- Published on
Infectious Diseases and Microbiology: Low Back Pain and Fever
Basics
Description
Back pain refers to acute or chronic pain arising from the spine or paraspinal structures. The combination of back pain and fever requires careful evaluation for nonmechanical causes. History should specifically assess weight loss, pain worse when lying down, morning stiffness, and sudden severe or colicky pain. Serial spinal and neurologic examinations are crucial, and any spinal tenderness or focal pain warrants full diagnostic assessment. Vertebral osteomyelitis is commonly suggested by pain worsened by movement and not relieved by rest, focal vertebral tenderness, and elevated erythrocyte sedimentation rate. Pain from neoplastic nerve infiltration is typically constant, progressively worse, and persists at night without relief, whereas mechanical low back pain usually improves with rest. Work-up often begins with plain radiography followed by bone scintigraphy, MRI, CT, laboratory testing, and biopsy based on abnormal findings.
Epidemiology
A definitive pain source is difficult to establish and is identified in fewer than one-quarter of cases. Mechanical causes account for about 97% of low back pain, with degenerative disk disease and lumbar sprain/strain comprising most cases. The spine is a frequent site of bone metastasis. Vertebral osteomyelitis is uncommon at roughly 1 per 100,000 persons annually, with rising rates attributed to vascular devices and intravenous drug use; it occurs more often in early childhood and in adults over 50. Spinal epidural abscess occurs in about 1 per 10,000 hospital admissions per year, and MRSA-related vertebral osteomyelitis and epidural abscess are increasingly reported. Despite global increases in tuberculosis, the rate of extrapulmonary spinal disease remains relatively stable; Pott disease, typically involving the lower thoracic vertebrae, is the most common musculoskeletal extrapulmonary manifestation. Improved survival in sickle cell disease has been accompanied by more Salmonella vertebral osteomyelitis.
Risk Factors
Infectious complications can follow bites from many animals, often linked to occupational exposure (farmers, laboratory workers, veterinarians) or recreation (hunters, campers, exotic pet owners). Systemic infection after animal or human bites is more likely with extremity edema or impaired lymphatic drainage and in immunocompromised hosts. Fever after a dog bite in an immunosuppressed patient should prompt concern for invasive Capnocytophaga canimorsus infection.
Etiology
Infectious sources of back pain with fever include biliary tract infection, chronic prostatitis, herpes zoster, pyelonephritis, retroperitoneal abscess, spinal epidural abscess, and vertebral osteomyelitis. Noninfectious causes include colonic cancer, pancreatic disease, histiocytosis X, metastatic malignancy (breast, lung, prostate, thyroid, kidney, gastrointestinal tract), multiple myeloma, neoplastic invasion of pelvic nerves, lymphoma, pregnancy, vertebral fracture, renal artery or vein thrombosis, renal stones, retroperitoneal hemorrhage or tumors, and tumors of the posterior stomach or duodenum. Staphylococcus aureus is the leading cause of spinal epidural abscess, accounting for most reported cases, with additional pathogens including Actinomyces israelii, Aspergillus, Blastomyces, Brucella, Cryptococcus, Haemophilus parainfluenzae, Mycobacterium tuberculosis, and Streptococcus milleri. Vertebral osteomyelitis is most often due to staphylococci but may be caused by other bacteria or tuberculosis; one multicenter retrospective study from southern Spain reported a high proportion due to Brucella, with the remainder split between pyogenic and tuberculous disease.
Commonly Associated Conditions
Vertebral osteomyelitis and spinal epidural abscess are frequently associated with diabetes, injection drug use, chronic renal failure, alcohol use disorder, bacteremia or focal infections, and malignancy. Most epidural abscesses arise via hematogenous spread from skin or mucosal sources, though direct extension from adjacent infection is also recognized. Postoperative abscesses account for a substantial minority, and epidural catheter placement is another risk factor. Blunt trauma may precede symptoms and may lead to an epidural hematoma that later becomes infected.
Diagnosis
Spinal epidural abscess classically presents with fever, spinal pain and tenderness, and radicular pain progressing to limb weakness, with pain being the most consistent feature. Early on, spinal pain with or without fever may be the only findings before sudden neurologic decline. When sepsis dominates or when patients are bedbound, neurologic deficits may be missed. Fever is absent in a notable minority of pyogenic vertebral osteomyelitis cases and is even more commonly absent in tuberculous vertebral osteomyelitis.
History
Key elements include age; systemic symptoms such as fever, weakness, weight loss, and night sweats; prior trauma, infection, or cancer; pain characteristics; immune status; glycemic control in diabetes; and injection drug use. Screen for neurologic complaints including weakness, paresthesias, numbness, and bowel, bladder, or sexual dysfunction. Risk is higher in patients over 50, those using steroids, individuals with HIV, those on immunosuppressants, and those with prior surgery.
Physical Examination
Assess general appearance, vital signs, peripheral pulses, and perform a focused cardiopulmonary and abdominal evaluation in unstable patients. Look for referred pain by examining potential primary sources of tenderness. Perform a complete neurologic examination to evaluate for spinal cord compromise and localize deficits; lesions below T12 can produce lower motor neuron findings, and cauda equina syndrome may include bowel or bladder incontinence. In older adults, fever may be low-grade and does not reliably indicate severity. Percussion of spinous processes may reveal focal vertebral tenderness due to trauma, malignancy, or infection. Examine for signs of endocarditis and septic emboli.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine blood tests are often nonspecific for vertebral osteomyelitis, but leukocytosis, neutrophilia, and markedly elevated ESR and C-reactive protein support pyogenic disease. Blood cultures are the most useful routine test and identify the organism in about half of pyogenic and Brucella vertebral osteomyelitis cases. Bone biopsy is often required to confirm the diagnosis, especially in tuberculous disease.
Imaging
Plain spinal radiographs may be normal early in vertebral osteomyelitis. MRI best defines the extent and location of spinal epidural abscess. MRI or CT myelography is preferred when spinal metastasis is suspected.
Diagnostic Procedures/Other
CT-guided needle biopsy reliably diagnoses carcinoma but is less dependable for lymphoma, though performance has improved with CT guidance, immunophenotyping, and larger needles; false-negative rates remain significant. Establishing an etiologic diagnosis of vertebral osteomyelitis often requires percutaneous or surgical vertebral biopsy.
Differential Diagnosis
Tuberculosis may appear early as an opportunistic infection in AIDS and can be AIDS-defining, while Mycobacterium avium complex typically occurs later with very low CD4 counts. Pertussis should be considered when cough is the predominant symptom, particularly with paroxysms, inspiratory whoop, posttussive vomiting, sleep-disrupting cough, or exposure to similar illness.
Treatment
Medications
Suspected vertebral osteomyelitis or epidural abscess warrants empiric vancomycin to cover MRSA, with addition of a third- or fourth-generation cephalosporin when gram-negative bacteremia is suspected, especially with concurrent pyelonephritis. Therapy should be narrowed once the pathogen is identified; for methicillin-sensitive S. aureus, options include nafcillin, oxacillin, or cefazolin. Typical duration is at least six weeks. Management of tuberculous, brucellar, and salmonella bone disease follows their respective regimens. Corticosteroids may help in acute spinal cord compression. NSAIDs provide symptomatic analgesia, and bisphosphonates may be used for fractures related to breast cancer metastases.
Additional Treatment
Prompt diagnosis with targeted therapy is essential. Epidural abscess requires urgent surgical management with early decompression plus antibiotics. Spinal cord compression is a neurosurgical emergency, and decompression via surgery or radiotherapy within 24 hours of symptom onset is needed to reduce permanent neurologic injury. In suspected spinal or paraspinal infection, bactericidal empiric antibiotics should be started immediately.
.
Ongoing Care and Follow-Up
If symptoms persist beyond six weeks, repeat laboratory testing and imaging are recommended. After six weeks of antibiotics for osteomyelitis or epidural abscess, reassessment is needed to determine whether treatment should continue. Ongoing monitoring for medication toxicity is important, particularly in older adults who are more susceptible to adverse drug effects.
Basics
Description
Back pain refers to acute or chronic pain arising from the spine or paraspinal structures. The combination of back pain and fever requires careful evaluation for nonmechanical causes. History should specifically assess weight loss, pain worse when lying down, morning stiffness, and sudden severe or colicky pain. Serial spinal and neurologic examinations are crucial, and any spinal tenderness or focal pain warrants full diagnostic assessment. Vertebral osteomyelitis is commonly suggested by pain worsened by movement and not relieved by rest, focal vertebral tenderness, and elevated erythrocyte sedimentation rate. Pain from neoplastic nerve infiltration is typically constant, progressively worse, and persists at night without relief, whereas mechanical low back pain usually improves with rest. Work-up often begins with plain radiography followed by bone scintigraphy, MRI, CT, laboratory testing, and biopsy based on abnormal findings.
Epidemiology
A definitive pain source is difficult to establish and is identified in fewer than one-quarter of cases. Mechanical causes account for about 97% of low back pain, with degenerative disk disease and lumbar sprain/strain comprising most cases. The spine is a frequent site of bone metastasis. Vertebral osteomyelitis is uncommon at roughly 1 per 100,000 persons annually, with rising rates attributed to vascular devices and intravenous drug use; it occurs more often in early childhood and in adults over 50. Spinal epidural abscess occurs in about 1 per 10,000 hospital admissions per year, and MRSA-related vertebral osteomyelitis and epidural abscess are increasingly reported. Despite global increases in tuberculosis, the rate of extrapulmonary spinal disease remains relatively stable; Pott disease, typically involving the lower thoracic vertebrae, is the most common musculoskeletal extrapulmonary manifestation. Improved survival in sickle cell disease has been accompanied by more Salmonella vertebral osteomyelitis.
Risk Factors
Infectious complications can follow bites from many animals, often linked to occupational exposure (farmers, laboratory workers, veterinarians) or recreation (hunters, campers, exotic pet owners). Systemic infection after animal or human bites is more likely with extremity edema or impaired lymphatic drainage and in immunocompromised hosts. Fever after a dog bite in an immunosuppressed patient should prompt concern for invasive Capnocytophaga canimorsus infection.
Etiology
Infectious sources of back pain with fever include biliary tract infection, chronic prostatitis, herpes zoster, pyelonephritis, retroperitoneal abscess, spinal epidural abscess, and vertebral osteomyelitis. Noninfectious causes include colonic cancer, pancreatic disease, histiocytosis X, metastatic malignancy (breast, lung, prostate, thyroid, kidney, gastrointestinal tract), multiple myeloma, neoplastic invasion of pelvic nerves, lymphoma, pregnancy, vertebral fracture, renal artery or vein thrombosis, renal stones, retroperitoneal hemorrhage or tumors, and tumors of the posterior stomach or duodenum. Staphylococcus aureus is the leading cause of spinal epidural abscess, accounting for most reported cases, with additional pathogens including Actinomyces israelii, Aspergillus, Blastomyces, Brucella, Cryptococcus, Haemophilus parainfluenzae, Mycobacterium tuberculosis, and Streptococcus milleri. Vertebral osteomyelitis is most often due to staphylococci but may be caused by other bacteria or tuberculosis; one multicenter retrospective study from southern Spain reported a high proportion due to Brucella, with the remainder split between pyogenic and tuberculous disease.
Commonly Associated Conditions
Vertebral osteomyelitis and spinal epidural abscess are frequently associated with diabetes, injection drug use, chronic renal failure, alcohol use disorder, bacteremia or focal infections, and malignancy. Most epidural abscesses arise via hematogenous spread from skin or mucosal sources, though direct extension from adjacent infection is also recognized. Postoperative abscesses account for a substantial minority, and epidural catheter placement is another risk factor. Blunt trauma may precede symptoms and may lead to an epidural hematoma that later becomes infected.
Diagnosis
Spinal epidural abscess classically presents with fever, spinal pain and tenderness, and radicular pain progressing to limb weakness, with pain being the most consistent feature. Early on, spinal pain with or without fever may be the only findings before sudden neurologic decline. When sepsis dominates or when patients are bedbound, neurologic deficits may be missed. Fever is absent in a notable minority of pyogenic vertebral osteomyelitis cases and is even more commonly absent in tuberculous vertebral osteomyelitis.
History
Key elements include age; systemic symptoms such as fever, weakness, weight loss, and night sweats; prior trauma, infection, or cancer; pain characteristics; immune status; glycemic control in diabetes; and injection drug use. Screen for neurologic complaints including weakness, paresthesias, numbness, and bowel, bladder, or sexual dysfunction. Risk is higher in patients over 50, those using steroids, individuals with HIV, those on immunosuppressants, and those with prior surgery.
Physical Examination
Assess general appearance, vital signs, peripheral pulses, and perform a focused cardiopulmonary and abdominal evaluation in unstable patients. Look for referred pain by examining potential primary sources of tenderness. Perform a complete neurologic examination to evaluate for spinal cord compromise and localize deficits; lesions below T12 can produce lower motor neuron findings, and cauda equina syndrome may include bowel or bladder incontinence. In older adults, fever may be low-grade and does not reliably indicate severity. Percussion of spinous processes may reveal focal vertebral tenderness due to trauma, malignancy, or infection. Examine for signs of endocarditis and septic emboli.
Diagnostic Tests and Interpretation
Laboratory Studies
Routine blood tests are often nonspecific for vertebral osteomyelitis, but leukocytosis, neutrophilia, and markedly elevated ESR and C-reactive protein support pyogenic disease. Blood cultures are the most useful routine test and identify the organism in about half of pyogenic and Brucella vertebral osteomyelitis cases. Bone biopsy is often required to confirm the diagnosis, especially in tuberculous disease.
Imaging
Plain spinal radiographs may be normal early in vertebral osteomyelitis. MRI best defines the extent and location of spinal epidural abscess. MRI or CT myelography is preferred when spinal metastasis is suspected.
Diagnostic Procedures/Other
CT-guided needle biopsy reliably diagnoses carcinoma but is less dependable for lymphoma, though performance has improved with CT guidance, immunophenotyping, and larger needles; false-negative rates remain significant. Establishing an etiologic diagnosis of vertebral osteomyelitis often requires percutaneous or surgical vertebral biopsy.
Differential Diagnosis
Tuberculosis may appear early as an opportunistic infection in AIDS and can be AIDS-defining, while Mycobacterium avium complex typically occurs later with very low CD4 counts. Pertussis should be considered when cough is the predominant symptom, particularly with paroxysms, inspiratory whoop, posttussive vomiting, sleep-disrupting cough, or exposure to similar illness.
Treatment
Medications
Suspected vertebral osteomyelitis or epidural abscess warrants empiric vancomycin to cover MRSA, with addition of a third- or fourth-generation cephalosporin when gram-negative bacteremia is suspected, especially with concurrent pyelonephritis. Therapy should be narrowed once the pathogen is identified; for methicillin-sensitive S. aureus, options include nafcillin, oxacillin, or cefazolin. Typical duration is at least six weeks. Management of tuberculous, brucellar, and salmonella bone disease follows their respective regimens. Corticosteroids may help in acute spinal cord compression. NSAIDs provide symptomatic analgesia, and bisphosphonates may be used for fractures related to breast cancer metastases.
Additional Treatment
Prompt diagnosis with targeted therapy is essential. Epidural abscess requires urgent surgical management with early decompression plus antibiotics. Spinal cord compression is a neurosurgical emergency, and decompression via surgery or radiotherapy within 24 hours of symptom onset is needed to reduce permanent neurologic injury. In suspected spinal or paraspinal infection, bactericidal empiric antibiotics should be started immediately.
.
Ongoing Care and Follow-Up
If symptoms persist beyond six weeks, repeat laboratory testing and imaging are recommended. After six weeks of antibiotics for osteomyelitis or epidural abscess, reassessment is needed to determine whether treatment should continue. Ongoing monitoring for medication toxicity is important, particularly in older adults who are more susceptible to adverse drug effects.
- Published on
Infectious Diseases and Microbiology: Diarrhea and Fever
Basics
Description
Diarrhea is defined as stool output exceeding 200 g/day and, in practice, as three or more loose stools daily. It is acute when <14 days and chronic when>4 weeks. Inflammatory diarrhea presents with frequent, small-volume stools that are mucoid and/or bloody and may include tenesmus, fever, or severe abdominal pain; stool leukocytes are a key feature. Noninflammatory diarrhea is typically watery, may be high volume (>1 L/day), and occurs without blood, pus, severe pain, or fever.
Epidemiology
Incidence
In the United States, acute diarrhea occurs hundreds of millions of times yearly, with tens of millions of episodes linked to identified pathogens, and foodborne spread accounting for a large proportion of known-pathogen disease. Surveillance data have identified non-typhoidal Salmonella, Campylobacter, Shigella, Cryptosporidium, and Shiga toxin–producing E. coli O157 as leading reported causes, with highest bacterial diarrhea rates from Salmonella, Campylobacter, and Yersinia in infants under one year. Post-diarrheal hemolytic uremic syndrome occurs infrequently overall but is most common in children under five. Traveler’s diarrhea affects a substantial fraction of international travelers.
Risk Factors
Risks include consuming undercooked eggs, meat, poultry, seafood, or unpasteurized dairy, and drinking untreated surface water. Greater severity or pathogen-specific risk occurs with HIV, immunosuppressive therapies (including glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic exposure, liver disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. Oral–anal sexual contact increases risk of enteric infection. Antibiotic exposure is a major risk factor for Clostridioides difficile–associated diarrhea.
General Prevention
Handwashing before eating or food preparation, avoiding undercooked animal products and unpasteurized dairy, and avoiding untreated stream or river water reduce risk. During travel in areas with unsafe water, avoid tap water and ice. Typhoid vaccination is available for travelers, and infant rotavirus vaccination is recommended in the United States; destination-based vaccine guidance is available through travel medicine resources.
Etiology
Bacterial causes include Campylobacter, Salmonella, Shigella, Yersinia enterocolitica, C. difficile, Vibrio cholerae, Vibrio parahaemolyticus, Aeromonas, Plesiomonas shigelloides, and multiple diarrheagenic E. coli pathotypes including ETEC, EPEC, EIEC, STEC (including O157:H7), and EAEC. Viral causes include rotavirus, human caliciviruses such as norovirus, adenovirus, and cytomegalovirus. Parasitic causes include Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis. Toxin-mediated syndromes include Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens.
Diagnosis
History
Evaluation should define likely cause, illness severity, and complications. Ask about travel, diet, antibiotic use, sexual practices, day-care exposure, sick contacts, outbreaks, seasonality, and other illnesses, and characterize stool frequency, duration, and appearance. Infectious diarrhea may include fever, chills, vomiting, nausea, abdominal pain, and tenesmus. Dizziness, presyncope, or syncope suggests volume depletion. Dysentery points to invasive pathogens such as Shigella, Salmonella, Campylobacter, STEC (often without fever), or Yersinia. STEC commonly starts watery and becomes bloody and is frequently associated with contaminated beef or produce; fever is often absent. Yersinia and Salmonella may involve the terminal ileum and cecum, producing right lower quadrant pain that mimics appendicitis. Watery diarrhea alone is nonspecific. Enterotoxin-mediated food poisoning from S. aureus, B. cereus, or C. perfringens typically has a short incubation and brief course, with vomiting alone more typical of S. aureus or C. perfringens and watery diarrhea more typical of B. cereus or C. perfringens; fever is usually absent. Extraintestinal features such as arthritis, skin lesions, or eye symptoms suggest inflammatory bowel disease. With recent international travel, likely pathogens depend on location, setting, and season, commonly including ETEC, EAEC, Campylobacter, Salmonella, and norovirus, and travel medicine resources can guide evaluation.
Physical Examination
Assess blood pressure, heart rate, respiratory rate, temperature, and mental status to gauge severity. Look for dehydration signs such as dry mucous membranes, reduced skin turgor, sunken eyes, delayed capillary refill, low jugular venous pressure, and orthostatic hypotension. Examine for abdominal tenderness, peritoneal signs, hepatomegaly, and splenomegaly.
Diagnostic Tests and Interpretation
Laboratory Studies
Testing is indicated with fever, systemic toxicity, bloody stools, dehydration, suspected foodborne outbreak, recent international travel, immunosuppression, or recent antibiotic exposure. Send stool for culture, noting that routine processing commonly targets Shigella, Salmonella, and Campylobacter, so the laboratory should be alerted if suspicion is high for STEC or other E. coli pathotypes, Yersinia, Vibrio, or other organisms. Stool culture yield is generally low. For bloody diarrhea, culture for Salmonella, Shigella, Campylobacter, and STEC and obtain a Shiga toxin immunoassay; if E. coli is isolated, arrange serotyping via a reference laboratory. If there is recent antibiotic exposure, recent hospitalization, day-care exposure, or recent chemotherapy, test stool for C. difficile toxins. If diarrhea persists beyond seven days, submit multiple stools for ova and parasite examination with attention to Giardia, Cryptosporidium, Isospora, and Cyclospora and consider noninfectious causes; in AIDS or immunosuppression, also evaluate for microsporidia, Mycobacterium avium complex, and cytomegalovirus. Fecal polymorphonuclear cells support an inflammatory process. If dehydration or severe illness is present, obtain electrolytes, renal and liver function tests, complete blood count, and blood cultures.
Imaging
If the diagnosis remains unclear in critical illness, with prominent abdominal pain or peritoneal signs, consider CT abdomen with oral and intravenous contrast.
t
Diagnostic Procedures/Other
Further evaluation may require upper endoscopy or colonoscopy with biopsies
.
Differential Diagnosis
Acute inflammatory diarrhea may be noninfectious, including ulcerative colitis, Crohn disease, radiation or ischemic colitis, partial obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple disease, pernicious anemia, diabetes-related enteropathy, malabsorption disorders, scleroderma, or celiac disease. Fever and diarrhea can also result from infections outside the gut such as malaria or sepsis.
Treatment
Medications
Core management is rehydration with selective antibiotic use. Oral rehydration is effective and cost-efficient across settings, while intravenous fluids are indicated for severe dehydration or major electrolyte disturbances; rice-based oral solutions are superior for cholera in children and adults. Antibiotics are recommended for severe infection and for persistent gastroenteritis and are favored in adults over 65, immunocompromised patients, those with prosthetic material, and invasive infections, except when STEC is suspected or confirmed. Empiric therapy for febrile community-acquired invasive diarrhea or moderate to severe traveler’s diarrhea includes ciprofloxacin 500 mg twice daily or levofloxacin 500 mg daily while awaiting studies unless STEC is suspected; travel to Southeast Asia raises concern for fluoroquinolone-resistant Campylobacter. For suspected antibiotic-associated or nosocomial diarrhea, treat empirically with metronidazole or vancomycin while awaiting C. difficile testing. Pathogen-directed therapy includes treating non-typhoidal Salmonella in high-risk or severe disease with fluoroquinolones, TMP-SMX, or ceftriaxone for typical short courses and longer courses in immunocompromised patients, recognizing antibiotics may prolong shedding; treating Shigella with short-course fluoroquinolones or TMP-SMX when susceptible and longer courses for severe or immunocompromised cases; treating Campylobacter with erythromycin while acknowledging high fluoroquinolone resistance especially in Southeast Asia; avoiding antibiotics in STEC due to increased HUS risk and providing supportive care; treating ETEC/EPEC/EIEC similarly to traveler’s diarrhea regimens; usually avoiding antibiotics in Yersinia unless severe or immunocompromised, in which case doxycycline plus an aminoglycoside, fluoroquinolones, or TMP-SMX may be used; managing C. difficile by stopping unnecessary antibiotics and using metronidazole for milder disease or oral vancomycin for 10–14 days; prioritizing fluids in cholera with antibiotics guided by local resistance; treating amebiasis with metronidazole followed by a luminal agent such as paromomycin or iodoquinol; treating giardiasis with metronidazole or single-dose tinidazole; and treating Cyclospora or Isospora with TMP-SMX with extended therapy and possible suppression in immunocompromised hosts.
Additional Treatment
Most mild cases resolve without specific therapy; supportive care includes hydration and symptom control. Loperamide is preferred for adults with mild to moderate nonbloody diarrhea but is contraindicated in severe inflammatory diarrhea, bloody diarrhea, C. difficile infection, and in children under two. Bismuth subsalicylate can reduce stool volume in adults and children. Severe or persistent unexplained diarrhea warrants gastroenterology and/or infectious diseases consultation, and cases due to major reportable pathogens or suspected outbreaks should be reported to public health authorities.
In-Patient Considerations
Initial Stabilization
Severe acute inflammatory diarrhea with systemic toxicity requires rapid rehydration and empiric antibiotics.
Admission Criteria
Hospitalize patients with severe dehydration or inability to maintain oral intake.
IV Fluids
Use intravenous volume repletion for severe dehydration or altered mental status.
Discharge Criteria
Discharge is appropriate when fever has been absent for more than 24 hours, vital signs are stable, and the patient can maintain adequate oral fluids and nutrition.
Ongoing Care and Follow-Up
Evaluate and treat household members with similar symptoms when appropriate.
Diet
Resume food about four hours after starting rehydration, using small frequent meals of easily digestible foods, and avoid hyperosmolar fruit juices that can worsen diarrhea.
Patient Education
Counsel on food safety and strategies to prevent foodborne illness, especially during travel.
Prognosis
Gastrointestinal illness contributes to a large burden of hospitalization and death annually in the United States.
Complications
Potential complications include dehydration, electrolyte derangements, bacteremia and sepsis, malnutrition and vitamin loss, hemolytic uremic syndrome, and systemic amebiasis.
Basics
Description
Diarrhea is defined as stool output exceeding 200 g/day and, in practice, as three or more loose stools daily. It is acute when <14 days and chronic when>4 weeks. Inflammatory diarrhea presents with frequent, small-volume stools that are mucoid and/or bloody and may include tenesmus, fever, or severe abdominal pain; stool leukocytes are a key feature. Noninflammatory diarrhea is typically watery, may be high volume (>1 L/day), and occurs without blood, pus, severe pain, or fever.
Epidemiology
Incidence
In the United States, acute diarrhea occurs hundreds of millions of times yearly, with tens of millions of episodes linked to identified pathogens, and foodborne spread accounting for a large proportion of known-pathogen disease. Surveillance data have identified non-typhoidal Salmonella, Campylobacter, Shigella, Cryptosporidium, and Shiga toxin–producing E. coli O157 as leading reported causes, with highest bacterial diarrhea rates from Salmonella, Campylobacter, and Yersinia in infants under one year. Post-diarrheal hemolytic uremic syndrome occurs infrequently overall but is most common in children under five. Traveler’s diarrhea affects a substantial fraction of international travelers.
Risk Factors
Risks include consuming undercooked eggs, meat, poultry, seafood, or unpasteurized dairy, and drinking untreated surface water. Greater severity or pathogen-specific risk occurs with HIV, immunosuppressive therapies (including glucocorticoids, TNF inhibitors, and chemotherapy), recent antibiotic exposure, liver disease, neutropenia, malnutrition, zinc deficiency, and IgA deficiency. Oral–anal sexual contact increases risk of enteric infection. Antibiotic exposure is a major risk factor for Clostridioides difficile–associated diarrhea.
General Prevention
Handwashing before eating or food preparation, avoiding undercooked animal products and unpasteurized dairy, and avoiding untreated stream or river water reduce risk. During travel in areas with unsafe water, avoid tap water and ice. Typhoid vaccination is available for travelers, and infant rotavirus vaccination is recommended in the United States; destination-based vaccine guidance is available through travel medicine resources.
Etiology
Bacterial causes include Campylobacter, Salmonella, Shigella, Yersinia enterocolitica, C. difficile, Vibrio cholerae, Vibrio parahaemolyticus, Aeromonas, Plesiomonas shigelloides, and multiple diarrheagenic E. coli pathotypes including ETEC, EPEC, EIEC, STEC (including O157:H7), and EAEC. Viral causes include rotavirus, human caliciviruses such as norovirus, adenovirus, and cytomegalovirus. Parasitic causes include Giardia intestinalis, Cryptosporidium parvum, Entamoeba histolytica, Cyclospora cayetanensis, Isospora belli, and Strongyloides stercoralis. Toxin-mediated syndromes include Staphylococcus aureus, Bacillus cereus, and Clostridium perfringens.
Diagnosis
History
Evaluation should define likely cause, illness severity, and complications. Ask about travel, diet, antibiotic use, sexual practices, day-care exposure, sick contacts, outbreaks, seasonality, and other illnesses, and characterize stool frequency, duration, and appearance. Infectious diarrhea may include fever, chills, vomiting, nausea, abdominal pain, and tenesmus. Dizziness, presyncope, or syncope suggests volume depletion. Dysentery points to invasive pathogens such as Shigella, Salmonella, Campylobacter, STEC (often without fever), or Yersinia. STEC commonly starts watery and becomes bloody and is frequently associated with contaminated beef or produce; fever is often absent. Yersinia and Salmonella may involve the terminal ileum and cecum, producing right lower quadrant pain that mimics appendicitis. Watery diarrhea alone is nonspecific. Enterotoxin-mediated food poisoning from S. aureus, B. cereus, or C. perfringens typically has a short incubation and brief course, with vomiting alone more typical of S. aureus or C. perfringens and watery diarrhea more typical of B. cereus or C. perfringens; fever is usually absent. Extraintestinal features such as arthritis, skin lesions, or eye symptoms suggest inflammatory bowel disease. With recent international travel, likely pathogens depend on location, setting, and season, commonly including ETEC, EAEC, Campylobacter, Salmonella, and norovirus, and travel medicine resources can guide evaluation.
Physical Examination
Assess blood pressure, heart rate, respiratory rate, temperature, and mental status to gauge severity. Look for dehydration signs such as dry mucous membranes, reduced skin turgor, sunken eyes, delayed capillary refill, low jugular venous pressure, and orthostatic hypotension. Examine for abdominal tenderness, peritoneal signs, hepatomegaly, and splenomegaly.
Diagnostic Tests and Interpretation
Laboratory Studies
Testing is indicated with fever, systemic toxicity, bloody stools, dehydration, suspected foodborne outbreak, recent international travel, immunosuppression, or recent antibiotic exposure. Send stool for culture, noting that routine processing commonly targets Shigella, Salmonella, and Campylobacter, so the laboratory should be alerted if suspicion is high for STEC or other E. coli pathotypes, Yersinia, Vibrio, or other organisms. Stool culture yield is generally low. For bloody diarrhea, culture for Salmonella, Shigella, Campylobacter, and STEC and obtain a Shiga toxin immunoassay; if E. coli is isolated, arrange serotyping via a reference laboratory. If there is recent antibiotic exposure, recent hospitalization, day-care exposure, or recent chemotherapy, test stool for C. difficile toxins. If diarrhea persists beyond seven days, submit multiple stools for ova and parasite examination with attention to Giardia, Cryptosporidium, Isospora, and Cyclospora and consider noninfectious causes; in AIDS or immunosuppression, also evaluate for microsporidia, Mycobacterium avium complex, and cytomegalovirus. Fecal polymorphonuclear cells support an inflammatory process. If dehydration or severe illness is present, obtain electrolytes, renal and liver function tests, complete blood count, and blood cultures.
Imaging
If the diagnosis remains unclear in critical illness, with prominent abdominal pain or peritoneal signs, consider CT abdomen with oral and intravenous contrast.
t
Diagnostic Procedures/Other
Further evaluation may require upper endoscopy or colonoscopy with biopsies
.
Differential Diagnosis
Acute inflammatory diarrhea may be noninfectious, including ulcerative colitis, Crohn disease, radiation or ischemic colitis, partial obstruction, diverticulitis, laxative abuse, rectosigmoid abscess, Whipple disease, pernicious anemia, diabetes-related enteropathy, malabsorption disorders, scleroderma, or celiac disease. Fever and diarrhea can also result from infections outside the gut such as malaria or sepsis.
Treatment
Medications
Core management is rehydration with selective antibiotic use. Oral rehydration is effective and cost-efficient across settings, while intravenous fluids are indicated for severe dehydration or major electrolyte disturbances; rice-based oral solutions are superior for cholera in children and adults. Antibiotics are recommended for severe infection and for persistent gastroenteritis and are favored in adults over 65, immunocompromised patients, those with prosthetic material, and invasive infections, except when STEC is suspected or confirmed. Empiric therapy for febrile community-acquired invasive diarrhea or moderate to severe traveler’s diarrhea includes ciprofloxacin 500 mg twice daily or levofloxacin 500 mg daily while awaiting studies unless STEC is suspected; travel to Southeast Asia raises concern for fluoroquinolone-resistant Campylobacter. For suspected antibiotic-associated or nosocomial diarrhea, treat empirically with metronidazole or vancomycin while awaiting C. difficile testing. Pathogen-directed therapy includes treating non-typhoidal Salmonella in high-risk or severe disease with fluoroquinolones, TMP-SMX, or ceftriaxone for typical short courses and longer courses in immunocompromised patients, recognizing antibiotics may prolong shedding; treating Shigella with short-course fluoroquinolones or TMP-SMX when susceptible and longer courses for severe or immunocompromised cases; treating Campylobacter with erythromycin while acknowledging high fluoroquinolone resistance especially in Southeast Asia; avoiding antibiotics in STEC due to increased HUS risk and providing supportive care; treating ETEC/EPEC/EIEC similarly to traveler’s diarrhea regimens; usually avoiding antibiotics in Yersinia unless severe or immunocompromised, in which case doxycycline plus an aminoglycoside, fluoroquinolones, or TMP-SMX may be used; managing C. difficile by stopping unnecessary antibiotics and using metronidazole for milder disease or oral vancomycin for 10–14 days; prioritizing fluids in cholera with antibiotics guided by local resistance; treating amebiasis with metronidazole followed by a luminal agent such as paromomycin or iodoquinol; treating giardiasis with metronidazole or single-dose tinidazole; and treating Cyclospora or Isospora with TMP-SMX with extended therapy and possible suppression in immunocompromised hosts.
Additional Treatment
Most mild cases resolve without specific therapy; supportive care includes hydration and symptom control. Loperamide is preferred for adults with mild to moderate nonbloody diarrhea but is contraindicated in severe inflammatory diarrhea, bloody diarrhea, C. difficile infection, and in children under two. Bismuth subsalicylate can reduce stool volume in adults and children. Severe or persistent unexplained diarrhea warrants gastroenterology and/or infectious diseases consultation, and cases due to major reportable pathogens or suspected outbreaks should be reported to public health authorities.
In-Patient Considerations
Initial Stabilization
Severe acute inflammatory diarrhea with systemic toxicity requires rapid rehydration and empiric antibiotics.
Admission Criteria
Hospitalize patients with severe dehydration or inability to maintain oral intake.
IV Fluids
Use intravenous volume repletion for severe dehydration or altered mental status.
Discharge Criteria
Discharge is appropriate when fever has been absent for more than 24 hours, vital signs are stable, and the patient can maintain adequate oral fluids and nutrition.
Ongoing Care and Follow-Up
Evaluate and treat household members with similar symptoms when appropriate.
Diet
Resume food about four hours after starting rehydration, using small frequent meals of easily digestible foods, and avoid hyperosmolar fruit juices that can worsen diarrhea.
Patient Education
Counsel on food safety and strategies to prevent foodborne illness, especially during travel.
Prognosis
Gastrointestinal illness contributes to a large burden of hospitalization and death annually in the United States.
Complications
Potential complications include dehydration, electrolyte derangements, bacteremia and sepsis, malnutrition and vitamin loss, hemolytic uremic syndrome, and systemic amebiasis.
- Published on
Infectious Diseases and Microbiology: Dysuria and Fever
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.
Basics
Description
Dysuria refers to painful urination. Acute urethral syndrome describes dysuria with urgency and frequency in the absence of significant bacteriuria.
Approach to the Patient
Irritation of urethral and bladder mucosa typically causes frequent, painful voiding of small urine volumes. Dysuria is often assumed to be a urinary tract infection and treated empirically, which can miss important diagnoses in some patients and lead to unnecessary antibiotics in others, so targeted evaluation is preferred. A focused history and examination, including pelvic and rectal examination when indicated, often clarifies the cause and enables directed therapy. Sexually transmitted infections including Chlamydia trachomatis, Neisseria gonorrhoeae, and herpes simplex virus can cause dysuria in any sex. Prostatitis is a key diagnosis in men because it is harder to eradicate and can recur. Fever is uncommon in cystitis but may occur with acute prostatitis; dysuria with fever should also raise concern for upper-tract infection such as pyelonephritis. Primary genital herpes can cause dysuria with fever, while chlamydia, gonorrhea, and nonspecific urethritis rarely cause fever unless complicated by pelvic inflammatory disease or Fitz-Hugh–Curtis syndrome. Dysuria with hematuria suggests infectious or noninfectious cystitis and also warrants consideration of tuberculous cystitis, bladder cancer, trauma, renal stones, and schistosomiasis. Dysuria with urethral or vaginal discharge suggests gonorrhea or chlamydia, nonspecific urethritis (with or without conjunctivitis and arthritis consistent with reactive arthritis), and prostatitis. Urinalysis and urine culture are standard initial tests, though young women with classic uncomplicated symptoms and no risk factors for complicated or recurrent infection may be treated empirically.
Epidemiology
Incidence
UTIs are among the most common infectious syndromes and carry substantial costs, including antibiotic expenditures exceeding one billion dollars annually in the United States. Most patients with primary symptomatic genital herpes experience dysuria, though dysuria is typically absent with recurrences. Sexual intercourse is linked to several dysuria etiologies, with symptom timing differing by syndrome: postcoital cystitis often appears within days, urethritis tends to appear after one to two weeks, and vaginitis may present weeks to months later. Pyelonephritis is a frequent cause of hospitalization, and UTIs account for over 100,000 U.S. admissions annually. Healthcare-associated infections are often UTIs, commonly catheter-related; bacteriuria develops in a substantial proportion of patients with prolonged catheterization with a daily incremental risk of infection, and even single catheterization can cause UTI. Escherichia coli causes most uncomplicated UTIs. In pregnancy, asymptomatic bacteriuria can progress to pyelonephritis and is associated with adverse obstetric outcomes including premature labor
.
Etiology
Beyond bacterial cystitis and pyelonephritis and sexually transmitted causes, dysuria may result from atrophic vaginitis, Candida-associated vaginitis, irritation from a distal urethral stone, chemical exposures, compression from an adnexal mass, radiation injury, and vaginal or urethral trauma including sexual abuse or foreign body insertion. Among women with acute dysuria and frequency, most have significant bacteriuria, and many without significant bacteriuria still have infections of the bladder, kidneys, or urethra. Ureaplasma urealyticum is often detected in symptomatic patients but is also found in asymptomatic individuals, and both U. urealyticum and Mycoplasma hominis have been identified in prostatic and renal tissues in patients with dysuria. Adenovirus can cause acute hemorrhagic cystitis in children and some young adults, sometimes in outbreaks, while other urinary viral isolates are generally not considered causes of infection in immunocompetent hosts.
Diagnosis
History
Dysuria with frequency, urgency, and suprapubic discomfort commonly reflects bladder or urethral inflammation. Prostatitis typically causes dysuria, frequency, and urgency and may be suggested by a boggy, tender prostate on rectal examination. Acute pyelonephritis usually evolves over hours to a day with fever, rigors, nausea, vomiting, and sometimes diarrhea; cystitis symptoms may be absent or present. Examination in pyelonephritis often shows fever, tachycardia, diffuse myalgias, and marked costovertebral angle tenderness. Evaluate predisposing factors for UTI or pyelonephritis, including atrophic vaginitis, which may present with reduced discharge, vaginal tenderness, postcoital spotting, and dyspareunia.
Physical Examination
Check vital signs and hydration, especially when pyelonephritis is possible. Suprapubic tenderness supports lower-tract infection, while flank tenderness suggests upper-tract involvement. Perform a genital examination when sexually transmitted infection is suspected, and perform a prostate examination in all men.
Diagnostic Tests and Interpretation
Laboratory Studies
Pyuria is the most sensitive indicator of UTI, and leukocyte esterase testing is highly sensitive for detecting infection-associated pyuria. Urine colony counts of 10^5 CFU/mL generally indicate infection, while lower thresholds (≥10^2 CFU/mL) can be diagnostic in symptomatic patients and in specimens obtained by suprapubic aspiration or catheterization. Most uropathogens convert nitrate to nitrite; nitrite positivity is highly specific but has low sensitivity. Rapid bacteriuria detection methods using techniques such as photometry or bioluminescence can yield results in one to two hours but may miss infections when lower colony counts are used as the comparison standard. Sterile pyuria suggests atypical infections such as chlamydia, ureaplasma, tuberculosis, or fungal infection and can also occur with prostatitis and noninfectious urologic conditions including stones, structural abnormalities, nephrocalcinosis, vesicoureteral reflux, interstitial nephritis, polycystic kidney disease, and related disorders.
Treatment
Therapy for acute urethritis depends on cause. Uncomplicated lower-tract infection in women is treated with short-course antibiotics (about 3–5 days), while men or those with upper-tract disease generally require longer courses (10–14 days). Suspected or confirmed prostatitis requires prolonged therapy, typically at least four weeks. Patients with acute dysuria and frequency who have negative urine cultures and no pyuria generally do not improve with antibiotics.
Ongoing Care and Follow-Up
Many women experience cystitis during their lifetime, and recurrent episodes are common. Most recurrent UTIs represent reinfections after at least one month without symptoms and are often related to vaginal and rectal colonization with uropathogens; anatomic abnormalities are uncommon in young women with recurrent cystitis.
Complications
Lower-tract infection can ascend and cause upper-tract disease.

- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocele
Basics
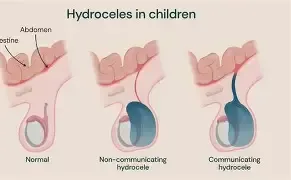
Description Hydrocele is the most common cause of painless scrotal swelling and is classified as congenital or acquired. Congenital hydrocele results from a patent processus vaginalis with communication between the tunica vaginalis and peritoneal cavity; most close spontaneously by 2 years of age. Acquired (secondary) hydrocele occurs due to intrascrotal infection, neoplasm, inguinal or scrotal surgery, or regional or systemic disease. Communicating hydrocele involves a patent processus vaginalis, with scrotal size fluctuating based on position and intra-abdominal pressure. Noncommunicating hydrocele results from excess serous fluid production or impaired absorption within the scrotum.
Etiology Hydrocele results from an imbalance between fluid production and resorption between the tunica vaginalis and tunica albuginea. Causes of adult noncommunicating hydrocele include epididymitis, trauma, mumps, tuberculosis, hypoalbuminemia, and spermatic vein ligation. In the developing world, filarial infections such as Wuchereria bancrofti or Loa loa are the most common causes worldwide. Rare causes include testicular malignancy or lymphoma and abdominoscrotal hydrocele, which may compress adjacent structures causing hydroureter or unilateral limb edema; ultrasound shows a single sac extending through the deep inguinal ring.
Pediatric considerations Congenital hydrocele occurs in approximately 6% of newborn boys and is commonly diagnosed in the newborn period. It is caused by a patent processus vaginalis, which remains open in most newborns. Size may vary with position or crying, and the mass may intermittently resolve. Most close spontaneously by age 2 years.
Diagnosis
Signs and symptoms Painless scrotal swelling with a sensation of heaviness, pulling, or dragging.
History Focus on onset, progression, variability in size, and exclusion of testicular torsion.
Physical exam The mass may feel soft and doughy or firm depending on fluid volume. Transillumination may show homogeneous light transmission but is increasingly replaced by bedside ultrasound.
Essential workup Bedside ultrasound is the diagnostic test of choice, allowing visualization of the hydrocele and testicle and helping identify underlying masses. In adults, the entire testicle must be palpated because hydrocele may obscure a primary neoplasm.
Diagnosis tests and interpretation
Laboratory No routine laboratory testing is required unless evaluating an underlying cause (e.g., urinalysis, AFP, β-hCG).
Imaging Ultrasound demonstrates a large anechoic fluid-filled collection surrounding the anterolateral aspect of the testicle.
Differential diagnosis Epididymitis, indirect inguinal hernia, orchitis, testicular neoplasm, testicular torsion, varicocele.
Treatment
Initial stabilization/therapy Address and stabilize any underlying cause such as trauma or infection.
Emergency department management Perform thorough testicular examination to exclude neoplasm and arrange appropriate referral.
Medication Treat underlying pathology if identified.
Follow-up and disposition
Admission criteria Secondary hydrocele with concern for underlying pathology such as trauma or malignancy.
Discharge criteria Otherwise healthy patients may be discharged with urology referral. Hydrocele repair is elective and performed for discomfort or cosmetic reasons. Options include surgical hydrocelectomy or aspiration with sclerotherapy.
Pediatric considerations Most infant hydroceles resolve spontaneously by 12 months; observation and referral are appropriate. Persistent hydroceles after 12–18 months should be referred for surgical repair due to associated inguinal hernia risk.
Follow-up recommendations Urology follow-up is recommended.
Key points Hydroceles may not transilluminate if the tunica vaginalis is thickened. Bedside ultrasound should always confirm both the fluid collection and normal testicular anatomy to avoid missing serious pathology.
Basics
Description Hydrocele is the most common cause of painless scrotal swelling and is classified as congenital or acquired. Congenital hydrocele results from a patent processus vaginalis with communication between the tunica vaginalis and peritoneal cavity; most close spontaneously by 2 years of age. Acquired (secondary) hydrocele occurs due to intrascrotal infection, neoplasm, inguinal or scrotal surgery, or regional or systemic disease. Communicating hydrocele involves a patent processus vaginalis, with scrotal size fluctuating based on position and intra-abdominal pressure. Noncommunicating hydrocele results from excess serous fluid production or impaired absorption within the scrotum.
Etiology Hydrocele results from an imbalance between fluid production and resorption between the tunica vaginalis and tunica albuginea. Causes of adult noncommunicating hydrocele include epididymitis, trauma, mumps, tuberculosis, hypoalbuminemia, and spermatic vein ligation. In the developing world, filarial infections such as Wuchereria bancrofti or Loa loa are the most common causes worldwide. Rare causes include testicular malignancy or lymphoma and abdominoscrotal hydrocele, which may compress adjacent structures causing hydroureter or unilateral limb edema; ultrasound shows a single sac extending through the deep inguinal ring.
Pediatric considerations Congenital hydrocele occurs in approximately 6% of newborn boys and is commonly diagnosed in the newborn period. It is caused by a patent processus vaginalis, which remains open in most newborns. Size may vary with position or crying, and the mass may intermittently resolve. Most close spontaneously by age 2 years.
Diagnosis
Signs and symptoms Painless scrotal swelling with a sensation of heaviness, pulling, or dragging.
History Focus on onset, progression, variability in size, and exclusion of testicular torsion.
Physical exam The mass may feel soft and doughy or firm depending on fluid volume. Transillumination may show homogeneous light transmission but is increasingly replaced by bedside ultrasound.
Essential workup Bedside ultrasound is the diagnostic test of choice, allowing visualization of the hydrocele and testicle and helping identify underlying masses. In adults, the entire testicle must be palpated because hydrocele may obscure a primary neoplasm.
Diagnosis tests and interpretation
Laboratory No routine laboratory testing is required unless evaluating an underlying cause (e.g., urinalysis, AFP, β-hCG).
Imaging Ultrasound demonstrates a large anechoic fluid-filled collection surrounding the anterolateral aspect of the testicle.
Differential diagnosis Epididymitis, indirect inguinal hernia, orchitis, testicular neoplasm, testicular torsion, varicocele.
Treatment
Initial stabilization/therapy Address and stabilize any underlying cause such as trauma or infection.
Emergency department management Perform thorough testicular examination to exclude neoplasm and arrange appropriate referral.
Medication Treat underlying pathology if identified.
Follow-up and disposition
Admission criteria Secondary hydrocele with concern for underlying pathology such as trauma or malignancy.
Discharge criteria Otherwise healthy patients may be discharged with urology referral. Hydrocele repair is elective and performed for discomfort or cosmetic reasons. Options include surgical hydrocelectomy or aspiration with sclerotherapy.
Pediatric considerations Most infant hydroceles resolve spontaneously by 12 months; observation and referral are appropriate. Persistent hydroceles after 12–18 months should be referred for surgical repair due to associated inguinal hernia risk.
Follow-up recommendations Urology follow-up is recommended.
Key points Hydroceles may not transilluminate if the tunica vaginalis is thickened. Bedside ultrasound should always confirm both the fluid collection and normal testicular anatomy to avoid missing serious pathology.
- Published on
Emergency And Acute Medicine-Hypercalcemia
Basics
Description Hypercalcemia severity depends on the absolute calcium level and the rate of rise. It is detected in approximately 0.1–1% of routine screenings. Most cases are mild (<12 mg/dL) and asymptomatic. Hypercalcemic crisis, typically >14 mg/dL, causes severe and potentially life-threatening manifestations. Circulating calcium exists as ionized (45%, the only physiologically active form), protein-bound (40%, mainly albumin), and complexed to anions (15%).
Etiology The most common causes are primary hyperparathyroidism and malignancy, followed by miscellaneous conditions.
Diagnosis
Signs and symptoms Neurologic features include headache, fatigue, lethargy, weakness, impaired concentration, confusion, depression, paranoia, stupor, or coma. Renal manifestations include polyuria, polydipsia, dehydration, oliguria in renal failure, nephrolithiasis, nephrocalcinosis, and interstitial nephritis. Gastrointestinal symptoms include anorexia, nausea, vomiting, abdominal pain, constipation, peptic ulcer disease, and pancreatitis. Dermatologic findings include pruritus. Classic mnemonic: “stones, bones, groans, thrones, and psychiatric overtones,” where “thrones” refers to polyuria.
Pediatric considerations Failure to thrive, delayed development, and potential intellectual impairment.
Physical exam Neurologic findings include irritability, lethargy, hyporeflexia, and coma. Cardiovascular findings include hypotension from volume depletion or hypertension, sinus bradycardia, and rarely cardiac arrest. Renal signs reflect dehydration. Dermatologic findings include band keratopathy and ectopic calcifications. Pediatric findings may include characteristic facies (pug nose, broad nasal bridge, cupid’s-bow upper lip) and hypotonia.
Essential workup Measure total and ionized calcium and albumin. Normal total calcium is <10.5 mg/dL. Corrected calcium (mg/dL) = measured calcium + 0.8 × (4.0 − albumin [g/dL]). Obtain electrolytes, BUN/creatinine, and glucose. ECG may show shortened QT interval, PR prolongation, QRS widening, sinus bradycardia, conduction blocks, digoxin sensitivity, and rarely Osborn J-waves.
Diagnosis tests and interpretation
Laboratory Assess phosphate, protein, urinalysis, and parathyroid hormone (PTH). Elevated or high-normal PTH suggests primary hyperparathyroidism; PTH <20 pg/mL warrants evaluation for PTH-related peptide and vitamin D metabolites. Elevated 25-hydroxyvitamin D suggests exogenous intake; elevated 1,25-dihydroxyvitamin D suggests lymphoma or sarcoidosis. Check digoxin levels if applicable and thyroid studies if indicated.
Imaging CT head for altered mental status and chest imaging with malignancy workup if no clear cause.
Diagnostic procedures Parathyroidectomy is indicated for symptomatic or severe primary hyperparathyroidism and may be urgent.
Differential diagnosis Primary hyperparathyroidism (most common outpatient cause; adenoma most frequent) typically causes mild chronic elevations. Malignancy is the most common inpatient cause, often with rapid onset, higher calcium levels, and greater symptom burden, commonly due to PTH-related peptide or osteolytic disease (e.g., breast, lung, kidney, head and neck, multiple myeloma, lymphoma). Miscellaneous causes include granulomatous disease, excess calcium or vitamin D intake, thiazides, familial hypocalciuric hypercalcemia, vitamin A toxicity, milk-alkali syndrome, lithium therapy, renal transplantation, hyperthyroidism, and acute tubular necrosis.
Pediatric considerations Primary hyperparathyroidism is less common; consider infantile hypercalcemia, immobilization hypercalcemia in adolescents, and vitamin D sensitivity.
Treatment
Prehospital Routine stabilization.
Initial stabilization/therapy ABCs, IV access, oxygen, cardiac monitoring. Administer 0.9% saline (1 L bolus or 20 mL/kg) for hypotension or severe dehydration. Address altered mental status with glucose assessment and supportive measures.
Emergency department management Treat immediately if corrected calcium >14 mg/dL or if symptomatic. Mild, asymptomatic cases do not require emergency therapy. Volume repletion with isotonic saline at 200–300 mL/hr targeting urine output 100–150 mL/hr; total 2–5 L/day may be required with close monitoring for overload. Correct electrolyte abnormalities. Renal elimination with loop diuretics (furosemide) only after adequate volume expansion; avoid thiazides. Dialysis may be required in renal failure. Inhibit bone resorption with bisphosphonates (first-line) and calcitonin for rapid but modest effect. Consider hydrocortisone for vitamin D–mediated or granulomatous causes. Encourage ambulation when appropriate. Treat the underlying cause and discontinue offending agents.
Medication First line Calcitonin 4 IU/kg IM/SC q12h; pamidronate 60–90 mg IV over 2–24 hr; etidronate 7.5 mg/kg IV daily for 3–7 days; furosemide 10–40 mg IV q6–8h (pediatrics 1–2 mg/kg). Second line Gallium nitrate 200 mg/m²/day IV ×5 days; hydrocortisone 200–400 mg/day IV for 3–5 days; plicamycin 25 μg/kg/day IV.
Pediatric considerations Loop diuretics are rarely needed and may worsen renal function; bisphosphonates appear safe but data are limited.
Follow-up and disposition
Admission criteria Corrected calcium >13 mg/dL, symptoms attributable to hypercalcemia, ECG changes, or need for monitored care; ICU for levels >14 mg/dL or severe manifestations.
Discharge criteria Corrected calcium <13 mg/dL with no symptoms.
Issues for referral Arrange prompt evaluation to determine etiology and long-term management; consider endocrinology consultation.
Follow-up recommendations Maintain hydration and monitor for mental status changes.
Key points Base treatment decisions on symptoms and corrected calcium levels. All patients with calcium >14 mg/dL require treatment regardless of symptoms. Monitor ECG closely and balance aggressive hydration against the risk of fluid overload.
Basics
Description Hypercalcemia severity depends on the absolute calcium level and the rate of rise. It is detected in approximately 0.1–1% of routine screenings. Most cases are mild (<12 mg/dL) and asymptomatic. Hypercalcemic crisis, typically >14 mg/dL, causes severe and potentially life-threatening manifestations. Circulating calcium exists as ionized (45%, the only physiologically active form), protein-bound (40%, mainly albumin), and complexed to anions (15%).
Etiology The most common causes are primary hyperparathyroidism and malignancy, followed by miscellaneous conditions.
Diagnosis
Signs and symptoms Neurologic features include headache, fatigue, lethargy, weakness, impaired concentration, confusion, depression, paranoia, stupor, or coma. Renal manifestations include polyuria, polydipsia, dehydration, oliguria in renal failure, nephrolithiasis, nephrocalcinosis, and interstitial nephritis. Gastrointestinal symptoms include anorexia, nausea, vomiting, abdominal pain, constipation, peptic ulcer disease, and pancreatitis. Dermatologic findings include pruritus. Classic mnemonic: “stones, bones, groans, thrones, and psychiatric overtones,” where “thrones” refers to polyuria.
Pediatric considerations Failure to thrive, delayed development, and potential intellectual impairment.
Physical exam Neurologic findings include irritability, lethargy, hyporeflexia, and coma. Cardiovascular findings include hypotension from volume depletion or hypertension, sinus bradycardia, and rarely cardiac arrest. Renal signs reflect dehydration. Dermatologic findings include band keratopathy and ectopic calcifications. Pediatric findings may include characteristic facies (pug nose, broad nasal bridge, cupid’s-bow upper lip) and hypotonia.
Essential workup Measure total and ionized calcium and albumin. Normal total calcium is <10.5 mg/dL. Corrected calcium (mg/dL) = measured calcium + 0.8 × (4.0 − albumin [g/dL]). Obtain electrolytes, BUN/creatinine, and glucose. ECG may show shortened QT interval, PR prolongation, QRS widening, sinus bradycardia, conduction blocks, digoxin sensitivity, and rarely Osborn J-waves.
Diagnosis tests and interpretation
Laboratory Assess phosphate, protein, urinalysis, and parathyroid hormone (PTH). Elevated or high-normal PTH suggests primary hyperparathyroidism; PTH <20 pg/mL warrants evaluation for PTH-related peptide and vitamin D metabolites. Elevated 25-hydroxyvitamin D suggests exogenous intake; elevated 1,25-dihydroxyvitamin D suggests lymphoma or sarcoidosis. Check digoxin levels if applicable and thyroid studies if indicated.
Imaging CT head for altered mental status and chest imaging with malignancy workup if no clear cause.
Diagnostic procedures Parathyroidectomy is indicated for symptomatic or severe primary hyperparathyroidism and may be urgent.
Differential diagnosis Primary hyperparathyroidism (most common outpatient cause; adenoma most frequent) typically causes mild chronic elevations. Malignancy is the most common inpatient cause, often with rapid onset, higher calcium levels, and greater symptom burden, commonly due to PTH-related peptide or osteolytic disease (e.g., breast, lung, kidney, head and neck, multiple myeloma, lymphoma). Miscellaneous causes include granulomatous disease, excess calcium or vitamin D intake, thiazides, familial hypocalciuric hypercalcemia, vitamin A toxicity, milk-alkali syndrome, lithium therapy, renal transplantation, hyperthyroidism, and acute tubular necrosis.
Pediatric considerations Primary hyperparathyroidism is less common; consider infantile hypercalcemia, immobilization hypercalcemia in adolescents, and vitamin D sensitivity.
Treatment
Prehospital Routine stabilization.
Initial stabilization/therapy ABCs, IV access, oxygen, cardiac monitoring. Administer 0.9% saline (1 L bolus or 20 mL/kg) for hypotension or severe dehydration. Address altered mental status with glucose assessment and supportive measures.
Emergency department management Treat immediately if corrected calcium >14 mg/dL or if symptomatic. Mild, asymptomatic cases do not require emergency therapy. Volume repletion with isotonic saline at 200–300 mL/hr targeting urine output 100–150 mL/hr; total 2–5 L/day may be required with close monitoring for overload. Correct electrolyte abnormalities. Renal elimination with loop diuretics (furosemide) only after adequate volume expansion; avoid thiazides. Dialysis may be required in renal failure. Inhibit bone resorption with bisphosphonates (first-line) and calcitonin for rapid but modest effect. Consider hydrocortisone for vitamin D–mediated or granulomatous causes. Encourage ambulation when appropriate. Treat the underlying cause and discontinue offending agents.
Medication First line Calcitonin 4 IU/kg IM/SC q12h; pamidronate 60–90 mg IV over 2–24 hr; etidronate 7.5 mg/kg IV daily for 3–7 days; furosemide 10–40 mg IV q6–8h (pediatrics 1–2 mg/kg). Second line Gallium nitrate 200 mg/m²/day IV ×5 days; hydrocortisone 200–400 mg/day IV for 3–5 days; plicamycin 25 μg/kg/day IV.
Pediatric considerations Loop diuretics are rarely needed and may worsen renal function; bisphosphonates appear safe but data are limited.
Follow-up and disposition
Admission criteria Corrected calcium >13 mg/dL, symptoms attributable to hypercalcemia, ECG changes, or need for monitored care; ICU for levels >14 mg/dL or severe manifestations.
Discharge criteria Corrected calcium <13 mg/dL with no symptoms.
Issues for referral Arrange prompt evaluation to determine etiology and long-term management; consider endocrinology consultation.
Follow-up recommendations Maintain hydration and monitor for mental status changes.
Key points Base treatment decisions on symptoms and corrected calcium levels. All patients with calcium >14 mg/dL require treatment regardless of symptoms. Monitor ECG closely and balance aggressive hydration against the risk of fluid overload.


- Published on
Emergency And Acute Medicine-Hyperbaric Oxygen Therapy
Basics
Description Hyperbaric oxygen therapy (HBOT) involves administration of 100% oxygen at pressures greater than 1 atmosphere (typically 2–3 atm). It increases oxygen delivery at the cellular level; at 3 atm, dissolved oxygen alone can support life without hemoglobin. HBOT also reduces the size of intravascular gas bubbles, making it effective for air embolism and decompression sickness. Two chamber types are used. Monoplace chambers accommodate a single supine patient, are pressurized with 100% oxygen, and monitored externally. Multiplace chambers treat multiple patients simultaneously, allow attendants inside, use air pressurization with oxygen delivered via mask, hood, or endotracheal tube, and permit transfer of equipment through airlocks.
Diagnosis
Indications Primary emergency indications include arterial gas embolism, decompression sickness, and carbon monoxide poisoning. Other indications include clostridial myonecrosis, necrotizing fasciitis, refractory osteomyelitis, chronic nonhealing wounds, radiation-induced tissue injury, crush injuries, thermal burns, and compromised skin grafts or flaps.
Alert In emergency medicine, focus should be on arterial gas embolism, decompression sickness, and carbon monoxide toxicity.
Essential workup Determine whether the clinical condition meets criteria for HBOT. Perform a thorough physical examination to establish a pretreatment baseline and identify contraindications. Absolute contraindication is untreated pneumothorax due to risk of tension pneumothorax. Relative contraindications include cardiovascular instability; unstable patients cannot be treated in monoplace chambers and may only be treated in multiplace chambers if benefit outweighs risk.
Diagnosis tests and interpretation
Laboratory Arterial blood gas to assess hypoxia when clinically indicated.
Imaging Chest radiograph to evaluate for occult pneumothorax prior to therapy.
Treatment
Initial stabilization/therapy Manage airway, breathing, and circulation. Establish IV access, administer 100% oxygen, and apply cardiac monitoring when appropriate.
Emergency department management Confirm indication for HBOT. Fill all balloon-containing devices (e.g., Foley catheters, endotracheal tube cuffs) with fluid to prevent rupture during pressurization. Pretreat patients with sinus congestion using decongestants. Place myringotomy tubes in obtunded or mechanically ventilated patients and in those with middle ear pathology.
Alert Complications include sinus or ear pain, barotrauma (ruptured tympanic membranes, tension pneumothorax), oxygen-toxicity–induced seizures, decompression sickness from rapid decompression, and limited access to unstable patients in monoplace chambers.
Follow-up and disposition
Admission criteria Arterial gas embolism, decompression sickness, and significant carbon monoxide toxicity.
Discharge criteria Stable patients with resolved symptoms after treatment.
Issues for referral Transfer may be required to a facility with hyperbaric capability; risks and benefits must be weighed carefully in unstable patients. The Divers Alert Network provides 24-hour consultation for dive-related injuries (919-684-9111).
Follow-up recommendations Arrange hyperbaric follow-up for repeat recompression therapy if indicated.
Key points Always exclude occult pneumothorax before therapy. Fill balloon-containing devices with fluid prior to pressurization. Emergency use of HBOT is most critical for gas embolism, decompression sickness, and carbon monoxide poisoning.
Basics
Description Hyperbaric oxygen therapy (HBOT) involves administration of 100% oxygen at pressures greater than 1 atmosphere (typically 2–3 atm). It increases oxygen delivery at the cellular level; at 3 atm, dissolved oxygen alone can support life without hemoglobin. HBOT also reduces the size of intravascular gas bubbles, making it effective for air embolism and decompression sickness. Two chamber types are used. Monoplace chambers accommodate a single supine patient, are pressurized with 100% oxygen, and monitored externally. Multiplace chambers treat multiple patients simultaneously, allow attendants inside, use air pressurization with oxygen delivered via mask, hood, or endotracheal tube, and permit transfer of equipment through airlocks.
Diagnosis
Indications Primary emergency indications include arterial gas embolism, decompression sickness, and carbon monoxide poisoning. Other indications include clostridial myonecrosis, necrotizing fasciitis, refractory osteomyelitis, chronic nonhealing wounds, radiation-induced tissue injury, crush injuries, thermal burns, and compromised skin grafts or flaps.
Alert In emergency medicine, focus should be on arterial gas embolism, decompression sickness, and carbon monoxide toxicity.
Essential workup Determine whether the clinical condition meets criteria for HBOT. Perform a thorough physical examination to establish a pretreatment baseline and identify contraindications. Absolute contraindication is untreated pneumothorax due to risk of tension pneumothorax. Relative contraindications include cardiovascular instability; unstable patients cannot be treated in monoplace chambers and may only be treated in multiplace chambers if benefit outweighs risk.
Diagnosis tests and interpretation
Laboratory Arterial blood gas to assess hypoxia when clinically indicated.
Imaging Chest radiograph to evaluate for occult pneumothorax prior to therapy.
Treatment
Initial stabilization/therapy Manage airway, breathing, and circulation. Establish IV access, administer 100% oxygen, and apply cardiac monitoring when appropriate.
Emergency department management Confirm indication for HBOT. Fill all balloon-containing devices (e.g., Foley catheters, endotracheal tube cuffs) with fluid to prevent rupture during pressurization. Pretreat patients with sinus congestion using decongestants. Place myringotomy tubes in obtunded or mechanically ventilated patients and in those with middle ear pathology.
Alert Complications include sinus or ear pain, barotrauma (ruptured tympanic membranes, tension pneumothorax), oxygen-toxicity–induced seizures, decompression sickness from rapid decompression, and limited access to unstable patients in monoplace chambers.
Follow-up and disposition
Admission criteria Arterial gas embolism, decompression sickness, and significant carbon monoxide toxicity.
Discharge criteria Stable patients with resolved symptoms after treatment.
Issues for referral Transfer may be required to a facility with hyperbaric capability; risks and benefits must be weighed carefully in unstable patients. The Divers Alert Network provides 24-hour consultation for dive-related injuries (919-684-9111).
Follow-up recommendations Arrange hyperbaric follow-up for repeat recompression therapy if indicated.
Key points Always exclude occult pneumothorax before therapy. Fill balloon-containing devices with fluid prior to pressurization. Emergency use of HBOT is most critical for gas embolism, decompression sickness, and carbon monoxide poisoning.
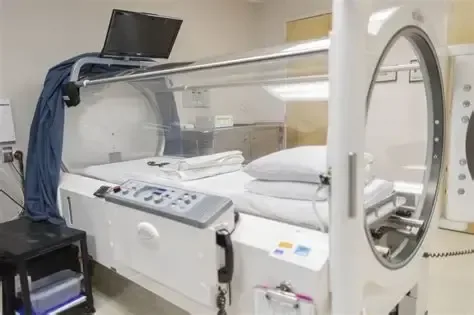
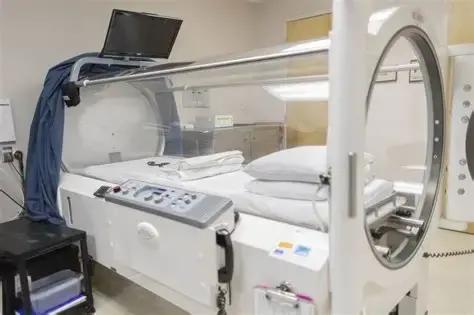
- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocephalus
Basics
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
Basics
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
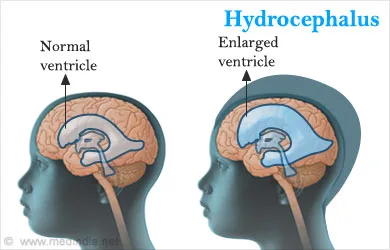
- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocarbon Poisoning
Basics
Description The most serious complication of hydrocarbon exposure is aspiration, primarily affecting the respiratory and central nervous systems. Toxicity is influenced by physical properties. Viscosity: lower viscosity increases aspiration risk. Volatility: highly volatile substances displace alveolar oxygen, leading to hypoxia. Surface tension: low surface tension facilitates spread from the oropharynx into the trachea, increasing aspiration risk (e.g., mineral oil, seal oil). Volatile-substance abuse commonly involves solvents such as typewriter correction fluid, adhesives, gasoline, and lighter fluid. Methods include sniffing (direct inhalation), huffing (from a soaked rag), and bagging (from a bag). Major hydrocarbon classes include aliphatics (kerosene, mineral oil, gasoline, solvents, paint thinners) causing pulmonary toxicity via aspiration and asphyxiation from methane or butane; halogenated hydrocarbons (carbon tetrachloride, trichloroethane) used industrially, well absorbed, and associated with hepatic and renal failure; aromatic or cyclic hydrocarbons (toluene, xylene) that are highly volatile and systemically absorbed, with fatal benzene ingestion reported at ~15 mL; and terpenes or wood distillates (turpentine, pine oil) causing significant gastrointestinal absorption and CNS depression.
Etiology Accidental exposure is most common in young children, while inhalant abuse and intentional self-harm are more frequent in adolescents and adults.
Diagnosis
Signs and symptoms Patients may be asymptomatic initially and often have a hydrocarbon odor on the breath. Early effects include euphoria and disinhibition; later effects include dysphoria, ataxia, confusion, and hallucinations. Sudden sniffing death can occur in volatile-substance abusers due to malignant dysrhythmias from myocardial sensitization. Pulmonary manifestations range from mild respiratory distress to cyanosis and aspiration pneumonitis. CNS effects include intoxication, slurred speech, lethargy, and coma. Gastrointestinal findings include mucosal irritation, gastritis, and diarrhea. Cardiac effects include tachycardia and dysrhythmias. Dermal findings include erythema, maculopapular or vesicular eruptions, defatting dermatitis, and “huffer face” rash with chronic exposure.
History Assess route, substance, amount, timing, intent, possible coingestions, symptoms, and any prehospital interventions.
Physical exam Evaluate airway protection in patients with vomiting or decreased consciousness. Respiratory symptoms usually appear within 30 minutes but may be delayed. Monitor for hypoxia, hypotension, and dysrhythmias. Early fever suggests chemical pneumonitis, whereas fever after 48 hours suggests secondary infection.
Essential workup Identify the exact product, manufacturer, ingredients, exposure type, and estimated quantity; review MSDS when applicable.
Diagnosis tests and interpretation
Laboratory Obtain ECG in volatile-substance abusers. Use pulse oximetry and ABG if abnormal. Check electrolytes, BUN, creatinine, glucose, and liver function tests for halogenated or aromatic exposures; metabolic acidosis and hypokalemia may be present. Measure carboxyhemoglobin for methylene chloride exposure.
Imaging Chest radiograph abnormalities may appear from 20 minutes to 24 hours (typically by 6 hours) and include increased bronchovascular markings with bibasilar or perihilar infiltrates. Lobar consolidation is uncommon; pneumothorax, pneumomediastinum, pleural effusion, and pneumatoceles are rare. Repeat imaging if respiratory status worsens.
Differential diagnosis Caustic ingestion, pesticide poisoning, toxic alcohol ingestion, assessment of accidental versus intentional exposure (psychiatric evaluation), and possible child neglect.
Treatment
Prehospital Remove contaminated clothing and decontaminate exposed skin and hair. Do not induce emesis; ipecac is contraindicated. Keep volatile-substance abusers calm and minimize agitation. Selected asymptomatic patients with known products and reliable observation may be managed at home.
Initial stabilization Follow ABCs, establish IV access with fluids if needed, administer oxygen, monitor cardiac rhythm, and give naloxone, thiamine, and dextrose for altered mental status as indicated.
Emergency department management Provide supportive care. Treat bronchospasm with oxygen and nebulized albuterol; intubate and ventilate for respiratory failure. Steroids are not recommended. Avoid epinephrine in volatile-substance abusers due to dysrhythmia risk. Alert Gastric decontamination is generally not indicated because aspiration risk outweighs benefit. Avoid if spontaneous emesis occurred. Consider limited gastric aspiration only for select CHAMP ingestions (camphor, halogenated hydrocarbons, aromatic hydrocarbons, metals, pesticides) within 60 minutes, with airway protection if needed. Activated charcoal and cathartics are not recommended.
Medication Albuterol 2.5–5 mg nebulized (pediatrics 0.15–0.3 mg/kg). Dextrose D50W 25 g IV (pediatrics D25W 2–4 mL/kg). Naloxone 2 mg IV or IM (pediatrics 0.1 mg/kg). Thiamine 100 mg IV or IM (pediatrics 50 mg).
Follow-up and disposition
Admission criteria Symptomatic patients or those at risk for delayed organ toxicity.
Discharge criteria Observe for at least 6 hours; discharge asymptomatic patients with normal pulse oximetry and chest radiograph, or those asymptomatic with abnormal imaging but normal oxygenation if reliable follow-up is ensured. Observe volatile-substance abusers until mental status normalizes.
Follow-up recommendations Reassess within 24 hours for patients who remain asymptomatic after observation. Repeat chest radiograph in 24 hours for asymptomatic patients with initial abnormalities.
Key points Aspiration is the dominant hazard in hydrocarbon exposure, with risk rising as viscosity and surface tension decrease and volatility increases. Prompt external decontamination is essential. Gastric decontamination and induced emesis are rarely appropriate. All patients should be observed for at least 6 hours, with hospital admission for those who are symptomatic or at risk for delayed toxicity.
Basics
Description The most serious complication of hydrocarbon exposure is aspiration, primarily affecting the respiratory and central nervous systems. Toxicity is influenced by physical properties. Viscosity: lower viscosity increases aspiration risk. Volatility: highly volatile substances displace alveolar oxygen, leading to hypoxia. Surface tension: low surface tension facilitates spread from the oropharynx into the trachea, increasing aspiration risk (e.g., mineral oil, seal oil). Volatile-substance abuse commonly involves solvents such as typewriter correction fluid, adhesives, gasoline, and lighter fluid. Methods include sniffing (direct inhalation), huffing (from a soaked rag), and bagging (from a bag). Major hydrocarbon classes include aliphatics (kerosene, mineral oil, gasoline, solvents, paint thinners) causing pulmonary toxicity via aspiration and asphyxiation from methane or butane; halogenated hydrocarbons (carbon tetrachloride, trichloroethane) used industrially, well absorbed, and associated with hepatic and renal failure; aromatic or cyclic hydrocarbons (toluene, xylene) that are highly volatile and systemically absorbed, with fatal benzene ingestion reported at ~15 mL; and terpenes or wood distillates (turpentine, pine oil) causing significant gastrointestinal absorption and CNS depression.
Etiology Accidental exposure is most common in young children, while inhalant abuse and intentional self-harm are more frequent in adolescents and adults.
Diagnosis
Signs and symptoms Patients may be asymptomatic initially and often have a hydrocarbon odor on the breath. Early effects include euphoria and disinhibition; later effects include dysphoria, ataxia, confusion, and hallucinations. Sudden sniffing death can occur in volatile-substance abusers due to malignant dysrhythmias from myocardial sensitization. Pulmonary manifestations range from mild respiratory distress to cyanosis and aspiration pneumonitis. CNS effects include intoxication, slurred speech, lethargy, and coma. Gastrointestinal findings include mucosal irritation, gastritis, and diarrhea. Cardiac effects include tachycardia and dysrhythmias. Dermal findings include erythema, maculopapular or vesicular eruptions, defatting dermatitis, and “huffer face” rash with chronic exposure.
History Assess route, substance, amount, timing, intent, possible coingestions, symptoms, and any prehospital interventions.
Physical exam Evaluate airway protection in patients with vomiting or decreased consciousness. Respiratory symptoms usually appear within 30 minutes but may be delayed. Monitor for hypoxia, hypotension, and dysrhythmias. Early fever suggests chemical pneumonitis, whereas fever after 48 hours suggests secondary infection.
Essential workup Identify the exact product, manufacturer, ingredients, exposure type, and estimated quantity; review MSDS when applicable.
Diagnosis tests and interpretation
Laboratory Obtain ECG in volatile-substance abusers. Use pulse oximetry and ABG if abnormal. Check electrolytes, BUN, creatinine, glucose, and liver function tests for halogenated or aromatic exposures; metabolic acidosis and hypokalemia may be present. Measure carboxyhemoglobin for methylene chloride exposure.
Imaging Chest radiograph abnormalities may appear from 20 minutes to 24 hours (typically by 6 hours) and include increased bronchovascular markings with bibasilar or perihilar infiltrates. Lobar consolidation is uncommon; pneumothorax, pneumomediastinum, pleural effusion, and pneumatoceles are rare. Repeat imaging if respiratory status worsens.
Differential diagnosis Caustic ingestion, pesticide poisoning, toxic alcohol ingestion, assessment of accidental versus intentional exposure (psychiatric evaluation), and possible child neglect.
Treatment
Prehospital Remove contaminated clothing and decontaminate exposed skin and hair. Do not induce emesis; ipecac is contraindicated. Keep volatile-substance abusers calm and minimize agitation. Selected asymptomatic patients with known products and reliable observation may be managed at home.
Initial stabilization Follow ABCs, establish IV access with fluids if needed, administer oxygen, monitor cardiac rhythm, and give naloxone, thiamine, and dextrose for altered mental status as indicated.
Emergency department management Provide supportive care. Treat bronchospasm with oxygen and nebulized albuterol; intubate and ventilate for respiratory failure. Steroids are not recommended. Avoid epinephrine in volatile-substance abusers due to dysrhythmia risk. Alert Gastric decontamination is generally not indicated because aspiration risk outweighs benefit. Avoid if spontaneous emesis occurred. Consider limited gastric aspiration only for select CHAMP ingestions (camphor, halogenated hydrocarbons, aromatic hydrocarbons, metals, pesticides) within 60 minutes, with airway protection if needed. Activated charcoal and cathartics are not recommended.
Medication Albuterol 2.5–5 mg nebulized (pediatrics 0.15–0.3 mg/kg). Dextrose D50W 25 g IV (pediatrics D25W 2–4 mL/kg). Naloxone 2 mg IV or IM (pediatrics 0.1 mg/kg). Thiamine 100 mg IV or IM (pediatrics 50 mg).
Follow-up and disposition
Admission criteria Symptomatic patients or those at risk for delayed organ toxicity.
Discharge criteria Observe for at least 6 hours; discharge asymptomatic patients with normal pulse oximetry and chest radiograph, or those asymptomatic with abnormal imaging but normal oxygenation if reliable follow-up is ensured. Observe volatile-substance abusers until mental status normalizes.
Follow-up recommendations Reassess within 24 hours for patients who remain asymptomatic after observation. Repeat chest radiograph in 24 hours for asymptomatic patients with initial abnormalities.
Key points Aspiration is the dominant hazard in hydrocarbon exposure, with risk rising as viscosity and surface tension decrease and volatility increases. Prompt external decontamination is essential. Gastric decontamination and induced emesis are rarely appropriate. All patients should be observed for at least 6 hours, with hospital admission for those who are symptomatic or at risk for delayed toxicity.
- Published on
Emergency And Acute Medicine – Horner’s Syndrome
Basics
Condition Summary
Horner’s syndrome results from unilateral interruption of the sympathetic pathway to the eye and face. Loss of sympathetic innervation produces a characteristic triad. Relaxation of the upper and lower eyelid retractors leads to ptosis (drooping of the eyelid). Disruption of pupillary dilator fibers causes miosis, with unopposed pupillary constriction. Loss of sympathetic input to facial sweat glands results in anhidrosis on the affected side.
Etiology And Causes
In approximately 40% of cases, no cause is identified. Neoplastic disease, particularly lung tumors or metastases to cervical lymph nodes, may interrupt preganglionic sympathetic fibers between the thoracic sympathetic trunk and the superior cervical ganglion.
Trauma, including penetrating neck injuries, may directly damage sympathetic fibers. Pneumothorax, especially tension pneumothorax, can cause traction on the sympathetic chain due to mediastinal shift.
Infiltration or infection of cervical lymph nodes, such as from sarcoidosis or tuberculosis, may also disrupt the pathway.
Vascular etiologies include migraine or cluster headaches and carotid artery dissection. Lateral medullary (Wallenberg) infarction may present with Horner’s syndrome accompanied by vertigo and ataxia, which can overshadow ocular findings. Cavernous sinus thrombosis may produce partial Horner-like features along with headache, eye pain, ocular motor palsies, chemosis, and proptosis.
Pediatric Considerations
Congenital or hereditary Horner’s syndrome may present with heterochromia iridis, characterized by a lighter (often blue) iris on the affected side and a darker iris on the unaffected side. Birth trauma can injure the sympathetic chain. New-onset Horner’s syndrome in a child warrants evaluation for an underlying tumor, particularly neuroblastoma.
Diagnosis
Clinical Features
Horner’s syndrome is defined by a classic triad: mild ptosis on the affected side, miosis with pupillary asymmetry of at least 1 mm, and ipsilateral facial anhidrosis. The clinical importance lies in its association with potentially serious underlying conditions rather than the ocular findings alone.
History
History should focus on conditions that predispose to Horner’s syndrome or its causes, including malignancy, vascular disease, and trauma. Minor trauma may precede carotid artery dissection. Cardiovascular risk factors and relevant exposures should be assessed. The presence of pain, particularly neck or facial pain, raises concern for carotid dissection.
Alert
Acute onset Horner’s syndrome associated with neck or facial pain should be presumed to be due to carotid artery dissection until proven otherwise, as approximately half of internal carotid dissections present with a painful Horner’s syndrome.
Physical Examination
A focused neurologic examination is essential to confirm Horner’s syndrome and identify additional neurologic deficits. The general examination should look for signs of associated conditions such as tumors, trauma, or pulmonary pathology.
Essential Evaluation
Assessment includes a thorough history and neurologic examination. A chest radiograph is recommended to screen for apical lung tumors or pneumothorax.
Diagnostic Studies And Interpretation
Provocative Testing
Pharmacologic confirmation can be achieved with ocular cocaine testing. One drop of 5% cocaine solution (2.5% in children) is instilled into each eye. Failure of the affected pupil to dilate compared with the unaffected pupil, resulting in increased anisocoria after approximately one hour, confirms a sympathetic denervation lesion.
Laboratory Testing
Laboratory studies are not useful for diagnosing Horner’s syndrome itself but may be indicated to evaluate suspected underlying conditions.
Imaging
Chest radiography is often indicated due to the association between Horner’s syndrome and intrathoracic pathology. CT or MRI of the head, neck, or chest should be guided by clinical findings.
When carotid artery dissection is suspected, CT angiography or MR angiography of the head and neck is appropriate, with the lesion expected on the same side as the Horner’s syndrome. If stroke is suspected, at minimum a noncontrast CT of the brain is required to exclude hemorrhage. Patients within the thrombolysis window should undergo emergent imaging per local stroke protocols.
Diagnostic Procedures
Ocular tonometry should be performed if acute glaucoma is a consideration.
Differential Diagnosis
Elevated intracranial pressure, typically associated with headache and altered consciousness
Physiologic anisocoria (pseudo–Horner’s syndrome), which is common and yields a negative cocaine test
Topical medications or exposures causing miosis
Migraine or cluster headache
Glaucoma, inflammatory eye disease, or ocular trauma
Management
Prehospital Considerations
Horner’s syndrome itself is benign, but associated life-threatening conditions must be rapidly identified. Increased intracranial pressure or tension pneumothorax requires immediate intervention. Patients with suspected acute stroke should be transported to a designated stroke center when feasible.
Initial Stabilization
If elevated intracranial pressure is suspected, initiate airway protection and intracranial pressure–lowering measures, including osmotic therapy. Tension pneumothorax requires immediate needle decompression followed by chest tube placement.
Emergency Department Care
Horner’s syndrome does not require direct treatment in the ED. Management is directed at identifying and treating the underlying cause.
Medications
Cocaine ophthalmic solution (5% in adults, 2.5% in children) is used diagnostically, with one drop placed in each eye.
Follow-Up And Disposition
Admission Criteria
Admission is not required for isolated Horner’s syndrome but may be necessary for associated conditions such as stroke, carotid dissection, malignancy, or infection.
Discharge Criteria
Stable patients with isolated Horner’s syndrome may be discharged with appropriate outpatient follow-up once emergent causes, particularly carotid dissection and stroke, have been reasonably excluded.
Follow-Up Recommendations
Ongoing evaluation often requires coordination with neurology and ophthalmology to identify the underlying etiology and guide further management.
Key Points And Common Pitfalls
The primary importance of Horner’s syndrome lies in recognizing its potential underlying causes. Failure to evaluate for serious etiologies such as carotid artery dissection, stroke, or malignancy is a critical pitfall.
Basics
Condition Summary
Horner’s syndrome results from unilateral interruption of the sympathetic pathway to the eye and face. Loss of sympathetic innervation produces a characteristic triad. Relaxation of the upper and lower eyelid retractors leads to ptosis (drooping of the eyelid). Disruption of pupillary dilator fibers causes miosis, with unopposed pupillary constriction. Loss of sympathetic input to facial sweat glands results in anhidrosis on the affected side.
Etiology And Causes
In approximately 40% of cases, no cause is identified. Neoplastic disease, particularly lung tumors or metastases to cervical lymph nodes, may interrupt preganglionic sympathetic fibers between the thoracic sympathetic trunk and the superior cervical ganglion.
Trauma, including penetrating neck injuries, may directly damage sympathetic fibers. Pneumothorax, especially tension pneumothorax, can cause traction on the sympathetic chain due to mediastinal shift.
Infiltration or infection of cervical lymph nodes, such as from sarcoidosis or tuberculosis, may also disrupt the pathway.
Vascular etiologies include migraine or cluster headaches and carotid artery dissection. Lateral medullary (Wallenberg) infarction may present with Horner’s syndrome accompanied by vertigo and ataxia, which can overshadow ocular findings. Cavernous sinus thrombosis may produce partial Horner-like features along with headache, eye pain, ocular motor palsies, chemosis, and proptosis.
Pediatric Considerations
Congenital or hereditary Horner’s syndrome may present with heterochromia iridis, characterized by a lighter (often blue) iris on the affected side and a darker iris on the unaffected side. Birth trauma can injure the sympathetic chain. New-onset Horner’s syndrome in a child warrants evaluation for an underlying tumor, particularly neuroblastoma.
Diagnosis
Clinical Features
Horner’s syndrome is defined by a classic triad: mild ptosis on the affected side, miosis with pupillary asymmetry of at least 1 mm, and ipsilateral facial anhidrosis. The clinical importance lies in its association with potentially serious underlying conditions rather than the ocular findings alone.
History
History should focus on conditions that predispose to Horner’s syndrome or its causes, including malignancy, vascular disease, and trauma. Minor trauma may precede carotid artery dissection. Cardiovascular risk factors and relevant exposures should be assessed. The presence of pain, particularly neck or facial pain, raises concern for carotid dissection.
Alert
Acute onset Horner’s syndrome associated with neck or facial pain should be presumed to be due to carotid artery dissection until proven otherwise, as approximately half of internal carotid dissections present with a painful Horner’s syndrome.
Physical Examination
A focused neurologic examination is essential to confirm Horner’s syndrome and identify additional neurologic deficits. The general examination should look for signs of associated conditions such as tumors, trauma, or pulmonary pathology.
Essential Evaluation
Assessment includes a thorough history and neurologic examination. A chest radiograph is recommended to screen for apical lung tumors or pneumothorax.
Diagnostic Studies And Interpretation
Provocative Testing
Pharmacologic confirmation can be achieved with ocular cocaine testing. One drop of 5% cocaine solution (2.5% in children) is instilled into each eye. Failure of the affected pupil to dilate compared with the unaffected pupil, resulting in increased anisocoria after approximately one hour, confirms a sympathetic denervation lesion.
Laboratory Testing
Laboratory studies are not useful for diagnosing Horner’s syndrome itself but may be indicated to evaluate suspected underlying conditions.
Imaging
Chest radiography is often indicated due to the association between Horner’s syndrome and intrathoracic pathology. CT or MRI of the head, neck, or chest should be guided by clinical findings.
When carotid artery dissection is suspected, CT angiography or MR angiography of the head and neck is appropriate, with the lesion expected on the same side as the Horner’s syndrome. If stroke is suspected, at minimum a noncontrast CT of the brain is required to exclude hemorrhage. Patients within the thrombolysis window should undergo emergent imaging per local stroke protocols.
Diagnostic Procedures
Ocular tonometry should be performed if acute glaucoma is a consideration.
Differential Diagnosis
Elevated intracranial pressure, typically associated with headache and altered consciousness
Physiologic anisocoria (pseudo–Horner’s syndrome), which is common and yields a negative cocaine test
Topical medications or exposures causing miosis
Migraine or cluster headache
Glaucoma, inflammatory eye disease, or ocular trauma
Management
Prehospital Considerations
Horner’s syndrome itself is benign, but associated life-threatening conditions must be rapidly identified. Increased intracranial pressure or tension pneumothorax requires immediate intervention. Patients with suspected acute stroke should be transported to a designated stroke center when feasible.
Initial Stabilization
If elevated intracranial pressure is suspected, initiate airway protection and intracranial pressure–lowering measures, including osmotic therapy. Tension pneumothorax requires immediate needle decompression followed by chest tube placement.
Emergency Department Care
Horner’s syndrome does not require direct treatment in the ED. Management is directed at identifying and treating the underlying cause.
Medications
Cocaine ophthalmic solution (5% in adults, 2.5% in children) is used diagnostically, with one drop placed in each eye.
Follow-Up And Disposition
Admission Criteria
Admission is not required for isolated Horner’s syndrome but may be necessary for associated conditions such as stroke, carotid dissection, malignancy, or infection.
Discharge Criteria
Stable patients with isolated Horner’s syndrome may be discharged with appropriate outpatient follow-up once emergent causes, particularly carotid dissection and stroke, have been reasonably excluded.
Follow-Up Recommendations
Ongoing evaluation often requires coordination with neurology and ophthalmology to identify the underlying etiology and guide further management.
Key Points And Common Pitfalls
The primary importance of Horner’s syndrome lies in recognizing its potential underlying causes. Failure to evaluate for serious etiologies such as carotid artery dissection, stroke, or malignancy is a critical pitfall.
- Published on
Emergency And Acute Medicine – Hordeolum And Chalazion
Basics
Clinical Overview
Hordeola and chalazia arise from inflammatory processes involving the eyelid glands along the lash margin. A hordeolum represents an acute obstruction of an eyelid gland that leads to inflammation and often abscess formation. A chalazion is the chronic consequence of retained, thickened glandular secretions, producing a granulomatous inflammatory response.
A hordeolum develops when outflow obstruction affects one or more eyelid glands. Secondary bacterial infection may occur, and progression to a localized abscess or, less commonly, periorbital cellulitis is possible.
A chalazion reflects chronic granulomatous inflammation of a meibomian gland. Blockage of the duct at the eyelid margin may cause glandular contents to leak into surrounding eyelid tissue, triggering a lipogranulomatous reaction. Chalazia are occasionally secondarily infected and may evolve from an incompletely resolved internal hordeolum.
Etiology And Risk Factors
Hordeola may become secondarily infected, most commonly with Staphylococcus species. Predisposing conditions include meibomian gland dysfunction, chronic blepharitis, rosacea, and a history of prior hordeola.
Diagnosis
Clinical Features
A hordeolum typically presents acutely as a red, tender, painful, swollen lesion along the eyelid margin. Lesions are usually solitary but may be multiple or recurrent. Inflammation is well localized, and presentation varies depending on the gland involved.
An external hordeolum (stye) originates from obstruction of superficial sebaceous or sweat glands with ducts between the eyelashes. It appears as an exquisitely tender lesion that often points anteriorly.
An internal hordeolum arises from obstruction of deeper sebaceous glands whose ducts open on the inner eyelid margin. It presents as a painful, palpable mass within the lid, may cause foreign body sensation or visual disturbance, and is often larger and more inflamed than external lesions. It may drain internally toward the conjunctiva or externally through the skin.
Hordeola are localized processes without systemic symptoms but may be complicated by conjunctivitis or periorbital cellulitis.
A chalazion presents as a firm, well-circumscribed, nontender or minimally tender eyelid nodule that is typically long-standing and noninflamed. Symptoms usually relate to its size and location, including cosmetic distortion, obstruction of the visual field, pressure on the globe, or corneal drying or injury from exposure. Chalazia are nonacute and nonemergent unless significant corneal compromise or globe pressure occurs.
History
Hordeolum is characterized by sudden onset of a well-localized, painful eyelid mass without systemic symptoms.
Physical Examination
Findings include focal tenderness and inflammation of an external or internal eyelid gland, with minimal surrounding edema. An abscess may point at the lash line, the palpebral conjunctiva, or externally through the skin.
Essential Evaluation
A complete ophthalmologic assessment should be performed, including slit-lamp examination and corneal evaluation. Patients should be assessed for associated cellulitis or systemic involvement.
For hordeola, identifying the gland of origin is important.
For chalazia, evaluation should focus on whether the lesion causes corneal exposure or injury.
Diagnostic Studies And Interpretation
Laboratory Testing
Cultures of expressed or draining material are rarely useful and typically do not alter management.
Differential Diagnosis
Blepharitis
Dacryocystitis
Dacryoadenitis
Pyogenic granuloma
Sebaceous cell carcinoma
Basal cell carcinoma
Squamous cell carcinoma
Management
Emergency Department Care
For hordeola, treatment focuses on relieving obstruction and preventing abscess formation. Warm compresses applied for 15 minutes, 4–6 times daily, are first-line therapy. Gentle massage of the lesion may help express obstructed material.
In rare severe cases, incision and drainage of an internal hordeolum may be required and is typically performed by an ophthalmologist. When drainage is toward the conjunctiva, a vertical incision is preferred to minimize meibomian gland injury and reduce the risk of corneal scarring. External skin incisions are rarely indicated; if required, a horizontal incision is used. In select severe external hordeola, removal of a single involved eyelash may be helpful.
Chalazia generally require no emergent intervention. Management is typically referral-based, with ophthalmologic options including incision and curettage or intralesional steroid injection. Lubricating eye drops may provide symptomatic relief.
Medications
Ophthalmic lubricating drops may be used as needed for comfort.
Follow-Up And Disposition
Discharge Criteria
Patients may be discharged if there is no evidence of secondary complications such as significant periorbital cellulitis with systemic symptoms.
Referral Considerations
Urgent ophthalmology consultation should be obtained if incision and drainage of an internal hordeolum is considered. Chalazia should be referred for definitive ophthalmologic management.
Follow-Up Recommendations
Ophthalmology follow-up within 1–2 days is recommended to assess response to conservative therapy. Most symptoms resolve completely within 1–2 weeks.
Key Points And Common Pitfalls
Conservative management with warm compresses and gentle massage is the standard of care for hordeola, with most cases resolving without further intervention.
Emergent incision and drainage is rarely necessary and carries risks including corneal injury, fistula formation, and cosmetic complications; ophthalmology consultation is preferred.
Chalazia do not require emergent treatment and are best managed with outpatient referral.
Basics
Clinical Overview
Hordeola and chalazia arise from inflammatory processes involving the eyelid glands along the lash margin. A hordeolum represents an acute obstruction of an eyelid gland that leads to inflammation and often abscess formation. A chalazion is the chronic consequence of retained, thickened glandular secretions, producing a granulomatous inflammatory response.
A hordeolum develops when outflow obstruction affects one or more eyelid glands. Secondary bacterial infection may occur, and progression to a localized abscess or, less commonly, periorbital cellulitis is possible.
A chalazion reflects chronic granulomatous inflammation of a meibomian gland. Blockage of the duct at the eyelid margin may cause glandular contents to leak into surrounding eyelid tissue, triggering a lipogranulomatous reaction. Chalazia are occasionally secondarily infected and may evolve from an incompletely resolved internal hordeolum.
Etiology And Risk Factors
Hordeola may become secondarily infected, most commonly with Staphylococcus species. Predisposing conditions include meibomian gland dysfunction, chronic blepharitis, rosacea, and a history of prior hordeola.
Diagnosis
Clinical Features
A hordeolum typically presents acutely as a red, tender, painful, swollen lesion along the eyelid margin. Lesions are usually solitary but may be multiple or recurrent. Inflammation is well localized, and presentation varies depending on the gland involved.
An external hordeolum (stye) originates from obstruction of superficial sebaceous or sweat glands with ducts between the eyelashes. It appears as an exquisitely tender lesion that often points anteriorly.
An internal hordeolum arises from obstruction of deeper sebaceous glands whose ducts open on the inner eyelid margin. It presents as a painful, palpable mass within the lid, may cause foreign body sensation or visual disturbance, and is often larger and more inflamed than external lesions. It may drain internally toward the conjunctiva or externally through the skin.
Hordeola are localized processes without systemic symptoms but may be complicated by conjunctivitis or periorbital cellulitis.
A chalazion presents as a firm, well-circumscribed, nontender or minimally tender eyelid nodule that is typically long-standing and noninflamed. Symptoms usually relate to its size and location, including cosmetic distortion, obstruction of the visual field, pressure on the globe, or corneal drying or injury from exposure. Chalazia are nonacute and nonemergent unless significant corneal compromise or globe pressure occurs.
History
Hordeolum is characterized by sudden onset of a well-localized, painful eyelid mass without systemic symptoms.
Physical Examination
Findings include focal tenderness and inflammation of an external or internal eyelid gland, with minimal surrounding edema. An abscess may point at the lash line, the palpebral conjunctiva, or externally through the skin.
Essential Evaluation
A complete ophthalmologic assessment should be performed, including slit-lamp examination and corneal evaluation. Patients should be assessed for associated cellulitis or systemic involvement.
For hordeola, identifying the gland of origin is important.
For chalazia, evaluation should focus on whether the lesion causes corneal exposure or injury.
Diagnostic Studies And Interpretation
Laboratory Testing
Cultures of expressed or draining material are rarely useful and typically do not alter management.
Differential Diagnosis
Blepharitis
Dacryocystitis
Dacryoadenitis
Pyogenic granuloma
Sebaceous cell carcinoma
Basal cell carcinoma
Squamous cell carcinoma
Management
Emergency Department Care
For hordeola, treatment focuses on relieving obstruction and preventing abscess formation. Warm compresses applied for 15 minutes, 4–6 times daily, are first-line therapy. Gentle massage of the lesion may help express obstructed material.
In rare severe cases, incision and drainage of an internal hordeolum may be required and is typically performed by an ophthalmologist. When drainage is toward the conjunctiva, a vertical incision is preferred to minimize meibomian gland injury and reduce the risk of corneal scarring. External skin incisions are rarely indicated; if required, a horizontal incision is used. In select severe external hordeola, removal of a single involved eyelash may be helpful.
Chalazia generally require no emergent intervention. Management is typically referral-based, with ophthalmologic options including incision and curettage or intralesional steroid injection. Lubricating eye drops may provide symptomatic relief.
Medications
Ophthalmic lubricating drops may be used as needed for comfort.
Follow-Up And Disposition
Discharge Criteria
Patients may be discharged if there is no evidence of secondary complications such as significant periorbital cellulitis with systemic symptoms.
Referral Considerations
Urgent ophthalmology consultation should be obtained if incision and drainage of an internal hordeolum is considered. Chalazia should be referred for definitive ophthalmologic management.
Follow-Up Recommendations
Ophthalmology follow-up within 1–2 days is recommended to assess response to conservative therapy. Most symptoms resolve completely within 1–2 weeks.
Key Points And Common Pitfalls
Conservative management with warm compresses and gentle massage is the standard of care for hordeola, with most cases resolving without further intervention.
Emergent incision and drainage is rarely necessary and carries risks including corneal injury, fistula formation, and cosmetic complications; ophthalmology consultation is preferred.
Chalazia do not require emergent treatment and are best managed with outpatient referral.