- Published on
KembaraXtra-Medicine- Anterior Cutaneous Nerve Entrapment Syndrome (ACNES)
Definition
Anterior cutaneous nerve entrapment syndrome (ACNES) is a pain disorder caused by entrapment of the cutaneous branches of the lower thoracoabdominal intercostal nerves (T8–T12) at the lateral border of the rectus abdominis muscle. As these nerves travel between the internal oblique and transversus abdominis muscles and then make a sharp turn to enter the rectus sheath, they become vulnerable to compression. Muscle contraction can further exacerbate this compression, resulting in sharp, localized abdominal wall pain that may radiate along the affected nerve on the same side of the abdomen. The pain is typically reproducible with palpation, and a positive Carnett sign supports the diagnosis. ACNES is frequently underdiagnosed or misdiagnosed.
Synonyms
ACNES.
ICD-10 Codes
G54.9 — Nerve root and plexus disorder, unspecified
G54.3 — Thoracic root disorders, not elsewhere classified
G58.0 — Intercostal neuropathy
G58.9 — Mononeuropathy, unspecified
Epidemiology and Demographics
ACNES accounts for approximately 2% of emergency department presentations with acute abdominal pain and may explain 15% to 30% of chronic abdominal pain cases, depending on diagnostic criteria. In adolescents, it has been identified in up to one in eight cases of acute abdominal pain. Females are affected more often than males, with a ratio of approximately 4:1. The median age of onset is between 40 and 50 years, with peak incidence in the third decade of life.
Risk Factors
Obesity is a recognized risk factor.
Clinical Presentation and Physical Findings
Patients typically report chronic, well-localized abdominal wall pain with a small (<2 cm²) point of maximal tenderness, often along the lateral edge rectus abdominis sheath, most commonly on right side. pain persists for at least one month and is aggravated by activities that tense abdominal muscles, such as standing, stretching, coughing, or sit-ups. carnett test positive, with remaining same worsening when muscles are tensed. additional findings may include a positive skin pinch test, altered sensation to light touch cold (hypoesthesia, hyperesthesia, hyperalgesia, allodynia), normal laboratory results, negative imaging studies, temporary relief following local anesthetic injection tender point.< />pan>
Etiology
The precise cause is often unclear. ACNES has been reported following laparoscopic abdominal surgery, trauma, pregnancy, infectious processes, or visceral events, suggesting that local nerve irritation or mechanical stress may precipitate symptoms.
Diagnosis
Diagnosis is clinical and supported by localized abdominal wall tenderness that worsens with muscle tensing, sensory changes over the painful area, exclusion of intra-abdominal pathology, and prompt pain relief after local anesthetic injection.
Differential Diagnosis
Consider other causes of localized abdominal pain, including visceral pathology, hernias, musculoskeletal disorders, and neuropathic pain syndromes.
Laboratory and Imaging Studies
Laboratory tests are typically normal and show no evidence of infection or inflammation. Imaging studies are used only to exclude other causes of abdominal pain based on clinical judgment and patient acuity.
Treatment
Initial management includes avoiding activities that excessively tense the abdominal muscles. First-line therapy is a trigger-point injection with local anesthetic, with or without a glucocorticoid. A repeat injection is commonly performed about one month later if symptoms recur. If multiple injections fail to provide sustained relief, chemical neurolysis may be considered.
Disposition and Follow-Up
Patients are typically managed on an outpatient basis and should return after one month for reassessment and possible repeat injection.
Complementary and Alternative Therapies
Nonsteroidal antiinflammatory drugs and tricyclic antidepressants may help with pain control, although they have not been specifically studied for ACNES.
Referral
If pain persists despite repeated trigger-point injections, referral for surgical management, chemical neurolysis, or reevaluation for alternative diagnoses is recommended.
Definition
Anterior cutaneous nerve entrapment syndrome (ACNES) is a pain disorder caused by entrapment of the cutaneous branches of the lower thoracoabdominal intercostal nerves (T8–T12) at the lateral border of the rectus abdominis muscle. As these nerves travel between the internal oblique and transversus abdominis muscles and then make a sharp turn to enter the rectus sheath, they become vulnerable to compression. Muscle contraction can further exacerbate this compression, resulting in sharp, localized abdominal wall pain that may radiate along the affected nerve on the same side of the abdomen. The pain is typically reproducible with palpation, and a positive Carnett sign supports the diagnosis. ACNES is frequently underdiagnosed or misdiagnosed.
Synonyms
ACNES.
ICD-10 Codes
G54.9 — Nerve root and plexus disorder, unspecified
G54.3 — Thoracic root disorders, not elsewhere classified
G58.0 — Intercostal neuropathy
G58.9 — Mononeuropathy, unspecified
Epidemiology and Demographics
ACNES accounts for approximately 2% of emergency department presentations with acute abdominal pain and may explain 15% to 30% of chronic abdominal pain cases, depending on diagnostic criteria. In adolescents, it has been identified in up to one in eight cases of acute abdominal pain. Females are affected more often than males, with a ratio of approximately 4:1. The median age of onset is between 40 and 50 years, with peak incidence in the third decade of life.
Risk Factors
Obesity is a recognized risk factor.
Clinical Presentation and Physical Findings
Patients typically report chronic, well-localized abdominal wall pain with a small (<2 cm²) point of maximal tenderness, often along the lateral edge rectus abdominis sheath, most commonly on right side. pain persists for at least one month and is aggravated by activities that tense abdominal muscles, such as standing, stretching, coughing, or sit-ups. carnett test positive, with remaining same worsening when muscles are tensed. additional findings may include a positive skin pinch test, altered sensation to light touch cold (hypoesthesia, hyperesthesia, hyperalgesia, allodynia), normal laboratory results, negative imaging studies, temporary relief following local anesthetic injection tender point.< />pan>
Etiology
The precise cause is often unclear. ACNES has been reported following laparoscopic abdominal surgery, trauma, pregnancy, infectious processes, or visceral events, suggesting that local nerve irritation or mechanical stress may precipitate symptoms.
Diagnosis
Diagnosis is clinical and supported by localized abdominal wall tenderness that worsens with muscle tensing, sensory changes over the painful area, exclusion of intra-abdominal pathology, and prompt pain relief after local anesthetic injection.
Differential Diagnosis
Consider other causes of localized abdominal pain, including visceral pathology, hernias, musculoskeletal disorders, and neuropathic pain syndromes.
Laboratory and Imaging Studies
Laboratory tests are typically normal and show no evidence of infection or inflammation. Imaging studies are used only to exclude other causes of abdominal pain based on clinical judgment and patient acuity.
Treatment
Initial management includes avoiding activities that excessively tense the abdominal muscles. First-line therapy is a trigger-point injection with local anesthetic, with or without a glucocorticoid. A repeat injection is commonly performed about one month later if symptoms recur. If multiple injections fail to provide sustained relief, chemical neurolysis may be considered.
Disposition and Follow-Up
Patients are typically managed on an outpatient basis and should return after one month for reassessment and possible repeat injection.
Complementary and Alternative Therapies
Nonsteroidal antiinflammatory drugs and tricyclic antidepressants may help with pain control, although they have not been specifically studied for ACNES.
Referral
If pain persists despite repeated trigger-point injections, referral for surgical management, chemical neurolysis, or reevaluation for alternative diagnoses is recommended.

- Published on
KembaraXtra-Medicine — Antiphospholipid Antibody Syndrome
Antiphospholipid antibody syndrome (APS) is the most common acquired thrombophilia and is defined by the occurrence of arterial or venous thrombosis and/or characteristic pregnancy morbidity in the presence of persistent antiphospholipid antibodies. These antibodies are directed against anionic phospholipids or phospholipid-binding protein cofactors and promote a hypercoagulable state by stimulating procoagulant pathways while inhibiting fibrinolysis. This process activates downstream mechanisms including mTOR upregulation, Toll-like receptor signaling, and activation of endothelial cells, monocytes, neutrophils, platelets, complement, and proinflammatory cytokines.
Three major antiphospholipid antibodies have been identified: anticardiolipin antibodies, lupus anticoagulant, and anti–β2-glycoprotein I antibodies. APS may occur as a primary disorder or secondary to rheumatologic disease, most commonly systemic lupus erythematosus. The syndrome can affect virtually all organ systems and is associated with venous and arterial thrombosis, recurrent fetal loss, and hematologic abnormalities such as thrombocytopenia and microangiopathic hemolytic anemia.
Antiphospholipid antibodies may be detected in up to 5% of healthy individuals, though only a subset develop clinical APS. These antibodies are found with increased frequency in patients with stroke, myocardial infarction, deep vein thrombosis, and pregnancy complications. APS most commonly affects young to middle-aged adults. Thrombotic risk is increased in the presence of autoimmune disease and is further amplified by acquired risk factors such as pregnancy, oral contraceptive use, smoking, malignancy, prolonged immobilization, and hyperlipidemia. Long-term prognosis is generally favorable with treatment, with high survival rates and improved pregnancy outcomes, although complications such as prematurity and fetal growth restriction remain common.
There are no pathognomonic physical findings in APS. Clinical manifestations are highly variable and reflect thrombotic involvement of multiple organ systems. Venous thrombosis is the most common presentation, particularly deep vein thrombosis of the lower extremities, though thrombosis may occur in atypical venous sites. Arterial thrombosis most frequently affects cerebral vessels, leading to stroke or transient ischemic attack, but may also involve coronary, renal, mesenteric, or peripheral arteries. Recurrent thrombosis is a hallmark feature of APS.
Other commonly involved systems include the pulmonary system, with pulmonary embolism and pulmonary hypertension; the cardiovascular system, with valvular disease, myocardial infarction, and intracardiac thrombosis; the gastrointestinal system, with ischemic abdominal pain and organ infarction; and the renal system, with hypertension, infarction, and glomerular disease. Cutaneous findings such as livedo reticularis, skin necrosis, and digital gangrene may be present. Obstetric manifestations include recurrent miscarriage, fetal death, preeclampsia, placental insufficiency, and premature delivery.
A rare but severe manifestation is catastrophic antiphospholipid syndrome, characterized by rapid development of widespread small-vessel thrombosis involving three or more organs within a short period. This condition carries a high mortality rate and requires prompt recognition and aggressive treatment.
Diagnosis of APS requires fulfillment of at least one clinical criterion and one laboratory criterion. Clinical criteria include objectively confirmed arterial, venous, or small-vessel thrombosis, or defined pregnancy morbidity. Laboratory criteria require persistent positivity of lupus anticoagulant, anticardiolipin antibodies, or anti–β2-glycoprotein I antibodies on two occasions at least 12 weeks apart. Evaluation should also exclude inherited and acquired hypercoagulable states and alternative causes of pregnancy loss.
Management of APS centers on anticoagulation. Acute thrombotic events are treated initially with unfractionated or low-molecular-weight heparin, followed by long-term vitamin K antagonist therapy such as warfarin. Standard-intensity anticoagulation is preferred for venous thrombosis, while arterial events may require combined anticoagulant and antiplatelet therapy. Direct oral anticoagulants are not recommended in high-risk APS, particularly in patients with triple-positive antibody profiles, due to increased rates of recurrent thrombosis.
In pregnancy, warfarin is contraindicated because of teratogenicity. Women with APS and pregnancy morbidity are treated with low-dose aspirin combined with unfractionated or low-molecular-weight heparin to improve pregnancy outcomes. Long-term anticoagulation is often required indefinitely because of the high risk of recurrence. Referral to hematology, rheumatology, and obstetric specialists is recommended for comprehensive management and long-term follow-up.
Antiphospholipid antibody syndrome (APS) is the most common acquired thrombophilia and is defined by the occurrence of arterial or venous thrombosis and/or characteristic pregnancy morbidity in the presence of persistent antiphospholipid antibodies. These antibodies are directed against anionic phospholipids or phospholipid-binding protein cofactors and promote a hypercoagulable state by stimulating procoagulant pathways while inhibiting fibrinolysis. This process activates downstream mechanisms including mTOR upregulation, Toll-like receptor signaling, and activation of endothelial cells, monocytes, neutrophils, platelets, complement, and proinflammatory cytokines.
Three major antiphospholipid antibodies have been identified: anticardiolipin antibodies, lupus anticoagulant, and anti–β2-glycoprotein I antibodies. APS may occur as a primary disorder or secondary to rheumatologic disease, most commonly systemic lupus erythematosus. The syndrome can affect virtually all organ systems and is associated with venous and arterial thrombosis, recurrent fetal loss, and hematologic abnormalities such as thrombocytopenia and microangiopathic hemolytic anemia.
Antiphospholipid antibodies may be detected in up to 5% of healthy individuals, though only a subset develop clinical APS. These antibodies are found with increased frequency in patients with stroke, myocardial infarction, deep vein thrombosis, and pregnancy complications. APS most commonly affects young to middle-aged adults. Thrombotic risk is increased in the presence of autoimmune disease and is further amplified by acquired risk factors such as pregnancy, oral contraceptive use, smoking, malignancy, prolonged immobilization, and hyperlipidemia. Long-term prognosis is generally favorable with treatment, with high survival rates and improved pregnancy outcomes, although complications such as prematurity and fetal growth restriction remain common.
There are no pathognomonic physical findings in APS. Clinical manifestations are highly variable and reflect thrombotic involvement of multiple organ systems. Venous thrombosis is the most common presentation, particularly deep vein thrombosis of the lower extremities, though thrombosis may occur in atypical venous sites. Arterial thrombosis most frequently affects cerebral vessels, leading to stroke or transient ischemic attack, but may also involve coronary, renal, mesenteric, or peripheral arteries. Recurrent thrombosis is a hallmark feature of APS.
Other commonly involved systems include the pulmonary system, with pulmonary embolism and pulmonary hypertension; the cardiovascular system, with valvular disease, myocardial infarction, and intracardiac thrombosis; the gastrointestinal system, with ischemic abdominal pain and organ infarction; and the renal system, with hypertension, infarction, and glomerular disease. Cutaneous findings such as livedo reticularis, skin necrosis, and digital gangrene may be present. Obstetric manifestations include recurrent miscarriage, fetal death, preeclampsia, placental insufficiency, and premature delivery.
A rare but severe manifestation is catastrophic antiphospholipid syndrome, characterized by rapid development of widespread small-vessel thrombosis involving three or more organs within a short period. This condition carries a high mortality rate and requires prompt recognition and aggressive treatment.
Diagnosis of APS requires fulfillment of at least one clinical criterion and one laboratory criterion. Clinical criteria include objectively confirmed arterial, venous, or small-vessel thrombosis, or defined pregnancy morbidity. Laboratory criteria require persistent positivity of lupus anticoagulant, anticardiolipin antibodies, or anti–β2-glycoprotein I antibodies on two occasions at least 12 weeks apart. Evaluation should also exclude inherited and acquired hypercoagulable states and alternative causes of pregnancy loss.
Management of APS centers on anticoagulation. Acute thrombotic events are treated initially with unfractionated or low-molecular-weight heparin, followed by long-term vitamin K antagonist therapy such as warfarin. Standard-intensity anticoagulation is preferred for venous thrombosis, while arterial events may require combined anticoagulant and antiplatelet therapy. Direct oral anticoagulants are not recommended in high-risk APS, particularly in patients with triple-positive antibody profiles, due to increased rates of recurrent thrombosis.
In pregnancy, warfarin is contraindicated because of teratogenicity. Women with APS and pregnancy morbidity are treated with low-dose aspirin combined with unfractionated or low-molecular-weight heparin to improve pregnancy outcomes. Long-term anticoagulation is often required indefinitely because of the high risk of recurrence. Referral to hematology, rheumatology, and obstetric specialists is recommended for comprehensive management and long-term follow-up.

- Published on
KembaraXtra-Medicine – Anxiety (Generalized Anxiety Disorder)
Generalized anxiety disorder (GAD) is a chronic psychiatric condition that commonly presents alongside other psychiatric or medical illnesses. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), GAD is characterized by excessive, persistent, and disproportionate anxiety or worry occurring on most days for at least six months. This worry involves multiple life domains such as work, health, finances, or family and causes significant impairment in daily functioning. The anxiety is accompanied by physical or cognitive symptoms, including restlessness, irritability, muscle tension, sleep disturbance, fatigue, and difficulty concentrating. The diagnosis cannot be made if the symptoms are better explained by another anxiety disorder, mood disorder, substance use, or medical condition.
GAD is relatively common, with a lifetime prevalence of approximately 5% in the general U.S. population and a point prevalence of 2% to 3%. It is the most frequently encountered anxiety disorder in primary care settings. Women are affected about twice as often as men, although men may be less likely to seek treatment. Onset can occur at any age, with nearly half of patients reporting symptoms beginning before age 18, and a median age of onset around 30 years. Genetic contributions appear modest, as twin studies show low concordance rates.
Clinically, patients often describe themselves as having been anxious for most of their lives. Excessive worry is typically accompanied by sleep disturbance, particularly difficulty falling asleep, chronic muscle tension (often in the neck and shoulders), headaches, fatigue, and impaired concentration. Many patients present with somatic complaints such as gastrointestinal symptoms, palpitations, or chest tightness rather than overt psychological distress. Comorbid conditions are common and include major depressive disorder, dysthymia, substance use disorders, and chronic pain syndromes.
The etiology of GAD is multifactorial and includes neurobiologic, psychological, and environmental components. Proposed mechanisms involve dysregulation of neurotransmitters such as serotonin, norepinephrine, and gamma-aminobutyric acid (GABA), as well as personality traits like behavioral inhibition and neuroticism. Risk is increased by family history, chronic stress, trauma exposure, and medical illness. Modifiable risk factors include tobacco use, alcohol or cannabis use, and occupational stress.
Diagnosis requires careful evaluation to exclude other psychiatric disorders and medical causes of anxiety, such as thyroid disease, cardiac arrhythmias, substance intoxication or withdrawal, and other anxiety disorders. Screening tools such as the GAD-2 and GAD-7 questionnaires are commonly used in primary care to aid detection and assess symptom severity. Additional laboratory or imaging studies are guided by the patient’s presentation and clinical suspicion for secondary causes.
Management of GAD typically involves a combination of psychotherapeutic and pharmacologic approaches. Cognitive-behavioral therapy is a first-line nonpharmacologic treatment and has strong evidence for efficacy. Other effective approaches include acceptance and commitment therapy, mindfulness-based interventions, relaxation training, and psychodynamic psychotherapy. Pharmacologic treatment most commonly includes selective serotonin reuptake inhibitors or serotonin-norepinephrine reuptake inhibitors, which have response rates of approximately 60% to 75%. Buspirone and pregabalin are additional effective options, while benzodiazepines are generally reserved for short-term or refractory cases due to risks of dependence and cognitive impairment.
GAD is a chronic condition with fluctuating severity over time. Treatment focuses on reducing symptom burden, improving functioning, and preventing complications such as major depression or suicidality. Referral to mental health specialists is appropriate for patients with refractory symptoms, diagnostic uncertainty, or significant psychiatric comorbidity. Early recognition and sustained treatment can substantially improve long-term outcomes and quality of life.
Generalized anxiety disorder (GAD) is a chronic psychiatric condition that commonly presents alongside other psychiatric or medical illnesses. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), GAD is characterized by excessive, persistent, and disproportionate anxiety or worry occurring on most days for at least six months. This worry involves multiple life domains such as work, health, finances, or family and causes significant impairment in daily functioning. The anxiety is accompanied by physical or cognitive symptoms, including restlessness, irritability, muscle tension, sleep disturbance, fatigue, and difficulty concentrating. The diagnosis cannot be made if the symptoms are better explained by another anxiety disorder, mood disorder, substance use, or medical condition.
GAD is relatively common, with a lifetime prevalence of approximately 5% in the general U.S. population and a point prevalence of 2% to 3%. It is the most frequently encountered anxiety disorder in primary care settings. Women are affected about twice as often as men, although men may be less likely to seek treatment. Onset can occur at any age, with nearly half of patients reporting symptoms beginning before age 18, and a median age of onset around 30 years. Genetic contributions appear modest, as twin studies show low concordance rates.
Clinically, patients often describe themselves as having been anxious for most of their lives. Excessive worry is typically accompanied by sleep disturbance, particularly difficulty falling asleep, chronic muscle tension (often in the neck and shoulders), headaches, fatigue, and impaired concentration. Many patients present with somatic complaints such as gastrointestinal symptoms, palpitations, or chest tightness rather than overt psychological distress. Comorbid conditions are common and include major depressive disorder, dysthymia, substance use disorders, and chronic pain syndromes.
The etiology of GAD is multifactorial and includes neurobiologic, psychological, and environmental components. Proposed mechanisms involve dysregulation of neurotransmitters such as serotonin, norepinephrine, and gamma-aminobutyric acid (GABA), as well as personality traits like behavioral inhibition and neuroticism. Risk is increased by family history, chronic stress, trauma exposure, and medical illness. Modifiable risk factors include tobacco use, alcohol or cannabis use, and occupational stress.
Diagnosis requires careful evaluation to exclude other psychiatric disorders and medical causes of anxiety, such as thyroid disease, cardiac arrhythmias, substance intoxication or withdrawal, and other anxiety disorders. Screening tools such as the GAD-2 and GAD-7 questionnaires are commonly used in primary care to aid detection and assess symptom severity. Additional laboratory or imaging studies are guided by the patient’s presentation and clinical suspicion for secondary causes.
Management of GAD typically involves a combination of psychotherapeutic and pharmacologic approaches. Cognitive-behavioral therapy is a first-line nonpharmacologic treatment and has strong evidence for efficacy. Other effective approaches include acceptance and commitment therapy, mindfulness-based interventions, relaxation training, and psychodynamic psychotherapy. Pharmacologic treatment most commonly includes selective serotonin reuptake inhibitors or serotonin-norepinephrine reuptake inhibitors, which have response rates of approximately 60% to 75%. Buspirone and pregabalin are additional effective options, while benzodiazepines are generally reserved for short-term or refractory cases due to risks of dependence and cognitive impairment.
GAD is a chronic condition with fluctuating severity over time. Treatment focuses on reducing symptom burden, improving functioning, and preventing complications such as major depression or suicidality. Referral to mental health specialists is appropriate for patients with refractory symptoms, diagnostic uncertainty, or significant psychiatric comorbidity. Early recognition and sustained treatment can substantially improve long-term outcomes and quality of life.

- Published on
KembaraXtra-Medicine – Aortic Coarctation
Coarctation of the aorta (CoA) is a congenital narrowing of the aorta, most commonly located near the ligamentum arteriosum just distal to the origin of the left subclavian artery. The narrowing may be preductal, juxtaductal, or postductal, depending on its relationship to the ductus arteriosus. This obstruction increases afterload on the left ventricle, leading to left ventricular hypertrophy and, in severe cases, heart failure. The stenosis may be discrete or long-segment and is often accompanied by the development of collateral circulation. Although CoA can occur in isolation, it is frequently associated with other congenital cardiac abnormalities, particularly bicuspid aortic valve, as well as mitral valve disease, patent ductus arteriosus, and atrial or ventricular septal defects.
Aortic coarctation occurs in approximately 4 per 10,000 live births and accounts for 4% to 8% of all congenital heart defects. It predominantly affects males, with a male-to-female ratio of about 1.5:1. The exact cause is not fully understood, but both genetic and environmental factors are implicated. Maternal exposure to alcohol, drugs, radiation, or infections such as rubella may contribute. While most cases are sporadic, genetic associations have been identified, including mutations in the NOTCH1 gene. CoA is strongly associated with certain genetic syndromes, most notably Turner syndrome, in which 10% to 15% of affected females have coarctation and an increased risk of aortic complications.
Clinical presentation varies with age, severity of narrowing, and adequacy of collateral circulation. Neonates with mild coarctation or a patent ductus arteriosus may be asymptomatic, whereas those with severe narrowing can present with heart failure or cardiogenic shock when the ductus closes. Symptoms in infants may include poor feeding, diaphoresis, dyspnea, pallor, and weak or absent femoral pulses. Beyond infancy, many patients remain asymptomatic, and the condition may be detected incidentally. When symptoms occur, they are often related to upper extremity hypertension and include headaches, epistaxis, dizziness, heart failure symptoms, claudication of the lower extremities, or abdominal angina.
Characteristic physical findings include diminished or delayed femoral pulses compared with brachial pulses, known as brachial–femoral delay. Upper extremity systolic hypertension with low or unobtainable blood pressure in the lower extremities is typical. A systolic ejection murmur is often heard at the left upper sternal border or over the left subscapular area, and a continuous murmur may be present if extensive collateral vessels have developed. Additional murmurs may reflect associated cardiac defects such as a bicuspid aortic valve.
The pathophysiology of CoA involves abnormal development of the aortic wall, with theories suggesting reduced intrauterine blood flow or abnormal extension of ductal tissue into the aorta. Structural abnormalities such as cystic medial necrosis, intimal hyperplasia, increased collagen content, and reduced smooth muscle contribute to arterial stiffness. The obstruction increases left ventricular afterload, resulting in compensatory hypertrophy and collateral vessel formation, while reducing perfusion to the lower body.
Diagnosis relies on careful clinical examination and imaging. Measurement of blood pressure in all four extremities and simultaneous palpation of brachial and femoral pulses are essential. Electrocardiography may show left ventricular hypertrophy. Transthoracic echocardiography is the initial imaging modality and can establish the diagnosis and assess severity, associated defects, and ventricular function. Cross-sectional imaging with cardiac MRI or CT is recommended in all patients for detailed evaluation of the thoracic aorta, collateral vessels, and associated anomalies, and for long-term surveillance after repair. Cardiac catheterization is reserved for cases requiring hemodynamic assessment or therapeutic intervention.
Management depends on age, anatomy, and severity. Critically ill neonates require stabilization with prostaglandin E1 to maintain ductal patency and inotropic support if needed, followed by definitive repair. Surgical correction is preferred in neonates and young children, with excellent outcomes when performed early. In older children and adults, transcatheter balloon angioplasty with stent placement is often the treatment of choice, particularly for native or recurrent coarctation. Covered stents are favored due to lower complication rates. Long-term management focuses on controlling systemic hypertension, which frequently persists even after successful repair, and on lifelong surveillance for complications such as recoarctation, aneurysm formation, and intracranial aneurysms.
Women with aortic coarctation require specialized counseling before pregnancy. Pregnancy is generally well tolerated in those with successful repair and no residual disease, but unrepaired or residual coarctation, uncontrolled hypertension, or aortic aneurysms significantly increase maternal and fetal risk. All patients with CoA, whether repaired or unrepaired, should receive lifelong follow-up with a congenital heart disease specialist, as systemic hypertension and vascular complications remain major long-term concerns.
Coarctation of the aorta (CoA) is a congenital narrowing of the aorta, most commonly located near the ligamentum arteriosum just distal to the origin of the left subclavian artery. The narrowing may be preductal, juxtaductal, or postductal, depending on its relationship to the ductus arteriosus. This obstruction increases afterload on the left ventricle, leading to left ventricular hypertrophy and, in severe cases, heart failure. The stenosis may be discrete or long-segment and is often accompanied by the development of collateral circulation. Although CoA can occur in isolation, it is frequently associated with other congenital cardiac abnormalities, particularly bicuspid aortic valve, as well as mitral valve disease, patent ductus arteriosus, and atrial or ventricular septal defects.
Aortic coarctation occurs in approximately 4 per 10,000 live births and accounts for 4% to 8% of all congenital heart defects. It predominantly affects males, with a male-to-female ratio of about 1.5:1. The exact cause is not fully understood, but both genetic and environmental factors are implicated. Maternal exposure to alcohol, drugs, radiation, or infections such as rubella may contribute. While most cases are sporadic, genetic associations have been identified, including mutations in the NOTCH1 gene. CoA is strongly associated with certain genetic syndromes, most notably Turner syndrome, in which 10% to 15% of affected females have coarctation and an increased risk of aortic complications.
Clinical presentation varies with age, severity of narrowing, and adequacy of collateral circulation. Neonates with mild coarctation or a patent ductus arteriosus may be asymptomatic, whereas those with severe narrowing can present with heart failure or cardiogenic shock when the ductus closes. Symptoms in infants may include poor feeding, diaphoresis, dyspnea, pallor, and weak or absent femoral pulses. Beyond infancy, many patients remain asymptomatic, and the condition may be detected incidentally. When symptoms occur, they are often related to upper extremity hypertension and include headaches, epistaxis, dizziness, heart failure symptoms, claudication of the lower extremities, or abdominal angina.
Characteristic physical findings include diminished or delayed femoral pulses compared with brachial pulses, known as brachial–femoral delay. Upper extremity systolic hypertension with low or unobtainable blood pressure in the lower extremities is typical. A systolic ejection murmur is often heard at the left upper sternal border or over the left subscapular area, and a continuous murmur may be present if extensive collateral vessels have developed. Additional murmurs may reflect associated cardiac defects such as a bicuspid aortic valve.
The pathophysiology of CoA involves abnormal development of the aortic wall, with theories suggesting reduced intrauterine blood flow or abnormal extension of ductal tissue into the aorta. Structural abnormalities such as cystic medial necrosis, intimal hyperplasia, increased collagen content, and reduced smooth muscle contribute to arterial stiffness. The obstruction increases left ventricular afterload, resulting in compensatory hypertrophy and collateral vessel formation, while reducing perfusion to the lower body.
Diagnosis relies on careful clinical examination and imaging. Measurement of blood pressure in all four extremities and simultaneous palpation of brachial and femoral pulses are essential. Electrocardiography may show left ventricular hypertrophy. Transthoracic echocardiography is the initial imaging modality and can establish the diagnosis and assess severity, associated defects, and ventricular function. Cross-sectional imaging with cardiac MRI or CT is recommended in all patients for detailed evaluation of the thoracic aorta, collateral vessels, and associated anomalies, and for long-term surveillance after repair. Cardiac catheterization is reserved for cases requiring hemodynamic assessment or therapeutic intervention.
Management depends on age, anatomy, and severity. Critically ill neonates require stabilization with prostaglandin E1 to maintain ductal patency and inotropic support if needed, followed by definitive repair. Surgical correction is preferred in neonates and young children, with excellent outcomes when performed early. In older children and adults, transcatheter balloon angioplasty with stent placement is often the treatment of choice, particularly for native or recurrent coarctation. Covered stents are favored due to lower complication rates. Long-term management focuses on controlling systemic hypertension, which frequently persists even after successful repair, and on lifelong surveillance for complications such as recoarctation, aneurysm formation, and intracranial aneurysms.
Women with aortic coarctation require specialized counseling before pregnancy. Pregnancy is generally well tolerated in those with successful repair and no residual disease, but unrepaired or residual coarctation, uncontrolled hypertension, or aortic aneurysms significantly increase maternal and fetal risk. All patients with CoA, whether repaired or unrepaired, should receive lifelong follow-up with a congenital heart disease specialist, as systemic hypertension and vascular complications remain major long-term concerns.

- Published on
Emergency and Acute Medicine – Laceration ManagementBasic description
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.

- Published on
Emergency and Acute Medicine – Laryngitis
Basic description
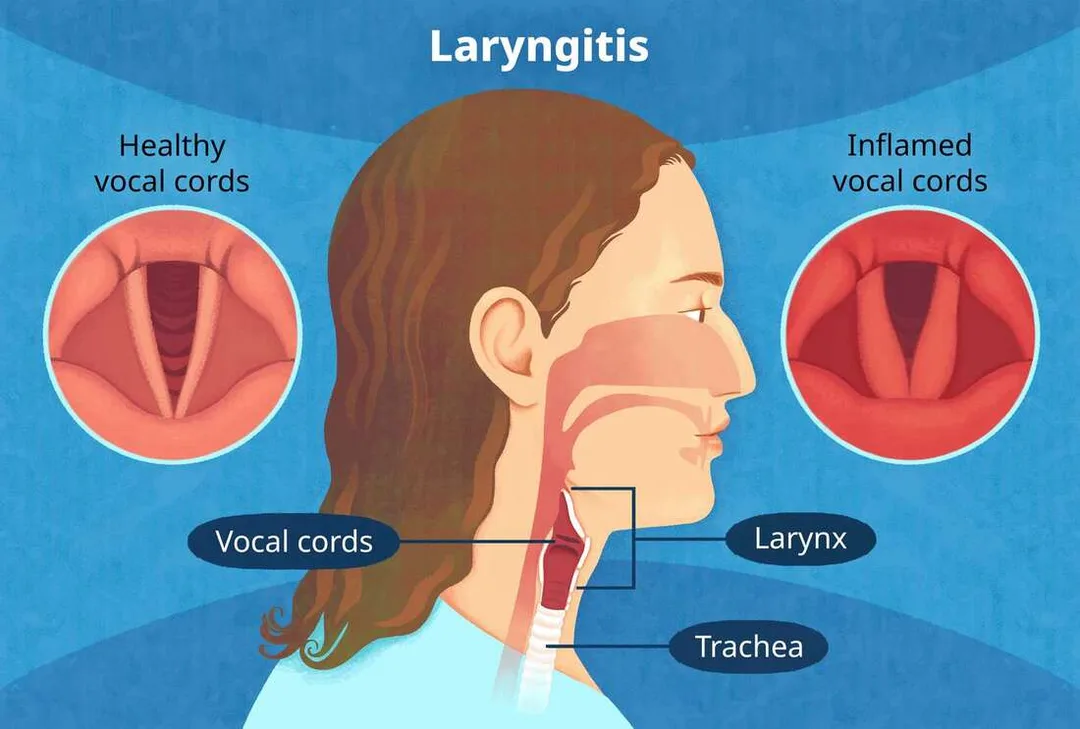
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
Basic description
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
- Published on
Emergency and Acute Medicine – Larynx Fracture
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
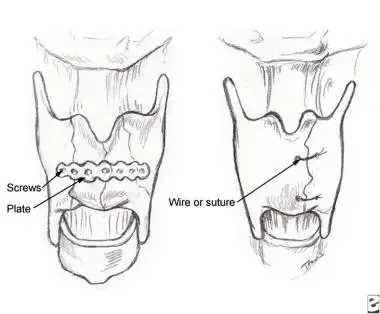
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.
- Published on
Emergency and Acute Medicine – Lead Poisoning
Basic description
Lead toxicity results from multiple mechanisms. Lead binds sulfhydryl groups, disrupting numerous enzymatic processes, and mimics calcium, interfering with calcium-dependent signaling pathways. High serum lead levels compromise the blood–brain barrier, allowing lead entry into the CNS and causing neurotoxicity. After absorption, up to 99% of lead binds to erythrocytes and is later redistributed into bone, where approximately 95% of total body lead resides in adults and 70% in children. Lead commonly coexists with iron deficiency, which increases gastrointestinal absorption. It also impairs heme synthesis, resulting in elevated free erythrocyte protoporphyrin that complexes with zinc, producing increased zinc protoporphyrin levels. Blood lead levels correlate poorly with symptoms but are associated with reduced IQ and increased behavioral problems.
Etiology
Acute lead toxicity most often results from inhalation of environmental sources or ingestion of lead-containing substances such as pottery glazes, folk remedies, cosmetics, jewelry, weights, home-distilled alcohol, or lead dust from ammunition. Chronic toxicity is usually occupational, particularly in battery manufacturing or recycling, bridge painting, construction, electronic waste recycling, firing ranges, mining, smelting, pottery work, and welding. Pediatric poisoning typically arises from home exposures, including lead-based paint ingestion or inhalation, contaminated water from old pipes, lead dust carried home on clothing, imported foods, and folk medicines.
Diagnosis: signs and symptoms
Neurologic manifestations include seizures, encephalopathy, learning disabilities, psychiatric disturbances, cerebral edema, and peripheral motor neuropathy such as wrist drop, which is classic but uncommon. Gastrointestinal findings include colicky abdominal pain (lead colic), ileus, nausea, vomiting, gingival Burton lines indicating lifetime burden, and occasionally hepatitis or pancreatitis. Cardiovascular effects include hypertension, often secondary to renal disease, as well as myocarditis and conduction abnormalities. Renal involvement presents as chronic renal insufficiency with prolonged exposure. Hematologic effects include anemia from impaired globin synthesis and shortened red blood cell lifespan. Musculoskeletal effects include metaphyseal “lead lines,” reflecting altered calcium deposition rather than lead itself, along with impaired bone growth and strength.
Essential workup
The cornerstone of diagnosis is measurement of a whole blood lead level (BLL). There is no normal BLL. In children, educational and environmental interventions begin at BLL ≥10 μg/dL, while chelation therapy is recommended at ≥45 μg/dL. In adults, chelation is usually considered at ≥70 μg/dL, with levels ≥100 μg/dL associated with severe encephalopathy.
Diagnostic tests and interpretation
Laboratory evaluation includes CBC to assess for anemia, RBC indices and iron studies, renal function tests, electrolytes, glucose, liver function tests prior to chelation, and FEP or ZPP levels. Imaging may include abdominal radiographs to detect radiopaque foreign bodies and long-bone radiographs in children to identify lead lines. Cranial CT and other imaging are guided by clinical status.
Differential diagnosis
Acute presentations may mimic appendicitis, gastroenteritis, colitis, cholera, distributive shock, encephalopathy, or other toxic ingestions. Chronic toxicity may resemble Addison disease, Guillain–Barré syndrome, vitamin deficiencies (B3, B6, B12), or Wernicke–Korsakoff syndrome.
Treatment: prehospital and initial stabilization
Management begins with airway, breathing, and circulation support, cardiac monitoring, and seizure control. Skin decontamination should be performed for dermal exposure when safe. Naloxone, thiamine, and dextrose are administered as indicated for altered mental status.
Emergency department management
Whole-bowel irrigation with polyethylene glycol is indicated if radiopaque material is seen on abdominal imaging; activated charcoal is ineffective. Decisions regarding chelation therapy depend on BLL, symptom severity, acuity of exposure, and consultation with a medical toxicologist or poison center. Adults with encephalopathy or BLL >100 μg/dL typically require chelation with dimercaprol followed by calcium disodium EDTA. Asymptomatic adults with BLL 70–100 μg/dL may be treated with oral succimer, while chelation is not indicated for asymptomatic adults with BLL <70 μg/dL. Children with BLL ≥45 μg/dL require chelation, with DMSA for asymptomatic cases and BAL plus CaNa₂EDTA for symptomatic or very high levels. Pregnant patients require multidisciplinary consultation.
Medications
Chelating agents include dimercaprol (BAL), calcium disodium EDTA, and succimer (DMSA). Supportive medications include benzodiazepines for seizures, dextrose for hypoglycemia, naloxone, and thiamine. BAL is contraindicated in patients with peanut allergy.
Disposition and follow-up
Admission is required for symptomatic patients, children at risk for re-exposure, those unable to tolerate oral chelation, and pregnant patients with elevated BLL. Asymptomatic patients not requiring IV chelation may be discharged once a safe environment is ensured and outpatient follow-up is arranged. Pediatric patients must demonstrate tolerance of oral chelation prior to discharge.
Pearls and pitfalls
Heel-stick testing may falsely elevate BLL and should be confirmed with venous sampling. Environmental assessment and social support are critical to prevent re-exposure. Family members and siblings should be screened when a patient is diagnosed with lead toxicity. Avoid BAL in patients with peanut allergy.
Basic description
Lead toxicity results from multiple mechanisms. Lead binds sulfhydryl groups, disrupting numerous enzymatic processes, and mimics calcium, interfering with calcium-dependent signaling pathways. High serum lead levels compromise the blood–brain barrier, allowing lead entry into the CNS and causing neurotoxicity. After absorption, up to 99% of lead binds to erythrocytes and is later redistributed into bone, where approximately 95% of total body lead resides in adults and 70% in children. Lead commonly coexists with iron deficiency, which increases gastrointestinal absorption. It also impairs heme synthesis, resulting in elevated free erythrocyte protoporphyrin that complexes with zinc, producing increased zinc protoporphyrin levels. Blood lead levels correlate poorly with symptoms but are associated with reduced IQ and increased behavioral problems.
Etiology
Acute lead toxicity most often results from inhalation of environmental sources or ingestion of lead-containing substances such as pottery glazes, folk remedies, cosmetics, jewelry, weights, home-distilled alcohol, or lead dust from ammunition. Chronic toxicity is usually occupational, particularly in battery manufacturing or recycling, bridge painting, construction, electronic waste recycling, firing ranges, mining, smelting, pottery work, and welding. Pediatric poisoning typically arises from home exposures, including lead-based paint ingestion or inhalation, contaminated water from old pipes, lead dust carried home on clothing, imported foods, and folk medicines.
Diagnosis: signs and symptoms
Neurologic manifestations include seizures, encephalopathy, learning disabilities, psychiatric disturbances, cerebral edema, and peripheral motor neuropathy such as wrist drop, which is classic but uncommon. Gastrointestinal findings include colicky abdominal pain (lead colic), ileus, nausea, vomiting, gingival Burton lines indicating lifetime burden, and occasionally hepatitis or pancreatitis. Cardiovascular effects include hypertension, often secondary to renal disease, as well as myocarditis and conduction abnormalities. Renal involvement presents as chronic renal insufficiency with prolonged exposure. Hematologic effects include anemia from impaired globin synthesis and shortened red blood cell lifespan. Musculoskeletal effects include metaphyseal “lead lines,” reflecting altered calcium deposition rather than lead itself, along with impaired bone growth and strength.
Essential workup
The cornerstone of diagnosis is measurement of a whole blood lead level (BLL). There is no normal BLL. In children, educational and environmental interventions begin at BLL ≥10 μg/dL, while chelation therapy is recommended at ≥45 μg/dL. In adults, chelation is usually considered at ≥70 μg/dL, with levels ≥100 μg/dL associated with severe encephalopathy.
Diagnostic tests and interpretation
Laboratory evaluation includes CBC to assess for anemia, RBC indices and iron studies, renal function tests, electrolytes, glucose, liver function tests prior to chelation, and FEP or ZPP levels. Imaging may include abdominal radiographs to detect radiopaque foreign bodies and long-bone radiographs in children to identify lead lines. Cranial CT and other imaging are guided by clinical status.
Differential diagnosis
Acute presentations may mimic appendicitis, gastroenteritis, colitis, cholera, distributive shock, encephalopathy, or other toxic ingestions. Chronic toxicity may resemble Addison disease, Guillain–Barré syndrome, vitamin deficiencies (B3, B6, B12), or Wernicke–Korsakoff syndrome.
Treatment: prehospital and initial stabilization
Management begins with airway, breathing, and circulation support, cardiac monitoring, and seizure control. Skin decontamination should be performed for dermal exposure when safe. Naloxone, thiamine, and dextrose are administered as indicated for altered mental status.
Emergency department management
Whole-bowel irrigation with polyethylene glycol is indicated if radiopaque material is seen on abdominal imaging; activated charcoal is ineffective. Decisions regarding chelation therapy depend on BLL, symptom severity, acuity of exposure, and consultation with a medical toxicologist or poison center. Adults with encephalopathy or BLL >100 μg/dL typically require chelation with dimercaprol followed by calcium disodium EDTA. Asymptomatic adults with BLL 70–100 μg/dL may be treated with oral succimer, while chelation is not indicated for asymptomatic adults with BLL <70 μg/dL. Children with BLL ≥45 μg/dL require chelation, with DMSA for asymptomatic cases and BAL plus CaNa₂EDTA for symptomatic or very high levels. Pregnant patients require multidisciplinary consultation.
Medications
Chelating agents include dimercaprol (BAL), calcium disodium EDTA, and succimer (DMSA). Supportive medications include benzodiazepines for seizures, dextrose for hypoglycemia, naloxone, and thiamine. BAL is contraindicated in patients with peanut allergy.
Disposition and follow-up
Admission is required for symptomatic patients, children at risk for re-exposure, those unable to tolerate oral chelation, and pregnant patients with elevated BLL. Asymptomatic patients not requiring IV chelation may be discharged once a safe environment is ensured and outpatient follow-up is arranged. Pediatric patients must demonstrate tolerance of oral chelation prior to discharge.
Pearls and pitfalls
Heel-stick testing may falsely elevate BLL and should be confirmed with venous sampling. Environmental assessment and social support are critical to prevent re-exposure. Family members and siblings should be screened when a patient is diagnosed with lead toxicity. Avoid BAL in patients with peanut allergy.
- Published on
Emergency and Acute Medicine – Leukemia
Basic description
Leukemia refers to a group of malignant neoplasms of white blood cells that result from uncontrolled proliferation of abnormal leukocytes. These malignant cells infiltrate the bone marrow and peripheral blood, impairing normal hematopoiesis. A dangerous complication is hyperleukocytosis, defined as a white blood cell count greater than 100,000/mm³, which can cause leukostasis with occlusion of small vessels, most commonly affecting the brain and lungs. Patients may present with confusion, stupor, hypoxia, or respiratory distress.
Classification and pathophysiology
Chronic myelogenous leukemia (CML) is characterized by overproduction of granulocytic white blood cells, primarily neutrophils, which typically retain normal function. Thrombocytosis and basophilia are common, and the Philadelphia chromosome is present in more than 95% of cases. Chronic lymphocytic leukemia (CLL), the most common leukemia in adults, involves overproduction of monoclonal lymphocytes that accumulate in lymph nodes, bone marrow, liver, and spleen, predisposing patients to herpes virus infections. Acute leukemias, including acute myelogenous leukemia (AML) and acute lymphocytic leukemia (ALL), involve rapid proliferation of immature blast cells and are rapidly fatal without treatment.
Etiology and risk factors
The exact cause of leukemia is unknown. Familial clustering is seen in CLL. Exposure to ionizing radiation increases the risk of AML, ALL, and CML. In pediatric patients, ALL is the most common leukemia and the most common childhood cancer, with remission rates of 60–80% in standard-risk patients. Prognosis is poorer in infants younger than one year. Pregnancy-associated leukemias are most often AML or ALL, and treatment should not be delayed despite potential fetal risks. Older adults more commonly present with CLL or CML.
Diagnosis: signs and symptoms
Clinical presentation varies by leukemia type. CML is often asymptomatic initially but may present with fatigue, weight loss, left upper quadrant pain from splenomegaly, and later leukostasis symptoms such as dyspnea, confusion, and drowsiness. CLL is frequently asymptomatic and discovered incidentally but may present with fatigue, weight loss, lymphadenopathy, hepatosplenomegaly, and recurrent infections. Acute leukemias present more dramatically with fever, fatigue, pallor, bone pain, bleeding due to thrombocytopenia, infections from neutropenia, and symptoms of organ infiltration. Leukemic meningitis may cause headache, nausea, seizures, and altered mental status.
Physical examination findings
Common findings include pallor, petechiae, purpura, ecchymoses, lymphadenopathy, hepatomegaly, and splenomegaly. Chloromas, or granulocytic sarcomas, may be seen in AML. Sausage-shaped hemorrhagic retinal veins are pathognomonic for hyperviscosity syndromes associated with hyperleukocytosis.
Essential workup
Initial evaluation includes a complete blood count with differential and platelet count. CML typically shows markedly elevated white blood cell counts with neutrophil predominance and thrombocytosis. CLL demonstrates absolute lymphocytosis, often greater than 5,000/mm³. Acute leukemias commonly show anemia, thrombocytopenia, and variable white blood cell counts. Bone marrow biopsy is required to confirm the diagnosis.
Diagnostic tests and interpretation
Laboratory studies should include electrolytes, renal function, glucose, calcium, uric acid, and lactate dehydrogenase, which is often elevated in acute leukemias. Coagulation studies are essential to evaluate for disseminated intravascular coagulation. Blood and urine cultures should be obtained in febrile patients. Imaging with chest radiography is useful in evaluating for infection or pulmonary leukostasis. Bone marrow biopsy findings distinguish leukemia subtypes, and cytogenetic testing identifies the Philadelphia chromosome in CML.
Differential diagnosis
The differential includes leukemoid reactions from infection, lymphoma, myeloproliferative disorders, autoimmune disease, viral infections such as Epstein–Barr virus, aplastic anemia, and other causes of cytopenias or lymphocytosis.
Initial stabilization and emergency management
Management begins with airway, breathing, and circulation stabilization. Supplemental oxygen is provided for hypoxia, and IV access is established with isotonic fluids. Platelet transfusions are indicated for significant bleeding, and packed red blood cells are given for symptomatic anemia. Febrile neutropenic patients require prompt broad-spectrum antibiotics. Disseminated intravascular coagulation should be treated aggressively if present.
Emergency department treatment
Leukostasis is treated with aggressive IV hydration, urine alkalinization, allopurinol or rasburicase to prevent tumor lysis syndrome, and urgent leukapheresis. Hydroxyurea is used for cytoreduction in CML. Corticosteroids or whole-brain radiation may be required for central nervous system involvement. Blood products may need to be irradiated or leukocyte-reduced. Definitive therapy, including chemotherapy, immunotherapy, or bone marrow transplantation, is initiated after hematology consultation.
Disposition and follow-up
Admission is required for most newly diagnosed patients, particularly those with symptomatic anemia, thrombocytopenia, hyperleukocytosis, or infection. ICU admission is indicated for unstable patients with bleeding, disseminated intravascular coagulation, blast crisis, or respiratory failure. Asymptomatic patients with minimal laboratory abnormalities may be considered for outpatient management only after hematology consultation.
Pearls and pitfalls
Hyperleukocytosis can present as respiratory failure or neurologic compromise and requires urgent treatment. Tumor lysis syndrome should be anticipated and prevented early. Do not delay hematology consultation in suspected leukemia, as early intervention significantly impacts outcomes.
Basic description
Leukemia refers to a group of malignant neoplasms of white blood cells that result from uncontrolled proliferation of abnormal leukocytes. These malignant cells infiltrate the bone marrow and peripheral blood, impairing normal hematopoiesis. A dangerous complication is hyperleukocytosis, defined as a white blood cell count greater than 100,000/mm³, which can cause leukostasis with occlusion of small vessels, most commonly affecting the brain and lungs. Patients may present with confusion, stupor, hypoxia, or respiratory distress.
Classification and pathophysiology
Chronic myelogenous leukemia (CML) is characterized by overproduction of granulocytic white blood cells, primarily neutrophils, which typically retain normal function. Thrombocytosis and basophilia are common, and the Philadelphia chromosome is present in more than 95% of cases. Chronic lymphocytic leukemia (CLL), the most common leukemia in adults, involves overproduction of monoclonal lymphocytes that accumulate in lymph nodes, bone marrow, liver, and spleen, predisposing patients to herpes virus infections. Acute leukemias, including acute myelogenous leukemia (AML) and acute lymphocytic leukemia (ALL), involve rapid proliferation of immature blast cells and are rapidly fatal without treatment.
Etiology and risk factors
The exact cause of leukemia is unknown. Familial clustering is seen in CLL. Exposure to ionizing radiation increases the risk of AML, ALL, and CML. In pediatric patients, ALL is the most common leukemia and the most common childhood cancer, with remission rates of 60–80% in standard-risk patients. Prognosis is poorer in infants younger than one year. Pregnancy-associated leukemias are most often AML or ALL, and treatment should not be delayed despite potential fetal risks. Older adults more commonly present with CLL or CML.
Diagnosis: signs and symptoms
Clinical presentation varies by leukemia type. CML is often asymptomatic initially but may present with fatigue, weight loss, left upper quadrant pain from splenomegaly, and later leukostasis symptoms such as dyspnea, confusion, and drowsiness. CLL is frequently asymptomatic and discovered incidentally but may present with fatigue, weight loss, lymphadenopathy, hepatosplenomegaly, and recurrent infections. Acute leukemias present more dramatically with fever, fatigue, pallor, bone pain, bleeding due to thrombocytopenia, infections from neutropenia, and symptoms of organ infiltration. Leukemic meningitis may cause headache, nausea, seizures, and altered mental status.
Physical examination findings
Common findings include pallor, petechiae, purpura, ecchymoses, lymphadenopathy, hepatomegaly, and splenomegaly. Chloromas, or granulocytic sarcomas, may be seen in AML. Sausage-shaped hemorrhagic retinal veins are pathognomonic for hyperviscosity syndromes associated with hyperleukocytosis.
Essential workup
Initial evaluation includes a complete blood count with differential and platelet count. CML typically shows markedly elevated white blood cell counts with neutrophil predominance and thrombocytosis. CLL demonstrates absolute lymphocytosis, often greater than 5,000/mm³. Acute leukemias commonly show anemia, thrombocytopenia, and variable white blood cell counts. Bone marrow biopsy is required to confirm the diagnosis.
Diagnostic tests and interpretation
Laboratory studies should include electrolytes, renal function, glucose, calcium, uric acid, and lactate dehydrogenase, which is often elevated in acute leukemias. Coagulation studies are essential to evaluate for disseminated intravascular coagulation. Blood and urine cultures should be obtained in febrile patients. Imaging with chest radiography is useful in evaluating for infection or pulmonary leukostasis. Bone marrow biopsy findings distinguish leukemia subtypes, and cytogenetic testing identifies the Philadelphia chromosome in CML.
Differential diagnosis
The differential includes leukemoid reactions from infection, lymphoma, myeloproliferative disorders, autoimmune disease, viral infections such as Epstein–Barr virus, aplastic anemia, and other causes of cytopenias or lymphocytosis.
Initial stabilization and emergency management
Management begins with airway, breathing, and circulation stabilization. Supplemental oxygen is provided for hypoxia, and IV access is established with isotonic fluids. Platelet transfusions are indicated for significant bleeding, and packed red blood cells are given for symptomatic anemia. Febrile neutropenic patients require prompt broad-spectrum antibiotics. Disseminated intravascular coagulation should be treated aggressively if present.
Emergency department treatment
Leukostasis is treated with aggressive IV hydration, urine alkalinization, allopurinol or rasburicase to prevent tumor lysis syndrome, and urgent leukapheresis. Hydroxyurea is used for cytoreduction in CML. Corticosteroids or whole-brain radiation may be required for central nervous system involvement. Blood products may need to be irradiated or leukocyte-reduced. Definitive therapy, including chemotherapy, immunotherapy, or bone marrow transplantation, is initiated after hematology consultation.
Disposition and follow-up
Admission is required for most newly diagnosed patients, particularly those with symptomatic anemia, thrombocytopenia, hyperleukocytosis, or infection. ICU admission is indicated for unstable patients with bleeding, disseminated intravascular coagulation, blast crisis, or respiratory failure. Asymptomatic patients with minimal laboratory abnormalities may be considered for outpatient management only after hematology consultation.
Pearls and pitfalls
Hyperleukocytosis can present as respiratory failure or neurologic compromise and requires urgent treatment. Tumor lysis syndrome should be anticipated and prevented early. Do not delay hematology consultation in suspected leukemia, as early intervention significantly impacts outcomes.
- Published on
KembaraXtra- Medicine- Aphasia
Aphasia is an acquired disorder of language caused by brain damage to the dominant hemisphere (most often the left). The injury can result from vascular, traumatic, neurodegenerative, neoplastic, infectious, or inflammatory causes, with stroke being the most common. Aphasia is a language disorder, not a problem of muscle control or voice production, so it is different from dysarthria (neuromuscular speech control disorder), dysphonia (voice disorder), apraxia of speech (impaired programming of speech sounds), aphemia (muteness with preserved reading/writing/comprehension), and stuttering. Because language has a specific neuroanatomy, the symptoms of aphasia vary depending on which part of the language network is affected, including Broca area, Wernicke area, the arcuate fasciculus, and surrounding cortical regions.
Aphasia may be described using several related terms and syndromes, including expressive aphasia, receptive aphasia, conduction aphasia, global aphasia, and mixed transcortical (isolation) aphasia. Common ICD-10 codes include R47.01 (Aphasia) and several “aphasia following cerebrovascular disease” codes such as I69.320 (following cerebral infarction), I69.020 (following nontraumatic subarachnoid hemorrhage), I69.120 (following nontraumatic intracerebral hemorrhage), and I69.920 (following unspecified cerebrovascular disease). In the United States, more than one million stroke survivors live with stroke-related aphasia. Aphasia occurs in approximately 21% to 38% of acute stroke patients, and nearly 80% may still have aphasia at 12 months after stroke.
Clinically, aphasia is evaluated by determining whether speech is fluent or nonfluent and then systematically testing core language functions. Bedside assessment includes analysis of spontaneous speech, comprehension (following simple and complex commands), naming (common and uncommon objects), repetition (simple and complex phrases), and reading and writing. Aphasia can be obvious during conversation, but in acute settings it may be mistaken for—or occur alongside—encephalopathy or delirium, making careful language testing important. Stroke-related aphasia typically begins suddenly and is often accompanied by other neurologic signs consistent with involvement of the left middle cerebral artery territory or, in severe cases, the left internal carotid artery territory. Once the patient is stabilized and time-sensitive stroke treatments are addressed, a more detailed language examination is performed to classify the aphasia and guide localization and diagnosis.
Aphasias are broadly categorized into nonfluent and fluent types, with distinct patterns of comprehension and repetition. In nonfluent aphasias, speech is effortful and reduced. Broca aphasia features relatively intact comprehension but impaired repetition, while transcortical motor aphasia has intact comprehension and intact repetition. Global aphasia has impaired comprehension and repetition, and mixed transcortical (isolation) aphasia has impaired comprehension but preserved repetition. In fluent aphasias, speech output is more abundant and well-formed but may be meaningless or error-filled. Wernicke aphasia has impaired comprehension and impaired repetition, while transcortical sensory aphasia has impaired comprehension with preserved repetition. Conduction aphasia typically preserves comprehension but impairs repetition, and anomic aphasia preserves comprehension and repetition but has prominent word-finding difficulty. Salient differences include that nonfluent aphasia often presents with “telegraphic” speech (paucity of words, mainly nouns and verbs) and may be associated with right-sided weakness, whereas fluent aphasia commonly includes paraphasic errors, circumlocutions, tangential speech, and may be associated with visual field deficits or sensory loss, reflecting temporal or parietal involvement.
The differential diagnosis depends heavily on onset and tempo. Acute onset points strongly to stroke, but aphasia can also arise from seizures, trauma, tumors, infections, inflammatory disorders, or metabolic/toxic states affecting language networks. Progressive or insidious language decline suggests neurodegenerative disease, including Alzheimer disease (which can affect language early) and the primary progressive aphasias (PPAs), where language impairment is the dominant early feature. The major PPA variants include the nonfluent/agrammatic variant (nfvPPA), typically linked to degeneration of the left posterior frontoinsular region and often associated with frontotemporal lobar degeneration pathology; the semantic variant (svPPA), associated with anterior and ventral temporal lobe degeneration and characterized by impaired naming, impaired single-word comprehension, loss of object knowledge, and surface dyslexia; and the logopenic variant (lvPPA), linked to left posterior temporal and inferior parietal degeneration and marked by impaired word retrieval, impaired repetition of phrases and sentences, long pauses, and phonologic errors. Some svPPA cases may begin in the right anterior temporal lobe, initially affecting face recognition and interpretation of facial expressions before progressing to classic semantic language deficits.
Workup is targeted to the suspected cause but always includes neuroimaging, preferably brain MRI. In nonstroke aphasia (and when kidney function allows), MRI should be performed with and without contrast. In suspected acute stroke, urgent evaluation typically includes brain CT and CT angiography of the head and neck, with MRI often performed after acute interventions. Advanced imaging such as FDG-PET may be helpful in neurodegenerative aphasias to support diagnosis and characterize patterns of cortical dysfunction. Laboratory testing is likewise cause-directed: stroke-related aphasia evaluation includes assessment of vascular risk factors, while neurodegenerative aphasia workup parallels the broader assessment used for Alzheimer disease and related dementias.
Treatment focuses on the underlying etiology and on rehabilitation of language function. In the acute setting, management targets the cause (for example, stroke therapies when indicated). Long-term care includes speech-language therapy, using approaches such as script training, response elaboration training, constraint-induced aphasia therapy, speech entrainment, and melodic intonation therapy. Supportive communication strategies for patients and families are essential and include speaking slowly with natural rhythm, using short simple sentences, offering limited choices, asking yes/no questions, allowing extra time for responses, confirming understanding by repeating back key points, and avoiding over-correction of minor errors that do not change meaning. Environmental adjustments (reducing distractions, ensuring good lighting, facing the patient, keeping communication tools nearby) and visual supports (gestures, writing key words, pointing to objects or pictures, using communication books) can significantly improve day-to-day communication.
Referral commonly involves neurology for diagnosis and medical management, speech-language pathology for therapy, and often neuropsychology for cognitive assessment. Depending on associated needs, referrals may also include physical medicine and rehabilitation, and psychiatry, especially when mood, behavioral symptoms, or adjustment difficulties arise. Prognosis after stroke-related aphasia is difficult to predict, but recovery is influenced by lesion location and size, aphasia type and severity, and response to early interventions. In general, smaller lesions and preserved left superior temporal gyrus correlate with better outcomes, and intact basal ganglia may also support recovery. Broca and conduction aphasia often have better recovery trajectories than global aphasia, and recovery patterns vary widely across individuals.
Prevention of stroke-related aphasia centers on stroke prevention through modification of vascular risk factors. Education of patients and families should emphasize practical communication techniques and consistent supportive strategies to reduce frustration and improve participation in daily life.
Aphasia is an acquired disorder of language caused by brain damage to the dominant hemisphere (most often the left). The injury can result from vascular, traumatic, neurodegenerative, neoplastic, infectious, or inflammatory causes, with stroke being the most common. Aphasia is a language disorder, not a problem of muscle control or voice production, so it is different from dysarthria (neuromuscular speech control disorder), dysphonia (voice disorder), apraxia of speech (impaired programming of speech sounds), aphemia (muteness with preserved reading/writing/comprehension), and stuttering. Because language has a specific neuroanatomy, the symptoms of aphasia vary depending on which part of the language network is affected, including Broca area, Wernicke area, the arcuate fasciculus, and surrounding cortical regions.
Aphasia may be described using several related terms and syndromes, including expressive aphasia, receptive aphasia, conduction aphasia, global aphasia, and mixed transcortical (isolation) aphasia. Common ICD-10 codes include R47.01 (Aphasia) and several “aphasia following cerebrovascular disease” codes such as I69.320 (following cerebral infarction), I69.020 (following nontraumatic subarachnoid hemorrhage), I69.120 (following nontraumatic intracerebral hemorrhage), and I69.920 (following unspecified cerebrovascular disease). In the United States, more than one million stroke survivors live with stroke-related aphasia. Aphasia occurs in approximately 21% to 38% of acute stroke patients, and nearly 80% may still have aphasia at 12 months after stroke.
Clinically, aphasia is evaluated by determining whether speech is fluent or nonfluent and then systematically testing core language functions. Bedside assessment includes analysis of spontaneous speech, comprehension (following simple and complex commands), naming (common and uncommon objects), repetition (simple and complex phrases), and reading and writing. Aphasia can be obvious during conversation, but in acute settings it may be mistaken for—or occur alongside—encephalopathy or delirium, making careful language testing important. Stroke-related aphasia typically begins suddenly and is often accompanied by other neurologic signs consistent with involvement of the left middle cerebral artery territory or, in severe cases, the left internal carotid artery territory. Once the patient is stabilized and time-sensitive stroke treatments are addressed, a more detailed language examination is performed to classify the aphasia and guide localization and diagnosis.
Aphasias are broadly categorized into nonfluent and fluent types, with distinct patterns of comprehension and repetition. In nonfluent aphasias, speech is effortful and reduced. Broca aphasia features relatively intact comprehension but impaired repetition, while transcortical motor aphasia has intact comprehension and intact repetition. Global aphasia has impaired comprehension and repetition, and mixed transcortical (isolation) aphasia has impaired comprehension but preserved repetition. In fluent aphasias, speech output is more abundant and well-formed but may be meaningless or error-filled. Wernicke aphasia has impaired comprehension and impaired repetition, while transcortical sensory aphasia has impaired comprehension with preserved repetition. Conduction aphasia typically preserves comprehension but impairs repetition, and anomic aphasia preserves comprehension and repetition but has prominent word-finding difficulty. Salient differences include that nonfluent aphasia often presents with “telegraphic” speech (paucity of words, mainly nouns and verbs) and may be associated with right-sided weakness, whereas fluent aphasia commonly includes paraphasic errors, circumlocutions, tangential speech, and may be associated with visual field deficits or sensory loss, reflecting temporal or parietal involvement.
The differential diagnosis depends heavily on onset and tempo. Acute onset points strongly to stroke, but aphasia can also arise from seizures, trauma, tumors, infections, inflammatory disorders, or metabolic/toxic states affecting language networks. Progressive or insidious language decline suggests neurodegenerative disease, including Alzheimer disease (which can affect language early) and the primary progressive aphasias (PPAs), where language impairment is the dominant early feature. The major PPA variants include the nonfluent/agrammatic variant (nfvPPA), typically linked to degeneration of the left posterior frontoinsular region and often associated with frontotemporal lobar degeneration pathology; the semantic variant (svPPA), associated with anterior and ventral temporal lobe degeneration and characterized by impaired naming, impaired single-word comprehension, loss of object knowledge, and surface dyslexia; and the logopenic variant (lvPPA), linked to left posterior temporal and inferior parietal degeneration and marked by impaired word retrieval, impaired repetition of phrases and sentences, long pauses, and phonologic errors. Some svPPA cases may begin in the right anterior temporal lobe, initially affecting face recognition and interpretation of facial expressions before progressing to classic semantic language deficits.
Workup is targeted to the suspected cause but always includes neuroimaging, preferably brain MRI. In nonstroke aphasia (and when kidney function allows), MRI should be performed with and without contrast. In suspected acute stroke, urgent evaluation typically includes brain CT and CT angiography of the head and neck, with MRI often performed after acute interventions. Advanced imaging such as FDG-PET may be helpful in neurodegenerative aphasias to support diagnosis and characterize patterns of cortical dysfunction. Laboratory testing is likewise cause-directed: stroke-related aphasia evaluation includes assessment of vascular risk factors, while neurodegenerative aphasia workup parallels the broader assessment used for Alzheimer disease and related dementias.
Treatment focuses on the underlying etiology and on rehabilitation of language function. In the acute setting, management targets the cause (for example, stroke therapies when indicated). Long-term care includes speech-language therapy, using approaches such as script training, response elaboration training, constraint-induced aphasia therapy, speech entrainment, and melodic intonation therapy. Supportive communication strategies for patients and families are essential and include speaking slowly with natural rhythm, using short simple sentences, offering limited choices, asking yes/no questions, allowing extra time for responses, confirming understanding by repeating back key points, and avoiding over-correction of minor errors that do not change meaning. Environmental adjustments (reducing distractions, ensuring good lighting, facing the patient, keeping communication tools nearby) and visual supports (gestures, writing key words, pointing to objects or pictures, using communication books) can significantly improve day-to-day communication.
Referral commonly involves neurology for diagnosis and medical management, speech-language pathology for therapy, and often neuropsychology for cognitive assessment. Depending on associated needs, referrals may also include physical medicine and rehabilitation, and psychiatry, especially when mood, behavioral symptoms, or adjustment difficulties arise. Prognosis after stroke-related aphasia is difficult to predict, but recovery is influenced by lesion location and size, aphasia type and severity, and response to early interventions. In general, smaller lesions and preserved left superior temporal gyrus correlate with better outcomes, and intact basal ganglia may also support recovery. Broca and conduction aphasia often have better recovery trajectories than global aphasia, and recovery patterns vary widely across individuals.
Prevention of stroke-related aphasia centers on stroke prevention through modification of vascular risk factors. Education of patients and families should emphasize practical communication techniques and consistent supportive strategies to reduce frustration and improve participation in daily life.

