- Published on
Pathology - Aortic dissection
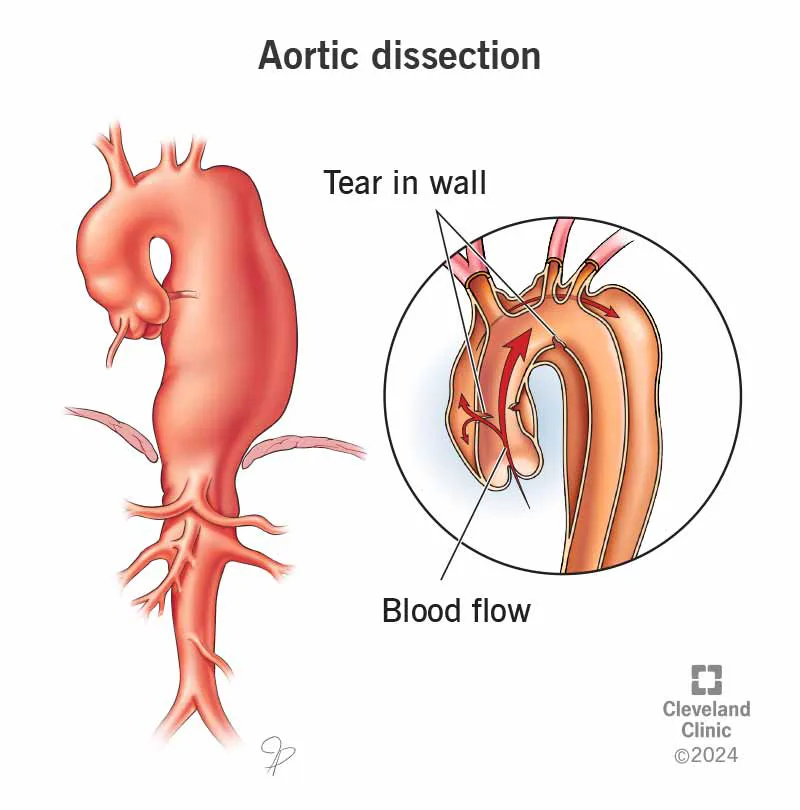
Definition: A rupture in the aortic wall allowing blood to flow through.
Epidemiology
• The majority of instances arise in persons aged 50 to 70 years. The 4:5 ratio equates to 2:1.
Aetiology
• The majority of instances are associated with hypertension. • Additional correlations include Marfan syndrome and congenital bicuspid aortic valve. The pathogenesis of aortic dissection in relation to hypertension remains contentious. • Suggested that the initial event is hemorrhage from a vasa vasorum into the media of the aorta. The intima experiences stress and ruptures, permitting blood to infiltrate the media and dissect along it. • Dissections may advance in the direction of the normal aortic blood flow (anterograde) or against it towards the aortic root (retrograde). • Dissections may re-enter the aortic lumen at a remote location, resulting in a 'double-barrelled' aorta, or may burst externally into the pericardial, pleural, or peritoneal cavities. Approximately 75% pertain to the ascending aorta or aortic arch (type A). Approximately 25% pertain to the descending aorta, without involvement of the ascending aorta or aortic arch (type B).
Presentation
• Intense, acute 'tearing' chest pain that may closely resemble acute myocardial infarction. • External rupture results in significant internal hemorrhage and shock.
Macroscopy
A rip is typically observable in the intima of the aorta at both the initiation and termination points of the dissection. • Should the dissection rupture externally, substantial volumes of blood clot will be present around the rupture site.
Histopathology
Microscopy offers limited insight into the reasons for dissection.
• The existence of significant degenerative alterations in the aorta wall of people under 60 years old suggests the potential for an inherited aortopathy, such as Marfan syndrome. Prognosis: Untreated cases have a significant death rate, with 50% succumbing within the first week.
• Treated cases exhibit favorable initial survival; but, they continue to be susceptible to mortality from rupture of the dissection or the emergence of a new dissection.
Definition: A rupture in the aortic wall allowing blood to flow through.
Epidemiology
• The majority of instances arise in persons aged 50 to 70 years. The 4:5 ratio equates to 2:1.
Aetiology
• The majority of instances are associated with hypertension. • Additional correlations include Marfan syndrome and congenital bicuspid aortic valve. The pathogenesis of aortic dissection in relation to hypertension remains contentious. • Suggested that the initial event is hemorrhage from a vasa vasorum into the media of the aorta. The intima experiences stress and ruptures, permitting blood to infiltrate the media and dissect along it. • Dissections may advance in the direction of the normal aortic blood flow (anterograde) or against it towards the aortic root (retrograde). • Dissections may re-enter the aortic lumen at a remote location, resulting in a 'double-barrelled' aorta, or may burst externally into the pericardial, pleural, or peritoneal cavities. Approximately 75% pertain to the ascending aorta or aortic arch (type A). Approximately 25% pertain to the descending aorta, without involvement of the ascending aorta or aortic arch (type B).
Presentation
• Intense, acute 'tearing' chest pain that may closely resemble acute myocardial infarction. • External rupture results in significant internal hemorrhage and shock.
Macroscopy
A rip is typically observable in the intima of the aorta at both the initiation and termination points of the dissection. • Should the dissection rupture externally, substantial volumes of blood clot will be present around the rupture site.
Histopathology
Microscopy offers limited insight into the reasons for dissection.
• The existence of significant degenerative alterations in the aorta wall of people under 60 years old suggests the potential for an inherited aortopathy, such as Marfan syndrome. Prognosis: Untreated cases have a significant death rate, with 50% succumbing within the first week.
• Treated cases exhibit favorable initial survival; but, they continue to be susceptible to mortality from rupture of the dissection or the emergence of a new dissection.
0 Comments
