- Published on
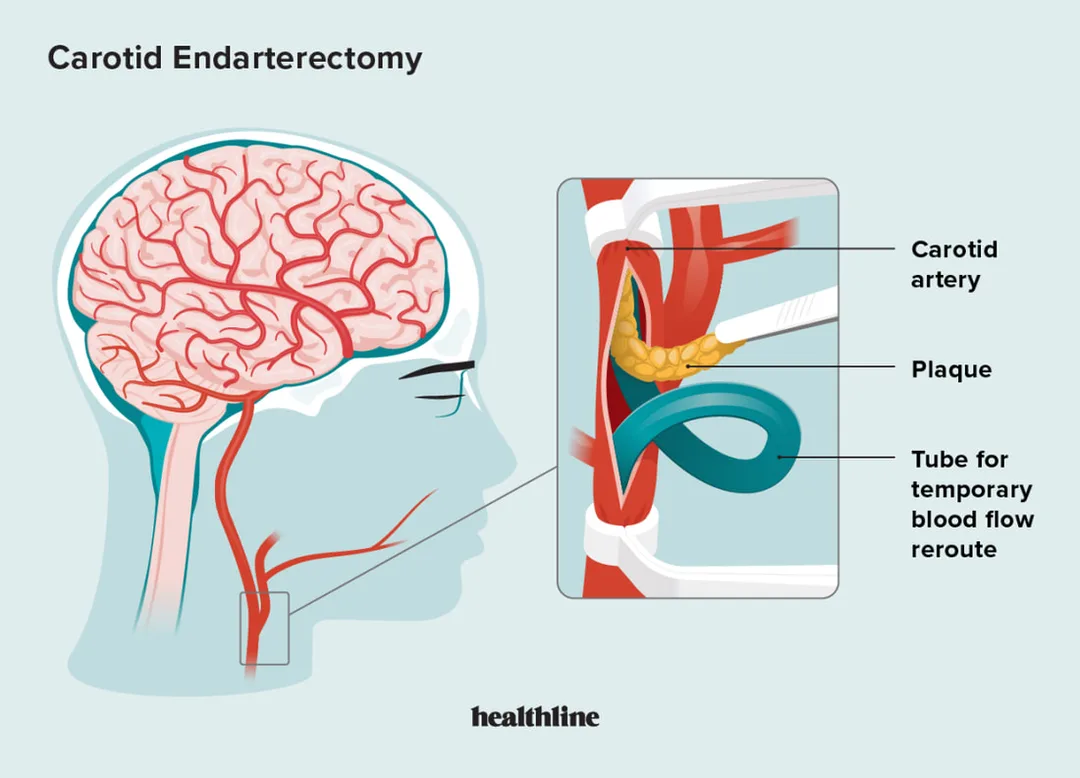
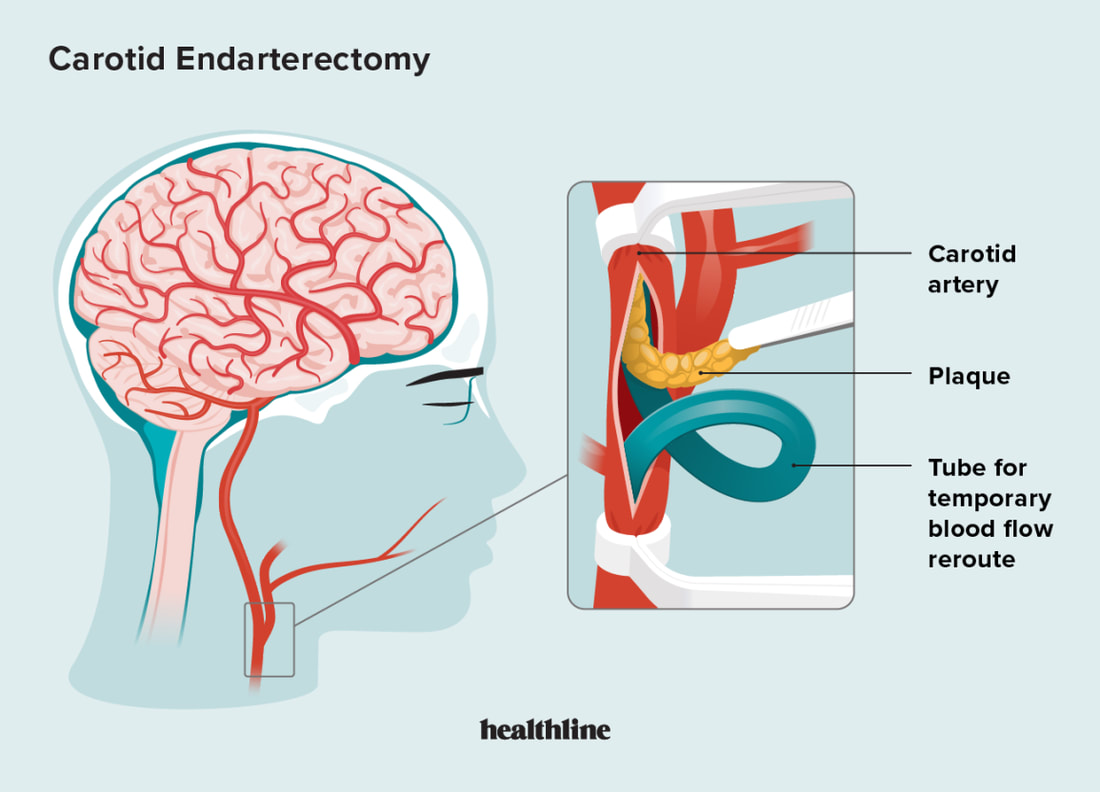
Surgery - Carotid Endarterectomy
Indications
More than 70–99% symptomatic carotid stenosis (Absolute).
(Relative) Symptomatic stenosis >50%, ideally within two weeks of the patient's last symptoms, if the perioperative stroke/death rate is <6%.
(Relative) Asymptomatic men under 75 years old with 70–99% stenosis, if there is less than 3% chance of stroke or death after surgery.
Anatomy
The left common carotid artery originates from the aortic arch, while the right common carotid arises at the innominate artery's bifurcation behind the right sternoclavicular joint. The external carotid, which supplies the outside skull, face, and most of the neck, and the internal carotid, which has no branches in the neck, split the common carotid (level can vary, C4). A number of nerves are at risk during carotid dissection: (1) the mandibular branch of the facial nerve; (2) the hypoglossal nerve courses medially across the anterior aspect of the external and internal carotids to supply the tongue; and (3) the vagus nerve exits the jugular foramen and courses caudally in the carotid sheath, putting its superior and recurrent laryngeal branches at risk. The carotids are located next to the internal jugular vein.
Investigations
Prior to surgery: The carotid duplex is the initial test used to measure the degree of stenosis. Digital subtraction angiography and CT and MR angiography are other imaging modalities. As concomitant coronary artery disease is frequently present, a coronary angiography, echocardiography, and ECG are recommended. Aspirin and statins ought to be administered prior to, during, and after surgery.
Post-operative care should include regular neurologic evaluation, hemodynamic testing, and electrocardiogram monitoring. Keep an eye out for any bleeding that could endanger the airway.
Aftercare: Controlling cardiovascular risk factors. A carotid duplex can be used to check for contralateral stenosis or restenosis at different intervals.
Procedure
Anaesthesia: Both local and general anesthesia are safe for use (GALA trial). The benefit of the latter is that it does not require sophisticated monitoring and allows for a direct assessment of the patient's neurological condition. Under GA, transcranial Doppler, stump pressures, and EEG can all be used to measure cerebral blood flow.
Incision: The anterior border of the sternocleidomastoid muscle is incised obliquely. Carotid bifurcation localization or preoperative labeling can be useful.
The common, internal, and exterior carotid arteries are dissected: vascular manipulation and dissection done carefully to prevent embolism. preventing damage to the hypoglossal and vagus nerves, as well as the internal jugular vein and its tributaries. Changes in blood pressure can be caused via carotid body manipulation.
A longitudinal arteriotomy is done from the common into the internal carotid after the arteries are constricted after heparinization. A shunt is installed if necessary, such as the Pruitt-Inahara or Javid shunts.
Plaque removal: Using a suitable tool, such as a Watson Cheyne dissector, the plaque is pulled away from the arterial wall, being careful not to cause intimal flaps. Debris and clots are then flushed out with heparinized saline.
Closure: If a shunt was inserted, it is removed and the arteriotomy is sealed using prolene suture. A prosthesis or vein patch can be used to close the arteriotomy directly.Adrain is frequently left in place till the next day.
Complications
cardiac ischaemia, hemorrhage, hypertension, hypotension, perioperative stroke, and nerve injury (2–7%, mandibular branch of the facial nerve, recurrent laryngeal nerve, or hypoglossal nerves). 1.8% to 0.5% is the perioperative mortality rate.
Indications
More than 70–99% symptomatic carotid stenosis (Absolute).
(Relative) Symptomatic stenosis >50%, ideally within two weeks of the patient's last symptoms, if the perioperative stroke/death rate is <6%.
(Relative) Asymptomatic men under 75 years old with 70–99% stenosis, if there is less than 3% chance of stroke or death after surgery.
Anatomy
The left common carotid artery originates from the aortic arch, while the right common carotid arises at the innominate artery's bifurcation behind the right sternoclavicular joint. The external carotid, which supplies the outside skull, face, and most of the neck, and the internal carotid, which has no branches in the neck, split the common carotid (level can vary, C4). A number of nerves are at risk during carotid dissection: (1) the mandibular branch of the facial nerve; (2) the hypoglossal nerve courses medially across the anterior aspect of the external and internal carotids to supply the tongue; and (3) the vagus nerve exits the jugular foramen and courses caudally in the carotid sheath, putting its superior and recurrent laryngeal branches at risk. The carotids are located next to the internal jugular vein.
Investigations
Prior to surgery: The carotid duplex is the initial test used to measure the degree of stenosis. Digital subtraction angiography and CT and MR angiography are other imaging modalities. As concomitant coronary artery disease is frequently present, a coronary angiography, echocardiography, and ECG are recommended. Aspirin and statins ought to be administered prior to, during, and after surgery.
Post-operative care should include regular neurologic evaluation, hemodynamic testing, and electrocardiogram monitoring. Keep an eye out for any bleeding that could endanger the airway.
Aftercare: Controlling cardiovascular risk factors. A carotid duplex can be used to check for contralateral stenosis or restenosis at different intervals.
Procedure
Anaesthesia: Both local and general anesthesia are safe for use (GALA trial). The benefit of the latter is that it does not require sophisticated monitoring and allows for a direct assessment of the patient's neurological condition. Under GA, transcranial Doppler, stump pressures, and EEG can all be used to measure cerebral blood flow.
Incision: The anterior border of the sternocleidomastoid muscle is incised obliquely. Carotid bifurcation localization or preoperative labeling can be useful.
The common, internal, and exterior carotid arteries are dissected: vascular manipulation and dissection done carefully to prevent embolism. preventing damage to the hypoglossal and vagus nerves, as well as the internal jugular vein and its tributaries. Changes in blood pressure can be caused via carotid body manipulation.
A longitudinal arteriotomy is done from the common into the internal carotid after the arteries are constricted after heparinization. A shunt is installed if necessary, such as the Pruitt-Inahara or Javid shunts.
Plaque removal: Using a suitable tool, such as a Watson Cheyne dissector, the plaque is pulled away from the arterial wall, being careful not to cause intimal flaps. Debris and clots are then flushed out with heparinized saline.
Closure: If a shunt was inserted, it is removed and the arteriotomy is sealed using prolene suture. A prosthesis or vein patch can be used to close the arteriotomy directly.Adrain is frequently left in place till the next day.
Complications
cardiac ischaemia, hemorrhage, hypertension, hypotension, perioperative stroke, and nerve injury (2–7%, mandibular branch of the facial nerve, recurrent laryngeal nerve, or hypoglossal nerves). 1.8% to 0.5% is the perioperative mortality rate.
0 Comments
