- Published on
Emergency and Acute Medicine – Osteoporosis
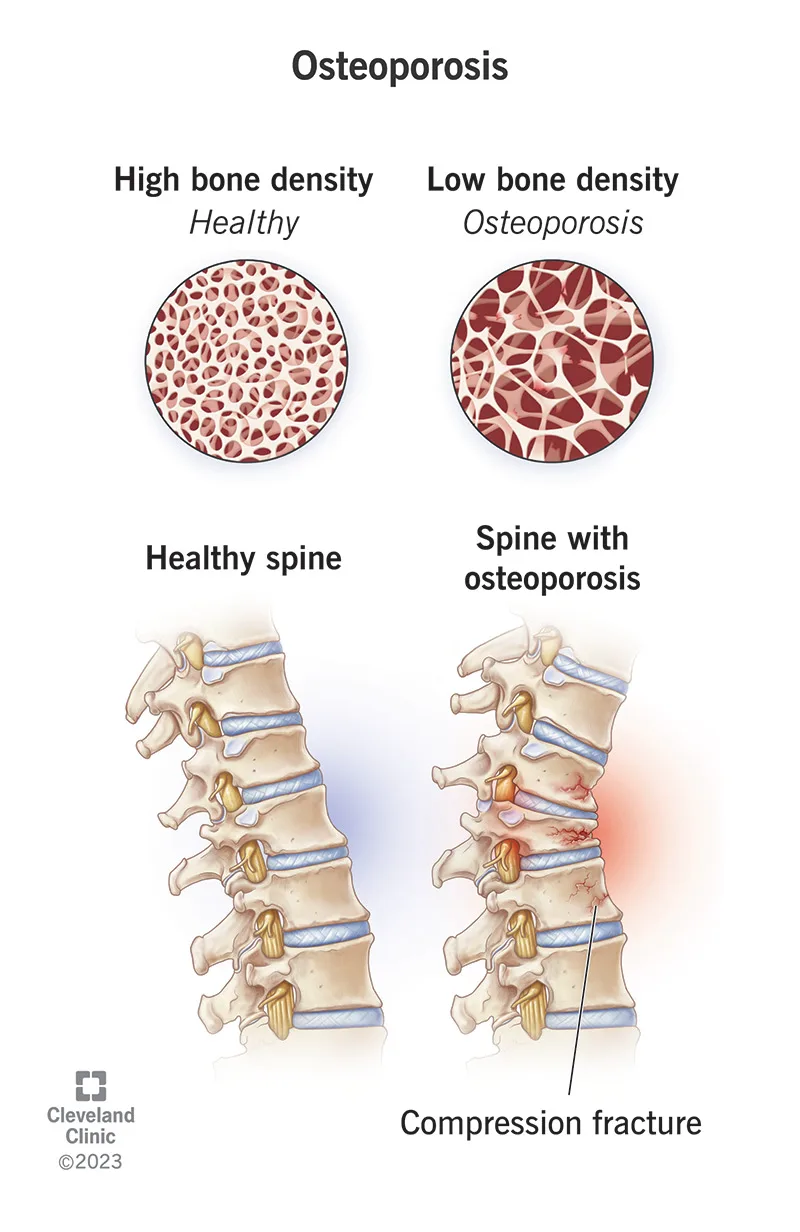
Osteoporosis is characterized by a diffuse decrease in skeletal mass, with trabecular bone—particularly in the vertebrae and femur—affected earlier and more severely than cortical bone. Although the disease process begins in adolescence, fractures typically do not manifest until age 50 years or older. Females are affected far more commonly than males, especially following menopause.
The underlying mechanism is an imbalance between bone resorption and bone formation, with resorption predominating. Advanced age is the most significant risk factor. Additional contributors include inadequate dietary calcium intake, particularly early in life, a sedentary lifestyle with lack of weight-bearing activity, and estrogen deficiency after menopause. Other important risk factors include long-term corticosteroid use, alcoholism, methotrexate therapy, tobacco use, low body weight, and familial predisposition. Pediatric patients are generally asymptomatic despite early onset of bone loss.
Osteoporosis is usually clinically silent until pathologic fractures occur. Fractures resulting from minimal trauma or recurrent fractures are hallmark features. The vertebral column is most commonly involved, with multiple compression fractures often leading to kyphosis and scoliosis. Hip fractures, including femoral neck and intertrochanteric fractures, are also frequent. A history of fractures after low-energy mechanisms or a family history of osteoporosis should raise suspicion. Physical examination findings typically relate to the acute fracture rather than the underlying disease itself.
Evaluation focuses on identifying fractures without significant mechanisms and assessing risk factors. A careful neurovascular examination distal to femoral or other extremity fractures is essential. In patients with vertebral fractures, rectal tone and postvoid residual should be assessed. Plain radiographs of suspected fractures may show osteopenia, though this is a late finding. Spine films may reveal old compression fractures. Computed tomography is recommended for vertebral fractures to assess for retropulsion and spinal canal compromise, which may not be evident on plain films.
Laboratory studies such as serum calcium, parathyroid hormone, and alkaline phosphatase can help differentiate osteoporosis from other metabolic bone disorders. Imaging with plain radiographs identifies fractures, but determining fracture age can be difficult. Bone scan or CT may help clarify fracture chronicity, particularly in the spine. Bone densitometry using dual-energy x-ray absorptiometry confirms the diagnosis, with a bone mineral density T-score of −2.5 or lower defining osteoporosis.
The differential diagnosis includes multiple myeloma or metastatic malignancy, osteogenesis imperfecta, hyperparathyroidism, and other demineralizing bone diseases. Management in the emergency setting prioritizes fracture care. Prehospital providers should minimize patient movement and report mechanism details suggestive of pathologic fracture. Initial treatment involves immobilization and standard fracture management, recognizing that healing may be delayed or incomplete. Orthotic back braces may be needed for vertebral fractures in consultation with orthopedics. Prevention remains more effective than acute treatment, and long-term therapy should be initiated or reinforced.
Pharmacologic therapy includes bisphosphonates such as alendronate or risedronate as first-line agents, with alternatives including zoledronic acid, raloxifene, denosumab, calcitonin, parathyroid hormone analogs, and, in selected cases, estrogen therapy. Adequate calcium and vitamin D supplementation are essential. Admission decisions follow standard orthopedic protocols, with particular attention to age, mobility, neurologic symptoms, and social factors. Compression fractures are often stable, but cervical fractures or those with neurologic deficits require admission and emergent specialty consultation.
Key points include recognizing recurrent or low-energy fractures as suggestive of osteoporosis, understanding that osteopenia on plain radiographs is a late but important clue, and initiating referral for definitive evaluation and treatment. Bisphosphonates remain first-line therapy for long-term management, and coordinated follow-up is critical to prevent future fractures.
- Published on
Emergency and Acute Medicine – Neonatal Jaundice
Neonatal jaundice results from an imbalance between bilirubin production and elimination. Newborns produce bilirubin at a higher rate than adults because of increased red blood cell mass and a shorter red blood cell lifespan. At the same time, especially in preterm infants, hepatic conjugation and biliary excretion of bilirubin are immature. Increased enterohepatic circulation and reduced bilirubin binding to albumin further contribute to elevated bilirubin levels. In most newborns, this process leads to physiologic jaundice, which is benign and self-limited.
In physiologic jaundice, bilirubin levels typically rise from approximately 1.5 mg/dL in cord blood to a mean peak of about 6.5 mg/dL by the third day of life, then gradually decline to less than 1.5 mg/dL by 10–12 days of age. However, when bilirubin levels rise excessively or rapidly, they may overwhelm neuroprotective mechanisms. Unbound bilirubin can cross the blood–brain barrier and deposit in the basal ganglia, hippocampus, brainstem nuclei, and cerebellum, leading to bilirubin-induced neurologic dysfunction (BIND). This spectrum ranges from mild neurologic dysfunction to acute bilirubin encephalopathy (ABE) in the first week of life, and to kernicterus, the chronic and often devastating form associated with permanent neurologic sequelae such as choreoathetoid cerebral palsy, gaze abnormalities, hearing loss, and dental dysplasia. Severe cases may result in coma, seizures, respiratory failure, and death.
The progression and severity of bilirubin neurotoxicity depend on multiple factors, including the rate and duration of bilirubin elevation, albumin-binding capacity, levels of unbound bilirubin, host susceptibility, and the presence of comorbidities. Risk factors for severe hyperbilirubinemia include jaundice in the first 24 hours of life, high predischarge total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) levels, lower gestational age (35–38 weeks), exclusive breastfeeding with inadequate intake and excessive weight loss, hemolytic disease, a family history of neonatal jaundice, cephalohematoma or significant bruising, and East Asian ethnicity. Neurotoxicity risk is further increased by isoimmune hemolytic disease, G6PD deficiency, asphyxia, sepsis, acidosis, low albumin levels, and post-phototherapy bilirubin rebound.
Etiologies of neonatal jaundice are broadly divided into unconjugated and conjugated hyperbilirubinemia. Unconjugated causes include physiologic jaundice, breastfeeding failure jaundice due to inadequate milk intake in the first week of life, and breast milk jaundice, which typically begins after day 3–5 and may persist for several weeks. Hemolytic causes include ABO or Rh incompatibility, red cell enzyme deficiencies such as G6PD deficiency, and membrane disorders like hereditary spherocytosis. Other contributors include sepsis, birth trauma with increased heme load, polycythemia, infants of diabetic mothers, congenital hypothyroidism, and inherited defects of bilirubin conjugation such as Gilbert syndrome or Crigler–Najjar syndrome. Conjugated hyperbilirubinemia reflects impaired excretion and is always pathologic, with causes including neonatal hepatitis, biliary atresia, extrahepatic obstruction, shock liver, and neonatal hemosiderosis.
Clinically, affected infants may present with sleepiness, poor feeding, decreased urine output, or signs of dehydration. Early ABE is characterized by feeding difficulties, hypotonia, irritability, and lethargy. Intermediate stages include a high-pitched cry, fever, and increased tone with retrocollis and opisthotonos. Advanced ABE presents with severe hypertonia, seizures, coma, and abnormal movements. On examination, jaundice manifests as yellow discoloration of the skin and sclera, progressing in a cephalocaudal pattern as bilirubin levels rise. Visual assessment alone is unreliable, particularly in infants with darker skin tones. Neurologic abnormalities such as altered tone and the “setting sun” sign should raise concern for neurotoxicity.
Evaluation requires prompt measurement of total serum bilirubin in any infant with suspected or visible jaundice. The initial bilirubin level must be fractionated into unconjugated and conjugated components. TSB values must always be interpreted according to the infant’s age in hours, not days, and plotted on an age-specific nomogram to assess risk and guide treatment decisions. TcB measurements correlate well with TSB when available. Further evaluation is warranted when jaundice appears in the first 24 hours, persists beyond the first week, reaches phototherapy thresholds, involves elevated conjugated bilirubin, or is associated with signs of ABE. Additional laboratory studies may include serum albumin, electrolytes, renal function, complete blood count, reticulocyte count, blood type, direct Coombs test, and sepsis evaluation when indicated.
Management is time-sensitive, as outcomes are closely linked to the duration and severity of bilirubin exposure. Infants with signs of encephalopathy require immediate treatment. Phototherapy should be initiated when TSB exceeds threshold levels based on age in hours and risk stratification. Intensive phototherapy involves high irradiance delivered to as much of the infant’s surface area as possible, with eye protection in place, and should result in a bilirubin decline of more than 0.5 mg/dL per hour. Exchange transfusion is indicated for infants who meet age-specific thresholds, fail to respond to intensive phototherapy, or exhibit signs of ABE, and requires neonatal intensive care support. Intravenous immunoglobulin may be considered in isoimmune hemolytic disease when bilirubin levels approach exchange thresholds.
Supportive care includes ensuring adequate hydration, correcting dehydration with intravenous fluids when necessary, and optimizing feeding. Breastfeeding should generally continue, with increased feeding frequency and supplementation as needed. Temporary cessation of breastfeeding may be considered in refractory breast milk jaundice, with maternal milk expression encouraged to maintain lactation. Underlying conditions such as sepsis, hypothyroidism, or polycythemia must be identified and treated promptly.
Hospital admission is required for infants needing intensive phototherapy, exchange transfusion, or evaluation of significant anemia, infection, dehydration, or suspected obstructive liver disease. Stable term infants with uncomplicated hyperbilirubinemia below treatment thresholds may be managed with close outpatient follow-up or home phototherapy when appropriate. Clear communication with primary care providers and timely follow-up—often within 8–12 hours—is essential to prevent progression to severe hyperbilirubinemia.
A key principle in the emergency setting is that bilirubin levels must always be interpreted in the context of postnatal age in hours and individual risk factors. Early recognition, prompt initiation of phototherapy when indicated, and careful assessment of feeding and hydration are critical to preventing irreversible neurologic injury.

- Published on
Emergency and Acute Medicine – Otitis Externa
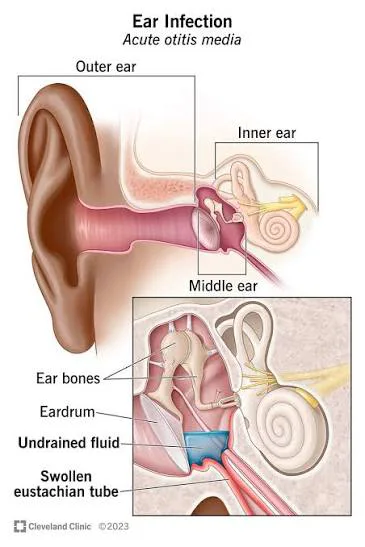
Otitis externa is an inflammation or infection of the auricle, external auditory canal, or the external surface of the tympanic membrane, while sparing the middle ear. It affects approximately 4 per 1,000 individuals in the United States and is commonly referred to as “swimmer’s ear” due to its frequent association with recent swimming or water exposure, although it may also occur after routine bathing. A severe form, necrotizing (malignant) otitis externa, begins in the ear canal and can extend into periauricular tissues and the skull base. This form occurs most often in elderly patients, those with diabetes, or immunocompromised individuals, is commonly caused by Pseudomonas aeruginosa, and carries a mortality rate of up to 20%.
The condition is often precipitated by trauma or abrasion of the ear canal or by maceration of the skin from prolonged moisture or excessive dryness. Predisposing factors include prior ear surgery or tympanic membrane perforation, narrow or abnormal ear canals, humidity, allergies, eczema, trauma, and abnormal cerumen production. Common pathogens include Pseudomonas aeruginosa, Staphylococcus aureus, streptococcal species, and less commonly fungal organisms.
Patients typically present with a history of recent swimming or water exposure and may report itching of the ear canal as the earliest symptom. This is often followed over one to two days by progressive ear pain, ear drainage, decreased hearing, and a sensation of ear fullness or clogging. In patients with diabetes or immunosuppression, clinicians should specifically inquire about systemic symptoms and risk factors. On examination, pain is elicited with movement of the pinna or tragus, and the external ear canal is usually swollen, erythematous, and tender, often with visible drainage or debris. Decreased auditory acuity and preauricular swelling may be present. Necrotizing otitis externa may present with severe otalgia, headache, otorrhea, periauricular swelling, and cranial nerve palsies, most commonly involving the facial nerve.
Diagnosis is primarily clinical, based on characteristic history and physical findings. Otoscopic examination typically reveals an edematous, erythematous ear canal with purulent, cheesy white, or gray-green exudate. Laboratory studies are not routinely required unless necrotizing otitis externa is suspected, in which case evaluation may include white blood cell count, erythrocyte sedimentation rate, serum glucose, and cultures. Computed tomography or magnetic resonance imaging is indicated when there are signs of systemic toxicity, suspected bony involvement, or concern for mastoiditis. Debris removal from the ear canal using gentle curettage or irrigation is both diagnostic and therapeutic, and wick placement may be necessary to ensure medication penetration in markedly edematous canals.
The differential diagnosis includes otitis media, folliculitis, foreign bodies in the ear canal, herpes zoster oticus, parotitis, mastoiditis, dental abscess, sinusitis, temporomandibular joint disorders, and cervical adenitis. In children, an ear canal foreign body should be considered when purulent drainage is present.
Management focuses on pain control, eradication of infection, and prevention of recurrence. Treatment begins with gentle cleansing of the external auditory canal to remove debris, sometimes requiring suction or curettage. A cotton or gauze wick may be placed in cases of severe canal edema. Most cases respond well to topical therapy using antiseptic, anti-inflammatory, and antibacterial ear drops. Acetic acid solutions, combination antibiotic-steroid drops, or fluoroquinolone drops such as ofloxacin are commonly used, with ofloxacin preferred when tympanic membrane perforation is suspected. Oral antibiotics are reserved for patients with facial or neck cellulitis, severe canal edema, concurrent otitis media, or immunocompromised status. Diabetic and immunocompromised patients should be treated with oral ciprofloxacin and monitored closely for progression to necrotizing otitis externa. Intravenous antibiotics and possible surgical debridement are required for necrotizing disease or severe systemic illness.
Most patients can be safely discharged with close follow-up. Admission is indicated for necrotizing otitis externa, significant pinna involvement, or signs of systemic illness. Discharge instructions should emphasize keeping the ear dry, avoiding swimming for three to four weeks, proper use of prescribed medications, and returning promptly for worsening pain, fever, hearing loss, or neurologic symptoms. Follow-up within two to three days is recommended, particularly for wick removal or if symptoms fail to improve.
Key clinical pearls include recognizing that erythema of the tympanic membrane in otitis externa may mimic otitis media, avoiding ear canal lavage until tympanic membrane integrity is confirmed, and ensuring adequate medication penetration by clearing obstructing debris. Recurrence can often be prevented through patient education focused on minimizing moisture, trauma, and irritant exposure to the external ear canal. Necrotizing otitis externa should always be suspected in diabetics or immunocompromised patients with severe ear pain, purulent otorrhea, and granulation tissue or exposed bone in the ear canal.

- Published on
Emergency and Acute Medicine – Paget Disease
Paget disease, also known as osteitis deformans, is a disorder of bone remodeling characterized by excessive resorption of normal bone followed by replacement with disorganized, fibrous, and sclerotic bone. The disease is usually focal and most commonly affects the pelvis, femur, skull, tibia, and spine, particularly the lumbar spine. It occurs in approximately 1–2% of individuals older than 55 years, with incidence increasing with age. Many patients are asymptomatic, and the disease is often discovered incidentally on radiographs or through elevated alkaline phosphatase levels.
The disease begins with an osteolytic phase in which osteoclasts aggressively resorb healthy bone. This phase is associated with increased bone vascularity, predisposing patients to hematoma formation and pathologic fractures. Over time, the resorbed bone is replaced by dense, irregular trabecular bone in the osteoplastic phase, forming a characteristic mosaic pattern. Although malignant transformation is rare, occurring in about 1% of cases, osteosarcoma is the primary malignancy of concern. Paget disease is more common in men and individuals of European descent and is rare in children.
The etiology remains unclear, though both genetic and environmental factors are implicated. Mutations in the SQSTM1 gene have been identified in many cases, and viral inclusions seen in osteoclasts suggest a possible association with paramyxoviruses. Environmental factors such as rural living and exposure to farm animals may also contribute.
Clinical presentation varies widely. Many patients remain asymptomatic, while others develop deep, aching bone pain later in the disease course. Pain may worsen with weight bearing when the femur or tibia is involved or with rest when non–weight-bearing bones are affected. During the acute osteolytic phase, patients are at risk for pathologic fractures, hypercalcemia, renal stones, and bleeding due to hypervascular bone. In widespread disease, increased bone blood flow may lead to high-output cardiac failure. In the osteoplastic phase, long-bone involvement can cause deformity, gait abnormalities, and swelling. Skull involvement may lead to headaches, cranial nerve compression, hearing loss, or changes in head size, while spinal disease can cause neurologic compression.
Diagnosis is usually suggested by characteristic radiographic findings and supported by laboratory abnormalities. Alkaline phosphatase is the most sensitive marker of disease activity, while calcium and phosphate levels are typically normal unless complications such as fracture or immobilization occur. Imaging with plain radiographs often reveals lytic lesions, bone expansion, cortical thickening, or dense “ivory” bone. Radionuclide bone scans are useful to assess the extent and activity of disease, while CT or MRI helps evaluate complications such as neoplasm, hematoma, or spinal cord compression.
Emergency management focuses on complications rather than the underlying disease. Pathologic fractures require prompt immobilization to limit bleeding, and analgesia is provided with acetaminophen or opioids. Hypercalcemia is treated with intravenous fluids, calcitonin, and bisphosphonates as needed. Suspected neurologic compromise mandates urgent neurosurgical consultation. Definitive medical therapy is indicated for symptomatic patients or those with disease in high-risk locations and typically involves nitrogen-containing bisphosphonates such as alendronate, risedronate, pamidronate, or zoledronic acid.
Admission is indicated for patients with major trauma, significant bleeding, hypercalcemia, high-output cardiac failure, or neurologic compression. Stable patients with adequate pain control and no acute complications may be discharged with appropriate orthopedic and endocrinology follow-up. A key clinical pearl is that Paget disease is often an incidental diagnosis, and unexplained elevation of alkaline phosphatase or pathologic fracture in an older adult should prompt consideration of this condition.


- Published on
Emergency and Acute Medicine – Ovarian Cyst and Adnexal Torsion
Ovarian cysts are common gynecologic findings and are usually asymptomatic unless complicated by rupture, hemorrhage, infection, or torsion. The most frequent type is the follicular cyst, which can occur from fetal life through menopause. These cysts are typically thin-walled, unilocular, and measure between 3 and 8 cm. Because of their thin walls, they may rupture easily, often causing minimal bleeding and little pain. Midcycle rupture during ovulation is known as mittelschmerz and is generally benign.
Corpus luteal cysts are clinically more significant. They are usually smaller than 10 cm but are prone to intracystic hemorrhage. Rapid bleeding can lead to cyst rupture, most commonly just before the onset of menses, and may result in severe intraperitoneal hemorrhage. In some cases, gradual bleeding into the cyst or ovary causes capsular distension and pain even without rupture. Anticoagulated patients are at particularly high risk for significant bleeding from corpus luteal cysts.
Adnexal torsion is a true gynecologic emergency and represents the fifth most common surgical emergency in gynecology. It occurs when the ovary, fallopian tube, or a paratubal cyst twists around its vascular pedicle, leading to impaired lymphatic and venous drainage followed by arterial compromise. This process causes rapid adnexal enlargement, ischemia, and eventual necrosis if not promptly treated. The greatest risk of torsion is associated with ovarian cysts measuring 8–12 cm. Although torsion can occur at any age, it is most common in reproductive-age women, with approximately 15% of cases occurring in children. During pregnancy, torsion is most likely in the first trimester, especially following ovarian stimulation or in vitro fertilization.
Patients with ovarian cysts typically present with unilateral lower abdominal or pelvic pain that may be sharp or aching and intermittent or constant. Pain may be precipitated by exercise, intercourse, trauma, or pelvic examination. Fever is uncommon and suggests an alternative diagnosis. Menstrual irregularities, infertility, pregnancy status, and prior sexually transmitted infections should be assessed. In contrast, adnexal torsion often presents with sudden-onset, severe, colicky abdominal pain that may localize to one side or radiate to the groin or flank. Nausea and vomiting are common, and symptoms may wax and wane due to intermittent torsion and detorsion. Fever and vaginal bleeding may occur but are not universal.
Physical examination in ovarian cysts may reveal abdominal or adnexal tenderness and, occasionally, a palpable pelvic mass. In cases of hemorrhagic cyst rupture, signs of hypovolemia such as orthostasis, tachycardia, or hypotension may be present. Adnexal torsion similarly causes abdominal and adnexal tenderness and may be associated with a palpable mass. Severe cases can mimic other acute abdominal emergencies.
A pregnancy test is essential in all patients of reproductive age to exclude ectopic pregnancy. Initial laboratory evaluation includes a complete blood count to assess for anemia or infection and urinalysis to evaluate urinary causes of pain. If significant hemorrhage is suspected, type and crossmatching for packed red blood cells should be performed. Cervical cultures may be indicated if pelvic inflammatory disease is a concern.
Transvaginal ultrasound is the imaging modality of choice. It can identify ovarian cysts, adnexal masses, free pelvic fluid, and an enlarged, edematous ovary suggestive of torsion. Doppler flow studies may demonstrate decreased or absent blood flow, but the presence of flow does not exclude torsion, particularly if detorsion has occurred. MRI may be useful in pregnant patients with nondiagnostic ultrasound findings, while CT imaging can help identify alternative diagnoses or provide supportive evidence of torsion when ultrasound is inconclusive. Ultimately, laparoscopy remains the gold standard for diagnosing adnexal torsion and allows for definitive treatment.
The differential diagnosis includes ectopic pregnancy, pelvic inflammatory disease, appendicitis, endometriosis, round ligament pain, ovarian or metastatic neoplasm, and uterine torsion. In postmenopausal women, ovarian cysts are concerning for malignancy until proven otherwise.
Management depends on the diagnosis and clinical stability. Suspected adnexal torsion requires urgent gynecologic consultation and surgical intervention, as early detorsion improves the likelihood of ovarian salvage, particularly in pediatric patients. Ruptured ovarian cysts without significant hemorrhage may be managed conservatively with analgesia and close follow-up. Patients with ongoing pain, hemodynamic instability, or significant hemoperitoneum require admission and possible surgical management.
A key clinical pearl is that adnexal torsion is primarily a clinical diagnosis. Imaging studies may appear reassuring, but normal Doppler flow does not rule out torsion. Therefore, adnexal torsion should always remain high on the differential diagnosis in women and girls presenting with acute abdominal or pelvic pain.


- Published on
Emergency and Acute Medicine – Otitis Media
Otitis media is an inflammatory condition of the middle ear and is one of the most common infections encountered in early childhood, particularly between 6 and 36 months of age. It is characterized by a rapid onset of local and systemic symptoms and has a high recurrence rate, with more than one-third of children experiencing more than five episodes by the age of seven. Although it predominantly affects children, otitis media can also occur in adults.
The condition most often develops in association with upper respiratory tract infections, which lead to eustachian tube dysfunction and impaired drainage of the middle ear. Viral pathogens commonly implicated include parainfluenza virus, respiratory syncytial virus, influenza virus, adenovirus, and rhinovirus. Bacterial causes include Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilus influenzae, Streptococcus pyogenes, and Mycoplasma pneumoniae. Predisposing factors include impaired mucociliary function, immunodeficiency, nasotracheal intubation, and certain populations such as American Indians, Eskimos, and individuals with Down syndrome, cleft palate, diabetes, vitamin A deficiency, or HIV. Additional risk factors include daycare attendance, family history, exposure to parental smoking, pacifier use, and bottle-feeding.
Diagnosis is primarily clinical and follows the American Academy of Pediatrics 2013 guidelines. Otitis media should be diagnosed when there is moderate to severe bulging of the tympanic membrane, mild bulging of the tympanic membrane accompanied by recent onset of ear pain, or new otorrhea not attributable to otitis externa. The diagnosis should not be made in the absence of middle ear effusion, which is best assessed using pneumatic otoscopy or tympanometry. Recurrent otitis media is defined as three episodes within six months or four episodes within one year, with at least one episode occurring in the preceding six months.
Patients typically present with ear pain, irritability, fever, and symptoms of an upper respiratory infection such as rhinorrhea. Younger children may exhibit poor feeding, vomiting, diarrhea, or tugging at the ear, while older children and adults may complain of a plugged-ear sensation, vertigo, tinnitus, or conjunctivitis. On physical examination, the tympanic membrane often appears erythematous, inflamed, and bulging, with decreased mobility and obscured landmarks. New-onset otorrhea in the absence of otitis externa is also a key finding.
The essential evaluation includes careful otoscopic examination with full visualization of the tympanic membrane and assessment of its mobility. Laboratory testing is generally unnecessary, and cultures are not helpful unless obtained via tympanocentesis. Imaging, such as computed tomography, is reserved for suspected complications like mastoiditis. Tympanocentesis may be indicated in cases of severe pain or toxicity, failure of antimicrobial therapy, suspected suppurative complications, illness in neonates, or immunocompromised patients.
Management depends on age, severity, and laterality of infection. Many mild cases resolve spontaneously without antibiotics. Antibiotic therapy is recommended for all infants younger than six months, children younger than two years with bilateral otitis media, children older than six months with severe symptoms (persistent otalgia for more than 48 hours or fever ≥102.2°F), and cases with tympanic membrane rupture and drainage. In otherwise healthy children aged six months or older with mild symptoms or uncertain diagnosis, a period of observation with close follow-up in two to three days is appropriate, provided caregivers are reliable. Antipyretics and analgesics are essential for symptom control, while antihistamines, decongestants, and steroids have not shown proven benefit.
First-line antibiotic therapy typically includes high-dose amoxicillin, with amoxicillin–clavulanate or alternative agents such as azithromycin or cefuroxime used based on allergy history, recent antibiotic use, or local resistance patterns. Parenteral antibiotics are reserved for toxic-appearing infants, immunocompromised patients, or those unable to tolerate oral therapy.
Most patients can be safely discharged with appropriate treatment and follow-up. Admission is indicated for febrile or toxic children younger than one year, immunocompromised patients, those with significant dehydration, inability to tolerate oral intake, suspected serious associated infection, unreliable caregivers, or concern for abuse. Follow-up is recommended within 10–14 days to ensure resolution, with earlier reassessment if symptoms fail to improve within 24–48 hours or worsen.
Important complications of otitis media include recurrent infections, tympanic membrane perforation, serous otitis media, hearing loss, facial nerve injury, mastoiditis, cholesteatoma, meningitis, and other intracranial infections. A key clinical pearl is that in otherwise healthy children aged six months or older with mild symptoms, observation without immediate antibiotics and close follow-up is often a safe and effective approach.
Otitis media is an inflammatory condition of the middle ear and is one of the most common infections encountered in early childhood, particularly between 6 and 36 months of age. It is characterized by a rapid onset of local and systemic symptoms and has a high recurrence rate, with more than one-third of children experiencing more than five episodes by the age of seven. Although it predominantly affects children, otitis media can also occur in adults.
The condition most often develops in association with upper respiratory tract infections, which lead to eustachian tube dysfunction and impaired drainage of the middle ear. Viral pathogens commonly implicated include parainfluenza virus, respiratory syncytial virus, influenza virus, adenovirus, and rhinovirus. Bacterial causes include Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilus influenzae, Streptococcus pyogenes, and Mycoplasma pneumoniae. Predisposing factors include impaired mucociliary function, immunodeficiency, nasotracheal intubation, and certain populations such as American Indians, Eskimos, and individuals with Down syndrome, cleft palate, diabetes, vitamin A deficiency, or HIV. Additional risk factors include daycare attendance, family history, exposure to parental smoking, pacifier use, and bottle-feeding.
Diagnosis is primarily clinical and follows the American Academy of Pediatrics 2013 guidelines. Otitis media should be diagnosed when there is moderate to severe bulging of the tympanic membrane, mild bulging of the tympanic membrane accompanied by recent onset of ear pain, or new otorrhea not attributable to otitis externa. The diagnosis should not be made in the absence of middle ear effusion, which is best assessed using pneumatic otoscopy or tympanometry. Recurrent otitis media is defined as three episodes within six months or four episodes within one year, with at least one episode occurring in the preceding six months.
Patients typically present with ear pain, irritability, fever, and symptoms of an upper respiratory infection such as rhinorrhea. Younger children may exhibit poor feeding, vomiting, diarrhea, or tugging at the ear, while older children and adults may complain of a plugged-ear sensation, vertigo, tinnitus, or conjunctivitis. On physical examination, the tympanic membrane often appears erythematous, inflamed, and bulging, with decreased mobility and obscured landmarks. New-onset otorrhea in the absence of otitis externa is also a key finding.
The essential evaluation includes careful otoscopic examination with full visualization of the tympanic membrane and assessment of its mobility. Laboratory testing is generally unnecessary, and cultures are not helpful unless obtained via tympanocentesis. Imaging, such as computed tomography, is reserved for suspected complications like mastoiditis. Tympanocentesis may be indicated in cases of severe pain or toxicity, failure of antimicrobial therapy, suspected suppurative complications, illness in neonates, or immunocompromised patients.
Management depends on age, severity, and laterality of infection. Many mild cases resolve spontaneously without antibiotics. Antibiotic therapy is recommended for all infants younger than six months, children younger than two years with bilateral otitis media, children older than six months with severe symptoms (persistent otalgia for more than 48 hours or fever ≥102.2°F), and cases with tympanic membrane rupture and drainage. In otherwise healthy children aged six months or older with mild symptoms or uncertain diagnosis, a period of observation with close follow-up in two to three days is appropriate, provided caregivers are reliable. Antipyretics and analgesics are essential for symptom control, while antihistamines, decongestants, and steroids have not shown proven benefit.
First-line antibiotic therapy typically includes high-dose amoxicillin, with amoxicillin–clavulanate or alternative agents such as azithromycin or cefuroxime used based on allergy history, recent antibiotic use, or local resistance patterns. Parenteral antibiotics are reserved for toxic-appearing infants, immunocompromised patients, or those unable to tolerate oral therapy.
Most patients can be safely discharged with appropriate treatment and follow-up. Admission is indicated for febrile or toxic children younger than one year, immunocompromised patients, those with significant dehydration, inability to tolerate oral intake, suspected serious associated infection, unreliable caregivers, or concern for abuse. Follow-up is recommended within 10–14 days to ensure resolution, with earlier reassessment if symptoms fail to improve within 24–48 hours or worsen.
Important complications of otitis media include recurrent infections, tympanic membrane perforation, serous otitis media, hearing loss, facial nerve injury, mastoiditis, cholesteatoma, meningitis, and other intracranial infections. A key clinical pearl is that in otherwise healthy children aged six months or older with mild symptoms, observation without immediate antibiotics and close follow-up is often a safe and effective approach.
- Published on
Emergency and Acute Medicine – Otologic Trauma
Otologic trauma involves injury to the external, middle, or inner ear and may result from blunt, penetrating, barotrauma, thermal, chemical, or blast mechanisms. Injuries to the pinna are particularly concerning because auricular cartilage lacks a direct blood supply and depends on the perichondrium for nutrition. Disruption of this relationship, especially from hematoma formation, can lead to ischemia, perichondritis, cartilage necrosis, and permanent deformity such as cauliflower ear. Penetrating injuries and bite wounds increase the risk of cartilage infection.
The middle ear is an air-filled cavity containing the ossicles and is vulnerable to pressure-related injuries such as blasts or diving accidents. Because it is bordered by the temporal and mastoid bones and adjacent to the cranial vault, fractures in this region may result in cerebrospinal fluid otorrhea or rhinorrhea and disruption of the vestibular system. The facial nerve traverses the middle ear, and injury can result in peripheral facial nerve paralysis. Pediatric patients with otologic trauma should always be evaluated for possible nonaccidental injury.
Patients may present with severe ear pain, bleeding, or visible deformity of the auricle. Auricular hematomas typically appear as bluish, fluctuant, or doughy swellings of the pinna and are associated with loss of normal contour. Lacerations, partial avulsions, or complete amputations may be seen. Signs of middle ear trauma include decreased hearing, tinnitus, vertigo, nystagmus, facial nerve weakness, and canal drainage. Partial hearing loss suggests tympanic membrane rupture, whereas complete hearing loss raises concern for ossicular chain or inner ear injury. Findings suggestive of basilar skull fracture include hemotympanum, Battle sign, and cerebrospinal fluid leakage from the ear or nose.
History should focus on the mechanism of injury, associated trauma, prior otologic disease, and medication use. Physical examination must include a complete head and neck evaluation with careful inspection of the pinna, external auditory canal, tympanic membrane, cranial nerves, and hearing assessment. Tuning fork tests such as Weber and Rinne are useful to differentiate conductive from sensorineural hearing loss. Concomitant injuries must always be excluded in trauma patients.
Diagnosis is primarily clinical. Wound cultures are reserved for signs of infection. Imaging with head or facial CT is indicated when intracranial injury or skull fracture is suspected, while CT of the temporal bone without contrast is recommended for significant middle ear injury or facial nerve involvement.
Initial management begins with standard trauma assessment and stabilization, including airway, breathing, and circulation. Injured ears should be covered with sterile dressings. If the auricle is amputated, it should be wrapped in moist gauze, placed in a plastic bag, and kept cool for possible reattachment. Adequate anesthesia is essential and may be achieved through auricular nerve blocks or a circumferential ring block at the base of the pinna.
Auricular hematomas require prompt drainage, ideally within 72 hours, to reapproximate the perichondrium and cartilage and prevent necrosis. Small, nonclotted hematomas may be aspirated, while larger or clotted collections are best managed with incision and drainage followed by a firm pressure dressing. Antistaphylococcal antibiotics are typically given for 7–10 days. Reaccumulation requires repeat drainage and possibly wick placement.
Lacerations should be thoroughly cleaned and debrided. Simple lacerations can be closed with nonabsorbable monofilament sutures and a pressure dressing, while exposed cartilage must be carefully covered to prevent perichondritis. Human or animal bite wounds warrant prophylactic antibiotics, most commonly amoxicillin–clavulanate. Small avulsions less than 2 cm may survive as grafts, but larger avulsions require urgent consultation with otolaryngology or plastic surgery.
Patients may be discharged if they can tolerate oral antibiotics, have no serious associated injuries, and can ensure close follow-up. Admission is indicated for patients with significant associated trauma, immunosuppression with infection, perichondritis, chondritis, or need for intravenous antibiotics. Follow-up is recommended within 24 hours for auricular hematomas to assess for reaccumulation and within five days for suture evaluation or removal.
A key clinical principle is that failure to promptly recognize and adequately treat auricular hematomas can result in permanent deformity. Early drainage, proper pressure dressing, and close follow-up are essential to prevent long-term complications.


- Published on
Emergency and Acute Medicine – Lymphogranuloma Venereum
Basics description
Lymphogranuloma venereum (LGV) is a sexually transmitted infection characterized by an initial painless genital lesion followed by regional lymphatic spread. The disease progresses through primary, secondary, and tertiary stages and is responsive to appropriate antibacterial therapy in early phases. LGV is endemic in Southeast Asia, Latin America, parts of Africa, and the Caribbean, with increasing incidence among men who have sex with men. It is also known as struma, tropical bubo, or Nicolas–Favre–Durand disease.
Etiology
LGV is caused by Chlamydia trachomatis serotypes L1, L2, and L3.
Diagnosis signs and symptoms
The primary stage occurs after an incubation period of 3–30 days and presents as a painless papule, pustule, vesicle, or ulcer in the anogenital region. These lesions are transient, often last only a few days, and are frequently unnoticed. The secondary stage develops 1–3 weeks later with systemic symptoms such as fever, malaise, and myalgias, along with tender inguinal lymphadenopathy that may be unilateral or bilateral. Large, fluctuant lymph nodes (buboes) can ulcerate and drain purulent material. Proctitis is common in anal-receptive patients and may cause rectal bleeding, tenesmus, and constipation. The tertiary stage occurs in untreated disease and results in chronic inflammatory changes including proctocolitis, strictures, fistulae, and elephantiasis of the genitalia or lower extremities, mimicking inflammatory bowel disease.
Physical examination
Findings in the primary stage include a painless anogenital lesion. During the secondary stage, tender inguinal or femoral lymphadenopathy is typical, with buboes forming in up to two-thirds of cases. The “groove sign,” caused by lymph node enlargement above and below the inguinal ligament, may be seen. Anal-receptive patients may demonstrate signs of hemorrhagic proctocolitis. Advanced tertiary disease shows chronic inflammatory damage with strictures, fistulae, and elephantiasis.
Diagnosis tests and interpretation
Routine chlamydia nucleic acid amplification tests do not differentiate LGV strains. Diagnosis is based on clinical suspicion, epidemiologic context, and serologic testing. Complement fixation titers greater than 1:64 support the diagnosis. False-positive VDRL tests may occur. Bubo aspiration is specific but rarely practical and is not routinely required.
Differential diagnosis
Conditions to consider include genital herpes, syphilis, chancroid, and granuloma inguinale. Compared with LGV, syphilis typically causes nontender lymphadenopathy with a longer incubation period, while chancroid presents with painful ulcers and granuloma inguinale causes painless, friable lesions that bleed easily.
Treatment
No prehospital or emergency stabilization is typically required. Large, fluctuant buboes may require aspiration or drainage to reduce pain and scarring. First-line therapy is doxycycline 100 mg orally twice daily for 21 days. Alternative regimens include azithromycin 1 g orally weekly for 3 weeks or erythromycin 500 mg orally four times daily for 3 weeks. In pregnancy or during lactation, erythromycin is the recommended treatment.
Disposition and follow-up
Hospitalization is rarely necessary and is reserved for patients with severe systemic illness or complications. Most immunocompetent patients without systemic involvement can be discharged with outpatient management. Sexual partners within the previous 60 days should be tested and treated with appropriate antichlamydial therapy. Follow-up is essential to confirm cure, particularly in cases of rectal involvement, which may require retreatment.
Pearls and pitfalls
LGV should be suspected in at-risk populations, particularly men who have sex with men presenting with inguinal lymphadenopathy or proctitis. Early recognition and treatment are critical to prevent progression to tertiary disease, which may cause irreversible tissue damage and is less responsive to antibiotics alone.
Basics description
Lymphogranuloma venereum (LGV) is a sexually transmitted infection characterized by an initial painless genital lesion followed by regional lymphatic spread. The disease progresses through primary, secondary, and tertiary stages and is responsive to appropriate antibacterial therapy in early phases. LGV is endemic in Southeast Asia, Latin America, parts of Africa, and the Caribbean, with increasing incidence among men who have sex with men. It is also known as struma, tropical bubo, or Nicolas–Favre–Durand disease.
Etiology
LGV is caused by Chlamydia trachomatis serotypes L1, L2, and L3.
Diagnosis signs and symptoms
The primary stage occurs after an incubation period of 3–30 days and presents as a painless papule, pustule, vesicle, or ulcer in the anogenital region. These lesions are transient, often last only a few days, and are frequently unnoticed. The secondary stage develops 1–3 weeks later with systemic symptoms such as fever, malaise, and myalgias, along with tender inguinal lymphadenopathy that may be unilateral or bilateral. Large, fluctuant lymph nodes (buboes) can ulcerate and drain purulent material. Proctitis is common in anal-receptive patients and may cause rectal bleeding, tenesmus, and constipation. The tertiary stage occurs in untreated disease and results in chronic inflammatory changes including proctocolitis, strictures, fistulae, and elephantiasis of the genitalia or lower extremities, mimicking inflammatory bowel disease.
Physical examination
Findings in the primary stage include a painless anogenital lesion. During the secondary stage, tender inguinal or femoral lymphadenopathy is typical, with buboes forming in up to two-thirds of cases. The “groove sign,” caused by lymph node enlargement above and below the inguinal ligament, may be seen. Anal-receptive patients may demonstrate signs of hemorrhagic proctocolitis. Advanced tertiary disease shows chronic inflammatory damage with strictures, fistulae, and elephantiasis.
Diagnosis tests and interpretation
Routine chlamydia nucleic acid amplification tests do not differentiate LGV strains. Diagnosis is based on clinical suspicion, epidemiologic context, and serologic testing. Complement fixation titers greater than 1:64 support the diagnosis. False-positive VDRL tests may occur. Bubo aspiration is specific but rarely practical and is not routinely required.
Differential diagnosis
Conditions to consider include genital herpes, syphilis, chancroid, and granuloma inguinale. Compared with LGV, syphilis typically causes nontender lymphadenopathy with a longer incubation period, while chancroid presents with painful ulcers and granuloma inguinale causes painless, friable lesions that bleed easily.
Treatment
No prehospital or emergency stabilization is typically required. Large, fluctuant buboes may require aspiration or drainage to reduce pain and scarring. First-line therapy is doxycycline 100 mg orally twice daily for 21 days. Alternative regimens include azithromycin 1 g orally weekly for 3 weeks or erythromycin 500 mg orally four times daily for 3 weeks. In pregnancy or during lactation, erythromycin is the recommended treatment.
Disposition and follow-up
Hospitalization is rarely necessary and is reserved for patients with severe systemic illness or complications. Most immunocompetent patients without systemic involvement can be discharged with outpatient management. Sexual partners within the previous 60 days should be tested and treated with appropriate antichlamydial therapy. Follow-up is essential to confirm cure, particularly in cases of rectal involvement, which may require retreatment.
Pearls and pitfalls
LGV should be suspected in at-risk populations, particularly men who have sex with men presenting with inguinal lymphadenopathy or proctitis. Early recognition and treatment are critical to prevent progression to tertiary disease, which may cause irreversible tissue damage and is less responsive to antibiotics alone.
- Published on
Emergency and Acute Medicine – Lymphadenitis
Basics description
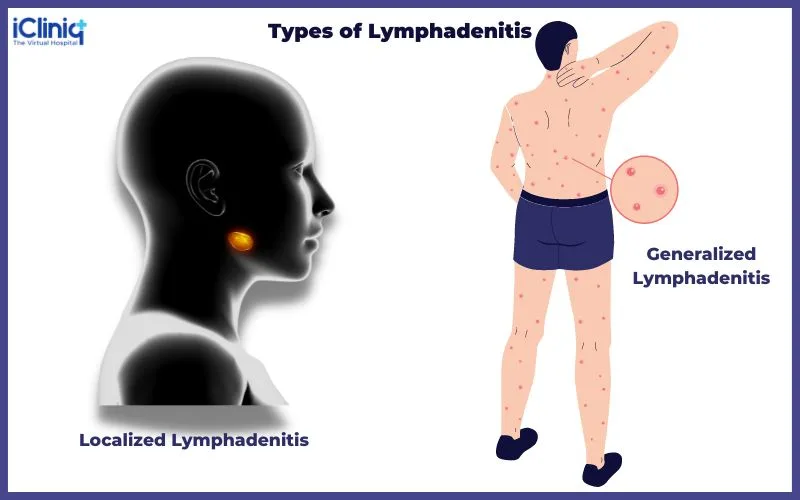
Lymphadenitis refers to inflammation and enlargement of lymph nodes, most commonly as part of a systemic response to infection. Nodes become engorged with lymphocytes and macrophages and may be secondarily involved from infection in a distal extremity, producing painful, tender adenopathy proximally. Acute suppurative lymphadenitis may follow pharyngeal or skin infections and can progress to abscess formation.
Etiology
Lymphadenitis is most frequently caused by bacterial infection. The most common organisms in pyogenic lymphadenitis are Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA), and group A β-hemolytic Streptococcus. CA-MRSA risk factors include prior MRSA infection, household exposure, military service, incarceration, contact sports, injection drug use, and men who have sex with men. Cervical lymphadenitis usually originates from pharyngeal or periodontal infections and commonly involves streptococci and anaerobes. Axillary lymphadenitis is often caused by group A streptococcus. Nosocomial MRSA should be suspected in patients with recent hospitalization, surgery, dialysis, vascular catheters, recent antibiotic use, or unresponsive infection. In children, acute unilateral cervical suppurative lymphadenitis is most common in those younger than six years and is typically caused by S. aureus, group A streptococcus, or anaerobes.
Diagnosis signs and symptoms
Patients typically present with painful swelling and inflammation of affected lymph nodes, often in association with cellulitis or abscess if the cause is pyogenic. Axillary lymphadenitis may present with fever, axillary pain, and acute lymphedema of the arm or chest and may be associated with ipsilateral pleural effusion. History should include duration of lymphadenopathy, pain, fever, night sweats, weight loss, fatigue, sore throat, cough, occupational and animal exposures, sexual history, drug use, and travel. Physical examination should assess whether lymphadenopathy is localized or generalized, node size, tenderness, overlying skin changes, presence of skin lesions, splenomegaly, and involvement of supraclavicular or scalene nodes, which is always abnormal.
Essential workup
Acute regional lymphadenitis is usually a clinical diagnosis and often part of a broader infectious syndrome such as cellulitis. History and physical examination should focus on identifying an infectious source.
Diagnosis tests and interpretation
Laboratory testing is not always required. A CBC may show leukocytosis with left shift or be normal. Serologic testing for EBV, CMV, HIV, or other pathogens should be guided by clinical suspicion. Ultrasound or CT imaging is indicated when patients fail to improve with therapy or when suppuration is suspected. Percutaneous needle aspiration or surgical drainage should be considered if abscess formation occurs or if there is poor clinical response.
Differential diagnosis
The differential diagnosis includes common infections such as adenovirus, scarlet fever, cat scratch disease, fungal infections, and herpes zoster, as well as unusual infections including sporotrichosis, diphtheria, plague, anthrax, typhoid, rubella, and West Nile virus. Sexually transmitted infections, systemic infections such as HIV, infectious mononucleosis, toxoplasmosis, tuberculosis, hepatitis, and dengue should be considered. Noninfectious causes include drug reactions, malignancy, rheumatologic disorders, and pediatric-specific conditions such as Kawasaki disease and PFAPA syndrome.
Treatment
Initial management includes ensuring airway, breathing, and circulation stability. Treatment is directed at the underlying cause and should account for local resistance patterns, including CA-MRSA prevalence. Outpatient therapy typically lasts 7–10 days and includes limb elevation, moist heat, analgesics, and antibiotics. Abscesses require drainage with culture when possible. Skin-source infections are commonly treated with oral cephalexin plus trimethoprim–sulfamethoxazole or alternatives such as clindamycin or doxycycline. Pharyngeal or periodontal sources are treated with penicillin VK or alternatives such as clindamycin or amoxicillin–clavulanate. Inpatient therapy may require IV penicillin-based regimens with MRSA coverage using vancomycin or clindamycin when indicated.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression or significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild infection who are nontoxic, can take oral antibiotics, and have reliable follow-up within 24–48 hours may be discharged. Failure to resolve promptly with antibiotics should prompt evaluation for malignancy or other serious causes, and lymph node biopsy may be indicated for persistent, large, or supraclavicular nodes.
Pearls and pitfalls
Staphylococcus species are the most common cause of acute regional pyogenic lymphadenitis. Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococci, particularly in unresponsive or high-risk infections.
Basics description
Lymphadenitis refers to inflammation and enlargement of lymph nodes, most commonly as part of a systemic response to infection. Nodes become engorged with lymphocytes and macrophages and may be secondarily involved from infection in a distal extremity, producing painful, tender adenopathy proximally. Acute suppurative lymphadenitis may follow pharyngeal or skin infections and can progress to abscess formation.
Etiology
Lymphadenitis is most frequently caused by bacterial infection. The most common organisms in pyogenic lymphadenitis are Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA), and group A β-hemolytic Streptococcus. CA-MRSA risk factors include prior MRSA infection, household exposure, military service, incarceration, contact sports, injection drug use, and men who have sex with men. Cervical lymphadenitis usually originates from pharyngeal or periodontal infections and commonly involves streptococci and anaerobes. Axillary lymphadenitis is often caused by group A streptococcus. Nosocomial MRSA should be suspected in patients with recent hospitalization, surgery, dialysis, vascular catheters, recent antibiotic use, or unresponsive infection. In children, acute unilateral cervical suppurative lymphadenitis is most common in those younger than six years and is typically caused by S. aureus, group A streptococcus, or anaerobes.
Diagnosis signs and symptoms
Patients typically present with painful swelling and inflammation of affected lymph nodes, often in association with cellulitis or abscess if the cause is pyogenic. Axillary lymphadenitis may present with fever, axillary pain, and acute lymphedema of the arm or chest and may be associated with ipsilateral pleural effusion. History should include duration of lymphadenopathy, pain, fever, night sweats, weight loss, fatigue, sore throat, cough, occupational and animal exposures, sexual history, drug use, and travel. Physical examination should assess whether lymphadenopathy is localized or generalized, node size, tenderness, overlying skin changes, presence of skin lesions, splenomegaly, and involvement of supraclavicular or scalene nodes, which is always abnormal.
Essential workup
Acute regional lymphadenitis is usually a clinical diagnosis and often part of a broader infectious syndrome such as cellulitis. History and physical examination should focus on identifying an infectious source.
Diagnosis tests and interpretation
Laboratory testing is not always required. A CBC may show leukocytosis with left shift or be normal. Serologic testing for EBV, CMV, HIV, or other pathogens should be guided by clinical suspicion. Ultrasound or CT imaging is indicated when patients fail to improve with therapy or when suppuration is suspected. Percutaneous needle aspiration or surgical drainage should be considered if abscess formation occurs or if there is poor clinical response.
Differential diagnosis
The differential diagnosis includes common infections such as adenovirus, scarlet fever, cat scratch disease, fungal infections, and herpes zoster, as well as unusual infections including sporotrichosis, diphtheria, plague, anthrax, typhoid, rubella, and West Nile virus. Sexually transmitted infections, systemic infections such as HIV, infectious mononucleosis, toxoplasmosis, tuberculosis, hepatitis, and dengue should be considered. Noninfectious causes include drug reactions, malignancy, rheumatologic disorders, and pediatric-specific conditions such as Kawasaki disease and PFAPA syndrome.
Treatment
Initial management includes ensuring airway, breathing, and circulation stability. Treatment is directed at the underlying cause and should account for local resistance patterns, including CA-MRSA prevalence. Outpatient therapy typically lasts 7–10 days and includes limb elevation, moist heat, analgesics, and antibiotics. Abscesses require drainage with culture when possible. Skin-source infections are commonly treated with oral cephalexin plus trimethoprim–sulfamethoxazole or alternatives such as clindamycin or doxycycline. Pharyngeal or periodontal sources are treated with penicillin VK or alternatives such as clindamycin or amoxicillin–clavulanate. Inpatient therapy may require IV penicillin-based regimens with MRSA coverage using vancomycin or clindamycin when indicated.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression or significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild infection who are nontoxic, can take oral antibiotics, and have reliable follow-up within 24–48 hours may be discharged. Failure to resolve promptly with antibiotics should prompt evaluation for malignancy or other serious causes, and lymph node biopsy may be indicated for persistent, large, or supraclavicular nodes.
Pearls and pitfalls
Staphylococcus species are the most common cause of acute regional pyogenic lymphadenitis. Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococci, particularly in unresponsive or high-risk infections.
- Published on
Emergency and Acute Medicine – Lymphangitis
Basics description
Lymphangitis is an infection of the lymphatic vessels that drain an area of inflammation or infection. Histologically, lymphatic channels become dilated and filled with lymphocytes and histiocytes. Inflammation often extends into surrounding perilymphatic tissues and may progress to cellulitis or abscess formation if untreated.
Etiology
Acute lymphangitis is most commonly caused by bacterial infection, particularly group A β-hemolytic Streptococcus. Less common causes include other streptococcal species and Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA). CA-MRSA risk factors include prior MRSA infection, close household contact, military service, incarceration, contact sports, injection drug use, and men who have sex with men. CA-MRSA is now prevalent enough to warrant empiric coverage in many settings, especially in unresponsive or recurrent infections. Other causes include Pasteurella multocida from animal bites, Spirillum minus in rat-bite fever, and Wuchereria bancrofti in filariasis, particularly in immigrants from endemic regions. Chronic lymphangitis is usually due to fungal, mycobacterial, or parasitic infections, most commonly Sporothrix schenckii, acquired through gardening or farming injuries, and Mycobacterium marinum, associated with fish tanks and swimming pools.
Diagnosis signs and symptoms
Acute lymphangitis presents with warm, tender, erythematous streaks extending proximally from a primary site of infection toward regional lymph nodes. Associated findings include painful lymphadenopathy, peripheral edema of the involved extremity, and systemic symptoms such as fever, rigors, tachycardia, and headache. Chronic nodular lymphangitis typically presents with painless erythematous nodules, chancriform ulcers, or wart-like lesions at the inoculation site, with possible progression along lymphatic channels and minimal systemic symptoms.
Essential workup
Lymphangitis is primarily a clinical diagnosis based on history and physical examination, with attention directed toward identifying the source of infection.
Diagnosis tests and interpretation
Laboratory testing is often unnecessary, though leukocytosis may be present. Gram stain and culture of aspirate or biopsy from the most inflamed area are recommended in cases of treatment failure or when resistant organisms such as MRSA are suspected. Culture confirmation is essential when sporotrichosis or M. marinum infection is considered. Blood cultures may be positive in severe cases. Imaging is rarely required but plain radiographs may help identify abscesses, subcutaneous gas, or foreign bodies, and Doppler ultrasound may be useful to exclude deep venous thrombosis.
Differential diagnosis
The differential diagnosis includes superficial or deep thrombophlebitis, which typically lacks an initial infectious focus or regional lymphadenopathy, IV line infiltration, vaccine-related reactions, and phytophotodermatitis, which can cause linear inflammatory skin changes mimicking lymphangitis.
Treatment
Initial management focuses on stabilizing septic patients with airway support and resuscitation as needed. Antimicrobial therapy should be initiated promptly, with the first dose given in the emergency department. Treatment typically lasts 7–10 days and includes limb elevation, moist heat, and antibiotics guided by local resistance patterns. Empiric outpatient therapy often includes oral cephalexin plus trimethoprim–sulfamethoxazole to cover CA-MRSA, with alternatives such as clindamycin or doxycycline. Inpatient therapy may require IV nafcillin or equivalent agents. Animal bite–associated lymphangitis is treated with IV ampicillin–sulbactam. Chronic infections require organism-specific therapy, such as itraconazole or potassium iodide for sporotrichosis and combination antimycobacterial therapy for M. marinum.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression, significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild disease who are clinically stable and able to take oral antibiotics may be discharged with close follow-up within 24–48 hours. Marking the borders of erythema before discharge helps assess treatment response.
Pearls and pitfalls
Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococcal species. Failure to recognize resistant organisms or chronic infectious causes can lead to treatment failure and progression of disease.
Basics description
Lymphangitis is an infection of the lymphatic vessels that drain an area of inflammation or infection. Histologically, lymphatic channels become dilated and filled with lymphocytes and histiocytes. Inflammation often extends into surrounding perilymphatic tissues and may progress to cellulitis or abscess formation if untreated.
Etiology
Acute lymphangitis is most commonly caused by bacterial infection, particularly group A β-hemolytic Streptococcus. Less common causes include other streptococcal species and Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA). CA-MRSA risk factors include prior MRSA infection, close household contact, military service, incarceration, contact sports, injection drug use, and men who have sex with men. CA-MRSA is now prevalent enough to warrant empiric coverage in many settings, especially in unresponsive or recurrent infections. Other causes include Pasteurella multocida from animal bites, Spirillum minus in rat-bite fever, and Wuchereria bancrofti in filariasis, particularly in immigrants from endemic regions. Chronic lymphangitis is usually due to fungal, mycobacterial, or parasitic infections, most commonly Sporothrix schenckii, acquired through gardening or farming injuries, and Mycobacterium marinum, associated with fish tanks and swimming pools.
Diagnosis signs and symptoms
Acute lymphangitis presents with warm, tender, erythematous streaks extending proximally from a primary site of infection toward regional lymph nodes. Associated findings include painful lymphadenopathy, peripheral edema of the involved extremity, and systemic symptoms such as fever, rigors, tachycardia, and headache. Chronic nodular lymphangitis typically presents with painless erythematous nodules, chancriform ulcers, or wart-like lesions at the inoculation site, with possible progression along lymphatic channels and minimal systemic symptoms.
Essential workup
Lymphangitis is primarily a clinical diagnosis based on history and physical examination, with attention directed toward identifying the source of infection.
Diagnosis tests and interpretation
Laboratory testing is often unnecessary, though leukocytosis may be present. Gram stain and culture of aspirate or biopsy from the most inflamed area are recommended in cases of treatment failure or when resistant organisms such as MRSA are suspected. Culture confirmation is essential when sporotrichosis or M. marinum infection is considered. Blood cultures may be positive in severe cases. Imaging is rarely required but plain radiographs may help identify abscesses, subcutaneous gas, or foreign bodies, and Doppler ultrasound may be useful to exclude deep venous thrombosis.
Differential diagnosis
The differential diagnosis includes superficial or deep thrombophlebitis, which typically lacks an initial infectious focus or regional lymphadenopathy, IV line infiltration, vaccine-related reactions, and phytophotodermatitis, which can cause linear inflammatory skin changes mimicking lymphangitis.
Treatment
Initial management focuses on stabilizing septic patients with airway support and resuscitation as needed. Antimicrobial therapy should be initiated promptly, with the first dose given in the emergency department. Treatment typically lasts 7–10 days and includes limb elevation, moist heat, and antibiotics guided by local resistance patterns. Empiric outpatient therapy often includes oral cephalexin plus trimethoprim–sulfamethoxazole to cover CA-MRSA, with alternatives such as clindamycin or doxycycline. Inpatient therapy may require IV nafcillin or equivalent agents. Animal bite–associated lymphangitis is treated with IV ampicillin–sulbactam. Chronic infections require organism-specific therapy, such as itraconazole or potassium iodide for sporotrichosis and combination antimycobacterial therapy for M. marinum.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression, significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild disease who are clinically stable and able to take oral antibiotics may be discharged with close follow-up within 24–48 hours. Marking the borders of erythema before discharge helps assess treatment response.
Pearls and pitfalls
Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococcal species. Failure to recognize resistant organisms or chronic infectious causes can lead to treatment failure and progression of disease.

