- Published on
Infectious Disease - Botulism
Fundamental Description: A syndrome caused by neurotoxins released by Clostridium botulinum. Botulinum neurotoxin (BoNT) ranks among the most hazardous chemicals recognized by humanity.
• Botulism manifests in five epidemiological types. – Foodborne botulism – Infant botulism – Wound botulism – Intestinal colonization and adult infectious botulism – Inhalational botulism
Incubation: Symptoms manifest 12–36 hours post-ingestion of the poison.
EPIDEMIOLOGY
Incidence
• Botulism is an uncommon yet potentially fatal condition. • Minor outbreaks may result from either commercially or home-canned foods.
In the United States, the majority of instances arise in babies, with roughly one-fourth attributed to dietary sources and a minor proportion resulting from wounds.
RISK FACTORS
Homemade food fermentation combined with home canning elevates dangers.
The mortality rate is elevated in patients above 60 years of age. The consumption of honey by newborns poses a danger for gastrointestinal colonization and toxin generation.
Iatrogenic botulism has been documented following the administration of unapproved botulinum toxin A.
Physicians must recognize the potential for wound botulism among intravenous drug users.
GENERAL PREVENTION MEASURES
• Exercise caution while canning low-acid foods, including corn, asparagus, beans, and beets.
• If goods have been home-canned, boil them for 10 minutes before consumption.
Avoid administering honey to infants under one year of age.
• Conduct an expedited assessment of prospective cases to prevent possible epidemics.
Avoid consuming food from bulging cans.
ETIOLOGY
• C. botulinum comprises a group of anaerobic, gram-positive bacilli that generate spores and highly potent neurotoxins.
The organism is classified from A to G based on the antibodies generated against the produced neurotoxic.
Human disease is linked to toxin types A, B, E, and F.
Type A is frequently located in the western United States and China.
Type B is located in the eastern United States and Europe.
Type F is prevalent in Alaska, has a global distribution, and is frequently linked to fish items.
• Spores are located in soil and marine sediment.
• Spores withstand boiling but can be eradicated by heating to 120°C.
• Owing to its extreme toxicity, BoNT is regarded as a possible biological warfare agent.
DIAGNOSIS
• Bilateral cranial neuropathies • Bilateral descending weakness • Absence of fever • The patient remains conscious and alert as the syndrome advances • No sensory abnormalities are present. Clinical suspicion is fundamental for diagnosis.
DIAGNOSTIC TESTS AND INTERPRETATION LABORATORY
• Identification of the toxin in serum, feces, or food samples • The sensitivity of the mouse bioassay has recently been established at 68% in patients with wound botulism
DIFFERENTIAL DIAGNOSIS
• Myasthenia gravis • Eaton–Lambert syndrome • Tick paralysis • Miller Fisher form of Guillain–Barré syndrome
• Cerebrovascular accident • Poliomyelitis • Heavy metal poisoning
ADDITIONAL TREATMENT
Comprehensive Strategies
• Supportive care is provided. • Antitoxin is available, targeting toxin types A, B, and E. • Antibiotic therapy is supplied for wound botulism following antitoxin administration. • Intravenous human botulism immunoglobulin (BIG-IV) has been produced and utilized in newborns. It should be administered promptly at the onset of the sickness.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
• Patients frequently require extended rehabilitation. • In comparison to controls, those who recovered from botulism were more prone to experience weariness, weakness, dizziness, and respiratory difficulties.
Fundamental Description: A syndrome caused by neurotoxins released by Clostridium botulinum. Botulinum neurotoxin (BoNT) ranks among the most hazardous chemicals recognized by humanity.
• Botulism manifests in five epidemiological types. – Foodborne botulism – Infant botulism – Wound botulism – Intestinal colonization and adult infectious botulism – Inhalational botulism
Incubation: Symptoms manifest 12–36 hours post-ingestion of the poison.
EPIDEMIOLOGY
Incidence
• Botulism is an uncommon yet potentially fatal condition. • Minor outbreaks may result from either commercially or home-canned foods.
In the United States, the majority of instances arise in babies, with roughly one-fourth attributed to dietary sources and a minor proportion resulting from wounds.
RISK FACTORS
Homemade food fermentation combined with home canning elevates dangers.
The mortality rate is elevated in patients above 60 years of age. The consumption of honey by newborns poses a danger for gastrointestinal colonization and toxin generation.
Iatrogenic botulism has been documented following the administration of unapproved botulinum toxin A.
Physicians must recognize the potential for wound botulism among intravenous drug users.
GENERAL PREVENTION MEASURES
• Exercise caution while canning low-acid foods, including corn, asparagus, beans, and beets.
• If goods have been home-canned, boil them for 10 minutes before consumption.
Avoid administering honey to infants under one year of age.
• Conduct an expedited assessment of prospective cases to prevent possible epidemics.
Avoid consuming food from bulging cans.
ETIOLOGY
• C. botulinum comprises a group of anaerobic, gram-positive bacilli that generate spores and highly potent neurotoxins.
The organism is classified from A to G based on the antibodies generated against the produced neurotoxic.
Human disease is linked to toxin types A, B, E, and F.
Type A is frequently located in the western United States and China.
Type B is located in the eastern United States and Europe.
Type F is prevalent in Alaska, has a global distribution, and is frequently linked to fish items.
• Spores are located in soil and marine sediment.
• Spores withstand boiling but can be eradicated by heating to 120°C.
• Owing to its extreme toxicity, BoNT is regarded as a possible biological warfare agent.
DIAGNOSIS
• Bilateral cranial neuropathies • Bilateral descending weakness • Absence of fever • The patient remains conscious and alert as the syndrome advances • No sensory abnormalities are present. Clinical suspicion is fundamental for diagnosis.
DIAGNOSTIC TESTS AND INTERPRETATION LABORATORY
• Identification of the toxin in serum, feces, or food samples • The sensitivity of the mouse bioassay has recently been established at 68% in patients with wound botulism
DIFFERENTIAL DIAGNOSIS
• Myasthenia gravis • Eaton–Lambert syndrome • Tick paralysis • Miller Fisher form of Guillain–Barré syndrome
• Cerebrovascular accident • Poliomyelitis • Heavy metal poisoning
ADDITIONAL TREATMENT
Comprehensive Strategies
• Supportive care is provided. • Antitoxin is available, targeting toxin types A, B, and E. • Antibiotic therapy is supplied for wound botulism following antitoxin administration. • Intravenous human botulism immunoglobulin (BIG-IV) has been produced and utilized in newborns. It should be administered promptly at the onset of the sickness.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
• Patients frequently require extended rehabilitation. • In comparison to controls, those who recovered from botulism were more prone to experience weariness, weakness, dizziness, and respiratory difficulties.

- Published on
Infectious Disease- Blepharitis and Chalazion
BASICS DESCRIPTION • Blepharitis is an eyelid infection characterized by inflammation of the lid edges. It encompasses the subsequent elements:
- Anterior – inflammation near the follicular root of the eyelashes – Posterior – internal segment of the eyelid – Granulomatous
Chalazion is a painless, granulomatous infection of a meibomian gland resulting in a nodule in the eyelid.
EPIDEMIOLOGY Incidence • Blepharitis is a prevalent ailment encountered by primary care physicians and ophthalmologists.
Posterior blepharitis is typically linked to rosacea and seborrheic dermatitis.
FACTORS OF RISK
Over seventy-five percent of individuals with blepharitis linked to atopic dermatitis exhibit a positive culture for Staphylococcus aureus. A positive culture does not inherently indicate an active infection, making clinical correlation essential.
PATHOPHYSIOLOGY • Bacterial organisms may influence meibomian gland secretion. • Associated alterations in the secretions from meibomian glands may also occur.
ETIOLOGY • Nearly all infections that impact the skin and colonize the eyelids from adjacent regions, such as the scalp and nostrils, can lead to infectious illnesses of the eyelid (1).
The predominant etiological agents are Staphylococcus species, especially Staphylococcus aureus. Additional pathogens encompass the following:
Bacillus anthracis, Bacillus cereus, Blastomyces dermatitidis, Candida species, Clostridium species, Cryptococcus neoformans
– Haemophilus ducreyi – Herpes simplex virus – Herpes zoster virus – Moraxella spp – Mycobacterium TB – Mycobacterium leprae – Phthirus pubis – Poxvirus spp – Proteus mirabilis – Pseudomonas spp – Streptococcus spp – Vaccinia virus
FREQUENTLY CO-OCCURRING CONDITIONS
• Rosacea • Seborrheic dermatitis
DIAGNOSTIC HISTORY
• Common symptoms encompass persistent irritation, a burning sensation, slight erythema, and intermittent pruritus of the eyelids.
• Certain patients report experiencing clouded eyesight
PHYSICAL EXAMINATION
• Acute blepharitis is characterized by the presence of pus collections and an ulcerative margin. • • Chronic blepharitis typically presents with loss or misdirection of eyelashes, telangiectasia, and a swollen lid margin.
Superficial eyelid involvement is the predominant manifestation of staphylococcal eyelid illness, typically characterized by hyperemia and telangiectasia at the eyelid edge.
DIAGNOSTIC TESTS AND INTERPRETATION
Imaging
Ophthalmologists may perform slit lamp examinations.
TREATMENT MEDICATION
• Typically, the management of blepharitis involves warm compresses, rigorous eyelid cleanliness, and topical antibiotics (2).
A firm massage utilizing a 50:50 blend of baby shampoo and water with a cotton-tipped applicator promotes the release of oils from the meibomian glands.
Topical ocular treatments for staphylococcal blepharitis comprise bacitracin or erythromycin (either b.i.d. or q.i.d. for 2 weeks), gentamicin, and 1% mercuric oxide.
In chronic instances of blepharitis, cultures should be collected when patients exhibit persistent blepharitis unresponsive to topical medicines. Systemic antibiotics applicable in these instances include dicloxacillin (500 mg q.i.d.), quinolones, or azithromycin.
• In cases of persistent, nontender chalazion, incision and curettage may be performed. The inflammatory material can be excised through a vertical or, if required, a horizontal conjunctival incision. In the absence of infection, corticosteroids may be administered via intralesional injection.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
In rare instances of necrotizing fasciitis affecting the eyelids, immediate surgical debridement is required.
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Basal cell carcinoma, squamous cell carcinoma, or meibomian gland carcinoma should be considered for any nonhealing, ulcerative eyelid lesion.
COMPLICATIONS
An external hordeolum (stye) results from a staphylococcal infection of the superficial accessory glands of Zeis or Moll, situated near the eyelid borders. An internal hordeolum arises from a suppurative infection of the oil-secreting meibomian glands located within the tarsal plate of the eyelid
BASICS DESCRIPTION • Blepharitis is an eyelid infection characterized by inflammation of the lid edges. It encompasses the subsequent elements:
- Anterior – inflammation near the follicular root of the eyelashes – Posterior – internal segment of the eyelid – Granulomatous
Chalazion is a painless, granulomatous infection of a meibomian gland resulting in a nodule in the eyelid.
EPIDEMIOLOGY Incidence • Blepharitis is a prevalent ailment encountered by primary care physicians and ophthalmologists.
Posterior blepharitis is typically linked to rosacea and seborrheic dermatitis.
FACTORS OF RISK
Over seventy-five percent of individuals with blepharitis linked to atopic dermatitis exhibit a positive culture for Staphylococcus aureus. A positive culture does not inherently indicate an active infection, making clinical correlation essential.
PATHOPHYSIOLOGY • Bacterial organisms may influence meibomian gland secretion. • Associated alterations in the secretions from meibomian glands may also occur.
ETIOLOGY • Nearly all infections that impact the skin and colonize the eyelids from adjacent regions, such as the scalp and nostrils, can lead to infectious illnesses of the eyelid (1).
The predominant etiological agents are Staphylococcus species, especially Staphylococcus aureus. Additional pathogens encompass the following:
Bacillus anthracis, Bacillus cereus, Blastomyces dermatitidis, Candida species, Clostridium species, Cryptococcus neoformans
– Haemophilus ducreyi – Herpes simplex virus – Herpes zoster virus – Moraxella spp – Mycobacterium TB – Mycobacterium leprae – Phthirus pubis – Poxvirus spp – Proteus mirabilis – Pseudomonas spp – Streptococcus spp – Vaccinia virus
FREQUENTLY CO-OCCURRING CONDITIONS
• Rosacea • Seborrheic dermatitis
DIAGNOSTIC HISTORY
• Common symptoms encompass persistent irritation, a burning sensation, slight erythema, and intermittent pruritus of the eyelids.
• Certain patients report experiencing clouded eyesight
PHYSICAL EXAMINATION
• Acute blepharitis is characterized by the presence of pus collections and an ulcerative margin. • • Chronic blepharitis typically presents with loss or misdirection of eyelashes, telangiectasia, and a swollen lid margin.
Superficial eyelid involvement is the predominant manifestation of staphylococcal eyelid illness, typically characterized by hyperemia and telangiectasia at the eyelid edge.
DIAGNOSTIC TESTS AND INTERPRETATION
Imaging
Ophthalmologists may perform slit lamp examinations.
TREATMENT MEDICATION
• Typically, the management of blepharitis involves warm compresses, rigorous eyelid cleanliness, and topical antibiotics (2).
A firm massage utilizing a 50:50 blend of baby shampoo and water with a cotton-tipped applicator promotes the release of oils from the meibomian glands.
Topical ocular treatments for staphylococcal blepharitis comprise bacitracin or erythromycin (either b.i.d. or q.i.d. for 2 weeks), gentamicin, and 1% mercuric oxide.
In chronic instances of blepharitis, cultures should be collected when patients exhibit persistent blepharitis unresponsive to topical medicines. Systemic antibiotics applicable in these instances include dicloxacillin (500 mg q.i.d.), quinolones, or azithromycin.
• In cases of persistent, nontender chalazion, incision and curettage may be performed. The inflammatory material can be excised through a vertical or, if required, a horizontal conjunctival incision. In the absence of infection, corticosteroids may be administered via intralesional injection.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
In rare instances of necrotizing fasciitis affecting the eyelids, immediate surgical debridement is required.
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Basal cell carcinoma, squamous cell carcinoma, or meibomian gland carcinoma should be considered for any nonhealing, ulcerative eyelid lesion.
COMPLICATIONS
An external hordeolum (stye) results from a staphylococcal infection of the superficial accessory glands of Zeis or Moll, situated near the eyelid borders. An internal hordeolum arises from a suppurative infection of the oil-secreting meibomian glands located within the tarsal plate of the eyelid

- Published on
Infectious Disease – Blastomycosis
FUNDAMENTAL DESCRIPTION
Acute or chronic infection resulting from Blastomyces dermatitidis, a dimorphic fungus present in soil.
EPIDEMIOLOGY
Occurrence
• Annual incidence ranges from 0.3 to 1.8 incidents per 100,000 (1).
• Up to 7.4 hospital admissions per 1 million individuals in endemic areas (1).
RISK FACTOR
• Location: Endemic in soil adjacent to aquatic environments in the Southeastern United States and the valleys of the Mississippi, Ohio, and St. Lawrence Rivers. Additionally, the Mediterranean coast, South America, Mexico, and Africa. Previously regarded as more common in middle-aged men, but more likely attributed to environmental exposures.
• Immunocompromised individuals are at heightened risk for more severe disease and adverse outcomes.
GENERAL PREVENTION MEASURES
Mitigation of exposure; utilization of breathing masks for individuals at occupational risk
Pathophysiology
• Inhalation of conidia from B. dermatitidis may lead to secondary hematogenous dissemination.
The immune system is more efficient against conidia than against the yeast form. Blastomyces transform into budding yeast within tissue, thereby exhibiting reduced vulnerability to immune system eradication.
• Reactivation in immunocompromised individuals.
ETIOLOGY
Dimorphic fungus, Blastomyces dermatitidis
HISTORY OF DIAGNOSIS
• Acute pneumonia: Abrupt manifestation of symptoms akin to bacterial pneumonia, encompassing:
- Pyrexia, nocturnal diaphoresis
- Productive cough, dyspnea, and pleuritic chest discomfort (60–90%)
– Rash (60 percent)
• Chronic pneumonia: Gradual emergence of symptoms akin to pulmonary tuberculosis
- Pyrexia, nocturnal diaphoresis, weight reduction
Mild productive cough, occasionally accompanied by chest discomfort and hemoptysis.
• Additional factors (contingent upon the infection site):
– Eruption – Asymptomatic soft-tissue edema
Meningitis or localized neurological impairment
PHYSICAL EXAMINATION
• Pulmonary: Auscultatory findings include crackles and rhonchi.
• Dermatological lesions: Generally non-painful papules or nodules.
. May present as either verrucous or ulcerated and cause discomfort.
• Non-tender soft tissue edema, occasionally accompanied by a draining tract.
DIAGNOSTIC EXAMINATIONS AND ANALYSIS
Laboratory
• There is no commercially available serological test due to cross-reactivity with other endemic mycoses.
• Urine antigen testing is accessible but not extensively utilized due to cross-reactivity.
Imaging
Preliminary strategy
Chest radiograph (CXR): Mass, many nodules, lobar infiltration, cavitation. Lymphadenopathy is infrequent.
Subsequent Actions & Unique Considerations
Additional clinical manifestations include genitourinary tract infections, septic arthritis, osteomyelitis, ocular infections, central nervous system infections (meningitis, cerebral abscess), and oropharyngeal abscess (1).
Diagnostic Procedures and Additional Methods
• Culture: 86% positive for sputum; 92% positive for bronchoalveolar lavage (BAL)
• Wet preparation: 46% sensitivity (multiple specimens utilizing KOH or calcofluor white)
• Attributes: Substantial yeast structures (8–15 mm in diameter) exhibiting a solitary broad-based bud
Pathological Observations
• Pyogranulomas
• Fungal elements are more readily observed with methenamine silver stain or Periodic acid-Schiff stain (PAS).
DIFFERENTIAL DIAGNOSIS
• Atypical pneumonia (acute pneumonia)
Lung carcinoma or mycobacterial infection (chronic pneumonia)
• Squamous cell carcinoma (cutaneous lesions)
MEDICATION FOR TREATMENT
• Pulmonary or disseminated non-central nervous system illness (2):
- Administer Amphotericin B (or lipid/liposomal formulation) for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 6–12 months.
For mild to moderate disease, administer itraconazole 200 mg orally three times daily for 3 days, followed by 200 mg orally twice daily for 6 to 12 months. • CNS disease: - Administer Amphotericin B (lipid/liposomal formulation) at a dosage of 3–5 mg/kg intravenously for a duration of 4–6 weeks, followed by oral azole therapy for a minimum of 12 months.
Itraconazole 200 mg orally three times daily or twice daily. Alternatively, provide Fluconazole 800 mg orally each day. Voriconazole 200–400 mg orally, twice daily. • In immunocompromised individuals: Administer Amphotericin B for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 12 months.
– Contemplate lifelong administration of itraconazole 200 milligrams orally daily.
Pediatric Considerations
• Treatment for mild disease: Itraconazole, 10 mg/kg daily for 6–12 months. • Treatment for severe disease: Amphotericin (or liposomal) followed by itraconazole.
Considerations During Pregnancy
• Prescription: Amphotericin B only, due to the contraindication of azoles during pregnancy.
SUPPLEMENTARY THERAPY
Comprehensive Measures
Continuous surveillance for the toxicity of antifungal medicines.
SURGERY/OTHER PROCEDURES
Uncommon, in instances of central nervous system mass or abscess.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
• The death rate for ARDS, even with proper treatment, ranges from 50% to 89%.
• Diligent monitoring of neurological assessments in central nervous system disorders.
Admission Criteria: • Immunosuppression • Respiratory distress • Requirement for intravenous therapy
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Surveillance of the patient following treatment for approximately six months, due to the potential for relapse.
Patient Surveillance
• Therapeutic drug monitoring for itraconazole is advised after two weeks of treatment: Does not require to be accurate through or peak. The objective is to exceed 1.0 μg/mL and remain below 10 μg/mL (2).
• Conduct liver function tests (LFTs) every three months at a minimum during azole therapy.
NUTRITION
Itraconazole must be administered with food.
PATIENT EDUCATION
• Address the possibility of drug–drug interactions associated with itraconazole administration.
• Anxiety of recurrence despite the availability of suitable treatment (2).
PROGNOSIS
• A cure without relapse occurs in 90–97% of immunocompetent individuals treated with amphotericin.
• 40% mortality rate in immunocompromised individuals (bone marrow transplant [BMT], AIDS); marginally improved outcomes in solid-organ transplant recipients.
Considerations During Pregnancy
Results: Early diagnosis can lead to favorable outcomes; however, pregnant women are at increased risk for more severe disease due to their mild immunosuppression.
FUNDAMENTAL DESCRIPTION
Acute or chronic infection resulting from Blastomyces dermatitidis, a dimorphic fungus present in soil.
EPIDEMIOLOGY
Occurrence
• Annual incidence ranges from 0.3 to 1.8 incidents per 100,000 (1).
• Up to 7.4 hospital admissions per 1 million individuals in endemic areas (1).
RISK FACTOR
• Location: Endemic in soil adjacent to aquatic environments in the Southeastern United States and the valleys of the Mississippi, Ohio, and St. Lawrence Rivers. Additionally, the Mediterranean coast, South America, Mexico, and Africa. Previously regarded as more common in middle-aged men, but more likely attributed to environmental exposures.
• Immunocompromised individuals are at heightened risk for more severe disease and adverse outcomes.
GENERAL PREVENTION MEASURES
Mitigation of exposure; utilization of breathing masks for individuals at occupational risk
Pathophysiology
• Inhalation of conidia from B. dermatitidis may lead to secondary hematogenous dissemination.
The immune system is more efficient against conidia than against the yeast form. Blastomyces transform into budding yeast within tissue, thereby exhibiting reduced vulnerability to immune system eradication.
• Reactivation in immunocompromised individuals.
ETIOLOGY
Dimorphic fungus, Blastomyces dermatitidis
HISTORY OF DIAGNOSIS
• Acute pneumonia: Abrupt manifestation of symptoms akin to bacterial pneumonia, encompassing:
- Pyrexia, nocturnal diaphoresis
- Productive cough, dyspnea, and pleuritic chest discomfort (60–90%)
– Rash (60 percent)
• Chronic pneumonia: Gradual emergence of symptoms akin to pulmonary tuberculosis
- Pyrexia, nocturnal diaphoresis, weight reduction
Mild productive cough, occasionally accompanied by chest discomfort and hemoptysis.
• Additional factors (contingent upon the infection site):
– Eruption – Asymptomatic soft-tissue edema
Meningitis or localized neurological impairment
PHYSICAL EXAMINATION
• Pulmonary: Auscultatory findings include crackles and rhonchi.
• Dermatological lesions: Generally non-painful papules or nodules.
. May present as either verrucous or ulcerated and cause discomfort.
• Non-tender soft tissue edema, occasionally accompanied by a draining tract.
DIAGNOSTIC EXAMINATIONS AND ANALYSIS
Laboratory
• There is no commercially available serological test due to cross-reactivity with other endemic mycoses.
• Urine antigen testing is accessible but not extensively utilized due to cross-reactivity.
Imaging
Preliminary strategy
Chest radiograph (CXR): Mass, many nodules, lobar infiltration, cavitation. Lymphadenopathy is infrequent.
Subsequent Actions & Unique Considerations
Additional clinical manifestations include genitourinary tract infections, septic arthritis, osteomyelitis, ocular infections, central nervous system infections (meningitis, cerebral abscess), and oropharyngeal abscess (1).
Diagnostic Procedures and Additional Methods
• Culture: 86% positive for sputum; 92% positive for bronchoalveolar lavage (BAL)
• Wet preparation: 46% sensitivity (multiple specimens utilizing KOH or calcofluor white)
• Attributes: Substantial yeast structures (8–15 mm in diameter) exhibiting a solitary broad-based bud
Pathological Observations
• Pyogranulomas
• Fungal elements are more readily observed with methenamine silver stain or Periodic acid-Schiff stain (PAS).
DIFFERENTIAL DIAGNOSIS
• Atypical pneumonia (acute pneumonia)
Lung carcinoma or mycobacterial infection (chronic pneumonia)
• Squamous cell carcinoma (cutaneous lesions)
MEDICATION FOR TREATMENT
• Pulmonary or disseminated non-central nervous system illness (2):
- Administer Amphotericin B (or lipid/liposomal formulation) for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 6–12 months.
For mild to moderate disease, administer itraconazole 200 mg orally three times daily for 3 days, followed by 200 mg orally twice daily for 6 to 12 months. • CNS disease: - Administer Amphotericin B (lipid/liposomal formulation) at a dosage of 3–5 mg/kg intravenously for a duration of 4–6 weeks, followed by oral azole therapy for a minimum of 12 months.
Itraconazole 200 mg orally three times daily or twice daily. Alternatively, provide Fluconazole 800 mg orally each day. Voriconazole 200–400 mg orally, twice daily. • In immunocompromised individuals: Administer Amphotericin B for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 12 months.
– Contemplate lifelong administration of itraconazole 200 milligrams orally daily.
Pediatric Considerations
• Treatment for mild disease: Itraconazole, 10 mg/kg daily for 6–12 months. • Treatment for severe disease: Amphotericin (or liposomal) followed by itraconazole.
Considerations During Pregnancy
• Prescription: Amphotericin B only, due to the contraindication of azoles during pregnancy.
SUPPLEMENTARY THERAPY
Comprehensive Measures
Continuous surveillance for the toxicity of antifungal medicines.
SURGERY/OTHER PROCEDURES
Uncommon, in instances of central nervous system mass or abscess.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
• The death rate for ARDS, even with proper treatment, ranges from 50% to 89%.
• Diligent monitoring of neurological assessments in central nervous system disorders.
Admission Criteria: • Immunosuppression • Respiratory distress • Requirement for intravenous therapy
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Surveillance of the patient following treatment for approximately six months, due to the potential for relapse.
Patient Surveillance
• Therapeutic drug monitoring for itraconazole is advised after two weeks of treatment: Does not require to be accurate through or peak. The objective is to exceed 1.0 μg/mL and remain below 10 μg/mL (2).
• Conduct liver function tests (LFTs) every three months at a minimum during azole therapy.
NUTRITION
Itraconazole must be administered with food.
PATIENT EDUCATION
• Address the possibility of drug–drug interactions associated with itraconazole administration.
• Anxiety of recurrence despite the availability of suitable treatment (2).
PROGNOSIS
• A cure without relapse occurs in 90–97% of immunocompetent individuals treated with amphotericin.
• 40% mortality rate in immunocompromised individuals (bone marrow transplant [BMT], AIDS); marginally improved outcomes in solid-organ transplant recipients.
Considerations During Pregnancy
Results: Early diagnosis can lead to favorable outcomes; however, pregnant women are at increased risk for more severe disease due to their mild immunosuppression.
- Published on
Infectious Disease - Bacillary Angiomatosis/Peliosis Hepatis
DESCRIPTION
• A rare, vascular proliferative infectious disease affecting the skin and internal organs, predominantly observed in immunosuppressed persons, particularly those with T-cell deficits, such as HIV-positive patients. The name bacillary angiomatosis (BA) mostly refers to the cutaneous or disseminated form, whereas peliosis hepatica (PH) denotes the visceral form of this feverish sickness associated with Bartonella species.
EPIDEMIOLOGY
Prevalence This disease, encountered globally, is rare; isolated cases have been reported from various regions worldwide.
RISK FACTORS • HIV infection (CD4 <100) (1) • Other types of immunosuppression • Unsanitary settings, exposure to felines
COMPREHENSIVE PREVENTION
• Concerning cats for people who are HIV-positive or otherwise immunocompromised: It is advisable to acquire a cat that is over one year old and in good health. The patient must practice meticulous hand hygiene following the cleaning of the litter box. Prevent bites and scratches; wash hands immediately if they occur. Declawing or subjecting a cat to testing is not recommended. • Primary prophylaxis is not advised. Prophylactic administration of a macrolide provides protection against Bartonella infection. The potential requirement for secondary prophylaxis or the indefinite duration of treatment in HIV-positive patients remains undefined.
ETIOLOGY • Bartonella henselae (predominantly BA) and Bartonella quintana (mostly bacteremia). Bartonella species are gram-negative bacteria belonging to the alpha Proteobacteria family. • Infection with B. henselae is associated with cat exposure in individuals with HIV infection. Conversely, BA attributed to B. quintana is linked to body louse infection and homelessness.
DIAGNOSIS HISTORY
• The incubation period lasts a minimum of one week. • Clinical manifestations vary from isolated bacteremia to cutaneous and visceral (PH) disease, together with involvement of several organs (skin, bones, central nervous system). • If left untreated, it may be lethal. • BA: – Constitutional: Pyrexia, malaise, cachexia, anemia • PH: – Constitutional: Chronic fever, fatigue, weight reduction, stomach discomfort - Gastrointestinal manifestations: Nausea, emesis • Symptoms related to other organs or systems are contingent upon the individual body component involved (e.g., ostealgia, neurological impairments, etc.).
PHYSICAL EXAMINATION
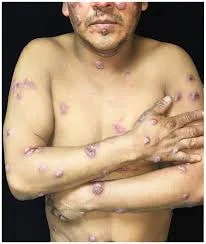
• BA: – Dermatological symptoms (93% of patients): — Elevated, vivid red papules, ranging from one to hundreds in quantity and measuring from 1 mm to several centimeters in size, observed in two-thirds of patients. – Minor lesions may be obscured by a thinned epidermis, whereas bigger lesions are prone to erosion and hemorrhage. A peripheral collarette is prevalent. Subcutaneous nodular lesions, observed in one-fourth of patients, are typically big and may not exhibit any changes in the overlying skin. Cellulitic plaque-like lesions occur in 5–10% of patients and frequently overlay deeper osseous lesions. Ulcerations and folliculitis lesions are infrequent. Lesions can manifest in any region of the body; many types may develop simultaneously or in succession. - Extracutaneous signs primarily include bone and visceral lesions (liver, spleen), however several other organ/system involvements have been documented, with or without vascular proliferative alterations, painful or painless lymphadenopathy, and cerebral abscesses. Bone disease may initially present solely with pain and may or may not be accompanied by superficial skin sores. • PH: – Significant hepatomegaly, progressing over weeks or months – Splenomegaly – Potential involvement of the skin or other organs
DIAGNOSTIC TESTS AND INTERPRETATION
LAB
Diagnosis is established through the identification of causative organisms in hematoxylin and eosin-stained tissue sections (granular purple material); it may also be confirmed using Warthin-Starry or Brown–Hopps tissue stains. • Organisms manifest either solitarily or in clusters and entanglements. • Acquiring culture is challenging and labor-intensive. The organism can be extracted from the blood using lysis centrifugation cultures. Incubate for a minimum of 21 days. Polymerase chain reaction (PCR) is used for detection and species identification. • The sensitivity of serological tests is diminished in immunocompromised individuals. • Mildly raised transaminases (average ×2 of normal), moderate to severe elevation of alkaline phosphatase (average ×5 of normal), and normal or slightly higher bilirubin levels. Mild to moderate pancytopenia may manifest in the visceral form of the disease. Imaging • Bone disease: Standard bone radiographs reveal well-defined lytic lesions or indistinct areas of significant cortical destruction accompanied by pronounced periosteal response. • CT imaging may demonstrate hepatosplenomegaly and enlargement of intra-abdominal and/or retroperitoneal lymph nodes. Visceral parenchyma may exhibit a diverse consistency. Histopathological Observations • Biopsy or fine-needle aspiration specimens from the skin, liver, and lymph nodes are typically utilized. The pathological pattern is contingent upon the organ affected. • Skin: Lesions exhibit a "epithelioid hemangioma" look, with the presence of organisms demonstrated. • PH: Liver biopsy specimens exhibit significantly dilated, blood-filled cystic areas within the parenchyma. They are frequently linked to a myxoid stroma. Foci of necrosis are observable in advanced instances.
DIFFERENTIAL DIAGNOSIS • BA: – Kaposi’s sarcoma – Pyogenic granulomas – Angiomas – Verruga peruana (bartonellosis, prevalent in South America) • PH: – Kaposi’s sarcoma • Extracutaneous manifestations: – Additional lesions occurring in space – The potential coexistence with Kaposi’s sarcoma must constantly be contemplated.
THERAPY PHARMACEUTICALS
Initial Statement An initial assessment is required to ascertain the degree of organ involvement. Erythromycin 500 mg orally every 6 hours or doxycycline 100 mg every 12 hours (AII) • Treatment duration: BA 3 months; PH 4 months. Extended therapy for immunocompromised individuals. Patients may encounter a Jarisch–Herxheimer reaction and should get prophylactic antipyretic medications within the initial 72 hours of treatment. Second Line • In cases of intolerance to erythromycin or doxycycline, azithromycin or clarithromycin have demonstrated a clinical response (BIII). Combination therapy, incorporating rifampin (300 mg orally twice day) alongside either erythromycin or doxycycline, is advised for immunocompromised patients experiencing acute, life-threatening infections or central nervous system disorders. • TMP-SMX and ciprofloxacin have demonstrated variable clinical efficacy.
INPATIENT CONSIDERATIONS
Criteria for Admission Patients are often managed on an outpatient basis; however, inpatient care and intravenous antibiotics are required for those with significant skin disease, lytic bone lesions, visceral lesions, or fulminant disease.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
• Following the commencement of treatment (about 4–7 days into therapy), substantial enhancement of cutaneous and visceral/other organ lesions is often observed. • Complete resolution typically occurs within 3 to 4 weeks. • Relapses manifest in around 15% of instances. • Treatment failure: Upon relapse, four months of uninterrupted suppressive therapy. Patient Surveillance Clinical monitoring is necessary. • Serial biochemical assays (e.g., liver function tests) may assist in evaluating the therapeutic response in visceral disease. Utilize x-rays or bone scans to assess bone pathology. • The potential for coexistence with Kaposi’s sarcoma should be explored if imaging results do not improve following adequate antibiotic therapy.
COMPLICATIONS
The visceral manifestation of the disease may be exacerbated by anemia, pancytopenia resulting from hypersplenism, and splenic rupture accompanied by hemoperitoneum.
DESCRIPTION
• A rare, vascular proliferative infectious disease affecting the skin and internal organs, predominantly observed in immunosuppressed persons, particularly those with T-cell deficits, such as HIV-positive patients. The name bacillary angiomatosis (BA) mostly refers to the cutaneous or disseminated form, whereas peliosis hepatica (PH) denotes the visceral form of this feverish sickness associated with Bartonella species.
EPIDEMIOLOGY
Prevalence This disease, encountered globally, is rare; isolated cases have been reported from various regions worldwide.
RISK FACTORS • HIV infection (CD4 <100) (1) • Other types of immunosuppression • Unsanitary settings, exposure to felines
COMPREHENSIVE PREVENTION
• Concerning cats for people who are HIV-positive or otherwise immunocompromised: It is advisable to acquire a cat that is over one year old and in good health. The patient must practice meticulous hand hygiene following the cleaning of the litter box. Prevent bites and scratches; wash hands immediately if they occur. Declawing or subjecting a cat to testing is not recommended. • Primary prophylaxis is not advised. Prophylactic administration of a macrolide provides protection against Bartonella infection. The potential requirement for secondary prophylaxis or the indefinite duration of treatment in HIV-positive patients remains undefined.
ETIOLOGY • Bartonella henselae (predominantly BA) and Bartonella quintana (mostly bacteremia). Bartonella species are gram-negative bacteria belonging to the alpha Proteobacteria family. • Infection with B. henselae is associated with cat exposure in individuals with HIV infection. Conversely, BA attributed to B. quintana is linked to body louse infection and homelessness.
DIAGNOSIS HISTORY
• The incubation period lasts a minimum of one week. • Clinical manifestations vary from isolated bacteremia to cutaneous and visceral (PH) disease, together with involvement of several organs (skin, bones, central nervous system). • If left untreated, it may be lethal. • BA: – Constitutional: Pyrexia, malaise, cachexia, anemia • PH: – Constitutional: Chronic fever, fatigue, weight reduction, stomach discomfort - Gastrointestinal manifestations: Nausea, emesis • Symptoms related to other organs or systems are contingent upon the individual body component involved (e.g., ostealgia, neurological impairments, etc.).
PHYSICAL EXAMINATION
• BA: – Dermatological symptoms (93% of patients): — Elevated, vivid red papules, ranging from one to hundreds in quantity and measuring from 1 mm to several centimeters in size, observed in two-thirds of patients. – Minor lesions may be obscured by a thinned epidermis, whereas bigger lesions are prone to erosion and hemorrhage. A peripheral collarette is prevalent. Subcutaneous nodular lesions, observed in one-fourth of patients, are typically big and may not exhibit any changes in the overlying skin. Cellulitic plaque-like lesions occur in 5–10% of patients and frequently overlay deeper osseous lesions. Ulcerations and folliculitis lesions are infrequent. Lesions can manifest in any region of the body; many types may develop simultaneously or in succession. - Extracutaneous signs primarily include bone and visceral lesions (liver, spleen), however several other organ/system involvements have been documented, with or without vascular proliferative alterations, painful or painless lymphadenopathy, and cerebral abscesses. Bone disease may initially present solely with pain and may or may not be accompanied by superficial skin sores. • PH: – Significant hepatomegaly, progressing over weeks or months – Splenomegaly – Potential involvement of the skin or other organs
DIAGNOSTIC TESTS AND INTERPRETATION
LAB
Diagnosis is established through the identification of causative organisms in hematoxylin and eosin-stained tissue sections (granular purple material); it may also be confirmed using Warthin-Starry or Brown–Hopps tissue stains. • Organisms manifest either solitarily or in clusters and entanglements. • Acquiring culture is challenging and labor-intensive. The organism can be extracted from the blood using lysis centrifugation cultures. Incubate for a minimum of 21 days. Polymerase chain reaction (PCR) is used for detection and species identification. • The sensitivity of serological tests is diminished in immunocompromised individuals. • Mildly raised transaminases (average ×2 of normal), moderate to severe elevation of alkaline phosphatase (average ×5 of normal), and normal or slightly higher bilirubin levels. Mild to moderate pancytopenia may manifest in the visceral form of the disease. Imaging • Bone disease: Standard bone radiographs reveal well-defined lytic lesions or indistinct areas of significant cortical destruction accompanied by pronounced periosteal response. • CT imaging may demonstrate hepatosplenomegaly and enlargement of intra-abdominal and/or retroperitoneal lymph nodes. Visceral parenchyma may exhibit a diverse consistency. Histopathological Observations • Biopsy or fine-needle aspiration specimens from the skin, liver, and lymph nodes are typically utilized. The pathological pattern is contingent upon the organ affected. • Skin: Lesions exhibit a "epithelioid hemangioma" look, with the presence of organisms demonstrated. • PH: Liver biopsy specimens exhibit significantly dilated, blood-filled cystic areas within the parenchyma. They are frequently linked to a myxoid stroma. Foci of necrosis are observable in advanced instances.
DIFFERENTIAL DIAGNOSIS • BA: – Kaposi’s sarcoma – Pyogenic granulomas – Angiomas – Verruga peruana (bartonellosis, prevalent in South America) • PH: – Kaposi’s sarcoma • Extracutaneous manifestations: – Additional lesions occurring in space – The potential coexistence with Kaposi’s sarcoma must constantly be contemplated.
THERAPY PHARMACEUTICALS
Initial Statement An initial assessment is required to ascertain the degree of organ involvement. Erythromycin 500 mg orally every 6 hours or doxycycline 100 mg every 12 hours (AII) • Treatment duration: BA 3 months; PH 4 months. Extended therapy for immunocompromised individuals. Patients may encounter a Jarisch–Herxheimer reaction and should get prophylactic antipyretic medications within the initial 72 hours of treatment. Second Line • In cases of intolerance to erythromycin or doxycycline, azithromycin or clarithromycin have demonstrated a clinical response (BIII). Combination therapy, incorporating rifampin (300 mg orally twice day) alongside either erythromycin or doxycycline, is advised for immunocompromised patients experiencing acute, life-threatening infections or central nervous system disorders. • TMP-SMX and ciprofloxacin have demonstrated variable clinical efficacy.
INPATIENT CONSIDERATIONS
Criteria for Admission Patients are often managed on an outpatient basis; however, inpatient care and intravenous antibiotics are required for those with significant skin disease, lytic bone lesions, visceral lesions, or fulminant disease.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
• Following the commencement of treatment (about 4–7 days into therapy), substantial enhancement of cutaneous and visceral/other organ lesions is often observed. • Complete resolution typically occurs within 3 to 4 weeks. • Relapses manifest in around 15% of instances. • Treatment failure: Upon relapse, four months of uninterrupted suppressive therapy. Patient Surveillance Clinical monitoring is necessary. • Serial biochemical assays (e.g., liver function tests) may assist in evaluating the therapeutic response in visceral disease. Utilize x-rays or bone scans to assess bone pathology. • The potential for coexistence with Kaposi’s sarcoma should be explored if imaging results do not improve following adequate antibiotic therapy.
COMPLICATIONS
The visceral manifestation of the disease may be exacerbated by anemia, pancytopenia resulting from hypersplenism, and splenic rupture accompanied by hemoperitoneum.


- Published on
Balanitis
FUNDAMENTAL DESCRIPTION
Inflammation and/or infection of the glans penis. Balanoposthitis encompasses inflammation of the prepuce. This chapter will examine the infectious etiologies.
Epidemiology
Frequency
• Sexual exposure; heightened prevalence in men with female partners suffering from Candida vaginitis. • Balanitis in young boys frequently occurs alongside diaper dermatitis.
RISK FACTORS • Men who are uncircumcised
• Diabetes, particularly new-onset diabetes • For Candida, both colonization and infection age serve as independent risk factors
• Comprehensive-spectrum antibiotics
• Immunodeficiency • Inadequate hygiene
GENERAL PREVENTION • Circumcision • Proper hygiene • Treatment of sexual partner(s) diagnosed with Candida vaginitis or Trichomonas CAUSES
The pathogens implicated in infectious balanitis include, among others:
• Candida species • Trichomonas species • Anaerobic bacteria/Bacteroides species/Gardnerella vaginalis • Chlamydia • Neisseria gonorrhoeae • Human papillomavirus (HPV) • Herpes simplex virus (HSV) • Treponema pallidum
• Mycoplasma • Mycobacterium [Bacillus Calmette–Guerin (BCG)]
• Streptococcus (groups A and B) • Staphylococcus aureus
Borrelia burgdorferi (Lyme illness) • Entamoeba histolytica
DIAGNOSIS • Pain and soreness • Erosions • Erythema • Pruritus • Pustules • Foul odor of the glans penis associated with anaerobic infections • Swelling
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Fungal preparations typically signify Candida.
• A recent study demonstrated that direct impression on CHROMagar Candida medium as a sampling technique yielded a higher quantity of Candida spp than swabs.
• A wet mount may reveal Trichomonas.
• Wet mount preparation for Gardnerella.
• Evaluate the urethral discharge for sexually transmitted infections.
• Titers or cultures to detect HIV, HPV, and HSV. • Glucose assessment to exclude diabetes mellitus.
DIFFERENTIAL DIAGNOSIS • Noninfectious etiologies of balanitis - Irritants, including soaps
– Inadequate hygiene – Trauma – Contact dermatitis – Circinate balanitis – Lichen sclerosus – Lichen planus – Zoon's balanitis – Erythroplasia of Queyrat – Pemphigus – Pemphigoid – Bowen's illness
– Leukoplakia – Fixed drug eruption – Psoriasis, especially inverse psoriasis – Paget’s illness – Nummular eczema – Scabies – Squamous cell carcinoma
ADDITIONAL TREATMENT
Comprehensive Strategies
• Maintain proper hygiene by retracting the foreskin and gently cleansing the glans penis.
Local treatment for Candida balanitis involves the application of topical imidazoles. 1% hydrocortisone cream may serve as an adjunctive treatment.
• Administer oral fluconazole for severe Candida balanitis. • Trichomonas is susceptible to metronidazole.
• Concurrently treat sexual partner(s) for Candida or Trichomonas.
• Manage anaerobic infections with oral metronidazole, oral amoxicillin/clavulanate, or topical clindamycin cream.
CONTINUING TREATMENT POST-CARE SUGGESTIONS
Patients require monitoring by a physician for signs of recurrence or the onset of diabetes.
COMPLICATIONS
• Phimosis • Paraphimosis • Preputial fissure • Scarring
FUNDAMENTAL DESCRIPTION
Inflammation and/or infection of the glans penis. Balanoposthitis encompasses inflammation of the prepuce. This chapter will examine the infectious etiologies.
Epidemiology
Frequency
• Sexual exposure; heightened prevalence in men with female partners suffering from Candida vaginitis. • Balanitis in young boys frequently occurs alongside diaper dermatitis.
RISK FACTORS • Men who are uncircumcised
• Diabetes, particularly new-onset diabetes • For Candida, both colonization and infection age serve as independent risk factors
• Comprehensive-spectrum antibiotics
• Immunodeficiency • Inadequate hygiene
GENERAL PREVENTION • Circumcision • Proper hygiene • Treatment of sexual partner(s) diagnosed with Candida vaginitis or Trichomonas CAUSES
The pathogens implicated in infectious balanitis include, among others:
• Candida species • Trichomonas species • Anaerobic bacteria/Bacteroides species/Gardnerella vaginalis • Chlamydia • Neisseria gonorrhoeae • Human papillomavirus (HPV) • Herpes simplex virus (HSV) • Treponema pallidum
• Mycoplasma • Mycobacterium [Bacillus Calmette–Guerin (BCG)]
• Streptococcus (groups A and B) • Staphylococcus aureus
Borrelia burgdorferi (Lyme illness) • Entamoeba histolytica
DIAGNOSIS • Pain and soreness • Erosions • Erythema • Pruritus • Pustules • Foul odor of the glans penis associated with anaerobic infections • Swelling
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
• Fungal preparations typically signify Candida.
• A recent study demonstrated that direct impression on CHROMagar Candida medium as a sampling technique yielded a higher quantity of Candida spp than swabs.
• A wet mount may reveal Trichomonas.
• Wet mount preparation for Gardnerella.
• Evaluate the urethral discharge for sexually transmitted infections.
• Titers or cultures to detect HIV, HPV, and HSV. • Glucose assessment to exclude diabetes mellitus.
DIFFERENTIAL DIAGNOSIS • Noninfectious etiologies of balanitis - Irritants, including soaps
– Inadequate hygiene – Trauma – Contact dermatitis – Circinate balanitis – Lichen sclerosus – Lichen planus – Zoon's balanitis – Erythroplasia of Queyrat – Pemphigus – Pemphigoid – Bowen's illness
– Leukoplakia – Fixed drug eruption – Psoriasis, especially inverse psoriasis – Paget’s illness – Nummular eczema – Scabies – Squamous cell carcinoma
ADDITIONAL TREATMENT
Comprehensive Strategies
• Maintain proper hygiene by retracting the foreskin and gently cleansing the glans penis.
Local treatment for Candida balanitis involves the application of topical imidazoles. 1% hydrocortisone cream may serve as an adjunctive treatment.
• Administer oral fluconazole for severe Candida balanitis. • Trichomonas is susceptible to metronidazole.
• Concurrently treat sexual partner(s) for Candida or Trichomonas.
• Manage anaerobic infections with oral metronidazole, oral amoxicillin/clavulanate, or topical clindamycin cream.
CONTINUING TREATMENT POST-CARE SUGGESTIONS
Patients require monitoring by a physician for signs of recurrence or the onset of diabetes.
COMPLICATIONS
• Phimosis • Paraphimosis • Preputial fissure • Scarring

- Published on
Infectious Disease – Bell’s Palsy
BASICS DESCRIPTION
• Bell’s palsy is characterized by acute, idiopathic, unilateral paralysis of the facial nerve. • Approximately fifty percent of facial nerve palsy cases are classified as “Bell’s palsy.”
Bilateral illness constitutes a rare subtype, accounting for 0.3%.
ETIOLOGY
• Herpes simplex virus • Herpes zoster virus, including herpes zoster oticus • Negative occurrence after to vaccination
Epidemiology
Incidence • Rates range from 13 to 34 instances per 100,000 in the United States. • Incidence peaks among individuals aged 20–35 years and those over 70 years.
• The distribution of boys and females is equal. • Bell's palsy is the predominant etiology of VII nerve palsy in pediatric patients.
RISK FACTORS
• Gestation • Diabetes mellitus • Hypertension in individuals over 40 years
GENERAL PREVENTION
Currently, there is no method to avert Bell's palsy.
DIAGNOSIS
• Sudden onset within one to two days, fast advancement of partial or complete unilateral facial nerve paralysis • Reduced tear and saliva secretion on the affected side • Hyperacusis • Dysgeusia • Retroauricular pain
DIFFERENTIAL DIAGNOSIS
The differential diagnoses list is extensive and includes, among others:
• Echovirus and enterovirus infections • Lyme disease • HIV infection, onset during seroconversion • Otitis media and mastoiditis • Mycobacterium tuberculosis • Syphilis • Infectious meningitis • Rubella • Tetanus • Mycoplasma • Cholesteatoma • Sarcoidosis
• Sjögren’s syndrome • Systemic lupus erythematosus • Melkersson–Rosenthal syndrome • Cerebral aneurysm • Tumor of the parotid gland • Melanoma of the head and neck • Meningioma • Carcinomatous meningitis • Granulomatous meningitis of unknown cause • Guillain-Barré syndrome • Pseudobulbar palsy • Birth trauma • Petrous bone fractures • Iatrogenic/surgical complications
• Paget's disease
• Consider bilateral facial nerve paralysis in the context of:
– Lyme disease – Sarcoidosis
DIAGNOSTIC TESTS & INTERPRETATION
Laboratory
• Electrodiagnostic examinations:
Patients with an incomplete, typical lesion who recover do not require additional investigation. - Electromyography (EMG)
Electroneurography (also known as evoked electromyography)
Imaging
Imaging is required if the clinical presentation is abnormal, development is gradual, or there is no improvement after six months. A CT or MRI scan may be necessary to exclude intracerebral pathology or middle ear disease in complex cases. Recent studies indicate that the ultrasonography diameter of the distal VII nerve is a reliable prognostic indicator for Bell's palsy at three months post-onset.
THERAPY
Early administration of prednisolone markedly enhances the likelihood of full recovery at 3 and 9 months (Recommendation Grade 1A).
Treatment must commence within three days.
The advised dosage is 60–80 mg each day for one week.
• Antivirals are designated for severe facial palsy (Recommendation Grade 2C).
• Safeguarding the ipsilateral eye with artificial tears and lubricating ointments throughout nocturnal hours.
The topic of surgical decompression remains contentious.
CONTINUOUS CARE
• Crucial for ocular health and mental well-being.
COMPLICATIONS
• Incomplete healing in one-third of patients • Keratitis and corneal abrasions
Recurrence has been noted in 7–15% of instances.
BASICS DESCRIPTION
• Bell’s palsy is characterized by acute, idiopathic, unilateral paralysis of the facial nerve. • Approximately fifty percent of facial nerve palsy cases are classified as “Bell’s palsy.”
Bilateral illness constitutes a rare subtype, accounting for 0.3%.
ETIOLOGY
• Herpes simplex virus • Herpes zoster virus, including herpes zoster oticus • Negative occurrence after to vaccination
Epidemiology
Incidence • Rates range from 13 to 34 instances per 100,000 in the United States. • Incidence peaks among individuals aged 20–35 years and those over 70 years.
• The distribution of boys and females is equal. • Bell's palsy is the predominant etiology of VII nerve palsy in pediatric patients.
RISK FACTORS
• Gestation • Diabetes mellitus • Hypertension in individuals over 40 years
GENERAL PREVENTION
Currently, there is no method to avert Bell's palsy.
DIAGNOSIS
• Sudden onset within one to two days, fast advancement of partial or complete unilateral facial nerve paralysis • Reduced tear and saliva secretion on the affected side • Hyperacusis • Dysgeusia • Retroauricular pain
DIFFERENTIAL DIAGNOSIS
The differential diagnoses list is extensive and includes, among others:
• Echovirus and enterovirus infections • Lyme disease • HIV infection, onset during seroconversion • Otitis media and mastoiditis • Mycobacterium tuberculosis • Syphilis • Infectious meningitis • Rubella • Tetanus • Mycoplasma • Cholesteatoma • Sarcoidosis
• Sjögren’s syndrome • Systemic lupus erythematosus • Melkersson–Rosenthal syndrome • Cerebral aneurysm • Tumor of the parotid gland • Melanoma of the head and neck • Meningioma • Carcinomatous meningitis • Granulomatous meningitis of unknown cause • Guillain-Barré syndrome • Pseudobulbar palsy • Birth trauma • Petrous bone fractures • Iatrogenic/surgical complications
• Paget's disease
• Consider bilateral facial nerve paralysis in the context of:
– Lyme disease – Sarcoidosis
DIAGNOSTIC TESTS & INTERPRETATION
Laboratory
• Electrodiagnostic examinations:
Patients with an incomplete, typical lesion who recover do not require additional investigation. - Electromyography (EMG)
Electroneurography (also known as evoked electromyography)
Imaging
Imaging is required if the clinical presentation is abnormal, development is gradual, or there is no improvement after six months. A CT or MRI scan may be necessary to exclude intracerebral pathology or middle ear disease in complex cases. Recent studies indicate that the ultrasonography diameter of the distal VII nerve is a reliable prognostic indicator for Bell's palsy at three months post-onset.
THERAPY
Early administration of prednisolone markedly enhances the likelihood of full recovery at 3 and 9 months (Recommendation Grade 1A).
Treatment must commence within three days.
The advised dosage is 60–80 mg each day for one week.
• Antivirals are designated for severe facial palsy (Recommendation Grade 2C).
• Safeguarding the ipsilateral eye with artificial tears and lubricating ointments throughout nocturnal hours.
The topic of surgical decompression remains contentious.
CONTINUOUS CARE
• Crucial for ocular health and mental well-being.
COMPLICATIONS
• Incomplete healing in one-third of patients • Keratitis and corneal abrasions
Recurrence has been noted in 7–15% of instances.
- Published on
Infectious Disease -Bartonellosis (Oroya Fever/Verruga Peruana)
A disease caused by Bartonella bacilliformis, transmitted by the Phlebotomus sandfly, occurring in endemic regions in two distinct manifestations:
• Nonimmune individuals exhibit an acute febrile sickness accompanied by severe anemia (Oroya fever). • Following a variable duration post-resolution, a persistent, benign cutaneous manifestation may arise, marked by angioproliferative skin lesions (verruga peruana). The former exhibit a notable resemblance to lesions of bacillary angiomatosis, induced by Bartonella henselae and Bartonella quintana.
EPIDEMIOLOGY
Frequency
The disease is only confined to the valleys of the Andes River at elevations ranging from 600 to 2,500 meters in Peru, Ecuador, and Colombia.
• The majority of Oroya fever cases arise in tourists or visitors who
are immunologically inexperienced. The majority of verruga peruana cases occur within the indigenous community, with infrequent instances identified in the United States.
RISK FACTORS
Life in endemic regions and exposure to the sandfly vector GENERAL PREVENTION
Prevention necessitates the regulation of the sandfly vector: Application of dichlorodiphenyltrichloroethane (DDT) on both the interiors and exteriors of residences, utilization of insect repellents, and implementation of bed netting.
PATHOPHYSIOLOGY • Bartonella spp. infiltrate erythrocytes and endothelial cells. • They proliferate within intracellular vacuoles in the erythrocytes. The latter are subsequently engulfed and eliminated by the reticuloendothelial system.
ETIOLOGY • B. bacilliformis is a diminutive, gram-negative bacillus belonging to the class Proteobacteria, closely associated with B. quintana.
• It is spread through an arthropod vector, specifically the sandfly (Phlebotomus).
DIAGNOSTIC HISTORY
The incubation period for Oroya fever is approximately 3 weeks, with a maximum duration of 100 days.
The development of symptoms, primarily due to elevated temperature and severe anemia, may be either acute or subacute.
• Infectious problems arise from temporary immunosuppression.
The acute phase is followed by the convalescent period.
• Verruca skin lesions (nodules) manifest in clusters during a period of 1 to 2 months, after a variable interval after the remission of Oroya fever.
Acute manifestation (Oroya Fever)
• Subacute presentation (mild fever, malaise, cephalalgia, anorexia).
• Abrupt onset (elevated temperature, chills, sweating, cephalalgia, and alterations in cognitive function, succeeded by the rapid emergence of severe anemia).
• Myalgia and arthralgia.
• Dyspnea and angina; the patient may get the sensation that
The heart pulse is conveyed to the head and ears. • Anasarca serves as an indicator of unfavorable prognosis.
• Insomnia, delirium, diminished awareness, coma.
• In the ensuing convalescent (critical) phase, fever abates and anemia symptoms ameliorate.
PHYSICAL EXAMINATION
Oroya Fever • Elevated temperature • Indicators of severe anemia
• Generalized, nontender lymphadenopathy • Splenomegaly is uncommon; if observed, it may suggest an additional concomitant infection
• Thrombocytopenic purpura
Peruvian Wart
Miliary lesions comprise many papular, erythematous, round lesions measuring 1–4 mm, often accompanied by pruritus (1).
Nodular lesions, typically located on the skin and subcutaneous tissues of exposed body areas, may also involve mucous membranes and interior organs.
Mular lesions generally exceed 5 mm in diameter.
Characterized by erythema and a propensity to hemorrhage quickly.
• Lesions at different stages of development may be simultaneously present.
• Local tenderness is absent unless the patient has a secondary infection.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
In the acute phase, diagnosis is established through a positive culture (blood or bone marrow) or the identification of many organisms attached to red blood cells in peripheral thin-film blood smears (utilizing Giemsa or Wright stain). The bacterial count decreases sharply during convalescence.
Peripheral blood smears may reveal macrocytosis, poikilocytosis, Howell–Jolly bodies, nucleated red blood cells, and immature myeloid cells. The leukocyte differential exhibits a leftward shift, but the total count may remain within normal limits.
• Severe anemia; negative Coombs' test
In the subacute form, initial peripheral blood smears may yield negative results; diagnosis can be established through positive blood cultures.
Diagnosis of the chronic type can be achieved through the identification of the causal agent in culture.
Samples from cutaneous lesions and bone marrow cultures. • Blood cultures may yield positive results in asymptomatic patients. • Serological assays (ELISA, indirect fluorescent antibody, western immunoblot) can assist in diagnosis (2,3).
Pathological Findings: Skin biopsy, bone marrow aspiration, and biopsy specimens from further afflicted organs are utilized.
Enhanced angiogenesis, Rocha-Lima inclusions within endothelial cells
The polymerase chain reaction (PCR) for the detection of B. bacilliformis is currently in development.
DIFFERENTIAL DIAGNOSIS
• The acute phase can be readily distinguished from other endemic febrile conditions (e.g., malaria, typhoid fever, leptospirosis) through the analysis of peripheral blood smears and bacterial cultures. • Verruga peruana lesions bear resemblance to those of bacillary angiomatosis, Kaposi’s sarcoma, lymphoproliferative disorders, and other neoplasms. The primary diagnostic indicator is epidemiology.
THERAPEUTIC PHARMACEUTICAL
Oroya fever: Administer chloramphenicol (500 mg orally or intravenously every 6 hours) in conjunction with a secondary antibiotic, preferably a beta-lactam (such as penicillin), for a duration of 14 days (AII) (4).
Chloramphenicol is effective against salmonellosis, the prevalent secondary infection. The suggestion to incorporate a beta-lactam stems from the understanding that chloramphenicol alone is not dependable.
• Verruga peruana: – Administer Rifampin at a dosage of 10 mg/kg daily, not exceeding 600 mg daily, for a duration of 10–14 days (AII) orally (4). Second Line • Oroya fever: – Administer Doxycycline 100 mg orally twice daily for 14 days
The bacteria exhibits a prevalent resistance to ciprofloxacin.
Consequently, quinolones are not advised. • Verruga peruana: – Administer streptomycin at a dosage of 15–20 mg/kg intramuscularly on a daily basis for a duration of 10 days (AII)
SUPPLEMENTARY THERAPY
Comprehensive Strategies
Supportive and symptomatic treatment is essential in the acute form; employ blood transfusion to ameliorate anemia.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Extensive and secondarily infected cutaneous nodules may require surgical removal.
INPATIENT CONSIDERATIONS
Criteria for Admission
The suitable health care environment is inpatient for acute conditions and outpatient for chronic conditions.
CONTINUING MANAGEMENT POST-TREATMENT GUIDELINES
• Assess hydration levels and perform a complete blood count during the acute phase.
Monitor indicators of further infections: Splenomegaly, recurrent fever accompanied by leukocytosis throughout the convalescent phase, and diarrhea.
Observe verruca lesions for indications of subsequent infections.
PROGNOSIS • Untreated Oroya fever may result in mortality rates of 50–88%.
• Fever resolves within 24 hours following suitable antibiotic therapy, however bacteremia may endure for extended durations.
COMPLICATIONS
• Verruca lesions exhibit a varied response to antimicrobial therapy.
• Secondary bacterial infections, such as salmonellosis and other intestinal infections, malaria, and tuberculosis, are prevalent (45%) during the convalescent phase of Oroya fever. • Verruga lesions may become secondarily infected, leading to pustulation, ulceration, and hemorrhage.
A disease caused by Bartonella bacilliformis, transmitted by the Phlebotomus sandfly, occurring in endemic regions in two distinct manifestations:
• Nonimmune individuals exhibit an acute febrile sickness accompanied by severe anemia (Oroya fever). • Following a variable duration post-resolution, a persistent, benign cutaneous manifestation may arise, marked by angioproliferative skin lesions (verruga peruana). The former exhibit a notable resemblance to lesions of bacillary angiomatosis, induced by Bartonella henselae and Bartonella quintana.
EPIDEMIOLOGY
Frequency
The disease is only confined to the valleys of the Andes River at elevations ranging from 600 to 2,500 meters in Peru, Ecuador, and Colombia.
• The majority of Oroya fever cases arise in tourists or visitors who
are immunologically inexperienced. The majority of verruga peruana cases occur within the indigenous community, with infrequent instances identified in the United States.
RISK FACTORS
Life in endemic regions and exposure to the sandfly vector GENERAL PREVENTION
Prevention necessitates the regulation of the sandfly vector: Application of dichlorodiphenyltrichloroethane (DDT) on both the interiors and exteriors of residences, utilization of insect repellents, and implementation of bed netting.
PATHOPHYSIOLOGY • Bartonella spp. infiltrate erythrocytes and endothelial cells. • They proliferate within intracellular vacuoles in the erythrocytes. The latter are subsequently engulfed and eliminated by the reticuloendothelial system.
ETIOLOGY • B. bacilliformis is a diminutive, gram-negative bacillus belonging to the class Proteobacteria, closely associated with B. quintana.
• It is spread through an arthropod vector, specifically the sandfly (Phlebotomus).
DIAGNOSTIC HISTORY
The incubation period for Oroya fever is approximately 3 weeks, with a maximum duration of 100 days.
The development of symptoms, primarily due to elevated temperature and severe anemia, may be either acute or subacute.
• Infectious problems arise from temporary immunosuppression.
The acute phase is followed by the convalescent period.
• Verruca skin lesions (nodules) manifest in clusters during a period of 1 to 2 months, after a variable interval after the remission of Oroya fever.
Acute manifestation (Oroya Fever)
• Subacute presentation (mild fever, malaise, cephalalgia, anorexia).
• Abrupt onset (elevated temperature, chills, sweating, cephalalgia, and alterations in cognitive function, succeeded by the rapid emergence of severe anemia).
• Myalgia and arthralgia.
• Dyspnea and angina; the patient may get the sensation that
The heart pulse is conveyed to the head and ears. • Anasarca serves as an indicator of unfavorable prognosis.
• Insomnia, delirium, diminished awareness, coma.
• In the ensuing convalescent (critical) phase, fever abates and anemia symptoms ameliorate.
PHYSICAL EXAMINATION
Oroya Fever • Elevated temperature • Indicators of severe anemia
• Generalized, nontender lymphadenopathy • Splenomegaly is uncommon; if observed, it may suggest an additional concomitant infection
• Thrombocytopenic purpura
Peruvian Wart
Miliary lesions comprise many papular, erythematous, round lesions measuring 1–4 mm, often accompanied by pruritus (1).
Nodular lesions, typically located on the skin and subcutaneous tissues of exposed body areas, may also involve mucous membranes and interior organs.
Mular lesions generally exceed 5 mm in diameter.
Characterized by erythema and a propensity to hemorrhage quickly.
• Lesions at different stages of development may be simultaneously present.
• Local tenderness is absent unless the patient has a secondary infection.
DIAGNOSTIC TESTS AND INTERPRETATION Laboratory
In the acute phase, diagnosis is established through a positive culture (blood or bone marrow) or the identification of many organisms attached to red blood cells in peripheral thin-film blood smears (utilizing Giemsa or Wright stain). The bacterial count decreases sharply during convalescence.
Peripheral blood smears may reveal macrocytosis, poikilocytosis, Howell–Jolly bodies, nucleated red blood cells, and immature myeloid cells. The leukocyte differential exhibits a leftward shift, but the total count may remain within normal limits.
• Severe anemia; negative Coombs' test
In the subacute form, initial peripheral blood smears may yield negative results; diagnosis can be established through positive blood cultures.
Diagnosis of the chronic type can be achieved through the identification of the causal agent in culture.
Samples from cutaneous lesions and bone marrow cultures. • Blood cultures may yield positive results in asymptomatic patients. • Serological assays (ELISA, indirect fluorescent antibody, western immunoblot) can assist in diagnosis (2,3).
Pathological Findings: Skin biopsy, bone marrow aspiration, and biopsy specimens from further afflicted organs are utilized.
Enhanced angiogenesis, Rocha-Lima inclusions within endothelial cells
The polymerase chain reaction (PCR) for the detection of B. bacilliformis is currently in development.
DIFFERENTIAL DIAGNOSIS
• The acute phase can be readily distinguished from other endemic febrile conditions (e.g., malaria, typhoid fever, leptospirosis) through the analysis of peripheral blood smears and bacterial cultures. • Verruga peruana lesions bear resemblance to those of bacillary angiomatosis, Kaposi’s sarcoma, lymphoproliferative disorders, and other neoplasms. The primary diagnostic indicator is epidemiology.
THERAPEUTIC PHARMACEUTICAL
Oroya fever: Administer chloramphenicol (500 mg orally or intravenously every 6 hours) in conjunction with a secondary antibiotic, preferably a beta-lactam (such as penicillin), for a duration of 14 days (AII) (4).
Chloramphenicol is effective against salmonellosis, the prevalent secondary infection. The suggestion to incorporate a beta-lactam stems from the understanding that chloramphenicol alone is not dependable.
• Verruga peruana: – Administer Rifampin at a dosage of 10 mg/kg daily, not exceeding 600 mg daily, for a duration of 10–14 days (AII) orally (4). Second Line • Oroya fever: – Administer Doxycycline 100 mg orally twice daily for 14 days
The bacteria exhibits a prevalent resistance to ciprofloxacin.
Consequently, quinolones are not advised. • Verruga peruana: – Administer streptomycin at a dosage of 15–20 mg/kg intramuscularly on a daily basis for a duration of 10 days (AII)
SUPPLEMENTARY THERAPY
Comprehensive Strategies
Supportive and symptomatic treatment is essential in the acute form; employ blood transfusion to ameliorate anemia.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Extensive and secondarily infected cutaneous nodules may require surgical removal.
INPATIENT CONSIDERATIONS
Criteria for Admission
The suitable health care environment is inpatient for acute conditions and outpatient for chronic conditions.
CONTINUING MANAGEMENT POST-TREATMENT GUIDELINES
• Assess hydration levels and perform a complete blood count during the acute phase.
Monitor indicators of further infections: Splenomegaly, recurrent fever accompanied by leukocytosis throughout the convalescent phase, and diarrhea.
Observe verruca lesions for indications of subsequent infections.
PROGNOSIS • Untreated Oroya fever may result in mortality rates of 50–88%.
• Fever resolves within 24 hours following suitable antibiotic therapy, however bacteremia may endure for extended durations.
COMPLICATIONS
• Verruca lesions exhibit a varied response to antimicrobial therapy.
• Secondary bacterial infections, such as salmonellosis and other intestinal infections, malaria, and tuberculosis, are prevalent (45%) during the convalescent phase of Oroya fever. • Verruga lesions may become secondarily infected, leading to pustulation, ulceration, and hemorrhage.
- Published on
Infectious Disease – Atypical Mycobacteria
FUNDAMENTALS AND DESCRIPTION
Infection by a species of nontuberculous mycobacteria (NTM). Pediatric Considerations Atypical mycobacteria must be contemplated in patients exhibiting unilateral cervical lymphadenitis. • This virus predominantly affects youngsters between the ages of 1 and 5 years. • Edema frequently manifests around the impacted nodes, typically in the anterior cervical chain. Adenitis may develop swiftly, and the creation of fistulas through the skin is prevalent. Enlarged lymph nodes are frequently asymptomatic. • Systemic symptoms are seldom. • The majority of symptoms are attributed to MAC; however, Mycobacterium scrofulaceum and Mycobacterium tuberculosis are also observed, but less commonly.
Epidemiology
Annually, there are 300 cases of MAC lymphadenitis in the United States. Prevalence: 1–7.2 cases per 100,000 in the United States. • Significantly changeable, contingent upon location. Approximately 50% of non-tuberculous mycobacteria isolates are pathogenic.
RISK FACTORS
• Age • Immunosuppression • HIV with diminished CD4 cell counts or other opportunistic infections • Interferon (IFN)-gamma deficiency • Preexisting structural pulmonary disease Genetics: Deficiency of IFNγR1 or IL-12βR1
COMPREHENSIVE PREVENTION
In individuals with AIDS (CD4 count <100 cells/mm3), weekly administration of 1200 mg azithromycin is recommended as primary prophylaxis. Alternative preventative regimens are clarithromycin 500 mg three times day or rifabutin 300 mg daily.
PATHOPHYSIOLOGY • Environmental exposures such as soil, water, hot tubs, and tap water are frequently implicated. • Human-to-human transmission has not been recorded. • Initial infection occurs through ingesting or inhalation; reactivation is not a risk. • Granuloma formation arises from the interaction among macrophages, lymphocytes, and natural killer cells. • Disseminated disease stems from a localized infection.
ETIOLOGY • Aerobic, non-spore-forming bacilli characterized by cell walls containing mycolic acid (2). • Rapidly growing organisms encompass the following rapid-growing mycobacteria (RGM) (growth within 7 days): – Mycobacterium fortuitum complex – Mycobacterium chelonae/abscessus – Mycobacterium smegmatis • Organisms with intermediate growth rates encompass the following: – Mycobacterium marinum – Mycobacterium gordonae • Organisms with a slow growth rate (10–21 days) encompass the following: – Mycobacterium avium complex (MAC) – Mycobacterium kansasii – Mycobacterium xenopi – Mycobacterium scrofulaceum – Mycobacterium haemophilum – Mycobacterium ulcerans
FREQUENTLY CO-OCCURRING CONDITIONS • Immunosuppression, such as AIDS or transplant recipients • Utilization of TNF inhibitors • Cystic fibrosis • Pre-existing pulmonary disorders: silicosis, resolved tuberculosis, bronchiectasis, or chronic obstructive pulmonary disease
DIAGNOSIS CLINICAL SYNDROMES • Pulmonary • Lymphadenitis • Cutaneous and soft tissue • Osteoarticular • Catheter-associated • Disseminated • Pulmonary: Persistent cough typically yielding sputum. Advanced disease correlates with constitutional symptoms (e.g., weight loss, fatigue) and may encompass dyspnea, hemoptysis, and chest discomfort (2). • Soft tissue: Frequently linked to inoculation or recent surgical procedures or instrumentation. • Osteoarticular. • Disseminated: Characterized by fevers, tiredness, and anorexia. • Exposures: Water (cutaneous/soft tissue), catheters (bacteremia) • Suppression of the immune system
PHYSICAL EXAM • Pulmonary: Rales, wheezes, rhonchi. Pectus excavatum (27%) and scoliosis (52%) are prevalent among patients with pulmonary MAC. • Soft tissue: Minor, papular lesions typically located on the extremities; may become ulcerated and disseminate locally or via lymphatics. Lymphadenitis: An swollen lymph node, typically located in the submandibular or jugular area, that is either painless or mildly uncomfortable, but not fluctuant.
DIAGNOSTIC TESTS AND INTERPRETATION LAB Pancytopenia may arise due to marrow suppression in disseminated illness. • Increased alkaline phosphatase may be observed in 5% of disseminated MAC (20–40 times the normal level). • Mycobacterial blood cultures yield positive results in 90% of dispersed cases. Imaging: Preliminary Strategy Chest X-ray (CXR) or chest CT (pulmonary): Upper lobe cavitary illness, nodular or reticulonodular disease, or adenopathy. Pleural effusions are infrequent. Subsequent Actions & Unique Considerations • Serial imaging will be conducted to monitor for progression (if asymptomatic) or improvement (during therapy). Cavitary illness occurs in 60–90% of Mycobacterium avium complex lung infections. Cavitations may range from 2 to 4 centimeters in size and are generally characterized by thin walls. Diagnostic Procedures and Additional Methods • Tissue for acid-fast bacillus (AFB) smear, mycobacterial culture, and pathology is crucial, as these organisms may behave as colonizers (2). In cases of pulmonary disease, it is advisable to obtain three or more sputum samples (or perform bronchoalveolar lavage) for culture analysis. RNA probes can facilitate the first identification of M. tuberculosis, MAC, and M. kansasii from positive cultures. • Upon isolation, mycobacterial cultures must be dispatched to a specialized facility for confirming identification and antibiotic susceptibility assessment. Pathological Observations • Granuloma containing large cells and acid-fast bacilli observed in localized infection. In widespread illness, the presence of well-formed granulomas is less probable.
DIFFERENTIAL DIAGNOSIS
• Mycobacterium tuberculosis (MTb) • Other non-tuberculous mycobacteria (NTM) • Endemic fungi (histoplasmosis, cryptococcosis, blastomycosis, nocardiosis) • Pre-existing structural lung disease
TREATMENT MEDICATION
Initial Line • MAC (pulmonary): Rifampin 600 mg daily, ethambutol 15 or 25 mg/kg daily based on radiographic pattern, azithromycin or clarithromycin 500 mg, with the addition of an aminoglycoside as necessary (2). • Kansasii (pulmonary): Isoniazid 300 mg daily, rifampin 600 mg daily, ethambutol 15 mg/kg daily. • RGM (soft tissue): Two of the following agents to which the isolate is susceptible: Trimethoprim-sulfamethoxazole (TMP-SMX), doxycycline, levofloxacin, clarithromycin. • Severe abscess: Amikacin + clarithromycin + cefoxitin or imipenem • Fortuitum or chelonae (severe): Amikacin or tobramycin combined with cefoxitin, with the option of adding imipenem or levofloxacin. • MAC (disseminated/HIV): Administer clarithromycin 500 mg orally twice daily or azithromycin 500–600 mg orally twice daily, along with ethambutol 15 mg/kg orally daily; consider adding rifampin with input from infectious disease specialists. • M. marinum (soft tissue): Administer clarithromycin 500 mg orally twice daily and ethambutol 15 mg/kg, with the inclusion of rifampin for osteomyelitis and the potential for surgical debridement. Mild illness may be managed alone with clarithromycin. Second Line • Moxifloxacin 400 mg daily • Amikacin • M. abscessus: Linezolid, doxycycline, TMP–SMX ADDITIONAL THERAPY Comprehensive Strategies • Susceptibility testing is required for MAC (clarithromycin), kansasii (rifampin), and RGM (eight medicines on the susceptibility panel) (2). Treatment duration is extended; for pulmonary MAC, administer therapy for 12 months following negative cultures (totaling 12–24 months), and for disseminated MAC, treat for 12 months or 6 months beyond when CD4 counts exceed 100 cells/mm³. Skin and soft tissue infections may require three months or more of treatment. Catheter-associated infections necessitate 6 to 12 weeks of therapy following catheter removal. Referral Issues Due of the drug resistance of these indolent organisms, doctors with expertise in these illnesses are required for therapy. Occasionally, people necessitate years of treatment.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
• MAC: Lung resection is advisable for patients with upper lobe disease, particularly if they are intolerant to medical therapy or exhibit culture positivity after six months of antibiotic treatment. • MAC lymphadenitis: Resection yields a 90% cure rate without the use of antimicrobials. • Incision and drainage for soft tissue infections or tenosynovitis, particularly for rapidly growing mycobacteria.
INPATIENT CONSIDERATIONS
Criteria for Admission • For diagnostic evaluation. • For the commencement of parenteral antibiotics. CONTINUING CARE FOLLOW-UP SUGGESTIONS Monthly follow-up during the initial phases of treatment is frequently advised due to antimicrobial toxicity. • Following patient tolerance of drugs, follow-up intervals may be extended. Patient Surveillance • Laboratories for assessing medication toxicity. • Assessment for pharmacological interactions. • Monitoring therapeutic medication levels for antibacterial peaks and troughs.
PROGNOSIS
It is contingent upon the disease's location, the detection of non-tuberculous mycobacteria (NTM), and the particular host.
COMPLICATIONS
• Laboratories for assessing medication toxicity. • Evaluation of pharmacological interactions between drugs. • Disseminated MAC: Intussusception, gastrointestinal hemorrhage, and bowel blockage may develop, however these are few. • MAC lymphadenitis: Ulceration and the development of fistulas.


- Published on
Infectious Disease – Anaerobic Infections
• Anaerobic infections are induced by bacteria that necessitate diminished oxygen levels for proliferation.
Anaerobes linked to human diseases are aerotolerant; they can endure, but not proliferate, for up to 72 hours in an oxygen-rich environment.
Anaerobic bacteria inhabit mucosal membranes and are predominant in illnesses originating from mucosal and surrounding areas.
EPIDEMIOLOGY Incidence
Anaerobes comprise up to 10% of blood culture isolates in patients with clinically severe bacteremia. No incidence data exists for anaerobic infections at other sites.
FACTORS OF RISK
• Disruption of the mucosal barrier due to neoplasm, chemotherapy, radiation, neutropenia, graft-versus-host disease, surgical intervention, trauma, inflammatory bowel disease, diverticulitis, and appendicitis • Inadequate dental hygiene • Altered mental state, diminished gag reflex, and impaired swallowing
GENERAL PREVENTION
• Bowel preparation and preoperative antibacterial prophylaxis • Excellent oral hygiene • Aspiration precautions
Pathophysiology
• Translocation of indigenous flora into sterile sites resulting from mucosal membrane disruption • Translocation of oral flora into the lungs due to aspiration • Proliferation of obligate anaerobes during polymicrobial infections caused by reduced oxidation–reduction potential from aerobic organisms • Virulence factors allow anaerobic bacteria to induce abscess formation (e.g., Bacteroides fragilis: capsular polysaccharide), evade host defenses (e.g., Prevotella: IgA proteases), and adhere to cell surfaces
For instance, Porphyromonas gingivalis produces proteases, while Fusobacterium necrophorum generates leukotoxin and endotoxin.
ETIOLOGY
• B. fragilis is the predominant isolated anaerobic Gram-negative bacillus. Other Gram-negative bacteria include Fusobacterium, Prevotella, and Porphyromonas species. Peptostreptococcus species are the predominant Gram-positive cocci, while Clostridia represent the primary Gram-positive rods responsible for disease.
FREQUENTLY CO-OCCURRING CONDITIONS
• Dental infections – Pulpitis – Periapical and dental abscess – Perimandibular space infection • Gingivitis – Periodontitis – Periodontal abscess • Extension of periodontal infection resulting in maxillary sinus osteomyelitis or submandibular space infection • Vincent’s stomatitis (trench mouth) • Ludwig’s angina: Bilateral infection of the sublingual region and submandibular regions
Lemierre Syndrome: Infection of the posterior compartment of the lateral pharyngeal space by F. necrophorum, resulting in suppurative thrombophlebitis of the jugular vein and subsequent metastases, predominantly to the lungs.
• Chronic sinusitis and otitis media • Pleuropulmonary infections – Aspiration pneumonia – Necrotizing pneumonia – Lung abscess – Empyema
• Intra-abdominal infections – Peritonitis – Abscesses – Neutropenic colitis (Typhlitis) • Female genital tract infections – Pelvic inflammatory illness – Pelvic abscess – Septic abortion – Endometritis – Tubo-ovarian abscess – Postoperative infection
– Bacterial vaginosis – Pelvic cellulitis – Amnionitis – Septic thrombosis of pelvic veins • Central nervous system infections
Cerebral abscess, epidural abscess, subdural empyema
Anaerobic meningitis: Uncommon, indicative of shunt infection or parameningeal collection.
• Dermatological and subcutaneous conditions – Necrotizing fasciitis – Gas gangrene – Crepitant cellulitis – Bite injuries – Surgical incisions
– Diabetic foot infections – Pressure ulcers
• Bone and joint – Osteomyelitis and septic arthritis in proximity to affected soft tissue locations • Bacteremia – Resulting from an intra-abdominal, vaginal tract, respiratory tract, or soft tissue infection – B. fragilis is the most prevalent isolate
HISTORY OF DIAGNOSIS
• Abrupt emergence of sensitive, hemorrhaging gums, halitosis, unpleasant taste, fever, and cervical lymphadenopathy - Vincent’s stomatitis (trench mouth) • Pain in the submandibular and/or sublingual regions, trismus, and lateral or posterior displacement of the tongue leading to dysphagia and/or airway obstruction – Ludwig’s angina
• Nasopharyngitis or tonsillar abscess, succeeded 1–2 weeks later by pyrexia, submandibular angle lymphadenopathy, discomfort along the lateral portion of the sternocleidomastoid muscle, and pulmonary metastases.
Lemierre's syndrome
• Weight reduction, thoracic discomfort, or pleuritic pain - Empyema
• Persistent malaise, weight reduction, pyrexia, chills, malodorous sputum, and anemia – Anaerobic pulmonary abscess • Impaired cognitive function, dysphagia, chronic respiratory manifestations, weight reduction, pyrexia, and anemia
Aspiration pneumonia
• Neutropenia, right lower quadrant stomach discomfort, fever, diarrhea – Typhlitis • Lack of progress in the infectious process on an antibiotic regimen devoid of anaerobic activity – Indicative of anaerobes
PHYSICAL EXAMINATION
• Deteriorated dental condition – Prevalence of anaerobic oral microbiota with potential for translocation
• Gas in tissue, crepitus – Infection with gas-producing bacteria • Malodorous discharge • Infection near mucosal surfaces • Tissue necrosis, abscess development – Suggestive of anaerobic organisms DIAGNOSTIC TESTS & INTERPRETATION Laboratory
Anaerobes present significant challenges in cultivation and identification. In numerous instances, the anaerobic origin of an infection remains unverified.
• Cultural methodology
Specimens must be obtained while preventing contamination of the indigenous flora of mucosal surfaces.
- Liquids or tissues are preferred over swab specimens.
Air must be removed from the syringe utilized for aspiration, and the needle must be sealed.
– Utilization of anaerobic transport media. – Expedited processing of samples.
All specimens must undergo Gram staining; the absence of growth in culture alongside the presence of Gram-positive and Gram-negative organisms in Gram staining indicates the potential existence of anaerobic organisms.
Imaging • Radiographs – Presence of air–fluid levels, cavity formation, and gas in tissue • CT and/or MRI scans – Frequently essential for delineating anatomical location and disease extent
Diagnostic Procedures/Other: CT- or ultrasound-guided aspiration or biopsy
DIFFERENTIAL DIAGNOSIS
Anaerobic lung abscesses must be distinguished from mycobacterial infections.
TREATMENT
• The treatment comprises a combination of surgical interventions (resection, debridement, drainage) and antimicrobial therapy. • Antibiotics administered must encompass both aerobic and anaerobic bacteria due to the polymicrobial characteristics of numerous illnesses.
Empirical selection of antibiotic regimen based on infection type, Gram stain results, tissue penetration, and toxicity. Susceptibility testing is challenging because to anaerobic culture methodologies, prolonged turnaround times, and inadequate quality control.
• Susceptibility testing is advised for patients requiring extended antibiotic treatment: cerebral abscess, osteomyelitis, and infections associated with prosthetic devices. • Anaerobic infections originating from below the diaphragm should be managed with targeted therapy against B. fragilis. Members of the B. fragilis group exhibit resistance to penicillin.
Antimicrobial drugs effective against anaerobes include carbapenems, β-lactam/β-lactamase inhibitor combinations, and metronidazole (note that metronidazole is ineffective against Actinomyces spp., Propionibacterium spp., peptostreptococci, and microaerophilic streptococci).
• Rising incidence of antibiotic resistance in B. fragilis.
Resistance to cephamycins is 8–14%, clindamycin 26% and moxifloxacin 38%
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patient Surveillance
Ensure sufficient drainage of abscesses with further imaging.
Surgical resection is warranted if drainage proves ineffective.
• Conduct repeat sampling if the infection does not respond to antimicrobial therapy to assess for drug-resistant organisms.
• Surveillance for antimicrobial drug toxicities.
COMPLICATIONS
Uninterrupted dissemination of untreated illnesses
• Anaerobic infections are induced by bacteria that necessitate diminished oxygen levels for proliferation.
Anaerobes linked to human diseases are aerotolerant; they can endure, but not proliferate, for up to 72 hours in an oxygen-rich environment.
Anaerobic bacteria inhabit mucosal membranes and are predominant in illnesses originating from mucosal and surrounding areas.
EPIDEMIOLOGY Incidence
Anaerobes comprise up to 10% of blood culture isolates in patients with clinically severe bacteremia. No incidence data exists for anaerobic infections at other sites.
FACTORS OF RISK
• Disruption of the mucosal barrier due to neoplasm, chemotherapy, radiation, neutropenia, graft-versus-host disease, surgical intervention, trauma, inflammatory bowel disease, diverticulitis, and appendicitis • Inadequate dental hygiene • Altered mental state, diminished gag reflex, and impaired swallowing
GENERAL PREVENTION
• Bowel preparation and preoperative antibacterial prophylaxis • Excellent oral hygiene • Aspiration precautions
Pathophysiology
• Translocation of indigenous flora into sterile sites resulting from mucosal membrane disruption • Translocation of oral flora into the lungs due to aspiration • Proliferation of obligate anaerobes during polymicrobial infections caused by reduced oxidation–reduction potential from aerobic organisms • Virulence factors allow anaerobic bacteria to induce abscess formation (e.g., Bacteroides fragilis: capsular polysaccharide), evade host defenses (e.g., Prevotella: IgA proteases), and adhere to cell surfaces
For instance, Porphyromonas gingivalis produces proteases, while Fusobacterium necrophorum generates leukotoxin and endotoxin.
ETIOLOGY
• B. fragilis is the predominant isolated anaerobic Gram-negative bacillus. Other Gram-negative bacteria include Fusobacterium, Prevotella, and Porphyromonas species. Peptostreptococcus species are the predominant Gram-positive cocci, while Clostridia represent the primary Gram-positive rods responsible for disease.
FREQUENTLY CO-OCCURRING CONDITIONS
• Dental infections – Pulpitis – Periapical and dental abscess – Perimandibular space infection • Gingivitis – Periodontitis – Periodontal abscess • Extension of periodontal infection resulting in maxillary sinus osteomyelitis or submandibular space infection • Vincent’s stomatitis (trench mouth) • Ludwig’s angina: Bilateral infection of the sublingual region and submandibular regions
Lemierre Syndrome: Infection of the posterior compartment of the lateral pharyngeal space by F. necrophorum, resulting in suppurative thrombophlebitis of the jugular vein and subsequent metastases, predominantly to the lungs.
• Chronic sinusitis and otitis media • Pleuropulmonary infections – Aspiration pneumonia – Necrotizing pneumonia – Lung abscess – Empyema
• Intra-abdominal infections – Peritonitis – Abscesses – Neutropenic colitis (Typhlitis) • Female genital tract infections – Pelvic inflammatory illness – Pelvic abscess – Septic abortion – Endometritis – Tubo-ovarian abscess – Postoperative infection
– Bacterial vaginosis – Pelvic cellulitis – Amnionitis – Septic thrombosis of pelvic veins • Central nervous system infections
Cerebral abscess, epidural abscess, subdural empyema
Anaerobic meningitis: Uncommon, indicative of shunt infection or parameningeal collection.
• Dermatological and subcutaneous conditions – Necrotizing fasciitis – Gas gangrene – Crepitant cellulitis – Bite injuries – Surgical incisions
– Diabetic foot infections – Pressure ulcers
• Bone and joint – Osteomyelitis and septic arthritis in proximity to affected soft tissue locations • Bacteremia – Resulting from an intra-abdominal, vaginal tract, respiratory tract, or soft tissue infection – B. fragilis is the most prevalent isolate
HISTORY OF DIAGNOSIS
• Abrupt emergence of sensitive, hemorrhaging gums, halitosis, unpleasant taste, fever, and cervical lymphadenopathy - Vincent’s stomatitis (trench mouth) • Pain in the submandibular and/or sublingual regions, trismus, and lateral or posterior displacement of the tongue leading to dysphagia and/or airway obstruction – Ludwig’s angina
• Nasopharyngitis or tonsillar abscess, succeeded 1–2 weeks later by pyrexia, submandibular angle lymphadenopathy, discomfort along the lateral portion of the sternocleidomastoid muscle, and pulmonary metastases.
Lemierre's syndrome
• Weight reduction, thoracic discomfort, or pleuritic pain - Empyema
• Persistent malaise, weight reduction, pyrexia, chills, malodorous sputum, and anemia – Anaerobic pulmonary abscess • Impaired cognitive function, dysphagia, chronic respiratory manifestations, weight reduction, pyrexia, and anemia
Aspiration pneumonia
• Neutropenia, right lower quadrant stomach discomfort, fever, diarrhea – Typhlitis • Lack of progress in the infectious process on an antibiotic regimen devoid of anaerobic activity – Indicative of anaerobes
PHYSICAL EXAMINATION
• Deteriorated dental condition – Prevalence of anaerobic oral microbiota with potential for translocation
• Gas in tissue, crepitus – Infection with gas-producing bacteria • Malodorous discharge • Infection near mucosal surfaces • Tissue necrosis, abscess development – Suggestive of anaerobic organisms DIAGNOSTIC TESTS & INTERPRETATION Laboratory
Anaerobes present significant challenges in cultivation and identification. In numerous instances, the anaerobic origin of an infection remains unverified.
• Cultural methodology
Specimens must be obtained while preventing contamination of the indigenous flora of mucosal surfaces.
- Liquids or tissues are preferred over swab specimens.
Air must be removed from the syringe utilized for aspiration, and the needle must be sealed.
– Utilization of anaerobic transport media. – Expedited processing of samples.
All specimens must undergo Gram staining; the absence of growth in culture alongside the presence of Gram-positive and Gram-negative organisms in Gram staining indicates the potential existence of anaerobic organisms.
Imaging • Radiographs – Presence of air–fluid levels, cavity formation, and gas in tissue • CT and/or MRI scans – Frequently essential for delineating anatomical location and disease extent
Diagnostic Procedures/Other: CT- or ultrasound-guided aspiration or biopsy
DIFFERENTIAL DIAGNOSIS
Anaerobic lung abscesses must be distinguished from mycobacterial infections.
TREATMENT
• The treatment comprises a combination of surgical interventions (resection, debridement, drainage) and antimicrobial therapy. • Antibiotics administered must encompass both aerobic and anaerobic bacteria due to the polymicrobial characteristics of numerous illnesses.
Empirical selection of antibiotic regimen based on infection type, Gram stain results, tissue penetration, and toxicity. Susceptibility testing is challenging because to anaerobic culture methodologies, prolonged turnaround times, and inadequate quality control.
• Susceptibility testing is advised for patients requiring extended antibiotic treatment: cerebral abscess, osteomyelitis, and infections associated with prosthetic devices. • Anaerobic infections originating from below the diaphragm should be managed with targeted therapy against B. fragilis. Members of the B. fragilis group exhibit resistance to penicillin.
Antimicrobial drugs effective against anaerobes include carbapenems, β-lactam/β-lactamase inhibitor combinations, and metronidazole (note that metronidazole is ineffective against Actinomyces spp., Propionibacterium spp., peptostreptococci, and microaerophilic streptococci).
• Rising incidence of antibiotic resistance in B. fragilis.
Resistance to cephamycins is 8–14%, clindamycin 26% and moxifloxacin 38%
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patient Surveillance
Ensure sufficient drainage of abscesses with further imaging.
Surgical resection is warranted if drainage proves ineffective.
• Conduct repeat sampling if the infection does not respond to antimicrobial therapy to assess for drug-resistant organisms.
• Surveillance for antimicrobial drug toxicities.
COMPLICATIONS
Uninterrupted dissemination of untreated illnesses

- Published on
Infectious Disease - Amebiasis
Protozoan infection induced by Entamoeba histolytica. Infection by these organisms results in diarrhea, colitis, and occasionally, extra-intestinal symptoms such as liver abscesses.
• Symptomatic illness manifests in fewer than 10% of affected persons. A minimal proportion of individuals with intestinal infections will progress to invasive illness.
Epidemiology
Frequency
Approximately ten percent of the global population is thought to be infected with E. histolytica.
• Prevalence varies from less than 5% in developed nations to 20–30% in tropical regions.
The estimated prevalence in the US is approximately 4%.
The disease manifests across all age groups and affects both genders equally.
RISK FACTORS • Risk factors in endemic regions encompass: – Low socioeconomic status – Inadequate sanitation
– Overcrowding • In nations with low prevalence:
- Immigrants or travelers from endemic areas – Institutionalized individuals – Males engaging in sexual relations with other males
• Risk factors linked to serious disease: - Newborns – Gestation
Corticosteroid treatment; malnutrition.
COMPREHENSIVE PREVENTION
• Humans constitute the sole reservoir of the infection.
Contaminated water or vegetables frequently serve as sources of infection in humans.
Cysts are not eliminated by chlorine; boiling water is essential for decontamination.
• Refrain from consuming polluted water and food. • Ensure that vegetables are thoroughly cleansed with potable water or treated with detergent and immersed in acetic acid or vinegar.
PATHOPHYSIOLOGY
• Infection transmits through the fecal–oral pathway • The organism manifests in two forms:
Trophozoite possessing a singular nucleus, with or without swallowed erythrocytes.
Cyst with four nuclei
The ingestion of the cyst leads to excystation in the small intestine. Trophozoites are generated, infecting the colon and causing symptoms.
• Under adverse conditions, the trophozoite encysts, and the cyst form is excreted in feces.
Cysts persist in a damp environment for several months.
• The majority of individuals infected with the bacterium exhibit minimal invasion of the intestinal mucosa and remain asymptomatic (cyst passers).
Patients exhibiting colonic invasion present with flask-shaped colonic ulcers.
ETIOLOGY • E. histolytica is one of the several Entamoeba species that infect people.
Nonpathogenic species encompass Entamoeba dispar, Entamoeba moshkovskii (both morphologically indistinguishable), Entamoeba hartmanni, and Entamoeba coli.
HISTORY OF DIAGNOSIS
• Patients exhibit symptoms of invasive illness within four weeks following the intake of cysts.
Amebic liver abscess typically requires approximately three months for development.
• Certain patients harbor the germs for extended durations prior to exhibiting notable clinical symptoms. • Intestinal disorder – Asymptomatic infection
— Symptomatic non-invasive infection
- Symptoms are minor; diarrhea is the sole manifestation. - Amebic colitis (dysentery) - Crampy abdominal discomfort - Hemorrhagic, mucoid diarrhea - Rectal hemorrhage may accompany diarrhea, particularly in pediatric patients - Fever is present in one-third of affected individuals – Weight reduction – Anorexia nervosa
• Extra-intestinal disease – Extra-intestinal amebiasis can impact the liver (abscess), spleen, lungs, or brain.
Amebic liver abscess manifests with fever and right upper quadrant pain.
ache in the upper quadrant. Fifty percent of patients with amebic liver abscess exhibit no prior history of colitis.
– Occasionally, the rupture of the abscess may result in peritonitis.
– Rupture of the liver abscess into the pleural cavity results in empyema. Patients exhibit fever, dyspnea, and pleuritic thoracic pain.
Cerebral amebiasis: Nausea, vomiting, cephalalgia, alterations in mental condition
PHYSICAL EXAMINATION
• Colitis – Widespread abdominal pain – Distension, rebound tenderness in severe colitis/perforation • Liver abscess – pain upon palpation of the liver Hepatomegaly - Jaundice is infrequent
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Stool microscopy and O&P examination may reveal the presence of stool leukocytes.
- Intracytoplasmic erythrocytes within trophozoites (observed)
In E. histolytica and E. dispar, a wet mount for motile trophozoites and formal-ether concentration, followed by an iodine-stained deposit, enhances the probability of finding cysts.
– To enhance the efficacy of microscopic diagnosis, many samples must be analyzed. • Antigen detection – Fecal antigen identified with ELISA. More sensitive than O&P, however less effective than PCR. Requires either fresh or frozen specimens.
Applicable in hepatic abscess fluid.
– The TechLab E. histolytica II ELISA differentiates between pathogenic and nonpathogenic amebae• Serology – Beneficial in diagnosing liver abscess and invasive colonic illness – ELISA (most frequently utilized), indirect immunofluorescent assay, indirect hemagglutination assay – False positives in the early stages of the disease – Titers persist at elevated levels for years – In endemic regions, high seropositivity precludes differentiation between active and prior infection.
• Culture is conducted exclusively in research laboratories. • PCR – Real-time PCR is technically intricate yet exhibits more sensitivity than the stool antigen.
- Applicable in hepatic abscess fluid. • Additional laboratory examinations
Leukocytosis absent of eosinophilia is frequently observed in individuals with invasive amebic illness. Elevated alkaline phosphatase levels and moderately increased transaminases are noted in liver abscess cases.
Imaging
Imaging modalities, including ultrasound, CT, and MRI scans, are beneficial in evaluating patients with suspected amebic liver abscess. The amebic abscess is typically situated in the right lobe, specifically in the right upper posterior section of the liver.
Diagnostic Procedures and Additional Methods
• Colonoscopy and biopsy for colonic pathology – Results may appear normal in the first stages of the condition
– Fragile, ulcerated mucosa exhibiting punctate hemorrhages – Lateral infiltration into the submucosal tissues results in the distinctive flask-shaped ulcer associated with amebic colitis – Amebomas manifest as annular lesions
The aspiration of a liver abscess produces dark, odorless, sterile pus, typically referred to as "anchovy paste," which may contain trophozoites. Aspiration of liver abscesses frequently does not yield the organism, as it resides within the abscess walls.
Pathological Observations
Intestinal biopsy specimens obtained from the margins of ulcers must be assessed for motile trophozoites.
• The biopsy reveals mucosal thickening with many distinct ulcers interspersed among areas of normal-appearing mucosa.
DIFFERENTIAL DIAGNOSIS
• Ulcerative colitis • Colorectal carcinoma • Crohn's disease • Diverticulitis • Abdominal abscess • Irritable bowel syndrome • Pyogenic abscess • Hepatoma • Echinococcal liver cyst
MEDICATION FOR TREATMENT
• Asymptomatic disease – Intra-luminal carriage necessitates treatment due to the potential risk of invasive disease.
Paromomycin 500 mg orally three times day for seven days should be used as the first-line treatment.
Diloxanide furoate 500 mg three times daily for 10 days Iodoquinol 650 mg orally three times daily for 20 days
• Colitis – Metronidazole 750 mg orally three times daily for 10 days or tinidazole 1 g orally twice daily for 3 days, followed by one of the subsequent treatments:
Iodoquinol 650 mg orally three times daily for 20 days
Paromomycin 500 mg orally three times daily for seven days • Liver abscess – Administer Metronidazole 750 mg orally or intravenously three times daily for 10 days, followed by Iodoquinol 650 mg orally three times daily for 20 days
CLINICAL INTERVENTIONS/ADDITIONAL PROCEDURES
For a substantial abscess (>3 cm), aspiration and needle intervention
Drainage is warranted. Minor abscesses dissolve with medical intervention.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patients undergoing treatment for liver abscesses should receive follow-up ultrasounds to confirm cyst clearance, which may require many months.
OUTLOOK
Amebiasis presents significant morbidity and mortality, particularly in underdeveloped nations.
COMPLICATIONS
Fulminant colitis accompanied with toxic megacolon, perforation, and peritonitis is uncommon however thoroughly documented.
Amebomas are mass lesions located in the colon, frequently found in the cecum or ascending colon, resulting from inflammation associated with amebic colitis. Amebomas can lead to blockage and may mimic colon cancer.
• Ruptured liver abscess with diaphragm perforation resulting in pleural or pericardial illness.
Protozoan infection induced by Entamoeba histolytica. Infection by these organisms results in diarrhea, colitis, and occasionally, extra-intestinal symptoms such as liver abscesses.
• Symptomatic illness manifests in fewer than 10% of affected persons. A minimal proportion of individuals with intestinal infections will progress to invasive illness.
Epidemiology
Frequency
Approximately ten percent of the global population is thought to be infected with E. histolytica.
• Prevalence varies from less than 5% in developed nations to 20–30% in tropical regions.
The estimated prevalence in the US is approximately 4%.
The disease manifests across all age groups and affects both genders equally.
RISK FACTORS • Risk factors in endemic regions encompass: – Low socioeconomic status – Inadequate sanitation
– Overcrowding • In nations with low prevalence:
- Immigrants or travelers from endemic areas – Institutionalized individuals – Males engaging in sexual relations with other males
• Risk factors linked to serious disease: - Newborns – Gestation
Corticosteroid treatment; malnutrition.
COMPREHENSIVE PREVENTION
• Humans constitute the sole reservoir of the infection.
Contaminated water or vegetables frequently serve as sources of infection in humans.
Cysts are not eliminated by chlorine; boiling water is essential for decontamination.
• Refrain from consuming polluted water and food. • Ensure that vegetables are thoroughly cleansed with potable water or treated with detergent and immersed in acetic acid or vinegar.
PATHOPHYSIOLOGY
• Infection transmits through the fecal–oral pathway • The organism manifests in two forms:
Trophozoite possessing a singular nucleus, with or without swallowed erythrocytes.
Cyst with four nuclei
The ingestion of the cyst leads to excystation in the small intestine. Trophozoites are generated, infecting the colon and causing symptoms.
• Under adverse conditions, the trophozoite encysts, and the cyst form is excreted in feces.
Cysts persist in a damp environment for several months.
• The majority of individuals infected with the bacterium exhibit minimal invasion of the intestinal mucosa and remain asymptomatic (cyst passers).
Patients exhibiting colonic invasion present with flask-shaped colonic ulcers.
ETIOLOGY • E. histolytica is one of the several Entamoeba species that infect people.
Nonpathogenic species encompass Entamoeba dispar, Entamoeba moshkovskii (both morphologically indistinguishable), Entamoeba hartmanni, and Entamoeba coli.
HISTORY OF DIAGNOSIS
• Patients exhibit symptoms of invasive illness within four weeks following the intake of cysts.
Amebic liver abscess typically requires approximately three months for development.
• Certain patients harbor the germs for extended durations prior to exhibiting notable clinical symptoms. • Intestinal disorder – Asymptomatic infection
— Symptomatic non-invasive infection
- Symptoms are minor; diarrhea is the sole manifestation. - Amebic colitis (dysentery) - Crampy abdominal discomfort - Hemorrhagic, mucoid diarrhea - Rectal hemorrhage may accompany diarrhea, particularly in pediatric patients - Fever is present in one-third of affected individuals – Weight reduction – Anorexia nervosa
• Extra-intestinal disease – Extra-intestinal amebiasis can impact the liver (abscess), spleen, lungs, or brain.
Amebic liver abscess manifests with fever and right upper quadrant pain.
ache in the upper quadrant. Fifty percent of patients with amebic liver abscess exhibit no prior history of colitis.
– Occasionally, the rupture of the abscess may result in peritonitis.
– Rupture of the liver abscess into the pleural cavity results in empyema. Patients exhibit fever, dyspnea, and pleuritic thoracic pain.
Cerebral amebiasis: Nausea, vomiting, cephalalgia, alterations in mental condition
PHYSICAL EXAMINATION
• Colitis – Widespread abdominal pain – Distension, rebound tenderness in severe colitis/perforation • Liver abscess – pain upon palpation of the liver Hepatomegaly - Jaundice is infrequent
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory
• Stool microscopy and O&P examination may reveal the presence of stool leukocytes.
- Intracytoplasmic erythrocytes within trophozoites (observed)
In E. histolytica and E. dispar, a wet mount for motile trophozoites and formal-ether concentration, followed by an iodine-stained deposit, enhances the probability of finding cysts.
– To enhance the efficacy of microscopic diagnosis, many samples must be analyzed. • Antigen detection – Fecal antigen identified with ELISA. More sensitive than O&P, however less effective than PCR. Requires either fresh or frozen specimens.
Applicable in hepatic abscess fluid.
– The TechLab E. histolytica II ELISA differentiates between pathogenic and nonpathogenic amebae• Serology – Beneficial in diagnosing liver abscess and invasive colonic illness – ELISA (most frequently utilized), indirect immunofluorescent assay, indirect hemagglutination assay – False positives in the early stages of the disease – Titers persist at elevated levels for years – In endemic regions, high seropositivity precludes differentiation between active and prior infection.
• Culture is conducted exclusively in research laboratories. • PCR – Real-time PCR is technically intricate yet exhibits more sensitivity than the stool antigen.
- Applicable in hepatic abscess fluid. • Additional laboratory examinations
Leukocytosis absent of eosinophilia is frequently observed in individuals with invasive amebic illness. Elevated alkaline phosphatase levels and moderately increased transaminases are noted in liver abscess cases.
Imaging
Imaging modalities, including ultrasound, CT, and MRI scans, are beneficial in evaluating patients with suspected amebic liver abscess. The amebic abscess is typically situated in the right lobe, specifically in the right upper posterior section of the liver.
Diagnostic Procedures and Additional Methods
• Colonoscopy and biopsy for colonic pathology – Results may appear normal in the first stages of the condition
– Fragile, ulcerated mucosa exhibiting punctate hemorrhages – Lateral infiltration into the submucosal tissues results in the distinctive flask-shaped ulcer associated with amebic colitis – Amebomas manifest as annular lesions
The aspiration of a liver abscess produces dark, odorless, sterile pus, typically referred to as "anchovy paste," which may contain trophozoites. Aspiration of liver abscesses frequently does not yield the organism, as it resides within the abscess walls.
Pathological Observations
Intestinal biopsy specimens obtained from the margins of ulcers must be assessed for motile trophozoites.
• The biopsy reveals mucosal thickening with many distinct ulcers interspersed among areas of normal-appearing mucosa.
DIFFERENTIAL DIAGNOSIS
• Ulcerative colitis • Colorectal carcinoma • Crohn's disease • Diverticulitis • Abdominal abscess • Irritable bowel syndrome • Pyogenic abscess • Hepatoma • Echinococcal liver cyst
MEDICATION FOR TREATMENT
• Asymptomatic disease – Intra-luminal carriage necessitates treatment due to the potential risk of invasive disease.
Paromomycin 500 mg orally three times day for seven days should be used as the first-line treatment.
Diloxanide furoate 500 mg three times daily for 10 days Iodoquinol 650 mg orally three times daily for 20 days
• Colitis – Metronidazole 750 mg orally three times daily for 10 days or tinidazole 1 g orally twice daily for 3 days, followed by one of the subsequent treatments:
Iodoquinol 650 mg orally three times daily for 20 days
Paromomycin 500 mg orally three times daily for seven days • Liver abscess – Administer Metronidazole 750 mg orally or intravenously three times daily for 10 days, followed by Iodoquinol 650 mg orally three times daily for 20 days
CLINICAL INTERVENTIONS/ADDITIONAL PROCEDURES
For a substantial abscess (>3 cm), aspiration and needle intervention
Drainage is warranted. Minor abscesses dissolve with medical intervention.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
Patients undergoing treatment for liver abscesses should receive follow-up ultrasounds to confirm cyst clearance, which may require many months.
OUTLOOK
Amebiasis presents significant morbidity and mortality, particularly in underdeveloped nations.
COMPLICATIONS
Fulminant colitis accompanied with toxic megacolon, perforation, and peritonitis is uncommon however thoroughly documented.
Amebomas are mass lesions located in the colon, frequently found in the cecum or ascending colon, resulting from inflammation associated with amebic colitis. Amebomas can lead to blockage and may mimic colon cancer.
• Ruptured liver abscess with diaphragm perforation resulting in pleural or pericardial illness.

