- Published on
Diagnostic Tests: Rouleaux Formations
Overview — What These Are
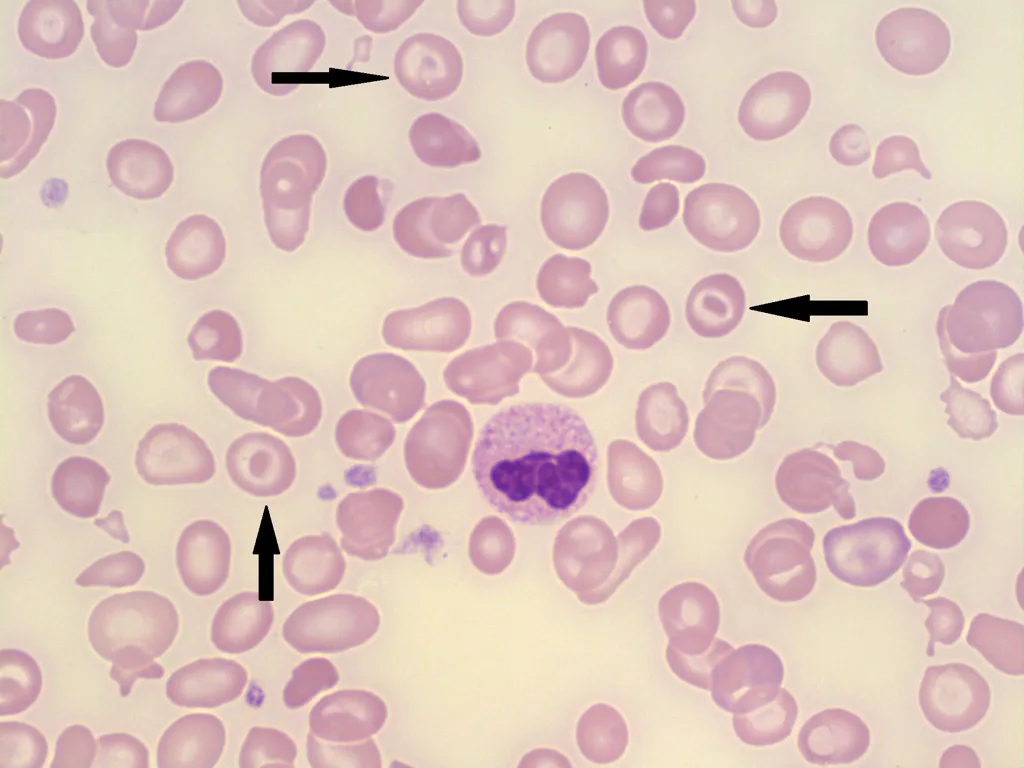
The structures shown are rouleaux formations, in which red blood cells stack together like coins. This stacking occurs when plasma proteins reduce the normal negative charge (zeta potential) between RBCs, allowing them to adhere to one another. Rouleaux formation is a nonspecific finding but often reflects elevated levels of certain plasma proteins.
Diseases Associated With Rouleaux Formation
Rouleaux commonly develops in conditions with increased abnormal globulins or elevated fibrinogen, including:
1. Multiple Myeloma
Other possible but less specific associations
But on board-style exams, multiple myeloma and macroglobulinemia are the classic associations.
Overview — What These Are
The structures shown are rouleaux formations, in which red blood cells stack together like coins. This stacking occurs when plasma proteins reduce the normal negative charge (zeta potential) between RBCs, allowing them to adhere to one another. Rouleaux formation is a nonspecific finding but often reflects elevated levels of certain plasma proteins.
Diseases Associated With Rouleaux Formation
Rouleaux commonly develops in conditions with increased abnormal globulins or elevated fibrinogen, including:
1. Multiple Myeloma
- Overproduction of monoclonal immunoglobulins (especially IgG) promotes RBC stacking.
- Supporting clues include:
- Anemia
- Hypercalcemia
- Renal failure
- Lytic bone lesions
- Abnormal SPEP (serum protein electrophoresis) or UPEP (urine protein electrophoresis) showing M-spik
- Characterized by high levels of IgM macroglobulin, which greatly increases blood viscosity.
- Also causes rouleaux due to elevated globulin levels.
Other possible but less specific associations
- Chronic inflammation
- Connective tissue disorders
- Certain infections
- Conditions with elevated fibrinogen (e.g., acute phase reactions)
But on board-style exams, multiple myeloma and macroglobulinemia are the classic associations.

- Published on
Diagnostic Tests: Spherocytes on Peripheral Smear
Overview — What These Are
The peripheral smear shows spherocytes, which are small, dense red blood cells lacking the normal central pallor. Their spherical shape results from loss of membrane surface area, making them less deformable and more prone to destruction, especially in the spleen. Spherocytes are a hallmark of hereditary spherocytosis, but can also appear in immune hemolysis.
Most Accurate Diagnostic Test
The most accurate diagnostic test for hereditary spherocytosis is the osmotic fragility test.
This test demonstrates that spherocytes lyse more easily than normal RBCs when placed in hypotonic solutions due to their decreased membrane surface area.
(Note: An elevated MCHC is supportive but not the most accurate test.)
Genetic Defect
Hereditary spherocytosis is caused by defects in red blood cell membrane proteins, most commonly involving:
Other possible but less common defects include band 3 and protein 4.2, but ankyrin/spectrin is the classic board answer.
When to Choose This Diagnosis/Test
You should think of hereditary spherocytosis—and choose osmotic fragility as the test—when the case involves:
Overview — What These Are
The peripheral smear shows spherocytes, which are small, dense red blood cells lacking the normal central pallor. Their spherical shape results from loss of membrane surface area, making them less deformable and more prone to destruction, especially in the spleen. Spherocytes are a hallmark of hereditary spherocytosis, but can also appear in immune hemolysis.
Most Accurate Diagnostic Test
The most accurate diagnostic test for hereditary spherocytosis is the osmotic fragility test.
This test demonstrates that spherocytes lyse more easily than normal RBCs when placed in hypotonic solutions due to their decreased membrane surface area.
(Note: An elevated MCHC is supportive but not the most accurate test.)
Genetic Defect
Hereditary spherocytosis is caused by defects in red blood cell membrane proteins, most commonly involving:
- Ankyrin gene mutation → leading to
- Spectrin deficiency → which
- Produces membrane instability and premature RBC destruction (extravascular hemolysis)
Other possible but less common defects include band 3 and protein 4.2, but ankyrin/spectrin is the classic board answer.
When to Choose This Diagnosis/Test
You should think of hereditary spherocytosis—and choose osmotic fragility as the test—when the case involves:
- Recurrent hemolysis
- Splenomegaly (often marked)
- Family history of anemia (autosomal dominant pattern in most cases)
- Increased MCHC on CBC (a high-yield clue)
- Spherocytes on peripheral smear
- Signs of hemolysis: jaundice, increased reticulocytes, gallstones (bilirubin stones)

- Published on
Diagnostic Tests: Sickled Cells
Overview — What This Is
The image shows sickled red blood cells, which are elongated, crescent-shaped RBCs formed due to polymerization of abnormal hemoglobin (HbS). Sickled cells are rigid, fragile, and prone to causing vaso-occlusion and hemolysis.
Diseases Associated With Sickled Cells
Sickled cells are seen only in:
Sickle Cell Disease (HbSS — Homozygous)
Important distinction:
Most Accurate Diagnostic Test
The most accurate test for diagnosing sickle cell disease is:
Hemoglobin Electrophoresis
This test identifies and quantifies hemoglobin variants and will show:
Electrophoresis provides definitive confirmation and distinguishes SS from AS and other hemoglobinopathies.
Overview — What This Is
The image shows sickled red blood cells, which are elongated, crescent-shaped RBCs formed due to polymerization of abnormal hemoglobin (HbS). Sickled cells are rigid, fragile, and prone to causing vaso-occlusion and hemolysis.
Diseases Associated With Sickled Cells
Sickled cells are seen only in:
Sickle Cell Disease (HbSS — Homozygous)
- Patients with homozygous hemoglobin S (SS) produce sickled cells, especially during episodes of dehydration, acidosis, hypoxia, or infection.
- These patients exhibit hemolytic anemia, vaso-occlusive crises, acute chest syndrome, splenic infarction, priapism, and other complications.
Important distinction:
- Sickle Cell Trait (AS — Heterozygous) does not produce sickled cells on a routine peripheral smear.
Individuals are generally hematologically normal, though they may sickle under extreme conditions (e.g., severe hypoxia).
Most Accurate Diagnostic Test
The most accurate test for diagnosing sickle cell disease is:
Hemoglobin Electrophoresis
This test identifies and quantifies hemoglobin variants and will show:
- HbS predominates in sickle cell disease (SS)
- A mixture of HbA and HbS in sickle cell trait (AS)
Electrophoresis provides definitive confirmation and distinguishes SS from AS and other hemoglobinopathies.
- Published on
Diagnostic Tests: Target Cells
Overview — What These Are?
The cells shown are target cells (codocytes). Target cells have a characteristic “bull’s-eye” appearance caused by an excess of cell membrane relative to cell volume. This altered surface-area–to–volume ratio creates a central area of hemoglobin surrounded by a pale ring and then an outer ring of hemoglobin.
Most Accurate Diagnostic Test
The most accurate diagnostic test when evaluating conditions associated with target cells is:
Hemoglobin Electrophoresis
This test helps identify hemoglobinopathies such as:
- Sickle cell disease
- Hemoglobin C disease
- Thalassemia
Electrophoresis will distinguish between different abnormal hemoglobins and determine specific genetic variants.
Associated Diseases
Target cells may appear in several hematologic and systemic conditions, including:
- Hemoglobinopathies
- Hemoglobin C disease (most strongly associated)
- Sickle cell disease (HbSS)
- Thalassemias (α and β)
- Liver disease
Due to increased membrane lipids, resulting in excess surface area. - Iron deficiency anemia
Though less classic, target cells may be seen in severe cases.
Do Target Cells Have a Shorter Survival?
Despite their abnormal morphology, target cells do NOT have a shorter survival than normal red blood cells.
They are structurally abnormal but not inherently more fragile, unlike spherocytes or sickled cells.

- Published on
Diagnostic Tests: Teardrop Cells
Overview — What the Peripheral Smear Shows
The smear demonstrates teardrop cells (also called dacrocytes). These red blood cells appear stretched into a teardrop shape, a sign that they were physically distorted during their passage out of a diseased bone marrow.
Diagnostic Significance — When This Is the Answer
When teardrop cells are shown or described in a question stem, the correct diagnostic answer is:
Infiltrative Bone Marrow Disease
The most classic and high-yield association is:
- Myelofibrosis (primary or secondary)
Additional supporting clues may include:
- Pancytopenia
- Massive splenomegaly
- Weight loss, fatigue, night sweats
- Leukoerythroblastic smear (nucleated RBCs + left-shifted myeloid cells)
Bone marrow biopsy in myelofibrosis will reveal reticulin or collagen fibrosis, often making aspiration difficult (“dry tap”).
The diagnosis is chosen after excluding other causes of massive splenomegaly, such as hairy cell leukemia.
- Published on
Diagnostic Tests – Papanicolaou (Pap) Smear
1. What Is a Pap Smear?
The Papanicolaou (Pap) smear is a cytologic screening test used to evaluate cells taken from the cervix in order to identify early precancerous changes or established cervical cancer. By examining exfoliated cervical cells under a microscope, clinicians can detect abnormalities caused primarily by high-risk HPV infections long before they progress to invasive disease. The Pap smear is one of the most effective screening tools in medicine and has significantly reduced cervical cancer mortality in populations where it is routinely used.
2. When Is Pap Smear the Correct Answer?
A Pap smear is indicated as a routine screening test for cervical cancer. Screening begins at age 21, regardless of sexual history, or earlier if guidelines specify onset within three years of first sexual activity; however, age 21 is the standard U.S. board-style answer. The test should be repeated every 2–3 years, depending on the screening strategy and incorporation of HPV co-testing. Screening may be discontinued at age 65 if the patient has had a history of adequate, consistently negative prior screenings and no recent abnormalities. Pap testing is used specifically for asymptomatic women as part of preventive care.
3. What Is the Next Best Test If Results Are Positive?
When a Pap smear shows abnormal cytology—whether atypical cells, low-grade changes, or high-grade lesions—the next step is to perform a colposcopy, during which the cervix is carefully examined under magnification. Suspicious areas are then biopsied to obtain tissue for definitive diagnosis. Colposcopy provides direct visualization of the transformation zone, allowing clinicians to identify the exact location and severity of cervical lesions and to determine appropriate management based on biopsy results.
1. What Is a Pap Smear?
The Papanicolaou (Pap) smear is a cytologic screening test used to evaluate cells taken from the cervix in order to identify early precancerous changes or established cervical cancer. By examining exfoliated cervical cells under a microscope, clinicians can detect abnormalities caused primarily by high-risk HPV infections long before they progress to invasive disease. The Pap smear is one of the most effective screening tools in medicine and has significantly reduced cervical cancer mortality in populations where it is routinely used.
2. When Is Pap Smear the Correct Answer?
A Pap smear is indicated as a routine screening test for cervical cancer. Screening begins at age 21, regardless of sexual history, or earlier if guidelines specify onset within three years of first sexual activity; however, age 21 is the standard U.S. board-style answer. The test should be repeated every 2–3 years, depending on the screening strategy and incorporation of HPV co-testing. Screening may be discontinued at age 65 if the patient has had a history of adequate, consistently negative prior screenings and no recent abnormalities. Pap testing is used specifically for asymptomatic women as part of preventive care.
3. What Is the Next Best Test If Results Are Positive?
When a Pap smear shows abnormal cytology—whether atypical cells, low-grade changes, or high-grade lesions—the next step is to perform a colposcopy, during which the cervix is carefully examined under magnification. Suspicious areas are then biopsied to obtain tissue for definitive diagnosis. Colposcopy provides direct visualization of the transformation zone, allowing clinicians to identify the exact location and severity of cervical lesions and to determine appropriate management based on biopsy results.

- Published on
Diagnostic Tests – PET Scanning
1. What Is a PET Scan?
A PET scan, or positron emission tomography, is an imaging technique that evaluates the metabolic activity of tissues rather than just their anatomical structure. Unlike CT or MRI, which show size, shape, and location, a PET scan uses a radioactive glucose analog—most commonly 18-fluorodeoxyglucose (FDG)—to assess how active a lesion is metabolically. Cancer cells typically have high glucose consumption, so they absorb more FDG and appear as areas of increased signal. PET scanning is noninvasive and is frequently used to determine whether a mass seen on other imaging studies is biologically active or whether it represents benign or inactive tissue.
2. What Makes a PET Scan Abnormal?
A PET scan is considered abnormal when there is increased uptake of FDG, indicating heightened metabolic activity. Malignant cells consume glucose rapidly because of their elevated growth and division rates, so they typically “light up” on PET imaging. Some infections, granulomatous diseases (e.g., TB, sarcoidosis), and inflammatory processes can also show increased uptake, which is why PET is not 100% specific for cancer. However, a low or absent uptake suggests that a lesion is metabolically inactive or benign, even if it appears concerning on CT or MRI.
3. When Is PET Scan the Correct Answer?
PET scanning is particularly useful when evaluating whether a lesion—such as a lung mass—is truly malignant or whether areas seen on CT represent metastatic disease. In oncology cases, PET is the answer when determining the functional status of a suspicious mass or when assessing for occult metastasis before deciding on surgical management. For example, if a patient is diagnosed with a localized lung tumor, a PET scan helps determine if there are metabolically active lesions elsewhere in the chest or body. If a contralateral mass or mediastinal lymph node lights up on PET, the disease is considered metastatic and surgery is no longer curative. Conversely, if additional lesions show low uptake, they are likely benign, and the patient may proceed safely to surgery to remove the primary tumor.
1. What Is a PET Scan?
A PET scan, or positron emission tomography, is an imaging technique that evaluates the metabolic activity of tissues rather than just their anatomical structure. Unlike CT or MRI, which show size, shape, and location, a PET scan uses a radioactive glucose analog—most commonly 18-fluorodeoxyglucose (FDG)—to assess how active a lesion is metabolically. Cancer cells typically have high glucose consumption, so they absorb more FDG and appear as areas of increased signal. PET scanning is noninvasive and is frequently used to determine whether a mass seen on other imaging studies is biologically active or whether it represents benign or inactive tissue.
2. What Makes a PET Scan Abnormal?
A PET scan is considered abnormal when there is increased uptake of FDG, indicating heightened metabolic activity. Malignant cells consume glucose rapidly because of their elevated growth and division rates, so they typically “light up” on PET imaging. Some infections, granulomatous diseases (e.g., TB, sarcoidosis), and inflammatory processes can also show increased uptake, which is why PET is not 100% specific for cancer. However, a low or absent uptake suggests that a lesion is metabolically inactive or benign, even if it appears concerning on CT or MRI.
3. When Is PET Scan the Correct Answer?
PET scanning is particularly useful when evaluating whether a lesion—such as a lung mass—is truly malignant or whether areas seen on CT represent metastatic disease. In oncology cases, PET is the answer when determining the functional status of a suspicious mass or when assessing for occult metastasis before deciding on surgical management. For example, if a patient is diagnosed with a localized lung tumor, a PET scan helps determine if there are metabolically active lesions elsewhere in the chest or body. If a contralateral mass or mediastinal lymph node lights up on PET, the disease is considered metastatic and surgery is no longer curative. Conversely, if additional lesions show low uptake, they are likely benign, and the patient may proceed safely to surgery to remove the primary tumor.

- Published on
Diagnostic Tests – Haptoglobin Levels
1. What Is Haptoglobin?
Haptoglobin is a plasma protein that binds freely circulating hemoglobin released from red blood cells during hemolysis. Under normal conditions, haptoglobin levels remain stable because little free hemoglobin circulates in the bloodstream. However, when red blood cells rupture—whether due to immune destruction, mechanical trauma, or inherited hemolytic disorders—large amounts of hemoglobin spill into the plasma. Haptoglobin binds this hemoglobin, forming complexes that are removed from circulation by the reticuloendothelial system. As a result, serum haptoglobin levels fall, making low haptoglobin a key indicator of intravascular hemolysis. Hemolysis is also typically accompanied by elevated LDH, increased reticulocyte count, and elevated indirect bilirubin due to increased RBC breakdown and compensatory marrow response.
2. When Do You Answer a Haptoglobin Level?
Haptoglobin should be ordered when a clinical scenario suggests acute hemolysis, particularly when a patient develops sudden-onset anemia that cannot be explained by gastrointestinal bleeding or other obvious sources of blood loss. Features that point toward hemolysis include jaundice, dark urine, elevated LDH, or a rapid drop in hemoglobin without external bleeding. In board-style questions, a combination such as acute anemia + no GI bleeding = hemolysis, making haptoglobin part of the appropriate workup. The test helps confirm hemolysis and distinguish it from other causes of anemia.
1. What Is Haptoglobin?
Haptoglobin is a plasma protein that binds freely circulating hemoglobin released from red blood cells during hemolysis. Under normal conditions, haptoglobin levels remain stable because little free hemoglobin circulates in the bloodstream. However, when red blood cells rupture—whether due to immune destruction, mechanical trauma, or inherited hemolytic disorders—large amounts of hemoglobin spill into the plasma. Haptoglobin binds this hemoglobin, forming complexes that are removed from circulation by the reticuloendothelial system. As a result, serum haptoglobin levels fall, making low haptoglobin a key indicator of intravascular hemolysis. Hemolysis is also typically accompanied by elevated LDH, increased reticulocyte count, and elevated indirect bilirubin due to increased RBC breakdown and compensatory marrow response.
2. When Do You Answer a Haptoglobin Level?
Haptoglobin should be ordered when a clinical scenario suggests acute hemolysis, particularly when a patient develops sudden-onset anemia that cannot be explained by gastrointestinal bleeding or other obvious sources of blood loss. Features that point toward hemolysis include jaundice, dark urine, elevated LDH, or a rapid drop in hemoglobin without external bleeding. In board-style questions, a combination such as acute anemia + no GI bleeding = hemolysis, making haptoglobin part of the appropriate workup. The test helps confirm hemolysis and distinguish it from other causes of anemia.

- Published on
Diagnostic Tests – Factor V Leiden Mutation
1. What Is Factor V Leiden?
Factor V Leiden is a genetic mutation that makes Factor V resistant to the inhibitory action of activated protein C (APC), one of the body’s natural anticoagulants. Normally, protein C slows the clotting cascade by inactivating Factor V; however, the Factor V Leiden mutation alters the structure of Factor V so that it no longer responds effectively to protein C. As a result, clotting continues unchecked, creating a hypercoagulable state. This condition is the most common inherited thrombophilia, significantly increasing a person’s risk of developing venous thromboembolism (VTE) such as deep vein thrombosis (DVT) or pulmonary embolism (PE).
2. When Do You Answer Factor V Leiden Mutation Testing?
Testing for the Factor V Leiden mutation is indicated in young patients who present with an unprovoked DVT or PE, especially when the event occurs without clear provoking factors such as recent surgery, trauma, or immobilization. Board-style scenarios often feature:
In these cases, Factor V Leiden testing is the most accurate test for identifying a hereditary cause of hypercoagulability. It is part of the evaluation when considering inherited thrombophilias.
3. What Other Tests Should Be Sent With It?
When evaluating a patient for possible inherited or acquired hypercoagulable states, several additional tests are typically ordered alongside Factor V Leiden. These include:
Together, these tests help create a comprehensive picture of a patient’s thrombotic risk and identify whether the cause is inherited, acquired, or multifactorial.
1. What Is Factor V Leiden?
Factor V Leiden is a genetic mutation that makes Factor V resistant to the inhibitory action of activated protein C (APC), one of the body’s natural anticoagulants. Normally, protein C slows the clotting cascade by inactivating Factor V; however, the Factor V Leiden mutation alters the structure of Factor V so that it no longer responds effectively to protein C. As a result, clotting continues unchecked, creating a hypercoagulable state. This condition is the most common inherited thrombophilia, significantly increasing a person’s risk of developing venous thromboembolism (VTE) such as deep vein thrombosis (DVT) or pulmonary embolism (PE).
2. When Do You Answer Factor V Leiden Mutation Testing?
Testing for the Factor V Leiden mutation is indicated in young patients who present with an unprovoked DVT or PE, especially when the event occurs without clear provoking factors such as recent surgery, trauma, or immobilization. Board-style scenarios often feature:
- A first-time clot in a young adult
- A thrombotic event after a long airplane flight or prolonged immobility
- A family history of recurrent clots
In these cases, Factor V Leiden testing is the most accurate test for identifying a hereditary cause of hypercoagulability. It is part of the evaluation when considering inherited thrombophilias.
3. What Other Tests Should Be Sent With It?
When evaluating a patient for possible inherited or acquired hypercoagulable states, several additional tests are typically ordered alongside Factor V Leiden. These include:
- Protein S levels – Low levels increase clotting risk.
- Protein C levels – Especially important when the case mentions skin necrosis, which may occur when patients with undiagnosed protein C deficiency receive warfarin.
- Lupus anticoagulant testing – Consider this when the patient has an unexplained prolonged PTT, recurrent spontaneous abortions, or autoimmune features; this suggests antiphospholipid syndrome.
- Antithrombin III deficiency testing – Suspect this when a patient shows resistance to heparin, as AT III is required for heparin’s anticoagulant effect.
Together, these tests help create a comprehensive picture of a patient’s thrombotic risk and identify whether the cause is inherited, acquired, or multifactorial.

- Published on
Diagnostic Tests – Sentinel Node Evaluation
1. What Is Sentinel Node Evaluation?
Sentinel node evaluation, or sentinel lymph node biopsy (SLNB), is a diagnostic procedure used primarily in the management of breast cancer (and also melanoma). Its purpose is to determine whether cancer has begun to spread beyond the primary tumor into the regional lymph nodes. Because cancer metastasizes in an orderly fashion through lymphatic drainage, the sentinel node—the first lymph node that receives lymph flow from the tumor site—acts as an early indicator of metastatic spread. Examining this node helps determine staging, prognosis, and the need for further lymph node removal.
2. How Is Sentinel Node Evaluation Done?
The procedure involves injecting a tracer dye, radioactive substance, or both into the breast at or near the tumor or biopsy cavity during surgery. This material travels through the lymphatic system, and the first lymph node it reaches is identified as the sentinel node. The surgeon then removes this node and sends it for pathological analysis.
3. When Is Sentinel Node Evaluation the Correct Answer?
A sentinel node biopsy is indicated after a diagnosis of breast cancer has already been established through either needle biopsy or excisional biopsy. You should choose sentinel node evaluation in cases where the patient has:
At this point, SLNB becomes the next best step because it provides essential staging information and helps determine whether cancer has begun to spread to the lymph nodes. It is particularly valuable because it can replace the need for full axillary lymph node dissection in patients whose sentinel node is free of cancer, thereby reducing surgical complications while still providing accurate staging.
1. What Is Sentinel Node Evaluation?
Sentinel node evaluation, or sentinel lymph node biopsy (SLNB), is a diagnostic procedure used primarily in the management of breast cancer (and also melanoma). Its purpose is to determine whether cancer has begun to spread beyond the primary tumor into the regional lymph nodes. Because cancer metastasizes in an orderly fashion through lymphatic drainage, the sentinel node—the first lymph node that receives lymph flow from the tumor site—acts as an early indicator of metastatic spread. Examining this node helps determine staging, prognosis, and the need for further lymph node removal.
2. How Is Sentinel Node Evaluation Done?
The procedure involves injecting a tracer dye, radioactive substance, or both into the breast at or near the tumor or biopsy cavity during surgery. This material travels through the lymphatic system, and the first lymph node it reaches is identified as the sentinel node. The surgeon then removes this node and sends it for pathological analysis.
- If the sentinel node contains cancer cells, this indicates lymphatic spread, and a full axillary lymph node dissection may be performed to remove additional nodes.
- If the sentinel node is negative, it suggests that cancer has not yet metastasized regionally, and axillary dissection can be safely avoided, sparing the patient significant morbidity such as lymphedema.
3. When Is Sentinel Node Evaluation the Correct Answer?
A sentinel node biopsy is indicated after a diagnosis of breast cancer has already been established through either needle biopsy or excisional biopsy. You should choose sentinel node evaluation in cases where the patient has:
- An abnormal mammogram
- A breast mass that has been biopsied
- Confirmed invasive breast cancer
At this point, SLNB becomes the next best step because it provides essential staging information and helps determine whether cancer has begun to spread to the lymph nodes. It is particularly valuable because it can replace the need for full axillary lymph node dissection in patients whose sentinel node is free of cancer, thereby reducing surgical complications while still providing accurate staging.

