- Published on
Pathology - Respiratory Acidosis
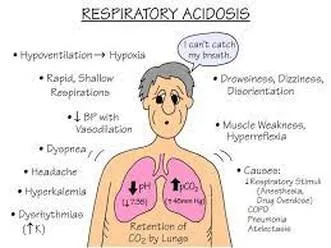
Resulting from acute lung disease such as ARDS and airway obstruction, chronic lung disease like COPD, CNS depression caused by opioids, sedatives, and narcotics, or weakened respiratory muscles due to conditions like ALS, kyphoscoliosis, MS, and polio.
Primary issue: Elevated Pco2 levels (hypercapnia) due to reduced alveolar ventilation.
Compensatory response: HCO3 increases due to enhanced renal HCO3 reabsorption triggered by low pH and high Pco2.
Symptoms include hypoventilation, drowsiness, cognitive impairment, muscle jerks with hand flapping, and indications of elevated pressure within the skull (such as swollen optic nerves and a condition resembling a brain tumor).
Laboratory results: pH decreased, Pco2 increased, HCO3 increased.
Address the root cause of acute respiratory acidosis and consider using short-term mechanical ventilation to assist with breathing.
No intervention required for persistent respiratory acidosis.
Acute compensation occurs with a 1 mEq/L increase in bicarbonate for every 10 mm Hg increase in partial pressure of carbon dioxide.
Chronic compensation occurs with a 3.5 mEq/L rise in HCO3 for every 10-mm Hg increase in PCO2.
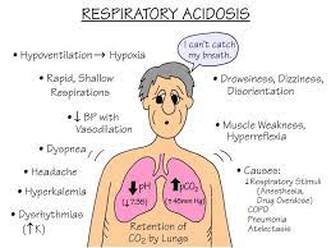
Resulting from acute lung disease such as ARDS and airway obstruction, chronic lung disease like COPD, CNS depression caused by opioids, sedatives, and narcotics, or weakened respiratory muscles due to conditions like ALS, kyphoscoliosis, MS, and polio.
Primary issue: Elevated Pco2 levels (hypercapnia) due to reduced alveolar ventilation.
Compensatory response: HCO3 increases due to enhanced renal HCO3 reabsorption triggered by low pH and high Pco2.
Symptoms include hypoventilation, drowsiness, cognitive impairment, muscle jerks with hand flapping, and indications of elevated pressure within the skull (such as swollen optic nerves and a condition resembling a brain tumor).
Laboratory results: pH decreased, Pco2 increased, HCO3 increased.
Address the root cause of acute respiratory acidosis and consider using short-term mechanical ventilation to assist with breathing.
No intervention required for persistent respiratory acidosis.
Acute compensation occurs with a 1 mEq/L increase in bicarbonate for every 10 mm Hg increase in partial pressure of carbon dioxide.
Chronic compensation occurs with a 3.5 mEq/L rise in HCO3 for every 10-mm Hg increase in PCO2.
0 Comments
