- Published on
Emergency and Acute Medicine – Knee Injuries: ACL, PCL, MCL, and Meniscus
Basic Description
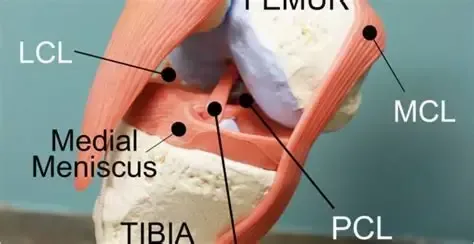
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
Basic Description
Knee ligament and meniscal injuries are common causes of acute knee pain and instability, particularly in athletes and patients involved in high-energy trauma. Cruciate ligament injuries involve the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), which provide primary anteroposterior and rotational stability to the knee. The ACL runs from the posteromedial aspect of the lateral femoral condyle to the interspinous area of the tibia and prevents excessive anterior tibial translation, internal rotation, and hyperextension. The PCL is thicker and stronger than the ACL and extends from the anterolateral aspect of the medial femoral condyle to the posterior tibia, limiting posterior tibial translation.
Meniscal injuries most commonly involve the medial meniscus, which is less mobile and more firmly attached to the joint capsule than the lateral meniscus. Tears occur due to compressive or rotational forces between the femur and tibia. Displaced meniscal fragments can cause a true locked knee with inability to extend. The medial collateral ligament (MCL) extends from the medial femoral condyle to the tibia distal to the joint and is frequently injured in association with other ligamentous injuries.
Epidemiology
ACL injuries are the most common ligamentous knee injury, with approximately 200,000 cases annually in the United States. Nearly two-thirds are noncontact injuries, and females have a threefold increased risk compared with males. About half of ACL injuries are associated with meniscal tears, and chondral or subchondral damage is common. Medial meniscus injuries are significantly more frequent than lateral meniscus injuries, although true mechanical locking occurs in only about 30% of cases.
Etiology
ACL injuries typically result from deceleration combined with rotation or hyperextension, often during sports such as football or skiing, using a plant-and-pivot or stop-and-jump mechanism. PCL injuries are classically caused by a “dashboard injury,” where a posterior force is applied to the proximal tibia with the knee flexed, or from a fall onto a flexed knee. Meniscal injuries usually occur with sudden twisting motions during squatting, pivoting, or kneeling, and are common in both athletes and certain occupations. MCL injuries most often result from valgus stress applied to a flexed knee, such as from a lateral blow or ski injury.
In children, the ACL is the most frequently injured knee ligament, while isolated MCL injuries are uncommon before closure of the growth plates.
Diagnosis: Signs and Symptoms
Patients with cruciate ligament injuries often report a popping sensation, tearing feeling, or the knee “giving way,” followed by immediate dysfunction. A large effusion developing within 2–3 hours suggests hemarthrosis, most commonly from ACL injury. MCL injuries cause medial knee pain and tenderness, sometimes more pronounced in partial tears. Meniscal injuries are characterized by joint-line pain, intermittent swelling, mechanical symptoms, and difficulty fully extending the knee; patients may still complete activity at the time of injury. Degenerative meniscal tears present more insidiously and are often associated with osteoarthritis.
Physical Examination
Examination should include assessment of weight-bearing ability, palpation of bony landmarks and joint lines, evaluation of range of motion, and identification of effusion or locking. Immediate effusion suggests significant intra-articular injury, whereas delayed swelling is more typical of MCL, PCL, or meniscal injuries. A thorough neurovascular exam is essential. Stress testing should always compare the injured knee to the uninjured side.
The Lachman test is the most reliable maneuver for ACL injury in the acute setting. Anterior and posterior drawer tests assess ACL and PCL integrity, respectively, while the quadriceps active test helps confirm PCL injury. Valgus and varus stress testing evaluate MCL and LCL stability. Meniscal tests such as McMurray and Apley are best performed once acute pain is controlled.
Diagnostic Testing and Imaging
Laboratory testing is rarely required unless infection or inflammatory disease is suspected. Plain radiographs are recommended in most acute knee injuries to exclude fractures, especially in suspected ACL injuries and in children, where growth plate or tibial spine fractures may occur. MRI is highly sensitive and specific for ligamentous and meniscal injuries but is rarely needed emergently. Ottawa knee rules guide imaging decisions in adults but do not apply to children.
Essential Workup
Key priorities include careful neurovascular assessment, exclusion of fracture or infection, evaluation for multidirectional instability, and focused ligament testing, particularly the Lachman test for suspected ACL injury.
Differential Diagnosis
Consider growth plate injuries, tibial plateau fractures, transient knee or patellar dislocation, referred hip pathology, septic arthritis, gout, osteoarthritis, and inflammatory arthritides.
Treatment and Initial Management
Initial management includes immobilization, ice, elevation, and analgesia, along with documentation of neurovascular status. In the emergency department, locked knees due to meniscal injury may sometimes be reduced with gentle traction and rotation. Arthrocentesis can relieve pain from large effusions. In the absence of fracture, treatment consists of rest, ice, compression, elevation, and weight bearing as tolerated, often with crutches. Knee immobilizers may be used for comfort, but early gentle motion is encouraged.
Disposition and Follow-Up
Most isolated ligament or meniscal injuries can be managed as outpatients. Admission is rarely required unless a knee dislocation or vascular injury is suspected. Orthopedic follow-up within 1–2 weeks is recommended for confirmed or suspected significant ligamentous injury, and re-examination within 48 hours is helpful when initial assessment is limited by pain or swelling.
Pearls and Pitfalls
Always perform and document a thorough neurovascular exam. Maintain a high index of suspicion for occult knee dislocation in patients with multidirectional instability or multiple ligament injuries. Do not miss fractures, septic joints, referred hip pathology, or vascular compromise.
- Published on
Emergency and Acute Medicine – Lead Poisoning
Basic description
Lead toxicity results from multiple mechanisms. Lead binds sulfhydryl groups, disrupting numerous enzymatic processes, and mimics calcium, interfering with calcium-dependent signaling pathways. High serum lead levels compromise the blood–brain barrier, allowing lead entry into the CNS and causing neurotoxicity. After absorption, up to 99% of lead binds to erythrocytes and is later redistributed into bone, where approximately 95% of total body lead resides in adults and 70% in children. Lead commonly coexists with iron deficiency, which increases gastrointestinal absorption. It also impairs heme synthesis, resulting in elevated free erythrocyte protoporphyrin that complexes with zinc, producing increased zinc protoporphyrin levels. Blood lead levels correlate poorly with symptoms but are associated with reduced IQ and increased behavioral problems.
Etiology
Acute lead toxicity most often results from inhalation of environmental sources or ingestion of lead-containing substances such as pottery glazes, folk remedies, cosmetics, jewelry, weights, home-distilled alcohol, or lead dust from ammunition. Chronic toxicity is usually occupational, particularly in battery manufacturing or recycling, bridge painting, construction, electronic waste recycling, firing ranges, mining, smelting, pottery work, and welding. Pediatric poisoning typically arises from home exposures, including lead-based paint ingestion or inhalation, contaminated water from old pipes, lead dust carried home on clothing, imported foods, and folk medicines.
Diagnosis: signs and symptoms
Neurologic manifestations include seizures, encephalopathy, learning disabilities, psychiatric disturbances, cerebral edema, and peripheral motor neuropathy such as wrist drop, which is classic but uncommon. Gastrointestinal findings include colicky abdominal pain (lead colic), ileus, nausea, vomiting, gingival Burton lines indicating lifetime burden, and occasionally hepatitis or pancreatitis. Cardiovascular effects include hypertension, often secondary to renal disease, as well as myocarditis and conduction abnormalities. Renal involvement presents as chronic renal insufficiency with prolonged exposure. Hematologic effects include anemia from impaired globin synthesis and shortened red blood cell lifespan. Musculoskeletal effects include metaphyseal “lead lines,” reflecting altered calcium deposition rather than lead itself, along with impaired bone growth and strength.
Essential workup
The cornerstone of diagnosis is measurement of a whole blood lead level (BLL). There is no normal BLL. In children, educational and environmental interventions begin at BLL ≥10 μg/dL, while chelation therapy is recommended at ≥45 μg/dL. In adults, chelation is usually considered at ≥70 μg/dL, with levels ≥100 μg/dL associated with severe encephalopathy.
Diagnostic tests and interpretation
Laboratory evaluation includes CBC to assess for anemia, RBC indices and iron studies, renal function tests, electrolytes, glucose, liver function tests prior to chelation, and FEP or ZPP levels. Imaging may include abdominal radiographs to detect radiopaque foreign bodies and long-bone radiographs in children to identify lead lines. Cranial CT and other imaging are guided by clinical status.
Differential diagnosis
Acute presentations may mimic appendicitis, gastroenteritis, colitis, cholera, distributive shock, encephalopathy, or other toxic ingestions. Chronic toxicity may resemble Addison disease, Guillain–Barré syndrome, vitamin deficiencies (B3, B6, B12), or Wernicke–Korsakoff syndrome.
Treatment: prehospital and initial stabilization
Management begins with airway, breathing, and circulation support, cardiac monitoring, and seizure control. Skin decontamination should be performed for dermal exposure when safe. Naloxone, thiamine, and dextrose are administered as indicated for altered mental status.
Emergency department management
Whole-bowel irrigation with polyethylene glycol is indicated if radiopaque material is seen on abdominal imaging; activated charcoal is ineffective. Decisions regarding chelation therapy depend on BLL, symptom severity, acuity of exposure, and consultation with a medical toxicologist or poison center. Adults with encephalopathy or BLL >100 μg/dL typically require chelation with dimercaprol followed by calcium disodium EDTA. Asymptomatic adults with BLL 70–100 μg/dL may be treated with oral succimer, while chelation is not indicated for asymptomatic adults with BLL <70 μg/dL. Children with BLL ≥45 μg/dL require chelation, with DMSA for asymptomatic cases and BAL plus CaNa₂EDTA for symptomatic or very high levels. Pregnant patients require multidisciplinary consultation.
Medications
Chelating agents include dimercaprol (BAL), calcium disodium EDTA, and succimer (DMSA). Supportive medications include benzodiazepines for seizures, dextrose for hypoglycemia, naloxone, and thiamine. BAL is contraindicated in patients with peanut allergy.
Disposition and follow-up
Admission is required for symptomatic patients, children at risk for re-exposure, those unable to tolerate oral chelation, and pregnant patients with elevated BLL. Asymptomatic patients not requiring IV chelation may be discharged once a safe environment is ensured and outpatient follow-up is arranged. Pediatric patients must demonstrate tolerance of oral chelation prior to discharge.
Pearls and pitfalls
Heel-stick testing may falsely elevate BLL and should be confirmed with venous sampling. Environmental assessment and social support are critical to prevent re-exposure. Family members and siblings should be screened when a patient is diagnosed with lead toxicity. Avoid BAL in patients with peanut allergy.
Basic description
Lead toxicity results from multiple mechanisms. Lead binds sulfhydryl groups, disrupting numerous enzymatic processes, and mimics calcium, interfering with calcium-dependent signaling pathways. High serum lead levels compromise the blood–brain barrier, allowing lead entry into the CNS and causing neurotoxicity. After absorption, up to 99% of lead binds to erythrocytes and is later redistributed into bone, where approximately 95% of total body lead resides in adults and 70% in children. Lead commonly coexists with iron deficiency, which increases gastrointestinal absorption. It also impairs heme synthesis, resulting in elevated free erythrocyte protoporphyrin that complexes with zinc, producing increased zinc protoporphyrin levels. Blood lead levels correlate poorly with symptoms but are associated with reduced IQ and increased behavioral problems.
Etiology
Acute lead toxicity most often results from inhalation of environmental sources or ingestion of lead-containing substances such as pottery glazes, folk remedies, cosmetics, jewelry, weights, home-distilled alcohol, or lead dust from ammunition. Chronic toxicity is usually occupational, particularly in battery manufacturing or recycling, bridge painting, construction, electronic waste recycling, firing ranges, mining, smelting, pottery work, and welding. Pediatric poisoning typically arises from home exposures, including lead-based paint ingestion or inhalation, contaminated water from old pipes, lead dust carried home on clothing, imported foods, and folk medicines.
Diagnosis: signs and symptoms
Neurologic manifestations include seizures, encephalopathy, learning disabilities, psychiatric disturbances, cerebral edema, and peripheral motor neuropathy such as wrist drop, which is classic but uncommon. Gastrointestinal findings include colicky abdominal pain (lead colic), ileus, nausea, vomiting, gingival Burton lines indicating lifetime burden, and occasionally hepatitis or pancreatitis. Cardiovascular effects include hypertension, often secondary to renal disease, as well as myocarditis and conduction abnormalities. Renal involvement presents as chronic renal insufficiency with prolonged exposure. Hematologic effects include anemia from impaired globin synthesis and shortened red blood cell lifespan. Musculoskeletal effects include metaphyseal “lead lines,” reflecting altered calcium deposition rather than lead itself, along with impaired bone growth and strength.
Essential workup
The cornerstone of diagnosis is measurement of a whole blood lead level (BLL). There is no normal BLL. In children, educational and environmental interventions begin at BLL ≥10 μg/dL, while chelation therapy is recommended at ≥45 μg/dL. In adults, chelation is usually considered at ≥70 μg/dL, with levels ≥100 μg/dL associated with severe encephalopathy.
Diagnostic tests and interpretation
Laboratory evaluation includes CBC to assess for anemia, RBC indices and iron studies, renal function tests, electrolytes, glucose, liver function tests prior to chelation, and FEP or ZPP levels. Imaging may include abdominal radiographs to detect radiopaque foreign bodies and long-bone radiographs in children to identify lead lines. Cranial CT and other imaging are guided by clinical status.
Differential diagnosis
Acute presentations may mimic appendicitis, gastroenteritis, colitis, cholera, distributive shock, encephalopathy, or other toxic ingestions. Chronic toxicity may resemble Addison disease, Guillain–Barré syndrome, vitamin deficiencies (B3, B6, B12), or Wernicke–Korsakoff syndrome.
Treatment: prehospital and initial stabilization
Management begins with airway, breathing, and circulation support, cardiac monitoring, and seizure control. Skin decontamination should be performed for dermal exposure when safe. Naloxone, thiamine, and dextrose are administered as indicated for altered mental status.
Emergency department management
Whole-bowel irrigation with polyethylene glycol is indicated if radiopaque material is seen on abdominal imaging; activated charcoal is ineffective. Decisions regarding chelation therapy depend on BLL, symptom severity, acuity of exposure, and consultation with a medical toxicologist or poison center. Adults with encephalopathy or BLL >100 μg/dL typically require chelation with dimercaprol followed by calcium disodium EDTA. Asymptomatic adults with BLL 70–100 μg/dL may be treated with oral succimer, while chelation is not indicated for asymptomatic adults with BLL <70 μg/dL. Children with BLL ≥45 μg/dL require chelation, with DMSA for asymptomatic cases and BAL plus CaNa₂EDTA for symptomatic or very high levels. Pregnant patients require multidisciplinary consultation.
Medications
Chelating agents include dimercaprol (BAL), calcium disodium EDTA, and succimer (DMSA). Supportive medications include benzodiazepines for seizures, dextrose for hypoglycemia, naloxone, and thiamine. BAL is contraindicated in patients with peanut allergy.
Disposition and follow-up
Admission is required for symptomatic patients, children at risk for re-exposure, those unable to tolerate oral chelation, and pregnant patients with elevated BLL. Asymptomatic patients not requiring IV chelation may be discharged once a safe environment is ensured and outpatient follow-up is arranged. Pediatric patients must demonstrate tolerance of oral chelation prior to discharge.
Pearls and pitfalls
Heel-stick testing may falsely elevate BLL and should be confirmed with venous sampling. Environmental assessment and social support are critical to prevent re-exposure. Family members and siblings should be screened when a patient is diagnosed with lead toxicity. Avoid BAL in patients with peanut allergy.

- Published on
Emergency and Acute Medicine – Labor
Basic description
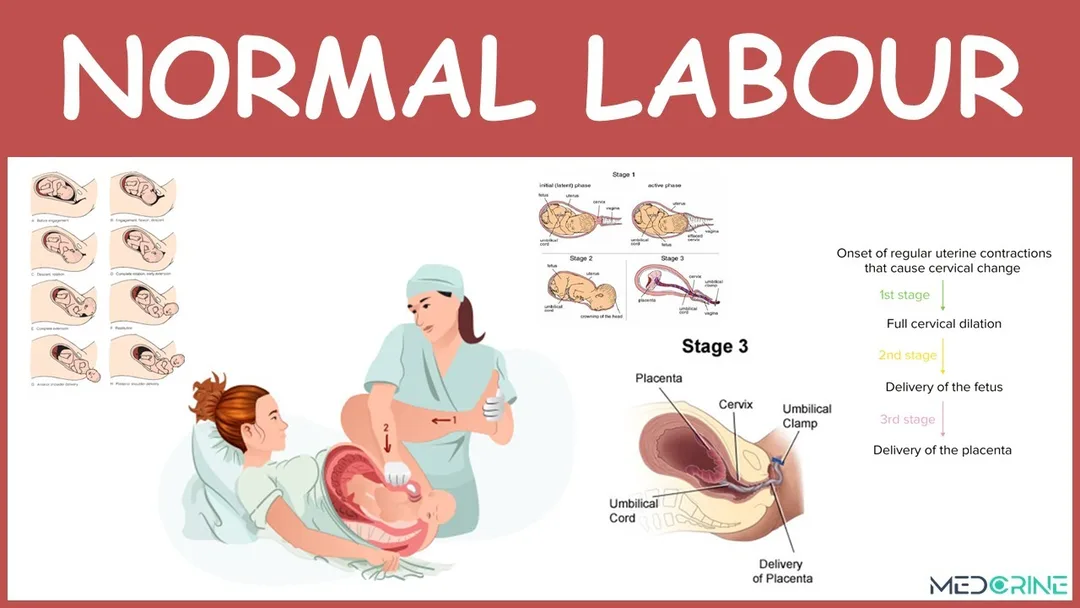
Labor is the sequence of physiologic processes that results in transport of the fetus from the uterus through the birth canal. It is characterized by synchronous, coordinated uterine contractions that progressively increase in strength, duration, and frequency, leading to cervical effacement, dilation, and eventual delivery of the fetus and placenta.
Physiology and stages of labor
Labor produces cervical changes that allow passage of the fetus through the birth canal and is divided into three stages. Stage one extends from the onset of regular uterine contractions to complete cervical dilation and is subdivided into latent and active phases. During the latent phase, contractions are mild, irregular, and short, usually lasting less than 45 seconds, with minimal cervical change. The active phase typically begins at 3–4 cm dilation, with strong, regular contractions occurring every 2–3 minutes and lasting longer than 45 seconds. Stage two spans from complete cervical dilation to delivery of the infant. Stage three begins after delivery of the infant and ends with placental delivery.
The total duration of labor varies among patients. Nulliparous patients generally have longer labor, with an average first stage of 14.4 hours and a second stage of 1 hour. Parous patients have shorter labors, with an average first stage of 7.7 hours and a second stage of 0.2 hours. Progression of the second stage is influenced by the “three Ps”: passenger (fetal size and presentation), passageway (pelvic anatomy and soft tissues), and powers (uterine contractions). Abnormalities in any of these factors may lead to dysfunctional labor.
False labor, or Braxton Hicks contractions, consists of irregular, nonsynchronous uterine contractions occurring days to weeks before true labor and does not result in cervical dilation.
Etiology
Preterm labor occurs in approximately 8–10% of pregnancies. Uterine, cervical, or urinary tract infections account for 30–40% of cases. Premature rupture of membranes, defined as rupture of membranes at least two hours before labor onset in patients under 37 weeks’ gestation, occurs in about 3% of pregnancies but accounts for 30–40% of premature births.
Diagnosis: signs and symptoms
True labor presents with regular uterine contractions occurring at least every five minutes, lasting 30–60 seconds, and associated with progressive cervical dilation or effacement. Pain is typically intermittent, located in the lower abdomen, and may radiate to the lower back. Preterm labor produces these changes before 37 weeks’ gestation. Labor is not associated with vaginal bleeding, and bleeding in the third trimester should prompt concern for placental abruption or placenta previa. Sudden release of clear vaginal fluid or persistent perineal wetness suggests rupture of membranes, which may precede labor.
History and physical examination
Assessment should include gestational age, adequacy of prenatal care, prior obstetric history including cesarean delivery, and recent infections. Fundal height should be measured and correlated with gestational age, particularly when dates are uncertain. A sterile pelvic examination is required to assess cervical dilation and effacement, but digital examination is contraindicated in patients with vaginal bleeding until placental location is confirmed.
Essential workup
Patients with suspected labor require immediate sterile pelvic examination to evaluate cervical status and determine the likelihood of imminent delivery. Suspected rupture of membranes should be evaluated with sterile speculum examination for pooling, ferning, and nitrazine testing. Patients with preterm labor and cervical changes require urinalysis with culture and cervical cultures. Continuous fetal monitoring should be initiated when available. Digital or bimanual pelvic examination should be avoided in third-trimester bleeding until ultrasound excludes placenta previa or abruption.
Diagnostic tests and interpretation
If labor is confirmed, obtain a complete blood count and type and screen. Urinalysis should assess for proteinuria. Patients without prenatal care require Rh factor and antibody screening. Imaging is not routinely required, but emergent ultrasound is indicated in third-trimester patients with abdominal pain and vaginal bleeding to evaluate for placental pathology.
Differential diagnosis
False labor presents with irregular contractions without cervical change. Other considerations include round ligament pain, musculoskeletal back pain, appendicitis, ovarian cysts, diverticulitis, nephrolithiasis, and urinary tract infection.
Treatment and initial management
Prehospital management includes oxygen administration and left lateral positioning to optimize uteroplacental perfusion. Transport of high-risk obstetric patients prior to delivery improves outcomes compared with neonatal transfer after birth. If delivery is imminent, prepare for immediate vaginal delivery in the emergency department. Otherwise, patients should be transferred promptly to the labor and delivery unit.
If transfer is delayed or preterm labor is suspected, initiate maternal and fetal monitoring, provide intravenous hydration, and consider antibiotics for unknown group B Streptococcus status. Tocolysis with agents such as magnesium sulfate or terbutaline may be initiated for preterm labor when appropriate, with careful monitoring for toxicity.
Disposition
All patients in true labor should be admitted to labor and delivery. Preterm labor requires immediate obstetric consultation and admission. Patients with false labor may be discharged only after obstetric evaluation, confirmation of fetal well-being, and arrangement of close follow-up.
Pearls and pitfalls
Vaginal bleeding in labor requires urgent evaluation for placental abruption or previa, and digital pelvic examination must be avoided in these cases. Pelvic examinations in labor should always be sterile. False labor can progress to true labor and requires appropriate counseling and follow-up.
Basic description
Labor is the sequence of physiologic processes that results in transport of the fetus from the uterus through the birth canal. It is characterized by synchronous, coordinated uterine contractions that progressively increase in strength, duration, and frequency, leading to cervical effacement, dilation, and eventual delivery of the fetus and placenta.
Physiology and stages of labor
Labor produces cervical changes that allow passage of the fetus through the birth canal and is divided into three stages. Stage one extends from the onset of regular uterine contractions to complete cervical dilation and is subdivided into latent and active phases. During the latent phase, contractions are mild, irregular, and short, usually lasting less than 45 seconds, with minimal cervical change. The active phase typically begins at 3–4 cm dilation, with strong, regular contractions occurring every 2–3 minutes and lasting longer than 45 seconds. Stage two spans from complete cervical dilation to delivery of the infant. Stage three begins after delivery of the infant and ends with placental delivery.
The total duration of labor varies among patients. Nulliparous patients generally have longer labor, with an average first stage of 14.4 hours and a second stage of 1 hour. Parous patients have shorter labors, with an average first stage of 7.7 hours and a second stage of 0.2 hours. Progression of the second stage is influenced by the “three Ps”: passenger (fetal size and presentation), passageway (pelvic anatomy and soft tissues), and powers (uterine contractions). Abnormalities in any of these factors may lead to dysfunctional labor.
False labor, or Braxton Hicks contractions, consists of irregular, nonsynchronous uterine contractions occurring days to weeks before true labor and does not result in cervical dilation.
Etiology
Preterm labor occurs in approximately 8–10% of pregnancies. Uterine, cervical, or urinary tract infections account for 30–40% of cases. Premature rupture of membranes, defined as rupture of membranes at least two hours before labor onset in patients under 37 weeks’ gestation, occurs in about 3% of pregnancies but accounts for 30–40% of premature births.
Diagnosis: signs and symptoms
True labor presents with regular uterine contractions occurring at least every five minutes, lasting 30–60 seconds, and associated with progressive cervical dilation or effacement. Pain is typically intermittent, located in the lower abdomen, and may radiate to the lower back. Preterm labor produces these changes before 37 weeks’ gestation. Labor is not associated with vaginal bleeding, and bleeding in the third trimester should prompt concern for placental abruption or placenta previa. Sudden release of clear vaginal fluid or persistent perineal wetness suggests rupture of membranes, which may precede labor.
History and physical examination
Assessment should include gestational age, adequacy of prenatal care, prior obstetric history including cesarean delivery, and recent infections. Fundal height should be measured and correlated with gestational age, particularly when dates are uncertain. A sterile pelvic examination is required to assess cervical dilation and effacement, but digital examination is contraindicated in patients with vaginal bleeding until placental location is confirmed.
Essential workup
Patients with suspected labor require immediate sterile pelvic examination to evaluate cervical status and determine the likelihood of imminent delivery. Suspected rupture of membranes should be evaluated with sterile speculum examination for pooling, ferning, and nitrazine testing. Patients with preterm labor and cervical changes require urinalysis with culture and cervical cultures. Continuous fetal monitoring should be initiated when available. Digital or bimanual pelvic examination should be avoided in third-trimester bleeding until ultrasound excludes placenta previa or abruption.
Diagnostic tests and interpretation
If labor is confirmed, obtain a complete blood count and type and screen. Urinalysis should assess for proteinuria. Patients without prenatal care require Rh factor and antibody screening. Imaging is not routinely required, but emergent ultrasound is indicated in third-trimester patients with abdominal pain and vaginal bleeding to evaluate for placental pathology.
Differential diagnosis
False labor presents with irregular contractions without cervical change. Other considerations include round ligament pain, musculoskeletal back pain, appendicitis, ovarian cysts, diverticulitis, nephrolithiasis, and urinary tract infection.
Treatment and initial management
Prehospital management includes oxygen administration and left lateral positioning to optimize uteroplacental perfusion. Transport of high-risk obstetric patients prior to delivery improves outcomes compared with neonatal transfer after birth. If delivery is imminent, prepare for immediate vaginal delivery in the emergency department. Otherwise, patients should be transferred promptly to the labor and delivery unit.
If transfer is delayed or preterm labor is suspected, initiate maternal and fetal monitoring, provide intravenous hydration, and consider antibiotics for unknown group B Streptococcus status. Tocolysis with agents such as magnesium sulfate or terbutaline may be initiated for preterm labor when appropriate, with careful monitoring for toxicity.
Disposition
All patients in true labor should be admitted to labor and delivery. Preterm labor requires immediate obstetric consultation and admission. Patients with false labor may be discharged only after obstetric evaluation, confirmation of fetal well-being, and arrangement of close follow-up.
Pearls and pitfalls
Vaginal bleeding in labor requires urgent evaluation for placental abruption or previa, and digital pelvic examination must be avoided in these cases. Pelvic examinations in labor should always be sterile. False labor can progress to true labor and requires appropriate counseling and follow-up.
- Published on
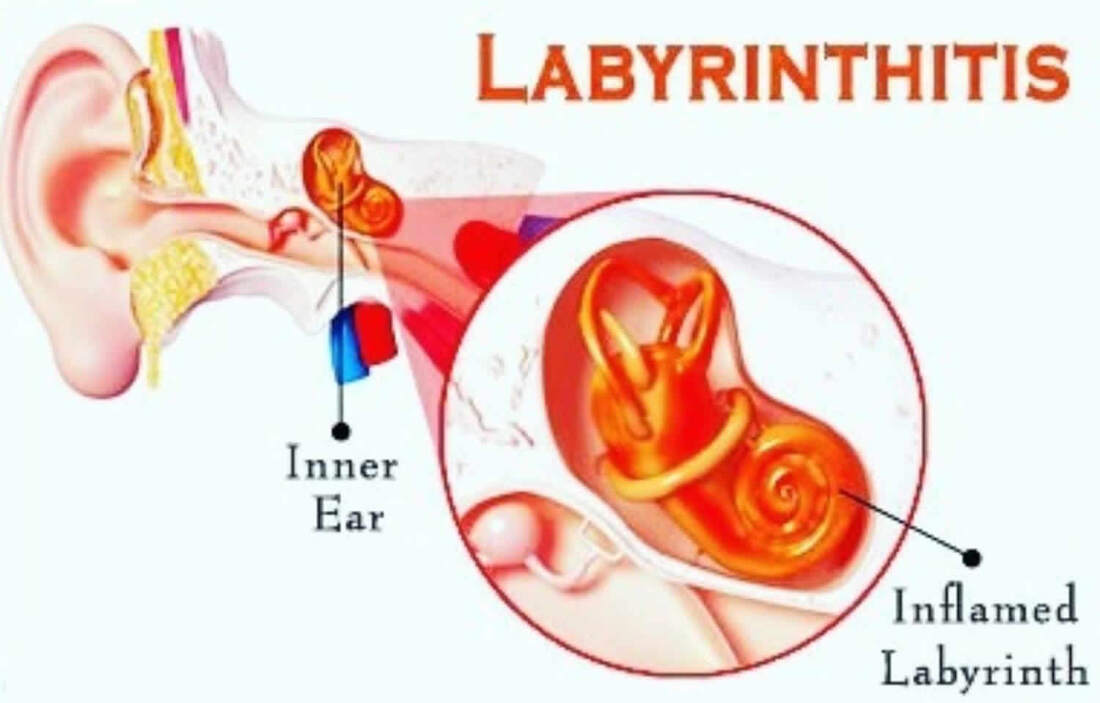
Emergency and Acute Medicine – Labyrinthitis
Basic description
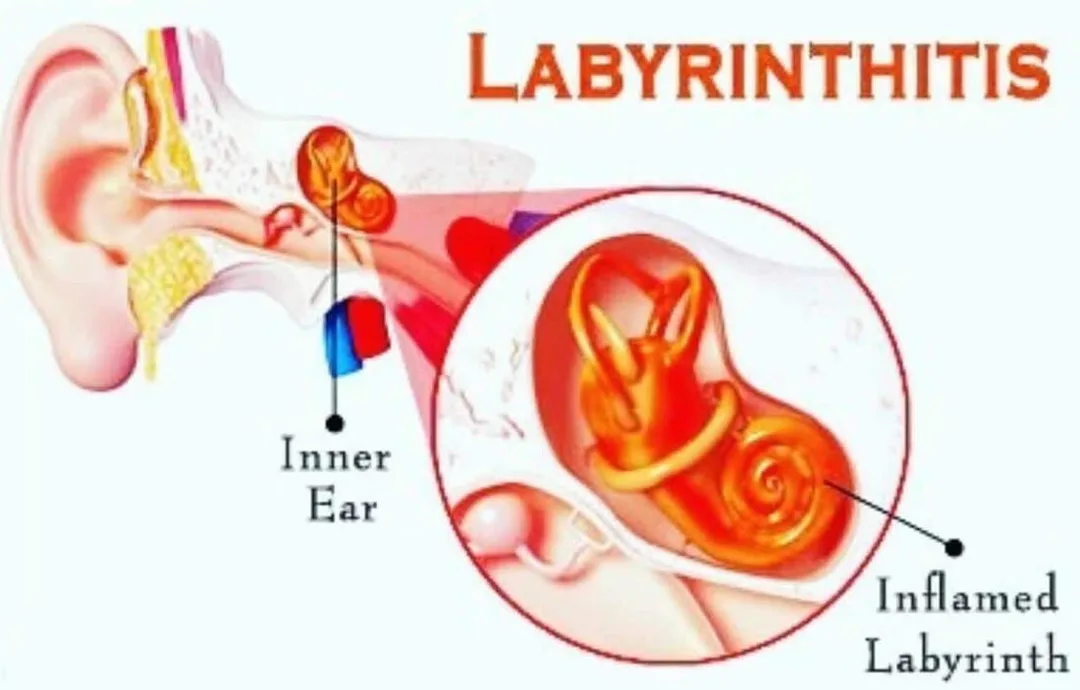
Labyrinthitis is an inflammatory disorder of the inner ear that results in unilateral vestibular dysfunction. Inflammation decreases afferent firing from the affected labyrinth, which the central nervous system interprets as head rotation away from the diseased side. This imbalance produces spontaneous nystagmus with the fast phase directed away from the pathologic ear. Labyrinthitis typically causes vertigo and balance disturbance and may be associated with hearing loss and tinnitus. Peak onset is between 30 and 60 years of age, and approximately half of patients report a recent upper respiratory tract infection. Symptoms are often worsened by head movement but may persist at rest, with gradual recovery over weeks to months.
Etiology
The three most common causes of peripheral vertigo are benign paroxysmal positional vertigo (BPPV), Ménière disease, and labyrinthitis. Labyrinthitis may be serous (viral or bacterial), suppurative (bacterial), autoimmune (e.g., Wegener granulomatosis or polyarteritis nodosa), vascular ischemic, traumatic, or medication-related. Ototoxic agents include aminoglycosides, loop diuretics, and antiepileptics such as phenytoin. Allergies and chronic BPPV may also contribute. Chronic BPPV may result from idiopathic otoconia dislodgement, post-traumatic causes, sequelae of labyrinthitis, or ischemic injury.
Pediatric considerations
In children, suppurative and serous labyrinthitis are usually secondary to acute otitis media, mastoiditis, or meningitis. BPPV may occur between 1 and 5 years of age, presenting with abrupt crying, nystagmus, diaphoresis, emesis, and ataxia, with recurrences for up to three years. Migraine–BPPV complex is the most common cause of pediatric vertigo. Ménière disease is rare before 10 years of age.
Diagnosis: signs and symptoms
Patients typically present with sudden-onset peripheral vertigo that is positional or movement-associated and described as a spinning sensation or imbalance. Nausea and vomiting are common. Hearing impairment may be unilateral or bilateral and range from mild to profound. Tinnitus suggests Ménière disease, while otorrhea or otalgia raises concern for otitis media, tympanic membrane perforation, mastoiditis, or cholesteatoma. Symptoms often follow recent infections or sick contacts. Risk factors include prior ear surgery, diabetes mellitus, stroke, migraine, and trauma.
Physical examination
A complete head and neck examination is essential. The external ear, ear canal, tympanic membrane, and middle ear should be inspected for erythema, swelling, vesicles, effusion, perforation, or cholesteatoma. Mastoid tenderness suggests mastoiditis. Ocular examination assesses extraocular movements, pupils, and fundi for papilledema. Nystagmus is typically horizontal with a rotational component, constant in direction, augmented by head movement, fatigable, and suppressed by fixation. A full neurologic and cardiac examination is required to exclude central causes, including assessment of cranial nerves, cerebellar function, gait, orthostatic vitals, and vascular bruits. Facial weakness may suggest Ramsay Hunt syndrome or stroke, while neck stiffness suggests meningitis.
Caloric testing may demonstrate partial or complete loss of response in the affected ear, but should only be performed after confirming an intact tympanic membrane. The Dix–Hallpike maneuver is used to evaluate for BPPV.
Essential workup
The priority is exclusion of central vertigo and serious underlying conditions. A careful neurologic examination is mandatory. Clinicians should evaluate for associated infections such as acute otitis media, meningitis, mastoiditis, and Ramsay Hunt syndrome. Orthostatic vitals and basic auditory assessment are recommended.
Diagnostic tests and interpretation
Laboratory testing is generally unnecessary unless evaluating for central vertigo or unusual peripheral causes. Basic labs, including electrolytes and glucose, may be obtained in patients with significant vomiting or dehydration. Lumbar puncture is indicated when meningitis or subarachnoid hemorrhage is suspected. Imaging is warranted when features suggest central vertigo, such as nonpositional symptoms, vertical or direction-changing nystagmus, nonfatigable nystagmus, focal neurologic deficits, or high cardiovascular risk. MRI with MRA of the posterior fossa and vertebrobasilar circulation is preferred, while CT may be used acutely to evaluate for hemorrhage. Brain imaging should be strongly considered in patients over 45 years of age, children, and those with vascular risk factors.
Differential diagnosis
Peripheral causes include vestibular neuritis, otitis media, acoustic neuroma, autoimmune inner ear disease, BPPV, cholesteatoma, Ménière disease, otosyphilis, ototoxic medications, herpes zoster oticus (Ramsay Hunt syndrome), perilymphatic fistula, post-traumatic vestibular concussion, suppurative labyrinthitis, and temporal bone fracture. Central causes include brainstem or cerebellar ischemia or hemorrhage, tumors, Chiari malformation, multiple sclerosis, vestibular migraine, Wallenberg syndrome, seizures, arrhythmias, hypoglycemia, hypotension, cervicogenic vertigo, hypothyroidism, and alcohol or drug intoxication.
Treatment
Prehospital care includes cardiac monitoring, finger-stick glucose assessment, evaluation for acute stroke, antiemetics, intravenous fluids for dehydration, and fall precautions. Initial ED management focuses on bed rest, hydration, and prevention of falls. Medications provide symptomatic relief but should be limited to short-term use, generally no more than 48 hours, to promote vestibular compensation. Vestibular suppressants such as meclizine, diazepam, or scopolamine and antiemetics such as ondansetron, prochlorperazine, or promethazine may be used. Corticosteroids have limited evidence of benefit. Canalith repositioning maneuvers, particularly the Epley maneuver, are the primary treatment for BPPV and provide relief in most patients. Surgery is reserved for refractory cases.
Disposition and follow-up
Admission is indicated for patients with concern for stroke or central causes, intractable nausea and vomiting, severe dehydration, or unsteady gait. Patients may be discharged if they can tolerate oral intake, ambulate safely, and have a normal neurologic examination, with counseling to avoid driving, heights, and hazardous activities. Neurology or otolaryngology referral is recommended for recurrent or persistent symptoms. Vestibular rehabilitation is beneficial for chronic symptoms.
Pearls and pitfalls
Always exclude life-threatening conditions such as meningitis, cerebrovascular ischemia, or intracranial tumors. Counsel patients regarding fall risk and occupational hazards. Use caution with positional maneuvers, as aggressive cervical hyperextension may precipitate vertebral artery dissection.
Basic description
Labyrinthitis is an inflammatory disorder of the inner ear that results in unilateral vestibular dysfunction. Inflammation decreases afferent firing from the affected labyrinth, which the central nervous system interprets as head rotation away from the diseased side. This imbalance produces spontaneous nystagmus with the fast phase directed away from the pathologic ear. Labyrinthitis typically causes vertigo and balance disturbance and may be associated with hearing loss and tinnitus. Peak onset is between 30 and 60 years of age, and approximately half of patients report a recent upper respiratory tract infection. Symptoms are often worsened by head movement but may persist at rest, with gradual recovery over weeks to months.
Etiology
The three most common causes of peripheral vertigo are benign paroxysmal positional vertigo (BPPV), Ménière disease, and labyrinthitis. Labyrinthitis may be serous (viral or bacterial), suppurative (bacterial), autoimmune (e.g., Wegener granulomatosis or polyarteritis nodosa), vascular ischemic, traumatic, or medication-related. Ototoxic agents include aminoglycosides, loop diuretics, and antiepileptics such as phenytoin. Allergies and chronic BPPV may also contribute. Chronic BPPV may result from idiopathic otoconia dislodgement, post-traumatic causes, sequelae of labyrinthitis, or ischemic injury.
Pediatric considerations
In children, suppurative and serous labyrinthitis are usually secondary to acute otitis media, mastoiditis, or meningitis. BPPV may occur between 1 and 5 years of age, presenting with abrupt crying, nystagmus, diaphoresis, emesis, and ataxia, with recurrences for up to three years. Migraine–BPPV complex is the most common cause of pediatric vertigo. Ménière disease is rare before 10 years of age.
Diagnosis: signs and symptoms
Patients typically present with sudden-onset peripheral vertigo that is positional or movement-associated and described as a spinning sensation or imbalance. Nausea and vomiting are common. Hearing impairment may be unilateral or bilateral and range from mild to profound. Tinnitus suggests Ménière disease, while otorrhea or otalgia raises concern for otitis media, tympanic membrane perforation, mastoiditis, or cholesteatoma. Symptoms often follow recent infections or sick contacts. Risk factors include prior ear surgery, diabetes mellitus, stroke, migraine, and trauma.
Physical examination
A complete head and neck examination is essential. The external ear, ear canal, tympanic membrane, and middle ear should be inspected for erythema, swelling, vesicles, effusion, perforation, or cholesteatoma. Mastoid tenderness suggests mastoiditis. Ocular examination assesses extraocular movements, pupils, and fundi for papilledema. Nystagmus is typically horizontal with a rotational component, constant in direction, augmented by head movement, fatigable, and suppressed by fixation. A full neurologic and cardiac examination is required to exclude central causes, including assessment of cranial nerves, cerebellar function, gait, orthostatic vitals, and vascular bruits. Facial weakness may suggest Ramsay Hunt syndrome or stroke, while neck stiffness suggests meningitis.
Caloric testing may demonstrate partial or complete loss of response in the affected ear, but should only be performed after confirming an intact tympanic membrane. The Dix–Hallpike maneuver is used to evaluate for BPPV.
Essential workup
The priority is exclusion of central vertigo and serious underlying conditions. A careful neurologic examination is mandatory. Clinicians should evaluate for associated infections such as acute otitis media, meningitis, mastoiditis, and Ramsay Hunt syndrome. Orthostatic vitals and basic auditory assessment are recommended.
Diagnostic tests and interpretation
Laboratory testing is generally unnecessary unless evaluating for central vertigo or unusual peripheral causes. Basic labs, including electrolytes and glucose, may be obtained in patients with significant vomiting or dehydration. Lumbar puncture is indicated when meningitis or subarachnoid hemorrhage is suspected. Imaging is warranted when features suggest central vertigo, such as nonpositional symptoms, vertical or direction-changing nystagmus, nonfatigable nystagmus, focal neurologic deficits, or high cardiovascular risk. MRI with MRA of the posterior fossa and vertebrobasilar circulation is preferred, while CT may be used acutely to evaluate for hemorrhage. Brain imaging should be strongly considered in patients over 45 years of age, children, and those with vascular risk factors.
Differential diagnosis
Peripheral causes include vestibular neuritis, otitis media, acoustic neuroma, autoimmune inner ear disease, BPPV, cholesteatoma, Ménière disease, otosyphilis, ototoxic medications, herpes zoster oticus (Ramsay Hunt syndrome), perilymphatic fistula, post-traumatic vestibular concussion, suppurative labyrinthitis, and temporal bone fracture. Central causes include brainstem or cerebellar ischemia or hemorrhage, tumors, Chiari malformation, multiple sclerosis, vestibular migraine, Wallenberg syndrome, seizures, arrhythmias, hypoglycemia, hypotension, cervicogenic vertigo, hypothyroidism, and alcohol or drug intoxication.
Treatment
Prehospital care includes cardiac monitoring, finger-stick glucose assessment, evaluation for acute stroke, antiemetics, intravenous fluids for dehydration, and fall precautions. Initial ED management focuses on bed rest, hydration, and prevention of falls. Medications provide symptomatic relief but should be limited to short-term use, generally no more than 48 hours, to promote vestibular compensation. Vestibular suppressants such as meclizine, diazepam, or scopolamine and antiemetics such as ondansetron, prochlorperazine, or promethazine may be used. Corticosteroids have limited evidence of benefit. Canalith repositioning maneuvers, particularly the Epley maneuver, are the primary treatment for BPPV and provide relief in most patients. Surgery is reserved for refractory cases.
Disposition and follow-up
Admission is indicated for patients with concern for stroke or central causes, intractable nausea and vomiting, severe dehydration, or unsteady gait. Patients may be discharged if they can tolerate oral intake, ambulate safely, and have a normal neurologic examination, with counseling to avoid driving, heights, and hazardous activities. Neurology or otolaryngology referral is recommended for recurrent or persistent symptoms. Vestibular rehabilitation is beneficial for chronic symptoms.
Pearls and pitfalls
Always exclude life-threatening conditions such as meningitis, cerebrovascular ischemia, or intracranial tumors. Counsel patients regarding fall risk and occupational hazards. Use caution with positional maneuvers, as aggressive cervical hyperextension may precipitate vertebral artery dissection.
- Published on
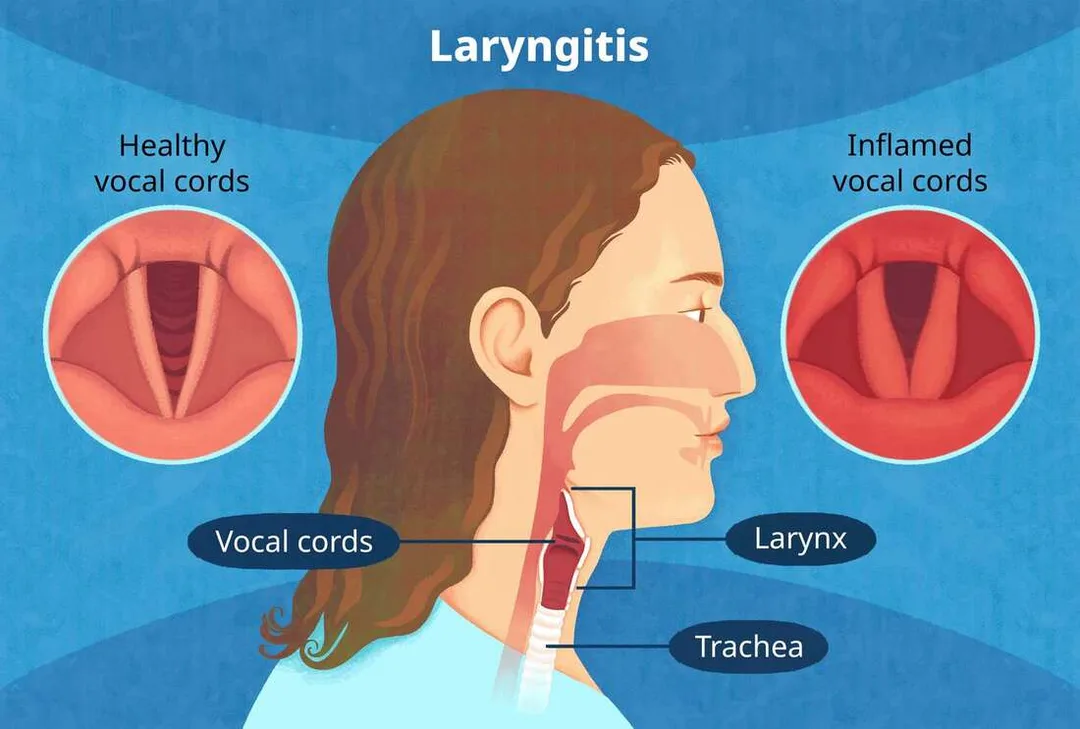
Emergency and Acute Medicine – Laryngitis
Basic description
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
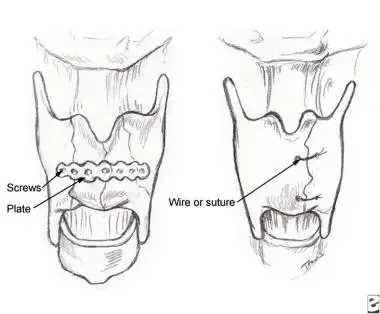
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
Basic description
Laryngitis is inflammation of the laryngeal mucosa, most commonly caused by viral upper respiratory infection. Incidence peaks in late fall, winter, and early spring and parallels viral epidemics. Inflammation reduces normal vocal cord vibration, resulting in hoarseness and voice changes.
Etiology
Acute laryngitis is most often viral, including influenza A and B, parainfluenza, adenovirus, coronavirus, coxsackievirus, respiratory syncytial virus, measles, and rhinovirus. Bacterial causes are uncommon but include β-hemolytic streptococcus, Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Bordetella pertussis, diphtheria, tuberculosis, syphilis, and leprosy. Noninfectious causes include laryngopharyngeal reflux related to GERD, fungal infection (often with inhaled steroid use or immunocompromise), allergy, voice abuse, inhalation or ingestion of irritants or caustics, autoimmune disease, trauma, and idiopathic causes. In children, acute spasmodic laryngitis (spasmodic croup) is more often infectious, and foreign body must be considered in unimmunized patients.
Diagnosis: signs and symptoms
Patients typically present with hoarseness or abnormal voice quality, throat irritation or rawness, throat swelling, frequent throat clearing, cough, malaise, fever, and occasionally dysphagia. Physical examination may reveal hoarse voice, pharyngeal erythema or edema, regional lymphadenopathy, stridor in infants, or asymmetric breath sounds if a foreign body is present.
Essential workup
Acute laryngitis is usually a clinical diagnosis based on history and throat inspection and typically resolves within 7–10 days. Increased suspicion for epiglottitis is required in unimmunized patients or those with respiratory distress. Chronic laryngitis lasting longer than 3 weeks warrants evaluation for GERD, chronic infection, neurologic disorders, or malignancy, with referral for laryngeal visualization by otolaryngology.
Diagnostic tests and interpretation
Laboratory studies are generally unnecessary, as leukocytosis does not reliably distinguish viral from bacterial disease. Throat cultures are reserved for cases with exam findings suggestive of bacterial infection. Imaging is rarely required; fiberoptic laryngoscopy is preferred when visualization is necessary. Soft-tissue neck radiographs are reserved for suspected epiglottitis or foreign body when laryngoscopy is unavailable and the patient is stable.
Differential diagnosis
Asthma, epiglottitis, GERD, vocal cord nodules, laryngeal or thyroid malignancy, croup or laryngotracheobronchitis, and foreign-body aspiration should be considered.
Treatment: prehospital care
Supportive care is usually sufficient. Stridor suggests potential airway obstruction, particularly in children, and warrants urgent evaluation. Neck trauma–associated laryngitis requires otolaryngology assessment. Caustic ingestion raises concern for esophageal injury. Suspected epiglottitis requires transport in the upright position with supplemental oxygen and avoidance of unnecessary airway manipulation.
Initial stabilization and therapy
Stabilization is required only for patients with respiratory distress. Management should follow epiglottitis protocols, including supplemental oxygen and preparation for advanced airway management in a controlled setting.
Emergency department treatment and procedures
Management is primarily supportive. Antibiotics are not recommended for routine adult acute laryngitis, as evidence shows no benefit over placebo. Vocal rest is essential, avoiding whispering; patients should use a soft, relaxed voice if speaking is necessary. Humidified air, increased oral fluids, analgesics, and smoking cessation are recommended. Symptoms typically resolve within 7–10 days if viral. Inhaled steroids are controversial and not standard therapy.
Medications
Treatment is cause-specific. Acetaminophen or NSAIDs may be used for pain and fever. Guaifenesin may help if associated with upper respiratory infection. Proton pump inhibitors are indicated for GERD-related laryngitis. Antifungal therapy is used for candidal infection. For croup, a single dose of dexamethasone is indicated. Antibiotics are reserved for confirmed bacterial infection or high-risk patients.
Follow-up and disposition
Admission is required for tuberculous laryngitis, respiratory distress, suspected epiglottitis, neck trauma, anaphylaxis, or airway compromise. Most patients with uncomplicated laryngitis can be discharged if breathing is normal and hydration is adequate. Chronic or nonresolving symptoms require otolaryngology referral.
Pearls and pitfalls
Most acute laryngitis is viral, and antibiotics provide no benefit. Always consider life-threatening causes of altered voice such as epiglottitis. Laryngitis without upper respiratory symptoms may indicate GERD. Persistent hoarseness beyond 3 weeks warrants evaluation to exclude malignancy.
- Published on
Emergency and Acute Medicine – Leukocytosis
Basic description
Leukocytosis is defined as any elevation in the total number of white blood cells (WBCs) above the expected normal range. Normal WBC values vary by age and physiologic state. In adults, the typical range is 4,500–11,000/mm³. In children, WBC counts are higher in infancy and gradually decrease with age. During pregnancy, normal ranges shift upward across all trimesters. Exercise, female gender, smoking, and daytime hours can also transiently increase WBC counts, making clinical context essential when interpreting results.
Patterns of leukocytosis
Leukocytosis can be further characterized by the predominant cell type. Neutrophilia is defined as an absolute neutrophil count greater than 7,500/mm³ and is the most common pattern. About half of circulating neutrophils are marginated along vessel walls and can rapidly demarginate in response to acute stress, potentially doubling the WBC count. Bone marrow stores of mature and immature neutrophils may also be released during infection or inflammation, producing a “left shift.”
Lymphocytosis is defined as an absolute lymphocyte count greater than 4,000/mm³ and typically reflects immune responses to viral infections or certain bacterial pathogens. Hyperleukocytosis, defined as a WBC count exceeding 100,000/mm³, is most often seen in hematologic malignancies and may result in leukostasis, a life-threatening condition causing cerebral or pulmonary vascular occlusion.
Epidemiology
A complete blood count is one of the most frequently ordered tests in the emergency department, and leukocytosis is among the most common laboratory abnormalities encountered. Elevated WBC counts are identified in approximately 17% of ED patients who undergo CBC testing, underscoring the importance of appropriate interpretation to avoid unnecessary testing or admission.
Etiology
Neutrophil-predominant leukocytosis is commonly caused by stress-related demargination from conditions such as trauma, surgery, seizures, pain, vomiting, hypoxia, or acute illness. Inflammatory disorders, including rheumatoid arthritis, gout, and inflammatory bowel disease, as well as bacterial infections, are frequent causes. Certain medications, such as corticosteroids, beta-agonists, lithium, and granulocyte colony–stimulating factor, can also elevate neutrophil counts. Metabolic disorders, malignancies, myeloproliferative diseases, pregnancy, hemorrhage, hemolysis, and tissue necrosis are additional contributors.
Lymphocyte-predominant leukocytosis is most often associated with viral infections, including infectious mononucleosis, cytomegalovirus, and viral hepatitis, but may also occur with pertussis, tuberculosis, syphilis, rickettsial infections, hypothyroidism, autoimmune disease, immunization responses, lymphoproliferative malignancies, or following splenectomy.
Diagnosis: signs and symptoms
Clinical presentation depends on the underlying cause rather than the degree of leukocytosis itself. Symptoms may suggest infection, such as fever, cough, rash, or gastrointestinal complaints. Chronic inflammatory states may present with joint pain or rash, while malignancy may be suggested by weight loss, fatigue, and night sweats.
Physical examination
Examination should focus on identifying focal sources of infection, such as cellulitis, abscesses, otitis, pharyngitis, or pneumonia. Signs concerning for malignancy include hepatosplenomegaly, lymphadenopathy, pallor, or bleeding. Chronic inflammatory conditions may present with joint swelling or characteristic rashes.
Diagnostic tests and interpretation
An elevated WBC count is highly nonspecific and rarely changes management by itself. Duration is important: leukocytosis lasting hours to days suggests an acute process such as infection or acute leukemia, whereas persistence over months to years raises concern for chronic inflammatory disease or hematologic malignancy. When a differential is obtained, absolute cell counts are more meaningful than percentages. A left shift may indicate acute infection or malignancy but is not expected with simple stress demargination. Automated differentials can be misleading, and a manual differential or peripheral smear may be helpful if laboratory error or malignancy is suspected. Low red blood cell or platelet counts raise concern for bone marrow pathology.
In pediatrics, febrile children younger than 36 months with WBC counts above 15,000/mm³ are at increased risk for serious bacterial infection, but moderate elevations do not reliably predict severity, and very high counts do not necessarily indicate worse illness.
Essential workup
Further evaluation should be guided by the clinical scenario. A CBC with differential and absolute counts may be useful when the etiology is unclear or malignancy is suspected. Patients with concern for hematologic malignancy require admission for peripheral smear, bone marrow biopsy, and specialist evaluation.
Differential diagnosis
The differential diagnosis is broad and mirrors the etiologic categories, including infection, inflammation, stress responses, medication effects, metabolic disorders, and hematologic or solid-organ malignancies. Clinical correlation is essential to narrow the diagnosis.
Treatment
Management is directed at the underlying cause rather than the leukocytosis itself. Extreme leukocytosis due to malignancy with leukostasis may require emergent therapy, including aggressive IV hydration, allopurinol, cytoreduction with hydroxyurea, transfusion support, and hematology consultation for possible leukapheresis.
Disposition and follow-up
Disposition decisions should not be based solely on the WBC count. Admission or discharge should be determined by the patient’s overall clinical status, suspected diagnosis, and response to treatment.
Pearls and pitfalls
Leukocytosis strongly influences clinician decision-making and is associated with increased testing, admissions, and costs despite limited diagnostic specificity. Many benign and physiologic conditions can cause elevated WBC counts. Extremely high WBC levels in the setting of hematologic malignancy may lead to leukostasis, which is life threatening and requires urgent recognition and treatment.
Basic description
Leukocytosis is defined as any elevation in the total number of white blood cells (WBCs) above the expected normal range. Normal WBC values vary by age and physiologic state. In adults, the typical range is 4,500–11,000/mm³. In children, WBC counts are higher in infancy and gradually decrease with age. During pregnancy, normal ranges shift upward across all trimesters. Exercise, female gender, smoking, and daytime hours can also transiently increase WBC counts, making clinical context essential when interpreting results.
Patterns of leukocytosis
Leukocytosis can be further characterized by the predominant cell type. Neutrophilia is defined as an absolute neutrophil count greater than 7,500/mm³ and is the most common pattern. About half of circulating neutrophils are marginated along vessel walls and can rapidly demarginate in response to acute stress, potentially doubling the WBC count. Bone marrow stores of mature and immature neutrophils may also be released during infection or inflammation, producing a “left shift.”
Lymphocytosis is defined as an absolute lymphocyte count greater than 4,000/mm³ and typically reflects immune responses to viral infections or certain bacterial pathogens. Hyperleukocytosis, defined as a WBC count exceeding 100,000/mm³, is most often seen in hematologic malignancies and may result in leukostasis, a life-threatening condition causing cerebral or pulmonary vascular occlusion.
Epidemiology
A complete blood count is one of the most frequently ordered tests in the emergency department, and leukocytosis is among the most common laboratory abnormalities encountered. Elevated WBC counts are identified in approximately 17% of ED patients who undergo CBC testing, underscoring the importance of appropriate interpretation to avoid unnecessary testing or admission.
Etiology
Neutrophil-predominant leukocytosis is commonly caused by stress-related demargination from conditions such as trauma, surgery, seizures, pain, vomiting, hypoxia, or acute illness. Inflammatory disorders, including rheumatoid arthritis, gout, and inflammatory bowel disease, as well as bacterial infections, are frequent causes. Certain medications, such as corticosteroids, beta-agonists, lithium, and granulocyte colony–stimulating factor, can also elevate neutrophil counts. Metabolic disorders, malignancies, myeloproliferative diseases, pregnancy, hemorrhage, hemolysis, and tissue necrosis are additional contributors.
Lymphocyte-predominant leukocytosis is most often associated with viral infections, including infectious mononucleosis, cytomegalovirus, and viral hepatitis, but may also occur with pertussis, tuberculosis, syphilis, rickettsial infections, hypothyroidism, autoimmune disease, immunization responses, lymphoproliferative malignancies, or following splenectomy.
Diagnosis: signs and symptoms
Clinical presentation depends on the underlying cause rather than the degree of leukocytosis itself. Symptoms may suggest infection, such as fever, cough, rash, or gastrointestinal complaints. Chronic inflammatory states may present with joint pain or rash, while malignancy may be suggested by weight loss, fatigue, and night sweats.
Physical examination
Examination should focus on identifying focal sources of infection, such as cellulitis, abscesses, otitis, pharyngitis, or pneumonia. Signs concerning for malignancy include hepatosplenomegaly, lymphadenopathy, pallor, or bleeding. Chronic inflammatory conditions may present with joint swelling or characteristic rashes.
Diagnostic tests and interpretation
An elevated WBC count is highly nonspecific and rarely changes management by itself. Duration is important: leukocytosis lasting hours to days suggests an acute process such as infection or acute leukemia, whereas persistence over months to years raises concern for chronic inflammatory disease or hematologic malignancy. When a differential is obtained, absolute cell counts are more meaningful than percentages. A left shift may indicate acute infection or malignancy but is not expected with simple stress demargination. Automated differentials can be misleading, and a manual differential or peripheral smear may be helpful if laboratory error or malignancy is suspected. Low red blood cell or platelet counts raise concern for bone marrow pathology.
In pediatrics, febrile children younger than 36 months with WBC counts above 15,000/mm³ are at increased risk for serious bacterial infection, but moderate elevations do not reliably predict severity, and very high counts do not necessarily indicate worse illness.
Essential workup
Further evaluation should be guided by the clinical scenario. A CBC with differential and absolute counts may be useful when the etiology is unclear or malignancy is suspected. Patients with concern for hematologic malignancy require admission for peripheral smear, bone marrow biopsy, and specialist evaluation.
Differential diagnosis
The differential diagnosis is broad and mirrors the etiologic categories, including infection, inflammation, stress responses, medication effects, metabolic disorders, and hematologic or solid-organ malignancies. Clinical correlation is essential to narrow the diagnosis.
Treatment
Management is directed at the underlying cause rather than the leukocytosis itself. Extreme leukocytosis due to malignancy with leukostasis may require emergent therapy, including aggressive IV hydration, allopurinol, cytoreduction with hydroxyurea, transfusion support, and hematology consultation for possible leukapheresis.
Disposition and follow-up
Disposition decisions should not be based solely on the WBC count. Admission or discharge should be determined by the patient’s overall clinical status, suspected diagnosis, and response to treatment.
Pearls and pitfalls
Leukocytosis strongly influences clinician decision-making and is associated with increased testing, admissions, and costs despite limited diagnostic specificity. Many benign and physiologic conditions can cause elevated WBC counts. Extremely high WBC levels in the setting of hematologic malignancy may lead to leukostasis, which is life threatening and requires urgent recognition and treatment.
- Published on
Emergency and Acute Medicine – Leukemia
Basic description
Leukemia refers to a group of malignant neoplasms of white blood cells that result from uncontrolled proliferation of abnormal leukocytes. These malignant cells infiltrate the bone marrow and peripheral blood, impairing normal hematopoiesis. A dangerous complication is hyperleukocytosis, defined as a white blood cell count greater than 100,000/mm³, which can cause leukostasis with occlusion of small vessels, most commonly affecting the brain and lungs. Patients may present with confusion, stupor, hypoxia, or respiratory distress.
Classification and pathophysiology
Chronic myelogenous leukemia (CML) is characterized by overproduction of granulocytic white blood cells, primarily neutrophils, which typically retain normal function. Thrombocytosis and basophilia are common, and the Philadelphia chromosome is present in more than 95% of cases. Chronic lymphocytic leukemia (CLL), the most common leukemia in adults, involves overproduction of monoclonal lymphocytes that accumulate in lymph nodes, bone marrow, liver, and spleen, predisposing patients to herpes virus infections. Acute leukemias, including acute myelogenous leukemia (AML) and acute lymphocytic leukemia (ALL), involve rapid proliferation of immature blast cells and are rapidly fatal without treatment.
Etiology and risk factors
The exact cause of leukemia is unknown. Familial clustering is seen in CLL. Exposure to ionizing radiation increases the risk of AML, ALL, and CML. In pediatric patients, ALL is the most common leukemia and the most common childhood cancer, with remission rates of 60–80% in standard-risk patients. Prognosis is poorer in infants younger than one year. Pregnancy-associated leukemias are most often AML or ALL, and treatment should not be delayed despite potential fetal risks. Older adults more commonly present with CLL or CML.
Diagnosis: signs and symptoms
Clinical presentation varies by leukemia type. CML is often asymptomatic initially but may present with fatigue, weight loss, left upper quadrant pain from splenomegaly, and later leukostasis symptoms such as dyspnea, confusion, and drowsiness. CLL is frequently asymptomatic and discovered incidentally but may present with fatigue, weight loss, lymphadenopathy, hepatosplenomegaly, and recurrent infections. Acute leukemias present more dramatically with fever, fatigue, pallor, bone pain, bleeding due to thrombocytopenia, infections from neutropenia, and symptoms of organ infiltration. Leukemic meningitis may cause headache, nausea, seizures, and altered mental status.
Physical examination findings
Common findings include pallor, petechiae, purpura, ecchymoses, lymphadenopathy, hepatomegaly, and splenomegaly. Chloromas, or granulocytic sarcomas, may be seen in AML. Sausage-shaped hemorrhagic retinal veins are pathognomonic for hyperviscosity syndromes associated with hyperleukocytosis.
Essential workup
Initial evaluation includes a complete blood count with differential and platelet count. CML typically shows markedly elevated white blood cell counts with neutrophil predominance and thrombocytosis. CLL demonstrates absolute lymphocytosis, often greater than 5,000/mm³. Acute leukemias commonly show anemia, thrombocytopenia, and variable white blood cell counts. Bone marrow biopsy is required to confirm the diagnosis.
Diagnostic tests and interpretation
Laboratory studies should include electrolytes, renal function, glucose, calcium, uric acid, and lactate dehydrogenase, which is often elevated in acute leukemias. Coagulation studies are essential to evaluate for disseminated intravascular coagulation. Blood and urine cultures should be obtained in febrile patients. Imaging with chest radiography is useful in evaluating for infection or pulmonary leukostasis. Bone marrow biopsy findings distinguish leukemia subtypes, and cytogenetic testing identifies the Philadelphia chromosome in CML.
Differential diagnosis
The differential includes leukemoid reactions from infection, lymphoma, myeloproliferative disorders, autoimmune disease, viral infections such as Epstein–Barr virus, aplastic anemia, and other causes of cytopenias or lymphocytosis.
Initial stabilization and emergency management
Management begins with airway, breathing, and circulation stabilization. Supplemental oxygen is provided for hypoxia, and IV access is established with isotonic fluids. Platelet transfusions are indicated for significant bleeding, and packed red blood cells are given for symptomatic anemia. Febrile neutropenic patients require prompt broad-spectrum antibiotics. Disseminated intravascular coagulation should be treated aggressively if present.
Emergency department treatment
Leukostasis is treated with aggressive IV hydration, urine alkalinization, allopurinol or rasburicase to prevent tumor lysis syndrome, and urgent leukapheresis. Hydroxyurea is used for cytoreduction in CML. Corticosteroids or whole-brain radiation may be required for central nervous system involvement. Blood products may need to be irradiated or leukocyte-reduced. Definitive therapy, including chemotherapy, immunotherapy, or bone marrow transplantation, is initiated after hematology consultation.
Disposition and follow-up
Admission is required for most newly diagnosed patients, particularly those with symptomatic anemia, thrombocytopenia, hyperleukocytosis, or infection. ICU admission is indicated for unstable patients with bleeding, disseminated intravascular coagulation, blast crisis, or respiratory failure. Asymptomatic patients with minimal laboratory abnormalities may be considered for outpatient management only after hematology consultation.
Pearls and pitfalls
Hyperleukocytosis can present as respiratory failure or neurologic compromise and requires urgent treatment. Tumor lysis syndrome should be anticipated and prevented early. Do not delay hematology consultation in suspected leukemia, as early intervention significantly impacts outcomes.
Basic description
Leukemia refers to a group of malignant neoplasms of white blood cells that result from uncontrolled proliferation of abnormal leukocytes. These malignant cells infiltrate the bone marrow and peripheral blood, impairing normal hematopoiesis. A dangerous complication is hyperleukocytosis, defined as a white blood cell count greater than 100,000/mm³, which can cause leukostasis with occlusion of small vessels, most commonly affecting the brain and lungs. Patients may present with confusion, stupor, hypoxia, or respiratory distress.
Classification and pathophysiology
Chronic myelogenous leukemia (CML) is characterized by overproduction of granulocytic white blood cells, primarily neutrophils, which typically retain normal function. Thrombocytosis and basophilia are common, and the Philadelphia chromosome is present in more than 95% of cases. Chronic lymphocytic leukemia (CLL), the most common leukemia in adults, involves overproduction of monoclonal lymphocytes that accumulate in lymph nodes, bone marrow, liver, and spleen, predisposing patients to herpes virus infections. Acute leukemias, including acute myelogenous leukemia (AML) and acute lymphocytic leukemia (ALL), involve rapid proliferation of immature blast cells and are rapidly fatal without treatment.
Etiology and risk factors
The exact cause of leukemia is unknown. Familial clustering is seen in CLL. Exposure to ionizing radiation increases the risk of AML, ALL, and CML. In pediatric patients, ALL is the most common leukemia and the most common childhood cancer, with remission rates of 60–80% in standard-risk patients. Prognosis is poorer in infants younger than one year. Pregnancy-associated leukemias are most often AML or ALL, and treatment should not be delayed despite potential fetal risks. Older adults more commonly present with CLL or CML.
Diagnosis: signs and symptoms
Clinical presentation varies by leukemia type. CML is often asymptomatic initially but may present with fatigue, weight loss, left upper quadrant pain from splenomegaly, and later leukostasis symptoms such as dyspnea, confusion, and drowsiness. CLL is frequently asymptomatic and discovered incidentally but may present with fatigue, weight loss, lymphadenopathy, hepatosplenomegaly, and recurrent infections. Acute leukemias present more dramatically with fever, fatigue, pallor, bone pain, bleeding due to thrombocytopenia, infections from neutropenia, and symptoms of organ infiltration. Leukemic meningitis may cause headache, nausea, seizures, and altered mental status.
Physical examination findings
Common findings include pallor, petechiae, purpura, ecchymoses, lymphadenopathy, hepatomegaly, and splenomegaly. Chloromas, or granulocytic sarcomas, may be seen in AML. Sausage-shaped hemorrhagic retinal veins are pathognomonic for hyperviscosity syndromes associated with hyperleukocytosis.
Essential workup
Initial evaluation includes a complete blood count with differential and platelet count. CML typically shows markedly elevated white blood cell counts with neutrophil predominance and thrombocytosis. CLL demonstrates absolute lymphocytosis, often greater than 5,000/mm³. Acute leukemias commonly show anemia, thrombocytopenia, and variable white blood cell counts. Bone marrow biopsy is required to confirm the diagnosis.
Diagnostic tests and interpretation
Laboratory studies should include electrolytes, renal function, glucose, calcium, uric acid, and lactate dehydrogenase, which is often elevated in acute leukemias. Coagulation studies are essential to evaluate for disseminated intravascular coagulation. Blood and urine cultures should be obtained in febrile patients. Imaging with chest radiography is useful in evaluating for infection or pulmonary leukostasis. Bone marrow biopsy findings distinguish leukemia subtypes, and cytogenetic testing identifies the Philadelphia chromosome in CML.
Differential diagnosis
The differential includes leukemoid reactions from infection, lymphoma, myeloproliferative disorders, autoimmune disease, viral infections such as Epstein–Barr virus, aplastic anemia, and other causes of cytopenias or lymphocytosis.
Initial stabilization and emergency management
Management begins with airway, breathing, and circulation stabilization. Supplemental oxygen is provided for hypoxia, and IV access is established with isotonic fluids. Platelet transfusions are indicated for significant bleeding, and packed red blood cells are given for symptomatic anemia. Febrile neutropenic patients require prompt broad-spectrum antibiotics. Disseminated intravascular coagulation should be treated aggressively if present.
Emergency department treatment
Leukostasis is treated with aggressive IV hydration, urine alkalinization, allopurinol or rasburicase to prevent tumor lysis syndrome, and urgent leukapheresis. Hydroxyurea is used for cytoreduction in CML. Corticosteroids or whole-brain radiation may be required for central nervous system involvement. Blood products may need to be irradiated or leukocyte-reduced. Definitive therapy, including chemotherapy, immunotherapy, or bone marrow transplantation, is initiated after hematology consultation.
Disposition and follow-up
Admission is required for most newly diagnosed patients, particularly those with symptomatic anemia, thrombocytopenia, hyperleukocytosis, or infection. ICU admission is indicated for unstable patients with bleeding, disseminated intravascular coagulation, blast crisis, or respiratory failure. Asymptomatic patients with minimal laboratory abnormalities may be considered for outpatient management only after hematology consultation.
Pearls and pitfalls
Hyperleukocytosis can present as respiratory failure or neurologic compromise and requires urgent treatment. Tumor lysis syndrome should be anticipated and prevented early. Do not delay hematology consultation in suspected leukemia, as early intervention significantly impacts outcomes.
- Published on
Emergency and Acute Medicine – Laceration ManagementBasic description
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.
A laceration is a disruption in skin integrity, most commonly resulting from trauma. Lacerations may involve single or multiple tissue layers and can be associated with deeper structural injury depending on mechanism and location.
Etiology
Lacerations result from multiple mechanisms including sharp objects, blunt trauma, crushing injuries, and bites.
Diagnosis: signs and symptoms
Lacerations may present with bleeding, pain, hematoma, retained foreign bodies, tissue loss, numbness, loss of motor function, diminished pulses, or delayed capillary refill. History should include mechanism and circumstances of injury, time of injury, possible foreign body exposure (glass, wood, teeth), tetanus immunization status, and comorbidities or medications that impair wound healing. Physical examination focuses on careful assessment of neurovascular status, tendon and motor function, and evaluation for devitalized tissue, contamination, joint or bone involvement, and tendon injury. Sharp objects should not be digitally explored if there is risk of further injury.
Essential workup
Consider operative repair if safe wound management cannot be achieved in the emergency department, particularly in children requiring deep sedation. Early surgical consultation is recommended for complex wounds, especially those involving the face, eyes, hands, or joints. Pediatric patients should be assessed for possible nonaccidental trauma.
Diagnostic tests and interpretation
Imaging is used when foreign bodies are suspected. Plain radiographs may identify radiopaque objects but will not reliably detect wood or plant material. Ultrasound can identify radiolucent foreign bodies. CT or MRI may be required for deep or complex injuries, with metal precautions as appropriate.
Differential diagnosis
Skin avulsion, abrasion, contusion, and crush injury should be considered.
Treatment: prehospital care
Initial care includes bleeding control with direct pressure, gentle realignment of skin flaps to preserve perfusion, splinting when indicated, and adherence to universal precautions.
Initial stabilization and therapy
Airway, breathing, and circulation are addressed first. Hemostasis is achieved, rings and constricting jewelry are removed to prevent ischemia, and the wound is protected.
Emergency department treatment and procedures
Primary closure timing depends on wound age and location. Most wounds may be closed within 8–12 hours, facial wounds up to 24 hours if clean and well irrigated. Older or contaminated wounds may require delayed primary closure or healing by secondary intention. Adequate analgesia is essential, using topical, local, or regional anesthesia, with procedural sedation when necessary. Wounds are irrigated with copious normal saline under appropriate pressure, avoiding antiseptics inside the wound. Devitalized tissue is debrided. Foreign bodies are removed when they pose risk of infection, toxicity, or functional impairment. Closure technique is selected based on wound tension, location, and depth, with careful reapproximation of anatomic landmarks. Dressings include antibiotic ointment and nonadherent coverings, and splinting is applied when needed. Prophylactic antibiotics are not required for uncomplicated wounds but are considered for high-risk injuries such as bites or heavily contaminated wounds. Tetanus prophylaxis is updated as indicated.
Medications
Local anesthetics include lidocaine and bupivacaine, with topical agents such as LET, EMLA, or TAC when appropriate. Tetanus immunization is administered according to age and immunization status. Analgesics are provided as needed.
Follow-up and disposition
Most lacerations do not require admission unless associated with major injury, infection risk requiring IV antibiotics, or social concerns such as suspected abuse. Discharge requires clear wound care instructions, infection precautions, and follow-up planning. Wound checks are recommended within 48 hours for high-risk injuries. Suture removal timing varies by anatomic location and perfusion.
Issues for referral
Immediate referral is required for suspected tear duct injuries, complex facial wounds, tendon or nerve involvement, and wounds requiring specialized surgical repair.
Pearls and pitfalls
Careful neurovascular examination before and after repair is essential. Inadequate irrigation and missed foreign bodies increase infection risk. Always consider deeper structural injury, especially in hand and joint lacerations, and maintain a low threshold for consultation when cosmetic or functional outcomes may be compromised.
- Published on
Emergency and Acute Medicine – Legg–Calvé–Perthes Disease
Basic description
Legg–Calvé–Perthes disease is an idiopathic avascular necrosis of the femoral head occurring exclusively in children. It is thought to result from repeated vascular insults to the developing femoral head, leading to ischemia, collapse, and subsequent remodeling. Genetic associations include increased frequency in children with factor V Leiden mutation and anticardiolipin antibodies, supporting a possible hypercoagulable contribution.
Etiology
The condition is believed to arise from successive vascular occlusions of the femoral head and is likely multifactorial. Risk factors include male sex, Caucasian race, exposure to tobacco or wood smoke, low birth weight, and short birth length. The disease progresses through four stages: an initial ischemic stage with dense femoral head and synovitis, a fragmentation stage with femoral head softening and deformation, a healing stage with reossification, and a residual stage with variable permanent deformity. It most commonly affects children aged 3–7 years, with a male predominance of approximately 4:1, and is bilateral in 10–15% of cases.
Diagnosis: signs and symptoms
Presentation is often insidious. Limping is the most common initial complaint. Pain is typically dull or aching and may localize to the hip, groin, anteromedial thigh, or knee. Pain is activity related and improves with rest. Muscle spasm is common early in the disease course. On examination, children are usually afebrile and well appearing. Early findings include limited internal rotation and abduction of the hip. Later findings may include adductor contractures, muscle atrophy, and leg-length discrepancy. Some patients may be minimally symptomatic or asymptomatic.
Essential workup
Plain radiographs of the hips are the most important initial diagnostic study in the emergency setting. Septic arthritis must be considered and excluded, particularly in children with fever, acute onset, or toxic appearance.
Diagnostic tests and interpretation
No laboratory test is diagnostic for Legg–Calvé–Perthes disease. CBC, ESR, and CRP may be obtained if infection is a concern. Imaging establishes the diagnosis. AP and frog-leg lateral radiographs of both hips should be obtained to assess disease stage and detect bilateral involvement. Early radiographs may be normal in the first 3–6 months. MRI is more sensitive and can detect early ischemic changes and assess the extent of femoral head infarction. Bone scintigraphy can identify disease before radiographic changes but is less commonly used. Ultrasound may show a hip effusion but is nonspecific. CT and arthrography are primarily used for surgical planning rather than initial diagnosis.
Differential diagnosis
Unilateral disease considerations include transient synovitis, septic arthritis, osteomyelitis, sickle cell disease, juvenile idiopathic arthritis, trauma, slipped capital femoral epiphysis, tuberculosis, and malignancy. Bilateral disease raises consideration of hypothyroidism, epiphyseal dysplasia, and Gaucher disease.
Treatment
This is not a life-threatening condition, and emergency management focuses on symptom control. Pain management with NSAIDs is the primary intervention. Activity restriction is recommended, and crutches may be required if weight bearing is painful. Clinical instability, fever, or toxic appearance should prompt evaluation for alternative diagnoses.
Medications
First-line therapy is ibuprofen at 10 mg/kg per dose orally every 6–8 hours as needed for pain. Diazepam may be used as a second-line agent for significant muscle spasm.
Disposition and follow-up
Admission is rarely required and is reserved for severe pain not controlled with oral medications or social situations where home care is not feasible. Most patients can be discharged once pain is controlled, with orthopedic follow-up arranged within 1–2 weeks. Long-term management is determined by orthopedics and may include observation, activity modification, bracing, traction, or surgical intervention depending on age at onset and disease severity.
Pearls and pitfalls
Acute onset, fever, toxic appearance, or inability to bear weight should raise concern for diagnoses other than Legg–Calvé–Perthes disease, particularly septic arthritis. Early disease may have normal radiographs, so persistent symptoms warrant close follow-up and repeat imaging.
Basic description
Legg–Calvé–Perthes disease is an idiopathic avascular necrosis of the femoral head occurring exclusively in children. It is thought to result from repeated vascular insults to the developing femoral head, leading to ischemia, collapse, and subsequent remodeling. Genetic associations include increased frequency in children with factor V Leiden mutation and anticardiolipin antibodies, supporting a possible hypercoagulable contribution.
Etiology
The condition is believed to arise from successive vascular occlusions of the femoral head and is likely multifactorial. Risk factors include male sex, Caucasian race, exposure to tobacco or wood smoke, low birth weight, and short birth length. The disease progresses through four stages: an initial ischemic stage with dense femoral head and synovitis, a fragmentation stage with femoral head softening and deformation, a healing stage with reossification, and a residual stage with variable permanent deformity. It most commonly affects children aged 3–7 years, with a male predominance of approximately 4:1, and is bilateral in 10–15% of cases.
Diagnosis: signs and symptoms
Presentation is often insidious. Limping is the most common initial complaint. Pain is typically dull or aching and may localize to the hip, groin, anteromedial thigh, or knee. Pain is activity related and improves with rest. Muscle spasm is common early in the disease course. On examination, children are usually afebrile and well appearing. Early findings include limited internal rotation and abduction of the hip. Later findings may include adductor contractures, muscle atrophy, and leg-length discrepancy. Some patients may be minimally symptomatic or asymptomatic.
Essential workup
Plain radiographs of the hips are the most important initial diagnostic study in the emergency setting. Septic arthritis must be considered and excluded, particularly in children with fever, acute onset, or toxic appearance.
Diagnostic tests and interpretation
No laboratory test is diagnostic for Legg–Calvé–Perthes disease. CBC, ESR, and CRP may be obtained if infection is a concern. Imaging establishes the diagnosis. AP and frog-leg lateral radiographs of both hips should be obtained to assess disease stage and detect bilateral involvement. Early radiographs may be normal in the first 3–6 months. MRI is more sensitive and can detect early ischemic changes and assess the extent of femoral head infarction. Bone scintigraphy can identify disease before radiographic changes but is less commonly used. Ultrasound may show a hip effusion but is nonspecific. CT and arthrography are primarily used for surgical planning rather than initial diagnosis.
Differential diagnosis
Unilateral disease considerations include transient synovitis, septic arthritis, osteomyelitis, sickle cell disease, juvenile idiopathic arthritis, trauma, slipped capital femoral epiphysis, tuberculosis, and malignancy. Bilateral disease raises consideration of hypothyroidism, epiphyseal dysplasia, and Gaucher disease.
Treatment
This is not a life-threatening condition, and emergency management focuses on symptom control. Pain management with NSAIDs is the primary intervention. Activity restriction is recommended, and crutches may be required if weight bearing is painful. Clinical instability, fever, or toxic appearance should prompt evaluation for alternative diagnoses.
Medications
First-line therapy is ibuprofen at 10 mg/kg per dose orally every 6–8 hours as needed for pain. Diazepam may be used as a second-line agent for significant muscle spasm.
Disposition and follow-up
Admission is rarely required and is reserved for severe pain not controlled with oral medications or social situations where home care is not feasible. Most patients can be discharged once pain is controlled, with orthopedic follow-up arranged within 1–2 weeks. Long-term management is determined by orthopedics and may include observation, activity modification, bracing, traction, or surgical intervention depending on age at onset and disease severity.
Pearls and pitfalls
Acute onset, fever, toxic appearance, or inability to bear weight should raise concern for diagnoses other than Legg–Calvé–Perthes disease, particularly septic arthritis. Early disease may have normal radiographs, so persistent symptoms warrant close follow-up and repeat imaging.
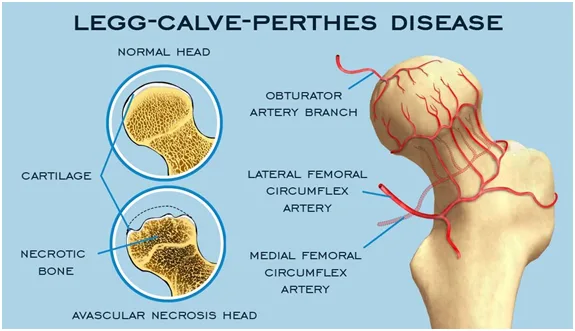
- Published on
Emergency and Acute Medicine – Larynx Fracture
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.
Basic description
Laryngeal fracture results from the direct transfer of severe force to the anterior neck, producing injuries that range from simple mucosal tears to fractured or comminuted laryngeal cartilages. Structures that may be involved include the epiglottis, thyroid, arytenoid, cricoid, corniculate, and cuneiform cartilages. Although rare, laryngeal fractures are life-threatening because of the risk of progressive airway compromise.
Etiology and epidemiology
Laryngeal fracture is uncommon, accounting for fewer than 1% of blunt trauma cases, with an incidence estimated at 1 in 5,000 to 1 in 42,000 emergency department visits. Mortality directly related to the injury ranges from 2% to 15%. Most cases result from blunt or penetrating trauma to the anterior neck during motor vehicle or motorcycle crashes, assaults, or recreational activities. A classic mechanism is the “clothesline” injury, in which the neck strikes a fixed object such as a wire or branch during forward motion. Hyperextension of the neck combined with a direct blow is typical. Iatrogenic injuries from intubation are increasingly recognized, particularly in older adults. In children, bicycle handlebar injuries are a common mechanism, with neck extension compressing the larynx against the cervical spine.
Diagnosis: signs and symptoms
Symptoms may be delayed for hours, making diagnosis challenging, especially in polytrauma patients or those immobilized in cervical collars. Clinical findings include anterior neck tenderness, bruising or abrasions, hoarseness or voice change, dysphonia, hemoptysis, stridor, dyspnea, and subcutaneous or mediastinal emphysema. Pneumothorax, loss of normal laryngeal landmarks, and difficulty with mechanical ventilation may also be present. Pediatric patients may initially appear minimally symptomatic but can deteriorate rapidly because of airway edema.
Essential workup
Airway evaluation is the priority. Endoscopic assessment should take precedence over plain radiography because mucosal edema may cause airway compromise even in the absence of obvious skeletal injury. Cervical spine CT is preferred over plain radiographs, which are often nondiagnostic. Chest radiography helps identify pneumothorax, pneumomediastinum, or subcutaneous emphysema. CT scan of the cervical spine with fine cuts through the larynx and IV contrast is recommended unless the patient proceeds directly to surgery, as it can identify cartilage fractures and associated vascular injury. Continuous pulse oximetry is essential. MRI is generally not useful due to time constraints and limited evaluation of cartilaginous injury.
Diagnostic tests and procedures
Arterial blood gas analysis may be helpful in patients with respiratory compromise. Flexible fiberoptic laryngoscopy is a key diagnostic tool for visualization of mucosal injuries, vocal cord mobility, and airway patency. CT angiography is preferred when vascular injury is suspected, particularly in penetrating trauma. Fiberoptic bronchoscopy and esophagoscopy may be required to evaluate associated aerodigestive injuries. Surgical exploration is indicated based on injury severity.
Differential diagnosis
Associated injuries must be considered, including intracranial injury, cervical spine injury, esophageal injury, carotid artery injury, phrenic nerve injury, aspiration pneumonitis, hypoxic cerebral injury, airway edema, air embolism, and pneumothorax. In children, massive edema and hematoma may occur without visible fractures on imaging.
Treatment: prehospital and initial stabilization
Airway protection is critical. Supplemental oxygen and gentle suctioning should be provided, with cervical spine immobilization maintained. Elective intubation is controversial and not routinely recommended, as repeated orotracheal attempts may worsen injury. In severe cases, early surgical airway management may be required.
Emergency department management
Airway control remains the highest priority. Early intubation may be necessary for impending airway compromise, but in patients with severe neck injury, formal tracheostomy under local anesthesia is often safer than endotracheal intubation. Cricothyrotomy may be used for injuries above the cricothyroid membrane but should be avoided if there is evidence of cricotracheal disruption or hematoma over the membrane. Supplemental humidified oxygen, head-of-bed elevation, strict NPO status, and voice rest are recommended. IV access should be established, and early otolaryngology consultation obtained. Mechanical ventilation strategies may be required for associated pulmonary injury.
Medications
Broad-spectrum antibiotics are indicated when subcutaneous emphysema suggests mucosal breach, commonly using ampicillin/sulbactam or clindamycin. Acid suppression with H2 blockers or proton pump inhibitors may reduce irritation of mucosal injuries. Corticosteroids are not routinely indicated but may be considered for severe laryngeal edema. In pediatric patients with stridor, nebulized racemic epinephrine may provide temporary relief.
Disposition and follow-up
All patients with confirmed or suspected laryngeal fracture require admission to a monitored setting for airway observation and serial examinations, often including repeat fiberoptic laryngoscopy. Pediatric patients should be admitted routinely because of the risk of rapid airway compromise. Discharge may be considered only after an adequate observation period, typically at least 6 hours, in patients with no evidence of airway injury, edema, or compromise. When in doubt, admission is recommended.
Pearls and pitfalls
Laryngeal fractures are rare but potentially fatal. Symptoms may be subtle or delayed, and airway deterioration can be rapid. Avoid repeated intubation attempts, and maintain a low threshold for surgical airway management. Early recognition, careful airway control, and otolaryngology involvement are key to improving outcomes.