- Published on
Surgery - Upper Gastrointestinal Hemorrhage
Introduction
bleeding that originates from the upper portion of the gastrointestinal tract, or close to the Treitz ligament.
Etiology
Acute or chronic conditions include the following: 50% of instances of stomach and duodenal ulcers; acute erosive gastritis; oesophagitis or duodenitis; oesophageal or gastric varices; Mallory-Weiss tear; gastric angiogenesis or Dieulafoy's malformation; tumors or, less frequently, haemobilia; aorto-enteric fistula; or amyloidosis.
Risk Factors
NSAIDs, steroids, and Helicobacter pylori are risk factors for the onset or aggravation of erosions and ulcers. Stress ulcers 2 in burn patients and Cushing's ulcer in head injuries are related to shock and decreased splanchnic perfusion. Gastric erosions can be triggered by binges of alcohol.
Vomiting frequently raises the danger of a Mallory-Weiss tear.
Epidemiology
An yearly average of 50–80–100,000 upper gastrointestinal bleeding cases occur in the United Kingdom.
more typical among older people.
History
Cause-related history (e.g., drunkenness, NSAID use, vomiting).
Acute: Haematemesis of freshly drawn blood or dark, partially digested blood (referred to as "coffee grounds"), melaena (loose, black, tarry, foul feces), which may indicate a bleeding episode larger than 50 mL or, in the event of fast bleeding, frank PR blood loss.
Chronic: positive faecal occult blood test, iron deficiency anemia.
Examination
indicators of chronic iron deficiency anemia or other indicators, such as spider naevi, palmar erythema, bruising, jaundice or ascites in liver illness, orofacial telangiectasia in Osler-Weber-Rendu syndrome.
signs of hypovolemia, tachycardia, hypotension, shock, and impaired mental status.
Investigations
Blood: LFT, crossmatch, clotting, U&Es, and FBC.
Oesophagogastroduodenoscopy (OGD): Allows for treatment by locating the bleeding site.
A visible vessel, an adhering clot, or ongoing bleeding are indicators of a recent hemorrhage.
Massive bleeding from the gastroduodenal artery can result from posterior duodenal ulcers.
Mesenteric angiography: Identifies the bleeding source, however the flow rate needs to be between 1 and 1.5 mL/minute in order to facilitate embolization therapy.
Management
Resuscitation techniques include the use of blood products and fluids, appropriate IV access, the ABCs, and the treatment of coagulopathy.
Medical: H2-antagonists or PPIs to lower the production of acid. elimination of H. pylori once a duodenal ulcer becomes stable. Vasopressin or somatostatin analogues, such as octreotide, are helpful in treating variceal hemorrhage because they lower portal pressure and splanchnic blood flow.
An oesophageal varices can be mechanically compressed by inserting a Sengstaken–Blakemore tube.
Endoscopic: Upper GI endoscopy for final upper gastrointestinal bleeding diagnosis and treatment.
For bleeding ulcers, treatments include photocoagulation, diathermy, adrenaline injection, or a combination of these. Injection sclerotherapy or band ligation are used to treat varices.
Radiological: In patients who are not candidates for surgery, embolishing the bleeding location might be feasible. In cases of uncontrollable variceal hemorrhage, transjugular intrahepatic portocaval shunts can be used instead of endoscopic procedures.
Surgical: In cases of potentially fatal bleeding, endoscopic treatment failure (10–12%), or concurrent surgical needs (such as perforations). The process is site- and cause-specific; for example, if a duodenal ulcer is under-running, a partial gastrectomy may be necessary for stomach ulcers.
Complications
anemia, shock from low blood volume, and collapse.
Prognosis
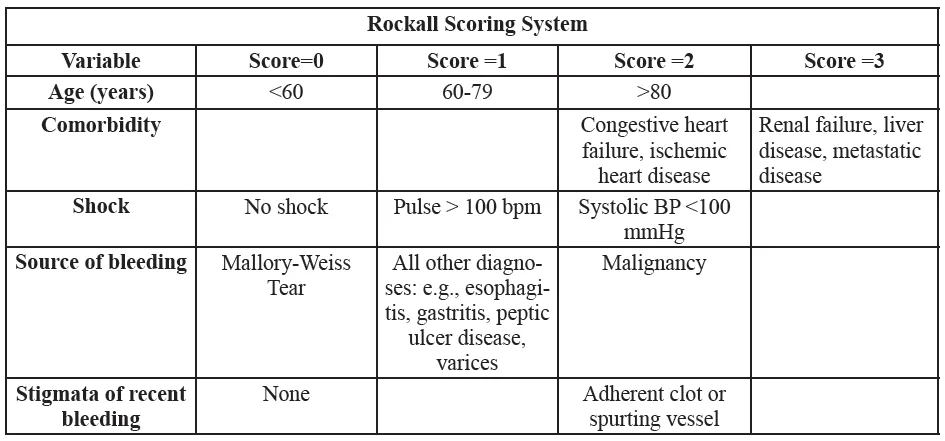
Depending on the etiology, early management and aggressive resuscitation improve outcomes for serious gastrointestinal bleeding. Patients who are at risk of a negative outcome are identified by the Rockall score (see table below).
Higher mortality in coagulopathy, cardiovascular disease, older age groups (14%) and those presenting with hemorrhagic shock (30%). Up to 20% of individuals may experience recurrent bleeding following endoscopic therapy.
Introduction
bleeding that originates from the upper portion of the gastrointestinal tract, or close to the Treitz ligament.
Etiology
Acute or chronic conditions include the following: 50% of instances of stomach and duodenal ulcers; acute erosive gastritis; oesophagitis or duodenitis; oesophageal or gastric varices; Mallory-Weiss tear; gastric angiogenesis or Dieulafoy's malformation; tumors or, less frequently, haemobilia; aorto-enteric fistula; or amyloidosis.
Risk Factors
NSAIDs, steroids, and Helicobacter pylori are risk factors for the onset or aggravation of erosions and ulcers. Stress ulcers 2 in burn patients and Cushing's ulcer in head injuries are related to shock and decreased splanchnic perfusion. Gastric erosions can be triggered by binges of alcohol.
Vomiting frequently raises the danger of a Mallory-Weiss tear.
Epidemiology
An yearly average of 50–80–100,000 upper gastrointestinal bleeding cases occur in the United Kingdom.
more typical among older people.
History
Cause-related history (e.g., drunkenness, NSAID use, vomiting).
Acute: Haematemesis of freshly drawn blood or dark, partially digested blood (referred to as "coffee grounds"), melaena (loose, black, tarry, foul feces), which may indicate a bleeding episode larger than 50 mL or, in the event of fast bleeding, frank PR blood loss.
Chronic: positive faecal occult blood test, iron deficiency anemia.
Examination
indicators of chronic iron deficiency anemia or other indicators, such as spider naevi, palmar erythema, bruising, jaundice or ascites in liver illness, orofacial telangiectasia in Osler-Weber-Rendu syndrome.
signs of hypovolemia, tachycardia, hypotension, shock, and impaired mental status.
Investigations
Blood: LFT, crossmatch, clotting, U&Es, and FBC.
Oesophagogastroduodenoscopy (OGD): Allows for treatment by locating the bleeding site.
A visible vessel, an adhering clot, or ongoing bleeding are indicators of a recent hemorrhage.
Massive bleeding from the gastroduodenal artery can result from posterior duodenal ulcers.
Mesenteric angiography: Identifies the bleeding source, however the flow rate needs to be between 1 and 1.5 mL/minute in order to facilitate embolization therapy.
Management
Resuscitation techniques include the use of blood products and fluids, appropriate IV access, the ABCs, and the treatment of coagulopathy.
Medical: H2-antagonists or PPIs to lower the production of acid. elimination of H. pylori once a duodenal ulcer becomes stable. Vasopressin or somatostatin analogues, such as octreotide, are helpful in treating variceal hemorrhage because they lower portal pressure and splanchnic blood flow.
An oesophageal varices can be mechanically compressed by inserting a Sengstaken–Blakemore tube.
Endoscopic: Upper GI endoscopy for final upper gastrointestinal bleeding diagnosis and treatment.
For bleeding ulcers, treatments include photocoagulation, diathermy, adrenaline injection, or a combination of these. Injection sclerotherapy or band ligation are used to treat varices.
Radiological: In patients who are not candidates for surgery, embolishing the bleeding location might be feasible. In cases of uncontrollable variceal hemorrhage, transjugular intrahepatic portocaval shunts can be used instead of endoscopic procedures.
Surgical: In cases of potentially fatal bleeding, endoscopic treatment failure (10–12%), or concurrent surgical needs (such as perforations). The process is site- and cause-specific; for example, if a duodenal ulcer is under-running, a partial gastrectomy may be necessary for stomach ulcers.
Complications
anemia, shock from low blood volume, and collapse.
Prognosis
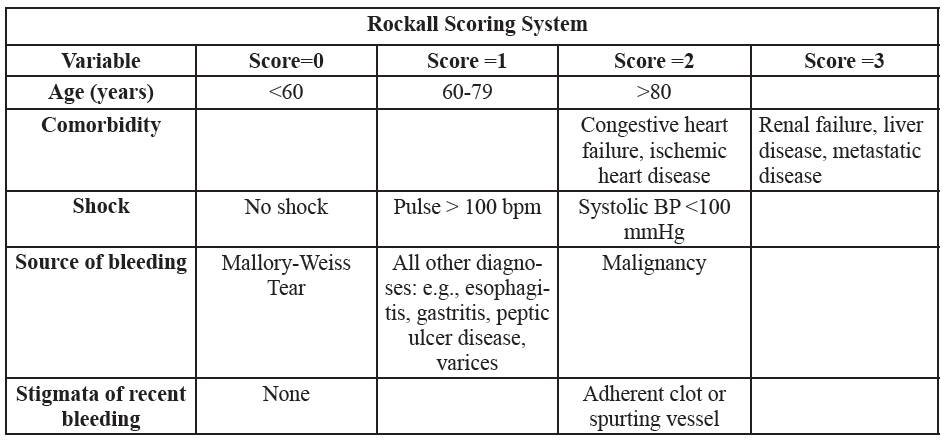
Depending on the etiology, early management and aggressive resuscitation improve outcomes for serious gastrointestinal bleeding. Patients who are at risk of a negative outcome are identified by the Rockall score (see table below).
Higher mortality in coagulopathy, cardiovascular disease, older age groups (14%) and those presenting with hemorrhagic shock (30%). Up to 20% of individuals may experience recurrent bleeding following endoscopic therapy.
0 Comments
