- Published on
Infectious Disease – Blastomycosis
FUNDAMENTAL DESCRIPTION
Acute or chronic infection resulting from Blastomyces dermatitidis, a dimorphic fungus present in soil.
EPIDEMIOLOGY
Occurrence
• Annual incidence ranges from 0.3 to 1.8 incidents per 100,000 (1).
• Up to 7.4 hospital admissions per 1 million individuals in endemic areas (1).
RISK FACTOR
• Location: Endemic in soil adjacent to aquatic environments in the Southeastern United States and the valleys of the Mississippi, Ohio, and St. Lawrence Rivers. Additionally, the Mediterranean coast, South America, Mexico, and Africa. Previously regarded as more common in middle-aged men, but more likely attributed to environmental exposures.
• Immunocompromised individuals are at heightened risk for more severe disease and adverse outcomes.
GENERAL PREVENTION MEASURES
Mitigation of exposure; utilization of breathing masks for individuals at occupational risk
Pathophysiology
• Inhalation of conidia from B. dermatitidis may lead to secondary hematogenous dissemination.
The immune system is more efficient against conidia than against the yeast form. Blastomyces transform into budding yeast within tissue, thereby exhibiting reduced vulnerability to immune system eradication.
• Reactivation in immunocompromised individuals.
ETIOLOGY
Dimorphic fungus, Blastomyces dermatitidis
HISTORY OF DIAGNOSIS
• Acute pneumonia: Abrupt manifestation of symptoms akin to bacterial pneumonia, encompassing:
- Pyrexia, nocturnal diaphoresis
- Productive cough, dyspnea, and pleuritic chest discomfort (60–90%)
– Rash (60 percent)
• Chronic pneumonia: Gradual emergence of symptoms akin to pulmonary tuberculosis
- Pyrexia, nocturnal diaphoresis, weight reduction
Mild productive cough, occasionally accompanied by chest discomfort and hemoptysis.
• Additional factors (contingent upon the infection site):
– Eruption – Asymptomatic soft-tissue edema
Meningitis or localized neurological impairment
PHYSICAL EXAMINATION
• Pulmonary: Auscultatory findings include crackles and rhonchi.
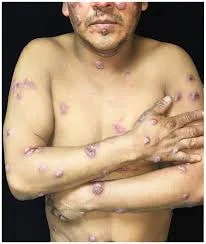
• Dermatological lesions: Generally non-painful papules or nodules.
. May present as either verrucous or ulcerated and cause discomfort.
• Non-tender soft tissue edema, occasionally accompanied by a draining tract.
DIAGNOSTIC EXAMINATIONS AND ANALYSIS
Laboratory
• There is no commercially available serological test due to cross-reactivity with other endemic mycoses.
• Urine antigen testing is accessible but not extensively utilized due to cross-reactivity.
Imaging
Preliminary strategy
Chest radiograph (CXR): Mass, many nodules, lobar infiltration, cavitation. Lymphadenopathy is infrequent.
Subsequent Actions & Unique Considerations
Additional clinical manifestations include genitourinary tract infections, septic arthritis, osteomyelitis, ocular infections, central nervous system infections (meningitis, cerebral abscess), and oropharyngeal abscess (1).
Diagnostic Procedures and Additional Methods
• Culture: 86% positive for sputum; 92% positive for bronchoalveolar lavage (BAL)
• Wet preparation: 46% sensitivity (multiple specimens utilizing KOH or calcofluor white)
• Attributes: Substantial yeast structures (8–15 mm in diameter) exhibiting a solitary broad-based bud
Pathological Observations
• Pyogranulomas
• Fungal elements are more readily observed with methenamine silver stain or Periodic acid-Schiff stain (PAS).
DIFFERENTIAL DIAGNOSIS
• Atypical pneumonia (acute pneumonia)
Lung carcinoma or mycobacterial infection (chronic pneumonia)
• Squamous cell carcinoma (cutaneous lesions)
MEDICATION FOR TREATMENT
• Pulmonary or disseminated non-central nervous system illness (2):
- Administer Amphotericin B (or lipid/liposomal formulation) for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 6–12 months.
For mild to moderate disease, administer itraconazole 200 mg orally three times daily for 3 days, followed by 200 mg orally twice daily for 6 to 12 months. • CNS disease: - Administer Amphotericin B (lipid/liposomal formulation) at a dosage of 3–5 mg/kg intravenously for a duration of 4–6 weeks, followed by oral azole therapy for a minimum of 12 months.
Itraconazole 200 mg orally three times daily or twice daily. Alternatively, provide Fluconazole 800 mg orally each day. Voriconazole 200–400 mg orally, twice daily. • In immunocompromised individuals: Administer Amphotericin B for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 12 months.
– Contemplate lifelong administration of itraconazole 200 milligrams orally daily.
Pediatric Considerations
• Treatment for mild disease: Itraconazole, 10 mg/kg daily for 6–12 months. • Treatment for severe disease: Amphotericin (or liposomal) followed by itraconazole.
Considerations During Pregnancy
• Prescription: Amphotericin B only, due to the contraindication of azoles during pregnancy.
SUPPLEMENTARY THERAPY
Comprehensive Measures
Continuous surveillance for the toxicity of antifungal medicines.
SURGERY/OTHER PROCEDURES
Uncommon, in instances of central nervous system mass or abscess.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
• The death rate for ARDS, even with proper treatment, ranges from 50% to 89%.
• Diligent monitoring of neurological assessments in central nervous system disorders.
Admission Criteria: • Immunosuppression • Respiratory distress • Requirement for intravenous therapy
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Surveillance of the patient following treatment for approximately six months, due to the potential for relapse.
Patient Surveillance
• Therapeutic drug monitoring for itraconazole is advised after two weeks of treatment: Does not require to be accurate through or peak. The objective is to exceed 1.0 μg/mL and remain below 10 μg/mL (2).
• Conduct liver function tests (LFTs) every three months at a minimum during azole therapy.
NUTRITION
Itraconazole must be administered with food.
PATIENT EDUCATION
• Address the possibility of drug–drug interactions associated with itraconazole administration.
• Anxiety of recurrence despite the availability of suitable treatment (2).
PROGNOSIS
• A cure without relapse occurs in 90–97% of immunocompetent individuals treated with amphotericin.
• 40% mortality rate in immunocompromised individuals (bone marrow transplant [BMT], AIDS); marginally improved outcomes in solid-organ transplant recipients.
Considerations During Pregnancy
Results: Early diagnosis can lead to favorable outcomes; however, pregnant women are at increased risk for more severe disease due to their mild immunosuppression.
FUNDAMENTAL DESCRIPTION
Acute or chronic infection resulting from Blastomyces dermatitidis, a dimorphic fungus present in soil.
EPIDEMIOLOGY
Occurrence
• Annual incidence ranges from 0.3 to 1.8 incidents per 100,000 (1).
• Up to 7.4 hospital admissions per 1 million individuals in endemic areas (1).
RISK FACTOR
• Location: Endemic in soil adjacent to aquatic environments in the Southeastern United States and the valleys of the Mississippi, Ohio, and St. Lawrence Rivers. Additionally, the Mediterranean coast, South America, Mexico, and Africa. Previously regarded as more common in middle-aged men, but more likely attributed to environmental exposures.
• Immunocompromised individuals are at heightened risk for more severe disease and adverse outcomes.
GENERAL PREVENTION MEASURES
Mitigation of exposure; utilization of breathing masks for individuals at occupational risk
Pathophysiology
• Inhalation of conidia from B. dermatitidis may lead to secondary hematogenous dissemination.
The immune system is more efficient against conidia than against the yeast form. Blastomyces transform into budding yeast within tissue, thereby exhibiting reduced vulnerability to immune system eradication.
• Reactivation in immunocompromised individuals.
ETIOLOGY
Dimorphic fungus, Blastomyces dermatitidis
HISTORY OF DIAGNOSIS
• Acute pneumonia: Abrupt manifestation of symptoms akin to bacterial pneumonia, encompassing:
- Pyrexia, nocturnal diaphoresis
- Productive cough, dyspnea, and pleuritic chest discomfort (60–90%)
– Rash (60 percent)
• Chronic pneumonia: Gradual emergence of symptoms akin to pulmonary tuberculosis
- Pyrexia, nocturnal diaphoresis, weight reduction
Mild productive cough, occasionally accompanied by chest discomfort and hemoptysis.
• Additional factors (contingent upon the infection site):
– Eruption – Asymptomatic soft-tissue edema
Meningitis or localized neurological impairment
PHYSICAL EXAMINATION
• Pulmonary: Auscultatory findings include crackles and rhonchi.
• Dermatological lesions: Generally non-painful papules or nodules.
. May present as either verrucous or ulcerated and cause discomfort.
• Non-tender soft tissue edema, occasionally accompanied by a draining tract.
DIAGNOSTIC EXAMINATIONS AND ANALYSIS
Laboratory
• There is no commercially available serological test due to cross-reactivity with other endemic mycoses.
• Urine antigen testing is accessible but not extensively utilized due to cross-reactivity.
Imaging
Preliminary strategy
Chest radiograph (CXR): Mass, many nodules, lobar infiltration, cavitation. Lymphadenopathy is infrequent.
Subsequent Actions & Unique Considerations
Additional clinical manifestations include genitourinary tract infections, septic arthritis, osteomyelitis, ocular infections, central nervous system infections (meningitis, cerebral abscess), and oropharyngeal abscess (1).
Diagnostic Procedures and Additional Methods
• Culture: 86% positive for sputum; 92% positive for bronchoalveolar lavage (BAL)
• Wet preparation: 46% sensitivity (multiple specimens utilizing KOH or calcofluor white)
• Attributes: Substantial yeast structures (8–15 mm in diameter) exhibiting a solitary broad-based bud
Pathological Observations
• Pyogranulomas
• Fungal elements are more readily observed with methenamine silver stain or Periodic acid-Schiff stain (PAS).
DIFFERENTIAL DIAGNOSIS
• Atypical pneumonia (acute pneumonia)
Lung carcinoma or mycobacterial infection (chronic pneumonia)
• Squamous cell carcinoma (cutaneous lesions)
MEDICATION FOR TREATMENT
• Pulmonary or disseminated non-central nervous system illness (2):
- Administer Amphotericin B (or lipid/liposomal formulation) for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 6–12 months.
For mild to moderate disease, administer itraconazole 200 mg orally three times daily for 3 days, followed by 200 mg orally twice daily for 6 to 12 months. • CNS disease: - Administer Amphotericin B (lipid/liposomal formulation) at a dosage of 3–5 mg/kg intravenously for a duration of 4–6 weeks, followed by oral azole therapy for a minimum of 12 months.
Itraconazole 200 mg orally three times daily or twice daily. Alternatively, provide Fluconazole 800 mg orally each day. Voriconazole 200–400 mg orally, twice daily. • In immunocompromised individuals: Administer Amphotericin B for 2 weeks, followed by itraconazole 200 mg orally three times daily for 3 days, then 200 mg orally twice daily for 12 months.
– Contemplate lifelong administration of itraconazole 200 milligrams orally daily.
Pediatric Considerations
• Treatment for mild disease: Itraconazole, 10 mg/kg daily for 6–12 months. • Treatment for severe disease: Amphotericin (or liposomal) followed by itraconazole.
Considerations During Pregnancy
• Prescription: Amphotericin B only, due to the contraindication of azoles during pregnancy.
SUPPLEMENTARY THERAPY
Comprehensive Measures
Continuous surveillance for the toxicity of antifungal medicines.
SURGERY/OTHER PROCEDURES
Uncommon, in instances of central nervous system mass or abscess.
INPATIENT CONSIDERATIONS
Preliminary Stabilization
• The death rate for ARDS, even with proper treatment, ranges from 50% to 89%.
• Diligent monitoring of neurological assessments in central nervous system disorders.
Admission Criteria: • Immunosuppression • Respiratory distress • Requirement for intravenous therapy
CONTINUED MANAGEMENT POST-TREATMENT GUIDELINES
Surveillance of the patient following treatment for approximately six months, due to the potential for relapse.
Patient Surveillance
• Therapeutic drug monitoring for itraconazole is advised after two weeks of treatment: Does not require to be accurate through or peak. The objective is to exceed 1.0 μg/mL and remain below 10 μg/mL (2).
• Conduct liver function tests (LFTs) every three months at a minimum during azole therapy.
NUTRITION
Itraconazole must be administered with food.
PATIENT EDUCATION
• Address the possibility of drug–drug interactions associated with itraconazole administration.
• Anxiety of recurrence despite the availability of suitable treatment (2).
PROGNOSIS
• A cure without relapse occurs in 90–97% of immunocompetent individuals treated with amphotericin.
• 40% mortality rate in immunocompromised individuals (bone marrow transplant [BMT], AIDS); marginally improved outcomes in solid-organ transplant recipients.
Considerations During Pregnancy
Results: Early diagnosis can lead to favorable outcomes; however, pregnant women are at increased risk for more severe disease due to their mild immunosuppression.
0 Comments
