- Published on
Infectious Disease - Appendicitis
FUNDAMENTALS OVERVIEW
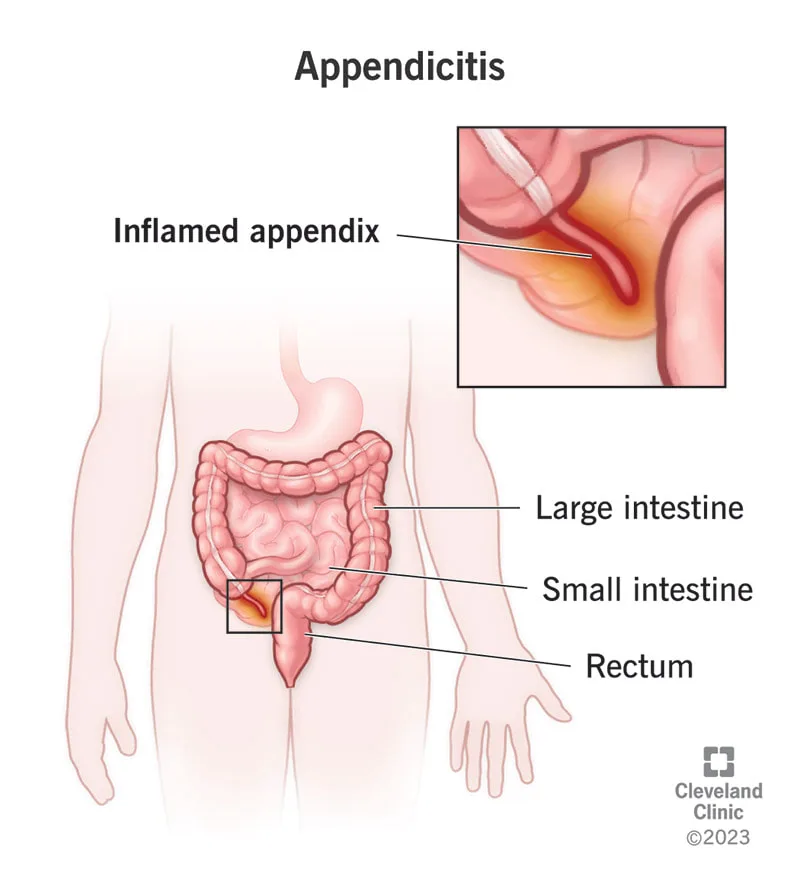
• Appendicitis refers to the inflammation of the appendix. • When the blood supply to the appendix is impaired, it is termed “gangrenous appendicitis.” When appendicitis is complicated by perforation, it is referred to as "perforating appendicitis." When appendicitis is caused by a blockage of the lumen, it is referred to as "obstructive appendicitis."
EPIDEMIOLOGY
Incidence Appendectomy is the most common indication for abdominal surgery. Annually in the United States, there are a minimum of 250,000 instances of appendicitis, necessitating over 1 million inpatient hospital days. • The appendix appears normal in around one-third of patients who need emergency appendectomy. • Missed appendicitis ranks among the most commonly successful malpractice claims against emergency room clinicians.
RISK FACTORS
Males exhibit a little greater rate than females, with a male-to-female ratio of 3:2. The lifetime risk of appendicitis is 8.5% for males and 6.7% for females. • Acute appendicitis may manifest at any age, with peak incidence observed during the second and third decades of life. • Perforation is more prevalent among infants and the elderly.
PATHOPHYSIOLOGY
• Luminal blockage is the principal etiology of appendicitis. • The obstruction is most frequently attributed to a fecalith, but may also result from foreign bodies, increased lymphoid hyperplasia linked to viral infections (e.g., measles), helminths, or neoplasms (e.g., carcinoid or carcinoma). • Mucus accumulates behind the obstruction, leading to bacterial proliferation and invasion of the appendiceal wall, which causes venous engorgement and subsequent arterial impairment and ischemia due to elevated intraluminal pressures. • Ultimately, gangrene and perforation ensue. Rupture of primary appendiceal abscesses may result in fistulas. • Acute appendicitis may, at times, serve as the initial symptom of Crohn’s disease. • Infrequently, recurrent acute appendicitis may manifest with complete remission of inflammation and symptoms between episodes.
ETIOLOGY • Proliferation of several gastrointestinal bacteria (E. coli, Peptostreptococcus, B. fragilis, Enterobacteriaceae, viridans streptococcus) transpires within the obstructed appendix. • Chronic appendiceal infection may arise from tuberculosis, amebiasis, and actinomycosis.
DIAGNOSIS HISTORY
The onset of pain transpires across several hours. The earliest visceral abdominal pain of appendicitis is colicky and typically poorly localized in the periumbilical or epigastric area. As inflammation spreads to the parietal peritoneal surfaces, the pain becomes somatic, steady, and more intense. The pain intensifies with movement or coughing and is localized in the right lower quadrant (McBurney's point). • An associated need to defecate or expel flatus frequently occurs, neither of which alleviates the discomfort. Anorexia is prevalent enough that the manifestation of hunger should raise concern for a diagnosis of acute appendicitis. Nausea and vomiting manifest in 50–60% of instances; however, vomiting is seldom severe and prolonged. The occurrence of nausea and vomiting prior to the onset of pain is exceedingly uncommon. • Urinary frequency and dysuria manifest when the appendix is positioned near to the bladder.
PHYSICAL EXAM • Physical results fluctuate over time following the commencement of the illness and are contingent upon the appendix's position. • Tenderness may initially be absent in the early visceral stage of the disease, but it eventually manifests in the area corresponding to the appendix's location. Pregnant women frequently exhibit pain in the right upper quadrant. Guarding is a result of parietal peritoneal involvement. Tenderness upon percussion, rebound tenderness, and referred rebound tenderness are frequently observed. Rebound soreness in the right lower quadrant during probing of the left lower quadrant is referred to as "Rovsing's sign." Pain induced by passive flexion of the right hip is referred to as "the psoas sign"; pain induced by internal rotation of the right hip is referred to as "the obturator sign." • The temperature is often normal or marginally elevated; however, a temperature beyond 38.3°C (101°F) indicates potential perforation. • A discernible mass in the right lower quadrant implies the possibility of an abscess or cecal cancer.
DIAGNOSTIC TESTS AND INTERPRETATION Lab
Leukocytosis ranging from 10,000 to 18,000 cells per milliliter with a left shift is prevalent; however, the lack of leukocytosis does not preclude the diagnosis of acute appendicitis. A pregnancy test must be conducted for all women of childbearing age to exclude the possibility of uterine or ectopic pregnancy. Imaging: Preliminary Strategy Among noninvasive diagnostic tools, appendiceal CT has demonstrated superior precision, achieving an accuracy of 90%. The greatest accuracy has been documented with helical CT following the administration of a 3% diatrizoate meglumine (Gastrografin)–saline solution into the colon. Appendiceal CT is safe, can be conducted in roughly 15 minutes, and necessitates only one-third of the radiation exposure compared to normal CT of the belly and pelvis. Routine appendiceal CT conducted in patients with probable appendicitis enhances patient care and diminishes the utilization of hospital resources. Ultrasound is particularly beneficial for women of childbearing age to rule out ovarian cysts, ectopic pregnancy, or tubo-ovarian abscess. It is also utilized in pediatrics. Normal ultrasonographic findings should not dissuade the surgeon from conducting an appendectomy if the clinical history suggests appendicitis and there is definitive discomfort in the right lower quadrant. Subsequent Actions & Unique Considerations The management strategies for clinicians assessing patients with suspected appendicitis including observation, diagnostic imaging, laparoscopy, and appendectomy. • Patients with a history strongly indicative of appendicitis are frequently sent to the operating room for laparoscopy, irrespective of imaging outcomes. • Patients with a less compelling history are typically subjected to imaging or monitoring. Histopathological Observations Pathology specimens from acute appendicitis exhibit indicators of inflammation, including polymorphonuclear leukocytes, edema, and vascular congestion in the appendiceal walls.
DIFFERENTIAL DIAGNOSIS • The lack of right lower quadrant pain, the absence of typical pain migration, and a history of analogous pain render appendicitis less probable. The absence of right lower quadrant discomfort, rigidity, or guarding during the physical examination diminishes the likelihood of appendicitis. • The differential diagnosis of acute appendicitis encompasses the following: – Acute cholecystitis – Acute diverticulitis – Acute gastroenteritis – Acute pancreatitis – Acute pelvic inflammatory illness – Endometriosis – Mesenteric lymphadenitis – Perforated ulcer – Pyelonephritis – Ruptured Graafian follicle or corpus luteum cyst – Ruptured ectopic pregnancy – Strangulating intestinal blockage – Torted ovarian cyst – Ureteral calculus The differential diagnosis of acute appendicitis is elaborated upon in Section I, chapter "Abdominal Pain and Fever."
THERAPY
The principal intervention for appendicitis is immediate surgical intervention. Antibiotics are the normal preoperative treatment and must be effective against gram-negative aerobes and anaerobes.
MEDICATION • Antibiotic care parallels that of other intra-abdominal infections, as elaborated in Section II chapters, “Peritonitis” and “Intra-abdominal Abscess.” • Options comprise: – Beta-lactam and beta-lactamase inhibitor (ampicillin–sulbactam, piperacillin–tazobactam, ticarcillin–clavulanate) – Ceftriaxone and metronidazole – Fluoroquinolone and metronidazole - Carbapenems (imipenem, meropenem)
SUPPLEMENTARY THERAPY
Referral Considerations Surgical intervention should be integrated into the management of a patient with suspected appendicitis from the moment of initial presentation.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Prompt surgical assessment of a patient with a compelling history and/or imaging indicative of appendicitis is essential. • Both laparoscopic and open techniques are permissible. Patients undergoing laparoscopic surgery experience fewer wound infections, reduced discomfort, and shorter hospital stays compared to those undergoing open surgery. Nonetheless, laparoscopic appendectomies are correlated with an increased incidence of intra-abdominal abscesses, extended operative durations, and elevated surgical expenses. • If a palpable mass is detected 3–5 days post-symptom onset, the procedure should be postponed, since a phlegmon rather than a definite abscess is likely to be present. Patients should get broad-spectrum antibiotics, parenteral fluids, and rest. An appendectomy should be performed safely three months later. If the tumor increases in size or the patient exhibits heightened toxicity, abscess drainage is required.
INPATIENT CONSIDERATIONS
Preliminary Stabilization If unstable, the patient with appendicitis is likely experiencing sepsis or has a perforated appendix with subsequent peritonitis. The patient requires resuscitation with intravenous fluids, and vasopressors should be administered if deemed required. Admission Criteria All patients with suspected appendicitis must be admitted. Intravenous Fluids Patients should be thoroughly hydrated preoperatively, and electrolyte imbalances must be corrected. Criteria for Discharge Discharge criteria encompass the normalization of white blood cell count, the resolution of fever, and the restoration of bowel function.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
Close monitoring of patients with stomach pain who do not undergo additional diagnostic testing is warranted.
NUTRITION
Individuals suspected of having appendicitis should refrain from eating.
PROGNOSIS • The mortality rate in Europe and the US has consistently declined to less than 1 per 100,000. The general mortality rate for perforated appendicitis is 3%, escalating to 15% in the elderly population.
COMPLICATIONS
The postponement of appendicitis diagnosis elevates the likelihood of appendiceal perforation, which is linked to postoperative complications in as many as 40% of patients, in contrast to 5–10% for uncomplicated appendicitis. Perforation is uncommon within the first 24 hours of symptom onset, but the incidence increases to 80% after 48 hours. The formation of intra-abdominal abscesses or phlegmon typically occurs subsequent to perforation accompanied by generalized peritonitis and can be prevented with early disease detection. • Wounds must be monitored for indications of infection. • Portal vein thrombophlebitis and pyogenic liver abscess are rare occurrences.
FUNDAMENTALS OVERVIEW
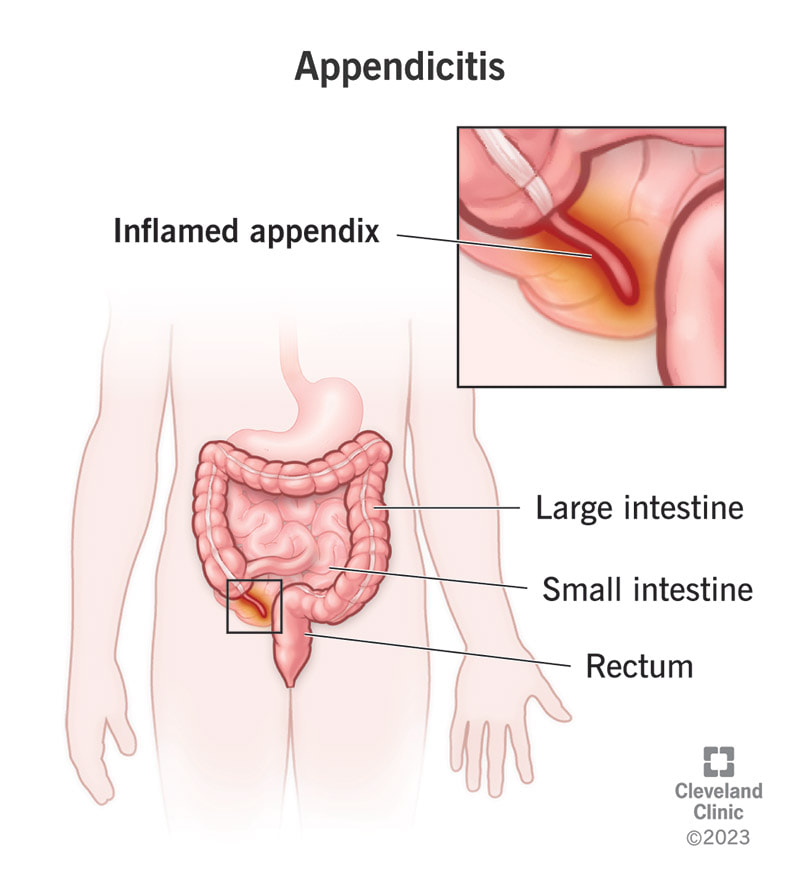
• Appendicitis refers to the inflammation of the appendix. • When the blood supply to the appendix is impaired, it is termed “gangrenous appendicitis.” When appendicitis is complicated by perforation, it is referred to as "perforating appendicitis." When appendicitis is caused by a blockage of the lumen, it is referred to as "obstructive appendicitis."
EPIDEMIOLOGY
Incidence Appendectomy is the most common indication for abdominal surgery. Annually in the United States, there are a minimum of 250,000 instances of appendicitis, necessitating over 1 million inpatient hospital days. • The appendix appears normal in around one-third of patients who need emergency appendectomy. • Missed appendicitis ranks among the most commonly successful malpractice claims against emergency room clinicians.
RISK FACTORS
Males exhibit a little greater rate than females, with a male-to-female ratio of 3:2. The lifetime risk of appendicitis is 8.5% for males and 6.7% for females. • Acute appendicitis may manifest at any age, with peak incidence observed during the second and third decades of life. • Perforation is more prevalent among infants and the elderly.
PATHOPHYSIOLOGY
• Luminal blockage is the principal etiology of appendicitis. • The obstruction is most frequently attributed to a fecalith, but may also result from foreign bodies, increased lymphoid hyperplasia linked to viral infections (e.g., measles), helminths, or neoplasms (e.g., carcinoid or carcinoma). • Mucus accumulates behind the obstruction, leading to bacterial proliferation and invasion of the appendiceal wall, which causes venous engorgement and subsequent arterial impairment and ischemia due to elevated intraluminal pressures. • Ultimately, gangrene and perforation ensue. Rupture of primary appendiceal abscesses may result in fistulas. • Acute appendicitis may, at times, serve as the initial symptom of Crohn’s disease. • Infrequently, recurrent acute appendicitis may manifest with complete remission of inflammation and symptoms between episodes.
ETIOLOGY • Proliferation of several gastrointestinal bacteria (E. coli, Peptostreptococcus, B. fragilis, Enterobacteriaceae, viridans streptococcus) transpires within the obstructed appendix. • Chronic appendiceal infection may arise from tuberculosis, amebiasis, and actinomycosis.
DIAGNOSIS HISTORY
The onset of pain transpires across several hours. The earliest visceral abdominal pain of appendicitis is colicky and typically poorly localized in the periumbilical or epigastric area. As inflammation spreads to the parietal peritoneal surfaces, the pain becomes somatic, steady, and more intense. The pain intensifies with movement or coughing and is localized in the right lower quadrant (McBurney's point). • An associated need to defecate or expel flatus frequently occurs, neither of which alleviates the discomfort. Anorexia is prevalent enough that the manifestation of hunger should raise concern for a diagnosis of acute appendicitis. Nausea and vomiting manifest in 50–60% of instances; however, vomiting is seldom severe and prolonged. The occurrence of nausea and vomiting prior to the onset of pain is exceedingly uncommon. • Urinary frequency and dysuria manifest when the appendix is positioned near to the bladder.
PHYSICAL EXAM • Physical results fluctuate over time following the commencement of the illness and are contingent upon the appendix's position. • Tenderness may initially be absent in the early visceral stage of the disease, but it eventually manifests in the area corresponding to the appendix's location. Pregnant women frequently exhibit pain in the right upper quadrant. Guarding is a result of parietal peritoneal involvement. Tenderness upon percussion, rebound tenderness, and referred rebound tenderness are frequently observed. Rebound soreness in the right lower quadrant during probing of the left lower quadrant is referred to as "Rovsing's sign." Pain induced by passive flexion of the right hip is referred to as "the psoas sign"; pain induced by internal rotation of the right hip is referred to as "the obturator sign." • The temperature is often normal or marginally elevated; however, a temperature beyond 38.3°C (101°F) indicates potential perforation. • A discernible mass in the right lower quadrant implies the possibility of an abscess or cecal cancer.
DIAGNOSTIC TESTS AND INTERPRETATION Lab
Leukocytosis ranging from 10,000 to 18,000 cells per milliliter with a left shift is prevalent; however, the lack of leukocytosis does not preclude the diagnosis of acute appendicitis. A pregnancy test must be conducted for all women of childbearing age to exclude the possibility of uterine or ectopic pregnancy. Imaging: Preliminary Strategy Among noninvasive diagnostic tools, appendiceal CT has demonstrated superior precision, achieving an accuracy of 90%. The greatest accuracy has been documented with helical CT following the administration of a 3% diatrizoate meglumine (Gastrografin)–saline solution into the colon. Appendiceal CT is safe, can be conducted in roughly 15 minutes, and necessitates only one-third of the radiation exposure compared to normal CT of the belly and pelvis. Routine appendiceal CT conducted in patients with probable appendicitis enhances patient care and diminishes the utilization of hospital resources. Ultrasound is particularly beneficial for women of childbearing age to rule out ovarian cysts, ectopic pregnancy, or tubo-ovarian abscess. It is also utilized in pediatrics. Normal ultrasonographic findings should not dissuade the surgeon from conducting an appendectomy if the clinical history suggests appendicitis and there is definitive discomfort in the right lower quadrant. Subsequent Actions & Unique Considerations The management strategies for clinicians assessing patients with suspected appendicitis including observation, diagnostic imaging, laparoscopy, and appendectomy. • Patients with a history strongly indicative of appendicitis are frequently sent to the operating room for laparoscopy, irrespective of imaging outcomes. • Patients with a less compelling history are typically subjected to imaging or monitoring. Histopathological Observations Pathology specimens from acute appendicitis exhibit indicators of inflammation, including polymorphonuclear leukocytes, edema, and vascular congestion in the appendiceal walls.
DIFFERENTIAL DIAGNOSIS • The lack of right lower quadrant pain, the absence of typical pain migration, and a history of analogous pain render appendicitis less probable. The absence of right lower quadrant discomfort, rigidity, or guarding during the physical examination diminishes the likelihood of appendicitis. • The differential diagnosis of acute appendicitis encompasses the following: – Acute cholecystitis – Acute diverticulitis – Acute gastroenteritis – Acute pancreatitis – Acute pelvic inflammatory illness – Endometriosis – Mesenteric lymphadenitis – Perforated ulcer – Pyelonephritis – Ruptured Graafian follicle or corpus luteum cyst – Ruptured ectopic pregnancy – Strangulating intestinal blockage – Torted ovarian cyst – Ureteral calculus The differential diagnosis of acute appendicitis is elaborated upon in Section I, chapter "Abdominal Pain and Fever."
THERAPY
The principal intervention for appendicitis is immediate surgical intervention. Antibiotics are the normal preoperative treatment and must be effective against gram-negative aerobes and anaerobes.
MEDICATION • Antibiotic care parallels that of other intra-abdominal infections, as elaborated in Section II chapters, “Peritonitis” and “Intra-abdominal Abscess.” • Options comprise: – Beta-lactam and beta-lactamase inhibitor (ampicillin–sulbactam, piperacillin–tazobactam, ticarcillin–clavulanate) – Ceftriaxone and metronidazole – Fluoroquinolone and metronidazole - Carbapenems (imipenem, meropenem)
SUPPLEMENTARY THERAPY
Referral Considerations Surgical intervention should be integrated into the management of a patient with suspected appendicitis from the moment of initial presentation.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Prompt surgical assessment of a patient with a compelling history and/or imaging indicative of appendicitis is essential. • Both laparoscopic and open techniques are permissible. Patients undergoing laparoscopic surgery experience fewer wound infections, reduced discomfort, and shorter hospital stays compared to those undergoing open surgery. Nonetheless, laparoscopic appendectomies are correlated with an increased incidence of intra-abdominal abscesses, extended operative durations, and elevated surgical expenses. • If a palpable mass is detected 3–5 days post-symptom onset, the procedure should be postponed, since a phlegmon rather than a definite abscess is likely to be present. Patients should get broad-spectrum antibiotics, parenteral fluids, and rest. An appendectomy should be performed safely three months later. If the tumor increases in size or the patient exhibits heightened toxicity, abscess drainage is required.
INPATIENT CONSIDERATIONS
Preliminary Stabilization If unstable, the patient with appendicitis is likely experiencing sepsis or has a perforated appendix with subsequent peritonitis. The patient requires resuscitation with intravenous fluids, and vasopressors should be administered if deemed required. Admission Criteria All patients with suspected appendicitis must be admitted. Intravenous Fluids Patients should be thoroughly hydrated preoperatively, and electrolyte imbalances must be corrected. Criteria for Discharge Discharge criteria encompass the normalization of white blood cell count, the resolution of fever, and the restoration of bowel function.
CONTINUING MANAGEMENT POST-TREATMENT SUGGESTIONS
Close monitoring of patients with stomach pain who do not undergo additional diagnostic testing is warranted.
NUTRITION
Individuals suspected of having appendicitis should refrain from eating.
PROGNOSIS • The mortality rate in Europe and the US has consistently declined to less than 1 per 100,000. The general mortality rate for perforated appendicitis is 3%, escalating to 15% in the elderly population.
COMPLICATIONS
The postponement of appendicitis diagnosis elevates the likelihood of appendiceal perforation, which is linked to postoperative complications in as many as 40% of patients, in contrast to 5–10% for uncomplicated appendicitis. Perforation is uncommon within the first 24 hours of symptom onset, but the incidence increases to 80% after 48 hours. The formation of intra-abdominal abscesses or phlegmon typically occurs subsequent to perforation accompanied by generalized peritonitis and can be prevented with early disease detection. • Wounds must be monitored for indications of infection. • Portal vein thrombophlebitis and pyogenic liver abscess are rare occurrences.
0 Comments
