- Published on
Infectious Disease - Aspergillosis
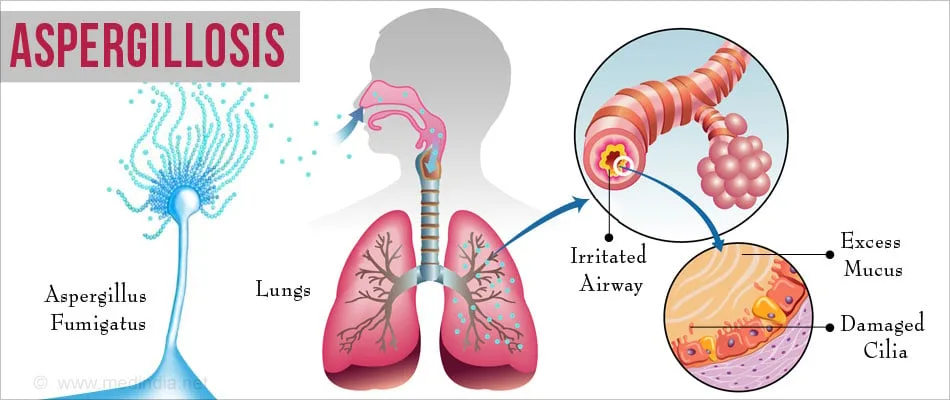
BASICS DESCRIPTION • The term “aspergillosis” encompasses a broad spectrum of conditions, ranging from mere colonization or allergic reactions to localized or widespread invasive diseases. The illness typically targets the lungs, while it can also affect any organ, with the paranasal sinuses and central nervous system (CNS) being less frequently implicated.
EPIDEMIOLOGY
Incidence • The variety of Aspergillus species responsible for invasive illness seems to be increasing. A. fumigatus is the predominant species; however, A. flavus, A. terreus, A. niger, and A. versicolor have also been implicated in aspergillosis. Invasive aspergillosis ranks second in prevalence to candidiasis among invasive mycoses in the majority of immunosuppressed patient populations.
RISK FACTORS
• Granulocytopenia (the most significant predisposing factor) • Hematopoietic cell transplant recipients • Solid-organ transplant recipients • Individuals with acute leukemia • Chronic obstructive pulmonary disease (COPD) patients undergoing steroid therapy • Extended corticosteroid or cytotoxic treatment • Prolonged antibiotic administration • Hepatic failure • Diabetes mellitus • Chronic granulomatous illness in childhood • Acquired immunodeficiency syndrome (AIDS) (CD4 count of 50 cells/mm³ or fewer) Genetics • Polymorphisms in Toll-like receptor 4 may elevate the risk of invasive aspergillosis. • Polymorphisms in Toll-like receptor 9 may influence the risk of allergic bronchopulmonary aspergillosis (ABPA).
GENERAL PREVENTION
• Implementation of environmental control measures, particularly during building operations, to prevent conidia from reaching at-risk patients. • Airflow units equipped with high-efficiency particle air filters. Prophylactic use of voriconazole or amphotericin B may be contemplated for individuals with a history of invasive illness who are at risk of becoming neutropenic.
PATHOPHYSIOLOGY
• ABPA – Aspergillus colonization in atopic individuals activates TH2 CD4+ T cells, resulting in increased IgE expression and eosinophilia. This inflammatory milieu aggravates asthma, resulting in worse symptoms. Airway injury and central bronchiectasis may develop. • Chronic pulmonary aspergillosis, including aspergilloma, typically manifests in patients with the following diseases. – History of tuberculosis – Allergic bronchopulmonary aspergillosis – Lung cancer with surgical excision – Bulla formation • COPD – Lesions exhibit persistent inflammatory alterations, fibrosis, and necrosis. – Invasion is not observed unless the patient enters an immunocompromised state. • Invasive aspergillosis – Conidia are omnipresent and sufficiently diminutive to reach the alveolus upon inhalation. Alveolar macrophages generally phagocytize these infections. – In an immunocompromised state, macrophages are unable to retain the conidia, allowing them to germinate into hyphae. The existence of hyphal forms induces the influx of macrophages and the release of inflammatory cytokines. Vascular invasion and subsequent tissue necrosis may occur. – Circulation via the bloodstream is feasible.
DIAGNOSIS HISTORY
• ABPA – Present in individuals with diagnosed asthma or cystic fibrosis – Possible bronchial obstruction – General malaise – Rare occurrence of hemoptysis • Chronic aspergillosis – Weight loss – Persistent cough – Hemoptysis – Shortness of breath – Dyspnea upon exertion • Invasive aspergillosis – Pleuritic chest pain – Cough – Hemoptysis – Dyspnea
PHYSICAL EXAMINATION
• ABPA – Wheezing may be seen, but is not mandatory. – Fever • Chronic aspergillosis – Abnormal pulmonary auscultation – Fever • Invasive aspergillosis – Fever – Abnormal pulmonary auscultation
DIAGNOSTIC TESTS AND INTERPRETATION
Diagnostic Procedures and Additional Methods • ABPA – Chest X-ray may reveal parenchymal infiltrates, typically affecting the higher lobes. CT scan reveals bronchial wall thickening, bronchiectasis, and ground-glass opacities. – Peripheral eosinophilia – Immediate reaction to skin tests for Aspergillus – Increased total serum IgE – Serum IgG to A. fumigatus • Chronic aspergillosis – Chest X-ray and/or Chest CT reveal one or more cavities – Aspergilloma masses may be observed within the cavity, typically encircled by air- Crescent shadow - Serum IgG to A. fumigatus - Elevated CRP or ESR • Invasive aspergillosis - Positive culture from tissue biopsy is the gold standard - Evidence of fungal invasion in tissue - Positive galactomannan level in serum - Positive β-glucan level in serum
THERAPY PHARMACEUTICALS
First Line • ABPA – A regimen of glucocorticoids and itraconazole is employed. – Steroids may be gradually reduced over a period of 3 to 6 months. – In certain instances, steroids cannot be reduced, necessitating ongoing steroid maintenance. • Chronic aspergillosis – Aspergilloma generally necessitates surgical resection in patients capable of enduring the procedure. Certain individuals derive advantages from antifungal treatment, predominantly voriconazole. Chronic pulmonary aspergillosis necessitates prolonged antifungal treatment. Embolization is employed in patients to mitigate the risk of hemoptysis. • Invasive aspergillosis – Voriconazole is regarded as the primary treatment. Surgical debridement is necessary whenever feasible. Second Line • For invasive aspergillosis, other medicines comprise amphotericin B, itraconazole, and echinocandins. – The efficacy of combination therapy involving the aforementioned antimicrobials remains unverified.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Aggressive debridement should be contemplated for patients with persistent or invasive diseases.
INPATIENT CONSIDERATIONS
Preliminary Stabilization • Antifungal therapy, either intravenous or oral, should be commenced promptly. • Hemodynamic parameters must be stabilized. Admission Criteria: • Patients exhibiting hemodynamic instability • Patients presenting with hemoptysis • Certain patients with fever and immunocompromised conditions
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patients with hypersensitivity lung disorders must be followed for relapses and the onset of pulmonary fibrosis or bronchiectasis. Patients with aspergillomas who do not get surgical intervention require clinical and radiological surveillance for lesion progression and the onset of hemoptysis. Patients who receive surgical intervention for aspergillomas require monitoring for potential return of the infection, despite initial surgical success. Patients with invasive illness require monitoring for relapses, particularly during episodes of neutropenia. Patient Surveillance Monitoring of voriconazole trough levels is essential for individuals undergoing prolonged treatment with the drug.
PROGNOSIS
The prognosis for patients with invasive aspergillosis is contingent upon the fungal load and the extent of immunosuppression.
COMPLICATIONS
The most dreaded consequence of chronic pulmonary aspergillosis is hemoptysis. • Dissemination and mortality are critical consequences in patients with invasive aspergillosis. Bronchiectasis may complicate allergic bronchopulmonary aspergillosis (ABPA). Pulmonary fibrosis may complicate both allergic bronchopulmonary aspergillosis (ABPA) and extrinsic allergic alveolitis. Hemoptysis, which can be substantial, particularly for lesions situated near the hilum, may aggravate both invasive and noninvasive pulmonary aspergillosis. Pneumothorax may arise in immunocompromised individuals and is typically linked to the enhancement of the immune system. The introduction of Aspergilli into the pleural space, resulting from pneumothorax or the formation of a bronchopleural fistula, may result in empyema. In instances of pulmonary and extrapulmonary invasive aspergillosis, persistent dissemination to other organs and lesion enlargement may occur, particularly in immunocompromised persons. Patients with central nervous system involvement may have occlusion of cerebral vessels due to Aspergillus.
BASICS DESCRIPTION • The term “aspergillosis” encompasses a broad spectrum of conditions, ranging from mere colonization or allergic reactions to localized or widespread invasive diseases. The illness typically targets the lungs, while it can also affect any organ, with the paranasal sinuses and central nervous system (CNS) being less frequently implicated.
EPIDEMIOLOGY
Incidence • The variety of Aspergillus species responsible for invasive illness seems to be increasing. A. fumigatus is the predominant species; however, A. flavus, A. terreus, A. niger, and A. versicolor have also been implicated in aspergillosis. Invasive aspergillosis ranks second in prevalence to candidiasis among invasive mycoses in the majority of immunosuppressed patient populations.
RISK FACTORS
• Granulocytopenia (the most significant predisposing factor) • Hematopoietic cell transplant recipients • Solid-organ transplant recipients • Individuals with acute leukemia • Chronic obstructive pulmonary disease (COPD) patients undergoing steroid therapy • Extended corticosteroid or cytotoxic treatment • Prolonged antibiotic administration • Hepatic failure • Diabetes mellitus • Chronic granulomatous illness in childhood • Acquired immunodeficiency syndrome (AIDS) (CD4 count of 50 cells/mm³ or fewer) Genetics • Polymorphisms in Toll-like receptor 4 may elevate the risk of invasive aspergillosis. • Polymorphisms in Toll-like receptor 9 may influence the risk of allergic bronchopulmonary aspergillosis (ABPA).
GENERAL PREVENTION
• Implementation of environmental control measures, particularly during building operations, to prevent conidia from reaching at-risk patients. • Airflow units equipped with high-efficiency particle air filters. Prophylactic use of voriconazole or amphotericin B may be contemplated for individuals with a history of invasive illness who are at risk of becoming neutropenic.
PATHOPHYSIOLOGY
• ABPA – Aspergillus colonization in atopic individuals activates TH2 CD4+ T cells, resulting in increased IgE expression and eosinophilia. This inflammatory milieu aggravates asthma, resulting in worse symptoms. Airway injury and central bronchiectasis may develop. • Chronic pulmonary aspergillosis, including aspergilloma, typically manifests in patients with the following diseases. – History of tuberculosis – Allergic bronchopulmonary aspergillosis – Lung cancer with surgical excision – Bulla formation • COPD – Lesions exhibit persistent inflammatory alterations, fibrosis, and necrosis. – Invasion is not observed unless the patient enters an immunocompromised state. • Invasive aspergillosis – Conidia are omnipresent and sufficiently diminutive to reach the alveolus upon inhalation. Alveolar macrophages generally phagocytize these infections. – In an immunocompromised state, macrophages are unable to retain the conidia, allowing them to germinate into hyphae. The existence of hyphal forms induces the influx of macrophages and the release of inflammatory cytokines. Vascular invasion and subsequent tissue necrosis may occur. – Circulation via the bloodstream is feasible.
DIAGNOSIS HISTORY
• ABPA – Present in individuals with diagnosed asthma or cystic fibrosis – Possible bronchial obstruction – General malaise – Rare occurrence of hemoptysis • Chronic aspergillosis – Weight loss – Persistent cough – Hemoptysis – Shortness of breath – Dyspnea upon exertion • Invasive aspergillosis – Pleuritic chest pain – Cough – Hemoptysis – Dyspnea
PHYSICAL EXAMINATION
• ABPA – Wheezing may be seen, but is not mandatory. – Fever • Chronic aspergillosis – Abnormal pulmonary auscultation – Fever • Invasive aspergillosis – Fever – Abnormal pulmonary auscultation
DIAGNOSTIC TESTS AND INTERPRETATION
Diagnostic Procedures and Additional Methods • ABPA – Chest X-ray may reveal parenchymal infiltrates, typically affecting the higher lobes. CT scan reveals bronchial wall thickening, bronchiectasis, and ground-glass opacities. – Peripheral eosinophilia – Immediate reaction to skin tests for Aspergillus – Increased total serum IgE – Serum IgG to A. fumigatus • Chronic aspergillosis – Chest X-ray and/or Chest CT reveal one or more cavities – Aspergilloma masses may be observed within the cavity, typically encircled by air- Crescent shadow - Serum IgG to A. fumigatus - Elevated CRP or ESR • Invasive aspergillosis - Positive culture from tissue biopsy is the gold standard - Evidence of fungal invasion in tissue - Positive galactomannan level in serum - Positive β-glucan level in serum
THERAPY PHARMACEUTICALS
First Line • ABPA – A regimen of glucocorticoids and itraconazole is employed. – Steroids may be gradually reduced over a period of 3 to 6 months. – In certain instances, steroids cannot be reduced, necessitating ongoing steroid maintenance. • Chronic aspergillosis – Aspergilloma generally necessitates surgical resection in patients capable of enduring the procedure. Certain individuals derive advantages from antifungal treatment, predominantly voriconazole. Chronic pulmonary aspergillosis necessitates prolonged antifungal treatment. Embolization is employed in patients to mitigate the risk of hemoptysis. • Invasive aspergillosis – Voriconazole is regarded as the primary treatment. Surgical debridement is necessary whenever feasible. Second Line • For invasive aspergillosis, other medicines comprise amphotericin B, itraconazole, and echinocandins. – The efficacy of combination therapy involving the aforementioned antimicrobials remains unverified.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Aggressive debridement should be contemplated for patients with persistent or invasive diseases.
INPATIENT CONSIDERATIONS
Preliminary Stabilization • Antifungal therapy, either intravenous or oral, should be commenced promptly. • Hemodynamic parameters must be stabilized. Admission Criteria: • Patients exhibiting hemodynamic instability • Patients presenting with hemoptysis • Certain patients with fever and immunocompromised conditions
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patients with hypersensitivity lung disorders must be followed for relapses and the onset of pulmonary fibrosis or bronchiectasis. Patients with aspergillomas who do not get surgical intervention require clinical and radiological surveillance for lesion progression and the onset of hemoptysis. Patients who receive surgical intervention for aspergillomas require monitoring for potential return of the infection, despite initial surgical success. Patients with invasive illness require monitoring for relapses, particularly during episodes of neutropenia. Patient Surveillance Monitoring of voriconazole trough levels is essential for individuals undergoing prolonged treatment with the drug.
PROGNOSIS
The prognosis for patients with invasive aspergillosis is contingent upon the fungal load and the extent of immunosuppression.
COMPLICATIONS
The most dreaded consequence of chronic pulmonary aspergillosis is hemoptysis. • Dissemination and mortality are critical consequences in patients with invasive aspergillosis. Bronchiectasis may complicate allergic bronchopulmonary aspergillosis (ABPA). Pulmonary fibrosis may complicate both allergic bronchopulmonary aspergillosis (ABPA) and extrinsic allergic alveolitis. Hemoptysis, which can be substantial, particularly for lesions situated near the hilum, may aggravate both invasive and noninvasive pulmonary aspergillosis. Pneumothorax may arise in immunocompromised individuals and is typically linked to the enhancement of the immune system. The introduction of Aspergilli into the pleural space, resulting from pneumothorax or the formation of a bronchopleural fistula, may result in empyema. In instances of pulmonary and extrapulmonary invasive aspergillosis, persistent dissemination to other organs and lesion enlargement may occur, particularly in immunocompromised persons. Patients with central nervous system involvement may have occlusion of cerebral vessels due to Aspergillus.
0 Comments
