- Published on
Symptoms and Signs – Differential Diagnosis of Fasciculations
Fasciculations are localized muscle contractions that occur when a muscle fiber bundle, innervated by a single motor neuron filament, spontaneously discharges. Although these contractions result in noticeable dimpling or wavelike twitching of the skin, they lack the strength to induce movement in a joint. Intermittently, they manifest at frequencies ranging from once every few seconds to two or three times per second; rarely, myokymia - uninterrupted, fast contractions that result in a rippling effect - may occur. Given their short duration and lack of pain, fasciculations often remain unnoticed or are disregarded.
Benign, nonpathologic fasciculations are frequently occurring and considered normal. These symptoms commonly manifest in those who are tense, worried, or highly fatigued, and usually impact the eyelid, thumb, or calf. Yet, fasciculations can also suggest a serious neurological condition, particularly a diffuse motor neuron dysfunction that results in impaired regulation of muscle fiber release. Furthermore, they serve as an initial indication of pesticide poisoning.
Urgent medical interventions
Ask the patient to describe the characteristics, beginning, and length of the fasciculations. If the onset occurred abruptly, inquire about triggering factors such as pesticide exposure. Although rare, pesticide poisoning is a medical emergency that demands immediate and forceful action. Patients may require airway patency maintenance, monitoring of vital signs, administration of oxygen, and stomach lavage or induction of vomiting.
Historical Background and Physical Assessment
In the absence of significant discomfort, ascertain whether the patient has encountered sensory alterations, such as paresthesia, or any impairment in speech, swallowing, respiration, or regulation of bowel or bladder function. Probe him for any signs of discomfort.
Review the patient's medical records for neurological diseases, malignancies, and recent infections. Additionally, inquire about his lifestyle, particularly aspects of stress experienced at home, work, or school.
Inquire with the patient regarding his dietary patterns and request a detailed account of his recent food and fluid consumption, as electrolyte imbalances can also contribute to muscle twitching responses.
Conduct a physical examination, specifically focusing on identifying any fasciculations when the afflicted muscle is completely relaxed. Conduct visual observations and assessments to identify motor and sensory abnormalities, namely muscle atrophy and weakening, as well as reduced deep tendon reflexes. If you observe these indications and symptoms, you should suspect the presence of motor neuron pathology and do a thorough neurological assessment.
Medical etiology
Amyotrophic Lateral Sclerosis (ALS)
Primary coarse fasciculations often originate in the tiny muscles of the hands and feet, subsequently extending to the forearms and legs. Dysarthria, characterized by widespread, symmetrical muscle atrophy and weakening, can lead to difficulties in eating, swallowing, and breathing, and, in rare cases, choking and excessive salivation.
Osteoporosis
Age-related fasciculations of the cheeks and tongue often manifest early. Advancements in the condition manifest as dysarthria, dysphagia, hoarseness, and drooling. In due course, debility extends to the respiratory muscles.
Spinal paralysis caused by poliomyelitis
Progressive muscle weakness, spasms, and atrophy are accompanied with coarse fasciculations, which are typically temporary but occasionally persistent. The patient may also present with reduced reflexes, paresthesia, coldness, and cyanosis in the afflicted extremities, bladder paralysis, shortness of breath, increased blood pressure, and rapid heart rate.
Spinal cord malignancies
The development of fasciculations may occur in conjunction with muscular atrophy and cramping, initially asymmetrically and subsequently bilaterally as cord compression advances. Further from the tumor, there are motor and sensory alterations characterized by weakness or paralysis, lack of reflexes, loss of sensation, and a constricted circle of pain. Disruption of bowel and bladder control may occur.
Pesticide poisoning. Ingestion of organophosphate or carbamate pesticides commonly produces an acute onset of long, wavelike fasciculations and muscle weakness that rapidly progresses to flaccid paralysis. Other common effects include nausea, vomiting, diarrhea, loss of bowel and
bladder control, hyperactive bowel sounds, and abdominal cramping. Cardiopulmonary findings include bradycardia, dyspnea or bradypnea, and pallor or cyanosis. Seizures, visual disturbances (pupillary constriction or blurred vision), and increased secretions (tearing, salivation, pulmonary secretions, or diaphoresis) may also occur.
Special Considerations
Prepare the patient for diagnostic studies, such as spinal X-rays, myelography, a computed tomography scan, magnetic resonance imaging, and electromyography with nerve conduction velocity tests. Prepare the patient for laboratory tests such as serum electrolyte levels. Help the patient with progressive neuromuscular degeneration to cope with activities of daily living, and provide appropriate assistive devices.
Patient Counseling
Explain the underlying cause of the disease, its progression, and its treatment options. Instruct the patient how to use assistive devices. Refer him to support groups as indicated.
Pediatric Pointers
Fasciculations, particularly of the tongue, are an important early sign of Werdnig-Hoffmann disease.
Fasciculations are localized muscle contractions that occur when a muscle fiber bundle, innervated by a single motor neuron filament, spontaneously discharges. Although these contractions result in noticeable dimpling or wavelike twitching of the skin, they lack the strength to induce movement in a joint. Intermittently, they manifest at frequencies ranging from once every few seconds to two or three times per second; rarely, myokymia - uninterrupted, fast contractions that result in a rippling effect - may occur. Given their short duration and lack of pain, fasciculations often remain unnoticed or are disregarded.
Benign, nonpathologic fasciculations are frequently occurring and considered normal. These symptoms commonly manifest in those who are tense, worried, or highly fatigued, and usually impact the eyelid, thumb, or calf. Yet, fasciculations can also suggest a serious neurological condition, particularly a diffuse motor neuron dysfunction that results in impaired regulation of muscle fiber release. Furthermore, they serve as an initial indication of pesticide poisoning.
Urgent medical interventions
Ask the patient to describe the characteristics, beginning, and length of the fasciculations. If the onset occurred abruptly, inquire about triggering factors such as pesticide exposure. Although rare, pesticide poisoning is a medical emergency that demands immediate and forceful action. Patients may require airway patency maintenance, monitoring of vital signs, administration of oxygen, and stomach lavage or induction of vomiting.
Historical Background and Physical Assessment
In the absence of significant discomfort, ascertain whether the patient has encountered sensory alterations, such as paresthesia, or any impairment in speech, swallowing, respiration, or regulation of bowel or bladder function. Probe him for any signs of discomfort.
Review the patient's medical records for neurological diseases, malignancies, and recent infections. Additionally, inquire about his lifestyle, particularly aspects of stress experienced at home, work, or school.
Inquire with the patient regarding his dietary patterns and request a detailed account of his recent food and fluid consumption, as electrolyte imbalances can also contribute to muscle twitching responses.
Conduct a physical examination, specifically focusing on identifying any fasciculations when the afflicted muscle is completely relaxed. Conduct visual observations and assessments to identify motor and sensory abnormalities, namely muscle atrophy and weakening, as well as reduced deep tendon reflexes. If you observe these indications and symptoms, you should suspect the presence of motor neuron pathology and do a thorough neurological assessment.
Medical etiology
Amyotrophic Lateral Sclerosis (ALS)
Primary coarse fasciculations often originate in the tiny muscles of the hands and feet, subsequently extending to the forearms and legs. Dysarthria, characterized by widespread, symmetrical muscle atrophy and weakening, can lead to difficulties in eating, swallowing, and breathing, and, in rare cases, choking and excessive salivation.
Osteoporosis
Age-related fasciculations of the cheeks and tongue often manifest early. Advancements in the condition manifest as dysarthria, dysphagia, hoarseness, and drooling. In due course, debility extends to the respiratory muscles.
Spinal paralysis caused by poliomyelitis
Progressive muscle weakness, spasms, and atrophy are accompanied with coarse fasciculations, which are typically temporary but occasionally persistent. The patient may also present with reduced reflexes, paresthesia, coldness, and cyanosis in the afflicted extremities, bladder paralysis, shortness of breath, increased blood pressure, and rapid heart rate.
Spinal cord malignancies
The development of fasciculations may occur in conjunction with muscular atrophy and cramping, initially asymmetrically and subsequently bilaterally as cord compression advances. Further from the tumor, there are motor and sensory alterations characterized by weakness or paralysis, lack of reflexes, loss of sensation, and a constricted circle of pain. Disruption of bowel and bladder control may occur.
Pesticide poisoning. Ingestion of organophosphate or carbamate pesticides commonly produces an acute onset of long, wavelike fasciculations and muscle weakness that rapidly progresses to flaccid paralysis. Other common effects include nausea, vomiting, diarrhea, loss of bowel and
bladder control, hyperactive bowel sounds, and abdominal cramping. Cardiopulmonary findings include bradycardia, dyspnea or bradypnea, and pallor or cyanosis. Seizures, visual disturbances (pupillary constriction or blurred vision), and increased secretions (tearing, salivation, pulmonary secretions, or diaphoresis) may also occur.
Special Considerations
Prepare the patient for diagnostic studies, such as spinal X-rays, myelography, a computed tomography scan, magnetic resonance imaging, and electromyography with nerve conduction velocity tests. Prepare the patient for laboratory tests such as serum electrolyte levels. Help the patient with progressive neuromuscular degeneration to cope with activities of daily living, and provide appropriate assistive devices.
Patient Counseling
Explain the underlying cause of the disease, its progression, and its treatment options. Instruct the patient how to use assistive devices. Refer him to support groups as indicated.
Pediatric Pointers
Fasciculations, particularly of the tongue, are an important early sign of Werdnig-Hoffmann disease.

- Published on
Symptoms and Signs – Differential Diagnosis of Eye Pain
Ocular pain can be characterized as a sensory perception of burning, throbbing, aching, or stabbing in or around the eye. It may instead be described as a perception of a foreign body. This symptom exhibits a range of severity, with its duration and precise location offering indications of the underlying diagnosis.
Ocular discomfort frequently arises from corneal abrasion, however it can also be caused by glaucoma or other ocular diseases, trauma, and neurological or systemic problems. The stimulation of nerve endings in the cornea or external eye by any of these may result in the generation of pain.
Urgent medical interventions
To alleviate eye pain caused by a chemical burn, remove any contact lenses and topically irrigate the eye with a minimum of 1 liter of normal saline solution for a duration of 10 minutes. After everting the lids, clean the fornices with a cotton-tipped swab to eliminate any particles or chemicals. Severe eye pain caused by acute angle-closure glaucoma is a critical ocular condition that needs prompt treatment to lower intraocular pressure (IOP). If medication therapy fails to decrease intraocular pressure (IOP), the patient will require laser iridotomy or surgical peripheral iridectomy in order to preserve his retinal function.
Historical Background and Physical Assessment
For eye pain not caused by a chemical burn, obtain a comprehensive medical history from the patient. Elicit a comprehensive description of the pain from the patient. Is it a dull discomfort or a penetrating cramp? For what duration does it endure? Does it present with sensations of burning, itching, or discharge? Determine its commencement time. Does it exhibit greater severity during the morning or late evening? Enquire about any recent traumatic events or surgical procedures, particularly if the patient reports abrupt and intense pain. Does he experience headaches? If such is the case, determine the frequency and timing of their occurrence.
When conducting a physical examination, refrain from manipulating the eye if evidence of trauma is suspected. Thoroughly examine the eyelids and conjunctiva for any signs of excessive redness, irritation, or swelling. Next, assess the eyes for ptosis or exophthalmos disorder. At last, evaluate visual acuity both with and without correction, and analyze extraocular motions. Description of any discharge.
Medical etiology
Angle-closure glaucoma of acute onset. Symptoms of acute angle-closure glaucoma include blurred vision and intense, sudden pain in and around the eye. The pain can be so intense that it induces nausea, vomiting, and abdominal discomfort.
Additional manifestations include halo vision, a rapid decline in visual acuity, and a stationary, unresponsive, slightly enlarged pupil.
Blepharitis
Burning discomfort in both eyelids is accompanied by pruritus, viscous secretion, and injection of conjunctival fluid. Additional results include a perception of a foreign object, ulcerations on the eyelid, and a missing of eyelashes.
Burns
Eye discomfort caused by chemical burns can manifest as abrupt and intense, accompanied by redness and blistering of the face and eyelids, sensitivity to light, excessive sweating, injection of conjunctival fluid, blurred vision, and difficulty in maintaining open eyelids. Ultraviolet radiation burns result in moderate to severe pain approximately 12 hours after exposure, commonly accompanied by photophobia and alterations in eyesight.
Chalazion
Localised discomfort and swelling on the upper or lower eyelid are symptoms of a chalazion. Opening the eyelid exposes conjunctival injection and a little erythematous mass.
Conjunctivitis
All four forms of conjunctivitis result in varying levels of ocular pain and profuse weeping. Allergic conjunctivitis is characterized by mild, burning, bilateral pain, along with itching, conjunctival injection, and a distinctive ropey discharge.
Pain is an exclusive symptom of bacterial conjunctivitis when it specifically target the cornea. Otherwise, it generates a sensation of burning and a palpable foreign body. A purulent discharge and conjunctival injection are characteristic for this condition.
Pain and photophobia may be experienced in cases of fungal conjunctivitis affecting the cornea. Even in the absence of corneal damage, it causes pruritus, ocular burning, a viscous, purulent secretion, and injection into the conjunctiva.
The symptoms of viral conjunctivitis include pruritus, ocular redness, a perception of foreign objects, observable conjunctival follicles, lacrimation, and swelling of the eyelids.
Corneal abrasions
Ocular pain in this particular injury is distinguished by a perception of a foreign object. Also prevalent are excessive tearing, photophobia, and conjunctival injection.
Corneal ulcers
Both bacterial and fungal corneal ulcers result in intense ocular discomfort.
Furthermore, they can induce a purulent ocular discharge, adhesive eyelids, sensitivity to light, and reduced visual acuity. Furthermore, bacterial corneal ulcers result in the formation of a grayish white, irregularly shaped ulcer on the cornea, complete constriction of the pupil on one side, and injection into the conjunctiva. Symptoms of fungal corneal ulcers include conjunctival injection, eyelid swelling and redness, and a compact, cloudy, central ulcer encircled by increasingly transparent rings.
Dacryocystitis
Acute dacryocystitis is characterized by pain and discomfort in the vicinity of the tear sac. Further indications include profuse weeping, a purulent secretion, redness of the eyelid, and enlargement in the lacrimal punctum region.
Episcleritis
Eye pain of profound intensity arises when the tissues covering the sclera become irritated. Other associated consequences are photophobia, profuse weeping, and conjunctival edema.
Erythema multiforme major
Ocular discomfort, entropion, trichiasis, purulent conjunctivitis, photophobia, and reduced tear production are often observed symptoms of Erythema multiforme major.
Foreign bodies in the cornea and conjunctiva. Common is abrupt intense pain, although vision typically remains unimpaired. Additional observations include profuse tearing, sensitivity to light, excessive salivation, a feeling of foreign objects, a dark spot on the cornea, and striking injection of the conjunctiva.
Hordeolum (styla)
A hordeolum typically causes localised eye pain that worsens as the cyst develops. Also prevalent are eyelid erythema and edema.
Acute iritis
Eye pain of moderate to severe intensity is accompanied by intense sensitivity to light, significant injection of the conjunctiva, and impaired vision. The restricted pupil may exhibit inadequate response to light.
Lacrimal gland tumor
A lacrimal gland tumor is a malignant growth that typically causes pain in one eye, reduced ability to see clearly, and a certain level of excessive inflammation of the eyelids.
Migraine headache
A migraine can cause so intense pain that it also causes ocular discomfort. Accompanying symptoms may include nausea, vomiting, blurred vision, and sensitivity to light and noise.
Ocular laceration and intraocular foreign bodies
The majority of penetrating eye injuries result in moderate to severe unilateral eye discomfort and reduced visual acuity. May also manifest as eyelid edema, conjunctival injection, and an atypical pupillary reaction.
Optic neuritis (ON)
Ocular optic neuritis is characterized by pain in and around the eye that is triggered by eye movement. Symptoms of severe vision loss and tunnel vision manifest but resolve within a period of 2 to 3 weeks. The pupils have a slow response to direct light but their response to consensual light is normal.
Chronic scleritis
Acute scleritis causes intense eye discomfort and sensitivity, as well as conjunctival injection, a bluish purple sclera, and potentially, sensitivity to light and excessive tearing.
Sclerokeratitis
Scleral and corneal inflammation results in pain, burning, irritation, and sensitivity to light.
Subdural hematoma
Following a head injury, a subdural hematoma often results in intense eye pain and headache. The placement and extent of the hematoma determine the associated neurological symptoms.
Trachoma
Besides causing pain in the afflicted eye, trachoma also results in profuse tears, sensitivity to light, discharge from the eye, swelling and redness of the eyelids, and visible conjunctival follicles.
Uveitis.
Anterior uveitis is characterized by the abrupt advent of intense pain, dramatic injection of the conjunctiva, sensitivity to light, and a small, unresponsive pupil. Posterior uveitis leads to a gradual develop of comparable symptoms, together with a progressive blurring of vision and a deformed shape of the pupil.
Uveitis caused by the lens results in substantial eye pain, injection of the conjunctiva, constriction of the pupils, and major loss of visual acuity. Indeed, the patient typically has sensation limited to light.
Therapeutic interventions
Contact lenses can induce ocular discomfort and a perception of contact with alien objects. Ocular surgery can also result in ocular pain, which can vary from a slight discomfort to a much intense feeling of pounding or stabbing.
Points of Special Consideration
In order to alleviate eye discomfort, instruct the patient to recline in a dimly lit and noise-free setting and shut his eyes. Assess his readiness for diagnostic examinations, such as tonometry and orbital X-rays.
Educational Instruction for Patients
Emphasise the need of adhering to drug therapy guidelines and provide detailed guidance on eye protecting measures. Articulate the need of the patient consistently seeking medical intervention for ocular discomfort.
Pediatric References
The primary aetiologies of childhood eye pain include trauma and infection. Monitor for nonverbal indicators of pain, such as involuntary closure or repeated rubbing.
ocular organs.
Resources for Geriatrics
Glaucoma, a condition that gives rise to ocular discomfort, typically affects individuals in their later years, reaching clinical significance after the age of 40. Commonly, it manifests bilaterally and results in gradually advancing vision impairment, particularly in the periphery visual areas.
Ocular pain can be characterized as a sensory perception of burning, throbbing, aching, or stabbing in or around the eye. It may instead be described as a perception of a foreign body. This symptom exhibits a range of severity, with its duration and precise location offering indications of the underlying diagnosis.
Ocular discomfort frequently arises from corneal abrasion, however it can also be caused by glaucoma or other ocular diseases, trauma, and neurological or systemic problems. The stimulation of nerve endings in the cornea or external eye by any of these may result in the generation of pain.
Urgent medical interventions
To alleviate eye pain caused by a chemical burn, remove any contact lenses and topically irrigate the eye with a minimum of 1 liter of normal saline solution for a duration of 10 minutes. After everting the lids, clean the fornices with a cotton-tipped swab to eliminate any particles or chemicals. Severe eye pain caused by acute angle-closure glaucoma is a critical ocular condition that needs prompt treatment to lower intraocular pressure (IOP). If medication therapy fails to decrease intraocular pressure (IOP), the patient will require laser iridotomy or surgical peripheral iridectomy in order to preserve his retinal function.
Historical Background and Physical Assessment
For eye pain not caused by a chemical burn, obtain a comprehensive medical history from the patient. Elicit a comprehensive description of the pain from the patient. Is it a dull discomfort or a penetrating cramp? For what duration does it endure? Does it present with sensations of burning, itching, or discharge? Determine its commencement time. Does it exhibit greater severity during the morning or late evening? Enquire about any recent traumatic events or surgical procedures, particularly if the patient reports abrupt and intense pain. Does he experience headaches? If such is the case, determine the frequency and timing of their occurrence.
When conducting a physical examination, refrain from manipulating the eye if evidence of trauma is suspected. Thoroughly examine the eyelids and conjunctiva for any signs of excessive redness, irritation, or swelling. Next, assess the eyes for ptosis or exophthalmos disorder. At last, evaluate visual acuity both with and without correction, and analyze extraocular motions. Description of any discharge.
Medical etiology
Angle-closure glaucoma of acute onset. Symptoms of acute angle-closure glaucoma include blurred vision and intense, sudden pain in and around the eye. The pain can be so intense that it induces nausea, vomiting, and abdominal discomfort.
Additional manifestations include halo vision, a rapid decline in visual acuity, and a stationary, unresponsive, slightly enlarged pupil.
Blepharitis
Burning discomfort in both eyelids is accompanied by pruritus, viscous secretion, and injection of conjunctival fluid. Additional results include a perception of a foreign object, ulcerations on the eyelid, and a missing of eyelashes.
Burns
Eye discomfort caused by chemical burns can manifest as abrupt and intense, accompanied by redness and blistering of the face and eyelids, sensitivity to light, excessive sweating, injection of conjunctival fluid, blurred vision, and difficulty in maintaining open eyelids. Ultraviolet radiation burns result in moderate to severe pain approximately 12 hours after exposure, commonly accompanied by photophobia and alterations in eyesight.
Chalazion
Localised discomfort and swelling on the upper or lower eyelid are symptoms of a chalazion. Opening the eyelid exposes conjunctival injection and a little erythematous mass.
Conjunctivitis
All four forms of conjunctivitis result in varying levels of ocular pain and profuse weeping. Allergic conjunctivitis is characterized by mild, burning, bilateral pain, along with itching, conjunctival injection, and a distinctive ropey discharge.
Pain is an exclusive symptom of bacterial conjunctivitis when it specifically target the cornea. Otherwise, it generates a sensation of burning and a palpable foreign body. A purulent discharge and conjunctival injection are characteristic for this condition.
Pain and photophobia may be experienced in cases of fungal conjunctivitis affecting the cornea. Even in the absence of corneal damage, it causes pruritus, ocular burning, a viscous, purulent secretion, and injection into the conjunctiva.
The symptoms of viral conjunctivitis include pruritus, ocular redness, a perception of foreign objects, observable conjunctival follicles, lacrimation, and swelling of the eyelids.
Corneal abrasions
Ocular pain in this particular injury is distinguished by a perception of a foreign object. Also prevalent are excessive tearing, photophobia, and conjunctival injection.
Corneal ulcers
Both bacterial and fungal corneal ulcers result in intense ocular discomfort.
Furthermore, they can induce a purulent ocular discharge, adhesive eyelids, sensitivity to light, and reduced visual acuity. Furthermore, bacterial corneal ulcers result in the formation of a grayish white, irregularly shaped ulcer on the cornea, complete constriction of the pupil on one side, and injection into the conjunctiva. Symptoms of fungal corneal ulcers include conjunctival injection, eyelid swelling and redness, and a compact, cloudy, central ulcer encircled by increasingly transparent rings.
Dacryocystitis
Acute dacryocystitis is characterized by pain and discomfort in the vicinity of the tear sac. Further indications include profuse weeping, a purulent secretion, redness of the eyelid, and enlargement in the lacrimal punctum region.
Episcleritis
Eye pain of profound intensity arises when the tissues covering the sclera become irritated. Other associated consequences are photophobia, profuse weeping, and conjunctival edema.
Erythema multiforme major
Ocular discomfort, entropion, trichiasis, purulent conjunctivitis, photophobia, and reduced tear production are often observed symptoms of Erythema multiforme major.
Foreign bodies in the cornea and conjunctiva. Common is abrupt intense pain, although vision typically remains unimpaired. Additional observations include profuse tearing, sensitivity to light, excessive salivation, a feeling of foreign objects, a dark spot on the cornea, and striking injection of the conjunctiva.
Hordeolum (styla)
A hordeolum typically causes localised eye pain that worsens as the cyst develops. Also prevalent are eyelid erythema and edema.
Acute iritis
Eye pain of moderate to severe intensity is accompanied by intense sensitivity to light, significant injection of the conjunctiva, and impaired vision. The restricted pupil may exhibit inadequate response to light.
Lacrimal gland tumor
A lacrimal gland tumor is a malignant growth that typically causes pain in one eye, reduced ability to see clearly, and a certain level of excessive inflammation of the eyelids.
Migraine headache
A migraine can cause so intense pain that it also causes ocular discomfort. Accompanying symptoms may include nausea, vomiting, blurred vision, and sensitivity to light and noise.
Ocular laceration and intraocular foreign bodies
The majority of penetrating eye injuries result in moderate to severe unilateral eye discomfort and reduced visual acuity. May also manifest as eyelid edema, conjunctival injection, and an atypical pupillary reaction.
Optic neuritis (ON)
Ocular optic neuritis is characterized by pain in and around the eye that is triggered by eye movement. Symptoms of severe vision loss and tunnel vision manifest but resolve within a period of 2 to 3 weeks. The pupils have a slow response to direct light but their response to consensual light is normal.
Chronic scleritis
Acute scleritis causes intense eye discomfort and sensitivity, as well as conjunctival injection, a bluish purple sclera, and potentially, sensitivity to light and excessive tearing.
Sclerokeratitis
Scleral and corneal inflammation results in pain, burning, irritation, and sensitivity to light.
Subdural hematoma
Following a head injury, a subdural hematoma often results in intense eye pain and headache. The placement and extent of the hematoma determine the associated neurological symptoms.
Trachoma
Besides causing pain in the afflicted eye, trachoma also results in profuse tears, sensitivity to light, discharge from the eye, swelling and redness of the eyelids, and visible conjunctival follicles.
Uveitis.
Anterior uveitis is characterized by the abrupt advent of intense pain, dramatic injection of the conjunctiva, sensitivity to light, and a small, unresponsive pupil. Posterior uveitis leads to a gradual develop of comparable symptoms, together with a progressive blurring of vision and a deformed shape of the pupil.
Uveitis caused by the lens results in substantial eye pain, injection of the conjunctiva, constriction of the pupils, and major loss of visual acuity. Indeed, the patient typically has sensation limited to light.
Therapeutic interventions
Contact lenses can induce ocular discomfort and a perception of contact with alien objects. Ocular surgery can also result in ocular pain, which can vary from a slight discomfort to a much intense feeling of pounding or stabbing.
Points of Special Consideration
In order to alleviate eye discomfort, instruct the patient to recline in a dimly lit and noise-free setting and shut his eyes. Assess his readiness for diagnostic examinations, such as tonometry and orbital X-rays.
Educational Instruction for Patients
Emphasise the need of adhering to drug therapy guidelines and provide detailed guidance on eye protecting measures. Articulate the need of the patient consistently seeking medical intervention for ocular discomfort.
Pediatric References
The primary aetiologies of childhood eye pain include trauma and infection. Monitor for nonverbal indicators of pain, such as involuntary closure or repeated rubbing.
ocular organs.
Resources for Geriatrics
Glaucoma, a condition that gives rise to ocular discomfort, typically affects individuals in their later years, reaching clinical significance after the age of 40. Commonly, it manifests bilaterally and results in gradually advancing vision impairment, particularly in the periphery visual areas.
- Published on
Symptoms and Signs – Differential Diagnosis of eye discharge
In the context of conjunctivitis, eye discharge refers to the expulsion of a substance other than tears. This prevalent symptom can manifest in either one or both eyes, resulting in a range of light to abundant discharge. The discharge may exhibit purulent, foamy, mucoid, cheesy, serous, or clear characteristics, or it may be a stringy white discharge. An alternative method of expressing the discharge is by applying pressure to the tear sac, punctum, meibomian glands, or canaliculus.
Ocular discharge often arises from inflammatory and infectious eye diseases, but it can also manifest in specific systemic diseases. The sources of eye discharge are listed below. Due to the potential association of this sign with a vision-threatening diagnosis, it is imperative to promptly evaluate and provide treatment.
Clinical Background and Physical Assessment
Firstly, initiate your assessment by determining the commencement time of the discharge. Does this phenomenon manifest at specific periods of the day or in correlation with particular activities? If the patient reports experiencing discomfort, request him to indicate its precise position and provide a detailed description of its nature. The pain may be characterized as dull, constant, sharp, or stabbing. Are his eyes pruritic or stinging? Do they exhibit excessive tearing? Do they exhibit light sensitivity? Is he experiencing a sensation of anything being inside them?
Following the measurement of the patient's vital signs, meticulously examine the eye discharge. Observe its quantity, hue, and uniformity. Next, assess visual acuity both with and without corrected vision. Conduct an examination of the exterior ocular structures, starting with the unaffected eye to avoid cross-contamination. Monitor for eyelid swelling, clefting, crusts, lesions, and sagging of the eyelids. Subsequently, instruct the patient to blink while you observe for any compromised movement of the eyelid. Consult an exophthalmometer to determine the size of any bulging eyes. Conduct an examination of the six cardinal fields of vision. Inspect for conjunctival injection and follicles, as well as for corneal deformation or white spots.
Sources of Eye Discharge
Discharge from the eye can originate from the tear sac, punctum, meibomian glands, or canaliculi. If the patient presents with a not readily visible discharge, you can extract a sample by gently applying pressure with your fingertip on certain anatomical structures. Next, describe the discharge and identify its origin.
Medical etiology
Conjunctivitis
There are five forms of conjunctivitis that can result in an eye discharge characterized by redness, hyperemia, foreign body sensation, periocular edema, and tears.
Acute allergic conjunctivitis is characterised by a bilateral, white, ropey discharge along with pruritus and tears.
When bacteria infect the conjunctiva, they produce a mild purulent or mucopurulent fluid that can develop adhesive crusts on the eyelids while sleeping. The discharge is often characterized by its greenish or yellowish color and typically manifests in one eye. In addition, the patient may have pruritus, pyrexia, profuse lacrimation, and the perception of an extraneous object located within the eye. Ocular discomfort suggests corneal involvement. Presence of preauricular adenopathy is rare.
Viral conjunctivitis is rather more prevalent than bacterial conjunctivitis. The typical presentation is a clear, serous discharge accompanied by preauricular adenopathy. The medical history includes a rhinorrhea, an upper respiratory tract illness, or recent exposure to an individual exhibiting these symptoms. Acute onset typically occurs unilaterally.
Fungal conjunctivitis results in the production of a plentiful, viscous, purulent secretion that becomes crusty and adhesive on the eyelids. Additional key features include eyelid swelling, pruritus, pyrexia, and lacrimation. Pain and photophobia exclusively manifest when the cornea is affected.
Inclusion conjunctivitis results in minimal mucoid discharge, particularly in the morning, in both eyes, along with pseudoptosis and bulging conjunctival follicles.
Corneal ulcers
A profuse, purulent unilateral eye discharge is produced by bacterial and fungal corneal ulcers. The associated symptoms include crusty, adhesive eyelids, and potentially intense pain, sensitivity to light, and reduced visual acuity. The clinical features of bacterial corneal ulcers include an uneven gray-white spot on the cornea, impaired vision, restriction of the pupil on one side, and injection into the conjunctiva.
The clinical presentation of fungal corneal ulcers includes conjunctival injection, eyelid edema, and erythema. An asymptomatic, compact, pale gray center ulcer forms gradually and may be circumscribed by increasingly transparent rings.
Erythema multiforme major (Stevens-Johnson syndrome)
The defining feature of Stevens-Johnson syndrome is a purulent discharge. Additional visual consequences may encompass intense anterior ocular discomfort, entropion, trichiasis, sensitivity to light, and reduced production of tears. Typical as well are erythematous, urticarial, bullous lesions that immediately appear on the skin.
Herpes zoster ophthalmicus.
A moderate to abundant serous ocular discharge accompanied by severe tearing characterizes herpes zoster ophthalmicus. A thorough examination shows swelling and redness of the eyelids, injection of conjunctival fluid, and a whitish, hazy cornea. In addition, the patient presents with ocular pain and intense unilateral face pain that manifests many days prior to the erupting of vesicles.
Keratoconjunctivitis sicca
Keratoconjunctivitis sicca, also referred to as dry eye syndrome, usually results in an excessive and continuous production of mucoid fluid, accompanied by inadequate tearing. The accompanying signs and symptoms include ocular pain, pruritus, pyrexia, a perception of a foreign object, and sudden injection of the conjunctiva. In addition, the patient may experience ocular closure difficulties.
Meibomianitis
Meibomianitis might present with a persistent foamy eye discharge. Applying pressure to the meibomian glands results in the production of a smooth, creamy yellow secretion. Furthermore, the eyes exhibit persistent redness, accompanied by irritated borders of the eyelids.
Orbital cellulitis
While exophthalmos is the characteristic manifestation of this condition, there may also be a unilateral purulent eye discharge. The associated symptoms include swelling of the eyelids, injection of conjunctiva, headache, pain in the orbits, reduced vision, restricted movement outside the eye, and fever.
Psoriasis vulgaris
Typically, psoriasis vulgaris results in a significant secretion of mucus in both eyes, accompanied by erythema. The distinct sores it generates on the eyelids can propagate into the conjunctiva, resulting in discomfort, profuse tearing, and a perception of a foreign object.
Trachoma
Bilateral eye discharge, together with intense pain, profuse crying, sensitivity to light, swelling of the eyelids, redness, and visible conjunctival follicles, is a characteristic feature of trachoma.
Points of Special Consideration
To soften crusts on the eyes and lashes, apply warm soaks accordingly. Next, delicately cleanse the eyes with a gentle gauze pad. Ensure proper disposal of all spent dressings, tissues, and cotton swabs to avoid the transmission of infection. Instruct the patient to prevent contamination of the unaffected eye and to abstain from sharing pillows, washcloths, eye drops, or eye-based cosmetics with others. Furthermore, ensure to sanitize ophthalmic equipment following its use.
Detail the prescribed diagnostic tests, such as culture and sensitivity procedures, used to detect infectious microorganisms.
Therapeutic Counseling for Patients
Outline strategies to minimize the transmission of infection.
Paediatric Guidelines
The preventative eye medicine silver nitrate often induces eye discomfort and discharge in newborns. Nevertheless, in children, discharges often occur due to ocular damage, eye infection, or upper respiratory tract pneumonia.
In the context of conjunctivitis, eye discharge refers to the expulsion of a substance other than tears. This prevalent symptom can manifest in either one or both eyes, resulting in a range of light to abundant discharge. The discharge may exhibit purulent, foamy, mucoid, cheesy, serous, or clear characteristics, or it may be a stringy white discharge. An alternative method of expressing the discharge is by applying pressure to the tear sac, punctum, meibomian glands, or canaliculus.
Ocular discharge often arises from inflammatory and infectious eye diseases, but it can also manifest in specific systemic diseases. The sources of eye discharge are listed below. Due to the potential association of this sign with a vision-threatening diagnosis, it is imperative to promptly evaluate and provide treatment.
Clinical Background and Physical Assessment
Firstly, initiate your assessment by determining the commencement time of the discharge. Does this phenomenon manifest at specific periods of the day or in correlation with particular activities? If the patient reports experiencing discomfort, request him to indicate its precise position and provide a detailed description of its nature. The pain may be characterized as dull, constant, sharp, or stabbing. Are his eyes pruritic or stinging? Do they exhibit excessive tearing? Do they exhibit light sensitivity? Is he experiencing a sensation of anything being inside them?
Following the measurement of the patient's vital signs, meticulously examine the eye discharge. Observe its quantity, hue, and uniformity. Next, assess visual acuity both with and without corrected vision. Conduct an examination of the exterior ocular structures, starting with the unaffected eye to avoid cross-contamination. Monitor for eyelid swelling, clefting, crusts, lesions, and sagging of the eyelids. Subsequently, instruct the patient to blink while you observe for any compromised movement of the eyelid. Consult an exophthalmometer to determine the size of any bulging eyes. Conduct an examination of the six cardinal fields of vision. Inspect for conjunctival injection and follicles, as well as for corneal deformation or white spots.
Sources of Eye Discharge
Discharge from the eye can originate from the tear sac, punctum, meibomian glands, or canaliculi. If the patient presents with a not readily visible discharge, you can extract a sample by gently applying pressure with your fingertip on certain anatomical structures. Next, describe the discharge and identify its origin.
Medical etiology
Conjunctivitis
There are five forms of conjunctivitis that can result in an eye discharge characterized by redness, hyperemia, foreign body sensation, periocular edema, and tears.
Acute allergic conjunctivitis is characterised by a bilateral, white, ropey discharge along with pruritus and tears.
When bacteria infect the conjunctiva, they produce a mild purulent or mucopurulent fluid that can develop adhesive crusts on the eyelids while sleeping. The discharge is often characterized by its greenish or yellowish color and typically manifests in one eye. In addition, the patient may have pruritus, pyrexia, profuse lacrimation, and the perception of an extraneous object located within the eye. Ocular discomfort suggests corneal involvement. Presence of preauricular adenopathy is rare.
Viral conjunctivitis is rather more prevalent than bacterial conjunctivitis. The typical presentation is a clear, serous discharge accompanied by preauricular adenopathy. The medical history includes a rhinorrhea, an upper respiratory tract illness, or recent exposure to an individual exhibiting these symptoms. Acute onset typically occurs unilaterally.
Fungal conjunctivitis results in the production of a plentiful, viscous, purulent secretion that becomes crusty and adhesive on the eyelids. Additional key features include eyelid swelling, pruritus, pyrexia, and lacrimation. Pain and photophobia exclusively manifest when the cornea is affected.
Inclusion conjunctivitis results in minimal mucoid discharge, particularly in the morning, in both eyes, along with pseudoptosis and bulging conjunctival follicles.
Corneal ulcers
A profuse, purulent unilateral eye discharge is produced by bacterial and fungal corneal ulcers. The associated symptoms include crusty, adhesive eyelids, and potentially intense pain, sensitivity to light, and reduced visual acuity. The clinical features of bacterial corneal ulcers include an uneven gray-white spot on the cornea, impaired vision, restriction of the pupil on one side, and injection into the conjunctiva.
The clinical presentation of fungal corneal ulcers includes conjunctival injection, eyelid edema, and erythema. An asymptomatic, compact, pale gray center ulcer forms gradually and may be circumscribed by increasingly transparent rings.
Erythema multiforme major (Stevens-Johnson syndrome)
The defining feature of Stevens-Johnson syndrome is a purulent discharge. Additional visual consequences may encompass intense anterior ocular discomfort, entropion, trichiasis, sensitivity to light, and reduced production of tears. Typical as well are erythematous, urticarial, bullous lesions that immediately appear on the skin.
Herpes zoster ophthalmicus.
A moderate to abundant serous ocular discharge accompanied by severe tearing characterizes herpes zoster ophthalmicus. A thorough examination shows swelling and redness of the eyelids, injection of conjunctival fluid, and a whitish, hazy cornea. In addition, the patient presents with ocular pain and intense unilateral face pain that manifests many days prior to the erupting of vesicles.
Keratoconjunctivitis sicca
Keratoconjunctivitis sicca, also referred to as dry eye syndrome, usually results in an excessive and continuous production of mucoid fluid, accompanied by inadequate tearing. The accompanying signs and symptoms include ocular pain, pruritus, pyrexia, a perception of a foreign object, and sudden injection of the conjunctiva. In addition, the patient may experience ocular closure difficulties.
Meibomianitis
Meibomianitis might present with a persistent foamy eye discharge. Applying pressure to the meibomian glands results in the production of a smooth, creamy yellow secretion. Furthermore, the eyes exhibit persistent redness, accompanied by irritated borders of the eyelids.
Orbital cellulitis
While exophthalmos is the characteristic manifestation of this condition, there may also be a unilateral purulent eye discharge. The associated symptoms include swelling of the eyelids, injection of conjunctiva, headache, pain in the orbits, reduced vision, restricted movement outside the eye, and fever.
Psoriasis vulgaris
Typically, psoriasis vulgaris results in a significant secretion of mucus in both eyes, accompanied by erythema. The distinct sores it generates on the eyelids can propagate into the conjunctiva, resulting in discomfort, profuse tearing, and a perception of a foreign object.
Trachoma
Bilateral eye discharge, together with intense pain, profuse crying, sensitivity to light, swelling of the eyelids, redness, and visible conjunctival follicles, is a characteristic feature of trachoma.
Points of Special Consideration
To soften crusts on the eyes and lashes, apply warm soaks accordingly. Next, delicately cleanse the eyes with a gentle gauze pad. Ensure proper disposal of all spent dressings, tissues, and cotton swabs to avoid the transmission of infection. Instruct the patient to prevent contamination of the unaffected eye and to abstain from sharing pillows, washcloths, eye drops, or eye-based cosmetics with others. Furthermore, ensure to sanitize ophthalmic equipment following its use.
Detail the prescribed diagnostic tests, such as culture and sensitivity procedures, used to detect infectious microorganisms.
Therapeutic Counseling for Patients
Outline strategies to minimize the transmission of infection.
Paediatric Guidelines
The preventative eye medicine silver nitrate often induces eye discomfort and discharge in newborns. Nevertheless, in children, discharges often occur due to ocular damage, eye infection, or upper respiratory tract pneumonia.

- Published on
Symptoms and Signs – Differential Diagnosis of Exophthalmos
Exophthalmos is the atypical protrusion of one or both eyeballs caused by hemorrhage, edema, or inflammation behind the eye, relaxation of an extraocular muscle, or space-occupying intraorbital lesions and metastatic malignancies. This symptom can manifest abruptly or gradually, resulting in a spectrum of mild to significant protrusion. Periodically, the afflicted eye also exhibits pulsations. The primary etiology of exophthalmos in adults is dysthyroid ocular illness.
Typically, exophthalmos is readily detectable. Yet, the process of retracting the eyelid may imitate exophthalmos even in the absence of protrusion. Equally, ptosis in a single eye may
Depict the opposite eye as exophthalmic in comparison. An exophthalmometer accurately distinguishes these indications by quantifying the protrusion of the eye.
Historical Background and Physical Assessment
Enquire about the initial occurrence of exophthalmos in the patient. Does it manifest as ocular or periocular pain? Does he report a foreign body sensation or dry, pruritic eyes? If such is the case, inquire about the extent of the severity and duration of the problem. Next, inquire about any recent sinus infections or visual impairments. Record the patient's vital signs, giving particular attention to a fever that may be present alongside an eye infection. Next, assess the extent of exophthalmos with an exophthalmometer. See the section on detecting unilateral exophthalmos. Severe bulging of the eyes should be examined for corneal cloudiness, since it could suggest the development of ulcers. Document any ocular discharge and monitor for ptosis. Next, assess visual acuity both with and without correction, and review extraocular motions. Assess the patient's thyroid for enlargement or goiter by palpation.
Investigative Guide for Identifying Unilateral Exophthalmos If one eye of the patient appears more conspicuous than the other, assess both eyes from a superior perspective as seen from above the patient's head. Cast a downward gaze across his face, delicately elevate his eyelids, and analyze the alignment of the corneas with the lower eyelids. Unilateral exophthalmos is indicated by the abnormal protrusion of one eye.
This test should not be conducted if there is suspicion of ocular injury.
Medical etiology
Cavernous sinus thrombosis
Commonly, cavernous sinus thrombosis results in the abrupt development of pulsing, unilateral exophthalmos. Potential concomitant symptoms include eyelid edema, reduced or nonexistent pupillary reflexes, and compromised extraocular movement and visual acuity. Additional characteristics include pyrexia accompanied by chills, papilledema, cephalalgia, emesis, drowsiness, and, infrequently, cerebrovascular accidents.
Dacryoadenitis
Exophthalmos that occurs unilaterally and gradually is the predominant indication of dacryoadenitis. Limited extraocular movements (particularly during elevation and abduction), ptosis, eyelid edema and erythema, conjunctival injection, eye discomfort, and diplopia may also be seen during screening.
Graves’ disease
. Exophthalmos is predominantly seen in individuals diagnosed with Graves' disease, an autoimmune condition that is the primary etiology of hyperthyroidism. Ocular bulging occurs when the tissues and muscles behind the eye enlarge, resulting in the forward displacement of the eyeball within the eye socket. Additional symptoms include heightened tear production, photophobia, ocular lid enlargement, ocular grit perception, and ocular redness. Additional common symptoms include anxiety, exhaustion, enlargement of the thyroid gland (goiter), unexpected weight loss, heightened appetite, sensitivity to heat, and paresthesia.
Haemangioma
Characterised by developing exophthalmos, this orbital tumour is more prevalent in young adults and can manifest as either mild or severe, unilateral or bilateral. Several additional indications and manifestations include ptosis, restricted extraocular movements, and impaired vision.
Lacrimal gland tumor
Retinal exophthalmos often progresses gradually in one eye, resulting in its downward movement towards the nose. Furthermore, the patient may exhibit ptosis, eye deviation, and discomfort.
Leiomyosarcoma
Primarily affecting those aged 45 and above, leiomyosarcoma is distinguished by a gradual progression of unilateral exophthalmos. Additional consequences include diplopia, compromised visual acuity, and sporadic ocular discomfort.
Orbital cellulitis
Unilateral exophthalmos, often caused by sinusitis, is an eye emergency characterized by the abrupt onset of either mild or severe symptoms. A fever, eye pain, headache, malaise, conjunctival injection, weeping, eyelid edema and erythema, purulent discharge, and restricted extraocular movements are all symptoms of orbital cellulitis.
Orbital choristoma
Progressive exophthalmos, a typical indication of this benign brain tumor, might be accompanied with diplopia and impaired vision.
Orbital emphysema
Unilateral exophthalmos is often caused by air seeping from the sinus into the orbit. Upon palpating the globe, crepitation is felt.
Parasite infestation
Parasitic infection often results in painless and gradual exophthalmos in one eye, which can thereafter extend to the other eye. The associated results consist of restricted movement outside the eye, diplopia, eye discomfort, and reduced visual acuity.
Scleritis (posterior)
Scleritis often produces a progressive development of mild to severe unilateral exophthalmos. Additional indications and manifestations encompass intense ocular discomfort, blurred vision, swelling of the retina, restricted movement outside the eye, and reduced ability to understand visual stimuli.
Tharotoxicosis
While exophthalmos is a typical hallmark of thyrotoxicosis, it is not present in most patients. Typically, when it is present, it is bilateral, progressive, and severe. Noteworthy ocular manifestations include ptosis, heightened tear production, delayed opening and closing of the eyelids, sensitivity to light, injection of conjunctival fluid, blurred vision, and reduced visual clarity. Additional symptoms seen include thyroid enlargement, anxiety, intolerance to heat, weight loss despite heightened appetite, perspiration, diarrhoea, tremors, palpitations, and rapid heart rate.
Points of Special Consideration
Typically, exophthalmos conditions induce self-consciousness in patients, thereby necessitating the provision of solitude and emotional support. Shield the afflicted eye against physical injury, particularly, desiccation of the cornea. However, avoid placing a gauze eye pad or any other object over the afflicted eye since its removal may potentially harm the corneal epithelium. Once a slit-lamp examination is deemed necessary, clearly elucidate the method to the patient. If required, direct him to an ophthalmologist for a comprehensive evaluation. The treatment prescribed depends on the underlying cause of exophthalmos. Arrange the patient for hematological examinations, including a thyroid panel and a leukocyte count.
Therapeutic Counseling for Patients
Detail methods for safeguarding the eye against injury, wind, and dust. Detail the correct use of eye lubricants.
Guidelines for Pediatrics
In youngsters about the age of 5, an uncommon malignancy known as optic nerve glioma can lead to exophthalmos. Rhabdomyosarcoma, a prevalent malignancy, typically arises in children aged 4 to 12 and causes the sudden development of exophthalmos. Exophthalmos commonly occurs within Hand-Schüller-Christian syndrome, often accompanied by indications of diabetes insipidus and bone disease.
Exophthalmos is the atypical protrusion of one or both eyeballs caused by hemorrhage, edema, or inflammation behind the eye, relaxation of an extraocular muscle, or space-occupying intraorbital lesions and metastatic malignancies. This symptom can manifest abruptly or gradually, resulting in a spectrum of mild to significant protrusion. Periodically, the afflicted eye also exhibits pulsations. The primary etiology of exophthalmos in adults is dysthyroid ocular illness.
Typically, exophthalmos is readily detectable. Yet, the process of retracting the eyelid may imitate exophthalmos even in the absence of protrusion. Equally, ptosis in a single eye may
Depict the opposite eye as exophthalmic in comparison. An exophthalmometer accurately distinguishes these indications by quantifying the protrusion of the eye.
Historical Background and Physical Assessment
Enquire about the initial occurrence of exophthalmos in the patient. Does it manifest as ocular or periocular pain? Does he report a foreign body sensation or dry, pruritic eyes? If such is the case, inquire about the extent of the severity and duration of the problem. Next, inquire about any recent sinus infections or visual impairments. Record the patient's vital signs, giving particular attention to a fever that may be present alongside an eye infection. Next, assess the extent of exophthalmos with an exophthalmometer. See the section on detecting unilateral exophthalmos. Severe bulging of the eyes should be examined for corneal cloudiness, since it could suggest the development of ulcers. Document any ocular discharge and monitor for ptosis. Next, assess visual acuity both with and without correction, and review extraocular motions. Assess the patient's thyroid for enlargement or goiter by palpation.
Investigative Guide for Identifying Unilateral Exophthalmos If one eye of the patient appears more conspicuous than the other, assess both eyes from a superior perspective as seen from above the patient's head. Cast a downward gaze across his face, delicately elevate his eyelids, and analyze the alignment of the corneas with the lower eyelids. Unilateral exophthalmos is indicated by the abnormal protrusion of one eye.
This test should not be conducted if there is suspicion of ocular injury.
Medical etiology
Cavernous sinus thrombosis
Commonly, cavernous sinus thrombosis results in the abrupt development of pulsing, unilateral exophthalmos. Potential concomitant symptoms include eyelid edema, reduced or nonexistent pupillary reflexes, and compromised extraocular movement and visual acuity. Additional characteristics include pyrexia accompanied by chills, papilledema, cephalalgia, emesis, drowsiness, and, infrequently, cerebrovascular accidents.
Dacryoadenitis
Exophthalmos that occurs unilaterally and gradually is the predominant indication of dacryoadenitis. Limited extraocular movements (particularly during elevation and abduction), ptosis, eyelid edema and erythema, conjunctival injection, eye discomfort, and diplopia may also be seen during screening.
Graves’ disease
. Exophthalmos is predominantly seen in individuals diagnosed with Graves' disease, an autoimmune condition that is the primary etiology of hyperthyroidism. Ocular bulging occurs when the tissues and muscles behind the eye enlarge, resulting in the forward displacement of the eyeball within the eye socket. Additional symptoms include heightened tear production, photophobia, ocular lid enlargement, ocular grit perception, and ocular redness. Additional common symptoms include anxiety, exhaustion, enlargement of the thyroid gland (goiter), unexpected weight loss, heightened appetite, sensitivity to heat, and paresthesia.
Haemangioma
Characterised by developing exophthalmos, this orbital tumour is more prevalent in young adults and can manifest as either mild or severe, unilateral or bilateral. Several additional indications and manifestations include ptosis, restricted extraocular movements, and impaired vision.
Lacrimal gland tumor
Retinal exophthalmos often progresses gradually in one eye, resulting in its downward movement towards the nose. Furthermore, the patient may exhibit ptosis, eye deviation, and discomfort.
Leiomyosarcoma
Primarily affecting those aged 45 and above, leiomyosarcoma is distinguished by a gradual progression of unilateral exophthalmos. Additional consequences include diplopia, compromised visual acuity, and sporadic ocular discomfort.
Orbital cellulitis
Unilateral exophthalmos, often caused by sinusitis, is an eye emergency characterized by the abrupt onset of either mild or severe symptoms. A fever, eye pain, headache, malaise, conjunctival injection, weeping, eyelid edema and erythema, purulent discharge, and restricted extraocular movements are all symptoms of orbital cellulitis.
Orbital choristoma
Progressive exophthalmos, a typical indication of this benign brain tumor, might be accompanied with diplopia and impaired vision.
Orbital emphysema
Unilateral exophthalmos is often caused by air seeping from the sinus into the orbit. Upon palpating the globe, crepitation is felt.
Parasite infestation
Parasitic infection often results in painless and gradual exophthalmos in one eye, which can thereafter extend to the other eye. The associated results consist of restricted movement outside the eye, diplopia, eye discomfort, and reduced visual acuity.
Scleritis (posterior)
Scleritis often produces a progressive development of mild to severe unilateral exophthalmos. Additional indications and manifestations encompass intense ocular discomfort, blurred vision, swelling of the retina, restricted movement outside the eye, and reduced ability to understand visual stimuli.
Tharotoxicosis
While exophthalmos is a typical hallmark of thyrotoxicosis, it is not present in most patients. Typically, when it is present, it is bilateral, progressive, and severe. Noteworthy ocular manifestations include ptosis, heightened tear production, delayed opening and closing of the eyelids, sensitivity to light, injection of conjunctival fluid, blurred vision, and reduced visual clarity. Additional symptoms seen include thyroid enlargement, anxiety, intolerance to heat, weight loss despite heightened appetite, perspiration, diarrhoea, tremors, palpitations, and rapid heart rate.
Points of Special Consideration
Typically, exophthalmos conditions induce self-consciousness in patients, thereby necessitating the provision of solitude and emotional support. Shield the afflicted eye against physical injury, particularly, desiccation of the cornea. However, avoid placing a gauze eye pad or any other object over the afflicted eye since its removal may potentially harm the corneal epithelium. Once a slit-lamp examination is deemed necessary, clearly elucidate the method to the patient. If required, direct him to an ophthalmologist for a comprehensive evaluation. The treatment prescribed depends on the underlying cause of exophthalmos. Arrange the patient for hematological examinations, including a thyroid panel and a leukocyte count.
Therapeutic Counseling for Patients
Detail methods for safeguarding the eye against injury, wind, and dust. Detail the correct use of eye lubricants.
Guidelines for Pediatrics
In youngsters about the age of 5, an uncommon malignancy known as optic nerve glioma can lead to exophthalmos. Rhabdomyosarcoma, a prevalent malignancy, typically arises in children aged 4 to 12 and causes the sudden development of exophthalmos. Exophthalmos commonly occurs within Hand-Schüller-Christian syndrome, often accompanied by indications of diabetes insipidus and bone disease.
- Published on
Symptoms and Signs – Differential Diagnosis of Erythema
Epidermal erythema (Erythroderma)
Dilatation or congestion of blood vessels results in the formation of red scaly skin, also known as erythema, which is the predominant indication of skin inflammation or irritation. Acute erythema can manifest as either localised or generalised and can develop abruptly or gradually. The hue of the skin can vary from a vivid red in individuals with acute disease to a mild violet or brown shade in those with chronic illnesses. Erythema should be distinguished from purpura, which results in redness due to intracutaneous hemorrhage. Application of pressure directly to the skin causes erythema to briefly blanch, while purpura does not.
Erythema sometimes arises from alterations in the arteries, veins, and tiny blood vessels that cause an elevation in intravascular perfusion. Pharmacological agents and neurogenic processes can facilitate increased blood flow into the tiny blood arteries. Furthermore, erythema can arise from trauma and tissue injury, alterations in supporting tissues that enhance the appearance of blood vessels, and certain uncommon diseases. Refer to the Rare Causes of Erythema.
Rare etiologies of erythema Under extraordinary circumstances, the
The patient's erythema may be attributed to one of the following uncommon conditions:
Acute febrile neutrophilic dermatosis is a condition characterized by the development of red lesions on the face, neck, and extremities following a severe fever.
Erythema ab igne is a condition characterised by the production of lacy erythema and telangiectases following exposure to radiant heat.
Erythema chronicum migrans is a skin condition characterized by the appearance of reddened patches and raised bumps on the trunk, upper arms, or thighs following transmission by ticks.
A condition characterized by the presence of wavy bands of erythema, Erythema gyratum repens is often linked to internal cancer.
Pharmacological agents are the primary cause of toxic epidermal necrolysis, a condition characterized by severe, widespread erythema, soreness, bullae development, and exfoliation. This condition can be fatal since it leads to epidermal destruction and its subsequent repercussions.
Urgent medical interventions
If the patient has abrupt and steadily increasing redness accompanied by a fast pulse, difficulty breathing, difficulty speaking clearly, and restlessness, promptly measure his vital signs. The following symptoms may suggest anaphylactic shock. Administer immediate respiratory assistance combined with epinephrine.
Historical Background and Physical Assessment
For erythema unrelated to anaphylaxis, get a comprehensive medical history. Determine the duration and location of the eruption in the patient. Has he had accompanying pain or pruritus? Was he recently afflicted with a fever, upper respiratory tract illness, or joint problem? Has he a previously documented medical history of skin disease or any other illness? Does he or any immediate family member suffer from allergies, asthma, or eczema? Determine whether he has had contact with someone who has or is currently afflicted with a comparable rash. Has he experienced a recent fall or injury in the region affected by erythema?
Record a comprehensive medication history, including recent vaccinations and non-prescription medications. Request information regarding dietary consumption and chemical exposure.
Commence the physical examination by evaluating the scope, dispersion, and severity of redness. Screen for alopecia, edema, and other dermatological abnormalities, including hives, scales, papules, and purpura. The affected area should be examined for warmth and gently palpated to assess for soreness or crepitus.
Cultural Competence
Diagnostically identifying erythema in individuals with darker skin tones can provide greater difficulty. individuals with darker skin may exhibit persistent patches of redness accompanied by blue or purple tints, whereas individuals with lighter skin may merely exhibit persistent areas of redness.
Medical etiology
Allergic reactions
Certain foods, medications, chemicals, and other allergens have the potential to induce an allergic response and erythema. Additionally, a localized allergic response results in hivelike outbreaks and edema.
Anaphylaxis is a potentially fatal illness characterized by a rapid flare-up of the skin known as urticaria. In addition, it causes flushing, facial edema, diaphoresis, weakness, sneezing, bronchospasm accompanying dyspnea and tachypnea, shock characterized by hypotension and cold, clammy skin, and potentially, airway edema accompanied by hoarseness and stridor.
Burns
Initial manifestations of thermal burns are erythema and swelling, which may be succeeded by the development of deep or superficial blisters and other indications of injury that differ according on the extent of the burn. Ultraviolet ray burns, such as sunburn, result in delayed redness and sensitivity on the skin parts that are exposed.
Candidiasis.
Candidasis, a fungal infection, causes erythema and a scaly, papular rash under the breasts and in the axillae, neck, umbilicus, and groin, sometimes referred to as intertrigo. Typically, little pustules develop at the outer edge of the rash, known as satellite pustulosis.
Cellulitis
Edema, soreness, and erythema are symptoms caused by a bacterial infection affecting the skin and subcutaneous tissue.
Dermatitis
Erythema is particularly prevalent in this group of inflammatory diseases. Prior to the formation of tiny papules that may redden, drip, scale, and lichenify, atopic dermatitis is characterized by erythema and severe itching. These most often manifest at the skin folds of the extremities, neck, and eyelids.
A contact dermatitis develops upon contact with an irritant. On exposed skin, it rapidly causes erythema and the formation of vesicles, blisters, or ulcerations.
Seborrheic dermatitis is characterised by the presence of dull red or yellow lesions accompanied by raised skin. Sharply delineated, these lesions are occasionally round in shape and coated with oily scales. Although they often manifest on the scalp, eyebrows, ears, and nasolabial folds, they can also give rise to a butterfly rash on the face which may move to the chest or to skin folds on the trunk. The condition is prevalent in individuals afflicted with human immunodeficiency virus and in newborns (known as cradle cap).
Dermatomyositis
A dusky lilac rash across the face, neck, upper torso, and nail beds is the most prevalent manifestation of Dermatomyositis in women over the age of 50. Gottron's papules, distinctive violet, flat-topped lesions, can manifest on the joints of the fingers.
The erythema annulare centrifugum
Minute, pink infiltrated papules manifest on the trunk, buttocks, and inner thighs, gradually expanding along the edges and resolving in the centrum. Common symptoms include pruritus, desquamation, and fibrosis of the tissues.
Erythema marginatum rheumaticum
Erythema marginatum rheumaticum is a condition linked to rheumatic fever, characterised by superficial, flat, and somewhat firm erythematous plaques. They undergo fast relocation, propagate swiftly, and can persist for extended periods, reoccurring periodically.
Erythema multiforme
The acute inflammatory skin illness known as erythema multiforme arises due to medication sensitivity following infection, namely herpes simplex and Mycoplasma; allergies; and pregnancy. Roughly 50% of the cases are of unknown cause.
The erythema multiforme minor is characterised by distinctive urticarial red-pink iris-shaped localised lesions that have minimal or no involvement of the mucous membranes. Lesions predominantly manifest on the flexor surfaces of the limbs. Burning or itching may manifest before to or concurrently with the formation of a lesion. Crop lesions manifest and persist for a duration of 2 to 3 weeks. Individual lesions become flat or hyperpigmented after one week. Initial manifestations may encompass a little pyrexia, cough, and pharyngitis.
In most cases, erythema multiforme major arises as a result of a medication reaction. It is characterised by extensive symmetrical, bullous lesions that may merge together and includes erosions of the mucosal membranes. Preceding erythema are typically blisters on the lips, tongue, and buccal mucosa, as well as a painful throat. Furthermore, early manifestations of the sickness include a cough, vomiting, diarrhea, coryza, and epistaxis. Subsequent manifestations encompass pyrexia, diplopia, impaired oral intake caused by lesions in the mouth and lips, conjunctivitis resulting from ulceration, vulvitis, and balanitis. Stevens-Johnson syndrome is widely regarded as the most severe form of this disease, characterized by a multisystem dysfunction that can sometimes culminate in death. Furthermore, apart from the aforementioned signs and symptoms, the patient experiences skin exfoliation due to disturbances of bullae, although the extent of affected body surface area is less than 10%. These regions bear a visual resemblance to second-degree heat burns and should be treated accordingly. Fever may increase to Temperature range: 102°F to 104°F (38.9°C to 40°C). The patient may also have tachypnea; a weak, quick pulse; chest pain; malaise; and muscle or joint pain
Erythema nodosum
Erythema nodosum is characterized by the abrupt bilateral appearance of palpable red nodules. These solid, spherical, projecting lesions often manifest in crops on the shins, knees, and ankles, but can also develop on the buttocks, arms, calves, and torso. Further symptoms encompass a slight pyrexia, chills, fatigue, muscular and articular discomfort, and potentially, edema of the feet and ankles. Erythema nodosum occurs commonly in association with a range of disorders, particularly inflammatory bowel disease, sarcoidosis, tuberculosis, as well as streptococcal and fungal infections.
Gout
It is typified by tight and erythematous skin over an inflammatory, edematous joint, and typically affects men aged 40 to 60.
Lupus erythematosus
The clinical presentation of discoid and systemic lupus erythematosus (SLE) often includes a distinctive butterfly rash. This erythematous eruption can vary in appearance from a slight redness with swelling to a rough, well defined, macular rash with patches that may extend to the forehead, chin, ears, chest, and other areas of the body exposed to solar radiation.
Patients with discoid lupus erythematosus may develop telangiectasia, hyperpigmentation, ear and nose deformities, as well as lesions in the mouth, tongue, and eyelids.
Symptoms of Systemic Lupus Erythematosus (SLE) include sudden redness of the skin, sensitivity to light, and ulcers on mucous membranes, particularly in the nose and mouth. The hands may exhibit mottled redness, accompanied by edema around the nails and macular reddish purple lesions on the fingers. In addition to purpura, petechiae, ecchymoses, and urticaria, telangiectasia manifests at the base of the nails or eyelids. Co-occurrence of joint pain and stiffness is frequent. Additional manifestations differ depending on the specific physiological systems impacted, but commonly encompass a mild fever, general malaise, debility, headache, joint pain, arthritis, depression, lymph node involvement, exhaustion, weight loss, loss of appetite, nausea, vomiting, diarrhea, and constipation.
Psoriasis
The elbows, knees, chest, scalp, and intergluteal folds are often typical sites of silvery white scales covering a thicker erythematous base. Fingernails may develop increased thickness and pitted appearance.
Raynaud's illness
Commonly, the skin on the hands and feet undergoes blanching and cooling in contact with cold and stress. Later, it turns a warm and reddish red color.
Rosaceae
An initial development of scattered redness occurs in the central region of the face, followed by superficial telangiectases, papules, pustules, and nodules. Rhinophyma tends to manifest on the inferior aspect of the nasal cavity.
Rubella
In this disease, flat solitary lesions usually merge together to create a blotchy pink erythematous rash that quickly spreads to the trunk and extremities. Small red lesions, known as Forschheimer spots, may sometimes develop on the soft palate. Lesions resolve typically within 4 to 5 days. The eruption often occurs after a fever (reaching 102°F [38.9°C]), a headache, fatigue, a sore throat, a gritty eye feeling, lymph nodenopathy, joint discomfort, and coryza.
Other Causes
Drugs. Many drugs commonly cause erythema.
Presume drug-induced erythema in a patient who exhibits this symptom within one week of initiating medication dosage. While erythematous lesions might exhibit variations in size, shape, kind, and quantity, they consistently manifest abruptly and symmetrically across the trunk and inner arms.
Certain medications, namely barbiturates, hormonal contraceptives, salicylates, sulfonamides, and tetracycline, have the potential to induce a protracted drug eruption. During this particular reaction, lesions might manifest on any anatomical region and then detach within a few days, resulting in a reddish purple colored appearance. Repetitive medication administration leads to the recurrence of the initial lesions and the formation of new ones.
Provide instructions to the patient with pruritic skin to refrain from scratching and to anticipate the use of soothing baths or open wet bandages containing starch, bran, or sodium bicarbonate. Additionally, deliver an antihistamine and analgesic as necessary. Instruct a patient experiencing leg erythema to maintain an elevated position of his legs above the level of the heart. To alleviate pain, edema, and erythema in a burn patient with erythema, either submerge the affected area in cold water or implement a cold water-soaked sheet. To manage a patient on extended bed rest, adjust their position according to instructions, examine the skin for signs of pressure-induced redness (stage 1 ulcer), and alleviate symptoms by using specialized foam cushions.
Perform necessary preparations for the patient to undergo diagnostic procedures, including skin biopsies for the detection of malignant lesions, cultures for the identification of pathogenic organisms, and sensitivity studies to verify allergies.
Administering the fruit pulp of Ginkgo biloba might result in intense redness and swelling of the mouth, as well as quick development of vesicles. St. John’s wort might induce increased sensitivity to sunlight, leading to redness or scorching of the skin.
Radiotherapy and other therapeutic interventions. Within a 24-hour period, radiation therapy might cause dull redness and excessive swelling. Following the resolution of the redness, the skin turns pale brown and slightly scaly. Erythema can also be caused by any therapy that elicits an allergic response.
Points of Special Consideration
Because erythema can lead to fluid loss, it is important to closely monitor and replenish fluids and electrolytes, particularly in patients with burns or extensive erythema. Administer all drugs only once the underlying reason of the redness has been determined. Following that, anticipate the administration of an antibiotic and either a topical or systemic corticosteroid.
Therapeutic Counseling for Patients
The patient should be instructed in identifying the indications and manifestations of exacerbations of the illness. The significance of minimizing sun exposure and applying sunscreen should be emphasized. Teach the patient techniques to alleviate pruritus.
Guidelines for Pediatrics
Neonatal rash, technically known as erythema toxicum neonatorum, is a pink papular rash that typically starts within the first 4 days after delivery and resolves on its own by the 10th day. Erythema can also progress in neonates and infants as a result of infections and other medical conditions. Specifically, candidiasis can cause the formation of thick white lesions on a red base of the oral mucosa, as well as a diaper rash characterized by beefy red erythema.
Rosacea, rubeola, scarlet fever, granuloma annulare, and cutis marmorata are additional conditions that can produce erythema in children. Neonatals and infants exhibiting erythema and fever should be evaluated for hospital admission for additional clinical assessment.
A Guide to Geriatrics
Geriatric patients often exhibit clearly defined purple macules or patches, typically located on the dorsal surfaces of the hands and forearms. Referred to as actinic purpura, this disorder arises from the retrograde flow of blood via delicate capillaries. The lesions spontaneously resolve.
Epidermal erythema (Erythroderma)
Dilatation or congestion of blood vessels results in the formation of red scaly skin, also known as erythema, which is the predominant indication of skin inflammation or irritation. Acute erythema can manifest as either localised or generalised and can develop abruptly or gradually. The hue of the skin can vary from a vivid red in individuals with acute disease to a mild violet or brown shade in those with chronic illnesses. Erythema should be distinguished from purpura, which results in redness due to intracutaneous hemorrhage. Application of pressure directly to the skin causes erythema to briefly blanch, while purpura does not.
Erythema sometimes arises from alterations in the arteries, veins, and tiny blood vessels that cause an elevation in intravascular perfusion. Pharmacological agents and neurogenic processes can facilitate increased blood flow into the tiny blood arteries. Furthermore, erythema can arise from trauma and tissue injury, alterations in supporting tissues that enhance the appearance of blood vessels, and certain uncommon diseases. Refer to the Rare Causes of Erythema.
Rare etiologies of erythema Under extraordinary circumstances, the
The patient's erythema may be attributed to one of the following uncommon conditions:
Acute febrile neutrophilic dermatosis is a condition characterized by the development of red lesions on the face, neck, and extremities following a severe fever.
Erythema ab igne is a condition characterised by the production of lacy erythema and telangiectases following exposure to radiant heat.
Erythema chronicum migrans is a skin condition characterized by the appearance of reddened patches and raised bumps on the trunk, upper arms, or thighs following transmission by ticks.
A condition characterized by the presence of wavy bands of erythema, Erythema gyratum repens is often linked to internal cancer.
Pharmacological agents are the primary cause of toxic epidermal necrolysis, a condition characterized by severe, widespread erythema, soreness, bullae development, and exfoliation. This condition can be fatal since it leads to epidermal destruction and its subsequent repercussions.
Urgent medical interventions
If the patient has abrupt and steadily increasing redness accompanied by a fast pulse, difficulty breathing, difficulty speaking clearly, and restlessness, promptly measure his vital signs. The following symptoms may suggest anaphylactic shock. Administer immediate respiratory assistance combined with epinephrine.
Historical Background and Physical Assessment
For erythema unrelated to anaphylaxis, get a comprehensive medical history. Determine the duration and location of the eruption in the patient. Has he had accompanying pain or pruritus? Was he recently afflicted with a fever, upper respiratory tract illness, or joint problem? Has he a previously documented medical history of skin disease or any other illness? Does he or any immediate family member suffer from allergies, asthma, or eczema? Determine whether he has had contact with someone who has or is currently afflicted with a comparable rash. Has he experienced a recent fall or injury in the region affected by erythema?
Record a comprehensive medication history, including recent vaccinations and non-prescription medications. Request information regarding dietary consumption and chemical exposure.
Commence the physical examination by evaluating the scope, dispersion, and severity of redness. Screen for alopecia, edema, and other dermatological abnormalities, including hives, scales, papules, and purpura. The affected area should be examined for warmth and gently palpated to assess for soreness or crepitus.
Cultural Competence
Diagnostically identifying erythema in individuals with darker skin tones can provide greater difficulty. individuals with darker skin may exhibit persistent patches of redness accompanied by blue or purple tints, whereas individuals with lighter skin may merely exhibit persistent areas of redness.
Medical etiology
Allergic reactions
Certain foods, medications, chemicals, and other allergens have the potential to induce an allergic response and erythema. Additionally, a localized allergic response results in hivelike outbreaks and edema.
Anaphylaxis is a potentially fatal illness characterized by a rapid flare-up of the skin known as urticaria. In addition, it causes flushing, facial edema, diaphoresis, weakness, sneezing, bronchospasm accompanying dyspnea and tachypnea, shock characterized by hypotension and cold, clammy skin, and potentially, airway edema accompanied by hoarseness and stridor.
Burns
Initial manifestations of thermal burns are erythema and swelling, which may be succeeded by the development of deep or superficial blisters and other indications of injury that differ according on the extent of the burn. Ultraviolet ray burns, such as sunburn, result in delayed redness and sensitivity on the skin parts that are exposed.
Candidiasis.
Candidasis, a fungal infection, causes erythema and a scaly, papular rash under the breasts and in the axillae, neck, umbilicus, and groin, sometimes referred to as intertrigo. Typically, little pustules develop at the outer edge of the rash, known as satellite pustulosis.
Cellulitis
Edema, soreness, and erythema are symptoms caused by a bacterial infection affecting the skin and subcutaneous tissue.
Dermatitis
Erythema is particularly prevalent in this group of inflammatory diseases. Prior to the formation of tiny papules that may redden, drip, scale, and lichenify, atopic dermatitis is characterized by erythema and severe itching. These most often manifest at the skin folds of the extremities, neck, and eyelids.
A contact dermatitis develops upon contact with an irritant. On exposed skin, it rapidly causes erythema and the formation of vesicles, blisters, or ulcerations.
Seborrheic dermatitis is characterised by the presence of dull red or yellow lesions accompanied by raised skin. Sharply delineated, these lesions are occasionally round in shape and coated with oily scales. Although they often manifest on the scalp, eyebrows, ears, and nasolabial folds, they can also give rise to a butterfly rash on the face which may move to the chest or to skin folds on the trunk. The condition is prevalent in individuals afflicted with human immunodeficiency virus and in newborns (known as cradle cap).
Dermatomyositis
A dusky lilac rash across the face, neck, upper torso, and nail beds is the most prevalent manifestation of Dermatomyositis in women over the age of 50. Gottron's papules, distinctive violet, flat-topped lesions, can manifest on the joints of the fingers.
The erythema annulare centrifugum
Minute, pink infiltrated papules manifest on the trunk, buttocks, and inner thighs, gradually expanding along the edges and resolving in the centrum. Common symptoms include pruritus, desquamation, and fibrosis of the tissues.
Erythema marginatum rheumaticum
Erythema marginatum rheumaticum is a condition linked to rheumatic fever, characterised by superficial, flat, and somewhat firm erythematous plaques. They undergo fast relocation, propagate swiftly, and can persist for extended periods, reoccurring periodically.
Erythema multiforme
The acute inflammatory skin illness known as erythema multiforme arises due to medication sensitivity following infection, namely herpes simplex and Mycoplasma; allergies; and pregnancy. Roughly 50% of the cases are of unknown cause.
The erythema multiforme minor is characterised by distinctive urticarial red-pink iris-shaped localised lesions that have minimal or no involvement of the mucous membranes. Lesions predominantly manifest on the flexor surfaces of the limbs. Burning or itching may manifest before to or concurrently with the formation of a lesion. Crop lesions manifest and persist for a duration of 2 to 3 weeks. Individual lesions become flat or hyperpigmented after one week. Initial manifestations may encompass a little pyrexia, cough, and pharyngitis.
In most cases, erythema multiforme major arises as a result of a medication reaction. It is characterised by extensive symmetrical, bullous lesions that may merge together and includes erosions of the mucosal membranes. Preceding erythema are typically blisters on the lips, tongue, and buccal mucosa, as well as a painful throat. Furthermore, early manifestations of the sickness include a cough, vomiting, diarrhea, coryza, and epistaxis. Subsequent manifestations encompass pyrexia, diplopia, impaired oral intake caused by lesions in the mouth and lips, conjunctivitis resulting from ulceration, vulvitis, and balanitis. Stevens-Johnson syndrome is widely regarded as the most severe form of this disease, characterized by a multisystem dysfunction that can sometimes culminate in death. Furthermore, apart from the aforementioned signs and symptoms, the patient experiences skin exfoliation due to disturbances of bullae, although the extent of affected body surface area is less than 10%. These regions bear a visual resemblance to second-degree heat burns and should be treated accordingly. Fever may increase to Temperature range: 102°F to 104°F (38.9°C to 40°C). The patient may also have tachypnea; a weak, quick pulse; chest pain; malaise; and muscle or joint pain
Erythema nodosum
Erythema nodosum is characterized by the abrupt bilateral appearance of palpable red nodules. These solid, spherical, projecting lesions often manifest in crops on the shins, knees, and ankles, but can also develop on the buttocks, arms, calves, and torso. Further symptoms encompass a slight pyrexia, chills, fatigue, muscular and articular discomfort, and potentially, edema of the feet and ankles. Erythema nodosum occurs commonly in association with a range of disorders, particularly inflammatory bowel disease, sarcoidosis, tuberculosis, as well as streptococcal and fungal infections.
Gout
It is typified by tight and erythematous skin over an inflammatory, edematous joint, and typically affects men aged 40 to 60.
Lupus erythematosus
The clinical presentation of discoid and systemic lupus erythematosus (SLE) often includes a distinctive butterfly rash. This erythematous eruption can vary in appearance from a slight redness with swelling to a rough, well defined, macular rash with patches that may extend to the forehead, chin, ears, chest, and other areas of the body exposed to solar radiation.
Patients with discoid lupus erythematosus may develop telangiectasia, hyperpigmentation, ear and nose deformities, as well as lesions in the mouth, tongue, and eyelids.
Symptoms of Systemic Lupus Erythematosus (SLE) include sudden redness of the skin, sensitivity to light, and ulcers on mucous membranes, particularly in the nose and mouth. The hands may exhibit mottled redness, accompanied by edema around the nails and macular reddish purple lesions on the fingers. In addition to purpura, petechiae, ecchymoses, and urticaria, telangiectasia manifests at the base of the nails or eyelids. Co-occurrence of joint pain and stiffness is frequent. Additional manifestations differ depending on the specific physiological systems impacted, but commonly encompass a mild fever, general malaise, debility, headache, joint pain, arthritis, depression, lymph node involvement, exhaustion, weight loss, loss of appetite, nausea, vomiting, diarrhea, and constipation.
Psoriasis
The elbows, knees, chest, scalp, and intergluteal folds are often typical sites of silvery white scales covering a thicker erythematous base. Fingernails may develop increased thickness and pitted appearance.
Raynaud's illness
Commonly, the skin on the hands and feet undergoes blanching and cooling in contact with cold and stress. Later, it turns a warm and reddish red color.
Rosaceae
An initial development of scattered redness occurs in the central region of the face, followed by superficial telangiectases, papules, pustules, and nodules. Rhinophyma tends to manifest on the inferior aspect of the nasal cavity.
Rubella
In this disease, flat solitary lesions usually merge together to create a blotchy pink erythematous rash that quickly spreads to the trunk and extremities. Small red lesions, known as Forschheimer spots, may sometimes develop on the soft palate. Lesions resolve typically within 4 to 5 days. The eruption often occurs after a fever (reaching 102°F [38.9°C]), a headache, fatigue, a sore throat, a gritty eye feeling, lymph nodenopathy, joint discomfort, and coryza.
Other Causes
Drugs. Many drugs commonly cause erythema.
Presume drug-induced erythema in a patient who exhibits this symptom within one week of initiating medication dosage. While erythematous lesions might exhibit variations in size, shape, kind, and quantity, they consistently manifest abruptly and symmetrically across the trunk and inner arms.
Certain medications, namely barbiturates, hormonal contraceptives, salicylates, sulfonamides, and tetracycline, have the potential to induce a protracted drug eruption. During this particular reaction, lesions might manifest on any anatomical region and then detach within a few days, resulting in a reddish purple colored appearance. Repetitive medication administration leads to the recurrence of the initial lesions and the formation of new ones.
Provide instructions to the patient with pruritic skin to refrain from scratching and to anticipate the use of soothing baths or open wet bandages containing starch, bran, or sodium bicarbonate. Additionally, deliver an antihistamine and analgesic as necessary. Instruct a patient experiencing leg erythema to maintain an elevated position of his legs above the level of the heart. To alleviate pain, edema, and erythema in a burn patient with erythema, either submerge the affected area in cold water or implement a cold water-soaked sheet. To manage a patient on extended bed rest, adjust their position according to instructions, examine the skin for signs of pressure-induced redness (stage 1 ulcer), and alleviate symptoms by using specialized foam cushions.
Perform necessary preparations for the patient to undergo diagnostic procedures, including skin biopsies for the detection of malignant lesions, cultures for the identification of pathogenic organisms, and sensitivity studies to verify allergies.
Administering the fruit pulp of Ginkgo biloba might result in intense redness and swelling of the mouth, as well as quick development of vesicles. St. John’s wort might induce increased sensitivity to sunlight, leading to redness or scorching of the skin.
Radiotherapy and other therapeutic interventions. Within a 24-hour period, radiation therapy might cause dull redness and excessive swelling. Following the resolution of the redness, the skin turns pale brown and slightly scaly. Erythema can also be caused by any therapy that elicits an allergic response.
Points of Special Consideration
Because erythema can lead to fluid loss, it is important to closely monitor and replenish fluids and electrolytes, particularly in patients with burns or extensive erythema. Administer all drugs only once the underlying reason of the redness has been determined. Following that, anticipate the administration of an antibiotic and either a topical or systemic corticosteroid.
Therapeutic Counseling for Patients
The patient should be instructed in identifying the indications and manifestations of exacerbations of the illness. The significance of minimizing sun exposure and applying sunscreen should be emphasized. Teach the patient techniques to alleviate pruritus.
Guidelines for Pediatrics
Neonatal rash, technically known as erythema toxicum neonatorum, is a pink papular rash that typically starts within the first 4 days after delivery and resolves on its own by the 10th day. Erythema can also progress in neonates and infants as a result of infections and other medical conditions. Specifically, candidiasis can cause the formation of thick white lesions on a red base of the oral mucosa, as well as a diaper rash characterized by beefy red erythema.
Rosacea, rubeola, scarlet fever, granuloma annulare, and cutis marmorata are additional conditions that can produce erythema in children. Neonatals and infants exhibiting erythema and fever should be evaluated for hospital admission for additional clinical assessment.
A Guide to Geriatrics
Geriatric patients often exhibit clearly defined purple macules or patches, typically located on the dorsal surfaces of the hands and forearms. Referred to as actinic purpura, this disorder arises from the retrograde flow of blood via delicate capillaries. The lesions spontaneously resolve.
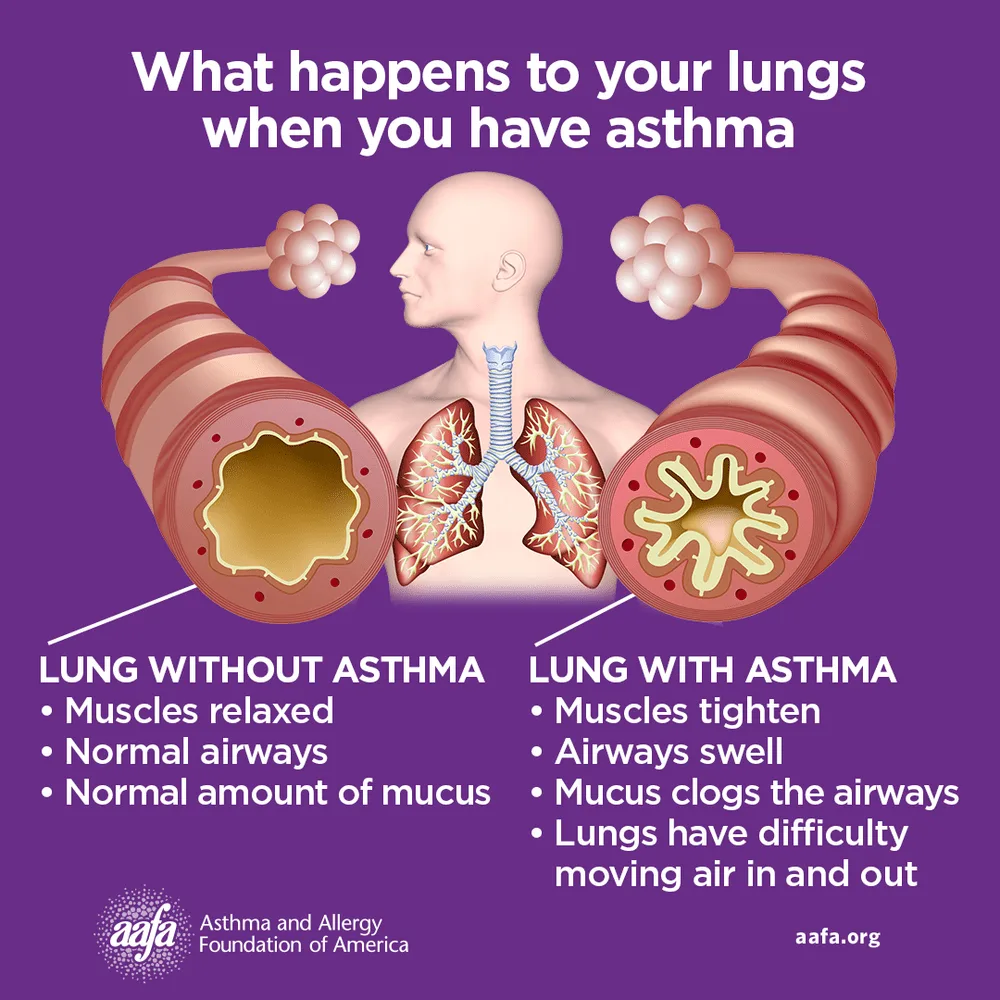
- Published on
Symptoms and Signs – Differential Diagnosis of Edema of the Face
Facial edema include both localised bulging, such as around the eyes, and more widespread facial swelling that can reach the neck and upper arms. This indication, which can be occasionally painful, may manifest either gradually or suddenly. In some cases, it occurs before the development of peripheral or widespread edema. Identifying mild edema can be challenging; the patient or an observer of their physical appearance may report it before it becomes apparent during the evaluation.
A facial edema occurs when the hydrostatic and osmotic pressures that control the flow of fluid between the arteries, veins, and lymphatics are disturbed. Please refer to Understanding Fluid Balance on page 278. It may arise from venous, inflammatory, and specific systemic diseases; trauma; allergy; malnutrition; or the consequences of certain medications, diagnostic procedures, and clinical interventions.
Urgent medical interventions
If the patient presents with facial edema related to burns or if he states recent contact with an allergen, promptly assess his respiratory condition. Furthermore, edema might impact his upper airway, leading to a potentially fatal blockage. The administration of epinephrine is recommended in the presence of audible wheezing, inspiratory stridor, or other indications of respiratory distress. For the patient experiencing acute distress, characterized by the absence of breath sounds and cyanosis, it may be necessary to perform tracheal intubation, cricothyroidotomy, or tracheotomy. Always provide oxygen therapy.
Historical Background and Physical Assessment
Assuming the patient is not experiencing significant distress, obtain his medical history. Determine whether facial edema manifested abruptly or gradually. Do its symptoms manifest more prominently in the early morning or deteriorate throughout the course of the day? Hs the patient experienced weight gain? If such is the case, what amounts and for what duration? Has he observed any alteration in the color or volume of his urine? Within his dietary intake? Obtain a medical history of drug use and inquire about any recent facial injuries.
Starting the physical examination, describe the edema. Does it exhibit localization to a specific region of the face, or does it manifest itself throughout the entire face or other anatomical regions? Ascertain whether the edema is pitting or non-pitting, and assess its level of severity.Next, measure the patient's vital signs and evaluate his neurological condition. Review the oral cavity to assess dental cleanliness and detect indications of infection. Examination of the oropharynx to detect any enlargement of the soft tissues.
Diagnosing Angioneurotic Edema
Angioneurotic edema in the lips, eyelids, and tongue often occurs as a consequence of an allergic response. It is marked by the sudden appearance of painless, nonpitting, swelling beneath the skin that often disappears within 1 to 2 days. This form of edema can also affect the hands, feet, genitalia, and vital organs; laryngeal edema can lead to potentially fatal blockage of the airways.
Medical etiology
Allergic reaction. Local alergic responses and anaphylaxis may be characterized by facial edema. Patients with life-threatening anaphylaxis may develop angioneurotic facial edema accompanied by urticaria and flushing. Refer to the section on Recognizing Angioneurotic Edema. Airway edema symptoms include hoarseness, stridor, bronchospasm accompanied by dyspnea and tachypnea. Symptoms of shock, such as low blood pressure and cold, moist skin, may also manifest. Facial edema, erythema, and urticaria are symptoms of a localized inflammation.
Cavernous sinus thrombosis
An uncommon but severe condition, cavernous sinus thrombosis may initially present with unilateral swelling that rapidly advances to bilateral swelling of the forehead, base of the nose, and eyelids. Additionally, it can cause chills, pyrexia, cephalalgia, and ocular discomfort.
Chalazion
A chalazion results in localised edema and sensitivity of the afflicted eyelid, accompanied by a little erythematous proliferation on the conjunctival surface.
conjunctivitis
Inflammation of the conjunctiva leads to swelling of the eyelids, profuse tears, and pruritic, scorching eyes. Upon examination, a viscous purulent fluid, crusty eyelids, and conjunctival injection are observed. Involvement of the cornea results in photophobia and pain.
Dacryoadenitis
Dacryoadenitis is characterized by intense swelling around the eye, typically accompanied by conjunctival injection, purulent discharge, and temporal pain.
Dacryocystitis
Chronic inflammation of the lacrimal sac leads to noticeable swelling of the eyelids and persistent weeping. In acute presentations, there is discomfort and sensitivity in the vicinity of the tear sac along with purulent discharge.
Facial burns
Profound edema resulting from burns can significantly hinder respiration. Other observations include jaundiced nasal hairs, erythematous mucosa, sputum with a sooty appearance, and indications of respiratory difficulty, such as stridor during inspiration.
Facial trauma
The magnitude of edema differs depending on the nature of the damage. For instance, a contusion might result in localised swelling, while a fracture of the nose or maxilla leads to the development of more widespread swelling. Associated characteristics are also contingent upon the kind of the injury.
Herpes zoster ophthalmicus (shingles)
Edematous and red eyelids caused by shingles are often accompanied by profuse tearing and a serous discharge. Intense unilateral face pain may manifest many days prior to the eruption of vesicles.
Myxedema
Myxedema ultimately leads to widespread face swelling, flaky, dry skin, hair loss or coarsening, and other symptoms of hypothyroidism.
Nephrotic syndrome
Frequently the initial indication of nephrotic disease, periorbital edema occurs before dependant and abdominal edema. Weight gain, nausea, anorexia, lethargy, weariness, and pallor are among the associated symptoms.
Orbital cellulitis
Acute periorbital edema is a characteristic feature of orbital cellulitis. Conjunctival injection, decreased extraocular movements, fever, and severe orbital pain may accompany a unilateral purulent discharge.
Preeclampsia
Early manifestation of preeclampsia is the presence of edema in the face, hands, and ankles. Additional features include significant weight increase, a strong headache, impaired vision, high blood pressure, and pain in the middle and lower abdomen.
Rhinitis (allergic)
Rhinositis is characterised by red and edematous eyelids, paroxysmal sneezing, itchy nose and eyes, and persistent, watery rhinorrhea. In addition, the patient may progress to nasal congestion, profuse weeping, a headache, sinus pain, and occasionally, malaise and a fever.
Sinusitis
Frontal sinusitis results in swelling of the forehead and eyelids. In addition to malaise, gingival swelling, and trismus, maxillary sinusitis causes edema in the maxillary region. Both forms are additionally characterized by facial discomfort, pyrexia, nasal congestion, purulent nasal secretion, and erythematous, vascularized nasal mucosa.
Superior vena cava syndrome
Symptoms of superior vena cava syndrome include progressive swelling of the face and neck, along with distension of the thoracic or jugular veins. Furthermore, it induces symptoms of the central nervous system, including headache, visual impairments, and vertigo.
Trachoma
Trachoma is characterized by tissue swelling in the eyelid and conjunctiva, along with symptoms such as eye pain, excessive crying, sensitivity to light, and eyes discharge. Upon examination, an inflammatory preauricular node and palpable conjunctival follicles are observed.
Trichinosis
Trichinosis is an uncommon infectious condition characterized by the abrupt development of swelling in the eyelids accompanied by a fever ranging from 102°F to 104°F (38.9°C to 40°C), conjunctivitis, muscle soreness, pruritus and irritation of the skin, perspiration, skin lesions, and altered mental state.
Additional Factors
Medical diagnostic testing. Facial edema may be precipitated by an allergic response to contrast media employed in radiologic examinations.
Substances
Chronic administration of glucocorticoids might result in facial edema. Any pharmaceutical substance that elicits an allergic response (such as aspirin, antipyretics, penicillin, and sulfa preparations) can equally produce the same outcome.
Surgeries and blood transfusions. Cervical, nasal, or mandibular surgery can result in facial edema, as can a blood transfusion that triggers an allergic response.
Botanical Alert
Consumption of the fruit pulp of Ginkgo biloba can result in intense redness and swelling, as well as the quick development of vesicles. The medications feverfew and Chrysanthemum parthenium can induce lip edema, tongue discomfort, and oral ulcers. Administering licorice before menstruation may result in face edema, water retention, and bloating.
Points of Special Consideration
Administer a pain-relieving medication and apply a topical treatment to alleviate itching. Should it not be contraindicated, administer cold compresses to the patient's eyes in order to reduce edema. Elevate the head of the bed to facilitate the drainage of the accumulated fluid. Commonly, urine and blood tests are requested to aid in the diagnosis of the underlying trigger of face edema.
Educational Instruction for Patients
Detail the hazards associated with delayed allergy symptoms and identify the specific signs and symptoms that should be reported. Elaborate on strategies to prevent allergies and insect bites or stings. Stress the need of possessing an anaphylaxis kit and a medical identification bracelet.
Guidelines for Pediatric Populations
Pediatric periorbital tissue pressure typically exhibits lower values compared to adults. Therefore, children have a higher probability of developing periorbital edema. Indeed, periorbital edema is more prevalent than peripheral edema in children suffering from conditions such as heart failure and acute glomerulonephritis. Furthermore, pertussis can induce periorbital edema.
Facial edema include both localised bulging, such as around the eyes, and more widespread facial swelling that can reach the neck and upper arms. This indication, which can be occasionally painful, may manifest either gradually or suddenly. In some cases, it occurs before the development of peripheral or widespread edema. Identifying mild edema can be challenging; the patient or an observer of their physical appearance may report it before it becomes apparent during the evaluation.
A facial edema occurs when the hydrostatic and osmotic pressures that control the flow of fluid between the arteries, veins, and lymphatics are disturbed. Please refer to Understanding Fluid Balance on page 278. It may arise from venous, inflammatory, and specific systemic diseases; trauma; allergy; malnutrition; or the consequences of certain medications, diagnostic procedures, and clinical interventions.
Urgent medical interventions
If the patient presents with facial edema related to burns or if he states recent contact with an allergen, promptly assess his respiratory condition. Furthermore, edema might impact his upper airway, leading to a potentially fatal blockage. The administration of epinephrine is recommended in the presence of audible wheezing, inspiratory stridor, or other indications of respiratory distress. For the patient experiencing acute distress, characterized by the absence of breath sounds and cyanosis, it may be necessary to perform tracheal intubation, cricothyroidotomy, or tracheotomy. Always provide oxygen therapy.
Historical Background and Physical Assessment
Assuming the patient is not experiencing significant distress, obtain his medical history. Determine whether facial edema manifested abruptly or gradually. Do its symptoms manifest more prominently in the early morning or deteriorate throughout the course of the day? Hs the patient experienced weight gain? If such is the case, what amounts and for what duration? Has he observed any alteration in the color or volume of his urine? Within his dietary intake? Obtain a medical history of drug use and inquire about any recent facial injuries.
Starting the physical examination, describe the edema. Does it exhibit localization to a specific region of the face, or does it manifest itself throughout the entire face or other anatomical regions? Ascertain whether the edema is pitting or non-pitting, and assess its level of severity.Next, measure the patient's vital signs and evaluate his neurological condition. Review the oral cavity to assess dental cleanliness and detect indications of infection. Examination of the oropharynx to detect any enlargement of the soft tissues.
Diagnosing Angioneurotic Edema
Angioneurotic edema in the lips, eyelids, and tongue often occurs as a consequence of an allergic response. It is marked by the sudden appearance of painless, nonpitting, swelling beneath the skin that often disappears within 1 to 2 days. This form of edema can also affect the hands, feet, genitalia, and vital organs; laryngeal edema can lead to potentially fatal blockage of the airways.
Medical etiology
Allergic reaction. Local alergic responses and anaphylaxis may be characterized by facial edema. Patients with life-threatening anaphylaxis may develop angioneurotic facial edema accompanied by urticaria and flushing. Refer to the section on Recognizing Angioneurotic Edema. Airway edema symptoms include hoarseness, stridor, bronchospasm accompanied by dyspnea and tachypnea. Symptoms of shock, such as low blood pressure and cold, moist skin, may also manifest. Facial edema, erythema, and urticaria are symptoms of a localized inflammation.
Cavernous sinus thrombosis
An uncommon but severe condition, cavernous sinus thrombosis may initially present with unilateral swelling that rapidly advances to bilateral swelling of the forehead, base of the nose, and eyelids. Additionally, it can cause chills, pyrexia, cephalalgia, and ocular discomfort.
Chalazion
A chalazion results in localised edema and sensitivity of the afflicted eyelid, accompanied by a little erythematous proliferation on the conjunctival surface.
conjunctivitis
Inflammation of the conjunctiva leads to swelling of the eyelids, profuse tears, and pruritic, scorching eyes. Upon examination, a viscous purulent fluid, crusty eyelids, and conjunctival injection are observed. Involvement of the cornea results in photophobia and pain.
Dacryoadenitis
Dacryoadenitis is characterized by intense swelling around the eye, typically accompanied by conjunctival injection, purulent discharge, and temporal pain.
Dacryocystitis
Chronic inflammation of the lacrimal sac leads to noticeable swelling of the eyelids and persistent weeping. In acute presentations, there is discomfort and sensitivity in the vicinity of the tear sac along with purulent discharge.
Facial burns
Profound edema resulting from burns can significantly hinder respiration. Other observations include jaundiced nasal hairs, erythematous mucosa, sputum with a sooty appearance, and indications of respiratory difficulty, such as stridor during inspiration.
Facial trauma
The magnitude of edema differs depending on the nature of the damage. For instance, a contusion might result in localised swelling, while a fracture of the nose or maxilla leads to the development of more widespread swelling. Associated characteristics are also contingent upon the kind of the injury.
Herpes zoster ophthalmicus (shingles)
Edematous and red eyelids caused by shingles are often accompanied by profuse tearing and a serous discharge. Intense unilateral face pain may manifest many days prior to the eruption of vesicles.
Myxedema
Myxedema ultimately leads to widespread face swelling, flaky, dry skin, hair loss or coarsening, and other symptoms of hypothyroidism.
Nephrotic syndrome
Frequently the initial indication of nephrotic disease, periorbital edema occurs before dependant and abdominal edema. Weight gain, nausea, anorexia, lethargy, weariness, and pallor are among the associated symptoms.
Orbital cellulitis
Acute periorbital edema is a characteristic feature of orbital cellulitis. Conjunctival injection, decreased extraocular movements, fever, and severe orbital pain may accompany a unilateral purulent discharge.
Preeclampsia
Early manifestation of preeclampsia is the presence of edema in the face, hands, and ankles. Additional features include significant weight increase, a strong headache, impaired vision, high blood pressure, and pain in the middle and lower abdomen.
Rhinitis (allergic)
Rhinositis is characterised by red and edematous eyelids, paroxysmal sneezing, itchy nose and eyes, and persistent, watery rhinorrhea. In addition, the patient may progress to nasal congestion, profuse weeping, a headache, sinus pain, and occasionally, malaise and a fever.
Sinusitis
Frontal sinusitis results in swelling of the forehead and eyelids. In addition to malaise, gingival swelling, and trismus, maxillary sinusitis causes edema in the maxillary region. Both forms are additionally characterized by facial discomfort, pyrexia, nasal congestion, purulent nasal secretion, and erythematous, vascularized nasal mucosa.
Superior vena cava syndrome
Symptoms of superior vena cava syndrome include progressive swelling of the face and neck, along with distension of the thoracic or jugular veins. Furthermore, it induces symptoms of the central nervous system, including headache, visual impairments, and vertigo.
Trachoma
Trachoma is characterized by tissue swelling in the eyelid and conjunctiva, along with symptoms such as eye pain, excessive crying, sensitivity to light, and eyes discharge. Upon examination, an inflammatory preauricular node and palpable conjunctival follicles are observed.
Trichinosis
Trichinosis is an uncommon infectious condition characterized by the abrupt development of swelling in the eyelids accompanied by a fever ranging from 102°F to 104°F (38.9°C to 40°C), conjunctivitis, muscle soreness, pruritus and irritation of the skin, perspiration, skin lesions, and altered mental state.
Additional Factors
Medical diagnostic testing. Facial edema may be precipitated by an allergic response to contrast media employed in radiologic examinations.
Substances
Chronic administration of glucocorticoids might result in facial edema. Any pharmaceutical substance that elicits an allergic response (such as aspirin, antipyretics, penicillin, and sulfa preparations) can equally produce the same outcome.
Surgeries and blood transfusions. Cervical, nasal, or mandibular surgery can result in facial edema, as can a blood transfusion that triggers an allergic response.
Botanical Alert
Consumption of the fruit pulp of Ginkgo biloba can result in intense redness and swelling, as well as the quick development of vesicles. The medications feverfew and Chrysanthemum parthenium can induce lip edema, tongue discomfort, and oral ulcers. Administering licorice before menstruation may result in face edema, water retention, and bloating.
Points of Special Consideration
Administer a pain-relieving medication and apply a topical treatment to alleviate itching. Should it not be contraindicated, administer cold compresses to the patient's eyes in order to reduce edema. Elevate the head of the bed to facilitate the drainage of the accumulated fluid. Commonly, urine and blood tests are requested to aid in the diagnosis of the underlying trigger of face edema.
Educational Instruction for Patients
Detail the hazards associated with delayed allergy symptoms and identify the specific signs and symptoms that should be reported. Elaborate on strategies to prevent allergies and insect bites or stings. Stress the need of possessing an anaphylaxis kit and a medical identification bracelet.
Guidelines for Pediatric Populations
Pediatric periorbital tissue pressure typically exhibits lower values compared to adults. Therefore, children have a higher probability of developing periorbital edema. Indeed, periorbital edema is more prevalent than peripheral edema in children suffering from conditions such as heart failure and acute glomerulonephritis. Furthermore, pertussis can induce periorbital edema.

- Published on
Symptoms and Signs – Differential Diagnosis of edema of the Arm
Edema of the arm
Arm edema is the consequence of prolonged accumulation of interstitial fluid in the arm. It can occur either unilaterally or bilaterally and may progress either slowly or suddenly. The condition can be worsened by lack of movement and relieved by raising the arm and increasing physical activity.
Edema in the arm indicates a specific fluid imbalance between the blood vessels and the gaps between tissues. Please refer to Understanding Fluid Balance on page 278. It often occurs as a consequence of trauma, venous diseases, poisons, or specific medicinal therapies.
Acute medical interventions
Detach rings, bracelets, and watches from the surgically impacted arm of the patient. Some of these objects may function as a tourniquet. Verify that the patient's sleeves do not impede the drainage of fluids or the circulation of blood.
Histories and Physical Assessment
An initial inquiry to make while obtaining the patient's medical history is, "What is the duration of your arm's swelling?" Next, ascertain whether the patient is experiencing arm pain, numbness, or tingling. Are exercise and arm elevation effective in reducing edema? Inquire specifically about any recent arm injuries, such as burns or bug bites. In addition, record any recent intravenous therapy, surgical procedures, or radiation therapy for breast cancer.
The severity of the edema can be determined by comparing the dimensions and symmetry of both arms. For precise girth determination, use a tape measure and indicate the precise location of the measurement to facilitate further comparison measures. Ensure to record if the swelling is localized or spread to both sides, and examine for the presence of pitting. (Refer to page 279 of Edema: Pitting or Nonpitting?.) Then, analyze and contrast the hue and temperature of each arm. Inspect for redness and ecchymoses, as well as for wounds indicative of injury. Assess and contrast the radial and brachial pulses via palpation. Assess for arm soreness and reduced feeling or motion. Elevate the arm if you encounter indications of neurovascular impairment.
Medical Causes
Angioneurotic edema
Angioneurotic edema is a frequently seen allergic response marked by the abrupt development of painless, nonpruritic swelling that affects the hands, feet, eyelids, lips, face, neck, genitalia, or viscera. While swelling often does not become itchy, it can cause burning and tingling sensations. Progression of edema to the larynx might lead to manifestations of respiratory distress.
Arm injury
Following a crush injury, there may be significant swelling that is present over the whole arm. Proliferation of ecchymoses or superficial bleeding, discomfort or numbness, and paralysis may manifest.
Burns
Two days or less after injury, arm burns may cause mild to severe edema, pain, and tissue damage.
Envenomation
Severe envenomation from snakes, aquatic creatures, or insects may first result in swelling around the bite or sting, which rapidly extends to the whole arm. Common symptoms at the location include pain, erythema, and pruritus; and infrequently paresthesia may occur. Subsequently, the patient may experience symptoms of generalized nature, including but not limited to nausea, vomiting, weakness, muscle cramps, fever, chills, hypotension, headache, and, in more severe instances, dyspnea, seizures, and paralysis.
Congenital superior vena cava syndrome
Typically, bilateral arm edema advances gradually and is accompanied by swelling in the face and neck. Venous dilatation characterizes these edematous regions. The patient presents with the additional symptoms of headache, vertigo, and visual impairments.
Idiopathic thromboplebitis
Peripherally placed central catheters and arm Port-A-Caths can lead to thromboplebitis, a condition characterized by arm edema, discomfort, and warmth. In addition to cyanosis, a fever, chills, and malaise, deep vein thrombophlebitis can also result in redness, soreness, and induration next to the vein.
Other Causes
Therapeutic Interventions. Localized arm edema can occur when intravenous fluid infiltrates the interstitial tissue. Edema of the entire arm can be caused by a radical or modified radical mastectomy that interferes with lymphatic drainage, as well as by axillary lymph node removal. Furthermore, radiation therapy for breast cancer can cause arm edema either immediately following the treatment or several months later
Points of Special Consideration
The management of arm edema should be tailored to the specific underlying cause. Important general care practices include raising the arm, regularly moving it, and using bandages and dressings correctly to facilitate drainage and circulation. In order to avoid the development of pressure ulcers, it is imperative to offer patients with thorough skin care. Moreover, provide an analgesic and anticoagulant as necessary.
Therapeutic Counseling for Patients
Educate the patient about postoperative arm care techniques. Instruct in arm exercises aimed at preventing lymphedema.
Guidelines for Pediatric Populations
Rarely does arm edema manifest in children, unless it is a component of generalized edema. However, it can arise from arm trauma, such as burns and crush injuries.
Edema of the arm
Arm edema is the consequence of prolonged accumulation of interstitial fluid in the arm. It can occur either unilaterally or bilaterally and may progress either slowly or suddenly. The condition can be worsened by lack of movement and relieved by raising the arm and increasing physical activity.
Edema in the arm indicates a specific fluid imbalance between the blood vessels and the gaps between tissues. Please refer to Understanding Fluid Balance on page 278. It often occurs as a consequence of trauma, venous diseases, poisons, or specific medicinal therapies.
Acute medical interventions
Detach rings, bracelets, and watches from the surgically impacted arm of the patient. Some of these objects may function as a tourniquet. Verify that the patient's sleeves do not impede the drainage of fluids or the circulation of blood.
Histories and Physical Assessment
An initial inquiry to make while obtaining the patient's medical history is, "What is the duration of your arm's swelling?" Next, ascertain whether the patient is experiencing arm pain, numbness, or tingling. Are exercise and arm elevation effective in reducing edema? Inquire specifically about any recent arm injuries, such as burns or bug bites. In addition, record any recent intravenous therapy, surgical procedures, or radiation therapy for breast cancer.
The severity of the edema can be determined by comparing the dimensions and symmetry of both arms. For precise girth determination, use a tape measure and indicate the precise location of the measurement to facilitate further comparison measures. Ensure to record if the swelling is localized or spread to both sides, and examine for the presence of pitting. (Refer to page 279 of Edema: Pitting or Nonpitting?.) Then, analyze and contrast the hue and temperature of each arm. Inspect for redness and ecchymoses, as well as for wounds indicative of injury. Assess and contrast the radial and brachial pulses via palpation. Assess for arm soreness and reduced feeling or motion. Elevate the arm if you encounter indications of neurovascular impairment.
Medical Causes
Angioneurotic edema
Angioneurotic edema is a frequently seen allergic response marked by the abrupt development of painless, nonpruritic swelling that affects the hands, feet, eyelids, lips, face, neck, genitalia, or viscera. While swelling often does not become itchy, it can cause burning and tingling sensations. Progression of edema to the larynx might lead to manifestations of respiratory distress.
Arm injury
Following a crush injury, there may be significant swelling that is present over the whole arm. Proliferation of ecchymoses or superficial bleeding, discomfort or numbness, and paralysis may manifest.
Burns
Two days or less after injury, arm burns may cause mild to severe edema, pain, and tissue damage.
Envenomation
Severe envenomation from snakes, aquatic creatures, or insects may first result in swelling around the bite or sting, which rapidly extends to the whole arm. Common symptoms at the location include pain, erythema, and pruritus; and infrequently paresthesia may occur. Subsequently, the patient may experience symptoms of generalized nature, including but not limited to nausea, vomiting, weakness, muscle cramps, fever, chills, hypotension, headache, and, in more severe instances, dyspnea, seizures, and paralysis.
Congenital superior vena cava syndrome
Typically, bilateral arm edema advances gradually and is accompanied by swelling in the face and neck. Venous dilatation characterizes these edematous regions. The patient presents with the additional symptoms of headache, vertigo, and visual impairments.
Idiopathic thromboplebitis
Peripherally placed central catheters and arm Port-A-Caths can lead to thromboplebitis, a condition characterized by arm edema, discomfort, and warmth. In addition to cyanosis, a fever, chills, and malaise, deep vein thrombophlebitis can also result in redness, soreness, and induration next to the vein.
Other Causes
Therapeutic Interventions. Localized arm edema can occur when intravenous fluid infiltrates the interstitial tissue. Edema of the entire arm can be caused by a radical or modified radical mastectomy that interferes with lymphatic drainage, as well as by axillary lymph node removal. Furthermore, radiation therapy for breast cancer can cause arm edema either immediately following the treatment or several months later
Points of Special Consideration
The management of arm edema should be tailored to the specific underlying cause. Important general care practices include raising the arm, regularly moving it, and using bandages and dressings correctly to facilitate drainage and circulation. In order to avoid the development of pressure ulcers, it is imperative to offer patients with thorough skin care. Moreover, provide an analgesic and anticoagulant as necessary.
Therapeutic Counseling for Patients
Educate the patient about postoperative arm care techniques. Instruct in arm exercises aimed at preventing lymphedema.
Guidelines for Pediatric Populations
Rarely does arm edema manifest in children, unless it is a component of generalized edema. However, it can arise from arm trauma, such as burns and crush injuries.

- Published on
Symptoms and Signs – Differential Diagnosis of Edematous Leg
Edema of the Leg
Leg edema is a prevalent indication that occurs when an excessive amount of interstitial fluid builds up in either one or both legs. The condition may impact only the foot and ankle or spread to the thigh, and can manifest as either minor or severe, pitting or nonpitting.
Venous diseases, trauma, and specific bone and heart illnesses that disrupt normal fluid balance can lead to leg edema. Please refer to Understanding Fluid Balance on page 278. Causes of this condition include nephrotic syndrome, cirrhosis, acute and chronic thrombophlebitis, chronic venous insufficiency (most often), cellulitis, lymphedema, and medication therapy. Yet, leg edema can also be caused by several nonpathological process. For instance, extended periods of sitting, standing, or lack of movement might lead to bilateral orthostatic edema. Typically, this pitting edema mostly affects the foot and resolves with rest and knee elevation. Prolonged elevation of venous pressure during the latter stages of pregnancy might lead to ankle edema. Constricting garters or pantyhose can mechanically induce edema in the lower extremities.
Historical Background and Physical Assessment
Initial assessment of the patient should include inquiring about the duration of the edema. Did it manifest abruptly or progressively? Does it diminish by leg elevation? Does it elicit pain upon contact or during ambulation? Is the condition more severe in the morning or does it worsen gradually during the day? Inquire about a recent spinal injury or recent musculoskeletal
surgical procedure or medical condition that may have rendered the patient immobile. Are there any records of cardiovascular illness in his medical history? Ultimately, acquire a comprehensive drug history.
Begin the physical examination by assessing each leg for the presence of pitting edema. Refer to Edema: Pitting or Nonpitting? on page 279. Palpate or use a Doppler to auscultate peripheral pulses to identify an insufficiency, as leg edema can impair arterial blood flow. Carefully examine leg pigmentation and search for atypical vascular patterns. Next, examine the calf muscle for warmth, tenderness, and cords before applying gentle pressure to squeeze it against the tibia to assess for any deep pain. In cases of unilateral leg edema, dorsiflex the foot to search for Homans' sign, which is characterized by calf pain. Finally, observe the thickening or ulceration of the skin in edematous regions.
Medical Causes
Burns
Leg burns can result in range of minor to severe swelling, discomfort, and tissue damage within two days of injury.
Cellulitis
Typically occurring in the lower extremities, pitting edema and orange peel skin are the result of a streptococcal or staphylococcal infection.
In addition to erythema, cellulitis is characterized by warmth and discomfort in the affected region.
Envenomation
A quick onset of mild to severe localised edema at the bite or sting site may be accompanied by erythema, discomfort, urticaria, pruritus, and a burning feeling.
Heart failure
Early indication of right-sided heart failure is bilateral leg edema. Additional indications and manifestations encompass weight increase despite a lack of appetite, nausea, constriction of the chest, low blood pressure, pallor, rapid breathing, difficulty breathing during physical activity, difficulty breathing during sleep, irregular heartbeats, premature contraction of the ventricles, and crackles on inspiration. The presence of pitting ankle edema, hepatomegaly, hemoptysis, and cyanosis indicates somewhat severe heart failure.
Leg trauma
Localised edema ranging from mild to severe may develop directly around the site of injury.
Osteomyelitis
Osteomyelitis, a bone infection, typically causes localized, mild to moderate swelling in the lower leg, which might potentially extend to the neighbouring joint. A fever, localized discomfort, and pain that worsens with leg movement usually precede edema.
Thrombophlebitis
Thrombosis in deep and superficial veins can result in unilateral mild to moderate swelling. The condition known as deep vein thrombophlebitis can manifest as either asymptomatic or as a range of symptoms including mild to severe pain, warmth, cyanosis in the affected leg, as well as fever, chills, and malaise. Common symptoms of superficial thrombophlebitis include pain, warmth, redness, tenderness, and induration along the afflicted vein.
Chronic venous insufficiency
Bilateral or unilateral leg edema of moderate to severe severity is observed in patients with venous insufficiency. Initially, the edema is pliable and pitting; subsequently, it solidifies as the tissues thicken. Additional symptoms include hyperpigmented skin and painless, readily contagious stasis ulcers around the ankle. Females are more commonly affected by venous insufficiency.
Additional factors
Medical diagnostic testing. Venous edema is an uncommon etiology of leg swelling.
Surgical coronary artery bypass grafting. Post-saphenous vein retrieval, unilateral venous insufficiency may occur.
Points of Special Consideration
Administer analgesic and oral antibiotic as necessary. Instruct the patient to refrain from extended periods of sitting or standing, raise his legs when needed, and explicitly advise him against crossing his legs. Employing a compression boot, also known as Unna's boot, can effectively alleviate edema. Continuously monitor the patient's caloric intake and output, and daily assess his weight and leg circumference to identify any alterations in the edema. Arrange for him diagnostic examinations, including blood and urine tests as well as X-rays. Assess whether dietary adjustments, such as limitations on water and sodium intake, are necessary. Observe the afflicted limb for signs of skin collapse.
Therapeutic Counseling for Patients
Explain the correct technique for applying antiembolism stockings or bandages. Provide the patient with guidance on suitable leg exercises. Clarify the specific meals or fluids that the patient should refrain from consuming.
Guidelines for Pediatric Populations
Although uncommon in children, leg edema can occur due to osteomyelitis, leg injury, or, in rare cases, heart failure. The presence of bilateral leg edema, polyuria, and eyelid swelling characterizes nephrotic syndrome.
Edema of the Leg
Leg edema is a prevalent indication that occurs when an excessive amount of interstitial fluid builds up in either one or both legs. The condition may impact only the foot and ankle or spread to the thigh, and can manifest as either minor or severe, pitting or nonpitting.
Venous diseases, trauma, and specific bone and heart illnesses that disrupt normal fluid balance can lead to leg edema. Please refer to Understanding Fluid Balance on page 278. Causes of this condition include nephrotic syndrome, cirrhosis, acute and chronic thrombophlebitis, chronic venous insufficiency (most often), cellulitis, lymphedema, and medication therapy. Yet, leg edema can also be caused by several nonpathological process. For instance, extended periods of sitting, standing, or lack of movement might lead to bilateral orthostatic edema. Typically, this pitting edema mostly affects the foot and resolves with rest and knee elevation. Prolonged elevation of venous pressure during the latter stages of pregnancy might lead to ankle edema. Constricting garters or pantyhose can mechanically induce edema in the lower extremities.
Historical Background and Physical Assessment
Initial assessment of the patient should include inquiring about the duration of the edema. Did it manifest abruptly or progressively? Does it diminish by leg elevation? Does it elicit pain upon contact or during ambulation? Is the condition more severe in the morning or does it worsen gradually during the day? Inquire about a recent spinal injury or recent musculoskeletal
surgical procedure or medical condition that may have rendered the patient immobile. Are there any records of cardiovascular illness in his medical history? Ultimately, acquire a comprehensive drug history.
Begin the physical examination by assessing each leg for the presence of pitting edema. Refer to Edema: Pitting or Nonpitting? on page 279. Palpate or use a Doppler to auscultate peripheral pulses to identify an insufficiency, as leg edema can impair arterial blood flow. Carefully examine leg pigmentation and search for atypical vascular patterns. Next, examine the calf muscle for warmth, tenderness, and cords before applying gentle pressure to squeeze it against the tibia to assess for any deep pain. In cases of unilateral leg edema, dorsiflex the foot to search for Homans' sign, which is characterized by calf pain. Finally, observe the thickening or ulceration of the skin in edematous regions.
Medical Causes
Burns
Leg burns can result in range of minor to severe swelling, discomfort, and tissue damage within two days of injury.
Cellulitis
Typically occurring in the lower extremities, pitting edema and orange peel skin are the result of a streptococcal or staphylococcal infection.
In addition to erythema, cellulitis is characterized by warmth and discomfort in the affected region.
Envenomation
A quick onset of mild to severe localised edema at the bite or sting site may be accompanied by erythema, discomfort, urticaria, pruritus, and a burning feeling.
Heart failure
Early indication of right-sided heart failure is bilateral leg edema. Additional indications and manifestations encompass weight increase despite a lack of appetite, nausea, constriction of the chest, low blood pressure, pallor, rapid breathing, difficulty breathing during physical activity, difficulty breathing during sleep, irregular heartbeats, premature contraction of the ventricles, and crackles on inspiration. The presence of pitting ankle edema, hepatomegaly, hemoptysis, and cyanosis indicates somewhat severe heart failure.
Leg trauma
Localised edema ranging from mild to severe may develop directly around the site of injury.
Osteomyelitis
Osteomyelitis, a bone infection, typically causes localized, mild to moderate swelling in the lower leg, which might potentially extend to the neighbouring joint. A fever, localized discomfort, and pain that worsens with leg movement usually precede edema.
Thrombophlebitis
Thrombosis in deep and superficial veins can result in unilateral mild to moderate swelling. The condition known as deep vein thrombophlebitis can manifest as either asymptomatic or as a range of symptoms including mild to severe pain, warmth, cyanosis in the affected leg, as well as fever, chills, and malaise. Common symptoms of superficial thrombophlebitis include pain, warmth, redness, tenderness, and induration along the afflicted vein.
Chronic venous insufficiency
Bilateral or unilateral leg edema of moderate to severe severity is observed in patients with venous insufficiency. Initially, the edema is pliable and pitting; subsequently, it solidifies as the tissues thicken. Additional symptoms include hyperpigmented skin and painless, readily contagious stasis ulcers around the ankle. Females are more commonly affected by venous insufficiency.
Additional factors
Medical diagnostic testing. Venous edema is an uncommon etiology of leg swelling.
Surgical coronary artery bypass grafting. Post-saphenous vein retrieval, unilateral venous insufficiency may occur.
Points of Special Consideration
Administer analgesic and oral antibiotic as necessary. Instruct the patient to refrain from extended periods of sitting or standing, raise his legs when needed, and explicitly advise him against crossing his legs. Employing a compression boot, also known as Unna's boot, can effectively alleviate edema. Continuously monitor the patient's caloric intake and output, and daily assess his weight and leg circumference to identify any alterations in the edema. Arrange for him diagnostic examinations, including blood and urine tests as well as X-rays. Assess whether dietary adjustments, such as limitations on water and sodium intake, are necessary. Observe the afflicted limb for signs of skin collapse.
Therapeutic Counseling for Patients
Explain the correct technique for applying antiembolism stockings or bandages. Provide the patient with guidance on suitable leg exercises. Clarify the specific meals or fluids that the patient should refrain from consuming.
Guidelines for Pediatric Populations
Although uncommon in children, leg edema can occur due to osteomyelitis, leg injury, or, in rare cases, heart failure. The presence of bilateral leg edema, polyuria, and eyelid swelling characterizes nephrotic syndrome.

- Published on
Symptoms and Signs – Differential Diagnosis of Dystonia
Slow, involuntary movements of major muscle groups in the limbs, trunk, and neck characterize dystonia. This extrapyramidal clinical manifestation may include foot flexion, leg hyperextension, arm extension and pronation, back arching, and neck extension and rotation (spasmodic torticollis). The condition is usually exacerbated by physical activity and psychological strain, and alleviated by rest. The dystonia can manifest as either sporadic, lasting only a few minutes, or persistent and agonizing. At times, it leads to enduring contractures, causing a malformed posture. Dystonia, while it might be inherited or due to unknown causes, often arises from extrapyramidal diseases or toxic substances.
Historical Background and Physical Assessment
Whenever feasible, involve the patient's family in the process of gathering medical history; they may possess a greater level of awareness regarding changes in behavior compared to the patient. Firstly, inquire about the onset of dystonia. Is it exacerbated by mental distress? Is it absent during sleep? Is there a familial predisposition to dystonia? Record a comprehensive drug history, particularly highlighting any use of phenothiazine or antipsychotic medications by the patient. An often observed side effect of these medications is dystonia, and it may be necessary to modify the dosage in order to reduce this impact.
Next, assess the patient's motor coordination and voluntary muscle activity. Carefully study his walking pattern as he traverses the room; then, instruct him to grip your
Manual evaluation of muscular strength using fingers. Assess coordination by instructing him to repeatedly touch your fingertip and then his nose. Next, proceed to assess the gross motor movement of the leg: Instruct him to position his heel on one knee, glide it down his shin to the apex of his big toe, and then, revert it back to his knee. To evaluate fine motor dexterity, instruct him to sequentially touch each finger to his thumb.
EXAMINATION TIP
Recognizing Dystonia
Dystonia, chorea, and athetosis may occur simultaneously. To differentiate between these three, keep these points in mind.
Dystonic movements are slow and twisting and involve large muscle groups in the head, neck, trunk, and limbs. They may be intermittent or continuous.
Choreiform movements are rapid, highly complex, and jerky.
Athetoid movements are slow, sinuous, and writhing, but always continuous; they typically affect the hands and extremities.
Medical Causes
Alzheimer’s disease
The late manifestation of Alzheimer's disease, dystonia is characterized by a gradual deterioration of cognitive function. The patient usually exhibits reduced attention span, forgetfulness, restlessness, an incapacity to do everyday tasks, difficulty speaking clearly, and excessive emotional volatility.
Muscular deformans dystonia
The defining characteristic of dystonia musculorum deformans is prolonged, widespread dystonia, often arising during childhood and worse as one ages. Initially, it results in foot inversion, which is subsequently followed by stunted growth and scoliosis. Signs of late onset include contorted and peculiar body positions, limb stiffness, and difficulty speaking.
Hallervorden-Spatz
Hallervorden-Spatz disease is a progressive, degenerative disorder characterised by dystonic trunk movements, choreoathetosis, ataxia, myoclonus, and generalised rigidity. Furthermore, the patient displays a gradual deterioration in cognitive function and difficulty in speaking clearly.
Huntington's disease (HD)
Dystonic motions indicate the advance stage of Huntington's disease. Distinguished by a gradual deterioration of cognitive abilities, this condition results in dementia and emotional instability. In addition to choreoathetosis, the patient exhibits dysarthria, dysphagia, facial grimacing, and a wide-based, prancing gait.
Parkinson’s disease
Parkinson’s disease often presents with dystonic spasms. Additional characteristic signs include consistent or abrupt stiffness, tremor characteristic of rolling pills, slow movement, difficulty speaking clearly, difficulty swallowing, excessive salivation, facial expressions like a mask, a monotonous voice, a stooped position, and a walking pace.
Wilson's disease
Wilson’s disease is characterised by the successive development of dystonia and chorea in the arms and legs. Common signs and symptoms of the condition include hoarseness, bradykinesia, alterations in behavior, difficulty swallowing, excessive salivation, difficulty speaking clearly, tremors, and the presence of Kayser-Fleischer rings (rusty brown rings located at the outer edge of the cornea).
Other Causes
Pharmaceuticals
All three categories of phenothiazines are capable of inducing dystonia. Piperazine phenothiazines, like acetophenazine and carphenazine, usually result in this symptom; aliphatics, including chlorpromazine, are less often responsible; and piperidines seldom induce it.
Antipsychotics such as haloperidol and loxapine often cause acute facial dystonia, as do very high doses of metoclopramide, risperidone, metyrosine, and excessive amounts of levodopa.
Key Factors to Consider
Motivate the patient to achieve sufficient rest and refrain from experiencing emotional distress. Minimize range-of-motion exercises to prevent exacerbation of dystonia. To prevent injury in cases of severe dystonia, elevate and cushion the bed rails for the patient. Ensure a clean and organized setting particularly for those who are able to walk.
Therapeutic Counseling for Patients
Provide the patient with information on dystonia and available therapy alternatives. Illustrate the need of obtaining sufficient sleep and refraining from emotional distress. Address the accessibility of support groups and services provided by mental health specialists, if necessary.
Guidelines for Pediatric Populations
Dystonia in children typically manifests once they have achieved ambulation. The condition seldom manifests until after the age of 10. Typical etiologies include Fahr's syndrome, dystonia musculorum deformans, athetoid cerebral palsy, and the lingering consequences of neonatal anoxia.
Slow, involuntary movements of major muscle groups in the limbs, trunk, and neck characterize dystonia. This extrapyramidal clinical manifestation may include foot flexion, leg hyperextension, arm extension and pronation, back arching, and neck extension and rotation (spasmodic torticollis). The condition is usually exacerbated by physical activity and psychological strain, and alleviated by rest. The dystonia can manifest as either sporadic, lasting only a few minutes, or persistent and agonizing. At times, it leads to enduring contractures, causing a malformed posture. Dystonia, while it might be inherited or due to unknown causes, often arises from extrapyramidal diseases or toxic substances.
Historical Background and Physical Assessment
Whenever feasible, involve the patient's family in the process of gathering medical history; they may possess a greater level of awareness regarding changes in behavior compared to the patient. Firstly, inquire about the onset of dystonia. Is it exacerbated by mental distress? Is it absent during sleep? Is there a familial predisposition to dystonia? Record a comprehensive drug history, particularly highlighting any use of phenothiazine or antipsychotic medications by the patient. An often observed side effect of these medications is dystonia, and it may be necessary to modify the dosage in order to reduce this impact.
Next, assess the patient's motor coordination and voluntary muscle activity. Carefully study his walking pattern as he traverses the room; then, instruct him to grip your
Manual evaluation of muscular strength using fingers. Assess coordination by instructing him to repeatedly touch your fingertip and then his nose. Next, proceed to assess the gross motor movement of the leg: Instruct him to position his heel on one knee, glide it down his shin to the apex of his big toe, and then, revert it back to his knee. To evaluate fine motor dexterity, instruct him to sequentially touch each finger to his thumb.
EXAMINATION TIP
Recognizing Dystonia
Dystonia, chorea, and athetosis may occur simultaneously. To differentiate between these three, keep these points in mind.
Dystonic movements are slow and twisting and involve large muscle groups in the head, neck, trunk, and limbs. They may be intermittent or continuous.
Choreiform movements are rapid, highly complex, and jerky.
Athetoid movements are slow, sinuous, and writhing, but always continuous; they typically affect the hands and extremities.
Medical Causes
Alzheimer’s disease
The late manifestation of Alzheimer's disease, dystonia is characterized by a gradual deterioration of cognitive function. The patient usually exhibits reduced attention span, forgetfulness, restlessness, an incapacity to do everyday tasks, difficulty speaking clearly, and excessive emotional volatility.
Muscular deformans dystonia
The defining characteristic of dystonia musculorum deformans is prolonged, widespread dystonia, often arising during childhood and worse as one ages. Initially, it results in foot inversion, which is subsequently followed by stunted growth and scoliosis. Signs of late onset include contorted and peculiar body positions, limb stiffness, and difficulty speaking.
Hallervorden-Spatz
Hallervorden-Spatz disease is a progressive, degenerative disorder characterised by dystonic trunk movements, choreoathetosis, ataxia, myoclonus, and generalised rigidity. Furthermore, the patient displays a gradual deterioration in cognitive function and difficulty in speaking clearly.
Huntington's disease (HD)
Dystonic motions indicate the advance stage of Huntington's disease. Distinguished by a gradual deterioration of cognitive abilities, this condition results in dementia and emotional instability. In addition to choreoathetosis, the patient exhibits dysarthria, dysphagia, facial grimacing, and a wide-based, prancing gait.
Parkinson’s disease
Parkinson’s disease often presents with dystonic spasms. Additional characteristic signs include consistent or abrupt stiffness, tremor characteristic of rolling pills, slow movement, difficulty speaking clearly, difficulty swallowing, excessive salivation, facial expressions like a mask, a monotonous voice, a stooped position, and a walking pace.
Wilson's disease
Wilson’s disease is characterised by the successive development of dystonia and chorea in the arms and legs. Common signs and symptoms of the condition include hoarseness, bradykinesia, alterations in behavior, difficulty swallowing, excessive salivation, difficulty speaking clearly, tremors, and the presence of Kayser-Fleischer rings (rusty brown rings located at the outer edge of the cornea).
Other Causes
Pharmaceuticals
All three categories of phenothiazines are capable of inducing dystonia. Piperazine phenothiazines, like acetophenazine and carphenazine, usually result in this symptom; aliphatics, including chlorpromazine, are less often responsible; and piperidines seldom induce it.
Antipsychotics such as haloperidol and loxapine often cause acute facial dystonia, as do very high doses of metoclopramide, risperidone, metyrosine, and excessive amounts of levodopa.
Key Factors to Consider
Motivate the patient to achieve sufficient rest and refrain from experiencing emotional distress. Minimize range-of-motion exercises to prevent exacerbation of dystonia. To prevent injury in cases of severe dystonia, elevate and cushion the bed rails for the patient. Ensure a clean and organized setting particularly for those who are able to walk.
Therapeutic Counseling for Patients
Provide the patient with information on dystonia and available therapy alternatives. Illustrate the need of obtaining sufficient sleep and refraining from emotional distress. Address the accessibility of support groups and services provided by mental health specialists, if necessary.
Guidelines for Pediatric Populations
Dystonia in children typically manifests once they have achieved ambulation. The condition seldom manifests until after the age of 10. Typical etiologies include Fahr's syndrome, dystonia musculorum deformans, athetoid cerebral palsy, and the lingering consequences of neonatal anoxia.
- Published on
Symptoms and Signs – Differential Diagnosis of Dyspnea
In general, dyspnea is a manifestation of cardiopulmonary malfunction, characterized by the perception of challenging or unpleasant respiration. Typically, it is described as dyspnea. The degree of its severity varies significantly and is often not correlated with the severity of the underlying reason. Symptoms of dyspnea can develop abruptly or gradually and may either disappear quickly or continue for years.
The majority of individuals typically perceive dyspnea during physical exertion, and the intensity of this sensation is contingent upon their physical state. In an individual in good health, dyspnea is promptly alleviated by rest. Possible pathological etiologies of dyspnea including pulmonary, cardiac, neuromuscular, and allergy conditions. Further aetiology may include anxiousness. Refer to Dyspnea: Common Causes and Associated Findings on pages 264 and 265 for further information.
Urgent medical interventions
Should a patient present with dyspnea, promptly assess for indications of respiratory distress, such as tachypnea, cyanosis, restlessness, and auxiliary muscular activity. Readied for the administration of oxygen via a nasal cannula, mask, or endotracheal tube. Establish patent intravenous access and initiate cardiac monitoring and oxygen saturation monitoring to identify arrhythmias and hypoxia, respectively. Anticipate the necessary insertion of a chest tube in cases of severe pneumothorax, and the use of constant positive airway pressure or rotating tourniquets for pulmonary edema.
Clinical Background and Physical Assessment
While the patient is capable of responding to inquiries without exacerbating his anguish, proceed with a full historical account. Query whether the onset of dyspnea occurred abruptly or gradually. Does it exhibit constancy or intermittency? Does it manifest during physical exertion or during periods of inactivity? If the patient has previously experienced dyspneic episodes, inquire about any observed escalation in their intensity. Is he able to determine the factors that worsen or relieve these attacks? Has he developed a productive or nonproductive cough or had chest pain? Inquire about any recent physical injuries and record any previous history of upper respiratory tract infection, deep vein phlebitis, or other medical conditions. Query the patient about his smoking habits or occupational exposure to hazardous vapors or irritants. Discover whether he additionally presents with orthopnea, paroxysmal nocturnal dyspnea, or increased weariness.
Due to the subjective nature of dyspnea and its potential exacerbation by anxiety, attentively listening to the patient's description of his dyspnea can aid in identifying the root cause. It is important to note that patients from various cultures may employ distinct vocabulary or expressions to articulate their difficulty breathing.
When conducting the physical examination, specifically search for indications of persistent difficulty breathing, such as excessive growth of muscles in the shoulders and neck. Assess for pursed-lip exhalation, clubbing, peripheral edema, barrel chest, diaphoresis, and distention of the jugular vein.
Monitor blood pressure and listen for crackles, atypical heart sounds or rhythms, egophony, bronchophony, and whispered pectoriloquy by auscultation. Lastly, examine the abdomen by palpation for hepatomegaly and evaluate the patient for edema.
Medical Causes
Acute respiratory distress syndrome (ARDS)
Acquired Respiratory Distress Syndrome (ARDS) is a potentially fatal kind of noncardiogenic pulmonary edema that often presents with acute dyspnea as the initial symptom. Progressive respiratory distress thereafter manifests with restlessness, anxiety, reduced cognitive function, rapid heart rate, and the presence of crackles and rhonchi in both lung fields. Among the additional observations are cyanosis, tachypnea, motor impairment, and intercostal and suprasternal retractions. ARDS of a severe nature might manifest as shock symptoms, including low blood pressure and cold, scaly skin.
Amyotrophic lateral sclerosis (ALS)
ALS results in a gradual progress of shortness of breath that progressively worsens over time. Additional characteristics encompass dysphagia, dysarthria, muscular weakness and atrophy, fasciculations, shallow respirations, tachypnea, and emotional instability.
Anthrax (inhalation)
Dyspnea is a presentation of the second phase of anthrax, accompanied by a fever, stridor, and hypotension (often resulting in death within 24 hours). The early manifestations of this condition, caused by the inhalation of aerosolized spores (emitted by infected animals or as a consequence of bioterrorism) from the bacterium Bacillus anthracis, resemble flu and encompass a fever, chills, weakness, cough, and chest distension.
Aspiration of a foreign body. This critical illness is characterized by acute dyspnea, as well as paroxysmal intercostal, suprasternal, and substernal retractions. Additional symptoms exhibited by the patient include auxiliary muscle use, inspiratory stridor, tachypnea, reduced or missing breath sounds, potentially asymmetrical chest expansion, anxiety, jaundice, excessive sweating, and low blood pressure
Asthma
Asthma is characterized by acute dyspneic episodes, audible wheezing, a dry cough, accessory muscle participation, nasal flaring, intercostal and supraclavicular retractions, tachypnea, tachycardia, diaphoresis, delayed expiration, flushing or cyanosis, and fear. Pharmacological agents that inhibit beta-receptors can worsen asthma episodes.
Atelectasis
Atelectasis is the collapse of part or all of a lung, leading to reduced lung distension. This patient presents with dyspnea and shortness of breath. Concomitant symptoms may encompass anxiousness, increased heart rate, redness of the skin, excessive sweating, and a cough that is not productive. In addition to physical examination findings of dullness to percussion, auscultation of diminished breath sounds, decreased vocal fremitus, inspiratory lag, and chest retractions, a chest X-ray revealing the collapsed area validates the diagnosis.
Blast lung injury
Persons afflicted with a blast lung injury may have an abrupt beginning of shortness of breath after the explosion of an explosive device that propels fragments of metal and chemical irritants at them with great speed. Timely treatment of dyspnea is crucial as prolonged dyspnea may lead to inadequate oxygenation. Additional symptoms encompass intense chest pain, cutaneous tears and contusions, edema, pulmonary bleeding, cough, coughing up blood, shortness of breath, lack of oxygen, wheezing, abrupt cessation of breathing, reduced breath sounds, and instability in normal blood pressure. Acts of terrorism on a global scale have heightened the prevalence of this disorder. Chest radiography, arterial blood gas analysis, computerised tomography scans, and Doppler technologies are frequently used diagnostic instruments. While specific recommendations for treating blast lung injury are lacking, the approach depends on the characteristics of the explosion, the surrounding environment, and any chemical or biological substances implicated.
Cor pulmonale.
Blast lung injury
Persons afflicted with a blast lung injury may have an abrupt beginning of shortness of breath after the explosion of an explosive device that propels fragments of metal and chemical irritants at them with great speed. Timely treatment of dyspnea is crucial as prolonged dyspnea may lead to inadequate oxygenation. Additional symptoms encompass intense chest pain, cutaneous tears and contusions, edema, pulmonary bleeding, cough, coughing up blood, shortness of breath, lack of oxygen, wheezing, abrupt cessation of breathing, reduced breath sounds, and instability in normal blood pressure. Acts of terrorism on a global scale have heightened the prevalence of this disorder. Chest radiography, arterial blood gas analysis, computerised tomography scans, and Doppler technologies are frequently used diagnostic instruments. While specific recommendations for treating blast lung injury are lacking, the approach depends on the characteristics of the explosion, the surrounding environment, and any chemical or biological substances implicated.
Cor pulmonale.
Chronic dyspnea onsets gradually after physical activity and steadily deteriorates until it manifests even during periods of rest. Commonly, there is an underlying heart or pulmonary illness. The patient presents with a persistent productive cough, wheezing, rapid breathing, distension of the jugular vein, swelling of the dependent knee, and enlarged liver. Furthermore, he may encounter escalating exhaustion, debility, and dizziness.
Emphysema
Emphysema is a long-lasting condition characterized by a gradual development of dyspnea with physical activity. Previous smoking history and use of an alpha1-antitrypsin Deficiency or exposure to an occupational irritant often corresponds to symptoms such as barrel chest, hypertrophy of accessory muscles, reduced breath sounds, anorexia, weight loss, malaise, peripheral cyanosis, tachypnea, pursed-lip breathing, protracted expiration, and even a persistent productive cough. Clubbing is a late-of-the-
Chronic dyspnea onsets gradually after physical activity and steadily deteriorates until it manifests even during periods of rest. Commonly, there is an underlying heart or pulmonary illness. The patient presents with a persistent productive cough, wheezing, rapid breathing, distension of the jugular vein, swelling of the dependent knee, and enlarged liver. Furthermore, he may encounter escalating exhaustion, debility, and dizziness.
Flail chest
As a consequence of several rib fractures, sudden dyspnea occurs together with paradoxical chest movement, intense chest pain, low blood pressure, rapid breathing, rapid heart rate, and cyanosis. Surface bruising and reduced or absent breath sounds manifest on the afflicted side.
Cardiovascular failure
Typically, dyspnea emerges gradually in individuals suffering from heart failure. Indications of potential adverse effects include chronic paroxysmal nocturnal dyspnea, orthopnea, tachypnea, tachycardia, palpitations, ventricular gallop, lethargy, dependent peripheral edema, hepatomegaly, a dry cough, weight gain, and loss of mental clarity. Abrupt onset of heart failure might result in jugular vein distension, bibasilar rates, oliguria, and hypotension.
Inhalation injury
Post-inhalation of chemicals or hot gasses, dyspnea can manifest either abruptly or gradually over a period of several hours. Present symptoms may include worsening hoarseness, a chronic cough, sputum that is either sooty or bloody, and swelling of the oropharynx. Furthermore, the patient may present with thermal burns, singed nose hairs, and orofacial burns, together with crackles, rhonchi, wheezing, and indications of respiratory distress.
Myasthenia gravis
By weakening the respiratory muscles, myasthenia gravis induces episodes of dyspnea. Myasthenic crises can progress to acute respiratory distress characterized by shallow respirations and tachypnea.
Myocardial infarction
Crushing substernal chest discomfort that may radiate to the back, neck, chin, and arms will result in sudden dyspnea. Other manifestations include emesis, perspiration, vertigo, hypertension or hypotension, rapid heart rate, anxiety, and pallid, cold, clammy skin.
Plague (Yersinia pestis).
Pneumonic plague is characterized by dyspnea, a productive cough, chest discomfort, tachypnea, hemoptysis, escalating respiratory distress, and cardiopulmonary failure. This virulent infection often manifests abruptly and is characterized by symptoms such as chills, fever, headache, and myalgia. Plague, if left untreated, is of the most potentially fatal illnesses now recognized.
Pleural effusion
Over time, dyspnea gradually worsens in the presence of pleural effusion. First observations reveal a pleural friction rub accompanied by pleuritic pain that exacerbates with coughing or heavy breathing. Additional observations include a non-productive cough; nodules on percussion; egophony, bronchophony, and murmured pectoriloquy; increased heart rate; tachypnea, weight loss, reduced chest movement, tactile fremitus, and diminished breath sounds. In the presence of infection, a fever may manifest.
Pneumonia
The onset of dyspnea is abrupt and often accompanied by a fever, trembling chills, pleuritic chest pain that exacerbates with deep inspiration, and a productive cough. Additional symptoms that may arise include fatigue, headache, myalgia, anorexia, stomach discomfort, crackles, rhonchi, tachycardia, tachypnea, cyanosis, reduced breath sounds, and diaphoresis.
Pneumothorax
Pneumothorax is a potentially fatal condition characterised by sudden difficulty in breathing that is not directly connected to the intensity of the pain. Abrupt, palpable chest discomfort can extend to the arms, face, back, or abdomen. Additional indications and manifestations encompass worry, agitation, a non-productive cough, cyanosis, reduced vocal output, rapid breathing, tympany, diminished or absent breath sounds on the afflicted side, asymmetrical expansion of the chest, use of splints, and usage of auxiliary muscles. In patients diagnosed with tension pneumothorax, tracheal deviation is observed alongside the other characteristic symptoms. Also present may be reduced blood pressure and tachycardia.
Poliomyelitis (bulbar)
The onset of dyspnea occurs gradually and progresses in severity. Other manifestations include pyrexia, facial debility, impaired speech, reduced deep tendon reflexes, diminished cognitive function, difficulty swallowing, nasal regurgitation, and shortness of breath.
Pulmonary edema.
Pulmonary edema, a life-threatening condition, often occurs before symptoms of heart failure, such as jugular vein distention and orthopnea, therefore causing acute dyspnea. Additional characteristics encompass rapid heart rate, rapid breathing, crackles in both lung fields, the presence of a third heart sound (S3 gallop), reduced urine output, a faint pulse, low blood pressure, excessive sweating, flushing of the skin, and pronounced anxiety. The patient may have a dry cough or produce significant quantities of pink, foamy sputum.
Pulmonary embolism. Acute dyspnea that’s generally followed by acute pleuritic chest discomfort describes pulmonary embolism, a life- threatening condition. Possible findings include increased heart rate, a mild fever, shortness of breath, a cough with blood-tinged sputum, a rub on the pleural membrane, crackles, widespread wheezing, dullness when tapped, reduced breath sounds, excessive sweating, restlessness, and sudden onset of anxiety. Signs of shock, such as hypotension and cold, clammy skin, may be caused by a large embolism.
Severe acute respiratory syndrome (SARS). The cause of SARS, an acute viral disease, is currently unknown; nonetheless, a new Coronavirus has been suggested as a potential explanation. While the majority of diagnoses have been documented in Asia (namely China, Vietnam, Singapore, and Thailand), there have also been reported cases in Europe and North America. The duration of the incubation period ranges from 2 to 7 days, and the disease typically starts with a temperature, often exceeding 100.4°F [38°C]. Additional symptoms include cephalalgia, fatigue, a low-grade nonproductive cough, and shortness of breath. The disease exhibits significant variability in its severity, encompassing mild sickness, pneumonia, and, in certain instances, advancing to respiratory failure and mortality.
Shock
The quick onset and progressive worsening of dyspnea in shock is a potentially life-threatening condition. Relevant observations encompass profound hypotension, tachypnea, tachycardia, reduced peripheral pulses, diminished cognitive clarity, agitation, anxiety, and cold, clammy skin.
Tuberculosis
Dyspnea often presents along with chest discomfort, crackles, and a strong cough. Additional symptoms include nocturnal perspiration, pyrexia, loss of appetite and weight, diffuse difficulty swallowing, palpitations during light physical activity, and lack of sound when tapped.
Tularemia. Tularemia, sometimes referred to as rabbit fever, is characterized by dyspnea, fever, chills, headache, generalized myalgia, a nonproductive cough, pleuritic chest discomfort, and empyema.
Points of Special Consideration
Conduct vigilant monitoring of the dyspneic patient. Maintain a composed and comforting demeanour to alleviate his worry and assist him in assuming a comfortable posture, often high Fowler's or the forward-leaning alignment. Administer oxygen if necessary, adjust his clothing, and provide support with pillows.
Arrange the patient for diagnostic examinations, including study of arterial blood gas levels, chest X-rays, and tests to measure pulmonary function. As required, administer a bronchodilator, an antiarrhythmic, a diuretic, and an analgesic to expand bronchioles, rectify cardiac arrhythmias, facilitate fluid excretion, and alleviate pain.
Therapeutic Counseling for Patients
Provide the patient with instruction on pursed-lip and diaphragmatic breathing techniques, as well as chest splinting. Advise the patient to refrain from contact with chemical irritants, pollutants, and those present with respiratory infections.
Guidelines for Pediatric Populations
Infants typically have abdominal respirations, which transition to costal respirations by the age of 7. Presume dyspnea in a newborn who exhibits costal breathing, in an older child who Respirates abdominally, or in any youngster who relies on their neck or shoulder muscles for respiration.
The combination of acute epiglottiditis and laryngotracheobronchitis (croup) can result in profound dyspnea in a kid and potentially provoke respiratory or cardiovascular failure. Expect to deliver oxygen therapy by means of a hood or cool mist tent.
Guidelines for Geriatrics
Elderly patients experiencing dyspnea as a result of chronic disease may not first demonstrate awareness of a notable alteration in their breathing pattern.
In general, dyspnea is a manifestation of cardiopulmonary malfunction, characterized by the perception of challenging or unpleasant respiration. Typically, it is described as dyspnea. The degree of its severity varies significantly and is often not correlated with the severity of the underlying reason. Symptoms of dyspnea can develop abruptly or gradually and may either disappear quickly or continue for years.
The majority of individuals typically perceive dyspnea during physical exertion, and the intensity of this sensation is contingent upon their physical state. In an individual in good health, dyspnea is promptly alleviated by rest. Possible pathological etiologies of dyspnea including pulmonary, cardiac, neuromuscular, and allergy conditions. Further aetiology may include anxiousness. Refer to Dyspnea: Common Causes and Associated Findings on pages 264 and 265 for further information.
Urgent medical interventions
Should a patient present with dyspnea, promptly assess for indications of respiratory distress, such as tachypnea, cyanosis, restlessness, and auxiliary muscular activity. Readied for the administration of oxygen via a nasal cannula, mask, or endotracheal tube. Establish patent intravenous access and initiate cardiac monitoring and oxygen saturation monitoring to identify arrhythmias and hypoxia, respectively. Anticipate the necessary insertion of a chest tube in cases of severe pneumothorax, and the use of constant positive airway pressure or rotating tourniquets for pulmonary edema.
Clinical Background and Physical Assessment
While the patient is capable of responding to inquiries without exacerbating his anguish, proceed with a full historical account. Query whether the onset of dyspnea occurred abruptly or gradually. Does it exhibit constancy or intermittency? Does it manifest during physical exertion or during periods of inactivity? If the patient has previously experienced dyspneic episodes, inquire about any observed escalation in their intensity. Is he able to determine the factors that worsen or relieve these attacks? Has he developed a productive or nonproductive cough or had chest pain? Inquire about any recent physical injuries and record any previous history of upper respiratory tract infection, deep vein phlebitis, or other medical conditions. Query the patient about his smoking habits or occupational exposure to hazardous vapors or irritants. Discover whether he additionally presents with orthopnea, paroxysmal nocturnal dyspnea, or increased weariness.
Due to the subjective nature of dyspnea and its potential exacerbation by anxiety, attentively listening to the patient's description of his dyspnea can aid in identifying the root cause. It is important to note that patients from various cultures may employ distinct vocabulary or expressions to articulate their difficulty breathing.
When conducting the physical examination, specifically search for indications of persistent difficulty breathing, such as excessive growth of muscles in the shoulders and neck. Assess for pursed-lip exhalation, clubbing, peripheral edema, barrel chest, diaphoresis, and distention of the jugular vein.
Monitor blood pressure and listen for crackles, atypical heart sounds or rhythms, egophony, bronchophony, and whispered pectoriloquy by auscultation. Lastly, examine the abdomen by palpation for hepatomegaly and evaluate the patient for edema.
Medical Causes
Acute respiratory distress syndrome (ARDS)
Acquired Respiratory Distress Syndrome (ARDS) is a potentially fatal kind of noncardiogenic pulmonary edema that often presents with acute dyspnea as the initial symptom. Progressive respiratory distress thereafter manifests with restlessness, anxiety, reduced cognitive function, rapid heart rate, and the presence of crackles and rhonchi in both lung fields. Among the additional observations are cyanosis, tachypnea, motor impairment, and intercostal and suprasternal retractions. ARDS of a severe nature might manifest as shock symptoms, including low blood pressure and cold, scaly skin.
Amyotrophic lateral sclerosis (ALS)
ALS results in a gradual progress of shortness of breath that progressively worsens over time. Additional characteristics encompass dysphagia, dysarthria, muscular weakness and atrophy, fasciculations, shallow respirations, tachypnea, and emotional instability.
Anthrax (inhalation)
Dyspnea is a presentation of the second phase of anthrax, accompanied by a fever, stridor, and hypotension (often resulting in death within 24 hours). The early manifestations of this condition, caused by the inhalation of aerosolized spores (emitted by infected animals or as a consequence of bioterrorism) from the bacterium Bacillus anthracis, resemble flu and encompass a fever, chills, weakness, cough, and chest distension.
Aspiration of a foreign body. This critical illness is characterized by acute dyspnea, as well as paroxysmal intercostal, suprasternal, and substernal retractions. Additional symptoms exhibited by the patient include auxiliary muscle use, inspiratory stridor, tachypnea, reduced or missing breath sounds, potentially asymmetrical chest expansion, anxiety, jaundice, excessive sweating, and low blood pressure
Asthma
Asthma is characterized by acute dyspneic episodes, audible wheezing, a dry cough, accessory muscle participation, nasal flaring, intercostal and supraclavicular retractions, tachypnea, tachycardia, diaphoresis, delayed expiration, flushing or cyanosis, and fear. Pharmacological agents that inhibit beta-receptors can worsen asthma episodes.
Atelectasis
Atelectasis is the collapse of part or all of a lung, leading to reduced lung distension. This patient presents with dyspnea and shortness of breath. Concomitant symptoms may encompass anxiousness, increased heart rate, redness of the skin, excessive sweating, and a cough that is not productive. In addition to physical examination findings of dullness to percussion, auscultation of diminished breath sounds, decreased vocal fremitus, inspiratory lag, and chest retractions, a chest X-ray revealing the collapsed area validates the diagnosis.
Blast lung injury
Persons afflicted with a blast lung injury may have an abrupt beginning of shortness of breath after the explosion of an explosive device that propels fragments of metal and chemical irritants at them with great speed. Timely treatment of dyspnea is crucial as prolonged dyspnea may lead to inadequate oxygenation. Additional symptoms encompass intense chest pain, cutaneous tears and contusions, edema, pulmonary bleeding, cough, coughing up blood, shortness of breath, lack of oxygen, wheezing, abrupt cessation of breathing, reduced breath sounds, and instability in normal blood pressure. Acts of terrorism on a global scale have heightened the prevalence of this disorder. Chest radiography, arterial blood gas analysis, computerised tomography scans, and Doppler technologies are frequently used diagnostic instruments. While specific recommendations for treating blast lung injury are lacking, the approach depends on the characteristics of the explosion, the surrounding environment, and any chemical or biological substances implicated.
Cor pulmonale.
Blast lung injury
Persons afflicted with a blast lung injury may have an abrupt beginning of shortness of breath after the explosion of an explosive device that propels fragments of metal and chemical irritants at them with great speed. Timely treatment of dyspnea is crucial as prolonged dyspnea may lead to inadequate oxygenation. Additional symptoms encompass intense chest pain, cutaneous tears and contusions, edema, pulmonary bleeding, cough, coughing up blood, shortness of breath, lack of oxygen, wheezing, abrupt cessation of breathing, reduced breath sounds, and instability in normal blood pressure. Acts of terrorism on a global scale have heightened the prevalence of this disorder. Chest radiography, arterial blood gas analysis, computerised tomography scans, and Doppler technologies are frequently used diagnostic instruments. While specific recommendations for treating blast lung injury are lacking, the approach depends on the characteristics of the explosion, the surrounding environment, and any chemical or biological substances implicated.
Cor pulmonale.
Chronic dyspnea onsets gradually after physical activity and steadily deteriorates until it manifests even during periods of rest. Commonly, there is an underlying heart or pulmonary illness. The patient presents with a persistent productive cough, wheezing, rapid breathing, distension of the jugular vein, swelling of the dependent knee, and enlarged liver. Furthermore, he may encounter escalating exhaustion, debility, and dizziness.
Emphysema
Emphysema is a long-lasting condition characterized by a gradual development of dyspnea with physical activity. Previous smoking history and use of an alpha1-antitrypsin Deficiency or exposure to an occupational irritant often corresponds to symptoms such as barrel chest, hypertrophy of accessory muscles, reduced breath sounds, anorexia, weight loss, malaise, peripheral cyanosis, tachypnea, pursed-lip breathing, protracted expiration, and even a persistent productive cough. Clubbing is a late-of-the-
Chronic dyspnea onsets gradually after physical activity and steadily deteriorates until it manifests even during periods of rest. Commonly, there is an underlying heart or pulmonary illness. The patient presents with a persistent productive cough, wheezing, rapid breathing, distension of the jugular vein, swelling of the dependent knee, and enlarged liver. Furthermore, he may encounter escalating exhaustion, debility, and dizziness.
Flail chest
As a consequence of several rib fractures, sudden dyspnea occurs together with paradoxical chest movement, intense chest pain, low blood pressure, rapid breathing, rapid heart rate, and cyanosis. Surface bruising and reduced or absent breath sounds manifest on the afflicted side.
Cardiovascular failure
Typically, dyspnea emerges gradually in individuals suffering from heart failure. Indications of potential adverse effects include chronic paroxysmal nocturnal dyspnea, orthopnea, tachypnea, tachycardia, palpitations, ventricular gallop, lethargy, dependent peripheral edema, hepatomegaly, a dry cough, weight gain, and loss of mental clarity. Abrupt onset of heart failure might result in jugular vein distension, bibasilar rates, oliguria, and hypotension.
Inhalation injury
Post-inhalation of chemicals or hot gasses, dyspnea can manifest either abruptly or gradually over a period of several hours. Present symptoms may include worsening hoarseness, a chronic cough, sputum that is either sooty or bloody, and swelling of the oropharynx. Furthermore, the patient may present with thermal burns, singed nose hairs, and orofacial burns, together with crackles, rhonchi, wheezing, and indications of respiratory distress.
Myasthenia gravis
By weakening the respiratory muscles, myasthenia gravis induces episodes of dyspnea. Myasthenic crises can progress to acute respiratory distress characterized by shallow respirations and tachypnea.
Myocardial infarction
Crushing substernal chest discomfort that may radiate to the back, neck, chin, and arms will result in sudden dyspnea. Other manifestations include emesis, perspiration, vertigo, hypertension or hypotension, rapid heart rate, anxiety, and pallid, cold, clammy skin.
Plague (Yersinia pestis).
Pneumonic plague is characterized by dyspnea, a productive cough, chest discomfort, tachypnea, hemoptysis, escalating respiratory distress, and cardiopulmonary failure. This virulent infection often manifests abruptly and is characterized by symptoms such as chills, fever, headache, and myalgia. Plague, if left untreated, is of the most potentially fatal illnesses now recognized.
Pleural effusion
Over time, dyspnea gradually worsens in the presence of pleural effusion. First observations reveal a pleural friction rub accompanied by pleuritic pain that exacerbates with coughing or heavy breathing. Additional observations include a non-productive cough; nodules on percussion; egophony, bronchophony, and murmured pectoriloquy; increased heart rate; tachypnea, weight loss, reduced chest movement, tactile fremitus, and diminished breath sounds. In the presence of infection, a fever may manifest.
Pneumonia
The onset of dyspnea is abrupt and often accompanied by a fever, trembling chills, pleuritic chest pain that exacerbates with deep inspiration, and a productive cough. Additional symptoms that may arise include fatigue, headache, myalgia, anorexia, stomach discomfort, crackles, rhonchi, tachycardia, tachypnea, cyanosis, reduced breath sounds, and diaphoresis.
Pneumothorax
Pneumothorax is a potentially fatal condition characterised by sudden difficulty in breathing that is not directly connected to the intensity of the pain. Abrupt, palpable chest discomfort can extend to the arms, face, back, or abdomen. Additional indications and manifestations encompass worry, agitation, a non-productive cough, cyanosis, reduced vocal output, rapid breathing, tympany, diminished or absent breath sounds on the afflicted side, asymmetrical expansion of the chest, use of splints, and usage of auxiliary muscles. In patients diagnosed with tension pneumothorax, tracheal deviation is observed alongside the other characteristic symptoms. Also present may be reduced blood pressure and tachycardia.
Poliomyelitis (bulbar)
The onset of dyspnea occurs gradually and progresses in severity. Other manifestations include pyrexia, facial debility, impaired speech, reduced deep tendon reflexes, diminished cognitive function, difficulty swallowing, nasal regurgitation, and shortness of breath.
Pulmonary edema.
Pulmonary edema, a life-threatening condition, often occurs before symptoms of heart failure, such as jugular vein distention and orthopnea, therefore causing acute dyspnea. Additional characteristics encompass rapid heart rate, rapid breathing, crackles in both lung fields, the presence of a third heart sound (S3 gallop), reduced urine output, a faint pulse, low blood pressure, excessive sweating, flushing of the skin, and pronounced anxiety. The patient may have a dry cough or produce significant quantities of pink, foamy sputum.
Pulmonary embolism. Acute dyspnea that’s generally followed by acute pleuritic chest discomfort describes pulmonary embolism, a life- threatening condition. Possible findings include increased heart rate, a mild fever, shortness of breath, a cough with blood-tinged sputum, a rub on the pleural membrane, crackles, widespread wheezing, dullness when tapped, reduced breath sounds, excessive sweating, restlessness, and sudden onset of anxiety. Signs of shock, such as hypotension and cold, clammy skin, may be caused by a large embolism.
Severe acute respiratory syndrome (SARS). The cause of SARS, an acute viral disease, is currently unknown; nonetheless, a new Coronavirus has been suggested as a potential explanation. While the majority of diagnoses have been documented in Asia (namely China, Vietnam, Singapore, and Thailand), there have also been reported cases in Europe and North America. The duration of the incubation period ranges from 2 to 7 days, and the disease typically starts with a temperature, often exceeding 100.4°F [38°C]. Additional symptoms include cephalalgia, fatigue, a low-grade nonproductive cough, and shortness of breath. The disease exhibits significant variability in its severity, encompassing mild sickness, pneumonia, and, in certain instances, advancing to respiratory failure and mortality.
Shock
The quick onset and progressive worsening of dyspnea in shock is a potentially life-threatening condition. Relevant observations encompass profound hypotension, tachypnea, tachycardia, reduced peripheral pulses, diminished cognitive clarity, agitation, anxiety, and cold, clammy skin.
Tuberculosis
Dyspnea often presents along with chest discomfort, crackles, and a strong cough. Additional symptoms include nocturnal perspiration, pyrexia, loss of appetite and weight, diffuse difficulty swallowing, palpitations during light physical activity, and lack of sound when tapped.
Tularemia. Tularemia, sometimes referred to as rabbit fever, is characterized by dyspnea, fever, chills, headache, generalized myalgia, a nonproductive cough, pleuritic chest discomfort, and empyema.
Points of Special Consideration
Conduct vigilant monitoring of the dyspneic patient. Maintain a composed and comforting demeanour to alleviate his worry and assist him in assuming a comfortable posture, often high Fowler's or the forward-leaning alignment. Administer oxygen if necessary, adjust his clothing, and provide support with pillows.
Arrange the patient for diagnostic examinations, including study of arterial blood gas levels, chest X-rays, and tests to measure pulmonary function. As required, administer a bronchodilator, an antiarrhythmic, a diuretic, and an analgesic to expand bronchioles, rectify cardiac arrhythmias, facilitate fluid excretion, and alleviate pain.
Therapeutic Counseling for Patients
Provide the patient with instruction on pursed-lip and diaphragmatic breathing techniques, as well as chest splinting. Advise the patient to refrain from contact with chemical irritants, pollutants, and those present with respiratory infections.
Guidelines for Pediatric Populations
Infants typically have abdominal respirations, which transition to costal respirations by the age of 7. Presume dyspnea in a newborn who exhibits costal breathing, in an older child who Respirates abdominally, or in any youngster who relies on their neck or shoulder muscles for respiration.
The combination of acute epiglottiditis and laryngotracheobronchitis (croup) can result in profound dyspnea in a kid and potentially provoke respiratory or cardiovascular failure. Expect to deliver oxygen therapy by means of a hood or cool mist tent.
Guidelines for Geriatrics
Elderly patients experiencing dyspnea as a result of chronic disease may not first demonstrate awareness of a notable alteration in their breathing pattern.

