- Published on
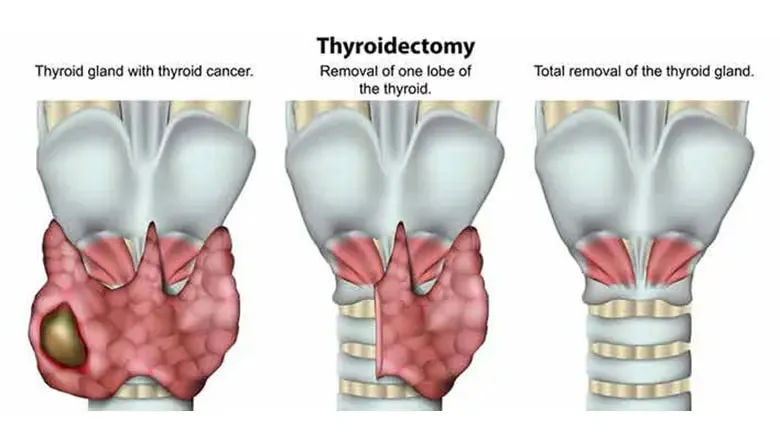
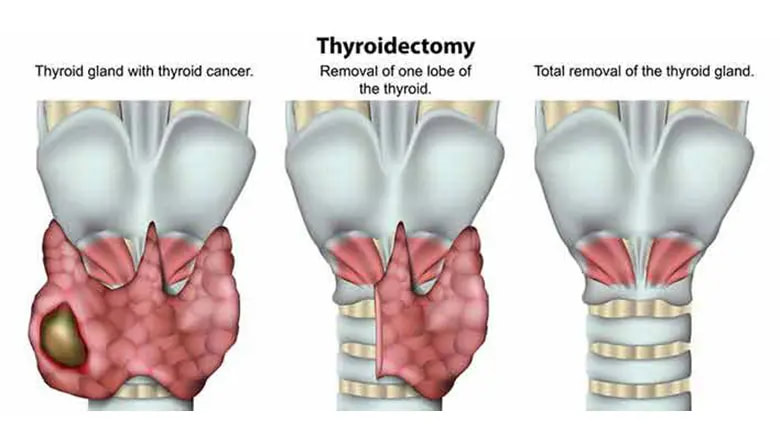
Surgery - Thyroidectomy
Indications
When a FNA is unclear, a thyroid mass can be definitively diagnosed as either benign or malignant. Symptomatic goiters (cosmesis or pressure effects). as a treatment for toxic nodular goitre, graves disease, or thyrotoxicosis.
Anatomy
The thyroid isthmus, which sits above the second and third tracheal rings, connects the thyroid gland's two lobes. The gland is located deep to the strap muscles and is encased in the pretracheal fascia.
Vascular: The gland is supplied by the lower thyroid artery from the subclavian thyrocervical trunk, the superior thyroid artery from the external carotid, and occasionally the thyroidea ima artery from the brachiocephalic or aortic arch. The internal jugular vein receives venous drainage from the superior, middle, and inferior thyroid veins.
Investigations
Bloods: Complete blood count, renal function, calcium, and thyroid function tests. Patients with hypo- or hyperthyroidism should receive medical treatment prior to surgery.
Ultrasound: To identify a goiter or characterize a lesion. To evaluate tracheal constriction and retrosternal extension, use a CT scan. scintigraphy in nuclear medicine, where applicable.
FNA or biopsy guided by ultrasound: For cytological diagnosis.
Indirect laryngoscopy: To evaluate vocal cord health prior to surgery.
After surgery: Continue to monitor and replace calcium as needed. replacement of thyroid.
Procedure
Head up, neck stretched, in a reverse Trendelenburg position.
Incision: Two fingerbreadths above the suprasternal notch, in the skin crease collar.
To prevent harm to the anterior jugular veins, subcutaneous tissue and platysma are split, and flaps are elevated superiorly to the thyroid cartilage and inferiorly to the sternum.
Thyroid exposure and mobilization: The subplatysma flaps are retracted using a Jolls retractor. To reveal the thyroid gland underneath, the midline raphe is divided, separating the strap muscles. The thyroid gland is visible. Carefully ligating the middle thyroid vein(s) involves locating and avoiding parathyroids, which are little tan glands. The vessels in the superior pole are separated, snipped off from the gland, and double ligated. The tracheooesophageal groove contains the recurrent laryngeal nerve, which needs to be properly identified and protected to prevent diathermy in the area around it. Though it normally runs between or in front of the lower pole vessels, it is usually deep. The thyroid is properly ligated in close proximity to the inferior thyroid vascular pedicle. Absorbable sutures are used to oversew the isthmus in cases of hemithyroidectomy.
Close: Maintaining proper hemostasis is crucial. A lot of surgeons choose to leave a vacuum drain in place.
Three layers make up the closure: the skin, platysma, subcutaneous tissue, and the opposition of the strap muscles.
Complications
Bleeding, hypocalcemia, hypothyroidism, wound infection, vocal abnormalities due to recurrent laryngeal nerve injury, breathing difficulties brought on by a hemorrhage compressing the trachea or bilaterally.
Indications
When a FNA is unclear, a thyroid mass can be definitively diagnosed as either benign or malignant. Symptomatic goiters (cosmesis or pressure effects). as a treatment for toxic nodular goitre, graves disease, or thyrotoxicosis.
Anatomy
The thyroid isthmus, which sits above the second and third tracheal rings, connects the thyroid gland's two lobes. The gland is located deep to the strap muscles and is encased in the pretracheal fascia.
Vascular: The gland is supplied by the lower thyroid artery from the subclavian thyrocervical trunk, the superior thyroid artery from the external carotid, and occasionally the thyroidea ima artery from the brachiocephalic or aortic arch. The internal jugular vein receives venous drainage from the superior, middle, and inferior thyroid veins.
Investigations
Bloods: Complete blood count, renal function, calcium, and thyroid function tests. Patients with hypo- or hyperthyroidism should receive medical treatment prior to surgery.
Ultrasound: To identify a goiter or characterize a lesion. To evaluate tracheal constriction and retrosternal extension, use a CT scan. scintigraphy in nuclear medicine, where applicable.
FNA or biopsy guided by ultrasound: For cytological diagnosis.
Indirect laryngoscopy: To evaluate vocal cord health prior to surgery.
After surgery: Continue to monitor and replace calcium as needed. replacement of thyroid.
Procedure
Head up, neck stretched, in a reverse Trendelenburg position.
Incision: Two fingerbreadths above the suprasternal notch, in the skin crease collar.
To prevent harm to the anterior jugular veins, subcutaneous tissue and platysma are split, and flaps are elevated superiorly to the thyroid cartilage and inferiorly to the sternum.
Thyroid exposure and mobilization: The subplatysma flaps are retracted using a Jolls retractor. To reveal the thyroid gland underneath, the midline raphe is divided, separating the strap muscles. The thyroid gland is visible. Carefully ligating the middle thyroid vein(s) involves locating and avoiding parathyroids, which are little tan glands. The vessels in the superior pole are separated, snipped off from the gland, and double ligated. The tracheooesophageal groove contains the recurrent laryngeal nerve, which needs to be properly identified and protected to prevent diathermy in the area around it. Though it normally runs between or in front of the lower pole vessels, it is usually deep. The thyroid is properly ligated in close proximity to the inferior thyroid vascular pedicle. Absorbable sutures are used to oversew the isthmus in cases of hemithyroidectomy.
Close: Maintaining proper hemostasis is crucial. A lot of surgeons choose to leave a vacuum drain in place.
Three layers make up the closure: the skin, platysma, subcutaneous tissue, and the opposition of the strap muscles.
Complications
Bleeding, hypocalcemia, hypothyroidism, wound infection, vocal abnormalities due to recurrent laryngeal nerve injury, breathing difficulties brought on by a hemorrhage compressing the trachea or bilaterally.
0 Comments
