- Published on
Emergency And Acute Medicine – Lunate Dislocation
Basics description
Lunate dislocation is a disruption of the lunate relative to the distal radius and the remaining carpal bones. Most dislocations are volar, though dorsal displacement can occur. The injury typically results from high-energy wrist hyperextension combined with ulnar deviation and represents a severe carpal instability pattern.
Etiology
Lunate dislocation implies complete disruption of all four perilunate ligaments as well as the radiocarpal ligament, corresponding to stage IV of the Mayfield classification. Volar dislocations are commonly associated with median nerve compression within the carpal tunnel. Concomitant fractures of the radial styloid, scaphoid, capitate, or triquetrum are frequent and should heighten suspicion for occult perilunate ligamentous injury.
Diagnosis signs and symptoms
This injury is frequently missed. Patients usually report wrist pain following a fall or motor vehicle collision. Examination may reveal swelling or a palpable mass on the volar or dorsal wrist depending on the direction of dislocation. Gross deformity can be obscured by edema. Symptoms or signs of median nerve dysfunction, including numbness or paresthesia in the radial digits, may be present.
Essential workup
Clinical examination alone is often insufficient for diagnosis. Skin integrity and full neurovascular status should be assessed, including two-point discrimination. Radiographic evaluation is essential.
Diagnosis tests and interpretation
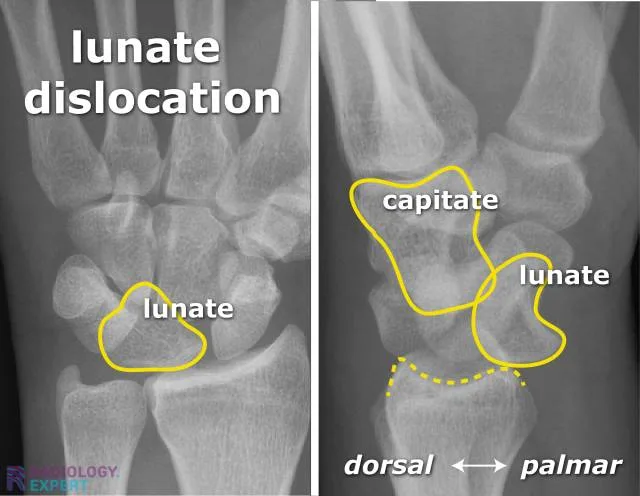
Standard wrist radiographs should include posteroanterior, lateral, and oblique views. The lateral view is most diagnostic, demonstrating disruption of the normal colinear alignment of the radius, lunate, and capitate. In volar dislocations, the lunate is tilted with its concavity facing the palm, producing the classic “spilled teacup” sign. On the posteroanterior view, the lunate often appears triangular rather than quadrangular, and disruption of Gilula’s arcs suggests carpal instability. Pediatric interpretation may be difficult due to incomplete ossification, while older adults commonly have associated fractures.
Differential diagnosis
Consider lunate fracture, perilunate dislocation, scapholunate dissociation, and scaphoid fracture.
Treatment pre hospital
Open wounds should be dressed and the wrist immobilized in a neutral position.
Initial stabilization therapy
Immobilize the wrist in a position of comfort using a volar splint or sugar-tong splint and provide adequate analgesia.
Ed treatment procedures
Evaluate for associated traumatic injuries. Early consultation with a hand or orthopedic surgeon is essential, as closed reduction is often unstable or unsuccessful. Definitive management frequently requires open reduction and internal fixation.
Medication
Pain control may be achieved with opioids or NSAIDs depending on severity. Morphine or combination acetaminophen–opioid preparations may be used for severe pain, while NSAIDs such as ibuprofen or naproxen are appropriate for moderate pain when not contraindicated. Caution is required with codeine in children due to variable metabolism.
Follow up disposition
Admission is commonly required for definitive surgical management, particularly in open injuries or polytrauma. Patients with closed dislocations that are successfully reduced and immobilized may be discharged with close orthopedic follow-up.
Follow up recommendations
Prompt outpatient follow-up with orthopedics or hand surgery is mandatory. Return to sports or heavy activity should be avoided until complete healing is confirmed.
Key points
Lunate dislocation is a commonly missed but serious wrist injury. Always assess for median nerve compromise. Early recognition and surgical consultation are critical to prevent complications such as avascular necrosis of the lunate and degenerative arthritis.
Basics description
Lunate dislocation is a disruption of the lunate relative to the distal radius and the remaining carpal bones. Most dislocations are volar, though dorsal displacement can occur. The injury typically results from high-energy wrist hyperextension combined with ulnar deviation and represents a severe carpal instability pattern.
Etiology
Lunate dislocation implies complete disruption of all four perilunate ligaments as well as the radiocarpal ligament, corresponding to stage IV of the Mayfield classification. Volar dislocations are commonly associated with median nerve compression within the carpal tunnel. Concomitant fractures of the radial styloid, scaphoid, capitate, or triquetrum are frequent and should heighten suspicion for occult perilunate ligamentous injury.
Diagnosis signs and symptoms
This injury is frequently missed. Patients usually report wrist pain following a fall or motor vehicle collision. Examination may reveal swelling or a palpable mass on the volar or dorsal wrist depending on the direction of dislocation. Gross deformity can be obscured by edema. Symptoms or signs of median nerve dysfunction, including numbness or paresthesia in the radial digits, may be present.
Essential workup
Clinical examination alone is often insufficient for diagnosis. Skin integrity and full neurovascular status should be assessed, including two-point discrimination. Radiographic evaluation is essential.
Diagnosis tests and interpretation
Standard wrist radiographs should include posteroanterior, lateral, and oblique views. The lateral view is most diagnostic, demonstrating disruption of the normal colinear alignment of the radius, lunate, and capitate. In volar dislocations, the lunate is tilted with its concavity facing the palm, producing the classic “spilled teacup” sign. On the posteroanterior view, the lunate often appears triangular rather than quadrangular, and disruption of Gilula’s arcs suggests carpal instability. Pediatric interpretation may be difficult due to incomplete ossification, while older adults commonly have associated fractures.
Differential diagnosis
Consider lunate fracture, perilunate dislocation, scapholunate dissociation, and scaphoid fracture.
Treatment pre hospital
Open wounds should be dressed and the wrist immobilized in a neutral position.
Initial stabilization therapy
Immobilize the wrist in a position of comfort using a volar splint or sugar-tong splint and provide adequate analgesia.
Ed treatment procedures
Evaluate for associated traumatic injuries. Early consultation with a hand or orthopedic surgeon is essential, as closed reduction is often unstable or unsuccessful. Definitive management frequently requires open reduction and internal fixation.
Medication
Pain control may be achieved with opioids or NSAIDs depending on severity. Morphine or combination acetaminophen–opioid preparations may be used for severe pain, while NSAIDs such as ibuprofen or naproxen are appropriate for moderate pain when not contraindicated. Caution is required with codeine in children due to variable metabolism.
Follow up disposition
Admission is commonly required for definitive surgical management, particularly in open injuries or polytrauma. Patients with closed dislocations that are successfully reduced and immobilized may be discharged with close orthopedic follow-up.
Follow up recommendations
Prompt outpatient follow-up with orthopedics or hand surgery is mandatory. Return to sports or heavy activity should be avoided until complete healing is confirmed.
Key points
Lunate dislocation is a commonly missed but serious wrist injury. Always assess for median nerve compromise. Early recognition and surgical consultation are critical to prevent complications such as avascular necrosis of the lunate and degenerative arthritis.
- Published on
Emergency and Acute Medicine – Lymphadenitis
Basics description
Lymphadenitis refers to inflammation and enlargement of lymph nodes, most commonly as part of a systemic response to infection. Nodes become engorged with lymphocytes and macrophages and may be secondarily involved from infection in a distal extremity, producing painful, tender adenopathy proximally. Acute suppurative lymphadenitis may follow pharyngeal or skin infections and can progress to abscess formation.
Etiology
Lymphadenitis is most frequently caused by bacterial infection. The most common organisms in pyogenic lymphadenitis are Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA), and group A β-hemolytic Streptococcus. CA-MRSA risk factors include prior MRSA infection, household exposure, military service, incarceration, contact sports, injection drug use, and men who have sex with men. Cervical lymphadenitis usually originates from pharyngeal or periodontal infections and commonly involves streptococci and anaerobes. Axillary lymphadenitis is often caused by group A streptococcus. Nosocomial MRSA should be suspected in patients with recent hospitalization, surgery, dialysis, vascular catheters, recent antibiotic use, or unresponsive infection. In children, acute unilateral cervical suppurative lymphadenitis is most common in those younger than six years and is typically caused by S. aureus, group A streptococcus, or anaerobes.
Diagnosis signs and symptoms
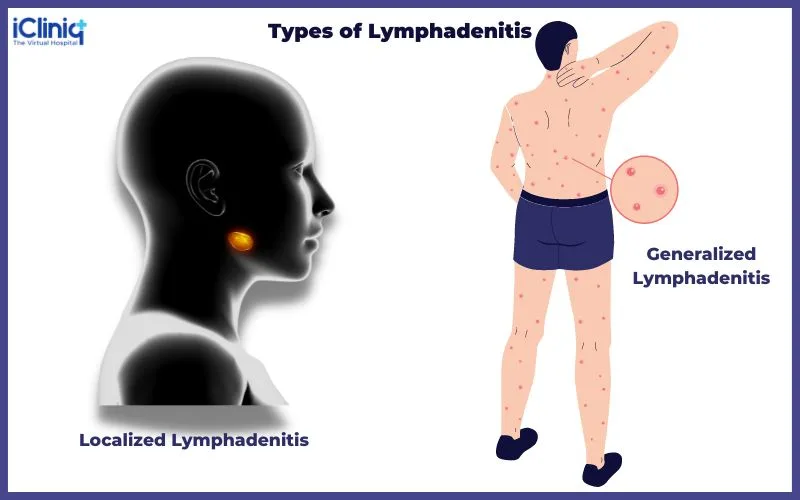
Patients typically present with painful swelling and inflammation of affected lymph nodes, often in association with cellulitis or abscess if the cause is pyogenic. Axillary lymphadenitis may present with fever, axillary pain, and acute lymphedema of the arm or chest and may be associated with ipsilateral pleural effusion. History should include duration of lymphadenopathy, pain, fever, night sweats, weight loss, fatigue, sore throat, cough, occupational and animal exposures, sexual history, drug use, and travel. Physical examination should assess whether lymphadenopathy is localized or generalized, node size, tenderness, overlying skin changes, presence of skin lesions, splenomegaly, and involvement of supraclavicular or scalene nodes, which is always abnormal.
Essential workup
Acute regional lymphadenitis is usually a clinical diagnosis and often part of a broader infectious syndrome such as cellulitis. History and physical examination should focus on identifying an infectious source.
Diagnosis tests and interpretation
Laboratory testing is not always required. A CBC may show leukocytosis with left shift or be normal. Serologic testing for EBV, CMV, HIV, or other pathogens should be guided by clinical suspicion. Ultrasound or CT imaging is indicated when patients fail to improve with therapy or when suppuration is suspected. Percutaneous needle aspiration or surgical drainage should be considered if abscess formation occurs or if there is poor clinical response.
Differential diagnosis
The differential diagnosis includes common infections such as adenovirus, scarlet fever, cat scratch disease, fungal infections, and herpes zoster, as well as unusual infections including sporotrichosis, diphtheria, plague, anthrax, typhoid, rubella, and West Nile virus. Sexually transmitted infections, systemic infections such as HIV, infectious mononucleosis, toxoplasmosis, tuberculosis, hepatitis, and dengue should be considered. Noninfectious causes include drug reactions, malignancy, rheumatologic disorders, and pediatric-specific conditions such as Kawasaki disease and PFAPA syndrome.
Treatment
Initial management includes ensuring airway, breathing, and circulation stability. Treatment is directed at the underlying cause and should account for local resistance patterns, including CA-MRSA prevalence. Outpatient therapy typically lasts 7–10 days and includes limb elevation, moist heat, analgesics, and antibiotics. Abscesses require drainage with culture when possible. Skin-source infections are commonly treated with oral cephalexin plus trimethoprim–sulfamethoxazole or alternatives such as clindamycin or doxycycline. Pharyngeal or periodontal sources are treated with penicillin VK or alternatives such as clindamycin or amoxicillin–clavulanate. Inpatient therapy may require IV penicillin-based regimens with MRSA coverage using vancomycin or clindamycin when indicated.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression or significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild infection who are nontoxic, can take oral antibiotics, and have reliable follow-up within 24–48 hours may be discharged. Failure to resolve promptly with antibiotics should prompt evaluation for malignancy or other serious causes, and lymph node biopsy may be indicated for persistent, large, or supraclavicular nodes.
Pearls and pitfalls
Staphylococcus species are the most common cause of acute regional pyogenic lymphadenitis. Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococci, particularly in unresponsive or high-risk infections.
Basics description
Lymphadenitis refers to inflammation and enlargement of lymph nodes, most commonly as part of a systemic response to infection. Nodes become engorged with lymphocytes and macrophages and may be secondarily involved from infection in a distal extremity, producing painful, tender adenopathy proximally. Acute suppurative lymphadenitis may follow pharyngeal or skin infections and can progress to abscess formation.
Etiology
Lymphadenitis is most frequently caused by bacterial infection. The most common organisms in pyogenic lymphadenitis are Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA), and group A β-hemolytic Streptococcus. CA-MRSA risk factors include prior MRSA infection, household exposure, military service, incarceration, contact sports, injection drug use, and men who have sex with men. Cervical lymphadenitis usually originates from pharyngeal or periodontal infections and commonly involves streptococci and anaerobes. Axillary lymphadenitis is often caused by group A streptococcus. Nosocomial MRSA should be suspected in patients with recent hospitalization, surgery, dialysis, vascular catheters, recent antibiotic use, or unresponsive infection. In children, acute unilateral cervical suppurative lymphadenitis is most common in those younger than six years and is typically caused by S. aureus, group A streptococcus, or anaerobes.
Diagnosis signs and symptoms
Patients typically present with painful swelling and inflammation of affected lymph nodes, often in association with cellulitis or abscess if the cause is pyogenic. Axillary lymphadenitis may present with fever, axillary pain, and acute lymphedema of the arm or chest and may be associated with ipsilateral pleural effusion. History should include duration of lymphadenopathy, pain, fever, night sweats, weight loss, fatigue, sore throat, cough, occupational and animal exposures, sexual history, drug use, and travel. Physical examination should assess whether lymphadenopathy is localized or generalized, node size, tenderness, overlying skin changes, presence of skin lesions, splenomegaly, and involvement of supraclavicular or scalene nodes, which is always abnormal.
Essential workup
Acute regional lymphadenitis is usually a clinical diagnosis and often part of a broader infectious syndrome such as cellulitis. History and physical examination should focus on identifying an infectious source.
Diagnosis tests and interpretation
Laboratory testing is not always required. A CBC may show leukocytosis with left shift or be normal. Serologic testing for EBV, CMV, HIV, or other pathogens should be guided by clinical suspicion. Ultrasound or CT imaging is indicated when patients fail to improve with therapy or when suppuration is suspected. Percutaneous needle aspiration or surgical drainage should be considered if abscess formation occurs or if there is poor clinical response.
Differential diagnosis
The differential diagnosis includes common infections such as adenovirus, scarlet fever, cat scratch disease, fungal infections, and herpes zoster, as well as unusual infections including sporotrichosis, diphtheria, plague, anthrax, typhoid, rubella, and West Nile virus. Sexually transmitted infections, systemic infections such as HIV, infectious mononucleosis, toxoplasmosis, tuberculosis, hepatitis, and dengue should be considered. Noninfectious causes include drug reactions, malignancy, rheumatologic disorders, and pediatric-specific conditions such as Kawasaki disease and PFAPA syndrome.
Treatment
Initial management includes ensuring airway, breathing, and circulation stability. Treatment is directed at the underlying cause and should account for local resistance patterns, including CA-MRSA prevalence. Outpatient therapy typically lasts 7–10 days and includes limb elevation, moist heat, analgesics, and antibiotics. Abscesses require drainage with culture when possible. Skin-source infections are commonly treated with oral cephalexin plus trimethoprim–sulfamethoxazole or alternatives such as clindamycin or doxycycline. Pharyngeal or periodontal sources are treated with penicillin VK or alternatives such as clindamycin or amoxicillin–clavulanate. Inpatient therapy may require IV penicillin-based regimens with MRSA coverage using vancomycin or clindamycin when indicated.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression or significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild infection who are nontoxic, can take oral antibiotics, and have reliable follow-up within 24–48 hours may be discharged. Failure to resolve promptly with antibiotics should prompt evaluation for malignancy or other serious causes, and lymph node biopsy may be indicated for persistent, large, or supraclavicular nodes.
Pearls and pitfalls
Staphylococcus species are the most common cause of acute regional pyogenic lymphadenitis. Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococci, particularly in unresponsive or high-risk infections.
- Published on
Emergency and Acute Medicine – Lymphangitis
Basics description
Lymphangitis is an infection of the lymphatic vessels that drain an area of inflammation or infection. Histologically, lymphatic channels become dilated and filled with lymphocytes and histiocytes. Inflammation often extends into surrounding perilymphatic tissues and may progress to cellulitis or abscess formation if untreated.
Etiology
Acute lymphangitis is most commonly caused by bacterial infection, particularly group A β-hemolytic Streptococcus. Less common causes include other streptococcal species and Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA). CA-MRSA risk factors include prior MRSA infection, close household contact, military service, incarceration, contact sports, injection drug use, and men who have sex with men. CA-MRSA is now prevalent enough to warrant empiric coverage in many settings, especially in unresponsive or recurrent infections. Other causes include Pasteurella multocida from animal bites, Spirillum minus in rat-bite fever, and Wuchereria bancrofti in filariasis, particularly in immigrants from endemic regions. Chronic lymphangitis is usually due to fungal, mycobacterial, or parasitic infections, most commonly Sporothrix schenckii, acquired through gardening or farming injuries, and Mycobacterium marinum, associated with fish tanks and swimming pools.
Diagnosis signs and symptoms
Acute lymphangitis presents with warm, tender, erythematous streaks extending proximally from a primary site of infection toward regional lymph nodes. Associated findings include painful lymphadenopathy, peripheral edema of the involved extremity, and systemic symptoms such as fever, rigors, tachycardia, and headache. Chronic nodular lymphangitis typically presents with painless erythematous nodules, chancriform ulcers, or wart-like lesions at the inoculation site, with possible progression along lymphatic channels and minimal systemic symptoms.
Essential workup
Lymphangitis is primarily a clinical diagnosis based on history and physical examination, with attention directed toward identifying the source of infection.
Diagnosis tests and interpretation
Laboratory testing is often unnecessary, though leukocytosis may be present. Gram stain and culture of aspirate or biopsy from the most inflamed area are recommended in cases of treatment failure or when resistant organisms such as MRSA are suspected. Culture confirmation is essential when sporotrichosis or M. marinum infection is considered. Blood cultures may be positive in severe cases. Imaging is rarely required but plain radiographs may help identify abscesses, subcutaneous gas, or foreign bodies, and Doppler ultrasound may be useful to exclude deep venous thrombosis.
Differential diagnosis
The differential diagnosis includes superficial or deep thrombophlebitis, which typically lacks an initial infectious focus or regional lymphadenopathy, IV line infiltration, vaccine-related reactions, and phytophotodermatitis, which can cause linear inflammatory skin changes mimicking lymphangitis.
Treatment
Initial management focuses on stabilizing septic patients with airway support and resuscitation as needed. Antimicrobial therapy should be initiated promptly, with the first dose given in the emergency department. Treatment typically lasts 7–10 days and includes limb elevation, moist heat, and antibiotics guided by local resistance patterns. Empiric outpatient therapy often includes oral cephalexin plus trimethoprim–sulfamethoxazole to cover CA-MRSA, with alternatives such as clindamycin or doxycycline. Inpatient therapy may require IV nafcillin or equivalent agents. Animal bite–associated lymphangitis is treated with IV ampicillin–sulbactam. Chronic infections require organism-specific therapy, such as itraconazole or potassium iodide for sporotrichosis and combination antimycobacterial therapy for M. marinum.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression, significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild disease who are clinically stable and able to take oral antibiotics may be discharged with close follow-up within 24–48 hours. Marking the borders of erythema before discharge helps assess treatment response.
Pearls and pitfalls
Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococcal species. Failure to recognize resistant organisms or chronic infectious causes can lead to treatment failure and progression of disease.
Basics description
Lymphangitis is an infection of the lymphatic vessels that drain an area of inflammation or infection. Histologically, lymphatic channels become dilated and filled with lymphocytes and histiocytes. Inflammation often extends into surrounding perilymphatic tissues and may progress to cellulitis or abscess formation if untreated.
Etiology
Acute lymphangitis is most commonly caused by bacterial infection, particularly group A β-hemolytic Streptococcus. Less common causes include other streptococcal species and Staphylococcus aureus, including community-associated methicillin-resistant S. aureus (CA-MRSA). CA-MRSA risk factors include prior MRSA infection, close household contact, military service, incarceration, contact sports, injection drug use, and men who have sex with men. CA-MRSA is now prevalent enough to warrant empiric coverage in many settings, especially in unresponsive or recurrent infections. Other causes include Pasteurella multocida from animal bites, Spirillum minus in rat-bite fever, and Wuchereria bancrofti in filariasis, particularly in immigrants from endemic regions. Chronic lymphangitis is usually due to fungal, mycobacterial, or parasitic infections, most commonly Sporothrix schenckii, acquired through gardening or farming injuries, and Mycobacterium marinum, associated with fish tanks and swimming pools.
Diagnosis signs and symptoms
Acute lymphangitis presents with warm, tender, erythematous streaks extending proximally from a primary site of infection toward regional lymph nodes. Associated findings include painful lymphadenopathy, peripheral edema of the involved extremity, and systemic symptoms such as fever, rigors, tachycardia, and headache. Chronic nodular lymphangitis typically presents with painless erythematous nodules, chancriform ulcers, or wart-like lesions at the inoculation site, with possible progression along lymphatic channels and minimal systemic symptoms.
Essential workup
Lymphangitis is primarily a clinical diagnosis based on history and physical examination, with attention directed toward identifying the source of infection.
Diagnosis tests and interpretation
Laboratory testing is often unnecessary, though leukocytosis may be present. Gram stain and culture of aspirate or biopsy from the most inflamed area are recommended in cases of treatment failure or when resistant organisms such as MRSA are suspected. Culture confirmation is essential when sporotrichosis or M. marinum infection is considered. Blood cultures may be positive in severe cases. Imaging is rarely required but plain radiographs may help identify abscesses, subcutaneous gas, or foreign bodies, and Doppler ultrasound may be useful to exclude deep venous thrombosis.
Differential diagnosis
The differential diagnosis includes superficial or deep thrombophlebitis, which typically lacks an initial infectious focus or regional lymphadenopathy, IV line infiltration, vaccine-related reactions, and phytophotodermatitis, which can cause linear inflammatory skin changes mimicking lymphangitis.
Treatment
Initial management focuses on stabilizing septic patients with airway support and resuscitation as needed. Antimicrobial therapy should be initiated promptly, with the first dose given in the emergency department. Treatment typically lasts 7–10 days and includes limb elevation, moist heat, and antibiotics guided by local resistance patterns. Empiric outpatient therapy often includes oral cephalexin plus trimethoprim–sulfamethoxazole to cover CA-MRSA, with alternatives such as clindamycin or doxycycline. Inpatient therapy may require IV nafcillin or equivalent agents. Animal bite–associated lymphangitis is treated with IV ampicillin–sulbactam. Chronic infections require organism-specific therapy, such as itraconazole or potassium iodide for sporotrichosis and combination antimycobacterial therapy for M. marinum.
Disposition and follow-up
Admission is indicated for toxic-appearing patients, those with immunosuppression, significant comorbidities, inability to tolerate oral therapy, or unreliable follow-up. Patients with mild disease who are clinically stable and able to take oral antibiotics may be discharged with close follow-up within 24–48 hours. Marking the borders of erythema before discharge helps assess treatment response.
Pearls and pitfalls
Empiric antibiotic therapy should include coverage for CA-MRSA in addition to streptococcal species. Failure to recognize resistant organisms or chronic infectious causes can lead to treatment failure and progression of disease.

- Published on
Emergency and Acute Medicine – Lymphogranuloma Venereum
Basics description
Lymphogranuloma venereum (LGV) is a sexually transmitted infection characterized by an initial painless genital lesion followed by regional lymphatic spread. The disease progresses through primary, secondary, and tertiary stages and is responsive to appropriate antibacterial therapy in early phases. LGV is endemic in Southeast Asia, Latin America, parts of Africa, and the Caribbean, with increasing incidence among men who have sex with men. It is also known as struma, tropical bubo, or Nicolas–Favre–Durand disease.
Etiology
LGV is caused by Chlamydia trachomatis serotypes L1, L2, and L3.
Diagnosis signs and symptoms
The primary stage occurs after an incubation period of 3–30 days and presents as a painless papule, pustule, vesicle, or ulcer in the anogenital region. These lesions are transient, often last only a few days, and are frequently unnoticed. The secondary stage develops 1–3 weeks later with systemic symptoms such as fever, malaise, and myalgias, along with tender inguinal lymphadenopathy that may be unilateral or bilateral. Large, fluctuant lymph nodes (buboes) can ulcerate and drain purulent material. Proctitis is common in anal-receptive patients and may cause rectal bleeding, tenesmus, and constipation. The tertiary stage occurs in untreated disease and results in chronic inflammatory changes including proctocolitis, strictures, fistulae, and elephantiasis of the genitalia or lower extremities, mimicking inflammatory bowel disease.
Physical examination
Findings in the primary stage include a painless anogenital lesion. During the secondary stage, tender inguinal or femoral lymphadenopathy is typical, with buboes forming in up to two-thirds of cases. The “groove sign,” caused by lymph node enlargement above and below the inguinal ligament, may be seen. Anal-receptive patients may demonstrate signs of hemorrhagic proctocolitis. Advanced tertiary disease shows chronic inflammatory damage with strictures, fistulae, and elephantiasis.
Diagnosis tests and interpretation
Routine chlamydia nucleic acid amplification tests do not differentiate LGV strains. Diagnosis is based on clinical suspicion, epidemiologic context, and serologic testing. Complement fixation titers greater than 1:64 support the diagnosis. False-positive VDRL tests may occur. Bubo aspiration is specific but rarely practical and is not routinely required.
Differential diagnosis
Conditions to consider include genital herpes, syphilis, chancroid, and granuloma inguinale. Compared with LGV, syphilis typically causes nontender lymphadenopathy with a longer incubation period, while chancroid presents with painful ulcers and granuloma inguinale causes painless, friable lesions that bleed easily.
Treatment
No prehospital or emergency stabilization is typically required. Large, fluctuant buboes may require aspiration or drainage to reduce pain and scarring. First-line therapy is doxycycline 100 mg orally twice daily for 21 days. Alternative regimens include azithromycin 1 g orally weekly for 3 weeks or erythromycin 500 mg orally four times daily for 3 weeks. In pregnancy or during lactation, erythromycin is the recommended treatment.
Disposition and follow-up
Hospitalization is rarely necessary and is reserved for patients with severe systemic illness or complications. Most immunocompetent patients without systemic involvement can be discharged with outpatient management. Sexual partners within the previous 60 days should be tested and treated with appropriate antichlamydial therapy. Follow-up is essential to confirm cure, particularly in cases of rectal involvement, which may require retreatment.
Pearls and pitfalls
LGV should be suspected in at-risk populations, particularly men who have sex with men presenting with inguinal lymphadenopathy or proctitis. Early recognition and treatment are critical to prevent progression to tertiary disease, which may cause irreversible tissue damage and is less responsive to antibiotics alone.
Basics description
Lymphogranuloma venereum (LGV) is a sexually transmitted infection characterized by an initial painless genital lesion followed by regional lymphatic spread. The disease progresses through primary, secondary, and tertiary stages and is responsive to appropriate antibacterial therapy in early phases. LGV is endemic in Southeast Asia, Latin America, parts of Africa, and the Caribbean, with increasing incidence among men who have sex with men. It is also known as struma, tropical bubo, or Nicolas–Favre–Durand disease.
Etiology
LGV is caused by Chlamydia trachomatis serotypes L1, L2, and L3.
Diagnosis signs and symptoms
The primary stage occurs after an incubation period of 3–30 days and presents as a painless papule, pustule, vesicle, or ulcer in the anogenital region. These lesions are transient, often last only a few days, and are frequently unnoticed. The secondary stage develops 1–3 weeks later with systemic symptoms such as fever, malaise, and myalgias, along with tender inguinal lymphadenopathy that may be unilateral or bilateral. Large, fluctuant lymph nodes (buboes) can ulcerate and drain purulent material. Proctitis is common in anal-receptive patients and may cause rectal bleeding, tenesmus, and constipation. The tertiary stage occurs in untreated disease and results in chronic inflammatory changes including proctocolitis, strictures, fistulae, and elephantiasis of the genitalia or lower extremities, mimicking inflammatory bowel disease.
Physical examination
Findings in the primary stage include a painless anogenital lesion. During the secondary stage, tender inguinal or femoral lymphadenopathy is typical, with buboes forming in up to two-thirds of cases. The “groove sign,” caused by lymph node enlargement above and below the inguinal ligament, may be seen. Anal-receptive patients may demonstrate signs of hemorrhagic proctocolitis. Advanced tertiary disease shows chronic inflammatory damage with strictures, fistulae, and elephantiasis.
Diagnosis tests and interpretation
Routine chlamydia nucleic acid amplification tests do not differentiate LGV strains. Diagnosis is based on clinical suspicion, epidemiologic context, and serologic testing. Complement fixation titers greater than 1:64 support the diagnosis. False-positive VDRL tests may occur. Bubo aspiration is specific but rarely practical and is not routinely required.
Differential diagnosis
Conditions to consider include genital herpes, syphilis, chancroid, and granuloma inguinale. Compared with LGV, syphilis typically causes nontender lymphadenopathy with a longer incubation period, while chancroid presents with painful ulcers and granuloma inguinale causes painless, friable lesions that bleed easily.
Treatment
No prehospital or emergency stabilization is typically required. Large, fluctuant buboes may require aspiration or drainage to reduce pain and scarring. First-line therapy is doxycycline 100 mg orally twice daily for 21 days. Alternative regimens include azithromycin 1 g orally weekly for 3 weeks or erythromycin 500 mg orally four times daily for 3 weeks. In pregnancy or during lactation, erythromycin is the recommended treatment.
Disposition and follow-up
Hospitalization is rarely necessary and is reserved for patients with severe systemic illness or complications. Most immunocompetent patients without systemic involvement can be discharged with outpatient management. Sexual partners within the previous 60 days should be tested and treated with appropriate antichlamydial therapy. Follow-up is essential to confirm cure, particularly in cases of rectal involvement, which may require retreatment.
Pearls and pitfalls
LGV should be suspected in at-risk populations, particularly men who have sex with men presenting with inguinal lymphadenopathy or proctitis. Early recognition and treatment are critical to prevent progression to tertiary disease, which may cause irreversible tissue damage and is less responsive to antibiotics alone.
- Published on
Emergency and Acute Medicine – Malaria
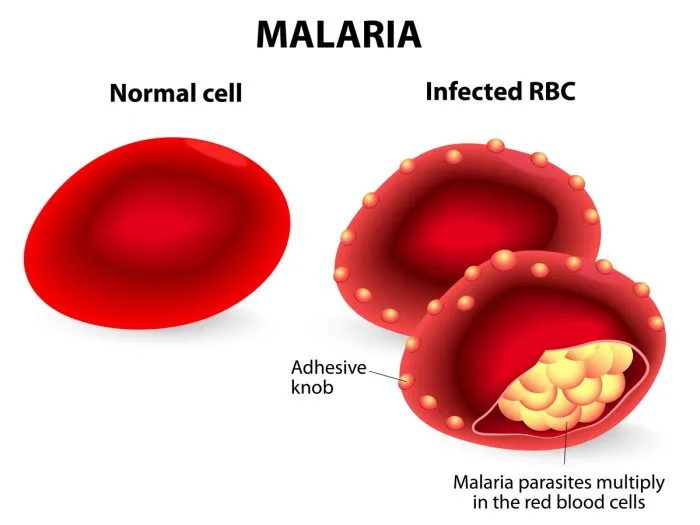
Basics description
Malaria is a protozoan infection transmitted through the bite of an infected female Anopheles mosquito. The incubation period is typically 8–16 days, although symptoms may be delayed for months depending on the species. The periodic nature of malaria symptoms reflects the parasite life cycle, which includes an exoerythrocytic phase in the liver followed by an erythrocytic phase in red blood cells. Fever corresponds to synchronous red blood cell lysis and release of merozoites into the circulation.
Pathophysiology and species differences
In the exoerythrocytic phase, sporozoites migrate to the liver and multiply into merozoites. These then enter the bloodstream and invade red blood cells, where replication leads to cell rupture every 48–72 hours. Plasmodium falciparum causes most severe disease and nearly all malaria-related deaths. It infects red blood cells of all ages, leading to profound hemolysis, anemia, and capillary obstruction with resultant end-organ hypoxia. Plasmodium vivax and Plasmodium ovale may cause relapsing disease due to dormant liver forms (hypnozoites), while Plasmodium malariae can persist at low levels in the bloodstream for decades.
Etiology and transmission
Transmission usually occurs via mosquito bite but may also result from blood transfusions or shared needles. Rare autochthonous transmission has been reported in North America due to the presence of Anopheles mosquitoes. Post-traumatic immunosuppression may precipitate relapse in individuals previously exposed in endemic regions. Children with sickle cell trait have partial protection, while pregnant patients—especially primigravidas—are at higher risk for severe disease.
Diagnosis signs and symptoms
Most patients become symptomatic within one year of exposure. Common symptoms include malaise, chills, fever greater than 38°C, myalgias, arthralgias, and orthostatic hypotension. The classic malaria paroxysm consists of chills followed by high fever and subsequent diaphoresis, although this pattern is uncommon in clinical practice. Hemolysis may lead to jaundice, dark urine (blackwater fever), anemia, and splenomegaly. Severe manifestations include cerebral malaria with headache, altered mental status, seizures, or coma; pulmonary edema; renal failure; abnormal bleeding; and circulatory collapse.
Essential workup and diagnostic testing
Diagnosis relies on oil immersion light microscopy of thick and thin Giemsa-stained blood smears, which demonstrate intraerythrocytic parasites. At least three negative smears over 48 hours are required to exclude malaria. Laboratory findings commonly include anemia, thrombocytopenia, leukocytopenia, elevated bilirubin and lactate dehydrogenase, electrolyte abnormalities, and evidence of renal or hepatic dysfunction. Chest radiography may reveal pulmonary edema. Advanced testing such as antigen detection assays or PCR can identify Plasmodium species and mixed infections. Lumbar puncture may be necessary to distinguish cerebral malaria from meningitis.
Differential diagnosis
The differential includes meningitis, encephalitis, sepsis, acute renal failure, viral hepatitis, acute hemolytic anemia, hypoglycemic coma, and heat stroke. In travelers or immigrants from endemic areas, malaria must be considered in any febrile illness.
Treatment and emergency management
Initial stabilization includes airway, breathing, and circulation management, isotonic fluid resuscitation for hypotension, active cooling for hyperthermia, and treatment of hypoglycemia or seizures as indicated. Antimalarial therapy depends on species, severity, and geographic resistance patterns, with artemisinin-based combination therapies recommended as first-line treatment worldwide. Severe P. falciparum infection requires intravenous artesunate. Supportive care for complications such as anemia, renal failure, and cerebral edema is critical.
Disposition and follow-up
ICU admission is indicated for severe P. falciparum malaria, high parasitemia, neurologic involvement, or inability to tolerate oral therapy. Patients with non–P. falciparum malaria who are clinically stable and able to take oral medications may be treated as outpatients with close follow-up.
Pearls and pitfalls
Malaria should always be considered in patients with fever and compatible exposure history, even months after travel. Fever patterns are unreliable, and early recognition is essential, as delays in treatment—especially with P. falciparum—are associated with high mortality.
Basics description
Malaria is a protozoan infection transmitted through the bite of an infected female Anopheles mosquito. The incubation period is typically 8–16 days, although symptoms may be delayed for months depending on the species. The periodic nature of malaria symptoms reflects the parasite life cycle, which includes an exoerythrocytic phase in the liver followed by an erythrocytic phase in red blood cells. Fever corresponds to synchronous red blood cell lysis and release of merozoites into the circulation.
Pathophysiology and species differences
In the exoerythrocytic phase, sporozoites migrate to the liver and multiply into merozoites. These then enter the bloodstream and invade red blood cells, where replication leads to cell rupture every 48–72 hours. Plasmodium falciparum causes most severe disease and nearly all malaria-related deaths. It infects red blood cells of all ages, leading to profound hemolysis, anemia, and capillary obstruction with resultant end-organ hypoxia. Plasmodium vivax and Plasmodium ovale may cause relapsing disease due to dormant liver forms (hypnozoites), while Plasmodium malariae can persist at low levels in the bloodstream for decades.
Etiology and transmission
Transmission usually occurs via mosquito bite but may also result from blood transfusions or shared needles. Rare autochthonous transmission has been reported in North America due to the presence of Anopheles mosquitoes. Post-traumatic immunosuppression may precipitate relapse in individuals previously exposed in endemic regions. Children with sickle cell trait have partial protection, while pregnant patients—especially primigravidas—are at higher risk for severe disease.
Diagnosis signs and symptoms
Most patients become symptomatic within one year of exposure. Common symptoms include malaise, chills, fever greater than 38°C, myalgias, arthralgias, and orthostatic hypotension. The classic malaria paroxysm consists of chills followed by high fever and subsequent diaphoresis, although this pattern is uncommon in clinical practice. Hemolysis may lead to jaundice, dark urine (blackwater fever), anemia, and splenomegaly. Severe manifestations include cerebral malaria with headache, altered mental status, seizures, or coma; pulmonary edema; renal failure; abnormal bleeding; and circulatory collapse.
Essential workup and diagnostic testing
Diagnosis relies on oil immersion light microscopy of thick and thin Giemsa-stained blood smears, which demonstrate intraerythrocytic parasites. At least three negative smears over 48 hours are required to exclude malaria. Laboratory findings commonly include anemia, thrombocytopenia, leukocytopenia, elevated bilirubin and lactate dehydrogenase, electrolyte abnormalities, and evidence of renal or hepatic dysfunction. Chest radiography may reveal pulmonary edema. Advanced testing such as antigen detection assays or PCR can identify Plasmodium species and mixed infections. Lumbar puncture may be necessary to distinguish cerebral malaria from meningitis.
Differential diagnosis
The differential includes meningitis, encephalitis, sepsis, acute renal failure, viral hepatitis, acute hemolytic anemia, hypoglycemic coma, and heat stroke. In travelers or immigrants from endemic areas, malaria must be considered in any febrile illness.
Treatment and emergency management
Initial stabilization includes airway, breathing, and circulation management, isotonic fluid resuscitation for hypotension, active cooling for hyperthermia, and treatment of hypoglycemia or seizures as indicated. Antimalarial therapy depends on species, severity, and geographic resistance patterns, with artemisinin-based combination therapies recommended as first-line treatment worldwide. Severe P. falciparum infection requires intravenous artesunate. Supportive care for complications such as anemia, renal failure, and cerebral edema is critical.
Disposition and follow-up
ICU admission is indicated for severe P. falciparum malaria, high parasitemia, neurologic involvement, or inability to tolerate oral therapy. Patients with non–P. falciparum malaria who are clinically stable and able to take oral medications may be treated as outpatients with close follow-up.
Pearls and pitfalls
Malaria should always be considered in patients with fever and compatible exposure history, even months after travel. Fever patterns are unreliable, and early recognition is essential, as delays in treatment—especially with P. falciparum—are associated with high mortality.
- Published on
Emergency and Acute Medicine – Mallory–Weiss Syndrome
Basics description
Mallory–Weiss syndrome is a partial-thickness, longitudinal mucosal tear of the distal esophagus or proximal stomach. It results from a sudden increase in intra-abdominal or transgastric pressure, leading to mild to moderate submucosal arterial or venous bleeding. Endoscopic observations suggest that transient “mushrooming” of the stomach into the esophagus during forceful retching contributes to tear formation. It accounts for approximately 5% of all cases of upper gastrointestinal bleeding.
Etiology and risk factors
The condition is most commonly associated with forceful vomiting or retching but may also occur with coughing, laughing, lifting, straining, blunt abdominal trauma, seizures, childbirth, or cardiopulmonary resuscitation. Alcohol use, particularly following binge drinking, and the presence of a hiatal hernia are significant risk factors. More severe bleeding is seen in patients with portal hypertension, esophageal varices, or underlying coagulopathy.
Diagnosis signs and symptoms
Patients typically report multiple episodes of nonbloody vomiting or retching followed by hematemesis. Most bleeding is self-limited, though severe or life-threatening hemorrhage can occur. Associated symptoms include epigastric or back pain and signs of volume depletion such as dizziness, light-headedness, or syncope. Physical examination may reveal hematemesis, melena, postural hypotension, or shock in severe cases.
Essential workup and diagnostic testing
Initial evaluation includes a complete blood count and rectal examination for occult blood. Additional laboratory studies include coagulation parameters, electrolytes, renal function tests, liver function tests, and type and cross-match if bleeding is significant. Upright chest radiography may be obtained to exclude esophageal or gastric perforation. Upper endoscopy is the diagnostic and therapeutic modality of choice, allowing direct visualization and management of the bleeding source.
Differential diagnosis
Conditions to consider include nasopharyngeal bleeding, hemoptysis, esophageal rupture (Boerhaave syndrome), esophagitis, gastritis, peptic ulcer disease, variceal bleeding, malignancy, and vascular-enteric fistula.
Treatment and emergency management
Initial management focuses on airway protection, oxygenation, and hemodynamic stabilization with large-bore intravenous access and fluid resuscitation. Blood transfusion is indicated for ongoing bleeding or hemodynamic instability. Most cases resolve with conservative therapy. Persistent or active bleeding requires urgent endoscopic intervention, which may include injection therapy, thermal coagulation, clipping, or band ligation. Proton pump inhibitors and antiemetics are used adjunctively. Surgical or angiographic intervention is reserved for refractory cases.
Disposition and follow-up
Patients with ongoing or massive hemorrhage, hemodynamic instability, significant comorbidities, or advanced age require ICU admission. Stable patients with minimal bleeding that has resolved and stable hematocrit may be admitted for observation or, in select cases, discharged with close follow-up and outpatient endoscopy.
Key points and cautions
Early placement of large-bore intravenous access and prompt resuscitation are critical in upper gastrointestinal bleeding. Early gastroenterology consultation is essential when bleeding is significant. Rebleeding most often occurs within the first 24 hours and is more likely in patients with coagulopathy or portal hypertension.
Basics description
Mallory–Weiss syndrome is a partial-thickness, longitudinal mucosal tear of the distal esophagus or proximal stomach. It results from a sudden increase in intra-abdominal or transgastric pressure, leading to mild to moderate submucosal arterial or venous bleeding. Endoscopic observations suggest that transient “mushrooming” of the stomach into the esophagus during forceful retching contributes to tear formation. It accounts for approximately 5% of all cases of upper gastrointestinal bleeding.
Etiology and risk factors
The condition is most commonly associated with forceful vomiting or retching but may also occur with coughing, laughing, lifting, straining, blunt abdominal trauma, seizures, childbirth, or cardiopulmonary resuscitation. Alcohol use, particularly following binge drinking, and the presence of a hiatal hernia are significant risk factors. More severe bleeding is seen in patients with portal hypertension, esophageal varices, or underlying coagulopathy.
Diagnosis signs and symptoms
Patients typically report multiple episodes of nonbloody vomiting or retching followed by hematemesis. Most bleeding is self-limited, though severe or life-threatening hemorrhage can occur. Associated symptoms include epigastric or back pain and signs of volume depletion such as dizziness, light-headedness, or syncope. Physical examination may reveal hematemesis, melena, postural hypotension, or shock in severe cases.
Essential workup and diagnostic testing
Initial evaluation includes a complete blood count and rectal examination for occult blood. Additional laboratory studies include coagulation parameters, electrolytes, renal function tests, liver function tests, and type and cross-match if bleeding is significant. Upright chest radiography may be obtained to exclude esophageal or gastric perforation. Upper endoscopy is the diagnostic and therapeutic modality of choice, allowing direct visualization and management of the bleeding source.
Differential diagnosis
Conditions to consider include nasopharyngeal bleeding, hemoptysis, esophageal rupture (Boerhaave syndrome), esophagitis, gastritis, peptic ulcer disease, variceal bleeding, malignancy, and vascular-enteric fistula.
Treatment and emergency management
Initial management focuses on airway protection, oxygenation, and hemodynamic stabilization with large-bore intravenous access and fluid resuscitation. Blood transfusion is indicated for ongoing bleeding or hemodynamic instability. Most cases resolve with conservative therapy. Persistent or active bleeding requires urgent endoscopic intervention, which may include injection therapy, thermal coagulation, clipping, or band ligation. Proton pump inhibitors and antiemetics are used adjunctively. Surgical or angiographic intervention is reserved for refractory cases.
Disposition and follow-up
Patients with ongoing or massive hemorrhage, hemodynamic instability, significant comorbidities, or advanced age require ICU admission. Stable patients with minimal bleeding that has resolved and stable hematocrit may be admitted for observation or, in select cases, discharged with close follow-up and outpatient endoscopy.
Key points and cautions
Early placement of large-bore intravenous access and prompt resuscitation are critical in upper gastrointestinal bleeding. Early gastroenterology consultation is essential when bleeding is significant. Rebleeding most often occurs within the first 24 hours and is more likely in patients with coagulopathy or portal hypertension.

- Published on
Emergency and Acute Medicine – Mastitis
Basics description
Mastitis is an infection of the breast characterized by pain, swelling, erythema, and warmth, most commonly occurring in women who are breast-feeding. Systemic symptoms such as malaise and fever are frequent. Incidence may reach up to one-third of lactating women, with onset typically between 2–3 weeks and several months postpartum, most often before the infant is 3 months old. It is uncommon during the first postpartum week and is more frequent in advanced maternal age and patients with diabetes. Potential complications include recurrence, abscess formation, sepsis, necrotizing fasciitis, fistula, scarring, and breast hypoplasia. In rare cases, mastitis can occur in full-term infants younger than 2 months.
Etiology and risk factors
Staphylococcus aureus is the most common causative organism. Less frequent pathogens include coagulase-negative Staphylococcus, Streptococcus species, Escherichia coli, Haemophilus influenzae, and Candida albicans. Predisposing factors include cracked nipples, poor infant latch, local milk stasis, nipple piercing, poor maternal nutrition, prior mastitis, primiparity, tight bras, sore nipples, short infant frenulum, use of manual breast pumps, and maternal yeast infection.
Diagnosis signs and symptoms
Patients typically present with fever and chills, often exceeding 38.3°C, along with generalized malaise and tachycardia. Local findings include unilateral breast pain, induration, erythema, warmth, and swelling, sometimes in a wedge-shaped distribution. Decreased milk outflow and purulent nipple discharge may occur. Axillary lymphadenopathy can be present.
Essential workup and diagnostic testing
Diagnosis is primarily clinical. Careful breast examination is essential to assess for abscess formation, which may be subtle and is often periareolar. Breast milk cultures are generally unnecessary. Ultrasound should be obtained if abscess is suspected, while mammography is not indicated acutely. In neonates, evaluation for abscess and systemic infection is critical, and a sepsis workup may be required if the infant is febrile or ill appearing.
Differential diagnosis
Conditions to consider include breast engorgement, which is typically bilateral and occurs early postpartum with transient low-grade fever, inflammatory breast carcinoma, cysts or tumors, and breast abscess.
Treatment and emergency management
Breast-feeding should be continued whenever possible, as milk drainage is therapeutic and does not harm the infant. If the infant refuses milk from the affected breast, pumping and discarding milk is recommended. Supportive care includes breast massage, warm or cold compresses, hydration, and optimization of breast-feeding technique, often with lactation consultant support. Mild early cases may resolve without antibiotics. When antibiotics are required, oral therapy for 7–14 days is standard, with dicloxacillin or a first-generation cephalosporin as first-line options. Clindamycin, trimethoprim/sulfamethoxazole, or erythromycin may be used in penicillin-allergic patients or when MRSA is suspected, guided by local resistance patterns. Surgical consultation is indicated for suspected abscess.
Disposition and follow-up
Most patients can be managed as outpatients, with clinical improvement expected within 48 hours of therapy. Admission is indicated for patients requiring incision and drainage under anesthesia, those who are immunocompromised or septic, patients with diabetes and severe infection, and neonates with mastitis. Follow-up with a primary care physician is recommended, and lactation consultant involvement is often beneficial. Persistent or atypical cases should be evaluated to exclude inflammatory breast carcinoma.
Key points and cautions
Discontinuation of breast-feeding increases milk stasis and the risk of abscess formation. Many cases respond to supportive care alone, and unnecessary cessation of breast-feeding is a common and avoidable complication.

- Published on
KembaraXtra-Medicine – Mandibular Fractures
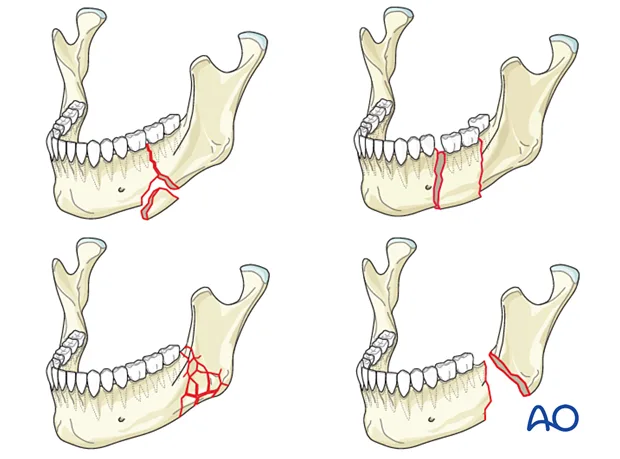
Mandibular fractures most commonly result from a direct force to the jaw and represent the third most frequent facial fracture after nasal and zygomatic fractures. The angle of the mandible is the most commonly fractured site, followed by the condyle, molar, and mental regions, while fractures of the mandibular symphysis are rare due to its thickness. Because the mandible forms a ring-like structure, multiple fractures occur in more than half of cases, and bilateral fractures are particularly common in motor vehicle accidents. Open fractures are frequent, often presenting with lacerations of the overlying gingiva.
The etiology of mandibular fractures includes motor vehicle accidents, interpersonal violence, contact sports, and industrial injuries. Patients are frequently intoxicated at the time of injury, which may limit the accuracy of the clinical history. Associated injuries are common, especially facial and head lacerations and other facial fractures. In children younger than six years, mandibular fractures are uncommon and often present as greenstick fractures that may be managed conservatively with a soft diet. However, because mandibular fractures can damage permanent tooth buds and affect growth plates, pediatric patients should be referred to specialists experienced in managing children.
Clinically, patients may present with mandibular pain, facial asymmetry or deformity, dysphagia, malocclusion, trismus, and decreased range of motion of the temporomandibular joint. A grating sensation conducted to the ear may be reported. Gum lacerations, hematomas, or bleeding around teeth are common, and paresthesia of the lower lip or gums suggests injury to the inferior alveolar nerve. Physical examination may reveal step-offs, bony tenderness along the mandible, loose or missing teeth, ecchymosis of the floor of the mouth, deviation of the jaw with opening, or inability to open the mouth sufficiently. A positive tongue blade test, where the patient cannot hold or break a tongue depressor between the teeth, strongly suggests a mandibular fracture.
Diagnosis requires imaging, most commonly plain radiographs or a panoramic dental radiograph (panorex). Mandibular series views are best for evaluating the condyles and neck, while panorex imaging is superior for assessing the symphysis and body of the mandible. If a condylar fracture is suspected but not visualized, computed tomography of the condyles in the coronal plane should be obtained. A low threshold for facial bone CT is recommended when associated facial injuries are suspected. Missing teeth must always be accounted for, and a chest radiograph is required if aspiration is a concern. Cervical spine imaging should be performed when the neck cannot be clinically cleared.
The differential diagnosis includes mandibular contusions, mandibular dislocation, and isolated dental trauma. In cases of dislocation, the jaw deviates away from the side of dislocation, whereas with fracture it deviates toward the fractured side. Initial management focuses on airway protection and cervical spine stabilization, as up to 40% of patients have associated injuries that may be life-threatening. If oral intubation is not feasible, nasotracheal intubation may be performed unless facial injuries contraindicate it, in which case a surgical airway may be required.
Most mandibular fractures, except isolated condylar fractures, are considered open fractures due to mucosal or gingival disruption and require antibiotic coverage against oral anaerobes as well as tetanus prophylaxis. Analgesia is provided as needed. Definitive treatment usually involves reduction and fixation, either by wiring the jaws in occlusion for several weeks or by open reduction and internal fixation. Linear, nondisplaced, or greenstick fractures may be managed conservatively with a soft diet. Mandibular dislocations should be reduced with appropriate technique, often aided by muscle relaxants or local anesthesia.
Patients with significant displacement, open fractures, associated dental trauma, unreliable follow-up, or risk of airway compromise should be admitted for specialist care. Stable patients with nondisplaced, closed fractures may be discharged with analgesics, antibiotics if indicated, and instructions for a soft diet, with close follow-up by an oral or maxillofacial surgeon within two to three days. Early recognition of malocclusion, proper imaging of the condyles, prompt antibiotic therapy for open fractures, and accounting for missing teeth are essential to avoid complications.
Mandibular fractures most commonly result from a direct force to the jaw and represent the third most frequent facial fracture after nasal and zygomatic fractures. The angle of the mandible is the most commonly fractured site, followed by the condyle, molar, and mental regions, while fractures of the mandibular symphysis are rare due to its thickness. Because the mandible forms a ring-like structure, multiple fractures occur in more than half of cases, and bilateral fractures are particularly common in motor vehicle accidents. Open fractures are frequent, often presenting with lacerations of the overlying gingiva.
The etiology of mandibular fractures includes motor vehicle accidents, interpersonal violence, contact sports, and industrial injuries. Patients are frequently intoxicated at the time of injury, which may limit the accuracy of the clinical history. Associated injuries are common, especially facial and head lacerations and other facial fractures. In children younger than six years, mandibular fractures are uncommon and often present as greenstick fractures that may be managed conservatively with a soft diet. However, because mandibular fractures can damage permanent tooth buds and affect growth plates, pediatric patients should be referred to specialists experienced in managing children.
Clinically, patients may present with mandibular pain, facial asymmetry or deformity, dysphagia, malocclusion, trismus, and decreased range of motion of the temporomandibular joint. A grating sensation conducted to the ear may be reported. Gum lacerations, hematomas, or bleeding around teeth are common, and paresthesia of the lower lip or gums suggests injury to the inferior alveolar nerve. Physical examination may reveal step-offs, bony tenderness along the mandible, loose or missing teeth, ecchymosis of the floor of the mouth, deviation of the jaw with opening, or inability to open the mouth sufficiently. A positive tongue blade test, where the patient cannot hold or break a tongue depressor between the teeth, strongly suggests a mandibular fracture.
Diagnosis requires imaging, most commonly plain radiographs or a panoramic dental radiograph (panorex). Mandibular series views are best for evaluating the condyles and neck, while panorex imaging is superior for assessing the symphysis and body of the mandible. If a condylar fracture is suspected but not visualized, computed tomography of the condyles in the coronal plane should be obtained. A low threshold for facial bone CT is recommended when associated facial injuries are suspected. Missing teeth must always be accounted for, and a chest radiograph is required if aspiration is a concern. Cervical spine imaging should be performed when the neck cannot be clinically cleared.
The differential diagnosis includes mandibular contusions, mandibular dislocation, and isolated dental trauma. In cases of dislocation, the jaw deviates away from the side of dislocation, whereas with fracture it deviates toward the fractured side. Initial management focuses on airway protection and cervical spine stabilization, as up to 40% of patients have associated injuries that may be life-threatening. If oral intubation is not feasible, nasotracheal intubation may be performed unless facial injuries contraindicate it, in which case a surgical airway may be required.
Most mandibular fractures, except isolated condylar fractures, are considered open fractures due to mucosal or gingival disruption and require antibiotic coverage against oral anaerobes as well as tetanus prophylaxis. Analgesia is provided as needed. Definitive treatment usually involves reduction and fixation, either by wiring the jaws in occlusion for several weeks or by open reduction and internal fixation. Linear, nondisplaced, or greenstick fractures may be managed conservatively with a soft diet. Mandibular dislocations should be reduced with appropriate technique, often aided by muscle relaxants or local anesthesia.
Patients with significant displacement, open fractures, associated dental trauma, unreliable follow-up, or risk of airway compromise should be admitted for specialist care. Stable patients with nondisplaced, closed fractures may be discharged with analgesics, antibiotics if indicated, and instructions for a soft diet, with close follow-up by an oral or maxillofacial surgeon within two to three days. Early recognition of malocclusion, proper imaging of the condyles, prompt antibiotic therapy for open fractures, and accounting for missing teeth are essential to avoid complications.
- Published on
KembaraXtra-Medicine – Methanol Poisoning
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.

- Published on
KembaraXtra – Medicine – Ménière Disease
Ménière disease is a chronic disorder of the inner ear characterized by recurrent, spontaneous episodes of vertigo accompanied by sensorineural hearing loss, tinnitus, and a sensation of aural fullness. The condition most commonly affects one ear, although bilateral involvement may occur in up to 40% of patients. The estimated incidence is approximately 15 per 100,000 people in the United States, with a slight female predominance. Although Ménière disease can occur at any age, it most frequently presents between 40 and 60 years of age. While benign and nonfatal, it can lead to significant morbidity due to the unpredictability and severity of symptoms.
The etiology of Ménière disease is idiopathic, with endolymphatic hydrops considered the primary underlying mechanism. This condition results from impaired drainage of endolymph from the endolymphatic sac and duct, leading to increased pressure within the endolymphatic system. Elevated pressure may cause rupture of the membrane separating potassium-rich endolymph from potassium-poor perilymph, resulting in abnormal stimulation and transient dysfunction of vestibular and cochlear nerve receptors. Additional proposed contributors include structural abnormalities of the endolymphatic system, autoimmune processes, genetic predisposition, remote viral injury, and ischemia of the inner ear. It is important to distinguish Ménière disease from secondary Ménière syndrome caused by conditions such as thyroid disease, syphilis, autoimmune inner ear disease, or medication effects.
Diagnosis is based primarily on clinical features supported by neurotologic evaluation. Definitive diagnosis requires histopathologic confirmation and therefore can only be made postmortem, though modern MRI techniques may provide supportive evidence. Diagnostic criteria include at least two spontaneous episodes of vertigo lasting 20 minutes or longer, at least one documented episode of sensorineural hearing loss on audiometric testing, and the presence of tinnitus or aural fullness in the affected ear. Based on the completeness of findings, cases are categorized as definite, probable, or possible Ménière disease.
Patients typically present with the classic tetrad of vertigo, hearing loss, tinnitus, and aural fullness. Vertigo attacks last from minutes to hours and are frequently associated with nausea and vomiting. Hearing loss is sensorineural, fluctuating, and progressive, often initially affecting low frequencies before potentially involving all frequencies over time. Tinnitus is commonly low-pitched and described as roaring, while aural fullness is perceived as pressure or congestion in the affected ear. Attacks usually reach peak intensity rapidly and resolve gradually, leaving patients fatigued and unsteady for hours to days. Some individuals may be asymptomatic between episodes, while others experience persistent imbalance. Sudden drop attacks without loss of consciousness may also occur.
Physical examination findings vary depending on whether the patient is evaluated during or between attacks. During acute episodes, patients may appear pale, diaphoretic, and distressed. Horizontal nystagmus and impaired hearing are commonly observed. Tuning fork testing often reveals lateralization away from the affected ear on Weber testing, with preserved air conduction on Rinne testing. Romberg testing may demonstrate postural instability, particularly with eyes closed. A thorough neurologic and otologic examination is essential to exclude central nervous system pathology or alternative peripheral ear disorders.
The essential evaluation includes a detailed history and complete neurologic examination. Neuroimaging is warranted when central causes of vertigo are suspected or when focal neurologic deficits are present, particularly in patients with new unilateral hearing loss. Audiometric testing is critical for documenting sensorineural hearing loss, and additional vestibular studies such as caloric testing, electronystagmography, or electrocochleography are typically performed in the outpatient setting. Laboratory investigations are reserved for suspected systemic or secondary causes.
Management in the acute setting focuses on symptom control and exclusion of life-threatening conditions such as stroke. Patients should be protected from falls and maintained in a comfortable position. Intravenous fluids are indicated for dehydration due to vomiting. Benzodiazepines and antiemetics are first-line therapies for acute vertigo and nausea, with antihistamines used as adjuncts. Long-term management aims to reduce the frequency and severity of attacks through dietary sodium restriction, avoidance of triggers such as caffeine and alcohol, diuretics, corticosteroids, and selected transtympanic therapies. Surgical interventions are reserved for patients with severe, refractory disease.
Disposition depends on symptom severity and response to treatment. Admission is indicated for patients with intractable vertigo, persistent vomiting, dehydration, or inability to ambulate safely. Most patients can be discharged once symptoms are controlled, oral intake is tolerated, gait is stable, and neurologic examination is normal. Discharged patients should receive fall precautions and counseling to avoid driving or hazardous activities until symptoms have resolved and sedating medications have been discontinued. Outpatient follow-up with otolaryngology, otology, or neurology is recommended for further evaluation, audiometry, and long-term management.