- Published on
KembaraXtra-Medicine – Mitral Valve Prolapse
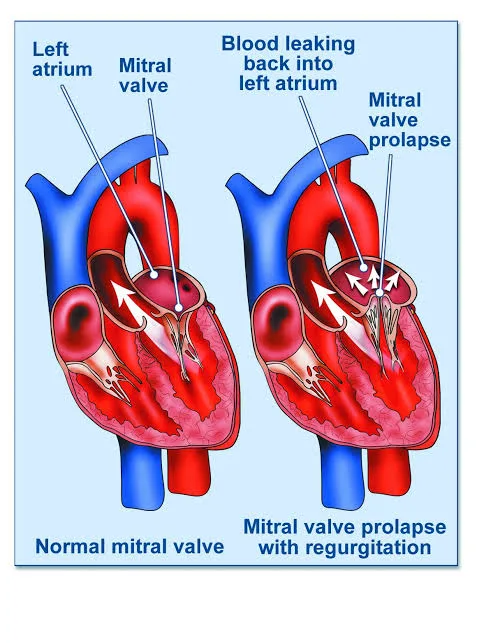
Mitral valve prolapse (MVP) is characterized by bulging of one or both mitral valve leaflets into the left atrium during systole due to incomplete coaptation of the valve leaflets. It is most commonly caused by myxomatous degeneration of the valve, involving proliferation of the spongiosa layer with disruption of the fibrosa layer, along with excessive stretching of the chordae tendineae that places traction on the papillary muscles. Mitral regurgitation (MR) may develop in some patients. MVP typically presents between 10 and 16 years of age and is more common in females than males. It is generally benign in young women, whereas men over 50 years of age are more likely to develop severe regurgitation and require surgical intervention. MVP has a strong hereditary component and may be inherited in an autosomal dominant pattern with variable penetrance. A range of neuroendocrine and autonomic disturbances may also be associated with the condition.
MVP is associated with several connective tissue and systemic disorders, including Marfan syndrome, Ehlers–Danlos syndrome, osteogenesis imperfecta, pseudoxanthoma elasticum, Stickler syndrome, systemic lupus erythematosus, polyarteritis nodosa, polycystic kidney disease, von Willebrand disease, and Duchenne muscular dystrophy. These conditions contribute to abnormal connective tissue structure, predisposing the mitral valve to prolapse.
Clinical manifestations can be grouped into symptoms related to autonomic dysfunction, symptoms resulting from progression of mitral regurgitation, and complications such as stroke, infective endocarditis, or arrhythmias. Palpitations occur in up to 40% of patients and are commonly due to premature ventricular beats or paroxysmal supraventricular tachycardia. Chest pain occurs in about 10% of patients and is typically sharp, localized, nonexertional, and of variable duration. Dysautonomia-related symptoms include anxiety, panic attacks, fatigue, depression, migraine headaches, irritable bowel symptoms, and orthostatic intolerance. Syncope or presyncope is uncommon, occurring in less than 1% of cases, while dyspnea and fatigue are generally infrequent unless significant MR is present.
Physical examination classically reveals a mid-to-late systolic click best heard at the cardiac apex, often followed by a late systolic murmur. Maneuvers that reduce left ventricular volume, such as standing or Valsalva, cause the click to occur earlier in systole, while squatting delays it. Many patients exhibit skeletal abnormalities, including an asthenic body habitus, increased arm span relative to height, scoliosis or kyphosis, pectus excavatum, arachnodactyly, joint hypermobility, hypomastia, and a high-arched (“cathedral”) palate.
Diagnosis is often made clinically based on history and auscultation, with echocardiography used to confirm uncertain cases. On echocardiography, classic MVP is defined by superior displacement of the mitral leaflets greater than 2 mm into the left atrium during systole with leaflet thickness of at least 5 mm, while nonclassic MVP shows similar displacement with thinner leaflets. Electrocardiography is usually normal but may show ST-T wave changes, premature atrial or ventricular contractions, or QT prolongation. Chest radiography is typically normal unless significant MR leads to left atrial or ventricular enlargement.
Management is generally conservative, as many patients are asymptomatic and do not require treatment. β-blockers may be used for troublesome palpitations or chest pain, while magnesium supplementation may alleviate symptoms related to classic MVP syndrome. Orthostatic symptoms may respond to increased salt intake or fludrocortisone. Antiplatelet therapy is indicated in patients with transient ischemic attack or stroke. Significant MR, particularly in the presence of hypertension, may benefit from ACE inhibitors. Antibiotic prophylaxis is recommended only for selected patients with MVP and MR undergoing high-risk procedures, and is not indicated for isolated clicks without MR.
Hospital admission is reserved for patients with severe mitral regurgitation, ischemic chest pain, syncope, life-threatening arrhythmias, or cerebrovascular events. Asymptomatic patients without significant MR or dysrhythmias can be safely discharged. Cardiology referral is warranted for ventricular arrhythmias, evidence of disease progression, or risk of sudden death, while cardiothoracic surgical evaluation is indicated for symptomatic severe MR, reduced ejection fraction, pulmonary hypertension, or atrial fibrillation. Valve repair is preferred over replacement when feasible.
Regular follow-up every 3–5 years is recommended to monitor for progression of disease. Patients with MVP and MR should receive appropriate endocarditis prophylaxis during at-risk procedures and undergo evaluation before participating in high-intensity sports. A key clinical pitfall is attributing symptoms such as chest pain or syncope solely to MVP without appropriate evaluation, as MVP remains a recognized cause of sudden death in athletes.
Mitral valve prolapse (MVP) is characterized by bulging of one or both mitral valve leaflets into the left atrium during systole due to incomplete coaptation of the valve leaflets. It is most commonly caused by myxomatous degeneration of the valve, involving proliferation of the spongiosa layer with disruption of the fibrosa layer, along with excessive stretching of the chordae tendineae that places traction on the papillary muscles. Mitral regurgitation (MR) may develop in some patients. MVP typically presents between 10 and 16 years of age and is more common in females than males. It is generally benign in young women, whereas men over 50 years of age are more likely to develop severe regurgitation and require surgical intervention. MVP has a strong hereditary component and may be inherited in an autosomal dominant pattern with variable penetrance. A range of neuroendocrine and autonomic disturbances may also be associated with the condition.
MVP is associated with several connective tissue and systemic disorders, including Marfan syndrome, Ehlers–Danlos syndrome, osteogenesis imperfecta, pseudoxanthoma elasticum, Stickler syndrome, systemic lupus erythematosus, polyarteritis nodosa, polycystic kidney disease, von Willebrand disease, and Duchenne muscular dystrophy. These conditions contribute to abnormal connective tissue structure, predisposing the mitral valve to prolapse.
Clinical manifestations can be grouped into symptoms related to autonomic dysfunction, symptoms resulting from progression of mitral regurgitation, and complications such as stroke, infective endocarditis, or arrhythmias. Palpitations occur in up to 40% of patients and are commonly due to premature ventricular beats or paroxysmal supraventricular tachycardia. Chest pain occurs in about 10% of patients and is typically sharp, localized, nonexertional, and of variable duration. Dysautonomia-related symptoms include anxiety, panic attacks, fatigue, depression, migraine headaches, irritable bowel symptoms, and orthostatic intolerance. Syncope or presyncope is uncommon, occurring in less than 1% of cases, while dyspnea and fatigue are generally infrequent unless significant MR is present.
Physical examination classically reveals a mid-to-late systolic click best heard at the cardiac apex, often followed by a late systolic murmur. Maneuvers that reduce left ventricular volume, such as standing or Valsalva, cause the click to occur earlier in systole, while squatting delays it. Many patients exhibit skeletal abnormalities, including an asthenic body habitus, increased arm span relative to height, scoliosis or kyphosis, pectus excavatum, arachnodactyly, joint hypermobility, hypomastia, and a high-arched (“cathedral”) palate.
Diagnosis is often made clinically based on history and auscultation, with echocardiography used to confirm uncertain cases. On echocardiography, classic MVP is defined by superior displacement of the mitral leaflets greater than 2 mm into the left atrium during systole with leaflet thickness of at least 5 mm, while nonclassic MVP shows similar displacement with thinner leaflets. Electrocardiography is usually normal but may show ST-T wave changes, premature atrial or ventricular contractions, or QT prolongation. Chest radiography is typically normal unless significant MR leads to left atrial or ventricular enlargement.
Management is generally conservative, as many patients are asymptomatic and do not require treatment. β-blockers may be used for troublesome palpitations or chest pain, while magnesium supplementation may alleviate symptoms related to classic MVP syndrome. Orthostatic symptoms may respond to increased salt intake or fludrocortisone. Antiplatelet therapy is indicated in patients with transient ischemic attack or stroke. Significant MR, particularly in the presence of hypertension, may benefit from ACE inhibitors. Antibiotic prophylaxis is recommended only for selected patients with MVP and MR undergoing high-risk procedures, and is not indicated for isolated clicks without MR.
Hospital admission is reserved for patients with severe mitral regurgitation, ischemic chest pain, syncope, life-threatening arrhythmias, or cerebrovascular events. Asymptomatic patients without significant MR or dysrhythmias can be safely discharged. Cardiology referral is warranted for ventricular arrhythmias, evidence of disease progression, or risk of sudden death, while cardiothoracic surgical evaluation is indicated for symptomatic severe MR, reduced ejection fraction, pulmonary hypertension, or atrial fibrillation. Valve repair is preferred over replacement when feasible.
Regular follow-up every 3–5 years is recommended to monitor for progression of disease. Patients with MVP and MR should receive appropriate endocarditis prophylaxis during at-risk procedures and undergo evaluation before participating in high-intensity sports. A key clinical pitfall is attributing symptoms such as chest pain or syncope solely to MVP without appropriate evaluation, as MVP remains a recognized cause of sudden death in athletes.
- Published on
KembaraXtra – Medicine – Molluscum Contagiosum
Molluscum contagiosum is a generally benign viral skin disease characterized by multiple small, painless, pearly papules. The infection is confined to the skin and mucous membranes and spreads through close personal contact or autoinoculation. It occurs worldwide with an estimated incidence of 2–8% and is more prevalent in tropical regions. Coinfection is common in immunocompromised patients, with up to 5–20% of individuals with HIV affected.
The condition is caused by a double-stranded DNA poxvirus of the Molluscipox genus. In children, transmission most commonly occurs through direct skin-to-skin contact, shared objects, or exposure to contaminated water such as swimming pools or baths. In adults, infection is most often acquired through sexual contact, although autoinoculation can occur at any age. Rarely, vertical transmission during childbirth has been reported.
After an incubation period of approximately 14–50 days, patients typically present with asymptomatic lesions, though mild pruritus or tenderness may occur. An eczematous reaction surrounding the lesions is seen in up to one-quarter of cases. In immunocompetent individuals, untreated lesions usually resolve spontaneously within several months but may persist for years. On examination, lesions appear as smooth, firm, dome-shaped papules measuring 2–6 mm in diameter. They may be flesh-colored, white, translucent, or light yellow and often contain a waxy, curd-like core composed of virion-rich material. A central umbilication is a classic feature, though it may be absent in some cases. Children most often have lesions on the face, trunk, and extremities, whereas healthy adults commonly have genital or lower abdominal involvement. In patients with HIV, lesions may be larger, disseminated, persistent, and involve the face, neck, and trunk, sometimes worsening with immune reconstitution after initiation of antiretroviral therapy.
Diagnosis is primarily clinical, based on history and characteristic skin findings. Skin biopsy may be performed when the diagnosis is uncertain. Adult men presenting with molluscum contagiosum should be evaluated for possible immunocompromise. In children, the condition is rarely associated with underlying immunodeficiency and typically does not require further investigation. Laboratory testing for immunosuppression, including HIV testing, may be indicated when lesions are extensive, atypical, or unexplained. Anogenital lesions warrant evaluation for other sexually transmitted infections.
Management is directed toward destruction or removal of infected epithelial cells to reduce autoinoculation and transmission. Active treatment is not always required, as lesions are self-limited in immunocompetent hosts. Immunocompromised patients are at higher risk for prolonged disease and secondary bacterial infection and more often require intervention. Physical treatment methods such as curettage, cryotherapy, or topical destructive agents are generally the most effective options. Patients should be advised to avoid scratching, shaving over lesions, sharing towels, contact sports, and swimming pools until lesions resolve. Sexual partners should be examined when genital involvement is present. Treated patients should be re-evaluated every 2–4 weeks, as multiple treatment sessions are often required.
Hospital admission is rarely necessary and is reserved for immunocompromised patients with extensive disease complicated by severe secondary infection. Most patients can be managed safely as outpatients, with dermatology referral considered when diagnosis is uncertain or disease is refractory to initial therapy. A key clinical pitfall is unnecessary aggressive treatment in immunocompetent patients, as observation alone is often appropriate, while failure to recognize underlying immunosuppression can delay appropriate management.

- Published on
Emergency and Acute Medicine – Myasthenia Gravis
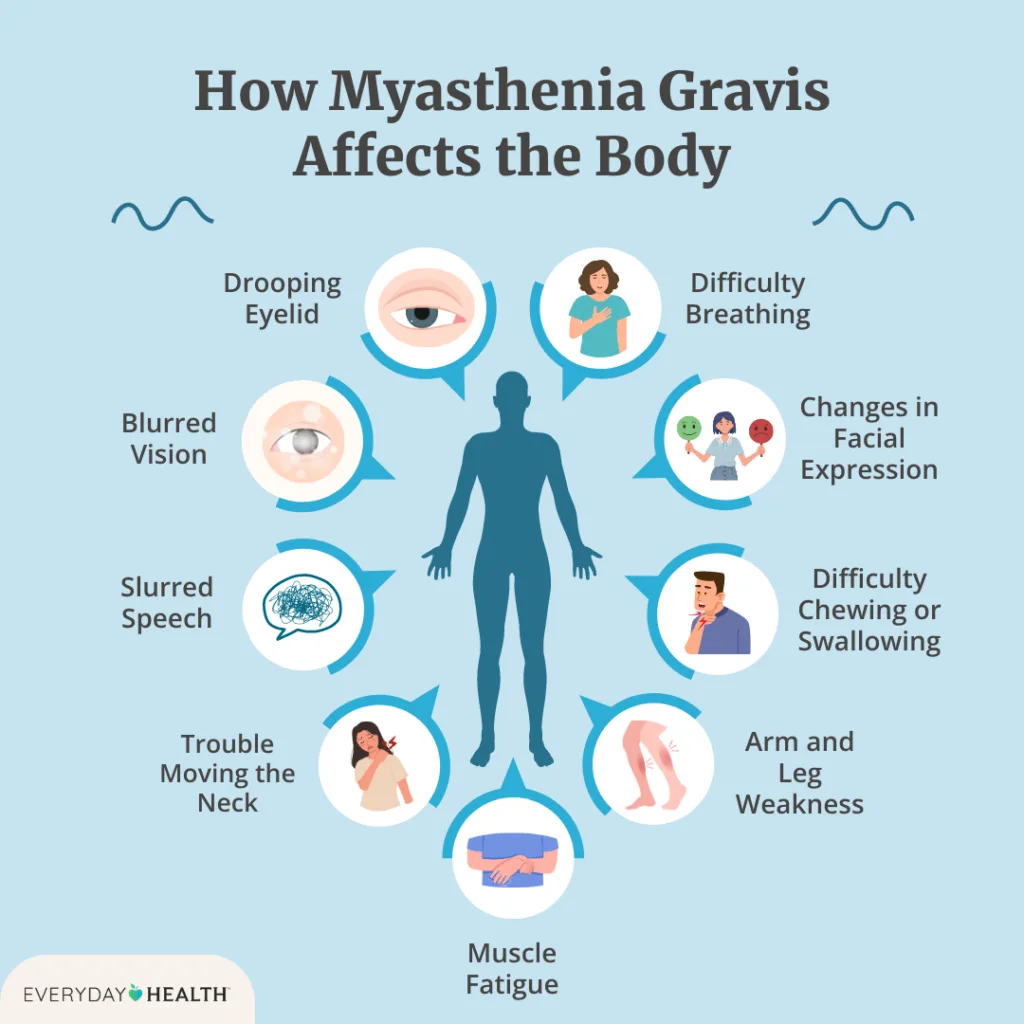
Myasthenia gravis (MG) is an antibody-mediated autoimmune disorder characterized by painless, fluctuating, and fatigable skeletal muscle weakness. Weakness typically worsens with repeated activity and improves with rest. The disease may present in an ocular form or as generalized myasthenia gravis. Ocular involvement, affecting the eyelids and extraocular muscles, is the most common initial presentation and accounts for approximately 60% of cases. Although symptoms may initially be limited to the eyes, nearly 80% of patients with ocular MG will progress to generalized disease within two years.
Generalized myasthenia gravis involves proximal limb muscles, axial musculature, and bulbar muscles, including those responsible for speech, chewing, and swallowing. The disease often follows an acute or subacute course with relapses and remissions. Thymic abnormalities are common, with thymic hyperplasia present in approximately 65% of patients and thymoma in about 15%. A life-threatening complication, known as myasthenic crisis, occurs when respiratory muscle weakness or bulbar dysfunction leads to respiratory failure or inability to protect the airway. Common triggers include infection, surgery, trauma, pregnancy, and medication changes, particularly rapid tapering of corticosteroids.
The pathophysiology of myasthenia gravis involves antibodies directed against nicotinic acetylcholine receptors at the neuromuscular junction, resulting in impaired neuromuscular transmission. Up to 20% of patients may be seronegative for acetylcholine receptor antibodies. Certain medications can induce or worsen myasthenic weakness, including aminoglycosides, macrolides, fluoroquinolones, beta-blockers, calcium-channel blockers, anticonvulsants, antipsychotics, and neuromuscular blocking agents. Penicillamine is a well-recognized cause of drug-induced MG.
Clinically, patients report fluctuating weakness that worsens with activity. Ocular symptoms include ptosis and diplopia, often noted during prolonged visual tasks such as reading or driving. Bulbar involvement leads to slurred or nasal speech, difficulty chewing, swallowing, and maintaining jaw closure. Limb weakness commonly affects proximal muscles, causing difficulty climbing stairs, rising from a seated position, or lifting objects overhead. On physical examination, ptosis, diplopia, and facial weakness may be evident, while reflexes and sensation remain normal. Repetitive testing of affected muscle groups typically reproduces weakness.
Emergency evaluation focuses on identifying respiratory compromise and precipitating factors such as infection. Diagnostic testing includes basic laboratory studies, thyroid function tests, and antibody testing for acetylcholine receptor antibodies. Imaging of the chest with CT is essential to evaluate for thymoma. Bedside diagnostic tools include the ice test, in which application of ice to the eyelid transiently improves ptosis, supporting the diagnosis. The edrophonium (Tensilon) test may produce short-lived improvement in strength but requires cardiac monitoring and atropine availability due to the risk of bradycardia and increased secretions.
Management in the emergency setting prioritizes airway protection and respiratory support. Patients in myasthenic crisis require early intubation and mechanical ventilation. Objective indicators of impending respiratory failure include reduced vital capacity and weak inspiratory pressures. In crisis, acetylcholinesterase inhibitors are typically withheld, and treatment includes plasmapheresis or intravenous immunoglobulin (IVIG), along with high-dose corticosteroids. Infections and other triggers must be identified and treated aggressively. Atropine may be used to counteract muscarinic effects in suspected cholinergic crisis.
Hospital admission is required for new-onset disease, diagnostic uncertainty, worsening weakness, or any evidence of respiratory compromise. Intensive care admission is mandatory for myasthenic crisis or borderline respiratory status. Patients who demonstrate improvement and have stable respiratory function may be discharged in consultation with neurology, with close outpatient follow-up arranged.
A key clinical pearl is that any patient with known myasthenia gravis presenting to the emergency department should be carefully evaluated for signs of myasthenic crisis and secondary precipitants. Early recognition and aggressive supportive management are essential to prevent respiratory failure and improve outcomes.
Myasthenia gravis (MG) is an antibody-mediated autoimmune disorder characterized by painless, fluctuating, and fatigable skeletal muscle weakness. Weakness typically worsens with repeated activity and improves with rest. The disease may present in an ocular form or as generalized myasthenia gravis. Ocular involvement, affecting the eyelids and extraocular muscles, is the most common initial presentation and accounts for approximately 60% of cases. Although symptoms may initially be limited to the eyes, nearly 80% of patients with ocular MG will progress to generalized disease within two years.
Generalized myasthenia gravis involves proximal limb muscles, axial musculature, and bulbar muscles, including those responsible for speech, chewing, and swallowing. The disease often follows an acute or subacute course with relapses and remissions. Thymic abnormalities are common, with thymic hyperplasia present in approximately 65% of patients and thymoma in about 15%. A life-threatening complication, known as myasthenic crisis, occurs when respiratory muscle weakness or bulbar dysfunction leads to respiratory failure or inability to protect the airway. Common triggers include infection, surgery, trauma, pregnancy, and medication changes, particularly rapid tapering of corticosteroids.
The pathophysiology of myasthenia gravis involves antibodies directed against nicotinic acetylcholine receptors at the neuromuscular junction, resulting in impaired neuromuscular transmission. Up to 20% of patients may be seronegative for acetylcholine receptor antibodies. Certain medications can induce or worsen myasthenic weakness, including aminoglycosides, macrolides, fluoroquinolones, beta-blockers, calcium-channel blockers, anticonvulsants, antipsychotics, and neuromuscular blocking agents. Penicillamine is a well-recognized cause of drug-induced MG.
Clinically, patients report fluctuating weakness that worsens with activity. Ocular symptoms include ptosis and diplopia, often noted during prolonged visual tasks such as reading or driving. Bulbar involvement leads to slurred or nasal speech, difficulty chewing, swallowing, and maintaining jaw closure. Limb weakness commonly affects proximal muscles, causing difficulty climbing stairs, rising from a seated position, or lifting objects overhead. On physical examination, ptosis, diplopia, and facial weakness may be evident, while reflexes and sensation remain normal. Repetitive testing of affected muscle groups typically reproduces weakness.
Emergency evaluation focuses on identifying respiratory compromise and precipitating factors such as infection. Diagnostic testing includes basic laboratory studies, thyroid function tests, and antibody testing for acetylcholine receptor antibodies. Imaging of the chest with CT is essential to evaluate for thymoma. Bedside diagnostic tools include the ice test, in which application of ice to the eyelid transiently improves ptosis, supporting the diagnosis. The edrophonium (Tensilon) test may produce short-lived improvement in strength but requires cardiac monitoring and atropine availability due to the risk of bradycardia and increased secretions.
Management in the emergency setting prioritizes airway protection and respiratory support. Patients in myasthenic crisis require early intubation and mechanical ventilation. Objective indicators of impending respiratory failure include reduced vital capacity and weak inspiratory pressures. In crisis, acetylcholinesterase inhibitors are typically withheld, and treatment includes plasmapheresis or intravenous immunoglobulin (IVIG), along with high-dose corticosteroids. Infections and other triggers must be identified and treated aggressively. Atropine may be used to counteract muscarinic effects in suspected cholinergic crisis.
Hospital admission is required for new-onset disease, diagnostic uncertainty, worsening weakness, or any evidence of respiratory compromise. Intensive care admission is mandatory for myasthenic crisis or borderline respiratory status. Patients who demonstrate improvement and have stable respiratory function may be discharged in consultation with neurology, with close outpatient follow-up arranged.
A key clinical pearl is that any patient with known myasthenia gravis presenting to the emergency department should be carefully evaluated for signs of myasthenic crisis and secondary precipitants. Early recognition and aggressive supportive management are essential to prevent respiratory failure and improve outcomes.
- Published on
Emergency and Acute Medicine – Necrotizing Ulcerative Gingivitis
Necrotizing ulcerative gingivitis (NUG) is an acute periodontal disease characterized by painful ulceration and necrosis of the gingival papillae, producing the classic “punched-out” appearance. It is also known as acute necrotizing ulcerative gingivitis, trench mouth, Vincent disease, or fusospirochetal gingivitis. The condition is not contagious and most commonly affects children and young adults, particularly in developing regions such as sub-Saharan Africa. In developed countries it is rare and is typically seen in severely immunocompromised individuals. Males are affected more often than females. If untreated, NUG can progress to more severe disease, including necrotizing stomatitis, necrotizing ulcerative periodontitis with alveolar bone involvement, or orofacial gangrene (noma).
The disease is caused by an overgrowth of normal oral flora, most notably Prevotella intermedia and spirochetes. While predisposing factors are not required for diagnosis, they are commonly present and include poor oral hygiene, gingivitis, malnutrition, smoking, emotional or physical stress, and immunodeficiency states such as HIV infection or other causes of immunosuppression. There is also a possible association with direct exposure to certain chemicals, including recreational drugs such as MDMA (ecstasy).
Clinically, NUG presents with acute onset of severe oral pain and bleeding gums that may occur spontaneously or with minimal manipulation. The hallmark finding on physical examination is loss of the interdental papillae, resulting in crater-like, “punched-out” ulcers that bleed easily. Necrotic debris often overlies the ulcerated areas, forming a grayish pseudomembrane that, when removed, reveals a bleeding surface. Patients frequently complain of foul breath and may have associated low-grade fever, malaise, and submandibular lymphadenopathy.
The diagnosis of necrotizing ulcerative gingivitis is primarily clinical, as laboratory tests and imaging studies are generally not helpful. Evaluation should focus on identifying underlying systemic disease, particularly immunosuppression, neutropenia, or HIV infection. It is also essential to assess for complications such as extension of lesions into the periodontal ligament and alveolar bone, progression to necrotizing stomatitis, or development of orofacial gangrene, which carries a high mortality rate if untreated.
Initial management focuses on supportive care and symptom relief. Dehydrated patients may require intravenous fluids. Pain control is achieved with topical agents such as viscous lidocaine and systemic analgesics, with narcotics rarely required. Gentle debridement of the pseudomembrane using gauze or a cotton-tipped applicator soaked in diluted hydrogen peroxide helps reduce bacterial load and improve healing. Antibiotic therapy is indicated in patients with fever, lymphadenopathy, or systemic symptoms, and in those who are immunocompromised. Common regimens include penicillin with metronidazole or clindamycin as an alternative.
Outpatient therapy is central to recovery and includes chlorhexidine gluconate mouth rinses, diluted hydrogen peroxide rinses, avoidance of oral irritants such as spicy foods and hot beverages, and reinforcement of good oral hygiene with gentle brushing and flossing. Nonsteroidal anti-inflammatory drugs or acetaminophen are usually sufficient for pain control. More extensive antimicrobial coverage, including antifungal or antiviral therapy, may be required in severely immunosuppressed patients.
Hospital admission is reserved for patients with extensive disease, significant systemic symptoms, severe dehydration with inability to tolerate oral intake, or evidence of progression to orofacial gangrene. Most patients who can maintain hydration and have no signs of advanced disease may be safely discharged with close follow-up. All patients require urgent referral to a dentist or periodontist for definitive care, including deep scaling and debridement.
Key clinical pearls include maintaining a high index of suspicion for underlying immunosuppression, particularly HIV infection, and recognizing that necrotizing ulcerative gingivitis can progress rapidly if left untreated. Early identification and prompt intervention are essential to prevent serious and potentially life-threatening complications.

- Published on
Emergency and Acute Medicine – Myocarditis
Myocarditis is an inflammatory disease of the heart muscle characterized by myocyte necrosis and subsequent myocardial destruction. The condition typically results from a direct cytotoxic injury to cardiac myocytes by an infectious or toxic agent, followed by a secondary immune-mediated response that worsens myocardial damage. The true incidence is unknown because many cases are mild or asymptomatic; however, autopsy studies suggest myocarditis is present in 1–7% of the general population and in more than 50% of patients with HIV. It is more common in males than females, with an average age at diagnosis of approximately 42 years, and is a major cause of unexpected sudden death in individuals younger than 40 years.
The etiology of myocarditis is broad and includes infectious, toxic, autoimmune, and hypersensitivity causes. Viral infections are the most common etiology, particularly enteroviruses such as coxsackievirus B, adenovirus, influenza, herpesviruses, hepatitis C, HIV, Epstein–Barr virus, and cytomegalovirus. Bacterial causes include diphtheria, tuberculosis, meningococcus, mycoplasma, and group A streptococcus. Parasitic infections such as Trypanosoma cruzi (Chagas disease) represent the most common global cause of myocarditis and heart failure, especially in Central and South America. Additional causes include fungal, rickettsial, helminthic infections, medications (notably anthracyclines, cocaine, and certain antibiotics), toxins, radiation, autoimmune diseases, and envenomation from insects or snakes.
Clinical presentation is variable and ranges from mild viral-like illness to fulminant heart failure and sudden cardiac death. Common symptoms include dyspnea, chest pain, palpitations, and fatigue. Chest pain is often pleuritic or sharp and may mimic acute coronary syndrome due to local inflammation or coronary spasm. Dyspnea on exertion is frequent, and orthopnea or paroxysmal nocturnal dyspnea suggests the development of congestive heart failure. Syncope is concerning and may indicate malignant ventricular dysrhythmias or high-grade conduction block. In children, myocarditis is the most common cause of heart failure in previously healthy patients and often presents with nonspecific findings such as poor feeding, respiratory distress, sweating with feeds, or new murmurs.
Physical examination findings depend on severity and may include fever, tachycardia disproportionate to fever, hypotension, cyanosis, jugular venous distention, bibasilar crackles, peripheral edema, hepatomegaly, ascites, and gallop rhythms. A diminished S1, murmurs of mitral or tricuspid regurgitation, or a pericardial friction rub may be present, particularly when myocarditis is associated with pericarditis. Hypotension and cardiogenic shock are uncommon early but indicate a poor prognosis when present.
Evaluation in the emergency setting includes electrocardiography, chest radiography, and targeted laboratory testing. ECG findings are often nonspecific and commonly show sinus tachycardia, ST- and T-wave changes, atrial or ventricular dysrhythmias, and conduction delays; up to 20% of patients may develop heart block or bundle branch block. Cardiac biomarkers may be elevated, reflecting myocardial necrosis, though normal values do not exclude myocarditis. Echocardiography is essential to assess ventricular function, wall-motion abnormalities, pericardial effusion, and intracardiac thrombus. Cardiac MRI with gadolinium enhancement is increasingly valuable, as it can identify myocardial inflammation and necrosis with high diagnostic accuracy. Endomyocardial biopsy is reserved for select cases, such as transplant recipients or patients with unexplained, rapidly progressive disease.
Management is largely supportive and focused on treating complications. All patients require close monitoring with attention to airway, breathing, and circulation. Dysrhythmias should be treated promptly, and patients with Mobitz II or complete heart block require pacing. Heart failure is managed with oxygen, diuretics, ACE inhibitors, and cautious use of digoxin. NSAIDs are contraindicated in the acute phase due to potential worsening of myocardial injury. Anticoagulation is indicated in patients with severe left ventricular dysfunction or documented intracardiac thrombus. In pediatric viral myocarditis, intravenous immunoglobulin has been shown to improve ventricular function and outcomes. Sympathomimetic agents and β-blockers should generally be avoided in the acute setting.
Disposition depends on severity. All symptomatic patients, particularly those with dysrhythmias, new-onset heart failure, conduction abnormalities, thromboembolic events, or cardiogenic shock, require hospital admission, often to a monitored or intensive care setting. Asymptomatic patients without evidence of cardiac dysfunction or arrhythmia may be considered for discharge with close follow-up. Early recognition and careful monitoring are critical, as myocarditis carries significant morbidity and mortality, and progression to chronic cardiomyopathy or need for cardiac transplantation can occur despite initial stabilization.

- Published on
Emergency and Acute Medicine – Nasal Fractures
Nasal fractures are the most common fractures of the facial skeleton and of the body overall. They usually result from blunt trauma, most commonly due to motor vehicle crashes, sports injuries, and interpersonal altercations. Lateral forces are more likely to cause displacement than direct frontal blows. Although many nasal fractures are isolated and uncomplicated, certain historical and physical features suggest more serious associated injuries, including high-force trauma, loss of consciousness, obvious facial bone injury, frontal bone crepitus, or cerebrospinal fluid (CSF) leakage.
The etiology of nasal fractures is overwhelmingly direct trauma. In adults, altercations are the most frequent cause, whereas in children, sports-related direct blows predominate. Because the pediatric nasal skeleton is more cartilaginous and flexible, significant injury may be present even when deformity appears minimal.
Patients typically present with nasal pain, swelling, deformity, asymmetry, ecchymosis, and epistaxis. Periorbital ecchymosis (“raccoon eyes”) may indicate injury to branches of the ethmoidal artery and raises concern for nasofrontoethmoid complex fractures. Palpable irregularities, sharp edges, crepitus, or abnormal mobility of nasal bones strongly suggest fracture. A critical associated finding is a septal hematoma, which appears as a bluish, fluctuant swelling of the nasal septum; failure to promptly identify and drain it can lead to septal necrosis and permanent deformity. Flattening of the nasal bridge with widening of the intercanthal distance (telecanthus) suggests a serious nasofrontoethmoid injury. Clear rhinorrhea raises concern for a CSF leak, which may be delayed, and anosmia suggests more significant trauma.
History should focus on the mechanism of injury, presence of epistaxis, visual or olfactory changes, and other associated injuries. Physical examination must include careful inspection and palpation of the nose and midface, with particular attention to identifying a septal hematoma and signs of telecanthus. Examination for CSF rhinorrhea is essential; blood-tinged CSF may produce a “double-ring” sign on filter paper, though this finding is not fully reliable.
Routine imaging is rarely required for simple nasal fractures, as radiographs seldom change management. Gross deformities warrant specialist referral regardless of imaging findings, and nondisplaced fractures are treated conservatively even if radiographically evident. Computed tomography is the imaging modality of choice when facial bone fractures, nasofrontoethmoid injuries, or skull base fractures are suspected, and clinicians should have a low threshold for ordering CT when associated injuries are possible.
Initial management prioritizes airway and cervical spine protection, especially in patients with multisystem trauma. Nasotracheal intubation is contraindicated; if airway control is required, orotracheal intubation or cricothyroidotomy should be performed. Epistaxis is often controlled with direct pressure but may require topical anesthetics and vasoconstrictors, cauterization, or nasal packing. Patients with nasal packing should receive prophylactic antibiotics to reduce the risk of sinus and staphylococcal infections.
Definitive reduction of displaced nasal fractures is usually deferred until swelling subsides, typically within 3–5 days, and is performed by an ENT, plastic surgeon, or oral and maxillofacial surgeon. Immediate reduction in the emergency department is generally unnecessary unless airway compromise exists. In contrast, septal hematomas require urgent drainage in the ED, followed by bilateral nasal packing and antibiotic therapy to prevent reaccumulation and infection.
Most patients with isolated nasal fractures can be discharged once epistaxis is controlled and no associated injuries are identified, provided they have reliable follow-up. Admission is reserved for patients with nasoethmoid fractures, CSF leaks, or significant craniofacial injuries. All patients should receive clear instructions to follow up with a specialist within 3–5 days, or sooner (within 24 hours) if a septal hematoma was drained. Careful documentation of the absence or presence of a septal hematoma is essential in every case, as missed hematomas are a common and preventable cause of long-term complications.

- Published on
Emergency and Acute Medicine – Neck Injury by Strangulation/Hanging
Neck injury from strangulation can occur through ligature strangulation (a material compressing the neck), manual strangulation (direct pressure using hands), or postural strangulation (airway obstruction from body weight over an object or positioning, most often in infants). Hanging is a form of strangulation and may be complete (judicial type), where the entire body is suspended, or incomplete (nonjudicial), where part of the body remains in contact with the ground. Typical hanging places the suspension point centrally over the occiput, while atypical hanging places it elsewhere. These events may be intentional (suicide, homicide, autoerotic activity, or “the choking game”) or accidental, especially in children. Near-hanging refers to survival following nonjudicial hanging.
In judicial hanging, the victim is dropped a distance at least equal to their height, producing forceful distraction of the head from the torso. This can cause severe cervical spine fracture and spinal cord transection. In nonjudicial hanging, the fall is usually from a lower height and injuries resemble those seen in strangulation. In strangulation, external neck pressure leads to cerebral hypoxia due to venous and arterial obstruction, and may also injure airway structures, soft tissues, and neck vessels. Cervical spine injuries are uncommon except with judicial-type hanging. Death may occur from mechanical closure of the airway or blood vessels, cardiac arrest caused by extreme bradycardia from carotid sinus stimulation, direct spinal cord injury, pulmonary complications in near-hanging victims, or cerebral hypoxia.
Commonly associated conditions include cervical spine injury, hypoxic brain injury, arterial or venous dissection or thrombosis, hyoid bone fracture (typically in nonjudicial strangulation), cricoid cartilage disruption (rare), and thyroid cartilage disruption (more common in nonjudicial strangulation deaths). Other complications include phrenic nerve injury, airway edema, aspiration pneumonitis (often delayed), neurogenic pulmonary edema (delayed, due to massive sympathetic discharge), postobstructive pulmonary edema (which may develop rapidly), and possible air embolism when subcutaneous air and vascular injury are present.
Symptoms and signs may involve multiple systems. Airway disruption can present with subcutaneous emphysema, dyspnea, dysphonia or stridor, and loss of normal neck cartilage landmarks. Cervical spine injury can cause respiratory arrest or paralysis. Neurologic injury may present with hoarseness, dysphagia, altered mental status, or focal neurologic deficits. Pulmonary sequelae can include respiratory distress, pulmonary edema, ARDS, or pneumonia. Soft tissue findings may include abrasions, contusions, ecchymoses, and ligature or hand marks. Vascular injuries may present with an expanding hematoma, pulse deficits, bruits, or evidence of cerebral infarction. Petechial hemorrhages above the ligature mark (Tardieu spots) may be seen on the skin, mucous membranes, or conjunctiva. In children, neck structures are more cartilaginous and mobile, making fractures less common, but airway compromise can occur quickly with relatively little edema because of the smaller airway diameter.
History should focus on the strangulation method and patient position to help predict injury patterns. A higher fall implies greater force and raises concern for decapitation-type injury. Knot position affects injury risk, with arterial occlusion more likely in typical hanging. Ligature material matters because elastic materials may limit peak force but venous obstruction can still cause unconsciousness and death. Circumstances should be clarified, including accidental injury, suicide/homicide, nonaccidental trauma, sexual context, or “choking game.” Physical examination should begin with ABCs and strict cervical spine precautions, followed by neurologic assessment for coma, altered mental status, paralysis, or focal deficits. A secondary survey should look for soft tissue injury, aero-digestive injury, and vascular trauma, as well as other trauma from falls, self-inflicted injuries, or assault.
Essential workup includes CT of the cervical spine through T1, CT of the head to assess for hemorrhage, edema, hematoma, subarachnoid hemorrhage, or hypoxic injury, and CT angiography of the neck to evaluate for thrombosis or intimal dissection. A chest radiograph helps detect subcutaneous emphysema, aspiration pneumonitis, and pulmonary edema. Continuous pulse oximetry and cardiac monitoring are required. Additional testing may include an ABG if respiratory compromise is suspected, hematocrit if significant blood loss is possible, type and cross-match if vascular injury is suspected, and coagulation studies for bleeding risk. Toxicology testing may be appropriate when intentional self-harm is suspected. MRI of the neck can be more sensitive than CT for soft tissue and cartilaginous injury, and arteriography remains a definitive test for vascular injury. Fiberoptic endoscopy can directly evaluate aero-digestive injury and may help with intubation decisions, while surgical exploration is reserved for indicated cases.
Prehospital care prioritizes rapid airway management with oxygen, suction, and intubation when indicated, while removing any ligature and maintaining cervical spine stabilization. In the emergency department, aggressive airway management with cervical spine precautions remains the priority, with early intubation for respiratory compromise and supplemental oxygen. Cricothyrotomy or tracheostomy may be required in severe facial trauma, but cricothyrotomy should be avoided if there is hematoma over the cricothyroid membrane or suspected cricotracheal disruption; emergent tracheostomy is preferred in that scenario. Bleeding should be controlled with direct pressure and the neck should not be explored in the ED.
Emergency treatment includes establishing IV access and consulting appropriate specialists: otolaryngology or trauma surgery for soft tissue and airway injuries, vascular surgery for suspected vascular injury, neurology for suspected ischemic insult, and neurosurgery if intracranial pressure monitoring or intervention is needed. Supportive care for suspected cerebral edema includes elevating the head of bed, maintaining oxygenation and cerebral perfusion, and preventing secondary neurologic injury. If subcutaneous emphysema is present, assume upper airway mucosal disruption communicating with deep tissues and administer antibiotics. Steroids may be considered for airway edema. Clinicians should also evaluate for associated harm such as co-ingestions in suicidal cases and must report suspected nonaccidental trauma in children.
Medications may include mannitol or hypertonic saline in selected cases of elevated intracranial pressure, and phenytoin for seizures when needed. For neck injury with subcutaneous emphysema, antibiotics such as ampicillin/sulbactam or clindamycin may be used. For airway edema, dexamethasone may be considered, with dosing adjusted for pediatric patients.
Disposition is typically admission to a monitored setting for all strangulation or hanging-mechanism injuries due to the risk of delayed airway compromise, pulmonary edema, or neurologic deterioration. Admission is required for altered consciousness, new neurologic deficits, coma, respiratory distress, or injuries requiring surgical correction, including laryngeal, esophageal, or vascular injuries. All suspected suicidal or homicidal cases require psychiatric or social work consultation, and pediatric cases with suspected nonaccidental trauma require safety evaluation. Discharge is appropriate only for patients without strangulation or hanging injuries after adequate ED observation confirms no airway compromise, vascular injury, neurologic deficit, or suicidal/homicidal risk.
Follow-up recommendations include neuropsychiatric evaluation when hypoxic encephalopathy is a concern, psychiatric follow-up for suicidal or homicidal patients, behavioral therapy for autoerotic or “choking game” cases, and surgical follow-up as indicated by the injuries. Key pitfalls include failing to recognize delayed airway or pulmonary complications, missing vascular injury or dissection, and underestimating severity in patients who initially appear stable. Cervical spine injury is uncommon in nonjudicial hanging, and cerebral hypoxia is the most common cause of death, so rapid airway control and full evaluation for associated injuries are essential.
- Published on
Emergency and Acute Medicine – Necrotizing Soft Tissue Infections
Necrotizing soft tissue infections (NSTIs) are rapidly progressive infections involving any layer of the skin and underlying soft tissues, characterized by widespread necrosis, severe systemic toxicity, and a high mortality rate. These infections spread quickly along tissue planes, often causing extensive fascial and muscle destruction with relative sparing of the skin in early stages. Clinical entities within this spectrum include necrotizing fasciitis, Fournier gangrene, clostridial and nonclostridial myonecrosis, crepitant anaerobic cellulitis, and progressive bacterial gangrene. Despite being uncommon, NSTIs carry mortality rates of 24–34% and are associated with significant morbidity such as amputations, renal failure, and prolonged critical illness.
NSTIs typically arise in the setting of local tissue trauma, ischemia, or impaired host defenses. Risk is increased in older adults, smokers, and patients with chronic systemic disease including diabetes mellitus, obesity, peripheral vascular disease, chronic kidney disease, alcohol abuse, immunosuppression, and intravenous drug use. Type I NSTIs, which account for approximately 80% of cases, are polymicrobial infections involving aerobic and anaerobic organisms and commonly occur after surgery or in patients with chronic illness. Type II NSTIs are usually monomicrobial, most often caused by group A β-hemolytic streptococcus, and can affect young, otherwise healthy individuals; these infections are the classic “flesh-eating” disease. Type III NSTIs are rare but fulminant, frequently clostridial in origin, and often follow penetrating trauma, crush injuries, or injection drug use. Pediatric cases are uncommon but may occur in neonates after omphalitis or circumcision, or in children following recent varicella infection, surgery, or in those with immunodeficiency.
The clinical presentation can be subtle early but deteriorates rapidly. Patients often report fever, malaise, altered mental status, and severe pain at the affected site. A hallmark feature is pain that is disproportionate to physical findings. Within the first 24 hours, localized swelling, warmth, erythema, and tenderness develop, followed over the next 24–48 hours by skin discoloration (purple or blue), hemorrhagic bullae, and foul-smelling, thin drainage due to necrosis of fascia and fat. Systemic toxicity is common and includes tachycardia, tachypnea, hypotension, fever, and mental status changes. Crepitus, while pathognomonic, is present in only a minority of cases. In children, localized pain and rash are the most common presenting features, while hypotension and shock are less frequent early findings.
Diagnosis is challenging and relies heavily on clinical suspicion, particularly in high-risk patients who appear severely ill or have pain out of proportion to examination findings. Laboratory abnormalities may include leukocytosis, electrolyte derangements, renal dysfunction, hypocalcemia from fat necrosis, and evidence of disseminated intravascular coagulation. Imaging studies such as plain radiographs, CT, MRI, or ultrasound may demonstrate soft tissue gas, fascial thickening, or fluid along fascial planes, but absence of these findings does not exclude NSTI. Importantly, imaging should never delay surgical intervention. Definitive diagnosis is established by surgical exploration with deep tissue biopsy and cultures, which remains the gold standard.
Management of NSTIs is a true surgical emergency. Initial stabilization focuses on airway protection, aggressive fluid resuscitation, oxygenation, and correction of metabolic disturbances. Broad-spectrum intravenous antibiotics must be initiated immediately, targeting aerobic gram-positive and gram-negative organisms, anaerobes, and methicillin-resistant Staphylococcus aureus until culture results are available. Clindamycin should be started early, particularly when group A streptococcal infection is suspected, due to its ability to suppress toxin production. However, antimicrobial therapy alone is insufficient; early and aggressive surgical debridement of all necrotic tissue with fasciotomy and drainage is the cornerstone of treatment and must not be delayed. Adjunctive therapies such as hyperbaric oxygen and intravenous immunoglobulin may be considered in select cases, though their roles remain controversial.
All patients with NSTI require hospital admission, typically to an intensive care setting, for ongoing surgical management, intravenous antibiotics, and close monitoring for complications such as acute respiratory distress syndrome, renal failure, myocardial dysfunction, and disseminated intravascular coagulation. No patient with NSTI is appropriate for discharge. Key clinical pearls include maintaining a high index of suspicion, recognizing pain out of proportion to examination as a critical clue, and understanding that mortality approaches 100% if treatment is limited to antibiotics without prompt surgical debridement.


- Published on
Emergency and Acute Medicine – Myocardial Contusion
Myocardial contusion, also referred to as blunt cardiac injury (BCI), is a form of cardiac trauma resulting from blunt force to the chest. Pathologically, it is characterized by a discrete, well-demarcated area of myocardial hemorrhage, most commonly involving the subendocardium. In some cases, the injury may extend in a pyramidal, transmural fashion. Due to its anatomic position, the anterior wall of the right ventricle or right atrium is most frequently affected.
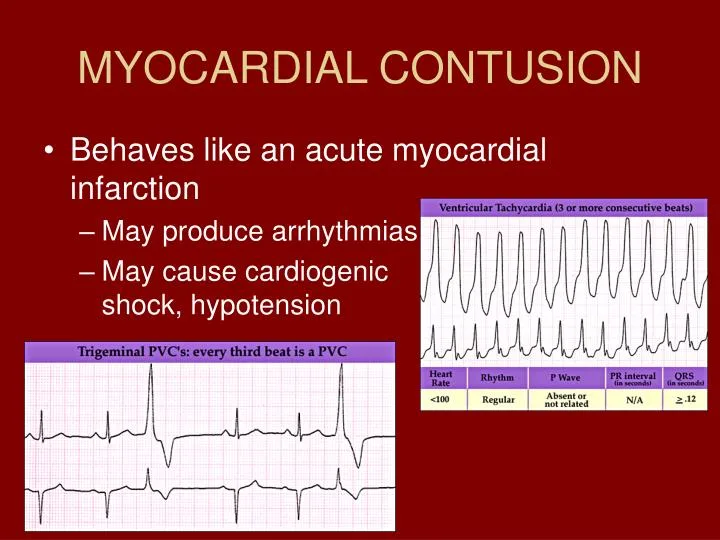
The etiology of myocardial contusion is blunt chest trauma. High-speed motor vehicle collisions are the most common cause, although injuries have been reported at speeds as low as 20–35 mph. Other mechanisms include auto–pedestrian accidents, falls, explosions, crush injuries, and prolonged closed-chest cardiac massage. Injury may occur through direct compression of the heart between the sternum and vertebral column, deceleration forces causing the heart to strike the sternum, or upward displacement of abdominal viscera transmitting force to the heart. Concussive forces may also contribute. Myocardial contusion may be associated with serious complications, including life-threatening dysrhythmias, cardiogenic shock, congestive heart failure, hemopericardium with tamponade, valvular or myocardial rupture, intraventricular thrombus, thromboembolic events, and, rarely, coronary artery occlusion due to intimal injury or edema.
Clinical presentation is highly variable and often nonspecific. Patients may complain of chest pain, develop cardiogenic shock, or exhibit only subtle electrocardiographic changes without symptoms. The most common clinical finding is sinus tachycardia that appears disproportionate to the degree of trauma or blood loss. Retrosternal chest pain, often unrelieved by nitroglycerin, may be delayed for up to 24 hours and may respond to supplemental oxygen. Other findings include friction rubs (rare), signs of thoracic trauma such as contusions or abrasions, crepitus, flail chest segments, or sternal fractures. Importantly, isolated sternal fracture with a normal ECG and negative serial troponin I does not predict blunt cardiac injury. Symptoms may be masked by other traumatic injuries. A history of syncope or loss of consciousness raises concern for dysrhythmia. In elderly patients, pre-existing cardiac disease and medications must be carefully considered, while in pediatric patients significant cardiac injury may occur despite minimal external signs due to the compliance of the chest wall.
There is no single diagnostic test that definitively confirms myocardial contusion. Electrocardiography is the best initial screening tool and should be obtained in all patients with suspected blunt cardiac injury. Sinus tachycardia is the most common finding, but ECG abnormalities may include nonspecific ST changes, right bundle branch block, or premature atrial or ventricular contractions. A normal ECG does not exclude myocardial injury, and repeat ECGs are recommended because abnormalities may evolve over time. Cardiac troponin I is the preferred laboratory marker and should be obtained in conjunction with ECG findings; levels should be repeated at 6–8 hours after injury. Any elevation warrants admission. Echocardiography is indicated in patients with ECG abnormalities or elevated troponins to assess for wall-motion abnormalities, effusions, or structural injury. Transesophageal echocardiography is more sensitive than transthoracic echocardiography but is more invasive. FAST examination should be performed to assess for pericardial effusion and associated intra-abdominal injuries. CT or MRI may assist in evaluating associated thoracic injuries but have no pathognomonic findings for myocardial contusion.
Management in the emergency setting focuses on supportive care and treatment of complications. Airway management, oxygen supplementation, intravenous access, and continuous cardiac monitoring are essential. Dysrhythmias are treated using standard protocols for nontraumatic arrhythmias, and prophylactic antiarrhythmic therapy is not recommended. Cardiogenic shock should be managed with cautious fluid resuscitation and inotropic support when necessary, with intra-aortic balloon counterpulsation reserved for severe cases. There is no specific therapy to reverse myocardial contusion itself; treatment is directed toward hemodynamic stabilization and management of associated injuries.
Disposition decisions require caution, as adverse outcomes—particularly dysrhythmias—most often occur within the first 24 hours. All patients in whom myocardial contusion is strongly suspected should be admitted to a monitored setting. Admission is indicated for any ECG abnormality, elevated cardiac enzymes, hemodynamic instability, or imaging suggestive of cardiac injury. Asymptomatic patients with normal ECGs and normal serial troponin I levels after 6–8 hours of observation may be safely discharged with close follow-up within 24 hours.
Key clinical pearls include the importance of obtaining an ECG in all patients with significant chest trauma and performing a FAST examination to assess for pericardial effusion. External signs of chest wall injury should heighten suspicion for blunt cardiac injury, while their absence—especially in pediatric patients—does not exclude it. Thrombolytic therapy should not be administered for ST-elevation myocardial infarction following trauma. A normal ECG combined with a negative troponin I level makes clinically significant blunt cardiac injury unlikely.
Myocardial contusion, also referred to as blunt cardiac injury (BCI), is a form of cardiac trauma resulting from blunt force to the chest. Pathologically, it is characterized by a discrete, well-demarcated area of myocardial hemorrhage, most commonly involving the subendocardium. In some cases, the injury may extend in a pyramidal, transmural fashion. Due to its anatomic position, the anterior wall of the right ventricle or right atrium is most frequently affected.
The etiology of myocardial contusion is blunt chest trauma. High-speed motor vehicle collisions are the most common cause, although injuries have been reported at speeds as low as 20–35 mph. Other mechanisms include auto–pedestrian accidents, falls, explosions, crush injuries, and prolonged closed-chest cardiac massage. Injury may occur through direct compression of the heart between the sternum and vertebral column, deceleration forces causing the heart to strike the sternum, or upward displacement of abdominal viscera transmitting force to the heart. Concussive forces may also contribute. Myocardial contusion may be associated with serious complications, including life-threatening dysrhythmias, cardiogenic shock, congestive heart failure, hemopericardium with tamponade, valvular or myocardial rupture, intraventricular thrombus, thromboembolic events, and, rarely, coronary artery occlusion due to intimal injury or edema.
Clinical presentation is highly variable and often nonspecific. Patients may complain of chest pain, develop cardiogenic shock, or exhibit only subtle electrocardiographic changes without symptoms. The most common clinical finding is sinus tachycardia that appears disproportionate to the degree of trauma or blood loss. Retrosternal chest pain, often unrelieved by nitroglycerin, may be delayed for up to 24 hours and may respond to supplemental oxygen. Other findings include friction rubs (rare), signs of thoracic trauma such as contusions or abrasions, crepitus, flail chest segments, or sternal fractures. Importantly, isolated sternal fracture with a normal ECG and negative serial troponin I does not predict blunt cardiac injury. Symptoms may be masked by other traumatic injuries. A history of syncope or loss of consciousness raises concern for dysrhythmia. In elderly patients, pre-existing cardiac disease and medications must be carefully considered, while in pediatric patients significant cardiac injury may occur despite minimal external signs due to the compliance of the chest wall.
There is no single diagnostic test that definitively confirms myocardial contusion. Electrocardiography is the best initial screening tool and should be obtained in all patients with suspected blunt cardiac injury. Sinus tachycardia is the most common finding, but ECG abnormalities may include nonspecific ST changes, right bundle branch block, or premature atrial or ventricular contractions. A normal ECG does not exclude myocardial injury, and repeat ECGs are recommended because abnormalities may evolve over time. Cardiac troponin I is the preferred laboratory marker and should be obtained in conjunction with ECG findings; levels should be repeated at 6–8 hours after injury. Any elevation warrants admission. Echocardiography is indicated in patients with ECG abnormalities or elevated troponins to assess for wall-motion abnormalities, effusions, or structural injury. Transesophageal echocardiography is more sensitive than transthoracic echocardiography but is more invasive. FAST examination should be performed to assess for pericardial effusion and associated intra-abdominal injuries. CT or MRI may assist in evaluating associated thoracic injuries but have no pathognomonic findings for myocardial contusion.
Management in the emergency setting focuses on supportive care and treatment of complications. Airway management, oxygen supplementation, intravenous access, and continuous cardiac monitoring are essential. Dysrhythmias are treated using standard protocols for nontraumatic arrhythmias, and prophylactic antiarrhythmic therapy is not recommended. Cardiogenic shock should be managed with cautious fluid resuscitation and inotropic support when necessary, with intra-aortic balloon counterpulsation reserved for severe cases. There is no specific therapy to reverse myocardial contusion itself; treatment is directed toward hemodynamic stabilization and management of associated injuries.
Disposition decisions require caution, as adverse outcomes—particularly dysrhythmias—most often occur within the first 24 hours. All patients in whom myocardial contusion is strongly suspected should be admitted to a monitored setting. Admission is indicated for any ECG abnormality, elevated cardiac enzymes, hemodynamic instability, or imaging suggestive of cardiac injury. Asymptomatic patients with normal ECGs and normal serial troponin I levels after 6–8 hours of observation may be safely discharged with close follow-up within 24 hours.
Key clinical pearls include the importance of obtaining an ECG in all patients with significant chest trauma and performing a FAST examination to assess for pericardial effusion. External signs of chest wall injury should heighten suspicion for blunt cardiac injury, while their absence—especially in pediatric patients—does not exclude it. Thrombolytic therapy should not be administered for ST-elevation myocardial infarction following trauma. A normal ECG combined with a negative troponin I level makes clinically significant blunt cardiac injury unlikely.
- Published on
Emergency and Acute Medicine – Neck Trauma, Blunt, Anterior
Blunt anterior neck trauma can result in injury to multiple critical structures, including vascular, laryngotracheal, pharyngoesophageal, neurologic, and cervical spine components. Vascular injuries may involve the carotid or vertebral arteries and include intramural hematoma, intimal tear, thrombosis, pseudoaneurysm, hemorrhage, or expanding neck hematoma. Laryngotracheal injuries include fractures of the hyoid bone, thyroid or cricoid cartilage, cricotracheal separation, vocal cord disruption, arytenoid dislocation, and tracheal hematoma or transection. Pharyngoesophageal injuries may present as hematoma or perforation of the pharynx or esophagus. Neurologic injury can involve the thoracic sympathetic chain causing Horner syndrome, the vagus or recurrent laryngeal nerves, cervical nerve roots, or spinal cord. Cervical spine fractures or dislocations may also be present.
The most common etiology is motor vehicle collisions, particularly frontal impacts in unrestrained occupants striking the dashboard or steering wheel (“padded dash syndrome”), or from shoulder harness–related shearing injury. Other causes include assault with blows to the anterior neck, “clothesline injuries” from motorcycles or recreational vehicles striking suspended wires or cords, and strangulation. In children, the proportionally larger head increases risk for acceleration–deceleration injury, and intraoral trauma to the soft palate may lead to carotid artery thrombosis.
Clinical presentation varies by injured structure. Vascular injury may cause hemorrhage, ecchymosis, edema, carotid bruit or thrill (highly suggestive of vascular injury), and delayed neurologic deficits. Laryngotracheal injury may present with hoarseness, aphonia, dyspnea, inspiratory stridor, labored breathing, air hunger, subcutaneous emphysema, and anterior neck tenderness. Pharyngoesophageal injury may cause dysphagia, odynophagia, hematemesis, blood in saliva, and delayed infection or sepsis. Neurologic injury may manifest as central or peripheral deficits. History should focus on mechanism, force, associated symptoms, and injuries beyond the neck, as blunt neck trauma is commonly associated with head and chest injuries.
Physical examination must prioritize airway protection and patency. The neck should be inspected for hemorrhage, hematoma, ecchymosis, edema, and anatomic distortion, auscultated for carotid bruits or stridor, and palpated for tenderness or subcutaneous emphysema. A complete neurologic examination is essential to detect ischemic events, spinal cord injury, or peripheral nerve damage, along with a full trauma examination for associated injuries.
Workup depends on clinical findings. Laboratory studies may include type and cross-match, CBC, and renal function prior to contrast imaging. Cervical spine and lateral neck radiographs have limited value but may show prevertebral swelling, subglottic narrowing, subcutaneous air, or calcified cartilage fractures. Chest radiograph is useful for detecting pneumothorax or pneumomediastinum. Carotid duplex ultrasonography is a rapid, noninvasive screening tool but is operator dependent and limited above the bifurcation. CT is useful in stable patients to evaluate laryngotracheal injury, cartilage disruption, and cervical spine trauma. CT angiography and magnetic resonance angiography have high specificity but limited sensitivity; four-vessel angiography remains the gold standard for arterial injury evaluation. Indications for angiography include carotid bruit, expanding neck hematoma, neurologic deficit with normal head CT, Horner syndrome, or decreased level of consciousness. Fiberoptic laryngoscopy can assess airway injury and assist with intubation, while suspected esophageal injury should be evaluated initially with a contrast swallow study. Unstable patients require immediate surgical intervention.
Prehospital and initial management focus on vigilant airway monitoring, as edema or hematoma may rapidly compromise the airway. Orotracheal intubation is preferred, while blind nasotracheal intubation should be avoided due to distorted anatomy and risk of hematoma rupture. Cervical spine stabilization is mandatory. Immediate airway control is indicated for respiratory distress, stridor, air hunger, or expanding neck hematoma. Cricothyrotomy or emergent tracheostomy may be required if intubation fails, but is contraindicated when bruising or hematoma overlies the thyroid or cricoid cartilage. Unstable patients should proceed directly to the operating room.
Emergency department management requires early surgical consultation for suspected vascular, tracheal, or esophageal injuries, with immediate repair for symptomatic vascular, tracheal, pharyngeal, or esophageal injuries. Laryngeal injuries may not always require immediate surgery. Anticoagulation is often recommended for vascular injuries to reduce thrombosis and improve neurologic outcomes, but only after surgical consultation. Prophylactic antibiotics with anaerobic coverage are indicated when esophageal injury is present.
Patients who are symptomatic, have abnormal imaging, or sustained significant blunt mechanisms require admission and observation for at least 24 hours, with ICU admission for suspected airway or vascular injury. Patients on anticoagulation should be observed for delayed neck hematoma. Only those with trivial injury and negative evaluation may be discharged with strict return precautions for delayed airway, vascular, or neurologic symptoms. Key pitfalls include underestimating delayed vascular injury, failing to anticipate a difficult airway, and missing associated injuries; preparation for airway deterioration and early specialty involvement are essential.

