- Published on
Emergency And Acute Medicine: Hypokalemia
Basics
Description
Hypokalemia is defined as a serum potassium <3.5 meq />. Mild 3–3.5 mEq/L, moderate 2.5–3 mEq/L, severe <2.5 meq />. Occurs in up to 20% of inpatients and 14% of outpatients, commonly from diuretics or GI losses. Potassium is the major intracellular cation (98% intracellular) maintained by Na–K ATPase, insulin, β-agonists, and mineralocorticoids. Hypokalemia increases the intracellular–extracellular potassium gradient, alters depolarization thresholds, prolongs action potentials, and disrupts cellular function.
Etiology
Renal losses Diuretics, renal tubular disorders (RTA I and II), interstitial nephritis, drug toxicity (amphotericin, cisplatin), myeloma kidney, hyperaldosteronism (primary, secondary, exogenous), hypomagnesemia, osmotic diuresis, Bartter and Gitelman syndromes, Liddle syndrome, delivery of nonreabsorbable anions (bicarbonate, ketones, hippurate, penicillins).
GI losses Diarrhea, villous adenomas, laxative abuse, vomiting or NG suction, ureterosigmoidostomy, intestinal fistulae, ileostomy, cystic fibrosis.
Intracellular shift Alkalosis, insulin administration or refeeding, adrenergic excess (stress, β-agonists, theophylline), stimulants, hypokalemic periodic paralysis (familial or thyrotoxic), hypothermia.
Poor intake Rare alone; seen with malnutrition, eating disorders, dementia, or esophageal disease.
Diagnosis
Signs And Symptoms Neuromuscular weakness beginning in lower extremities and progressing proximally, paralysis with rapid severe hypokalemia, muscle cramps, tetany, rhabdomyolysis, paresthesias, fatigue. GI ileus and constipation. Cardiac dysrhythmias including PACs, PVCs, AV block, atrial or junctional tachycardias, VT/VF, and potentiation of digoxin toxicity. Renal concentrating defect causing polyuria and polydipsia.
Physical Exam Hypertension suggests mineralocorticoid excess or renal artery stenosis. Hypotension suggests GI loss or diuretics. Decreased reflexes and muscle tenderness may be present.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose. Elevated bicarbonate suggests diuretics, vomiting, or mineralocorticoid excess; low bicarbonate suggests RTA or diarrhea. Urine potassium <20 meq /> suggests nonrenal loss or intracellular shift; >20 mEq/L suggests renal loss. Urine potassium–creatinine ratio <13 meq /> favors nonrenal loss; >13 mEq/g favors renal loss. Urine sodium <20 meq /> with high urine potassium suggests secondary hyperaldosteronism. Plasma renin differentiates primary vs secondary hyperaldosteronism. Check TSH and free T4 if indicated.
ECG Flattened T waves, ST depression, prominent U waves mimicking QT prolongation, small P waves, atrial and ventricular dysrhythmias.
Differential Diagnosis Primary cardiac disease, neuromuscular junction disorders, spinal cord disease, polyneuropathies, acute myopathies, cataplexy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, cardiac monitoring.
Emergency Department Treatment/Procedures Replace potassium based on severity, symptoms, and comorbidities. Oral replacement preferred when possible. Identify and stop ongoing losses, treat vomiting or diarrhea, avoid glucose-containing fluids, and correct volume depletion and hypochloremia.
Medications
Oral potassium chloride Preferred. Mild to moderate: 10–20 mEq q6–12h. Moderate to severe: 40–60 mEq q8–12h.
Oral potassium citrate or gluconate Use in acidosis; less effective in alkalosis.
IV potassium chloride Indicated for severe hypokalemia, dysrhythmias, paralysis, or ongoing losses. Typical rate 10 mEq/h via peripheral line; higher rates require central access and close monitoring. Avoid dextrose solutions.
Adjuncts Magnesium sulfate 2 g IV if hypomagnesemia present. Correct volume and chloride deficits with normal saline.
Follow-Up And Disposition
Admission Criteria Need for IV potassium, dysrhythmias, profound weakness, ongoing losses, K <2.5 meq />, significant hypotension or hypertension, major comorbidities.
Discharge Criteria Asymptomatic, able to take oral potassium, reliable follow-up. Recheck electrolytes in 2–3 days.
Follow-Up Recommendations Continue replacement until potassium remains ≥3–3.5 mEq/L. Refer to nephrology if renal wasting suspected.
Pearls And Pitfalls
Correct hypokalemia before treating acidosis to prevent dangerous intracellular shifts. Avoid glucose during replacement. Check and correct magnesium if hypokalemia is refractory. Small potassium doses are sufficient in periodic paralysis or adrenergic states; excessive replacement risks rebound hyperkalemia.
Basics
Description
Hypokalemia is defined as a serum potassium <3.5 meq />. Mild 3–3.5 mEq/L, moderate 2.5–3 mEq/L, severe <2.5 meq />. Occurs in up to 20% of inpatients and 14% of outpatients, commonly from diuretics or GI losses. Potassium is the major intracellular cation (98% intracellular) maintained by Na–K ATPase, insulin, β-agonists, and mineralocorticoids. Hypokalemia increases the intracellular–extracellular potassium gradient, alters depolarization thresholds, prolongs action potentials, and disrupts cellular function.
Etiology
Renal losses Diuretics, renal tubular disorders (RTA I and II), interstitial nephritis, drug toxicity (amphotericin, cisplatin), myeloma kidney, hyperaldosteronism (primary, secondary, exogenous), hypomagnesemia, osmotic diuresis, Bartter and Gitelman syndromes, Liddle syndrome, delivery of nonreabsorbable anions (bicarbonate, ketones, hippurate, penicillins).
GI losses Diarrhea, villous adenomas, laxative abuse, vomiting or NG suction, ureterosigmoidostomy, intestinal fistulae, ileostomy, cystic fibrosis.
Intracellular shift Alkalosis, insulin administration or refeeding, adrenergic excess (stress, β-agonists, theophylline), stimulants, hypokalemic periodic paralysis (familial or thyrotoxic), hypothermia.
Poor intake Rare alone; seen with malnutrition, eating disorders, dementia, or esophageal disease.
Diagnosis
Signs And Symptoms Neuromuscular weakness beginning in lower extremities and progressing proximally, paralysis with rapid severe hypokalemia, muscle cramps, tetany, rhabdomyolysis, paresthesias, fatigue. GI ileus and constipation. Cardiac dysrhythmias including PACs, PVCs, AV block, atrial or junctional tachycardias, VT/VF, and potentiation of digoxin toxicity. Renal concentrating defect causing polyuria and polydipsia.
Physical Exam Hypertension suggests mineralocorticoid excess or renal artery stenosis. Hypotension suggests GI loss or diuretics. Decreased reflexes and muscle tenderness may be present.
Diagnosis Tests And Interpretation
Lab Electrolytes, BUN, creatinine, glucose. Elevated bicarbonate suggests diuretics, vomiting, or mineralocorticoid excess; low bicarbonate suggests RTA or diarrhea. Urine potassium <20 meq /> suggests nonrenal loss or intracellular shift; >20 mEq/L suggests renal loss. Urine potassium–creatinine ratio <13 meq /> favors nonrenal loss; >13 mEq/g favors renal loss. Urine sodium <20 meq /> with high urine potassium suggests secondary hyperaldosteronism. Plasma renin differentiates primary vs secondary hyperaldosteronism. Check TSH and free T4 if indicated.
ECG Flattened T waves, ST depression, prominent U waves mimicking QT prolongation, small P waves, atrial and ventricular dysrhythmias.
Differential Diagnosis Primary cardiac disease, neuromuscular junction disorders, spinal cord disease, polyneuropathies, acute myopathies, cataplexy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, cardiac monitoring.
Emergency Department Treatment/Procedures Replace potassium based on severity, symptoms, and comorbidities. Oral replacement preferred when possible. Identify and stop ongoing losses, treat vomiting or diarrhea, avoid glucose-containing fluids, and correct volume depletion and hypochloremia.
Medications
Oral potassium chloride Preferred. Mild to moderate: 10–20 mEq q6–12h. Moderate to severe: 40–60 mEq q8–12h.
Oral potassium citrate or gluconate Use in acidosis; less effective in alkalosis.
IV potassium chloride Indicated for severe hypokalemia, dysrhythmias, paralysis, or ongoing losses. Typical rate 10 mEq/h via peripheral line; higher rates require central access and close monitoring. Avoid dextrose solutions.
Adjuncts Magnesium sulfate 2 g IV if hypomagnesemia present. Correct volume and chloride deficits with normal saline.
Follow-Up And Disposition
Admission Criteria Need for IV potassium, dysrhythmias, profound weakness, ongoing losses, K <2.5 meq />, significant hypotension or hypertension, major comorbidities.
Discharge Criteria Asymptomatic, able to take oral potassium, reliable follow-up. Recheck electrolytes in 2–3 days.
Follow-Up Recommendations Continue replacement until potassium remains ≥3–3.5 mEq/L. Refer to nephrology if renal wasting suspected.
Pearls And Pitfalls
Correct hypokalemia before treating acidosis to prevent dangerous intracellular shifts. Avoid glucose during replacement. Check and correct magnesium if hypokalemia is refractory. Small potassium doses are sufficient in periodic paralysis or adrenergic states; excessive replacement risks rebound hyperkalemia.
- Published on
Emergency And Acute Medicine: Hypoglycemic Agent Poisoning
Basics
Description Hypoglycemic agent poisoning results from oral or parenteral agents that cause hypoglycemia or metabolic derangements. Poisoning may be intentional or accidental.
Etiology
Insulin Enhances cellular glucose uptake, limits cerebral glucose availability, and shifts potassium intracellularly causing hypokalemia.
Sulfonylureas And Meglitinides Increase pancreatic insulin release, reduce hepatic glucose production, and increase peripheral insulin sensitivity. Effects are potentiated by polypharmacy, alcohol use, hepatic dysfunction, and renal insufficiency.
GLP-1 Modulators Exenatide and DPP-4 inhibitors (e.g., sitagliptin, saxagliptin) enhance insulin secretion and delay gastric emptying. Effects in overdose are unclear.
Biguanides (Metformin) Rarely cause hypoglycemia alone but, with insulin, increase cellular glucose uptake, inhibit gluconeogenesis, reduce GI glucose absorption, and promote lactate accumulation leading to lactic acidosis.
Thiazolidinediones Increase insulin sensitivity and glucose uptake in the presence of insulin.
α-Glucosidase Inhibitors Reduce carbohydrate absorption and systemic glucose.
Diagnosis
Signs And Symptoms
Insulin Or Sulfonylureas Hypoglycemia often when glucose <40–60 mg />L. Symptoms include diaphoresis, pallor, tremor, hunger, nausea, headache, blurred vision, paresthesias, weakness, anxiety, confusion, seizures, coma, tachycardia or late bradycardia, hypertension, and hypothermia. β-blockers may blunt adrenergic signs.
Biguanides Lactic acidosis with nausea, vomiting, abdominal pain, agitation, lethargy, coma, Kussmaul respirations, hypotension, and tachycardia.
Pediatric Considerations Neonatal hypoglycemia may occur after maternal sulfonylurea use. Ingestion of a single sulfonylurea tablet can cause severe hypoglycemia or death. Onset may be delayed up to 8 hr.
History
Diabetes diagnosis, access to medications, dosing errors, renal or hepatic disease, alcohol use, and possible malicious or intentional ingestion.
Physical Exam Tachycardia (may be blunted), altered mental status, ataxia, seizures, or coma.
Essential Workup
Frequent glucose monitoring, vital signs, and neurologic assessment. Check electrolytes and lactate for biguanides and liver function tests for thiazolidinediones.
Diagnosis Tests And Interpretation
Lab Serum glucose pre- and post-treatment, electrolytes (hypokalemia, anion gap acidosis), BUN/creatinine, CBC, ethanol level, lactate, LFTs, ABG. Insulin and C-peptide levels may confirm exogenous insulin use.
Imaging/Other ECG for dysrhythmias, EEG for persistent coma, CT head for prolonged hypoglycemia, CXR for aspiration or pulmonary edema.
Differential Diagnosis Adrenal insufficiency, panhypopituitarism, sepsis, insulinoma, neuroendocrine tumors, cirrhosis, ethanol or salicylate ingestion, β-blocker overdose, Ackee fruit poisoning.
Treatment
Prehospital Transport medications and pill bottles with patient.
Initial Stabilization/Therapy ABCs, oxygen, IV access, cardiac monitoring, pulse oximetry. Give naloxone, thiamine, and dextrose if altered mental status.
Emergency Department Treatment/Procedures Treat hypoglycemia with IV dextrose bolus followed by D5W or D10W infusion. Allow oral intake when mental status improves. Persistent neuroglycopenia requires repeat dextrose. Consider activated charcoal for recent oral ingestions. Treat hypotension with IV fluids and cautious vasopressors. Give bicarbonate for severe metformin-associated acidosis (pH <7). use benzodiazepines for seizures. sulfonylurea-induced recurrent hypoglycemia, inhibit insulin secretion with octreotide or diazoxide. consider early hemodialysis severe biguanide-associated lactic acidosis.< />pan>
Medications
Activated charcoal 1 g/kg PO. Dextrose 50–100 mL D50 IV (peds: D25 2 mL/kg). Octreotide 50–100 μg SC/IV q8–12h. Diazoxide 200 mg PO or 1–3 mg/kg IV. Glucagon 1–2 mg IM/SC/IV. Benzodiazepines for seizures. Thiamine 100 mg IV/IM.
Follow-Up And Disposition
Admission Criteria
Sulfonylurea or long-acting insulin exposure, recurrent or refractory hypoglycemia, need for continuous dextrose infusion, intentional overdose, all pediatric sulfonylurea ingestions, or metabolic complications from biguanides.
Discharge Criteria
Short-acting insulin error with dietary insufficiency, normal mental status, stable glucose after ≥4 hr observation, and tolerating oral intake.
Issues For Referral Poison prevention counseling for accidental exposure; psychiatric evaluation for intentional poisoning.
Follow-Up Recommendations
Close outpatient follow-up for glucose monitoring and medication adjustment.
Pearls And Pitfalls Sulfonylureas have prolonged effects with delayed or recurrent hypoglycemia—observe carefully. Metformin must be withheld 48 hr after IV contrast due to lactic acidosis risk. Persistent hypoglycemia requires octreotide, not repeated dextrose alone.
Basics
Description Hypoglycemic agent poisoning results from oral or parenteral agents that cause hypoglycemia or metabolic derangements. Poisoning may be intentional or accidental.
Etiology
Insulin Enhances cellular glucose uptake, limits cerebral glucose availability, and shifts potassium intracellularly causing hypokalemia.
Sulfonylureas And Meglitinides Increase pancreatic insulin release, reduce hepatic glucose production, and increase peripheral insulin sensitivity. Effects are potentiated by polypharmacy, alcohol use, hepatic dysfunction, and renal insufficiency.
GLP-1 Modulators Exenatide and DPP-4 inhibitors (e.g., sitagliptin, saxagliptin) enhance insulin secretion and delay gastric emptying. Effects in overdose are unclear.
Biguanides (Metformin) Rarely cause hypoglycemia alone but, with insulin, increase cellular glucose uptake, inhibit gluconeogenesis, reduce GI glucose absorption, and promote lactate accumulation leading to lactic acidosis.
Thiazolidinediones Increase insulin sensitivity and glucose uptake in the presence of insulin.
α-Glucosidase Inhibitors Reduce carbohydrate absorption and systemic glucose.
Diagnosis
Signs And Symptoms
Insulin Or Sulfonylureas Hypoglycemia often when glucose <40–60 mg />L. Symptoms include diaphoresis, pallor, tremor, hunger, nausea, headache, blurred vision, paresthesias, weakness, anxiety, confusion, seizures, coma, tachycardia or late bradycardia, hypertension, and hypothermia. β-blockers may blunt adrenergic signs.
Biguanides Lactic acidosis with nausea, vomiting, abdominal pain, agitation, lethargy, coma, Kussmaul respirations, hypotension, and tachycardia.
Pediatric Considerations Neonatal hypoglycemia may occur after maternal sulfonylurea use. Ingestion of a single sulfonylurea tablet can cause severe hypoglycemia or death. Onset may be delayed up to 8 hr.
History
Diabetes diagnosis, access to medications, dosing errors, renal or hepatic disease, alcohol use, and possible malicious or intentional ingestion.
Physical Exam Tachycardia (may be blunted), altered mental status, ataxia, seizures, or coma.
Essential Workup
Frequent glucose monitoring, vital signs, and neurologic assessment. Check electrolytes and lactate for biguanides and liver function tests for thiazolidinediones.
Diagnosis Tests And Interpretation
Lab Serum glucose pre- and post-treatment, electrolytes (hypokalemia, anion gap acidosis), BUN/creatinine, CBC, ethanol level, lactate, LFTs, ABG. Insulin and C-peptide levels may confirm exogenous insulin use.
Imaging/Other ECG for dysrhythmias, EEG for persistent coma, CT head for prolonged hypoglycemia, CXR for aspiration or pulmonary edema.
Differential Diagnosis Adrenal insufficiency, panhypopituitarism, sepsis, insulinoma, neuroendocrine tumors, cirrhosis, ethanol or salicylate ingestion, β-blocker overdose, Ackee fruit poisoning.
Treatment
Prehospital Transport medications and pill bottles with patient.
Initial Stabilization/Therapy ABCs, oxygen, IV access, cardiac monitoring, pulse oximetry. Give naloxone, thiamine, and dextrose if altered mental status.
Emergency Department Treatment/Procedures Treat hypoglycemia with IV dextrose bolus followed by D5W or D10W infusion. Allow oral intake when mental status improves. Persistent neuroglycopenia requires repeat dextrose. Consider activated charcoal for recent oral ingestions. Treat hypotension with IV fluids and cautious vasopressors. Give bicarbonate for severe metformin-associated acidosis (pH <7). use benzodiazepines for seizures. sulfonylurea-induced recurrent hypoglycemia, inhibit insulin secretion with octreotide or diazoxide. consider early hemodialysis severe biguanide-associated lactic acidosis.< />pan>
Medications
Activated charcoal 1 g/kg PO. Dextrose 50–100 mL D50 IV (peds: D25 2 mL/kg). Octreotide 50–100 μg SC/IV q8–12h. Diazoxide 200 mg PO or 1–3 mg/kg IV. Glucagon 1–2 mg IM/SC/IV. Benzodiazepines for seizures. Thiamine 100 mg IV/IM.
Follow-Up And Disposition
Admission Criteria
Sulfonylurea or long-acting insulin exposure, recurrent or refractory hypoglycemia, need for continuous dextrose infusion, intentional overdose, all pediatric sulfonylurea ingestions, or metabolic complications from biguanides.
Discharge Criteria
Short-acting insulin error with dietary insufficiency, normal mental status, stable glucose after ≥4 hr observation, and tolerating oral intake.
Issues For Referral Poison prevention counseling for accidental exposure; psychiatric evaluation for intentional poisoning.
Follow-Up Recommendations
Close outpatient follow-up for glucose monitoring and medication adjustment.
Pearls And Pitfalls Sulfonylureas have prolonged effects with delayed or recurrent hypoglycemia—observe carefully. Metformin must be withheld 48 hr after IV contrast due to lactic acidosis risk. Persistent hypoglycemia requires octreotide, not repeated dextrose alone.
- Published on
KembaraXtra-Emergency And Acute Medicine: Hypoglycemia
Basics
Description
Hypoglycemia results from deficiency of counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone) or excessive insulin response. Defined as serum glucose <70 mg />L.
Risk Factors
Strict glycemic control with insulin, prior hypoglycemia, hypoglycemia unawareness, impaired counterregulation (<5 years or elderly), renal disease, malnutrition, coronary artery liver congenital metabolic endocrine disorders, hyperinsulinism, and neonatal diabetes mellitus.< />pan>
Etiology
Increased insulin levels due to insulin or oral hypoglycemic overdose, sepsis, insulinoma, autoimmune hypoglycemia, alimentary hyperinsulinism, renal failure, or liver cirrhosis. Decreased glucose production from alcohol use, drugs (salicylates, β-blockers including eye drops, SSRIs, some antibiotics), adrenal insufficiency, malnutrition, dehydration, cerebral edema, extremes of age, heart failure, endocrine disorders, and pregnancy-related substrate deficiency.
Pediatric considerations
Most common cause in first 3 months of life is persistent hyperinsulinemic hypoglycemia of infancy, especially in infants of diabetic mothers.
Diagnosis
Signs And Symptoms Adrenergic symptoms include diaphoresis, anxiety, tachycardia, hunger, paresthesias, chest pain, and ischemic ECG changes. Neuroglycopenic symptoms include dizziness, confusion, behavioral changes, slurred speech, focal deficits, seizures, hemiplegia, coma, and CVA mimic. Neonates may present with poor feeding, irritability, tremors, seizures, or bradycardia.
Alert
Patients with hypoglycemia unawareness may present only with late findings such as seizures or coma.
History
Assess diabetes status, renal or liver disease, alcohol use, medication exposure, and possible overdose.
Physical Exam Findings reflect adrenergic or neuroglycopenic manifestations.
Essential Workup Diagnosis requires neuroglycopenic symptoms, documented low glucose, and symptom resolution after glucose administration.
Diagnosis Tests And Interpretation
Lab Blood glucose (pre- and post-treatment), electrolytes, BUN/creatinine, PT, urinalysis, cultures if infection suspected, C-peptide if exogenous insulin overdose suspected.
Imaging CXR for aspiration or pneumonia if indicated.
ECG Evaluate for ischemia or dysrhythmias.
Differential Diagnosis
Stroke/TIA, seizure, intoxication, hypoxia, sepsis, metabolic or endocrine disorders, psychiatric disease.
Pediatric Growth hormone deficiency, inborn errors of metabolism, ketotic hypoglycemia, Reye syndrome, salicylate ingestion.
Treatment
Prehospital Check finger-stick glucose. Give IV dextrose if possible, oral glucose if awake, or glucagon if IV access unavailable.
Initial Stabilization/Therapy ABCs with seizure and aspiration precautions.
Emergency Department Treatment/Procedures Give D50W 50 mL IV for altered mental status; repeat as needed. Start continuous dextrose infusion (D5–D20) if persistent hypoglycemia or unable to eat. Use octreotide for sulfonylurea-induced or refractory hypoglycemia. Use glucagon if IV access delayed (ineffective in alcohol-related hypoglycemia or severe liver disease). Give hydrocortisone if adrenal insufficiency suspected.
Geriatric considerations Recovery may be prolonged despite correction.
Medications
First Line D50W 25 g IVP (Zimmerman rule: adults 1 mL/kg D50W; children 2 mL/kg D25W; infants 5 mL/kg D10W).
Second Line Octreotide 50 μg IV bolus then infusion or SC dosing; glucagon 0.5–2 mg IV/IM/SC; hydrocortisone 100 mg IV. Oral glucose 20 g if awake and safe.
Follow-Up And Disposition
Admission Criteria Long-acting insulin or sulfonylurea overdose, recurrent hypoglycemia, inability to tolerate oral intake, suicidal intent, persistent neurologic symptoms, or elderly patients with severe episodes.
Discharge Criteria Mild, resolved hypoglycemia with normal glucose, symptom resolution, oral tolerance, and observation for ≥3 hr.
Issues For Referral Primary care follow-up for medication or dietary adjustment.
Follow-Up Recommendations Re-evaluation within 48 hr.
Pearls And Pitfalls
IV dextrose is preferred over oral glucose. Multiple D50 boluses are often required. Do not rely solely on D10/D20. Consider hypoglycemia in all neurologic or psychiatric presentations. Recurrent episodes may require prolonged recovery.
Basics
Description
Hypoglycemia results from deficiency of counterregulatory hormones (glucagon, epinephrine, cortisol, growth hormone) or excessive insulin response. Defined as serum glucose <70 mg />L.
Risk Factors
Strict glycemic control with insulin, prior hypoglycemia, hypoglycemia unawareness, impaired counterregulation (<5 years or elderly), renal disease, malnutrition, coronary artery liver congenital metabolic endocrine disorders, hyperinsulinism, and neonatal diabetes mellitus.< />pan>
Etiology
Increased insulin levels due to insulin or oral hypoglycemic overdose, sepsis, insulinoma, autoimmune hypoglycemia, alimentary hyperinsulinism, renal failure, or liver cirrhosis. Decreased glucose production from alcohol use, drugs (salicylates, β-blockers including eye drops, SSRIs, some antibiotics), adrenal insufficiency, malnutrition, dehydration, cerebral edema, extremes of age, heart failure, endocrine disorders, and pregnancy-related substrate deficiency.
Pediatric considerations
Most common cause in first 3 months of life is persistent hyperinsulinemic hypoglycemia of infancy, especially in infants of diabetic mothers.
Diagnosis
Signs And Symptoms Adrenergic symptoms include diaphoresis, anxiety, tachycardia, hunger, paresthesias, chest pain, and ischemic ECG changes. Neuroglycopenic symptoms include dizziness, confusion, behavioral changes, slurred speech, focal deficits, seizures, hemiplegia, coma, and CVA mimic. Neonates may present with poor feeding, irritability, tremors, seizures, or bradycardia.
Alert
Patients with hypoglycemia unawareness may present only with late findings such as seizures or coma.
History
Assess diabetes status, renal or liver disease, alcohol use, medication exposure, and possible overdose.
Physical Exam Findings reflect adrenergic or neuroglycopenic manifestations.
Essential Workup Diagnosis requires neuroglycopenic symptoms, documented low glucose, and symptom resolution after glucose administration.
Diagnosis Tests And Interpretation
Lab Blood glucose (pre- and post-treatment), electrolytes, BUN/creatinine, PT, urinalysis, cultures if infection suspected, C-peptide if exogenous insulin overdose suspected.
Imaging CXR for aspiration or pneumonia if indicated.
ECG Evaluate for ischemia or dysrhythmias.
Differential Diagnosis
Stroke/TIA, seizure, intoxication, hypoxia, sepsis, metabolic or endocrine disorders, psychiatric disease.
Pediatric Growth hormone deficiency, inborn errors of metabolism, ketotic hypoglycemia, Reye syndrome, salicylate ingestion.
Treatment
Prehospital Check finger-stick glucose. Give IV dextrose if possible, oral glucose if awake, or glucagon if IV access unavailable.
Initial Stabilization/Therapy ABCs with seizure and aspiration precautions.
Emergency Department Treatment/Procedures Give D50W 50 mL IV for altered mental status; repeat as needed. Start continuous dextrose infusion (D5–D20) if persistent hypoglycemia or unable to eat. Use octreotide for sulfonylurea-induced or refractory hypoglycemia. Use glucagon if IV access delayed (ineffective in alcohol-related hypoglycemia or severe liver disease). Give hydrocortisone if adrenal insufficiency suspected.
Geriatric considerations Recovery may be prolonged despite correction.
Medications
First Line D50W 25 g IVP (Zimmerman rule: adults 1 mL/kg D50W; children 2 mL/kg D25W; infants 5 mL/kg D10W).
Second Line Octreotide 50 μg IV bolus then infusion or SC dosing; glucagon 0.5–2 mg IV/IM/SC; hydrocortisone 100 mg IV. Oral glucose 20 g if awake and safe.
Follow-Up And Disposition
Admission Criteria Long-acting insulin or sulfonylurea overdose, recurrent hypoglycemia, inability to tolerate oral intake, suicidal intent, persistent neurologic symptoms, or elderly patients with severe episodes.
Discharge Criteria Mild, resolved hypoglycemia with normal glucose, symptom resolution, oral tolerance, and observation for ≥3 hr.
Issues For Referral Primary care follow-up for medication or dietary adjustment.
Follow-Up Recommendations Re-evaluation within 48 hr.
Pearls And Pitfalls
IV dextrose is preferred over oral glucose. Multiple D50 boluses are often required. Do not rely solely on D10/D20. Consider hypoglycemia in all neurologic or psychiatric presentations. Recurrent episodes may require prolonged recovery.
- Published on
Emergency And Acute Medicine: Hypocalcemia
Basics
Description Hypocalcemia is defined as a total plasma calcium level <8.7 mg/dL. Ionized calcium may be normal and therefore asymptomatic. Normal total serum calcium is 8.7–10.5 mg/dL.
Etiology Incidence is ~0.6% in the general population. Mechanisms include increased calcium loss from or decreased entry into the circulation. Circulating calcium exists as protein bound (45–50%, mainly albumin), complexed to anions (5–10%), and ionized free calcium (45–50%, physiologically active). Calcium homeostasis is regulated by parathyroid hormone, vitamin D (1,25-dihydroxyvitamin D), and calcitonin. Hypoalbuminemia is the most common cause; for each 1 g/dL decrease in albumin, total calcium decreases by ~0.8 mg/dL while ionized calcium remains unchanged.
Pediatric considerations Children have higher normal calcium levels (9.2–11 mg/dL). Neonatal hypocalcemia is defined as total calcium <7.5 mg/dL or ionized calcium <4 mg/dL and may present with jitteriness, tachypnea, apnea with cyanosis, and vomiting.
Diagnosis
Signs And Symptoms Occur when ionized calcium <3.2 mg/dL and depend on severity and rate of decline. Neuromuscular findings include paresthesias, hyperreflexia, muscle spasms, tetany, Chvostek sign, Trousseau sign, laryngeal stridor, seizures, and choreoathetosis. Cardiovascular effects include torsades de pointes, heart block, hypotension, impaired contractility, bradycardia, QT and ST prolongation, and T-wave abnormalities. Psychiatric manifestations include anxiety, irritability, depression, psychosis, confusion, and movement disorders. Ocular findings include papilledema and cataracts in acute cases.
Essential Workup Confirm diagnosis with serum ionized calcium level.
Diagnosis Tests And Interpretation
Lab ABG (pH changes affect ionized calcium), serum albumin, electrolytes, BUN/creatinine, glucose, magnesium, phosphate, PTH, and vitamin D metabolites as indicated.
ECG Prolonged QT interval and possible heart block.
Differential Diagnosis Impaired PTH secretion or action (post-surgical hypoparathyroidism, autoimmune or congenital hypoparathyroidism, pseudohypoparathyroidism), impaired vitamin D synthesis or action (malabsorption, renal disease), calcium sequestration or complexing (hyperphosphatemia, transfusion citrate, pancreatitis, rhabdomyolysis, alkalosis), hypomagnesemia, medications (bisphosphonates, calcitonin, phenytoin, cisplatin, PPIs), malignancy, sepsis, burns, and hungry bone syndrome after parathyroidectomy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, and cardiac monitoring.
Emergency Department Treatment/Procedures Treat symptomatic hypocalcemia as an emergency. Give IV calcium gluconate 1–2 g in 50 mL D5W over 20 min. Faster infusion may cause dysrhythmias. Follow bolus with continuous infusion (0.5–1.5 mg/kg/hr elemental calcium). Do not mix calcium with bicarbonate or phosphate. Monitor calcium every 1–4 hr and titrate to symptoms or ECG changes. Correct hypomagnesemia if present (Mg 2 g IV). Use caution in patients on digoxin.
Chronic management Oral calcium 1.5–2 g/day (up to 4 g/day if malabsorption) plus vitamin D supplementation. Calcitriol is preferred for rapid onset.
Medications
IV calcium Calcium gluconate, calcium chloride, or calcium gluceptate (dose by elemental calcium).
Oral calcium Calcium carbonate, citrate, gluconate, lactate, or glubionate.
Vitamin D Calcitriol, ergocalciferol, or related preparations as indicated.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ionized calcium <3.2 mg/dL, or need for continuous IV calcium.
Discharge Criteria Asymptomatic patients with ionized calcium >3.2 mg/dL and no significant comorbidities.
Follow-Up Recommendations Endocrinology follow-up for disorders of PTH or vitamin D metabolism.
Pearls And Pitfalls Hypocalcemia has multiple causes; treatment depends on severity and etiology. Severe symptoms require IV calcium. Hypocalcemia will not correct if magnesium deficiency is not treated first.
Basics
Description Hypocalcemia is defined as a total plasma calcium level <8.7 mg/dL. Ionized calcium may be normal and therefore asymptomatic. Normal total serum calcium is 8.7–10.5 mg/dL.
Etiology Incidence is ~0.6% in the general population. Mechanisms include increased calcium loss from or decreased entry into the circulation. Circulating calcium exists as protein bound (45–50%, mainly albumin), complexed to anions (5–10%), and ionized free calcium (45–50%, physiologically active). Calcium homeostasis is regulated by parathyroid hormone, vitamin D (1,25-dihydroxyvitamin D), and calcitonin. Hypoalbuminemia is the most common cause; for each 1 g/dL decrease in albumin, total calcium decreases by ~0.8 mg/dL while ionized calcium remains unchanged.
Pediatric considerations Children have higher normal calcium levels (9.2–11 mg/dL). Neonatal hypocalcemia is defined as total calcium <7.5 mg/dL or ionized calcium <4 mg/dL and may present with jitteriness, tachypnea, apnea with cyanosis, and vomiting.
Diagnosis
Signs And Symptoms Occur when ionized calcium <3.2 mg/dL and depend on severity and rate of decline. Neuromuscular findings include paresthesias, hyperreflexia, muscle spasms, tetany, Chvostek sign, Trousseau sign, laryngeal stridor, seizures, and choreoathetosis. Cardiovascular effects include torsades de pointes, heart block, hypotension, impaired contractility, bradycardia, QT and ST prolongation, and T-wave abnormalities. Psychiatric manifestations include anxiety, irritability, depression, psychosis, confusion, and movement disorders. Ocular findings include papilledema and cataracts in acute cases.
Essential Workup Confirm diagnosis with serum ionized calcium level.
Diagnosis Tests And Interpretation
Lab ABG (pH changes affect ionized calcium), serum albumin, electrolytes, BUN/creatinine, glucose, magnesium, phosphate, PTH, and vitamin D metabolites as indicated.
ECG Prolonged QT interval and possible heart block.
Differential Diagnosis Impaired PTH secretion or action (post-surgical hypoparathyroidism, autoimmune or congenital hypoparathyroidism, pseudohypoparathyroidism), impaired vitamin D synthesis or action (malabsorption, renal disease), calcium sequestration or complexing (hyperphosphatemia, transfusion citrate, pancreatitis, rhabdomyolysis, alkalosis), hypomagnesemia, medications (bisphosphonates, calcitonin, phenytoin, cisplatin, PPIs), malignancy, sepsis, burns, and hungry bone syndrome after parathyroidectomy.
Treatment
Initial Stabilization/Therapy ABCs, IV access, and cardiac monitoring.
Emergency Department Treatment/Procedures Treat symptomatic hypocalcemia as an emergency. Give IV calcium gluconate 1–2 g in 50 mL D5W over 20 min. Faster infusion may cause dysrhythmias. Follow bolus with continuous infusion (0.5–1.5 mg/kg/hr elemental calcium). Do not mix calcium with bicarbonate or phosphate. Monitor calcium every 1–4 hr and titrate to symptoms or ECG changes. Correct hypomagnesemia if present (Mg 2 g IV). Use caution in patients on digoxin.
Chronic management Oral calcium 1.5–2 g/day (up to 4 g/day if malabsorption) plus vitamin D supplementation. Calcitriol is preferred for rapid onset.
Medications
IV calcium Calcium gluconate, calcium chloride, or calcium gluceptate (dose by elemental calcium).
Oral calcium Calcium carbonate, citrate, gluconate, lactate, or glubionate.
Vitamin D Calcitriol, ergocalciferol, or related preparations as indicated.
Follow-Up And Disposition
Admission Criteria Symptomatic hypocalcemia, ionized calcium <3.2 mg/dL, or need for continuous IV calcium.
Discharge Criteria Asymptomatic patients with ionized calcium >3.2 mg/dL and no significant comorbidities.
Follow-Up Recommendations Endocrinology follow-up for disorders of PTH or vitamin D metabolism.
Pearls And Pitfalls Hypocalcemia has multiple causes; treatment depends on severity and etiology. Severe symptoms require IV calcium. Hypocalcemia will not correct if magnesium deficiency is not treated first.

- Published on
Emergency And Acute Medicine: Hyphema
Basics
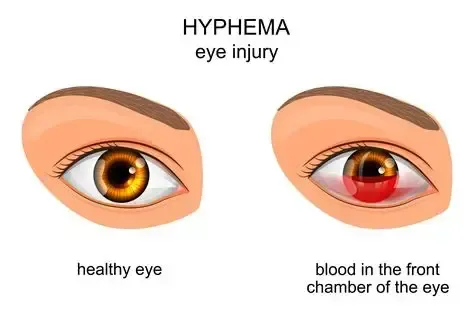
Description Blood in the anterior chamber of the eye between the iris and cornea. Hyphema refers to grossly visible layered blood. Microhyphema refers to suspended red blood cells seen only on slit-lamp exam. Genetic predisposition is related to hereditary blood dyscrasias.
Etiology Blunt trauma is the most common cause (70–80%) due to anteroposterior compression with equatorial globe expansion causing rupture of iris or ciliary body vessels. Penetrating trauma causes direct vessel injury or sudden ocular decompression. Spontaneous causes include ocular tumors (melanoma, retinoblastoma, xanthogranuloma, metastatic tumors), blood dyscrasias (hemophilia, leukemia, thrombocytopenia, von Willebrand disease), anticoagulant or antiplatelet use (aspirin, warfarin, heparin), iris neovascularization (proliferative diabetic retinopathy, retinal vein occlusion, carotid stenosis), and postsurgical causes such as cataract extraction, trabeculectomy, or vitrectomy. In children without trauma, suspect nonaccidental injury.
Diagnosis
Signs And Symptoms Photophobia, blurred vision, decreased visual acuity, ocular pain, nausea, and vomiting.
History Assess prior visual acuity, prior ocular surgery or glaucoma treatment, bleeding disorders including sickle cell disease, mechanism and timing of injury, onset of visual loss, and history of excessive tearing (suggestive of open globe injury).
Physical Exam Perform full trauma exam. Look for periorbital ecchymosis, eyelid lacerations, enophthalmos, limited ocular movement with diplopia, or proptosis. Ocular exam includes visual acuity, exclusion of open globe injury before tonometry, pupillary response, slit-lamp exam, and dilated fundus exam without pressure on the globe. Hyphema grading: Grade I <1/3 AC, Grade II 1/3–1/2 AC, Grade III >1/2 AC, Grade IV total (“8-ball” hyphema). Higher grades have increased risk of rebleeding, glaucoma, corneal staining, and poor visual recovery.
Diagnosis Tests And Interpretation
Lab Obtain platelet count, PT/PTT if bleeding disorder or anticoagulant use is suspected. Screen for sickle cell disease when indicated.
Imaging CT orbits for suspected open globe, intraocular foreign body, or orbital fracture. B-scan ultrasound only if globe integrity is confirmed and posterior structures cannot be visualized.
Essential Workup Visual acuity, globe integrity, intraocular pressure, assessment for associated injuries, targeted labs, and imaging when indicated.
Differential Diagnosis Uveitis, endophthalmitis.
Treatment
Prehospital Place eye shield if open globe is suspected.
Initial Stabilization/Therapy Keep head elevated, limit activity, avoid straining, place rigid eye shield, and avoid eye patching.
Emergency Department Treatment/Procedures Provide mild analgesia (avoid NSAIDs) and antiemetics. Use cycloplegics (atropine 1% or cyclopentolate 1%) and topical steroids (prednisolone acetate 1%). Aminocaproic acid may be used in consultation with ophthalmology. Oral prednisone may be indicated in selected high-risk cases. Manage elevated intraocular pressure with topical beta-blockers first, then alpha-agonists, carbonic anhydrase inhibitors, and systemic agents if needed. Avoid carbonic anhydrase inhibitors and mannitol in sickle cell disease. Surgical evacuation is indicated for uncontrolled intraocular pressure.
Medications
First Line Atropine 1% TID, prednisolone acetate 1% QID.
Second Line Timolol or levobunolol, brimonidine or apraclonidine, dorzolamide or brinzolamide, acetazolamide.
Follow-Up And Disposition
Admission Criteria Uncontrolled intraocular pressure, open globe injury, noncompliance, associated injuries, children <7 years, or high-risk conditions such as sickle cell disease or hemophilia.
Discharge Criteria Controlled intraocular pressure and absence of admission criteria.
Follow-Up Recommendations Daily ophthalmology follow-up for the first 3 days to monitor for rebleeding, corneal staining, and pressure elevation.
Pearls And Pitfalls Always exclude ruptured globe before tonometry or treatment. Intraocular pressure reduction is not immediate. Screen for sickle cell disease in at-risk populations.
Basics
Description Blood in the anterior chamber of the eye between the iris and cornea. Hyphema refers to grossly visible layered blood. Microhyphema refers to suspended red blood cells seen only on slit-lamp exam. Genetic predisposition is related to hereditary blood dyscrasias.
Etiology Blunt trauma is the most common cause (70–80%) due to anteroposterior compression with equatorial globe expansion causing rupture of iris or ciliary body vessels. Penetrating trauma causes direct vessel injury or sudden ocular decompression. Spontaneous causes include ocular tumors (melanoma, retinoblastoma, xanthogranuloma, metastatic tumors), blood dyscrasias (hemophilia, leukemia, thrombocytopenia, von Willebrand disease), anticoagulant or antiplatelet use (aspirin, warfarin, heparin), iris neovascularization (proliferative diabetic retinopathy, retinal vein occlusion, carotid stenosis), and postsurgical causes such as cataract extraction, trabeculectomy, or vitrectomy. In children without trauma, suspect nonaccidental injury.
Diagnosis
Signs And Symptoms Photophobia, blurred vision, decreased visual acuity, ocular pain, nausea, and vomiting.
History Assess prior visual acuity, prior ocular surgery or glaucoma treatment, bleeding disorders including sickle cell disease, mechanism and timing of injury, onset of visual loss, and history of excessive tearing (suggestive of open globe injury).
Physical Exam Perform full trauma exam. Look for periorbital ecchymosis, eyelid lacerations, enophthalmos, limited ocular movement with diplopia, or proptosis. Ocular exam includes visual acuity, exclusion of open globe injury before tonometry, pupillary response, slit-lamp exam, and dilated fundus exam without pressure on the globe. Hyphema grading: Grade I <1/3 AC, Grade II 1/3–1/2 AC, Grade III >1/2 AC, Grade IV total (“8-ball” hyphema). Higher grades have increased risk of rebleeding, glaucoma, corneal staining, and poor visual recovery.
Diagnosis Tests And Interpretation
Lab Obtain platelet count, PT/PTT if bleeding disorder or anticoagulant use is suspected. Screen for sickle cell disease when indicated.
Imaging CT orbits for suspected open globe, intraocular foreign body, or orbital fracture. B-scan ultrasound only if globe integrity is confirmed and posterior structures cannot be visualized.
Essential Workup Visual acuity, globe integrity, intraocular pressure, assessment for associated injuries, targeted labs, and imaging when indicated.
Differential Diagnosis Uveitis, endophthalmitis.
Treatment
Prehospital Place eye shield if open globe is suspected.
Initial Stabilization/Therapy Keep head elevated, limit activity, avoid straining, place rigid eye shield, and avoid eye patching.
Emergency Department Treatment/Procedures Provide mild analgesia (avoid NSAIDs) and antiemetics. Use cycloplegics (atropine 1% or cyclopentolate 1%) and topical steroids (prednisolone acetate 1%). Aminocaproic acid may be used in consultation with ophthalmology. Oral prednisone may be indicated in selected high-risk cases. Manage elevated intraocular pressure with topical beta-blockers first, then alpha-agonists, carbonic anhydrase inhibitors, and systemic agents if needed. Avoid carbonic anhydrase inhibitors and mannitol in sickle cell disease. Surgical evacuation is indicated for uncontrolled intraocular pressure.
Medications
First Line Atropine 1% TID, prednisolone acetate 1% QID.
Second Line Timolol or levobunolol, brimonidine or apraclonidine, dorzolamide or brinzolamide, acetazolamide.
Follow-Up And Disposition
Admission Criteria Uncontrolled intraocular pressure, open globe injury, noncompliance, associated injuries, children <7 years, or high-risk conditions such as sickle cell disease or hemophilia.
Discharge Criteria Controlled intraocular pressure and absence of admission criteria.
Follow-Up Recommendations Daily ophthalmology follow-up for the first 3 days to monitor for rebleeding, corneal staining, and pressure elevation.
Pearls And Pitfalls Always exclude ruptured globe before tonometry or treatment. Intraocular pressure reduction is not immediate. Screen for sickle cell disease in at-risk populations.
- Published on
Emergency And Acute Medicine: Hyperviscosity Syndrome
Basics
Description Hyperviscosity syndrome is the clinical consequence of increased blood viscosity leading to impaired microcirculatory flow and reduced tissue oxygen delivery. As viscosity rises, greater cardiac output is required to maintain perfusion, yet oxygen delivery worsens because blood transit through the microcirculation slows. The classic clinical presentation is a triad of mucosal bleeding, visual disturbances, and neurologic symptoms.
Etiology Hyperviscosity results from elevation of cellular or acellular blood components. Acellular (protein) hyperviscosity is the most common cause (85–90%) and is usually due to increased gamma globulins from monoclonal gammopathies such as Waldenström macroglobulinemia and multiple myeloma; polyclonal gammopathies from rheumatologic disease are rare. Cellular hyperviscosity (10–15%) occurs with markedly increased blood cells, including erythrocytosis in polycythemia vera, extreme leukocytosis (>100,000) in acute or chronic leukemia, and severe thrombocytosis.
Diagnosis
Signs and symptoms The classic triad includes bleeding, visual changes, and neurologic dysfunction. Hematologic manifestations are most common and include epistaxis, gingival, rectal, or uterine bleeding, prolonged postprocedural bleeding, and pruritus. Ocular findings include blurred vision, diplopia, visual loss, and characteristic funduscopic changes such as the “link-sausage” appearance of retinal veins, retinal hemorrhages, exudates, microaneurysms, and papilledema. Neurologic symptoms include headache, dizziness, vertigo, ataxia, tinnitus, hearing loss, paresthesias, peripheral neuropathy, seizures, altered mental status, coma, and intracranial hemorrhage. Renal manifestations include hematuria, sterile pyuria, and nephritic or nephrotic syndromes. Cardiovascular findings may include angina, myocardial infarction, dysrhythmias, and heart failure. Dermatologic features include Raynaud phenomenon, livedo reticularis, palpable purpura, digital infarcts, and peripheral gangrene.
History Suspect hyperviscosity syndrome in patients with the classic triad, known immunoglobulin-producing disorders, or hypercellular hematologic diseases presenting with microvascular ischemia or cardiac decompensation.
Physical exam No pathognomonic findings exist; exam reflects end-organ involvement such as mucosal bleeding, petechiae, focal neurologic deficits, heart failure signs, or abnormal funduscopic findings.
Essential workup Assess for bleeding and end-organ ischemia. Measure serum or whole blood viscosity when available. Suspect the diagnosis when laboratory processing is difficult due to serum stasis or analyzer obstruction from viscous samples.
Diagnosis tests and interpretation
Laboratory Obtain CBC with differential to assess anemia, erythrocytosis, leukocytosis, or thrombocytosis; normocytic normochromic anemia is common. Peripheral smear may show rouleaux formation, a key diagnostic clue. Check electrolytes, BUN, creatinine, and glucose; renal dysfunction is common, and pseudohyponatremia or hypercalcemia may occur in multiple myeloma. Urinalysis may show proteinuria or hematuria. Obtain coagulation studies. Perform serum and urine protein electrophoresis. Serum viscosity measurement (when available) is diagnostic; normal relative viscosity is 1.4–1.8, and symptoms usually develop at ≥4 centipoise.
Imaging Head CT is indicated in patients with neurologic symptoms to exclude intracranial hemorrhage.
Differential diagnosis Platelet disorders, inherited or acquired coagulation factor deficiencies, liver disease, vitamin K deficiency, and disseminated intravascular coagulation.
Treatment
Prehospital Initiate IV fluid resuscitation in patients with bleeding or suspected hypovolemia.
Initial stabilization/therapy Rehydrate with isotonic saline. Bleeding or ischemia often does not respond to routine therapy and requires viscosity reduction. In patients with anemia and leukemia, avoid transfusion before plasmapheresis as it may worsen viscosity.
Emergency department management Provide supportive care and obtain early hematology consultation. Phlebotomy is a temporizing measure in severe cases with coma or seizures when plasmapheresis is not immediately available; remove 100–200 mL of whole blood and replace with isotonic saline, ideally after consultation, and is first-line in polycythemia vera. Plasmapheresis or leukapheresis is definitive therapy; typical volumes are 40 mL/kg in stable patients and up to 60 mL/kg in critically ill patients. Multiple sessions are often required. Monitor for hypocalcemia from citrate anticoagulation and rare dysrhythmias. Leukapheresis is preferred for hyperleukocytosis. ED clinicians may assist by establishing large-bore central access with caution due to bleeding risk.
Follow-up and disposition
Admission criteria Admit all patients with symptomatic hyperviscosity or evidence of bleeding or end-organ ischemia; ICU admission is indicated for hemorrhage, altered mental status, or acute myocardial infarction.
Discharge criteria Discharge only after definitive treatment of the underlying disorder and symptom resolution.
Issues for referral All patients require hematology consultation.
Key points Avoid diuretics as they can worsen viscosity. The hallmark triad consists of visual disturbances, bleeding, and neurologic symptoms. Early recognition and rapid viscosity reduction are critical to prevent irreversible end-organ damage.
Basics
Description Hyperviscosity syndrome is the clinical consequence of increased blood viscosity leading to impaired microcirculatory flow and reduced tissue oxygen delivery. As viscosity rises, greater cardiac output is required to maintain perfusion, yet oxygen delivery worsens because blood transit through the microcirculation slows. The classic clinical presentation is a triad of mucosal bleeding, visual disturbances, and neurologic symptoms.
Etiology Hyperviscosity results from elevation of cellular or acellular blood components. Acellular (protein) hyperviscosity is the most common cause (85–90%) and is usually due to increased gamma globulins from monoclonal gammopathies such as Waldenström macroglobulinemia and multiple myeloma; polyclonal gammopathies from rheumatologic disease are rare. Cellular hyperviscosity (10–15%) occurs with markedly increased blood cells, including erythrocytosis in polycythemia vera, extreme leukocytosis (>100,000) in acute or chronic leukemia, and severe thrombocytosis.
Diagnosis
Signs and symptoms The classic triad includes bleeding, visual changes, and neurologic dysfunction. Hematologic manifestations are most common and include epistaxis, gingival, rectal, or uterine bleeding, prolonged postprocedural bleeding, and pruritus. Ocular findings include blurred vision, diplopia, visual loss, and characteristic funduscopic changes such as the “link-sausage” appearance of retinal veins, retinal hemorrhages, exudates, microaneurysms, and papilledema. Neurologic symptoms include headache, dizziness, vertigo, ataxia, tinnitus, hearing loss, paresthesias, peripheral neuropathy, seizures, altered mental status, coma, and intracranial hemorrhage. Renal manifestations include hematuria, sterile pyuria, and nephritic or nephrotic syndromes. Cardiovascular findings may include angina, myocardial infarction, dysrhythmias, and heart failure. Dermatologic features include Raynaud phenomenon, livedo reticularis, palpable purpura, digital infarcts, and peripheral gangrene.
History Suspect hyperviscosity syndrome in patients with the classic triad, known immunoglobulin-producing disorders, or hypercellular hematologic diseases presenting with microvascular ischemia or cardiac decompensation.
Physical exam No pathognomonic findings exist; exam reflects end-organ involvement such as mucosal bleeding, petechiae, focal neurologic deficits, heart failure signs, or abnormal funduscopic findings.
Essential workup Assess for bleeding and end-organ ischemia. Measure serum or whole blood viscosity when available. Suspect the diagnosis when laboratory processing is difficult due to serum stasis or analyzer obstruction from viscous samples.
Diagnosis tests and interpretation
Laboratory Obtain CBC with differential to assess anemia, erythrocytosis, leukocytosis, or thrombocytosis; normocytic normochromic anemia is common. Peripheral smear may show rouleaux formation, a key diagnostic clue. Check electrolytes, BUN, creatinine, and glucose; renal dysfunction is common, and pseudohyponatremia or hypercalcemia may occur in multiple myeloma. Urinalysis may show proteinuria or hematuria. Obtain coagulation studies. Perform serum and urine protein electrophoresis. Serum viscosity measurement (when available) is diagnostic; normal relative viscosity is 1.4–1.8, and symptoms usually develop at ≥4 centipoise.
Imaging Head CT is indicated in patients with neurologic symptoms to exclude intracranial hemorrhage.
Differential diagnosis Platelet disorders, inherited or acquired coagulation factor deficiencies, liver disease, vitamin K deficiency, and disseminated intravascular coagulation.
Treatment
Prehospital Initiate IV fluid resuscitation in patients with bleeding or suspected hypovolemia.
Initial stabilization/therapy Rehydrate with isotonic saline. Bleeding or ischemia often does not respond to routine therapy and requires viscosity reduction. In patients with anemia and leukemia, avoid transfusion before plasmapheresis as it may worsen viscosity.
Emergency department management Provide supportive care and obtain early hematology consultation. Phlebotomy is a temporizing measure in severe cases with coma or seizures when plasmapheresis is not immediately available; remove 100–200 mL of whole blood and replace with isotonic saline, ideally after consultation, and is first-line in polycythemia vera. Plasmapheresis or leukapheresis is definitive therapy; typical volumes are 40 mL/kg in stable patients and up to 60 mL/kg in critically ill patients. Multiple sessions are often required. Monitor for hypocalcemia from citrate anticoagulation and rare dysrhythmias. Leukapheresis is preferred for hyperleukocytosis. ED clinicians may assist by establishing large-bore central access with caution due to bleeding risk.
Follow-up and disposition
Admission criteria Admit all patients with symptomatic hyperviscosity or evidence of bleeding or end-organ ischemia; ICU admission is indicated for hemorrhage, altered mental status, or acute myocardial infarction.
Discharge criteria Discharge only after definitive treatment of the underlying disorder and symptom resolution.
Issues for referral All patients require hematology consultation.
Key points Avoid diuretics as they can worsen viscosity. The hallmark triad consists of visual disturbances, bleeding, and neurologic symptoms. Early recognition and rapid viscosity reduction are critical to prevent irreversible end-organ damage.
- Published on
Emergency And Acute Medicine: Hyperventilation Syndrome
Basics
Description Hyperventilation syndrome is a clinical constellation of symptoms most commonly including dyspnea, chest pain, lightheadedness, and paresthesias. Symptoms result from a nonphysiologic increase in minute ventilation due to increased respiratory rate and/or increased tidal volume such as frequent sighing. The diagnosis can only be made after excluding physiologic and pathologic causes of hyperventilation. It affects approximately 10–15% of the general population and is more common in women, possibly related to progesterone effects.
Etiology The precise mechanism is unclear. Episodes are most often triggered by psychological stressors. Proposed contributing mechanisms include hypocapnia, hypophosphatemia, and hypocalcemia, although their exact roles remain controversial.
Diagnosis
Signs and symptoms
History Patients often report prior similar episodes, identifiable triggers, duration of symptoms, time of onset during the day, and response to previous treatments.
Cardiac Chest pain, dyspnea, air hunger, palpitations.
Neurologic Dizziness, lightheadedness, syncope, paresthesias, headache, carpopedal spasm, tetany.
Psychiatric Anxiety, intense fear, giddiness, depersonalization, sense of unreality.
General Fatigue, weakness, malaise.
Physical exam Findings are often minimal. Tachypnea is common but not universal, as some patients hyperventilate by increasing tidal volume rather than respiratory rate. Carpopedal spasm may be prominent, and Chvostek sign may be present.
Essential workup Hyperventilation syndrome is a diagnosis of exclusion. A careful history and physical examination are essential. Vital signs including pulse oximetry should be obtained; oxygen saturation is normal in isolated hyperventilation syndrome.
Diagnosis tests and interpretation
Laboratory Obtain arterial blood gas analysis if hypoxia is present. Check electrolytes, BUN, creatinine, and glucose when metabolic acidosis or diabetic ketoacidosis is suspected.
ECG Perform when chest pain or palpitations are present.
Imaging Chest radiograph is indicated in patients with hypoxia or focal lung findings.
Diagnostic procedures A hyperventilation provocation test may be attempted after symptom resolution by voluntary overbreathing for three minutes. Reproduction of symptoms may help patient understanding, though diagnostic accuracy is debated.
Differential diagnosis
Pathologic Asthma, congestive heart failure, pulmonary embolism, pneumonia, severe pain, CNS lesions, metabolic acidosis including DKA, pulmonary hypertension, hypoglycemia, drug intoxication such as salicylates, and withdrawal syndromes including alcohol or benzodiazepines.
Physiologic Pregnancy, fever, altitude exposure.
Treatment
Prehospital Patients with abnormal vital signs require IV access and pulse oximetry. Provide supplemental oxygen only if hypoxic.
Initial stabilization/therapy Establish monitoring and initiate evaluation and treatment for suspected physiologic or pathologic causes.
Emergency department management If evaluation excludes organic causes and history is consistent, initiate treatment for hyperventilation syndrome. Reassurance, calm explanation, and coaching often result in rapid symptom resolution. Paper bag rebreathing should not be used, as it is unsupported by evidence and may be dangerous in patients with hypoxia or occult pathology. Address underlying psychological stressors and assess for psychiatric risk including suicidal ideation. Short-acting anxiolytics may be used to interrupt the anxiety–hyperventilation cycle when symptoms persist.
Medication Benzodiazepines such as alprazolam 0.25–0.5 mg PO, lorazepam 1–2 mg PO or IV, or diazepam 2–5 mg PO or IV. Outpatient options include buspirone 5 mg PO three times daily or diazepam 2–5 mg PO two to four times daily for selected patients.
Follow-up and disposition
Admission criteria Hyperventilation syndrome alone does not require hospital admission.
Discharge criteria Pathologic and physiologic causes have been excluded or treated, no acute psychiatric concerns are present, and reliable follow-up is available.
Follow-up recommendations Arrange primary care follow-up and assess the need for psychiatric referral.
Key points Always exclude organic causes before diagnosing hyperventilation syndrome. Isolated hyperventilation syndrome does not cause hypoxia. Avoid paper bag rebreathing due to potential harm.
Basics
Description Hyperventilation syndrome is a clinical constellation of symptoms most commonly including dyspnea, chest pain, lightheadedness, and paresthesias. Symptoms result from a nonphysiologic increase in minute ventilation due to increased respiratory rate and/or increased tidal volume such as frequent sighing. The diagnosis can only be made after excluding physiologic and pathologic causes of hyperventilation. It affects approximately 10–15% of the general population and is more common in women, possibly related to progesterone effects.
Etiology The precise mechanism is unclear. Episodes are most often triggered by psychological stressors. Proposed contributing mechanisms include hypocapnia, hypophosphatemia, and hypocalcemia, although their exact roles remain controversial.
Diagnosis
Signs and symptoms
History Patients often report prior similar episodes, identifiable triggers, duration of symptoms, time of onset during the day, and response to previous treatments.
Cardiac Chest pain, dyspnea, air hunger, palpitations.
Neurologic Dizziness, lightheadedness, syncope, paresthesias, headache, carpopedal spasm, tetany.
Psychiatric Anxiety, intense fear, giddiness, depersonalization, sense of unreality.
General Fatigue, weakness, malaise.
Physical exam Findings are often minimal. Tachypnea is common but not universal, as some patients hyperventilate by increasing tidal volume rather than respiratory rate. Carpopedal spasm may be prominent, and Chvostek sign may be present.
Essential workup Hyperventilation syndrome is a diagnosis of exclusion. A careful history and physical examination are essential. Vital signs including pulse oximetry should be obtained; oxygen saturation is normal in isolated hyperventilation syndrome.
Diagnosis tests and interpretation
Laboratory Obtain arterial blood gas analysis if hypoxia is present. Check electrolytes, BUN, creatinine, and glucose when metabolic acidosis or diabetic ketoacidosis is suspected.
ECG Perform when chest pain or palpitations are present.
Imaging Chest radiograph is indicated in patients with hypoxia or focal lung findings.
Diagnostic procedures A hyperventilation provocation test may be attempted after symptom resolution by voluntary overbreathing for three minutes. Reproduction of symptoms may help patient understanding, though diagnostic accuracy is debated.
Differential diagnosis
Pathologic Asthma, congestive heart failure, pulmonary embolism, pneumonia, severe pain, CNS lesions, metabolic acidosis including DKA, pulmonary hypertension, hypoglycemia, drug intoxication such as salicylates, and withdrawal syndromes including alcohol or benzodiazepines.
Physiologic Pregnancy, fever, altitude exposure.
Treatment
Prehospital Patients with abnormal vital signs require IV access and pulse oximetry. Provide supplemental oxygen only if hypoxic.
Initial stabilization/therapy Establish monitoring and initiate evaluation and treatment for suspected physiologic or pathologic causes.
Emergency department management If evaluation excludes organic causes and history is consistent, initiate treatment for hyperventilation syndrome. Reassurance, calm explanation, and coaching often result in rapid symptom resolution. Paper bag rebreathing should not be used, as it is unsupported by evidence and may be dangerous in patients with hypoxia or occult pathology. Address underlying psychological stressors and assess for psychiatric risk including suicidal ideation. Short-acting anxiolytics may be used to interrupt the anxiety–hyperventilation cycle when symptoms persist.
Medication Benzodiazepines such as alprazolam 0.25–0.5 mg PO, lorazepam 1–2 mg PO or IV, or diazepam 2–5 mg PO or IV. Outpatient options include buspirone 5 mg PO three times daily or diazepam 2–5 mg PO two to four times daily for selected patients.
Follow-up and disposition
Admission criteria Hyperventilation syndrome alone does not require hospital admission.
Discharge criteria Pathologic and physiologic causes have been excluded or treated, no acute psychiatric concerns are present, and reliable follow-up is available.
Follow-up recommendations Arrange primary care follow-up and assess the need for psychiatric referral.
Key points Always exclude organic causes before diagnosing hyperventilation syndrome. Isolated hyperventilation syndrome does not cause hypoxia. Avoid paper bag rebreathing due to potential harm.
- Published on
KembaraXtra-Emergency and Acute Medicine: Hydatidiform Mole
Basics
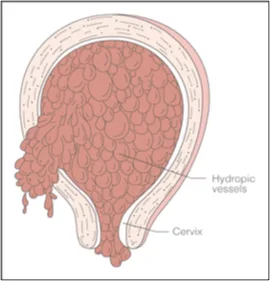
Description Hydatidiform mole is a noninvasive, localized tumor arising from trophoblastic tissue and may be associated with malignancy. Twinning with a normal pregnancy is possible but carries a higher risk of persistent maternal disease and metastasis, although a normal infant may occasionally result. Complete mole occurs in ~1/1,500 pregnancies, with no fetal tissue, diffuse chorionic villi swelling, and diffuse trophoblastic hyperplasia; malignancy develops in 15–20% (commonly lung). Genetics are typically 46,XX (90%) or 46,XY (10%) with paternal-only DNA due to fertilization of an enucleated ovum by two sperm or duplication of a haploid sperm. Partial mole occurs in ~1/750 pregnancies, often with fetal or embryonic tissue, focal villous swelling, and focal trophoblastic hyperplasia; malignancy risk is 4–12%. Genetics are usually triploid (69XXX, 69XXY, rarely 69XYY) with both maternal and paternal DNA.
Etiology Largely unknown. Risk factors include extremes of maternal age (>35 years with 5–10× risk; <20 years), prior molar pregnancy (1–2% recurrence), higher prevalence in Asian and Latin American regions, dietary deficiency of animal fat and vitamin A, smoking (>15 cigarettes/day), maternal blood types AB/A/B, infertility or nulliparity, and occurrence in ~1 of 600 therapeutic abortions.
Diagnosis
Signs and symptoms Usually exaggerated pregnancy symptoms. Complete mole commonly presents with painless vaginal bleeding (97%) described as “prune juice,” passage of grapelike vesicles, hyperemesis from high β-hCG, preeclampsia (27%), hyperthyroidism (7%), and acute respiratory distress (2%) from trophoblastic emboli or related cardiopulmonary effects. Partial mole often resembles threatened or spontaneous abortion with vaginal bleeding, possible fetal heart tones, and later presentation.
History Missed menses, positive pregnancy test, nausea, vomiting, vaginal bleeding.
Physical exam Uterine size–date discrepancy in 50–66% (larger in complete, smaller in partial). Ovarian enlargement with bilateral theca lutein cysts is common in complete moles.
Essential workup
Laboratory β-hCG (often >100,000 mIU/mL in complete moles; lower in partial; >40,000 mIU/mL indicates poorer prognosis), blood type/Rh and cross-match, CBC, coagulation profile, electrolytes with BUN/creatinine, LFTs, TSH/free T4 if hyperthyroidism suspected, urinalysis for proteinuria.
Imaging
Ultrasound shows a “snowstorm” pattern with absent fetus and no amniotic fluid in complete moles and a “Swiss-cheese” placental appearance with possible fetus in partial moles. Chest X-ray assesses pulmonary edema and metastatic disease.
Pathology
All products of conception require histology. Complete moles show edematous villi with diffuse trophoblastic hyperplasia; partial moles show fetal tissue, vessels, amnion, and edematous villi.
Differential diagnosis
Threatened, missed, or incomplete abortion; ectopic pregnancy; hyperthyroidism; hyperemesis gravidarum; hypertension and preeclampsia.
Treatment
Prehospital Secure airway, provide oxygen, establish IV access, treat seizures with benzodiazepines, and save passed tissue.
Initial stabilization IV access, cardiac monitoring, and blood preparation if evacuation is planned.
Emergency department management Intubate for respiratory distress; give β-blockers before evacuation for hyperthyroidism; manage preeclampsia/eclampsia with benzodiazepines and magnesium sulfate and control blood pressure with hydralazine or labetalol; transfuse blood products for coagulopathy; administer Rho(D) immune globulin; perform suction curettage (fertility-sparing and curative in ~80%) with oxytocin; consider chemoprophylaxis only in selected high-risk cases with reliable follow-up; consider hysterectomy for older patients, those not desiring fertility, or high-risk disease.
Follow-up and disposition
Admission criteria Uterine size >16 weeks, clinical preeclampsia/hyperthyroidism/respiratory distress, hemodynamic instability, partial mole, or hysterectomy.
Discharge criteria Uncomplicated curettage of a small, low-risk mole with reliable follow-up.
Follow-up recommendations Close OB-GYN follow-up with serial β-hCG weekly for ≥4 weeks then monthly until undetectable; any rise prompts evaluation for metastasis. Use contraception and avoid pregnancy for 12 months; perform early ultrasound in future pregnancies. Recurrence risk is 1–1.5% after one mole and up to 20% after two.
Pearls and pitfalls Diagnosis may be missed with apparent normal pregnancy, preeclampsia before 24 weeks, or severe hyperemesis. Strict β-hCG follow-up is essential; up to 20% may develop malignancy if not monitored.
Basics
Description Hydatidiform mole is a noninvasive, localized tumor arising from trophoblastic tissue and may be associated with malignancy. Twinning with a normal pregnancy is possible but carries a higher risk of persistent maternal disease and metastasis, although a normal infant may occasionally result. Complete mole occurs in ~1/1,500 pregnancies, with no fetal tissue, diffuse chorionic villi swelling, and diffuse trophoblastic hyperplasia; malignancy develops in 15–20% (commonly lung). Genetics are typically 46,XX (90%) or 46,XY (10%) with paternal-only DNA due to fertilization of an enucleated ovum by two sperm or duplication of a haploid sperm. Partial mole occurs in ~1/750 pregnancies, often with fetal or embryonic tissue, focal villous swelling, and focal trophoblastic hyperplasia; malignancy risk is 4–12%. Genetics are usually triploid (69XXX, 69XXY, rarely 69XYY) with both maternal and paternal DNA.
Etiology Largely unknown. Risk factors include extremes of maternal age (>35 years with 5–10× risk; <20 years), prior molar pregnancy (1–2% recurrence), higher prevalence in Asian and Latin American regions, dietary deficiency of animal fat and vitamin A, smoking (>15 cigarettes/day), maternal blood types AB/A/B, infertility or nulliparity, and occurrence in ~1 of 600 therapeutic abortions.
Diagnosis
Signs and symptoms Usually exaggerated pregnancy symptoms. Complete mole commonly presents with painless vaginal bleeding (97%) described as “prune juice,” passage of grapelike vesicles, hyperemesis from high β-hCG, preeclampsia (27%), hyperthyroidism (7%), and acute respiratory distress (2%) from trophoblastic emboli or related cardiopulmonary effects. Partial mole often resembles threatened or spontaneous abortion with vaginal bleeding, possible fetal heart tones, and later presentation.
History Missed menses, positive pregnancy test, nausea, vomiting, vaginal bleeding.
Physical exam Uterine size–date discrepancy in 50–66% (larger in complete, smaller in partial). Ovarian enlargement with bilateral theca lutein cysts is common in complete moles.
Essential workup
Laboratory β-hCG (often >100,000 mIU/mL in complete moles; lower in partial; >40,000 mIU/mL indicates poorer prognosis), blood type/Rh and cross-match, CBC, coagulation profile, electrolytes with BUN/creatinine, LFTs, TSH/free T4 if hyperthyroidism suspected, urinalysis for proteinuria.
Imaging
Ultrasound shows a “snowstorm” pattern with absent fetus and no amniotic fluid in complete moles and a “Swiss-cheese” placental appearance with possible fetus in partial moles. Chest X-ray assesses pulmonary edema and metastatic disease.
Pathology
All products of conception require histology. Complete moles show edematous villi with diffuse trophoblastic hyperplasia; partial moles show fetal tissue, vessels, amnion, and edematous villi.
Differential diagnosis
Threatened, missed, or incomplete abortion; ectopic pregnancy; hyperthyroidism; hyperemesis gravidarum; hypertension and preeclampsia.
Treatment
Prehospital Secure airway, provide oxygen, establish IV access, treat seizures with benzodiazepines, and save passed tissue.
Initial stabilization IV access, cardiac monitoring, and blood preparation if evacuation is planned.
Emergency department management Intubate for respiratory distress; give β-blockers before evacuation for hyperthyroidism; manage preeclampsia/eclampsia with benzodiazepines and magnesium sulfate and control blood pressure with hydralazine or labetalol; transfuse blood products for coagulopathy; administer Rho(D) immune globulin; perform suction curettage (fertility-sparing and curative in ~80%) with oxytocin; consider chemoprophylaxis only in selected high-risk cases with reliable follow-up; consider hysterectomy for older patients, those not desiring fertility, or high-risk disease.
Follow-up and disposition
Admission criteria Uterine size >16 weeks, clinical preeclampsia/hyperthyroidism/respiratory distress, hemodynamic instability, partial mole, or hysterectomy.
Discharge criteria Uncomplicated curettage of a small, low-risk mole with reliable follow-up.
Follow-up recommendations Close OB-GYN follow-up with serial β-hCG weekly for ≥4 weeks then monthly until undetectable; any rise prompts evaluation for metastasis. Use contraception and avoid pregnancy for 12 months; perform early ultrasound in future pregnancies. Recurrence risk is 1–1.5% after one mole and up to 20% after two.
Pearls and pitfalls Diagnosis may be missed with apparent normal pregnancy, preeclampsia before 24 weeks, or severe hyperemesis. Strict β-hCG follow-up is essential; up to 20% may develop malignancy if not monitored.
- Published on
Emergency And Acute Medicine-Hypercalcemia
Basics
Description Hypercalcemia severity depends on the absolute calcium level and the rate of rise. It is detected in approximately 0.1–1% of routine screenings. Most cases are mild (<12 mg/dL) and asymptomatic. Hypercalcemic crisis, typically >14 mg/dL, causes severe and potentially life-threatening manifestations. Circulating calcium exists as ionized (45%, the only physiologically active form), protein-bound (40%, mainly albumin), and complexed to anions (15%).
Etiology The most common causes are primary hyperparathyroidism and malignancy, followed by miscellaneous conditions.
Diagnosis
Signs and symptoms Neurologic features include headache, fatigue, lethargy, weakness, impaired concentration, confusion, depression, paranoia, stupor, or coma. Renal manifestations include polyuria, polydipsia, dehydration, oliguria in renal failure, nephrolithiasis, nephrocalcinosis, and interstitial nephritis. Gastrointestinal symptoms include anorexia, nausea, vomiting, abdominal pain, constipation, peptic ulcer disease, and pancreatitis. Dermatologic findings include pruritus. Classic mnemonic: “stones, bones, groans, thrones, and psychiatric overtones,” where “thrones” refers to polyuria.
Pediatric considerations Failure to thrive, delayed development, and potential intellectual impairment.
Physical exam Neurologic findings include irritability, lethargy, hyporeflexia, and coma. Cardiovascular findings include hypotension from volume depletion or hypertension, sinus bradycardia, and rarely cardiac arrest. Renal signs reflect dehydration. Dermatologic findings include band keratopathy and ectopic calcifications. Pediatric findings may include characteristic facies (pug nose, broad nasal bridge, cupid’s-bow upper lip) and hypotonia.
Essential workup Measure total and ionized calcium and albumin. Normal total calcium is <10.5 mg/dL. Corrected calcium (mg/dL) = measured calcium + 0.8 × (4.0 − albumin [g/dL]). Obtain electrolytes, BUN/creatinine, and glucose. ECG may show shortened QT interval, PR prolongation, QRS widening, sinus bradycardia, conduction blocks, digoxin sensitivity, and rarely Osborn J-waves.
Diagnosis tests and interpretation
Laboratory Assess phosphate, protein, urinalysis, and parathyroid hormone (PTH). Elevated or high-normal PTH suggests primary hyperparathyroidism; PTH <20 pg/mL warrants evaluation for PTH-related peptide and vitamin D metabolites. Elevated 25-hydroxyvitamin D suggests exogenous intake; elevated 1,25-dihydroxyvitamin D suggests lymphoma or sarcoidosis. Check digoxin levels if applicable and thyroid studies if indicated.
Imaging CT head for altered mental status and chest imaging with malignancy workup if no clear cause.
Diagnostic procedures Parathyroidectomy is indicated for symptomatic or severe primary hyperparathyroidism and may be urgent.
Differential diagnosis Primary hyperparathyroidism (most common outpatient cause; adenoma most frequent) typically causes mild chronic elevations. Malignancy is the most common inpatient cause, often with rapid onset, higher calcium levels, and greater symptom burden, commonly due to PTH-related peptide or osteolytic disease (e.g., breast, lung, kidney, head and neck, multiple myeloma, lymphoma). Miscellaneous causes include granulomatous disease, excess calcium or vitamin D intake, thiazides, familial hypocalciuric hypercalcemia, vitamin A toxicity, milk-alkali syndrome, lithium therapy, renal transplantation, hyperthyroidism, and acute tubular necrosis.
Pediatric considerations Primary hyperparathyroidism is less common; consider infantile hypercalcemia, immobilization hypercalcemia in adolescents, and vitamin D sensitivity.
Treatment
Prehospital Routine stabilization.
Initial stabilization/therapy ABCs, IV access, oxygen, cardiac monitoring. Administer 0.9% saline (1 L bolus or 20 mL/kg) for hypotension or severe dehydration. Address altered mental status with glucose assessment and supportive measures.
Emergency department management Treat immediately if corrected calcium >14 mg/dL or if symptomatic. Mild, asymptomatic cases do not require emergency therapy. Volume repletion with isotonic saline at 200–300 mL/hr targeting urine output 100–150 mL/hr; total 2–5 L/day may be required with close monitoring for overload. Correct electrolyte abnormalities. Renal elimination with loop diuretics (furosemide) only after adequate volume expansion; avoid thiazides. Dialysis may be required in renal failure. Inhibit bone resorption with bisphosphonates (first-line) and calcitonin for rapid but modest effect. Consider hydrocortisone for vitamin D–mediated or granulomatous causes. Encourage ambulation when appropriate. Treat the underlying cause and discontinue offending agents.
Medication First line Calcitonin 4 IU/kg IM/SC q12h; pamidronate 60–90 mg IV over 2–24 hr; etidronate 7.5 mg/kg IV daily for 3–7 days; furosemide 10–40 mg IV q6–8h (pediatrics 1–2 mg/kg). Second line Gallium nitrate 200 mg/m²/day IV ×5 days; hydrocortisone 200–400 mg/day IV for 3–5 days; plicamycin 25 μg/kg/day IV.
Pediatric considerations Loop diuretics are rarely needed and may worsen renal function; bisphosphonates appear safe but data are limited.
Follow-up and disposition
Admission criteria Corrected calcium >13 mg/dL, symptoms attributable to hypercalcemia, ECG changes, or need for monitored care; ICU for levels >14 mg/dL or severe manifestations.
Discharge criteria Corrected calcium <13 mg/dL with no symptoms.
Issues for referral Arrange prompt evaluation to determine etiology and long-term management; consider endocrinology consultation.
Follow-up recommendations Maintain hydration and monitor for mental status changes.
Key points Base treatment decisions on symptoms and corrected calcium levels. All patients with calcium >14 mg/dL require treatment regardless of symptoms. Monitor ECG closely and balance aggressive hydration against the risk of fluid overload.
Basics
Description Hypercalcemia severity depends on the absolute calcium level and the rate of rise. It is detected in approximately 0.1–1% of routine screenings. Most cases are mild (<12 mg/dL) and asymptomatic. Hypercalcemic crisis, typically >14 mg/dL, causes severe and potentially life-threatening manifestations. Circulating calcium exists as ionized (45%, the only physiologically active form), protein-bound (40%, mainly albumin), and complexed to anions (15%).
Etiology The most common causes are primary hyperparathyroidism and malignancy, followed by miscellaneous conditions.
Diagnosis
Signs and symptoms Neurologic features include headache, fatigue, lethargy, weakness, impaired concentration, confusion, depression, paranoia, stupor, or coma. Renal manifestations include polyuria, polydipsia, dehydration, oliguria in renal failure, nephrolithiasis, nephrocalcinosis, and interstitial nephritis. Gastrointestinal symptoms include anorexia, nausea, vomiting, abdominal pain, constipation, peptic ulcer disease, and pancreatitis. Dermatologic findings include pruritus. Classic mnemonic: “stones, bones, groans, thrones, and psychiatric overtones,” where “thrones” refers to polyuria.
Pediatric considerations Failure to thrive, delayed development, and potential intellectual impairment.
Physical exam Neurologic findings include irritability, lethargy, hyporeflexia, and coma. Cardiovascular findings include hypotension from volume depletion or hypertension, sinus bradycardia, and rarely cardiac arrest. Renal signs reflect dehydration. Dermatologic findings include band keratopathy and ectopic calcifications. Pediatric findings may include characteristic facies (pug nose, broad nasal bridge, cupid’s-bow upper lip) and hypotonia.
Essential workup Measure total and ionized calcium and albumin. Normal total calcium is <10.5 mg/dL. Corrected calcium (mg/dL) = measured calcium + 0.8 × (4.0 − albumin [g/dL]). Obtain electrolytes, BUN/creatinine, and glucose. ECG may show shortened QT interval, PR prolongation, QRS widening, sinus bradycardia, conduction blocks, digoxin sensitivity, and rarely Osborn J-waves.
Diagnosis tests and interpretation
Laboratory Assess phosphate, protein, urinalysis, and parathyroid hormone (PTH). Elevated or high-normal PTH suggests primary hyperparathyroidism; PTH <20 pg/mL warrants evaluation for PTH-related peptide and vitamin D metabolites. Elevated 25-hydroxyvitamin D suggests exogenous intake; elevated 1,25-dihydroxyvitamin D suggests lymphoma or sarcoidosis. Check digoxin levels if applicable and thyroid studies if indicated.
Imaging CT head for altered mental status and chest imaging with malignancy workup if no clear cause.
Diagnostic procedures Parathyroidectomy is indicated for symptomatic or severe primary hyperparathyroidism and may be urgent.
Differential diagnosis Primary hyperparathyroidism (most common outpatient cause; adenoma most frequent) typically causes mild chronic elevations. Malignancy is the most common inpatient cause, often with rapid onset, higher calcium levels, and greater symptom burden, commonly due to PTH-related peptide or osteolytic disease (e.g., breast, lung, kidney, head and neck, multiple myeloma, lymphoma). Miscellaneous causes include granulomatous disease, excess calcium or vitamin D intake, thiazides, familial hypocalciuric hypercalcemia, vitamin A toxicity, milk-alkali syndrome, lithium therapy, renal transplantation, hyperthyroidism, and acute tubular necrosis.
Pediatric considerations Primary hyperparathyroidism is less common; consider infantile hypercalcemia, immobilization hypercalcemia in adolescents, and vitamin D sensitivity.
Treatment
Prehospital Routine stabilization.
Initial stabilization/therapy ABCs, IV access, oxygen, cardiac monitoring. Administer 0.9% saline (1 L bolus or 20 mL/kg) for hypotension or severe dehydration. Address altered mental status with glucose assessment and supportive measures.
Emergency department management Treat immediately if corrected calcium >14 mg/dL or if symptomatic. Mild, asymptomatic cases do not require emergency therapy. Volume repletion with isotonic saline at 200–300 mL/hr targeting urine output 100–150 mL/hr; total 2–5 L/day may be required with close monitoring for overload. Correct electrolyte abnormalities. Renal elimination with loop diuretics (furosemide) only after adequate volume expansion; avoid thiazides. Dialysis may be required in renal failure. Inhibit bone resorption with bisphosphonates (first-line) and calcitonin for rapid but modest effect. Consider hydrocortisone for vitamin D–mediated or granulomatous causes. Encourage ambulation when appropriate. Treat the underlying cause and discontinue offending agents.
Medication First line Calcitonin 4 IU/kg IM/SC q12h; pamidronate 60–90 mg IV over 2–24 hr; etidronate 7.5 mg/kg IV daily for 3–7 days; furosemide 10–40 mg IV q6–8h (pediatrics 1–2 mg/kg). Second line Gallium nitrate 200 mg/m²/day IV ×5 days; hydrocortisone 200–400 mg/day IV for 3–5 days; plicamycin 25 μg/kg/day IV.
Pediatric considerations Loop diuretics are rarely needed and may worsen renal function; bisphosphonates appear safe but data are limited.
Follow-up and disposition
Admission criteria Corrected calcium >13 mg/dL, symptoms attributable to hypercalcemia, ECG changes, or need for monitored care; ICU for levels >14 mg/dL or severe manifestations.
Discharge criteria Corrected calcium <13 mg/dL with no symptoms.
Issues for referral Arrange prompt evaluation to determine etiology and long-term management; consider endocrinology consultation.
Follow-up recommendations Maintain hydration and monitor for mental status changes.
Key points Base treatment decisions on symptoms and corrected calcium levels. All patients with calcium >14 mg/dL require treatment regardless of symptoms. Monitor ECG closely and balance aggressive hydration against the risk of fluid overload.

- Published on
Emergency And Acute Medicine-Hyperbaric Oxygen Therapy
Basics
Description Hyperbaric oxygen therapy (HBOT) involves administration of 100% oxygen at pressures greater than 1 atmosphere (typically 2–3 atm). It increases oxygen delivery at the cellular level; at 3 atm, dissolved oxygen alone can support life without hemoglobin. HBOT also reduces the size of intravascular gas bubbles, making it effective for air embolism and decompression sickness. Two chamber types are used. Monoplace chambers accommodate a single supine patient, are pressurized with 100% oxygen, and monitored externally. Multiplace chambers treat multiple patients simultaneously, allow attendants inside, use air pressurization with oxygen delivered via mask, hood, or endotracheal tube, and permit transfer of equipment through airlocks.
Diagnosis
Indications Primary emergency indications include arterial gas embolism, decompression sickness, and carbon monoxide poisoning. Other indications include clostridial myonecrosis, necrotizing fasciitis, refractory osteomyelitis, chronic nonhealing wounds, radiation-induced tissue injury, crush injuries, thermal burns, and compromised skin grafts or flaps.
Alert In emergency medicine, focus should be on arterial gas embolism, decompression sickness, and carbon monoxide toxicity.
Essential workup Determine whether the clinical condition meets criteria for HBOT. Perform a thorough physical examination to establish a pretreatment baseline and identify contraindications. Absolute contraindication is untreated pneumothorax due to risk of tension pneumothorax. Relative contraindications include cardiovascular instability; unstable patients cannot be treated in monoplace chambers and may only be treated in multiplace chambers if benefit outweighs risk.
Diagnosis tests and interpretation
Laboratory Arterial blood gas to assess hypoxia when clinically indicated.
Imaging Chest radiograph to evaluate for occult pneumothorax prior to therapy.
Treatment
Initial stabilization/therapy Manage airway, breathing, and circulation. Establish IV access, administer 100% oxygen, and apply cardiac monitoring when appropriate.
Emergency department management Confirm indication for HBOT. Fill all balloon-containing devices (e.g., Foley catheters, endotracheal tube cuffs) with fluid to prevent rupture during pressurization. Pretreat patients with sinus congestion using decongestants. Place myringotomy tubes in obtunded or mechanically ventilated patients and in those with middle ear pathology.
Alert Complications include sinus or ear pain, barotrauma (ruptured tympanic membranes, tension pneumothorax), oxygen-toxicity–induced seizures, decompression sickness from rapid decompression, and limited access to unstable patients in monoplace chambers.
Follow-up and disposition
Admission criteria Arterial gas embolism, decompression sickness, and significant carbon monoxide toxicity.
Discharge criteria Stable patients with resolved symptoms after treatment.
Issues for referral Transfer may be required to a facility with hyperbaric capability; risks and benefits must be weighed carefully in unstable patients. The Divers Alert Network provides 24-hour consultation for dive-related injuries (919-684-9111).
Follow-up recommendations Arrange hyperbaric follow-up for repeat recompression therapy if indicated.
Key points Always exclude occult pneumothorax before therapy. Fill balloon-containing devices with fluid prior to pressurization. Emergency use of HBOT is most critical for gas embolism, decompression sickness, and carbon monoxide poisoning.
Basics
Description Hyperbaric oxygen therapy (HBOT) involves administration of 100% oxygen at pressures greater than 1 atmosphere (typically 2–3 atm). It increases oxygen delivery at the cellular level; at 3 atm, dissolved oxygen alone can support life without hemoglobin. HBOT also reduces the size of intravascular gas bubbles, making it effective for air embolism and decompression sickness. Two chamber types are used. Monoplace chambers accommodate a single supine patient, are pressurized with 100% oxygen, and monitored externally. Multiplace chambers treat multiple patients simultaneously, allow attendants inside, use air pressurization with oxygen delivered via mask, hood, or endotracheal tube, and permit transfer of equipment through airlocks.
Diagnosis
Indications Primary emergency indications include arterial gas embolism, decompression sickness, and carbon monoxide poisoning. Other indications include clostridial myonecrosis, necrotizing fasciitis, refractory osteomyelitis, chronic nonhealing wounds, radiation-induced tissue injury, crush injuries, thermal burns, and compromised skin grafts or flaps.
Alert In emergency medicine, focus should be on arterial gas embolism, decompression sickness, and carbon monoxide toxicity.
Essential workup Determine whether the clinical condition meets criteria for HBOT. Perform a thorough physical examination to establish a pretreatment baseline and identify contraindications. Absolute contraindication is untreated pneumothorax due to risk of tension pneumothorax. Relative contraindications include cardiovascular instability; unstable patients cannot be treated in monoplace chambers and may only be treated in multiplace chambers if benefit outweighs risk.
Diagnosis tests and interpretation
Laboratory Arterial blood gas to assess hypoxia when clinically indicated.
Imaging Chest radiograph to evaluate for occult pneumothorax prior to therapy.
Treatment
Initial stabilization/therapy Manage airway, breathing, and circulation. Establish IV access, administer 100% oxygen, and apply cardiac monitoring when appropriate.
Emergency department management Confirm indication for HBOT. Fill all balloon-containing devices (e.g., Foley catheters, endotracheal tube cuffs) with fluid to prevent rupture during pressurization. Pretreat patients with sinus congestion using decongestants. Place myringotomy tubes in obtunded or mechanically ventilated patients and in those with middle ear pathology.
Alert Complications include sinus or ear pain, barotrauma (ruptured tympanic membranes, tension pneumothorax), oxygen-toxicity–induced seizures, decompression sickness from rapid decompression, and limited access to unstable patients in monoplace chambers.
Follow-up and disposition
Admission criteria Arterial gas embolism, decompression sickness, and significant carbon monoxide toxicity.
Discharge criteria Stable patients with resolved symptoms after treatment.
Issues for referral Transfer may be required to a facility with hyperbaric capability; risks and benefits must be weighed carefully in unstable patients. The Divers Alert Network provides 24-hour consultation for dive-related injuries (919-684-9111).
Follow-up recommendations Arrange hyperbaric follow-up for repeat recompression therapy if indicated.
Key points Always exclude occult pneumothorax before therapy. Fill balloon-containing devices with fluid prior to pressurization. Emergency use of HBOT is most critical for gas embolism, decompression sickness, and carbon monoxide poisoning.