- Published on
Surgery - intestinal Obstruction
Introduction
obstruction of the bowel's regular flow of contents. categorized by site: simple or strangulated, partial or whole, small or big bowel (SBO or LBO).
Etiology
Bowel blockage without vascular impairment is known as simple obstruction. Bowel above the obstruction dilates with gas and fluid, whereas the intestine distal to the obstruction quickly empties and collapses. Distension impairs the blood supply to the intestinal wall, increasing the risk of bowel perforation and mucosal ulcers.
Strangulated obstruction: When the blood supply to the afflicted segment is cut off, the usual mucosal barrier is weakened, bacteria can penetrate into the peritoneal cavity and cause peritonitis. If the intestine is left untreated, it can develop gangrene and burst.
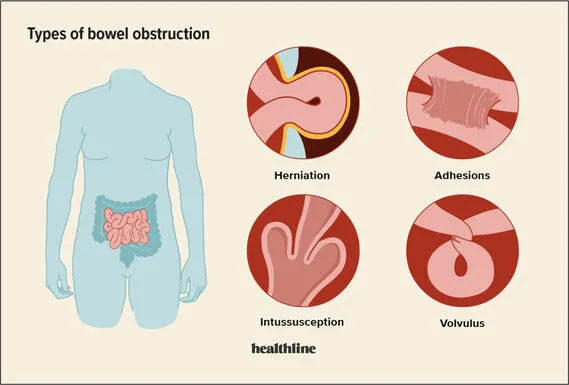
The obstruction's cause is divided into the following categories. Extramural: External compression caused by a space-occupying lesion, bands, hernias, volvulus.
Intramural: Tumors, inflammatory strictures (such as those associated with diverticulitis or Crohn's disease), and intussusception.
Intraluminal: fecal impaction/constipation, worm infestation, pedunculated tumors, foreign objects (bezoars, gallstones), etc.
Epidemiology
Typical. more prevalent in older people as a result of an increase in adhesions, hernias, and cancer.
History
Severe, clenching, colicky pain in the lower abdomen (large intestine) or central abdomen (small intestine), that sometimes eases.
stomach distension.
Greenish-stained vomit that frequently comes up, either early in SBO or late with faeculent vomiting in distal SBO or LBO.
total constipation, defined as the inability to move gas or stool.
Examination
stomach distension accompanied by widespread soreness.
Peristalsis is observable.
bowel noises, or "tinkling" as they are called. Guarding and rebound indicate the development of peritonitis, and there may not be any bowel sounds.
Check for any hernias. Adhesions are a potential with any abdominal scarring.
Look for any masses in the abdomen (such as those caused by faecal impaction, cancer, intussusception, or a mass in the Douglas pouch).
Investigational studies
Blood: ABG: Lactic acidosis may indicate imminent perforation and intestinal ischaemia.
A big bowel cancer may be indicated by microcytic anemia. For electrolyte imbalance and dehydration brought on by vomiting, use urea and electrolytes.
AXR: Aids in blockage localization and diagnosis. SBO is suggested by the central ladder pattern, which consists of dilated loops with valvulae conniventes spanning the entire bowel's breadth. LBO is suggested if the distended bowel is more peripheral and has haustrations that do not overlap the intestinal breadth. One can see the fluid levels.
Raise the CXR to rule out perforation.
Water-soluble contrast enema: Helps identify the obstruction's location in LBO.
Water-soluble follow-through for contrast: to look into the obstruction's level.
CT scan: Enables care to be planned in accordance with the cause and/or degree of obstruction, as well as its level, prior to surgery. It can show a perforation or metastases.
Management
General: Inserting a nasogastric tube, closely monitoring vital signs, fluid balance, urine output, and clinical condition; resuscitation with IV fluids and electrolyte supplementation. Gastrografin follow-through for adhesive blockage may have therapeutic as well as diagnostic purposes. It is believed that the hyperosmotic contrast will lessen intestinal wall oedema and ease the obstruction. An early surgery can be scheduled if the study points to a different diagnosis.
Acute obstructions may resolve with conservative therapy; if not, or if problems appear, surgical surgery should be performed.
Surgical: To treat the cause, a laparoscopy or laparotomy.may entail band division, adhesiolysis, or bowel resection with or without a stoma. In small-bowel resection, primary anastomosis; in large-bowel resection, Hartmann's operation or hemicolectomy with non-functioning stoma. Post-operative care in an ICU or HDU may be necessary.
Endoscopic: Stenting obstructing colonic tumors can be done as a palliative measure or as a preoperative measure to prevent the need for urgent surgery. Endoscopic treatment options for obstruction resulting from a sigmoid volvulus include the use of a flexible sigmoidoscope and the insertion of a flatus tube.
Complications
diarrhea, intestinal perforation, toxaemia, and necrosis of the ischemic colon wall.
Prognosis
Variable. based on the patients' overall health and the frequency of problems.
Introduction
obstruction of the bowel's regular flow of contents. categorized by site: simple or strangulated, partial or whole, small or big bowel (SBO or LBO).
Etiology
Bowel blockage without vascular impairment is known as simple obstruction. Bowel above the obstruction dilates with gas and fluid, whereas the intestine distal to the obstruction quickly empties and collapses. Distension impairs the blood supply to the intestinal wall, increasing the risk of bowel perforation and mucosal ulcers.
Strangulated obstruction: When the blood supply to the afflicted segment is cut off, the usual mucosal barrier is weakened, bacteria can penetrate into the peritoneal cavity and cause peritonitis. If the intestine is left untreated, it can develop gangrene and burst.
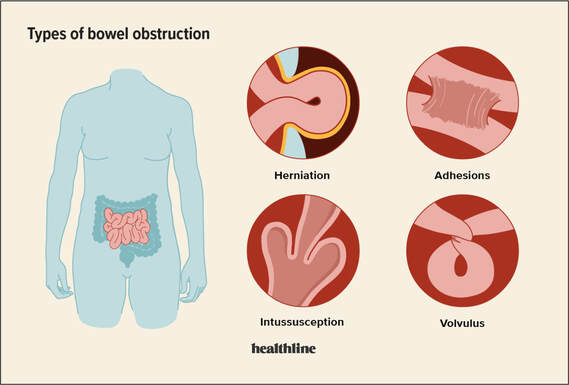
The obstruction's cause is divided into the following categories. Extramural: External compression caused by a space-occupying lesion, bands, hernias, volvulus.
Intramural: Tumors, inflammatory strictures (such as those associated with diverticulitis or Crohn's disease), and intussusception.
Intraluminal: fecal impaction/constipation, worm infestation, pedunculated tumors, foreign objects (bezoars, gallstones), etc.
Epidemiology
Typical. more prevalent in older people as a result of an increase in adhesions, hernias, and cancer.
History
Severe, clenching, colicky pain in the lower abdomen (large intestine) or central abdomen (small intestine), that sometimes eases.
stomach distension.
Greenish-stained vomit that frequently comes up, either early in SBO or late with faeculent vomiting in distal SBO or LBO.
total constipation, defined as the inability to move gas or stool.
Examination
stomach distension accompanied by widespread soreness.
Peristalsis is observable.
bowel noises, or "tinkling" as they are called. Guarding and rebound indicate the development of peritonitis, and there may not be any bowel sounds.
Check for any hernias. Adhesions are a potential with any abdominal scarring.
Look for any masses in the abdomen (such as those caused by faecal impaction, cancer, intussusception, or a mass in the Douglas pouch).
Investigational studies
Blood: ABG: Lactic acidosis may indicate imminent perforation and intestinal ischaemia.
A big bowel cancer may be indicated by microcytic anemia. For electrolyte imbalance and dehydration brought on by vomiting, use urea and electrolytes.
AXR: Aids in blockage localization and diagnosis. SBO is suggested by the central ladder pattern, which consists of dilated loops with valvulae conniventes spanning the entire bowel's breadth. LBO is suggested if the distended bowel is more peripheral and has haustrations that do not overlap the intestinal breadth. One can see the fluid levels.
Raise the CXR to rule out perforation.
Water-soluble contrast enema: Helps identify the obstruction's location in LBO.
Water-soluble follow-through for contrast: to look into the obstruction's level.
CT scan: Enables care to be planned in accordance with the cause and/or degree of obstruction, as well as its level, prior to surgery. It can show a perforation or metastases.
Management
General: Inserting a nasogastric tube, closely monitoring vital signs, fluid balance, urine output, and clinical condition; resuscitation with IV fluids and electrolyte supplementation. Gastrografin follow-through for adhesive blockage may have therapeutic as well as diagnostic purposes. It is believed that the hyperosmotic contrast will lessen intestinal wall oedema and ease the obstruction. An early surgery can be scheduled if the study points to a different diagnosis.
Acute obstructions may resolve with conservative therapy; if not, or if problems appear, surgical surgery should be performed.
Surgical: To treat the cause, a laparoscopy or laparotomy.may entail band division, adhesiolysis, or bowel resection with or without a stoma. In small-bowel resection, primary anastomosis; in large-bowel resection, Hartmann's operation or hemicolectomy with non-functioning stoma. Post-operative care in an ICU or HDU may be necessary.
Endoscopic: Stenting obstructing colonic tumors can be done as a palliative measure or as a preoperative measure to prevent the need for urgent surgery. Endoscopic treatment options for obstruction resulting from a sigmoid volvulus include the use of a flexible sigmoidoscope and the insertion of a flatus tube.
Complications
diarrhea, intestinal perforation, toxaemia, and necrosis of the ischemic colon wall.
Prognosis
Variable. based on the patients' overall health and the frequency of problems.
0 Comments
