- Published on
Diagnostic Tests – Holter Monitoring (24-Hour Ambulatory Cardiac Monitoring)
What Is Holter Monitoring?
Holter monitoring is a form of continuous ambulatory EKG recording that captures a patient’s cardiac rhythm over a full 24-hour period (or sometimes longer). Unlike a single snapshot EKG performed in the clinic, a Holter monitor records every heartbeat over an extended time, making it possible to detect intermittent arrhythmias that may not be present during a brief office visit.
How Does It Work?
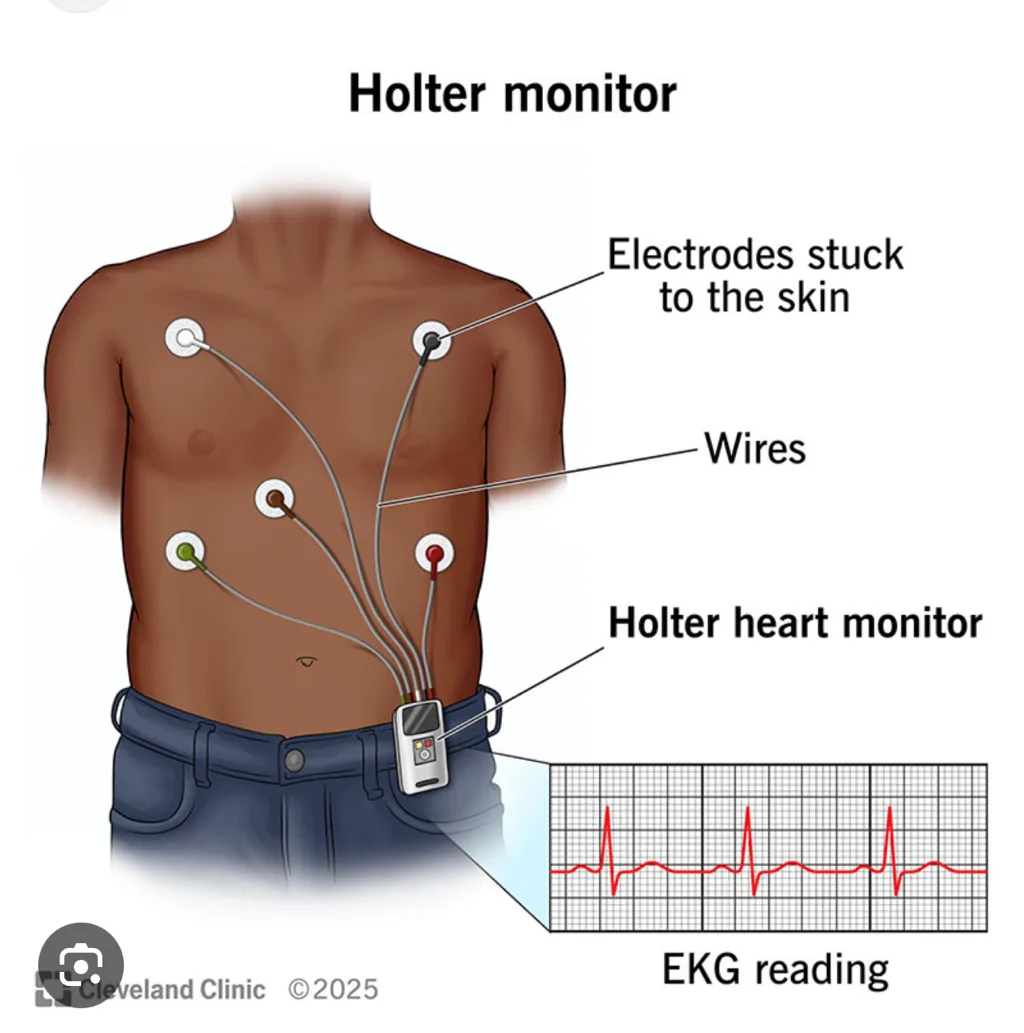
The patient wears several adhesive EKG leads on the chest, which are connected to a small portable recorder worn on a strap around the neck or clipped to the belt. The device continuously records a single-lead or multi-lead EKG while the patient goes about normal daily activities.
After 24 hours, the recording is reviewed—often at high speed—to identify brief rhythm disturbances such as premature beats, paroxysmal atrial fibrillation, supraventricular tachycardia, pauses, or transient conduction blocks. In this way, Holter monitoring captures arrhythmias that a standard EKG might easily miss.
What Is the Most Accurate Test?
Abnormalities detected on Holter monitoring can be evaluated further with:
Thus, while Holter monitors are excellent for detection, EP studies are more accurate for definitive diagnosis and treatment planning.
When Do You Answer Holter Monitoring?
Holter monitoring is the correct diagnostic choice when a patient has symptoms suggestive of an arrhythmia, but an in-office EKG is normal or nondiagnostic. Common indications include:
If the symptom is brief, infrequent, and unpredictable—and especially if the resting EKG is normal—Holter monitoring is the best initial test to capture the electrical event.
What Is Holter Monitoring?
Holter monitoring is a form of continuous ambulatory EKG recording that captures a patient’s cardiac rhythm over a full 24-hour period (or sometimes longer). Unlike a single snapshot EKG performed in the clinic, a Holter monitor records every heartbeat over an extended time, making it possible to detect intermittent arrhythmias that may not be present during a brief office visit.
How Does It Work?
The patient wears several adhesive EKG leads on the chest, which are connected to a small portable recorder worn on a strap around the neck or clipped to the belt. The device continuously records a single-lead or multi-lead EKG while the patient goes about normal daily activities.
After 24 hours, the recording is reviewed—often at high speed—to identify brief rhythm disturbances such as premature beats, paroxysmal atrial fibrillation, supraventricular tachycardia, pauses, or transient conduction blocks. In this way, Holter monitoring captures arrhythmias that a standard EKG might easily miss.
What Is the Most Accurate Test?
Abnormalities detected on Holter monitoring can be evaluated further with:
- Electrophysiologic (EP) studies, which provide the most accurate mapping and diagnosis of rhythm disorders
- Echocardiography, to assess structural causes of arrhythmias
Thus, while Holter monitors are excellent for detection, EP studies are more accurate for definitive diagnosis and treatment planning.
When Do You Answer Holter Monitoring?
Holter monitoring is the correct diagnostic choice when a patient has symptoms suggestive of an arrhythmia, but an in-office EKG is normal or nondiagnostic. Common indications include:
- Palpitations
- Syncope or near-syncope
- Intermittent dizziness
- Suspected paroxysmal arrhythmias not captured on a standard EKG
If the symptom is brief, infrequent, and unpredictable—and especially if the resting EKG is normal—Holter monitoring is the best initial test to capture the electrical event.
- Published on
Diagnostic Tests – Cardiac Electrophysiological (EP) Studies
What Is an EP Study?
A cardiac electrophysiological (EP) study is an invasive diagnostic procedure in which specialized catheters equipped with electrical sensing and stimulating electrodes are inserted into the heart via peripheral veins. These catheters record electrical activity directly from within the cardiac chambers and can deliver controlled electrical impulses.
This allows clinicians to identify abnormal rhythm disturbances, test the heart’s conduction pathways, and provoke arrhythmias under controlled conditions. The technique provides precise information about the site of origin, mechanism, and severity of cardiac arrhythmias.
When Is an EP Study the Correct Answer?
EP studies are used when definitive diagnosis or direct treatment of cardiac arrhythmias is required. They are typically chosen in the following situations:
In short, EP studies provide both definitive diagnosis and therapeutic options for complex rhythm disorders.
What Is an EP Study?
A cardiac electrophysiological (EP) study is an invasive diagnostic procedure in which specialized catheters equipped with electrical sensing and stimulating electrodes are inserted into the heart via peripheral veins. These catheters record electrical activity directly from within the cardiac chambers and can deliver controlled electrical impulses.
This allows clinicians to identify abnormal rhythm disturbances, test the heart’s conduction pathways, and provoke arrhythmias under controlled conditions. The technique provides precise information about the site of origin, mechanism, and severity of cardiac arrhythmias.
When Is an EP Study the Correct Answer?
EP studies are used when definitive diagnosis or direct treatment of cardiac arrhythmias is required. They are typically chosen in the following situations:
- Unexplained syncope, especially when arrhythmia is suspected and noninvasive testing is inconclusive.
- Detailed mapping of the cardiac conduction system, useful for complex arrhythmias or pre-ablation planning.
- Ablation therapy for arrhythmias such as supraventricular tachycardia (SVT) or Wolff-Parkinson-White (WPW) syndrome, where identifying and destroying the aberrant pathway cures the condition.
- Evaluation and placement of implantable cardioverter-defibrillators (ICDs) in patients at risk for malignant arrhythmias.
- Localization of the origin of sustained ventricular tachycardia, which is essential for targeted ablation or device therapy.
In short, EP studies provide both definitive diagnosis and therapeutic options for complex rhythm disorders.

- Published on
Diagnostic Tests– Transthoracic or 2D Echocardiogram (TTE)
What Is a Transthoracic Echocardiogram (TTE)?
A transthoracic echocardiogram (TTE) is the standard, noninvasive ultrasound study of the heart. It provides detailed information about cardiac chamber size, ventricular function, valvular structure and motion, intracardiac masses, pericardial effusion, and aspects of aortic disease. Because it is safe, painless, and widely available, TTE is one of the most commonly used imaging tests in cardiology and serves as a cornerstone of cardiac evaluation.
How Is a TTE Performed?
The test is done by placing a sonographic transducer on the anterior chest wall (usually in the parasternal, apical, and subcostal windows). The transducer emits ultrasound waves that bounce off cardiac structures and return as high-resolution images. TTE provides real-time visualization of heart motion, wall thickening, valve opening and closing, and blood flow patterns when combined with Doppler imaging.
When Should You Choose or Answer TTE?
TTE is appropriate in a wide range of clinical situations, including:
TTE is the second most commonly performed cardiac test after the EKG.
What Is the Most Accurate Diagnostic Test?
Although TTE provides extensive structural and functional information, other tests are more accurate for specific purposes:
Thus, while TTE is an excellent first-line imaging study, it is not the single most accurate test for many specific conditions.
What Is a Transthoracic Echocardiogram (TTE)?
A transthoracic echocardiogram (TTE) is the standard, noninvasive ultrasound study of the heart. It provides detailed information about cardiac chamber size, ventricular function, valvular structure and motion, intracardiac masses, pericardial effusion, and aspects of aortic disease. Because it is safe, painless, and widely available, TTE is one of the most commonly used imaging tests in cardiology and serves as a cornerstone of cardiac evaluation.
How Is a TTE Performed?
The test is done by placing a sonographic transducer on the anterior chest wall (usually in the parasternal, apical, and subcostal windows). The transducer emits ultrasound waves that bounce off cardiac structures and return as high-resolution images. TTE provides real-time visualization of heart motion, wall thickening, valve opening and closing, and blood flow patterns when combined with Doppler imaging.
When Should You Choose or Answer TTE?
TTE is appropriate in a wide range of clinical situations, including:
- Any patient with an auscultated murmur or valvular abnormality to assess severity and structural impact.
- All patients with suspected or known congestive heart failure (CHF) to measure ejection fraction, which helps distinguish systolic vs. diastolic dysfunction—a crucial step because treatment differs significantly between the two.
- Evaluation of intracardiac masses, suspected tumors, thrombi, or vegetations when TEE is not yet indicated.
- Initial evaluation of pericardial effusion or suspected tamponade.
- General assessment of structural heart disease and ventricular function.
TTE is the second most commonly performed cardiac test after the EKG.
What Is the Most Accurate Diagnostic Test?
Although TTE provides extensive structural and functional information, other tests are more accurate for specific purposes:
- Transesophageal echocardiography (TEE) is more sensitive for evaluating the posterior cardiac structures, left atrial appendage, valves, and thoracic aorta.
- Coronary angiography remains the gold standard for identifying coronary artery stenosis and is more accurate for diagnosing obstructive coronary disease.
Thus, while TTE is an excellent first-line imaging study, it is not the single most accurate test for many specific conditions.

- Published on
Diagnostic Tests – Transesophageal Echocardiography (TEE)
What Is Transesophageal Echocardiography (TEE)?
Transesophageal echocardiography is a highly sensitive and detailed form of cardiac ultrasound in which images of the heart are obtained from within the esophagus rather than across the chest wall. Because the esophagus sits directly behind the heart, TEE provides superior visualization of posterior cardiac structures and is far more sensitive than transthoracic echocardiography (TTE) for detecting abnormalities of the left atrium, atrial appendage, mitral valve, and thoracic aorta.
TEE is especially useful for identifying conditions such as aortic dissection, thoracic aortic aneurysm, atrial thrombi, patent foramen ovale, and infective endocarditis vegetations.
How Is TEE Performed?
TEE is conducted by passing a flexible endoscopic probe with an ultrasound transducer at its tip through the patient’s mouth and into the esophagus. After mild sedation and local throat anesthesia, the probe is positioned behind the heart, where it emits ultrasound waves and captures high-resolution images unobstructed by the chest wall, lungs, or ribs.
This proximity allows for exceptionally clear visualization of cardiac chambers, valves, and the proximal aorta.
When Should You Choose or Answer TEE?
TEE is indicated when:
What Is the Most Accurate Diagnostic Test?
Although TEE is the most sensitive noninvasive method for visualizing many cardiac structures, the most accurate diagnostic test overall for coronary anatomy is left-heart cardiac catheterization (coronary angiography).
Catheterization provides direct measurement of coronary stenosis and remains the gold standard for diagnosing obstructive coronary artery disease.
What Is Transesophageal Echocardiography (TEE)?
Transesophageal echocardiography is a highly sensitive and detailed form of cardiac ultrasound in which images of the heart are obtained from within the esophagus rather than across the chest wall. Because the esophagus sits directly behind the heart, TEE provides superior visualization of posterior cardiac structures and is far more sensitive than transthoracic echocardiography (TTE) for detecting abnormalities of the left atrium, atrial appendage, mitral valve, and thoracic aorta.
TEE is especially useful for identifying conditions such as aortic dissection, thoracic aortic aneurysm, atrial thrombi, patent foramen ovale, and infective endocarditis vegetations.
How Is TEE Performed?
TEE is conducted by passing a flexible endoscopic probe with an ultrasound transducer at its tip through the patient’s mouth and into the esophagus. After mild sedation and local throat anesthesia, the probe is positioned behind the heart, where it emits ultrasound waves and captures high-resolution images unobstructed by the chest wall, lungs, or ribs.
This proximity allows for exceptionally clear visualization of cardiac chambers, valves, and the proximal aorta.
When Should You Choose or Answer TEE?
TEE is indicated when:
- Transthoracic echo is inadequate due to poor acoustic windows (obesity, COPD, chest wall deformities).
- There is a need to evaluate posterior cardiac structures, including:
- Left atrial or left atrial appendage thrombus
- Endocarditis with suspected valvular vegetations
- Suspected PFO or intracardiac shunts
- Suspected aortic dissection or aneurysm
What Is the Most Accurate Diagnostic Test?
Although TEE is the most sensitive noninvasive method for visualizing many cardiac structures, the most accurate diagnostic test overall for coronary anatomy is left-heart cardiac catheterization (coronary angiography).
Catheterization provides direct measurement of coronary stenosis and remains the gold standard for diagnosing obstructive coronary artery disease.

- Published on
Diagnostic Tests – Tilt-Table Testing
What Is Tilt-Table Testing?
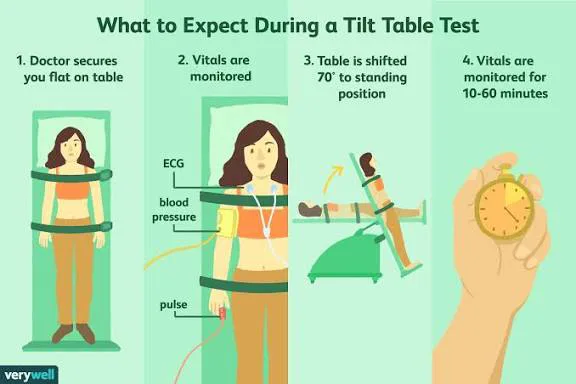
Tilt-table testing is a diagnostic procedure used to evaluate unexplained syncope, particularly when fainting episodes may be related to autonomic dysfunction or abnormal cardiovascular reflexes. The test involves monitoring blood pressure and heart rate while the patient is gradually tilted from a lying to an upright position. By changing the angle of the patient’s body, clinicians can observe how the cardiovascular system responds to positional changes that mimic everyday standing.
How Is Tilt-Table Testing Performed?
The patient is secured on a motorized table that can be tilted to various angles. Blood pressure and heart rate are recorded at baseline and during each positional shift. The test attempts to reproduce symptoms such as dizziness, lightheadedness, or syncope.
An abnormal result occurs when tilting produces:
- Syncope or near-syncope
- Significant dizziness
- An inappropriate or exaggerated drop in blood pressure
- Inadequate compensatory heart rate response (e.g., inappropriate bradycardia)
To enhance sensitivity, medications such as isoproterenol or nitroglycerin may be used as provocative agents, increasing the likelihood of triggering symptoms in susceptible patients.
When Is Tilt-Table Testing the Correct Answer?
Tilt-table testing is appropriate in cases of unexplained syncope, particularly when initial evaluation (history, physical exam, EKG, and routine labs) does not reveal a clear cause. It is especially valuable when syncope appears related to orthostatic changes, such as:
- Episodes of fainting when standing
- Symptoms consistent with neurocardiogenic (vasovagal) syncope
- A paradoxical or inappropriate bradycardia upon standing
- Suspected autonomic dysfunction
In these situations, a tilt-table test helps confirm whether syncope is due to abnormal autonomic reflexes rather than cardiac arrhythmias, structural disease, or neurologic disorders.
- Published on
Click here to start customizing
- Published on
Diagnostic Tests – Sestamibi Testing
What Is Sestamibi Testing?
Sestamibi testing—often referred to by its tracer name Tc-99m sestamibi—is a form of nuclear stress testing used to evaluate myocardial perfusion. It involves injecting a radiopharmaceutical (technetium-99m) that accumulates in healthy, well-perfused myocardial tissue. Because the tracer depends on both blood flow and viable cardiac cells, areas of ischemia or infarction appear as perfusion defects on imaging. Like other nuclear stress tests, it helps determine whether chest pain or abnormal EKG findings are due to underlying coronary artery disease.
How Is the Test Performed?
During the procedure, Tc-99m–labeled compounds are injected into the bloodstream during both stress and rest phases. A gamma camera then captures images of tracer uptake in the myocardium.
Healthy tissue receives adequate blood flow and shows normal tracer uptake, whereas diseased, ischemic, or infarcted myocardium demonstrates reduced uptake. The pattern of defect behavior is key:
- Reversible defect: reduced uptake during stress but improved at rest → ischemia (viable myocardium that becomes underperfused during stress).
- Fixed defect: reduced uptake on both stress and rest images → infarcted or scarred myocardium.
This allows clinicians to distinguish between viable, at-risk myocardium and areas of permanent damage.
When Should You Choose Sestamibi Testing?
The most practical “Kaplan-style” indication is that Tc-99m sestamibi is the preferred nuclear stress test in certain patient populations where standard imaging methods are limited by technical barriers. It is particularly useful in:
- Obese patients, where ultrasound penetration for stress echocardiography is poor
- Female patients with large breasts, where breast tissue can interfere with echo imaging or make exercise EKG less reliable
Because sestamibi imaging provides clearer results in these scenarios, it is often selected when other stress modalities may produce nondiagnostic images or false results.
- Published on
Diagnostic Tests – Dobutamine Stress Testing
What Is Dobutamine Stress Testing?
Dobutamine stress testing is a type of pharmacologic stress test used to evaluate myocardial perfusion and detect ischemia without requiring physical exercise. It is a noninvasive alternative to traditional treadmill testing and is particularly valuable when assessing patients who cannot achieve adequate exercise levels due to physical limitations, illness, or frailty. By stimulating the heart pharmacologically, the test reproduces the physiologic effects of exercise, allowing clinicians to identify areas of the myocardium that become ischemic under increased demand.
How Is the Test Performed?
Dobutamine, a beta-1 adrenergic agonist, is administered intravenously in gradually increasing doses. This medication increases heart rate and myocardial contractility, creating inotropic and chronotropic stress similar to exercise.
During infusion, a stress echocardiogram is performed. Clinicians watch for the development of new regional wall motion abnormalities, which indicate ischemia. Normal myocardium contracts more vigorously with dobutamine, while ischemic segments show impaired or reduced motion when stressed. This imaging pattern helps pinpoint areas of inadequate coronary blood flow.
When Should Dobutamine Stress Testing Be Used?
Dobutamine stress testing is the correct choice when a patient cannot perform adequate physical exercise and needs evaluation for ischemic heart disease. Typical scenarios include:
• A patient with a history of chest pain, but with an equivocal clinical picture
• A case where the resting EKG is nondiagnostic or uninterpretable
• Situations where pharmacologic stress is needed but Persantine (dipyridamole) cannot be used—particularly in patients with reactive airway diseases such as asthma, COPD, or emphysema
• Any patient with contraindications to vasodilator stress agents who still requires noninvasive assessment of myocardial perfusion
Its indications closely mirror those for Persantine thallium testing, but dobutamine is preferred in respiratory disease.
What Is the Most Accurate Diagnostic Test?
Although dobutamine stress testing is an effective and widely used noninvasive method for detecting myocardial ischemia, the most accurate test of myocardial perfusion remains the coronary angiogram. Angiography provides direct visualization of coronary artery anatomy and remains the gold standard for confirming obstructive coronary artery disease.
Diagnostic Tests – Dobutamine Stress Testing
What Is Dobutamine Stress Testing?
Dobutamine stress testing is a type of pharmacologic stress test used to evaluate myocardial perfusion and detect ischemia without requiring physical exercise. It is a noninvasive alternative to traditional treadmill testing and is particularly valuable when assessing patients who cannot achieve adequate exercise levels due to physical limitations, illness, or frailty. By stimulating the heart pharmacologically, the test reproduces the physiologic effects of exercise, allowing clinicians to identify areas of the myocardium that become ischemic under increased demand.
How Is the Test Performed?
Dobutamine, a beta-1 adrenergic agonist, is administered intravenously in gradually increasing doses. This medication increases heart rate and myocardial contractility, creating inotropic and chronotropic stress similar to exercise.
During infusion, a stress echocardiogram is performed. Clinicians watch for the development of new regional wall motion abnormalities, which indicate ischemia. Normal myocardium contracts more vigorously with dobutamine, while ischemic segments show impaired or reduced motion when stressed. This imaging pattern helps pinpoint areas of inadequate coronary blood flow.
When Should Dobutamine Stress Testing Be Used?
Dobutamine stress testing is the correct choice when a patient cannot perform adequate physical exercise and needs evaluation for ischemic heart disease. Typical scenarios include:
• A patient with a history of chest pain, but with an equivocal clinical picture
• A case where the resting EKG is nondiagnostic or uninterpretable
• Situations where pharmacologic stress is needed but Persantine (dipyridamole) cannot be used—particularly in patients with reactive airway diseases such as asthma, COPD, or emphysema
• Any patient with contraindications to vasodilator stress agents who still requires noninvasive assessment of myocardial perfusion
Its indications closely mirror those for Persantine thallium testing, but dobutamine is preferred in respiratory disease.
What Is the Most Accurate Diagnostic Test?
Although dobutamine stress testing is an effective and widely used noninvasive method for detecting myocardial ischemia, the most accurate test of myocardial perfusion remains the coronary angiogram. Angiography provides direct visualization of coronary artery anatomy and remains the gold standard for confirming obstructive coronary artery disease.

- Published on
Diagnostic Tests – Thallium Stress Testing
What Is Thallium Stress Testing?
Thallium stress testing is a nuclear imaging method used to evaluate myocardial perfusion and detect areas of ischemia. It is considered the most accurate noninvasive technique for assessing blood flow to the heart muscle without performing coronary angiography. During this test, a radioactive tracer—thallium-201—is injected into the bloodstream. Because thallium behaves similarly to potassium, healthy myocardial cells take it up readily. Areas with reduced blood flow, however, demonstrate decreased tracer uptake, allowing clinicians to visualize perfusion deficits both at rest and under stress conditions.
When Is Thallium Stress Testing the Correct Answer?
Thallium stress testing is often chosen as an alternative to stress echocardiography, especially when evaluation of ischemia requires imaging that does not rely on ultrasound. It is particularly indicated when resting EKG abnormalities make standard exercise EKG interpretation unreliable, such as in patients with:
In these cases, EKG changes alone cannot reliably detect ischemia, so thallium imaging provides crucial additional information.
Thallium scanning is also used to:
What Is the Most Accurate Test?
Although thallium stress testing is the most accurate noninvasive method of assessing myocardial perfusion, the gold standard—and most accurate overall diagnostic test—is coronary angiography. Angiography allows direct visualization of the coronary arteries and provides precise information about the presence, location, and severity of stenosis.
What Is Thallium Stress Testing?
Thallium stress testing is a nuclear imaging method used to evaluate myocardial perfusion and detect areas of ischemia. It is considered the most accurate noninvasive technique for assessing blood flow to the heart muscle without performing coronary angiography. During this test, a radioactive tracer—thallium-201—is injected into the bloodstream. Because thallium behaves similarly to potassium, healthy myocardial cells take it up readily. Areas with reduced blood flow, however, demonstrate decreased tracer uptake, allowing clinicians to visualize perfusion deficits both at rest and under stress conditions.
When Is Thallium Stress Testing the Correct Answer?
Thallium stress testing is often chosen as an alternative to stress echocardiography, especially when evaluation of ischemia requires imaging that does not rely on ultrasound. It is particularly indicated when resting EKG abnormalities make standard exercise EKG interpretation unreliable, such as in patients with:
- Left bundle branch block (LBBB)
- Baseline ST-segment abnormalities
- Left ventricular hypertrophy with strain pattern
- A ventricular pacemaker
- Digoxin effects on the EKG
In these cases, EKG changes alone cannot reliably detect ischemia, so thallium imaging provides crucial additional information.
Thallium scanning is also used to:
- Localize the specific region of ischemia within the myocardium
- Assess the success of revascularization after coronary artery bypass grafting (CABG) or angioplasty
- Provide a perfusion map that helps guide further testing or management
What Is the Most Accurate Test?
Although thallium stress testing is the most accurate noninvasive method of assessing myocardial perfusion, the gold standard—and most accurate overall diagnostic test—is coronary angiography. Angiography allows direct visualization of the coronary arteries and provides precise information about the presence, location, and severity of stenosis.

- Published on
Diagnostic Tests – Persantine Thallium
What Is Persantine Thallium Testing?
Persantine thallium testing is a type of pharmacologic stress test used to evaluate myocardial perfusion in patients who cannot perform adequate physical exercise. Instead of using a treadmill or bicycle to increase the heart’s oxygen demand, this test uses medication to mimic the physiologic effects of exercise. It is noninvasive and helps determine whether areas of the heart receive sufficient blood flow under conditions that simulate stress.
How Is the Test Performed?
The test involves two major components: Persantine (dipyridamole) and thallium imaging.
Persantine is a phosphodiesterase inhibitor that causes coronary artery vasodilation, increasing blood flow to healthy myocardium. Diseased or stenotic coronary arteries, however, do not dilate as effectively, creating a “steal phenomenon” in which more blood flows to normal areas and less to ischemic areas.
After Persantine is administered, thallium, a radioactive tracer, is injected. Normal cardiac muscle takes up thallium readily, whereas ischemic or infarcted areas absorb significantly less. Imaging with a gamma camera then reveals patterns of perfusion, highlighting areas of reduced blood flow.
When Should You Choose Persantine Thallium Testing?
Persantine thallium is the correct diagnostic choice when a patient cannot exercise adequately for a standard treadmill stress test—but still requires evaluation of possible ischemic heart disease. This includes individuals with orthopedic limitations, neurologic conditions, deconditioning, or severe physical frailty.
It is also useful in preoperative cardiac risk assessment for patients with chest pain, when there is uncertainty about whether the pain represents ischemia.
When Is Persantine Thallium the Wrong Answer?
This test should NOT be selected in patients with asthma, COPD, or emphysema, because Persantine can provoke bronchospasm and worsen respiratory symptoms.
Additionally, any form of stress testing—including pharmacologic testing—is contraindicated in cases of acute myocardial infarction or unstable angina, where stressing the heart is unsafe and inappropriate.
What Is the Alternative Choice?
If Persantine cannot be used—especially due to respiratory disease—the preferred alternative is a dobutamine stress echocardiogram. Dobutamine increases myocardial oxygen demand by raising heart rate and contractility, functioning as a safe pharmacologic stress agent for patients who cannot tolerate Persantine.
What Is the Most Accurate Diagnostic Test?
Regardless of the stress modality used, the single most accurate test of myocardial perfusion and coronary anatomy is coronary angiography. It provides direct visualization of the coronary vessels, allowing clinicians to identify and quantify stenoses with precision

