- Published on
Emergency and Acute Medicine-Gillian–Barré Syndrome
Basics Description
Guillain–Barré syndrome (GBS) is a group of peripheral nerve disorders characterized by autoimmune-mediated demyelination and axonal degeneration of peripheral nerves, leading to acute ascending paralysis. The disease involves both humoral and cellular immune mechanisms and is the leading cause of acute flaccid paralysis worldwide since the advent of polio vaccination. It is often triggered by a preceding bacterial or viral infection and has an increasing incidence with advancing age and male gender. The average incidence is approximately 1.1 per 100,000 persons per year. Weakness typically reaches its maximum severity within 2–4 weeks, followed by spontaneous recovery over weeks to months. About 80% of patients achieve full recovery at 1 year, 20% are unable to walk at 6 months, and approximately 5% die from complications such as pulmonary embolism, infection, or cardiac arrhythmias.
The most common subtype is acute inflammatory demyelinating polyradiculoneuropathy (AIDP), accounting for about 90% of cases. Other forms include acute motor axonal neuropathy (AMAN), acute motor sensory axonal neuropathy (AMSAN), acute panautonomic neuropathy, and Miller Fisher syndrome. These variants differ in pathophysiology, clinical features, and recovery patterns.
Etiology
GBS is most commonly postinfectious, with approximately two-thirds of patients reporting an antecedent illness, usually respiratory or gastrointestinal, occurring 1–3 weeks before neurologic symptoms. Different autoantibodies are associated with different subtypes. Campylobacter jejuni is the most common bacterial trigger, while cytomegalovirus is the most frequent viral antecedent. Other associated infections include Epstein–Barr virus, varicella-zoster virus, HIV, and Mycoplasma pneumoniae. A causal relationship with vaccines is not well supported, aside from a slight increased risk noted with the 1976 swine influenza vaccine.
Diagnosis Signs And Symptoms
Patients typically present with rapidly progressive, symmetric, ascending weakness. Sensory symptoms are usually mild or absent, though paresthesias of the fingers or toes may occur. Pain is common, especially involving the pelvis, shoulder girdle, or posterior thighs. Cranial nerve involvement may lead to dysphagia, facial weakness, or ophthalmoplegia. Autonomic dysfunction can manifest as blood pressure instability, cardiac dysrhythmias, ileus, or urinary retention. Respiratory insufficiency occurs in approximately 25% of patients. Progression beyond 8 weeks suggests an alternative diagnosis such as chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).
Diagnosis Tests And Interpretation
Diagnosis is primarily clinical. Laboratory and imaging studies support the diagnosis and help exclude other conditions. Cerebrospinal fluid analysis typically shows albuminocytologic dissociation, with elevated protein and few or no white blood cells, often becoming apparent after 7–10 days. A CSF white blood cell count greater than 10–50 cells/mm³ suggests an alternative diagnosis. Electrolytes may reveal hyponatremia due to SIADH. CT or MRI is used to rule out spinal cord compression. Electrophysiologic studies demonstrate abnormalities consistent with demyelination or axonal injury and are confirmatory.
Differential Diagnosis
The differential diagnosis includes other polyneuropathies, spinal cord disorders, neuromuscular junction diseases, muscle disorders, metabolic abnormalities, and functional neurologic conditions.
Treatment Pre Hospital
Early attention to airway protection is essential due to the risk of rapid respiratory compromise.
Initial Stabilization Therapy
Careful and repeated airway assessment is critical, as progression to respiratory failure can occur quickly.
Ed Treatment Procedures
Approximately 30% of patients require ventilatory support, sometimes within 24–48 hours of symptom onset. Frequent monitoring of respiratory function using forced vital capacity (FVC) or negative inspiratory force (NIF) is recommended. ICU admission is indicated if FVC is less than 20 mL/kg or NIF is less than 30 cm H₂O, with intubation strongly considered if FVC drops below 15 mL/kg. Autonomic instability should be closely monitored. Early neurology consultation is essential.
Medication
Disease-modifying therapy includes plasmapheresis or intravenous immunoglobulin (IVIG), initiated in consultation with neurology. IVIG is typically given at 400 mg/kg/day for 5 days. Pain management may include acetaminophen, NSAIDs, or gabapentin. Corticosteroids are not beneficial and may delay recovery.
Follow-Up Disposition
All patients with suspected or confirmed GBS require hospital admission for close monitoring. ICU admission is necessary for those with respiratory compromise, autonomic dysfunction, or rapidly progressive weakness. Discharge should only be considered after neurologic consultation.
Follow-Up Recommendations
Ongoing follow-up is determined by neurology. Factors associated with poorer outcomes include advanced age, longer time to symptom nadir, need for mechanical ventilation, and preceding diarrheal illness, particularly due to C. jejuni.
Clinical Insights And Common Diagnostic Errors
Frequent assessment of respiratory parameters such as FVC and NIF is essential to anticipate airway compromise. A CSF white blood cell count exceeding 10–50 cells/mm³ should prompt reconsideration of the diagnosis. Common errors include failing to obtain appropriate neuroimaging to exclude alternative causes, delaying neurology consultation, and not admitting or closely observing patients with suspected GBS.
Basics Description
Guillain–Barré syndrome (GBS) is a group of peripheral nerve disorders characterized by autoimmune-mediated demyelination and axonal degeneration of peripheral nerves, leading to acute ascending paralysis. The disease involves both humoral and cellular immune mechanisms and is the leading cause of acute flaccid paralysis worldwide since the advent of polio vaccination. It is often triggered by a preceding bacterial or viral infection and has an increasing incidence with advancing age and male gender. The average incidence is approximately 1.1 per 100,000 persons per year. Weakness typically reaches its maximum severity within 2–4 weeks, followed by spontaneous recovery over weeks to months. About 80% of patients achieve full recovery at 1 year, 20% are unable to walk at 6 months, and approximately 5% die from complications such as pulmonary embolism, infection, or cardiac arrhythmias.
The most common subtype is acute inflammatory demyelinating polyradiculoneuropathy (AIDP), accounting for about 90% of cases. Other forms include acute motor axonal neuropathy (AMAN), acute motor sensory axonal neuropathy (AMSAN), acute panautonomic neuropathy, and Miller Fisher syndrome. These variants differ in pathophysiology, clinical features, and recovery patterns.
Etiology
GBS is most commonly postinfectious, with approximately two-thirds of patients reporting an antecedent illness, usually respiratory or gastrointestinal, occurring 1–3 weeks before neurologic symptoms. Different autoantibodies are associated with different subtypes. Campylobacter jejuni is the most common bacterial trigger, while cytomegalovirus is the most frequent viral antecedent. Other associated infections include Epstein–Barr virus, varicella-zoster virus, HIV, and Mycoplasma pneumoniae. A causal relationship with vaccines is not well supported, aside from a slight increased risk noted with the 1976 swine influenza vaccine.
Diagnosis Signs And Symptoms
Patients typically present with rapidly progressive, symmetric, ascending weakness. Sensory symptoms are usually mild or absent, though paresthesias of the fingers or toes may occur. Pain is common, especially involving the pelvis, shoulder girdle, or posterior thighs. Cranial nerve involvement may lead to dysphagia, facial weakness, or ophthalmoplegia. Autonomic dysfunction can manifest as blood pressure instability, cardiac dysrhythmias, ileus, or urinary retention. Respiratory insufficiency occurs in approximately 25% of patients. Progression beyond 8 weeks suggests an alternative diagnosis such as chronic inflammatory demyelinating polyradiculoneuropathy (CIDP).
Diagnosis Tests And Interpretation
Diagnosis is primarily clinical. Laboratory and imaging studies support the diagnosis and help exclude other conditions. Cerebrospinal fluid analysis typically shows albuminocytologic dissociation, with elevated protein and few or no white blood cells, often becoming apparent after 7–10 days. A CSF white blood cell count greater than 10–50 cells/mm³ suggests an alternative diagnosis. Electrolytes may reveal hyponatremia due to SIADH. CT or MRI is used to rule out spinal cord compression. Electrophysiologic studies demonstrate abnormalities consistent with demyelination or axonal injury and are confirmatory.
Differential Diagnosis
The differential diagnosis includes other polyneuropathies, spinal cord disorders, neuromuscular junction diseases, muscle disorders, metabolic abnormalities, and functional neurologic conditions.
Treatment Pre Hospital
Early attention to airway protection is essential due to the risk of rapid respiratory compromise.
Initial Stabilization Therapy
Careful and repeated airway assessment is critical, as progression to respiratory failure can occur quickly.
Ed Treatment Procedures
Approximately 30% of patients require ventilatory support, sometimes within 24–48 hours of symptom onset. Frequent monitoring of respiratory function using forced vital capacity (FVC) or negative inspiratory force (NIF) is recommended. ICU admission is indicated if FVC is less than 20 mL/kg or NIF is less than 30 cm H₂O, with intubation strongly considered if FVC drops below 15 mL/kg. Autonomic instability should be closely monitored. Early neurology consultation is essential.
Medication
Disease-modifying therapy includes plasmapheresis or intravenous immunoglobulin (IVIG), initiated in consultation with neurology. IVIG is typically given at 400 mg/kg/day for 5 days. Pain management may include acetaminophen, NSAIDs, or gabapentin. Corticosteroids are not beneficial and may delay recovery.
Follow-Up Disposition
All patients with suspected or confirmed GBS require hospital admission for close monitoring. ICU admission is necessary for those with respiratory compromise, autonomic dysfunction, or rapidly progressive weakness. Discharge should only be considered after neurologic consultation.
Follow-Up Recommendations
Ongoing follow-up is determined by neurology. Factors associated with poorer outcomes include advanced age, longer time to symptom nadir, need for mechanical ventilation, and preceding diarrheal illness, particularly due to C. jejuni.
Clinical Insights And Common Diagnostic Errors
Frequent assessment of respiratory parameters such as FVC and NIF is essential to anticipate airway compromise. A CSF white blood cell count exceeding 10–50 cells/mm³ should prompt reconsideration of the diagnosis. Common errors include failing to obtain appropriate neuroimaging to exclude alternative causes, delaying neurology consultation, and not admitting or closely observing patients with suspected GBS.

- Published on
Emergency And Acute Medicine - Granulocytopenia
Basics Description
Granulocytopenia is a significant reduction in circulating granulocytes in peripheral blood. The three granulocyte classes are neutrophils (polymorphonuclear cells and bands), eosinophils, and basophils. Because neutrophils predominate, granulocytopenia is commonly used interchangeably with neutropenia. Granulocytes are essential components of innate immunity.
Clinical risk is best assessed by the absolute neutrophil count (ANC), calculated as WBC × (% PMNs + bands). Modern analyzers typically report ANC automatically. Neutropenia is defined as ANC <1,500 cells />m³: mild (1,000–1,500), moderate (500–1,000), severe (<500). agranulocytosis refers to anc <100. patients with rapidly falling counts are at higher infection risk than those low but recovering counts. myelodysplastic syndromes may be functionally granulocytopenic due impaired neutrophil function.< />pan>
Four mechanisms lead to granulocytopenia: decreased production, ineffective granulopoiesis, margination of neutrophils to the vascular endothelium, and increased peripheral destruction. Untreated febrile neutropenia carries mortality rates up to 50%, closely related to severity, duration, and delay to antibiotic therapy. Approximately 21% of oncology patients with neutropenic fever develop serious complications.
Pediatric considerations include physiologically elevated neonatal ANC during the first days of life and lower infection risk in otherwise healthy children older than 3 months with isolated moderate neutropenia.
Etiology
The most common cause is myelosuppressive chemotherapy or radiation, typically occurring 5–10 days after treatment. Drug-induced granulocytopenia is the second most common cause and usually requires at least 4 weeks of exposure, resolving within 30 days of discontinuation. High-risk drugs include clozapine, sulfasalazine, thioamides, antiplatelet agents, antiepileptics, NSAIDs, methotrexate, cyclophosphamide, colchicine, azathioprine, and ganciclovir.
Infectious causes include bacterial (typhoid, Shigella, brucellosis, tularemia, tuberculosis), parasitic (malaria, kala-azar), rickettsial (ehrlichiosis, RMSF), and viral infections, particularly HIV, hepatitis B, and EBV.
Immune-mediated causes include primary immune neutropenia, autoimmune diseases, thymoma, complement activation, transfusion reactions, alcoholism, nutritional deficiencies (vitamin B12, folate, copper), chronic idiopathic neutropenia, and pure white cell aplasia. Numerous congenital causes exist in pediatric populations.
Diagnosis Signs And Symptoms
Patients may present with fever or subtle signs of bacterial or fungal infection. Symptoms of pancytopenia include fatigue, pallor, petechiae, epistaxis, and spontaneous bleeding. Medication history, prior ANC values, and family history are essential. Patients should be questioned carefully about systemic and localizing symptoms of infection.
Physical examination focuses on identifying infection, including careful oral, pulmonary, abdominal, skin, catheter site, and perirectal assessment. Rectal examination is relatively contraindicated until antibiotics are initiated.
Essential Workup
A complete physical examination with emphasis on oral mucosa, perianal region, skin, lungs, and abdomen is required. Rectal examination may be performed after initiation of antibiotics if clinically indicated.
Diagnosis Tests And Interpretation
CBC with differential to determine ANC is mandatory. Additional studies include liver function tests, blood cultures from two sites (including catheter if present), urinalysis and urine culture, sputum or stool cultures when indicated, and CSF analysis if neurologic symptoms are present. Chest radiography should be obtained even in the absence of respiratory findings.
Differential Diagnosis
Laboratory error, malignancy, chemotherapy effects, medication reactions, infections, autoimmune disease, genetic conditions, transfusion reactions, nutritional deficiencies, tumor lysis syndrome, and hypersplenism. Some African American patients may have a normal baseline ANC around 1,000 cells/mm³.
Treatment Initial Stabilization Therapy
Patients in shock require immediate resuscitation with 1 L of 0.9% NS (pediatrics: 20 mL/kg), vasopressors if needed, and early goal-directed therapy when appropriate.
Ed Treatment Procedures
Initiate protective isolation when possible. After cultures are obtained, administer empiric broad-spectrum antibiotics promptly for suspected infection. Appropriate regimens include cefepime, ceftazidime (with or without an aminoglycoside), imipenem/cilastatin, fluoroquinolones, or an aminoglycoside combined with an antipseudomonal β-lactam. Vancomycin should be added when MRSA risk is present.
Medication
Common agents include cefepime, ceftazidime, imipenem/cilastatin, levofloxacin, aminoglycosides, mezlocillin, and vancomycin. Dosing should be adjusted for renal function and patient age.
Follow-Up Disposition
Admission is indicated for any signs of infection, unreliable follow-up, or inability to ensure close monitoring. Selected asymptomatic patients with known chronic granulocytopenia and reliable follow-up may be discharged.
Issues For Referral
All patients with granulocytopenia should be referred to their primary physician or a hematologist.
Follow-Up Recommendations
Patients should return immediately for fever or new symptoms and follow up within 48 hours with their physician.
Key Clinical Insights And Frequent Errors
Infections may present subtly or without classic signs due to impaired inflammatory response. Rectal exams and rectal temperatures should be avoided until antibiotics are started to reduce the risk of perirectal abscess and bacteremia. Febrile patients with ANC <500 require immediate aggressive management with iv fluids and broad-spectrum antibiotics. hepatosplenic candidiasis may emerge during neutrophil recovery presents abscess formation, requiring antifungal therapy such as amphotericin b.< />pan>
Basics Description
Granulocytopenia is a significant reduction in circulating granulocytes in peripheral blood. The three granulocyte classes are neutrophils (polymorphonuclear cells and bands), eosinophils, and basophils. Because neutrophils predominate, granulocytopenia is commonly used interchangeably with neutropenia. Granulocytes are essential components of innate immunity.
Clinical risk is best assessed by the absolute neutrophil count (ANC), calculated as WBC × (% PMNs + bands). Modern analyzers typically report ANC automatically. Neutropenia is defined as ANC <1,500 cells />m³: mild (1,000–1,500), moderate (500–1,000), severe (<500). agranulocytosis refers to anc <100. patients with rapidly falling counts are at higher infection risk than those low but recovering counts. myelodysplastic syndromes may be functionally granulocytopenic due impaired neutrophil function.< />pan>
Four mechanisms lead to granulocytopenia: decreased production, ineffective granulopoiesis, margination of neutrophils to the vascular endothelium, and increased peripheral destruction. Untreated febrile neutropenia carries mortality rates up to 50%, closely related to severity, duration, and delay to antibiotic therapy. Approximately 21% of oncology patients with neutropenic fever develop serious complications.
Pediatric considerations include physiologically elevated neonatal ANC during the first days of life and lower infection risk in otherwise healthy children older than 3 months with isolated moderate neutropenia.
Etiology
The most common cause is myelosuppressive chemotherapy or radiation, typically occurring 5–10 days after treatment. Drug-induced granulocytopenia is the second most common cause and usually requires at least 4 weeks of exposure, resolving within 30 days of discontinuation. High-risk drugs include clozapine, sulfasalazine, thioamides, antiplatelet agents, antiepileptics, NSAIDs, methotrexate, cyclophosphamide, colchicine, azathioprine, and ganciclovir.
Infectious causes include bacterial (typhoid, Shigella, brucellosis, tularemia, tuberculosis), parasitic (malaria, kala-azar), rickettsial (ehrlichiosis, RMSF), and viral infections, particularly HIV, hepatitis B, and EBV.
Immune-mediated causes include primary immune neutropenia, autoimmune diseases, thymoma, complement activation, transfusion reactions, alcoholism, nutritional deficiencies (vitamin B12, folate, copper), chronic idiopathic neutropenia, and pure white cell aplasia. Numerous congenital causes exist in pediatric populations.
Diagnosis Signs And Symptoms
Patients may present with fever or subtle signs of bacterial or fungal infection. Symptoms of pancytopenia include fatigue, pallor, petechiae, epistaxis, and spontaneous bleeding. Medication history, prior ANC values, and family history are essential. Patients should be questioned carefully about systemic and localizing symptoms of infection.
Physical examination focuses on identifying infection, including careful oral, pulmonary, abdominal, skin, catheter site, and perirectal assessment. Rectal examination is relatively contraindicated until antibiotics are initiated.
Essential Workup
A complete physical examination with emphasis on oral mucosa, perianal region, skin, lungs, and abdomen is required. Rectal examination may be performed after initiation of antibiotics if clinically indicated.
Diagnosis Tests And Interpretation
CBC with differential to determine ANC is mandatory. Additional studies include liver function tests, blood cultures from two sites (including catheter if present), urinalysis and urine culture, sputum or stool cultures when indicated, and CSF analysis if neurologic symptoms are present. Chest radiography should be obtained even in the absence of respiratory findings.
Differential Diagnosis
Laboratory error, malignancy, chemotherapy effects, medication reactions, infections, autoimmune disease, genetic conditions, transfusion reactions, nutritional deficiencies, tumor lysis syndrome, and hypersplenism. Some African American patients may have a normal baseline ANC around 1,000 cells/mm³.
Treatment Initial Stabilization Therapy
Patients in shock require immediate resuscitation with 1 L of 0.9% NS (pediatrics: 20 mL/kg), vasopressors if needed, and early goal-directed therapy when appropriate.
Ed Treatment Procedures
Initiate protective isolation when possible. After cultures are obtained, administer empiric broad-spectrum antibiotics promptly for suspected infection. Appropriate regimens include cefepime, ceftazidime (with or without an aminoglycoside), imipenem/cilastatin, fluoroquinolones, or an aminoglycoside combined with an antipseudomonal β-lactam. Vancomycin should be added when MRSA risk is present.
Medication
Common agents include cefepime, ceftazidime, imipenem/cilastatin, levofloxacin, aminoglycosides, mezlocillin, and vancomycin. Dosing should be adjusted for renal function and patient age.
Follow-Up Disposition
Admission is indicated for any signs of infection, unreliable follow-up, or inability to ensure close monitoring. Selected asymptomatic patients with known chronic granulocytopenia and reliable follow-up may be discharged.
Issues For Referral
All patients with granulocytopenia should be referred to their primary physician or a hematologist.
Follow-Up Recommendations
Patients should return immediately for fever or new symptoms and follow up within 48 hours with their physician.
Key Clinical Insights And Frequent Errors
Infections may present subtly or without classic signs due to impaired inflammatory response. Rectal exams and rectal temperatures should be avoided until antibiotics are started to reduce the risk of perirectal abscess and bacteremia. Febrile patients with ANC <500 require immediate aggressive management with iv fluids and broad-spectrum antibiotics. hepatosplenic candidiasis may emerge during neutrophil recovery presents abscess formation, requiring antifungal therapy such as amphotericin b.< />pan>
- Published on
Emergency And Acute Medicine – Hallucinations
Overview And Definitions
Hallucinations represent a clinical symptom rather than a definitive diagnosis. They may be auditory, visual, tactile, gustatory, or olfactory in nature. A hallucination is defined as a sensory perception experienced as real in the absence of external stimulation of the relevant sensory organ and is perceived as originating from that organ. Insight into the unreality of the experience may or may not be present. An illusion refers to a misinterpretation of an actual external stimulus. A flashback is the re-experiencing of a prior memory, sensation, or perceptual event with a compelling sense of reality. A pseudohallucination describes a hallucination-like experience that is not perceived through a sensory organ, such as voices perceived internally rather than externally.
Epidemiology And Frequency
The lifetime prevalence of auditory hallucinations in the general population is estimated at 4–8%, although rates vary depending on definitions and inclusion of pseudohallucinations. More than half of elderly patients with dementia experience hallucinations or paranoid symptoms.
Causes And Contributing Factors
Hallucinations arise from a wide range of psychiatric, medical, neurologic, metabolic, infectious, and substance-related causes. Psychiatric causes include schizophrenia, bipolar disorder with mania, and major depressive disorder. Acute intoxications associated with hallucinations include ethanol, cannabis, and synthetic cannabinoids such as K2 and Spice. Sympathomimetic agents include amphetamine, methamphetamine, cocaine, and synthetic cathinones. NMDA antagonists such as ketamine, PCP, and dextromethorphan are well-known precipitants. Serotonergic substances include MDMA, LSD, mescaline, psilocybin, 2C compounds, and 5-MeO derivatives. Salvia divinorum acts as a kappa opioid receptor agonist and may cause synesthesia. Opiates and inhalants such as toluene and nitrous oxide are additional contributors. Medications associated with hallucinations include anticholinergic agents, corticosteroids, and methylphenidate. Withdrawal states from ethanol, benzodiazepines, barbiturates, and GHB commonly produce hallucinations. Substance-induced psychotic disorders include methamphetamine-associated psychosis, which may persist or recur even without ongoing use, and cannabis-induced psychosis. Infectious causes include meningitis and encephalitis, and in patients with dementia, common infections such as urinary tract infection or pneumonia may trigger hallucinations. Metabolic causes include hypoglycemia, electrolyte disturbances, thyroid or adrenal disease, Wilson disease, and thiamine deficiency. Neurologic etiologies include seizures, migraines, intracranial hemorrhage, brain tumors, stroke, and Tourette syndrome. Neurodegenerative disorders such as Parkinson disease, Lewy body dementia, Alzheimer disease, and HIV are also associated. Ocular conditions include glaucoma, macular degeneration, and Charles Bonnet syndrome. Other causes include sensory or sleep deprivation, extreme fatigue or stress, heat illness, religious or ritual practices, and transitions between sleep and wakefulness.
Special Population Considerations
In pediatric patients, hallucinations are relatively common and often developmentally normal. Most children with hallucinations do not have psychosis. Hallucinations may occur during delirium associated with fever, and a medical or neurologic cause should always be considered. In geriatric patients, hallucinations are most often due to organic causes and commonly accompany dementia, depression, medication reactions, or substance use. They are frequently associated with agitation, and atypical antipsychotics may be effective but must be used cautiously due to adverse effects.
Clinical Evaluation And Presentation
Obtaining an accurate history is often challenging, and collateral information from family, EMS, police, or caregivers is critical. Clinicians should assess for behavioral changes from baseline, delusions, persecutory beliefs, prior hallucinations, medication changes, and substance use. Rapidly fluctuating cognition suggests delirium. Headache may indicate migraine or intracranial pathology. Physical examination findings vary by etiology. Acute psychosis may present with disorganized thought and response to internal stimuli. Mania is characterized by pressured speech and excessive talking. Delirium presents with altered consciousness, disorientation, and abnormal vital signs. CNS lesions may cause cranial nerve deficits, aphasia, focal neurologic findings, or gait abnormalities. Systemic or infectious illness may present with fever, nuchal rigidity, asterixis, myoclonus, jaundice, or ascites. Intoxication or withdrawal syndromes may show mydriasis, tachycardia, hypertension, hyperthermia, diaphoresis, agitation, miosis, bradypnea, hyperreflexia, clonus, tremor, or nystagmus depending on the agent involved.
Diagnostic Testing And Interpretation
Initial evaluation commonly includes a complete blood count, serum chemistries, ethanol, acetaminophen, and salicylate levels, and urinalysis. Additional testing is guided by clinical suspicion and may include urine drug screening, ECG, thyroid studies, liver function tests, RPR, folate, vitamin B12, thiamine levels, and specific drug concentrations. Brain imaging with CT or MRI and chest radiography may be indicated. Lumbar puncture should be considered if infection is suspected, and EEG may be useful when seizures are a concern. Emergent psychiatric consultation is indicated for acute psychiatric illness or decompensation of chronic psychiatric disease.
Core Emergency Department Workup
Patients with a known psychiatric disorder and characteristic symptoms typically require limited testing. Patients with undifferentiated hallucinations, especially those in high-risk populations, require comprehensive medical evaluation to exclude organic causes.
Differential Diagnosis Considerations
The primary goal of emergency evaluation is to distinguish psychiatric from nonpsychiatric causes. Psychiatric etiologies are more likely when hallucinations are auditory or command in nature, incorporated into a delusional system, occur between ages 13 and 40, and are associated with flat affect, normal orientation, and disorganized attention. Nonpsychiatric causes are more likely in elderly patients, individuals with substance use history, those without prior psychiatric illness, patients with underlying medical conditions, and those of lower socioeconomic status. Visual hallucinations are more common in delirium, dementia, migraines, dopamine agonist therapy, posterior cerebral infarcts, and narcolepsy.
Management Principles
Prehospital providers should note environmental clues such as unsafe living conditions or drug paraphernalia. Initial management focuses on airway, breathing, and circulation, correction of abnormal vital signs, finger-stick glucose testing, and consideration of thiamine administration. Agitation should be managed with de-escalation techniques, physical restraints when necessary, and chemical sedation. Identified medical causes should be treated directly, and antipsychotics are often unnecessary in these cases. Acute psychosis or psychiatric decompensation is treated with antipsychotics and benzodiazepines. Hallucinations associated with intoxication and excited delirium require supportive care and benzodiazepines. In dementia-related hallucinations, reversible causes should be treated first, and antipsychotics used cautiously due to risks.
Safety Alert
In patients with hallucinations and excited delirium due to acute intoxication, except ethanol-related cases, benzodiazepines are preferred and antipsychotics should be avoided.
Disposition And Follow-Up
Hospital admission is required for patients with medical conditions necessitating inpatient care or acute psychiatric illness requiring hospitalization. Discharge may be considered when symptoms resolve after treatment of a reversible cause or when psychiatric decompensation is stabilized with a safe home environment and reliable follow-up. Referral for substance use treatment should be arranged when appropriate. Follow-up should be tailored to the underlying medical or psychiatric condition.
Clinical Pearls And Common Errors
Do not assume auditory hallucinations are psychiatric or that visual or tactile hallucinations are medical without a full evaluation. In older adults, hallucinations should never be attributed to psychiatric disease without extensive medical workup. Antipsychotics should not be used for excited delirium due to acute intoxication except in ethanol withdrawal; benzodiazepines are the treatment of choice.

- Published on
Emergency And Acute Medicine – Head Pain Syndromes
Overview And Pathophysiology
Headache is pain perceived in the cranium, orbits, or upper cervical region. Pain originating from intracranial structures is often projected to the surface. Intracranial pain-sensitive structures include arteries, veins, dura, and meninges. Extracranial sources include the skin, scalp, fascia, muscles, mucosal linings of the sinuses, arteries, temporomandibular joints, and teeth. Pain transmission occurs primarily via the trigeminal (V) cranial nerve. Mechanisms include nerve irritation, traction on pain-sensitive vessels, vasodilation, hypoxia, hypercapnia, fever, histamine exposure, or nitroglycerin ingestion. Headache accounts for 2–4% of ED visits; approximately 95% are benign, though serious etiologies are more common in patients older than 50 years.
Causes And Risk Factors
Migraine results from intra- and extracranial vasodilation and constriction of pain-sensitive vessels and may involve cortical spreading depression. Pain is typically throbbing. Tension-type headache requires at least ten similar episodes and has an unclear etiology, possibly involving serotonin imbalance, reduced endorphins, or muscle spasm. It is the most common recurrent headache, often triggered by poor posture, stress, anxiety, depression, or cervical osteoarthritis. Pain is usually bilateral, nonpulsatile, band-like, mild to moderate, and lasts 4–13 hours.
Cluster headache may be triggered by alcohol, certain foods, sleep disruption, or strong emotions and may involve vasospasm near cranial nerves.
Intracranial pressure or traction causes include mass lesions and idiopathic intracranial hypertension. Extracranial compression headaches arise from peripheral nerve pathology of the head and neck. Inflammatory causes include temporal arteritis and cerebral vasculitis. Thrombotic causes include cerebral venous sinus thrombosis. Disorders of vascular autoregulation include posterior reversible leukoencephalopathy syndrome and reversible cerebral vasoconstriction syndrome.
Children rarely have serious headache causes but require follow-up. Older adults with new-onset headache have higher risk for serious disease and warrant low thresholds for imaging. Pregnancy and the postpartum period increase risk for CVST, eclampsia, PRES, and RCVS.
Clinical Assessment
History should characterize pain using PQRST. Provoking factors include head position, coughing, or straining; worsening with these suggests elevated intracranial pressure. Quality may be throbbing or continuous, deep or superficial. Assess region, severity, “worst headache of life,” timing (sudden vs. gradual), and associated symptoms such as visual changes, dizziness, nausea, or vomiting.
Red flags include new onset, age >50 years, immunosuppression, malignancy, trauma or falls, persistent vomiting, focal neurologic or visual deficits, and risk factors for CVST (pregnancy/postpartum, malignancy, oral contraceptives, protein C/S deficiency, ulcerative colitis, Behçet syndrome).
Physical Examination
Perform a complete neurologic exam including cranial nerves, motor and sensory testing, reflexes, and gait. Examine fundi for papilledema. Inspect skin for rashes (e.g., zoster, purpura). Palpate temporal arteries for tenderness or thickening.
Initial Evaluation Strategy
A thorough history and focused CNS, HEENT, and neck examination are essential. Additional testing is indicated with severe hypertension, fever, altered mental status, papilledema, abnormal neurologic findings, or meningismus.
Diagnostic Studies
Laboratory testing includes cerebrospinal fluid analysis when meningitis or subarachnoid hemorrhage is suspected and ESR when temporal arteritis or inflammatory disease is considered.
Noncontrast head CT is indicated for uncertain diagnosis, signs of increased ICP, first or worst headache, abrupt onset, new focal deficits, papilledema, recurrent morning headaches, persistent vomiting, headache with fever or rash, trauma with LOC, altered mental status, or meningismus. CT within 6 hours of onset is highly sensitive for SAH; sensitivity declines after 24 hours.
MRI evaluates posterior fossa lesions, pituitary apoplexy, CVST, and causes missed by CT and LP. MRA is indicated when SAH is suspected with negative CT and LP cannot be performed, or when arterial dissection or nonmigrainous vascular causes are suspected.
Lumbar puncture is required after CT when focal deficits, papilledema, abnormal mental status, or immunosuppression are present. It detects infection, occult SAH, opening pressure abnormalities, and distinguishes traumatic tap from hemorrhage. Xanthochromia is typically present by 12 hours after SAH onset.
Differential Diagnosis
Acute single headache includes SAH, meningitis, intracerebral hemorrhage, hypertensive encephalopathy, arterial dissection, CVST, cerebellar stroke, acute angle-closure glaucoma, pituitary apoplexy, temporal neuritis, trauma, acute sinusitis, toxic or metabolic states, withdrawal syndromes, and post–lumbar puncture headache.
Acute recurrent headache over days to weeks includes migraine, cluster, tension, CVST, pseudotumor cerebri, temporal arteritis, SAH rebleed, hypoxia-related headache, trigeminal neuralgia, postherpetic neuralgia, exertional and coital headaches.
Subacute headache over weeks to months suggests chronic subdural hematoma, brain tumor, brain abscess, chronic sinusitis, temporomandibular joint disorders, chronic post-traumatic headache, pseudotumor cerebri, or temporal arteritis.
Chronic headache over months to years includes chronic tension headache, medication overuse headache, depression-related headache, trigeminal neuralgia, severe anemia, acute glaucoma, and cervical spine disease.
Management Principles
Initial stabilization focuses on airway, breathing, and circulation in patients with altered mental status. Start empiric antibiotics promptly for suspected bacterial meningitis and add acyclovir in immunocompromised patients.
ED management is etiology-specific. Migraine, cluster, and tension headaches receive symptomatic therapy. Temporal arteritis, intracranial infection, and intracranial hemorrhage require targeted treatment.
Disposition And Follow-Up
Admit patients with suspected organic disease, intractable vomiting with dehydration, or pain refractory to outpatient therapy. Consider ICU admission for suspected aneurysm, acute subdural hematoma, SAH, stroke, increased ICP, or intracranial infection.
Discharge is appropriate for resolved migraine, cluster, or tension headaches and minor infections with adequate follow-up. Patients with recurrent headaches should follow up with a primary care physician or neurologist.
Medications Commonly Used
Common agents include chlorpromazine, dexamethasone, dihydroergotamine, ergotamine, ketorolac, intranasal lidocaine, metoclopramide, morphine, prochlorperazine, and sumatriptan, selected based on headache type and patient factors.
Clinical Warnings And Pitfalls
Do not use treatment response to determine benign etiology. CT sensitivity for SAH decreases rapidly after 24 hours; lumbar puncture remains essential after delayed presentation. Neurology consultation should not delay urgent imaging in high-risk cases. Use dopamine antagonists cautiously in QT prolongation or electrolyte abnormalities. Use triptans and ergotamines cautiously in coronary artery disease. Chronic headache patients benefit from consistent plans, but new or changing features require reassessment. Never delay empiric treatment of suspected meningitis while awaiting lumbar puncture results.
Overview And Pathophysiology
Headache is pain perceived in the cranium, orbits, or upper cervical region. Pain originating from intracranial structures is often projected to the surface. Intracranial pain-sensitive structures include arteries, veins, dura, and meninges. Extracranial sources include the skin, scalp, fascia, muscles, mucosal linings of the sinuses, arteries, temporomandibular joints, and teeth. Pain transmission occurs primarily via the trigeminal (V) cranial nerve. Mechanisms include nerve irritation, traction on pain-sensitive vessels, vasodilation, hypoxia, hypercapnia, fever, histamine exposure, or nitroglycerin ingestion. Headache accounts for 2–4% of ED visits; approximately 95% are benign, though serious etiologies are more common in patients older than 50 years.
Causes And Risk Factors
Migraine results from intra- and extracranial vasodilation and constriction of pain-sensitive vessels and may involve cortical spreading depression. Pain is typically throbbing. Tension-type headache requires at least ten similar episodes and has an unclear etiology, possibly involving serotonin imbalance, reduced endorphins, or muscle spasm. It is the most common recurrent headache, often triggered by poor posture, stress, anxiety, depression, or cervical osteoarthritis. Pain is usually bilateral, nonpulsatile, band-like, mild to moderate, and lasts 4–13 hours.
Cluster headache may be triggered by alcohol, certain foods, sleep disruption, or strong emotions and may involve vasospasm near cranial nerves.
Intracranial pressure or traction causes include mass lesions and idiopathic intracranial hypertension. Extracranial compression headaches arise from peripheral nerve pathology of the head and neck. Inflammatory causes include temporal arteritis and cerebral vasculitis. Thrombotic causes include cerebral venous sinus thrombosis. Disorders of vascular autoregulation include posterior reversible leukoencephalopathy syndrome and reversible cerebral vasoconstriction syndrome.
Children rarely have serious headache causes but require follow-up. Older adults with new-onset headache have higher risk for serious disease and warrant low thresholds for imaging. Pregnancy and the postpartum period increase risk for CVST, eclampsia, PRES, and RCVS.
Clinical Assessment
History should characterize pain using PQRST. Provoking factors include head position, coughing, or straining; worsening with these suggests elevated intracranial pressure. Quality may be throbbing or continuous, deep or superficial. Assess region, severity, “worst headache of life,” timing (sudden vs. gradual), and associated symptoms such as visual changes, dizziness, nausea, or vomiting.
Red flags include new onset, age >50 years, immunosuppression, malignancy, trauma or falls, persistent vomiting, focal neurologic or visual deficits, and risk factors for CVST (pregnancy/postpartum, malignancy, oral contraceptives, protein C/S deficiency, ulcerative colitis, Behçet syndrome).
Physical Examination
Perform a complete neurologic exam including cranial nerves, motor and sensory testing, reflexes, and gait. Examine fundi for papilledema. Inspect skin for rashes (e.g., zoster, purpura). Palpate temporal arteries for tenderness or thickening.
Initial Evaluation Strategy
A thorough history and focused CNS, HEENT, and neck examination are essential. Additional testing is indicated with severe hypertension, fever, altered mental status, papilledema, abnormal neurologic findings, or meningismus.
Diagnostic Studies
Laboratory testing includes cerebrospinal fluid analysis when meningitis or subarachnoid hemorrhage is suspected and ESR when temporal arteritis or inflammatory disease is considered.
Noncontrast head CT is indicated for uncertain diagnosis, signs of increased ICP, first or worst headache, abrupt onset, new focal deficits, papilledema, recurrent morning headaches, persistent vomiting, headache with fever or rash, trauma with LOC, altered mental status, or meningismus. CT within 6 hours of onset is highly sensitive for SAH; sensitivity declines after 24 hours.
MRI evaluates posterior fossa lesions, pituitary apoplexy, CVST, and causes missed by CT and LP. MRA is indicated when SAH is suspected with negative CT and LP cannot be performed, or when arterial dissection or nonmigrainous vascular causes are suspected.
Lumbar puncture is required after CT when focal deficits, papilledema, abnormal mental status, or immunosuppression are present. It detects infection, occult SAH, opening pressure abnormalities, and distinguishes traumatic tap from hemorrhage. Xanthochromia is typically present by 12 hours after SAH onset.
Differential Diagnosis
Acute single headache includes SAH, meningitis, intracerebral hemorrhage, hypertensive encephalopathy, arterial dissection, CVST, cerebellar stroke, acute angle-closure glaucoma, pituitary apoplexy, temporal neuritis, trauma, acute sinusitis, toxic or metabolic states, withdrawal syndromes, and post–lumbar puncture headache.
Acute recurrent headache over days to weeks includes migraine, cluster, tension, CVST, pseudotumor cerebri, temporal arteritis, SAH rebleed, hypoxia-related headache, trigeminal neuralgia, postherpetic neuralgia, exertional and coital headaches.
Subacute headache over weeks to months suggests chronic subdural hematoma, brain tumor, brain abscess, chronic sinusitis, temporomandibular joint disorders, chronic post-traumatic headache, pseudotumor cerebri, or temporal arteritis.
Chronic headache over months to years includes chronic tension headache, medication overuse headache, depression-related headache, trigeminal neuralgia, severe anemia, acute glaucoma, and cervical spine disease.
Management Principles
Initial stabilization focuses on airway, breathing, and circulation in patients with altered mental status. Start empiric antibiotics promptly for suspected bacterial meningitis and add acyclovir in immunocompromised patients.
ED management is etiology-specific. Migraine, cluster, and tension headaches receive symptomatic therapy. Temporal arteritis, intracranial infection, and intracranial hemorrhage require targeted treatment.
Disposition And Follow-Up
Admit patients with suspected organic disease, intractable vomiting with dehydration, or pain refractory to outpatient therapy. Consider ICU admission for suspected aneurysm, acute subdural hematoma, SAH, stroke, increased ICP, or intracranial infection.
Discharge is appropriate for resolved migraine, cluster, or tension headaches and minor infections with adequate follow-up. Patients with recurrent headaches should follow up with a primary care physician or neurologist.
Medications Commonly Used
Common agents include chlorpromazine, dexamethasone, dihydroergotamine, ergotamine, ketorolac, intranasal lidocaine, metoclopramide, morphine, prochlorperazine, and sumatriptan, selected based on headache type and patient factors.
Clinical Warnings And Pitfalls
Do not use treatment response to determine benign etiology. CT sensitivity for SAH decreases rapidly after 24 hours; lumbar puncture remains essential after delayed presentation. Neurology consultation should not delay urgent imaging in high-risk cases. Use dopamine antagonists cautiously in QT prolongation or electrolyte abnormalities. Use triptans and ergotamines cautiously in coronary artery disease. Chronic headache patients benefit from consistent plans, but new or changing features require reassessment. Never delay empiric treatment of suspected meningitis while awaiting lumbar puncture results.
- Published on
Emergency And Acute Medicine – Pediatric Fractures
Basics Description
Approximately 20% of children presenting with acute traumatic injuries sustain fractures, with boys affected more frequently than girls. Pediatric bone anatomy differs from adults and includes the diaphysis (shaft between growth plates), metaphysis (rapidly growing trabecular bone adjacent to the growth plate), epiphysis (cartilaginous growth center near the bone end), and the epiphyseal or growth plate, which is cartilaginous and radiolucent on imaging. Children’s bones are more elastic and resilient, allowing unique fracture patterns such as greenstick fractures (incomplete cortical disruption), torus or buckle fractures (compression injury at the metaphyseal–diaphyseal junction), and plastic deformities (bowing without cortical break). Growth plate involvement is common, as ligaments are stronger than physes. The Salter–Harris classification describes physeal fractures, with increasing risk of growth disturbance from type I through type V.
Etiology
Mechanism of injury helps predict fracture type and severity. Risk factors include obesity and rapid growth spurts. Nonaccidental trauma must be considered, particularly in children younger than 1 year with fractures inconsistent with the history. Highly suggestive findings include metaphyseal corner fractures, posterior rib fractures, spiral femur fractures, fractures at different stages of healing, skull fractures crossing suture lines in infants, and concerning child or caregiver behavior.
Diagnosis Signs And Symptoms
Children may present with refusal to use a limb, decreased movement, swelling, tenderness, deformity, ecchymosis, crepitus, limp, or abnormal neurovascular findings. Compartment syndrome should be suspected with severe pain (especially in forearm, calf, or foot), pain on passive stretch, sensory deficits, cool extremity, or absent pulses. Open fractures may be subtle and appear as localized bleeding with fat globules.
History
Obtain a detailed mechanism of injury including fall height, vehicle speed, and events surrounding trauma. Assess for neurologic symptoms and associated injuries, and ensure the history is consistent with findings.
Physical Exam
Perform a thorough secondary survey. Assess deformities, bruising, and associated injuries. Carefully evaluate neurovascular status, including motor function, sensation, distal pulses, capillary refill, and joint range of motion.
Essential Workup
Prompt immobilization followed by appropriate imaging.
Diagnosis Tests And Interpretation
Lab
Laboratory studies are required only when infection, surgery, or multisystem trauma is suspected and may include CBC and inflammatory markers.
Imaging
Obtain AP, lateral, and oblique radiographs as needed, including joints above and below the injury. Comparison views can be helpful when growth plate injury is suspected. Repeat radiographs in 7–10 days may identify occult fractures or Salter–Harris type I injuries. Bone scan, CT, or MRI may be used when plain films are inconclusive or to evaluate infection.
Diagnostic Procedures/Surgery
Arthrocentesis is indicated if joint infection is suspected.
Differential Diagnosis
Sprain, strain, contusion, infection, tumor, neurologic injury, subtle dislocations such as nursemaid’s elbow, and nonaccidental trauma.
Treatment
Prehospital
Immobilization of the affected extremity.
Initial Stabilization/Therapy
Address life-threatening injuries and immobilize fractures.
ED Treatment/Procedures
Provide adequate analgesia and manage concurrent injuries. Dislocations require urgent reduction with careful neurovascular assessment. Alignment is critical, especially for intra-articular fractures. Suspected nonaccidental trauma must be reported appropriately.
Salter–Harris type I and II fractures are treated with immobilization and orthopedic follow-up. Type III, IV, distal femur type II, and type V fractures require urgent orthopedic consultation; even with anatomic reduction, growth disturbance may occur.
Clavicle fractures are treated with a sling or figure-of-eight brace; distal third injuries require referral.
Elbow fractures, especially supracondylar injuries, require orthopedic consultation due to risk of neurovascular compromise and compartment syndrome.
Distal radius and ulna fractures are the most common pediatric fractures; angulated fractures often require reduction and immobilization. Torus fractures require immobilization only, while greenstick fractures may need reduction if angulated.
Tibial and fibular fractures are managed based on displacement, with toddler’s fractures often requiring immobilization despite subtle imaging findings.
Slipped capital femoral epiphysis requires nonweight bearing and urgent orthopedic referral.
Open fractures require irrigation, sterile dressing, immobilization, and early antibiotics in consultation with orthopedics.
Children presenting with limp require evaluation for infection, rheumatologic disease, malignancy, transient synovitis, or septic arthritis.
Medication
Acetaminophen 10–15 mg/kg PO or PR q4–6h.
Ibuprofen 10 mg/kg PO q6–8h as first-line therapy.
Morphine 0.05–0.2 mg/kg IV/IM/SC q2–4h for severe pain.
Cefazolin and gentamicin dosing as indicated for open fractures.
Local hematoma block with 1% lidocaine without epinephrine when appropriate.
Follow Up Disposition
Admission Criteria
Suspected nonaccidental trauma, open fractures, or fractures with neurovascular compromise or compartment syndrome.
Discharge Criteria
Uncomplicated fractures without associated injuries or neurovascular compromise, with reliable caregivers and arranged follow-up.
Issues For Referral
All Salter–Harris fractures and complex injuries require orthopedic follow-up.
Key Practice Insights And Common Pitfalls
A careful history is essential when evaluating for nonaccidental trauma. Fully undress the child when abuse is suspected. Maintain a low threshold for splinting or orthopedic consultation. Adequate pain control is frequently underdosed. Distal radius fractures often coexist with ulna, elbow, or carpal injuries and should be evaluated carefully.
Basics Description
Approximately 20% of children presenting with acute traumatic injuries sustain fractures, with boys affected more frequently than girls. Pediatric bone anatomy differs from adults and includes the diaphysis (shaft between growth plates), metaphysis (rapidly growing trabecular bone adjacent to the growth plate), epiphysis (cartilaginous growth center near the bone end), and the epiphyseal or growth plate, which is cartilaginous and radiolucent on imaging. Children’s bones are more elastic and resilient, allowing unique fracture patterns such as greenstick fractures (incomplete cortical disruption), torus or buckle fractures (compression injury at the metaphyseal–diaphyseal junction), and plastic deformities (bowing without cortical break). Growth plate involvement is common, as ligaments are stronger than physes. The Salter–Harris classification describes physeal fractures, with increasing risk of growth disturbance from type I through type V.
Etiology
Mechanism of injury helps predict fracture type and severity. Risk factors include obesity and rapid growth spurts. Nonaccidental trauma must be considered, particularly in children younger than 1 year with fractures inconsistent with the history. Highly suggestive findings include metaphyseal corner fractures, posterior rib fractures, spiral femur fractures, fractures at different stages of healing, skull fractures crossing suture lines in infants, and concerning child or caregiver behavior.
Diagnosis Signs And Symptoms
Children may present with refusal to use a limb, decreased movement, swelling, tenderness, deformity, ecchymosis, crepitus, limp, or abnormal neurovascular findings. Compartment syndrome should be suspected with severe pain (especially in forearm, calf, or foot), pain on passive stretch, sensory deficits, cool extremity, or absent pulses. Open fractures may be subtle and appear as localized bleeding with fat globules.
History
Obtain a detailed mechanism of injury including fall height, vehicle speed, and events surrounding trauma. Assess for neurologic symptoms and associated injuries, and ensure the history is consistent with findings.
Physical Exam
Perform a thorough secondary survey. Assess deformities, bruising, and associated injuries. Carefully evaluate neurovascular status, including motor function, sensation, distal pulses, capillary refill, and joint range of motion.
Essential Workup
Prompt immobilization followed by appropriate imaging.
Diagnosis Tests And Interpretation
Lab
Laboratory studies are required only when infection, surgery, or multisystem trauma is suspected and may include CBC and inflammatory markers.
Imaging
Obtain AP, lateral, and oblique radiographs as needed, including joints above and below the injury. Comparison views can be helpful when growth plate injury is suspected. Repeat radiographs in 7–10 days may identify occult fractures or Salter–Harris type I injuries. Bone scan, CT, or MRI may be used when plain films are inconclusive or to evaluate infection.
Diagnostic Procedures/Surgery
Arthrocentesis is indicated if joint infection is suspected.
Differential Diagnosis
Sprain, strain, contusion, infection, tumor, neurologic injury, subtle dislocations such as nursemaid’s elbow, and nonaccidental trauma.
Treatment
Prehospital
Immobilization of the affected extremity.
Initial Stabilization/Therapy
Address life-threatening injuries and immobilize fractures.
ED Treatment/Procedures
Provide adequate analgesia and manage concurrent injuries. Dislocations require urgent reduction with careful neurovascular assessment. Alignment is critical, especially for intra-articular fractures. Suspected nonaccidental trauma must be reported appropriately.
Salter–Harris type I and II fractures are treated with immobilization and orthopedic follow-up. Type III, IV, distal femur type II, and type V fractures require urgent orthopedic consultation; even with anatomic reduction, growth disturbance may occur.
Clavicle fractures are treated with a sling or figure-of-eight brace; distal third injuries require referral.
Elbow fractures, especially supracondylar injuries, require orthopedic consultation due to risk of neurovascular compromise and compartment syndrome.
Distal radius and ulna fractures are the most common pediatric fractures; angulated fractures often require reduction and immobilization. Torus fractures require immobilization only, while greenstick fractures may need reduction if angulated.
Tibial and fibular fractures are managed based on displacement, with toddler’s fractures often requiring immobilization despite subtle imaging findings.
Slipped capital femoral epiphysis requires nonweight bearing and urgent orthopedic referral.
Open fractures require irrigation, sterile dressing, immobilization, and early antibiotics in consultation with orthopedics.
Children presenting with limp require evaluation for infection, rheumatologic disease, malignancy, transient synovitis, or septic arthritis.
Medication
Acetaminophen 10–15 mg/kg PO or PR q4–6h.
Ibuprofen 10 mg/kg PO q6–8h as first-line therapy.
Morphine 0.05–0.2 mg/kg IV/IM/SC q2–4h for severe pain.
Cefazolin and gentamicin dosing as indicated for open fractures.
Local hematoma block with 1% lidocaine without epinephrine when appropriate.
Follow Up Disposition
Admission Criteria
Suspected nonaccidental trauma, open fractures, or fractures with neurovascular compromise or compartment syndrome.
Discharge Criteria
Uncomplicated fractures without associated injuries or neurovascular compromise, with reliable caregivers and arranged follow-up.
Issues For Referral
All Salter–Harris fractures and complex injuries require orthopedic follow-up.
Key Practice Insights And Common Pitfalls
A careful history is essential when evaluating for nonaccidental trauma. Fully undress the child when abuse is suspected. Maintain a low threshold for splinting or orthopedic consultation. Adequate pain control is frequently underdosed. Distal radius fractures often coexist with ulna, elbow, or carpal injuries and should be evaluated carefully.
- Published on
Click here to start customizing
- Published on
Emergency And Acute Medicine – Frostbite
Basics Description
Frostbite is tissue injury caused by exposure to cold temperatures. Tissue damage occurs through direct cellular injury from intracellular ice crystal formation, indirect injury from extracellular ice crystals causing cellular dehydration and enzymatic disruption, and reperfusion injury during rewarming. Reperfusion leads to release of inflammatory mediators such as prostaglandins and thromboxane, resulting in vasoconstriction, platelet aggregation, endothelial injury, and thrombosis. Clear blisters result from extracellular fluid exudation, while hemorrhagic blisters indicate deeper vascular injury. Progressive arterial thrombosis leads to ischemia and necrosis. Tissue demarcation evolves over weeks to months, leading to delayed definitive surgical decisions.
Etiology
Cold exposure severity depends on duration, wind chill, humidity, and wet skin or clothing. Predisposing factors include extremes of age, altered mental status from intoxication or psychiatric illness, and impaired circulation.
Diagnosis Signs And Symptoms
Fingers, toes, ears, and nose are most commonly affected. Classification after rewarming helps describe injury severity but does not change initial management.
Superficial frostbite involves skin only and usually heals without tissue loss. First-degree injuries present with erythema, edema, burning, and throbbing without blisters. Second-degree injuries cause marked edema, clear blisters, and numbness.
Deep frostbite results in inevitable tissue loss. Third-degree injuries involve subcutaneous tissue with hemorrhagic blisters and severe pain after rewarming. Fourth-degree injuries extend to muscle, tendon, and bone with deep cyanosis, mottling, or anesthesia. Poor prognostic signs include hemorrhagic blisters, persistent cyanosis, mottling, anesthesia, and impaired mobility after rewarming.
Essential Workup
Diagnosis is clinical. Document skin color, temperature, blister type, and tissue consistency. Perform vascular and neurologic exams including pulses, Doppler assessment, capillary refill, and two-point discrimination. Evaluate for associated conditions such as hypothermia, trauma, hypoglycemia, intoxication, cardiac or neurologic illness, and compartment syndrome.
Diagnosis Tests And Interpretation
Lab
Not required for mild cases. Severe frostbite may require CBC, electrolytes, renal function, glucose, creatine kinase, urinalysis for myoglobinuria, and cultures if infection is suspected.
Imaging
Technetium-99 scintigraphy or MR angiography may help identify viable tissue early and guide surgical planning.
Diagnostic Procedures
Rapid rewarming is performed using a water bath maintained at 40–42°C. Temperatures outside this range increase risk of thermal injury or worsen tissue loss.
Differential Diagnosis
Frostnip causes reversible numbness without tissue injury. Trench foot results from prolonged wet cold exposure without ice crystal formation and presents with neurovascular compromise. Chilblains occur with chronic cold exposure and present as erythematous or cyanotic plaques.
Treatment Prehospital
Protect and immobilize affected areas. Remove wet or constrictive clothing. Avoid rubbing, massage, snow application, or dry rewarming if refreezing is possible. Treat hypothermia cautiously to prevent arrhythmias.
Initial Stabilization Therapy
Address airway, breathing, and circulation. Correct hypothermia. Provide IV fluids for severe cases. Minimize handling of frozen tissue.
ED Treatment Procedures
If injury is recent and not rewarmed, initiate rapid rewarming in a 40–42°C water bath for 15–30 minutes until tissue is pliable and erythematous. Provide aggressive analgesia with opioids and NSAIDs. Apply topical aloe vera to intact skin. Debride or aspirate clear blisters but avoid hemorrhagic blister intervention. Provide tetanus prophylaxis. Consider short-term antibiotics during hyperemic recovery for severe injuries. Elevate and splint affected areas and change dressings frequently. Avoid vasoconstrictive agents including nicotine. Thrombolytic therapy within 24 hours may improve tissue salvage and requires specialist consultation.
Medication
Aloe vera topical cream applied every 6 hours.
Ibuprofen 800 mg PO TID (pediatric dosing weight-based).
Morphine sulfate titrated IV or IM for pain control.
Antibiotics such as cephalexin, dicloxacillin, or ciprofloxacin when indicated.
Follow Up Disposition
Admission Criteria
All but minimal superficial injuries should be admitted, especially when refreezing risk exists.
Discharge Criteria
Only very mild superficial frostbite with reliable follow-up.
Issues For Referral
Consult burn, plastic, hand, or general surgery for all but the mildest cases.
Key Practice Insights And Common Pitfalls
Avoid freeze–thaw–refreeze cycles. Maintain correct rewarming temperature. Always address hypothermia and systemic illness. Consider compartment syndrome in pulseless or tense extremities.
Basics Description
Frostbite is tissue injury caused by exposure to cold temperatures. Tissue damage occurs through direct cellular injury from intracellular ice crystal formation, indirect injury from extracellular ice crystals causing cellular dehydration and enzymatic disruption, and reperfusion injury during rewarming. Reperfusion leads to release of inflammatory mediators such as prostaglandins and thromboxane, resulting in vasoconstriction, platelet aggregation, endothelial injury, and thrombosis. Clear blisters result from extracellular fluid exudation, while hemorrhagic blisters indicate deeper vascular injury. Progressive arterial thrombosis leads to ischemia and necrosis. Tissue demarcation evolves over weeks to months, leading to delayed definitive surgical decisions.
Etiology
Cold exposure severity depends on duration, wind chill, humidity, and wet skin or clothing. Predisposing factors include extremes of age, altered mental status from intoxication or psychiatric illness, and impaired circulation.
Diagnosis Signs And Symptoms
Fingers, toes, ears, and nose are most commonly affected. Classification after rewarming helps describe injury severity but does not change initial management.
Superficial frostbite involves skin only and usually heals without tissue loss. First-degree injuries present with erythema, edema, burning, and throbbing without blisters. Second-degree injuries cause marked edema, clear blisters, and numbness.
Deep frostbite results in inevitable tissue loss. Third-degree injuries involve subcutaneous tissue with hemorrhagic blisters and severe pain after rewarming. Fourth-degree injuries extend to muscle, tendon, and bone with deep cyanosis, mottling, or anesthesia. Poor prognostic signs include hemorrhagic blisters, persistent cyanosis, mottling, anesthesia, and impaired mobility after rewarming.
Essential Workup
Diagnosis is clinical. Document skin color, temperature, blister type, and tissue consistency. Perform vascular and neurologic exams including pulses, Doppler assessment, capillary refill, and two-point discrimination. Evaluate for associated conditions such as hypothermia, trauma, hypoglycemia, intoxication, cardiac or neurologic illness, and compartment syndrome.
Diagnosis Tests And Interpretation
Lab
Not required for mild cases. Severe frostbite may require CBC, electrolytes, renal function, glucose, creatine kinase, urinalysis for myoglobinuria, and cultures if infection is suspected.
Imaging
Technetium-99 scintigraphy or MR angiography may help identify viable tissue early and guide surgical planning.
Diagnostic Procedures
Rapid rewarming is performed using a water bath maintained at 40–42°C. Temperatures outside this range increase risk of thermal injury or worsen tissue loss.
Differential Diagnosis
Frostnip causes reversible numbness without tissue injury. Trench foot results from prolonged wet cold exposure without ice crystal formation and presents with neurovascular compromise. Chilblains occur with chronic cold exposure and present as erythematous or cyanotic plaques.
Treatment Prehospital
Protect and immobilize affected areas. Remove wet or constrictive clothing. Avoid rubbing, massage, snow application, or dry rewarming if refreezing is possible. Treat hypothermia cautiously to prevent arrhythmias.
Initial Stabilization Therapy
Address airway, breathing, and circulation. Correct hypothermia. Provide IV fluids for severe cases. Minimize handling of frozen tissue.
ED Treatment Procedures
If injury is recent and not rewarmed, initiate rapid rewarming in a 40–42°C water bath for 15–30 minutes until tissue is pliable and erythematous. Provide aggressive analgesia with opioids and NSAIDs. Apply topical aloe vera to intact skin. Debride or aspirate clear blisters but avoid hemorrhagic blister intervention. Provide tetanus prophylaxis. Consider short-term antibiotics during hyperemic recovery for severe injuries. Elevate and splint affected areas and change dressings frequently. Avoid vasoconstrictive agents including nicotine. Thrombolytic therapy within 24 hours may improve tissue salvage and requires specialist consultation.
Medication
Aloe vera topical cream applied every 6 hours.
Ibuprofen 800 mg PO TID (pediatric dosing weight-based).
Morphine sulfate titrated IV or IM for pain control.
Antibiotics such as cephalexin, dicloxacillin, or ciprofloxacin when indicated.
Follow Up Disposition
Admission Criteria
All but minimal superficial injuries should be admitted, especially when refreezing risk exists.
Discharge Criteria
Only very mild superficial frostbite with reliable follow-up.
Issues For Referral
Consult burn, plastic, hand, or general surgery for all but the mildest cases.
Key Practice Insights And Common Pitfalls
Avoid freeze–thaw–refreeze cycles. Maintain correct rewarming temperature. Always address hypothermia and systemic illness. Consider compartment syndrome in pulseless or tense extremities.


- Published on
Emergency And Acute Medicine – Fournier Gangrene
Basics Description
Inadequate hygiene can lead to maceration and excoriation of scrotal skin, creating a portal of entry for bacteria. Once the skin barrier is disrupted, polymicrobial organisms spread rapidly along fascial planes of the perineum. Colles fascia fuses with the urogenital diaphragm, limiting posterior and lateral spread, while continuity of Buck and Scarpa fascia allows rapid anterior extension to the abdominal wall and lateral spread along the fascia lata. The testes and urethra are typically spared.
Most cases originate from three anatomic sources: lower urinary tract infections such as urethral strictures or indwelling catheters, penile or scrotal sources including condom catheters, hidradenitis, or balanitis, and anorectal sources such as fistulas, perirectal infections, or hemorrhoids. Rarely, intra-abdominal pathology including perforated appendicitis, diverticulitis, or pancreatitis may spread contiguously.
Etiology
Fournier gangrene is caused by polymicrobial infection involving mixed aerobic and anaerobic organisms that act synergistically to destroy tissue. End-arterial thrombosis in subcutaneous tissues creates an anaerobic environment that promotes rapid progression. Bacterial toxins and tissue necrosis factors contribute to systemic toxicity. Predisposing risk factors include trauma, diabetes mellitus, alcoholism, immunocompromised states, morbid obesity, and recent abdominal surgery.
Diagnosis Signs And Symptoms
This condition is a rapidly progressive necrotizing infection of the perineum involving subcutaneous tissue, fascia, and often muscle. It most commonly affects diabetic or immunocompromised patients. Early pain is often severe and out of proportion to physical findings; as necrosis progresses, affected tissue may become insensate. Associated symptoms include fever, chills, nausea, vomiting, urinary symptoms, lethargy, and inappropriate indifference to illness.
On examination, patients are often toxic appearing. Findings may include bronze or violaceous skin discoloration, thin brown malodorous discharge, ulceration, bullae, crepitus from subcutaneous air, frank necrosis, and eschar formation.
Essential Workup
Fournier gangrene is primarily a clinical diagnosis. A thorough history and focused examination of the perineum are critical. Evaluation for sepsis is mandatory, and early surgical consultation for emergent débridement is essential. Additional assessment should address underlying comorbidities such as diabetes or immunosuppression.
Diagnosis Tests And Interpretation
No laboratory test is diagnostic, but supportive findings include leukocytosis, anemia, electrolyte abnormalities, metabolic acidosis, renal failure, and possible disseminated intravascular coagulation. Urinalysis should be obtained. If diabetes is suspected or known, serum glucose, electrolytes, and ketones should be checked to evaluate for diabetic ketoacidosis. Blood, urine, and tissue cultures should be obtained when possible.
Imaging may show subcutaneous emphysema or ileus on plain pelvic radiographs. CT imaging is helpful when an intra-abdominal or ischiorectal source is suspected. Ultrasound may assist in differentiating Fournier gangrene from other causes of acute scrotum.
Differential Diagnosis
Epididymitis or orchitis, insect or human bites, perirectal infections, scrotal or inguinal abscess, scrotal cellulitis, testicular torsion, and tinea cruris.
Treatment
Prehospital care focuses on early recognition of septic shock with aggressive fluid resuscitation and vasopressor support if needed. Initial stabilization includes airway management, hemodynamic resuscitation, and avoidance of femoral venous access when possible.
Emergency department management requires immediate broad-spectrum intravenous antibiotics and emergent aggressive surgical débridement. Adjunctive hyperbaric oxygen therapy may be considered in coordination with surgical teams. Metabolic derangements, dehydration, anemia, and coagulopathy should be corrected, and tetanus prophylaxis administered as indicated.
Medication
Empiric antibiotic therapy should provide broad aerobic and anaerobic coverage and include agents such as ampicillin with clindamycin and gentamicin, or single-agent regimens like piperacillin–tazobactam, ampicillin–sulbactam, or carbapenems. Coverage for methicillin-resistant Staphylococcus aureus with vancomycin should be added when indicated. Insulin therapy is required for glycemic control, and vasopressors may be necessary for persistent hypotension.
Follow Up Disposition
All patients with Fournier gangrene require admission to a surgical intensive care unit. Mortality remains high despite treatment, emphasizing the importance of early recognition and aggressive management. Transfer to a facility capable of providing hyperbaric oxygen therapy should be considered when appropriate.
Key Practice Insights And Common Pitfalls
Failure to perform a careful genital and perineal examination can delay diagnosis. Delayed initiation of broad-spectrum antibiotics and surgical consultation significantly worsens outcomes. Early suspicion, prompt antibiotics, and immediate surgical intervention are critical to survival.
Basics Description
Inadequate hygiene can lead to maceration and excoriation of scrotal skin, creating a portal of entry for bacteria. Once the skin barrier is disrupted, polymicrobial organisms spread rapidly along fascial planes of the perineum. Colles fascia fuses with the urogenital diaphragm, limiting posterior and lateral spread, while continuity of Buck and Scarpa fascia allows rapid anterior extension to the abdominal wall and lateral spread along the fascia lata. The testes and urethra are typically spared.
Most cases originate from three anatomic sources: lower urinary tract infections such as urethral strictures or indwelling catheters, penile or scrotal sources including condom catheters, hidradenitis, or balanitis, and anorectal sources such as fistulas, perirectal infections, or hemorrhoids. Rarely, intra-abdominal pathology including perforated appendicitis, diverticulitis, or pancreatitis may spread contiguously.
Etiology
Fournier gangrene is caused by polymicrobial infection involving mixed aerobic and anaerobic organisms that act synergistically to destroy tissue. End-arterial thrombosis in subcutaneous tissues creates an anaerobic environment that promotes rapid progression. Bacterial toxins and tissue necrosis factors contribute to systemic toxicity. Predisposing risk factors include trauma, diabetes mellitus, alcoholism, immunocompromised states, morbid obesity, and recent abdominal surgery.
Diagnosis Signs And Symptoms
This condition is a rapidly progressive necrotizing infection of the perineum involving subcutaneous tissue, fascia, and often muscle. It most commonly affects diabetic or immunocompromised patients. Early pain is often severe and out of proportion to physical findings; as necrosis progresses, affected tissue may become insensate. Associated symptoms include fever, chills, nausea, vomiting, urinary symptoms, lethargy, and inappropriate indifference to illness.
On examination, patients are often toxic appearing. Findings may include bronze or violaceous skin discoloration, thin brown malodorous discharge, ulceration, bullae, crepitus from subcutaneous air, frank necrosis, and eschar formation.
Essential Workup
Fournier gangrene is primarily a clinical diagnosis. A thorough history and focused examination of the perineum are critical. Evaluation for sepsis is mandatory, and early surgical consultation for emergent débridement is essential. Additional assessment should address underlying comorbidities such as diabetes or immunosuppression.
Diagnosis Tests And Interpretation
No laboratory test is diagnostic, but supportive findings include leukocytosis, anemia, electrolyte abnormalities, metabolic acidosis, renal failure, and possible disseminated intravascular coagulation. Urinalysis should be obtained. If diabetes is suspected or known, serum glucose, electrolytes, and ketones should be checked to evaluate for diabetic ketoacidosis. Blood, urine, and tissue cultures should be obtained when possible.
Imaging may show subcutaneous emphysema or ileus on plain pelvic radiographs. CT imaging is helpful when an intra-abdominal or ischiorectal source is suspected. Ultrasound may assist in differentiating Fournier gangrene from other causes of acute scrotum.
Differential Diagnosis
Epididymitis or orchitis, insect or human bites, perirectal infections, scrotal or inguinal abscess, scrotal cellulitis, testicular torsion, and tinea cruris.
Treatment
Prehospital care focuses on early recognition of septic shock with aggressive fluid resuscitation and vasopressor support if needed. Initial stabilization includes airway management, hemodynamic resuscitation, and avoidance of femoral venous access when possible.
Emergency department management requires immediate broad-spectrum intravenous antibiotics and emergent aggressive surgical débridement. Adjunctive hyperbaric oxygen therapy may be considered in coordination with surgical teams. Metabolic derangements, dehydration, anemia, and coagulopathy should be corrected, and tetanus prophylaxis administered as indicated.
Medication
Empiric antibiotic therapy should provide broad aerobic and anaerobic coverage and include agents such as ampicillin with clindamycin and gentamicin, or single-agent regimens like piperacillin–tazobactam, ampicillin–sulbactam, or carbapenems. Coverage for methicillin-resistant Staphylococcus aureus with vancomycin should be added when indicated. Insulin therapy is required for glycemic control, and vasopressors may be necessary for persistent hypotension.
Follow Up Disposition
All patients with Fournier gangrene require admission to a surgical intensive care unit. Mortality remains high despite treatment, emphasizing the importance of early recognition and aggressive management. Transfer to a facility capable of providing hyperbaric oxygen therapy should be considered when appropriate.
Key Practice Insights And Common Pitfalls
Failure to perform a careful genital and perineal examination can delay diagnosis. Delayed initiation of broad-spectrum antibiotics and surgical consultation significantly worsens outcomes. Early suspicion, prompt antibiotics, and immediate surgical intervention are critical to survival.
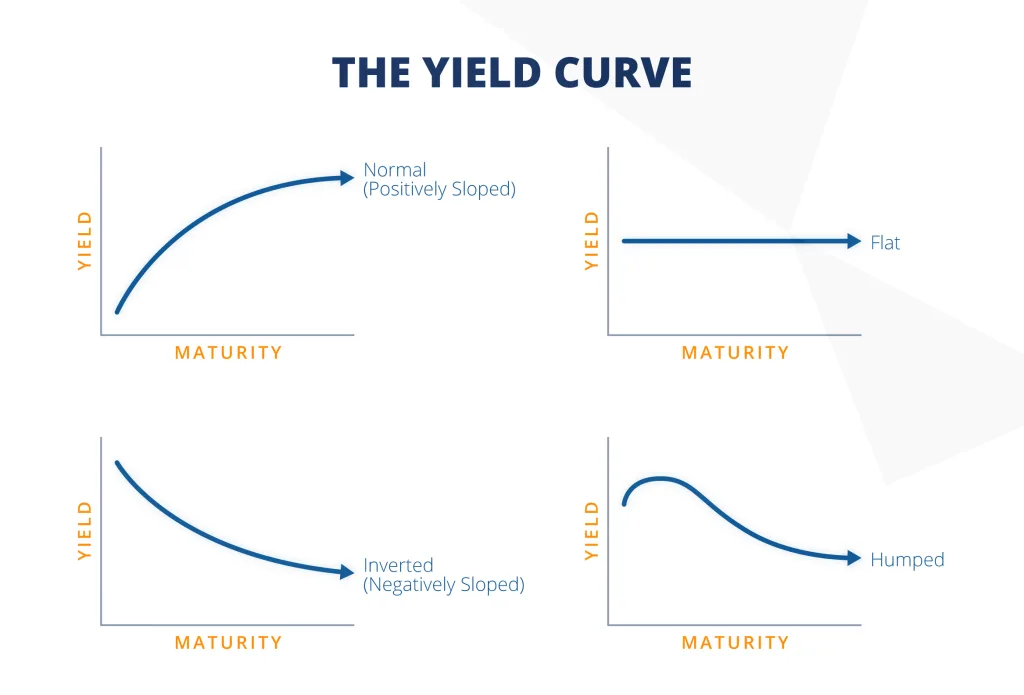
- Published on
Emergency And Acute Medicine – Foreign Body, Esophageal
Basics Description
Esophageal foreign bodies typically lodge at physiologic narrowing points: the cricopharyngeal muscle at C6 (≈63%, most common), the level of the aortic arch at T4 (≈10%), and the gastroesophageal junction at T11 (≈20%). Approximately 90% of ingested foreign bodies pass spontaneously, 10–20% require endoscopic removal, and fewer than 1% require surgical intervention.
Etiology
In adults and adolescents, food boluses and bones are most common. Risk is increased in edentulous patients, intoxicated individuals, and those with underlying esophageal pathology such as Schatzki B-rings or peptic strictures.
Pediatric ingestions account for about 80% of cases, most commonly between 6 months and 6 years of age, especially under 2 years. Coins are the most frequent pediatric esophageal foreign body. Additional pediatric constriction sites include the thoracic inlet (T1) and the tracheal bifurcation (T6).
Diagnosis Signs And Symptoms
Acute ingestion may cause dysphagia, odynophagia, drooling, gagging, choking, retching, blood-stained saliva, or chest discomfort. Chronically retained foreign bodies often present with respiratory symptoms such as cough, stridor, or hoarseness due to paraesophageal swelling compressing the airway.
Sharp object ingestion carries a 15–35% risk of esophageal perforation, with findings including neck swelling, erythema, crepitus, chest pain, pleurisy, or peritonitis.
Adults usually provide a clear history and often present within 24 hours. Children may be asymptomatic or present with drooling, refusal to eat, unexplained gagging, cough, wheeze, or choking; history may be unclear if ingestion was unwitnessed.
Essential Workup
Obtain a detailed history regarding the type, size, and timing of ingestion. Physical examination should assess for obstruction, perforation, aspiration, hemorrhage, and airway compromise, including evaluation of the neck, chest, lungs, abdomen, and oropharynx.
Diagnosis Tests And Interpretation
Biplane chest and neck radiographs are used to localize radiopaque foreign bodies; esophageal objects often align in the coronal plane. Signs of perforation include retropharyngeal air, cervical soft tissue air, or pneumomediastinum. Many bones and food boluses are radiolucent.
CT scanning is increasingly used for radiolucent objects and to detect perforation or infection.
Endoscopy is the diagnostic and therapeutic modality of choice, allowing direct visualization, removal, and evaluation of underlying mucosal pathology.
Differential Diagnosis
Globus sensation, esophagitis, esophageal mucosal irritation, croup, epiglottitis, upper respiratory tract infection, and retropharyngeal abscess.
Treatment
Prehospital care prioritizes airway protection and aspiration prevention; emetics and cathartics are contraindicated.
In the emergency department, airway, breathing, and circulation take priority. Direct laryngoscopy may remove very proximal objects.
Urgent endoscopy is indicated for sharp or elongated objects (>6 cm long or >2.5 cm wide), irregular edges, multiple objects (especially magnets), suspected perforation, airway compromise, food bolus with complete obstruction, foreign bodies present for more than 24 hours, or coins lodged at the cricopharyngeus in children.
Asymptomatic patients with smooth objects in the distal esophagus (excluding button batteries) may be observed for up to 24 hours.
Glucagon may be considered for recent distal food bolus impaction but is less effective with strictures and is falling out of favor.
Fluoroscopically guided Foley catheter extraction or bougienage may be used in selected cases by experienced providers.
Button batteries require emergent removal due to rapid liquefaction necrosis. Magnets require early GI or surgical consultation. Surgical intervention is reserved for failed endoscopic removal or complications.
Medication
Glucagon 1–2 mg IV may be used selectively for distal food bolus impaction after assessing for contraindications.
Follow Up Disposition
Admission is required for airway compromise, perforation, significant bleeding, migration of the foreign body, or failed removal.
Discharge is appropriate for asymptomatic patients after removal or confirmed passage into the stomach, with re-evaluation within 12–24 hours if distal esophageal objects are observed.
Follow Up Recommendations
GI referral is recommended when underlying esophageal pathology is suspected or for follow-up after complicated ingestions.
Key Practice Insights And Common Pitfalls
Always localize radiopaque foreign bodies with imaging and maintain a high index of suspicion for esophageal perforation, particularly with sharp objects or delayed presentation.
Basics Description
Esophageal foreign bodies typically lodge at physiologic narrowing points: the cricopharyngeal muscle at C6 (≈63%, most common), the level of the aortic arch at T4 (≈10%), and the gastroesophageal junction at T11 (≈20%). Approximately 90% of ingested foreign bodies pass spontaneously, 10–20% require endoscopic removal, and fewer than 1% require surgical intervention.
Etiology
In adults and adolescents, food boluses and bones are most common. Risk is increased in edentulous patients, intoxicated individuals, and those with underlying esophageal pathology such as Schatzki B-rings or peptic strictures.
Pediatric ingestions account for about 80% of cases, most commonly between 6 months and 6 years of age, especially under 2 years. Coins are the most frequent pediatric esophageal foreign body. Additional pediatric constriction sites include the thoracic inlet (T1) and the tracheal bifurcation (T6).
Diagnosis Signs And Symptoms
Acute ingestion may cause dysphagia, odynophagia, drooling, gagging, choking, retching, blood-stained saliva, or chest discomfort. Chronically retained foreign bodies often present with respiratory symptoms such as cough, stridor, or hoarseness due to paraesophageal swelling compressing the airway.
Sharp object ingestion carries a 15–35% risk of esophageal perforation, with findings including neck swelling, erythema, crepitus, chest pain, pleurisy, or peritonitis.
Adults usually provide a clear history and often present within 24 hours. Children may be asymptomatic or present with drooling, refusal to eat, unexplained gagging, cough, wheeze, or choking; history may be unclear if ingestion was unwitnessed.
Essential Workup
Obtain a detailed history regarding the type, size, and timing of ingestion. Physical examination should assess for obstruction, perforation, aspiration, hemorrhage, and airway compromise, including evaluation of the neck, chest, lungs, abdomen, and oropharynx.
Diagnosis Tests And Interpretation
Biplane chest and neck radiographs are used to localize radiopaque foreign bodies; esophageal objects often align in the coronal plane. Signs of perforation include retropharyngeal air, cervical soft tissue air, or pneumomediastinum. Many bones and food boluses are radiolucent.
CT scanning is increasingly used for radiolucent objects and to detect perforation or infection.
Endoscopy is the diagnostic and therapeutic modality of choice, allowing direct visualization, removal, and evaluation of underlying mucosal pathology.
Differential Diagnosis
Globus sensation, esophagitis, esophageal mucosal irritation, croup, epiglottitis, upper respiratory tract infection, and retropharyngeal abscess.
Treatment
Prehospital care prioritizes airway protection and aspiration prevention; emetics and cathartics are contraindicated.
In the emergency department, airway, breathing, and circulation take priority. Direct laryngoscopy may remove very proximal objects.
Urgent endoscopy is indicated for sharp or elongated objects (>6 cm long or >2.5 cm wide), irregular edges, multiple objects (especially magnets), suspected perforation, airway compromise, food bolus with complete obstruction, foreign bodies present for more than 24 hours, or coins lodged at the cricopharyngeus in children.
Asymptomatic patients with smooth objects in the distal esophagus (excluding button batteries) may be observed for up to 24 hours.
Glucagon may be considered for recent distal food bolus impaction but is less effective with strictures and is falling out of favor.
Fluoroscopically guided Foley catheter extraction or bougienage may be used in selected cases by experienced providers.
Button batteries require emergent removal due to rapid liquefaction necrosis. Magnets require early GI or surgical consultation. Surgical intervention is reserved for failed endoscopic removal or complications.
Medication
Glucagon 1–2 mg IV may be used selectively for distal food bolus impaction after assessing for contraindications.
Follow Up Disposition
Admission is required for airway compromise, perforation, significant bleeding, migration of the foreign body, or failed removal.
Discharge is appropriate for asymptomatic patients after removal or confirmed passage into the stomach, with re-evaluation within 12–24 hours if distal esophageal objects are observed.
Follow Up Recommendations
GI referral is recommended when underlying esophageal pathology is suspected or for follow-up after complicated ingestions.
Key Practice Insights And Common Pitfalls
Always localize radiopaque foreign bodies with imaging and maintain a high index of suspicion for esophageal perforation, particularly with sharp objects or delayed presentation.

- Published on
Emergency And Acute Medicine – Fracture, Open
Basics Description
An open fracture is defined by continuity between a skin violation and the fracture site, ranging from a small puncture wound to grossly exposed bone. These injuries represent a surgical urgency because delays in care significantly increase infection risk and complication rates. Certain factors increase morbidity, including massive soft tissue damage, severe wound contamination, compromised vascular supply, fracture instability, and host factors such as diabetes or peripheral vascular disease.
Etiology
Open fractures usually result from significant blunt trauma or penetrating injury.
Diagnosis Signs And Symptoms
Patients typically present with deformity and a nearby break in skin integrity. Neurovascular compromise may be present, and associated traumatic injuries are common.
History
A history of significant trauma is typical.
Physical Exam
Perform a complete neurologic and vascular examination of the affected limb. A thorough trauma evaluation is essential to identify associated injuries.
Essential Workup
Obtain plain radiographs including the joints above and below the injury. Additional diagnostic evaluation should be guided by the mechanism of injury and evidence of multisystem trauma.
Diagnosis Tests And Interpretation
Lab
CBC, basic chemistry panel, and coagulation studies are indicated for large-bone fractures (e.g., femur, pelvis) or in polytrauma. Type and screen or type and cross-match should be obtained if significant blood loss is anticipated. Pre- and post-débridement wound cultures have limited value and are not recommended.
Imaging
Doppler ultrasonography or angiography is indicated when vascular injury is suspected, such as with posterior knee dislocation, ischemic extremity, or extensive soft tissue damage in high-risk areas.
Diagnostic Procedures/Surgery
Measure compartment pressures if compartment syndrome is suspected. Consider saline or methylene blue arthrogram if joint violation is a concern. Angiography is warranted if noninvasive testing cannot adequately exclude vascular compromise.
Differential Diagnosis
Noncontiguous laceration or abrasion unrelated to the fracture site.
Treatment
Prehospital
Cover open wounds with moist, sterile dressings. Immobilize joints above and below the fracture. Control bleeding with direct pressure; use a tourniquet for traumatic amputations or uncontrolled hemorrhage. Apply gentle longitudinal traction if distal pulses are absent.
Initial Stabilization/Therapy
Prioritize airway, breathing, and circulation. Perform gentle reduction and immobilization when indicated.
ED Treatment/Procedures
Establish intravenous access and keep the patient NPO. Administer tetanus prophylaxis as indicated. Initiate intravenous antibiotics as early as possible to reduce infection risk. Minimize repeated wound exposure to prevent secondary contamination. Reassess frequently for compartment syndrome and neurovascular compromise. Certain large joint open fracture–dislocations (ankle, elbow, knee) require emergent reduction in the ED. Obtain urgent orthopedic consultation for formal irrigation, débridement, and possible operative fixation. Consult vascular surgery when vascular injury is suspected.
Medication
Cefazolin 1–2 g IM/IV (pediatric: 20 mg/kg).
Add gentamicin 1.5–2 mg/kg IV for severe or highly contaminated wounds (pediatric: 2–2.5 mg/kg).
Add penicillin G 4–5 million units IV for farm-related injuries, vascular injuries, or wounds at risk for Clostridium contamination (pediatric: 50,000 U/kg).
Tetanus booster 0.5 mL IM; tetanus immunoglobulin 250 IU IM if not previously immunized.
Morphine sulfate 2–10 mg IV (pediatric: 0.05–0.1 mg/kg per dose) or equivalent analgesia.
Pediatric Considerations
Administer DTaP booster in children younger than 7 years when indicated.
Follow Up Disposition
Admission Criteria
Most patients require admission for operative irrigation, débridement, intravenous antibiotics, and possible fixation.
Discharge Criteria
Selected simple open fractures may be irrigated and immobilized in the ED after orthopedic consultation, with discharge on oral antibiotics and close follow-up.
Issues For Referral
Nearly all open fractures require emergent orthopedic consultation and may necessitate trauma team involvement due to associated injuries.
Follow Up Recommendations
Patients discharged from the ED should be evaluated by an orthopedic surgeon within 1–2 days.
Key Practice Insights And Common Pitfalls
Open fractures are surgical urgencies requiring prompt antibiotics and orthopedic consultation. A high proportion of patients have associated traumatic injuries, which must not be overlooked. Early, thorough emergency department management significantly reduces morbidity and infection risk.
Basics Description
An open fracture is defined by continuity between a skin violation and the fracture site, ranging from a small puncture wound to grossly exposed bone. These injuries represent a surgical urgency because delays in care significantly increase infection risk and complication rates. Certain factors increase morbidity, including massive soft tissue damage, severe wound contamination, compromised vascular supply, fracture instability, and host factors such as diabetes or peripheral vascular disease.
Etiology
Open fractures usually result from significant blunt trauma or penetrating injury.
Diagnosis Signs And Symptoms
Patients typically present with deformity and a nearby break in skin integrity. Neurovascular compromise may be present, and associated traumatic injuries are common.
History
A history of significant trauma is typical.
Physical Exam
Perform a complete neurologic and vascular examination of the affected limb. A thorough trauma evaluation is essential to identify associated injuries.
Essential Workup
Obtain plain radiographs including the joints above and below the injury. Additional diagnostic evaluation should be guided by the mechanism of injury and evidence of multisystem trauma.
Diagnosis Tests And Interpretation
Lab
CBC, basic chemistry panel, and coagulation studies are indicated for large-bone fractures (e.g., femur, pelvis) or in polytrauma. Type and screen or type and cross-match should be obtained if significant blood loss is anticipated. Pre- and post-débridement wound cultures have limited value and are not recommended.
Imaging
Doppler ultrasonography or angiography is indicated when vascular injury is suspected, such as with posterior knee dislocation, ischemic extremity, or extensive soft tissue damage in high-risk areas.
Diagnostic Procedures/Surgery
Measure compartment pressures if compartment syndrome is suspected. Consider saline or methylene blue arthrogram if joint violation is a concern. Angiography is warranted if noninvasive testing cannot adequately exclude vascular compromise.
Differential Diagnosis
Noncontiguous laceration or abrasion unrelated to the fracture site.
Treatment
Prehospital
Cover open wounds with moist, sterile dressings. Immobilize joints above and below the fracture. Control bleeding with direct pressure; use a tourniquet for traumatic amputations or uncontrolled hemorrhage. Apply gentle longitudinal traction if distal pulses are absent.
Initial Stabilization/Therapy
Prioritize airway, breathing, and circulation. Perform gentle reduction and immobilization when indicated.
ED Treatment/Procedures
Establish intravenous access and keep the patient NPO. Administer tetanus prophylaxis as indicated. Initiate intravenous antibiotics as early as possible to reduce infection risk. Minimize repeated wound exposure to prevent secondary contamination. Reassess frequently for compartment syndrome and neurovascular compromise. Certain large joint open fracture–dislocations (ankle, elbow, knee) require emergent reduction in the ED. Obtain urgent orthopedic consultation for formal irrigation, débridement, and possible operative fixation. Consult vascular surgery when vascular injury is suspected.
Medication
Cefazolin 1–2 g IM/IV (pediatric: 20 mg/kg).
Add gentamicin 1.5–2 mg/kg IV for severe or highly contaminated wounds (pediatric: 2–2.5 mg/kg).
Add penicillin G 4–5 million units IV for farm-related injuries, vascular injuries, or wounds at risk for Clostridium contamination (pediatric: 50,000 U/kg).
Tetanus booster 0.5 mL IM; tetanus immunoglobulin 250 IU IM if not previously immunized.
Morphine sulfate 2–10 mg IV (pediatric: 0.05–0.1 mg/kg per dose) or equivalent analgesia.
Pediatric Considerations
Administer DTaP booster in children younger than 7 years when indicated.
Follow Up Disposition
Admission Criteria
Most patients require admission for operative irrigation, débridement, intravenous antibiotics, and possible fixation.
Discharge Criteria
Selected simple open fractures may be irrigated and immobilized in the ED after orthopedic consultation, with discharge on oral antibiotics and close follow-up.
Issues For Referral
Nearly all open fractures require emergent orthopedic consultation and may necessitate trauma team involvement due to associated injuries.
Follow Up Recommendations
Patients discharged from the ED should be evaluated by an orthopedic surgeon within 1–2 days.
Key Practice Insights And Common Pitfalls
Open fractures are surgical urgencies requiring prompt antibiotics and orthopedic consultation. A high proportion of patients have associated traumatic injuries, which must not be overlooked. Early, thorough emergency department management significantly reduces morbidity and infection risk.

