- Published on
Symptoms and Signs – Differential Diagnosis of Diaphoresis
Diaphoresis
Diaphoresis is excessive perspiration, sometimes exceeding 1 liter of sweat each hour. This indication manifests as a reaction of the autonomic nervous system to either physical or psychological stress, as well as to a fever or elevated ambient temperature. When induced by stress, diaphoresis can manifest as either widespread or confined to the palms, soles, and forehead. When precipitated by a fever or elevated ambient temperature, it often manifests as a widespread condition.
Acute diaphoresis often starts suddenly and may be accompanied by other symptoms of the autonomic system, such as rapid heart rate and elevated blood pressure. Nevertheless, this indicator also differs according to age since sweat glands operate at an early stage in newborns and exhibit reduced activity in older individuals. Consequently, patients in these age groups may not exhibit diaphoresis linked to its typical aetiology. Chronic diseases defined by a recurrent fever may be accompanied by intermittent diaphoresis, while isolated diaphoresis may highlight an episode of intense pain or fever. The presence of night sweats may indicate intermittent fever, as the body temperature often rebounds to its normal range between 2 a.m. and 4 a.m. before ultimately increasing once more. Temperature typically reaches its minimum at approximately 6 a.m.
Diaphoresis is a typical physiological reaction when triggered by a high external air temperature. Acclimatization often necessitates a prolonged period of constant exposure to elevated temperatures. Throughout this process, diaphoresis plays a crucial role in regulating the body's natural temperature. Diaphoresis frequently starts during menopause, followed by a feeling of high temperature (a hot flash). Further factors contributing to this phenomenon are physical activity or effort that speeds up the metabolic rate, generating internal heat, and slight to moderate anxiety that triggers the fight-or-flight reaction.
Urgent interventions during episodes of diaphoresis spells crisis
Symptoms of diaphoresis are indicative of specific potentially fatal diseases. These principles will enable you to quickly identify such illnesses and actively intervene to reduce any potential harm to the patient.
Hyperglycemia
Upon noticing diaphoresis in a patient presenting with hazy vision, inquire about heightened irritation and anxiousness. Has he experienced atypical hunger sensations recently? Is there evidence of tremors? Ascertain the patient's vital signs, specifically observing hypotension and tachycardia. Next, inquire about any past occurrence of type 2 diabetes or active use of antidiabetic medication. In the event of suspected hypoglycemia, assess the patient's blood glucose level by means of a glucose reagent strip or submit a serum sample to the laboratory. Administer the prescribed intravenous glucose at a concentration of 50% to restore the patient's glucose level to its normal range. Monitor his physiological parameters and heart rhythm. Ensure an unobstructed airway, and be ready to aid with respiration and circulation if needed.
The presence of excessive sweating in a patient who is weak, fatigued, and anxious raises suspicion of heatstroke, a condition that may advance to circulatory collapse. Measure his vital signs, observing whether his temperature is within the normal or subnormal range. Inspect for patches of pale gray skin and enlarged pupils. Did the patient experience recent exposure to elevated temperatures and humidity? Did he don bulky attire or engage in intense physical exertion during that period? Is he using a diuretic, which disrupts regular perspiration, also?
Next, escort the patient to a chilling chamber, have him disrobe, and use a fan to channel chilled air across his person. Establish an intravenous line and make necessary arrangements for electrolyte and fluid replenishment. Assess him for indications of shock. Ascertain his urine flow meticulously, as well as any other sources of output including catheters, drains, and ostomies.
Autonomic hyperreflexia
For patients with spinal cord injuries above T6 or T7 who exhibit diaphoresis, inquire about the presence of a pounding headache, restlessness, blurred vision, or nasal congestion. Perform a vital sign assessment on the patient, observing bradycardia and severe
High blood pressure. Upon suspicion of autonomic hyperreflexia, promptly exclude its typical consequences. Assess the patient for ocular pain linked to intraocular hemorrhage and for facial paralysis, impaired speech, or limb weakness linked to intracerebral hemorrhage.
Promptly readjust the patient's position to eliminate any pressure sensations. Furthermore, examine for a dilated bladder or fecal blockage. If needed, proceed to remove any obstructions from the urine catheter, or alternatively, provide a suppository or manually extract any obstructed stomach contents. In the event that the underlying cause cannot be identified and alleviated, begin an intravenous line. Make preparations to deliver hydralazine for the treatment of hypertension.
Cardiac infarction or cardiac failure
The suspicion of a myocardial infarction or heart failure arises when the diaphoretic patient presents with chest discomfort and dyspnea, or exhibits arrhythmias or ECG abnormalities. Attach the patient to a cardiac monitor, verify the presence of an unobstructed airway, and provide more oxygenation. Initiate an intravenous line and provide an analgesic pain medication. Ensure readiness to initiate immediate resuscitation in the event of cardiac or respiratory arrest.
Historical Background and Physical Assessment
Timely exclude the potential for a life-threatening aetiology if the patient exhibits diaphoresis. Start the medical history by asking the patient to articulate his primary concern. Proceed to investigate related indications and manifestations. Note overall exhaustion and debility. Does the patient experience sleeplessness, headache, and alterations in visual or auditory function? Frequently experiences dizziness? Does he experience palpitations? Seek information on pleuritic pain, cough, sputum, dyspnea, nausea, vomiting, stomach pain, and changes in bowel or bladder patterns. Prompt the female patient to discuss amenorrhea and any alterations in her menstrual cycle. Has she reached menopause? Inquire about the presence of paresthesia, muscular cramping or stiffness, and orthopedic discomfort. Have any alterations in elimination patterns been observed? Monitor changes in body weight. Was the patient recently required to alter the size of her gloves or shoes?
Expand the historical account by inquiring about travel to tropical destinations. Document any recent instances of exposure to elevated environmental temps or chemicals. Has the patient recently been bitten by an insect? Ensure there is no record of a previous partial gastrectomy or any instances of drug or alcohol misuse. Lastly, acquire a comprehensive drug history.
Proceed to do a physical examination. Initially, assess the degree of diaphoresis by examining the trunk, limbs, palms, soles, and forehead visually. Furthermore, inspect the patient's garments and mattress for any signs of moisture. Remark
Does diaphoresis manifest during diurnal or nocturnal periods? Assess the patient for signs of flushing, an atypical skin texture or lesions, and an augmented presence of coarse body hair. Note diminished skin elasticity and desiccated mucosal linings. Inspect for splinter hemorrhages and Plummer's nails, which is the condition characterized by the detachment of the fingernail ends from the nail beds.
Next, assess the neurological condition of the patient and measure his vital signs. Examine him for the presence of fasciculations and flaccid paralysis. Exercise vigilance for seizures. Document the patient's facial expression and assess the eyes for any signs of pupillary dilatation or constriction, exophthalmos, or excessive tears. Assess visual fields. In addition, assess for auditory impairment and dental or periodontal disease. Conduct a pulmonary auscultation to detect dullness, and listen for crackles, reduced or bronchial breath sounds, and heightened vocal fremitus. Monitor for reduced respiratory excursion. Assess for lymphadenopathy and hepatosplenomegaly by palpation.
Underlying physiological factors that contribute to a medical condition.
Acquired immunodeficiency syndrome
Early on, night sweats might develop either as a direct symptom of the disease or as a result of an opportunistic infection. The patient exhibits furthermore a fever, exhaustion, lymphadenopathy, anorexia, significant and inexplicable weight loss, diarrhea, and a chronic cough.
Acromegaly
Diaphoresis is a highly selective indicator of disease activity in acromegaly, characterized by excessive production of growth hormone and an elevated metabolic rate. The patient presents with a voluminous physical appearance characterized by an expanded supraorbital ridge, as well as thicker ears and nose. Additional indicators include cutaneous hyperthyroidism; edema of the hands, feet, and jaw; arthralgia; weight rise; hoarseness; and heightened presence of coarse body hair. May also manifest as elevated blood pressure, a profound headache, and visual field impairments or complete loss of vision.
Anxiety disorders.
Acute anxiety is distinguishable by panic, while chronic anxiety is characterized by phobias, conversion disorders, obsessions, and compulsions. Regardless of whether it is acute or chronic, anxiety can trigger sympathetic activation, leading to diaphoresis. The diaphoresis is most apparent on the palms, soles, and forehead and is accompanied by palpitations, tachycardia, tachypnea, tremors, and GI distress. Psychological signs and symptoms – panic, difficulties concentrating, and behavior changes — also occur.
Autonomic hyperreflexia
Occurring after resolution of spinal shock after a spinal cord injury above T6, hyperreflexia causes profuse diaphoresis, a pounding headache, clouded vision, and drastically increased blood pressure. Diaphoresis occurs above the level of the injury, often on the forehead, and is accompanied with flushing. Other findings include restlessness, nausea, nasal congestion, and bradycardia.
Drug and alcohol withdrawal symptoms.
Withdrawal from alcohol or an opioid analgesic may cause generalized diaphoresis, dilated pupils, tachycardia, tremors, and an altered mental condition (confusion, delusions, hallucinations, agitation). Associated signs and symptoms include severe muscle cramps, generalized paresthesia, tachypnea, elevated or reduced blood pressure and, possibly, seizures. Nausea and vomiting are typical.
Empyema
Presence of pus in the pleural cavity results in profuse nocturnal perspiration and elevated body temperature. The patient additionally presents with chest pain, a cough, and unintentional weight loss. Examination indicates reduced respiratory excursion on the afflicted side and the absence or remote presence of breath sounds.
Heart failure
In patients with left-sided heart failure, diaphoresis commonly occurs secondary to tiredness, dyspnea, orthopnea, and tachycardia. In patients with right-sided heart failure, diaphoresis often accompanies jugular vein distension and a dry cough. Additional symptoms described are tachypnea, cyanosis, dependent edema, crackles, a cardiac gallop, and anxiety.
Heat exhaustion.
Heat exhaustion is characterized by the inability of heat to disperse, hence initially resulting in excessive sweating, fatigue, weakness, and anxiety. Subsequent signs and symptoms may advance to circulatory collapse and shock, characterized by confusion, a weak pulse, low blood pressure, rapid heart rate, and cold, damp skin. Additional characteristics include a pale gray pallor, enlarged pupils, and a temperature that is either normal or below the usual range.
Heat exhaustion
Heat exhaustion is characterized by the inability of the body to effectively release heat. This condition might initially lead to excessive sweating, tiredness, weakness, and feelings of unease. Subsequent signs and symptoms may advance to circulatory collapse and shock, characterized by confusion, a weak pulse, low blood pressure, rapid heart rate, and cold, damp skin. Additional characteristics include a pale gray pallor, enlarged pupils, and a temperature that is either normal or below the usual range.
Hodgkin’s disease
Especially in elderly patients, early features of Hodgkin’s disease may include night sweats, a fever, fatigue, pruritus, and weight loss. Typically, however, this condition first occurs in painless enlargement of a cervical lymph node. Seldom does a Pel-Ebstein fever pattern manifest, characterized by several days or weeks of fever and chills followed by intervals of afebrile state without chills. The presence of systemic signs and symptoms, such as weight loss, fever, and night sweats, suggests a highly unfavourable prognosis. Hepatomegaly and dyspnea are among the extensive consequences that progressive lymphadenopathy ultimately produces.
Hypoglycemia
Rapidly induced hypoglycemia can lead to diaphoresis accompanied by agitation, tremors, hypotension, blurred vision, increased heart rate, lack of appetite, and loss of consciousness.
Infective endocarditis (subacute)
Generalized night sweats occur early with infective endocarditis. Accompanying signs and symptoms include an intermittent low-grade fever, weakness, fatigue, weight loss, anorexia, and arthralgia. A sudden change in a murmur or the discovery of a new murmur is a classic sign. Petechiae and splinter hemorrhages are also common.
Lung abscess
Drenching night sweats are common with lung abscess. Its chief sign, however, is a cough that produces copious purulent, foul- smelling, and typically bloody sputum. Associated findings include a fever with chills, pleuritic chest pain, dyspnea, weakness, anorexia, weight loss, a headache, malaise, clubbing, tubular or amphoric breath sounds, and dullness on percussion.
Malaria
Profuse diaphoresis marks the third stage of paroxysmal malaria; the first two stages are chills (first stage) and a high fever (second stage). A headache, arthralgia, and hepatosplenomegaly may also occur. In the benign form of malaria, these paroxysms alternate with periods of well-being. The severe form may progress to delirium, seizures, and coma.
Myocardial infarction (MI)
Typically, diaphoresis occurs alongside acute, substernal, radiating chest pain in myocardial infarction (MI), a potentially fatal condition.
Anxiety, shortness of breath, nausea, vomiting, rapid heart rate, irregular pulse, fluctuations in blood pressure, small crackles, pallor, and clammy skin are among the associated signs and symptoms.
Pheochromocytoma.
A pheochromocytoma often causes diaphoresis, but its key characteristic is the presence of continuous or paroxysmal hypertension. Additional symptoms include headache, palpitations, rapid heart rate, anxiety, tremors, pallor, flushing, sensitivity to light, abdominal pain, rapid breathing, nausea, vomiting, and orthostatic hypotension.
Pneumonia
Patients with pneumonia experience intermittent, widespread diaphoresis together with fever and chills. The patient presents with pleuritic chest pain that intensifies on deep inspiration. Additional symptoms include rapid breathing, difficulty breathing, a cough that produces mucus (either thin and mucoid or thick and purulent), a headache, exhaustion, muscle soreness, abdominal discomfort, loss of appetite, and cutaneous cyanosis. The auscultation indicates the presence of bronchial breath sounds.
Tetanus often results in excessive perspiration followed with a mild fever, rapid heart rate, and heightened deep tendon reflexes. Initial restlessness, pain, and stiffness in the jaw, belly, and back advance to spasms often known as lockjaw, risus sardonicus, dysphagia, and opisthotonos. Cyanosis or sudden death by asphyxiation may occur as a consequence of laryngospasm.
Thyrotoxicosis
Thyrotoxicosis often causes polydipsia followed by intolerance to heat, weight loss despite increased appetite, rapid heart rate, palpitations, thyroid enlargement, shortness of breath, anxiety, diarrhea, tremors, Plummer's nails, and perhaps, loss of vision. Gallopysis may also manifest.
TB (tuberculosis)
Despite the lack of symptoms in most individuals with primary infection, tuberculosis can lead to nocturnal perspiration, a mild fever, exhaustion, debility, loss of appetite, and weight loss. Reactivation may manifest as a productive cough complete with mucopurulent sputum, intermittent hemoptysis, and chest pain.
Drugs.
Diaphoresis may be caused by sympathomimetics, certain antipsychotics, thyroid hormones, corticosteroids, and antipyretics. This symptom may also be caused by poisoning with aspirin and acetaminophen.
Dumping syndrome
This syndrome presents as a consequence of the fast emptying of stomach contents into the small intestine following partial gastrectomy. It is characterized by diaphoresis, palpitations, severe weakness, epigastric pain, nausea, and explosive diarrhea. This syndrome manifests shortly after consuming solid food.
Pesticide poisoning. The harmful consequences of pesticides include diaphoresis, nausea, vomiting, diarrhea, impaired vision, miosis, and excessive lacrimation and salivation. The patient may exhibit symptoms such as fasciculations, muscular weakness, and flaccid paralysis. Symptoms of respiratory depression and coma may also manifest.
Points of Special Consideration
Following a bout of diaphoresis, cleanse the patient's face and body with a sponge and replace damp clothing and linens. To minimise skin irritation, apply cornstarch to the skin folds in the groin and axillae, as well as under the sagging breasts, or insert gauze or fabric into the folds. Advancing consistent bathing.
Replenish fluids and electrolytes. Administer intravenous saline or lactated Ringer's solution infusions and track urine output. Promote the consumption of electrolyte-rich oral fluids, such as sports drinks. Strictly enforce bed rest and ensure a noise-free environment. Maintain the patient's ambient temperature at a modest level to avoid more perspiration.
Arrange the patient for diagnostic examinations including blood tests, cultures, chest X-rays, immunologic testing, biopsies, a computed tomography scan, and audiometry screenings. Assure continuous monitoring of the patient's vital signs, including temperature.
Therapeutic Counseling for Patients
Aelucidate the pathogenesis of the condition and appropriate skincare practices. Please elaborate on the significance of fluid replacement and provide strategies to ensure sufficient fluid consumption.
Guidelines for Pediatric Populations
Diaphoresis in children often occurs due to exposure to high temperatures in the environment or excessive clothing—it is often most noticeable around the head. Additional etiologies encompass drug withdrawal linked to maternal addiction, cardiac failure, thyrotoxicosis, and the metabolic consequences of medications such as antihistamines, ephedrine, haloperidol, and thyroid hormone.
Carefully evaluate the fluid state of the youngster. Children may experience more rapid onset of hypovolemia due to fluid loss through diaphoresis compared to adults. Monitor the child's nutritional intake and output, measure their daily weight, and record the length of each diaphoresis episode.
Guidelines for Geriatrics
The characteristic symptoms of tuberculosis, fever and night sweats, may not manifest in older patients. Instead, they may display alterations in their level of physical activity or weight. Finally, it is important to note that elderly patients may not show diaphoresis due to a reduced sweating mechanism. Consequently, they are more susceptible to acquiring heatstroke in extreme temperatures.

- Published on
Symptoms and Signs – Differential Diagnosis of Diarrhea
Diarrhea
Diarrhoea is the presence of loose, watery stools. Diarrhoea, often a primary indicator of an intestinal disease, is a prodigious rise in stool volume relative to the patient's usual bowel patterns. It exhibits a range of severity and can manifest as either acute or chronic. Acute diarrhea can occur due to acute infection, stress, fecal impaction, or therapeutic effects of a medication. Chronic diarrhea can become a consequence of persistent infection, obstructive and inflammatory bowel illness, malabsorption syndrome, an endocrine problem, or gastrointestinal surgery. Intermittent episodes of diarrhea can occur due to food intolerance or the use of spicy or high-fiber meals or caffeine.
Multiple pathophysiologic pathways can contribute to the occurrence of diarrhea. Explore the Causes of Diarrhea The disruption of fluid and electrolyte balances it causes can lead to potentially fatal arrhythmias or hypovolemic shock.
Urgent medical interventions
If the patient experiences excessive diarrhea, examine for indications of shock such as rapid heart rate, low blood pressure, and cold, pale, fluid-soaked skin. Upon detecting these symptoms, arrange the patient in the supine posture and raise his legs by 20 degrees. Establish an intravenous line for the purpose of fluid restoration. Monitor him for electrolyte imbalances, and observe for an irregular pulse, muscular weakness, loss of appetite, and episodes of nausea and vomiting. Retain readily available emergency resuscitation equipment.
Histories and Physical Assessment
Provided that the patient is not experiencing shock, continue with a physical examination. Assess the patient's hydration status, examine skin turgor and mucous membranes, and measure blood pressure while the patient is reclining, seated, and standing. Thoroughly examine the abdomen for any signs of distension and feel for any pain. Perform auscultation of bowel sounds. Examination for tympany affecting the abdominal region. Measure the patient's body temperature and make a record of any chills reported. Examine for any cutaneous eruption. If deemed necessary, perform a rectal examination and a pelvic examination.
Identify and examine indications and manifestations linked to diarrhea. Presenting with abdominal ache and cramps? Insufficiency of respiration? Is he malnourished or exhausted? Ascertain his drug past. Has he lately undergone gastrointestinal surgery or radiation therapy? Solicit a concise account of the patient's dietary habits. Have any documented food allergies been identified in him? Finally, determine if he is experiencing atypical levels of stress.
Medical etiology
Anthrax, gastrointestinal.
Following the consumption of tainted meat from an animal infected with Bacillus anthracis, the human develops symptoms of anthrax. Indicators and manifestations of the condition include reduced appetite, nausea, emesis, and pyrexia. Additional manifestations include intense hemorrhagic diarrhea, abdominal discomfort, and hematemesis.
Carcinoid syndrome.
Carcinoid syndrome is characterized by intense diarrhea accompanied by flushing, typically affecting the head and neck. This flushing is often triggered by emotional responses or the use of food, hot water, or alcohol. Common manifestations include abdominal pains, shortness of breath, loss of body weight, loss of appetite, debility, irregular heartbeats, valvular heart disease, and apathy.
Cholera.
Upon consumption of water or food contaminated with the bacteria Vibrio cholerae, the patient undergoes sudden onset of watery diarrhea and vomiting. Additional indicators and manifestations include extreme thirst (caused by excessive water intake and Adverse effects include electrolyte depletion, muscular cramps, reduced skin elasticity, reduced urine output, increased heart rate, and low blood pressure. Untreated, death can ensue within a few hours.
Clostridium difficile infection
The patient may exhibit no symptoms or may present with soft, irregular stools or watery diarrhea that may have an unpleasant odor or be visibly bloody; stomach pain, cramps, and soreness; a fever; and a white blood cell count rising to 20,000/μL. Extreme cases may result in the patient developing toxic megacolon, colon perforation, or peritonitis.
Crohn’s disease.
Crohn’s disease is a chronic inflammatory condition characterised by the presence of diarrhea, stomach discomfort with guarding and tenderness, and nausea. Additional symptoms exhibited by the patient include fever, chills, weakness, anorexia, and weight loss.
Gram-positive Escherichia coli 0157:H7
Following the consumption of undercooked beef or other foods contaminated with this specific strain of bacteria, the patient experiences watery or bloody diarrhea, nausea, vomiting, fever, and abdominal cramps. Hemolytic uremic syndrome, which causes red blood cell destruction and eventually acute renal failure, is a complication of E. coli 0157:H7 in children age 5 and younger and elderly people.
Infections
Acute viral, bacterial, and protozoal diseases, including cryptosporidiosis, elicit the abrupt emergence of watery diarrhea accompanied by abdominal pain, cramps, nausea, vomiting, and fever. Profound depletion of fluids and electrolytes can lead to symptoms of dehydration and shock. Chronic tuberculosis and fungal and parasite infections can cause a milder yet more prolonged diarrhea, accompanied by epigastric pain, vomiting, weight loss, and perhaps, discharge of blood and mucus.
Gastrointestinal blockage
Partial intestinal blockage enhances intestinal motility, leading to symptoms such as diarrhea, stomach pain accompanied by soreness and guarding, nausea, and potentially, expansion of the abdomen.
Duchenne muscular dystrophy.
Diarrhea is characterized by alternating episodes of constipation or minor infections. Acute viral, bacterial, and protozoal diseases, including cryptosporidiosis, elicit the abrupt emergence of watery diarrhea accompanied by abdominal pain, cramps, nausea, vomiting, and fever. Profound depletion of fluids and electrolytes can lead to symptoms of dehydration and shock. Chronic tuberculosis and fungal and parasite infections can cause a milder yet more prolonged diarrhea, accompanied by epigastric pain, vomiting, weight loss, and perhaps, discharge of blood and mucus.
Intestinal obstruction
Partial intestinal blockage enhances intestinal motility, leading to symptoms such as diarrhea, stomach pain accompanied by soreness and guarding, nausea, and potentially, expansion of the abdomen.
Irritable bowel syndrome
Diarrhea intersperses with either constipation or regular bowel function. Correlating symptoms include stomach pain, soreness, distension, dyspepsia, and nausea. Other associated symptoms include stomach discomfort, soreness, distension, dyspepsia, and nausea.
Ischemic bowel disease
Ischemic bowel disease is a life-threatening disorder that causes bloody diarrhea with abdominal pain. If severe, shock may occur, requiring surgery.
Lactose intolerance
Diarrhea occurs within several hours of ingesting milk or milk products. It’s accompanied by cramps, abdominal pain, borborygmi, bloating, nausea, and flatus.
Listeriosis
With listeriosis, diarrhea occurs in conjunction with a fever, myalgia, abdominal pain, nausea, and vomiting. A fever, a headache, nuchal
rigidity, and an altered level of consciousness may occur if the infection spreads to the nervous system and causes meningitis. This infection, caused by the ingestion of food contaminated with the bacterium Listeria monocytogenes, primarily affects pregnant women, neonates, and those with weakened immune systems.
Norovirus.
Diarrhea induced by Norovirus initially occurs suddenly; it is characterized by watery, nonbloody, and typically self-limiting symptoms that range from 24 to 60 hours. Primary modes of transmission for noroviruses are through the fecal-oral pathway or direct person-to-person contact. Concomitant gastrointestinal symptoms encompass nausea, abdominal pain, abdominal cramps, weight loss, mild fever, and lack of energy. Still, in older and very young patients, as well as those with pre-existing medical conditions, diarrhea can be rather severe. Patients have been observed to excrete the Norovirus in their feces for a period of many weeks after to infection.
Inflammation of the pseudomembranous entericolitis
Typically occurring after the use of antibiotics, pseudomembranous enterocolitis is a potentially life-threatening condition. It generates abundant watery, green, malodorous, bloody diarrhea that quickly triggers acute symptoms of shock. Additional indications and manifestations encompass colicky stomach pain, muscular distension, pyrexia, and dehydration.
Q fever
Q fever is a syndrome caused by the bacterium Coxiella burnetii, characterized by diarrhea, fever, chills, a severe headache, malaise, chest discomfort, and vomiting. In instances of great severity, hepatitis or pneumonia may ensue.
Rotavirus gastroenteritis.
The onset of rotavirus gastroenteritis often involves a fever, nausea, and vomiting, subsequently followed by diarrhea. The sickness may vary in intensity from moderate to severe and exhibit a duration ranging from 3 to 9 days. Dehydration may occur as a consequence of diarrhoea and vomiting.
Tharotoxicosis
Co-occurring symptoms of thyrotoxicosis include agitation, tremors, diaphoresis, weight loss despite increased appetite, dyspnea, palpitations, tachycardia, thyroid enlargement, heat intolerance, and perhaps, exophthalmos.
Ulcerative colitis
The characteristic feature of ulcerative colitis is the repeated occurrence of bloody diarrhea accompanied by pus or mucus. Other indications and manifestations include tenesmus, hyperactive bowel sounds, cramping lower abdomen pain, a mild temperature, loss of appetite, and occasionally, nausea and vomiting. Fatigue, anaemia, and weight loss manifest as late diagnostic findings.
Drugs. Certain antibiotics, including ampicillin, cephalosporins, tetracyclines, and clindamycin, induce diarrhea. Additional medications commonly associated with diarrhea include magnesium-containing antacids, colchicine, guanethidine, lactulose, dantrolene, ethacrynic acid, mefenamic acid, methotrexate, metyrosine, and, when used in excessive amounts, cardiac glycosides and quinidine. Misuse of laxatives can lead to either acute or persistent diarrhea.
Radiation therapy
Diarrhea can manifest as a component of radiation illness following the administration of typically high levels of radiation to a patient.
Therapeutic interventions. Gastroenterostomy, pyloroplasty, and gastric dilation may result in diarrhea. Exposure to high-dose radiation therapy can cause enteritis accompanied by diarrhea.
Key Factors to Consider
Prescribe an analgesic to alleviate pain and an opiate to reduce intestinal motility, unless the patient has a suspected or confirmed fecal infection. Safeguard the patient's confidentiality during bowel movements and swiftly empty bedpans. Ensure meticulous cleansing of the perineum and administer ointment to avoid skin deterioration. Measure and quantify the volume of liquid feces. Track and record information on intake and output on an hourly basis. Acquire serum samples for electrolyte analysis and address any irregularities.
Emphasize the significance of providing medical monitoring to those with inflammatory bowel illness, namely ulcerative colitis, who are at a higher risk of future colon cancer development.
Therapeutic Counseling for Patients
Highlighting the need of maintaining sufficient hydration and elucidating any
Foods or fluids that the patient should refrain from consuming. Elaborate on stress reduction strategies and emphasize the need of medical monitoring for those with an inflammatory bowel illness. Consult for counselling as necessary.
Guidelines for Pediatric Populations
While illness is the primary cause of diarrhoea in children, persistent diarrhea can also arise from malabsorption syndrome, an anatomical abnormality, or allergies. The quick onset of dehydration and electrolyte imbalance in youngsters makes diarrhea potentially life-threatening. Be vigilant in monitoring all instances of diarrhea and promptly replenish depleted fluids.
Guidelines for Geriatrics
Prior to diagnosing Crohn's disease in an elderly patient with new-onset segmental colitis, it is important to always exclude the possibility of ischemia.
Diarrhea
Diarrhoea is the presence of loose, watery stools. Diarrhoea, often a primary indicator of an intestinal disease, is a prodigious rise in stool volume relative to the patient's usual bowel patterns. It exhibits a range of severity and can manifest as either acute or chronic. Acute diarrhea can occur due to acute infection, stress, fecal impaction, or therapeutic effects of a medication. Chronic diarrhea can become a consequence of persistent infection, obstructive and inflammatory bowel illness, malabsorption syndrome, an endocrine problem, or gastrointestinal surgery. Intermittent episodes of diarrhea can occur due to food intolerance or the use of spicy or high-fiber meals or caffeine.
Multiple pathophysiologic pathways can contribute to the occurrence of diarrhea. Explore the Causes of Diarrhea The disruption of fluid and electrolyte balances it causes can lead to potentially fatal arrhythmias or hypovolemic shock.
Urgent medical interventions
If the patient experiences excessive diarrhea, examine for indications of shock such as rapid heart rate, low blood pressure, and cold, pale, fluid-soaked skin. Upon detecting these symptoms, arrange the patient in the supine posture and raise his legs by 20 degrees. Establish an intravenous line for the purpose of fluid restoration. Monitor him for electrolyte imbalances, and observe for an irregular pulse, muscular weakness, loss of appetite, and episodes of nausea and vomiting. Retain readily available emergency resuscitation equipment.
Histories and Physical Assessment
Provided that the patient is not experiencing shock, continue with a physical examination. Assess the patient's hydration status, examine skin turgor and mucous membranes, and measure blood pressure while the patient is reclining, seated, and standing. Thoroughly examine the abdomen for any signs of distension and feel for any pain. Perform auscultation of bowel sounds. Examination for tympany affecting the abdominal region. Measure the patient's body temperature and make a record of any chills reported. Examine for any cutaneous eruption. If deemed necessary, perform a rectal examination and a pelvic examination.
Identify and examine indications and manifestations linked to diarrhea. Presenting with abdominal ache and cramps? Insufficiency of respiration? Is he malnourished or exhausted? Ascertain his drug past. Has he lately undergone gastrointestinal surgery or radiation therapy? Solicit a concise account of the patient's dietary habits. Have any documented food allergies been identified in him? Finally, determine if he is experiencing atypical levels of stress.
Medical etiology
Anthrax, gastrointestinal.
Following the consumption of tainted meat from an animal infected with Bacillus anthracis, the human develops symptoms of anthrax. Indicators and manifestations of the condition include reduced appetite, nausea, emesis, and pyrexia. Additional manifestations include intense hemorrhagic diarrhea, abdominal discomfort, and hematemesis.
Carcinoid syndrome.
Carcinoid syndrome is characterized by intense diarrhea accompanied by flushing, typically affecting the head and neck. This flushing is often triggered by emotional responses or the use of food, hot water, or alcohol. Common manifestations include abdominal pains, shortness of breath, loss of body weight, loss of appetite, debility, irregular heartbeats, valvular heart disease, and apathy.
Cholera.
Upon consumption of water or food contaminated with the bacteria Vibrio cholerae, the patient undergoes sudden onset of watery diarrhea and vomiting. Additional indicators and manifestations include extreme thirst (caused by excessive water intake and Adverse effects include electrolyte depletion, muscular cramps, reduced skin elasticity, reduced urine output, increased heart rate, and low blood pressure. Untreated, death can ensue within a few hours.
Clostridium difficile infection
The patient may exhibit no symptoms or may present with soft, irregular stools or watery diarrhea that may have an unpleasant odor or be visibly bloody; stomach pain, cramps, and soreness; a fever; and a white blood cell count rising to 20,000/μL. Extreme cases may result in the patient developing toxic megacolon, colon perforation, or peritonitis.
Crohn’s disease.
Crohn’s disease is a chronic inflammatory condition characterised by the presence of diarrhea, stomach discomfort with guarding and tenderness, and nausea. Additional symptoms exhibited by the patient include fever, chills, weakness, anorexia, and weight loss.
Gram-positive Escherichia coli 0157:H7
Following the consumption of undercooked beef or other foods contaminated with this specific strain of bacteria, the patient experiences watery or bloody diarrhea, nausea, vomiting, fever, and abdominal cramps. Hemolytic uremic syndrome, which causes red blood cell destruction and eventually acute renal failure, is a complication of E. coli 0157:H7 in children age 5 and younger and elderly people.
Infections
Acute viral, bacterial, and protozoal diseases, including cryptosporidiosis, elicit the abrupt emergence of watery diarrhea accompanied by abdominal pain, cramps, nausea, vomiting, and fever. Profound depletion of fluids and electrolytes can lead to symptoms of dehydration and shock. Chronic tuberculosis and fungal and parasite infections can cause a milder yet more prolonged diarrhea, accompanied by epigastric pain, vomiting, weight loss, and perhaps, discharge of blood and mucus.
Gastrointestinal blockage
Partial intestinal blockage enhances intestinal motility, leading to symptoms such as diarrhea, stomach pain accompanied by soreness and guarding, nausea, and potentially, expansion of the abdomen.
Duchenne muscular dystrophy.
Diarrhea is characterized by alternating episodes of constipation or minor infections. Acute viral, bacterial, and protozoal diseases, including cryptosporidiosis, elicit the abrupt emergence of watery diarrhea accompanied by abdominal pain, cramps, nausea, vomiting, and fever. Profound depletion of fluids and electrolytes can lead to symptoms of dehydration and shock. Chronic tuberculosis and fungal and parasite infections can cause a milder yet more prolonged diarrhea, accompanied by epigastric pain, vomiting, weight loss, and perhaps, discharge of blood and mucus.
Intestinal obstruction
Partial intestinal blockage enhances intestinal motility, leading to symptoms such as diarrhea, stomach pain accompanied by soreness and guarding, nausea, and potentially, expansion of the abdomen.
Irritable bowel syndrome
Diarrhea intersperses with either constipation or regular bowel function. Correlating symptoms include stomach pain, soreness, distension, dyspepsia, and nausea. Other associated symptoms include stomach discomfort, soreness, distension, dyspepsia, and nausea.
Ischemic bowel disease
Ischemic bowel disease is a life-threatening disorder that causes bloody diarrhea with abdominal pain. If severe, shock may occur, requiring surgery.
Lactose intolerance
Diarrhea occurs within several hours of ingesting milk or milk products. It’s accompanied by cramps, abdominal pain, borborygmi, bloating, nausea, and flatus.
Listeriosis
With listeriosis, diarrhea occurs in conjunction with a fever, myalgia, abdominal pain, nausea, and vomiting. A fever, a headache, nuchal
rigidity, and an altered level of consciousness may occur if the infection spreads to the nervous system and causes meningitis. This infection, caused by the ingestion of food contaminated with the bacterium Listeria monocytogenes, primarily affects pregnant women, neonates, and those with weakened immune systems.
Norovirus.
Diarrhea induced by Norovirus initially occurs suddenly; it is characterized by watery, nonbloody, and typically self-limiting symptoms that range from 24 to 60 hours. Primary modes of transmission for noroviruses are through the fecal-oral pathway or direct person-to-person contact. Concomitant gastrointestinal symptoms encompass nausea, abdominal pain, abdominal cramps, weight loss, mild fever, and lack of energy. Still, in older and very young patients, as well as those with pre-existing medical conditions, diarrhea can be rather severe. Patients have been observed to excrete the Norovirus in their feces for a period of many weeks after to infection.
Inflammation of the pseudomembranous entericolitis
Typically occurring after the use of antibiotics, pseudomembranous enterocolitis is a potentially life-threatening condition. It generates abundant watery, green, malodorous, bloody diarrhea that quickly triggers acute symptoms of shock. Additional indications and manifestations encompass colicky stomach pain, muscular distension, pyrexia, and dehydration.
Q fever
Q fever is a syndrome caused by the bacterium Coxiella burnetii, characterized by diarrhea, fever, chills, a severe headache, malaise, chest discomfort, and vomiting. In instances of great severity, hepatitis or pneumonia may ensue.
Rotavirus gastroenteritis.
The onset of rotavirus gastroenteritis often involves a fever, nausea, and vomiting, subsequently followed by diarrhea. The sickness may vary in intensity from moderate to severe and exhibit a duration ranging from 3 to 9 days. Dehydration may occur as a consequence of diarrhoea and vomiting.
Tharotoxicosis
Co-occurring symptoms of thyrotoxicosis include agitation, tremors, diaphoresis, weight loss despite increased appetite, dyspnea, palpitations, tachycardia, thyroid enlargement, heat intolerance, and perhaps, exophthalmos.
Ulcerative colitis
The characteristic feature of ulcerative colitis is the repeated occurrence of bloody diarrhea accompanied by pus or mucus. Other indications and manifestations include tenesmus, hyperactive bowel sounds, cramping lower abdomen pain, a mild temperature, loss of appetite, and occasionally, nausea and vomiting. Fatigue, anaemia, and weight loss manifest as late diagnostic findings.
Drugs. Certain antibiotics, including ampicillin, cephalosporins, tetracyclines, and clindamycin, induce diarrhea. Additional medications commonly associated with diarrhea include magnesium-containing antacids, colchicine, guanethidine, lactulose, dantrolene, ethacrynic acid, mefenamic acid, methotrexate, metyrosine, and, when used in excessive amounts, cardiac glycosides and quinidine. Misuse of laxatives can lead to either acute or persistent diarrhea.
Radiation therapy
Diarrhea can manifest as a component of radiation illness following the administration of typically high levels of radiation to a patient.
Therapeutic interventions. Gastroenterostomy, pyloroplasty, and gastric dilation may result in diarrhea. Exposure to high-dose radiation therapy can cause enteritis accompanied by diarrhea.
Key Factors to Consider
Prescribe an analgesic to alleviate pain and an opiate to reduce intestinal motility, unless the patient has a suspected or confirmed fecal infection. Safeguard the patient's confidentiality during bowel movements and swiftly empty bedpans. Ensure meticulous cleansing of the perineum and administer ointment to avoid skin deterioration. Measure and quantify the volume of liquid feces. Track and record information on intake and output on an hourly basis. Acquire serum samples for electrolyte analysis and address any irregularities.
Emphasize the significance of providing medical monitoring to those with inflammatory bowel illness, namely ulcerative colitis, who are at a higher risk of future colon cancer development.
Therapeutic Counseling for Patients
Highlighting the need of maintaining sufficient hydration and elucidating any
Foods or fluids that the patient should refrain from consuming. Elaborate on stress reduction strategies and emphasize the need of medical monitoring for those with an inflammatory bowel illness. Consult for counselling as necessary.
Guidelines for Pediatric Populations
While illness is the primary cause of diarrhoea in children, persistent diarrhea can also arise from malabsorption syndrome, an anatomical abnormality, or allergies. The quick onset of dehydration and electrolyte imbalance in youngsters makes diarrhea potentially life-threatening. Be vigilant in monitoring all instances of diarrhea and promptly replenish depleted fluids.
Guidelines for Geriatrics
Prior to diagnosing Crohn's disease in an elderly patient with new-onset segmental colitis, it is important to always exclude the possibility of ischemia.

- Published on
Symptoms and Signs – Differential Diagnosis of Depression
Depression is a mood condition marked by feelings of sadness, despair,and loss of interest or pleasure in activities. These sensations may be accompanied by somatic problems, such as changes in appetite, sleep disruptions, restlessness or lethargy, and impaired focus. Thoughts of hurting one’s self, death, or suicide may also occur.
Clinical depression should be differentiated from "the blues," which refer to occasional episodes of dysphoria that are less long-lasting and intense than the established clinical condition. The criterion for major depression is one or more episodes of low mood, or diminished interest or the ability to take pleasure in all or most activities, lasting at least 2 weeks.
An estimated 20.9 million Americans (9.5%) experience major depression annually. Approximately 12 million women (12%), 6 million men (7%), and 3 million adolescents (4%) experience depression each year. It affects all racial, ethnic, and socioeconomic categories, and it is twice as common in women as in men. It is the top cause of disability of women and men of all ages in the United States and internationally. The causes of depression are multifaceted, encompassing genetic and familial predisposition, medical and psychiatric diseases, and the consumption of specific medications. It can also occur in the postpartum period. Thorough psychiatric and physical examination should be performed to rule out any medical underlying factors.
History and Physical Examination
During the assessment, determine how the patient feels about herself, her family, and her environment. The objective is to investigate the manifestation of her depression, the degree to which other variables influence it, and her coping strategies and their efficacy. Begin by inquiring about her current concerns. How does her current mood differ from her regular mood? Then, ask her to express the way she feels about herself. What are her prospects and aspirations? In what degree are they realistic? Is she generally content with what she has accomplished in her work, relationships, and other interests? Inquire about any alterations in her social contacts, sleep patterns, eating, regular activities, or cognitive competence in decision-making and concentration. Determine trends of drug and alcohol use. Listen for signals that she may be suicidal. (See Suicide: Caring for the High-Risk Patient.)
Ask the patient about her family — its patterns of interaction and characteristic responses to success and disappointment. What role does she perceive herself to have in her family life? Find out if other family members have been depressed and whether someone important to the patient has been sick or has died in the past year. Finally, inquire about the patient's surroundings. Has her lifestyle undergone any changes throughout the the last month? Six months? Calendar year? When she’s feeling blue, where does she go and what does she do to feel better? Ascertain her sentiments regarding her position within the community and the various resources at her disposal. Evaluate whether she has a sufficient support system to assist her in managing her depression.
Medical Causes
Organic diseases
Various organic ailments and chronic illnesses create mild, moderate, or severe depression. Among these are metabolic and endocrine disorders, such as hypothyroidism, hyperthyroidism, and diabetes; infectious diseases, such as influenza, hepatitis, and encephalitis; degenerative diseases, such as Alzheimer’s disease, multiple sclerosis, and multi-infarct dementia; and neoplastic disorders such as cancer.
Psychiatric disorders
Affective disorders are often characterized by sudden mood swings from sadness to exaltation (mania) or by extended periods of either mood. In fact, severe depression may continue for weeks. More mild depression occurs in cyclothymic diseases and frequently alternates with moderate mania. Prolonged and consistent moderate depression over a period of two years usually arises from dysthymic disorders. In addition, several persistent anxiety disorders, such panic and obsessive-compulsive disorder, may coexist with depression.
Alcohol abuse.
Long-term alcohol use, intoxication, or withdrawal commonly produces depression.
Drugs
Various drugs cause depression as an adverse effect. Among the more common are barbiturates; chemotherapeutic drugs, such as asparaginase; anticonvulsants, such as diazepam; and antiarrhythmics, such as disopyramide. Other depression-inducing drugs include centrally acting antihypertensives, such as reserpine (common in high dosages), methyldopa, and clonidine; beta-adrenergic blockers, such as propranolol; levodopa; indomethacin; cycloserine; corticosteroids; and hormonal contraceptives.
Postpartum period
Although the cause hasn’t been proved, depression occurs in about 1 in every 2,000 to 3,000 pregnancies and is characterized by various symptoms. Symptoms range from mild postpartum blues to an intense, suicidal, depressive psychosis.
Special Considerations
Caring for a depressed patient needs time, tact, and energy. It also takes a knowledge of your own vulnerability to sentiments of despair that can come from engaging with a depressed patient. Assist the patient in establishing attainable objectives; facilitate her development of self-esteem by expressing her viewpoints and exercising autonomy in decision-making. Try to evaluate her suicide potential, and take steps to help secure her safety. The patient may require strict observation to prevent a suicide attempt.
Ensure that the patient is provided with sufficient sustenance and relaxation, while maintaining a stress-free and stimulating living environment. Arrange for ordered diagnostic tests to evaluate if her depression has an organic basis, and deliver recommended medicines. Additionally, schedule a follow-up counseling session or reach out to a mental health specialist for direct referral.
Patient Counseling
Education the patient about depression; underscore the existence of efficacious interventions to alleviate symptoms. Reassure the patient that she may help to ease depression by expressing her thoughts, engaging in joyful activities, and enhancing her grooming and cleanliness. Stress the significance of compliance with antidepressant drugs, and evaluate adverse effects.
Guidelines for Pediatrics
Because emotional lability is natural throughout adolescence, depression can be difficult to measure and diagnose in teenagers. Manifestations of underlying depression may encompass physical symptoms, sexual promiscuity, academic underachievement, and substance misuse.
Using a family systems model typically helps establish the etiology of depression in adolescents. Once family roles have been established, counseling sessions with family members or group therapy with peers might assist the patient in overcoming her depression. In instances of great severity, the use of an antidepressant may be necessary.
Guidelines for Geriatrics
The diagnosis of depression in elderly people is often challenging due to the presence of physical disorders, somatic symptoms, restlessness, or alterations in cognitive function, such as memory impairment. Depressed older individuals at most risk for suicide are those who are aged 85 and older, have low self-esteem, and need to be in control. Even a feeble nursing home resident with these traits may have the strength to murder herself.
Depression is a mood condition marked by feelings of sadness, despair,and loss of interest or pleasure in activities. These sensations may be accompanied by somatic problems, such as changes in appetite, sleep disruptions, restlessness or lethargy, and impaired focus. Thoughts of hurting one’s self, death, or suicide may also occur.
Clinical depression should be differentiated from "the blues," which refer to occasional episodes of dysphoria that are less long-lasting and intense than the established clinical condition. The criterion for major depression is one or more episodes of low mood, or diminished interest or the ability to take pleasure in all or most activities, lasting at least 2 weeks.
An estimated 20.9 million Americans (9.5%) experience major depression annually. Approximately 12 million women (12%), 6 million men (7%), and 3 million adolescents (4%) experience depression each year. It affects all racial, ethnic, and socioeconomic categories, and it is twice as common in women as in men. It is the top cause of disability of women and men of all ages in the United States and internationally. The causes of depression are multifaceted, encompassing genetic and familial predisposition, medical and psychiatric diseases, and the consumption of specific medications. It can also occur in the postpartum period. Thorough psychiatric and physical examination should be performed to rule out any medical underlying factors.
History and Physical Examination
During the assessment, determine how the patient feels about herself, her family, and her environment. The objective is to investigate the manifestation of her depression, the degree to which other variables influence it, and her coping strategies and their efficacy. Begin by inquiring about her current concerns. How does her current mood differ from her regular mood? Then, ask her to express the way she feels about herself. What are her prospects and aspirations? In what degree are they realistic? Is she generally content with what she has accomplished in her work, relationships, and other interests? Inquire about any alterations in her social contacts, sleep patterns, eating, regular activities, or cognitive competence in decision-making and concentration. Determine trends of drug and alcohol use. Listen for signals that she may be suicidal. (See Suicide: Caring for the High-Risk Patient.)
Ask the patient about her family — its patterns of interaction and characteristic responses to success and disappointment. What role does she perceive herself to have in her family life? Find out if other family members have been depressed and whether someone important to the patient has been sick or has died in the past year. Finally, inquire about the patient's surroundings. Has her lifestyle undergone any changes throughout the the last month? Six months? Calendar year? When she’s feeling blue, where does she go and what does she do to feel better? Ascertain her sentiments regarding her position within the community and the various resources at her disposal. Evaluate whether she has a sufficient support system to assist her in managing her depression.
Medical Causes
Organic diseases
Various organic ailments and chronic illnesses create mild, moderate, or severe depression. Among these are metabolic and endocrine disorders, such as hypothyroidism, hyperthyroidism, and diabetes; infectious diseases, such as influenza, hepatitis, and encephalitis; degenerative diseases, such as Alzheimer’s disease, multiple sclerosis, and multi-infarct dementia; and neoplastic disorders such as cancer.
Psychiatric disorders
Affective disorders are often characterized by sudden mood swings from sadness to exaltation (mania) or by extended periods of either mood. In fact, severe depression may continue for weeks. More mild depression occurs in cyclothymic diseases and frequently alternates with moderate mania. Prolonged and consistent moderate depression over a period of two years usually arises from dysthymic disorders. In addition, several persistent anxiety disorders, such panic and obsessive-compulsive disorder, may coexist with depression.
Alcohol abuse.
Long-term alcohol use, intoxication, or withdrawal commonly produces depression.
Drugs
Various drugs cause depression as an adverse effect. Among the more common are barbiturates; chemotherapeutic drugs, such as asparaginase; anticonvulsants, such as diazepam; and antiarrhythmics, such as disopyramide. Other depression-inducing drugs include centrally acting antihypertensives, such as reserpine (common in high dosages), methyldopa, and clonidine; beta-adrenergic blockers, such as propranolol; levodopa; indomethacin; cycloserine; corticosteroids; and hormonal contraceptives.
Postpartum period
Although the cause hasn’t been proved, depression occurs in about 1 in every 2,000 to 3,000 pregnancies and is characterized by various symptoms. Symptoms range from mild postpartum blues to an intense, suicidal, depressive psychosis.
Special Considerations
Caring for a depressed patient needs time, tact, and energy. It also takes a knowledge of your own vulnerability to sentiments of despair that can come from engaging with a depressed patient. Assist the patient in establishing attainable objectives; facilitate her development of self-esteem by expressing her viewpoints and exercising autonomy in decision-making. Try to evaluate her suicide potential, and take steps to help secure her safety. The patient may require strict observation to prevent a suicide attempt.
Ensure that the patient is provided with sufficient sustenance and relaxation, while maintaining a stress-free and stimulating living environment. Arrange for ordered diagnostic tests to evaluate if her depression has an organic basis, and deliver recommended medicines. Additionally, schedule a follow-up counseling session or reach out to a mental health specialist for direct referral.
Patient Counseling
Education the patient about depression; underscore the existence of efficacious interventions to alleviate symptoms. Reassure the patient that she may help to ease depression by expressing her thoughts, engaging in joyful activities, and enhancing her grooming and cleanliness. Stress the significance of compliance with antidepressant drugs, and evaluate adverse effects.
Guidelines for Pediatrics
Because emotional lability is natural throughout adolescence, depression can be difficult to measure and diagnose in teenagers. Manifestations of underlying depression may encompass physical symptoms, sexual promiscuity, academic underachievement, and substance misuse.
Using a family systems model typically helps establish the etiology of depression in adolescents. Once family roles have been established, counseling sessions with family members or group therapy with peers might assist the patient in overcoming her depression. In instances of great severity, the use of an antidepressant may be necessary.
Guidelines for Geriatrics
The diagnosis of depression in elderly people is often challenging due to the presence of physical disorders, somatic symptoms, restlessness, or alterations in cognitive function, such as memory impairment. Depressed older individuals at most risk for suicide are those who are aged 85 and older, have low self-esteem, and need to be in control. Even a feeble nursing home resident with these traits may have the strength to murder herself.

- Published on
Symptoms and Signs – Differential Diagnosis of Hypoactive Deep Tendon Reflexes
A hypoactive deep tendon reflex (DTR) is a pathologically reduced muscular contraction that arises when the tendon of insertion of a muscle is abruptly stretched by a forceful tapping. It may be classified as either minimal (+) or nonexistent (0). Symmetrically diminished (+) reflexes are generally considered normal.
A direct transmission receptor (DTR) often relies on a fully functional receptor, a fully functional sensory-motor nerve fiber, a fully functioning neuromuscular-glandular junction, and a fully operational synapse in the spinal cord. Hypoactive deep tubal reflexes (DTRs) can occur when the reflex arc involving a particular muscle, peripheral nerve, nerve roots, or spinal cord at that level is damaged. Hypoactive Dopamine Transport Receptors (DTRs) are a significant indicator of several diseases, particularly when they co-occur with other neurological signs and symptoms.
Histories and Physical Assessment
Once hypoactive DTRs have been obtained, gather a comprehensive medical history from the patient or a
kin. Solicit his detailed description of the present signs and symptoms. Next, obtain a family and drug history.
Next, assess the patient's degree of awareness. Assess motor function in his extremities and examine for muscular wasting or enlarged muscle mass by palpation. Conduct sensory function tests to assess pain, touch, temperature, and vibration perception. Request information regarding paresthesia. In order to assess gait and coordination, instruct the patient to perform multiple steps. To assess for Romberg's sign, instruct him to assume a standing position with his feet pressed together and his eyes shut. Assess verbal communication throughout a conversation. Assess for indications of visual impairment or auditory impairment. In cases of life-threatening Guillain-Barré syndrome, botulism, or spinal cord injuries resulting in spinal shock, acute development of hypoactive DTRs accompanied by muscle weakness may occur.
Detect autonomic nervous system effects by assessing vital signs and seeing elevated heart rate and blood pressure. Furthermore, examine the skin for signs of pallor, dryness, flushing, or extreme sweating. Assess for hypoactive bowel sounds by auscultation and examine for bladder distention by palpation. Request information regarding symptoms of nausea, vomiting, constipation, and incontinence.
Clinical etiology
Botulism
Generalized hypoactive deep trigeminal nerves (DTRs) are present with gradual descending muscular paralysis in cases of botulism. The patient typically presents with first symptoms of blurred and double vision, and sometimes develops anorexia, nausea, and vomiting. Additional initial bulbar symptoms include dizziness, auditory impairment, difficulty vocalizing, and difficulty swallowing. The individual may exhibit indications of respiratory discomfort and profound constipation characterized by hypoactive bowel sounds.
Eaton-Lambert Syndrome
Eaton-Lambert syndrome results in widespread hypoactive delayed trophic responses (DTRs). Initial indicators include challenges with ankle mobility, stair climbing, and ambulation. The patient may present with complaints of increased muscle soreness, sensitivity to touch, and particularly intense muscle weakness in the morning. Mild activity ameliorates weakness, while vigorous exercise exacerbates it.
Physical activity.
Syndrome of Guillain-Barré.
Guillain-Barré syndrome results in bilateral hypoactive delayed tricuspid regurgitation (DTR) that rapidly advances from initial hypotonia to areflexia within a few days. This condition commonly results in muscular weakness that initial manifests in the legs and subsequently spreads to the arms, and perhaps to the muscles of the trunk and neck. Occasionally, loss of muscle strength may advance to complete paralysis. In addition, there are indications of cranial nerve palsies, discomfort, paresthesia, and transient autonomic dysfunction characterized by sinus tachycardia or bradycardia, flushing, fluctuating blood pressure, and anhidrosis or episodic diaphoresis.
Typically, muscle weakness and hypoactive delayed onset retinal reflexes reach their highest level of intensity within 10 to 14 days, after which symptoms start to subside. In severe situations, persistent hypoactive delayed trophic reflexes (DTRs) and motor weakness may continue after the treatment.
Peripheral neuropathy
Progressive hypoactive diabetic retinopathy (DTR) is a consequence of end-stage diabetes mellitus, renal failure, alcoholism, and peripheral neuropathy caused by drug side effects. Additional effects encompass muscular weakness, sensory impairment, paresthesia, tremors, and potential autonomic dysfunction, including orthostatic hypotension and incontinence.
Polymyositis
Polymyositis is characterized by the presence of hypoactive DTRs, which are accompanied by muscle weakness, discomfort, stiffness, spasms, and perhaps, increased size or atrophy. These effects are often transient; their specific site differs depending on the afflicted muscles.
Spinal cord lesions
Spinal shock caused by spinal cord injury or total transection leads to paralysis of the dorsal thoracic reflexes (areflexia) below the lesion level. Possible manifestations include quadriplegia or paraplegia, flaccidity, diminished feeling below the lesion site, and dry, pallid skin. Also typical are urinary retention accompanied by overflow incontinence, reduced bowel noises, constipation, and loss of genital reflexes. Hypoactive delayed tricuspid regurgitation (DTR) and flaccidity are often temporary; reflex activity may renormalize within a few weeks.
Syringomyelia
Profound bilateral hypoactive DTRs manifest early in syringomyelia, a gradually advancing condition. Additional manifestations include muscular weakness and atrophy; diminished sensory perception, often spreading in a cape-like manner over the arms, shoulders, neck, back, and sometimes the legs; intense, monotonous pain (despite pain relief) in the extremities; and indications of brain stem involvement (nystagmus, facial numbness, unilateral paralysis or weakness of the vocal cord, and unilateral atrophy of the tongue). This condition is more prevalent in males than in females.
Other Causes Pharmaceuticals. Barbiturates and paralytic medications, notably pancuronium and curare, can induce hypoactive delayed thrombotropic reactions (DTRs).
Points of Special Consideration
Facilitate the sufferer in carrying out his routine tasks. Strive to achieve a harmonious equilibrium between fostering autonomy and garantieing his well-being. Motivationate him to engage in ambulation with aid. Assure that personal care items are easily accessible and offer a clear pathway from his bed to the bathroom, free from any obstacles.
If the patient has sensory impairments, ensure appropriate protection against heat, cold, or pressure-induced injuries. Administer a bath water test and regularly move the patient to provide a comfortable and even bed surface. Maintain proper hygiene and dryness of his skin to avoid any deterioration. Execute or promote workouts that enhance range of motion. Furthermore, promote a well-rounded diet supplemented with abundant protein and sufficient hydration.
Therapeutic Counseling for Patients
Educate individuals in abilities that can enhance their autonomy in everyday activities. Expound upon safety protocols, including the use of aids for walking.
Guidelines for Pediatric Populations
In patients with muscular dystrophy, Friedreich’s ataxia, syringomyelia, and spinal cord damage, hypoactive DTRs are frequently observed. They also concomitantly occur with progressive muscle atrophy, a condition that impacts preschoolers and teenagers.
Implement distraction strategies to evaluate Developmental Task Requirements (DTRs); evaluate motor skills by observing the infant or kid during play.
A hypoactive deep tendon reflex (DTR) is a pathologically reduced muscular contraction that arises when the tendon of insertion of a muscle is abruptly stretched by a forceful tapping. It may be classified as either minimal (+) or nonexistent (0). Symmetrically diminished (+) reflexes are generally considered normal.
A direct transmission receptor (DTR) often relies on a fully functional receptor, a fully functional sensory-motor nerve fiber, a fully functioning neuromuscular-glandular junction, and a fully operational synapse in the spinal cord. Hypoactive deep tubal reflexes (DTRs) can occur when the reflex arc involving a particular muscle, peripheral nerve, nerve roots, or spinal cord at that level is damaged. Hypoactive Dopamine Transport Receptors (DTRs) are a significant indicator of several diseases, particularly when they co-occur with other neurological signs and symptoms.
Histories and Physical Assessment
Once hypoactive DTRs have been obtained, gather a comprehensive medical history from the patient or a
kin. Solicit his detailed description of the present signs and symptoms. Next, obtain a family and drug history.
Next, assess the patient's degree of awareness. Assess motor function in his extremities and examine for muscular wasting or enlarged muscle mass by palpation. Conduct sensory function tests to assess pain, touch, temperature, and vibration perception. Request information regarding paresthesia. In order to assess gait and coordination, instruct the patient to perform multiple steps. To assess for Romberg's sign, instruct him to assume a standing position with his feet pressed together and his eyes shut. Assess verbal communication throughout a conversation. Assess for indications of visual impairment or auditory impairment. In cases of life-threatening Guillain-Barré syndrome, botulism, or spinal cord injuries resulting in spinal shock, acute development of hypoactive DTRs accompanied by muscle weakness may occur.
Detect autonomic nervous system effects by assessing vital signs and seeing elevated heart rate and blood pressure. Furthermore, examine the skin for signs of pallor, dryness, flushing, or extreme sweating. Assess for hypoactive bowel sounds by auscultation and examine for bladder distention by palpation. Request information regarding symptoms of nausea, vomiting, constipation, and incontinence.
Clinical etiology
Botulism
Generalized hypoactive deep trigeminal nerves (DTRs) are present with gradual descending muscular paralysis in cases of botulism. The patient typically presents with first symptoms of blurred and double vision, and sometimes develops anorexia, nausea, and vomiting. Additional initial bulbar symptoms include dizziness, auditory impairment, difficulty vocalizing, and difficulty swallowing. The individual may exhibit indications of respiratory discomfort and profound constipation characterized by hypoactive bowel sounds.
Eaton-Lambert Syndrome
Eaton-Lambert syndrome results in widespread hypoactive delayed trophic responses (DTRs). Initial indicators include challenges with ankle mobility, stair climbing, and ambulation. The patient may present with complaints of increased muscle soreness, sensitivity to touch, and particularly intense muscle weakness in the morning. Mild activity ameliorates weakness, while vigorous exercise exacerbates it.
Physical activity.
Syndrome of Guillain-Barré.
Guillain-Barré syndrome results in bilateral hypoactive delayed tricuspid regurgitation (DTR) that rapidly advances from initial hypotonia to areflexia within a few days. This condition commonly results in muscular weakness that initial manifests in the legs and subsequently spreads to the arms, and perhaps to the muscles of the trunk and neck. Occasionally, loss of muscle strength may advance to complete paralysis. In addition, there are indications of cranial nerve palsies, discomfort, paresthesia, and transient autonomic dysfunction characterized by sinus tachycardia or bradycardia, flushing, fluctuating blood pressure, and anhidrosis or episodic diaphoresis.
Typically, muscle weakness and hypoactive delayed onset retinal reflexes reach their highest level of intensity within 10 to 14 days, after which symptoms start to subside. In severe situations, persistent hypoactive delayed trophic reflexes (DTRs) and motor weakness may continue after the treatment.
Peripheral neuropathy
Progressive hypoactive diabetic retinopathy (DTR) is a consequence of end-stage diabetes mellitus, renal failure, alcoholism, and peripheral neuropathy caused by drug side effects. Additional effects encompass muscular weakness, sensory impairment, paresthesia, tremors, and potential autonomic dysfunction, including orthostatic hypotension and incontinence.
Polymyositis
Polymyositis is characterized by the presence of hypoactive DTRs, which are accompanied by muscle weakness, discomfort, stiffness, spasms, and perhaps, increased size or atrophy. These effects are often transient; their specific site differs depending on the afflicted muscles.
Spinal cord lesions
Spinal shock caused by spinal cord injury or total transection leads to paralysis of the dorsal thoracic reflexes (areflexia) below the lesion level. Possible manifestations include quadriplegia or paraplegia, flaccidity, diminished feeling below the lesion site, and dry, pallid skin. Also typical are urinary retention accompanied by overflow incontinence, reduced bowel noises, constipation, and loss of genital reflexes. Hypoactive delayed tricuspid regurgitation (DTR) and flaccidity are often temporary; reflex activity may renormalize within a few weeks.
Syringomyelia
Profound bilateral hypoactive DTRs manifest early in syringomyelia, a gradually advancing condition. Additional manifestations include muscular weakness and atrophy; diminished sensory perception, often spreading in a cape-like manner over the arms, shoulders, neck, back, and sometimes the legs; intense, monotonous pain (despite pain relief) in the extremities; and indications of brain stem involvement (nystagmus, facial numbness, unilateral paralysis or weakness of the vocal cord, and unilateral atrophy of the tongue). This condition is more prevalent in males than in females.
Other Causes Pharmaceuticals. Barbiturates and paralytic medications, notably pancuronium and curare, can induce hypoactive delayed thrombotropic reactions (DTRs).
Points of Special Consideration
Facilitate the sufferer in carrying out his routine tasks. Strive to achieve a harmonious equilibrium between fostering autonomy and garantieing his well-being. Motivationate him to engage in ambulation with aid. Assure that personal care items are easily accessible and offer a clear pathway from his bed to the bathroom, free from any obstacles.
If the patient has sensory impairments, ensure appropriate protection against heat, cold, or pressure-induced injuries. Administer a bath water test and regularly move the patient to provide a comfortable and even bed surface. Maintain proper hygiene and dryness of his skin to avoid any deterioration. Execute or promote workouts that enhance range of motion. Furthermore, promote a well-rounded diet supplemented with abundant protein and sufficient hydration.
Therapeutic Counseling for Patients
Educate individuals in abilities that can enhance their autonomy in everyday activities. Expound upon safety protocols, including the use of aids for walking.
Guidelines for Pediatric Populations
In patients with muscular dystrophy, Friedreich’s ataxia, syringomyelia, and spinal cord damage, hypoactive DTRs are frequently observed. They also concomitantly occur with progressive muscle atrophy, a condition that impacts preschoolers and teenagers.
Implement distraction strategies to evaluate Developmental Task Requirements (DTRs); evaluate motor skills by observing the infant or kid during play.

- Published on
Symptoms and Signs – Differential Diagnosis of Decerebrate Posture
The decerebrate posture is defined by the adduction (internal rotation) and extension of the arms, accompanied by the pronation of the wrists and the flexion of the fingers' joints. The legs exhibit rigid extension, accompanied by compelled plantar flexion of the foot. Severe cases result in acute arthritis of the back (opisthotonos). This symptom is indicative of damage to the upper brain stem, which can occur due to primary lesions such as infarction, hemorrhage, or tumor; metabolic encephalopathy; a head injury; or compression of the brain stem caused by elevated intracranial pressure [ICP].
The decerebrate posture can be induced by harmful stimuli or arise spontaneously. It can manifest as either unilateral or bilateral. Concurrent brain stem and cerebral injury can result in decerebrate posture affecting mainly the arms, while the legs remain weak. Conversely, the decerebrate posture might impact one side of the body while the decorticate posture affects the opposite side. Furthermore, the two positions may alternate in response to the patient's changing neurological condition. In general, the length of each posturing episode is directly related to the extent of brain stem injury.
Urgent medical interventions
Ensuring a patent airway is your foremost concern. Implant a prosthetic airway and implement precautions to avoid aspiration. (Do not disturb spinal alignment if you have suspicion of neurological damage.) Administer suction to the patient as required.
Proceed to analyze spontaneous respirations. Administer supplementary oxygen and, if needed, initiate ventilation of the patient using a portable resuscitation bag.
Medical intervention such as intubation and mechanical ventilation may be necessary. Ensure that emergency resuscitation equipment is readily available. Be sure to review the patient's medical record for a do-not-resuscitate directive.
Historical Background and Physical Assessment
Following the measurement of the patient's vital signs, ascertain his degree of consciousness (LOC). For reference purposes, consult the Glasgow Coma Scale. Next, assess the pupils for diameter, uniformity, and sensitivity to light. Examine deep tendon reflexes and cranial nerve reflexes, and assess for the presence of doll's eye sign phenomenon.
Concurrently, investigate the historical background of the patient's coma. Should you be unable to acquire this information, seek indications of the underlying condition, such as hepatomegaly, cyanosis, alterations in diabetic skin, needle tracks, or evident cases of injury. If a family member is present, determine the initial time at when the patient's level of consciousness started to decline. Did it manifest suddenly? What symptoms did the patient report previous to his loss of consciousness? Are there any documented medical conditions in his medical history such as diabetes, liver illness, cancer, blood clots, or aneurysm? Request information regarding any accident or trauma that caused the coma.
Medical Causes
Brain stem Infarction
Decerebrate posture may be induced when a brain stem infarction leads to a coma. The associated signs and symptoms differ depending on the extent of the infarction and may involve cranial nerve palsies, bilateral cerebellar ataxia, and sensory impairment. A severe coma often leads to the loss of all normal reflexes, which manifests as the lack of the doll's eye sign, a positive Babinski's response, and flaccidity.
Cerebral lesion
If a cerebral lesion, whether caused by trauma, a tumor, an abscess, or an infarction, raises intracranial pressure (ICP), it can also result in decerebrate posture. This stance is usually indicative of a delayed response. Variations in associated observations depend on the location and size of the lesion, but often include coma, atypical pupil size and reaction to light, and the typical combination of elevated intracranial pressure (ICP) - bradycardia, rising systolic blood pressure, and a broadening pulse pressure.
Hepatic encephalopathy
Hepatic encephalopathy is pathological damage of the brain caused by impaired liver function in eliminating harmful chemicals, therefore enabling their entry into the brain and nervous system. The comatose stage of hepatic encephalopathy is characterised by decerebrate posture and coma, which manifest as the patient's condition worsens. Some further indicators include heightened reflexes, a positive Babinski's reflex, and fetor hepaticus. At earlier stages, other symptoms such as disorientation, slurred speech, amnesia, tremors, asterixis, lethargy, stupor, and hyperventilation manifest.
Hypoglycemic encephalopathy
Distinctive by very low blood glucose levels, hypoglycemia encephalopathy can result in decerebrate posture and coma. Furthermore, it induces dilated pupils, sluggish respirations, and bradycardia. Spasms, twitching, and convulsions of the muscles ultimately advance to flaccidity.
Hypoxic Encephalopathy
Decerebrate posture may occur as a consequence of brain stem compression caused by severe hypoxia, which is linked to anaerobic conditions.
Pontine hemorrhage
A pontine hemorrhage, a potentially fatal condition, usually results in a quick onset of decerebrate posture accompanied by coma. Concomitant symptoms include complete paralysis, lack of doll's eye sign, a positive Babinski's reaction, and small, responsive pupils.
Posterior fossa hemorrhage
A posterior fossa hemorrhage is a subtentorial injury that results in a decerebrate anatomical position. Initial manifestations of this condition encompass emesis, cephalalgia, dizziness, lack of coordination, cervical rigidity, somnolence, papilledema, and palsy of the cranial nerves. In due course, the patient enters a state of unconsciousness and may encounter respiratory arrest.
Other causes Diagnostic testing. Extraction of spinal fluid via a lumbar puncture to alleviate high intracranial pressure (ICP) can lead to cerebral compression of the brain stem, resulting in decerebrate posture and coma.
Points of Special Consideration
Facilitate the preparation of the patient and his family for diagnostic testing aimed at identifying the underlying reason of his decerebrate posture. Additional diagnostic tests include cranial radiography, computed tomography scan, magnetic resonance imaging, cerebral angiography, digital subtraction angiography, electroencephalography (EEG), brain scan, and intracranial pressure (ICP) monitoring.
Continuously assess the patient's neurological condition and vital signs at intervals of 30 minutes or as otherwise directed. Also, be vigilant for indications of elevated intracranial pressure (bradycardia, rising systolic blood pressure, and a broadening pulse pressure) and neurological decline (a modified breathing pattern and abnormal temperature).
The patient's family should be informed that decerebrate posture is an automatic reaction, not a deliberate reaction to discomfort or an indication of healing status. Provide psychological assistance.
Therapeutic Counseling for Patients
Clarify that the decerebrate posture is an automatic psychological reaction. Offer psychological assistance to the patient and his accompanying family members.
Paediatric Guidelines
Children under 2 years old may not exhibit decerebrate posture due to lack of development.
The neurological system retains its immaturity. Nevertheless, if the posture is present, it typically presents as the more severe opisthotonos. Opisthotonos is indeed more prevalent in newborns and young children compared to adults and typically serves as a terminal indication. Head trauma is the primary cause of decerebrate posture in children. It also manifests in Reye's syndrome, which is caused by elevated intracranial pressure leading to compression of the brain stem.
A Comparative Analysis of Decerebrate and Decorticate Postures
A decerebrate posture is caused by injury to the upper brain stem. Assuming this position, the arms are brought front and stretched outward, while the wrists are raised and
The fingers exhibited flexion. The lower limbs are rigidly extended, accompanied by plantar flexion of the feet.
A decorticate posture is the consequence of injury to either one or both corticospinal pathways. Assuming this position, the arms are brought forward and bent, while the wrists and fingers are contracted against the chest. The legs exhibit rigid extension and internal rotation, accompanied by plantar flexion of the foot.
The decerebrate posture is defined by the adduction (internal rotation) and extension of the arms, accompanied by the pronation of the wrists and the flexion of the fingers' joints. The legs exhibit rigid extension, accompanied by compelled plantar flexion of the foot. Severe cases result in acute arthritis of the back (opisthotonos). This symptom is indicative of damage to the upper brain stem, which can occur due to primary lesions such as infarction, hemorrhage, or tumor; metabolic encephalopathy; a head injury; or compression of the brain stem caused by elevated intracranial pressure [ICP].
The decerebrate posture can be induced by harmful stimuli or arise spontaneously. It can manifest as either unilateral or bilateral. Concurrent brain stem and cerebral injury can result in decerebrate posture affecting mainly the arms, while the legs remain weak. Conversely, the decerebrate posture might impact one side of the body while the decorticate posture affects the opposite side. Furthermore, the two positions may alternate in response to the patient's changing neurological condition. In general, the length of each posturing episode is directly related to the extent of brain stem injury.
Urgent medical interventions
Ensuring a patent airway is your foremost concern. Implant a prosthetic airway and implement precautions to avoid aspiration. (Do not disturb spinal alignment if you have suspicion of neurological damage.) Administer suction to the patient as required.
Proceed to analyze spontaneous respirations. Administer supplementary oxygen and, if needed, initiate ventilation of the patient using a portable resuscitation bag.
Medical intervention such as intubation and mechanical ventilation may be necessary. Ensure that emergency resuscitation equipment is readily available. Be sure to review the patient's medical record for a do-not-resuscitate directive.
Historical Background and Physical Assessment
Following the measurement of the patient's vital signs, ascertain his degree of consciousness (LOC). For reference purposes, consult the Glasgow Coma Scale. Next, assess the pupils for diameter, uniformity, and sensitivity to light. Examine deep tendon reflexes and cranial nerve reflexes, and assess for the presence of doll's eye sign phenomenon.
Concurrently, investigate the historical background of the patient's coma. Should you be unable to acquire this information, seek indications of the underlying condition, such as hepatomegaly, cyanosis, alterations in diabetic skin, needle tracks, or evident cases of injury. If a family member is present, determine the initial time at when the patient's level of consciousness started to decline. Did it manifest suddenly? What symptoms did the patient report previous to his loss of consciousness? Are there any documented medical conditions in his medical history such as diabetes, liver illness, cancer, blood clots, or aneurysm? Request information regarding any accident or trauma that caused the coma.
Medical Causes
Brain stem Infarction
Decerebrate posture may be induced when a brain stem infarction leads to a coma. The associated signs and symptoms differ depending on the extent of the infarction and may involve cranial nerve palsies, bilateral cerebellar ataxia, and sensory impairment. A severe coma often leads to the loss of all normal reflexes, which manifests as the lack of the doll's eye sign, a positive Babinski's response, and flaccidity.
Cerebral lesion
If a cerebral lesion, whether caused by trauma, a tumor, an abscess, or an infarction, raises intracranial pressure (ICP), it can also result in decerebrate posture. This stance is usually indicative of a delayed response. Variations in associated observations depend on the location and size of the lesion, but often include coma, atypical pupil size and reaction to light, and the typical combination of elevated intracranial pressure (ICP) - bradycardia, rising systolic blood pressure, and a broadening pulse pressure.
Hepatic encephalopathy
Hepatic encephalopathy is pathological damage of the brain caused by impaired liver function in eliminating harmful chemicals, therefore enabling their entry into the brain and nervous system. The comatose stage of hepatic encephalopathy is characterised by decerebrate posture and coma, which manifest as the patient's condition worsens. Some further indicators include heightened reflexes, a positive Babinski's reflex, and fetor hepaticus. At earlier stages, other symptoms such as disorientation, slurred speech, amnesia, tremors, asterixis, lethargy, stupor, and hyperventilation manifest.
Hypoglycemic encephalopathy
Distinctive by very low blood glucose levels, hypoglycemia encephalopathy can result in decerebrate posture and coma. Furthermore, it induces dilated pupils, sluggish respirations, and bradycardia. Spasms, twitching, and convulsions of the muscles ultimately advance to flaccidity.
Hypoxic Encephalopathy
Decerebrate posture may occur as a consequence of brain stem compression caused by severe hypoxia, which is linked to anaerobic conditions.
Pontine hemorrhage
A pontine hemorrhage, a potentially fatal condition, usually results in a quick onset of decerebrate posture accompanied by coma. Concomitant symptoms include complete paralysis, lack of doll's eye sign, a positive Babinski's reaction, and small, responsive pupils.
Posterior fossa hemorrhage
A posterior fossa hemorrhage is a subtentorial injury that results in a decerebrate anatomical position. Initial manifestations of this condition encompass emesis, cephalalgia, dizziness, lack of coordination, cervical rigidity, somnolence, papilledema, and palsy of the cranial nerves. In due course, the patient enters a state of unconsciousness and may encounter respiratory arrest.
Other causes Diagnostic testing. Extraction of spinal fluid via a lumbar puncture to alleviate high intracranial pressure (ICP) can lead to cerebral compression of the brain stem, resulting in decerebrate posture and coma.
Points of Special Consideration
Facilitate the preparation of the patient and his family for diagnostic testing aimed at identifying the underlying reason of his decerebrate posture. Additional diagnostic tests include cranial radiography, computed tomography scan, magnetic resonance imaging, cerebral angiography, digital subtraction angiography, electroencephalography (EEG), brain scan, and intracranial pressure (ICP) monitoring.
Continuously assess the patient's neurological condition and vital signs at intervals of 30 minutes or as otherwise directed. Also, be vigilant for indications of elevated intracranial pressure (bradycardia, rising systolic blood pressure, and a broadening pulse pressure) and neurological decline (a modified breathing pattern and abnormal temperature).
The patient's family should be informed that decerebrate posture is an automatic reaction, not a deliberate reaction to discomfort or an indication of healing status. Provide psychological assistance.
Therapeutic Counseling for Patients
Clarify that the decerebrate posture is an automatic psychological reaction. Offer psychological assistance to the patient and his accompanying family members.
Paediatric Guidelines
Children under 2 years old may not exhibit decerebrate posture due to lack of development.
The neurological system retains its immaturity. Nevertheless, if the posture is present, it typically presents as the more severe opisthotonos. Opisthotonos is indeed more prevalent in newborns and young children compared to adults and typically serves as a terminal indication. Head trauma is the primary cause of decerebrate posture in children. It also manifests in Reye's syndrome, which is caused by elevated intracranial pressure leading to compression of the brain stem.
A Comparative Analysis of Decerebrate and Decorticate Postures
A decerebrate posture is caused by injury to the upper brain stem. Assuming this position, the arms are brought front and stretched outward, while the wrists are raised and
The fingers exhibited flexion. The lower limbs are rigidly extended, accompanied by plantar flexion of the feet.
A decorticate posture is the consequence of injury to either one or both corticospinal pathways. Assuming this position, the arms are brought forward and bent, while the wrists and fingers are contracted against the chest. The legs exhibit rigid extension and internal rotation, accompanied by plantar flexion of the foot.

- Published on
Symptoms and Signs – Differential Diagnosis of Cyanosis
Cyanosis is a disorder characterized by a bluish or bluish black pigmentation of the skin and mucous membranes caused by an excessive amount of unoxygenated hemoglobin in the blood serum. This prevalent symptom might manifest either suddenly or gradually. The condition can be categorized as either central or peripheral, but both forms may present simultaneously.
Insufficient oxygenation of systemic arterial blood resulting from right-to-left cardiac shunting, pulmonary illness, or hematologic diseases is shown by central cyanosis. It can manifest on any part of the skin as well as on the mucous membranes of the nasal passages, lips, and conjunctiva.
Peripheral cyanosis is a manifestation of slow peripheral circulation resulting from vasoconstriction, decreased cardiac output, or vascular blockage. While the condition may be either widespread or localised in one extremity, it does not impact mucosal membranes. Commonly, peripheral cyanosis manifests on parts that are visible, such as the fingers, nail beds, feet, nose, and ears.
While cyanosis is a significant indicator of cardiovascular and pulmonary illness, it may not always provide an accurate measure of oxygen saturation. The development of this condition is influenced by several factors, including hemoglobin concentration and oxygen saturation, cardiac output, and partial pressure of arterial oxygen (PaO2). Typically, cyanosis remains undetectable until the oxygen saturation of hemoglobin drops below 80%. The manifestation of severe cyanosis is readily apparent, while the detection of mild cyanosis is more challenging, especially under natural, intense illumination. Cyanosis is especially evident in the mucous membranes and nail beds of individuals with dark complexion.
Environmental causes can cause transient, nonpathologic cyanosis. For instance, peripheral cyanosis can occur when the blood vessels in the skin narrow after a short period of contact to cold air or water. Low atmospheric oxygen levels at high altitudes can lead to central cyanosis.
Urgent medical interventions
Place the affected limb in a dependent position and shield it from harm if the patient exhibits acute, localized cyanosis and other indications of vascular occlusion; but, refrain from massaging the limb. If you observe central cyanosis resulting from a pulmonary medical condition or shock, promptly do an assessment. Promptly institute measures to preserve an airway, aid respiration, and regulate circulation.
Clinical Background and Physical Assessment
A comprehensive examination should be conducted if cyanosis is seen alongside less severe disorders. Start with a medical history, specifically addressing cardiac, pulmonary, and hematologic conditions. Request information regarding prior surgical procedures, administration of prescribed medications, and history of smoking. Next, initiate the physical examination by obtaining the patient's vital signs. Examination of the skin and mucous membranes to ascertain the degree of cyanosis severity. Ask the patient to indicate the initial onset of cyanosis. Does the phenomenon subside and reoccur? Is it worse by cold, smoking, or chronic stress? Does massage or rewarming offer relief? Inspect the skin for signs of warmth, pallor, erythema, discomfort, and ulceration. Note clubbing as well.
Proceed to assess the patient's degree of consciousness. Inquire about the presence of headaches, dizziness, or blurral vision. Next, assess his motor strength. Request information regarding symptoms of pain in the arms and legs, particularly during walking, as well as any unusual feelings such as numbness, tingling, and coldness.
Enquire about the intensity of chest pain. Is it possible for the patient to recognize both aggravating and relieving factors? Assess peripheral pulses by palpation and measure the capillary refill time. Edema should also be noted. Evaluate heart rate and rhythm by auscultation, particularly observing gallops and murmurs. Furthermore, perform auscultation on the abdominal aorta and femoral arteries in order to identify any bruits.
Did the patient present with a cough? Has it been productive? If such is the case, instruct the patient to articulate the sputum. Assess his pulmonary expiratory rate and cardiac rhythm. Monitor for nasal flare and the activation of auxiliary muscles. Inquire about sleep apnea. Does the patient undergo nocturnal elevation with his head supported by pillows? Evaluate the patient for asymmetrical chest expansion or the presence of a barrel chest. Perform pulmonary auscultation to detect dullness or hyperresonance, and auscultate for reduced or adventitious breath sounds.
Perform an abdominal examination to detect ascites, and assess for any changes in dullness or fluid wave. Perform percussive and palpable examination to detect liver enlargement and soreness. Request information on nausea, anorexia, and weight loss.
Medical Causes
Arteriosclerotic occlusive disease (chronic)
Peripheral cyanosis in the legs is a characteristic feature of arteriosclerotic occlusive disease, which manifests whenever the legs are in a dependent position. Signs and symptoms associated with this condition include sporadic claudication and burning pain while at rest, paresthesia, pallor, muscle atrophy, weak leg pulses, and impotence. Late manifestations include leg ulcers and gangrene.
Bronchiectasis
Chronic central cyanosis is a consequence of bronchiectasis. The characteristic presentation, however, is a persistent productive cough accompanied with abundant, unpleasant- malodorous, mucopurulent sputum or coughing up blood. Upon auscultation, rhonchi and coarse crackles are seen during inspiration. Additional manifestations include shortness of breath, repeated episodes of fever and chills, loss of body weight, general malaise, clumping of the joints, and indications of anemia.
Buerger's disease
Buerger's disease is characterized by the initial experience of cold, cyanosis, and numbness in the feet, followed by subsequent reddening, increased temperature, and tingling. Intermittent claudication of the instep is a distinctive feature, further exacerbated by physical activity and smoking, and alleviated by periods of rest. Common manifestations include hypotonic peripheral pulses and, in advanced phases, ulceration, muscular wasting, and gangrene.
Chronic obstructive pulmonary disease (COPD). Chronic central cyanosis manifests in the later stages of chronic obstructive pulmonary disease (COPD) and can be worsened by physical activity. The associated signs and symptoms include dyspnea during physical activity, a cough that produces thick sputum, lack of appetite, weight loss, breathing with pursed lips, rapid breathing, and the usage of auxiliary muscles. Upon examination, wheezing and hyperresonant lung fields are observed. Indicators of late onset include barrel chest and clubbing. Tachycardia, diaphoresis, and flushing may also be present in conjunction with COPD.
Deep vein thrombosis
In cases of deep vein thrombosis, the affected extremity experiences acute peripheral cyanosis, accompanied by soreness, painful movement, edema, warmth, and conspicuous superficial veins. An elicitation of Homans' sign is also possible.
Heart failure
Cardiological failure patients may have either acute or persistent cyanosis. In general, it is a delayed indication and can manifest as either central, peripheral, or both. Central cyanosis accompanying left-sided heart failure is characterized by tachycardia, tiredness, dyspnea, cold intolerance, orthopnea, cough, ventricular or atrial gallop, bibasilar crackles, and a diffuse apical impulse. Onset of right-sided heart failure is accompanied by peripheral cyanosis, tiredness, peripheral edema, ascites, jugular vein distention, and hepatomegaly.
Lung cancer
Long-term lung cancer results in persistent central cyanosis, along with symptoms such as fever, weakness, weight loss, anorexia, difficulty breathing, chest pain, coughing up blood, and wheezing. Atelectasis results in a shift of the mediastinal region, reduced diaphragmatic excursion, asymmetrical expansion of the chest, a dull percussion sound, and reduced breath sounds.
Peripheral arterial occlusion (acute)
Peripheral artery occlusion results in the sudden onset of cyanosis in either one arm or either both legs. Cyanosis is characterized by acute or agonizing discomfort that exacerbates with mobilization. The affected limb also displays paresthesia, muscular weakness, and pallid, chilled skin. The examination indicates a reduced or nonexistent pulse and an elevated capillary refill.
Pneumonia
Typically, pneumonia is preceded by acute central cyanosis, which is characterized by a fever, shaking chills, a cough with purulent sputum, crackles, rhonchi, and pleuritic chest discomfort that worsens with deep inspiration. Manifestations of the condition include increased heart rate, difficulty breathing, rapid breathing, reduced breath sounds, excessive sweating, muscle soreness, exhaustion, headache, and loss of appetite.
Pleumothorax
Acute central cyanosis, a prime indicator of pneumothorax, is characterized by intense chest discomfort that worsens with movement, deep breathing, and coughing; asymmetrical enlargement of the chest wall; and shortness of breath. In addition, the patient may have accelerated, superficial breathing, a feeble, quick pulse, pallor, jugular vein enlargement, anxiousness, and the lack of breath sounds in the enlarged lobe.
Polycythemia vera
In polycythemia vera, a chronic myeloproliferative disease, a rosy complexion that may appear cyanotic is a defining feature. Additional observations comprise hepatosplenomegaly, cephalalgia, vertigo, exhaustion, cutaneous itching, visual impairment, angina, sporadic cramping, and lipid abnormalities.
Pulmonary edema
The clinical presentation of pulmonary edema includes abrupt central cyanosis, dyspnea, orthopnea, frothy, blood-tinged sputum, tachycardia, tachypnea, dependent crackles, a ventricular gallop, cold, clammy skin, hypotension, a weak, thready pulse, and confusion.
Pulmonary embolism
Acute central cyanosis is the result of a substantial blockage of the pulmonary circulation being caused by a massive embolus. Syncope and distension of the jugular vein may also manifest. Further typical indications and manifestations encompass dyspnea, angina, increased heart rate, an irregular pulse, a dry or productive cough with sputum stained with blood, a mild fever, restlessness, and excessive sweating.
Raynaud’s disease
Raynaud's illness is characterised by the first blanching and subsequent coldness, followed by cyanosis, and ultimately reddening subsequent to a restoration of normal temperature in the fingers or hands. In addition, numbness and tingling may manifest. Raynaud's phenomena refers to the parallel manifestation observed in cases with comorbidities such as rheumatoid arthritis, scleroderma, or lupus erythematosus.
Shock
In cases of shock, the hands and feet may exhibit acute peripheral cyanosis, characterized by coldness, clammyness, and pallor. Additional distinguishing features include tiredness, cognitive impairment, an accelerated capillary refill time, and a fast, feeble pulse. In addition, tachypnea, hyperpnea, and hypotension may also manifest.
Apnea. Chronic and severe sleep apnea can lead to pulmonary hypertension and cor pulmonale, which constitute right-sided heart failure.
induce persistent cyanosis.
Key Factors to Consider
Administer more oxygen to alleviate dyspnea, enhance oxygen saturation, and reduce cyanosis. Nevertheless, administer modest dosages (2 liters per minute) to patients with COPD and those experiencing moderate COPD exacerbations. This group of patients may exhibit carbon dioxide retention. Nevertheless, in cases of acute conditions, an initial high-flow oxygen rate may be necessary. It is important to attentively monitor the patient's respiratory drive and make appropriate adjustments to the oxygen dosage. Align the patient in a comfortable position to facilitate respiration. Administer a diuretic, bronchodilator, antibiotic, or cardiac medication as necessary without delay. Assure that the patient has enough intervals of rest between activities to avoid experiencing shortness of breath.
Prepare the patient for diagnostic testing such as arterial blood gas analysis and complete blood count in order to ascertain the underlying cause of cyanosis.
Therapeutic Counseling for Patients
Assure the patient to promptly seek medical intervention in the event of cyanosis. Discuss the proper and secure use of oxygen in residential settings.
Guidelines for Pediatric Populations
Many lung diseases that cause cyanosis in adults also result in cyanosis in children. Furthermore, central cyanosis can arise from cystic fibrosis, asthma, foreign body-induced airway blockage, acute laryngotracheobronchitis, or epiglottitis. Furthermore, it can arise from a congenital cardiac anomaly, such as transposition of the major arteries, which leads to right-to-left intracardiac shunting.
In pediatric patients, circumoral cyanosis may occur before global cyanosis. Infants may develop acrocyanosis, sometimes known as "glove and bootee" cyanosis, due to profuse weeping or exposure to frigid temperatures. Physical exertion and restlessness worsen cyanosis, so it is important to ensure comfort and frequent intervals of rest. Furthermore, provide additional oxygen during periods of cyanosis.
Geriatric Guidelines
With diminished tissue perfusion in older patients, peripheral cyanosis may manifest even with a minor decline in cardiac output or systemic blood pressure.
Cyanosis is a disorder characterized by a bluish or bluish black pigmentation of the skin and mucous membranes caused by an excessive amount of unoxygenated hemoglobin in the blood serum. This prevalent symptom might manifest either suddenly or gradually. The condition can be categorized as either central or peripheral, but both forms may present simultaneously.
Insufficient oxygenation of systemic arterial blood resulting from right-to-left cardiac shunting, pulmonary illness, or hematologic diseases is shown by central cyanosis. It can manifest on any part of the skin as well as on the mucous membranes of the nasal passages, lips, and conjunctiva.
Peripheral cyanosis is a manifestation of slow peripheral circulation resulting from vasoconstriction, decreased cardiac output, or vascular blockage. While the condition may be either widespread or localised in one extremity, it does not impact mucosal membranes. Commonly, peripheral cyanosis manifests on parts that are visible, such as the fingers, nail beds, feet, nose, and ears.
While cyanosis is a significant indicator of cardiovascular and pulmonary illness, it may not always provide an accurate measure of oxygen saturation. The development of this condition is influenced by several factors, including hemoglobin concentration and oxygen saturation, cardiac output, and partial pressure of arterial oxygen (PaO2). Typically, cyanosis remains undetectable until the oxygen saturation of hemoglobin drops below 80%. The manifestation of severe cyanosis is readily apparent, while the detection of mild cyanosis is more challenging, especially under natural, intense illumination. Cyanosis is especially evident in the mucous membranes and nail beds of individuals with dark complexion.
Environmental causes can cause transient, nonpathologic cyanosis. For instance, peripheral cyanosis can occur when the blood vessels in the skin narrow after a short period of contact to cold air or water. Low atmospheric oxygen levels at high altitudes can lead to central cyanosis.
Urgent medical interventions
Place the affected limb in a dependent position and shield it from harm if the patient exhibits acute, localized cyanosis and other indications of vascular occlusion; but, refrain from massaging the limb. If you observe central cyanosis resulting from a pulmonary medical condition or shock, promptly do an assessment. Promptly institute measures to preserve an airway, aid respiration, and regulate circulation.
Clinical Background and Physical Assessment
A comprehensive examination should be conducted if cyanosis is seen alongside less severe disorders. Start with a medical history, specifically addressing cardiac, pulmonary, and hematologic conditions. Request information regarding prior surgical procedures, administration of prescribed medications, and history of smoking. Next, initiate the physical examination by obtaining the patient's vital signs. Examination of the skin and mucous membranes to ascertain the degree of cyanosis severity. Ask the patient to indicate the initial onset of cyanosis. Does the phenomenon subside and reoccur? Is it worse by cold, smoking, or chronic stress? Does massage or rewarming offer relief? Inspect the skin for signs of warmth, pallor, erythema, discomfort, and ulceration. Note clubbing as well.
Proceed to assess the patient's degree of consciousness. Inquire about the presence of headaches, dizziness, or blurral vision. Next, assess his motor strength. Request information regarding symptoms of pain in the arms and legs, particularly during walking, as well as any unusual feelings such as numbness, tingling, and coldness.
Enquire about the intensity of chest pain. Is it possible for the patient to recognize both aggravating and relieving factors? Assess peripheral pulses by palpation and measure the capillary refill time. Edema should also be noted. Evaluate heart rate and rhythm by auscultation, particularly observing gallops and murmurs. Furthermore, perform auscultation on the abdominal aorta and femoral arteries in order to identify any bruits.
Did the patient present with a cough? Has it been productive? If such is the case, instruct the patient to articulate the sputum. Assess his pulmonary expiratory rate and cardiac rhythm. Monitor for nasal flare and the activation of auxiliary muscles. Inquire about sleep apnea. Does the patient undergo nocturnal elevation with his head supported by pillows? Evaluate the patient for asymmetrical chest expansion or the presence of a barrel chest. Perform pulmonary auscultation to detect dullness or hyperresonance, and auscultate for reduced or adventitious breath sounds.
Perform an abdominal examination to detect ascites, and assess for any changes in dullness or fluid wave. Perform percussive and palpable examination to detect liver enlargement and soreness. Request information on nausea, anorexia, and weight loss.
Medical Causes
Arteriosclerotic occlusive disease (chronic)
Peripheral cyanosis in the legs is a characteristic feature of arteriosclerotic occlusive disease, which manifests whenever the legs are in a dependent position. Signs and symptoms associated with this condition include sporadic claudication and burning pain while at rest, paresthesia, pallor, muscle atrophy, weak leg pulses, and impotence. Late manifestations include leg ulcers and gangrene.
Bronchiectasis
Chronic central cyanosis is a consequence of bronchiectasis. The characteristic presentation, however, is a persistent productive cough accompanied with abundant, unpleasant- malodorous, mucopurulent sputum or coughing up blood. Upon auscultation, rhonchi and coarse crackles are seen during inspiration. Additional manifestations include shortness of breath, repeated episodes of fever and chills, loss of body weight, general malaise, clumping of the joints, and indications of anemia.
Buerger's disease
Buerger's disease is characterized by the initial experience of cold, cyanosis, and numbness in the feet, followed by subsequent reddening, increased temperature, and tingling. Intermittent claudication of the instep is a distinctive feature, further exacerbated by physical activity and smoking, and alleviated by periods of rest. Common manifestations include hypotonic peripheral pulses and, in advanced phases, ulceration, muscular wasting, and gangrene.
Chronic obstructive pulmonary disease (COPD). Chronic central cyanosis manifests in the later stages of chronic obstructive pulmonary disease (COPD) and can be worsened by physical activity. The associated signs and symptoms include dyspnea during physical activity, a cough that produces thick sputum, lack of appetite, weight loss, breathing with pursed lips, rapid breathing, and the usage of auxiliary muscles. Upon examination, wheezing and hyperresonant lung fields are observed. Indicators of late onset include barrel chest and clubbing. Tachycardia, diaphoresis, and flushing may also be present in conjunction with COPD.
Deep vein thrombosis
In cases of deep vein thrombosis, the affected extremity experiences acute peripheral cyanosis, accompanied by soreness, painful movement, edema, warmth, and conspicuous superficial veins. An elicitation of Homans' sign is also possible.
Heart failure
Cardiological failure patients may have either acute or persistent cyanosis. In general, it is a delayed indication and can manifest as either central, peripheral, or both. Central cyanosis accompanying left-sided heart failure is characterized by tachycardia, tiredness, dyspnea, cold intolerance, orthopnea, cough, ventricular or atrial gallop, bibasilar crackles, and a diffuse apical impulse. Onset of right-sided heart failure is accompanied by peripheral cyanosis, tiredness, peripheral edema, ascites, jugular vein distention, and hepatomegaly.
Lung cancer
Long-term lung cancer results in persistent central cyanosis, along with symptoms such as fever, weakness, weight loss, anorexia, difficulty breathing, chest pain, coughing up blood, and wheezing. Atelectasis results in a shift of the mediastinal region, reduced diaphragmatic excursion, asymmetrical expansion of the chest, a dull percussion sound, and reduced breath sounds.
Peripheral arterial occlusion (acute)
Peripheral artery occlusion results in the sudden onset of cyanosis in either one arm or either both legs. Cyanosis is characterized by acute or agonizing discomfort that exacerbates with mobilization. The affected limb also displays paresthesia, muscular weakness, and pallid, chilled skin. The examination indicates a reduced or nonexistent pulse and an elevated capillary refill.
Pneumonia
Typically, pneumonia is preceded by acute central cyanosis, which is characterized by a fever, shaking chills, a cough with purulent sputum, crackles, rhonchi, and pleuritic chest discomfort that worsens with deep inspiration. Manifestations of the condition include increased heart rate, difficulty breathing, rapid breathing, reduced breath sounds, excessive sweating, muscle soreness, exhaustion, headache, and loss of appetite.
Pleumothorax
Acute central cyanosis, a prime indicator of pneumothorax, is characterized by intense chest discomfort that worsens with movement, deep breathing, and coughing; asymmetrical enlargement of the chest wall; and shortness of breath. In addition, the patient may have accelerated, superficial breathing, a feeble, quick pulse, pallor, jugular vein enlargement, anxiousness, and the lack of breath sounds in the enlarged lobe.
Polycythemia vera
In polycythemia vera, a chronic myeloproliferative disease, a rosy complexion that may appear cyanotic is a defining feature. Additional observations comprise hepatosplenomegaly, cephalalgia, vertigo, exhaustion, cutaneous itching, visual impairment, angina, sporadic cramping, and lipid abnormalities.
Pulmonary edema
The clinical presentation of pulmonary edema includes abrupt central cyanosis, dyspnea, orthopnea, frothy, blood-tinged sputum, tachycardia, tachypnea, dependent crackles, a ventricular gallop, cold, clammy skin, hypotension, a weak, thready pulse, and confusion.
Pulmonary embolism
Acute central cyanosis is the result of a substantial blockage of the pulmonary circulation being caused by a massive embolus. Syncope and distension of the jugular vein may also manifest. Further typical indications and manifestations encompass dyspnea, angina, increased heart rate, an irregular pulse, a dry or productive cough with sputum stained with blood, a mild fever, restlessness, and excessive sweating.
Raynaud’s disease
Raynaud's illness is characterised by the first blanching and subsequent coldness, followed by cyanosis, and ultimately reddening subsequent to a restoration of normal temperature in the fingers or hands. In addition, numbness and tingling may manifest. Raynaud's phenomena refers to the parallel manifestation observed in cases with comorbidities such as rheumatoid arthritis, scleroderma, or lupus erythematosus.
Shock
In cases of shock, the hands and feet may exhibit acute peripheral cyanosis, characterized by coldness, clammyness, and pallor. Additional distinguishing features include tiredness, cognitive impairment, an accelerated capillary refill time, and a fast, feeble pulse. In addition, tachypnea, hyperpnea, and hypotension may also manifest.
Apnea. Chronic and severe sleep apnea can lead to pulmonary hypertension and cor pulmonale, which constitute right-sided heart failure.
induce persistent cyanosis.
Key Factors to Consider
Administer more oxygen to alleviate dyspnea, enhance oxygen saturation, and reduce cyanosis. Nevertheless, administer modest dosages (2 liters per minute) to patients with COPD and those experiencing moderate COPD exacerbations. This group of patients may exhibit carbon dioxide retention. Nevertheless, in cases of acute conditions, an initial high-flow oxygen rate may be necessary. It is important to attentively monitor the patient's respiratory drive and make appropriate adjustments to the oxygen dosage. Align the patient in a comfortable position to facilitate respiration. Administer a diuretic, bronchodilator, antibiotic, or cardiac medication as necessary without delay. Assure that the patient has enough intervals of rest between activities to avoid experiencing shortness of breath.
Prepare the patient for diagnostic testing such as arterial blood gas analysis and complete blood count in order to ascertain the underlying cause of cyanosis.
Therapeutic Counseling for Patients
Assure the patient to promptly seek medical intervention in the event of cyanosis. Discuss the proper and secure use of oxygen in residential settings.
Guidelines for Pediatric Populations
Many lung diseases that cause cyanosis in adults also result in cyanosis in children. Furthermore, central cyanosis can arise from cystic fibrosis, asthma, foreign body-induced airway blockage, acute laryngotracheobronchitis, or epiglottitis. Furthermore, it can arise from a congenital cardiac anomaly, such as transposition of the major arteries, which leads to right-to-left intracardiac shunting.
In pediatric patients, circumoral cyanosis may occur before global cyanosis. Infants may develop acrocyanosis, sometimes known as "glove and bootee" cyanosis, due to profuse weeping or exposure to frigid temperatures. Physical exertion and restlessness worsen cyanosis, so it is important to ensure comfort and frequent intervals of rest. Furthermore, provide additional oxygen during periods of cyanosis.
Geriatric Guidelines
With diminished tissue perfusion in older patients, peripheral cyanosis may manifest even with a minor decline in cardiac output or systemic blood pressure.

- Published on
Symptoms and Signs – Differential Diagnosis of Hyperactive Deep tendon reflexes
A hyperactive deep tendon reflex (DTR) is an unusually rapid muscular contraction that happens when the tendon of insertion of a muscle is abruptly stretched by vigorous tapping. This evoked indication can be classified as either brisk or pathologically overactive. Frequently, hyperactive DTRs are accompanied by clonus activity.
The corticospinal tract and other descending tracts regulate the reflex arc, which is the sequential process that generates any form of reflex reaction. Hyperactive delayed tricuspid reflexes (DTRs) may occur when a corticospinal lesion is located above the level of the reflex arc being evaluated. Aberrant neuromuscular transmission at the termination of the reflex arc can also lead to excessively active delayed tricuspid reflexes (DTRs). For instance, a lack of calcium or magnesium might lead to the development of hyperactive DTRs as these electrolytes control excitation of the neuromuscular system.
While high levels of DTRs often coexist with other neurological symptoms, they often do not have precise diagnostic significance. Specifically, they serve as an early and crucial indication of hypocalcemia.
Historical Background and Physical Assessment
Obtain the patient's medical history after generating hyperactive DTRs. Inquire about any history of spinal cord injury or other traumatic events, as well as any extended periods of exposure to cold, wind, or water. Is it possible that the patient is pregnant? Answering any of these questions affirmatively necessitates immediate assessment to exclude the possibility of life-threatening autonomic hyperreflexia, tetanus, preeclampsia, or hypothermia. Request information regarding the beginning and development of related indications and symptoms. Next, conduct a neurological assessment. Ascertain the patient's degree of awareness and assess the motor and sensory capabilities in the extremities. Inquire about paresthesia. Assess for ataxia or tremors, as well as for impairments in speech and vision. Check for Chvostek's (an atypical contraction of the facial muscles caused by gentle stimulation of the facial nerve in a patient with low calcium levels) and Trousseau's (a spasm of the carpal nerve caused by inflating a sphygmomanometer cuff on the upper arm to a pressure higher than the systolic blood pressure for 3 minutes in a patient with low calcium or low magnesium levels) indications, as well as for carpopedal spasm. Enquire about any episodes of vomiting or changes in bladder patterns. Ensure documentation of the patient's vital signs.
Medical Causes
Amyotrophic lateral sclerosis (ALS)
Amyotrophic lateral sclerosis (ALS) causes widespread hyperactive dextrose-dependent response (DTR) followed by hand and forearm weakness and leg stiffness. In due course, the patient has muscle atrophy in the neck and tongue, fasciculations, leg weakness, and potentially bulbar symptoms such as dysphagia, dysphonia, face weakness, and dyspnea.
Brain tumor
A brain tumor induces overactive dendritic tissue receptors on the side transverse to the lesion. The associated signs and symptoms manifest gradually and may encompass unilateral paresis or paralysis, anesthesia, limitations in the visual field, spasticity, and a positive Babinski's reflex.
Hypocalcemia
Hypocalcemia can cause a rapid or slow development of widespread hyperactive diabetic dilated reflexes (DTRs) accompanied by paresthesia, muscle twitching and cramping, positive Chvostek's and Trousseau's signs, carpopedal spasm, and tetany.
Hypomagnesemia
Hypomagnesemia leads to the progressive development of widespread hyperactive diffuse thrombocytopenias (DTRs) accompanied by muscle cramps, low blood pressure, rapid heart rate, sensitivity to light, lack of coordination, tetany, and perhaps, seizures.
Hypothermia
Mild hypothermia within the temperature range of 90°F to 94°F [32.2°C to 34.4°C] leads to the development of widespread hyperactive DTRs. Other manifestations include shivering, exhaustion, debility, lethargy, slurred speech, ataxia, muscular rigidity, rapid heart rate, increased urine production, difficulty breathing, low blood pressure, and cold, pale skin.
Preeclampsia
Preeclampsia, which occurs during pregnancy at least 20 weeks gestation, can lead to a slow development of widespread hyperactive diabetic talonopathy (DTRs). Common manifestations include elevated blood pressure, atypical weight increase, swelling of the face, fingers, and abdomen following periods of bed rest, presence of albumin in the urine, reduced urine production, intense headache, impaired or double vision, epigastric pain, nausea and vomiting, irritability, cyanosis, dyspnea, and crackles. In the event that preeclampsia advances to eclampsia, the patient experiences convulsions.
Spinal cord lesion
Incomplete spinal cord lesions result in overactive dendritic tissue receptors (DTRs) located below the damage site. Hyperactive delayed T-reactions (DTRs) occur after the resolution of spinal shock in a traumatic lesion. Over time, hyperactive dendritic tissue receptors (DTRs) progressively replace normal DTRs in a malignant lesion. Additional manifestations include paralysis and sensory impairment below the lesion site, urinary retention and overflow incontinence, as well as recurrent episodes of constipation and diarrhea. Lesions located above the T6 vertebra may also cause autonomic hyperreflexia characterized by excessive sweating and flushing above the lesion level, headache, nasal congestion, nausea, elevated blood pressure, and bradycardia.
Cerebrovascular accident
A stroke impacting the source of the corticospinal tracts leads to the abrupt development of overactive dorsal tegmental receptors on the side opposed to the injury. Furthermore, the patient may have unilateral paresis or paralysis, anaesthesia, visual field impairments, spasticity, and a positive Babinski's reflex.
Tetanus
Tetanus is characterized by the abrupt development of widespread hyperactive DTRs, along with tachycardia, diaphoresis, a mild fever, painful and involuntary muscle spasms, trismus (lockjaw), and risus sardonicus (a masklike grin).
Points of Special Consideration
Prepare the patient for diagnostic tests to assess hyperactive Delirium Tremens Retinopathy (DTR). These may encompass assays for serum calcium, magnesium, and ammonia concentrations, radiography of the spine, magnetic resonance imaging, a computed tomography scan, puncture of the lumbar region, and myelography.
When motor weakness is present alongside hyperactive deep vein thrombosis (DTRs), it is advisable to carry out or promote range-of-motion exercises in order to maintain muscle integrity and avoid the formation of deep vein thrombosis. Furthermore, it is important to regularly reposition the patient, offer a specialized mattress, massage his back, and guarantee sufficient nourishment to avoid skin breakdown. The use of a muscle relaxant and sedative is recommended to alleviate intense muscle spasms. Retain readily available emergency resuscitation equipment. Provide a serene and tranquil
A conducive environment to reduce neuromuscular excitability. Provide assistance with tasks related to everyday living and offer emotional support.
Therapeutic Counseling for Patients
Outline to the caregiver the necessary procedures and therapies that the patient may require. Elaborate on safety protocols and offer necessary emotional assistance.
Key Pediatric Resources
In neonates, hyperreflexia can be considered a typical abnormality. Reflex reactions in children beyond the age of 6 resemble those of healthy adults. Employing distraction strategies during the assessment of DTRs in young children will enhance the reliability of the results.
Pediatric cerebral palsy often leads to overactive delayed trophic responses (DTRs). Stage II of Reye's syndrome results in widespread hyperactive DTRs, while stage V is characterized by the absence of DTRs. Causing factors of overactive DTRs in adults may also manifest in youngsters.
A hyperactive deep tendon reflex (DTR) is an unusually rapid muscular contraction that happens when the tendon of insertion of a muscle is abruptly stretched by vigorous tapping. This evoked indication can be classified as either brisk or pathologically overactive. Frequently, hyperactive DTRs are accompanied by clonus activity.
The corticospinal tract and other descending tracts regulate the reflex arc, which is the sequential process that generates any form of reflex reaction. Hyperactive delayed tricuspid reflexes (DTRs) may occur when a corticospinal lesion is located above the level of the reflex arc being evaluated. Aberrant neuromuscular transmission at the termination of the reflex arc can also lead to excessively active delayed tricuspid reflexes (DTRs). For instance, a lack of calcium or magnesium might lead to the development of hyperactive DTRs as these electrolytes control excitation of the neuromuscular system.
While high levels of DTRs often coexist with other neurological symptoms, they often do not have precise diagnostic significance. Specifically, they serve as an early and crucial indication of hypocalcemia.
Historical Background and Physical Assessment
Obtain the patient's medical history after generating hyperactive DTRs. Inquire about any history of spinal cord injury or other traumatic events, as well as any extended periods of exposure to cold, wind, or water. Is it possible that the patient is pregnant? Answering any of these questions affirmatively necessitates immediate assessment to exclude the possibility of life-threatening autonomic hyperreflexia, tetanus, preeclampsia, or hypothermia. Request information regarding the beginning and development of related indications and symptoms. Next, conduct a neurological assessment. Ascertain the patient's degree of awareness and assess the motor and sensory capabilities in the extremities. Inquire about paresthesia. Assess for ataxia or tremors, as well as for impairments in speech and vision. Check for Chvostek's (an atypical contraction of the facial muscles caused by gentle stimulation of the facial nerve in a patient with low calcium levels) and Trousseau's (a spasm of the carpal nerve caused by inflating a sphygmomanometer cuff on the upper arm to a pressure higher than the systolic blood pressure for 3 minutes in a patient with low calcium or low magnesium levels) indications, as well as for carpopedal spasm. Enquire about any episodes of vomiting or changes in bladder patterns. Ensure documentation of the patient's vital signs.
Medical Causes
Amyotrophic lateral sclerosis (ALS)
Amyotrophic lateral sclerosis (ALS) causes widespread hyperactive dextrose-dependent response (DTR) followed by hand and forearm weakness and leg stiffness. In due course, the patient has muscle atrophy in the neck and tongue, fasciculations, leg weakness, and potentially bulbar symptoms such as dysphagia, dysphonia, face weakness, and dyspnea.
Brain tumor
A brain tumor induces overactive dendritic tissue receptors on the side transverse to the lesion. The associated signs and symptoms manifest gradually and may encompass unilateral paresis or paralysis, anesthesia, limitations in the visual field, spasticity, and a positive Babinski's reflex.
Hypocalcemia
Hypocalcemia can cause a rapid or slow development of widespread hyperactive diabetic dilated reflexes (DTRs) accompanied by paresthesia, muscle twitching and cramping, positive Chvostek's and Trousseau's signs, carpopedal spasm, and tetany.
Hypomagnesemia
Hypomagnesemia leads to the progressive development of widespread hyperactive diffuse thrombocytopenias (DTRs) accompanied by muscle cramps, low blood pressure, rapid heart rate, sensitivity to light, lack of coordination, tetany, and perhaps, seizures.
Hypothermia
Mild hypothermia within the temperature range of 90°F to 94°F [32.2°C to 34.4°C] leads to the development of widespread hyperactive DTRs. Other manifestations include shivering, exhaustion, debility, lethargy, slurred speech, ataxia, muscular rigidity, rapid heart rate, increased urine production, difficulty breathing, low blood pressure, and cold, pale skin.
Preeclampsia
Preeclampsia, which occurs during pregnancy at least 20 weeks gestation, can lead to a slow development of widespread hyperactive diabetic talonopathy (DTRs). Common manifestations include elevated blood pressure, atypical weight increase, swelling of the face, fingers, and abdomen following periods of bed rest, presence of albumin in the urine, reduced urine production, intense headache, impaired or double vision, epigastric pain, nausea and vomiting, irritability, cyanosis, dyspnea, and crackles. In the event that preeclampsia advances to eclampsia, the patient experiences convulsions.
Spinal cord lesion
Incomplete spinal cord lesions result in overactive dendritic tissue receptors (DTRs) located below the damage site. Hyperactive delayed T-reactions (DTRs) occur after the resolution of spinal shock in a traumatic lesion. Over time, hyperactive dendritic tissue receptors (DTRs) progressively replace normal DTRs in a malignant lesion. Additional manifestations include paralysis and sensory impairment below the lesion site, urinary retention and overflow incontinence, as well as recurrent episodes of constipation and diarrhea. Lesions located above the T6 vertebra may also cause autonomic hyperreflexia characterized by excessive sweating and flushing above the lesion level, headache, nasal congestion, nausea, elevated blood pressure, and bradycardia.
Cerebrovascular accident
A stroke impacting the source of the corticospinal tracts leads to the abrupt development of overactive dorsal tegmental receptors on the side opposed to the injury. Furthermore, the patient may have unilateral paresis or paralysis, anaesthesia, visual field impairments, spasticity, and a positive Babinski's reflex.
Tetanus
Tetanus is characterized by the abrupt development of widespread hyperactive DTRs, along with tachycardia, diaphoresis, a mild fever, painful and involuntary muscle spasms, trismus (lockjaw), and risus sardonicus (a masklike grin).
Points of Special Consideration
Prepare the patient for diagnostic tests to assess hyperactive Delirium Tremens Retinopathy (DTR). These may encompass assays for serum calcium, magnesium, and ammonia concentrations, radiography of the spine, magnetic resonance imaging, a computed tomography scan, puncture of the lumbar region, and myelography.
When motor weakness is present alongside hyperactive deep vein thrombosis (DTRs), it is advisable to carry out or promote range-of-motion exercises in order to maintain muscle integrity and avoid the formation of deep vein thrombosis. Furthermore, it is important to regularly reposition the patient, offer a specialized mattress, massage his back, and guarantee sufficient nourishment to avoid skin breakdown. The use of a muscle relaxant and sedative is recommended to alleviate intense muscle spasms. Retain readily available emergency resuscitation equipment. Provide a serene and tranquil
A conducive environment to reduce neuromuscular excitability. Provide assistance with tasks related to everyday living and offer emotional support.
Therapeutic Counseling for Patients
Outline to the caregiver the necessary procedures and therapies that the patient may require. Elaborate on safety protocols and offer necessary emotional assistance.
Key Pediatric Resources
In neonates, hyperreflexia can be considered a typical abnormality. Reflex reactions in children beyond the age of 6 resemble those of healthy adults. Employing distraction strategies during the assessment of DTRs in young children will enhance the reliability of the results.
Pediatric cerebral palsy often leads to overactive delayed trophic responses (DTRs). Stage II of Reye's syndrome results in widespread hyperactive DTRs, while stage V is characterized by the absence of DTRs. Causing factors of overactive DTRs in adults may also manifest in youngsters.
- Published on
Symptoms and Signs – Differential Diagnosis of Bony Crepitus
Bony crepitation is a detectable vibration or an audible crunching sound caused by the grating of one bone against another. This indication often arises from a fracture, but it can also occur when bones that have been deprived of their protecting articular cartilage collapse against one other during articulation, as seen in individuals with advanced arthritic or degenerative joint diseases.
The induction of bone crepitation can serve as a means to validate the diagnosis of a fracture; but, it can also result in further damage to soft tissue, nerve and blood vessels. It is imperative to always assess distal pulses and conduct neurological examinations distal to the suspected fracture site prior to moving an extremity. Furthermore, the process of pressing the ends of broken bones together can transform a closed fracture into an open one if one of the bone ends has penetrated the skin. Thus, it is advisable to refrain from further elicitation of crepitation in a patient with a fracture after the initial identification of this indication.
Historical Background and Physical Assessment
Upon identifying bony crepitation in a patient with a suspected fracture, inquire about the presence of pain and seek confirmation of the specific location of the discomfort. To avoid causing damage to nerves, blood vessels, or other tissues, immobilize the afflicted region by placing a splint that fully covers the joints both above and below the affected area. Increase the elevation of the afflicted region, if feasible, and administer cold compresses. Examine for any signs of abrasions or lacerations. Ascertain the manner and timing of the injury. Pulse distal to the location of damage; examine the skin for pallor or coldness. Assess peripheral motor and sensory function beyond the site of damage.
In the absence of a suspected fracture, inquire about any prior incidents of osteoarthritis or rheumatoid arthritis in the patient. What pharmaceuticals does he consume? Have any pharmaceutical interventions alleviated arthritic pain? Perform a comprehensive assessment of the patient's vital signs and evaluate his joint range of motion (ROM).
Clinical etiology
Fracture
A fracture not only presents with bony crepitation but also results in acute local pain, hemorrhage, edema, and reduced range of motion. Additional findings may encompass limb deformity, point discomfort, limb discolouration, and limb function impairment. Neurovascular injury can result in prolonged capillary refill time, reduced or absent pulses, spotted cyanosis, paresthesia, and hypotension.
Sensory perception (located distal to the location of fracture). Of course, an open fracture results in a conspicuous skin wound.
Osteoarthritis
At its most advanced stage, joint crepitation can be induced during range of motion testing. Palpating a soft small crepitus may suggest roughening of the articular cartilage, while a coarse grating may confirm severely injured cartilage. The primary indication of osteoarthritis is inflamed joint discomfort, particularly experienced during movement and bearing weight. Further observations include the presence of joint rigidity that usually manifests after periods of inactivity and diminishes within a few minutes once the patient initiates movement.
Rheumatoid arthritis
Bony crepitation, at its advanced stage, is audible when the afflicted joint is rotated. Nevertheless, rheumatoid arthritis sometimes manifests gradually, causing nonspecific indications and symptoms, including exhaustion, malaise, loss of appetite, a chronic low-grade fever, weight loss, and vague swelling and pain in the joints and muscles. Later, more precise and localized articular symptoms emerge, often at the joints of the proximal fingers. The symptoms often manifest bilaterally and symmetrically, radiating to the wrists, knees, elbows, and ankles. The joints in question become rigid after periods of inactivity. Furthermore, the patient exhibits heightened warmth, edema, and soreness in the afflicted joints, together with restricted range of motion.
Points of Special Consideration
If a fracture is suspected, the patient should be prepared for X-ray imaging of the afflicted region and undergo regular reassessment of his neurovascular profile. Maintain immobility and elevation of the afflicted area until treatment commences. Administer an analgesic to alleviate acute pain.
It is important to note that degenerative joint changes, often initiated by age 20 or 30, escalate more quickly after age 40 and mostly manifest in weight-bearing joints, including the lumbar spine, hips, knees, and ankles.
Conducting Patient Counseling
Educate the patient on the concept of activity restriction. Demonstrate to the patient the proper use of ambulatory aids, including walkers, canes, and crutches, as well as the protocols for skin and foot care. Elaborate on the application of correct body mechanics to avoid harm. Promote the patient's engagement in activities of daily living to the greatest extent feasible in order to preserve independence, muscular strength, and joint range of motion. If the patient is wearing a cast, provide instructions on appropriate cast maintenance and when to seek medical assistance.
Guidelines for Pediatric Populations
In children, bone crepitation often develops subsequent to a fracture. Collect a precise medical record of the injuries and remain vigilant for any signs of child abuse. Bony crepitation and discomfort in the patellofemoral joint are diagnostic indicators for chondromalacia of the patella in adolescents.
Bony crepitation is a detectable vibration or an audible crunching sound caused by the grating of one bone against another. This indication often arises from a fracture, but it can also occur when bones that have been deprived of their protecting articular cartilage collapse against one other during articulation, as seen in individuals with advanced arthritic or degenerative joint diseases.
The induction of bone crepitation can serve as a means to validate the diagnosis of a fracture; but, it can also result in further damage to soft tissue, nerve and blood vessels. It is imperative to always assess distal pulses and conduct neurological examinations distal to the suspected fracture site prior to moving an extremity. Furthermore, the process of pressing the ends of broken bones together can transform a closed fracture into an open one if one of the bone ends has penetrated the skin. Thus, it is advisable to refrain from further elicitation of crepitation in a patient with a fracture after the initial identification of this indication.
Historical Background and Physical Assessment
Upon identifying bony crepitation in a patient with a suspected fracture, inquire about the presence of pain and seek confirmation of the specific location of the discomfort. To avoid causing damage to nerves, blood vessels, or other tissues, immobilize the afflicted region by placing a splint that fully covers the joints both above and below the affected area. Increase the elevation of the afflicted region, if feasible, and administer cold compresses. Examine for any signs of abrasions or lacerations. Ascertain the manner and timing of the injury. Pulse distal to the location of damage; examine the skin for pallor or coldness. Assess peripheral motor and sensory function beyond the site of damage.
In the absence of a suspected fracture, inquire about any prior incidents of osteoarthritis or rheumatoid arthritis in the patient. What pharmaceuticals does he consume? Have any pharmaceutical interventions alleviated arthritic pain? Perform a comprehensive assessment of the patient's vital signs and evaluate his joint range of motion (ROM).
Clinical etiology
Fracture
A fracture not only presents with bony crepitation but also results in acute local pain, hemorrhage, edema, and reduced range of motion. Additional findings may encompass limb deformity, point discomfort, limb discolouration, and limb function impairment. Neurovascular injury can result in prolonged capillary refill time, reduced or absent pulses, spotted cyanosis, paresthesia, and hypotension.
Sensory perception (located distal to the location of fracture). Of course, an open fracture results in a conspicuous skin wound.
Osteoarthritis
At its most advanced stage, joint crepitation can be induced during range of motion testing. Palpating a soft small crepitus may suggest roughening of the articular cartilage, while a coarse grating may confirm severely injured cartilage. The primary indication of osteoarthritis is inflamed joint discomfort, particularly experienced during movement and bearing weight. Further observations include the presence of joint rigidity that usually manifests after periods of inactivity and diminishes within a few minutes once the patient initiates movement.
Rheumatoid arthritis
Bony crepitation, at its advanced stage, is audible when the afflicted joint is rotated. Nevertheless, rheumatoid arthritis sometimes manifests gradually, causing nonspecific indications and symptoms, including exhaustion, malaise, loss of appetite, a chronic low-grade fever, weight loss, and vague swelling and pain in the joints and muscles. Later, more precise and localized articular symptoms emerge, often at the joints of the proximal fingers. The symptoms often manifest bilaterally and symmetrically, radiating to the wrists, knees, elbows, and ankles. The joints in question become rigid after periods of inactivity. Furthermore, the patient exhibits heightened warmth, edema, and soreness in the afflicted joints, together with restricted range of motion.
Points of Special Consideration
If a fracture is suspected, the patient should be prepared for X-ray imaging of the afflicted region and undergo regular reassessment of his neurovascular profile. Maintain immobility and elevation of the afflicted area until treatment commences. Administer an analgesic to alleviate acute pain.
It is important to note that degenerative joint changes, often initiated by age 20 or 30, escalate more quickly after age 40 and mostly manifest in weight-bearing joints, including the lumbar spine, hips, knees, and ankles.
Conducting Patient Counseling
Educate the patient on the concept of activity restriction. Demonstrate to the patient the proper use of ambulatory aids, including walkers, canes, and crutches, as well as the protocols for skin and foot care. Elaborate on the application of correct body mechanics to avoid harm. Promote the patient's engagement in activities of daily living to the greatest extent feasible in order to preserve independence, muscular strength, and joint range of motion. If the patient is wearing a cast, provide instructions on appropriate cast maintenance and when to seek medical assistance.
Guidelines for Pediatric Populations
In children, bone crepitation often develops subsequent to a fracture. Collect a precise medical record of the injuries and remain vigilant for any signs of child abuse. Bony crepitation and discomfort in the patellofemoral joint are diagnostic indicators for chondromalacia of the patella in adolescents.

- Published on
Symptoms and Signs – Differential Diagnosis of Nonproductive Cough
An unproductive cough is a loud and vigorous expulsion of air from the lungs that is devoid of moisture, does not stimulate the production of mucus, and may produce a little quantity of sputum. Among individuals with respiratory problems, it is one of the most often reported concerns.
The act of coughing serves as a defensive strategy to empty the airway spaces. Nevertheless, a nonproductive cough is ineffectual and can result in harm, such as the collapse of the airway or the rupture of alveoli or protuberances. An initially nonproductive cough that subsequently turns productive is a characteristic indication of a developing respiratory illness, such as pneumonia.
The cough reflex often arises from the activation of cough receptors by mechanical, chemical, thermal, inflammatory, or psychogenic stimuli. Refer to Nevertheless, external pressure, such as, Viral inflammation of the subdiaphragm or a mediastinal tumor can also trigger it, along with voluntary exhalation of air, which sometimes happens as a neurological habit. Nonproductive cough may also be caused by specific medications, such as angiotensin-converting enzyme inhibitors.
A nonproductive cough might manifest as paroxysms and may then exacerbate by increasing in frequency. A quick onset acute cough may go away on its own; a cough lasting more than one month is classified as chronic and often arises from cigarette smoking.
An individual with a persistent nonproductive cough may minimize or disregard it, instead accepting it as a typical symptom. Indeed, he typically will not seek medical intervention unless he presents with additional symptoms. Cystoid cough may occur when a foreign object enters the external auditory canal of a youngster. Thoroughly inspect the child's ears.
Ask the patient about recent illness (especially a cardiovascular or pulmonary disorder), surgery, or trauma. Also, ask about hypersensitivity to drugs, foods, pets, dust, or pollen. Find out which medications the patient takes, if any, and ask about recent changes in schedule or dosages. Also, ask about recent changes in his appetite, weight, exercise tolerance, or energy level and recent exposure to irritating fumes, chemicals, or smoke.
As you’re taking his history, observe the patient’s general appearance and manner: Is he agitated, restless, or lethargic; pale, diaphoretic, or flushed; anxious, confused, or nervous? Also, note whether he’s cyanotic or has clubbed fingers or peripheral edema.
Given the apprehension of being identified as someone afflicted with tuberculosis (TB), the patient may hesitate to provide details on his indications and manifestations, such as a cough. Request information from the patient who is at risk for tuberculosis (TB) - whether they were born in a different country, had contact with acute TB, or engaged in high-risk activities - on possible exposure to TB.
Proceed to do a physical examination. Begin by assessing the patient's vital signs. Assess the depth and cadence of his respirations, and make a record of any wheezing or "crowing" sounds. Feel the patient's dermal surface: Is it rather cold?
Is it warm, clammy, or dry? Assess his nasal and oral cavities for congestion, irritation, discharge, or indications of infection. Examine his neck for dilated jugular veins and deviation of the trachea, and examine for any firm lumps or swollen lymph nodes by palpation.
Inspect his chest, carefully analyzing its structure and searching for any atypical movement of the chest wall. Do any retractions or use of auxiliary muscles come to your attention? Detect dullness, tympany, or flatness via percussion. Conduct auscultation to detect wheezing, crackles, rhonchi, pleural friction rubs, and reduced or missing breath sounds. Lastly, visually inspect his belly for any signs of distension, pain, lumps, or abnormal bowel noises.
A Critical Analysis of the Cough Mechanism The anatomical distribution of cough receptors is believed to include the nose, sinuses, auditory canals, nasopharynx, larynx, trachea, bronchi, pleurae, diaphragm, and potentially the pericardium and gastrointestinal system. Upon stimulation of a cough receptor, the vagus and glossopharyngeal nerves convey the impulse to the "cough center" located in the medulla. Subsequently, the impulse is conveyed to the larynx as well as to the intercostal and abdominal muscles. Profound inspiration is
then the glottis closes, the diaphragm relaxes, and the abdominal and intercostal muscles contract. The subsequent elevation in lung pressure causes the glottis to open, allowing for the expulsion of a powerful and loud exhalation referred to as a cough.
Medical Causes
Airway occlusion
Upper airway partial blockage results in an abrupt onset of dry, paroxysmal coughing. The patient is experiencing dyspnea, wheezing, and hoarseness, accompanied by stridor, rapid heart rate, and reduced breath sounds.
Anthrax (inhalation)
The acute infectious disease known as anthrax is attributed to the gram-positive, spore-forming bacterium Bacillus anthracis. While the disease mostly affects wild and domestic grazing animals, such as cattle, sheep, and goats, the spores can persist in the soil for an extended period through many years. The disease can manifest in humans who are exposed to infectious animals, diseased animal tissue, or as a result of biological warfare. Primarily, natural cases manifest in agricultural areas across the globe. The anthrax might manifest as cutaneous, inhalational, or gastrointestinal type.
Inhalation anthrax is contracted by the inhalation of aerosolized spores. Initial manifestations resemble those of influenza and encompass a fever, chills, weakness, a cough, and chest discomfort. The illness typically manifests in two phases, during which there is a phase of recuperation following the first indications and symptoms. The second stage progresses suddenly with swift decline characterized by a fever, difficulty breathing, shortness of breath, and decrease in blood pressure, often resulting in death within 24 hours. The radiological examination reveals mediastinitis and symmetric mediastinal widening.
Thoracic aortic aneurysm
An aortic aneurysm exerting pressure on the trachea can result in a dry cough accompanied by difficulty breathing, hoarseness, wheezing, and a pain in the shoulders, lower back, or belly below the sternum. Furthermore, the patient may have facial or neck edema, distention of the jugular vein, difficulty swallowing, conspicuous veins throughout the chest, stridor, and potentially, paresthesia or neuralgia.
Asthma
Attacks of asthma usually manifest during the nighttime, beginning with a cough that is not productive and accompanied by little wheezing. This gradually advances to intense difficulty breathing, audible wheezing, chest constriction, and a cough that generates viscous mucus.
Additional indicators include anxiety, rhonchi, extended exhalations, intercostal and supraclavicular retractions during inhalation, auxiliary muscular activity, flared nostrils, rapid breathing, increased heart rate, excessive sweating, and flushing or cyanosis.
Atelectasis
The deflation of lung tissue has the effect of activating cough receptors, therefore inducing a nonproductive cough. Furthermore, the patient may experience pleuritic chest pain, anxiety, dyspnea, tachypnea, and increase in heart rate. The patient may have cyanotic and diaphoretic skin, reduced breath sounds, a dull chest upon percussion, inspiratory delay, substernal or intercostal retractions, reduced vocal fremitus, and distortion of the trachea towards the affected side.
Avian flu
The avian flu, or bird flu (H5N1), is a virus exclusively present in ill birds and poultry, and typically does not cause infection in humans. Indeed, the initial documented instances of human infection with H5N1 (the most highly pathogenic variant) took place globally in 1996. A nonproductive cough is a defining feature of an infection caused by the avian flu virus, similar to its manifestation with typical human influenza viruses. Presenting symptoms include fever, sore throat, rhinorrhea, headache, myalgia, and conjunctivitis; viral pneumonia and acute respiratory distress are severe and potentially fatal consequences that may arise.
Blast lung injury
Those afflicted with a blast lung injury may have an abrupt emergence of a severe, unproductive cough. Blast lung injury refers to the deliberate release and direction of an explosive device against a victim, usually occurring in times of war or, more recently, in worldwide terrorism incidents. The involvement of metalic fragments or aerosol chemical irritants in an explosive device depends on its composition. The patient may present with chest pain, a sensation of burning in the chest or throat, respiration and speech difficulties, shortness of breath, headache, and fainting. Further observations encompass cutaneous tears and contusions, edema, pulmonary bleeding, tachypnea, hypoxia, wheezing, apnea, cyanosis, reduced breath sounds, and hemodynamic instability. Diagnostic procedures for this condition include a chest X-ray which shows a distinctive "butterfly" pattern.
Chronic bronchitis.
Bronchitis first presents with a nonproductive, hacking cough that will eventually progress to a productive cough. Additional symptoms observed include extended expiration, wheezing, difficulty breathing, use of auxiliary muscles, barrel chest, cyanosis, rapid breathing, crackles, and sporadic rhonchi. Clubbing may manifest throughout advanced-stages.
Bronchogenic carcinoma
Initial symptoms of bronchogenic carcinoma may include a persistent, unproductive cough, difficulty breathing, and indistinct angina. Furthermore, the patient may have wheezing.
Common cold
The typical course of the common cold begins with a nonproductive, hacking cough and advances to a combination of symptoms including sneezing, headaches, malaise, fatigue, rhinorrhea, myalgia, arthralgia, nasal congestion, and a rough throat.
Esophageal achalasia
An esophageal achalasia is characterised by a dry cough upon regurgitation and aspiration. Moreover, the patient may experience recurring pulmonary infections and dysphagia.
Esophageal diverticula
The patient suffering from esophageal diverticula presents with a nighttime cough that is not productive, regurgitation and aspiration, dyspepsia, and dysphagia. His cervical region may exhibit edema and produce a gurgling sound. The patient may also present with halitosis and weight loss.
Esophageal occlusion
Indications of esophageal occlusion include acute nonproductive coughing and gagging, accompanied by a feeling of obstruction in the throat. Additional symptoms include dysphagia, neck or chest pain, and the inability to swallow.
Chronic gastroesophageal reflux disease (GER)
A nonproductive cough linked to gastroesophageal reflux disease can be attributed to inflammation of the larynx. Peptic reflux is the retrograde movement of food or liquid from the stomach to the esophagus and subsequent leakage into the hypopharynx. Additional symptoms encompass chest pain characterized by a burning sensation (heartburn), throat soreness, hoarseness, belching, dysphagia, and occasionally wheezing.
Hantavirus pulmonary syndrome.
Patients diagnosed with Hantavirus pulmonary syndrome often experience a nonproductive cough, characterized by noncardiogenic pulmonary edema. Additional symptoms include headache, muscle soreness, elevated body temperature, nausea, and vomiting.
Hypersensitivity pneumonitis.
In hypersensitivity pneumonitis, an acute nonproductive cough, fever, shortness of breath, and general malaise typically manifest 5 to 6 hours following exposure to an antigen.
Interstitial lung disease
An interstitial lung disease patient presents with a nonproductive cough and a gradual increase in difficulty breathing. Besides, he may exhibit cyanosis, clubbing, fine crackles, weariness, fluctuating chest discomfort, and weight loss.
Laryngeal tumor
In addition to slight throat discomfort and hoarseness, a mild, nonproductive cough is an early indication of a laryngeal pathology. In due course, dysphagia, dyspnea, cervical lymphadenopathy, stridor, and an earache may manifest.
Laryngitis
The acute manifestation of laryngitis is characterized by a nonproductive cough accompanied by localised pain, particularly on swallowing or speaking, together with fever and malaise. The severity of his hoarseness can vary from slight to total.
loss of voice.
Pulmonary abscess. An initial symptom of lung abscess is often a nonproductive cough, accompanied by weakness, difficulty breathing, and pleuritic chest pain. Furthermore, the patient may present with diaphoresis, pyrexia, cephalalgia, lethargy, exhaustion, crackles, reduced respiratory sounds, anorexia, and weight loss. Later on, his cough generates copious quantities of purulent, malodorous, and potentially hematochezic sputum.
Pleural effusion
Characteristic of pleural effusion are a nonproductive cough, dyspnea, pleuritic chest pain, and reduced chest mobility. Additional observations include a pleural friction rub, increased heart rate, rapid breathing, excessive vocalization, lack of distinct noises when tapped, reduced or missing breath sounds, and reduced tactile sensitivity.
Pneumonia
The onset of bacterial pneumonia often involves an initially nonproductive, hacking, and unpleasant cough that quickly progresses to become productive. Additional symptoms noted include tremors, cephalalgia, pyrexia, dyspnea, chest pain in the pleuritic region, rapid breathing, increased heart rate, labored breathing, nasal flaring, reduced breath sounds, little crackles, rhonchi, and discoloration of the skin. On percussion, the patient's chest may exhibit dullness.
In mycoplasma pneumonia, a nonproductive cough typically develops 2 to 3 days after the initial symptoms of malaise, including a headache and a sore throat. This cough may be paroxysmal, resulting in substernal chest discomfort. Frequently, fever manifests, although, the patient does not exhibit signs of severe illness.
Viral pneumonia is characterized by a nonproductive, hacking cough and the progressive development of lethargy, headache, anorexia, and a low-grade fever.
Pneumothorax
A life-threatening condition, pneumothorax is characterized by a dry cough and symptoms of respiratory distress, including intense shortness of breath, rapid heart rate, rapid breathing, and redness of the skin. The patient presents with abrupt, acute chest pain that exacerbates with chest expansion, along with subcutaneous crepitation, hyperresonance or tympany, reduced vocal fremitus, and diminished or missing breath sounds on the afflicted side.
Pulmonary edema. Pulmonary edema first presents with a dry cough that advances to a frothy or blood-tinged sputum, difficulty breathing during physical activity, repeated episodes of shortness of breath during the night, difficulty breathing, increased heart rate, rapid breathing, crackles in the chest, and a sensation of pressure in the ventricles. Severe pulmonary edema is characterised by increased respiratory rate and effort, coupled with coarse diffuse crackles and coughing that generates frothy, bloody sputum.
Pulmonary embolism
An acute pulmonary embolism can rapidly cause a dry cough accompanied by shortness of breath and chest discomfort that is either pleuritic or anginal. However, the cough usually generates phlegm with a blood-tinged appearance. In addition to tachycardia and a low-grade fever, less frequent indications and symptoms include excessive coughing up of blood, splinting of the chest, swelling of the legs, and, in cases of a significant embolism, cyanosis, fainting, and distension of the jugular vein. In addition, the patient may exhibit a pleural friction rub, widespread wheezing, dullness upon percussion, and reduced breath sounds.
Sarcoidosis
Sarcoidosis is characterised by a nonproductive cough, with accompanying symptoms of dyspnea, substernal discomfort, and malaise. Furthermore, the patient may experience fatigue, arthralgia, myalgia, weight loss, tachypnea, crackles, lymphadenopathy, hepatosplenomegaly, skin lesions, vision impairment, dysphagia, and arrhythmias.
Severe acute respiratory syndrome (SARS)
The cause of SARS, an acute viral disease, is currently unknown; nonetheless, a new Coronavirus has been suggested as a potential explanation. While the majority of cases have been documented in Asia, namely in China, Vietnam, Singapore, and Thailand, others have emerged in Europe and North America. The incubation period ranges from 2 to 7 days, beginning with a temperature often exceeding 100.4°F [38°C]. Additional symptoms seen are headache, lethargy, dry, nonproductive cough, and dyspnea. The disease exhibits significant variability in its severity, encompassing mild sickness, pneumonia, and, in certain instances, advancing to respiratory failure and mortality.
Tracheobronchitis (acute)
Initially, tracheobronchitis causes a nonproductive cough that subsequently becomes productive as the amount of secretions increases. Common symptoms that often occur before the cough begins include chills, a sore throat, a mild fever, muscle and back pain, and substernal tightness. Commonly heard are rhonchi and wheezes. Severe sickness results in a raised body temperature ranging from 101°F to 102°F (38.3°C to 38.9°C) and maybe bronchospasm, characterized by intense wheezing and heightened coughing.
Tularemia
Tularemia, typically referred to as rabbit fever, is the result of infection by the gram-negative, non-spore-forming bacterium Francisella tularensis. Usually a rural ailment, it is prevalent in wild animals, water, and damp soil. Transmission of the disease to humans occurs via the bite of a diseased bug or tick, direct contact with infected animal corpses, consumption of contaminated water, or inhalation of the germs. It is identified as a potential airborne agent for use in biological warfare. Following inhalation of the organism, signs and symptoms include sudden onset of fever, chills, headache, widespread muscle soreness, nonproductive cough, shortness of breath, chest discomfort with pleuria, and swelling of the chest.
Additional contributing factors
Medical diagnostic testing. Clinical evaluations of pulmonary function (PFTs) and bronchoscopy may activatemay activate cough receptors and elicit coughing.
Therapies. Pruritus of the carina during suctioning or the insertion of deep endotracheal or tracheal tubes might induce a paroxysmal or hacking cough. Coughing that is not productive can also be caused by intermittent positive-pressure breathing or spirometry. Several inhalants, including pentamidine, can induce coughing.
Guidelines for Pediatric Populations
Evaluation of a nonproductive cough in newborns and young children can be challenging due to its inability to be deliberately caused and the need for careful observation.
Aspiration of a foreign body, particularly in children aged 6 months to 4 years, may be indicated by a quick beginning of paroxysmal nonproductive coughing. Nonproductive coughing can also arise from many syndromes that impact neonates and young children. Within the context of asthma, a distinctive nonproductive "tight" cough might manifest abruptly or gradually at the onset of an attack. In most cases, the cough becomes productive towards the latter stages of the disease. In cases of bacterial pneumonia, a nonproductive, hacking cough develops (
Rapidly and effectively gets productive throughout a span of 2 to 3 days. The onset of acute bronchiolitis is most common at the age of 6, characterized by intermittent bouts of nonproductive coughing that increase in frequency as the condition advances. Acute otitis media, a prevalent condition in newborns and young children because to their constricted eustachian tubes, also results in unproductive coughing.
Generally, a kid afflicted with measles experiences a mild, unproductive, hacking cough that worsens with time. Cystic fibrosis may initially manifest as a nonproductive, paroxysmal cough caused by retained secretions. Life-threatening pertussis causes a cough that transitions to paroxysmal, characterized by an inspiratory "whoop" or crowing sound upon inspiration. Allergic airway hyperactivity leads to a persistent nonproductive cough that worsens with physical activity or contact with cold air. Psychogenic coughing can manifest in children experiencing stress, strong emotional stimulation, or a desire for attention.
Guidelines for Geriatrics
Elderly people should always be questioned about nonproductive coughing since it could suggest a severe acute or chronic disease.
An unproductive cough is a loud and vigorous expulsion of air from the lungs that is devoid of moisture, does not stimulate the production of mucus, and may produce a little quantity of sputum. Among individuals with respiratory problems, it is one of the most often reported concerns.
The act of coughing serves as a defensive strategy to empty the airway spaces. Nevertheless, a nonproductive cough is ineffectual and can result in harm, such as the collapse of the airway or the rupture of alveoli or protuberances. An initially nonproductive cough that subsequently turns productive is a characteristic indication of a developing respiratory illness, such as pneumonia.
The cough reflex often arises from the activation of cough receptors by mechanical, chemical, thermal, inflammatory, or psychogenic stimuli. Refer to Nevertheless, external pressure, such as, Viral inflammation of the subdiaphragm or a mediastinal tumor can also trigger it, along with voluntary exhalation of air, which sometimes happens as a neurological habit. Nonproductive cough may also be caused by specific medications, such as angiotensin-converting enzyme inhibitors.
A nonproductive cough might manifest as paroxysms and may then exacerbate by increasing in frequency. A quick onset acute cough may go away on its own; a cough lasting more than one month is classified as chronic and often arises from cigarette smoking.
An individual with a persistent nonproductive cough may minimize or disregard it, instead accepting it as a typical symptom. Indeed, he typically will not seek medical intervention unless he presents with additional symptoms. Cystoid cough may occur when a foreign object enters the external auditory canal of a youngster. Thoroughly inspect the child's ears.
Ask the patient about recent illness (especially a cardiovascular or pulmonary disorder), surgery, or trauma. Also, ask about hypersensitivity to drugs, foods, pets, dust, or pollen. Find out which medications the patient takes, if any, and ask about recent changes in schedule or dosages. Also, ask about recent changes in his appetite, weight, exercise tolerance, or energy level and recent exposure to irritating fumes, chemicals, or smoke.
As you’re taking his history, observe the patient’s general appearance and manner: Is he agitated, restless, or lethargic; pale, diaphoretic, or flushed; anxious, confused, or nervous? Also, note whether he’s cyanotic or has clubbed fingers or peripheral edema.
Given the apprehension of being identified as someone afflicted with tuberculosis (TB), the patient may hesitate to provide details on his indications and manifestations, such as a cough. Request information from the patient who is at risk for tuberculosis (TB) - whether they were born in a different country, had contact with acute TB, or engaged in high-risk activities - on possible exposure to TB.
Proceed to do a physical examination. Begin by assessing the patient's vital signs. Assess the depth and cadence of his respirations, and make a record of any wheezing or "crowing" sounds. Feel the patient's dermal surface: Is it rather cold?
Is it warm, clammy, or dry? Assess his nasal and oral cavities for congestion, irritation, discharge, or indications of infection. Examine his neck for dilated jugular veins and deviation of the trachea, and examine for any firm lumps or swollen lymph nodes by palpation.
Inspect his chest, carefully analyzing its structure and searching for any atypical movement of the chest wall. Do any retractions or use of auxiliary muscles come to your attention? Detect dullness, tympany, or flatness via percussion. Conduct auscultation to detect wheezing, crackles, rhonchi, pleural friction rubs, and reduced or missing breath sounds. Lastly, visually inspect his belly for any signs of distension, pain, lumps, or abnormal bowel noises.
A Critical Analysis of the Cough Mechanism The anatomical distribution of cough receptors is believed to include the nose, sinuses, auditory canals, nasopharynx, larynx, trachea, bronchi, pleurae, diaphragm, and potentially the pericardium and gastrointestinal system. Upon stimulation of a cough receptor, the vagus and glossopharyngeal nerves convey the impulse to the "cough center" located in the medulla. Subsequently, the impulse is conveyed to the larynx as well as to the intercostal and abdominal muscles. Profound inspiration is
then the glottis closes, the diaphragm relaxes, and the abdominal and intercostal muscles contract. The subsequent elevation in lung pressure causes the glottis to open, allowing for the expulsion of a powerful and loud exhalation referred to as a cough.
Medical Causes
Airway occlusion
Upper airway partial blockage results in an abrupt onset of dry, paroxysmal coughing. The patient is experiencing dyspnea, wheezing, and hoarseness, accompanied by stridor, rapid heart rate, and reduced breath sounds.
Anthrax (inhalation)
The acute infectious disease known as anthrax is attributed to the gram-positive, spore-forming bacterium Bacillus anthracis. While the disease mostly affects wild and domestic grazing animals, such as cattle, sheep, and goats, the spores can persist in the soil for an extended period through many years. The disease can manifest in humans who are exposed to infectious animals, diseased animal tissue, or as a result of biological warfare. Primarily, natural cases manifest in agricultural areas across the globe. The anthrax might manifest as cutaneous, inhalational, or gastrointestinal type.
Inhalation anthrax is contracted by the inhalation of aerosolized spores. Initial manifestations resemble those of influenza and encompass a fever, chills, weakness, a cough, and chest discomfort. The illness typically manifests in two phases, during which there is a phase of recuperation following the first indications and symptoms. The second stage progresses suddenly with swift decline characterized by a fever, difficulty breathing, shortness of breath, and decrease in blood pressure, often resulting in death within 24 hours. The radiological examination reveals mediastinitis and symmetric mediastinal widening.
Thoracic aortic aneurysm
An aortic aneurysm exerting pressure on the trachea can result in a dry cough accompanied by difficulty breathing, hoarseness, wheezing, and a pain in the shoulders, lower back, or belly below the sternum. Furthermore, the patient may have facial or neck edema, distention of the jugular vein, difficulty swallowing, conspicuous veins throughout the chest, stridor, and potentially, paresthesia or neuralgia.
Asthma
Attacks of asthma usually manifest during the nighttime, beginning with a cough that is not productive and accompanied by little wheezing. This gradually advances to intense difficulty breathing, audible wheezing, chest constriction, and a cough that generates viscous mucus.
Additional indicators include anxiety, rhonchi, extended exhalations, intercostal and supraclavicular retractions during inhalation, auxiliary muscular activity, flared nostrils, rapid breathing, increased heart rate, excessive sweating, and flushing or cyanosis.
Atelectasis
The deflation of lung tissue has the effect of activating cough receptors, therefore inducing a nonproductive cough. Furthermore, the patient may experience pleuritic chest pain, anxiety, dyspnea, tachypnea, and increase in heart rate. The patient may have cyanotic and diaphoretic skin, reduced breath sounds, a dull chest upon percussion, inspiratory delay, substernal or intercostal retractions, reduced vocal fremitus, and distortion of the trachea towards the affected side.
Avian flu
The avian flu, or bird flu (H5N1), is a virus exclusively present in ill birds and poultry, and typically does not cause infection in humans. Indeed, the initial documented instances of human infection with H5N1 (the most highly pathogenic variant) took place globally in 1996. A nonproductive cough is a defining feature of an infection caused by the avian flu virus, similar to its manifestation with typical human influenza viruses. Presenting symptoms include fever, sore throat, rhinorrhea, headache, myalgia, and conjunctivitis; viral pneumonia and acute respiratory distress are severe and potentially fatal consequences that may arise.
Blast lung injury
Those afflicted with a blast lung injury may have an abrupt emergence of a severe, unproductive cough. Blast lung injury refers to the deliberate release and direction of an explosive device against a victim, usually occurring in times of war or, more recently, in worldwide terrorism incidents. The involvement of metalic fragments or aerosol chemical irritants in an explosive device depends on its composition. The patient may present with chest pain, a sensation of burning in the chest or throat, respiration and speech difficulties, shortness of breath, headache, and fainting. Further observations encompass cutaneous tears and contusions, edema, pulmonary bleeding, tachypnea, hypoxia, wheezing, apnea, cyanosis, reduced breath sounds, and hemodynamic instability. Diagnostic procedures for this condition include a chest X-ray which shows a distinctive "butterfly" pattern.
Chronic bronchitis.
Bronchitis first presents with a nonproductive, hacking cough that will eventually progress to a productive cough. Additional symptoms observed include extended expiration, wheezing, difficulty breathing, use of auxiliary muscles, barrel chest, cyanosis, rapid breathing, crackles, and sporadic rhonchi. Clubbing may manifest throughout advanced-stages.
Bronchogenic carcinoma
Initial symptoms of bronchogenic carcinoma may include a persistent, unproductive cough, difficulty breathing, and indistinct angina. Furthermore, the patient may have wheezing.
Common cold
The typical course of the common cold begins with a nonproductive, hacking cough and advances to a combination of symptoms including sneezing, headaches, malaise, fatigue, rhinorrhea, myalgia, arthralgia, nasal congestion, and a rough throat.
Esophageal achalasia
An esophageal achalasia is characterised by a dry cough upon regurgitation and aspiration. Moreover, the patient may experience recurring pulmonary infections and dysphagia.
Esophageal diverticula
The patient suffering from esophageal diverticula presents with a nighttime cough that is not productive, regurgitation and aspiration, dyspepsia, and dysphagia. His cervical region may exhibit edema and produce a gurgling sound. The patient may also present with halitosis and weight loss.
Esophageal occlusion
Indications of esophageal occlusion include acute nonproductive coughing and gagging, accompanied by a feeling of obstruction in the throat. Additional symptoms include dysphagia, neck or chest pain, and the inability to swallow.
Chronic gastroesophageal reflux disease (GER)
A nonproductive cough linked to gastroesophageal reflux disease can be attributed to inflammation of the larynx. Peptic reflux is the retrograde movement of food or liquid from the stomach to the esophagus and subsequent leakage into the hypopharynx. Additional symptoms encompass chest pain characterized by a burning sensation (heartburn), throat soreness, hoarseness, belching, dysphagia, and occasionally wheezing.
Hantavirus pulmonary syndrome.
Patients diagnosed with Hantavirus pulmonary syndrome often experience a nonproductive cough, characterized by noncardiogenic pulmonary edema. Additional symptoms include headache, muscle soreness, elevated body temperature, nausea, and vomiting.
Hypersensitivity pneumonitis.
In hypersensitivity pneumonitis, an acute nonproductive cough, fever, shortness of breath, and general malaise typically manifest 5 to 6 hours following exposure to an antigen.
Interstitial lung disease
An interstitial lung disease patient presents with a nonproductive cough and a gradual increase in difficulty breathing. Besides, he may exhibit cyanosis, clubbing, fine crackles, weariness, fluctuating chest discomfort, and weight loss.
Laryngeal tumor
In addition to slight throat discomfort and hoarseness, a mild, nonproductive cough is an early indication of a laryngeal pathology. In due course, dysphagia, dyspnea, cervical lymphadenopathy, stridor, and an earache may manifest.
Laryngitis
The acute manifestation of laryngitis is characterized by a nonproductive cough accompanied by localised pain, particularly on swallowing or speaking, together with fever and malaise. The severity of his hoarseness can vary from slight to total.
loss of voice.
Pulmonary abscess. An initial symptom of lung abscess is often a nonproductive cough, accompanied by weakness, difficulty breathing, and pleuritic chest pain. Furthermore, the patient may present with diaphoresis, pyrexia, cephalalgia, lethargy, exhaustion, crackles, reduced respiratory sounds, anorexia, and weight loss. Later on, his cough generates copious quantities of purulent, malodorous, and potentially hematochezic sputum.
Pleural effusion
Characteristic of pleural effusion are a nonproductive cough, dyspnea, pleuritic chest pain, and reduced chest mobility. Additional observations include a pleural friction rub, increased heart rate, rapid breathing, excessive vocalization, lack of distinct noises when tapped, reduced or missing breath sounds, and reduced tactile sensitivity.
Pneumonia
The onset of bacterial pneumonia often involves an initially nonproductive, hacking, and unpleasant cough that quickly progresses to become productive. Additional symptoms noted include tremors, cephalalgia, pyrexia, dyspnea, chest pain in the pleuritic region, rapid breathing, increased heart rate, labored breathing, nasal flaring, reduced breath sounds, little crackles, rhonchi, and discoloration of the skin. On percussion, the patient's chest may exhibit dullness.
In mycoplasma pneumonia, a nonproductive cough typically develops 2 to 3 days after the initial symptoms of malaise, including a headache and a sore throat. This cough may be paroxysmal, resulting in substernal chest discomfort. Frequently, fever manifests, although, the patient does not exhibit signs of severe illness.
Viral pneumonia is characterized by a nonproductive, hacking cough and the progressive development of lethargy, headache, anorexia, and a low-grade fever.
Pneumothorax
A life-threatening condition, pneumothorax is characterized by a dry cough and symptoms of respiratory distress, including intense shortness of breath, rapid heart rate, rapid breathing, and redness of the skin. The patient presents with abrupt, acute chest pain that exacerbates with chest expansion, along with subcutaneous crepitation, hyperresonance or tympany, reduced vocal fremitus, and diminished or missing breath sounds on the afflicted side.
Pulmonary edema. Pulmonary edema first presents with a dry cough that advances to a frothy or blood-tinged sputum, difficulty breathing during physical activity, repeated episodes of shortness of breath during the night, difficulty breathing, increased heart rate, rapid breathing, crackles in the chest, and a sensation of pressure in the ventricles. Severe pulmonary edema is characterised by increased respiratory rate and effort, coupled with coarse diffuse crackles and coughing that generates frothy, bloody sputum.
Pulmonary embolism
An acute pulmonary embolism can rapidly cause a dry cough accompanied by shortness of breath and chest discomfort that is either pleuritic or anginal. However, the cough usually generates phlegm with a blood-tinged appearance. In addition to tachycardia and a low-grade fever, less frequent indications and symptoms include excessive coughing up of blood, splinting of the chest, swelling of the legs, and, in cases of a significant embolism, cyanosis, fainting, and distension of the jugular vein. In addition, the patient may exhibit a pleural friction rub, widespread wheezing, dullness upon percussion, and reduced breath sounds.
Sarcoidosis
Sarcoidosis is characterised by a nonproductive cough, with accompanying symptoms of dyspnea, substernal discomfort, and malaise. Furthermore, the patient may experience fatigue, arthralgia, myalgia, weight loss, tachypnea, crackles, lymphadenopathy, hepatosplenomegaly, skin lesions, vision impairment, dysphagia, and arrhythmias.
Severe acute respiratory syndrome (SARS)
The cause of SARS, an acute viral disease, is currently unknown; nonetheless, a new Coronavirus has been suggested as a potential explanation. While the majority of cases have been documented in Asia, namely in China, Vietnam, Singapore, and Thailand, others have emerged in Europe and North America. The incubation period ranges from 2 to 7 days, beginning with a temperature often exceeding 100.4°F [38°C]. Additional symptoms seen are headache, lethargy, dry, nonproductive cough, and dyspnea. The disease exhibits significant variability in its severity, encompassing mild sickness, pneumonia, and, in certain instances, advancing to respiratory failure and mortality.
Tracheobronchitis (acute)
Initially, tracheobronchitis causes a nonproductive cough that subsequently becomes productive as the amount of secretions increases. Common symptoms that often occur before the cough begins include chills, a sore throat, a mild fever, muscle and back pain, and substernal tightness. Commonly heard are rhonchi and wheezes. Severe sickness results in a raised body temperature ranging from 101°F to 102°F (38.3°C to 38.9°C) and maybe bronchospasm, characterized by intense wheezing and heightened coughing.
Tularemia
Tularemia, typically referred to as rabbit fever, is the result of infection by the gram-negative, non-spore-forming bacterium Francisella tularensis. Usually a rural ailment, it is prevalent in wild animals, water, and damp soil. Transmission of the disease to humans occurs via the bite of a diseased bug or tick, direct contact with infected animal corpses, consumption of contaminated water, or inhalation of the germs. It is identified as a potential airborne agent for use in biological warfare. Following inhalation of the organism, signs and symptoms include sudden onset of fever, chills, headache, widespread muscle soreness, nonproductive cough, shortness of breath, chest discomfort with pleuria, and swelling of the chest.
Additional contributing factors
Medical diagnostic testing. Clinical evaluations of pulmonary function (PFTs) and bronchoscopy may activatemay activate cough receptors and elicit coughing.
Therapies. Pruritus of the carina during suctioning or the insertion of deep endotracheal or tracheal tubes might induce a paroxysmal or hacking cough. Coughing that is not productive can also be caused by intermittent positive-pressure breathing or spirometry. Several inhalants, including pentamidine, can induce coughing.
Guidelines for Pediatric Populations
Evaluation of a nonproductive cough in newborns and young children can be challenging due to its inability to be deliberately caused and the need for careful observation.
Aspiration of a foreign body, particularly in children aged 6 months to 4 years, may be indicated by a quick beginning of paroxysmal nonproductive coughing. Nonproductive coughing can also arise from many syndromes that impact neonates and young children. Within the context of asthma, a distinctive nonproductive "tight" cough might manifest abruptly or gradually at the onset of an attack. In most cases, the cough becomes productive towards the latter stages of the disease. In cases of bacterial pneumonia, a nonproductive, hacking cough develops (
Rapidly and effectively gets productive throughout a span of 2 to 3 days. The onset of acute bronchiolitis is most common at the age of 6, characterized by intermittent bouts of nonproductive coughing that increase in frequency as the condition advances. Acute otitis media, a prevalent condition in newborns and young children because to their constricted eustachian tubes, also results in unproductive coughing.
Generally, a kid afflicted with measles experiences a mild, unproductive, hacking cough that worsens with time. Cystic fibrosis may initially manifest as a nonproductive, paroxysmal cough caused by retained secretions. Life-threatening pertussis causes a cough that transitions to paroxysmal, characterized by an inspiratory "whoop" or crowing sound upon inspiration. Allergic airway hyperactivity leads to a persistent nonproductive cough that worsens with physical activity or contact with cold air. Psychogenic coughing can manifest in children experiencing stress, strong emotional stimulation, or a desire for attention.
Guidelines for Geriatrics
Elderly people should always be questioned about nonproductive coughing since it could suggest a severe acute or chronic disease.
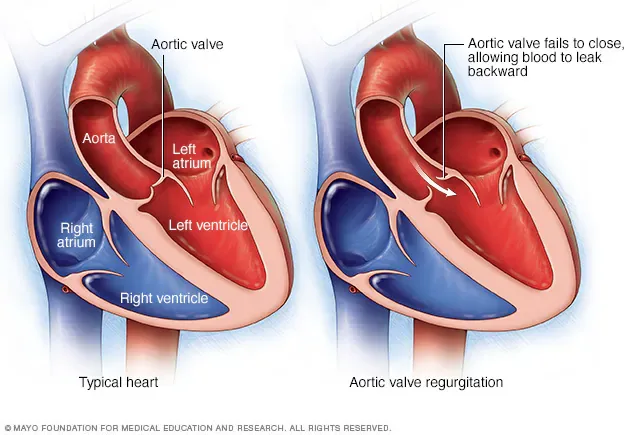
- Published on
Symptoms and Signs – Differential Diagnosis Crackles [Rales, crepitations]
Crackles are nonmusical clicking or rattling sounds that are encountered during the auscultation of breath sounds in individuals with specific cardiovascular and pulmonary diseases. Typically, they manifest during the act of inhalation and periodically repeat between consecutive respiratory cycles. These can manifest unilaterally or bilaterally, and may be moist or dry. Pitch, volume, location, persistence, and recurrence during the respiratory cycle are the defining characteristics of these sounds.
Crackles are indicative of atypical airflow in airways loaded with fluid. Their distribution might be sporadic, as in pneumonia, or confined, as in bronchiectasis. The normal lungs may have a few basilar crackles after Extended periods of shallow respiration. Typically, these crackles resolve with a few deep inhalations. Typically, crackles serve as an indicator of the severity of an underlying disease. Typically, crackles arising from a widespread problem manifest in the less enlarged and more reliant regions of the lungs, such as the lung bases, when the patient is in an upright position. Passage of air through inflammatory exudate may not produce audible crackles if the affected section of the lung is not being ventilated due to shallow respirations.
Formation Mechanisms of Crackles
Crackles arise as air flows through airways filled with fluid, resulting in the collapse of alveoli as the pressure in the airways equalizes. Furthermore, they can arise from inflammation of the membranes that line the chest cavity and the lungs. The following drawings depict a typical alveolus and two abnormal alveolar pathologies that result in crackles.
EMERGENCY INTERVENTIONS
Quickly measure the patient's vital signs and assess him for indications of respiratory distress or blockage of the airways. Verify the measure of the depth and frequency of respirations. Has he developed dyspnea? Inspect for heightened utilization of auxiliary muscles and palpable chest wall movement, retractions, stridor, or nasal flaring. Conduct an evaluation of the patient to identify any further indications and manifestations of fluid overload, such as jugular vein distension and edema. Administer more oxygen and, if required, a diuretic pharmaceutical. Percutaneous endotracheal intubation may also be required.
Historical Background and Physical Assessment
If the patient presents with a cough, inquire about its onset and whether it is persistent or occurring sporadically. Determine the aural characteristics of the cough and ascertain whether he is aspirating sputum or blood. To assess the productive cough, ascertain the consistency, quantity, odor, and color of the sputum.
Query the patient about the presence of any pain. If that is the case, where is it situated? When did he initially become aware of it? Does it emit forth radiation to other regions? The patient should also be asked if movement, coughing, or breathing exacerbates or alleviates his pain. Observe the patient's posture: Does he lie motionless or is he exhibiting restless movement?
Collect a concise medical history. Is the patient diagnosed with cancer or has a documented respiratory or cardiovascular system condition? Inquire about either recent surgical procedures, traumas, or illnesses. Does he engage in smoking or imbibe alcohol? Is he suffering from hoarseness or dysphagia? Learn the specific drugs he is now prescribed. In addition, inquire about any recent episodes of weight loss, anorexia, nausea, vomiting, exhaustion, weakness, vertigo, and syncope. Does the patient have any history of exposure to irritants, such as vapors, fumes, or smoke?
Proceed to do a physical examination. Inspect the patient's nasal and oral cavities.
Monitor for indications of infection, such as inflammation or heightened secretions. Observe his breath smell; hyperhalitosis may suggest a lung infection. Examine his neck for any anatomical abnormalities such as tumors, discomfort, edema, lymphadenopathy, or venous retention.
Anatomically examine the patient's chest for any atypical shape or unequal enlargement. Assess for dullness, tympany, or flatness using percussion. Analyze his lungs for any other atypical, reduced, or nonexistent respiratory sounds. Auditory examination of his heart for atypical sounds, and examination of his hands and feet for swelling or swollen joints.
Medical etiology
ARDS (acute respiratory distress syndrome)
Alveolar respiratory distress syndrome (ARDS) is a potentially fatal condition characterized by the presence of widespread, fine to coarse crackles often detected in the affected areas of the lungs. In addition, it causes cyanosis, nasal nasal flaring, tachypnea, tachycardia, grunting respirations, rhonchi, dyspnea, anxiety, and reduced consciousness.
Bronchiectasis
In bronchiectasis, there are continuous, rough crackles audible over the afflicted region of the lung. These symptoms are accompanied by a persistent cough that generates substantial quantities of mucopurulent sputum. Additional features manifest as halitosis, intermittent wheezes, dyspnea during exertion, rhonchi, weight loss, weariness, malaise, weakness, a recurring fever, and late-stage clubbing.
Bronchitis (chronic)
Bristle cell bronchitis results in the production of coarse crackles typically detected at the lung bases. Elevated bronchial secretions lead to prolonged expirations, wheezing, rhonchi, exertional dyspnea, tachypnea, and a persistent, productive cough. As a late indication, clubbing and cyanosis may manifest.
Legionnaires’ disease
Legionnaires’ illness is characterised by the production of diffuse, wet crackles and a cough that generates pale, nonpurulent, and potentially blood-streaked sputum. Prodromal signs and symptoms often manifest as malaise, weariness, weakness, anorexia, widespread myalgia, and perhaps, diarrhea. Within 12 to 48 hours, the patient experiences a non-productive cough and an abrupt onset of elevated body temperature accompanied by chills. Additional symptoms he may have include pleuritic chest discomfort, headache, tachypnea, tachycardia, nausea, vomiting, dyspnea, moderate transient amnesia, confusion, flushing, minor diaphoresis, and prostration.
Pneumonia
Bacterial pneumonia is characterized by the presence of diffuse fine crackles, prompt start of shivering chills, elevated body temperature, tachypnea, and pleuritic chest discomfort.
Clinical manifestations include cyanosis, grunting respirations, nasal flaring, reduced breath sounds, myalgia, headache, tachycardia, dyspnea, diaphoresis, and rhonchi. The patient presents with a dry cough that subsequently progresses to include productive coughing. The clinical presentation of mycoplasma pneumonia includes the presence of medium to fine crackles, a nonproductive cough, malaise, a sore throat, a headache, and a fever. Possible presence of blood-flecked sputum in the patient. Viral pneumonia results in typically emerging, widespread crackles. In addition, the patient may have a nonproductive cough, malaise, a headache, anorexia, a low-grade temperature, and reduced breath sounds.
Pulmonary edema
Presence of moist, bubbling crackles on inspiration is an early indication of pulmonary edema, a potentially fatal condition. Additional initial symptoms include difficulty breathing during physical activity, repeated episodes of difficulty breathing throughout the night, followed by difficulty breathing during sleep, and coughing, which may first be unproductive but eventually produces foamy, bloody sputum. Associated clinical manifestations include rapid heart rate, rapid breathing, and the presence of a third heart sound (S3 gallop). The patient's respiratory rate and effortfulness escalate, leading to the development of diffuse crackles, worsening tachycardia, hypotension, a fast and thready pulse, cyanosis, and cold, clammy skin.
Pulmonary Embolism
A pulmonary embolism is a potentially fatal condition characterized by the presence of fine to coarse crackles and a cough that can be either dry or productive of blood-tinged sputum. Typically, the initial indication of pulmonary embolism is intense shortness of breath, frequently accompanied by angina or pleuritic chest discomfort. The patient presents with pronounced anxiety, a little fever, rapid heart rate, rapid breathing, and excessive sweating. Occasionally seen indications include excessive coughing up of blood, splinting of the chest, swelling of the legs, and, in cases of a significant embolism, cyanosis, fainting, and distension of the jugular vein. In addition, the patient may exhibit a pleural friction rub, widespread wheezing, chest dullness upon percussion, reduced breath sounds, and indications of circulatory collapse.
Chronic pulmonary tuberculosis (TB)
Fine crackles manifest after coughing in cases with pulmonary tuberculosis. The patient presents with a confluence of hemoptysis, lethargy, dyspnea, and pleuritic chest discomfort. The sputum might be either thin and mucoid or profuse and purulent. In general, the patient is prone to weariness and suffers from nocturnal perspiration, debility, and unintentional weight loss. The breath noises he produces are amphoric.
Tracheobronchitis. The acute manifestation of tracheobronchitis is characterized by the production of moist or coarse crackles, a productive cough, chills, a sore throat, a mild fever, muscle and back pain, and substernal tightness. Typically, the patient presents with rhonchi and wheezes. Tracheobronchitis of severe severity can result in a moderate
pyrexia with bronchoconstriction.
Special Considerations
To maintain the patient's unobstructed airway and aid his respiration, raise the head of his inpatient bed. Fluids, humidified air, or oxygen should be administered to liquefy thick secretions and alleviate inflammation of the mucosal membrane. Interstitial crackles caused by cardiogenic pulmonary edema may require the use of diuretics. Limitation of fluid intake may also be required. Rotate the patient every 1 to 2 hours and advise him to engage in slow, deep breathing.
Strategically schedule daily uninterrupted intervals of rest to facilitate the patient's relaxation and sleep. Prepare the patient for diagnostic examinations including chest radiography, a pulmonary computed tomography, and sputum analysis.
Therapeutic Counseling for Patients
Provide the patient with instruction on efficient coughing methods and the need of avoiding respiratory irritants. Underline the significance of smoking cessation and direct him to suitable resources to facilitate his cessation.
Key Pediatric Resources
Infants or youngsters exhibiting crackles may be indicative of a severe cardiovascular or respiratory condition. Children with pneumonias display diffuse, abrupt crackles. Both esophageal atresia and tracheoesophageal fistula can result in the production of bubbling, moist crackles when food or secretions are aspirated into the lungs, particularly in newborns. The presence of pulmonary edema results in the formation of fine crackles at the lung bases, while bronchiectasis leads to the production of moist crackles. Among babies, cystic fibrosis causes extensive, fine to coarse inspiratory crackles and wheezing. Chronic sickle cell anemia might result in crackles when it leads to pulmonary infarction or infection. An infection caused by respiratory syncytial virus in the lower respiratory tract usually results in the production of fine crackles and wheezes.
Guidelines for Geriatrics
Crackles that resolve with deep inhalation may suggest the presence of mild basilar atelectasis. Conduct auscultation on the lung bases of elderly individuals both before and after auscultating the apices.
Crackles are nonmusical clicking or rattling sounds that are encountered during the auscultation of breath sounds in individuals with specific cardiovascular and pulmonary diseases. Typically, they manifest during the act of inhalation and periodically repeat between consecutive respiratory cycles. These can manifest unilaterally or bilaterally, and may be moist or dry. Pitch, volume, location, persistence, and recurrence during the respiratory cycle are the defining characteristics of these sounds.
Crackles are indicative of atypical airflow in airways loaded with fluid. Their distribution might be sporadic, as in pneumonia, or confined, as in bronchiectasis. The normal lungs may have a few basilar crackles after Extended periods of shallow respiration. Typically, these crackles resolve with a few deep inhalations. Typically, crackles serve as an indicator of the severity of an underlying disease. Typically, crackles arising from a widespread problem manifest in the less enlarged and more reliant regions of the lungs, such as the lung bases, when the patient is in an upright position. Passage of air through inflammatory exudate may not produce audible crackles if the affected section of the lung is not being ventilated due to shallow respirations.
Formation Mechanisms of Crackles
Crackles arise as air flows through airways filled with fluid, resulting in the collapse of alveoli as the pressure in the airways equalizes. Furthermore, they can arise from inflammation of the membranes that line the chest cavity and the lungs. The following drawings depict a typical alveolus and two abnormal alveolar pathologies that result in crackles.
EMERGENCY INTERVENTIONS
Quickly measure the patient's vital signs and assess him for indications of respiratory distress or blockage of the airways. Verify the measure of the depth and frequency of respirations. Has he developed dyspnea? Inspect for heightened utilization of auxiliary muscles and palpable chest wall movement, retractions, stridor, or nasal flaring. Conduct an evaluation of the patient to identify any further indications and manifestations of fluid overload, such as jugular vein distension and edema. Administer more oxygen and, if required, a diuretic pharmaceutical. Percutaneous endotracheal intubation may also be required.
Historical Background and Physical Assessment
If the patient presents with a cough, inquire about its onset and whether it is persistent or occurring sporadically. Determine the aural characteristics of the cough and ascertain whether he is aspirating sputum or blood. To assess the productive cough, ascertain the consistency, quantity, odor, and color of the sputum.
Query the patient about the presence of any pain. If that is the case, where is it situated? When did he initially become aware of it? Does it emit forth radiation to other regions? The patient should also be asked if movement, coughing, or breathing exacerbates or alleviates his pain. Observe the patient's posture: Does he lie motionless or is he exhibiting restless movement?
Collect a concise medical history. Is the patient diagnosed with cancer or has a documented respiratory or cardiovascular system condition? Inquire about either recent surgical procedures, traumas, or illnesses. Does he engage in smoking or imbibe alcohol? Is he suffering from hoarseness or dysphagia? Learn the specific drugs he is now prescribed. In addition, inquire about any recent episodes of weight loss, anorexia, nausea, vomiting, exhaustion, weakness, vertigo, and syncope. Does the patient have any history of exposure to irritants, such as vapors, fumes, or smoke?
Proceed to do a physical examination. Inspect the patient's nasal and oral cavities.
Monitor for indications of infection, such as inflammation or heightened secretions. Observe his breath smell; hyperhalitosis may suggest a lung infection. Examine his neck for any anatomical abnormalities such as tumors, discomfort, edema, lymphadenopathy, or venous retention.
Anatomically examine the patient's chest for any atypical shape or unequal enlargement. Assess for dullness, tympany, or flatness using percussion. Analyze his lungs for any other atypical, reduced, or nonexistent respiratory sounds. Auditory examination of his heart for atypical sounds, and examination of his hands and feet for swelling or swollen joints.
Medical etiology
ARDS (acute respiratory distress syndrome)
Alveolar respiratory distress syndrome (ARDS) is a potentially fatal condition characterized by the presence of widespread, fine to coarse crackles often detected in the affected areas of the lungs. In addition, it causes cyanosis, nasal nasal flaring, tachypnea, tachycardia, grunting respirations, rhonchi, dyspnea, anxiety, and reduced consciousness.
Bronchiectasis
In bronchiectasis, there are continuous, rough crackles audible over the afflicted region of the lung. These symptoms are accompanied by a persistent cough that generates substantial quantities of mucopurulent sputum. Additional features manifest as halitosis, intermittent wheezes, dyspnea during exertion, rhonchi, weight loss, weariness, malaise, weakness, a recurring fever, and late-stage clubbing.
Bronchitis (chronic)
Bristle cell bronchitis results in the production of coarse crackles typically detected at the lung bases. Elevated bronchial secretions lead to prolonged expirations, wheezing, rhonchi, exertional dyspnea, tachypnea, and a persistent, productive cough. As a late indication, clubbing and cyanosis may manifest.
Legionnaires’ disease
Legionnaires’ illness is characterised by the production of diffuse, wet crackles and a cough that generates pale, nonpurulent, and potentially blood-streaked sputum. Prodromal signs and symptoms often manifest as malaise, weariness, weakness, anorexia, widespread myalgia, and perhaps, diarrhea. Within 12 to 48 hours, the patient experiences a non-productive cough and an abrupt onset of elevated body temperature accompanied by chills. Additional symptoms he may have include pleuritic chest discomfort, headache, tachypnea, tachycardia, nausea, vomiting, dyspnea, moderate transient amnesia, confusion, flushing, minor diaphoresis, and prostration.
Pneumonia
Bacterial pneumonia is characterized by the presence of diffuse fine crackles, prompt start of shivering chills, elevated body temperature, tachypnea, and pleuritic chest discomfort.
Clinical manifestations include cyanosis, grunting respirations, nasal flaring, reduced breath sounds, myalgia, headache, tachycardia, dyspnea, diaphoresis, and rhonchi. The patient presents with a dry cough that subsequently progresses to include productive coughing. The clinical presentation of mycoplasma pneumonia includes the presence of medium to fine crackles, a nonproductive cough, malaise, a sore throat, a headache, and a fever. Possible presence of blood-flecked sputum in the patient. Viral pneumonia results in typically emerging, widespread crackles. In addition, the patient may have a nonproductive cough, malaise, a headache, anorexia, a low-grade temperature, and reduced breath sounds.
Pulmonary edema
Presence of moist, bubbling crackles on inspiration is an early indication of pulmonary edema, a potentially fatal condition. Additional initial symptoms include difficulty breathing during physical activity, repeated episodes of difficulty breathing throughout the night, followed by difficulty breathing during sleep, and coughing, which may first be unproductive but eventually produces foamy, bloody sputum. Associated clinical manifestations include rapid heart rate, rapid breathing, and the presence of a third heart sound (S3 gallop). The patient's respiratory rate and effortfulness escalate, leading to the development of diffuse crackles, worsening tachycardia, hypotension, a fast and thready pulse, cyanosis, and cold, clammy skin.
Pulmonary Embolism
A pulmonary embolism is a potentially fatal condition characterized by the presence of fine to coarse crackles and a cough that can be either dry or productive of blood-tinged sputum. Typically, the initial indication of pulmonary embolism is intense shortness of breath, frequently accompanied by angina or pleuritic chest discomfort. The patient presents with pronounced anxiety, a little fever, rapid heart rate, rapid breathing, and excessive sweating. Occasionally seen indications include excessive coughing up of blood, splinting of the chest, swelling of the legs, and, in cases of a significant embolism, cyanosis, fainting, and distension of the jugular vein. In addition, the patient may exhibit a pleural friction rub, widespread wheezing, chest dullness upon percussion, reduced breath sounds, and indications of circulatory collapse.
Chronic pulmonary tuberculosis (TB)
Fine crackles manifest after coughing in cases with pulmonary tuberculosis. The patient presents with a confluence of hemoptysis, lethargy, dyspnea, and pleuritic chest discomfort. The sputum might be either thin and mucoid or profuse and purulent. In general, the patient is prone to weariness and suffers from nocturnal perspiration, debility, and unintentional weight loss. The breath noises he produces are amphoric.
Tracheobronchitis. The acute manifestation of tracheobronchitis is characterized by the production of moist or coarse crackles, a productive cough, chills, a sore throat, a mild fever, muscle and back pain, and substernal tightness. Typically, the patient presents with rhonchi and wheezes. Tracheobronchitis of severe severity can result in a moderate
pyrexia with bronchoconstriction.
Special Considerations
To maintain the patient's unobstructed airway and aid his respiration, raise the head of his inpatient bed. Fluids, humidified air, or oxygen should be administered to liquefy thick secretions and alleviate inflammation of the mucosal membrane. Interstitial crackles caused by cardiogenic pulmonary edema may require the use of diuretics. Limitation of fluid intake may also be required. Rotate the patient every 1 to 2 hours and advise him to engage in slow, deep breathing.
Strategically schedule daily uninterrupted intervals of rest to facilitate the patient's relaxation and sleep. Prepare the patient for diagnostic examinations including chest radiography, a pulmonary computed tomography, and sputum analysis.
Therapeutic Counseling for Patients
Provide the patient with instruction on efficient coughing methods and the need of avoiding respiratory irritants. Underline the significance of smoking cessation and direct him to suitable resources to facilitate his cessation.
Key Pediatric Resources
Infants or youngsters exhibiting crackles may be indicative of a severe cardiovascular or respiratory condition. Children with pneumonias display diffuse, abrupt crackles. Both esophageal atresia and tracheoesophageal fistula can result in the production of bubbling, moist crackles when food or secretions are aspirated into the lungs, particularly in newborns. The presence of pulmonary edema results in the formation of fine crackles at the lung bases, while bronchiectasis leads to the production of moist crackles. Among babies, cystic fibrosis causes extensive, fine to coarse inspiratory crackles and wheezing. Chronic sickle cell anemia might result in crackles when it leads to pulmonary infarction or infection. An infection caused by respiratory syncytial virus in the lower respiratory tract usually results in the production of fine crackles and wheezes.
Guidelines for Geriatrics
Crackles that resolve with deep inhalation may suggest the presence of mild basilar atelectasis. Conduct auscultation on the lung bases of elderly individuals both before and after auscultating the apices.
