- Published on
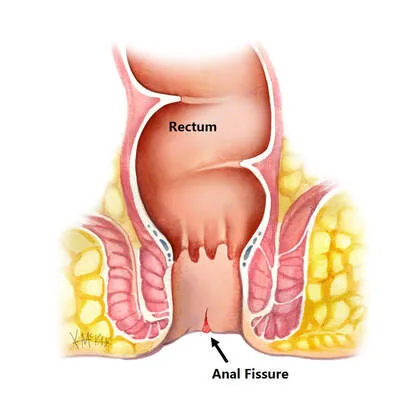
Surgery - Anal fissure
Introduction
a fissure-in-ano, or extended ulcer in the lower anal canal's long axis.
Etiology
traumatic Constipation: the posterior anal lining is torn by straining and passing hard stool. After childbirth, anterior fissures are more common in women because the anterior anal tissues are less supported by a compromised pelvic floor. Inflammatory: ulcerative colitis, Crohn's disease.
Epidemiology
Most prevalent in those under 40. First incidence: 350, gender equals male.
History
intense scorching discomfort when passing gas. Patients may try to prevent bowel motions as a result of pain that lasts for hours. Bleeding per rectum is a regular occurrence; on paper, it typically appears bright red and modest in volume. Pruritus ani may be present in conjunction.
Examination
A sentinel pile is often visible upon inspection. The distal portion of the fissure can be seen by gently pulling on the anal skin. Pain may prevent a digital rectal examination from being performed. It could be able to feel a hard, indurated ridge in chronic cracks.
Pathogenesis
The sphincter muscle beneath the anal mucosa experiences a mechanical tear, resulting in spasm. In addition to being excruciating, the spasm exacerbates the issue by tearing the margins of the rip apart. Poor healing is a result of reduced blood flow in the posterior midline of the anoderm compared to other areas of the anal canal.
Investigational studies
A diagnosis may be reached by investigation and history. The goal of the investigation is to rule out other illnesses such rectal cancer and inflammatory bowel disease.
If treatment is not working, an examination under anesthesia is necessary to rule out additional pathologies.
Management
Conservative: Make sure the stools are easily passed and soft.
Medical: Diltiazem or topical GTN. They promote wound healing by decreasing sphincter spasm and boosting local blood flow.
Surgery: Traditionally, a partial lateral division of the internal sphincter is done during a lateral internal sphincterotomy to lessen spasm and facilitate posterior midline wound healing. The same result has been achieved more recently by paralyzing a portion of the internal sphincter with botulinum toxin, or Botox. flap of anal advancement in persistent fissures.
Complications
Both chronic pain and chronic fissure.
Recurrence of bleeding and faecal incontinence are among the surgical complications.
Prognosis
Recurrence is common, occurring in fewer than 10% of patients after lateral sphincterotomy and up to 50% of individuals treated with topical nitrates.
Introduction
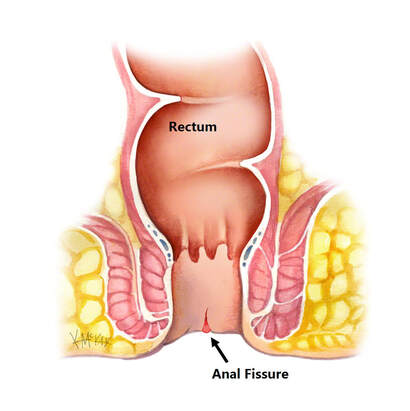
a fissure-in-ano, or extended ulcer in the lower anal canal's long axis.
Etiology
traumatic Constipation: the posterior anal lining is torn by straining and passing hard stool. After childbirth, anterior fissures are more common in women because the anterior anal tissues are less supported by a compromised pelvic floor. Inflammatory: ulcerative colitis, Crohn's disease.
Epidemiology
Most prevalent in those under 40. First incidence: 350, gender equals male.
History
intense scorching discomfort when passing gas. Patients may try to prevent bowel motions as a result of pain that lasts for hours. Bleeding per rectum is a regular occurrence; on paper, it typically appears bright red and modest in volume. Pruritus ani may be present in conjunction.
Examination
A sentinel pile is often visible upon inspection. The distal portion of the fissure can be seen by gently pulling on the anal skin. Pain may prevent a digital rectal examination from being performed. It could be able to feel a hard, indurated ridge in chronic cracks.
Pathogenesis
The sphincter muscle beneath the anal mucosa experiences a mechanical tear, resulting in spasm. In addition to being excruciating, the spasm exacerbates the issue by tearing the margins of the rip apart. Poor healing is a result of reduced blood flow in the posterior midline of the anoderm compared to other areas of the anal canal.
Investigational studies
A diagnosis may be reached by investigation and history. The goal of the investigation is to rule out other illnesses such rectal cancer and inflammatory bowel disease.
If treatment is not working, an examination under anesthesia is necessary to rule out additional pathologies.
Management
Conservative: Make sure the stools are easily passed and soft.
Medical: Diltiazem or topical GTN. They promote wound healing by decreasing sphincter spasm and boosting local blood flow.
Surgery: Traditionally, a partial lateral division of the internal sphincter is done during a lateral internal sphincterotomy to lessen spasm and facilitate posterior midline wound healing. The same result has been achieved more recently by paralyzing a portion of the internal sphincter with botulinum toxin, or Botox. flap of anal advancement in persistent fissures.
Complications
Both chronic pain and chronic fissure.
Recurrence of bleeding and faecal incontinence are among the surgical complications.
Prognosis
Recurrence is common, occurring in fewer than 10% of patients after lateral sphincterotomy and up to 50% of individuals treated with topical nitrates.
0 Comments
