- Published on
Diagnostic Tests – Mammogram
1. When Do You Answer Mammogram?
A screening mammogram is the correct answer for women beginning at age 40, with the test repeated every 1–2 years depending on guidelines or individual risk. Once a woman reaches age 50, annual screening becomes standard because the incidence of breast cancer increases significantly with age. Mammography is used specifically for asymptomatic women as part of routine cancer detection. It is not a diagnostic test for symptoms—rather, it is a population-based screening tool aimed at identifying early, nonpalpable lesions before they become clinically evident.
2. What Is the Next Best Step When There Is an Abnormality?
If a screening mammogram reveals an abnormal finding—such as clustered, irregular microcalcifications, architectural distortion, or a suspicious density—the next best step is a core needle biopsy. This may include evaluation of the sentinel lymph node if cancer is confirmed or strongly suspected. A core biopsy provides tissue for histology and receptor testing (ER/PR, HER2). Mammography may also be used diagnostically when a breast mass is palpated on clinical exam, helping to identify additional lesions in the same breast or detect bilateral involvement. However, the key step after any suspicious finding on imaging is obtaining tissue for definitive diagnosis.
3. When Does Screening Lower Mortality the Most?
Mammography demonstrates the greatest reduction in breast cancer mortality in women older than 50. The benefit is more pronounced in this age group than in younger women because postmenopausal breast tissue is less dense and mammograms are more sensitive. Notably, the mortality reduction from mammography in this age range is greater than the mortality reductions achieved through colon cancer screening or cervical cancer screening. Boards often emphasize that the strongest population-level benefit of mammography is seen after age 50.
1. When Do You Answer Mammogram?
A screening mammogram is the correct answer for women beginning at age 40, with the test repeated every 1–2 years depending on guidelines or individual risk. Once a woman reaches age 50, annual screening becomes standard because the incidence of breast cancer increases significantly with age. Mammography is used specifically for asymptomatic women as part of routine cancer detection. It is not a diagnostic test for symptoms—rather, it is a population-based screening tool aimed at identifying early, nonpalpable lesions before they become clinically evident.
2. What Is the Next Best Step When There Is an Abnormality?
If a screening mammogram reveals an abnormal finding—such as clustered, irregular microcalcifications, architectural distortion, or a suspicious density—the next best step is a core needle biopsy. This may include evaluation of the sentinel lymph node if cancer is confirmed or strongly suspected. A core biopsy provides tissue for histology and receptor testing (ER/PR, HER2). Mammography may also be used diagnostically when a breast mass is palpated on clinical exam, helping to identify additional lesions in the same breast or detect bilateral involvement. However, the key step after any suspicious finding on imaging is obtaining tissue for definitive diagnosis.
3. When Does Screening Lower Mortality the Most?
Mammography demonstrates the greatest reduction in breast cancer mortality in women older than 50. The benefit is more pronounced in this age group than in younger women because postmenopausal breast tissue is less dense and mammograms are more sensitive. Notably, the mortality reduction from mammography in this age range is greater than the mortality reductions achieved through colon cancer screening or cervical cancer screening. Boards often emphasize that the strongest population-level benefit of mammography is seen after age 50.

- Published on
Diagnostic Tests – Estrogen and Progesterone Receptors (ER/PR)
1. What Are These Tests?
Estrogen and progesterone receptor (ER/PR) testing is performed on all newly diagnosed breast cancer specimens to determine whether the tumor expresses hormone receptors. These receptors, when present on cancer cells, indicate that the tumor’s growth is influenced by estrogen or progesterone signaling. Identifying ER/PR positivity is crucial because it predicts whether the cancer is likely to respond to hormone-blocking therapy. In practice, a tissue sample from the breast tumor is analyzed using immunohistochemistry (IHC) to detect receptor presence. A tumor may be positive for estrogen receptors alone, progesterone receptors alone, or both.
2. What Is the Therapy?
Patients whose tumors express either estrogen receptors, progesterone receptors, or both are candidates for hormone (endocrine) therapy. The standard treatments include medications such as tamoxifen or raloxifene, which block estrogen’s action on breast tissue. Tamoxifen is most commonly used and is particularly effective when both estrogen and progesterone receptors are positive, as dual positivity predicts a stronger therapeutic response. These agents help reduce recurrence risk, shrink residual disease, and improve long-term outcomes by preventing estrogen-driven tumor growth. In some cases—especially in postmenopausal women—aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) may also be used, although the classic board-style answer based on your content focuses on tamoxifen or raloxifene.
1. What Are These Tests?
Estrogen and progesterone receptor (ER/PR) testing is performed on all newly diagnosed breast cancer specimens to determine whether the tumor expresses hormone receptors. These receptors, when present on cancer cells, indicate that the tumor’s growth is influenced by estrogen or progesterone signaling. Identifying ER/PR positivity is crucial because it predicts whether the cancer is likely to respond to hormone-blocking therapy. In practice, a tissue sample from the breast tumor is analyzed using immunohistochemistry (IHC) to detect receptor presence. A tumor may be positive for estrogen receptors alone, progesterone receptors alone, or both.
2. What Is the Therapy?
Patients whose tumors express either estrogen receptors, progesterone receptors, or both are candidates for hormone (endocrine) therapy. The standard treatments include medications such as tamoxifen or raloxifene, which block estrogen’s action on breast tissue. Tamoxifen is most commonly used and is particularly effective when both estrogen and progesterone receptors are positive, as dual positivity predicts a stronger therapeutic response. These agents help reduce recurrence risk, shrink residual disease, and improve long-term outcomes by preventing estrogen-driven tumor growth. In some cases—especially in postmenopausal women—aromatase inhibitors (e.g., anastrozole, letrozole, exemestane) may also be used, although the classic board-style answer based on your content focuses on tamoxifen or raloxifene.

- Published on
Diagnostic Tests – Carcinoembryonic Antigen (CEA)
1. What Is CEA?
Carcinoembryonic antigen (CEA) is a glycoprotein normally produced during fetal development, but after birth its levels fall to very low concentrations. In adults, CEA can become elevated in the serum when certain cancers—most notably colorectal cancer (CRC)—reactivate the expression of this embryonic protein. While CEA can rise with other malignancies (pancreatic, gastric, lung, breast) and even some benign conditions (smoking, inflammation), its clinical value is primarily tied to colorectal cancer. It is not specific enough to diagnose cancer, but it is extremely useful for tracking disease activity.
2. Prognostic Value in Disease
CEA levels hold significant prognostic importance in patients newly diagnosed with colorectal cancer. Individuals who present with high baseline CEA levels generally have a more aggressive disease course and worse overall outcomes compared with those whose levels are normal or only mildly elevated. High pre-treatment CEA correlates with a greater likelihood of advanced tumor stage, nodal involvement, and future recurrence. Because of this, CEA serves as a marker that helps clinicians risk-stratify patients and anticipate their clinical trajectory.
3. When CEA Is the Correct Answer
CEA is most appropriately ordered for monitoring patients after surgical resection of colorectal cancer. Once the tumor is removed, declining or normalized CEA levels indicate successful treatment, while a subsequent rise strongly suggests persistent disease, recurrence, or metastatic spread. Postoperative surveillance using periodic CEA measurements is a standard component of colorectal cancer follow-up. In board-style questions, the correct use of CEA is almost always framed around detecting recurrence after treatment rather than diagnosing the initial disease.
4. When CEA Is the Right Screening Test
CEA is never the correct answer for screening for colorectal cancer. It lacks both sensitivity and specificity and cannot reliably detect early or premalignant disease. Screening for colon cancer should always involve colonoscopy, or in some cases stool-based tests (FIT, FOBT, FIT-DNA), but never serum CEA. On exams, any option suggesting CEA as a screening test is intentionally incorrect.
1. What Is CEA?
Carcinoembryonic antigen (CEA) is a glycoprotein normally produced during fetal development, but after birth its levels fall to very low concentrations. In adults, CEA can become elevated in the serum when certain cancers—most notably colorectal cancer (CRC)—reactivate the expression of this embryonic protein. While CEA can rise with other malignancies (pancreatic, gastric, lung, breast) and even some benign conditions (smoking, inflammation), its clinical value is primarily tied to colorectal cancer. It is not specific enough to diagnose cancer, but it is extremely useful for tracking disease activity.
2. Prognostic Value in Disease
CEA levels hold significant prognostic importance in patients newly diagnosed with colorectal cancer. Individuals who present with high baseline CEA levels generally have a more aggressive disease course and worse overall outcomes compared with those whose levels are normal or only mildly elevated. High pre-treatment CEA correlates with a greater likelihood of advanced tumor stage, nodal involvement, and future recurrence. Because of this, CEA serves as a marker that helps clinicians risk-stratify patients and anticipate their clinical trajectory.
3. When CEA Is the Correct Answer
CEA is most appropriately ordered for monitoring patients after surgical resection of colorectal cancer. Once the tumor is removed, declining or normalized CEA levels indicate successful treatment, while a subsequent rise strongly suggests persistent disease, recurrence, or metastatic spread. Postoperative surveillance using periodic CEA measurements is a standard component of colorectal cancer follow-up. In board-style questions, the correct use of CEA is almost always framed around detecting recurrence after treatment rather than diagnosing the initial disease.
4. When CEA Is the Right Screening Test
CEA is never the correct answer for screening for colorectal cancer. It lacks both sensitivity and specificity and cannot reliably detect early or premalignant disease. Screening for colon cancer should always involve colonoscopy, or in some cases stool-based tests (FIT, FOBT, FIT-DNA), but never serum CEA. On exams, any option suggesting CEA as a screening test is intentionally incorrect.

- Published on
Diagnostic Tests – Colposcopy
1. What Is a Colposcopy?
A colposcopy is a gynecologic procedure that allows direct, magnified visualization of the cervix, vagina, and transformation zone using a specialized instrument called a colposcope—a lighted binocular microscope. The device is placed at the vaginal introitus (not inside the vagina like a speculum) and provides enhanced detail of cervical epithelial changes. Clinicians often apply acetic acid or Lugol’s iodine during the procedure to highlight abnormal areas, making precancerous lesions easier to identify and biopsy. The purpose of a colposcopy is to further evaluate abnormalities detected on cervical cancer screening tests, particularly when cytology suggests dysplasia.
2. What Must Be Visualized for an Adequate Study?
For a colposcopy to be considered adequate, the provider must be able to clearly visualize the transformation zone—the area where squamous epithelium of the ectocervix meets the columnar epithelium of the endocervix. This squamocolumnar junction is the region most susceptible to HPV-related dysplastic changes and is where cervical intraepithelial neoplasia (CIN) typically arises. If the transformation zone cannot be fully seen—either because it resides high in the endocervical canal, or the view is obstructed—the colposcopy is termed inadequate and may require an endocervical curettage or additional management.
3. When Is Colposcopy the Correct Next Step?
Colposcopy is most appropriate when a patient has an abnormal Pap smear requiring further evaluation. It becomes the next diagnostic step when cytology suggests premalignant or high-risk cervical disease. Specifically, colposcopy is indicated when any of the following appear on Pap testing:
In these scenarios, colposcopy allows for direct inspection and targeted biopsy of abnormal cervical areas, which is essential for diagnosing and grading CIN and determining appropriate management.
1. What Is a Colposcopy?
A colposcopy is a gynecologic procedure that allows direct, magnified visualization of the cervix, vagina, and transformation zone using a specialized instrument called a colposcope—a lighted binocular microscope. The device is placed at the vaginal introitus (not inside the vagina like a speculum) and provides enhanced detail of cervical epithelial changes. Clinicians often apply acetic acid or Lugol’s iodine during the procedure to highlight abnormal areas, making precancerous lesions easier to identify and biopsy. The purpose of a colposcopy is to further evaluate abnormalities detected on cervical cancer screening tests, particularly when cytology suggests dysplasia.
2. What Must Be Visualized for an Adequate Study?
For a colposcopy to be considered adequate, the provider must be able to clearly visualize the transformation zone—the area where squamous epithelium of the ectocervix meets the columnar epithelium of the endocervix. This squamocolumnar junction is the region most susceptible to HPV-related dysplastic changes and is where cervical intraepithelial neoplasia (CIN) typically arises. If the transformation zone cannot be fully seen—either because it resides high in the endocervical canal, or the view is obstructed—the colposcopy is termed inadequate and may require an endocervical curettage or additional management.
3. When Is Colposcopy the Correct Next Step?
Colposcopy is most appropriate when a patient has an abnormal Pap smear requiring further evaluation. It becomes the next diagnostic step when cytology suggests premalignant or high-risk cervical disease. Specifically, colposcopy is indicated when any of the following appear on Pap testing:
- ASC-H (Atypical Squamous Cells—cannot exclude HSIL)
- LSIL (Low-Grade Squamous Intraepithelial Lesion)
- HSIL (High-Grade Squamous Intraepithelial Lesion)
- ASC-US (Atypical Squamous Cells of Undetermined Significance) when the HPV DNA test is positive
In these scenarios, colposcopy allows for direct inspection and targeted biopsy of abnormal cervical areas, which is essential for diagnosing and grading CIN and determining appropriate management.

- Published on
Diagnostic Tests – Multifocal Atrial Tachycardia (MAT)
Overview of MAT
Multifocal atrial tachycardia (MAT) is an arrhythmia in which the atria initiate electrical impulses from multiple different pacemaker sites rather than a single dominant focus. This leads to a rapid heart rhythm—typically over 100 beats per minute—with identifiable but variable P waves, each originating from a different atrial location. Unlike atrial fibrillation, where the baseline is chaotic and true P waves are absent, MAT shows distinct P-wave activity even though the atrial rhythm is disorganized. The impulses still travel through the AV node, producing normal, narrow QRS complexes that appear at irregular intervals.
EKG Characteristics
One of the key diagnostic features of MAT is its irregular timing between beats. Both P–P intervals and R–R intervals vary continuously, giving the rhythm an “irregularly irregular” appearance. What sets MAT apart from similar arrhythmias is the presence of at least three different P-wave morphologies, reflecting shifting atrial pacemaker sites. Because each focus conducts through the AV node differently, the PR intervals also change from beat to beat. When the heart rate is below 100 beats per minute but the same shifting pacemaker pattern is present, the rhythm is called a wandering atrial pacemaker, which represents a slower version of the same phenomenon.
Most Common Causes
The condition is most strongly linked to chronic lung disease, particularly during exacerbations of chronic obstructive pulmonary disease (COPD). Chronic hypoxia, hypercapnia, and increased sympathetic tone disrupt atrial electrical stability, causing multiple atrial sites to fire chaotically. Right atrial enlargement or stretch from long-standing pulmonary hypertension further destabilizes atrial conduction. Electrolyte abnormalities—especially low potassium or magnesium—often worsen atrial irritability. Medications such as theophylline, historically used for COPD, can also provoke MAT due to their stimulatory effects on the heart. Although conditions like pulmonary embolism and severe congestive heart failure can also produce similar arrhythmias, COPD remains the most common underlying cause.

- Published on
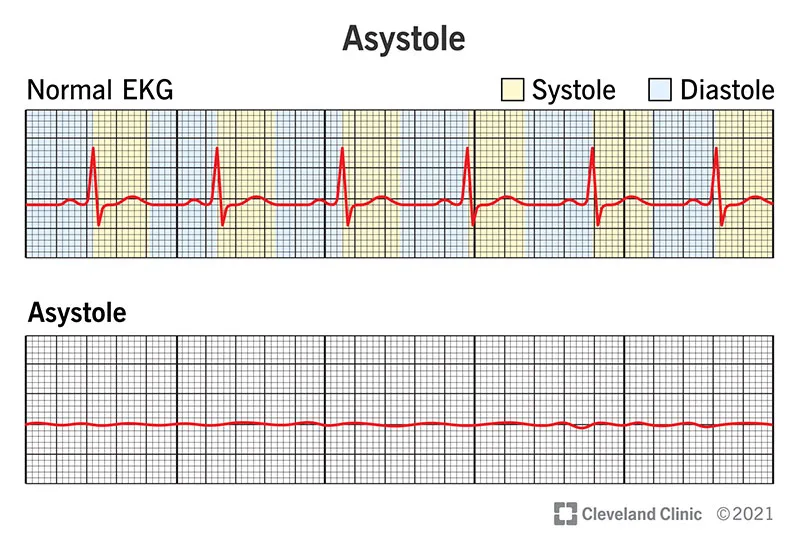
Diagnostic Tests – Asystole
What Is This?
The EKG demonstrates asystole, a rhythm that indicates the near-complete absence of electrical activity in the heart. In asystole, the myocardium is electrically silent and unable to generate a coordinated contraction, resulting in the absence of a pulse or blood pressure. Although commonly referred to as “flatline,” true asystole does not usually produce a perfectly straight line—small baseline undulations may still appear—but there are no identifiable P-waves, QRS complexes, or organized rhythm. Asystole represents one of the most severe and final forms of cardiac arrest.
What Is the Characteristic EKG Feature That Gives the Diagnosis?
The defining characteristic of asystole on EKG is the lack of any meaningful electrical activity whatsoever. Unlike ventricular fibrillation—which shows chaotic, irregular electrical waves—or ventricular tachycardia—which shows wide, organized complexes—asystole shows no complexes at all. The tracing consists of minimal, non-specific baseline oscillation. If you can identify any organized rhythm, such as QRS complexes or discernible P-waves, the diagnosis is not asystole. The flat, near-silent pattern is what establishes the diagnosis.
What Case Will Go Along With This EKG?
A patient with asystole will be in full cardiac arrest with no pulse, no blood pressure, and no respirations. The onset is sudden, and the patient collapses immediately. Asystole is typically the result of prolonged cardiac arrest, massive myocardial infarction, severe hypoxia, advanced metabolic derangements, or final-stage deterioration following ventricular fibrillation. Clinically, asystole cannot be distinguished from other causes of pulselessness—such as ventricular fibrillation, pulseless electrical activity (PEA), cardiac tamponade, or tension pneumothorax—without obtaining an EKG. Therefore, rhythm identification is essential to determine the correct management pathway, though asystole itself is not shockable, unlike Vfib.
What Is This?
The EKG demonstrates asystole, a rhythm that indicates the near-complete absence of electrical activity in the heart. In asystole, the myocardium is electrically silent and unable to generate a coordinated contraction, resulting in the absence of a pulse or blood pressure. Although commonly referred to as “flatline,” true asystole does not usually produce a perfectly straight line—small baseline undulations may still appear—but there are no identifiable P-waves, QRS complexes, or organized rhythm. Asystole represents one of the most severe and final forms of cardiac arrest.
What Is the Characteristic EKG Feature That Gives the Diagnosis?
The defining characteristic of asystole on EKG is the lack of any meaningful electrical activity whatsoever. Unlike ventricular fibrillation—which shows chaotic, irregular electrical waves—or ventricular tachycardia—which shows wide, organized complexes—asystole shows no complexes at all. The tracing consists of minimal, non-specific baseline oscillation. If you can identify any organized rhythm, such as QRS complexes or discernible P-waves, the diagnosis is not asystole. The flat, near-silent pattern is what establishes the diagnosis.
What Case Will Go Along With This EKG?
A patient with asystole will be in full cardiac arrest with no pulse, no blood pressure, and no respirations. The onset is sudden, and the patient collapses immediately. Asystole is typically the result of prolonged cardiac arrest, massive myocardial infarction, severe hypoxia, advanced metabolic derangements, or final-stage deterioration following ventricular fibrillation. Clinically, asystole cannot be distinguished from other causes of pulselessness—such as ventricular fibrillation, pulseless electrical activity (PEA), cardiac tamponade, or tension pneumothorax—without obtaining an EKG. Therefore, rhythm identification is essential to determine the correct management pathway, though asystole itself is not shockable, unlike Vfib.
- Published on
Diagnostic Tests – Ventricular Fibrillation (Vfib)
What Is This?
The EKG demonstrates ventricular fibrillation (Vfib), a lethal cardiac arrhythmia and one of the primary causes of sudden cardiac death. Ventricular fibrillation occurs when the ventricles quiver in a chaotic, uncoordinated manner rather than contracting effectively. Because there is no organized ventricular activity, the heart cannot generate a pulse or maintain any blood pressure. Recognizing Vfib on an EKG is critical because it requires immediate defibrillation to restore organized cardiac rhythm and perfusion.
What Is the Characteristic EKG Feature That Gives the Diagnosis?
The characteristic feature of Vfib on an EKG is the complete absence of organized electrical activity. The tracing shows no P-waves, no QRS complexes, and no discernible rhythm. Instead, the strip displays a chaotic, irregular pattern with either low-amplitude fine fibrillation waves or high-amplitude coarse fibrillation waves. Despite the disorganized activity, Vfib is not the same as asystole—the line is not flat, and electrical activity is still present, but it is functionally useless. If you can identify any organized complexes or repeating rhythm, the diagnosis is not Vfib.
What Case Will Go Along With This EKG?
A typical case involving Vfib describes a patient in full cardiac arrest. These patients have no pulse, no blood pressure, and no respirations, and they collapse suddenly. They may have a prior history of coronary artery disease, myocardial infarction, cardiomyopathy, severe electrolyte imbalance (such as hypokalemia), or acute ischemia, but Vfib can also occur without warning. Clinically, Vfib cannot be distinguished from other forms of pulseless arrest—such as asystole, pulseless electrical activity (PEA), or pulseless ventricular tachycardia—without an EKG. Therefore, rapid rhythm identification is essential so that immediate defibrillation can be performed, which is the only lifesaving treatment for Vfib.
What Is This?
The EKG demonstrates ventricular fibrillation (Vfib), a lethal cardiac arrhythmia and one of the primary causes of sudden cardiac death. Ventricular fibrillation occurs when the ventricles quiver in a chaotic, uncoordinated manner rather than contracting effectively. Because there is no organized ventricular activity, the heart cannot generate a pulse or maintain any blood pressure. Recognizing Vfib on an EKG is critical because it requires immediate defibrillation to restore organized cardiac rhythm and perfusion.
What Is the Characteristic EKG Feature That Gives the Diagnosis?
The characteristic feature of Vfib on an EKG is the complete absence of organized electrical activity. The tracing shows no P-waves, no QRS complexes, and no discernible rhythm. Instead, the strip displays a chaotic, irregular pattern with either low-amplitude fine fibrillation waves or high-amplitude coarse fibrillation waves. Despite the disorganized activity, Vfib is not the same as asystole—the line is not flat, and electrical activity is still present, but it is functionally useless. If you can identify any organized complexes or repeating rhythm, the diagnosis is not Vfib.
What Case Will Go Along With This EKG?
A typical case involving Vfib describes a patient in full cardiac arrest. These patients have no pulse, no blood pressure, and no respirations, and they collapse suddenly. They may have a prior history of coronary artery disease, myocardial infarction, cardiomyopathy, severe electrolyte imbalance (such as hypokalemia), or acute ischemia, but Vfib can also occur without warning. Clinically, Vfib cannot be distinguished from other forms of pulseless arrest—such as asystole, pulseless electrical activity (PEA), or pulseless ventricular tachycardia—without an EKG. Therefore, rapid rhythm identification is essential so that immediate defibrillation can be performed, which is the only lifesaving treatment for Vfib.

- Published on
Diagnostic Tests – Ventricular Tachycardia (VT)
What Is the Diagnosis?
The EKG demonstrates ventricular tachycardia (VT), a dangerous arrhythmia characterized by a wide-complex tachycardia, with QRS complexes greater than 120 milliseconds. VT originates from the ventricles rather than the atria, which results in broad, abnormal QRS complexes that appear uniform or slightly varied depending on the underlying mechanism. By board exam convention, any regular wide-complex tachycardia should be assumed to be VT unless proven otherwise, making this an essential recognition pattern in cardiology.
What Case Will Go Along With This EKG?
Ventricular tachycardia can present with a wide range of symptoms, from mild palpitations to life-threatening instability. A typical case might involve a patient who develops syncope, lightheadedness, shortness of breath, or symptoms of congestive heart failure. In severe situations, VT may cause sudden cardiac death, emphasizing the need for rapid diagnosis and treatment. VT commonly occurs in patients with underlying structural heart disease, such as prior myocardial infarction, cardiomyopathy, severe electrolyte disturbances, or antiarrhythmic drug toxicity. Because symptoms alone cannot reliably identify VT, the EKG is essential for diagnosis.
How Do You Treat It?
Treatment of ventricular tachycardia depends entirely on patient stability. When the patient is unstable—with hypotension, chest pain, altered mental status, or signs of shock—the correct and immediate treatment is synchronized electrical cardioversion, which is lifesaving. For stable patients who are maintaining blood pressure and mentation, pharmacologic therapy is appropriate. Intravenous amiodarone is typically first-line, while lidocaine (especially in post–MI patients) and procainamide are effective alternatives. Regardless of the initial approach, VT is a serious arrhythmia that demands prompt intervention and frequently leads to further diagnostic evaluation, such as electrophysiology studies, to determine its etiology.
What Is the Diagnosis?
The EKG demonstrates ventricular tachycardia (VT), a dangerous arrhythmia characterized by a wide-complex tachycardia, with QRS complexes greater than 120 milliseconds. VT originates from the ventricles rather than the atria, which results in broad, abnormal QRS complexes that appear uniform or slightly varied depending on the underlying mechanism. By board exam convention, any regular wide-complex tachycardia should be assumed to be VT unless proven otherwise, making this an essential recognition pattern in cardiology.
What Case Will Go Along With This EKG?
Ventricular tachycardia can present with a wide range of symptoms, from mild palpitations to life-threatening instability. A typical case might involve a patient who develops syncope, lightheadedness, shortness of breath, or symptoms of congestive heart failure. In severe situations, VT may cause sudden cardiac death, emphasizing the need for rapid diagnosis and treatment. VT commonly occurs in patients with underlying structural heart disease, such as prior myocardial infarction, cardiomyopathy, severe electrolyte disturbances, or antiarrhythmic drug toxicity. Because symptoms alone cannot reliably identify VT, the EKG is essential for diagnosis.
How Do You Treat It?
Treatment of ventricular tachycardia depends entirely on patient stability. When the patient is unstable—with hypotension, chest pain, altered mental status, or signs of shock—the correct and immediate treatment is synchronized electrical cardioversion, which is lifesaving. For stable patients who are maintaining blood pressure and mentation, pharmacologic therapy is appropriate. Intravenous amiodarone is typically first-line, while lidocaine (especially in post–MI patients) and procainamide are effective alternatives. Regardless of the initial approach, VT is a serious arrhythmia that demands prompt intervention and frequently leads to further diagnostic evaluation, such as electrophysiology studies, to determine its etiology.

- Published on
Diagnostic Topic – Supraventricular Tachycardia (SVT)
1. What Is the Diagnosis?
The EKG demonstrates supraventricular tachycardia (SVT). SVT is characterized by a regular, rapid rhythm originating above the ventricles, with a narrow QRS complex (<120 ms). on the strip, rate is fast and qrs complexes are uniform narrow, p-waves usually absent or hidden within preceding t-wave. there no visible flutter waves fibrillatory waves, helping distinguish svt from atrial fibrillation. this combination of a fast, regular tachycardia with narrow classic for svt.
2. What Case Will Go Along With This EKG?
The typical clinical scenario is a patient presenting with:
Common triggers or associations include:
3. How Do You Treat SVT?
Initial treatment focuses on slowing the AV node to interrupt the reentry circuit most commonly responsible for SVT.
Step-by-step treatment:
1. Vagal maneuvers
(first-line)
These increase vagal tone and may terminate the rhythm.
2. Intravenous adenosine
(drug of choice)
If vagal maneuvers fail, adenosine is given as a rapid IV push. It transiently blocks AV nodal conduction and can stop the arrhythmia immediately. It is the most effective acute therapy.
3. If adenosine does not work
Use medications that slow AV nodal conduction:
4. If the patient is unstable
If there is hypotension, altered mental status, or signs of shock, immediate synchronized cardioversion is required.
1. What Is the Diagnosis?
The EKG demonstrates supraventricular tachycardia (SVT). SVT is characterized by a regular, rapid rhythm originating above the ventricles, with a narrow QRS complex (<120 ms). on the strip, rate is fast and qrs complexes are uniform narrow, p-waves usually absent or hidden within preceding t-wave. there no visible flutter waves fibrillatory waves, helping distinguish svt from atrial fibrillation. this combination of a fast, regular tachycardia with narrow classic for svt.
2. What Case Will Go Along With This EKG?
The typical clinical scenario is a patient presenting with:
- Sudden-onset rapid palpitations
- Lightheadedness or dizziness
- Possible shortness of breath, anxiety, or diaphoresis
- Symptoms that begin abruptly and may stop abruptly
Common triggers or associations include:
- Caffeine intake (coffee, energy drinks)
- Sympathetic stimulants (decongestants, cocaine, amphetamines)
- Psychological stress or anxiety
- Hyperthyroidism
- History of paroxysmal episodes of rapid heartbeat that resolve spontaneously
3. How Do You Treat SVT?
Initial treatment focuses on slowing the AV node to interrupt the reentry circuit most commonly responsible for SVT.
Step-by-step treatment:
1. Vagal maneuvers
(first-line)
- Carotid sinus massage (unilateral, gentle, after checking for carotid bruit)
- Valsalva maneuver
- Cold water immersion or face-in-ice-water technique
These increase vagal tone and may terminate the rhythm.
2. Intravenous adenosine
(drug of choice)
If vagal maneuvers fail, adenosine is given as a rapid IV push. It transiently blocks AV nodal conduction and can stop the arrhythmia immediately. It is the most effective acute therapy.
3. If adenosine does not work
Use medications that slow AV nodal conduction:
- Calcium channel blockers such as verapamil or diltiazem
- Beta blockers
- Digoxin (less commonly used today but historically included in exam materials)
4. If the patient is unstable
If there is hypotension, altered mental status, or signs of shock, immediate synchronized cardioversion is required.

- Published on
Diagnostic Topic – Torsade de Pointes
1. What Is This?
The EKG described is showing Torsade de pointes, a specific form of polymorphic ventricular tachycardia associated with a prolonged QT interval. Torsade is a dangerous ventricular arrhythmia that can rapidly deteriorate into ventricular fibrillation and sudden cardiac death if not recognized and treated promptly. It is considered a subtype of wide-complex tachycardia with a characteristic cyclical change in QRS shape and amplitude.
2. What Is the Characteristic EKG Feature?
The most distinctive EKG finding in Torsade de pointes is its “twisting of the points” appearance. This refers to the way the QRS amplitude gradually increases and decreases in a sinusoidal pattern, giving the impression that the complexes are spiraling or “twisting” around the baseline.
Additional key features include:
This unusual undulating pattern is what sets Torsade apart from other forms of ventricular tachycardia.
3. What Clinical Scenario Goes With This EKG?
Torsade can present with a wide spectrum of symptoms, ranging from palpitations to dizziness, syncope, or even sudden cardiac death. You cannot diagnose it based on symptoms alone—the EKG is essential.
Classic exam clues that point to Torsade include:
1. What Is This?
The EKG described is showing Torsade de pointes, a specific form of polymorphic ventricular tachycardia associated with a prolonged QT interval. Torsade is a dangerous ventricular arrhythmia that can rapidly deteriorate into ventricular fibrillation and sudden cardiac death if not recognized and treated promptly. It is considered a subtype of wide-complex tachycardia with a characteristic cyclical change in QRS shape and amplitude.
2. What Is the Characteristic EKG Feature?
The most distinctive EKG finding in Torsade de pointes is its “twisting of the points” appearance. This refers to the way the QRS amplitude gradually increases and decreases in a sinusoidal pattern, giving the impression that the complexes are spiraling or “twisting” around the baseline.
Additional key features include:
- Polymorphic wide QRS complexes (>120 ms)
- Beat-to-beat variation in QRS axis and morphology
- Prolonged QT interval before the onset of the arrhythmia
This unusual undulating pattern is what sets Torsade apart from other forms of ventricular tachycardia.
3. What Clinical Scenario Goes With This EKG?
Torsade can present with a wide spectrum of symptoms, ranging from palpitations to dizziness, syncope, or even sudden cardiac death. You cannot diagnose it based on symptoms alone—the EKG is essential.
Classic exam clues that point to Torsade include:
- Hypomagnesemia—one of the most common metabolic triggers
- Hypokalemia—exacerbates QT prolongation
- Drug-induced QT prolongation, especially from medications such as:
- Tricyclic antidepressants (TCAs)
- Class III antiarrhythmics (amiodarone, dofetilide, ibutilide)
- Macrolide antibiotics (e.g., azithromycin, erythromycin)
- Quinolone antibiotics (rarely)
- Certain antipsychotics and antiemetics

