- Published on
KembaraXtra-Medicine – Methanol Poisoning
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.

- Published on
KembaraXtra-Medicine – Methanol Poisoning
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.
Methanol is a colorless, volatile liquid that is rapidly absorbed within 30–60 minutes and metabolized by the liver, with a half-life of approximately 4–8 hours. Methanol itself is relatively nontoxic and produces inebriation similar to ethanol. Toxicity results from its metabolites, formaldehyde and formic acid, which inhibit cytochrome oxidase and disrupt cellular respiration. Formic acid is primarily responsible for severe metabolic acidosis, visual toxicity, and mortality, as it is directly toxic to the retina and optic nerve. Methanol is metabolized in three steps: conversion to formaldehyde by alcohol dehydrogenase, rapid conversion of formaldehyde to formic acid by aldehyde dehydrogenase, and folate-dependent degradation of formic acid to carbon dioxide and water. The first and third steps are rate-limiting.
Common sources of methanol exposure include windshield washer fluid, wood alcohol, carburetor cleaners, fuel antifreeze solutions, formalin, gasoline, paint solvents, household cleaners, Sterno cans, moonshine, model airplane fuel, photocopying fluids, and perfumes. Ingestion may be intentional or accidental, and inhalational exposure can occur with solvent abuse.
Clinical manifestations often begin with gastrointestinal symptoms such as anorexia, nausea, vomiting, and abdominal pain. Central nervous system findings include headache, dizziness, confusion, inebriation, seizures, and coma. Ophthalmologic symptoms are characteristic and include blurry or hazy vision, photophobia, “snowfield” vision, central scotomas, and potentially permanent blindness. Patients may present without a clear ingestion history but instead with an unexplained high anion gap metabolic acidosis and elevated osmol gap. On examination, findings may include tachypnea, altered mental status, optic disc hyperemia or pallor, papilledema, and afferent pupillary defects.
Evaluation requires a careful history of all possible ingestions and attention to visual complaints, along with a funduscopic examination. Essential laboratory tests include arterial blood gas analysis, serum electrolytes, glucose, BUN, creatinine, measured serum osmolality, and serum levels of methanol, ethanol, ethylene glycol, and isopropyl alcohol. The anion gap and osmol gap should be calculated. The osmol gap is most useful early in poisoning, as methanol is osmotically active, whereas its toxic metabolites are not. Importantly, a normal osmol gap does not exclude methanol poisoning, especially in late presenters. Serum methanol levels confirm the diagnosis, though levels may be undetectable late in the course when severe acidosis is present.
Management begins with prompt stabilization of airway, breathing, and circulation, along with administration of dextrose, naloxone, and thiamine for altered mental status. Further absorption is limited by supportive care, as gastric lavage and activated charcoal have limited benefit due to rapid methanol absorption. The cornerstone of treatment is inhibition of alcohol dehydrogenase to prevent formation of toxic metabolites. Fomepizole is the preferred antidote and should be initiated promptly when methanol ingestion is suspected, even before serum levels return. Ethanol infusion is an alternative when fomepizole is unavailable but is associated with significant adverse effects and requires close monitoring.
Hemodialysis plays a critical role by enhancing elimination of methanol and its metabolites and correcting severe acidosis. Indications include visual symptoms, severe or refractory metabolic acidosis, renal failure, ingestion of large amounts of methanol, or serum methanol levels greater than 25 mg/dL. Hemodialysis is continued until methanol levels fall below 25 mg/dL and acidosis resolves. Adjunctive therapy with folic or folinic acid is recommended to enhance metabolism of formic acid. Sodium bicarbonate is used to correct severe acidosis, with the goal of maintaining a normal serum pH.
Patients with significant exposure require hospital admission, often to the intensive care unit, and transfer to a facility with antidote availability and hemodialysis capability if needed. Asymptomatic patients with low methanol levels, normal acid–base status, and stable electrolytes may be considered for discharge. Psychiatric evaluation is important in cases of intentional ingestion. Early recognition and treatment are essential, as delays greatly increase the risk of blindness and death.

- Published on
KembaraXtra-Medicine – Mercury Poisoning
Mercury poisoning results from exposure to mercury in one of three primary forms: elemental, inorganic salts, or organic mercury. Mercury exerts its toxic effects by reacting with sulfhydryl groups, leading to enzyme inhibition and disruption of cellular membranes. It also binds to phosphoryl, carboxyl, amide, and amine groups of enzymes, further impairing normal cellular function.
Exposure most commonly occurs through inhalation or ingestion, and less frequently through dermal contact. Occupational and environmental exposures are well recognized and include industries such as chlorine and caustic soda manufacturing, dentistry, photography, taxidermy, mercury mining, and the production of thermometers, batteries, lamps, plastics, paints, pigments, fireworks, and explosives. Contaminated seafood is a major source of organic mercury exposure in the general population.
The clinical presentation varies depending on the form of mercury involved. Elemental mercury exposure most often occurs through inhalation, with symptoms developing within hours. Patients may experience cough and dyspnea that can progress to noncardiogenic pulmonary edema, along with metallic taste, excessive salivation, weakness, nausea, diarrhea, fever, headaches, and visual disturbances. Subcutaneous or intravenous exposure may lead to granulomas, abscesses, or pulmonary embolization. Elemental mercury is relatively nontoxic when ingested orally due to poor gastrointestinal absorption.
Inorganic mercurial salt ingestion causes severe caustic gastrointestinal injury. Symptoms include abdominal pain, nausea, vomiting, diarrhea, sore throat, and a metallic taste. Hemorrhagic gastroenteritis with hematemesis and hematochezia may occur, along with acute tubular necrosis and renal failure. Acrodynia, also known as pink disease, is an idiosyncratic reaction seen mainly in children and is characterized by painful extremities, pink discoloration, and desquamation.
Organic mercury exposure, commonly through contaminated seafood, primarily affects the central nervous system. While mild gastrointestinal symptoms may occur acutely, delayed neurologic toxicity predominates and may take weeks to months to appear. Manifestations include paresthesias, ataxia, paralysis, visual field constriction, dysarthria, hearing loss, progressive cognitive decline, and death. Fetal exposure in utero is associated with particularly severe neurologic outcomes.
Diagnosis relies heavily on a detailed exposure history, including occupational risks and recent seafood consumption. Physical examination focuses on identifying respiratory distress, signs of caustic gastrointestinal injury, and neuropsychiatric abnormalities. Laboratory evaluation may reveal renal dysfunction, but mercury levels in blood or urine can be misleading, especially after recent seafood ingestion. Imaging studies such as chest radiographs may show pulmonary edema or metallic deposits, abdominal radiographs can identify ingested mercury, and head CT may demonstrate cerebellar atrophy in chronic cases.
Management begins with immediate removal from the source of exposure and stabilization of airway, breathing, and circulation. Supportive care includes oxygen, intravenous fluids for hypotension, and treatment of altered mental status with dextrose, thiamine, and naloxone when indicated. Elemental mercury inhalation requires close observation for delayed pulmonary edema. Inorganic mercury ingestion warrants aggressive fluid resuscitation and early treatment of shock or renal failure.
Chelation therapy is indicated for symptomatic patients. Dimercaptosuccinic acid (DMSA) is commonly used for organic and some elemental mercury exposures, while dimercaprol (British anti-Lewisite) is preferred for severe inorganic mercury poisoning. Activated charcoal may be used for recent ingestions. Surgical incision and drainage may be required for subcutaneous mercury deposits.
Hospital admission is recommended for patients with respiratory compromise, renal impairment, caustic gastrointestinal injury, or those requiring chelation therapy. Asymptomatic patients exposed to elemental mercury may be discharged after an adequate observation period. Follow-up includes repeat mercury testing, avoidance of seafood before testing, and referral to medical toxicology. Early recognition, thorough exposure history, and appropriate chelation are critical to reducing morbidity and preventing long-term neurologic sequelae.
Mercury poisoning results from exposure to mercury in one of three primary forms: elemental, inorganic salts, or organic mercury. Mercury exerts its toxic effects by reacting with sulfhydryl groups, leading to enzyme inhibition and disruption of cellular membranes. It also binds to phosphoryl, carboxyl, amide, and amine groups of enzymes, further impairing normal cellular function.
Exposure most commonly occurs through inhalation or ingestion, and less frequently through dermal contact. Occupational and environmental exposures are well recognized and include industries such as chlorine and caustic soda manufacturing, dentistry, photography, taxidermy, mercury mining, and the production of thermometers, batteries, lamps, plastics, paints, pigments, fireworks, and explosives. Contaminated seafood is a major source of organic mercury exposure in the general population.
The clinical presentation varies depending on the form of mercury involved. Elemental mercury exposure most often occurs through inhalation, with symptoms developing within hours. Patients may experience cough and dyspnea that can progress to noncardiogenic pulmonary edema, along with metallic taste, excessive salivation, weakness, nausea, diarrhea, fever, headaches, and visual disturbances. Subcutaneous or intravenous exposure may lead to granulomas, abscesses, or pulmonary embolization. Elemental mercury is relatively nontoxic when ingested orally due to poor gastrointestinal absorption.
Inorganic mercurial salt ingestion causes severe caustic gastrointestinal injury. Symptoms include abdominal pain, nausea, vomiting, diarrhea, sore throat, and a metallic taste. Hemorrhagic gastroenteritis with hematemesis and hematochezia may occur, along with acute tubular necrosis and renal failure. Acrodynia, also known as pink disease, is an idiosyncratic reaction seen mainly in children and is characterized by painful extremities, pink discoloration, and desquamation.
Organic mercury exposure, commonly through contaminated seafood, primarily affects the central nervous system. While mild gastrointestinal symptoms may occur acutely, delayed neurologic toxicity predominates and may take weeks to months to appear. Manifestations include paresthesias, ataxia, paralysis, visual field constriction, dysarthria, hearing loss, progressive cognitive decline, and death. Fetal exposure in utero is associated with particularly severe neurologic outcomes.
Diagnosis relies heavily on a detailed exposure history, including occupational risks and recent seafood consumption. Physical examination focuses on identifying respiratory distress, signs of caustic gastrointestinal injury, and neuropsychiatric abnormalities. Laboratory evaluation may reveal renal dysfunction, but mercury levels in blood or urine can be misleading, especially after recent seafood ingestion. Imaging studies such as chest radiographs may show pulmonary edema or metallic deposits, abdominal radiographs can identify ingested mercury, and head CT may demonstrate cerebellar atrophy in chronic cases.
Management begins with immediate removal from the source of exposure and stabilization of airway, breathing, and circulation. Supportive care includes oxygen, intravenous fluids for hypotension, and treatment of altered mental status with dextrose, thiamine, and naloxone when indicated. Elemental mercury inhalation requires close observation for delayed pulmonary edema. Inorganic mercury ingestion warrants aggressive fluid resuscitation and early treatment of shock or renal failure.
Chelation therapy is indicated for symptomatic patients. Dimercaptosuccinic acid (DMSA) is commonly used for organic and some elemental mercury exposures, while dimercaprol (British anti-Lewisite) is preferred for severe inorganic mercury poisoning. Activated charcoal may be used for recent ingestions. Surgical incision and drainage may be required for subcutaneous mercury deposits.
Hospital admission is recommended for patients with respiratory compromise, renal impairment, caustic gastrointestinal injury, or those requiring chelation therapy. Asymptomatic patients exposed to elemental mercury may be discharged after an adequate observation period. Follow-up includes repeat mercury testing, avoidance of seafood before testing, and referral to medical toxicology. Early recognition, thorough exposure history, and appropriate chelation are critical to reducing morbidity and preventing long-term neurologic sequelae.

- Published on
KembaraXtra – Medicine – Ménière Disease
Ménière disease is a chronic disorder of the inner ear characterized by recurrent, spontaneous episodes of vertigo accompanied by sensorineural hearing loss, tinnitus, and a sensation of aural fullness. The condition most commonly affects one ear, although bilateral involvement may occur in up to 40% of patients. The estimated incidence is approximately 15 per 100,000 people in the United States, with a slight female predominance. Although Ménière disease can occur at any age, it most frequently presents between 40 and 60 years of age. While benign and nonfatal, it can lead to significant morbidity due to the unpredictability and severity of symptoms.
The etiology of Ménière disease is idiopathic, with endolymphatic hydrops considered the primary underlying mechanism. This condition results from impaired drainage of endolymph from the endolymphatic sac and duct, leading to increased pressure within the endolymphatic system. Elevated pressure may cause rupture of the membrane separating potassium-rich endolymph from potassium-poor perilymph, resulting in abnormal stimulation and transient dysfunction of vestibular and cochlear nerve receptors. Additional proposed contributors include structural abnormalities of the endolymphatic system, autoimmune processes, genetic predisposition, remote viral injury, and ischemia of the inner ear. It is important to distinguish Ménière disease from secondary Ménière syndrome caused by conditions such as thyroid disease, syphilis, autoimmune inner ear disease, or medication effects.
Diagnosis is based primarily on clinical features supported by neurotologic evaluation. Definitive diagnosis requires histopathologic confirmation and therefore can only be made postmortem, though modern MRI techniques may provide supportive evidence. Diagnostic criteria include at least two spontaneous episodes of vertigo lasting 20 minutes or longer, at least one documented episode of sensorineural hearing loss on audiometric testing, and the presence of tinnitus or aural fullness in the affected ear. Based on the completeness of findings, cases are categorized as definite, probable, or possible Ménière disease.
Patients typically present with the classic tetrad of vertigo, hearing loss, tinnitus, and aural fullness. Vertigo attacks last from minutes to hours and are frequently associated with nausea and vomiting. Hearing loss is sensorineural, fluctuating, and progressive, often initially affecting low frequencies before potentially involving all frequencies over time. Tinnitus is commonly low-pitched and described as roaring, while aural fullness is perceived as pressure or congestion in the affected ear. Attacks usually reach peak intensity rapidly and resolve gradually, leaving patients fatigued and unsteady for hours to days. Some individuals may be asymptomatic between episodes, while others experience persistent imbalance. Sudden drop attacks without loss of consciousness may also occur.
Physical examination findings vary depending on whether the patient is evaluated during or between attacks. During acute episodes, patients may appear pale, diaphoretic, and distressed. Horizontal nystagmus and impaired hearing are commonly observed. Tuning fork testing often reveals lateralization away from the affected ear on Weber testing, with preserved air conduction on Rinne testing. Romberg testing may demonstrate postural instability, particularly with eyes closed. A thorough neurologic and otologic examination is essential to exclude central nervous system pathology or alternative peripheral ear disorders.
The essential evaluation includes a detailed history and complete neurologic examination. Neuroimaging is warranted when central causes of vertigo are suspected or when focal neurologic deficits are present, particularly in patients with new unilateral hearing loss. Audiometric testing is critical for documenting sensorineural hearing loss, and additional vestibular studies such as caloric testing, electronystagmography, or electrocochleography are typically performed in the outpatient setting. Laboratory investigations are reserved for suspected systemic or secondary causes.
Management in the acute setting focuses on symptom control and exclusion of life-threatening conditions such as stroke. Patients should be protected from falls and maintained in a comfortable position. Intravenous fluids are indicated for dehydration due to vomiting. Benzodiazepines and antiemetics are first-line therapies for acute vertigo and nausea, with antihistamines used as adjuncts. Long-term management aims to reduce the frequency and severity of attacks through dietary sodium restriction, avoidance of triggers such as caffeine and alcohol, diuretics, corticosteroids, and selected transtympanic therapies. Surgical interventions are reserved for patients with severe, refractory disease.
Disposition depends on symptom severity and response to treatment. Admission is indicated for patients with intractable vertigo, persistent vomiting, dehydration, or inability to ambulate safely. Most patients can be discharged once symptoms are controlled, oral intake is tolerated, gait is stable, and neurologic examination is normal. Discharged patients should receive fall precautions and counseling to avoid driving or hazardous activities until symptoms have resolved and sedating medications have been discontinued. Outpatient follow-up with otolaryngology, otology, or neurology is recommended for further evaluation, audiometry, and long-term management.
- Published on
Emergency and Acute Medicine-MDMA Poisoning
Basics description
MDMA (3,4-methylenedioxymethamphetamine), commonly known as ecstasy, is a Schedule I illicit drug used recreationally at rave parties, dance clubs, and college campuses. Onset of effects typically occurs 15–30 minutes after ingestion, with a duration of 2–6 hours. Pills often contain contaminants such as caffeine, ephedrine, dextromethorphan, or ketamine. Related compounds include MDA, MDEA, MDBA, and PMA. MDMA has an amphetamine-like structure that increases catecholamine release and a mescaline-like ring that enhances serotonergic and dopaminergic activity.
Etiology
Toxicity results from deliberate or accidental ingestion of MDMA, often compounded by coingestants or adulterants.
Diagnosis signs and symptoms
Patients may present with altered mental status, severe sympathomimetic features, or hyperthermia. Neurologic findings include excitation, delirium, hallucinations, seizures, coma, and cerebral edema. Cardiovascular manifestations include early hypertension, late hypotension, palpitations, ventricular dysrhythmias, and ectopy. Pulmonary edema may occur. Metabolic complications include hyponatremia, hypoglycemia, and syndrome of inappropriate antidiuretic hormone secretion. Musculoskeletal findings include bruxism, rigidity, and restlessness, with rhabdomyolysis leading to renal failure. Hepatic injury ranges from hepatitis to jaundice, and hematologic complications include disseminated intravascular coagulation. Gastrointestinal symptoms include nausea, vomiting, diarrhea, and abdominal cramping. Other features include hyperthermia, mydriasis, and nystagmus.
Essential workup and diagnostic testing
Diagnosis is primarily clinical, supported by history and examination. Core temperature measurement is critical. Laboratory evaluation includes electrolytes, glucose, BUN, creatinine, coagulation studies, creatine phosphokinase, liver function tests, and urine studies for myoglobin. Urine toxicology screening may show amphetamines but is unreliable for MDMA specificity. ECG commonly shows sinus tachycardia with possible dysrhythmias. Imaging is guided by presentation, with chest radiography for aspiration or pulmonary edema and head CT for suspected intracranial pathology.
Differential diagnosis
Cocaine or amphetamine overdose, anticholinergic toxicity, synthetic cathinone intoxication, serotonin syndrome, sepsis, thyroid storm, pheochromocytoma, or occult head injury.
Treatment and emergency management
Management is supportive and focused on airway protection, oxygenation, IV access, and continuous monitoring. Benzodiazepines are first-line for agitation, anxiety, and seizures. Aggressive IV hydration with isotonic fluids is essential, particularly in rhabdomyolysis. Hyperthermia is treated with active cooling and sedation. Hypertension may require agents such as nitroprusside or phentolamine, while hypotension is treated with fluids and vasopressors as needed. Severe rhabdomyolysis or renal failure may require hemodialysis. Patients should be monitored for at least 6 hours.
Disposition and follow-up
Admission is required for patients with altered mental status, seizures, cardiovascular instability, rhabdomyolysis, disseminated intravascular coagulation, or loss of behavioral control. Asymptomatic patients may be discharged after 6 hours of observation. Substance use counseling is recommended, with psychiatric evaluation for intentional overdose.
Key points and pitfalls
Always obtain a core temperature and evaluate for hyponatremia in patients with persistent altered mental status. Routine toxicology screens may not detect MDMA or coingestants. Consider non-toxicologic causes of deterioration and recognize that hyperthermia and rhabdomyolysis are major causes of morbidity and mortality.

- Published on
Emergency and Acute Medicine – Meningitis
Basics description
Meningitis is an infection of the central nervous system characterized by inflammation of the leptomeninges and an increased white blood cell count in the cerebrospinal fluid (CSF). It commonly presents with fever, headache, neck stiffness, and altered mental status, although manifestations vary by age and immune status.
Etiology
Meningitis may be bacterial, viral, fungal, or noninfectious in origin. In neonates, common bacterial causes include group B Streptococcus, Escherichia coli, other enteric bacilli, and Listeria monocytogenes. In children and adults, Streptococcus pneumoniae and Neisseria meningitidis predominate, while elderly patients and those with alcoholism are at increased risk for pneumococcal infection, gram-negative bacilli, and Listeria. Neurosurgical patients are more likely to develop infections due to staphylococcal or gram-negative organisms. Immunocompromised patients, including those with AIDS, may develop tuberculosis, fungal, or syphilitic meningitis in addition to typical pathogens. Viral meningitis is common and often less severe, while chemical, drug-induced, or toxin-related meningitis is rare.
Clinical presentation
Typical symptoms include fever, headache, photophobia, and neck stiffness. Kernig and Brudzinski signs may be present but are neither sensitive nor specific. Patients may also develop altered mental status, seizures, focal neurologic deficits, papilledema, or a petechial or purpuric rash suggestive of meningococcal disease. Associated infections such as sinusitis, otitis media, or pneumonia may provide clues to the source.
Infants and young children often present atypically, with fever or hypothermia, lethargy, poor feeding, vomiting, respiratory distress, apnea, cyanosis, hypotonia, or a bulging fontanelle. Classic meningeal signs are frequently absent in children under one year of age. Elderly or immunocompromised patients may present primarily with confusion and fewer classic symptoms.
Essential workup
Management should begin immediately when meningitis is suspected. Blood cultures should be obtained promptly, followed by empiric antimicrobial therapy without delay, especially if the patient is unstable. Lumbar puncture is recommended for all patients with suspected meningitis unless contraindicated. Neuroimaging prior to lumbar puncture is reserved for patients at risk for herniation, including those with immunodeficiency, recent seizures, focal neurologic deficits, altered consciousness, papilledema, a history of central nervous system disease, or age over 60 years.
CSF analysis includes cell count and differential, glucose, protein, Gram stain, and culture, with additional studies added as clinically indicated. Elevated opening pressure may be present. Typical bacterial meningitis is associated with low CSF glucose, elevated protein, and a high white blood cell count with neutrophil predominance, although early disease may show fewer abnormalities.
Diagnostic tests and interpretation
Laboratory evaluation includes blood cultures, complete blood count, electrolytes, renal function tests, coagulation studies, and serum glucose for comparison with CSF glucose. Imaging such as head CT is used selectively to assess for contraindications to lumbar puncture or complications. Chest radiography may identify pneumonia or tuberculosis when suspected. Polymerase chain reaction testing and antigen detection may assist in identifying viral or bacterial pathogens when cultures are nondiagnostic.
Differential diagnosis
Conditions that may mimic meningitis include encephalitis, intracranial abscess, epidural or spinal abscess, febrile seizures, intracranial hemorrhage, stroke, systemic or central nervous system lupus, malignancy, venous sinus thrombosis, trauma, and metabolic or toxic encephalopathies.
Treatment and emergency management
Initial management focuses on airway, breathing, and circulation, seizure control, and isolation when appropriate. Empiric intravenous antibiotics should be administered as soon as possible, ideally after blood cultures but without delaying treatment for imaging or lumbar puncture. Antimicrobial regimens are selected based on patient age, immune status, and risk factors, with coverage for likely organisms. Vancomycin is added when resistant pneumococcal infection is a concern, and ampicillin is included in older adults and immunocompromised patients for Listeria coverage. Acyclovir should be started when herpes simplex encephalitis is suspected.
Adjunctive corticosteroids may reduce neurologic complications in selected patients, particularly those with pneumococcal meningitis, and should be given before or with the first dose of antibiotics when indicated.
Disposition and follow-up
Hospital admission is required for all patients with known or suspected bacterial meningitis, immunocompromised patients, and any toxic-appearing individual. Discharge from the emergency department is reserved for carefully selected patients with confirmed viral meningitis, stable clinical status, reliable follow-up, and clear discharge instructions coordinated with primary care.
Pearls and pitfalls
Meningitis rarely presents as a simple febrile seizure in children. Delayed recognition or treatment can lead to severe neurologic injury or death, making early empiric therapy essential. When clinical suspicion is high, treatment should never be postponed while awaiting diagnostic confirmation.

- Published on
Emergency and Acute Medicine – Meckel Diverticulum
Basics description
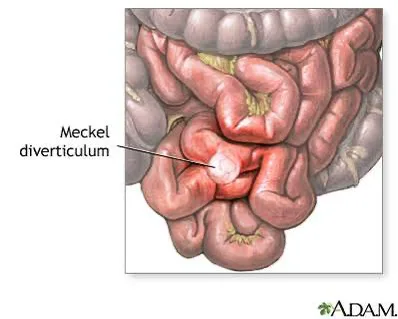
Meckel diverticulum is the most common congenital abnormality of the gastrointestinal tract and results from incomplete obliteration of the omphalomesenteric duct. It is a true diverticulum containing all layers of the bowel wall. Approximately half contain normal ileal mucosa, while the remainder contain ectopic tissue, most commonly gastric, but also pancreatic, duodenal, colonic, endometrial, or hepatobiliary mucosa. The classic “rule of 2’s” applies: it occurs in about 2% of the population, carries a 2% lifetime risk of complications that decreases with age, is usually around 2 inches long, and is located within 2 feet of the ileocecal valve. Symptoms commonly occur around 2 years of age, with nearly half of symptomatic patients presenting before age 2. Although prevalence is similar in males and females, males are more often symptomatic. Complications differ by age, with obstruction and diverticulitis more common in adults and hemorrhage and obstruction more common in children. The mean age of presentation is about 10 years, and current mortality is extremely low.
Etiology
Meckel diverticulum arises from a remnant of the omphalomesenteric duct, which normally regresses by the seventh week of gestation.
Pathophysiology and complications
Obstruction can occur when the diverticulum is attached to the umbilicus, abdominal wall, or other viscera, or when it is free and acts as a lead point. This may result in intussusception, with the diverticulum serving as the leading edge, or volvulus caused by a persistent fibrous band that allows bowel rotation. Diverticulitis occurs when the opening of the diverticulum becomes obstructed, followed by bacterial infection, and often presents similarly to acute appendicitis, which is the most common preoperative diagnosis.
Pediatric considerations
Meckel diverticulum is the most common cause of significant lower gastrointestinal bleeding in children. It typically presents before 5 years of age with episodic, painless, brisk, bright-red rectal bleeding.
Diagnosis, signs, and symptoms
Patients generally present in one of three ways. Rectal bleeding occurs due to hemorrhage from mucosal ulceration associated with ectopic gastric tissue. Vomiting may result from bowel obstruction caused by volvulus, intussusception, or intraperitoneal bands. Abdominal pain, often appendicitis-like, may occur with an inflamed or perforated diverticulum. Associated findings include fever, malaise, weakness, fatigue, abdominal distention, changes in bowel habits, hematochezia or melena, and in advanced cases, peritonitis or septic shock. Tachycardia and hypotension may be present due to pain or blood loss.
Essential workup
Meckel diverticulum can produce a wide variety of nonspecific symptoms, and fewer than 10% of cases are diagnosed preoperatively. It should be considered in patients with recurrent nonspecific abdominal pain, nausea and vomiting, or rectal bleeding. History and physical examination may narrow the diagnosis but are not definitive. Rectal examination is mandatory, and nasogastric tube placement may help rule out an upper gastrointestinal bleed.
Diagnostic tests and interpretation
Laboratory evaluation may reveal a decreased hematocrit from bleeding or leukocytosis in cases of diverticulitis, perforation, or gangrene. Electrolytes, renal function, and coagulation studies should be obtained, and type and screen or cross-match is required with significant bleeding. Computed tomography of the abdomen and pelvis is useful for suspected infection or bowel obstruction but cannot reliably diagnose Meckel diverticulum. Abdominal radiographs may screen for obstruction but are not diagnostic. A technetium-99m pertechnetate scan (Meckel scan) can identify heterotopic gastric mucosa and is highly accurate in children but less sensitive in adults. Small bowel enteroclysis, barium enema, angiography, ultrasound, or laparoscopic evaluation may be used in selected cases. Colonoscopy is not helpful.
Differential diagnosis
In adults, the differential includes appendicitis, adhesions, bowel obstruction, diverticulitis, hemorrhoids, inflammatory bowel disease, internal hernias, intussusception, peptic ulcer disease, pseudomembranous colitis, and volvulus. In children, considerations include anal fissures, appendicitis, atresia, gastroenteritis, hemolytic–uremic syndrome, Henoch–Schönlein purpura, intussusception, malrotation, milk allergy, strictures, and volvulus.
Treatment and emergency management
Prehospital management includes establishing intravenous access for patients with rectal bleeding or abdominal pain. Initial stabilization focuses on resuscitation and early surgical consultation. Hypotension is treated with aggressive fluid resuscitation, packed red blood cell transfusion for brisk bleeding, and vasopressors if septic shock is present. In the emergency department, gastrointestinal bleeding is managed with fluids and transfusion as indicated, Foley catheter placement to monitor urine output, and nasogastric tube placement to exclude brisk upper gastrointestinal bleeding. Obstruction requires nasogastric decompression and surgical consultation. Suspected diverticulitis or perforation requires nil per os status, preoperative antibiotics, and urgent surgical evaluation.
Definitive management
Symptomatic Meckel diverticula should be surgically resected. In children, asymptomatic Meckel diverticula discovered incidentally during laparotomy are generally resected to prevent future complications.
Disposition and follow-up
Admission is required for presumptive or confirmed Meckel diverticulum associated with diverticulitis, obstruction, intussusception, hemorrhage, or volvulus. There are no discharge criteria from the emergency department for suspected cases. Postoperative surgical follow-up is required.
Pearls and pitfalls
Painless, brisk, bright-red rectal bleeding in an infant is most often caused by Meckel diverticulum. The condition presents with a broad range of complications, including obstruction, intussusception, and hemorrhage, and is frequently diagnosed intraoperatively during surgery for presumed appendicitis. Remember the rule of 2’s to aid clinical recognition.
- Published on
Emergency and Acute Medicine – Measles
Basics description
Measles, also known as rubeola, is a vaccine-preventable infectious disease that primarily affects children and is characterized by fever, cough, coryza, conjunctivitis, and an erythematous maculopapular rash. Due to widespread immunization, incidence is now low, but outbreaks continue to occur in nonimmunized or underimmunized populations.
Etiology
Measles is caused by the rubeola virus, a morbillivirus in the paramyxovirus family with negative-strand RNA. Humans are the only known reservoir. The virus is highly contagious and transmitted via respiratory droplets or direct contact; therefore, respiratory isolation must be initiated when measles is suspected. Outbreaks are most often associated with lapses in vaccination coverage.
Special populations
During pregnancy, measles infection increases the risk of spontaneous abortion and premature contractions but does not appear to cause congenital malformations. Pregnant patients should not receive MMR or MMRV vaccines. Adults born before 1957 are generally considered immune; however, health care workers should receive vaccination if serologic testing shows negative titers. In pediatrics, routine immunization with MMR or MMRV begins at ≥12 months of age, with a second dose at 4–6 years; catch-up doses must be spaced at least 4 weeks apart.
Diagnosis, signs, and symptoms
After an incubation period of approximately 10–12 days, patients develop a prodrome lasting 1–7 days with fever, malaise, cough, coryza, and conjunctivitis. Koplik spots—small white to grayish-blue lesions on the buccal mucosa—are pathognomonic and appear 1–2 days before the rash, disappearing shortly after rash onset. The classic maculopapular blanching rash develops 3–7 days into illness, beginning on the head and spreading downward. It may become confluent and occasionally petechial, rarely involving the palms and soles. Rash resolution occurs over several days and may be followed by desquamation.
Complications
Respiratory complications are common, with pneumonia occurring in approximately 6% of cases and representing the most frequent cause of death, particularly in immunocompromised patients. Otitis media, sinusitis, and diarrhea are also frequent. Neurologic complications include seizures and encephalitis, which may develop days after rash onset due to postinfectious autoimmune mechanisms. A rare but fatal late complication is subacute sclerosing panencephalitis, occurring years after infection. Cardiovascular complications such as myocarditis or conduction defects are uncommon but may be clinically significant in older adults.
Essential workup and diagnostic testing
Diagnosis is primarily clinical, based on the combination of fever, cough, coryza, conjunctivitis, and characteristic rash. Laboratory confirmation may include measles IgM and IgG serology or PCR for measles RNA. Viral isolation from blood, throat, nasopharynx, or urine is mainly for epidemiologic surveillance. CSF analysis is indicated if encephalitis is suspected, and chest radiography is obtained when pneumonia is a concern.
Differential diagnosis
Conditions to consider include rubella, scarlet fever, infectious mononucleosis, roseola, erythema infectiosum, enteroviral infections, Kawasaki disease, secondary syphilis, toxic shock syndrome, and drug reactions.
Treatment and emergency management
Management is primarily supportive, focusing on antipyretics, hydration, and monitoring for complications. Strict isolation is required. Postexposure prophylaxis for susceptible individuals includes MMR vaccination within 72 hours of exposure or intramuscular immune globulin within 6 days for high-risk contacts such as infants, pregnant patients, and immunocompromised individuals. Oxygenation and airway protection are essential in cases complicated by pneumonia or encephalitis.
Medications
The World Health Organization recommends vitamin A supplementation for children with measles, particularly in areas of deficiency, as it reduces morbidity and mortality. Dosing is age-based and administered once daily for two days.
Disposition and follow-up
Hospital admission is indicated for patients with severe pneumonia, dehydration, encephalitis, SSPE, immunocompromise, or significant comorbidities. Patients are contagious from 4 days before symptom onset until 4 days after rash appearance; immunocompromised individuals may remain contagious longer. Discharge is appropriate for stable patients without complications, with clear instructions on isolation and follow-up.
Pearls and pitfalls
Measles is one of the most contagious infectious diseases, with significant morbidity and mortality despite modern care. Early recognition and respiratory isolation are critical in health care settings. Immunocompromised patients may not develop the classic rash, increasing the risk of missed diagnosis. Vaccination remains the most effective preventive measure.

- Published on
Emergency and Acute Medicine – Knee Injuries: ACL, PCL, MCL, and Meniscus
Basic Description
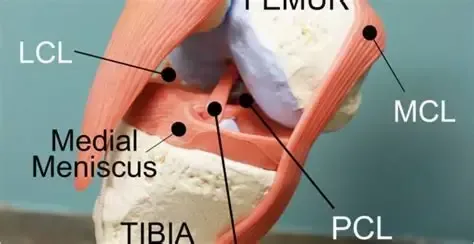
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
Basic Description
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
- Published on
Emergency and Acute Medicine – Isopropanol Poisoning
Basics Description
Isopropanol (isopropyl alcohol) is a potent central nervous system depressant, with effects that are two to three times stronger than ethanol. It is rapidly absorbed after oral ingestion and is metabolized by alcohol dehydrogenase to acetone, which itself is a CNS depressant. Unlike other toxic alcohols, isopropanol is ketogenic but does not usually cause significant metabolic acidosis. Concomitant ethanol ingestion prolongs the half-life of isopropanol but not acetone. Isopropanol has a half-life of approximately 3–16 hours, while acetone persists longer, with a half-life of 7.5–26 hours. Acetone is eliminated through the lungs and kidneys.
Etiology
Isopropanol is a clear, colorless, volatile liquid with a bitter taste and a faint odor of acetone. It is commonly available as a 70% rubbing alcohol solution, sometimes containing blue dye (“blue heaven”) to discourage abuse. It is found in many household and industrial products, including toiletries, disinfectants, window cleaners, paint removers, solvents, jewelry cleaners, detergents, antifreeze, and hand sanitizers. The typical adult patient is a chronic alcoholic who has depleted their ethanol supply and substitutes isopropanol. Systemic toxicity can also occur from dermal absorption or rectal administration.
Diagnosis: Signs and Symptoms
Symptoms usually develop within 30–60 minutes of ingestion. Neurologic manifestations include lethargy, weakness, headache, inebriation, vertigo, ataxia, apnea, and coma. Unlike ethanol, an initial excitation phase is typically absent. Gastrointestinal symptoms are common and include nausea, vomiting, abdominal pain, gastritis, and hematemesis. Cardiovascular findings may include hypotension, tachycardia, myocardial depression, and peripheral vasodilation. Pulmonary effects include respiratory depression and hemorrhagic tracheobronchitis. Dermatologic exposure can cause skin irritation or burns, and ocular exposure leads to irritation and lacrimation.
In children, accidental ingestions are common in those younger than 6 years, and rubbing alcohol sponge baths may cause inhalational toxicity. Pediatric patients are particularly prone to hypoglycemia.
Essential Workup
Diagnosis is supported by a history of ingestion and the presence of an acetone or isopropanol odor on the patient’s breath.
Diagnosis Tests and Interpretation
Laboratory evaluation should include electrolytes, BUN, creatinine, and glucose. Hypoglycemia may be present. Significant acidosis is uncommon unless there is associated hypoperfusion or a coingestant. Acetone can falsely elevate serum creatinine; when acetone levels exceed 40 mg/dL, creatinine may rise approximately 1 mg/dL for every 100 mg/dL of acetone, returning to baseline as acetone is cleared. CBC may show decreased hematocrit in cases of hemorrhagic gastritis. Arterial blood gas analysis typically shows little or no acidosis. Urinalysis and serum testing reveal ketosis.
Serum isopropanol levels correlate with severity, with coma often occurring at levels above 150 mg/dL. Serum osmolarity should be assessed, as an elevated osmolar gap (>10) is common. Each 5.9 mg/dL of isopropanol and 5.5 mg/dL of acetone increases the osmolar gap by approximately 1 mOsm/kg. Chest radiography is indicated if aspiration pneumonia is suspected, and head CT should be considered when altered mental status or head injury is possible.
Differential Diagnosis
The differential diagnosis for CNS depression with an elevated osmolar gap includes ethanol, ethylene glycol, methanol, glycerol, and mannitol.
Treatment Prehospital
All potentially ingested bottles and medications should be located and transported with the patient to the emergency department.
Initial Stabilization and Therapy
Management begins with airway, breathing, and circulation. Airway protection and ventilatory support may be required. Hypotension should initially be treated with IV 0.9% normal saline; vasopressors such as dopamine or norepinephrine may be required if hypotension persists. Patients with significant hemorrhagic gastritis may require packed red blood cell transfusion. Nasogastric tube placement and irrigation may be indicated for hematemesis. Naloxone, thiamine, and dextrose should be administered for altered mental status as indicated.
ED Treatment and Procedures
Treatment is primarily supportive, as there is no specific antidote. Skin and eye exposures should be treated with copious irrigation. Activated charcoal may be considered for coingestants and, in large doses, can adsorb some isopropanol. Ethanol infusion and fomepizole (4-methylpyrazole) are not indicated. Hemodialysis effectively removes both isopropanol and acetone but is rarely required. Indications for dialysis include persistent hemodynamic instability despite fluids and pressors or very high serum levels (>400 mg/dL), which are associated with severe hypotension and prolonged coma.
Medication
Supportive medications may include activated charcoal, IV dextrose for hypoglycemia, dopamine for refractory hypotension, naloxone if opioid exposure is suspected, and thiamine for patients at risk of deficiency.
Follow-Up Disposition
Patients with moderate to severe toxicity, including altered mental status or hypotension, should be admitted. Asymptomatic patients should be observed for 2–4 hours after ingestion before discharge. Mild intoxication that resolves within 4–6 hours may be safely discharged.
Follow-Up Recommendations
Patients with intentional ingestion should be referred for alcohol detoxification or psychiatric evaluation. Gastroenterology referral is recommended for those with recurrent hematemesis requiring endoscopic evaluation.
Pearls and Pitfalls
Supportive care is the cornerstone of treatment for isopropanol poisoning. Unlike other toxic alcohol ingestions, ethanol infusion and fomepizole should not be used.
Basics Description
Isopropanol (isopropyl alcohol) is a potent central nervous system depressant, with effects that are two to three times stronger than ethanol. It is rapidly absorbed after oral ingestion and is metabolized by alcohol dehydrogenase to acetone, which itself is a CNS depressant. Unlike other toxic alcohols, isopropanol is ketogenic but does not usually cause significant metabolic acidosis. Concomitant ethanol ingestion prolongs the half-life of isopropanol but not acetone. Isopropanol has a half-life of approximately 3–16 hours, while acetone persists longer, with a half-life of 7.5–26 hours. Acetone is eliminated through the lungs and kidneys.
Etiology
Isopropanol is a clear, colorless, volatile liquid with a bitter taste and a faint odor of acetone. It is commonly available as a 70% rubbing alcohol solution, sometimes containing blue dye (“blue heaven”) to discourage abuse. It is found in many household and industrial products, including toiletries, disinfectants, window cleaners, paint removers, solvents, jewelry cleaners, detergents, antifreeze, and hand sanitizers. The typical adult patient is a chronic alcoholic who has depleted their ethanol supply and substitutes isopropanol. Systemic toxicity can also occur from dermal absorption or rectal administration.
Diagnosis: Signs and Symptoms
Symptoms usually develop within 30–60 minutes of ingestion. Neurologic manifestations include lethargy, weakness, headache, inebriation, vertigo, ataxia, apnea, and coma. Unlike ethanol, an initial excitation phase is typically absent. Gastrointestinal symptoms are common and include nausea, vomiting, abdominal pain, gastritis, and hematemesis. Cardiovascular findings may include hypotension, tachycardia, myocardial depression, and peripheral vasodilation. Pulmonary effects include respiratory depression and hemorrhagic tracheobronchitis. Dermatologic exposure can cause skin irritation or burns, and ocular exposure leads to irritation and lacrimation.
In children, accidental ingestions are common in those younger than 6 years, and rubbing alcohol sponge baths may cause inhalational toxicity. Pediatric patients are particularly prone to hypoglycemia.
Essential Workup
Diagnosis is supported by a history of ingestion and the presence of an acetone or isopropanol odor on the patient’s breath.
Diagnosis Tests and Interpretation
Laboratory evaluation should include electrolytes, BUN, creatinine, and glucose. Hypoglycemia may be present. Significant acidosis is uncommon unless there is associated hypoperfusion or a coingestant. Acetone can falsely elevate serum creatinine; when acetone levels exceed 40 mg/dL, creatinine may rise approximately 1 mg/dL for every 100 mg/dL of acetone, returning to baseline as acetone is cleared. CBC may show decreased hematocrit in cases of hemorrhagic gastritis. Arterial blood gas analysis typically shows little or no acidosis. Urinalysis and serum testing reveal ketosis.
Serum isopropanol levels correlate with severity, with coma often occurring at levels above 150 mg/dL. Serum osmolarity should be assessed, as an elevated osmolar gap (>10) is common. Each 5.9 mg/dL of isopropanol and 5.5 mg/dL of acetone increases the osmolar gap by approximately 1 mOsm/kg. Chest radiography is indicated if aspiration pneumonia is suspected, and head CT should be considered when altered mental status or head injury is possible.
Differential Diagnosis
The differential diagnosis for CNS depression with an elevated osmolar gap includes ethanol, ethylene glycol, methanol, glycerol, and mannitol.
Treatment Prehospital
All potentially ingested bottles and medications should be located and transported with the patient to the emergency department.
Initial Stabilization and Therapy
Management begins with airway, breathing, and circulation. Airway protection and ventilatory support may be required. Hypotension should initially be treated with IV 0.9% normal saline; vasopressors such as dopamine or norepinephrine may be required if hypotension persists. Patients with significant hemorrhagic gastritis may require packed red blood cell transfusion. Nasogastric tube placement and irrigation may be indicated for hematemesis. Naloxone, thiamine, and dextrose should be administered for altered mental status as indicated.
ED Treatment and Procedures
Treatment is primarily supportive, as there is no specific antidote. Skin and eye exposures should be treated with copious irrigation. Activated charcoal may be considered for coingestants and, in large doses, can adsorb some isopropanol. Ethanol infusion and fomepizole (4-methylpyrazole) are not indicated. Hemodialysis effectively removes both isopropanol and acetone but is rarely required. Indications for dialysis include persistent hemodynamic instability despite fluids and pressors or very high serum levels (>400 mg/dL), which are associated with severe hypotension and prolonged coma.
Medication
Supportive medications may include activated charcoal, IV dextrose for hypoglycemia, dopamine for refractory hypotension, naloxone if opioid exposure is suspected, and thiamine for patients at risk of deficiency.
Follow-Up Disposition
Patients with moderate to severe toxicity, including altered mental status or hypotension, should be admitted. Asymptomatic patients should be observed for 2–4 hours after ingestion before discharge. Mild intoxication that resolves within 4–6 hours may be safely discharged.
Follow-Up Recommendations
Patients with intentional ingestion should be referred for alcohol detoxification or psychiatric evaluation. Gastroenterology referral is recommended for those with recurrent hematemesis requiring endoscopic evaluation.
Pearls and Pitfalls
Supportive care is the cornerstone of treatment for isopropanol poisoning. Unlike other toxic alcohol ingestions, ethanol infusion and fomepizole should not be used.

