- Published on
Infectious Disease - Endocarditis (Native Valves)
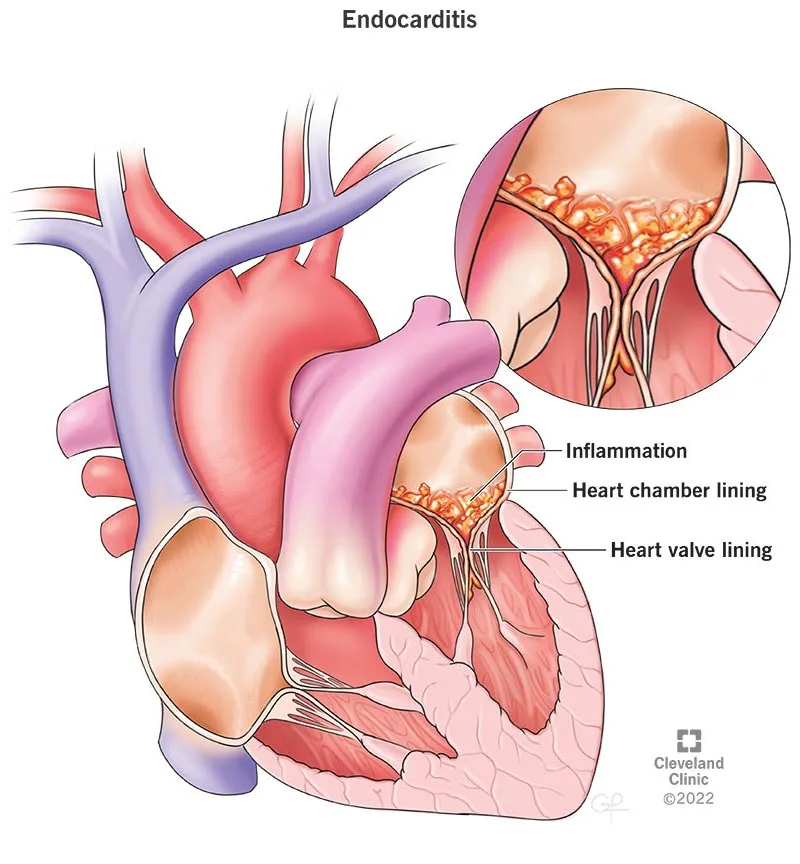
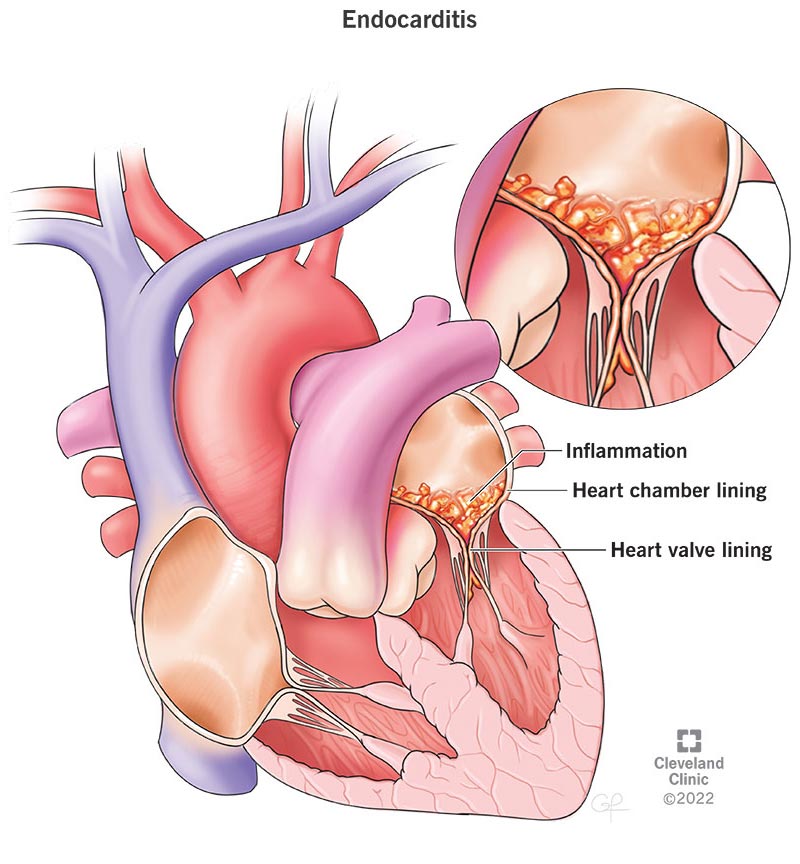
Endocarditis is an infection of the heart valves or endocardium caused by bacteria, fungus, or, less commonly, chlamydiae or rickettsiae. The mitral valve (41%) and aortic valve (38%) are the most frequently implicated in native valve infective endocarditis (NVIE). Tricuspid valve endocarditis is more prevalent among intravenous drug users. Pulmonic valve endocarditis is exceedingly uncommon. Several valves may be affected.
EPIDEMIOLOGY Incidence The prevalence of NVIE is between 1.7–6.2 cases per 100,000 patient-years. The incidence among intravenous drug users is estimated to be 1500–3300 cases per 100,000 patient-years.
Risk Factors
Predisposing factors encompass active intravenous drug use, a history of endocarditis, chronic intravascular access, the presence of an implantable cardiac device, congenital heart anomalies, a bicuspid aortic valve, rheumatic heart disease, and degenerative valvular disease.
GENERAL PREVENTION • Antibiotic prophylaxis for endocarditis is advised for people with the following conditions: – Prosthetic heart valve or valve repair utilizing prosthetic material – History of endocarditis - Congenital heart disease (unrepaired cyanotic CHD, treated CHD with residual abnormality) - Recipients of cardiac transplants with valvular heart disease
Prophylaxis is advised for dental procedures that include disruption of the oral mucosa and manipulation of the gingiva.
Prophylaxis is advisable for individuals with high-risk disorders, as previously mentioned, who are undergoing procedures involving the respiratory tract, skin, soft tissue, or muscle. Antibiotics for the prophylaxis of infective endocarditis are not advised for gastrointestinal or genitourinary surgeries.
Antibiotic protocols consist of a single dosage of amoxicillin 2 g or clindamycin 600 mg administered 30–60 minutes before the surgery.
ETIOLOGY • The predominant causal pathogens are gram-positive bacteria. Staphylococcus aureus has recently emerged as the predominant cause of NVIE. • The prevalent microbiological etiologies for NVIE are enumerated below: S. aureus (25–35%) — Coagulase-negative Staphylococcus (3–11%) - Viridans group streptococci (17–40 percent) - Streptococcus bovis (6 percent) - Additional streptococcus (6–19%) - Enterococcus species (10–18%) - HACEK (2–5 percent) Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella species. - Fungi/yeast (2–4 percent) • Culture-negative endocarditis (10%) The predominant cause is the administration of antibiotics within the preceding 7 days. – Alternative potential etiologies encompass slow-growing fastidious anaerobes, non-Candida fungal species, Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., and Brucella spp. In intravenous drug users, polymicrobial non-valvular infective endocarditis (NVIE) is more prevalent.
DIAGNOSIS HISTORY
The clinical manifestations of NVIE exhibit significant variability, encompassing symptoms and indications attributable to the infected valve, embolic events, metastatic infection locations, and circulating immune complexes. Fever occurs in more than 90% of people with NVIE. General symptoms including weakness, chills, diaphoresis, anorexia, weight loss, nausea, and malaise may occur (3). • The revised Duke criteria are extensively utilized diagnostic standards for NVIE. • Principal criteria: – Microbiological evidence includes two sets of blood cultures positive for typical microorganisms such as Viridans streptococci, S. bovis, HACEK group, S. aureus; or community-acquired enterococci without a primary focus; or microorganisms consistent with infective endocarditis from persistently positive blood cultures; or a single positive blood culture for Coxiella burnetii or an anti-phase 1 IgG antibody titer exceeding 1:800. - Indications of endocardial involvement Favorable echocardiography (oscillating intracardiac mass on valve, abscess, or fresh partial dehiscence of prosthetic valve) New valvular regurgitation (deterioration or alteration of a preexisting murmur is inadequate)
• Minor criterion – Predisposition, preexisting cardiac disease, or intravenous drug use (IDU) – Pyrexia – Vascular manifestations: Significant artery emboli, septic pulmonary infarcts, mycotic aneurysms, cerebral hemorrhage, conjunctival hemorrhages, and Janeway lesions - Immunological manifestations: Glomerulonephritis, Osler's nodes, Roth's spots, and rheumatoid factor - Microbiological evidence: Positive blood culture; however, it does not fulfill a significant requirement as previously indicated, nor is there serological evidence of current infection with an organism consistent with infective endocarditis. • Definitive endocarditis (clinical criteria): 2 main criteria; or 1 major criterion in conjunction with 3 minor criteria; or 5 minor criteria • Conclusive endocarditis (pathological criteria): Microorganisms discovered through culture or pathological study of vegetation, embolized vegetation, or intracardiac abscess; or vegetation or intracardiac abscess exhibiting active endocarditis via histological evaluation. • Potential endocarditis: 1 major criterion + 1 minor criterion; or 3 minor criteria • Rejected: Definitive alternative diagnosis; symptom remission within 4 days of antibiotic treatment; absence of pathological evidence of infective endocarditis during surgery after fewer than 4 days of antibiotics; does not fulfill clinical criteria for probable infective endocarditis.
PHYSICAL EXAM • Clinical manifestations of infective endocarditis (IE) may present as a new or altered murmur in up to 85% of cases. • Petechiae occur in 20–40% of patients. Other cutaneous manifestations (Osler nodes, Janeway lesions, splinter hemorrhages) or Roth spots are observed in a minority of patients. A comprehensive examination is necessary to detect further infection sites (epidural abscess, psoas abscess, septic arthritis) or to discover embolic occurrences (stroke).
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Preliminary laboratory assessments In cases of suspected NVIE, the initial laboratory assessment include a full blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and erythrocyte sedimentation rate (ESR). • Within the initial 24 hours, get a minimum of 3 sets of blood cultures. Obtain multiple sets of blood cultures prior to administering antibiotics to enhance the likelihood of identifying the causal bacteria. The initial two sets yield positive results in up to 90% of patients. Leukocytosis is prevalent. Over fifty percent of patients exhibit elevated serum inflammatory markers (ESR, C-reactive protein). The urinalysis often indicates the presence of proteinuria or microscopic hematuria.
Subsequent Actions & Unique Considerations
• In instances of culture-negative endocarditis, serological assessment for uncommon pathogens such as Q fever and Bartonella spp. may be warranted. • Acquire two sets of blood cultures every 24 to 48 hours until the endovascular infection has resolved. Imaging: Preliminary Approach Echocardiography is the preferred imaging modality and should be conducted promptly in all instances of suspected NVIE.
• The sensitivity of transthoracic echocardiography (TTE) for identifying left-sided vegetations varies between 40% and 63%, with a specificity of 91% to 98%. The sensitivity for right-sided lesions is elevated due to the proximity of the tricuspid and pulmonic valves to the chest wall. Transesophageal echocardiography may be constrained by obesity, chronic pulmonary illness, or thoracic wall deformities.
Transesophageal echocardiography (TEE) exhibits a sensitivity of 90–100% and a specificity of 91–98% in the identification of vegetations. TEE exhibits greater sensitivity than TTE in detecting valve perforation, pacemaker-associated infective endocarditis, and cardiac abscess.
Transesophageal echocardiography (TEE) is advised as the primary diagnostic test when transthoracic echocardiography (TTE) is anticipated to yield suboptimal results, there is a strong clinical suspicion of infective endocarditis (IE), or perivalvular extension is predicted. If the initial TTE is negative and there is a moderate to high clinical suspicion for IE, proceed with a TEE.
Subsequent Actions & Unique Considerations
Further imaging of the chest, abdomen, spine, or brain is necessary if emboli, abscesses, or mycotic aneurysms are suspected. Diagnostic Procedures and Additional Methods Acquire an EKG to determine a baseline heart rhythm and detect any conduction abnormalities. A repeat EKG is indicated for alterations in clinical status, bradycardia, syncope, or presyncope. Pathological Observations Histopathologic investigation reveals that vegetations comprise fibrin, platelet aggregates, and bacterial or fungal masses. PCR-based assays for detecting organisms such as Bartonella spp. and T. whippleii in blood or valvular tissue are accessible at some laboratories.
DIFFERENTIAL DIAGNOSIS
Noninfective endocarditis, alternative systemic infection, bacteremia, or fungemia absent of infective endocarditis.
Treatment Medication
Extended antibacterial treatment is necessary to infiltrate the vegetation and avert recurrence. Identifying the causative organism and its therapeutic susceptibilities is essential. Empiric therapy is predicated on patient risk factors for diverse infections, the severity of sickness, and local resistance patterns. • Below are the recommended treatment regimens for specific pathogens (1). • Penicillin-susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks. – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily, in addition to gentamicin 3 mg/kg/day in a single dose for 2 weeks. – Vancomycin 30 mg/kg/day in 2 divided doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Streptococci exhibit relative resistance to penicillin (MIC >0.12 μg/mL or ≤0.5 μg/mL) – Penicillin G 24 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks, in conjunction with gentamicin 3 mg/kg daily in a single dosage for 2 weeks. – Vancomycin 30 mg/kg daily in 2 split doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Penicillin-resistant streptococci (MIC >0.5 μg/mL) and enterococci: - Administer ampicillin 12 g/day in 6 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 4–6 weeks. - If allergic to ampicillin, use vancomycin 30 mg/kg/day in 2 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 6 weeks. • Methicillin-susceptible S. aureus: - Administer nafcillin 12 g/day IV in 4–6 divided doses for 6 weeks, optionally with gentamicin 3 mg/kg/day in 2 or 3 divided doses for 3–5 days. - If allergic to penicillin (without anaphylactoid reactions) but tolerant of cephalosporins, use cefazolin 6 g/day in 3 divided doses for 6 weeks. • Methicillin-resistant S. aureus: - Administer vancomycin 30 mg/kg/day in 2 divided doses for 6 weeks. • Target vancomycin trough level is 15–20 μg/mL. The aforementioned doses are predicated on standard renal function.
SUPPLEMENTARY THERAPY
Concerns for Referral Infective endocarditis of native valves and its complications can be fatal, and intricate management challenges frequently arise. A multidisciplinary approach involving cardiology, cardiovascular surgery, and infectious diseases is advised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Approximately 30–50% of individuals with NVIE receive a combination of antibacterial and surgical interventions for IE. Patients with decompensated heart failure must be promptly assessed for the possibility of early surgical intervention. The timing and urgency of valve replacement are tailored to each patient with NVIE. Other potential criteria for valve replacement encompass substantial valvular dysfunction, uncontrolled infection, multiple severe systemic emboli, insufficient antibiotic therapy (very resistant bacteria), and cardiac consequences such as perivalvular or myocardial abscesses.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Evaluate and stabilize the respiratory and cardiovascular systems in cases of suspected acute endocarditis. A prompt assessment of volume status and heart rhythm is necessary. Criteria for Admission Patients diagnosed with endocarditis require hospitalization for observation, commencement of intravenous antibiotics, and prompt evaluation. Criteria for Discharge Patients may be discharged when fevers have subsided for over 24 hours, vital signs are stable, and antibiotic and follow-up protocols are established.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
• In the immediate term, monitor patients diligently for complications or recurrence of endocarditis and adverse reactions associated with antimicrobial treatment. • Upon conclusion of therapy for infective endocarditis, a transthoracic echocardiogram is advised to establish a new baseline of valve and heart function. Patient Monitoring For patients undergoing intravenous antibiotic treatment, do weekly laboratory monitoring in accordance with established guidelines (http://www.idsociety.org/content.aspx?id=4428#opat) or the package insert.
INFORMATION FOR PATIENTS
Patients with infective endocarditis require knowledge regarding the significance of proper oral hygiene, methods to prevent infective endocarditis related to dental treatments, and the symptoms and signs of valve dysfunction.
PROGNOSIS • Congestive heart failure, infection extension beyond the valve annulus, concomitant diseases, advanced age, immunosuppression, and S. aureus infection are correlated with elevated mortality rates. Infection with Viridians group streptococci is linked to reduced mortality. • In-hospital mortality linked to infective endocarditis is reduced in drug abusers (10% vs to 17% in a recent research). The one-year mortality rate for all individuals with infective endocarditis is approximately 40%.
COMPLICATIONS
Congestive heart failure, cerebral emboli, stroke, renal infarctions, immune complex glomerulonephritis, mycotic aneurysm, meningitis, cerebritis, splenic infarctions, splenic abscess, and pulmonary embolism with or without infarction in right-sided endocarditis.
Endocarditis is an infection of the heart valves or endocardium caused by bacteria, fungus, or, less commonly, chlamydiae or rickettsiae. The mitral valve (41%) and aortic valve (38%) are the most frequently implicated in native valve infective endocarditis (NVIE). Tricuspid valve endocarditis is more prevalent among intravenous drug users. Pulmonic valve endocarditis is exceedingly uncommon. Several valves may be affected.
EPIDEMIOLOGY Incidence The prevalence of NVIE is between 1.7–6.2 cases per 100,000 patient-years. The incidence among intravenous drug users is estimated to be 1500–3300 cases per 100,000 patient-years.
Risk Factors
Predisposing factors encompass active intravenous drug use, a history of endocarditis, chronic intravascular access, the presence of an implantable cardiac device, congenital heart anomalies, a bicuspid aortic valve, rheumatic heart disease, and degenerative valvular disease.
GENERAL PREVENTION • Antibiotic prophylaxis for endocarditis is advised for people with the following conditions: – Prosthetic heart valve or valve repair utilizing prosthetic material – History of endocarditis - Congenital heart disease (unrepaired cyanotic CHD, treated CHD with residual abnormality) - Recipients of cardiac transplants with valvular heart disease
Prophylaxis is advised for dental procedures that include disruption of the oral mucosa and manipulation of the gingiva.
Prophylaxis is advisable for individuals with high-risk disorders, as previously mentioned, who are undergoing procedures involving the respiratory tract, skin, soft tissue, or muscle. Antibiotics for the prophylaxis of infective endocarditis are not advised for gastrointestinal or genitourinary surgeries.
Antibiotic protocols consist of a single dosage of amoxicillin 2 g or clindamycin 600 mg administered 30–60 minutes before the surgery.
ETIOLOGY • The predominant causal pathogens are gram-positive bacteria. Staphylococcus aureus has recently emerged as the predominant cause of NVIE. • The prevalent microbiological etiologies for NVIE are enumerated below: S. aureus (25–35%) — Coagulase-negative Staphylococcus (3–11%) - Viridans group streptococci (17–40 percent) - Streptococcus bovis (6 percent) - Additional streptococcus (6–19%) - Enterococcus species (10–18%) - HACEK (2–5 percent) Haemophilus species, Aggregatibacter actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella species. - Fungi/yeast (2–4 percent) • Culture-negative endocarditis (10%) The predominant cause is the administration of antibiotics within the preceding 7 days. – Alternative potential etiologies encompass slow-growing fastidious anaerobes, non-Candida fungal species, Bartonella spp., Coxiella burnetii (Q fever), Legionella spp., Tropheryma whippelii, Chlamydia spp., and Brucella spp. In intravenous drug users, polymicrobial non-valvular infective endocarditis (NVIE) is more prevalent.
DIAGNOSIS HISTORY
The clinical manifestations of NVIE exhibit significant variability, encompassing symptoms and indications attributable to the infected valve, embolic events, metastatic infection locations, and circulating immune complexes. Fever occurs in more than 90% of people with NVIE. General symptoms including weakness, chills, diaphoresis, anorexia, weight loss, nausea, and malaise may occur (3). • The revised Duke criteria are extensively utilized diagnostic standards for NVIE. • Principal criteria: – Microbiological evidence includes two sets of blood cultures positive for typical microorganisms such as Viridans streptococci, S. bovis, HACEK group, S. aureus; or community-acquired enterococci without a primary focus; or microorganisms consistent with infective endocarditis from persistently positive blood cultures; or a single positive blood culture for Coxiella burnetii or an anti-phase 1 IgG antibody titer exceeding 1:800. - Indications of endocardial involvement Favorable echocardiography (oscillating intracardiac mass on valve, abscess, or fresh partial dehiscence of prosthetic valve) New valvular regurgitation (deterioration or alteration of a preexisting murmur is inadequate)
• Minor criterion – Predisposition, preexisting cardiac disease, or intravenous drug use (IDU) – Pyrexia – Vascular manifestations: Significant artery emboli, septic pulmonary infarcts, mycotic aneurysms, cerebral hemorrhage, conjunctival hemorrhages, and Janeway lesions - Immunological manifestations: Glomerulonephritis, Osler's nodes, Roth's spots, and rheumatoid factor - Microbiological evidence: Positive blood culture; however, it does not fulfill a significant requirement as previously indicated, nor is there serological evidence of current infection with an organism consistent with infective endocarditis. • Definitive endocarditis (clinical criteria): 2 main criteria; or 1 major criterion in conjunction with 3 minor criteria; or 5 minor criteria • Conclusive endocarditis (pathological criteria): Microorganisms discovered through culture or pathological study of vegetation, embolized vegetation, or intracardiac abscess; or vegetation or intracardiac abscess exhibiting active endocarditis via histological evaluation. • Potential endocarditis: 1 major criterion + 1 minor criterion; or 3 minor criteria • Rejected: Definitive alternative diagnosis; symptom remission within 4 days of antibiotic treatment; absence of pathological evidence of infective endocarditis during surgery after fewer than 4 days of antibiotics; does not fulfill clinical criteria for probable infective endocarditis.
PHYSICAL EXAM • Clinical manifestations of infective endocarditis (IE) may present as a new or altered murmur in up to 85% of cases. • Petechiae occur in 20–40% of patients. Other cutaneous manifestations (Osler nodes, Janeway lesions, splinter hemorrhages) or Roth spots are observed in a minority of patients. A comprehensive examination is necessary to detect further infection sites (epidural abscess, psoas abscess, septic arthritis) or to discover embolic occurrences (stroke).
DIAGNOSTIC TESTS AND INTERPRETATION
Laboratory Preliminary laboratory assessments In cases of suspected NVIE, the initial laboratory assessment include a full blood count with differential, electrolytes, blood urea nitrogen, creatinine, liver function tests, several sets of blood cultures, urinalysis, and erythrocyte sedimentation rate (ESR). • Within the initial 24 hours, get a minimum of 3 sets of blood cultures. Obtain multiple sets of blood cultures prior to administering antibiotics to enhance the likelihood of identifying the causal bacteria. The initial two sets yield positive results in up to 90% of patients. Leukocytosis is prevalent. Over fifty percent of patients exhibit elevated serum inflammatory markers (ESR, C-reactive protein). The urinalysis often indicates the presence of proteinuria or microscopic hematuria.
Subsequent Actions & Unique Considerations
• In instances of culture-negative endocarditis, serological assessment for uncommon pathogens such as Q fever and Bartonella spp. may be warranted. • Acquire two sets of blood cultures every 24 to 48 hours until the endovascular infection has resolved. Imaging: Preliminary Approach Echocardiography is the preferred imaging modality and should be conducted promptly in all instances of suspected NVIE.
• The sensitivity of transthoracic echocardiography (TTE) for identifying left-sided vegetations varies between 40% and 63%, with a specificity of 91% to 98%. The sensitivity for right-sided lesions is elevated due to the proximity of the tricuspid and pulmonic valves to the chest wall. Transesophageal echocardiography may be constrained by obesity, chronic pulmonary illness, or thoracic wall deformities.
Transesophageal echocardiography (TEE) exhibits a sensitivity of 90–100% and a specificity of 91–98% in the identification of vegetations. TEE exhibits greater sensitivity than TTE in detecting valve perforation, pacemaker-associated infective endocarditis, and cardiac abscess.
Transesophageal echocardiography (TEE) is advised as the primary diagnostic test when transthoracic echocardiography (TTE) is anticipated to yield suboptimal results, there is a strong clinical suspicion of infective endocarditis (IE), or perivalvular extension is predicted. If the initial TTE is negative and there is a moderate to high clinical suspicion for IE, proceed with a TEE.
Subsequent Actions & Unique Considerations
Further imaging of the chest, abdomen, spine, or brain is necessary if emboli, abscesses, or mycotic aneurysms are suspected. Diagnostic Procedures and Additional Methods Acquire an EKG to determine a baseline heart rhythm and detect any conduction abnormalities. A repeat EKG is indicated for alterations in clinical status, bradycardia, syncope, or presyncope. Pathological Observations Histopathologic investigation reveals that vegetations comprise fibrin, platelet aggregates, and bacterial or fungal masses. PCR-based assays for detecting organisms such as Bartonella spp. and T. whippleii in blood or valvular tissue are accessible at some laboratories.
DIFFERENTIAL DIAGNOSIS
Noninfective endocarditis, alternative systemic infection, bacteremia, or fungemia absent of infective endocarditis.
Treatment Medication
Extended antibacterial treatment is necessary to infiltrate the vegetation and avert recurrence. Identifying the causative organism and its therapeutic susceptibilities is essential. Empiric therapy is predicated on patient risk factors for diverse infections, the severity of sickness, and local resistance patterns. • Below are the recommended treatment regimens for specific pathogens (1). • Penicillin-susceptible Viridans streptococci, S. bovis, or other streptococci (minimum inhibitory concentration ≤0.12 μg/mL) – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks. – Penicillin G 12–18 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily, in addition to gentamicin 3 mg/kg/day in a single dose for 2 weeks. – Vancomycin 30 mg/kg/day in 2 divided doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Streptococci exhibit relative resistance to penicillin (MIC >0.12 μg/mL or ≤0.5 μg/mL) – Penicillin G 24 million units per 24 hours (administered continuously or in 4–6 doses) or ceftriaxone 2 grams intravenously daily for 4 weeks, in conjunction with gentamicin 3 mg/kg daily in a single dosage for 2 weeks. – Vancomycin 30 mg/kg daily in 2 split doses for 4 weeks if there is intolerance or allergy to penicillin and ceftriaxone. • Penicillin-resistant streptococci (MIC >0.5 μg/mL) and enterococci: - Administer ampicillin 12 g/day in 6 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 4–6 weeks. - If allergic to ampicillin, use vancomycin 30 mg/kg/day in 2 divided doses plus gentamicin 3 mg/kg/day in 3 divided doses for 6 weeks. • Methicillin-susceptible S. aureus: - Administer nafcillin 12 g/day IV in 4–6 divided doses for 6 weeks, optionally with gentamicin 3 mg/kg/day in 2 or 3 divided doses for 3–5 days. - If allergic to penicillin (without anaphylactoid reactions) but tolerant of cephalosporins, use cefazolin 6 g/day in 3 divided doses for 6 weeks. • Methicillin-resistant S. aureus: - Administer vancomycin 30 mg/kg/day in 2 divided doses for 6 weeks. • Target vancomycin trough level is 15–20 μg/mL. The aforementioned doses are predicated on standard renal function.
SUPPLEMENTARY THERAPY
Concerns for Referral Infective endocarditis of native valves and its complications can be fatal, and intricate management challenges frequently arise. A multidisciplinary approach involving cardiology, cardiovascular surgery, and infectious diseases is advised.
OPERATIVE INTERVENTIONS/ADDITIONAL PROCEDURES
Approximately 30–50% of individuals with NVIE receive a combination of antibacterial and surgical interventions for IE. Patients with decompensated heart failure must be promptly assessed for the possibility of early surgical intervention. The timing and urgency of valve replacement are tailored to each patient with NVIE. Other potential criteria for valve replacement encompass substantial valvular dysfunction, uncontrolled infection, multiple severe systemic emboli, insufficient antibiotic therapy (very resistant bacteria), and cardiac consequences such as perivalvular or myocardial abscesses.
INPATIENT CONSIDERATIONS
Preliminary Stabilization Evaluate and stabilize the respiratory and cardiovascular systems in cases of suspected acute endocarditis. A prompt assessment of volume status and heart rhythm is necessary. Criteria for Admission Patients diagnosed with endocarditis require hospitalization for observation, commencement of intravenous antibiotics, and prompt evaluation. Criteria for Discharge Patients may be discharged when fevers have subsided for over 24 hours, vital signs are stable, and antibiotic and follow-up protocols are established.
CONTINUED MANAGEMENT POST-TREATMENT SUGGESTIONS
• In the immediate term, monitor patients diligently for complications or recurrence of endocarditis and adverse reactions associated with antimicrobial treatment. • Upon conclusion of therapy for infective endocarditis, a transthoracic echocardiogram is advised to establish a new baseline of valve and heart function. Patient Monitoring For patients undergoing intravenous antibiotic treatment, do weekly laboratory monitoring in accordance with established guidelines (http://www.idsociety.org/content.aspx?id=4428#opat) or the package insert.
INFORMATION FOR PATIENTS
Patients with infective endocarditis require knowledge regarding the significance of proper oral hygiene, methods to prevent infective endocarditis related to dental treatments, and the symptoms and signs of valve dysfunction.
PROGNOSIS • Congestive heart failure, infection extension beyond the valve annulus, concomitant diseases, advanced age, immunosuppression, and S. aureus infection are correlated with elevated mortality rates. Infection with Viridians group streptococci is linked to reduced mortality. • In-hospital mortality linked to infective endocarditis is reduced in drug abusers (10% vs to 17% in a recent research). The one-year mortality rate for all individuals with infective endocarditis is approximately 40%.
COMPLICATIONS
Congestive heart failure, cerebral emboli, stroke, renal infarctions, immune complex glomerulonephritis, mycotic aneurysm, meningitis, cerebritis, splenic infarctions, splenic abscess, and pulmonary embolism with or without infarction in right-sided endocarditis.
0 Comments
