a hematologic, autoimmune, neoplastic, or hepatic disease, infection, or trauma. Since the spleen is the largest lymph node in the body, any process that causes lymphadenopathy can lead to splenomegaly. It could be a sign of extramedullary hemopoiesis, phagocytic cell proliferation, vascular congestion linked to portal hypertension, reactive hyperplasia (a reaction to infection or inflammation), or neoplastic cell proliferation or infiltration.
TIP FOR EXAMINATION
How to Check for Splenomegaly via Palpating Careful and delicate probing is necessary to detect splenomegaly without rupturing the enlarged spleen. Pay close attention to these steps: Position yourself at the patient's right side while she is in the supine position. To move the spleen forward, place your left hand beneath the left costovertebral angle and provide a slight push. Next, lightly place your right hand beneath the front costal edge on the left. Ask the patient to inhale deeply and then release it. Feel for the edge of the spleen with your right hand when she exhales by moving it along the tissue contours beneath the rib border. When you touch the enlarged spleen, it should feel like a solid lump. Don't forget to start your abdominal palpation low enough to reach the edge of a large spleen. The splenomegaly can be categorized as moderate (1½ to 3″ [4 to 8 cm] below the costal margin), considerable (more than or equal to 3″ [8 cm] below the costal margin), or minor (½ to 1½″ [1 to 4 cm] below the costal margin). To shift the spleen forward, place the patient back on her right side with her hips and knees slightly bent. The palpation process should then be repeated. Light palpation beneath the left costal border can reveal splenomegaly.
However, as this method isn't always recommended or successful, a computed tomography or radionuclide scan would be required to confirm splenomegaly.
Interventions for Emergencies
Avoid palpating the abdomen if the patient has a history of thoracic or abdominal injuries since this could worsen internal bleeding. Instead, look for symptoms of shock, like tachypnea and tachycardia, as well as pain in the left upper quadrant. You should consider splenic rupture if you notice these symptoms. For emergency blood and fluid replacement, establish an intravenous line and give oxygen. Additionally, start cardiac monitoring and catheterize the patient to assess urine output. Get the patient ready for any upcoming procedure. Physical examination and history Start by looking into related symptoms and indicators if splenomegaly is discovered during a standard physical examination. Inquire as to whether the patient has been abnormally exhausted recently. Does he have sore throats, colds, or other diseases often? Is he prone to bruises? Inquire about early satiety, stomach fullness, and pain in the left upper quadrant. Lastly, check for pallor and ecchymoses on the patient's skin and feel for lymphadenopathy in his neck, groin, and axillae.
Medical Reasons
Brucellosis
Splenomegaly is a significant symptom of severe cases of brucellosis, an uncommon infection. Fatigue, headache, backache, anorexia, arthralgia, fever, chills, sweating, and malaise are the typical sneaky symptoms of brucellosis. Hepatomegaly, lymphadenopathy, weight loss, and pressure-induced spinal or peripheral nerve discomfort are possible later symptoms.
Cirrhosis
Moderate to significant splenomegaly develops in about one-third of people with severe cirrhosis. Jaundice, hepatomegaly, leg edema, hematemesis, and ascites are among additional late symptoms. Hepatic encephalopathy symptoms include slurred speech, asterixis, fetor hepaticus, and a lowered state of consciousness that could lead to a coma. Serious pruritus, poor tissue turgor, spider angiomas, palmar erythema, pallor, and indications of bleeding tendencies are possible cutaneous side effects in addition to jaundice. Menstrual abnormalities or testicular atrophy, gynecomastia, and axillary and chest hair loss are examples of endocrine consequences. Additionally, the patient may experience fever and right upper abdomen pain that gets worse when they sit up or lean forward.
Feely's syndrome
Felty's syndrome, which is associated with persistent rheumatoid arthritis, is characterized by splenomegaly. Rheumatoid nodules, palmar erythema, lymphadenopathy, leg ulcers, joint discomfort and deformity, and sensory or motor loss are all associated findings.
Histoplasmosis
Both hepatomegaly and splenomegaly are frequently caused by acute disseminated histoplasmosis. Additionally, it may result in lymphadenopathy, jaundice, fever, anorexia, emaciation, and anemia symptoms like malaise, weakness, exhaustion, and pallor. Pain, hoarseness, and dysphagia can occasionally be caused by ulceration of the patient's tongue, palate, epiglottis, and larynx.
Leukemia
An early indicator of both acute and chronic leukemia is moderate to severe splenomegaly. Splenomegaly in patients with chronic granulocytic leukemia can occasionally be unpleasant. Hepatomegaly, lymphadenopathy, exhaustion, malaise, pallor, fever, gum edema, bleeding disorders, anorexia, weight loss, and discomfort in the bones, joints, and abdomen may accompany it. Acute leukemia can also occasionally result in palpitations, tachycardia, and dyspnea. Confusion, headache, vomiting, seizures, papilledema, and nuchal rigidity are all possible symptoms of severe disease.
infectious mononucleosis
Splenomegaly, a frequent symptom of mononucleosis, is most noticeable in the second and third weeks of the illness. A sore throat, cervical lymphadenopathy, and a fluctuating fever with an evening peak of 101°F to 102°F (38.3°C to 38.9°C) are the three main symptoms that are typically present. Hepatomegaly, jaundice, and a maculopapular rash can also occasionally happen. carcinoma of the pancreas. If the splenic vein is compressed by tumor growth, pancreatic cancer may result in moderate to severe splenomegaly. Back or abdominal discomfort, anorexia, nausea, vomiting, weight loss, gastrointestinal hemorrhage, jaundice, pruritus, skin lesions, emotional instability, weakness, and exhaustion are further distinctive symptoms. Hepatomegaly and a painful abdominal mass may be palpable; auscultation indicates a bruit in the left upper quadrant and periumbilical region.
Vera polycythemia
The spleen may grow significantly in the latter stages of polycythemia vera, causing pleuritic chest discomfort, stomach fullness, and easy satiety. Splenomegaly has several different and common signs and symptoms. The patient may have headache, vertigo, weakness, exhaustion, disorientation, and deep, purplish-red oral mucous membranes. In addition, he might experience tinnitus, hazy or double vision, scotoma, elevated blood pressure, intermittent claudication, finger and toe paresthesia, and impaired mentation. Pruritus, urticaria, reddish cyanosis, epigastric pain, weight loss, hepatomegaly, and bleeding tendencies are other symptoms.
Sarcoidosis
Sarcoidosis is a granulomatous disease that can cause hepatomegaly and splenomegaly, as well as possibly some nebulous stomach pain. A nonproductive cough, dyspnea, malaise, exhaustion, arthralgia, myalgia, weight loss, lymphadenopathy, skin lesions, an irregular pulse, blurred vision, dysphagia, and seizures are some of its further symptoms, which differ depending on the body system that is impacted. rupture of the spleen. Splenomegaly can be caused by a ruptured spleen and significant bleeding. Additionally, the patient may have Kehr's sign, abdominal rigidity, and pain in the left upper quadrant.
Purpura caused by thrombotic thrombocytopenia
Along with fever, pallor, jaundice, vaginal bleeding, hematuria, and splenomegaly and hepatomegaly, thrombotic thrombocytopenic purpura can also cause these symptoms. Additional side effects include arthralgia, headache, pallor, weakness, exhaustion, and abdominal pain. The patient eventually exhibits symptoms of renal failure and neurologic decline.
Get the patient ready for diagnostic procedures such a full blood count, blood cultures, and splenic computed tomography and radionuclide scans. Counseling for Patients Emphasize the value of adhering to medication therapy and teach the patient how to prevent infection.
In addition to the previously mentioned causes, children may develop splenomegaly as a result of sickle cell disease, Gaucher's disease, Niemann-Pick disease, congenital hemolytic anemia, hereditary spherocytosis, sickle cell disease, or beta-thalassemia (Cooley's anemia). The most frequent cause of splenomegaly in children with impaired immune systems is a splenic abscess.

- Published on
Symptoms and Signs – Differential Diagnosis of Complex Partial Seizures
A complex partial seizure transpires when a focal seizure originates in the temporal lobe, resulting in a partial disturbance of consciousness, typically manifested as bewilderment. Psychomotor seizures may manifest at any age, though their prevalence often escalates between adolescence and adulthood. Sixty-six percent of patients also experience generalized seizures. An aura, often a multifaceted hallucination, illusion, or sensation, generally accompanies a psychomotor seizure.
The hallucination may be audiovisual (pictures accompanied by noises), auditory (abnormal or familiar sounds or voices from the patient's past), or olfactory (unpleasant odors, such as decaying eggs or burning substances). Additional forms of auras encompass sensations of déjà vu, unfamiliarity with one's environment, or depersonalization. The patient may exhibit dread or anxiety, demonstrate lip smacking, or suffer discomfort in the epigastric area that ascends toward the chest and throat. The patient typically identifies the aura and reclines prior to losing consciousness. An interval of unresponsiveness ensues after the aura. The patient may exhibit automatisms, appear disoriented and walk without purpose, engage in improper behaviors (such as public undressing), display unresponsiveness, articulate incomprehensible statements, or (infrequently) exhibit fury or tantrums. Post-seizure, the patient exhibits confusion and drowsiness, lacking recollection of the event. Behavioral automatisms often do not exceed 5 minutes; nevertheless, postictal disorientation, agitation, and amnesia may last. During intervals between episodes, the patient may display sluggish and inflexible cognition, episodes of rage and aggression, monotonous dialogue, an obsession with simplistic philosophical concepts, reduced sexual desire, emotional fluctuations, and paranoid inclinations. Chronicle Do not attempt to restrain the patient if you observe a complex partial seizure. Instead, guide him softly to a secure location. Do not approach him if he is furious or violent. Gently prompt him to take a seat and stay with him until he is completely alert. Inquire whether he experienced an aura subsequent to the seizure. Document all observations and findings.
Etiological Factors in Medicine
Cerebral abscess. Complex partial seizures frequently manifest following the resolution of a brain abscess located in the temporal lobe. Associated issues may encompass cephalalgia, nausea, emesis, generalized seizures, and a diminished degree of consciousness (LOC). The patient may additionally exhibit central facial paralysis, auditory receptive aphasia, hemiparesis, and ocular abnormalities.
Cranial injury
Significant trauma to the temporal lobe, particularly from a penetrating injury, may result in complicated partial seizures occurring months or years subsequently. The seizures may diminish in frequency and ultimately cease. Head trauma also induces widespread seizures as well as alterations in behavior and personality.
Herpes simplex encephalitis
The herpes simplex virus frequently targets the temporal lobe, leading to complicated partial seizures. Additional symptoms encompass fever, headache, coma, and generalized seizures.
Neoplasm of the temporal lobe
Complex partial seizures may indicate the initial manifestation of a temporal lobe tumor. Additional indications and symptoms encompass cephalalgia, alterations in pupillary response, and cognitive lethargy. Elevated intracranial pressure may result in diminished level of consciousness, emesis, and potentially, papilledema.
Post-seizure, stay with the patient to reorient him to his environment and safeguard him from harm. Maintain him in bed until he is completely alert, and eliminate hazardous objects from the vicinity. Provide emotional support to the patient and their family, and instruct them on coping strategies for seizures. Prepare the patient for diagnostic procedures, including electroencephalography, computed tomography scans, or magnetic resonance imaging. Patient Consultation Educate the patient and their family on safety protocols to implement during a seizure, and elucidate the significance of possessing medical identification. Examine strategies for managing seizures, with a focus on adherence to pharmacological treatment.
Complex partial seizures in children may mimic absence seizures. They may arise from birth trauma, maltreatment, infection, or neoplasia. In around one-third of patients, the etiology remains unidentified. Frequent complex partial seizures sometimes result in generalized seizures. The youngster may encounter a subtle aura, which is seldom as distinctly characterized as that observed in generalized tonic.-clonic seizures
A complex partial seizure transpires when a focal seizure originates in the temporal lobe, resulting in a partial disturbance of consciousness, typically manifested as bewilderment. Psychomotor seizures may manifest at any age, though their prevalence often escalates between adolescence and adulthood. Sixty-six percent of patients also experience generalized seizures. An aura, often a multifaceted hallucination, illusion, or sensation, generally accompanies a psychomotor seizure.
The hallucination may be audiovisual (pictures accompanied by noises), auditory (abnormal or familiar sounds or voices from the patient's past), or olfactory (unpleasant odors, such as decaying eggs or burning substances). Additional forms of auras encompass sensations of déjà vu, unfamiliarity with one's environment, or depersonalization. The patient may exhibit dread or anxiety, demonstrate lip smacking, or suffer discomfort in the epigastric area that ascends toward the chest and throat. The patient typically identifies the aura and reclines prior to losing consciousness. An interval of unresponsiveness ensues after the aura. The patient may exhibit automatisms, appear disoriented and walk without purpose, engage in improper behaviors (such as public undressing), display unresponsiveness, articulate incomprehensible statements, or (infrequently) exhibit fury or tantrums. Post-seizure, the patient exhibits confusion and drowsiness, lacking recollection of the event. Behavioral automatisms often do not exceed 5 minutes; nevertheless, postictal disorientation, agitation, and amnesia may last. During intervals between episodes, the patient may display sluggish and inflexible cognition, episodes of rage and aggression, monotonous dialogue, an obsession with simplistic philosophical concepts, reduced sexual desire, emotional fluctuations, and paranoid inclinations. Chronicle Do not attempt to restrain the patient if you observe a complex partial seizure. Instead, guide him softly to a secure location. Do not approach him if he is furious or violent. Gently prompt him to take a seat and stay with him until he is completely alert. Inquire whether he experienced an aura subsequent to the seizure. Document all observations and findings.
Etiological Factors in Medicine
Cerebral abscess. Complex partial seizures frequently manifest following the resolution of a brain abscess located in the temporal lobe. Associated issues may encompass cephalalgia, nausea, emesis, generalized seizures, and a diminished degree of consciousness (LOC). The patient may additionally exhibit central facial paralysis, auditory receptive aphasia, hemiparesis, and ocular abnormalities.
Cranial injury
Significant trauma to the temporal lobe, particularly from a penetrating injury, may result in complicated partial seizures occurring months or years subsequently. The seizures may diminish in frequency and ultimately cease. Head trauma also induces widespread seizures as well as alterations in behavior and personality.
Herpes simplex encephalitis
The herpes simplex virus frequently targets the temporal lobe, leading to complicated partial seizures. Additional symptoms encompass fever, headache, coma, and generalized seizures.
Neoplasm of the temporal lobe
Complex partial seizures may indicate the initial manifestation of a temporal lobe tumor. Additional indications and symptoms encompass cephalalgia, alterations in pupillary response, and cognitive lethargy. Elevated intracranial pressure may result in diminished level of consciousness, emesis, and potentially, papilledema.
Post-seizure, stay with the patient to reorient him to his environment and safeguard him from harm. Maintain him in bed until he is completely alert, and eliminate hazardous objects from the vicinity. Provide emotional support to the patient and their family, and instruct them on coping strategies for seizures. Prepare the patient for diagnostic procedures, including electroencephalography, computed tomography scans, or magnetic resonance imaging. Patient Consultation Educate the patient and their family on safety protocols to implement during a seizure, and elucidate the significance of possessing medical identification. Examine strategies for managing seizures, with a focus on adherence to pharmacological treatment.
Complex partial seizures in children may mimic absence seizures. They may arise from birth trauma, maltreatment, infection, or neoplasia. In around one-third of patients, the etiology remains unidentified. Frequent complex partial seizures sometimes result in generalized seizures. The youngster may encounter a subtle aura, which is seldom as distinctly characterized as that observed in generalized tonic.-clonic seizures

- Published on
Symptoms and Signs - Differential Diagnosis of Generalized Tonic-Clonic Seizures
Similar to other seizure types, generalized tonic-clonic seizures are induced by the paroxysmal, unregulated discharge of central nervous system neurons, resulting resulting in neurological impairment. In contrast to the majority of seizure types, this cerebral hyperactivity is not restricted to the initial focus or a specific region but encompasses the entire brain. A generalized tonic-clonic seizure may commence with or without an aura. Since Seizure activity disseminates to the subcortical structures, resulting in the patient's loss consciousness, collapses, and may emit a loud cry triggered by the influx of air From the lungs via the voice cords. His body becomes rigid (tonic phase), and thereafter experiences fast, synchronized muscular contractions and hyperventilation (clonic) phase). Tongue biting, incontinence, diaphoresis, excessive salivation, and indications of Respiratory distress may also manifest. The seizure typically ceases after 2 to 5 minutes. minutes.
The patient subsequently regains consciousness but exhibits perplexity. He might Report experiencing cephalalgia, lethargy, myalgia, and weakness in the extremities. Generalized tonic-clonic seizures typically manifest individually. The patient could potentially be either in a state of slumber or in a state of alertness and activity.
Observe the Events Occurring During a Generalized Tonic- Clonic seizure. Potential complications encompass respiratory arrest resulting from airway obstruction. blockage due to secretions, status epilepticus (occurring in 5% to 8% of cases) patients), cranial or spinal traumas and contusions, Todd's paralysis, and, infrequently, cardiac arrest. Status epilepticus, which poses a life-threatening risk, is characterized by extended seizures. activity or by swiftly repeating seizures without intervening recovery intervals. It is most frequently induced by the sudden cessation of anticonvulsants. psychotherapy. Generalized seizures may be induced by a brain tumor, vascular disease, or head trauma. trauma, infection, metabolic disorder, substance withdrawal syndrome. exposure to chemicals or a genetic anomaly. Generalized seizures may also arise from a focused seizure. The etiology of recurrent seizures, or epilepsy, may be indeterminate.
URGENT INTERVENTIONS
Upon observing the onset of the seizure, first assess the patient's airway. assess respiration and circulation, ensuring that the cause is neither asystole or a obstructed airway. Remain with the patient and guarantee an unobstructed airway. Concentration Your vigilance in monitoring the seizure and safeguarding the patient. Position a towel place under his head to avert damage, loosen his garments, and remove any sharp objects or obstacles from his path. Do not attempt to confine the sufferer or compel a Inserting a hard object into his mouth may result in chipped teeth or a fractured jaw. Insertion of a soft item is permissible solely during the onset of the ictal phase. oral cavity. If feasible, position the patient laterally during the seizure to facilitate Drain secretions to avert aspiration. Alternatively, execute this at the conclusion. during the clonic phase when respiration resumes. If they do not return, verify Address airway blockage and perform suction on the patient if required. Cardiopulmonary resuscitation, intubation, and mechanical ventilation may be necessary. Ensure the patient’s safety post-seizure by creating a secure environment. where he can repose.
Upon his awakening, provide reassurance and reorientation. Examine his Physiological indicators and neurological condition. Ensure meticulous documentation of this data Describe your observations during the convulsion. Should the seizure last beyond four minutes or if a further seizure transpires Prior to complete recovery from the initial episode, suspect status epilepticus. Formulate an Establish airway and initiate intravenous access. administer supplementary oxygen and initiate cardiac Surveillance.
Collect blood for relevant analyses. Position the patient on his laterally, with his head in a semi-dependent posture, to facilitate the drainage of secretions and Mitigate ambition. Occasionally reposition him to the alternate side, assess his Assess arterial blood gas levels for hypoxemia and provide oxygen via mask. augmenting the flow rate if required. Administer diazepam or lorazepam via delayed intravenous administration administer a push, repeated two or three times at intervals of 10 to 20 minutes, to Cease the seizures. If the patient is not known to have epilepsy, an intravenous (I.V.) administration is indicated.
administration of a bolus Dextrose 50% (50 mL) plus thiamine (100 mg) may be prescribed. Dextrose May terminate the seizures if the patient is experiencing hypoglycemia. If his thiamine concentration Administer thiamine to mitigate the risk of further harm due to low levels. If the patient is intubated, anticipate the insertion of a nasogastric (NG) tube to Inhibit emesis and aspiration. Note that if the patient has not been The nasogastric tube can induce the gag reflex and result in vomiting when intubated. Ensure the documentation of your observations and the intervals between seizures
. What Occurs During a Generalized Tonic-Clonic Seizure Pre-Seizure Prodromal signs and symptoms, include myoclonic jerks and a pulsating sensation Headaches and mood alterations may manifest over the course of many hours or days. The The patient may have premonitory sensations prior to the seizure. For instance, he might convey an aura, exemplified by the perception of a flashing light or the detection of a distinctive odor.
DURING THE EPILEPTIC EVENT
the onset of a generalized seizure is preceded by an aura. Irritability in a certain region of the brain rapidly disseminated. Common auras encompass palpitations and epigastric discomfort that escalates swiftly to the Throat, cephalic or ocular rotation, and sensory hallucinations. Subsequently, loss of consciousness transpires due to an abrupt discharge of intense The electrical activity surpasses the brain's subcortical center. The individual receiving medical care experiences falls accompanied by transient, bilateral myoclonic contractions. Compressed air Spasmodic vocal chords may provide a birdlike, piercing shriek. In the tonic phase, skeletal muscles contract for a duration of 10 to 20 seconds. The patient's eyes are retracted, his arms are flexed, and his legs are prolonged. His mouth opens broadly, then closes abruptly; he risks biting his tongue. His breathing halts due to a spasm of the respiratory muscles, and initial pallor of the integument and mucous membranes (consequent to compromised venous) Return of cyanosis due to apnea. The patient flexes his spine. He gradually descends his arms (as illustrated below). Additional effects encompass dilation. nonreactive pupils, significantly elevated heart rate and blood pressure, increased salivation and tracheobronchial secretions, and copious excessive sweating. In the clonic phase, which endures approximately 60 seconds, there is slight tremoring. advances to severe contractions or spasms. Additional motor activity include facial contortions (perhaps accompanied by tongue biting) and forceful exhalation of Hemorrhagic, frothy saliva resulting from clonic contractions of the thoracic cage muscles. Clonic jerks gradually diminish in intensity and frequency. The patient remains stationary. Apneic.
SUBSEQUENT TO THE SEIZURE
The patient's motions progressively halt, rendering him unresponsive. to environmental stimuli. Additional postictal characteristics encompass stertorous breathing. respirations resulting from augmented tracheobronchial secretions, whether equal or unequal pupils (albeit increasingly reactive) and urine incontinence resulting from short muscular relaxation. After approximately five minutes, the patient's level of Consciousness elevates, resulting in confusion and disorientation. His Muscle tone, heart rate, and blood pressure normalize. Following several hours of sleep, the patient awakens fatigued and may experience headache, myalgia, and forgetfulness regarding the seizure.
Medical History and Physical Assessment
If you did not observe the seizure, acquire a description from the patient. associate. Inquire about the onset of the seizure and its duration. Was the patient Document atypical sensations prior to the onset of the seizure. Did the seizure originate in one Did it initially affect a certain section of the body and subsequently spread, or did it impact the entire body immediately? Was the Did the patient fall upon a hard surface? Did his eyes or head rotate? Did he become cyanotic? Did Does he experience loss of bladder control? Did he experience other seizures before to recovery? If the patient may have incurred a brain injury, monitor him cautiously for any loss. Altered consciousness, asymmetrical or nonresponsive pupils, and localized neurological deficits. Does he report experiencing a headache and myalgia? Is he becoming progressively Is it challenging to awaken him when you check on him at 20-minute intervals? Analyze his arms, legs, and face (including tongue) for trauma, residual paralysis, or limb impairment vulnerability. Subsequently, acquire a history. Has the patient ever experienced widespread or focal seizures? prior? Do they occur with regularity? Do other relatives also possess Whom? Is the patient undergoing pharmacological treatment? Is he obedient? Additionally, inquire about sleep deprivation and mental or physical stress during the seizure transpired.
Etiological Factors
Intracranial abscess
Generalized seizures may manifest during the acute phase of an abscess. creation or subsequent to the resolution of the abscess. Contingent upon the magnitude and The location of the abscess and the degree of altered awareness (LOC) fluctuate. from lethargy to profound stupor. Initial indications and manifestations indicate heightened Intracranial pressure (ICP) manifests as a persistent headache and nausea.
Emesis and focal convulsions
Subsequent characteristics often encompass ocular Disruptions, including nystagmus, compromised vision, and asymmetrical pupils. Additional findings differ based on the abscess location but may encompass aphasia. Hemiparesis, atypical conduct, and alterations in personality. Neoplasm of the brain. Generalized seizures may manifest, contingent upon the tumor's Geographical position and classification. Additional studies indicate a gradual decline in level of consciousness. Morning headache, dizziness, disorientation, focal seizures, visual impairment, motor dysfunction and sensory impairments, aphasia, and ataxia. Subsequent discoveries encompass papilledema, emesis, elevated systolic blood pressure, widened pulse pressure pressure and, ultimately, a decorticate posture.
Chronic kidney failure
End-stage renal failure results in the swift emergence of Involuntary muscle contractions, tremors, myoclonic jerks, and generalized seizures. Connected Signs and symptoms encompass anuria or oliguria, weariness, malaise, and irritability. reduced cognitive sharpness, muscular spasms, peripheral nerve disorders, loss of appetite, and constipation or diarrhea. The integumentary consequences encompass skin pigmentation. Color alterations (yellow, brown, or bronze), itching, and uremic frost. Additional effects characterized by an ammonia-like breath odor, nausea and vomiting, and ecchymoses. petechiae, gastrointestinal hemorrhage, oral and gingival ulcers, hypertension, and Kussmaul respirations.
Eclampsia
Generalized seizures are a defining characteristic of eclampsia. Connected Findings encompass a severe frontal headache, nausea, vomiting, and visual disturbances. disruptions, elevated blood pressure, a temperature reaching 104°F (40°C), peripheral edema and abrupt weight increase. The patient may additionally demonstrate oliguria, irritability, and hyperactive deep tendon reflexes (DTRs) reduced level of consciousness.
Encephalitis
Seizures are an initial indication of encephalitis, signifying a negative prognosis. Prognosis; they may also manifest post-recovery due to lingering effects. harm. Additional observations encompass fever, headache, photophobia, and nuchal rigidity. stiffness, cervical discomfort, emesis, language impairment, lack of coordination, unilateral weakness, involuntary eye movement, irritability, cranial nerve palsies (resulting in facial paralysis, ptosis, dysphagia and myoclonic jerks.
Idiopathic epilepsy
The etiology of repeated seizures is, in the majority of instances, Unidentified. Cerebral injury. In extreme instances, generalized seizures may manifest together. pertaining to harm. Severe head trauma may result in focal seizures months later. may also result in diminished level of consciousness, potentially leading to coma; facial soft tissue injuries, cranial or cervical region; transparent or sanguineous exudate from the oral cavity, nasal passages, or auditory canals; face edema; osseous malformation of the face, cranium, or cervical region; Battle's sign; and an absence Response to oculocephalic and oculovestibular stimuli. Motor and Sensory impairments may accompany changed respirations. Assessment may indicate indicators of elevated intracranial pressure, such as a diminished reaction to painful stimuli stimuli, nonresponsive pupils, bradycardia, elevated systolic pressure, and increasing pulse pressure. If the patient is alert, he may display visual impairments, alterations in behavior, and cephalalgia.
Hepatic encephalopathy
Generalized seizures may manifest in advanced hepatic conditions. Encephalopathy. Related late-stage observations in the comatose patient With fetor hepaticus, asterixis, hyperactive deep tendon reflexes, and a positive Babinski's reflex.
Hypoglycemia
Generalized seizures typically manifest with intensity. Hypoglycemia, accompanied by visual disturbances such as blurred or double vision, and muscle weakness. hemiplegia, tremors, profuse sweating, tachycardia, myoclonic jerks Myoclonic jerking and diminished level of consciousness.
Hyponatremia
Seizures occur when serum sodium levels decline beneath 125. mEq/L, particularly if the reduction is abrupt. Hyponatremia furthermore induces orthostatic hypotension, cephalalgia, myoclonus, and muscular weakness, exhaustion, oliguria or anuria, cool and moist skin, diminished skin turgor, irritability, lethargy, confusion, and stupor or coma. Polydipsia, Tachycardia, nausea, vomiting, and abdominal cramps may also manifest. Severe hyponatremia can result in cyanosis and vasomotor collapse, accompanied by a Weak pulse.
Hypoparathyroidism
Progressive tetany induces generalized seizures. Chronic hypoparathyroidism induces neuromuscular excitability and exaggerated deep tendon reflexes. Hypoxic encephalopathy. In addition to generalized seizures, hypoxia Encephalopathy may induce myoclonic jerks and coma. Subsequently, if the The patient has recovered from dementia, visual agnosia, choreoathetosis, and ataxia. may transpire.
Neurofibromatosis
Neurofibromatosis induces several cerebral lesions. Focal and generalized seizures. Examination uncovers café-au-lait macules, Numerous cutaneous neoplasms, scoliosis, and kyphoscoliosis. Associated discoveries Symptoms encompass dizziness, ataxia, monocular blindness, and nystagmus. Cerebrovascular accident. Seizures, predominantly localized rather than generalized, may occur inside Six months post-ischemic stroke. Accompanying signs and symptoms differ according on The site and severity of cerebral injury. They encompass a diminished level of consciousness. contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory deficits loss, apraxia, agnosia, and aphasia. The patient may also experience visual disturbances. impairments, cognitive impairment, impaired judgment, alterations in personality, emotional disturbances lability, urinary retention or incontinence, constipation, headache, and emesis.
Alternative Causes
Arsenic toxicity. In addition to widespread seizures, arsenic poisoning may induce a garlicky breath odor, heightened salivation, and widespread pruritus. Gastrointestinal consequences including diarrhea, nausea, vomiting, and intense stomach discomfort. Associated consequences encompass widespread hyperpigmentation and strongly delineated edema. eyelid, facial, and ankle edema; extremity paresthesia; baldness; inflamed mucous membranes; fatigue; myalgia; and peripheral Neuropathy. Withdrawal from barbiturates. In patients with persistent intoxication, barbiturate Withdrawal may induce generalized seizures 2 to 4 days following the final dose. Status epilepticus may occur.
Diagnostic assessments
Contrast chemicals utilized in radiologic examinations may induce generalized seizures. Pharmaceutical substances. Toxic concentrations of several medications, including theophylline and lidocaine, Meperidine, penicillins, and cimetidine may induce generalized seizures. Phenothiazines, tricyclic antidepressants, amphetamines, isoniazid, and Vincristine may induce seizures in persons with preexisting epilepsy.
Carefully observe the patient post-seizure for any recurrence of seizure activity. Prepare him for a computed tomography scan or magnetic resonance imaging. and electroencephalogram.
Instruct the patient's family on how to monitor and document seizure occurrences, and Elucidate the rationale for undertaking such actions. Highlight the significance of adherence to pharmacological treatment and monitoring, and elucidate potential harmful effects of prescription medications Instruct the patient to consistently possess medical identification.
Generalized seizures frequently occur in pediatric populations. Indeed, between 75% and 90% of Individuals with epilepsy typically encounter their initial seizure prior to the age of 20. A multitude of children Generalized seizures occur between the ages of 3 months and 3 years. Accompanied with a temperature; some of these youngsters subsequently experience seizures in the absence of fever. Generalized seizures may also arise from congenital metabolic disorders and prenatal factors. trauma, cerebral infection, Reye's syndrome, Sturge-Weber syndrome, arteriovenous malformation Malformation, lead toxicity, hypoglycemia, and idiopathic origins. The the pertussis component of the DPT vaccine may induce seizures; however, this is uncommon.
Similar to other seizure types, generalized tonic-clonic seizures are induced by the paroxysmal, unregulated discharge of central nervous system neurons, resulting resulting in neurological impairment. In contrast to the majority of seizure types, this cerebral hyperactivity is not restricted to the initial focus or a specific region but encompasses the entire brain. A generalized tonic-clonic seizure may commence with or without an aura. Since Seizure activity disseminates to the subcortical structures, resulting in the patient's loss consciousness, collapses, and may emit a loud cry triggered by the influx of air From the lungs via the voice cords. His body becomes rigid (tonic phase), and thereafter experiences fast, synchronized muscular contractions and hyperventilation (clonic) phase). Tongue biting, incontinence, diaphoresis, excessive salivation, and indications of Respiratory distress may also manifest. The seizure typically ceases after 2 to 5 minutes. minutes.
The patient subsequently regains consciousness but exhibits perplexity. He might Report experiencing cephalalgia, lethargy, myalgia, and weakness in the extremities. Generalized tonic-clonic seizures typically manifest individually. The patient could potentially be either in a state of slumber or in a state of alertness and activity.
Observe the Events Occurring During a Generalized Tonic- Clonic seizure. Potential complications encompass respiratory arrest resulting from airway obstruction. blockage due to secretions, status epilepticus (occurring in 5% to 8% of cases) patients), cranial or spinal traumas and contusions, Todd's paralysis, and, infrequently, cardiac arrest. Status epilepticus, which poses a life-threatening risk, is characterized by extended seizures. activity or by swiftly repeating seizures without intervening recovery intervals. It is most frequently induced by the sudden cessation of anticonvulsants. psychotherapy. Generalized seizures may be induced by a brain tumor, vascular disease, or head trauma. trauma, infection, metabolic disorder, substance withdrawal syndrome. exposure to chemicals or a genetic anomaly. Generalized seizures may also arise from a focused seizure. The etiology of recurrent seizures, or epilepsy, may be indeterminate.
URGENT INTERVENTIONS
Upon observing the onset of the seizure, first assess the patient's airway. assess respiration and circulation, ensuring that the cause is neither asystole or a obstructed airway. Remain with the patient and guarantee an unobstructed airway. Concentration Your vigilance in monitoring the seizure and safeguarding the patient. Position a towel place under his head to avert damage, loosen his garments, and remove any sharp objects or obstacles from his path. Do not attempt to confine the sufferer or compel a Inserting a hard object into his mouth may result in chipped teeth or a fractured jaw. Insertion of a soft item is permissible solely during the onset of the ictal phase. oral cavity. If feasible, position the patient laterally during the seizure to facilitate Drain secretions to avert aspiration. Alternatively, execute this at the conclusion. during the clonic phase when respiration resumes. If they do not return, verify Address airway blockage and perform suction on the patient if required. Cardiopulmonary resuscitation, intubation, and mechanical ventilation may be necessary. Ensure the patient’s safety post-seizure by creating a secure environment. where he can repose.
Upon his awakening, provide reassurance and reorientation. Examine his Physiological indicators and neurological condition. Ensure meticulous documentation of this data Describe your observations during the convulsion. Should the seizure last beyond four minutes or if a further seizure transpires Prior to complete recovery from the initial episode, suspect status epilepticus. Formulate an Establish airway and initiate intravenous access. administer supplementary oxygen and initiate cardiac Surveillance.
Collect blood for relevant analyses. Position the patient on his laterally, with his head in a semi-dependent posture, to facilitate the drainage of secretions and Mitigate ambition. Occasionally reposition him to the alternate side, assess his Assess arterial blood gas levels for hypoxemia and provide oxygen via mask. augmenting the flow rate if required. Administer diazepam or lorazepam via delayed intravenous administration administer a push, repeated two or three times at intervals of 10 to 20 minutes, to Cease the seizures. If the patient is not known to have epilepsy, an intravenous (I.V.) administration is indicated.
administration of a bolus Dextrose 50% (50 mL) plus thiamine (100 mg) may be prescribed. Dextrose May terminate the seizures if the patient is experiencing hypoglycemia. If his thiamine concentration Administer thiamine to mitigate the risk of further harm due to low levels. If the patient is intubated, anticipate the insertion of a nasogastric (NG) tube to Inhibit emesis and aspiration. Note that if the patient has not been The nasogastric tube can induce the gag reflex and result in vomiting when intubated. Ensure the documentation of your observations and the intervals between seizures
. What Occurs During a Generalized Tonic-Clonic Seizure Pre-Seizure Prodromal signs and symptoms, include myoclonic jerks and a pulsating sensation Headaches and mood alterations may manifest over the course of many hours or days. The The patient may have premonitory sensations prior to the seizure. For instance, he might convey an aura, exemplified by the perception of a flashing light or the detection of a distinctive odor.
DURING THE EPILEPTIC EVENT
the onset of a generalized seizure is preceded by an aura. Irritability in a certain region of the brain rapidly disseminated. Common auras encompass palpitations and epigastric discomfort that escalates swiftly to the Throat, cephalic or ocular rotation, and sensory hallucinations. Subsequently, loss of consciousness transpires due to an abrupt discharge of intense The electrical activity surpasses the brain's subcortical center. The individual receiving medical care experiences falls accompanied by transient, bilateral myoclonic contractions. Compressed air Spasmodic vocal chords may provide a birdlike, piercing shriek. In the tonic phase, skeletal muscles contract for a duration of 10 to 20 seconds. The patient's eyes are retracted, his arms are flexed, and his legs are prolonged. His mouth opens broadly, then closes abruptly; he risks biting his tongue. His breathing halts due to a spasm of the respiratory muscles, and initial pallor of the integument and mucous membranes (consequent to compromised venous) Return of cyanosis due to apnea. The patient flexes his spine. He gradually descends his arms (as illustrated below). Additional effects encompass dilation. nonreactive pupils, significantly elevated heart rate and blood pressure, increased salivation and tracheobronchial secretions, and copious excessive sweating. In the clonic phase, which endures approximately 60 seconds, there is slight tremoring. advances to severe contractions or spasms. Additional motor activity include facial contortions (perhaps accompanied by tongue biting) and forceful exhalation of Hemorrhagic, frothy saliva resulting from clonic contractions of the thoracic cage muscles. Clonic jerks gradually diminish in intensity and frequency. The patient remains stationary. Apneic.
SUBSEQUENT TO THE SEIZURE
The patient's motions progressively halt, rendering him unresponsive. to environmental stimuli. Additional postictal characteristics encompass stertorous breathing. respirations resulting from augmented tracheobronchial secretions, whether equal or unequal pupils (albeit increasingly reactive) and urine incontinence resulting from short muscular relaxation. After approximately five minutes, the patient's level of Consciousness elevates, resulting in confusion and disorientation. His Muscle tone, heart rate, and blood pressure normalize. Following several hours of sleep, the patient awakens fatigued and may experience headache, myalgia, and forgetfulness regarding the seizure.
Medical History and Physical Assessment
If you did not observe the seizure, acquire a description from the patient. associate. Inquire about the onset of the seizure and its duration. Was the patient Document atypical sensations prior to the onset of the seizure. Did the seizure originate in one Did it initially affect a certain section of the body and subsequently spread, or did it impact the entire body immediately? Was the Did the patient fall upon a hard surface? Did his eyes or head rotate? Did he become cyanotic? Did Does he experience loss of bladder control? Did he experience other seizures before to recovery? If the patient may have incurred a brain injury, monitor him cautiously for any loss. Altered consciousness, asymmetrical or nonresponsive pupils, and localized neurological deficits. Does he report experiencing a headache and myalgia? Is he becoming progressively Is it challenging to awaken him when you check on him at 20-minute intervals? Analyze his arms, legs, and face (including tongue) for trauma, residual paralysis, or limb impairment vulnerability. Subsequently, acquire a history. Has the patient ever experienced widespread or focal seizures? prior? Do they occur with regularity? Do other relatives also possess Whom? Is the patient undergoing pharmacological treatment? Is he obedient? Additionally, inquire about sleep deprivation and mental or physical stress during the seizure transpired.
Etiological Factors
Intracranial abscess
Generalized seizures may manifest during the acute phase of an abscess. creation or subsequent to the resolution of the abscess. Contingent upon the magnitude and The location of the abscess and the degree of altered awareness (LOC) fluctuate. from lethargy to profound stupor. Initial indications and manifestations indicate heightened Intracranial pressure (ICP) manifests as a persistent headache and nausea.
Emesis and focal convulsions
Subsequent characteristics often encompass ocular Disruptions, including nystagmus, compromised vision, and asymmetrical pupils. Additional findings differ based on the abscess location but may encompass aphasia. Hemiparesis, atypical conduct, and alterations in personality. Neoplasm of the brain. Generalized seizures may manifest, contingent upon the tumor's Geographical position and classification. Additional studies indicate a gradual decline in level of consciousness. Morning headache, dizziness, disorientation, focal seizures, visual impairment, motor dysfunction and sensory impairments, aphasia, and ataxia. Subsequent discoveries encompass papilledema, emesis, elevated systolic blood pressure, widened pulse pressure pressure and, ultimately, a decorticate posture.
Chronic kidney failure
End-stage renal failure results in the swift emergence of Involuntary muscle contractions, tremors, myoclonic jerks, and generalized seizures. Connected Signs and symptoms encompass anuria or oliguria, weariness, malaise, and irritability. reduced cognitive sharpness, muscular spasms, peripheral nerve disorders, loss of appetite, and constipation or diarrhea. The integumentary consequences encompass skin pigmentation. Color alterations (yellow, brown, or bronze), itching, and uremic frost. Additional effects characterized by an ammonia-like breath odor, nausea and vomiting, and ecchymoses. petechiae, gastrointestinal hemorrhage, oral and gingival ulcers, hypertension, and Kussmaul respirations.
Eclampsia
Generalized seizures are a defining characteristic of eclampsia. Connected Findings encompass a severe frontal headache, nausea, vomiting, and visual disturbances. disruptions, elevated blood pressure, a temperature reaching 104°F (40°C), peripheral edema and abrupt weight increase. The patient may additionally demonstrate oliguria, irritability, and hyperactive deep tendon reflexes (DTRs) reduced level of consciousness.
Encephalitis
Seizures are an initial indication of encephalitis, signifying a negative prognosis. Prognosis; they may also manifest post-recovery due to lingering effects. harm. Additional observations encompass fever, headache, photophobia, and nuchal rigidity. stiffness, cervical discomfort, emesis, language impairment, lack of coordination, unilateral weakness, involuntary eye movement, irritability, cranial nerve palsies (resulting in facial paralysis, ptosis, dysphagia and myoclonic jerks.
Idiopathic epilepsy
The etiology of repeated seizures is, in the majority of instances, Unidentified. Cerebral injury. In extreme instances, generalized seizures may manifest together. pertaining to harm. Severe head trauma may result in focal seizures months later. may also result in diminished level of consciousness, potentially leading to coma; facial soft tissue injuries, cranial or cervical region; transparent or sanguineous exudate from the oral cavity, nasal passages, or auditory canals; face edema; osseous malformation of the face, cranium, or cervical region; Battle's sign; and an absence Response to oculocephalic and oculovestibular stimuli. Motor and Sensory impairments may accompany changed respirations. Assessment may indicate indicators of elevated intracranial pressure, such as a diminished reaction to painful stimuli stimuli, nonresponsive pupils, bradycardia, elevated systolic pressure, and increasing pulse pressure. If the patient is alert, he may display visual impairments, alterations in behavior, and cephalalgia.
Hepatic encephalopathy
Generalized seizures may manifest in advanced hepatic conditions. Encephalopathy. Related late-stage observations in the comatose patient With fetor hepaticus, asterixis, hyperactive deep tendon reflexes, and a positive Babinski's reflex.
Hypoglycemia
Generalized seizures typically manifest with intensity. Hypoglycemia, accompanied by visual disturbances such as blurred or double vision, and muscle weakness. hemiplegia, tremors, profuse sweating, tachycardia, myoclonic jerks Myoclonic jerking and diminished level of consciousness.
Hyponatremia
Seizures occur when serum sodium levels decline beneath 125. mEq/L, particularly if the reduction is abrupt. Hyponatremia furthermore induces orthostatic hypotension, cephalalgia, myoclonus, and muscular weakness, exhaustion, oliguria or anuria, cool and moist skin, diminished skin turgor, irritability, lethargy, confusion, and stupor or coma. Polydipsia, Tachycardia, nausea, vomiting, and abdominal cramps may also manifest. Severe hyponatremia can result in cyanosis and vasomotor collapse, accompanied by a Weak pulse.
Hypoparathyroidism
Progressive tetany induces generalized seizures. Chronic hypoparathyroidism induces neuromuscular excitability and exaggerated deep tendon reflexes. Hypoxic encephalopathy. In addition to generalized seizures, hypoxia Encephalopathy may induce myoclonic jerks and coma. Subsequently, if the The patient has recovered from dementia, visual agnosia, choreoathetosis, and ataxia. may transpire.
Neurofibromatosis
Neurofibromatosis induces several cerebral lesions. Focal and generalized seizures. Examination uncovers café-au-lait macules, Numerous cutaneous neoplasms, scoliosis, and kyphoscoliosis. Associated discoveries Symptoms encompass dizziness, ataxia, monocular blindness, and nystagmus. Cerebrovascular accident. Seizures, predominantly localized rather than generalized, may occur inside Six months post-ischemic stroke. Accompanying signs and symptoms differ according on The site and severity of cerebral injury. They encompass a diminished level of consciousness. contralateral hemiplegia, dysarthria, dysphagia, ataxia, unilateral sensory deficits loss, apraxia, agnosia, and aphasia. The patient may also experience visual disturbances. impairments, cognitive impairment, impaired judgment, alterations in personality, emotional disturbances lability, urinary retention or incontinence, constipation, headache, and emesis.
Alternative Causes
Arsenic toxicity. In addition to widespread seizures, arsenic poisoning may induce a garlicky breath odor, heightened salivation, and widespread pruritus. Gastrointestinal consequences including diarrhea, nausea, vomiting, and intense stomach discomfort. Associated consequences encompass widespread hyperpigmentation and strongly delineated edema. eyelid, facial, and ankle edema; extremity paresthesia; baldness; inflamed mucous membranes; fatigue; myalgia; and peripheral Neuropathy. Withdrawal from barbiturates. In patients with persistent intoxication, barbiturate Withdrawal may induce generalized seizures 2 to 4 days following the final dose. Status epilepticus may occur.
Diagnostic assessments
Contrast chemicals utilized in radiologic examinations may induce generalized seizures. Pharmaceutical substances. Toxic concentrations of several medications, including theophylline and lidocaine, Meperidine, penicillins, and cimetidine may induce generalized seizures. Phenothiazines, tricyclic antidepressants, amphetamines, isoniazid, and Vincristine may induce seizures in persons with preexisting epilepsy.
Carefully observe the patient post-seizure for any recurrence of seizure activity. Prepare him for a computed tomography scan or magnetic resonance imaging. and electroencephalogram.
Instruct the patient's family on how to monitor and document seizure occurrences, and Elucidate the rationale for undertaking such actions. Highlight the significance of adherence to pharmacological treatment and monitoring, and elucidate potential harmful effects of prescription medications Instruct the patient to consistently possess medical identification.
Generalized seizures frequently occur in pediatric populations. Indeed, between 75% and 90% of Individuals with epilepsy typically encounter their initial seizure prior to the age of 20. A multitude of children Generalized seizures occur between the ages of 3 months and 3 years. Accompanied with a temperature; some of these youngsters subsequently experience seizures in the absence of fever. Generalized seizures may also arise from congenital metabolic disorders and prenatal factors. trauma, cerebral infection, Reye's syndrome, Sturge-Weber syndrome, arteriovenous malformation Malformation, lead toxicity, hypoglycemia, and idiopathic origins. The the pertussis component of the DPT vaccine may induce seizures; however, this is uncommon.

- Published on
Symptoms and Signs – Differential Diagnosis of Absence seizures
Absence seizures are benign, widespread seizures believed to originate subcortically. These transient episodes of unconsciousness typically endure for 3 to 20 seconds and may occur over 100 times daily, resulting in intervals of inattention. Absence seizures often commence between the ages of 4 and 12. Their initial indicators may include declining academic performance and behavioral issues.
The etiology of these seizures is uncertain
Absence seizures manifest unexpectedly. The patient abruptly ceases all intentional activity and gazes vacantly forward, like a state of daydreaming. Absence seizures can result in automatisms, such as repetitive lip smacking, or modest clonic or myoclonic movements, including slight jerking of the eyelids. The patient may release an object he is holding, and muscle relaxation may result in the dropping of his head or arms or cause him to slouch. Subsequent to the attack, the patient resumes activity, generally oblivious to the incident. Absence status, an uncommon variant of absence seizure, manifests as an extended absence seizure or as recurrent occurrences of such seizures. Typically not life-threatening, it predominantly occurs in individuals with a history of absence seizures.
Medical History and Physical Assessment
To assess a suspected absence seizure, monitor its occurrence and length by reciting a sequence of numbers and thereafter requesting the patient to repeat them once the episode concludes. If the patient has experienced an absence seizure, he is unable to perform this task. Conversely, if the seizures transpire within minutes of one another, instruct the patient to count for around 5 minutes. He will cease counting during a seizure and recommence after it concludes. Identify associated automatisms. Ascertain whether the family has observed a change in behavior or a decline in academic performance. Etiological Factors in Medicine
Idiopathic epilepsy. Certain types of absence seizures are associated with learning impairments.
Prepare the patient for diagnostic examinations, including computed tomography scans, magnetic resonance imaging, and electroencephalograms. Administer the prescribed anticonvulsant. Offer emotional assistance to the sufferer and his family. Guarantee a secure atmosphere for the patient.
Identify the indications and symptoms necessitating urgent intervention, and underscore the significance of subsequent treatment. Incorporate the patient's educator and school nurse into the instructional process, if feasible. Examine the necessity of wearing medical identification.
Absence seizures are benign, widespread seizures believed to originate subcortically. These transient episodes of unconsciousness typically endure for 3 to 20 seconds and may occur over 100 times daily, resulting in intervals of inattention. Absence seizures often commence between the ages of 4 and 12. Their initial indicators may include declining academic performance and behavioral issues.
The etiology of these seizures is uncertain
Absence seizures manifest unexpectedly. The patient abruptly ceases all intentional activity and gazes vacantly forward, like a state of daydreaming. Absence seizures can result in automatisms, such as repetitive lip smacking, or modest clonic or myoclonic movements, including slight jerking of the eyelids. The patient may release an object he is holding, and muscle relaxation may result in the dropping of his head or arms or cause him to slouch. Subsequent to the attack, the patient resumes activity, generally oblivious to the incident. Absence status, an uncommon variant of absence seizure, manifests as an extended absence seizure or as recurrent occurrences of such seizures. Typically not life-threatening, it predominantly occurs in individuals with a history of absence seizures.
Medical History and Physical Assessment
To assess a suspected absence seizure, monitor its occurrence and length by reciting a sequence of numbers and thereafter requesting the patient to repeat them once the episode concludes. If the patient has experienced an absence seizure, he is unable to perform this task. Conversely, if the seizures transpire within minutes of one another, instruct the patient to count for around 5 minutes. He will cease counting during a seizure and recommence after it concludes. Identify associated automatisms. Ascertain whether the family has observed a change in behavior or a decline in academic performance. Etiological Factors in Medicine
Idiopathic epilepsy. Certain types of absence seizures are associated with learning impairments.
Prepare the patient for diagnostic examinations, including computed tomography scans, magnetic resonance imaging, and electroencephalograms. Administer the prescribed anticonvulsant. Offer emotional assistance to the sufferer and his family. Guarantee a secure atmosphere for the patient.
Identify the indications and symptoms necessitating urgent intervention, and underscore the significance of subsequent treatment. Incorporate the patient's educator and school nurse into the instructional process, if feasible. Examine the necessity of wearing medical identification.

- Published on
Symptoms and Signs – Differential Diagnosis of Scrotal Swelling
Scrotal swelling arises when a disorder impacting the testicles, epididymis, or scrotal skin leads to edema or a mass; the penis may also be affected. Scrotal swelling can occur in males of any age. It may be unilateral or bilateral and can be either painful or painless. The abrupt emergence of acute scrotal edema indicates potential torsion of a testicle or its appendages, particularly in a prepubescent boy. This emergency necessitates urgent surgery to untwist and stabilize the spermatic cord or to excise the appendage.
URGENT INTERVENTIONS
In the presence of significant pain alongside scrotal edema, inquire about the onset of the swelling. Utilize a Doppler stethoscope to assess blood flow to the testis. If diminished or absent, suspect testicular torsion and prepare the patient for surgical intervention. Restrict food and water, establish an intravenous line, and put an ice pack to the scrotum to alleviate pain and swelling. A manual attempt to untwist the cord may be undertaken; however, even if successful, the patient may still necessitate surgical intervention for stability.
Medical History and Physical Assessment
If the patient is not in distress, continue with the history taking. Inquire regarding scrotal injury, urethral discharge, turbid urine, heightened urinary frequency, and dysuria. Is the patient engaged in sexual activity? When did he last engage in sexual activity? Does he possess a history of sexually transmitted infections? Investigate modern diseases, specifically mumps. Does he possess a history of prostate surgery or extended catheterization? Does altering his body position or activity level influence the swelling? Assess the patient's vital signs, with particular attention to fever, and palpate the abdomen for soreness. Subsequently, inspect the entire genital region. Evaluate the scrotum with the patient in both supine and upright positions. Observe its dimensions and hue. Is the swelling unilateral or bilateral? Do you observe indications of trauma or contusions? Are there any rashes or lesions observed? Carefully examine the scrotum for any cysts or masses. Observe particularly for sensitivity or heightened stiffness. Examine the location of the testicles within the scrotum. Ultimately, transilluminate the scrotum to differentiate a fluid-filled cyst from a solid mass. A solid mass cannot be transilluminated.
Etiological Factors
Epididymal cysts
Epididymal cysts, situated at the apex of the epididymis, result in painless scrotal enlargement. Epididymitis. The primary characteristics of inflammation are pain, significant soreness, and swelling in the groin and scrotum. The patient ambulates with a waddle to alleviate strain on the groin and scrotum when walking. He may have a high temperature, malaise, urethral discharge, hazy urine, and lower abdominal pain on the affected side. His scrotal skin may exhibit heat, erythema, dryness, flakiness, and thinning. Hydrocele. Fluid accumulation results in progressive scrotal enlargement that is typically asymptomatic. The scrotum may exhibit a soft and cystic texture or a stiff and tense consistency. Palpation identifies a spherical, nontender lump in the scrotum.
Idiopathic scrotal edema
Idiopathic scrotal edema manifests rapidly, typically resolving within 24 hours. The impacted testicle exhibits a pink hue.
Acute orchitis
Mumps, syphilis, or tuberculosis can trigger orchitis, resulting in abrupt, painful enlargement of one or occasionally both testicles. Associated symptoms encompass a hyperemic scrotum; a fever reaching 104°F (40°C); chills; lower abdomen discomfort; nausea; emesis; and profound fatigue. Urinary manifestations are typically absent. Trauma to the scrotum. Blunt trauma results in scrotal edema accompanied by contusions and intense pain. The scrotum may exhibit a dark or bluish hue. Spermatocele. Spermatocele is typically a painless cystic formation located superiorly and posteriorly to the testicle, containing opaque fluid and spermatozoa. The onset may be either acute or gradual. Measuring under 1 cm in diameter, it is mobile and may exhibit transillumination.
Testicular torsion
Testicular torsion, predominantly occurring prior to puberty, is a urologic emergency characterized by scrotal enlargement, acute intense pain, and perhaps the elevation of the afflicted testicle inside the scrotum. It may also induce nausea and emesis.
Testicular neoplasm
A testicular tumor is generally painless, smooth, and firm, resulting in enlargement and a feeling of increased weight in the scrotum. Torsion of a Morgagni hydatid. Torsion of this diminutive, pea-sized cyst disrupts its blood supply, resulting in a firm, painful swelling on the upper pole of the testicle.
Alternative Causes
Operative procedure
A surgical blood effusion might result in a hematocele, causing scrotal edema. Maintain the patient in a state of bed rest and provide an antibiotic treatment. Administer sufficient water, fiber, and stool softeners. Position a rolled towel between the patient's legs and beneath the scrotum to alleviate significant swelling. If the patient exhibits mild or moderate swelling, recommend the use of a loose-fitting athletic supporter lined with a soft cotton dressing. Administer an analgesic for several days to alleviate his pain. Advocate for sitz baths and utilize heat or ice packs to mitigate irritation. Prepare the patient for needle aspiration of fluid-filled cysts and other diagnostic procedures, including lung tomography and abdominal computed tomography, to exclude malignant tumors.
Articulate to the patient the significance of conducting testicular self-examinations, and provide guidance on the appropriate method, if necessary. A comprehensive physical examination is particularly crucial for children with scrotal enlargement, as they may be unable to furnish historical information. In children under one year of age, a hernia or hydrocele of the spermatic cord may arise from atypical prenatal development. In babies, scrotal edema may result from ammonia-induced dermatitis due to infrequent diaper changes. In prepubescent males, it typically arises from spermatic cord torsion. Additional conditions that may cause scrotal enlargement in youngsters encompass epididymitis (uncommon prior to age 10), traumatic orchitis resulting from contact sports, and mumps, typically occurring post-puberty.
Scrotal swelling arises when a disorder impacting the testicles, epididymis, or scrotal skin leads to edema or a mass; the penis may also be affected. Scrotal swelling can occur in males of any age. It may be unilateral or bilateral and can be either painful or painless. The abrupt emergence of acute scrotal edema indicates potential torsion of a testicle or its appendages, particularly in a prepubescent boy. This emergency necessitates urgent surgery to untwist and stabilize the spermatic cord or to excise the appendage.
URGENT INTERVENTIONS
In the presence of significant pain alongside scrotal edema, inquire about the onset of the swelling. Utilize a Doppler stethoscope to assess blood flow to the testis. If diminished or absent, suspect testicular torsion and prepare the patient for surgical intervention. Restrict food and water, establish an intravenous line, and put an ice pack to the scrotum to alleviate pain and swelling. A manual attempt to untwist the cord may be undertaken; however, even if successful, the patient may still necessitate surgical intervention for stability.
Medical History and Physical Assessment
If the patient is not in distress, continue with the history taking. Inquire regarding scrotal injury, urethral discharge, turbid urine, heightened urinary frequency, and dysuria. Is the patient engaged in sexual activity? When did he last engage in sexual activity? Does he possess a history of sexually transmitted infections? Investigate modern diseases, specifically mumps. Does he possess a history of prostate surgery or extended catheterization? Does altering his body position or activity level influence the swelling? Assess the patient's vital signs, with particular attention to fever, and palpate the abdomen for soreness. Subsequently, inspect the entire genital region. Evaluate the scrotum with the patient in both supine and upright positions. Observe its dimensions and hue. Is the swelling unilateral or bilateral? Do you observe indications of trauma or contusions? Are there any rashes or lesions observed? Carefully examine the scrotum for any cysts or masses. Observe particularly for sensitivity or heightened stiffness. Examine the location of the testicles within the scrotum. Ultimately, transilluminate the scrotum to differentiate a fluid-filled cyst from a solid mass. A solid mass cannot be transilluminated.
Etiological Factors
Epididymal cysts
Epididymal cysts, situated at the apex of the epididymis, result in painless scrotal enlargement. Epididymitis. The primary characteristics of inflammation are pain, significant soreness, and swelling in the groin and scrotum. The patient ambulates with a waddle to alleviate strain on the groin and scrotum when walking. He may have a high temperature, malaise, urethral discharge, hazy urine, and lower abdominal pain on the affected side. His scrotal skin may exhibit heat, erythema, dryness, flakiness, and thinning. Hydrocele. Fluid accumulation results in progressive scrotal enlargement that is typically asymptomatic. The scrotum may exhibit a soft and cystic texture or a stiff and tense consistency. Palpation identifies a spherical, nontender lump in the scrotum.
Idiopathic scrotal edema
Idiopathic scrotal edema manifests rapidly, typically resolving within 24 hours. The impacted testicle exhibits a pink hue.
Acute orchitis
Mumps, syphilis, or tuberculosis can trigger orchitis, resulting in abrupt, painful enlargement of one or occasionally both testicles. Associated symptoms encompass a hyperemic scrotum; a fever reaching 104°F (40°C); chills; lower abdomen discomfort; nausea; emesis; and profound fatigue. Urinary manifestations are typically absent. Trauma to the scrotum. Blunt trauma results in scrotal edema accompanied by contusions and intense pain. The scrotum may exhibit a dark or bluish hue. Spermatocele. Spermatocele is typically a painless cystic formation located superiorly and posteriorly to the testicle, containing opaque fluid and spermatozoa. The onset may be either acute or gradual. Measuring under 1 cm in diameter, it is mobile and may exhibit transillumination.
Testicular torsion
Testicular torsion, predominantly occurring prior to puberty, is a urologic emergency characterized by scrotal enlargement, acute intense pain, and perhaps the elevation of the afflicted testicle inside the scrotum. It may also induce nausea and emesis.
Testicular neoplasm
A testicular tumor is generally painless, smooth, and firm, resulting in enlargement and a feeling of increased weight in the scrotum. Torsion of a Morgagni hydatid. Torsion of this diminutive, pea-sized cyst disrupts its blood supply, resulting in a firm, painful swelling on the upper pole of the testicle.
Alternative Causes
Operative procedure
A surgical blood effusion might result in a hematocele, causing scrotal edema. Maintain the patient in a state of bed rest and provide an antibiotic treatment. Administer sufficient water, fiber, and stool softeners. Position a rolled towel between the patient's legs and beneath the scrotum to alleviate significant swelling. If the patient exhibits mild or moderate swelling, recommend the use of a loose-fitting athletic supporter lined with a soft cotton dressing. Administer an analgesic for several days to alleviate his pain. Advocate for sitz baths and utilize heat or ice packs to mitigate irritation. Prepare the patient for needle aspiration of fluid-filled cysts and other diagnostic procedures, including lung tomography and abdominal computed tomography, to exclude malignant tumors.
Articulate to the patient the significance of conducting testicular self-examinations, and provide guidance on the appropriate method, if necessary. A comprehensive physical examination is particularly crucial for children with scrotal enlargement, as they may be unable to furnish historical information. In children under one year of age, a hernia or hydrocele of the spermatic cord may arise from atypical prenatal development. In babies, scrotal edema may result from ammonia-induced dermatitis due to infrequent diaper changes. In prepubescent males, it typically arises from spermatic cord torsion. Additional conditions that may cause scrotal enlargement in youngsters encompass epididymitis (uncommon prior to age 10), traumatic orchitis resulting from contact sports, and mumps, typically occurring post-puberty.

- Published on
Symptoms and Signs -Differential Diagnosis of Stertorous Respirations
Stertorous respirations, marked by a loud, rattling, or snoring sound, typically arise from the vibration of relaxed oropharyngeal structures during sleep or coma, leading to partial airway blockage. Occasionally, these respirations arise from residual mucus in the upper airway. This ubiquitous symptom manifests in approximately 10% of healthy persons, particularly among middle-aged males with obesity. The condition may be exacerbated by the consumption of alcohol or sedatives prior to sleep, which heightens oropharyngeal flaccidity, and by sleeping in the supine position, permitting the relaxed tongue to obstruct the airway. The primary pathological causes of stertorous respirations are obstructive sleep apnea and critical upper airway obstruction linked to an oropharyngeal tumor or uvular or palatal edema. This obstruction may also arise during the postictal phase of a generalized seizure when mucous secretions or a floppy tongue occlude the airway. At times, stertorous respirations are erroneously identified as stridor, another indicator of upper airway blockage. Stridor signifies laryngeal or tracheal blockage, while stertorous respirations suggest obstruction of the upper airway.
URGENT INTERVENTIONS
Upon observing stertorous respirations, examine the patient's oral cavity and pharynx for edema, erythema, lumps, or foreign bodies. In cases of pronounced edema, promptly assess the patient's vital signs, particularly oxygen saturation. Monitor him for indicators of respiratory distress, including dyspnea, tachypnea, utilization of accessory muscles, intercostal muscular retractions, and cyanosis. Elevate the head of the bed by 30 degrees to facilitate respiration and diminish edema. Subsequently, deliver supplemental oxygen by nasal cannula or face mask, and prepare for intubation, tracheostomy, or mechanical breathing. Establish an intravenous line for fluid and medication administration, and initiate cardiac monitoring. Upon detecting stertorous respirations during the patient's sleep, monitor the breathing pattern for a duration of 3 to 4 minutes. Do the noisy respirations terminate when he lies on his side and reemerge when he adopts a supine position? Monitor attentively for episodes of apnea and record their duration. When feasible, inquire with the patient's partner regarding his snoring patterns. Is she often disturbed by the patient's snoring? Does snoring ameliorate when the patient sleeps with the window ajar? Has she also noted the patient engaging in somniloquy or somnambulism? Inquire about indicators of sleep loss, such alterations in personality, headaches, diurnal drowsiness, or diminished cognitive sharpness.
Etiological Factors
Obstruction of the airway
Partial airway blockage, irrespective of its origin, can result in stertorous breathing, accompanied by wheezing, dyspnea, tachypnea, and subsequently, intercostal retractions and nasal flaring. In the event of a full obstruction, the patient suddenly loses the capacity to speak and exhibits diaphoresis, tachycardia, and inspiratory chest movement, although breath sounds are absent. Severe hypoxemia rapidly occurs, leading to cyanosis, loss of consciousness, and cardiopulmonary collapse.
Obstructive sleep apnea
Loud and disturbing snoring is a prominent feature of obstructive sleep apnea, frequently impacting those with obesity. Snoring typically alternates with episodes of sleep apnea, which generally conclude with loud gasps. Tachycardia and bradycardia may alternate. Episodes of snoring and apnea manifest in a cyclical rhythm during the night. Sleep abnormalities, including somnambulism and sleep talking, may also manifest. Certain patients exhibit hypertension and ankle edema. Many individuals arise in the morning with a pervasive headache, experiencing fatigue and a lack of refreshment. The predominant grievance is excessive diurnal somnolence. Insufficient sleep may lead to depression, aggression, and diminished cognitive function.
Alternative Causes
Endotracheal intubation, suctioning, or surgical intervention. Endotracheal intubation, suctioning, or surgical intervention may induce considerable palatal or uvular edema, leading to stertorous respirations.
Persist in meticulously observing the patient's breathing condition. Administer a corticosteroid or an antibiotic, along with cool, humidified oxygen, to alleviate palatal and uvular inflammation and edema. Laryngoscopy and bronchoscopy (to exclude airway obstruction) or formal sleep tests may be required. Patient Consultation Elucidate the fundamental etiology of the condition and its therapeutic alternatives. Examine the significance and techniques of weight reduction and the initiation of a smoking cessation program for patients who smoke. Instruct him on how to raise his head during sleep. Elucidate the correct configuration and utilization of a bilevel positive airway pressure or continuous positive airway pressure apparatus.
The predominant cause of stertorous respirations in children is nasal or pharyngeal obstruction resulting from tonsillar or adenoid hypertrophy or the presence of a foreign body. Advise the patient to pursue therapy for sleep apnea or considerable enlargement of the tonsils or adenoids.
Stertorous respirations, marked by a loud, rattling, or snoring sound, typically arise from the vibration of relaxed oropharyngeal structures during sleep or coma, leading to partial airway blockage. Occasionally, these respirations arise from residual mucus in the upper airway. This ubiquitous symptom manifests in approximately 10% of healthy persons, particularly among middle-aged males with obesity. The condition may be exacerbated by the consumption of alcohol or sedatives prior to sleep, which heightens oropharyngeal flaccidity, and by sleeping in the supine position, permitting the relaxed tongue to obstruct the airway. The primary pathological causes of stertorous respirations are obstructive sleep apnea and critical upper airway obstruction linked to an oropharyngeal tumor or uvular or palatal edema. This obstruction may also arise during the postictal phase of a generalized seizure when mucous secretions or a floppy tongue occlude the airway. At times, stertorous respirations are erroneously identified as stridor, another indicator of upper airway blockage. Stridor signifies laryngeal or tracheal blockage, while stertorous respirations suggest obstruction of the upper airway.
URGENT INTERVENTIONS
Upon observing stertorous respirations, examine the patient's oral cavity and pharynx for edema, erythema, lumps, or foreign bodies. In cases of pronounced edema, promptly assess the patient's vital signs, particularly oxygen saturation. Monitor him for indicators of respiratory distress, including dyspnea, tachypnea, utilization of accessory muscles, intercostal muscular retractions, and cyanosis. Elevate the head of the bed by 30 degrees to facilitate respiration and diminish edema. Subsequently, deliver supplemental oxygen by nasal cannula or face mask, and prepare for intubation, tracheostomy, or mechanical breathing. Establish an intravenous line for fluid and medication administration, and initiate cardiac monitoring. Upon detecting stertorous respirations during the patient's sleep, monitor the breathing pattern for a duration of 3 to 4 minutes. Do the noisy respirations terminate when he lies on his side and reemerge when he adopts a supine position? Monitor attentively for episodes of apnea and record their duration. When feasible, inquire with the patient's partner regarding his snoring patterns. Is she often disturbed by the patient's snoring? Does snoring ameliorate when the patient sleeps with the window ajar? Has she also noted the patient engaging in somniloquy or somnambulism? Inquire about indicators of sleep loss, such alterations in personality, headaches, diurnal drowsiness, or diminished cognitive sharpness.
Etiological Factors
Obstruction of the airway
Partial airway blockage, irrespective of its origin, can result in stertorous breathing, accompanied by wheezing, dyspnea, tachypnea, and subsequently, intercostal retractions and nasal flaring. In the event of a full obstruction, the patient suddenly loses the capacity to speak and exhibits diaphoresis, tachycardia, and inspiratory chest movement, although breath sounds are absent. Severe hypoxemia rapidly occurs, leading to cyanosis, loss of consciousness, and cardiopulmonary collapse.
Obstructive sleep apnea
Loud and disturbing snoring is a prominent feature of obstructive sleep apnea, frequently impacting those with obesity. Snoring typically alternates with episodes of sleep apnea, which generally conclude with loud gasps. Tachycardia and bradycardia may alternate. Episodes of snoring and apnea manifest in a cyclical rhythm during the night. Sleep abnormalities, including somnambulism and sleep talking, may also manifest. Certain patients exhibit hypertension and ankle edema. Many individuals arise in the morning with a pervasive headache, experiencing fatigue and a lack of refreshment. The predominant grievance is excessive diurnal somnolence. Insufficient sleep may lead to depression, aggression, and diminished cognitive function.
Alternative Causes
Endotracheal intubation, suctioning, or surgical intervention. Endotracheal intubation, suctioning, or surgical intervention may induce considerable palatal or uvular edema, leading to stertorous respirations.
Persist in meticulously observing the patient's breathing condition. Administer a corticosteroid or an antibiotic, along with cool, humidified oxygen, to alleviate palatal and uvular inflammation and edema. Laryngoscopy and bronchoscopy (to exclude airway obstruction) or formal sleep tests may be required. Patient Consultation Elucidate the fundamental etiology of the condition and its therapeutic alternatives. Examine the significance and techniques of weight reduction and the initiation of a smoking cessation program for patients who smoke. Instruct him on how to raise his head during sleep. Elucidate the correct configuration and utilization of a bilevel positive airway pressure or continuous positive airway pressure apparatus.
The predominant cause of stertorous respirations in children is nasal or pharyngeal obstruction resulting from tonsillar or adenoid hypertrophy or the presence of a foreign body. Advise the patient to pursue therapy for sleep apnea or considerable enlargement of the tonsils or adenoids.
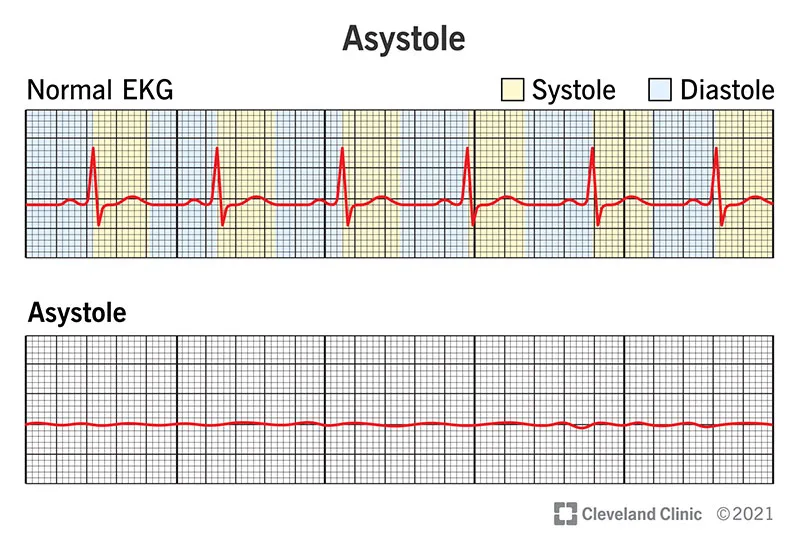
- Published on
Symptoms and Signs – Differential Diagnosis of Shallow respirations
Shallow respirations occur when a reduced volume of air reaches the lungs during inhalation. To acquire sufficient oxygen, the patient with shallow respirations often breathes at an increased rate. As he fatigues or his muscles weaken, the compensatory rise in respiration decreases, resulting in insufficient gas exchange and symptoms such as dyspnea, cyanosis, disorientation, agitation, loss of consciousness, and tachycardia. Shallow respirations may manifest abruptly or progressively and might be transient or persistent. They are a critical indicator of respiratory distress and neurological decline. Causes encompass insufficient central respiratory regulation, neuromuscular problems, heightened airflow resistance, respiratory muscle exhaustion or weakness, voluntary modifications in breathing, reduced activity due to prolonged bed rest, and pain.
URGENT INTERVENTIONS
Monitor for shallow respirations, as they may indicate imminent respiratory failure or arrest. Is the patient experiencing significant dyspnea? Disturbed or apprehensive? Identify indicators of airway blockage. In the event of a choking patient, administer four back strikes followed by four abdominal thrusts to dislodge the obstructing object. Employ suctioning if secretions obstruct the patient's airway. In the presence of wheezing, assess for stridor, nasal flare, and the utilization of accessory muscles. Administer oxygen using a facial mask or a handheld resuscitation bag. Strive to soothe the patient. Administer intravenous epinephrine. In the event of the patient losing consciousness, install an artificial airway and prepare for endotracheal intubation and mechanical ventilation. Assess his tidal volume and minute volume using a Wright respirometer to evaluate the necessity for mechanical ventilation.Assess arterial blood gas (ABG) levels, heart rate, blood pressure, and oxygen saturation. Tachycardia, altered blood pressure, inadequate minute volume, and declining ABG levels or oxygen saturation indicate the necessity for intubation and mechanical breathing.
Medical History and Physical Assessment
Commence with the patient's history if they are not experiencing acute respiratory distress. Inquire regarding chronic sickness in relation to surgical procedures or traumatic events. Has he received a tetanus booster within the last decade? Does he have asthma, allergies, or a history of cardiac failure or vascular disease? Does he have a persistent respiratory condition, respiratory tract infection, TB, or a neurological or neuromuscular disorder? Does he engage in smoking? Acquire a comprehensive drug history and investigate the potential for substance abuse. Quantifying Pulmonary Capacities Utilize a Wright respirometer to quantify tidal volume (the volume of air inhaled every breath) and minute volume (the total air inhaled in one minute, calculated as tidal volume multiplied by respiratory rate). The respirometer can be connected to the airway of an intubated patient either an endotracheal tube or a tracheostomy tube. Should the patient remain unintubated, attach the respirometer to a facial mask, ensuring an airtight seal over the patient's mouth and nose. Inquire regarding the onset of the patient's shallow respirations: When did they commence? What is their duration? What causes their diminishment? What provokes their irritation? Inquire about alterations in appetite, weight, activity level, and behavior. Commence the physical examination by evaluating the patient's state of consciousness (LOC) and orientation to time, person, and place. Examine involuntary movements, assess muscle strength, and evaluate deep tendon reflexes. Subsequently, examine the chest for abnormalities or atypical movements, including intercostal retractions. Examine the extremities for cyanosis and digital clubbing. Palpate for expansion and diaphragmatic tactile fremitus, and percuss for hyperresonance or dullness. Assess for reduced, nonexistent, or aberrant breath sounds, as well as for irregular or distant heart sounds. Do you observe peripheral edema? Finally, assess the abdomen for distension, discomfort, or tumors.
Etiological Factors
Acute Respiratory Distress Syndrome (ARDS)
ARDS initially manifests as fast, shallow respirations and dyspnea. Hypoxemia results in intercostal and suprasternal retractions, diaphoresis, and fluid buildup, which produce rhonchi and crackles. As hypoxemia intensifies, the patient demonstrates increased respiratory distress, agitation, anxiety, diminished level of consciousness, cyanosis, and maybe tachycardia.
Amyotrophic lateral sclerosis (ALS)
Respiratory muscle weakening in ALS results in progressively shallow respirations. Physical exertion may lead to heightened weakness and respiratory discomfort. Amyotrophic lateral sclerosis (ALS) initially causes muscle weakness and atrophy in the upper extremities, which over several years progresses to involve the trunk, neck, tongue, laryngeal, pharyngeal, and lower extremity muscles. Accompanying signs and symptoms encompass muscle cramps and atrophy, hyperreflexia, mild spasticity of the legs, coarse fasciculations of the afflicted muscle, decreased speech, and challenges with eating and swallowing.
Asthma
Asthma leads to bronchospasm and lung hyperinflation, resulting in fast, shallow breathing. In adults, minor persistent signs and symptoms may exacerbate during severe episodes. Associated respiratory manifestations encompass wheezing, rhonchi, a nonproductive cough, dyspnea, extended expiratory phases, intercostal and supraclavicular retractions during inspiration, nasal flaring, and utilization of accessory muscles. Chest constriction, rapid heartbeat, excessive sweating, and either flushing or cyanosis may manifest.
Atelectasis
Reduced lung expansion or pleuritic discomfort precipitates an abrupt commencement of fast, shallow breathing. Additional indications and symptoms encompass a dry cough, dyspnea, tachycardia, anxiety, cyanosis, and diaphoresis. The examination indicates dullness to percussion, diminished breath sounds and vocal fremitus, inspiratory lag, and substernal or intercostal retractions.
Bronchiectasis
Elevated secretions impede airflow in the lungs, resulting in shallow respirations and a productive cough characterized by abundant, malodorous, mucopurulent sputum, a hallmark observation. Additional findings encompass hemoptysis, wheezing, rhonchi, coarse crackles upon inspiration, and late-stage clubbing. The patient may report weight loss, weariness, exertional weakness, dyspnea on exertion, fever, malaise, and halitosis.
Coma
Accelerated, superficial breathing arises from neurological impairment or limited thoracic mobility.
Emphysema
Elevated respiratory effort results in muscular weariness, culminating in persistent shallow breathing. The patient may exhibit dyspnea, anorexia, lethargy, tachypnea, reduced breath sounds, cyanosis, pursed-lip breathing, use of accessory muscles, barrel chest, a persistent productive cough, and clubbing (a late manifestation).
Flail chest syndrome
Flail chest is characterized by diminished air movement, leading to fast, shallow respirations, paradoxical motion of the chest wall due to rib instability, tachycardia, hypotension, ecchymosis, cyanosis, and localized discomfort.
Guillain-Barré syndrome
Progressive ascending paralysis results in a swift or gradual onset of shallow respirations. Muscle weakness originates in the lower extremities and ultimately progresses to the facial region. Related findings encompass paresthesia, dysarthria, a reduced or nonexistent corneal reflex, nasal speech, dysphagia, ipsilateral facial muscle weakness, and flaccid paralysis.
Multiple sclerosis
Muscle weakening results in progressively shallow respirations. Initial symptoms encompass diplopia, hazy vision, and paresthesia. Additional potential findings include nystagmus, constipation, paralysis, spasticity, hyperreflexia, intention tremor, ataxic gait, dysphagia, dysarthria, urinary dysfunction, impotence, and emotional lability.
Myasthenia gravis
The advancement of myasthenia gravis results in respiratory muscle weakening characterized by shallow breathing, dyspnea, and cyanosis. Additional impacts encompass weariness, diminished eye closure, ptosis, diplopia, and challenges in mastication and deglutition.
Pleural effusion
Pleural effusion leads to restricted lung expansion, resulting in shallow respirations that may onset abruptly or progressively. Additional findings encompass a nonproductive cough, weight loss, dyspnea, and pleuritic chest pain. The examination indicates the presence of a pleural friction rub, tachycardia, tachypnea, diminished chest movement, flatness upon percussion, egophony, reduced or missing breath sounds, and decreased tactile fremitus.
Pneumothorax
Pneumothorax results in an abrupt emergence of shallow breathing and dyspnea. Associated effects encompass tachycardia, tachypnea, acute unilateral chest pain exacerbated by movement, a nonproductive cough, cyanosis, utilization of accessory muscles, asymmetrical chest expansion, anxiety, restlessness, hyperresonance or tympany on the affected side, subcutaneous crepitation, reduced vocal fremitus, and diminished or absent breath sounds on the affected side
Pulmonary edema
Pulmonary vascular congestion induces fast, shallow respirations. Initial manifestations including exertional dyspnea, paroxysmal nocturnal dyspnea, a nonproductive cough, tachycardia, tachypnea, dependent crackles, and a ventricular gallop. Severe pulmonary edema results in accelerated, laborious breathing; diffuse crackles; a productive cough with frothy, sanguine sputum; exacerbated tachycardia; arrhythmias; cold, clammy skin; cyanosis; hypotension; and a thready pulse.
Pulmonary embolism
Pulmonary embolism induces abrupt, fast, shallow breathing and intense dyspnea accompanied by angina or pleuritic chest pain. Additional clinical manifestations encompass tachycardia, tachypnea, a nonproductive cough or a productive cough with hemoptysis, low-grade fever, restlessness, diaphoresis, pleural friction rub, crackles, diffuse wheezing, dullness to percussion, diminished breath sounds, and indicators of circulatory collapse. Infrequent manifestations include significant hemoptysis, chest splinting, lower extremity edema, and, in cases of substantial embolism, cyanosis, syncope, and distension of the jugular veins.
Alternative Causes Pharmaceuticals
Opioids, sedatives, hypnotics, tranquilizers, neuromuscular blockers, magnesium sulfate, and anesthetics may induce slow, shallow respirations. Operative procedure. Post-abdominal or thoracic surgery, pain from chest splinting and reduced chest wall mobility may lead to short respirations.
Prepare the patient for diagnostic evaluations: arterial blood gas analysis, pulmonary function assessments, chest radiographs, or bronchoscopy. Position the patient in an upright orientation to facilitate respiration. Assist a postoperative patient in splinting their incision during coughing. If he is administering a respiratory depressant, adhere to all precautions and observe him diligently. Maintain sufficient hydration and employ humidification as necessary to liquefy secretions and alleviate inflammatory, dry, or irritated airway mucosa. Administer humidified oxygen, a bronchodilator, a mucolytic, an expectorant, or an antibiotic as prescribed. Conduct tracheal suctioning as necessary to remove secretions. Reposition the patient regularly. He may necessitate chest physiotherapy, incentive spirometry, or intermittent positive pressure ventilation. Observe the patient for escalating lethargy, which may signify elevated carbon dioxide levels. Ensure emergency equipment is positioned at the patient's bedside.
Elucidate the significance of coughing and deep breathing exercises. Offer emotional support and instruct the caregiver to do the same. Pediatric Guidelines In pediatric patients, shallow respirations frequently signify a critical medical condition. Airway obstruction may develop swiftly due to constricted passages; if it occurs, apply back blows or chest thrusts, avoiding abdominal thrusts, since they may harm internal organs. Factors contributing to shallow respirations in infants and children including idiopathic respiratory distress syndrome, acute epiglottitis, diphtheria, aspiration of a foreign body, croup, acute bronchiolitis, cystic fibrosis, and bacterial pneumonia. Monitor the youngster to identify apnea. Utilize humidification and suction as required, and provide supplemental oxygen. Administer parenteral fluids to maintain sufficient hydration. Chest physiotherapy and postural drainage may be necessary. Age-related stiffness or malformation of the chest wall may result in shallow respirations.
Shallow respirations occur when a reduced volume of air reaches the lungs during inhalation. To acquire sufficient oxygen, the patient with shallow respirations often breathes at an increased rate. As he fatigues or his muscles weaken, the compensatory rise in respiration decreases, resulting in insufficient gas exchange and symptoms such as dyspnea, cyanosis, disorientation, agitation, loss of consciousness, and tachycardia. Shallow respirations may manifest abruptly or progressively and might be transient or persistent. They are a critical indicator of respiratory distress and neurological decline. Causes encompass insufficient central respiratory regulation, neuromuscular problems, heightened airflow resistance, respiratory muscle exhaustion or weakness, voluntary modifications in breathing, reduced activity due to prolonged bed rest, and pain.
URGENT INTERVENTIONS
Monitor for shallow respirations, as they may indicate imminent respiratory failure or arrest. Is the patient experiencing significant dyspnea? Disturbed or apprehensive? Identify indicators of airway blockage. In the event of a choking patient, administer four back strikes followed by four abdominal thrusts to dislodge the obstructing object. Employ suctioning if secretions obstruct the patient's airway. In the presence of wheezing, assess for stridor, nasal flare, and the utilization of accessory muscles. Administer oxygen using a facial mask or a handheld resuscitation bag. Strive to soothe the patient. Administer intravenous epinephrine. In the event of the patient losing consciousness, install an artificial airway and prepare for endotracheal intubation and mechanical ventilation. Assess his tidal volume and minute volume using a Wright respirometer to evaluate the necessity for mechanical ventilation.Assess arterial blood gas (ABG) levels, heart rate, blood pressure, and oxygen saturation. Tachycardia, altered blood pressure, inadequate minute volume, and declining ABG levels or oxygen saturation indicate the necessity for intubation and mechanical breathing.
Medical History and Physical Assessment
Commence with the patient's history if they are not experiencing acute respiratory distress. Inquire regarding chronic sickness in relation to surgical procedures or traumatic events. Has he received a tetanus booster within the last decade? Does he have asthma, allergies, or a history of cardiac failure or vascular disease? Does he have a persistent respiratory condition, respiratory tract infection, TB, or a neurological or neuromuscular disorder? Does he engage in smoking? Acquire a comprehensive drug history and investigate the potential for substance abuse. Quantifying Pulmonary Capacities Utilize a Wright respirometer to quantify tidal volume (the volume of air inhaled every breath) and minute volume (the total air inhaled in one minute, calculated as tidal volume multiplied by respiratory rate). The respirometer can be connected to the airway of an intubated patient either an endotracheal tube or a tracheostomy tube. Should the patient remain unintubated, attach the respirometer to a facial mask, ensuring an airtight seal over the patient's mouth and nose. Inquire regarding the onset of the patient's shallow respirations: When did they commence? What is their duration? What causes their diminishment? What provokes their irritation? Inquire about alterations in appetite, weight, activity level, and behavior. Commence the physical examination by evaluating the patient's state of consciousness (LOC) and orientation to time, person, and place. Examine involuntary movements, assess muscle strength, and evaluate deep tendon reflexes. Subsequently, examine the chest for abnormalities or atypical movements, including intercostal retractions. Examine the extremities for cyanosis and digital clubbing. Palpate for expansion and diaphragmatic tactile fremitus, and percuss for hyperresonance or dullness. Assess for reduced, nonexistent, or aberrant breath sounds, as well as for irregular or distant heart sounds. Do you observe peripheral edema? Finally, assess the abdomen for distension, discomfort, or tumors.
Etiological Factors
Acute Respiratory Distress Syndrome (ARDS)
ARDS initially manifests as fast, shallow respirations and dyspnea. Hypoxemia results in intercostal and suprasternal retractions, diaphoresis, and fluid buildup, which produce rhonchi and crackles. As hypoxemia intensifies, the patient demonstrates increased respiratory distress, agitation, anxiety, diminished level of consciousness, cyanosis, and maybe tachycardia.
Amyotrophic lateral sclerosis (ALS)
Respiratory muscle weakening in ALS results in progressively shallow respirations. Physical exertion may lead to heightened weakness and respiratory discomfort. Amyotrophic lateral sclerosis (ALS) initially causes muscle weakness and atrophy in the upper extremities, which over several years progresses to involve the trunk, neck, tongue, laryngeal, pharyngeal, and lower extremity muscles. Accompanying signs and symptoms encompass muscle cramps and atrophy, hyperreflexia, mild spasticity of the legs, coarse fasciculations of the afflicted muscle, decreased speech, and challenges with eating and swallowing.
Asthma
Asthma leads to bronchospasm and lung hyperinflation, resulting in fast, shallow breathing. In adults, minor persistent signs and symptoms may exacerbate during severe episodes. Associated respiratory manifestations encompass wheezing, rhonchi, a nonproductive cough, dyspnea, extended expiratory phases, intercostal and supraclavicular retractions during inspiration, nasal flaring, and utilization of accessory muscles. Chest constriction, rapid heartbeat, excessive sweating, and either flushing or cyanosis may manifest.
Atelectasis
Reduced lung expansion or pleuritic discomfort precipitates an abrupt commencement of fast, shallow breathing. Additional indications and symptoms encompass a dry cough, dyspnea, tachycardia, anxiety, cyanosis, and diaphoresis. The examination indicates dullness to percussion, diminished breath sounds and vocal fremitus, inspiratory lag, and substernal or intercostal retractions.
Bronchiectasis
Elevated secretions impede airflow in the lungs, resulting in shallow respirations and a productive cough characterized by abundant, malodorous, mucopurulent sputum, a hallmark observation. Additional findings encompass hemoptysis, wheezing, rhonchi, coarse crackles upon inspiration, and late-stage clubbing. The patient may report weight loss, weariness, exertional weakness, dyspnea on exertion, fever, malaise, and halitosis.
Coma
Accelerated, superficial breathing arises from neurological impairment or limited thoracic mobility.
Emphysema
Elevated respiratory effort results in muscular weariness, culminating in persistent shallow breathing. The patient may exhibit dyspnea, anorexia, lethargy, tachypnea, reduced breath sounds, cyanosis, pursed-lip breathing, use of accessory muscles, barrel chest, a persistent productive cough, and clubbing (a late manifestation).
Flail chest syndrome
Flail chest is characterized by diminished air movement, leading to fast, shallow respirations, paradoxical motion of the chest wall due to rib instability, tachycardia, hypotension, ecchymosis, cyanosis, and localized discomfort.
Guillain-Barré syndrome
Progressive ascending paralysis results in a swift or gradual onset of shallow respirations. Muscle weakness originates in the lower extremities and ultimately progresses to the facial region. Related findings encompass paresthesia, dysarthria, a reduced or nonexistent corneal reflex, nasal speech, dysphagia, ipsilateral facial muscle weakness, and flaccid paralysis.
Multiple sclerosis
Muscle weakening results in progressively shallow respirations. Initial symptoms encompass diplopia, hazy vision, and paresthesia. Additional potential findings include nystagmus, constipation, paralysis, spasticity, hyperreflexia, intention tremor, ataxic gait, dysphagia, dysarthria, urinary dysfunction, impotence, and emotional lability.
Myasthenia gravis
The advancement of myasthenia gravis results in respiratory muscle weakening characterized by shallow breathing, dyspnea, and cyanosis. Additional impacts encompass weariness, diminished eye closure, ptosis, diplopia, and challenges in mastication and deglutition.
Pleural effusion
Pleural effusion leads to restricted lung expansion, resulting in shallow respirations that may onset abruptly or progressively. Additional findings encompass a nonproductive cough, weight loss, dyspnea, and pleuritic chest pain. The examination indicates the presence of a pleural friction rub, tachycardia, tachypnea, diminished chest movement, flatness upon percussion, egophony, reduced or missing breath sounds, and decreased tactile fremitus.
Pneumothorax
Pneumothorax results in an abrupt emergence of shallow breathing and dyspnea. Associated effects encompass tachycardia, tachypnea, acute unilateral chest pain exacerbated by movement, a nonproductive cough, cyanosis, utilization of accessory muscles, asymmetrical chest expansion, anxiety, restlessness, hyperresonance or tympany on the affected side, subcutaneous crepitation, reduced vocal fremitus, and diminished or absent breath sounds on the affected side
Pulmonary edema
Pulmonary vascular congestion induces fast, shallow respirations. Initial manifestations including exertional dyspnea, paroxysmal nocturnal dyspnea, a nonproductive cough, tachycardia, tachypnea, dependent crackles, and a ventricular gallop. Severe pulmonary edema results in accelerated, laborious breathing; diffuse crackles; a productive cough with frothy, sanguine sputum; exacerbated tachycardia; arrhythmias; cold, clammy skin; cyanosis; hypotension; and a thready pulse.
Pulmonary embolism
Pulmonary embolism induces abrupt, fast, shallow breathing and intense dyspnea accompanied by angina or pleuritic chest pain. Additional clinical manifestations encompass tachycardia, tachypnea, a nonproductive cough or a productive cough with hemoptysis, low-grade fever, restlessness, diaphoresis, pleural friction rub, crackles, diffuse wheezing, dullness to percussion, diminished breath sounds, and indicators of circulatory collapse. Infrequent manifestations include significant hemoptysis, chest splinting, lower extremity edema, and, in cases of substantial embolism, cyanosis, syncope, and distension of the jugular veins.
Alternative Causes Pharmaceuticals
Opioids, sedatives, hypnotics, tranquilizers, neuromuscular blockers, magnesium sulfate, and anesthetics may induce slow, shallow respirations. Operative procedure. Post-abdominal or thoracic surgery, pain from chest splinting and reduced chest wall mobility may lead to short respirations.
Prepare the patient for diagnostic evaluations: arterial blood gas analysis, pulmonary function assessments, chest radiographs, or bronchoscopy. Position the patient in an upright orientation to facilitate respiration. Assist a postoperative patient in splinting their incision during coughing. If he is administering a respiratory depressant, adhere to all precautions and observe him diligently. Maintain sufficient hydration and employ humidification as necessary to liquefy secretions and alleviate inflammatory, dry, or irritated airway mucosa. Administer humidified oxygen, a bronchodilator, a mucolytic, an expectorant, or an antibiotic as prescribed. Conduct tracheal suctioning as necessary to remove secretions. Reposition the patient regularly. He may necessitate chest physiotherapy, incentive spirometry, or intermittent positive pressure ventilation. Observe the patient for escalating lethargy, which may signify elevated carbon dioxide levels. Ensure emergency equipment is positioned at the patient's bedside.
Elucidate the significance of coughing and deep breathing exercises. Offer emotional support and instruct the caregiver to do the same. Pediatric Guidelines In pediatric patients, shallow respirations frequently signify a critical medical condition. Airway obstruction may develop swiftly due to constricted passages; if it occurs, apply back blows or chest thrusts, avoiding abdominal thrusts, since they may harm internal organs. Factors contributing to shallow respirations in infants and children including idiopathic respiratory distress syndrome, acute epiglottitis, diphtheria, aspiration of a foreign body, croup, acute bronchiolitis, cystic fibrosis, and bacterial pneumonia. Monitor the youngster to identify apnea. Utilize humidification and suction as required, and provide supplemental oxygen. Administer parenteral fluids to maintain sufficient hydration. Chest physiotherapy and postural drainage may be necessary. Age-related stiffness or malformation of the chest wall may result in shallow respirations.

- Published on
Symptoms and Signs – Differential Diagnosis of Rectal Pain
Rectal pain, a prevalent symptom of anorectal diseases, is discomfort originating in the anorectal region. The anal canal, delineated from the rectum by the internal sphincter, may lead the patient to describe all localized discomfort as rectal pain. The mucocutaneous border of the anal canal and the perianal skin includes somatic nerve fibers, making injuries in this region very painful. This pain may arise from or be exacerbated by diarrhea, constipation, or the passage of hardened stools. Intense pruritus and persistent scratching may exacerbate the condition, particularly when accompanied by the discharge of mucus, blood, or fecal matter that irritates the skin and nerve endings.
Medical History and Physical Assessment
Upon the patient's description of rectal pain, examine the region for hemorrhage; atypical exudate, including purulence; or protrusions, such as skin tags or thrombosed hemorrhoids. Additionally, assess for inflammation and other lesions. A rectal examination can be required. Subsequent to the examination, conduct your assessment by obtaining the patient's history. Request that he elucidate the nature of the pain. Is it acute or obtuse, caustic or resembling a blade? What is the frequency of its occurrence? Inquire whether the pain intensifies during or immediately following defecation. Does the patient refrain from bowel movements due to expected discomfort? Determine the factors that mitigate the pain. Ensure to inquire about the progression of related indications and symptoms. For instance, does the patient exhibit hemorrhaging in conjunction with rectal discomfort? Determine the frequency of this occurrence and ascertain whether the blood is present on the toilet tissue, on the stool's surface, or in the toilet bowl. Is the blood a vivid or a deep red? Additionally, inquire if the patient has observed any other leakage, such as mucus or pus, and whether he is having constipation or diarrhea. Inquire about the timing of his most recent bowel movement. Acquire a nutritional history.
Etiological Factors
Perirectal abscess
A perirectal abscess may develop in multiple sites within the rectum and anus, resulting in discomfort in the perianal region. A superficial abscess generally causes persistent, pulsating localized discomfort that intensifies with sitting or walking. The localized discomfort linked to a deeper abscess may commence gradually, often in the upper rectum or lower abdomen, and is accompanied by a hardened anal mass. The patient may exhibit concomitant signs and symptoms, including fever, malaise, anal enlargement and inflammation, purulent discharge, and localized discomfort.
Anal fissure
An anal fissure is a linear tear in the anal mucosa that induces acute rectal pain during feces. The patient generally endures a burning sensation and persistent gnawing pain that may last for up to 4 hours post-defecation. The apprehension of inciting this discomfort may result in acute constipation. The patient may have anal itchiness and significant discomfort, and may report the presence of blood stains on toilet tissue following feces.
Anorectal fistula
Pain arises when a passage between the anal canal and the skin becomes briefly occluded. It continues until drainage is restored. Additional primary complaints encompass pruritus and the exudation of pus, blood, mucus, and, on occasion, fecal matter.
Hemorrhoids
Thrombosed or prolapsed hemorrhoids induce rectal pain that may intensify during defecation and diminish thereafter. The patient's apprehension of exacerbating the discomfort may result in constipation. Typically, rectal discomfort is associated with intense pruritus. Internal hemorrhoids may cause minor, sporadic bleeding, typically manifesting as spotting on toilet tissue or the surface of the stool. External hemorrhoids are observable beyond the anal sphincter.
Administer analgesic ointment or suppositories, and provide a stool softener if necessary. If rectal pain is due to prolapsed hemorrhoids, apply cold compresses to diminish protruding hemorrhoids, avert thrombosis, and alleviate pain. Should the patient's condition allow, position him in Trendelenburg's posture with his buttocks lifted to alleviate pain further. You may need to prepare the patient for an anoscopic examination and proctosigmoidoscopy to ascertain the etiology of rectal pain. He might also be required to submit a stool specimen. Due to potential embarrassment associated with rectal treatments and diagnostic testing, offer emotional support and ensure maximum privacy.
Advise the patient on methods to alleviate discomfort. Additionally, address the significance of an appropriate diet and adequate fluid consumption, as well as the necessity for stool softeners.
Monitor children experiencing rectal pain for concomitant bleeding, discharge, and indicators of infection, such as fever and agitation. Acute anal fissure is a prevalent source of rectal pain and hemorrhage in youngsters, whose apprehension of exacerbating the pain may result in constipation. Infants exhibiting pain during defecation should be assessed for congenital rectal abnormalities. Evaluate the potential for sexual abuse in all youngsters reporting rectal discomfort.
Elderly individuals often underreport symptoms and possess a heightened risk of neoplastic illnesses; hence, they should undergo comprehensive evaluation.
Rectal pain, a prevalent symptom of anorectal diseases, is discomfort originating in the anorectal region. The anal canal, delineated from the rectum by the internal sphincter, may lead the patient to describe all localized discomfort as rectal pain. The mucocutaneous border of the anal canal and the perianal skin includes somatic nerve fibers, making injuries in this region very painful. This pain may arise from or be exacerbated by diarrhea, constipation, or the passage of hardened stools. Intense pruritus and persistent scratching may exacerbate the condition, particularly when accompanied by the discharge of mucus, blood, or fecal matter that irritates the skin and nerve endings.
Medical History and Physical Assessment
Upon the patient's description of rectal pain, examine the region for hemorrhage; atypical exudate, including purulence; or protrusions, such as skin tags or thrombosed hemorrhoids. Additionally, assess for inflammation and other lesions. A rectal examination can be required. Subsequent to the examination, conduct your assessment by obtaining the patient's history. Request that he elucidate the nature of the pain. Is it acute or obtuse, caustic or resembling a blade? What is the frequency of its occurrence? Inquire whether the pain intensifies during or immediately following defecation. Does the patient refrain from bowel movements due to expected discomfort? Determine the factors that mitigate the pain. Ensure to inquire about the progression of related indications and symptoms. For instance, does the patient exhibit hemorrhaging in conjunction with rectal discomfort? Determine the frequency of this occurrence and ascertain whether the blood is present on the toilet tissue, on the stool's surface, or in the toilet bowl. Is the blood a vivid or a deep red? Additionally, inquire if the patient has observed any other leakage, such as mucus or pus, and whether he is having constipation or diarrhea. Inquire about the timing of his most recent bowel movement. Acquire a nutritional history.
Etiological Factors
Perirectal abscess
A perirectal abscess may develop in multiple sites within the rectum and anus, resulting in discomfort in the perianal region. A superficial abscess generally causes persistent, pulsating localized discomfort that intensifies with sitting or walking. The localized discomfort linked to a deeper abscess may commence gradually, often in the upper rectum or lower abdomen, and is accompanied by a hardened anal mass. The patient may exhibit concomitant signs and symptoms, including fever, malaise, anal enlargement and inflammation, purulent discharge, and localized discomfort.
Anal fissure
An anal fissure is a linear tear in the anal mucosa that induces acute rectal pain during feces. The patient generally endures a burning sensation and persistent gnawing pain that may last for up to 4 hours post-defecation. The apprehension of inciting this discomfort may result in acute constipation. The patient may have anal itchiness and significant discomfort, and may report the presence of blood stains on toilet tissue following feces.
Anorectal fistula
Pain arises when a passage between the anal canal and the skin becomes briefly occluded. It continues until drainage is restored. Additional primary complaints encompass pruritus and the exudation of pus, blood, mucus, and, on occasion, fecal matter.
Hemorrhoids
Thrombosed or prolapsed hemorrhoids induce rectal pain that may intensify during defecation and diminish thereafter. The patient's apprehension of exacerbating the discomfort may result in constipation. Typically, rectal discomfort is associated with intense pruritus. Internal hemorrhoids may cause minor, sporadic bleeding, typically manifesting as spotting on toilet tissue or the surface of the stool. External hemorrhoids are observable beyond the anal sphincter.
Administer analgesic ointment or suppositories, and provide a stool softener if necessary. If rectal pain is due to prolapsed hemorrhoids, apply cold compresses to diminish protruding hemorrhoids, avert thrombosis, and alleviate pain. Should the patient's condition allow, position him in Trendelenburg's posture with his buttocks lifted to alleviate pain further. You may need to prepare the patient for an anoscopic examination and proctosigmoidoscopy to ascertain the etiology of rectal pain. He might also be required to submit a stool specimen. Due to potential embarrassment associated with rectal treatments and diagnostic testing, offer emotional support and ensure maximum privacy.
Advise the patient on methods to alleviate discomfort. Additionally, address the significance of an appropriate diet and adequate fluid consumption, as well as the necessity for stool softeners.
Monitor children experiencing rectal pain for concomitant bleeding, discharge, and indicators of infection, such as fever and agitation. Acute anal fissure is a prevalent source of rectal pain and hemorrhage in youngsters, whose apprehension of exacerbating the pain may result in constipation. Infants exhibiting pain during defecation should be assessed for congenital rectal abnormalities. Evaluate the potential for sexual abuse in all youngsters reporting rectal discomfort.
Elderly individuals often underreport symptoms and possess a heightened risk of neoplastic illnesses; hence, they should undergo comprehensive evaluation.

