- Published on
Infectious Disease - Babesiosis
FUNDAMENTALS AND DESCRIPTION
Babesia is a protozoan that exhibits a preference for human erythrocytes. It is a prevalent etiology of hemolytic illness in endemic regions. The primary mode of transmission for Babesia microti is by bites from deer ticks (Ixodid species). Alternative, less prevalent transmission methods encompass blood transfusions and maternal transmission of babesiosis. The majority of B. microti is predominantly located in the Northeastern and Midwestern regions of the United States. Additional Babesia species are present in the western United States and Europe.
EPIDEMIOLOGY
• Babesia is classified as an emerging infectious illness due to the rising incidence of reported cases over the past decade. • The escalation of deer populations, tick density, and heightened human activity in endemic regions are believed to contribute to the increase in Babesia infections. • Numerous cases of Babesia remain subclinical in younger persons, suggesting that the incidence of this infection is likely underestimated. Data from blood donors indicate that 0.5–15% of individuals have been exposed in highly endemic regions.
FACTORS OF RISK
• Residing in or visiting endemic areas. • Patients without a spleen. • Immunosuppression (e.g., HIV, chemotherapy).
COMPREHENSIVE PREVENTION
• Individuals who are asplenic or immunocompromised, and so at heightened risk of severe illness, should avoid endemic locations during periods of elevated transmission, namely from May to October (3). Insect repellent is effective in preventing tick bites, particularly ones containing N-diethyl-meta-toluamide (DEET). Early removal of ticks is crucial; the tick must be attached for a minimum of 24 hours before transmission commences. Daily self-assessment is advised for individuals participating in outdoor activities in endemic regions. It is advisable to inspect pets for ticks in endemic regions. Clothing can be treated with permethrin to avert infection.
PATHOPHYSIOLOGY
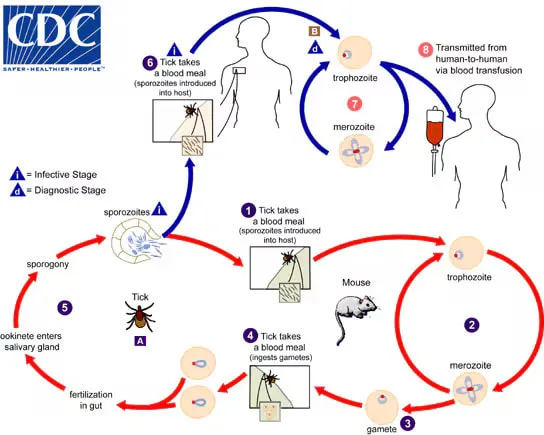
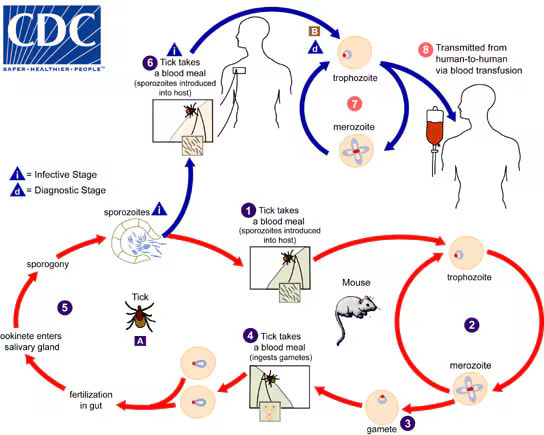
The life cycle include the transmission of Babesia between vertebrate hosts and Ixodes ticks. Humans serve as "dead end" and "accidental" hosts, with the predominant transmission vectors for B. microti being white-footed mice and ticks. Humans may become unwell upon infection; yet, they do not contribute to the transmission of the pathogen. Ixodes ticks deliver sporozoites to the host's bloodstream. The sporozoites infiltrate the erythrocytes and transform into trophozoites. The trophozoites reproduce asexually through budding, resulting in 2–4 merozoites. The merozoites compromise red blood cells (RBCs) and infiltrate other RBCs, resulting in hemolysis and anemia. ETIOLOGY • The predominant cause of Babesia in the United States is B. microti, which is prevalent in New England, coastal New York, and the Midwest. Other prevalent Babesia species that induce sickness in humans are Babesia divergens in Europe and Babesia duncani in the Western United States.
FREQUENTLY CO-OCCURRING CONDITIONS
Co-infection with Lyme disease and human granulocytic anaplasmosis frequently occurs, as both are transmitted by Ixodes ticks in endemic areas. In endemic regions, up to 10% of those diagnosed with Lyme disease are concurrently infected with Babesia.
DIAGNOSIS HISTORY
Patients may be asymptomatic or exhibit the following symptoms: • Pyrexia • Rigors • Asthenia • Cephalalgia • Nausea/emesis • Abdominal discomfort • Diarrhea • Arthralgia • Dyspnea/thoracic pain • Darkened urine Inquire about recent Lyme disease illness, residence or travel in endemic regions, outdoor exposures, pet ownership, and recent tick bites.
PHYSICAL EXAMINATION
• Pyrexia • Splenomegaly • Hepatomegaly • Pallor • Icterus • Absence of lymphadenopathy • Assess for a rash indicative of erythema chronicum migrans in instances of Lyme co-infection
DIAGNOSTIC EXAMINATIONS & ANALYSIS
Laboratory Initial Assessments • Prepare thin blood smears to evaluate for intra-erythrocytic parasites and indications of hemolysis. In instances of low parasitemia and early infection, multiple blood smears may be required over several days. • Complete blood count: Anemia and thrombocytopenia detected. • Indicators of hemolysis: Increased reticulocyte count, LDH, and indirect bilirubin levels. Additionally, haptoglobin levels are low. • Hepatic function assays. Subsequent Actions & Unique Considerations • If the bacterium is undetected via blood smear, PCR amplification of 18S rRNA is advised. In patients with a significant likelihood of infection, indirect immunofluorescent antibody testing is advised when both blood smear and PCR results are negative. Imaging Imaging is typically unnecessary in moderate situations. Abdominal ultrasonography will verify hepatomegaly or splenomegaly. Pathological Observations Similar to malaria, Babesia manifests as an intra-erythrocytic parasite. Babesia parasites may be observed outside of red blood cells during severe infections, a phenomenon not present in malarial infections. At times, Babesia parasites (in the internal merozoite phase) manifest in tetrads, referred to as the "Maltese cross."
Differential Diagnosis: • Sepsis • Lyme Disease • Human Granulocytic Anaplasmosis • Hepatitis • Malaria • Lymphoma
TREATMENT MEDICATION
For B. microti infection: administer oral atovaquone 750 mg twice daily for 7–10 days, in conjunction with oral azithromycin 500–1,000 mg on day 1, followed by 250 mg daily thereafter. Second Line For B. microti infection: Administer oral quinine 650 mg three or four times daily in conjunction with oral clindamycin 600 mg three times daily for a duration of 7 to 10 days. Intravenous formulations are applicable. Quinine and clindamycin are utilized in critical instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies Asymptomatic immunocompetent people with detectable parasites on blood smear for less than three months do not necessitate treatment (5). Extended treatment durations may be required for immunocompromised individuals or in instances of significant parasite load. Treatment must persist for a minimum of 6 weeks, encompassing 2 weeks of therapy following the undetectability of parasites in blood smears. Concerns for Referral An infectious disease specialist should be consulted if there are indications of serious infection or infection in an immunocompromised individual. Supplementary Treatments Red blood cell exchange transfusions may be required in severe instances of excessive parasitemia (>10%) or the presence of shock/ARDS symptoms.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patient Surveillance Hospitalized patients should undergo daily CBC and blood smear assessments to monitor for hemolysis, anemia, and parasite load.
INFORMATION FOR PATIENTS
Educate patients of the risk factors associated with Babesia transmission and implement measures to prevent re-infection.
COMPLICATIONS
• Disseminated Intravascular Coagulation (DIC) • Anemia • Congestive Heart Failure (CHF) • Acute Respiratory Distress Syndrome (ARDS) • Renal Dysfunction • Hypotension
FUNDAMENTALS AND DESCRIPTION
Babesia is a protozoan that exhibits a preference for human erythrocytes. It is a prevalent etiology of hemolytic illness in endemic regions. The primary mode of transmission for Babesia microti is by bites from deer ticks (Ixodid species). Alternative, less prevalent transmission methods encompass blood transfusions and maternal transmission of babesiosis. The majority of B. microti is predominantly located in the Northeastern and Midwestern regions of the United States. Additional Babesia species are present in the western United States and Europe.
EPIDEMIOLOGY
• Babesia is classified as an emerging infectious illness due to the rising incidence of reported cases over the past decade. • The escalation of deer populations, tick density, and heightened human activity in endemic regions are believed to contribute to the increase in Babesia infections. • Numerous cases of Babesia remain subclinical in younger persons, suggesting that the incidence of this infection is likely underestimated. Data from blood donors indicate that 0.5–15% of individuals have been exposed in highly endemic regions.
FACTORS OF RISK
• Residing in or visiting endemic areas. • Patients without a spleen. • Immunosuppression (e.g., HIV, chemotherapy).
COMPREHENSIVE PREVENTION
• Individuals who are asplenic or immunocompromised, and so at heightened risk of severe illness, should avoid endemic locations during periods of elevated transmission, namely from May to October (3). Insect repellent is effective in preventing tick bites, particularly ones containing N-diethyl-meta-toluamide (DEET). Early removal of ticks is crucial; the tick must be attached for a minimum of 24 hours before transmission commences. Daily self-assessment is advised for individuals participating in outdoor activities in endemic regions. It is advisable to inspect pets for ticks in endemic regions. Clothing can be treated with permethrin to avert infection.
PATHOPHYSIOLOGY
The life cycle include the transmission of Babesia between vertebrate hosts and Ixodes ticks. Humans serve as "dead end" and "accidental" hosts, with the predominant transmission vectors for B. microti being white-footed mice and ticks. Humans may become unwell upon infection; yet, they do not contribute to the transmission of the pathogen. Ixodes ticks deliver sporozoites to the host's bloodstream. The sporozoites infiltrate the erythrocytes and transform into trophozoites. The trophozoites reproduce asexually through budding, resulting in 2–4 merozoites. The merozoites compromise red blood cells (RBCs) and infiltrate other RBCs, resulting in hemolysis and anemia. ETIOLOGY • The predominant cause of Babesia in the United States is B. microti, which is prevalent in New England, coastal New York, and the Midwest. Other prevalent Babesia species that induce sickness in humans are Babesia divergens in Europe and Babesia duncani in the Western United States.
FREQUENTLY CO-OCCURRING CONDITIONS
Co-infection with Lyme disease and human granulocytic anaplasmosis frequently occurs, as both are transmitted by Ixodes ticks in endemic areas. In endemic regions, up to 10% of those diagnosed with Lyme disease are concurrently infected with Babesia.
DIAGNOSIS HISTORY
Patients may be asymptomatic or exhibit the following symptoms: • Pyrexia • Rigors • Asthenia • Cephalalgia • Nausea/emesis • Abdominal discomfort • Diarrhea • Arthralgia • Dyspnea/thoracic pain • Darkened urine Inquire about recent Lyme disease illness, residence or travel in endemic regions, outdoor exposures, pet ownership, and recent tick bites.
PHYSICAL EXAMINATION
• Pyrexia • Splenomegaly • Hepatomegaly • Pallor • Icterus • Absence of lymphadenopathy • Assess for a rash indicative of erythema chronicum migrans in instances of Lyme co-infection
DIAGNOSTIC EXAMINATIONS & ANALYSIS
Laboratory Initial Assessments • Prepare thin blood smears to evaluate for intra-erythrocytic parasites and indications of hemolysis. In instances of low parasitemia and early infection, multiple blood smears may be required over several days. • Complete blood count: Anemia and thrombocytopenia detected. • Indicators of hemolysis: Increased reticulocyte count, LDH, and indirect bilirubin levels. Additionally, haptoglobin levels are low. • Hepatic function assays. Subsequent Actions & Unique Considerations • If the bacterium is undetected via blood smear, PCR amplification of 18S rRNA is advised. In patients with a significant likelihood of infection, indirect immunofluorescent antibody testing is advised when both blood smear and PCR results are negative. Imaging Imaging is typically unnecessary in moderate situations. Abdominal ultrasonography will verify hepatomegaly or splenomegaly. Pathological Observations Similar to malaria, Babesia manifests as an intra-erythrocytic parasite. Babesia parasites may be observed outside of red blood cells during severe infections, a phenomenon not present in malarial infections. At times, Babesia parasites (in the internal merozoite phase) manifest in tetrads, referred to as the "Maltese cross."
Differential Diagnosis: • Sepsis • Lyme Disease • Human Granulocytic Anaplasmosis • Hepatitis • Malaria • Lymphoma
TREATMENT MEDICATION
For B. microti infection: administer oral atovaquone 750 mg twice daily for 7–10 days, in conjunction with oral azithromycin 500–1,000 mg on day 1, followed by 250 mg daily thereafter. Second Line For B. microti infection: Administer oral quinine 650 mg three or four times daily in conjunction with oral clindamycin 600 mg three times daily for a duration of 7 to 10 days. Intravenous formulations are applicable. Quinine and clindamycin are utilized in critical instances.
SUPPLEMENTARY THERAPY
Comprehensive Strategies Asymptomatic immunocompetent people with detectable parasites on blood smear for less than three months do not necessitate treatment (5). Extended treatment durations may be required for immunocompromised individuals or in instances of significant parasite load. Treatment must persist for a minimum of 6 weeks, encompassing 2 weeks of therapy following the undetectability of parasites in blood smears. Concerns for Referral An infectious disease specialist should be consulted if there are indications of serious infection or infection in an immunocompromised individual. Supplementary Treatments Red blood cell exchange transfusions may be required in severe instances of excessive parasitemia (>10%) or the presence of shock/ARDS symptoms.
CONTINUING CARE FOLLOW-UP SUGGESTIONS
Patient Surveillance Hospitalized patients should undergo daily CBC and blood smear assessments to monitor for hemolysis, anemia, and parasite load.
INFORMATION FOR PATIENTS
Educate patients of the risk factors associated with Babesia transmission and implement measures to prevent re-infection.
COMPLICATIONS
• Disseminated Intravascular Coagulation (DIC) • Anemia • Congestive Heart Failure (CHF) • Acute Respiratory Distress Syndrome (ARDS) • Renal Dysfunction • Hypotension
0 Comments
