- Published on
Emergency and Acute Medicine – Paronychia
Paronychia is an inflammatory condition of the nail folds surrounding the nail plate that occurs when disruption of the protective seal between the nail plate and nail fold allows microorganisms to enter the eponychial space. This disruption commonly follows minor trauma and leads to localized infection and inflammation.
The etiology differs between acute and chronic paronychia. Acute paronychia is most commonly caused by *Staphylococcus aureus*, although streptococci, *Pseudomonas*, and anaerobic organisms may also be involved. Chronic paronychia is multifactorial and results from repeated exposure to allergens and irritants, with fungal organisms—most commonly *Candida albicans*—frequently coexisting alongside *Staphylococcus* species.
Clinically, paronychia presents with pain, warmth, swelling, and erythema of the proximal or lateral nail folds, usually developing two to five days after trauma. For symptoms to meet criteria for chronic paronychia, they must persist for more than six weeks. A careful history is important. Acute paronychia is often associated with nail biting, finger sucking, aggressive manicuring, or direct trauma. Chronic paronychia is commonly seen in individuals with occupations involving persistent moisture exposure, such as dishwashers or bartenders, and occurs more frequently in patients with diabetes or peripheral vascular disease. In children, infections often involve anaerobic oral flora due to nail biting.
On physical examination, early paronychia begins as localized erythema, swelling, and tenderness at the dorsolateral nail fold, which may bulge over the nail plate. As the condition progresses, a subcuticular or subungual abscess may form. Green discoloration of the nail suggests *Pseudomonas* infection, while nail plate hypertrophy raises concern for a fungal etiology.
The diagnosis of paronychia is primarily clinical and based on history and physical examination. Evaluation should include assessment for associated infections such as felon or cellulitis and confirmation of tetanus immunization status. Laboratory testing is generally not helpful, and cultures are not routinely indicated. If herpetic whitlow is suspected, a Tzanck smear or viral culture may be considered. Imaging with soft tissue radiographs is reserved for suspected foreign bodies or possible osteomyelitis. A digital pressure test, using opposing pressure between the thumb and affected finger, may help identify early subungual abscess formation.
Management depends on the stage and type of paronychia. Early acute paronychia without purulence can often be treated with warm-water soaks four times daily, with or without topical antibiotics or corticosteroids. If a superficial abscess is present, elevation of the eponychial fold using a small blade or needle may allow adequate drainage; local anesthesia or a digital nerve block may be required. When infection extends beneath the nail plate, partial nail removal may be necessary, while extensive subungual abscesses may require complete nail removal. Runaround abscesses involving both sides of the nail fold require partial proximal nail removal with packing to prevent re-adhesion.
Antibiotic therapy is recommended when there is cellulitis, abscess formation, or systemic signs of infection. Appropriate first-line oral agents include trimethoprim–sulfamethoxazole, dicloxacillin, or amoxicillin–clavulanate, typically for five to ten days depending on severity. Clindamycin or amoxicillin–clavulanate is preferred when infection is associated with nail biting or oral exposure. Chronic paronychia management focuses on avoidance of irritants and moisture, with topical corticosteroids considered first-line therapy, often combined with a broad-spectrum topical antifungal. Refractory cases may require surgical eponychial marsupialization or oral antifungal therapy.
Admission is rarely required for paronychia alone. Patients with uncomplicated infections may be discharged with appropriate wound care instructions and follow-up. Those with packing in place should be re-evaluated within 24 hours. Referral is indicated for chronic or recurrent paronychia that does not respond to standard therapy.
Key clinical pearls include recognizing that acute paronychia generally responds well to timely drainage with or without antibiotics, while chronic paronychia is usually driven by repeated exposure to irritants rather than infection alone. Conditions such as psoriasis, Reiter syndrome, and herpetic whitlow can mimic paronychia and should be considered in recurrent or atypical cases.
Paronychia is an inflammatory condition of the nail folds surrounding the nail plate that occurs when disruption of the protective seal between the nail plate and nail fold allows microorganisms to enter the eponychial space. This disruption commonly follows minor trauma and leads to localized infection and inflammation.
The etiology differs between acute and chronic paronychia. Acute paronychia is most commonly caused by *Staphylococcus aureus*, although streptococci, *Pseudomonas*, and anaerobic organisms may also be involved. Chronic paronychia is multifactorial and results from repeated exposure to allergens and irritants, with fungal organisms—most commonly *Candida albicans*—frequently coexisting alongside *Staphylococcus* species.
Clinically, paronychia presents with pain, warmth, swelling, and erythema of the proximal or lateral nail folds, usually developing two to five days after trauma. For symptoms to meet criteria for chronic paronychia, they must persist for more than six weeks. A careful history is important. Acute paronychia is often associated with nail biting, finger sucking, aggressive manicuring, or direct trauma. Chronic paronychia is commonly seen in individuals with occupations involving persistent moisture exposure, such as dishwashers or bartenders, and occurs more frequently in patients with diabetes or peripheral vascular disease. In children, infections often involve anaerobic oral flora due to nail biting.
On physical examination, early paronychia begins as localized erythema, swelling, and tenderness at the dorsolateral nail fold, which may bulge over the nail plate. As the condition progresses, a subcuticular or subungual abscess may form. Green discoloration of the nail suggests *Pseudomonas* infection, while nail plate hypertrophy raises concern for a fungal etiology.
The diagnosis of paronychia is primarily clinical and based on history and physical examination. Evaluation should include assessment for associated infections such as felon or cellulitis and confirmation of tetanus immunization status. Laboratory testing is generally not helpful, and cultures are not routinely indicated. If herpetic whitlow is suspected, a Tzanck smear or viral culture may be considered. Imaging with soft tissue radiographs is reserved for suspected foreign bodies or possible osteomyelitis. A digital pressure test, using opposing pressure between the thumb and affected finger, may help identify early subungual abscess formation.
Management depends on the stage and type of paronychia. Early acute paronychia without purulence can often be treated with warm-water soaks four times daily, with or without topical antibiotics or corticosteroids. If a superficial abscess is present, elevation of the eponychial fold using a small blade or needle may allow adequate drainage; local anesthesia or a digital nerve block may be required. When infection extends beneath the nail plate, partial nail removal may be necessary, while extensive subungual abscesses may require complete nail removal. Runaround abscesses involving both sides of the nail fold require partial proximal nail removal with packing to prevent re-adhesion.
Antibiotic therapy is recommended when there is cellulitis, abscess formation, or systemic signs of infection. Appropriate first-line oral agents include trimethoprim–sulfamethoxazole, dicloxacillin, or amoxicillin–clavulanate, typically for five to ten days depending on severity. Clindamycin or amoxicillin–clavulanate is preferred when infection is associated with nail biting or oral exposure. Chronic paronychia management focuses on avoidance of irritants and moisture, with topical corticosteroids considered first-line therapy, often combined with a broad-spectrum topical antifungal. Refractory cases may require surgical eponychial marsupialization or oral antifungal therapy.
Admission is rarely required for paronychia alone. Patients with uncomplicated infections may be discharged with appropriate wound care instructions and follow-up. Those with packing in place should be re-evaluated within 24 hours. Referral is indicated for chronic or recurrent paronychia that does not respond to standard therapy.
Key clinical pearls include recognizing that acute paronychia generally responds well to timely drainage with or without antibiotics, while chronic paronychia is usually driven by repeated exposure to irritants rather than infection alone. Conditions such as psoriasis, Reiter syndrome, and herpetic whitlow can mimic paronychia and should be considered in recurrent or atypical cases.

- Published on
Emergency and Acute Medicine – Parkinson Disease
Parkinson disease (PD) is a gradually progressive neurodegenerative disorder that typically affects individuals in middle or late life. It is characterized by degeneration of dopaminergic neurons in the substantia nigra, formation of Lewy bodies in remaining neurons, and accelerated cortical atrophy. Although symptoms often begin unilaterally, the disease usually progresses to symmetric involvement. Parkinson disease affects approximately 1% of people over 60 years of age and up to 4% of those over 80. Importantly, nonspecific symptoms such as fatigue, constipation, and hyposmia may precede the diagnosis by many years, sometimes up to two decades.
The etiology of Parkinson disease is most often sporadic or idiopathic. However, several other conditions can present with parkinsonism and must be considered, especially in the emergency setting. These include drug-induced causes such as neuroleptics and sudden withdrawal of dopaminergic medications leading to parkinsonism–hyperpyrexia syndrome, as well as exposure to toxins like carbon monoxide, methanol, cyanide, organophosphates, and MPTP. Structural brain lesions involving the basal ganglia or midbrain, hydrocephalus, infections such as viral encephalitis or Mycoplasma, and other neurologic conditions like central pontine myelinolysis and encephalitis lethargica can also produce parkinsonian features.
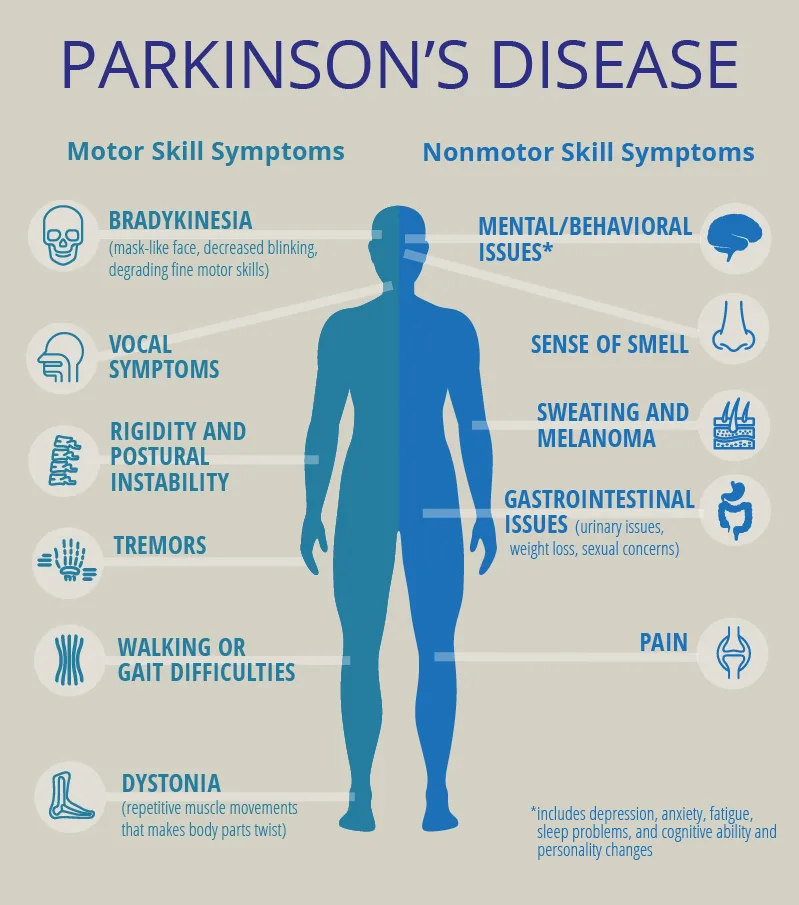
Clinical manifestations of Parkinson disease are divided into nonmotor and motor symptoms. Nonmotor symptoms include orthostatic hypotension, constipation, delayed gastric emptying, dysphagia, pain and sensory disturbances, depression, hallucinations, dementia, and sleep disorders. Motor symptoms are classically defined by resting “pill-rolling” tremor, cogwheel rigidity due to increased muscle tone, bradykinesia with marked slowness of movement, postural instability, stooped posture, and a reduced facial expression often described as a “masked face.” A sudden change in baseline motor function or mental status in a patient with known PD may be the only sign of an underlying systemic illness such as infection.
History is the cornerstone of diagnosis and emergency assessment. Important elements include the onset and progression of symptoms, whether the presentation was gradual or sudden, medication adherence, and exposure to drugs or toxins that may cause parkinsonism. Sudden withdrawal or noncompliance with dopaminergic therapy can precipitate parkinsonism–hyperpyrexia syndrome, a life-threatening condition marked by rigidity, hyperthermia, reduced consciousness, autonomic instability, and complications such as acute renal failure, rhabdomyolysis, venous thrombosis, and disseminated intravascular coagulation.
Physical examination typically reveals cogwheel rigidity, resting tremor, bradykinesia, and postural abnormalities. Diagnosis of Parkinson disease is primarily clinical, and no specific laboratory test is required to confirm it. In the emergency department, investigations are directed toward identifying alternative diagnoses, complications, or precipitants of deterioration. Laboratory studies may be indicated if parkinsonism–hyperpyrexia syndrome or infection is suspected. Neuroimaging with CT or MRI is not required to diagnose PD but may be performed to evaluate dementia or exclude other neurologic conditions. Chest radiography may be useful when respiratory infection is suspected.
The differential diagnosis of Parkinson disease is broad and includes essential tremor, benign familial tremor, major depression, Wilson disease, Huntington disease, Alzheimer disease, dementia with Lewy bodies, Creutzfeldt–Jakob disease, vitamin B12 deficiency, hypothyroidism, hydrocephalus, multi-infarct dementia, and toxic exposures such as carbon monoxide poisoning. Careful clinical assessment is essential to avoid misdiagnosis.
Management in the emergency department focuses on symptom control, identification and treatment of triggers, and prevention of complications. Antiparkinsonian medications may be initiated or adjusted in consultation with neurology. Patients with mild disease may not require immediate pharmacologic therapy, while those with moderate disease often benefit from dopaminergic or anticholinergic agents. Underlying infections or metabolic disturbances should be treated promptly. Parkinsonism–hyperpyrexia syndrome requires urgent replacement of dopaminergic therapy, supportive care, and management of associated complications.
Common medications used in Parkinson disease include carbidopa/levodopa as first-line therapy, dopamine agonists such as pramipexole and ropinirole, MAO-B inhibitors like selegiline and rasagiline, anticholinergics such as benztropine for tremor-dominant disease, and amantadine to stimulate dopamine release. Adjunctive agents like entacapone may be used to enhance levodopa bioavailability. In parkinsonism–hyperpyrexia syndrome, intravenous or enteral levodopa and bromocriptine are essential.
Admission is indicated for patients with Parkinson disease who present with serious medical conditions such as infection, trauma, cardiovascular or cerebrovascular emergencies, electrolyte disturbances, altered mental status, medication complications, failure to thrive, or suspected abuse. Patients with depression and suicidal intent or complications related to deep brain stimulation devices also require inpatient care. Stable patients with mild to moderate disease may be discharged with medications and urgent outpatient neurology follow-up.
Key clinical pearls include recognizing that Parkinson disease can be difficult to diagnose and is frequently confused with other neurologic conditions. Sudden withdrawal of dopaminergic medications is a medical emergency and must be avoided. In the emergency setting, vigilance for systemic illness, medication noncompliance, and life-threatening complications is critical to optimal patient outcomes.
Parkinson disease (PD) is a gradually progressive neurodegenerative disorder that typically affects individuals in middle or late life. It is characterized by degeneration of dopaminergic neurons in the substantia nigra, formation of Lewy bodies in remaining neurons, and accelerated cortical atrophy. Although symptoms often begin unilaterally, the disease usually progresses to symmetric involvement. Parkinson disease affects approximately 1% of people over 60 years of age and up to 4% of those over 80. Importantly, nonspecific symptoms such as fatigue, constipation, and hyposmia may precede the diagnosis by many years, sometimes up to two decades.
The etiology of Parkinson disease is most often sporadic or idiopathic. However, several other conditions can present with parkinsonism and must be considered, especially in the emergency setting. These include drug-induced causes such as neuroleptics and sudden withdrawal of dopaminergic medications leading to parkinsonism–hyperpyrexia syndrome, as well as exposure to toxins like carbon monoxide, methanol, cyanide, organophosphates, and MPTP. Structural brain lesions involving the basal ganglia or midbrain, hydrocephalus, infections such as viral encephalitis or Mycoplasma, and other neurologic conditions like central pontine myelinolysis and encephalitis lethargica can also produce parkinsonian features.
Clinical manifestations of Parkinson disease are divided into nonmotor and motor symptoms. Nonmotor symptoms include orthostatic hypotension, constipation, delayed gastric emptying, dysphagia, pain and sensory disturbances, depression, hallucinations, dementia, and sleep disorders. Motor symptoms are classically defined by resting “pill-rolling” tremor, cogwheel rigidity due to increased muscle tone, bradykinesia with marked slowness of movement, postural instability, stooped posture, and a reduced facial expression often described as a “masked face.” A sudden change in baseline motor function or mental status in a patient with known PD may be the only sign of an underlying systemic illness such as infection.
History is the cornerstone of diagnosis and emergency assessment. Important elements include the onset and progression of symptoms, whether the presentation was gradual or sudden, medication adherence, and exposure to drugs or toxins that may cause parkinsonism. Sudden withdrawal or noncompliance with dopaminergic therapy can precipitate parkinsonism–hyperpyrexia syndrome, a life-threatening condition marked by rigidity, hyperthermia, reduced consciousness, autonomic instability, and complications such as acute renal failure, rhabdomyolysis, venous thrombosis, and disseminated intravascular coagulation.
Physical examination typically reveals cogwheel rigidity, resting tremor, bradykinesia, and postural abnormalities. Diagnosis of Parkinson disease is primarily clinical, and no specific laboratory test is required to confirm it. In the emergency department, investigations are directed toward identifying alternative diagnoses, complications, or precipitants of deterioration. Laboratory studies may be indicated if parkinsonism–hyperpyrexia syndrome or infection is suspected. Neuroimaging with CT or MRI is not required to diagnose PD but may be performed to evaluate dementia or exclude other neurologic conditions. Chest radiography may be useful when respiratory infection is suspected.
The differential diagnosis of Parkinson disease is broad and includes essential tremor, benign familial tremor, major depression, Wilson disease, Huntington disease, Alzheimer disease, dementia with Lewy bodies, Creutzfeldt–Jakob disease, vitamin B12 deficiency, hypothyroidism, hydrocephalus, multi-infarct dementia, and toxic exposures such as carbon monoxide poisoning. Careful clinical assessment is essential to avoid misdiagnosis.
Management in the emergency department focuses on symptom control, identification and treatment of triggers, and prevention of complications. Antiparkinsonian medications may be initiated or adjusted in consultation with neurology. Patients with mild disease may not require immediate pharmacologic therapy, while those with moderate disease often benefit from dopaminergic or anticholinergic agents. Underlying infections or metabolic disturbances should be treated promptly. Parkinsonism–hyperpyrexia syndrome requires urgent replacement of dopaminergic therapy, supportive care, and management of associated complications.
Common medications used in Parkinson disease include carbidopa/levodopa as first-line therapy, dopamine agonists such as pramipexole and ropinirole, MAO-B inhibitors like selegiline and rasagiline, anticholinergics such as benztropine for tremor-dominant disease, and amantadine to stimulate dopamine release. Adjunctive agents like entacapone may be used to enhance levodopa bioavailability. In parkinsonism–hyperpyrexia syndrome, intravenous or enteral levodopa and bromocriptine are essential.
Admission is indicated for patients with Parkinson disease who present with serious medical conditions such as infection, trauma, cardiovascular or cerebrovascular emergencies, electrolyte disturbances, altered mental status, medication complications, failure to thrive, or suspected abuse. Patients with depression and suicidal intent or complications related to deep brain stimulation devices also require inpatient care. Stable patients with mild to moderate disease may be discharged with medications and urgent outpatient neurology follow-up.
Key clinical pearls include recognizing that Parkinson disease can be difficult to diagnose and is frequently confused with other neurologic conditions. Sudden withdrawal of dopaminergic medications is a medical emergency and must be avoided. In the emergency setting, vigilance for systemic illness, medication noncompliance, and life-threatening complications is critical to optimal patient outcomes.
- Published on
Emergency and Acute Medicine – Paraphimosis
Paraphimosis is a urologic emergency defined by entrapment of the retracted foreskin proximal to the glans penis. This entrapment leads to progressive lymphatic congestion and venous obstruction, which can ultimately compromise arterial blood flow to the glans. If not promptly recognized and treated, paraphimosis may result in ischemia, necrosis, and permanent penile injury.
The condition most commonly occurs when the foreskin is retracted and not returned to its normal position. Predisposing factors include phimosis, inflammation, trauma, and sexual inexperience, particularly in individuals unaware of the need to reduce the foreskin after intercourse. Paraphimosis is frequently iatrogenic, occurring after physical examination, urinary catheterization, cystoscopy, or genital hygiene when the foreskin is left retracted.
Patients typically present with penile pain, a visibly retracted foreskin, and a swollen, edematous glans. The glans may appear erythematous, dusky, or cyanotic as venous congestion progresses. Local cellulitis may be present, and in advanced or untreated cases, necrosis of the glans can develop. Physical examination should include careful inspection of the entire penis to exclude constricting foreign bodies or bands, such as hair tourniquets, wire, or string, which can mimic paraphimosis.
The diagnosis of paraphimosis is clinical and should be made based on history and physical examination alone. Treatment must not be delayed for laboratory or imaging studies. Imaging is generally unnecessary unless a foreign body is suspected, in which case radiographs may be obtained after restoration of adequate perfusion.
Initial management focuses on rapid reduction of edema and prompt return of the foreskin to its normal position to restore blood flow. Pain control is essential and may require local anesthesia, a penile nerve block, systemic analgesia, or conscious sedation, especially in children. Ice packs may be applied to the glans to reduce swelling while preparations for reduction are made. Manual reduction is the first-line treatment and involves circumferential compression of the edematous glans while simultaneously applying traction to advance the foreskin distally over the glans.
If manual reduction is unsuccessful, additional techniques may be employed to reduce edema. These include the multiple puncture technique, in which small-gauge needle punctures are made in the swollen foreskin to allow expression of edema fluid, followed by another attempt at manual reduction. Osmotic methods, such as application of gauze soaked in 50% dextrose, may also help decrease edema if immediate reduction is delayed. When noninvasive methods fail, a dorsal slit of the foreskin may be required to release the constricting ring. In some cases, suturing may be necessary after reduction if the incision is extensive.
Antibiotics are generally not required unless there is associated cellulitis or balanoposthitis. Once reduction is successful and symptoms resolve, most patients can be discharged with close urologic follow-up. Admission is indicated for patients with penile necrosis, severe infection, or inability to achieve reduction. Urologic consultation is recommended in all cases, and circumcision may be considered to prevent recurrence, although this remains a topic of clinical debate.
Patient education is essential to prevent recurrence. Patients should be instructed on proper foreskin hygiene and the importance of returning the foreskin to its normal position after retraction for cleaning, sexual activity, or medical procedures. Early recognition and prompt management are key to preventing serious complications of paraphimosis.
Paraphimosis is a urologic emergency defined by entrapment of the retracted foreskin proximal to the glans penis. This entrapment leads to progressive lymphatic congestion and venous obstruction, which can ultimately compromise arterial blood flow to the glans. If not promptly recognized and treated, paraphimosis may result in ischemia, necrosis, and permanent penile injury.
The condition most commonly occurs when the foreskin is retracted and not returned to its normal position. Predisposing factors include phimosis, inflammation, trauma, and sexual inexperience, particularly in individuals unaware of the need to reduce the foreskin after intercourse. Paraphimosis is frequently iatrogenic, occurring after physical examination, urinary catheterization, cystoscopy, or genital hygiene when the foreskin is left retracted.
Patients typically present with penile pain, a visibly retracted foreskin, and a swollen, edematous glans. The glans may appear erythematous, dusky, or cyanotic as venous congestion progresses. Local cellulitis may be present, and in advanced or untreated cases, necrosis of the glans can develop. Physical examination should include careful inspection of the entire penis to exclude constricting foreign bodies or bands, such as hair tourniquets, wire, or string, which can mimic paraphimosis.
The diagnosis of paraphimosis is clinical and should be made based on history and physical examination alone. Treatment must not be delayed for laboratory or imaging studies. Imaging is generally unnecessary unless a foreign body is suspected, in which case radiographs may be obtained after restoration of adequate perfusion.
Initial management focuses on rapid reduction of edema and prompt return of the foreskin to its normal position to restore blood flow. Pain control is essential and may require local anesthesia, a penile nerve block, systemic analgesia, or conscious sedation, especially in children. Ice packs may be applied to the glans to reduce swelling while preparations for reduction are made. Manual reduction is the first-line treatment and involves circumferential compression of the edematous glans while simultaneously applying traction to advance the foreskin distally over the glans.
If manual reduction is unsuccessful, additional techniques may be employed to reduce edema. These include the multiple puncture technique, in which small-gauge needle punctures are made in the swollen foreskin to allow expression of edema fluid, followed by another attempt at manual reduction. Osmotic methods, such as application of gauze soaked in 50% dextrose, may also help decrease edema if immediate reduction is delayed. When noninvasive methods fail, a dorsal slit of the foreskin may be required to release the constricting ring. In some cases, suturing may be necessary after reduction if the incision is extensive.
Antibiotics are generally not required unless there is associated cellulitis or balanoposthitis. Once reduction is successful and symptoms resolve, most patients can be discharged with close urologic follow-up. Admission is indicated for patients with penile necrosis, severe infection, or inability to achieve reduction. Urologic consultation is recommended in all cases, and circumcision may be considered to prevent recurrence, although this remains a topic of clinical debate.
Patient education is essential to prevent recurrence. Patients should be instructed on proper foreskin hygiene and the importance of returning the foreskin to its normal position after retraction for cleaning, sexual activity, or medical procedures. Early recognition and prompt management are key to preventing serious complications of paraphimosis.

- Published on
Emergency and Acute Medicine – Panic Attack
Panic attacks are characterized by sudden episodes of intense fear accompanied by prominent physical symptoms that peak rapidly, usually within 10 minutes, and resolve within approximately 20–30 minutes. Some patients, particularly those with medical illness, may experience a nonfearful variant dominated by somatic symptoms. Panic disorder is defined by recurrent, unexpected panic attacks followed by at least one month of persistent concern about additional attacks, worry about their implications, or maladaptive behavioral changes such as avoidance. Panic disorder may occur with or without agoraphobia, which reflects anxiety related to fear of being unable to escape or obtain help. The condition is often episodic or chronic and is frequently comorbid with depression, substance use disorders, functional disability, and increased suicidal risk.
The underlying mechanism involves dysregulation of the limbic system with excessive norepinephrine release and altered serotonergic and benzodiazepine receptor function, triggering a maladaptive “fight-or-flight” response. Genetic factors play an important role, with family history of panic or anxiety disorders commonly reported. Risk factors include major life stressors in the year preceding onset, childhood shyness or separation anxiety, female sex, and stimulant use such as cocaine. Panic attacks may initially arise in the context of physical illness or substance use and persist even after the precipitating condition has resolved.
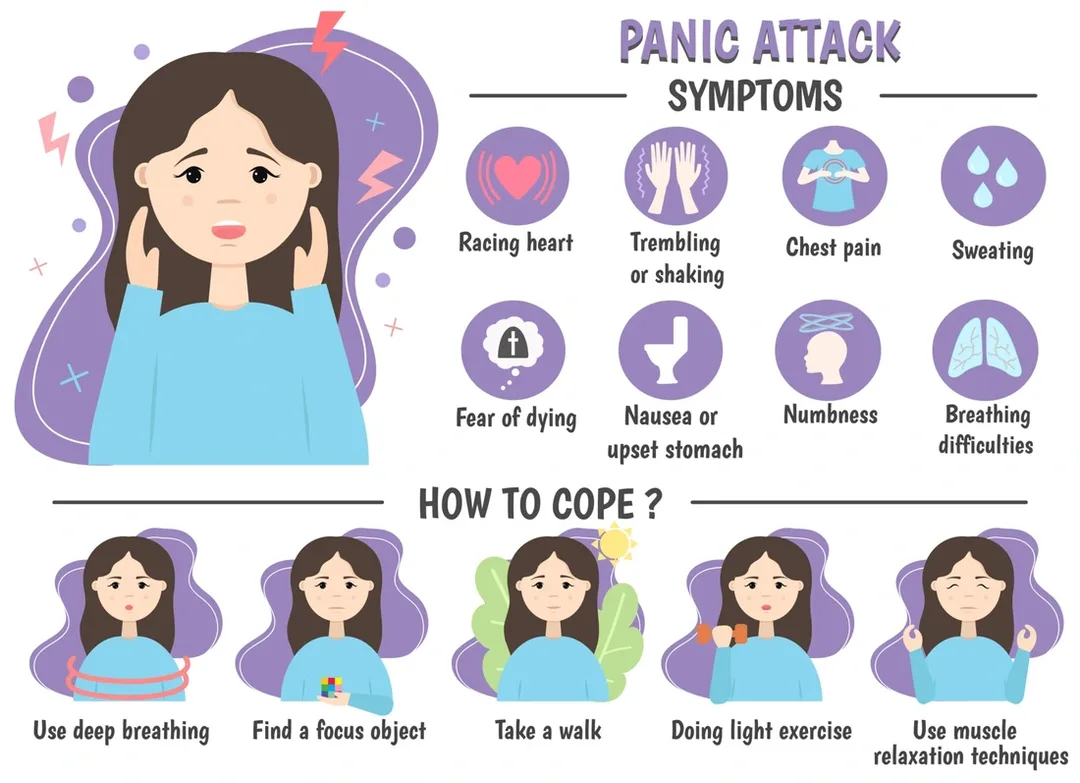
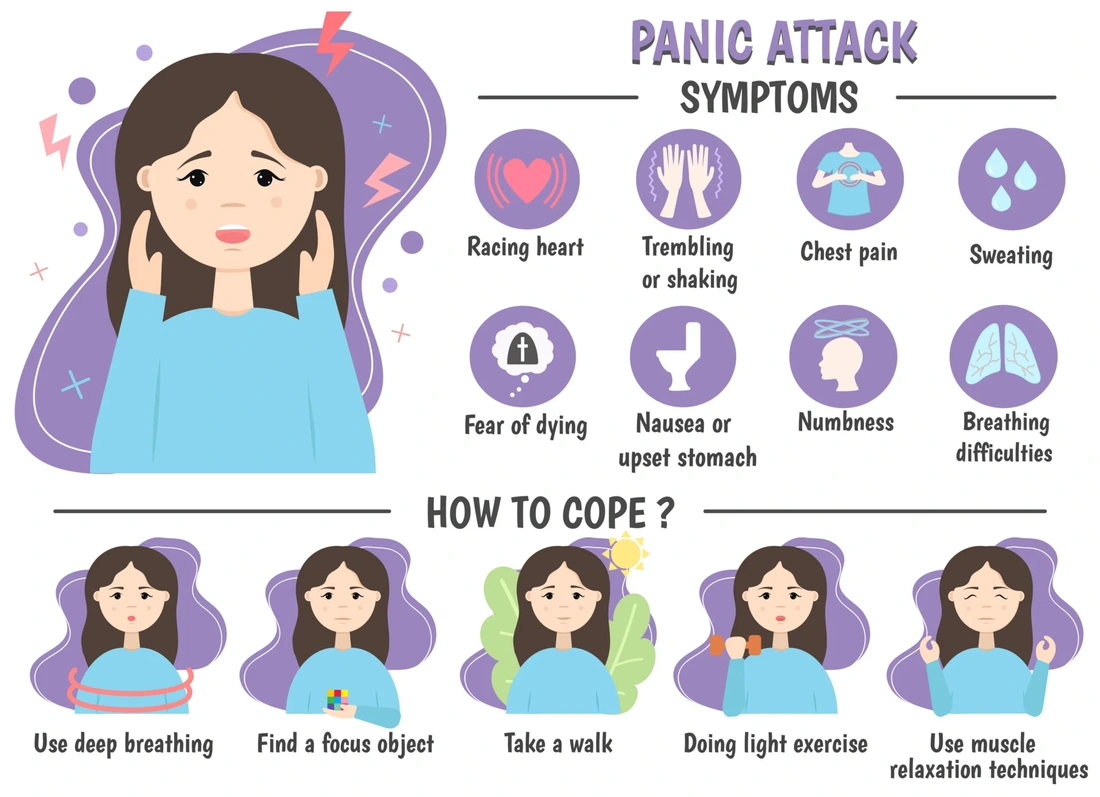
Clinical presentation reflects widespread autonomic activation. Cardiac symptoms include palpitations, tachycardia, and chest discomfort. Respiratory complaints such as shortness of breath, choking sensations, or smothering feelings are common. Neurologic and systemic symptoms include tremor, dizziness, lightheadedness, paresthesias, sweating, chills, flushing, and feelings of unreality or depersonalization. Gastrointestinal symptoms such as nausea, cramping, and abdominal pain may occur. Intense, stereotyped fears often center on imminent death, having a heart attack, losing control, or “going crazy.” A thorough history should explore medical conditions, medications (including over-the-counter and herbal products), substance and caffeine use, age at onset, triggering stressors, avoidance behaviors, prior treatment response, and family history of anxiety or substance use.
Physical examination should be complete and focused on cardiopulmonary and neurologic systems, guided by presenting symptoms. The essential workup is individualized and often minimal, aimed at excluding organic causes suggested by the history or exam. Laboratory evaluation may include basic metabolic studies, glucose, thyroid-stimulating hormone, and toxicology screening. Electrocardiography is appropriate for patients over 40 years of age, those with cardiac symptoms, or those taking tricyclic antidepressants. Additional testing such as Holter monitoring, arterial blood gases, or EEG is reserved for specific indications.
The differential diagnosis is broad and must be carefully considered, particularly in first presentations, late-onset cases, or atypical features. Cardiopulmonary causes include myocardial ischemia, arrhythmias, pulmonary embolism, asthma, and pneumonia. Metabolic and endocrine disorders include hypoglycemia, hyperthyroidism, electrolyte abnormalities, and pheochromocytoma. Neurologic conditions such as seizures or transient ischemic attack, medication effects, substance intoxication or withdrawal, and other psychiatric disorders including PTSD, obsessive-compulsive disorder, and somatoform disorders must also be considered.
Initial management focuses on calm reassurance and patient education. Most panic attacks resolve spontaneously, and excessive medical intervention may reinforce fear. Explaining the physiologic basis of symptoms can reduce distress and interrupt the cycle of escalating anxiety. In the emergency department, short-acting, high-potency benzodiazepines may be used for severe or persistent symptoms. Lorazepam is often preferred due to its rapid onset and smoother offset. Clonazepam is effective but has a slower onset and is better suited for maintenance therapy rather than acute control. Alprazolam should generally be avoided due to rapid offset and risk of rebound anxiety. Long-term management of recurrent panic attacks or panic disorder relies on cognitive–behavioral therapy and selective serotonin reuptake inhibitors, which should be initiated in the outpatient setting when follow-up is assured.
Admission is rarely required unless needed to exclude a serious medical condition or for psychiatric indications such as suicidality. Most patients can be safely discharged once symptoms resolve, with reassurance and clear follow-up plans. Referral to primary care or mental health services is recommended for recurrent attacks, interepisode anxiety, or avoidance behaviors. Patients should be counseled to avoid triggers such as caffeine, stimulants, and alcohol. Key pearls include recognizing that panic attacks are self-limited, maintaining a calm clinical approach, using medications judiciously, and emphasizing nonpharmacologic strategies such as cognitive–behavioral therapy to achieve durable symptom control.
Panic attacks are characterized by sudden episodes of intense fear accompanied by prominent physical symptoms that peak rapidly, usually within 10 minutes, and resolve within approximately 20–30 minutes. Some patients, particularly those with medical illness, may experience a nonfearful variant dominated by somatic symptoms. Panic disorder is defined by recurrent, unexpected panic attacks followed by at least one month of persistent concern about additional attacks, worry about their implications, or maladaptive behavioral changes such as avoidance. Panic disorder may occur with or without agoraphobia, which reflects anxiety related to fear of being unable to escape or obtain help. The condition is often episodic or chronic and is frequently comorbid with depression, substance use disorders, functional disability, and increased suicidal risk.
The underlying mechanism involves dysregulation of the limbic system with excessive norepinephrine release and altered serotonergic and benzodiazepine receptor function, triggering a maladaptive “fight-or-flight” response. Genetic factors play an important role, with family history of panic or anxiety disorders commonly reported. Risk factors include major life stressors in the year preceding onset, childhood shyness or separation anxiety, female sex, and stimulant use such as cocaine. Panic attacks may initially arise in the context of physical illness or substance use and persist even after the precipitating condition has resolved.
Clinical presentation reflects widespread autonomic activation. Cardiac symptoms include palpitations, tachycardia, and chest discomfort. Respiratory complaints such as shortness of breath, choking sensations, or smothering feelings are common. Neurologic and systemic symptoms include tremor, dizziness, lightheadedness, paresthesias, sweating, chills, flushing, and feelings of unreality or depersonalization. Gastrointestinal symptoms such as nausea, cramping, and abdominal pain may occur. Intense, stereotyped fears often center on imminent death, having a heart attack, losing control, or “going crazy.” A thorough history should explore medical conditions, medications (including over-the-counter and herbal products), substance and caffeine use, age at onset, triggering stressors, avoidance behaviors, prior treatment response, and family history of anxiety or substance use.
Physical examination should be complete and focused on cardiopulmonary and neurologic systems, guided by presenting symptoms. The essential workup is individualized and often minimal, aimed at excluding organic causes suggested by the history or exam. Laboratory evaluation may include basic metabolic studies, glucose, thyroid-stimulating hormone, and toxicology screening. Electrocardiography is appropriate for patients over 40 years of age, those with cardiac symptoms, or those taking tricyclic antidepressants. Additional testing such as Holter monitoring, arterial blood gases, or EEG is reserved for specific indications.
The differential diagnosis is broad and must be carefully considered, particularly in first presentations, late-onset cases, or atypical features. Cardiopulmonary causes include myocardial ischemia, arrhythmias, pulmonary embolism, asthma, and pneumonia. Metabolic and endocrine disorders include hypoglycemia, hyperthyroidism, electrolyte abnormalities, and pheochromocytoma. Neurologic conditions such as seizures or transient ischemic attack, medication effects, substance intoxication or withdrawal, and other psychiatric disorders including PTSD, obsessive-compulsive disorder, and somatoform disorders must also be considered.
Initial management focuses on calm reassurance and patient education. Most panic attacks resolve spontaneously, and excessive medical intervention may reinforce fear. Explaining the physiologic basis of symptoms can reduce distress and interrupt the cycle of escalating anxiety. In the emergency department, short-acting, high-potency benzodiazepines may be used for severe or persistent symptoms. Lorazepam is often preferred due to its rapid onset and smoother offset. Clonazepam is effective but has a slower onset and is better suited for maintenance therapy rather than acute control. Alprazolam should generally be avoided due to rapid offset and risk of rebound anxiety. Long-term management of recurrent panic attacks or panic disorder relies on cognitive–behavioral therapy and selective serotonin reuptake inhibitors, which should be initiated in the outpatient setting when follow-up is assured.
Admission is rarely required unless needed to exclude a serious medical condition or for psychiatric indications such as suicidality. Most patients can be safely discharged once symptoms resolve, with reassurance and clear follow-up plans. Referral to primary care or mental health services is recommended for recurrent attacks, interepisode anxiety, or avoidance behaviors. Patients should be counseled to avoid triggers such as caffeine, stimulants, and alcohol. Key pearls include recognizing that panic attacks are self-limited, maintaining a calm clinical approach, using medications judiciously, and emphasizing nonpharmacologic strategies such as cognitive–behavioral therapy to achieve durable symptom control.
- Published on
Emergency and Acute Medicine – Pelvic Fracture
Pelvic fractures account for approximately 3% of all bony fractures but are associated with disproportionately high morbidity and mortality. The pelvis consists of the sacrum and two innominate bones, each formed by the ilium, ischium, and pubis. Stability of the pelvic ring depends on strong ligamentous, muscular, and soft tissue support. The anterior pelvis is stabilized by the symphysis pubis and pubic rami, while posterior stability is provided by the sacroiliac (SI) complex and pelvic floor. Because the pelvis protects major vascular structures as well as genitourinary, gastrointestinal, gynecologic, neurologic, and musculoskeletal systems, fractures often coexist with life-threatening injuries and require urgent recognition and management.
Most pelvic fractures result from high-energy trauma. Approximately 65% are caused by vehicular mechanisms, including pedestrians struck by automobiles, while falls and crush injuries account for another 20%. Athletic, penetrating, and nontraumatic causes are less common. Mortality ranges from 6–19% and increases significantly in open fractures or when hemorrhagic shock is present. Unstable fractures, particularly those involving the posterior pelvis, are prone to severe hemorrhage due to disruption of arterial branches and venous plexuses, often with associated retroperitoneal hematoma. In children, hemorrhage may be more severe, and nonaccidental trauma must be considered. In pregnancy, pelvic fractures pose additional risk to the gravid uterus, including uterine rupture.
Clinically, patients typically present with pelvic, hip, groin, or lower back pain, often accompanied by swelling, ecchymosis, and tenderness. Many have associated injuries involving the abdomen, genitourinary tract, neurologic system, or vascular structures. Signs of pelvic instability, deformity, limb shortening or rotation, and inability to bear weight are concerning. In severe cases, hemorrhagic shock may dominate the presentation, with tachycardia, hypotension, altered mental status, and cool, pale extremities. Bleeding from the urethra, rectum, or vagina, as well as open wounds over the pelvis, suggests an open pelvic fracture.
Initial evaluation follows standard trauma principles. A single anteroposterior (AP) pelvic radiograph is the most important early diagnostic test and should be obtained promptly when pelvic fracture is suspected. Additional views such as inlet, outlet, or Judet oblique projections may further define injury patterns, particularly involving the posterior pelvis or acetabulum. Computed tomography (CT) provides detailed assessment of fracture anatomy, retroperitoneal hematoma, and associated visceral injuries, and CT angiography can identify arterial bleeding in hemodynamically stable patients. Focused abdominal sonography for trauma (FAST) may help detect intraperitoneal bleeding but has limited ability to distinguish pelvic from abdominal sources. Laboratory studies include type and cross-match, hemoglobin and hematocrit, platelet count, and coagulation profile.
Pelvic fractures are commonly categorized using the Tile classification system, which helps guide management. Type A fractures are stable and include avulsion injuries, isolated pubic rami fractures, and transverse sacral fractures. Type B fractures are rotationally unstable but vertically stable, such as open-book and lateral compression injuries. Type C fractures are both rotationally and vertically unstable, including vertical shear (Malgaigne) fractures, and are associated with the highest risk of hemorrhage and mortality. Acetabular fractures represent a distinct subgroup requiring specialized orthopedic evaluation.
Management priorities focus on rapid resuscitation, hemorrhage control, and stabilization. Early application of a pelvic binder or improvised sheet wrap at the level of the greater trochanters is critical in suspected unstable fractures, as it reduces pelvic volume and limits bleeding. Fluid resuscitation with crystalloids and early blood transfusion is indicated for shock, avoiding lower extremity IV access when possible. External fixation, angiographic embolization, or surgical pelvic packing may be required for ongoing hemorrhage. Type A fractures are generally managed conservatively with analgesia and mobilization as tolerated, whereas Type B and C fractures require urgent orthopedic and trauma consultation, close monitoring, and often operative intervention.
Patients with hemodynamic instability, unstable pelvic fractures, acetabular fractures, pelvic hemorrhage, or associated injuries should be admitted, frequently to the intensive care unit. Hemodynamically stable patients with isolated, stable Type A fractures and no other injuries may be discharged with appropriate analgesia and close orthopedic follow-up. A key clinical principle is that pelvic fractures signal high-energy trauma; clinicians must maintain a high index of suspicion for associated abdominal, genitourinary, vascular, and neurologic injuries. Early stabilization of the pelvis and management decisions guided by hemodynamic status are essential to improving outcomes.
Pelvic fractures account for approximately 3% of all bony fractures but are associated with disproportionately high morbidity and mortality. The pelvis consists of the sacrum and two innominate bones, each formed by the ilium, ischium, and pubis. Stability of the pelvic ring depends on strong ligamentous, muscular, and soft tissue support. The anterior pelvis is stabilized by the symphysis pubis and pubic rami, while posterior stability is provided by the sacroiliac (SI) complex and pelvic floor. Because the pelvis protects major vascular structures as well as genitourinary, gastrointestinal, gynecologic, neurologic, and musculoskeletal systems, fractures often coexist with life-threatening injuries and require urgent recognition and management.
Most pelvic fractures result from high-energy trauma. Approximately 65% are caused by vehicular mechanisms, including pedestrians struck by automobiles, while falls and crush injuries account for another 20%. Athletic, penetrating, and nontraumatic causes are less common. Mortality ranges from 6–19% and increases significantly in open fractures or when hemorrhagic shock is present. Unstable fractures, particularly those involving the posterior pelvis, are prone to severe hemorrhage due to disruption of arterial branches and venous plexuses, often with associated retroperitoneal hematoma. In children, hemorrhage may be more severe, and nonaccidental trauma must be considered. In pregnancy, pelvic fractures pose additional risk to the gravid uterus, including uterine rupture.
Clinically, patients typically present with pelvic, hip, groin, or lower back pain, often accompanied by swelling, ecchymosis, and tenderness. Many have associated injuries involving the abdomen, genitourinary tract, neurologic system, or vascular structures. Signs of pelvic instability, deformity, limb shortening or rotation, and inability to bear weight are concerning. In severe cases, hemorrhagic shock may dominate the presentation, with tachycardia, hypotension, altered mental status, and cool, pale extremities. Bleeding from the urethra, rectum, or vagina, as well as open wounds over the pelvis, suggests an open pelvic fracture.
Initial evaluation follows standard trauma principles. A single anteroposterior (AP) pelvic radiograph is the most important early diagnostic test and should be obtained promptly when pelvic fracture is suspected. Additional views such as inlet, outlet, or Judet oblique projections may further define injury patterns, particularly involving the posterior pelvis or acetabulum. Computed tomography (CT) provides detailed assessment of fracture anatomy, retroperitoneal hematoma, and associated visceral injuries, and CT angiography can identify arterial bleeding in hemodynamically stable patients. Focused abdominal sonography for trauma (FAST) may help detect intraperitoneal bleeding but has limited ability to distinguish pelvic from abdominal sources. Laboratory studies include type and cross-match, hemoglobin and hematocrit, platelet count, and coagulation profile.
Pelvic fractures are commonly categorized using the Tile classification system, which helps guide management. Type A fractures are stable and include avulsion injuries, isolated pubic rami fractures, and transverse sacral fractures. Type B fractures are rotationally unstable but vertically stable, such as open-book and lateral compression injuries. Type C fractures are both rotationally and vertically unstable, including vertical shear (Malgaigne) fractures, and are associated with the highest risk of hemorrhage and mortality. Acetabular fractures represent a distinct subgroup requiring specialized orthopedic evaluation.
Management priorities focus on rapid resuscitation, hemorrhage control, and stabilization. Early application of a pelvic binder or improvised sheet wrap at the level of the greater trochanters is critical in suspected unstable fractures, as it reduces pelvic volume and limits bleeding. Fluid resuscitation with crystalloids and early blood transfusion is indicated for shock, avoiding lower extremity IV access when possible. External fixation, angiographic embolization, or surgical pelvic packing may be required for ongoing hemorrhage. Type A fractures are generally managed conservatively with analgesia and mobilization as tolerated, whereas Type B and C fractures require urgent orthopedic and trauma consultation, close monitoring, and often operative intervention.
Patients with hemodynamic instability, unstable pelvic fractures, acetabular fractures, pelvic hemorrhage, or associated injuries should be admitted, frequently to the intensive care unit. Hemodynamically stable patients with isolated, stable Type A fractures and no other injuries may be discharged with appropriate analgesia and close orthopedic follow-up. A key clinical principle is that pelvic fractures signal high-energy trauma; clinicians must maintain a high index of suspicion for associated abdominal, genitourinary, vascular, and neurologic injuries. Early stabilization of the pelvis and management decisions guided by hemodynamic status are essential to improving outcomes.
- Published on
Emergency and Acute Medicine – Pediculosis
Pediculosis is an infestation caused by lice that live in close association with humans. Bites are typically painless, and symptoms arise from the host’s inflammatory response to saliva and anticoagulants injected during feeding. Transmission occurs through direct contact and fomites such as combs, pillows, hats, and clothing. Head lice spread primarily through head-to-head contact and are more common in children and females. Pubic lice are usually transmitted through sexual contact. All lice are obligate human parasites and generally cannot survive away from a host for more than 7–10 days.
The condition is caused by three main species. *Pediculus capitis* (head lice) is the most common and affects all socioeconomic groups. *Pediculus corporis* (body lice) is associated with poor hygiene, poverty, and overcrowding, living primarily in clothing seams and transferring to the skin for feeding. *Phthirus pubis* (pubic or crab lice) typically infests coarse hair in the pubic region and is sexually transmitted. In children, pubic lice should raise concern for possible sexual abuse.
Clinical presentation varies by type. Head lice may cause scalp pruritus or be asymptomatic, often mistaken for dandruff. Body lice present with pruritus and excoriations, especially along clothing seams. Pubic lice cause intense itching, often worse at night. Physical examination focuses on identifying live lice or nits cemented to hair shafts, which cannot be easily brushed off. Empty nits alone do not confirm active infestation. Findings may include erythema, excoriations, secondary bacterial infection, posterior cervical lymphadenopathy, or bluish macules (maculae ceruleae) in pubic lice. Body lice are confirmed by finding nits in clothing seams rather than on the skin.
Diagnosis is clinical, based on careful history and physical examination with universal precautions. Laboratory testing is rarely necessary, although nits may be visualized under low-power microscopy and may fluoresce under a Wood lamp. Imaging has no role. Differential diagnoses include scabies, contact or allergic dermatitis, seborrheic dermatitis, and bed bug bites.
Management is primarily outpatient and supportive. Pruritus may be relieved with oral antihistamines or topical steroids. Head lice are treated with topical pediculicides such as permethrin 1% cream rinse or pyrethrin-based products, with nit removal using a fine-toothed comb. Reapplication in 7–10 days is usually required due to incomplete ovicidal activity. All household contacts should be examined, and infested individuals treated. Clothing, bedding, towels, and headgear should be washed and dried using hot cycles, and personal items such as combs and brushes disinfected.
Body lice management emphasizes hygiene, laundering clothing and bedding at high temperatures, and applying topical pediculicides when needed. Pubic lice are treated with topical pediculicides applied to affected hair-bearing areas, with simultaneous treatment of sexual contacts. Eyelash involvement is managed with petrolatum applied twice daily for several days. Second-line agents such as ivermectin or spinosad may be used for resistant cases.
Admission is rarely required and is reserved for patients with extensive bacterial superinfection or severe hypersensitivity reactions. Most patients can be discharged after treatment with appropriate education. Children may return to school after initial therapy, provided repeat treatment is completed. Follow-up is recommended to ensure eradication and to address social or safeguarding concerns when indicated.
Key points include confirming diagnosis by direct visualization, repeating treatment after 7–10 days, thorough environmental decontamination, and awareness of increasing resistance to first-line agents. Lindane is no longer recommended due to toxicity, and second-line treatments are effective but more costly.
Pediculosis is an infestation caused by lice that live in close association with humans. Bites are typically painless, and symptoms arise from the host’s inflammatory response to saliva and anticoagulants injected during feeding. Transmission occurs through direct contact and fomites such as combs, pillows, hats, and clothing. Head lice spread primarily through head-to-head contact and are more common in children and females. Pubic lice are usually transmitted through sexual contact. All lice are obligate human parasites and generally cannot survive away from a host for more than 7–10 days.
The condition is caused by three main species. *Pediculus capitis* (head lice) is the most common and affects all socioeconomic groups. *Pediculus corporis* (body lice) is associated with poor hygiene, poverty, and overcrowding, living primarily in clothing seams and transferring to the skin for feeding. *Phthirus pubis* (pubic or crab lice) typically infests coarse hair in the pubic region and is sexually transmitted. In children, pubic lice should raise concern for possible sexual abuse.
Clinical presentation varies by type. Head lice may cause scalp pruritus or be asymptomatic, often mistaken for dandruff. Body lice present with pruritus and excoriations, especially along clothing seams. Pubic lice cause intense itching, often worse at night. Physical examination focuses on identifying live lice or nits cemented to hair shafts, which cannot be easily brushed off. Empty nits alone do not confirm active infestation. Findings may include erythema, excoriations, secondary bacterial infection, posterior cervical lymphadenopathy, or bluish macules (maculae ceruleae) in pubic lice. Body lice are confirmed by finding nits in clothing seams rather than on the skin.
Diagnosis is clinical, based on careful history and physical examination with universal precautions. Laboratory testing is rarely necessary, although nits may be visualized under low-power microscopy and may fluoresce under a Wood lamp. Imaging has no role. Differential diagnoses include scabies, contact or allergic dermatitis, seborrheic dermatitis, and bed bug bites.
Management is primarily outpatient and supportive. Pruritus may be relieved with oral antihistamines or topical steroids. Head lice are treated with topical pediculicides such as permethrin 1% cream rinse or pyrethrin-based products, with nit removal using a fine-toothed comb. Reapplication in 7–10 days is usually required due to incomplete ovicidal activity. All household contacts should be examined, and infested individuals treated. Clothing, bedding, towels, and headgear should be washed and dried using hot cycles, and personal items such as combs and brushes disinfected.
Body lice management emphasizes hygiene, laundering clothing and bedding at high temperatures, and applying topical pediculicides when needed. Pubic lice are treated with topical pediculicides applied to affected hair-bearing areas, with simultaneous treatment of sexual contacts. Eyelash involvement is managed with petrolatum applied twice daily for several days. Second-line agents such as ivermectin or spinosad may be used for resistant cases.
Admission is rarely required and is reserved for patients with extensive bacterial superinfection or severe hypersensitivity reactions. Most patients can be discharged after treatment with appropriate education. Children may return to school after initial therapy, provided repeat treatment is completed. Follow-up is recommended to ensure eradication and to address social or safeguarding concerns when indicated.
Key points include confirming diagnosis by direct visualization, repeating treatment after 7–10 days, thorough environmental decontamination, and awareness of increasing resistance to first-line agents. Lindane is no longer recommended due to toxicity, and second-line treatments are effective but more costly.

- Published on
Emergency and Acute Medicine – Pelvic Inflammatory Disease
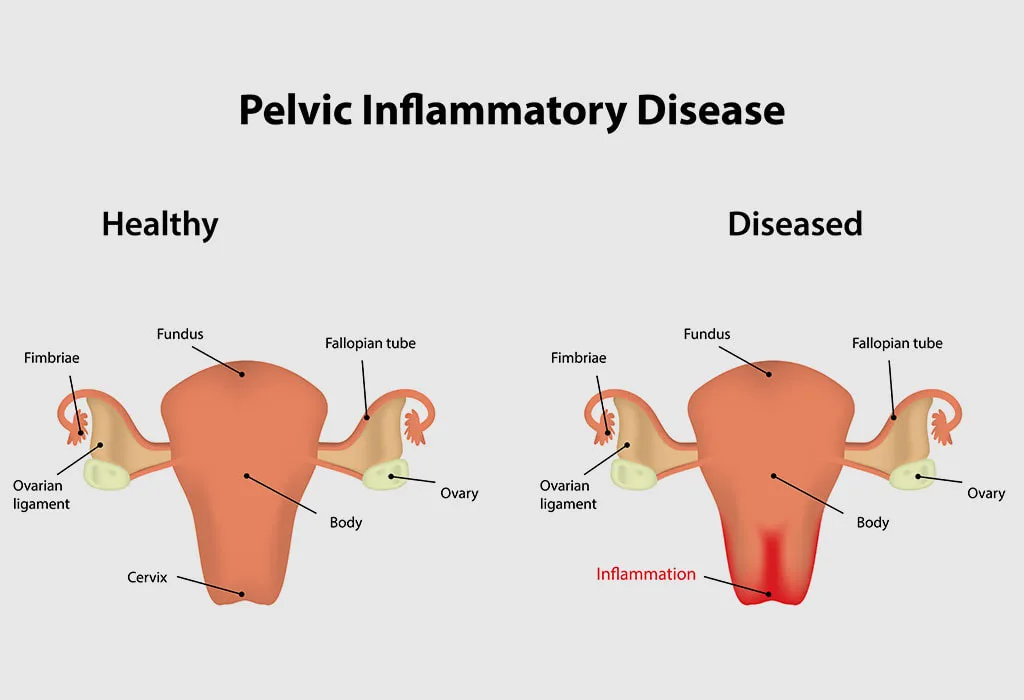
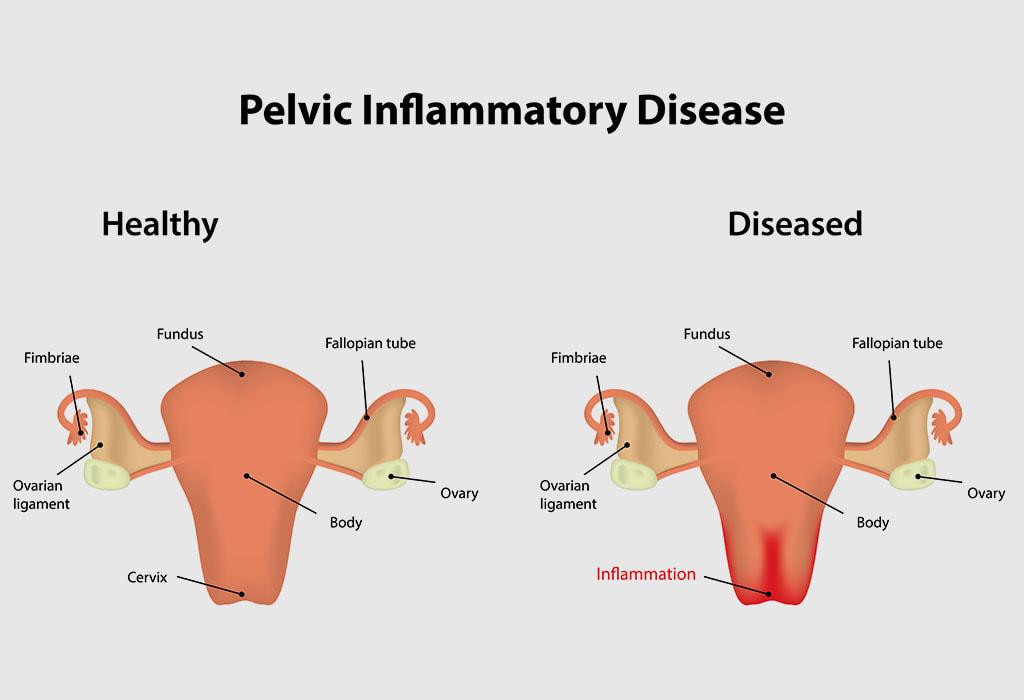
Pelvic inflammatory disease (PID) is an acute, community-acquired, sexually transmitted infection involving the upper female genital tract, including the uterus, fallopian tubes, ovaries, and adjacent pelvic structures. It is one of the most common gynecologic reasons for emergency department visits, accounting for hundreds of thousands of cases annually. PID represents a spectrum of disease rather than a single entity, and there is no definitive diagnostic gold standard. Because delayed treatment increases the risk of infertility, chronic pelvic pain, and ectopic pregnancy, clinicians must maintain a low threshold for diagnosis and initiate empiric antibiotic therapy when PID is suspected. Progressive or untreated infection may result in complications such as tubo-ovarian abscess (TOA). An important associated condition is Fitz-Hugh–Curtis syndrome, a perihepatic capsular inflammation that presents with sharp right upper quadrant pain worsened by movement, coughing, or inspiration.
The most important risk factors for PID include age younger than 25 years, multiple or symptomatic sexual partners, a prior history of PID, nonbarrier contraception, and certain demographic factors such as African American ethnicity. The most common causative organisms are *Chlamydia trachomatis* and *Neisseria gonorrhoeae*, although PID is frequently polymicrobial. Other implicated pathogens include group A and B streptococci, staphylococci, gram-negative rods such as *Escherichia coli*, *Klebsiella* spp., *Proteus* spp., and various anaerobes. Because of this broad microbiologic spectrum, treatment regimens must provide wide antimicrobial coverage.
Clinically, PID most often presents with bilateral lower abdominal or pelvic pain, which may range from mild and subtle to severe. Pain that worsens during intercourse or occurs shortly after or during menses is particularly suggestive. Associated symptoms commonly include abnormal vaginal discharge, abnormal uterine bleeding, dysmenorrhea, dyspareunia, dysuria, nausea, vomiting, fever, and chills. On examination, only about half of patients are febrile. Abdominal examination typically reveals lower quadrant tenderness, often bilateral, with possible rebound tenderness and decreased bowel sounds. Pelvic examination may demonstrate purulent endocervical discharge, cervical motion tenderness, and uterine or adnexal tenderness. Right upper quadrant tenderness in the context of PID suggests Fitz-Hugh–Curtis syndrome. Importantly, the absence of prominent uterine or adnexal tenderness should prompt consideration of alternative diagnoses.
The diagnosis of PID is primarily clinical and based on history and physical examination, including a pelvic exam. A pregnancy test is mandatory in all patients to exclude ectopic pregnancy or complications of intrauterine pregnancy. Minimum diagnostic criteria include the presence of lower abdominal tenderness, uterine or adnexal tenderness, or cervical motion tenderness. Supportive findings include fever above 38.3°C, abnormal cervical or vaginal discharge, leukocytosis, elevated inflammatory markers such as ESR or C-reactive protein, and microbiologic evidence of gonococcal or chlamydial infection. Laboratory studies may include a complete blood count, nucleic acid amplification testing for *N. gonorrhoeae* and *C. trachomatis*, and microscopic evaluation of vaginal discharge. Imaging is not routinely required but transvaginal ultrasound is indicated when adnexal fullness or mass is present, when TOA is suspected, when pelvic examination is limited, or when outpatient therapy fails.
Management depends on disease severity and patient reliability for follow-up. Most patients with mild to moderate PID can be treated as outpatients with intramuscular ceftriaxone or cefoxitin (with probenecid) plus oral doxycycline, with the addition of metronidazole when anaerobic coverage is indicated. Inpatient therapy is reserved for patients with severe illness, pregnancy, suspected TOA, immunodeficiency, inability to tolerate oral medications, failure of outpatient therapy, or concern for noncompliance. Recommended inpatient regimens include doxycycline combined with cefoxitin or cefotetan, or alternatives such as gentamicin plus clindamycin or ampicillin/sulbactam plus doxycycline. Parenteral therapy should continue for at least 24 hours after clinical improvement, followed by oral antibiotics to complete a 14-day course. Sexual partners should be evaluated and treated, and patients should receive counseling and testing for other sexually transmitted infections, including HIV.
Patients who do not meet admission criteria may be safely discharged with close follow-up arranged within 48–72 hours to ensure clinical improvement. Failure to improve within this timeframe warrants reassessment and possible inpatient management. Key clinical principles include recognizing that PID exists along a disease continuum, that early empiric treatment is essential to prevent long-term sequelae, and that quinolones and oral cephalosporins are no longer recommended in the United States for gonorrhea-related infections due to resistance. Comprehensive patient education, partner treatment, and reliable follow-up are critical components of effective PID management.
Pelvic inflammatory disease (PID) is an acute, community-acquired, sexually transmitted infection involving the upper female genital tract, including the uterus, fallopian tubes, ovaries, and adjacent pelvic structures. It is one of the most common gynecologic reasons for emergency department visits, accounting for hundreds of thousands of cases annually. PID represents a spectrum of disease rather than a single entity, and there is no definitive diagnostic gold standard. Because delayed treatment increases the risk of infertility, chronic pelvic pain, and ectopic pregnancy, clinicians must maintain a low threshold for diagnosis and initiate empiric antibiotic therapy when PID is suspected. Progressive or untreated infection may result in complications such as tubo-ovarian abscess (TOA). An important associated condition is Fitz-Hugh–Curtis syndrome, a perihepatic capsular inflammation that presents with sharp right upper quadrant pain worsened by movement, coughing, or inspiration.
The most important risk factors for PID include age younger than 25 years, multiple or symptomatic sexual partners, a prior history of PID, nonbarrier contraception, and certain demographic factors such as African American ethnicity. The most common causative organisms are *Chlamydia trachomatis* and *Neisseria gonorrhoeae*, although PID is frequently polymicrobial. Other implicated pathogens include group A and B streptococci, staphylococci, gram-negative rods such as *Escherichia coli*, *Klebsiella* spp., *Proteus* spp., and various anaerobes. Because of this broad microbiologic spectrum, treatment regimens must provide wide antimicrobial coverage.
Clinically, PID most often presents with bilateral lower abdominal or pelvic pain, which may range from mild and subtle to severe. Pain that worsens during intercourse or occurs shortly after or during menses is particularly suggestive. Associated symptoms commonly include abnormal vaginal discharge, abnormal uterine bleeding, dysmenorrhea, dyspareunia, dysuria, nausea, vomiting, fever, and chills. On examination, only about half of patients are febrile. Abdominal examination typically reveals lower quadrant tenderness, often bilateral, with possible rebound tenderness and decreased bowel sounds. Pelvic examination may demonstrate purulent endocervical discharge, cervical motion tenderness, and uterine or adnexal tenderness. Right upper quadrant tenderness in the context of PID suggests Fitz-Hugh–Curtis syndrome. Importantly, the absence of prominent uterine or adnexal tenderness should prompt consideration of alternative diagnoses.
The diagnosis of PID is primarily clinical and based on history and physical examination, including a pelvic exam. A pregnancy test is mandatory in all patients to exclude ectopic pregnancy or complications of intrauterine pregnancy. Minimum diagnostic criteria include the presence of lower abdominal tenderness, uterine or adnexal tenderness, or cervical motion tenderness. Supportive findings include fever above 38.3°C, abnormal cervical or vaginal discharge, leukocytosis, elevated inflammatory markers such as ESR or C-reactive protein, and microbiologic evidence of gonococcal or chlamydial infection. Laboratory studies may include a complete blood count, nucleic acid amplification testing for *N. gonorrhoeae* and *C. trachomatis*, and microscopic evaluation of vaginal discharge. Imaging is not routinely required but transvaginal ultrasound is indicated when adnexal fullness or mass is present, when TOA is suspected, when pelvic examination is limited, or when outpatient therapy fails.
Management depends on disease severity and patient reliability for follow-up. Most patients with mild to moderate PID can be treated as outpatients with intramuscular ceftriaxone or cefoxitin (with probenecid) plus oral doxycycline, with the addition of metronidazole when anaerobic coverage is indicated. Inpatient therapy is reserved for patients with severe illness, pregnancy, suspected TOA, immunodeficiency, inability to tolerate oral medications, failure of outpatient therapy, or concern for noncompliance. Recommended inpatient regimens include doxycycline combined with cefoxitin or cefotetan, or alternatives such as gentamicin plus clindamycin or ampicillin/sulbactam plus doxycycline. Parenteral therapy should continue for at least 24 hours after clinical improvement, followed by oral antibiotics to complete a 14-day course. Sexual partners should be evaluated and treated, and patients should receive counseling and testing for other sexually transmitted infections, including HIV.
Patients who do not meet admission criteria may be safely discharged with close follow-up arranged within 48–72 hours to ensure clinical improvement. Failure to improve within this timeframe warrants reassessment and possible inpatient management. Key clinical principles include recognizing that PID exists along a disease continuum, that early empiric treatment is essential to prevent long-term sequelae, and that quinolones and oral cephalosporins are no longer recommended in the United States for gonorrhea-related infections due to resistance. Comprehensive patient education, partner treatment, and reliable follow-up are critical components of effective PID management.
- Published on
Emergency and Acute Medicine – Pediatric Trauma
Pediatric trauma accounts for a significant cause of morbidity and mortality, with blunt trauma representing approximately 80% of cases and head injury present in most multisystem trauma. Trauma remains the leading cause of death and disability in children older than one year in developed countries. Young children are particularly vulnerable, with a high proportion of abuse-related injuries occurring in those younger than three years, especially infants under six months of age.
Most pediatric trauma results from single-system, minor blunt injuries. Common mechanisms include motor vehicle collisions, bicycle accidents, pedestrian versus vehicle incidents, and falls from height. Penetrating trauma is uncommon in younger children. Risk factors include inadequate supervision, developmental immaturity, poor judgment, risk-taking behaviors, and exposure to drugs or alcohol. Inconsistent history or injury patterns should raise concern for nonaccidental trauma.
History is typically obtained from caregivers, witnesses, or emergency personnel. Discrepancies between the history and observed injuries should prompt evaluation for abuse. Mechanism of injury alone is a poor predictor of severity, although certain factors such as handlebar injuries, intrusion into passenger space, lack of restraints, or absence of helmet use increase the likelihood of serious injury. A complete AMPLE history, including allergies, medications, past medical history, last oral intake, and events surrounding the injury, is essential.
Evaluation follows a structured primary survey using the ABCDE approach, addressing airway, breathing, circulation, disability, and exposure. Children may maintain compensation until significant blood loss occurs, after which rapid decompensation may follow. Unique anatomic features include a proportionally larger head, smaller blood volume, flexible chest wall, larger solid abdominal organs, and an intra-abdominal bladder in young children. Secondary survey focuses on detailed head-to-toe examination, including neurologic status, cervical spine assessment, chest and abdominal findings, extremity injuries, and skin evaluation. Certain injury patterns, such as lap belt syndrome or handlebar injuries, suggest specific internal injuries.
History and a thorough, age-appropriate physical examination are the cornerstone of evaluation. Routine trauma panels and blanket imaging are not evidence based in children and should be avoided. Laboratory testing and imaging should be individualized. Normal initial hemoglobin does not exclude hemorrhage. Elevated liver enzymes may guide abdominal imaging but should not be the sole determinant. Gross hematuria is concerning for genitourinary injury, while microscopic hematuria alone is not. Imaging decisions should be selective, with CT reserved for specific indications such as abnormal mental status, focal neurologic deficits, significant abdominal findings, or concerning mechanisms.
Prehospital priorities include rapid transport, airway stabilization, cervical spine immobilization, and hemorrhage control. In the emergency department, most children remain stable but require close monitoring. Management includes early oxygen, intravenous access with isotonic fluid resuscitation, pain control, blood transfusion if indicated, airway management when necessary, and treatment of identified injuries. Reassessment is critical, and family presence during resuscitation is encouraged when appropriate.
Admission is required for children with altered mental status, airway compromise, hemodynamic instability, significant imaging findings, operative injuries, suspected abuse, or lack of a reliable caregiver. Children with normal mental status, reassuring examinations, and negative indicated imaging may be safely discharged to reliable caregivers with appropriate instructions. Follow-up should be tailored to injuries sustained, with attention to potential post-traumatic stress, neurologic sequelae, and psychosocial needs.
Pediatric trauma accounts for a significant cause of morbidity and mortality, with blunt trauma representing approximately 80% of cases and head injury present in most multisystem trauma. Trauma remains the leading cause of death and disability in children older than one year in developed countries. Young children are particularly vulnerable, with a high proportion of abuse-related injuries occurring in those younger than three years, especially infants under six months of age.
Most pediatric trauma results from single-system, minor blunt injuries. Common mechanisms include motor vehicle collisions, bicycle accidents, pedestrian versus vehicle incidents, and falls from height. Penetrating trauma is uncommon in younger children. Risk factors include inadequate supervision, developmental immaturity, poor judgment, risk-taking behaviors, and exposure to drugs or alcohol. Inconsistent history or injury patterns should raise concern for nonaccidental trauma.
History is typically obtained from caregivers, witnesses, or emergency personnel. Discrepancies between the history and observed injuries should prompt evaluation for abuse. Mechanism of injury alone is a poor predictor of severity, although certain factors such as handlebar injuries, intrusion into passenger space, lack of restraints, or absence of helmet use increase the likelihood of serious injury. A complete AMPLE history, including allergies, medications, past medical history, last oral intake, and events surrounding the injury, is essential.
Evaluation follows a structured primary survey using the ABCDE approach, addressing airway, breathing, circulation, disability, and exposure. Children may maintain compensation until significant blood loss occurs, after which rapid decompensation may follow. Unique anatomic features include a proportionally larger head, smaller blood volume, flexible chest wall, larger solid abdominal organs, and an intra-abdominal bladder in young children. Secondary survey focuses on detailed head-to-toe examination, including neurologic status, cervical spine assessment, chest and abdominal findings, extremity injuries, and skin evaluation. Certain injury patterns, such as lap belt syndrome or handlebar injuries, suggest specific internal injuries.
History and a thorough, age-appropriate physical examination are the cornerstone of evaluation. Routine trauma panels and blanket imaging are not evidence based in children and should be avoided. Laboratory testing and imaging should be individualized. Normal initial hemoglobin does not exclude hemorrhage. Elevated liver enzymes may guide abdominal imaging but should not be the sole determinant. Gross hematuria is concerning for genitourinary injury, while microscopic hematuria alone is not. Imaging decisions should be selective, with CT reserved for specific indications such as abnormal mental status, focal neurologic deficits, significant abdominal findings, or concerning mechanisms.
Prehospital priorities include rapid transport, airway stabilization, cervical spine immobilization, and hemorrhage control. In the emergency department, most children remain stable but require close monitoring. Management includes early oxygen, intravenous access with isotonic fluid resuscitation, pain control, blood transfusion if indicated, airway management when necessary, and treatment of identified injuries. Reassessment is critical, and family presence during resuscitation is encouraged when appropriate.
Admission is required for children with altered mental status, airway compromise, hemodynamic instability, significant imaging findings, operative injuries, suspected abuse, or lack of a reliable caregiver. Children with normal mental status, reassuring examinations, and negative indicated imaging may be safely discharged to reliable caregivers with appropriate instructions. Follow-up should be tailored to injuries sustained, with attention to potential post-traumatic stress, neurologic sequelae, and psychosocial needs.
- Published on
Emergency and Acute Medicine – Pelvic Fracture
Pelvic fractures account for approximately 3% of all bony fractures but are associated with disproportionately high morbidity and mortality. The pelvis consists of the sacrum and two innominate bones, each formed by the ilium, ischium, and pubis. Stability of the pelvic ring depends on strong ligamentous, muscular, and soft tissue support. The anterior pelvis is stabilized by the symphysis pubis and pubic rami, while posterior stability is provided by the sacroiliac (SI) complex and pelvic floor. Because the pelvis protects major vascular structures as well as genitourinary, gastrointestinal, gynecologic, neurologic, and musculoskeletal systems, fractures often coexist with life-threatening injuries and require urgent recognition and management.
Most pelvic fractures result from high-energy trauma. Approximately 65% are caused by vehicular mechanisms, including pedestrians struck by automobiles, while falls and crush injuries account for another 20%. Athletic, penetrating, and nontraumatic causes are less common. Mortality ranges from 6–19% and increases significantly in open fractures or when hemorrhagic shock is present. Unstable fractures, particularly those involving the posterior pelvis, are prone to severe hemorrhage due to disruption of arterial branches and venous plexuses, often with associated retroperitoneal hematoma. In children, hemorrhage may be more severe, and nonaccidental trauma must be considered. In pregnancy, pelvic fractures pose additional risk to the gravid uterus, including uterine rupture.
Clinically, patients typically present with pelvic, hip, groin, or lower back pain, often accompanied by swelling, ecchymosis, and tenderness. Many have associated injuries involving the abdomen, genitourinary tract, neurologic system, or vascular structures. Signs of pelvic instability, deformity, limb shortening or rotation, and inability to bear weight are concerning. In severe cases, hemorrhagic shock may dominate the presentation, with tachycardia, hypotension, altered mental status, and cool, pale extremities. Bleeding from the urethra, rectum, or vagina, as well as open wounds over the pelvis, suggests an open pelvic fracture.
Initial evaluation follows standard trauma principles. A single anteroposterior (AP) pelvic radiograph is the most important early diagnostic test and should be obtained promptly when pelvic fracture is suspected. Additional views such as inlet, outlet, or Judet oblique projections may further define injury patterns, particularly involving the posterior pelvis or acetabulum. Computed tomography (CT) provides detailed assessment of fracture anatomy, retroperitoneal hematoma, and associated visceral injuries, and CT angiography can identify arterial bleeding in hemodynamically stable patients. Focused abdominal sonography for trauma (FAST) may help detect intraperitoneal bleeding but has limited ability to distinguish pelvic from abdominal sources. Laboratory studies include type and cross-match, hemoglobin and hematocrit, platelet count, and coagulation profile.
Pelvic fractures are commonly categorized using the Tile classification system, which helps guide management. Type A fractures are stable and include avulsion injuries, isolated pubic rami fractures, and transverse sacral fractures. Type B fractures are rotationally unstable but vertically stable, such as open-book and lateral compression injuries. Type C fractures are both rotationally and vertically unstable, including vertical shear (Malgaigne) fractures, and are associated with the highest risk of hemorrhage and mortality. Acetabular fractures represent a distinct subgroup requiring specialized orthopedic evaluation.
Management priorities focus on rapid resuscitation, hemorrhage control, and stabilization. Early application of a pelvic binder or improvised sheet wrap at the level of the greater trochanters is critical in suspected unstable fractures, as it reduces pelvic volume and limits bleeding. Fluid resuscitation with crystalloids and early blood transfusion is indicated for shock, avoiding lower extremity IV access when possible. External fixation, angiographic embolization, or surgical pelvic packing may be required for ongoing hemorrhage. Type A fractures are generally managed conservatively with analgesia and mobilization as tolerated, whereas Type B and C fractures require urgent orthopedic and trauma consultation, close monitoring, and often operative intervention.
Patients with hemodynamic instability, unstable pelvic fractures, acetabular fractures, pelvic hemorrhage, or associated injuries should be admitted, frequently to the intensive care unit. Hemodynamically stable patients with isolated, stable Type A fractures and no other injuries may be discharged with appropriate analgesia and close orthopedic follow-up. A key clinical principle is that pelvic fractures signal high-energy trauma; clinicians must maintain a high index of suspicion for associated abdominal, genitourinary, vascular, and neurologic injuries. Early stabilization of the pelvis and management decisions guided by hemodynamic status are essential to improving outcomes.
Pelvic fractures account for approximately 3% of all bony fractures but are associated with disproportionately high morbidity and mortality. The pelvis consists of the sacrum and two innominate bones, each formed by the ilium, ischium, and pubis. Stability of the pelvic ring depends on strong ligamentous, muscular, and soft tissue support. The anterior pelvis is stabilized by the symphysis pubis and pubic rami, while posterior stability is provided by the sacroiliac (SI) complex and pelvic floor. Because the pelvis protects major vascular structures as well as genitourinary, gastrointestinal, gynecologic, neurologic, and musculoskeletal systems, fractures often coexist with life-threatening injuries and require urgent recognition and management.
Most pelvic fractures result from high-energy trauma. Approximately 65% are caused by vehicular mechanisms, including pedestrians struck by automobiles, while falls and crush injuries account for another 20%. Athletic, penetrating, and nontraumatic causes are less common. Mortality ranges from 6–19% and increases significantly in open fractures or when hemorrhagic shock is present. Unstable fractures, particularly those involving the posterior pelvis, are prone to severe hemorrhage due to disruption of arterial branches and venous plexuses, often with associated retroperitoneal hematoma. In children, hemorrhage may be more severe, and nonaccidental trauma must be considered. In pregnancy, pelvic fractures pose additional risk to the gravid uterus, including uterine rupture.
Clinically, patients typically present with pelvic, hip, groin, or lower back pain, often accompanied by swelling, ecchymosis, and tenderness. Many have associated injuries involving the abdomen, genitourinary tract, neurologic system, or vascular structures. Signs of pelvic instability, deformity, limb shortening or rotation, and inability to bear weight are concerning. In severe cases, hemorrhagic shock may dominate the presentation, with tachycardia, hypotension, altered mental status, and cool, pale extremities. Bleeding from the urethra, rectum, or vagina, as well as open wounds over the pelvis, suggests an open pelvic fracture.
Initial evaluation follows standard trauma principles. A single anteroposterior (AP) pelvic radiograph is the most important early diagnostic test and should be obtained promptly when pelvic fracture is suspected. Additional views such as inlet, outlet, or Judet oblique projections may further define injury patterns, particularly involving the posterior pelvis or acetabulum. Computed tomography (CT) provides detailed assessment of fracture anatomy, retroperitoneal hematoma, and associated visceral injuries, and CT angiography can identify arterial bleeding in hemodynamically stable patients. Focused abdominal sonography for trauma (FAST) may help detect intraperitoneal bleeding but has limited ability to distinguish pelvic from abdominal sources. Laboratory studies include type and cross-match, hemoglobin and hematocrit, platelet count, and coagulation profile.
Pelvic fractures are commonly categorized using the Tile classification system, which helps guide management. Type A fractures are stable and include avulsion injuries, isolated pubic rami fractures, and transverse sacral fractures. Type B fractures are rotationally unstable but vertically stable, such as open-book and lateral compression injuries. Type C fractures are both rotationally and vertically unstable, including vertical shear (Malgaigne) fractures, and are associated with the highest risk of hemorrhage and mortality. Acetabular fractures represent a distinct subgroup requiring specialized orthopedic evaluation.
Management priorities focus on rapid resuscitation, hemorrhage control, and stabilization. Early application of a pelvic binder or improvised sheet wrap at the level of the greater trochanters is critical in suspected unstable fractures, as it reduces pelvic volume and limits bleeding. Fluid resuscitation with crystalloids and early blood transfusion is indicated for shock, avoiding lower extremity IV access when possible. External fixation, angiographic embolization, or surgical pelvic packing may be required for ongoing hemorrhage. Type A fractures are generally managed conservatively with analgesia and mobilization as tolerated, whereas Type B and C fractures require urgent orthopedic and trauma consultation, close monitoring, and often operative intervention.
Patients with hemodynamic instability, unstable pelvic fractures, acetabular fractures, pelvic hemorrhage, or associated injuries should be admitted, frequently to the intensive care unit. Hemodynamically stable patients with isolated, stable Type A fractures and no other injuries may be discharged with appropriate analgesia and close orthopedic follow-up. A key clinical principle is that pelvic fractures signal high-energy trauma; clinicians must maintain a high index of suspicion for associated abdominal, genitourinary, vascular, and neurologic injuries. Early stabilization of the pelvis and management decisions guided by hemodynamic status are essential to improving outcomes.
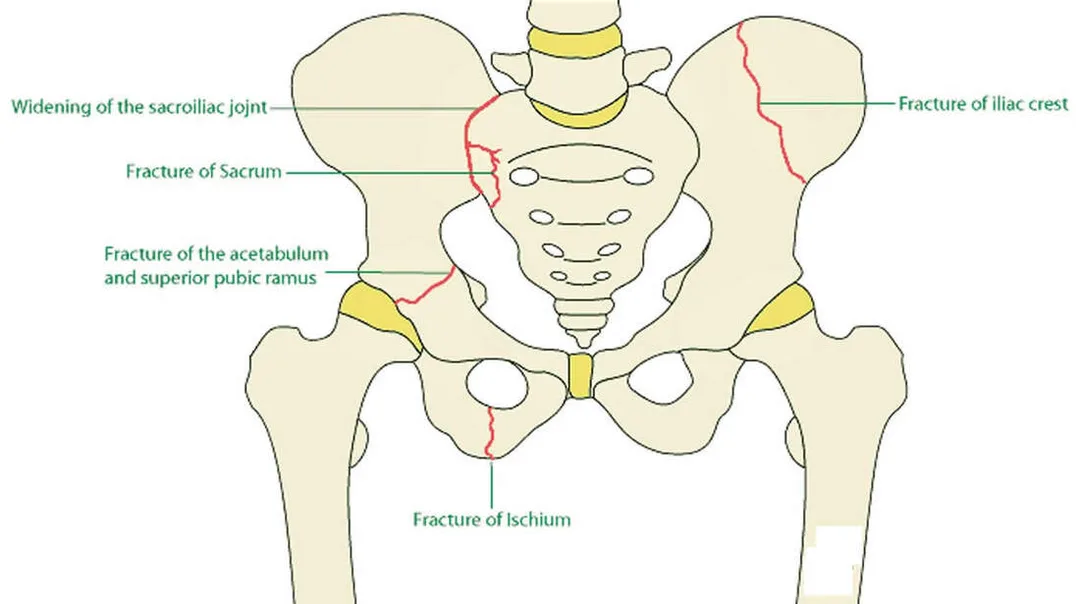
- Published on
KembaraXtra-Medicine – Mitral Valve Prolapse
Mitral valve prolapse (MVP) is characterized by bulging of one or both mitral valve leaflets into the left atrium during systole due to incomplete coaptation of the valve leaflets. It is most commonly caused by myxomatous degeneration of the valve, involving proliferation of the spongiosa layer with disruption of the fibrosa layer, along with excessive stretching of the chordae tendineae that places traction on the papillary muscles. Mitral regurgitation (MR) may develop in some patients. MVP typically presents between 10 and 16 years of age and is more common in females than males. It is generally benign in young women, whereas men over 50 years of age are more likely to develop severe regurgitation and require surgical intervention. MVP has a strong hereditary component and may be inherited in an autosomal dominant pattern with variable penetrance. A range of neuroendocrine and autonomic disturbances may also be associated with the condition.
MVP is associated with several connective tissue and systemic disorders, including Marfan syndrome, Ehlers–Danlos syndrome, osteogenesis imperfecta, pseudoxanthoma elasticum, Stickler syndrome, systemic lupus erythematosus, polyarteritis nodosa, polycystic kidney disease, von Willebrand disease, and Duchenne muscular dystrophy. These conditions contribute to abnormal connective tissue structure, predisposing the mitral valve to prolapse.
Clinical manifestations can be grouped into symptoms related to autonomic dysfunction, symptoms resulting from progression of mitral regurgitation, and complications such as stroke, infective endocarditis, or arrhythmias. Palpitations occur in up to 40% of patients and are commonly due to premature ventricular beats or paroxysmal supraventricular tachycardia. Chest pain occurs in about 10% of patients and is typically sharp, localized, nonexertional, and of variable duration. Dysautonomia-related symptoms include anxiety, panic attacks, fatigue, depression, migraine headaches, irritable bowel symptoms, and orthostatic intolerance. Syncope or presyncope is uncommon, occurring in less than 1% of cases, while dyspnea and fatigue are generally infrequent unless significant MR is present.
Physical examination classically reveals a mid-to-late systolic click best heard at the cardiac apex, often followed by a late systolic murmur. Maneuvers that reduce left ventricular volume, such as standing or Valsalva, cause the click to occur earlier in systole, while squatting delays it. Many patients exhibit skeletal abnormalities, including an asthenic body habitus, increased arm span relative to height, scoliosis or kyphosis, pectus excavatum, arachnodactyly, joint hypermobility, hypomastia, and a high-arched (“cathedral”) palate.
Diagnosis is often made clinically based on history and auscultation, with echocardiography used to confirm uncertain cases. On echocardiography, classic MVP is defined by superior displacement of the mitral leaflets greater than 2 mm into the left atrium during systole with leaflet thickness of at least 5 mm, while nonclassic MVP shows similar displacement with thinner leaflets. Electrocardiography is usually normal but may show ST-T wave changes, premature atrial or ventricular contractions, or QT prolongation. Chest radiography is typically normal unless significant MR leads to left atrial or ventricular enlargement.
Management is generally conservative, as many patients are asymptomatic and do not require treatment. β-blockers may be used for troublesome palpitations or chest pain, while magnesium supplementation may alleviate symptoms related to classic MVP syndrome. Orthostatic symptoms may respond to increased salt intake or fludrocortisone. Antiplatelet therapy is indicated in patients with transient ischemic attack or stroke. Significant MR, particularly in the presence of hypertension, may benefit from ACE inhibitors. Antibiotic prophylaxis is recommended only for selected patients with MVP and MR undergoing high-risk procedures, and is not indicated for isolated clicks without MR.
Hospital admission is reserved for patients with severe mitral regurgitation, ischemic chest pain, syncope, life-threatening arrhythmias, or cerebrovascular events. Asymptomatic patients without significant MR or dysrhythmias can be safely discharged. Cardiology referral is warranted for ventricular arrhythmias, evidence of disease progression, or risk of sudden death, while cardiothoracic surgical evaluation is indicated for symptomatic severe MR, reduced ejection fraction, pulmonary hypertension, or atrial fibrillation. Valve repair is preferred over replacement when feasible.
Regular follow-up every 3–5 years is recommended to monitor for progression of disease. Patients with MVP and MR should receive appropriate endocarditis prophylaxis during at-risk procedures and undergo evaluation before participating in high-intensity sports. A key clinical pitfall is attributing symptoms such as chest pain or syncope solely to MVP without appropriate evaluation, as MVP remains a recognized cause of sudden death in athletes.
Mitral valve prolapse (MVP) is characterized by bulging of one or both mitral valve leaflets into the left atrium during systole due to incomplete coaptation of the valve leaflets. It is most commonly caused by myxomatous degeneration of the valve, involving proliferation of the spongiosa layer with disruption of the fibrosa layer, along with excessive stretching of the chordae tendineae that places traction on the papillary muscles. Mitral regurgitation (MR) may develop in some patients. MVP typically presents between 10 and 16 years of age and is more common in females than males. It is generally benign in young women, whereas men over 50 years of age are more likely to develop severe regurgitation and require surgical intervention. MVP has a strong hereditary component and may be inherited in an autosomal dominant pattern with variable penetrance. A range of neuroendocrine and autonomic disturbances may also be associated with the condition.
MVP is associated with several connective tissue and systemic disorders, including Marfan syndrome, Ehlers–Danlos syndrome, osteogenesis imperfecta, pseudoxanthoma elasticum, Stickler syndrome, systemic lupus erythematosus, polyarteritis nodosa, polycystic kidney disease, von Willebrand disease, and Duchenne muscular dystrophy. These conditions contribute to abnormal connective tissue structure, predisposing the mitral valve to prolapse.
Clinical manifestations can be grouped into symptoms related to autonomic dysfunction, symptoms resulting from progression of mitral regurgitation, and complications such as stroke, infective endocarditis, or arrhythmias. Palpitations occur in up to 40% of patients and are commonly due to premature ventricular beats or paroxysmal supraventricular tachycardia. Chest pain occurs in about 10% of patients and is typically sharp, localized, nonexertional, and of variable duration. Dysautonomia-related symptoms include anxiety, panic attacks, fatigue, depression, migraine headaches, irritable bowel symptoms, and orthostatic intolerance. Syncope or presyncope is uncommon, occurring in less than 1% of cases, while dyspnea and fatigue are generally infrequent unless significant MR is present.
Physical examination classically reveals a mid-to-late systolic click best heard at the cardiac apex, often followed by a late systolic murmur. Maneuvers that reduce left ventricular volume, such as standing or Valsalva, cause the click to occur earlier in systole, while squatting delays it. Many patients exhibit skeletal abnormalities, including an asthenic body habitus, increased arm span relative to height, scoliosis or kyphosis, pectus excavatum, arachnodactyly, joint hypermobility, hypomastia, and a high-arched (“cathedral”) palate.
Diagnosis is often made clinically based on history and auscultation, with echocardiography used to confirm uncertain cases. On echocardiography, classic MVP is defined by superior displacement of the mitral leaflets greater than 2 mm into the left atrium during systole with leaflet thickness of at least 5 mm, while nonclassic MVP shows similar displacement with thinner leaflets. Electrocardiography is usually normal but may show ST-T wave changes, premature atrial or ventricular contractions, or QT prolongation. Chest radiography is typically normal unless significant MR leads to left atrial or ventricular enlargement.
Management is generally conservative, as many patients are asymptomatic and do not require treatment. β-blockers may be used for troublesome palpitations or chest pain, while magnesium supplementation may alleviate symptoms related to classic MVP syndrome. Orthostatic symptoms may respond to increased salt intake or fludrocortisone. Antiplatelet therapy is indicated in patients with transient ischemic attack or stroke. Significant MR, particularly in the presence of hypertension, may benefit from ACE inhibitors. Antibiotic prophylaxis is recommended only for selected patients with MVP and MR undergoing high-risk procedures, and is not indicated for isolated clicks without MR.
Hospital admission is reserved for patients with severe mitral regurgitation, ischemic chest pain, syncope, life-threatening arrhythmias, or cerebrovascular events. Asymptomatic patients without significant MR or dysrhythmias can be safely discharged. Cardiology referral is warranted for ventricular arrhythmias, evidence of disease progression, or risk of sudden death, while cardiothoracic surgical evaluation is indicated for symptomatic severe MR, reduced ejection fraction, pulmonary hypertension, or atrial fibrillation. Valve repair is preferred over replacement when feasible.
Regular follow-up every 3–5 years is recommended to monitor for progression of disease. Patients with MVP and MR should receive appropriate endocarditis prophylaxis during at-risk procedures and undergo evaluation before participating in high-intensity sports. A key clinical pitfall is attributing symptoms such as chest pain or syncope solely to MVP without appropriate evaluation, as MVP remains a recognized cause of sudden death in athletes.