- Published on
Surgery - Acute Pancreatitis
Introduction
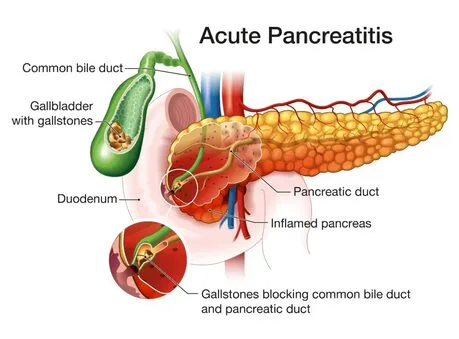
a pancreatic acute inflammatory condition that may or may not infiltrate distant organ systems or other local tissues. Mild: Linked to little organ dysfunction and a smooth recuperation. Severe: Linked to local consequences like necrosis, abscess, or pseudocyst, as well as organ failure (1992 Atlanta Classification).
Etiology
Insult causes tissue damage and inflammation by activating pancreatic proenzymes within the ducts and acini. Gallstones and alcohol are the most prevalent (80% instances). Infectious diseases (such as mumps, EBV, CMV, Coxsackie B, mycoplasma), drugs (such as steroids, azathioprine, thiazides, valproate), trauma, ERCP or abdominal surgery, hyperlipidemia, hyperparathyroidism, structural diseases (such as pancreatic divisum, annular pancreas), and idiopathic diseases are among the others.
Epidemiology
Typical. UK incidence per year is 10/10,000. Peak age is sixty years; gallstones are the main cause in women, whereas alcohol-induced illness is more common in men.
History
severe stomach or epigastric discomfort that radiates to the back and is made worse by moving or is eased by sitting forward. linked to nausea, vomiting, and anorexia. Alcohol consumption or gallstones may run in the family.
Examination
Fever and soreness in the stomach. tachycardia, tachypnea, and shock. #bowel noises as a result of ileus. If severe and hemorrhagic, consider either Cullen's sign (periumbilical bruises) or Turner's sign (flank bruises).
Investigations
Blood tests: high lipase, FBC (increased WCC), U&Es, elevated glucose, increased CRP, decreased Ca2+, elevated Amylase (typically >3 normal but does not correlate with severity), LFTs (may be deranged if gallstone pancreatitis or alcohol), and ABG (for hypoxia or metabolic acidosis). USS: For biliary dilatation or gallstones. Pleural effusion may be present in an erect CXR. primarily to rule out other explanations. AXR: To rule out alternative reasons for the acute abdomen. Maybe Psoas's shadow is gone. CT scan: In cases where there is doubt about the diagnosis, ongoing organ failure, or indications of necrosis, degeneration, or sepsis. Balthazar score: a scoring system that combines the degree of necrosis and the pancreatitis grade.
Management
Severity assessment: The following two measures have received the greatest validation: A combination of the modified Glasgow criteria and CRP (>220 mg/L) 2. The score on the APACHE-II (see to Gut 1998;42(Suppl 2):S1–S13). As an alternative, consider Ranson's requirements.†
Glasgow criteria modified (a score of three or above denotes a serious illness):
pO2 < 8 kPa (uR) in (P) > 16 mmol/L of urea (A) Over 55 years old (Enz) > 600 units/L (N) for LDH WCC > 15 109/L (A) < 32 g/L albumin (sugar) CA2+ < 2 mmol/L and glucose > 10 mmol/L †
Ranson's criteria (specific to pancreatitis caused by alcohol): Upon admission: hyperglycemia >11 mmol/L, AST >250, LDH >350, age >55, and WCC > 16109/L. pO2 < 8 kPa, Ca2Í < 2 mmol/L, urea > 16 mmol/L, base deficit > 4, haematocrit decline >10%, fluid sequestration > 600 ml within the first 48 hours.
Medical: NG tube if vomiting, urinary catheter, fluid and electrolyte replacement. management of blood sugar and analgesia. If severe, early HDU or critical care support. Enteral feeding, as opposed to parenteral feeding, has been proven in meta-analyses to reduce infective complications and mortality in cases of severe pancreatitis. It has not been demonstrated that preventive antibiotics lower mortality rates, unless infected pancreatic necrosis occurs. ERCP with sphincterotomy: Preferably within 72 hours for gallstone pancreatitis, cholangitis, jaundice, or dilated common bile duct. Within two weeks after admission, or on the same visit, all patients should receive definitive care for their gallstones. Early detection and treatment of complications: according to BSG guidelines, image-guided fine-needle aspiration for culture should be performed if there are persistent symptoms, more than 30% pancreatic necrosis, or evidence of sepsis. Surgical: A specialized facility should be used to address patients with necrotizing pancreatitis. Open necrosectomy or minimal access (draining and debridement of all necrotic tissue).
Complications
Local conditions include pancreatic necrosis, ascites, pseudo-aneurysm, abscess, pseudocyst (peripancreatic fluid accumulation lasting longer than four weeks), and venous thrombosis. Systemic: hypocalcemia, diabetes, ARDS, DIC, sepsis, renal failure, and hypocalcemia. Long-term: Diabetes and malabsorption together with chronic pancreatitis.
Prognosis
80% have a milder course with 5% mortality, while 20% have a severe fulminating course with significant mortality (infected pancreatic necrosis linked to 70% mortality).
Introduction
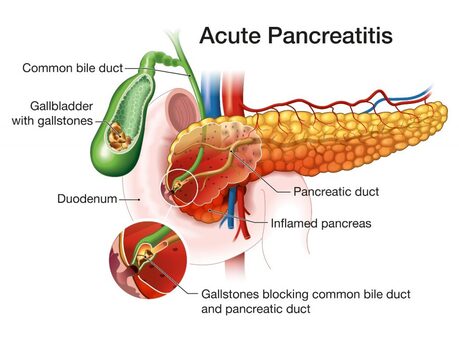
a pancreatic acute inflammatory condition that may or may not infiltrate distant organ systems or other local tissues. Mild: Linked to little organ dysfunction and a smooth recuperation. Severe: Linked to local consequences like necrosis, abscess, or pseudocyst, as well as organ failure (1992 Atlanta Classification).
Etiology
Insult causes tissue damage and inflammation by activating pancreatic proenzymes within the ducts and acini. Gallstones and alcohol are the most prevalent (80% instances). Infectious diseases (such as mumps, EBV, CMV, Coxsackie B, mycoplasma), drugs (such as steroids, azathioprine, thiazides, valproate), trauma, ERCP or abdominal surgery, hyperlipidemia, hyperparathyroidism, structural diseases (such as pancreatic divisum, annular pancreas), and idiopathic diseases are among the others.
Epidemiology
Typical. UK incidence per year is 10/10,000. Peak age is sixty years; gallstones are the main cause in women, whereas alcohol-induced illness is more common in men.
History
severe stomach or epigastric discomfort that radiates to the back and is made worse by moving or is eased by sitting forward. linked to nausea, vomiting, and anorexia. Alcohol consumption or gallstones may run in the family.
Examination
Fever and soreness in the stomach. tachycardia, tachypnea, and shock. #bowel noises as a result of ileus. If severe and hemorrhagic, consider either Cullen's sign (periumbilical bruises) or Turner's sign (flank bruises).
Investigations
Blood tests: high lipase, FBC (increased WCC), U&Es, elevated glucose, increased CRP, decreased Ca2+, elevated Amylase (typically >3 normal but does not correlate with severity), LFTs (may be deranged if gallstone pancreatitis or alcohol), and ABG (for hypoxia or metabolic acidosis). USS: For biliary dilatation or gallstones. Pleural effusion may be present in an erect CXR. primarily to rule out other explanations. AXR: To rule out alternative reasons for the acute abdomen. Maybe Psoas's shadow is gone. CT scan: In cases where there is doubt about the diagnosis, ongoing organ failure, or indications of necrosis, degeneration, or sepsis. Balthazar score: a scoring system that combines the degree of necrosis and the pancreatitis grade.
Management
Severity assessment: The following two measures have received the greatest validation: A combination of the modified Glasgow criteria and CRP (>220 mg/L) 2. The score on the APACHE-II (see to Gut 1998;42(Suppl 2):S1–S13). As an alternative, consider Ranson's requirements.†
Glasgow criteria modified (a score of three or above denotes a serious illness):
pO2 < 8 kPa (uR) in (P) > 16 mmol/L of urea (A) Over 55 years old (Enz) > 600 units/L (N) for LDH WCC > 15 109/L (A) < 32 g/L albumin (sugar) CA2+ < 2 mmol/L and glucose > 10 mmol/L †
Ranson's criteria (specific to pancreatitis caused by alcohol): Upon admission: hyperglycemia >11 mmol/L, AST >250, LDH >350, age >55, and WCC > 16109/L. pO2 < 8 kPa, Ca2Í < 2 mmol/L, urea > 16 mmol/L, base deficit > 4, haematocrit decline >10%, fluid sequestration > 600 ml within the first 48 hours.
Medical: NG tube if vomiting, urinary catheter, fluid and electrolyte replacement. management of blood sugar and analgesia. If severe, early HDU or critical care support. Enteral feeding, as opposed to parenteral feeding, has been proven in meta-analyses to reduce infective complications and mortality in cases of severe pancreatitis. It has not been demonstrated that preventive antibiotics lower mortality rates, unless infected pancreatic necrosis occurs. ERCP with sphincterotomy: Preferably within 72 hours for gallstone pancreatitis, cholangitis, jaundice, or dilated common bile duct. Within two weeks after admission, or on the same visit, all patients should receive definitive care for their gallstones. Early detection and treatment of complications: according to BSG guidelines, image-guided fine-needle aspiration for culture should be performed if there are persistent symptoms, more than 30% pancreatic necrosis, or evidence of sepsis. Surgical: A specialized facility should be used to address patients with necrotizing pancreatitis. Open necrosectomy or minimal access (draining and debridement of all necrotic tissue).
Complications
Local conditions include pancreatic necrosis, ascites, pseudo-aneurysm, abscess, pseudocyst (peripancreatic fluid accumulation lasting longer than four weeks), and venous thrombosis. Systemic: hypocalcemia, diabetes, ARDS, DIC, sepsis, renal failure, and hypocalcemia. Long-term: Diabetes and malabsorption together with chronic pancreatitis.
Prognosis
80% have a milder course with 5% mortality, while 20% have a severe fulminating course with significant mortality (infected pancreatic necrosis linked to 70% mortality).
0 Comments
