- Published on
Pathology - Systemic Lupus Erythematosus
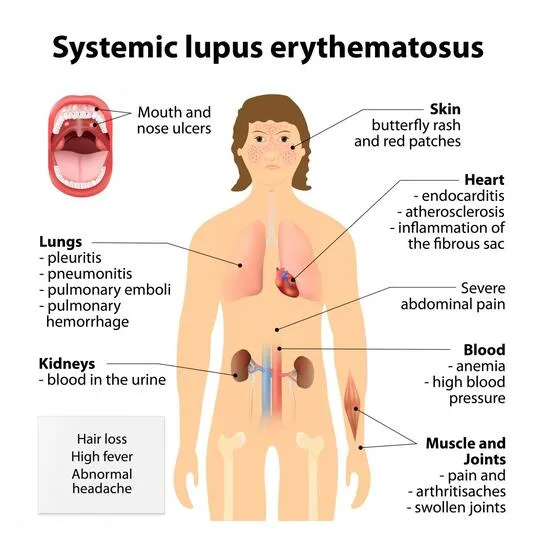
systemic lupus erythematosus (SLE) is an inflammatory autoimmune illness that affects numerous organ systems. The most common manifestations are skin rashes (as this patient’s characteristic malar butterfly rash), joint pains, and constitutional symptoms; however, renal, cardiac, pulmonary, and neurologic sequelae are also common (mnemonic – SOAP BRAIN MD: serositis, oral ulcers, arthritis, photosensitivity, blood disorders, renal dysfunction, ANA positive, immunologic phenomena, neurologic symptoms, malar rash and discoid rash). It is significantly more common in females and incidence is higher in the African American community. The pathogenesis of SLE likely starts with interaction of susceptibility genes and environmental variables resulting in aberrant immune responses.
Immune responses, which may differ between patients, result in the formation of antigens, autoantibodies and immune complexes (type III hypersensitivity response), which circulate and deposit in tissue, resulting in inflammatory processes and damage to multisystem organs. The presence of ANA is frequent in virtually all patients with SLE, but not specific for SLE. However, follow-up testing for anti-dsDNA or anti-Smith antibodies (anti-Sm) is specific for SLE and confirms the diagnosis. The most common cardiac symptom is pericarditis, which responds favorably to NSAIDs.
Headaches are very prevalent and periods of psychosis can occasionally occur, but must be separated from glucocorticoidinduced psychosis as immunosuppression is a cornerstone of care of SLE. Diffuse proliferative glomerulonephritis is the most prevalent renal manifestation and the major cause of morbidity and mortality. Anticardiolipin antibodies may also be present and will generate a false-positive in syphilis screening.
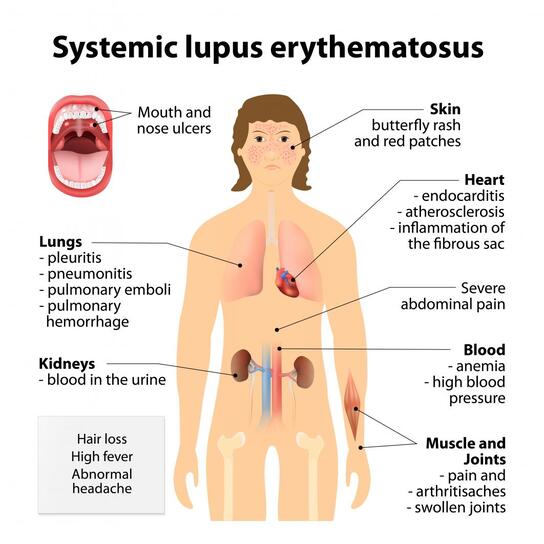
systemic lupus erythematosus (SLE) is an inflammatory autoimmune illness that affects numerous organ systems. The most common manifestations are skin rashes (as this patient’s characteristic malar butterfly rash), joint pains, and constitutional symptoms; however, renal, cardiac, pulmonary, and neurologic sequelae are also common (mnemonic – SOAP BRAIN MD: serositis, oral ulcers, arthritis, photosensitivity, blood disorders, renal dysfunction, ANA positive, immunologic phenomena, neurologic symptoms, malar rash and discoid rash). It is significantly more common in females and incidence is higher in the African American community. The pathogenesis of SLE likely starts with interaction of susceptibility genes and environmental variables resulting in aberrant immune responses.
Immune responses, which may differ between patients, result in the formation of antigens, autoantibodies and immune complexes (type III hypersensitivity response), which circulate and deposit in tissue, resulting in inflammatory processes and damage to multisystem organs. The presence of ANA is frequent in virtually all patients with SLE, but not specific for SLE. However, follow-up testing for anti-dsDNA or anti-Smith antibodies (anti-Sm) is specific for SLE and confirms the diagnosis. The most common cardiac symptom is pericarditis, which responds favorably to NSAIDs.
Headaches are very prevalent and periods of psychosis can occasionally occur, but must be separated from glucocorticoidinduced psychosis as immunosuppression is a cornerstone of care of SLE. Diffuse proliferative glomerulonephritis is the most prevalent renal manifestation and the major cause of morbidity and mortality. Anticardiolipin antibodies may also be present and will generate a false-positive in syphilis screening.
0 Comments
