- Published on
Pathology - Idiopathic Pulmonary Arterial Hypertension
The cause is unclear.
Primarily impacts females in the age range of 20 to 40.
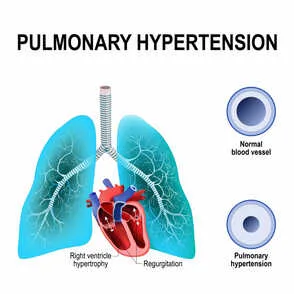
Lung: Medial hypertrophy and intimal fibrosis of the pulmonary arterioles.
Cardiac findings: Right ventricular hypertrophy and dilatation, observed in cases of acute cor pulmonale.
Patients exhibit symptoms of dyspnea, tiredness, chest discomfort, and exertional syncope.
The physical examination reveals a prominent P wave, an S3 sound on the right side, a noticeable enlargement of the right ventricle, and indications of right-sided heart failure such as swelling in the lower extremities, distended jugular veins, and fluid accumulation in the abdomen (ascites).
Complications including cyanosis, thrombosis, enlargement of the right ventricle, and cor pulmonale (heart failure on the right side due to pulmonary hypertension).
Treatment options for this condition include administering oxygen, using diuretics to address right heart failure, prescribing anticoagulant medications, utilizing phosphodiesterase 5 inhibitors, employing prostacyclin analogues, administering endothelin receptor blockers, and considering calcium channel blockers for individuals who have a good response to vasodilator challenge during right heart catheterization.
The prognosis is uncertain, with an estimated 3-year survival rate of approximately 60%.
Increased pressures in the pulmonary vasculature can also be linked to connective tissue disorders such as systemic lupus erythematosus (SLE) and CREST syndrome, congenital heart disease with left-to-right shunts, left heart failure, interstitial lung diseases such as chronic obstructive pulmonary disease (COPD), sarcoidosis, and chronic thromboembolic disease, obstructive sleep apnea (OSA), cirrhosis, or HIV infection.
The cause is unclear.
Primarily impacts females in the age range of 20 to 40.
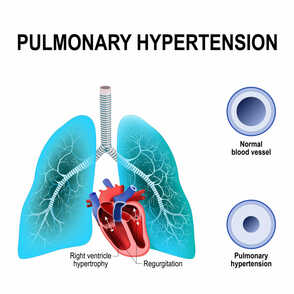
Lung: Medial hypertrophy and intimal fibrosis of the pulmonary arterioles.
Cardiac findings: Right ventricular hypertrophy and dilatation, observed in cases of acute cor pulmonale.
Patients exhibit symptoms of dyspnea, tiredness, chest discomfort, and exertional syncope.
The physical examination reveals a prominent P wave, an S3 sound on the right side, a noticeable enlargement of the right ventricle, and indications of right-sided heart failure such as swelling in the lower extremities, distended jugular veins, and fluid accumulation in the abdomen (ascites).
Complications including cyanosis, thrombosis, enlargement of the right ventricle, and cor pulmonale (heart failure on the right side due to pulmonary hypertension).
Treatment options for this condition include administering oxygen, using diuretics to address right heart failure, prescribing anticoagulant medications, utilizing phosphodiesterase 5 inhibitors, employing prostacyclin analogues, administering endothelin receptor blockers, and considering calcium channel blockers for individuals who have a good response to vasodilator challenge during right heart catheterization.
The prognosis is uncertain, with an estimated 3-year survival rate of approximately 60%.
Increased pressures in the pulmonary vasculature can also be linked to connective tissue disorders such as systemic lupus erythematosus (SLE) and CREST syndrome, congenital heart disease with left-to-right shunts, left heart failure, interstitial lung diseases such as chronic obstructive pulmonary disease (COPD), sarcoidosis, and chronic thromboembolic disease, obstructive sleep apnea (OSA), cirrhosis, or HIV infection.
0 Comments
