- Published on
KembaraXtra-Medicine – Atrial Fibrillation
Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by chaotic atrial electrical activity and ineffective atrial contraction, resulting in an irregularly irregular ventricular rhythm. It develops when structural or electrophysiologic abnormalities of the atria promote abnormal impulse formation or conduction. Ventricular rate depends on atrioventricular (AV) nodal conduction, which is influenced by autonomic tone, medications, and intrinsic AV nodal disease.
AF is classified by the American College of Cardiology (ACC) and American Heart Association (AHA) into paroxysmal AF, which terminates spontaneously or with intervention within seven days; persistent AF, which lasts longer than seven days and includes early persistent AF (7 days to less than 3 months) and long-standing persistent AF (more than 1 year); and permanent AF, in which both patient and clinician decide not to pursue rhythm restoration. Additional clinical categories include lone AF in younger patients without structural heart disease, nonvalvular AF (absence of moderate-to-severe mitral stenosis or mechanical valve), secondary AF due to a reversible precipitating condition, and silent AF detected incidentally on electrocardiography.
The prevalence of AF increases markedly with age and affects more than three million people in the United States. It is more common in men than women and more frequently diagnosed in white populations. Stroke is the most serious complication, with AF conferring a two- to sevenfold increased risk of ischemic stroke. Stroke risk rises substantially with advancing age and comorbidities, independent of whether AF is paroxysmal or persistent.
Clinical presentation varies widely. Patients may experience palpitations, fatigue, dizziness, dyspnea, chest discomfort, or reduced exercise tolerance, while others remain asymptomatic. Physical examination typically reveals an irregularly irregular pulse and heart rhythm. AF may also present with thromboembolic complications such as ischemic stroke or systemic embolism.
The pathophysiology of AF involves atrial fibrosis, loss of atrial muscle mass, and abnormal impulse generation, often originating from the pulmonary veins. Both reentrant and focal mechanisms contribute. Common etiologies include hypertension, valvular heart disease, coronary artery disease, heart failure, cardiomyopathies, pulmonary disorders, hyperthyroidism, obesity, electrolyte disturbances, systemic illness, alcohol use, medications, and postoperative stress.
Diagnosis is confirmed by electrocardiography showing absent P waves, fibrillatory baseline activity, and an irregular ventricular response. Evaluation includes history, physical examination, ECG, transthoracic echocardiography to assess structural heart disease, and laboratory testing to identify secondary causes such as thyroid dysfunction or electrolyte abnormalities. Transesophageal echocardiography is useful to detect left atrial thrombus when cardioversion or ablation is considered.
Management of acute AF depends on hemodynamic stability. Hemodynamically unstable patients require immediate synchronized electrical cardioversion. Stable patients are typically managed initially with rate control using beta-blockers, nondihydropyridine calcium channel blockers, or digoxin in selected cases. Rhythm control with pharmacologic or electrical cardioversion may be considered based on symptoms, duration of AF, and patient preference.
Long-term management involves either rate control or rhythm control strategies, both of which require appropriate anticoagulation to reduce stroke risk. Large trials have shown no significant difference in mortality between rate and rhythm control strategies, although early rhythm control may benefit selected patients. Risk factor modification, including treatment of hypertension, obesity, sleep apnea, and alcohol avoidance, is essential in reducing AF burden.
Stroke prevention is central to AF management. The CHA₂DS₂-VASc score is used to estimate thromboembolic risk and guide anticoagulation decisions. Oral anticoagulation is recommended for patients at moderate to high risk, with direct oral anticoagulants preferred over warfarin in eligible patients. Anticoagulation decisions are independent of AF type and must balance bleeding risk, commonly assessed using the HAS-BLED score.
Nonpharmacologic therapies include catheter ablation, which is effective for symptomatic, drug-refractory AF, particularly paroxysmal AF. Pulmonary vein isolation is the cornerstone of ablation therapy, with high success rates in experienced centers. Surgical approaches such as the Cox-Maze procedure may be used in selected patients, often during concomitant cardiac surgery.
AF is associated with increased mortality, heart failure progression, myocardial infarction, and reduced quality of life. Prognosis depends on underlying heart disease, comorbidities, atrial size, and duration of AF. Referral to a cardiologist or electrophysiologist is recommended when considering antiarrhythmic therapy, catheter ablation, or complex anticoagulation decisions.
Early recognition, appropriate anticoagulation, individualized rate or rhythm control, and aggressive management of risk factors are essential to reducing morbidity and mortality associated with atrial fibrillation.
Atrial fibrillation (AF) is a supraventricular tachyarrhythmia characterized by chaotic atrial electrical activity and ineffective atrial contraction, resulting in an irregularly irregular ventricular rhythm. It develops when structural or electrophysiologic abnormalities of the atria promote abnormal impulse formation or conduction. Ventricular rate depends on atrioventricular (AV) nodal conduction, which is influenced by autonomic tone, medications, and intrinsic AV nodal disease.
AF is classified by the American College of Cardiology (ACC) and American Heart Association (AHA) into paroxysmal AF, which terminates spontaneously or with intervention within seven days; persistent AF, which lasts longer than seven days and includes early persistent AF (7 days to less than 3 months) and long-standing persistent AF (more than 1 year); and permanent AF, in which both patient and clinician decide not to pursue rhythm restoration. Additional clinical categories include lone AF in younger patients without structural heart disease, nonvalvular AF (absence of moderate-to-severe mitral stenosis or mechanical valve), secondary AF due to a reversible precipitating condition, and silent AF detected incidentally on electrocardiography.
The prevalence of AF increases markedly with age and affects more than three million people in the United States. It is more common in men than women and more frequently diagnosed in white populations. Stroke is the most serious complication, with AF conferring a two- to sevenfold increased risk of ischemic stroke. Stroke risk rises substantially with advancing age and comorbidities, independent of whether AF is paroxysmal or persistent.
Clinical presentation varies widely. Patients may experience palpitations, fatigue, dizziness, dyspnea, chest discomfort, or reduced exercise tolerance, while others remain asymptomatic. Physical examination typically reveals an irregularly irregular pulse and heart rhythm. AF may also present with thromboembolic complications such as ischemic stroke or systemic embolism.
The pathophysiology of AF involves atrial fibrosis, loss of atrial muscle mass, and abnormal impulse generation, often originating from the pulmonary veins. Both reentrant and focal mechanisms contribute. Common etiologies include hypertension, valvular heart disease, coronary artery disease, heart failure, cardiomyopathies, pulmonary disorders, hyperthyroidism, obesity, electrolyte disturbances, systemic illness, alcohol use, medications, and postoperative stress.
Diagnosis is confirmed by electrocardiography showing absent P waves, fibrillatory baseline activity, and an irregular ventricular response. Evaluation includes history, physical examination, ECG, transthoracic echocardiography to assess structural heart disease, and laboratory testing to identify secondary causes such as thyroid dysfunction or electrolyte abnormalities. Transesophageal echocardiography is useful to detect left atrial thrombus when cardioversion or ablation is considered.
Management of acute AF depends on hemodynamic stability. Hemodynamically unstable patients require immediate synchronized electrical cardioversion. Stable patients are typically managed initially with rate control using beta-blockers, nondihydropyridine calcium channel blockers, or digoxin in selected cases. Rhythm control with pharmacologic or electrical cardioversion may be considered based on symptoms, duration of AF, and patient preference.
Long-term management involves either rate control or rhythm control strategies, both of which require appropriate anticoagulation to reduce stroke risk. Large trials have shown no significant difference in mortality between rate and rhythm control strategies, although early rhythm control may benefit selected patients. Risk factor modification, including treatment of hypertension, obesity, sleep apnea, and alcohol avoidance, is essential in reducing AF burden.
Stroke prevention is central to AF management. The CHA₂DS₂-VASc score is used to estimate thromboembolic risk and guide anticoagulation decisions. Oral anticoagulation is recommended for patients at moderate to high risk, with direct oral anticoagulants preferred over warfarin in eligible patients. Anticoagulation decisions are independent of AF type and must balance bleeding risk, commonly assessed using the HAS-BLED score.
Nonpharmacologic therapies include catheter ablation, which is effective for symptomatic, drug-refractory AF, particularly paroxysmal AF. Pulmonary vein isolation is the cornerstone of ablation therapy, with high success rates in experienced centers. Surgical approaches such as the Cox-Maze procedure may be used in selected patients, often during concomitant cardiac surgery.
AF is associated with increased mortality, heart failure progression, myocardial infarction, and reduced quality of life. Prognosis depends on underlying heart disease, comorbidities, atrial size, and duration of AF. Referral to a cardiologist or electrophysiologist is recommended when considering antiarrhythmic therapy, catheter ablation, or complex anticoagulation decisions.
Early recognition, appropriate anticoagulation, individualized rate or rhythm control, and aggressive management of risk factors are essential to reducing morbidity and mortality associated with atrial fibrillation.

- Published on
KembaraXtra-Medicine – Atopic Dermatitis (Eczema)
Atopic dermatitis is a chronic inflammatory skin condition characterized by intense itching and recurrent eczematous flares. It is commonly associated with a personal or family history of allergic diseases such as asthma, food allergies, and allergic rhinitis, a constellation referred to as atopy.
The disease typically presents early in life, with many cases beginning within the first year, most often between three and six months of age. Children with widespread atopic dermatitis are at increased risk of later developing asthma and allergic rhinitis, a progression known as the atopic march. Although common in childhood, atopic dermatitis may persist into adulthood or recur after periods of remission.
Clinically, atopic dermatitis evolves through acute, subacute, and chronic phases. Acute disease presents with erythematous papules or plaques that may ooze and crust. Subacute disease is marked by dry, scaly, erythematous lesions, while chronic disease leads to skin thickening and lichenification as a result of repeated scratching. Pruritus is the most prominent and burdensome symptom at all stages.
The distribution of lesions varies with age. In infants and young children, lesions commonly involve the cheeks, face, neck, trunk, and extensor surfaces of the limbs. In older children and adults, the disease predominantly affects flexural areas such as the antecubital and popliteal fossae, with sparing of the groin. In adults, involvement of the hands, especially the dorsal hands and fingers, is particularly common.
Diagnosis is primarily clinical and based on characteristic features including pruritus, typical morphology and distribution, chronic or relapsing course, and a personal or family history of atopy. Minor features such as xerosis, elevated immunoglobulin E levels, and recurrent skin infections may support the diagnosis. Laboratory testing is usually unnecessary, and skin biopsy is reserved for atypical or treatment-resistant cases.
Management centers on restoring and maintaining the skin barrier and controlling inflammation. Daily skin care with regular use of emollients, particularly immediately after bathing, is essential. Baths or showers should be brief and lukewarm, and fragrance-free cleansers and detergents are recommended. Avoidance of known triggers such as heat, sweating, harsh soaps, wool, stress, and environmental allergens is an important preventive strategy.
Topical corticosteroids remain the first-line treatment for disease flares, with potency selected according to disease severity and body site. Low-potency steroids are preferred for the face and intertriginous areas, while medium- to high-potency agents may be used for thicker lesions on the trunk and extremities for limited durations. Topical calcineurin inhibitors serve as steroid-sparing agents, particularly for sensitive areas such as the face and skin folds.
Secondary bacterial skin infections, most commonly due to Staphylococcus aureus, should be treated promptly with appropriate antimicrobial therapy. Antihistamines do not directly treat the itch of atopic dermatitis but may be used at night to promote sleep and reduce scratching. In moderate to severe or refractory cases, phototherapy, systemic immunomodulatory agents, or targeted biologic therapy such as dupilumab may be required under specialist supervision.
The overall prognosis is favorable, with many children experiencing significant improvement or complete resolution by adolescence. However, atopic dermatitis often follows a relapsing and remitting course, and long-term management focuses on symptom control, prevention of flares, and maintenance of quality of life.
Atopic dermatitis is a chronic inflammatory skin condition characterized by intense itching and recurrent eczematous flares. It is commonly associated with a personal or family history of allergic diseases such as asthma, food allergies, and allergic rhinitis, a constellation referred to as atopy.
The disease typically presents early in life, with many cases beginning within the first year, most often between three and six months of age. Children with widespread atopic dermatitis are at increased risk of later developing asthma and allergic rhinitis, a progression known as the atopic march. Although common in childhood, atopic dermatitis may persist into adulthood or recur after periods of remission.
Clinically, atopic dermatitis evolves through acute, subacute, and chronic phases. Acute disease presents with erythematous papules or plaques that may ooze and crust. Subacute disease is marked by dry, scaly, erythematous lesions, while chronic disease leads to skin thickening and lichenification as a result of repeated scratching. Pruritus is the most prominent and burdensome symptom at all stages.
The distribution of lesions varies with age. In infants and young children, lesions commonly involve the cheeks, face, neck, trunk, and extensor surfaces of the limbs. In older children and adults, the disease predominantly affects flexural areas such as the antecubital and popliteal fossae, with sparing of the groin. In adults, involvement of the hands, especially the dorsal hands and fingers, is particularly common.
Diagnosis is primarily clinical and based on characteristic features including pruritus, typical morphology and distribution, chronic or relapsing course, and a personal or family history of atopy. Minor features such as xerosis, elevated immunoglobulin E levels, and recurrent skin infections may support the diagnosis. Laboratory testing is usually unnecessary, and skin biopsy is reserved for atypical or treatment-resistant cases.
Management centers on restoring and maintaining the skin barrier and controlling inflammation. Daily skin care with regular use of emollients, particularly immediately after bathing, is essential. Baths or showers should be brief and lukewarm, and fragrance-free cleansers and detergents are recommended. Avoidance of known triggers such as heat, sweating, harsh soaps, wool, stress, and environmental allergens is an important preventive strategy.
Topical corticosteroids remain the first-line treatment for disease flares, with potency selected according to disease severity and body site. Low-potency steroids are preferred for the face and intertriginous areas, while medium- to high-potency agents may be used for thicker lesions on the trunk and extremities for limited durations. Topical calcineurin inhibitors serve as steroid-sparing agents, particularly for sensitive areas such as the face and skin folds.
Secondary bacterial skin infections, most commonly due to Staphylococcus aureus, should be treated promptly with appropriate antimicrobial therapy. Antihistamines do not directly treat the itch of atopic dermatitis but may be used at night to promote sleep and reduce scratching. In moderate to severe or refractory cases, phototherapy, systemic immunomodulatory agents, or targeted biologic therapy such as dupilumab may be required under specialist supervision.
The overall prognosis is favorable, with many children experiencing significant improvement or complete resolution by adolescence. However, atopic dermatitis often follows a relapsing and remitting course, and long-term management focuses on symptom control, prevention of flares, and maintenance of quality of life.

- Published on
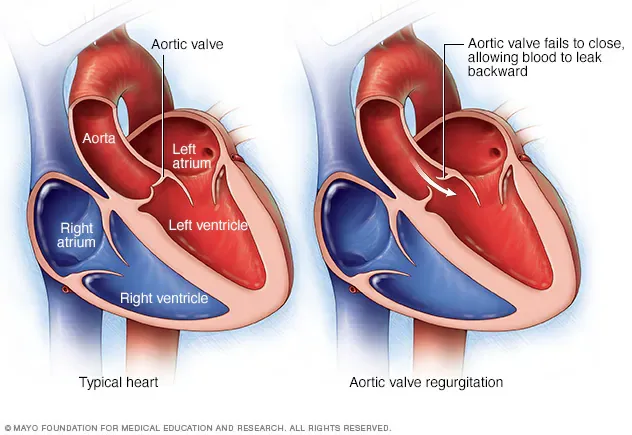
KembaraXtra- Medicine- Aortic Regurgitation
Aortic regurgitation (AR), also known as aortic insufficiency, is a condition characterized by abnormal retrograde flow of blood from the aorta into the left ventricle during diastole due to incomplete closure of the aortic valve. This inadequate valve closure may result from intrinsic disease of the aortic valve leaflets or from pathology involving the aortic root or ascending aorta, such as dilation. Aortic regurgitation may be acute or chronic in nature. Chronic AR is further classified into stages: Stage A refers to patients at risk for AR without even trace regurgitation (for example, those with bicuspid aortic valves, aortic valve sclerosis, aortic root disease, or a history of rheumatic heart disease or infective endocarditis); Stage B includes patients with progressive mild to moderate AR and preserved left ventricular ejection fraction (LVEF); Stage C includes asymptomatic patients with severe AR, subdivided into those with preserved LVEF (C1) and those with reduced LVEF (C2); and Stage D includes patients with symptomatic severe AR.
The epidemiology of AR varies according to severity, age, and sex. Mild AR becomes increasingly common with advancing age, while moderate to severe AR remains less frequent but rises in prevalence among older adults. In developing countries, the most common cause of AR is rheumatic heart disease. In developed countries, aortic root dilation, congenital bicuspid aortic valve, and degenerative calcific valve disease are the predominant causes. Infective endocarditis is the most common cause of acute AR. Other causes include leaflet abnormalities such as trauma with valvular rupture, myxomatous degeneration, drug-induced valve disease (e.g., fenfluramine, dexfenfluramine, pergolide, cabergoline), congenital heart disease (including bicuspid aortic valve and sinus of Valsalva aneurysm), systemic inflammatory or rheumatologic disorders (such as ankylosing spondylitis, rheumatoid arthritis, and systemic lupus erythematosus), and iatrogenic injury (e.g., following aortic balloon valvotomy). Abnormalities of the aortic root or ascending aorta, including annuloaortic ectasia, connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome), trauma, syphilitic aortitis, systemic hypertension, and aortic dissection, are also important etiologies. Postprocedural AR, most often due to paravalvular leak, occurs in a notable proportion of patients after transcatheter aortic valve replacement (TAVR) and is associated with worse outcomes when more than mild.
Clinical presentation depends on whether AR is acute or chronic. Chronic AR is often well tolerated for many years because of compensatory left ventricular dilation and hypertrophy. Symptoms typically appear when left ventricular systolic function deteriorates and include dyspnea on exertion, decreased exercise tolerance, chest pain, syncope, and signs of congestive heart failure. Acute severe AR presents dramatically, often with hypotension, pulmonary edema, and cardiogenic shock, due to the inability of the left ventricle to accommodate the sudden volume overload. In acute AR, the rapid rise in left ventricular diastolic pressure reduces coronary perfusion, further worsening hemodynamics.
Physical examination findings in chronic AR are largely related to increased stroke volume and widened pulse pressure. These include bounding or “water-hammer” pulses (Corrigan pulse), head bobbing with each heartbeat (de Musset sign), loud systolic and diastolic femoral sounds (“pistol-shot” femorals or Traube sign), capillary pulsations of the nail beds or lips (Quincke sign), and a to-and-fro femoral murmur with compression of the femoral artery (Duroziez sign). A significant increase in popliteal systolic pressure compared with brachial pressure (Hill sign) may be present. Historical signs such as uvular pulsation (Mueller sign), retinal arterial pulsations (Becker sign), diastolic blood pressure drop with arm elevation (Mayne sign), hepatic pulsations (Rosenbach sign), splenic pulsations (Gerhard sign), and pupillary changes (Landolfi sign) are neither sensitive nor specific but may be noted. Cardiac auscultation typically reveals a high-pitched, blowing, decrescendo diastolic murmur best heard along the left sternal border, an S3 at the apex, displacement of the apical impulse downward and laterally, and sometimes an Austin Flint murmur, which is a low-pitched apical diastolic rumble related to altered mitral inflow dynamics. In acute AR, these classic peripheral signs are often absent, and a short, soft diastolic murmur may be the only auscultatory finding.
The diagnostic evaluation of AR includes a careful history and physical examination, with particular attention to symptoms of exertional dyspnea, chest pain, syncope, and heart failure. Echocardiography is the cornerstone of diagnosis and is used to confirm AR, determine severity, assess valve anatomy, and evaluate left ventricular size and systolic function. Severity can be assessed qualitatively (e.g., vena contracta width) and quantitatively using effective regurgitant orifice area, regurgitant volume, and regurgitant fraction. Evidence of left ventricular dilation is required for the diagnosis of chronic severe AR. Chest radiography may demonstrate left ventricular enlargement and aortic dilation in chronic AR, while acute AR may show pulmonary edema with a relatively normal cardiac silhouette. Electrocardiography is not diagnostic but often reveals left ventricular hypertrophy in chronic AR and helps assess for associated arrhythmias. When transthoracic echocardiographic images are suboptimal or discordant with clinical findings, transesophageal echocardiography, cardiac magnetic resonance imaging, or cardiac catheterization may be used to further define AR severity, ventricular function, and aortic dimensions.
Management strategies differ between acute and chronic AR. Acute severe AR is a medical and surgical emergency. Definitive treatment is urgent aortic valve replacement or repair. Medical stabilization includes afterload reduction with vasodilators such as nitroprusside and treatment of pulmonary edema with diuretics. Beta-blockers are avoided because they prolong diastole and worsen regurgitation, and intra-aortic balloon pump support is contraindicated. Immediate surgical referral is required in cases of cardiogenic shock.
Chronic AR management depends on symptom status, severity of regurgitation, left ventricular systolic function, and ventricular dimensions. According to ACC/AHA guidelines, aortic valve replacement is indicated for symptomatic patients with severe AR regardless of LVEF and for asymptomatic patients with severe AR and LVEF less than 55%. Surgery is also indicated in patients with severe AR who are undergoing other cardiac surgery. In selected asymptomatic patients with preserved LVEF but significant left ventricular dilation, surgery may be reasonable if surgical risk is low. Medical therapy plays a supportive role and focuses on treating hypertension and heart failure symptoms. ACE inhibitors or angiotensin receptor blockers are recommended for blood pressure control, and diuretics with sodium restriction are used for congestive heart failure. Long-term vasodilator therapy has not consistently been shown to delay surgery in asymptomatic patients with severe AR but is appropriate for concomitant hypertension. Beta-blockers may be considered in patients with symptomatic severe AR or left ventricular dysfunction when surgery is not feasible, and observational studies suggest a potential survival benefit in such cases. For patients with pure aortic insufficiency who are not surgical candidates, TAVR may be considered, although it is associated with higher rates of certain complications compared with surgical valve replacement.
Referral for surgical or advanced cardiac evaluation is indicated in patients with acute severe AR, symptomatic severe AR, evidence of left ventricular systolic dysfunction, or significant ventricular dilation even in the absence of symptoms. With timely intervention and appropriate long-term follow-up, outcomes in patients with chronic AR can be significantly improved, particularly when surgery is performed before irreversible left ventricular dysfunction develops.
Aortic regurgitation (AR), also known as aortic insufficiency, is a condition characterized by abnormal retrograde flow of blood from the aorta into the left ventricle during diastole due to incomplete closure of the aortic valve. This inadequate valve closure may result from intrinsic disease of the aortic valve leaflets or from pathology involving the aortic root or ascending aorta, such as dilation. Aortic regurgitation may be acute or chronic in nature. Chronic AR is further classified into stages: Stage A refers to patients at risk for AR without even trace regurgitation (for example, those with bicuspid aortic valves, aortic valve sclerosis, aortic root disease, or a history of rheumatic heart disease or infective endocarditis); Stage B includes patients with progressive mild to moderate AR and preserved left ventricular ejection fraction (LVEF); Stage C includes asymptomatic patients with severe AR, subdivided into those with preserved LVEF (C1) and those with reduced LVEF (C2); and Stage D includes patients with symptomatic severe AR.
The epidemiology of AR varies according to severity, age, and sex. Mild AR becomes increasingly common with advancing age, while moderate to severe AR remains less frequent but rises in prevalence among older adults. In developing countries, the most common cause of AR is rheumatic heart disease. In developed countries, aortic root dilation, congenital bicuspid aortic valve, and degenerative calcific valve disease are the predominant causes. Infective endocarditis is the most common cause of acute AR. Other causes include leaflet abnormalities such as trauma with valvular rupture, myxomatous degeneration, drug-induced valve disease (e.g., fenfluramine, dexfenfluramine, pergolide, cabergoline), congenital heart disease (including bicuspid aortic valve and sinus of Valsalva aneurysm), systemic inflammatory or rheumatologic disorders (such as ankylosing spondylitis, rheumatoid arthritis, and systemic lupus erythematosus), and iatrogenic injury (e.g., following aortic balloon valvotomy). Abnormalities of the aortic root or ascending aorta, including annuloaortic ectasia, connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome), trauma, syphilitic aortitis, systemic hypertension, and aortic dissection, are also important etiologies. Postprocedural AR, most often due to paravalvular leak, occurs in a notable proportion of patients after transcatheter aortic valve replacement (TAVR) and is associated with worse outcomes when more than mild.
Clinical presentation depends on whether AR is acute or chronic. Chronic AR is often well tolerated for many years because of compensatory left ventricular dilation and hypertrophy. Symptoms typically appear when left ventricular systolic function deteriorates and include dyspnea on exertion, decreased exercise tolerance, chest pain, syncope, and signs of congestive heart failure. Acute severe AR presents dramatically, often with hypotension, pulmonary edema, and cardiogenic shock, due to the inability of the left ventricle to accommodate the sudden volume overload. In acute AR, the rapid rise in left ventricular diastolic pressure reduces coronary perfusion, further worsening hemodynamics.
Physical examination findings in chronic AR are largely related to increased stroke volume and widened pulse pressure. These include bounding or “water-hammer” pulses (Corrigan pulse), head bobbing with each heartbeat (de Musset sign), loud systolic and diastolic femoral sounds (“pistol-shot” femorals or Traube sign), capillary pulsations of the nail beds or lips (Quincke sign), and a to-and-fro femoral murmur with compression of the femoral artery (Duroziez sign). A significant increase in popliteal systolic pressure compared with brachial pressure (Hill sign) may be present. Historical signs such as uvular pulsation (Mueller sign), retinal arterial pulsations (Becker sign), diastolic blood pressure drop with arm elevation (Mayne sign), hepatic pulsations (Rosenbach sign), splenic pulsations (Gerhard sign), and pupillary changes (Landolfi sign) are neither sensitive nor specific but may be noted. Cardiac auscultation typically reveals a high-pitched, blowing, decrescendo diastolic murmur best heard along the left sternal border, an S3 at the apex, displacement of the apical impulse downward and laterally, and sometimes an Austin Flint murmur, which is a low-pitched apical diastolic rumble related to altered mitral inflow dynamics. In acute AR, these classic peripheral signs are often absent, and a short, soft diastolic murmur may be the only auscultatory finding.
The diagnostic evaluation of AR includes a careful history and physical examination, with particular attention to symptoms of exertional dyspnea, chest pain, syncope, and heart failure. Echocardiography is the cornerstone of diagnosis and is used to confirm AR, determine severity, assess valve anatomy, and evaluate left ventricular size and systolic function. Severity can be assessed qualitatively (e.g., vena contracta width) and quantitatively using effective regurgitant orifice area, regurgitant volume, and regurgitant fraction. Evidence of left ventricular dilation is required for the diagnosis of chronic severe AR. Chest radiography may demonstrate left ventricular enlargement and aortic dilation in chronic AR, while acute AR may show pulmonary edema with a relatively normal cardiac silhouette. Electrocardiography is not diagnostic but often reveals left ventricular hypertrophy in chronic AR and helps assess for associated arrhythmias. When transthoracic echocardiographic images are suboptimal or discordant with clinical findings, transesophageal echocardiography, cardiac magnetic resonance imaging, or cardiac catheterization may be used to further define AR severity, ventricular function, and aortic dimensions.
Management strategies differ between acute and chronic AR. Acute severe AR is a medical and surgical emergency. Definitive treatment is urgent aortic valve replacement or repair. Medical stabilization includes afterload reduction with vasodilators such as nitroprusside and treatment of pulmonary edema with diuretics. Beta-blockers are avoided because they prolong diastole and worsen regurgitation, and intra-aortic balloon pump support is contraindicated. Immediate surgical referral is required in cases of cardiogenic shock.
Chronic AR management depends on symptom status, severity of regurgitation, left ventricular systolic function, and ventricular dimensions. According to ACC/AHA guidelines, aortic valve replacement is indicated for symptomatic patients with severe AR regardless of LVEF and for asymptomatic patients with severe AR and LVEF less than 55%. Surgery is also indicated in patients with severe AR who are undergoing other cardiac surgery. In selected asymptomatic patients with preserved LVEF but significant left ventricular dilation, surgery may be reasonable if surgical risk is low. Medical therapy plays a supportive role and focuses on treating hypertension and heart failure symptoms. ACE inhibitors or angiotensin receptor blockers are recommended for blood pressure control, and diuretics with sodium restriction are used for congestive heart failure. Long-term vasodilator therapy has not consistently been shown to delay surgery in asymptomatic patients with severe AR but is appropriate for concomitant hypertension. Beta-blockers may be considered in patients with symptomatic severe AR or left ventricular dysfunction when surgery is not feasible, and observational studies suggest a potential survival benefit in such cases. For patients with pure aortic insufficiency who are not surgical candidates, TAVR may be considered, although it is associated with higher rates of certain complications compared with surgical valve replacement.
Referral for surgical or advanced cardiac evaluation is indicated in patients with acute severe AR, symptomatic severe AR, evidence of left ventricular systolic dysfunction, or significant ventricular dilation even in the absence of symptoms. With timely intervention and appropriate long-term follow-up, outcomes in patients with chronic AR can be significantly improved, particularly when surgery is performed before irreversible left ventricular dysfunction develops.
- Published on
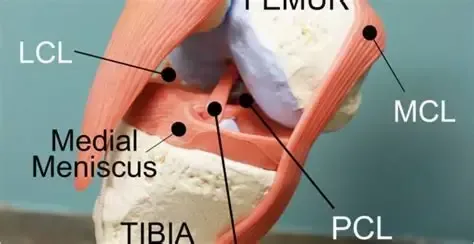
Emergency and Acute Medicine – Knee Injuries: ACL, PCL, MCL, and Meniscus
Basic Description
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
Basic Description
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
- Published on
Emergency And Acute Medicine – Isoniazid Poisoning
Basics Description
Isoniazid (INH) toxicity results from interference with pyridoxine (vitamin B6) metabolism. INH complexes with and inactivates pyridoxal-5-phosphate, the active form of pyridoxine, and inhibits pyridoxine phosphokinase, preventing conversion to its active form. This leads to a net decrease in γ-aminobutyric acid (GABA) production, causing cerebral excitability and seizures. INH also inhibits lactate dehydrogenase, impairing conversion of lactate to pyruvate and contributing to profound anion gap metabolic acidosis. Free effects include mitochondrial dysfunction and impaired oxidative metabolism.
Chronic toxicity interferes with nicotinic acid (niacin) synthesis and may produce a pellagra-like syndrome after months of therapy. INH has some monoamine oxidase inhibitor–like effects, with rare reports of tyramine reactions, mania, depression, obsessive–compulsive symptoms, and psychosis. Pharmacokinetically, INH is rapidly absorbed with peak levels within 1–2 hours. It has a volume of distribution of 0.6 L/kg, low protein binding, hepatic acetylation, and renal excretion within 24 hours. Half-life is less than 1 hour in fast acetylators and 2–4 hours in slow acetylators.
Etiology
High-risk populations include immigrants, individuals experiencing homelessness, people with HIV infection, alcohol use disorder, and those of lower socioeconomic status. Slow acetylators are more prone to chronic toxicity. The estimated LD50 is 80–150 mg/kg. Ingestions less than 1.5 g typically cause mild toxicity, while ingestions of 10 g or more are often fatal.
Diagnosis: Signs and Symptoms
Acute toxicity primarily affects the nervous system and presents with altered mental status, seizures refractory to standard therapy, agitation, coma, dizziness, ataxia, hyperreflexia, slurred speech, hallucinations, and psychosis. Gastrointestinal symptoms include nausea and vomiting. Renal findings may include oliguria or anuria. Cardiovascular manifestations include hypotension, tachycardia, shock, and cyanosis. Metabolically, patients develop profound anion gap metabolic acidosis with elevated lactate and may be hyperthermic.
Chronic toxicity presents with peripheral neuropathy, optic neuritis or atrophy, insomnia, vertigo, psychosis, and features of pellagra. Hepatic involvement may include hepatitis or liver failure, along with anorexia, nausea, vomiting, and constipation.
Essential Workup
In the absence of a clear ingestion history, evaluation should focus on unexplained altered mental status, seizures, and metabolic acidosis.
Diagnosis Tests and Interpretation
Laboratory evaluation typically reveals severe metabolic acidosis on arterial blood gas. Serum chemistries show elevated anion gap acidosis and possible hyperglycemia. CBC may show leukocytosis and eosinophilia in acute toxicity, or agranulocytosis, hemolysis, anemia, and eosinophilia in chronic toxicity. Chest radiography may show evidence of tuberculosis or aspiration pneumonia. CT imaging or lumbar puncture may be required if the history is unclear.
Differential Diagnosis
The differential includes other toxicologic causes such as tricyclic antidepressants, salicylates, theophylline, methanol, ethylene glycol, lithium, carbon monoxide, and cyanide. Non-toxicologic causes include stroke, intracranial hemorrhage or mass, trauma, abscess, hypoglycemia, uremia, and thyrotoxicosis.
Treatment Prehospital
All prescription bottles and medications should be collected and transported with the patient for identification.
Initial Stabilization and Therapy
Initial management prioritizes airway, breathing, and circulation. Supplemental oxygen should be provided, and intubation performed if airway protection is required. Establish IV access, initiate cardiac monitoring, and administer isotonic fluids. For altered mental status, give naloxone, thiamine, and dextrose as indicated.
ED Treatment and Procedures
Pyridoxine (vitamin B6) is the specific antidote for INH toxicity. The goal dose is 1 g of pyridoxine for each gram of INH ingested, administered IV in divided doses every 2–3 minutes. If the amount ingested is unknown, give 5 g IV. Doses may be repeated after 20 minutes for refractory seizures or persistent coma. If IV pyridoxine is unavailable, tablets may be crushed and administered via nasogastric tube.
Seizure control relies on pyridoxine replacement; benzodiazepines are synergistic and should be used as needed. Phenytoin is ineffective and should not be used. After stabilization, gastric decontamination may be considered in life-threatening ingestions presenting within one hour, provided the airway is protected. Activated charcoal may be given at a 10:1 charcoal-to-drug ratio. Hemodialysis is reserved for persistent symptoms despite adequate therapy or in patients with renal insufficiency. Metabolic acidosis usually resolves after seizure control and does not routinely require bicarbonate therapy.
Medication
Supportive medications may include IV dextrose, benzodiazepines such as diazepam or lorazepam for seizures, naloxone if indicated, pyridoxine as the antidote, and thiamine.
Follow-Up Disposition
ICU admission is required for refractory seizures, severe acidosis, coma, or persistent altered mental status. Patients with unclear ingestion history, uncontrolled vomiting, or intentional overdose also require admission and toxicology consultation. Asymptomatic patients may be discharged after at least 6 hours of observation, as symptoms typically develop within 45 minutes to 2 hours.
Follow-Up Recommendations
Psychiatric evaluation is recommended for all intentional ingestions or suicidal patients.
Pearls and Pitfalls
Refractory seizures unresponsive to standard therapy are a key clue to INH poisoning. Severe lactic acidosis in a patient with seizures and altered mental status should raise suspicion for INH toxicity. Pyridoxine dosing should be gram-for-gram relative to INH ingestion, and additional doses may be given if seizures resolve but coma persists. Never paralyze an actively seizing patient without continuous EEG monitoring.
Basics Description
Isoniazid (INH) toxicity results from interference with pyridoxine (vitamin B6) metabolism. INH complexes with and inactivates pyridoxal-5-phosphate, the active form of pyridoxine, and inhibits pyridoxine phosphokinase, preventing conversion to its active form. This leads to a net decrease in γ-aminobutyric acid (GABA) production, causing cerebral excitability and seizures. INH also inhibits lactate dehydrogenase, impairing conversion of lactate to pyruvate and contributing to profound anion gap metabolic acidosis. Free effects include mitochondrial dysfunction and impaired oxidative metabolism.
Chronic toxicity interferes with nicotinic acid (niacin) synthesis and may produce a pellagra-like syndrome after months of therapy. INH has some monoamine oxidase inhibitor–like effects, with rare reports of tyramine reactions, mania, depression, obsessive–compulsive symptoms, and psychosis. Pharmacokinetically, INH is rapidly absorbed with peak levels within 1–2 hours. It has a volume of distribution of 0.6 L/kg, low protein binding, hepatic acetylation, and renal excretion within 24 hours. Half-life is less than 1 hour in fast acetylators and 2–4 hours in slow acetylators.
Etiology
High-risk populations include immigrants, individuals experiencing homelessness, people with HIV infection, alcohol use disorder, and those of lower socioeconomic status. Slow acetylators are more prone to chronic toxicity. The estimated LD50 is 80–150 mg/kg. Ingestions less than 1.5 g typically cause mild toxicity, while ingestions of 10 g or more are often fatal.
Diagnosis: Signs and Symptoms
Acute toxicity primarily affects the nervous system and presents with altered mental status, seizures refractory to standard therapy, agitation, coma, dizziness, ataxia, hyperreflexia, slurred speech, hallucinations, and psychosis. Gastrointestinal symptoms include nausea and vomiting. Renal findings may include oliguria or anuria. Cardiovascular manifestations include hypotension, tachycardia, shock, and cyanosis. Metabolically, patients develop profound anion gap metabolic acidosis with elevated lactate and may be hyperthermic.
Chronic toxicity presents with peripheral neuropathy, optic neuritis or atrophy, insomnia, vertigo, psychosis, and features of pellagra. Hepatic involvement may include hepatitis or liver failure, along with anorexia, nausea, vomiting, and constipation.
Essential Workup
In the absence of a clear ingestion history, evaluation should focus on unexplained altered mental status, seizures, and metabolic acidosis.
Diagnosis Tests and Interpretation
Laboratory evaluation typically reveals severe metabolic acidosis on arterial blood gas. Serum chemistries show elevated anion gap acidosis and possible hyperglycemia. CBC may show leukocytosis and eosinophilia in acute toxicity, or agranulocytosis, hemolysis, anemia, and eosinophilia in chronic toxicity. Chest radiography may show evidence of tuberculosis or aspiration pneumonia. CT imaging or lumbar puncture may be required if the history is unclear.
Differential Diagnosis
The differential includes other toxicologic causes such as tricyclic antidepressants, salicylates, theophylline, methanol, ethylene glycol, lithium, carbon monoxide, and cyanide. Non-toxicologic causes include stroke, intracranial hemorrhage or mass, trauma, abscess, hypoglycemia, uremia, and thyrotoxicosis.
Treatment Prehospital
All prescription bottles and medications should be collected and transported with the patient for identification.
Initial Stabilization and Therapy
Initial management prioritizes airway, breathing, and circulation. Supplemental oxygen should be provided, and intubation performed if airway protection is required. Establish IV access, initiate cardiac monitoring, and administer isotonic fluids. For altered mental status, give naloxone, thiamine, and dextrose as indicated.
ED Treatment and Procedures
Pyridoxine (vitamin B6) is the specific antidote for INH toxicity. The goal dose is 1 g of pyridoxine for each gram of INH ingested, administered IV in divided doses every 2–3 minutes. If the amount ingested is unknown, give 5 g IV. Doses may be repeated after 20 minutes for refractory seizures or persistent coma. If IV pyridoxine is unavailable, tablets may be crushed and administered via nasogastric tube.
Seizure control relies on pyridoxine replacement; benzodiazepines are synergistic and should be used as needed. Phenytoin is ineffective and should not be used. After stabilization, gastric decontamination may be considered in life-threatening ingestions presenting within one hour, provided the airway is protected. Activated charcoal may be given at a 10:1 charcoal-to-drug ratio. Hemodialysis is reserved for persistent symptoms despite adequate therapy or in patients with renal insufficiency. Metabolic acidosis usually resolves after seizure control and does not routinely require bicarbonate therapy.
Medication
Supportive medications may include IV dextrose, benzodiazepines such as diazepam or lorazepam for seizures, naloxone if indicated, pyridoxine as the antidote, and thiamine.
Follow-Up Disposition
ICU admission is required for refractory seizures, severe acidosis, coma, or persistent altered mental status. Patients with unclear ingestion history, uncontrolled vomiting, or intentional overdose also require admission and toxicology consultation. Asymptomatic patients may be discharged after at least 6 hours of observation, as symptoms typically develop within 45 minutes to 2 hours.
Follow-Up Recommendations
Psychiatric evaluation is recommended for all intentional ingestions or suicidal patients.
Pearls and Pitfalls
Refractory seizures unresponsive to standard therapy are a key clue to INH poisoning. Severe lactic acidosis in a patient with seizures and altered mental status should raise suspicion for INH toxicity. Pyridoxine dosing should be gram-for-gram relative to INH ingestion, and additional doses may be given if seizures resolve but coma persists. Never paralyze an actively seizing patient without continuous EEG monitoring.

- Published on
Emergency and Acute Medicine – Isopropanol Poisoning
Basics Description
Isopropanol (isopropyl alcohol) is a potent central nervous system depressant, with effects that are two to three times stronger than ethanol. It is rapidly absorbed after oral ingestion and is metabolized by alcohol dehydrogenase to acetone, which itself is a CNS depressant. Unlike other toxic alcohols, isopropanol is ketogenic but does not usually cause significant metabolic acidosis. Concomitant ethanol ingestion prolongs the half-life of isopropanol but not acetone. Isopropanol has a half-life of approximately 3–16 hours, while acetone persists longer, with a half-life of 7.5–26 hours. Acetone is eliminated through the lungs and kidneys.
Etiology
Isopropanol is a clear, colorless, volatile liquid with a bitter taste and a faint odor of acetone. It is commonly available as a 70% rubbing alcohol solution, sometimes containing blue dye (“blue heaven”) to discourage abuse. It is found in many household and industrial products, including toiletries, disinfectants, window cleaners, paint removers, solvents, jewelry cleaners, detergents, antifreeze, and hand sanitizers. The typical adult patient is a chronic alcoholic who has depleted their ethanol supply and substitutes isopropanol. Systemic toxicity can also occur from dermal absorption or rectal administration.
Diagnosis: Signs and Symptoms
Symptoms usually develop within 30–60 minutes of ingestion. Neurologic manifestations include lethargy, weakness, headache, inebriation, vertigo, ataxia, apnea, and coma. Unlike ethanol, an initial excitation phase is typically absent. Gastrointestinal symptoms are common and include nausea, vomiting, abdominal pain, gastritis, and hematemesis. Cardiovascular findings may include hypotension, tachycardia, myocardial depression, and peripheral vasodilation. Pulmonary effects include respiratory depression and hemorrhagic tracheobronchitis. Dermatologic exposure can cause skin irritation or burns, and ocular exposure leads to irritation and lacrimation.
In children, accidental ingestions are common in those younger than 6 years, and rubbing alcohol sponge baths may cause inhalational toxicity. Pediatric patients are particularly prone to hypoglycemia.
Essential Workup
Diagnosis is supported by a history of ingestion and the presence of an acetone or isopropanol odor on the patient’s breath.
Diagnosis Tests and Interpretation
Laboratory evaluation should include electrolytes, BUN, creatinine, and glucose. Hypoglycemia may be present. Significant acidosis is uncommon unless there is associated hypoperfusion or a coingestant. Acetone can falsely elevate serum creatinine; when acetone levels exceed 40 mg/dL, creatinine may rise approximately 1 mg/dL for every 100 mg/dL of acetone, returning to baseline as acetone is cleared. CBC may show decreased hematocrit in cases of hemorrhagic gastritis. Arterial blood gas analysis typically shows little or no acidosis. Urinalysis and serum testing reveal ketosis.
Serum isopropanol levels correlate with severity, with coma often occurring at levels above 150 mg/dL. Serum osmolarity should be assessed, as an elevated osmolar gap (>10) is common. Each 5.9 mg/dL of isopropanol and 5.5 mg/dL of acetone increases the osmolar gap by approximately 1 mOsm/kg. Chest radiography is indicated if aspiration pneumonia is suspected, and head CT should be considered when altered mental status or head injury is possible.
Differential Diagnosis
The differential diagnosis for CNS depression with an elevated osmolar gap includes ethanol, ethylene glycol, methanol, glycerol, and mannitol.
Treatment Prehospital
All potentially ingested bottles and medications should be located and transported with the patient to the emergency department.
Initial Stabilization and Therapy
Management begins with airway, breathing, and circulation. Airway protection and ventilatory support may be required. Hypotension should initially be treated with IV 0.9% normal saline; vasopressors such as dopamine or norepinephrine may be required if hypotension persists. Patients with significant hemorrhagic gastritis may require packed red blood cell transfusion. Nasogastric tube placement and irrigation may be indicated for hematemesis. Naloxone, thiamine, and dextrose should be administered for altered mental status as indicated.
ED Treatment and Procedures
Treatment is primarily supportive, as there is no specific antidote. Skin and eye exposures should be treated with copious irrigation. Activated charcoal may be considered for coingestants and, in large doses, can adsorb some isopropanol. Ethanol infusion and fomepizole (4-methylpyrazole) are not indicated. Hemodialysis effectively removes both isopropanol and acetone but is rarely required. Indications for dialysis include persistent hemodynamic instability despite fluids and pressors or very high serum levels (>400 mg/dL), which are associated with severe hypotension and prolonged coma.
Medication
Supportive medications may include activated charcoal, IV dextrose for hypoglycemia, dopamine for refractory hypotension, naloxone if opioid exposure is suspected, and thiamine for patients at risk of deficiency.
Follow-Up Disposition
Patients with moderate to severe toxicity, including altered mental status or hypotension, should be admitted. Asymptomatic patients should be observed for 2–4 hours after ingestion before discharge. Mild intoxication that resolves within 4–6 hours may be safely discharged.
Follow-Up Recommendations
Patients with intentional ingestion should be referred for alcohol detoxification or psychiatric evaluation. Gastroenterology referral is recommended for those with recurrent hematemesis requiring endoscopic evaluation.
Pearls and Pitfalls
Supportive care is the cornerstone of treatment for isopropanol poisoning. Unlike other toxic alcohol ingestions, ethanol infusion and fomepizole should not be used.
Basics Description
Isopropanol (isopropyl alcohol) is a potent central nervous system depressant, with effects that are two to three times stronger than ethanol. It is rapidly absorbed after oral ingestion and is metabolized by alcohol dehydrogenase to acetone, which itself is a CNS depressant. Unlike other toxic alcohols, isopropanol is ketogenic but does not usually cause significant metabolic acidosis. Concomitant ethanol ingestion prolongs the half-life of isopropanol but not acetone. Isopropanol has a half-life of approximately 3–16 hours, while acetone persists longer, with a half-life of 7.5–26 hours. Acetone is eliminated through the lungs and kidneys.
Etiology
Isopropanol is a clear, colorless, volatile liquid with a bitter taste and a faint odor of acetone. It is commonly available as a 70% rubbing alcohol solution, sometimes containing blue dye (“blue heaven”) to discourage abuse. It is found in many household and industrial products, including toiletries, disinfectants, window cleaners, paint removers, solvents, jewelry cleaners, detergents, antifreeze, and hand sanitizers. The typical adult patient is a chronic alcoholic who has depleted their ethanol supply and substitutes isopropanol. Systemic toxicity can also occur from dermal absorption or rectal administration.
Diagnosis: Signs and Symptoms
Symptoms usually develop within 30–60 minutes of ingestion. Neurologic manifestations include lethargy, weakness, headache, inebriation, vertigo, ataxia, apnea, and coma. Unlike ethanol, an initial excitation phase is typically absent. Gastrointestinal symptoms are common and include nausea, vomiting, abdominal pain, gastritis, and hematemesis. Cardiovascular findings may include hypotension, tachycardia, myocardial depression, and peripheral vasodilation. Pulmonary effects include respiratory depression and hemorrhagic tracheobronchitis. Dermatologic exposure can cause skin irritation or burns, and ocular exposure leads to irritation and lacrimation.
In children, accidental ingestions are common in those younger than 6 years, and rubbing alcohol sponge baths may cause inhalational toxicity. Pediatric patients are particularly prone to hypoglycemia.
Essential Workup
Diagnosis is supported by a history of ingestion and the presence of an acetone or isopropanol odor on the patient’s breath.
Diagnosis Tests and Interpretation
Laboratory evaluation should include electrolytes, BUN, creatinine, and glucose. Hypoglycemia may be present. Significant acidosis is uncommon unless there is associated hypoperfusion or a coingestant. Acetone can falsely elevate serum creatinine; when acetone levels exceed 40 mg/dL, creatinine may rise approximately 1 mg/dL for every 100 mg/dL of acetone, returning to baseline as acetone is cleared. CBC may show decreased hematocrit in cases of hemorrhagic gastritis. Arterial blood gas analysis typically shows little or no acidosis. Urinalysis and serum testing reveal ketosis.
Serum isopropanol levels correlate with severity, with coma often occurring at levels above 150 mg/dL. Serum osmolarity should be assessed, as an elevated osmolar gap (>10) is common. Each 5.9 mg/dL of isopropanol and 5.5 mg/dL of acetone increases the osmolar gap by approximately 1 mOsm/kg. Chest radiography is indicated if aspiration pneumonia is suspected, and head CT should be considered when altered mental status or head injury is possible.
Differential Diagnosis
The differential diagnosis for CNS depression with an elevated osmolar gap includes ethanol, ethylene glycol, methanol, glycerol, and mannitol.
Treatment Prehospital
All potentially ingested bottles and medications should be located and transported with the patient to the emergency department.
Initial Stabilization and Therapy
Management begins with airway, breathing, and circulation. Airway protection and ventilatory support may be required. Hypotension should initially be treated with IV 0.9% normal saline; vasopressors such as dopamine or norepinephrine may be required if hypotension persists. Patients with significant hemorrhagic gastritis may require packed red blood cell transfusion. Nasogastric tube placement and irrigation may be indicated for hematemesis. Naloxone, thiamine, and dextrose should be administered for altered mental status as indicated.
ED Treatment and Procedures
Treatment is primarily supportive, as there is no specific antidote. Skin and eye exposures should be treated with copious irrigation. Activated charcoal may be considered for coingestants and, in large doses, can adsorb some isopropanol. Ethanol infusion and fomepizole (4-methylpyrazole) are not indicated. Hemodialysis effectively removes both isopropanol and acetone but is rarely required. Indications for dialysis include persistent hemodynamic instability despite fluids and pressors or very high serum levels (>400 mg/dL), which are associated with severe hypotension and prolonged coma.
Medication
Supportive medications may include activated charcoal, IV dextrose for hypoglycemia, dopamine for refractory hypotension, naloxone if opioid exposure is suspected, and thiamine for patients at risk of deficiency.
Follow-Up Disposition
Patients with moderate to severe toxicity, including altered mental status or hypotension, should be admitted. Asymptomatic patients should be observed for 2–4 hours after ingestion before discharge. Mild intoxication that resolves within 4–6 hours may be safely discharged.
Follow-Up Recommendations
Patients with intentional ingestion should be referred for alcohol detoxification or psychiatric evaluation. Gastroenterology referral is recommended for those with recurrent hematemesis requiring endoscopic evaluation.
Pearls and Pitfalls
Supportive care is the cornerstone of treatment for isopropanol poisoning. Unlike other toxic alcohol ingestions, ethanol infusion and fomepizole should not be used.
- Published on
Emergency and Acute Medicine – Laryngitis
Basic description
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
Basic description
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
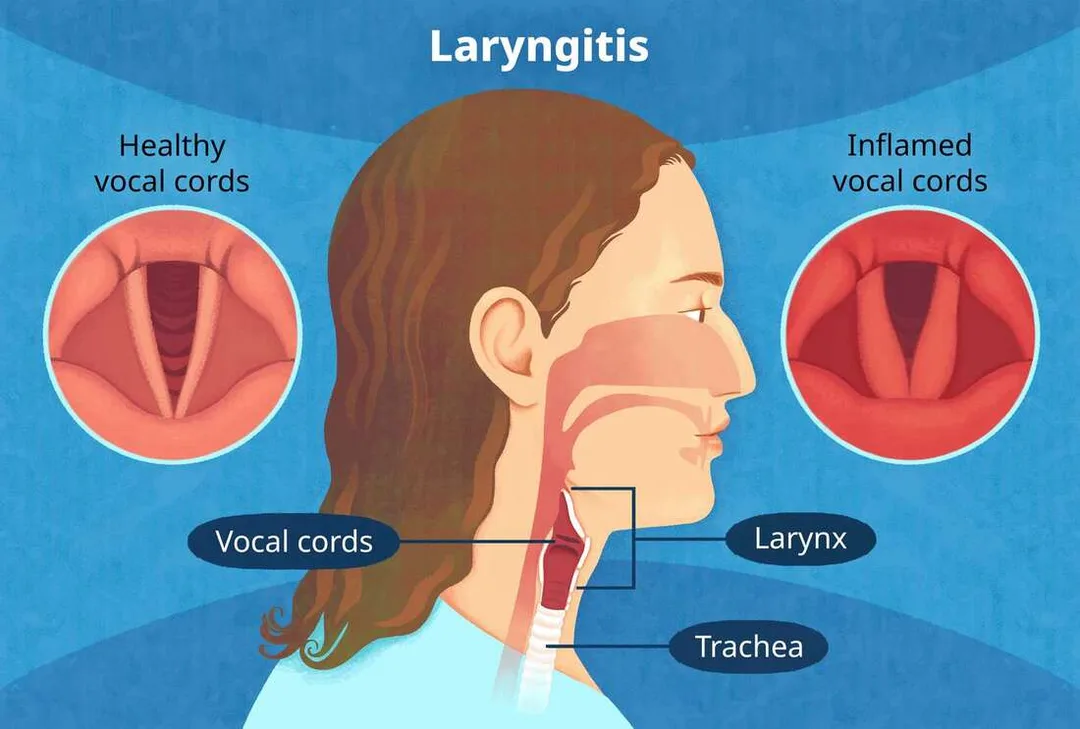
- Published on
KembaraXtra-Medicine – Aortic Coarctation
Coarctation of the aorta (CoA) is a congenital narrowing of the aorta, most commonly located near the ligamentum arteriosum just distal to the origin of the left subclavian artery. The narrowing may be preductal, juxtaductal, or postductal, depending on its relationship to the ductus arteriosus. This obstruction increases afterload on the left ventricle, leading to left ventricular hypertrophy and, in severe cases, heart failure. The stenosis may be discrete or long-segment and is often accompanied by the development of collateral circulation. Although CoA can occur in isolation, it is frequently associated with other congenital cardiac abnormalities, particularly bicuspid aortic valve, as well as mitral valve disease, patent ductus arteriosus, and atrial or ventricular septal defects.
Aortic coarctation occurs in approximately 4 per 10,000 live births and accounts for 4% to 8% of all congenital heart defects. It predominantly affects males, with a male-to-female ratio of about 1.5:1. The exact cause is not fully understood, but both genetic and environmental factors are implicated. Maternal exposure to alcohol, drugs, radiation, or infections such as rubella may contribute. While most cases are sporadic, genetic associations have been identified, including mutations in the NOTCH1 gene. CoA is strongly associated with certain genetic syndromes, most notably Turner syndrome, in which 10% to 15% of affected females have coarctation and an increased risk of aortic complications.
Clinical presentation varies with age, severity of narrowing, and adequacy of collateral circulation. Neonates with mild coarctation or a patent ductus arteriosus may be asymptomatic, whereas those with severe narrowing can present with heart failure or cardiogenic shock when the ductus closes. Symptoms in infants may include poor feeding, diaphoresis, dyspnea, pallor, and weak or absent femoral pulses. Beyond infancy, many patients remain asymptomatic, and the condition may be detected incidentally. When symptoms occur, they are often related to upper extremity hypertension and include headaches, epistaxis, dizziness, heart failure symptoms, claudication of the lower extremities, or abdominal angina.
Characteristic physical findings include diminished or delayed femoral pulses compared with brachial pulses, known as brachial–femoral delay. Upper extremity systolic hypertension with low or unobtainable blood pressure in the lower extremities is typical. A systolic ejection murmur is often heard at the left upper sternal border or over the left subscapular area, and a continuous murmur may be present if extensive collateral vessels have developed. Additional murmurs may reflect associated cardiac defects such as a bicuspid aortic valve.
The pathophysiology of CoA involves abnormal development of the aortic wall, with theories suggesting reduced intrauterine blood flow or abnormal extension of ductal tissue into the aorta. Structural abnormalities such as cystic medial necrosis, intimal hyperplasia, increased collagen content, and reduced smooth muscle contribute to arterial stiffness. The obstruction increases left ventricular afterload, resulting in compensatory hypertrophy and collateral vessel formation, while reducing perfusion to the lower body.
Diagnosis relies on careful clinical examination and imaging. Measurement of blood pressure in all four extremities and simultaneous palpation of brachial and femoral pulses are essential. Electrocardiography may show left ventricular hypertrophy. Transthoracic echocardiography is the initial imaging modality and can establish the diagnosis and assess severity, associated defects, and ventricular function. Cross-sectional imaging with cardiac MRI or CT is recommended in all patients for detailed evaluation of the thoracic aorta, collateral vessels, and associated anomalies, and for long-term surveillance after repair. Cardiac catheterization is reserved for cases requiring hemodynamic assessment or therapeutic intervention.
Management depends on age, anatomy, and severity. Critically ill neonates require stabilization with prostaglandin E1 to maintain ductal patency and inotropic support if needed, followed by definitive repair. Surgical correction is preferred in neonates and young children, with excellent outcomes when performed early. In older children and adults, transcatheter balloon angioplasty with stent placement is often the treatment of choice, particularly for native or recurrent coarctation. Covered stents are favored due to lower complication rates. Long-term management focuses on controlling systemic hypertension, which frequently persists even after successful repair, and on lifelong surveillance for complications such as recoarctation, aneurysm formation, and intracranial aneurysms.
Women with aortic coarctation require specialized counseling before pregnancy. Pregnancy is generally well tolerated in those with successful repair and no residual disease, but unrepaired or residual coarctation, uncontrolled hypertension, or aortic aneurysms significantly increase maternal and fetal risk. All patients with CoA, whether repaired or unrepaired, should receive lifelong follow-up with a congenital heart disease specialist, as systemic hypertension and vascular complications remain major long-term concerns.
Coarctation of the aorta (CoA) is a congenital narrowing of the aorta, most commonly located near the ligamentum arteriosum just distal to the origin of the left subclavian artery. The narrowing may be preductal, juxtaductal, or postductal, depending on its relationship to the ductus arteriosus. This obstruction increases afterload on the left ventricle, leading to left ventricular hypertrophy and, in severe cases, heart failure. The stenosis may be discrete or long-segment and is often accompanied by the development of collateral circulation. Although CoA can occur in isolation, it is frequently associated with other congenital cardiac abnormalities, particularly bicuspid aortic valve, as well as mitral valve disease, patent ductus arteriosus, and atrial or ventricular septal defects.
Aortic coarctation occurs in approximately 4 per 10,000 live births and accounts for 4% to 8% of all congenital heart defects. It predominantly affects males, with a male-to-female ratio of about 1.5:1. The exact cause is not fully understood, but both genetic and environmental factors are implicated. Maternal exposure to alcohol, drugs, radiation, or infections such as rubella may contribute. While most cases are sporadic, genetic associations have been identified, including mutations in the NOTCH1 gene. CoA is strongly associated with certain genetic syndromes, most notably Turner syndrome, in which 10% to 15% of affected females have coarctation and an increased risk of aortic complications.
Clinical presentation varies with age, severity of narrowing, and adequacy of collateral circulation. Neonates with mild coarctation or a patent ductus arteriosus may be asymptomatic, whereas those with severe narrowing can present with heart failure or cardiogenic shock when the ductus closes. Symptoms in infants may include poor feeding, diaphoresis, dyspnea, pallor, and weak or absent femoral pulses. Beyond infancy, many patients remain asymptomatic, and the condition may be detected incidentally. When symptoms occur, they are often related to upper extremity hypertension and include headaches, epistaxis, dizziness, heart failure symptoms, claudication of the lower extremities, or abdominal angina.
Characteristic physical findings include diminished or delayed femoral pulses compared with brachial pulses, known as brachial–femoral delay. Upper extremity systolic hypertension with low or unobtainable blood pressure in the lower extremities is typical. A systolic ejection murmur is often heard at the left upper sternal border or over the left subscapular area, and a continuous murmur may be present if extensive collateral vessels have developed. Additional murmurs may reflect associated cardiac defects such as a bicuspid aortic valve.
The pathophysiology of CoA involves abnormal development of the aortic wall, with theories suggesting reduced intrauterine blood flow or abnormal extension of ductal tissue into the aorta. Structural abnormalities such as cystic medial necrosis, intimal hyperplasia, increased collagen content, and reduced smooth muscle contribute to arterial stiffness. The obstruction increases left ventricular afterload, resulting in compensatory hypertrophy and collateral vessel formation, while reducing perfusion to the lower body.
Diagnosis relies on careful clinical examination and imaging. Measurement of blood pressure in all four extremities and simultaneous palpation of brachial and femoral pulses are essential. Electrocardiography may show left ventricular hypertrophy. Transthoracic echocardiography is the initial imaging modality and can establish the diagnosis and assess severity, associated defects, and ventricular function. Cross-sectional imaging with cardiac MRI or CT is recommended in all patients for detailed evaluation of the thoracic aorta, collateral vessels, and associated anomalies, and for long-term surveillance after repair. Cardiac catheterization is reserved for cases requiring hemodynamic assessment or therapeutic intervention.
Management depends on age, anatomy, and severity. Critically ill neonates require stabilization with prostaglandin E1 to maintain ductal patency and inotropic support if needed, followed by definitive repair. Surgical correction is preferred in neonates and young children, with excellent outcomes when performed early. In older children and adults, transcatheter balloon angioplasty with stent placement is often the treatment of choice, particularly for native or recurrent coarctation. Covered stents are favored due to lower complication rates. Long-term management focuses on controlling systemic hypertension, which frequently persists even after successful repair, and on lifelong surveillance for complications such as recoarctation, aneurysm formation, and intracranial aneurysms.
Women with aortic coarctation require specialized counseling before pregnancy. Pregnancy is generally well tolerated in those with successful repair and no residual disease, but unrepaired or residual coarctation, uncontrolled hypertension, or aortic aneurysms significantly increase maternal and fetal risk. All patients with CoA, whether repaired or unrepaired, should receive lifelong follow-up with a congenital heart disease specialist, as systemic hypertension and vascular complications remain major long-term concerns.

- Published on
Emergency and Acute Medicine – Laceration ManagementBasic description
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.
- Published on
Emergency and Acute Medicine – Larynx Fracture
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.