- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocephalus
Basics
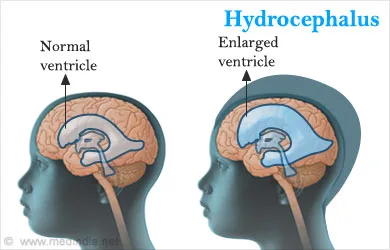
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
Basics
Description Hydrocephalus is an abnormal increase in cerebrospinal fluid (CSF) volume within the cranial cavity. Cerebral atrophy may also increase CSF volume but without elevated CSF pressure. Obstructive hydrocephalus is the most common form and results from blockage within the ventricular system or subarachnoid space, potentially causing rapid rises in intracranial pressure (ICP) leading to death or permanent brain injury. Nonobstructive hydrocephalus produces subacute symptoms and represents a potentially reversible cause of dementia. Hydrocephalus is also classified as communicating, where CSF flow is blocked after exiting the ventricles, and noncommunicating, where flow is blocked within ventricular pathways.
Etiology Obstructive hydrocephalus results from blockage at specific anatomic sites. Aqueduct of Sylvius obstruction is most common, causing dilation of the lateral and third ventricles with sparing of the fourth ventricle; causes include congenital stenosis, tumor, subarachnoid hemorrhage, postmeningitic scarring, or idiopathic disease. Foramen of Monro obstruction leads to dilation of one or both lateral ventricles. Obstruction at the foramina of Luschka and Magendie causes fourth ventricle blockage with subsequent dilation of the entire ventricular system. Subarachnoid space obstruction around the brainstem may occur after infection or subarachnoid hemorrhage, producing global ventricular dilation. Acute presentations are often due to CSF shunt malfunction, subarachnoid hemorrhage, or severe head trauma. Nonobstructive hydrocephalus, including normal pressure hydrocephalus, involves impaired CSF absorption with ventricular enlargement but no sustained intracranial hypertension and is sometimes termed chronic hydrocephalus. Pediatric hydrocephalus may be congenital or acquired and is commonly related to neonatal hemorrhage, congenital malformations, or postinfectious scarring.
Diagnosis
Signs and symptoms Obstructive hydrocephalus presents with headache, nausea, vomiting, decreased consciousness, urinary incontinence, ocular palsies, papilledema, visual loss, pupillary dilation, and Cushing response with hypertension and bradycardia. Pediatric patients may show a full fontanelle, irritability, lethargy, and elevated blood pressure. Slowly progressive obstruction may resemble nonobstructive hydrocephalus. Nonobstructive hydrocephalus presents with insidious dementia, somnolence, gait disturbance, urinary incontinence, impaired upward gaze, generalized weakness, and lethargy, typically without headache or papilledema.
Pediatric considerations Gradual CSF accumulation may cause craniomegaly, developmental delay, prominent scalp veins, and impaired upward gaze (setting-sun sign).
History Assess symptom onset, presence of a CSF shunt, headache, nausea or vomiting, weakness, confusion, visual changes, and urinary incontinence.
Physical exam Perform a complete neurologic examination including motor, sensory, reflexes, gait, and cranial nerves. Assess mental status and look for papilledema. Palpate any CSF shunt; inability to compress suggests distal malfunction, and failure to refill suggests proximal obstruction. In children, evaluate the anterior fontanelle.
Essential workup Noncontrast CT of the head assesses ventricular size and symmetry and helps identify hemorrhage, mass lesions, or cerebral edema.
Diagnosis tests and interpretation
Laboratory Lumbar puncture is performed only after CT and only for suspected nonobstructive causes; opening pressure may be elevated. Send CSF for routine studies if infection is suspected.
Imaging MRI provides detailed assessment of ventricular anatomy and improved detection of masses compared with CT.
Diagnostic procedures Lumbar puncture may be diagnostic or therapeutic in selected nonobstructive cases.
Differential diagnosis Acute ischemic stroke, intracranial hemorrhage, CNS infection, mass effect from tumor or hematoma, other causes of dementia or delirium, and toxic or metabolic encephalopathies.
Pediatric considerations Consider congenital anomalies such as Dandy–Walker malformation, Arnold–Chiari malformation, meningomyelocele, choroid plexus papilloma, or arachnoid villi dysfunction, as well as infections (rubella, CMV, toxoplasmosis, syphilis, bacterial meningitis), tumors of the posterior fossa, and intraventricular or subarachnoid hemorrhage.
Treatment
Prehospital Hydrocephalus cannot be definitively diagnosed in the field. Provide supplemental oxygen and airway support as needed. Transport with the head elevated to approximately 30° unless hypotension is present, in which case prioritize cerebral perfusion with fluid resuscitation.
Initial stabilization/therapy For signs of impending herniation, perform rapid-sequence intubation using agents such as etomidate or thiopental. Maintain controlled ventilation with PaCO₂ around 35 mm Hg and systolic blood pressure above 100 mm Hg in adults. Administer mannitol as indicated. In patients with CSF shunts and impending herniation, shunt pumping or controlled CSF drainage may be attempted to reduce pressure.
Emergency department management ED intervention is required for acute shunt malfunction or impending herniation. Definitive therapy involves shunt placement or revision or treatment of the underlying cause such as tumor. Symptoms of normal pressure hydrocephalus may transiently improve after removal of 20–30 mL of CSF via lumbar puncture. Acute obstructive hydrocephalus from intraventricular hemorrhage may require ventriculostomy. Provide sedation for agitated or intubated patients, maintain head elevation unless hypotensive, consider mannitol, and use seizure prophylaxis when appropriate.
Medication Atropine 0.02 mg/kg IV (max 0.1 mg), etomidate 0.2–0.3 mg/kg IV, lidocaine 1 mg/kg IV, mannitol 0.5–1.5 g/kg IV, rocuronium 0.6 mg/kg IV, succinylcholine 1–1.5 mg/kg IV, vecuronium 0.1 mg/kg IV, fosphenytoin 15–20 mg/kg loading dose.
Follow-up and disposition
Admission criteria Evidence of increased ICP or suspected shunt malfunction.
Discharge criteria Selected patients with presumed normal pressure hydrocephalus and no acute findings may be discharged with close follow-up.
Issues for referral Early neurosurgical consultation is essential for acute obstructive hydrocephalus or shunt malfunction; transfer should be considered if neurosurgical care is unavailable, with airway secured when indicated.
Follow-up recommendations Stable patients require prompt follow-up with neurology and/or neurosurgery.
Key points Lumbar puncture is contraindicated in obstructive hydrocephalus due to herniation risk. Rapid head growth in children should prompt evaluation for hydrocephalus. Any neurologic complaint in a patient with a CSF shunt should raise concern for shunt malfunction.
- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocele
Basics
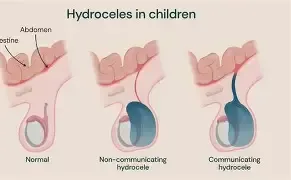
Description Hydrocele is the most common cause of painless scrotal swelling and is classified as congenital or acquired. Congenital hydrocele results from a patent processus vaginalis with communication between the tunica vaginalis and peritoneal cavity; most close spontaneously by 2 years of age. Acquired (secondary) hydrocele occurs due to intrascrotal infection, neoplasm, inguinal or scrotal surgery, or regional or systemic disease. Communicating hydrocele involves a patent processus vaginalis, with scrotal size fluctuating based on position and intra-abdominal pressure. Noncommunicating hydrocele results from excess serous fluid production or impaired absorption within the scrotum.
Etiology Hydrocele results from an imbalance between fluid production and resorption between the tunica vaginalis and tunica albuginea. Causes of adult noncommunicating hydrocele include epididymitis, trauma, mumps, tuberculosis, hypoalbuminemia, and spermatic vein ligation. In the developing world, filarial infections such as Wuchereria bancrofti or Loa loa are the most common causes worldwide. Rare causes include testicular malignancy or lymphoma and abdominoscrotal hydrocele, which may compress adjacent structures causing hydroureter or unilateral limb edema; ultrasound shows a single sac extending through the deep inguinal ring.
Pediatric considerations Congenital hydrocele occurs in approximately 6% of newborn boys and is commonly diagnosed in the newborn period. It is caused by a patent processus vaginalis, which remains open in most newborns. Size may vary with position or crying, and the mass may intermittently resolve. Most close spontaneously by age 2 years.
Diagnosis
Signs and symptoms Painless scrotal swelling with a sensation of heaviness, pulling, or dragging.
History Focus on onset, progression, variability in size, and exclusion of testicular torsion.
Physical exam The mass may feel soft and doughy or firm depending on fluid volume. Transillumination may show homogeneous light transmission but is increasingly replaced by bedside ultrasound.
Essential workup Bedside ultrasound is the diagnostic test of choice, allowing visualization of the hydrocele and testicle and helping identify underlying masses. In adults, the entire testicle must be palpated because hydrocele may obscure a primary neoplasm.
Diagnosis tests and interpretation
Laboratory No routine laboratory testing is required unless evaluating an underlying cause (e.g., urinalysis, AFP, β-hCG).
Imaging Ultrasound demonstrates a large anechoic fluid-filled collection surrounding the anterolateral aspect of the testicle.
Differential diagnosis Epididymitis, indirect inguinal hernia, orchitis, testicular neoplasm, testicular torsion, varicocele.
Treatment
Initial stabilization/therapy Address and stabilize any underlying cause such as trauma or infection.
Emergency department management Perform thorough testicular examination to exclude neoplasm and arrange appropriate referral.
Medication Treat underlying pathology if identified.
Follow-up and disposition
Admission criteria Secondary hydrocele with concern for underlying pathology such as trauma or malignancy.
Discharge criteria Otherwise healthy patients may be discharged with urology referral. Hydrocele repair is elective and performed for discomfort or cosmetic reasons. Options include surgical hydrocelectomy or aspiration with sclerotherapy.
Pediatric considerations Most infant hydroceles resolve spontaneously by 12 months; observation and referral are appropriate. Persistent hydroceles after 12–18 months should be referred for surgical repair due to associated inguinal hernia risk.
Follow-up recommendations Urology follow-up is recommended.
Key points Hydroceles may not transilluminate if the tunica vaginalis is thickened. Bedside ultrasound should always confirm both the fluid collection and normal testicular anatomy to avoid missing serious pathology.
Basics
Description Hydrocele is the most common cause of painless scrotal swelling and is classified as congenital or acquired. Congenital hydrocele results from a patent processus vaginalis with communication between the tunica vaginalis and peritoneal cavity; most close spontaneously by 2 years of age. Acquired (secondary) hydrocele occurs due to intrascrotal infection, neoplasm, inguinal or scrotal surgery, or regional or systemic disease. Communicating hydrocele involves a patent processus vaginalis, with scrotal size fluctuating based on position and intra-abdominal pressure. Noncommunicating hydrocele results from excess serous fluid production or impaired absorption within the scrotum.
Etiology Hydrocele results from an imbalance between fluid production and resorption between the tunica vaginalis and tunica albuginea. Causes of adult noncommunicating hydrocele include epididymitis, trauma, mumps, tuberculosis, hypoalbuminemia, and spermatic vein ligation. In the developing world, filarial infections such as Wuchereria bancrofti or Loa loa are the most common causes worldwide. Rare causes include testicular malignancy or lymphoma and abdominoscrotal hydrocele, which may compress adjacent structures causing hydroureter or unilateral limb edema; ultrasound shows a single sac extending through the deep inguinal ring.
Pediatric considerations Congenital hydrocele occurs in approximately 6% of newborn boys and is commonly diagnosed in the newborn period. It is caused by a patent processus vaginalis, which remains open in most newborns. Size may vary with position or crying, and the mass may intermittently resolve. Most close spontaneously by age 2 years.
Diagnosis
Signs and symptoms Painless scrotal swelling with a sensation of heaviness, pulling, or dragging.
History Focus on onset, progression, variability in size, and exclusion of testicular torsion.
Physical exam The mass may feel soft and doughy or firm depending on fluid volume. Transillumination may show homogeneous light transmission but is increasingly replaced by bedside ultrasound.
Essential workup Bedside ultrasound is the diagnostic test of choice, allowing visualization of the hydrocele and testicle and helping identify underlying masses. In adults, the entire testicle must be palpated because hydrocele may obscure a primary neoplasm.
Diagnosis tests and interpretation
Laboratory No routine laboratory testing is required unless evaluating an underlying cause (e.g., urinalysis, AFP, β-hCG).
Imaging Ultrasound demonstrates a large anechoic fluid-filled collection surrounding the anterolateral aspect of the testicle.
Differential diagnosis Epididymitis, indirect inguinal hernia, orchitis, testicular neoplasm, testicular torsion, varicocele.
Treatment
Initial stabilization/therapy Address and stabilize any underlying cause such as trauma or infection.
Emergency department management Perform thorough testicular examination to exclude neoplasm and arrange appropriate referral.
Medication Treat underlying pathology if identified.
Follow-up and disposition
Admission criteria Secondary hydrocele with concern for underlying pathology such as trauma or malignancy.
Discharge criteria Otherwise healthy patients may be discharged with urology referral. Hydrocele repair is elective and performed for discomfort or cosmetic reasons. Options include surgical hydrocelectomy or aspiration with sclerotherapy.
Pediatric considerations Most infant hydroceles resolve spontaneously by 12 months; observation and referral are appropriate. Persistent hydroceles after 12–18 months should be referred for surgical repair due to associated inguinal hernia risk.
Follow-up recommendations Urology follow-up is recommended.
Key points Hydroceles may not transilluminate if the tunica vaginalis is thickened. Bedside ultrasound should always confirm both the fluid collection and normal testicular anatomy to avoid missing serious pathology.
- Published on
KembaraXtra-Emergency And Acute Medicine: Hydrocarbon Poisoning
Basics
Description The most serious complication of hydrocarbon exposure is aspiration, primarily affecting the respiratory and central nervous systems. Toxicity is influenced by physical properties. Viscosity: lower viscosity increases aspiration risk. Volatility: highly volatile substances displace alveolar oxygen, leading to hypoxia. Surface tension: low surface tension facilitates spread from the oropharynx into the trachea, increasing aspiration risk (e.g., mineral oil, seal oil). Volatile-substance abuse commonly involves solvents such as typewriter correction fluid, adhesives, gasoline, and lighter fluid. Methods include sniffing (direct inhalation), huffing (from a soaked rag), and bagging (from a bag). Major hydrocarbon classes include aliphatics (kerosene, mineral oil, gasoline, solvents, paint thinners) causing pulmonary toxicity via aspiration and asphyxiation from methane or butane; halogenated hydrocarbons (carbon tetrachloride, trichloroethane) used industrially, well absorbed, and associated with hepatic and renal failure; aromatic or cyclic hydrocarbons (toluene, xylene) that are highly volatile and systemically absorbed, with fatal benzene ingestion reported at ~15 mL; and terpenes or wood distillates (turpentine, pine oil) causing significant gastrointestinal absorption and CNS depression.
Etiology Accidental exposure is most common in young children, while inhalant abuse and intentional self-harm are more frequent in adolescents and adults.
Diagnosis
Signs and symptoms Patients may be asymptomatic initially and often have a hydrocarbon odor on the breath. Early effects include euphoria and disinhibition; later effects include dysphoria, ataxia, confusion, and hallucinations. Sudden sniffing death can occur in volatile-substance abusers due to malignant dysrhythmias from myocardial sensitization. Pulmonary manifestations range from mild respiratory distress to cyanosis and aspiration pneumonitis. CNS effects include intoxication, slurred speech, lethargy, and coma. Gastrointestinal findings include mucosal irritation, gastritis, and diarrhea. Cardiac effects include tachycardia and dysrhythmias. Dermal findings include erythema, maculopapular or vesicular eruptions, defatting dermatitis, and “huffer face” rash with chronic exposure.
History Assess route, substance, amount, timing, intent, possible coingestions, symptoms, and any prehospital interventions.
Physical exam Evaluate airway protection in patients with vomiting or decreased consciousness. Respiratory symptoms usually appear within 30 minutes but may be delayed. Monitor for hypoxia, hypotension, and dysrhythmias. Early fever suggests chemical pneumonitis, whereas fever after 48 hours suggests secondary infection.
Essential workup Identify the exact product, manufacturer, ingredients, exposure type, and estimated quantity; review MSDS when applicable.
Diagnosis tests and interpretation
Laboratory Obtain ECG in volatile-substance abusers. Use pulse oximetry and ABG if abnormal. Check electrolytes, BUN, creatinine, glucose, and liver function tests for halogenated or aromatic exposures; metabolic acidosis and hypokalemia may be present. Measure carboxyhemoglobin for methylene chloride exposure.
Imaging Chest radiograph abnormalities may appear from 20 minutes to 24 hours (typically by 6 hours) and include increased bronchovascular markings with bibasilar or perihilar infiltrates. Lobar consolidation is uncommon; pneumothorax, pneumomediastinum, pleural effusion, and pneumatoceles are rare. Repeat imaging if respiratory status worsens.
Differential diagnosis Caustic ingestion, pesticide poisoning, toxic alcohol ingestion, assessment of accidental versus intentional exposure (psychiatric evaluation), and possible child neglect.
Treatment
Prehospital Remove contaminated clothing and decontaminate exposed skin and hair. Do not induce emesis; ipecac is contraindicated. Keep volatile-substance abusers calm and minimize agitation. Selected asymptomatic patients with known products and reliable observation may be managed at home.
Initial stabilization Follow ABCs, establish IV access with fluids if needed, administer oxygen, monitor cardiac rhythm, and give naloxone, thiamine, and dextrose for altered mental status as indicated.
Emergency department management Provide supportive care. Treat bronchospasm with oxygen and nebulized albuterol; intubate and ventilate for respiratory failure. Steroids are not recommended. Avoid epinephrine in volatile-substance abusers due to dysrhythmia risk. Alert Gastric decontamination is generally not indicated because aspiration risk outweighs benefit. Avoid if spontaneous emesis occurred. Consider limited gastric aspiration only for select CHAMP ingestions (camphor, halogenated hydrocarbons, aromatic hydrocarbons, metals, pesticides) within 60 minutes, with airway protection if needed. Activated charcoal and cathartics are not recommended.
Medication Albuterol 2.5–5 mg nebulized (pediatrics 0.15–0.3 mg/kg). Dextrose D50W 25 g IV (pediatrics D25W 2–4 mL/kg). Naloxone 2 mg IV or IM (pediatrics 0.1 mg/kg). Thiamine 100 mg IV or IM (pediatrics 50 mg).
Follow-up and disposition
Admission criteria Symptomatic patients or those at risk for delayed organ toxicity.
Discharge criteria Observe for at least 6 hours; discharge asymptomatic patients with normal pulse oximetry and chest radiograph, or those asymptomatic with abnormal imaging but normal oxygenation if reliable follow-up is ensured. Observe volatile-substance abusers until mental status normalizes.
Follow-up recommendations Reassess within 24 hours for patients who remain asymptomatic after observation. Repeat chest radiograph in 24 hours for asymptomatic patients with initial abnormalities.
Key points Aspiration is the dominant hazard in hydrocarbon exposure, with risk rising as viscosity and surface tension decrease and volatility increases. Prompt external decontamination is essential. Gastric decontamination and induced emesis are rarely appropriate. All patients should be observed for at least 6 hours, with hospital admission for those who are symptomatic or at risk for delayed toxicity.
Basics
Description The most serious complication of hydrocarbon exposure is aspiration, primarily affecting the respiratory and central nervous systems. Toxicity is influenced by physical properties. Viscosity: lower viscosity increases aspiration risk. Volatility: highly volatile substances displace alveolar oxygen, leading to hypoxia. Surface tension: low surface tension facilitates spread from the oropharynx into the trachea, increasing aspiration risk (e.g., mineral oil, seal oil). Volatile-substance abuse commonly involves solvents such as typewriter correction fluid, adhesives, gasoline, and lighter fluid. Methods include sniffing (direct inhalation), huffing (from a soaked rag), and bagging (from a bag). Major hydrocarbon classes include aliphatics (kerosene, mineral oil, gasoline, solvents, paint thinners) causing pulmonary toxicity via aspiration and asphyxiation from methane or butane; halogenated hydrocarbons (carbon tetrachloride, trichloroethane) used industrially, well absorbed, and associated with hepatic and renal failure; aromatic or cyclic hydrocarbons (toluene, xylene) that are highly volatile and systemically absorbed, with fatal benzene ingestion reported at ~15 mL; and terpenes or wood distillates (turpentine, pine oil) causing significant gastrointestinal absorption and CNS depression.
Etiology Accidental exposure is most common in young children, while inhalant abuse and intentional self-harm are more frequent in adolescents and adults.
Diagnosis
Signs and symptoms Patients may be asymptomatic initially and often have a hydrocarbon odor on the breath. Early effects include euphoria and disinhibition; later effects include dysphoria, ataxia, confusion, and hallucinations. Sudden sniffing death can occur in volatile-substance abusers due to malignant dysrhythmias from myocardial sensitization. Pulmonary manifestations range from mild respiratory distress to cyanosis and aspiration pneumonitis. CNS effects include intoxication, slurred speech, lethargy, and coma. Gastrointestinal findings include mucosal irritation, gastritis, and diarrhea. Cardiac effects include tachycardia and dysrhythmias. Dermal findings include erythema, maculopapular or vesicular eruptions, defatting dermatitis, and “huffer face” rash with chronic exposure.
History Assess route, substance, amount, timing, intent, possible coingestions, symptoms, and any prehospital interventions.
Physical exam Evaluate airway protection in patients with vomiting or decreased consciousness. Respiratory symptoms usually appear within 30 minutes but may be delayed. Monitor for hypoxia, hypotension, and dysrhythmias. Early fever suggests chemical pneumonitis, whereas fever after 48 hours suggests secondary infection.
Essential workup Identify the exact product, manufacturer, ingredients, exposure type, and estimated quantity; review MSDS when applicable.
Diagnosis tests and interpretation
Laboratory Obtain ECG in volatile-substance abusers. Use pulse oximetry and ABG if abnormal. Check electrolytes, BUN, creatinine, glucose, and liver function tests for halogenated or aromatic exposures; metabolic acidosis and hypokalemia may be present. Measure carboxyhemoglobin for methylene chloride exposure.
Imaging Chest radiograph abnormalities may appear from 20 minutes to 24 hours (typically by 6 hours) and include increased bronchovascular markings with bibasilar or perihilar infiltrates. Lobar consolidation is uncommon; pneumothorax, pneumomediastinum, pleural effusion, and pneumatoceles are rare. Repeat imaging if respiratory status worsens.
Differential diagnosis Caustic ingestion, pesticide poisoning, toxic alcohol ingestion, assessment of accidental versus intentional exposure (psychiatric evaluation), and possible child neglect.
Treatment
Prehospital Remove contaminated clothing and decontaminate exposed skin and hair. Do not induce emesis; ipecac is contraindicated. Keep volatile-substance abusers calm and minimize agitation. Selected asymptomatic patients with known products and reliable observation may be managed at home.
Initial stabilization Follow ABCs, establish IV access with fluids if needed, administer oxygen, monitor cardiac rhythm, and give naloxone, thiamine, and dextrose for altered mental status as indicated.
Emergency department management Provide supportive care. Treat bronchospasm with oxygen and nebulized albuterol; intubate and ventilate for respiratory failure. Steroids are not recommended. Avoid epinephrine in volatile-substance abusers due to dysrhythmia risk. Alert Gastric decontamination is generally not indicated because aspiration risk outweighs benefit. Avoid if spontaneous emesis occurred. Consider limited gastric aspiration only for select CHAMP ingestions (camphor, halogenated hydrocarbons, aromatic hydrocarbons, metals, pesticides) within 60 minutes, with airway protection if needed. Activated charcoal and cathartics are not recommended.
Medication Albuterol 2.5–5 mg nebulized (pediatrics 0.15–0.3 mg/kg). Dextrose D50W 25 g IV (pediatrics D25W 2–4 mL/kg). Naloxone 2 mg IV or IM (pediatrics 0.1 mg/kg). Thiamine 100 mg IV or IM (pediatrics 50 mg).
Follow-up and disposition
Admission criteria Symptomatic patients or those at risk for delayed organ toxicity.
Discharge criteria Observe for at least 6 hours; discharge asymptomatic patients with normal pulse oximetry and chest radiograph, or those asymptomatic with abnormal imaging but normal oxygenation if reliable follow-up is ensured. Observe volatile-substance abusers until mental status normalizes.
Follow-up recommendations Reassess within 24 hours for patients who remain asymptomatic after observation. Repeat chest radiograph in 24 hours for asymptomatic patients with initial abnormalities.
Key points Aspiration is the dominant hazard in hydrocarbon exposure, with risk rising as viscosity and surface tension decrease and volatility increases. Prompt external decontamination is essential. Gastric decontamination and induced emesis are rarely appropriate. All patients should be observed for at least 6 hours, with hospital admission for those who are symptomatic or at risk for delayed toxicity.
- Published on
Infectious Diseases and Microbiology: Cough and Fever
Basics
Description
Cough is a forceful expiratory reflex that helps clear secretions and foreign material from the tracheobronchial tree. Fever is typically defined as a temperature rise of about 2°F above baseline or a measured temperature above 100.4°F and commonly reflects an immune-mediated increase in the hypothalamic set point. Cough duration is classified as acute (<3 weeks), subacute (3-8 or chronic (≥8 though in high-tuberculosis-burden settings, “chronic cough” is often considered>2–3 weeks.
Epidemiology
Cough is one of the most frequent outpatient complaints. The combination of cough and fever commonly indicates respiratory illness but may also occur with nonrespiratory conditions.
Risk Factors
Risk increases with immunodeficiency, smoking, asthma, or COPD. Pneumonia risk is highest at the extremes of age. Aspiration risk rises with swallowing dysfunction from neurologic disease (including stroke and Parkinson disease) and after surgery or radiation involving the oral cavity, pharynx, or esophagus. Specific environmental or occupational exposures point to particular infections, including unpasteurized dairy (brucellosis), birds (psittacosis due to Chlamydia psittaci), residence or travel to the U.S. Southwest (coccidioidomycosis), rodents (hantavirus), bat guano (histoplasmosis), aerosolized water sources (legionellosis), and water contaminated with animal urine (leptospirosis). Unusually severe pneumonia in a previously healthy person or clustered cases should raise concern for inhalational anthrax, tularemia, plague, other high-consequence infections, pandemic influenza, or SARS, including possible bioterrorism scenarios.
General Prevention
Maintain current vaccination against influenza and Streptococcus pneumoniae, ensure pertussis and Haemophilus influenzae type b immunization in children, and encourage smoking cessation.
Pathophysiology
Cough is triggered as a protective reflex by airway irritation from inhaled substances such as smoke, dust, or fumes, or by aspirated material such as upper-airway secretions, gastric contents, or foreign bodies.
Etiology
Acute cough with fever is most often due to viral nasopharyngitis, including influenza, parainfluenza, respiratory syncytial virus, rhinovirus, coronavirus, and adenovirus. In adults with typical “common cold” syndromes, only mild temperature elevation is expected, and higher fever is atypical. Other acute causes include upper respiratory infections such as acute sinusitis and bronchitis, which are frequently viral and in which cough predominates, and lower respiratory infections such as pneumonia of bacterial, viral, fungal, or aspiration origin, bronchiectasis exacerbations, and lung abscess, as well as mediastinitis, endocarditis, malaria, and pulmonary embolism; several of these may also cause chronic cough with intermittent fever. Subacute cough may result from bacterial sinusitis or be postinfectious; even with minimal fever, pertussis must be considered because it can be mild or atypical after immunization yet remains highly contagious and dangerous to infants. Chronic cough with fever suggests tuberculosis in at-risk populations such as those with homelessness, HIV/AIDS, or exposure in endemic regions, and may also reflect chronic sinusitis, chronic melioidosis due to Burkholderia pseudomallei in Southeast Asia, endobronchial sarcoidosis, Kaposi sarcoma, lymphoma, airway-infiltrating tumors such as bronchogenic carcinoma or carcinoid, pulmonary embolism, or inflammatory pseudotumor. Cough and fever may also represent unrelated processes when their onsets differ, and chronic cough may stem from noninfectious causes such as gastroesophageal reflux, postnasal drip, ACE-inhibitor effect, or asthma.
Commonly Associated Conditions
HIV/AIDS and other immunodeficiency states are frequently linked to cough with fever and broaden the infectious and noninfectious differential.
Diagnosis
History
Because severe febrile respiratory syndromes can rapidly progress to respiratory failure, the first step is to identify life-threatening illness or systemic toxicity, including bacterial pneumonia, influenza, SARS-like syndromes, high-consequence or bioterrorism-related infections, and pulmonary embolism. Assess for dyspnea, hemoptysis, sputum production, other infectious symptoms, and immunodeficiency. A detailed exposure and travel history is essential, and history may also point toward noninfectious causes such as pulmonary embolism after prolonged immobility or malignancy suggested by smoking, weight loss, and hemoptysis without tuberculosis risk factors.
Physical Examination
Examine lungs plus upper airway structures (mouth, throat, nose, sinuses) and ears, and judge overall appearance for severity, fatigue, and impending respiratory compromise. Evaluate for tachycardia (>100/min), tachypnea (>24/min), and impaired oxygenation. Focal rales and egophony support lower respiratory infection, but examination alone often cannot confirm pneumonia.
Diagnostic Tests and Interpretation
Laboratory Studies
Purulent sputum suggests chronic bronchitis, bronchiectasis, pneumonia, or lung abscess, while hemoptysis can occur in these disorders and may also indicate an endobronchial tumor. Sputum microscopy and Gram stain can sometimes identify pathogens and guide antibiotics, but overall yield is limited by variability in collection and interpretation and by inability of many pneumonia patients to produce sputum. For chronic cough in high–tuberculosis-prevalence settings, obtain sputum smears and cultures for acid-fast bacilli and a chest radiograph.
Imaging
Chest radiography helps distinguish upper versus lower respiratory involvement, detect pneumonia, and identify intrathoracic masses. Patients with a syndrome consistent with acute bronchitis who have normal vital signs and a normal lung exam generally do not need chest radiography because pneumonia likelihood is low. Radiographic infiltrate patterns can suggest but do not confirm specific causes: lobar consolidation, cavitation, and large pleural effusions favor bacterial infection; bilateral diffuse involvement may occur with Pneumocystis jirovecii, Legionella, viral infections, or Mycoplasma pneumoniae; necrotizing pneumonia with cavitation and empyema suggests aspiration, gram-negative organisms, or staphylococci; nodular or cavitary patterns may reflect lung abscess or infections such as Nocardia, actinomycosis, atypical mycobacteria, cryptococcosis, or aspergillosis; and focal infiltrates are common with bacteria (including Nocardia), mycobacteria, Cryptococcus, and Aspergillus. High-resolution CT is preferred to demonstrate airway dilation and confirm bronchiectasis, and chest CT helps assess infections not responding to therapy, delineate lung abscess, and evaluate postobstructive pneumonia due to a mass. If the diagnosis remains unclear, consider sinus imaging and otolaryngology evaluation, and assess for extrapulmonary spread such as brain abscess when neurologic or other systemic findings are present.
Diagnostic Procedures/Other
Fiberoptic bronchoscopy assists with specimen collection and histopathologic evaluation of suspected endobronchial tumors and can help define organism susceptibilities in pneumonia unresponsive to therapy using protected sampling techniques. Pleural fluid analysis and pleural biopsy can support diagnosis of tuberculosis or malignancy.
Treatment
Medications
Management depends on identifying the underlying cause and treating it specifically. Antibiotics are generally unnecessary for acute viral upper respiratory infection, and when bacterial sinusitis cannot be distinguished from viral URI at presentation, delaying antibiotics for about seven days is appropriate. Antibiotics are indicated for pneumonia, tuberculosis, and pertussis. Irritative nonproductive cough can be suppressed with antitussives that raise cough threshold such as codeine 15 mg four times daily or dextromethorphan 15 mg four times daily. Additional agents that may reduce cough include NSAIDs such as naproxen, sedating antihistamines for common-cold–related cough (with newer nonsedating antihistamines generally ineffective), and inhaled ipratropium 2–4 puffs four times daily in chronic bronchitis. Productive cough with substantial sputum should usually not be suppressed because secretion retention can worsen ventilation, impair aeration, and reduce host defense. Hydration and expectorants such as guaifenesin may help thin mucus and improve clearance. Inflammatory pseudotumors, though typically resected, have also responded to antibiotics, radiation, or corticosteroids, and may occasionally regress spontaneously.
Additional Treatment
Maintain hydration and support smoking cessation.
In-Patient Considerations
Initial Stabilization
Consider intubation and positive-pressure ventilation for respiratory fatigue or severe oxygenation/ventilation failure based on arterial blood gases. Implement infection control measures, including isolation and airborne precautions, when severe febrile respiratory illness occurs with epidemiologic features suggesting transmissible high-consequence infection, relevant travel, animal or laboratory exposure, or potential bioterrorism.
Admission Criteria
Tools such as the Pneumonia Severity Index, though developed for pneumonia, can help guide disposition in febrile respiratory illness. Advanced age, significant comorbidities, and abnormal vital signs such as tachypnea, tachycardia, hypotension, and altered physiology indicate higher risk of morbidity and mortality.
Ongoing Care and Follow-Up
Reinforce smoking cessation.
Prognosis
Community-acquired pneumonia carries an approximate mortality of 13%.
Complications
Severe coughing paroxysms can trigger syncope. Patients with tuberculosis and cough are infectious and can transmit disease.
Basics
Description
Cough is a forceful expiratory reflex that helps clear secretions and foreign material from the tracheobronchial tree. Fever is typically defined as a temperature rise of about 2°F above baseline or a measured temperature above 100.4°F and commonly reflects an immune-mediated increase in the hypothalamic set point. Cough duration is classified as acute (<3 weeks), subacute (3-8 or chronic (≥8 though in high-tuberculosis-burden settings, “chronic cough” is often considered>2–3 weeks.
Epidemiology
Cough is one of the most frequent outpatient complaints. The combination of cough and fever commonly indicates respiratory illness but may also occur with nonrespiratory conditions.
Risk Factors
Risk increases with immunodeficiency, smoking, asthma, or COPD. Pneumonia risk is highest at the extremes of age. Aspiration risk rises with swallowing dysfunction from neurologic disease (including stroke and Parkinson disease) and after surgery or radiation involving the oral cavity, pharynx, or esophagus. Specific environmental or occupational exposures point to particular infections, including unpasteurized dairy (brucellosis), birds (psittacosis due to Chlamydia psittaci), residence or travel to the U.S. Southwest (coccidioidomycosis), rodents (hantavirus), bat guano (histoplasmosis), aerosolized water sources (legionellosis), and water contaminated with animal urine (leptospirosis). Unusually severe pneumonia in a previously healthy person or clustered cases should raise concern for inhalational anthrax, tularemia, plague, other high-consequence infections, pandemic influenza, or SARS, including possible bioterrorism scenarios.
General Prevention
Maintain current vaccination against influenza and Streptococcus pneumoniae, ensure pertussis and Haemophilus influenzae type b immunization in children, and encourage smoking cessation.
Pathophysiology
Cough is triggered as a protective reflex by airway irritation from inhaled substances such as smoke, dust, or fumes, or by aspirated material such as upper-airway secretions, gastric contents, or foreign bodies.
Etiology
Acute cough with fever is most often due to viral nasopharyngitis, including influenza, parainfluenza, respiratory syncytial virus, rhinovirus, coronavirus, and adenovirus. In adults with typical “common cold” syndromes, only mild temperature elevation is expected, and higher fever is atypical. Other acute causes include upper respiratory infections such as acute sinusitis and bronchitis, which are frequently viral and in which cough predominates, and lower respiratory infections such as pneumonia of bacterial, viral, fungal, or aspiration origin, bronchiectasis exacerbations, and lung abscess, as well as mediastinitis, endocarditis, malaria, and pulmonary embolism; several of these may also cause chronic cough with intermittent fever. Subacute cough may result from bacterial sinusitis or be postinfectious; even with minimal fever, pertussis must be considered because it can be mild or atypical after immunization yet remains highly contagious and dangerous to infants. Chronic cough with fever suggests tuberculosis in at-risk populations such as those with homelessness, HIV/AIDS, or exposure in endemic regions, and may also reflect chronic sinusitis, chronic melioidosis due to Burkholderia pseudomallei in Southeast Asia, endobronchial sarcoidosis, Kaposi sarcoma, lymphoma, airway-infiltrating tumors such as bronchogenic carcinoma or carcinoid, pulmonary embolism, or inflammatory pseudotumor. Cough and fever may also represent unrelated processes when their onsets differ, and chronic cough may stem from noninfectious causes such as gastroesophageal reflux, postnasal drip, ACE-inhibitor effect, or asthma.
Commonly Associated Conditions
HIV/AIDS and other immunodeficiency states are frequently linked to cough with fever and broaden the infectious and noninfectious differential.
Diagnosis
History
Because severe febrile respiratory syndromes can rapidly progress to respiratory failure, the first step is to identify life-threatening illness or systemic toxicity, including bacterial pneumonia, influenza, SARS-like syndromes, high-consequence or bioterrorism-related infections, and pulmonary embolism. Assess for dyspnea, hemoptysis, sputum production, other infectious symptoms, and immunodeficiency. A detailed exposure and travel history is essential, and history may also point toward noninfectious causes such as pulmonary embolism after prolonged immobility or malignancy suggested by smoking, weight loss, and hemoptysis without tuberculosis risk factors.
Physical Examination
Examine lungs plus upper airway structures (mouth, throat, nose, sinuses) and ears, and judge overall appearance for severity, fatigue, and impending respiratory compromise. Evaluate for tachycardia (>100/min), tachypnea (>24/min), and impaired oxygenation. Focal rales and egophony support lower respiratory infection, but examination alone often cannot confirm pneumonia.
Diagnostic Tests and Interpretation
Laboratory Studies
Purulent sputum suggests chronic bronchitis, bronchiectasis, pneumonia, or lung abscess, while hemoptysis can occur in these disorders and may also indicate an endobronchial tumor. Sputum microscopy and Gram stain can sometimes identify pathogens and guide antibiotics, but overall yield is limited by variability in collection and interpretation and by inability of many pneumonia patients to produce sputum. For chronic cough in high–tuberculosis-prevalence settings, obtain sputum smears and cultures for acid-fast bacilli and a chest radiograph.
Imaging
Chest radiography helps distinguish upper versus lower respiratory involvement, detect pneumonia, and identify intrathoracic masses. Patients with a syndrome consistent with acute bronchitis who have normal vital signs and a normal lung exam generally do not need chest radiography because pneumonia likelihood is low. Radiographic infiltrate patterns can suggest but do not confirm specific causes: lobar consolidation, cavitation, and large pleural effusions favor bacterial infection; bilateral diffuse involvement may occur with Pneumocystis jirovecii, Legionella, viral infections, or Mycoplasma pneumoniae; necrotizing pneumonia with cavitation and empyema suggests aspiration, gram-negative organisms, or staphylococci; nodular or cavitary patterns may reflect lung abscess or infections such as Nocardia, actinomycosis, atypical mycobacteria, cryptococcosis, or aspergillosis; and focal infiltrates are common with bacteria (including Nocardia), mycobacteria, Cryptococcus, and Aspergillus. High-resolution CT is preferred to demonstrate airway dilation and confirm bronchiectasis, and chest CT helps assess infections not responding to therapy, delineate lung abscess, and evaluate postobstructive pneumonia due to a mass. If the diagnosis remains unclear, consider sinus imaging and otolaryngology evaluation, and assess for extrapulmonary spread such as brain abscess when neurologic or other systemic findings are present.
Diagnostic Procedures/Other
Fiberoptic bronchoscopy assists with specimen collection and histopathologic evaluation of suspected endobronchial tumors and can help define organism susceptibilities in pneumonia unresponsive to therapy using protected sampling techniques. Pleural fluid analysis and pleural biopsy can support diagnosis of tuberculosis or malignancy.
Treatment
Medications
Management depends on identifying the underlying cause and treating it specifically. Antibiotics are generally unnecessary for acute viral upper respiratory infection, and when bacterial sinusitis cannot be distinguished from viral URI at presentation, delaying antibiotics for about seven days is appropriate. Antibiotics are indicated for pneumonia, tuberculosis, and pertussis. Irritative nonproductive cough can be suppressed with antitussives that raise cough threshold such as codeine 15 mg four times daily or dextromethorphan 15 mg four times daily. Additional agents that may reduce cough include NSAIDs such as naproxen, sedating antihistamines for common-cold–related cough (with newer nonsedating antihistamines generally ineffective), and inhaled ipratropium 2–4 puffs four times daily in chronic bronchitis. Productive cough with substantial sputum should usually not be suppressed because secretion retention can worsen ventilation, impair aeration, and reduce host defense. Hydration and expectorants such as guaifenesin may help thin mucus and improve clearance. Inflammatory pseudotumors, though typically resected, have also responded to antibiotics, radiation, or corticosteroids, and may occasionally regress spontaneously.
Additional Treatment
Maintain hydration and support smoking cessation.
In-Patient Considerations
Initial Stabilization
Consider intubation and positive-pressure ventilation for respiratory fatigue or severe oxygenation/ventilation failure based on arterial blood gases. Implement infection control measures, including isolation and airborne precautions, when severe febrile respiratory illness occurs with epidemiologic features suggesting transmissible high-consequence infection, relevant travel, animal or laboratory exposure, or potential bioterrorism.
Admission Criteria
Tools such as the Pneumonia Severity Index, though developed for pneumonia, can help guide disposition in febrile respiratory illness. Advanced age, significant comorbidities, and abnormal vital signs such as tachypnea, tachycardia, hypotension, and altered physiology indicate higher risk of morbidity and mortality.
Ongoing Care and Follow-Up
Reinforce smoking cessation.
Prognosis
Community-acquired pneumonia carries an approximate mortality of 13%.
Complications
Severe coughing paroxysms can trigger syncope. Patients with tuberculosis and cough are infectious and can transmit disease.


- Published on
Emergency And Acute Medicine – Humerus Fracture
Basics
Overview And Definitions
Humerus fractures include injuries to the proximal humerus and the humeral shaft. Proximal humeral fractures are commonly categorized as nondisplaced, displaced, or fracture–dislocations and account for approximately 5% of all fractures. Incidence increases with age, with a female-to-male ratio of 4:1, and the majority of patients are older than 60 years. These fractures represent the third most common osteoporotic fracture, following hip and distal radius fractures.
The Neer classification system is widely used for proximal humeral fractures and describes injuries based on the number and location of fracture fragments. Fractures are classified as 2-, 3-, or 4-part injuries involving the anatomic neck, surgical neck, greater tuberosity, or lesser tuberosity. Fracture–dislocations are also included in this system.
Humeral shaft fractures account for less than 3% of all fractures and may be spiral, oblique, or transverse in pattern. The AO classification categorizes these injuries as simple, wedge, or comminuted (complex) fractures.
Mechanisms And Causes
Proximal humeral fractures most commonly result from low-energy mechanisms, particularly falls, often onto an outstretched hand. Less frequently, they occur due to violent muscle contraction during seizures or electrical shock, or from higher-energy trauma.
Humeral shaft fractures are typically caused by high-energy direct trauma, either penetrating or blunt, or by bending forces. Less commonly, they result from falls or repetitive stress injuries, such as those seen in throwing athletes.
Diagnosis
Clinical Features
Patients usually present with pain, swelling, and localized tenderness over the humerus. There is often difficulty initiating active movement, and the arm may be held tightly against the chest. Shortening of the extremity, crepitus, ecchymosis, and signs of neurovascular compromise may be present.
History
Key historical elements include the mechanism of injury, patient age, fall risk, underlying malignancy, and associated injuries.
Physical Examination
A complete examination of the affected extremity is essential. Inspection should assess for deformity, shortening, swelling, and open wounds. Range of motion at the shoulder and elbow should be evaluated as tolerated. A detailed neurovascular examination is mandatory.
Essential Evaluation
Individual nerve function must be assessed, with special attention to the radial nerve, particularly in midshaft fractures. Median, ulnar, axillary (sensation over the lateral shoulder), and musculocutaneous nerves (sensation over the lateral forearm) should also be evaluated.
Vascular assessment includes palpation of radial, ulnar, and brachial pulses and confirmation of adequate capillary refill. Imaging is required to define the extent and type of injury.
Pediatric Considerations
Humerus fractures are most common in children younger than 3 years or older than 12 years. Neonatal fractures may occur due to birth trauma, especially in infants weighing more than 4.5 kg or in breech deliveries, and may present as pseudoparalysis.
In older children, mechanisms are similar to adults. The thicker periosteum in children often limits displacement of humeral shaft fractures. Proximal humeral Salter–Harris type I injuries should be suspected when radiographs are normal but significant pain persists, with Salter–Harris type II being most common. Nonaccidental trauma must be considered, particularly in children younger than 3 years, especially with suspicious fracture patterns.
Diagnostic Studies And Interpretation
Imaging
Plain radiographs are the initial imaging modality. Proximal humeral fractures require at least three views: anteroposterior, lateral, and axillary. The axillary view is critical for evaluating tuberosity displacement, glenoid involvement, and humeral head alignment.
Humeral shaft fractures require anteroposterior and lateral views of the entire humerus, including both the shoulder and elbow joints to rule out associated injuries.
CT scanning is useful in complex or comminuted proximal humeral fractures and in suspected fracture–dislocations, helping define fracture anatomy and surgical planning.
Differential Diagnosis
Acute hemorrhagic bursitis
Traumatic rotator cuff tear
Shoulder dislocation
Acromioclavicular joint separation
Calcific tendinitis
Contusion
Tendon rupture
Neurapraxia
Pathologic fracture
Management
Prehospital Care
Excessive movement of the injured arm should be avoided to prevent further neurovascular injury. Immobilization with a sling and swath is recommended, with rapid transport for patients exhibiting neurologic or vascular deficits.
Initial Stabilization
Primary and secondary trauma surveys should be performed to identify associated injuries. Immobilization helps reduce pain, prevent displacement, and minimize neurovascular injury. An axillary pad may improve comfort. Ice application helps limit swelling. Open fractures require sterile coverage, tetanus prophylaxis, and parenteral antibiotics.
Emergency Department Management
Adequate analgesia is essential, with narcotics administered orally, intramuscularly, or intravenously as first-line therapy.
Most proximal humeral fractures are single-part injuries and can be managed nonoperatively with sling and swath immobilization and early range-of-motion exercises. Displaced or multipart fractures should be described using the Neer classification. Fractures with more than 1 cm of displacement or more than 45 degrees of angulation are considered displaced and require orthopedic consultation.
Two-part fractures may often be managed nonoperatively after reduction, whereas three- and four-part fractures may require operative fixation or hemiarthroplasty, depending on patient age, comorbidities, and functional expectations. Emergent orthopedic consultation is indicated for open fractures, irreducible fracture–dislocations, or vascular compromise.
Most humeral shaft fractures can be managed nonoperatively without reduction. Up to 20 degrees of anterior angulation, 30 degrees of varus angulation, and 3 cm of shortening are generally well tolerated. Nondisplaced fractures may be treated with a coaptation splint, except for transverse fractures, which are better managed with a sling and swath. Displaced fractures may require a hanging cast under orthopedic guidance. Emergent consultation is required for neurovascular compromise, open fractures, segmental fractures, articular involvement, or a “floating elbow.”
Medications
Pain control is achieved primarily with narcotic analgesics. NSAIDs may be used as adjunctive therapy. Procedural sedation may be required for closed reductions.
Follow-Up And Disposition
Admission Criteria
Open fractures
Fractures with vascular compromise
Displaced fractures not amenable to closed management
Significant associated injuries requiring observation
Discharge Criteria
Nondisplaced fractures
Fractures successfully treated with closed reduction
Most isolated humeral shaft fractures
Selected complex proximal humeral fractures after orthopedic consultation
Referral Considerations
Most patients require outpatient orthopedic follow-up. Proximal humeral fractures classified as Neer type 2–4 should be reviewed with orthopedics for definitive planning. Displaced humeral shaft fractures require orthopedic management with functional bracing, casting, or surgical fixation.
Follow-Up Recommendations
Early follow-up is recommended to reassess neurovascular status, pain control, and fracture alignment. Stable proximal humeral fractures should be evaluated for early range-of-motion therapy to reduce the risk of adhesive capsulitis.
Key Points And Common Pitfalls
A thorough neurovascular examination is essential for all humeral fractures and should be repeated after manipulation. Radial nerve injury is the most common neurologic deficit associated with humeral shaft fractures and typically resolves spontaneously over months. Proximal humeral fractures involving the surgical neck or articular surface carry a risk of avascular necrosis. Multipart proximal humeral fractures often do not require admission but must have a clear orthopedic management plan due to the potential need for surgical intervention.
Basics
Overview And Definitions
Humerus fractures include injuries to the proximal humerus and the humeral shaft. Proximal humeral fractures are commonly categorized as nondisplaced, displaced, or fracture–dislocations and account for approximately 5% of all fractures. Incidence increases with age, with a female-to-male ratio of 4:1, and the majority of patients are older than 60 years. These fractures represent the third most common osteoporotic fracture, following hip and distal radius fractures.
The Neer classification system is widely used for proximal humeral fractures and describes injuries based on the number and location of fracture fragments. Fractures are classified as 2-, 3-, or 4-part injuries involving the anatomic neck, surgical neck, greater tuberosity, or lesser tuberosity. Fracture–dislocations are also included in this system.
Humeral shaft fractures account for less than 3% of all fractures and may be spiral, oblique, or transverse in pattern. The AO classification categorizes these injuries as simple, wedge, or comminuted (complex) fractures.
Mechanisms And Causes
Proximal humeral fractures most commonly result from low-energy mechanisms, particularly falls, often onto an outstretched hand. Less frequently, they occur due to violent muscle contraction during seizures or electrical shock, or from higher-energy trauma.
Humeral shaft fractures are typically caused by high-energy direct trauma, either penetrating or blunt, or by bending forces. Less commonly, they result from falls or repetitive stress injuries, such as those seen in throwing athletes.
Diagnosis
Clinical Features
Patients usually present with pain, swelling, and localized tenderness over the humerus. There is often difficulty initiating active movement, and the arm may be held tightly against the chest. Shortening of the extremity, crepitus, ecchymosis, and signs of neurovascular compromise may be present.
History
Key historical elements include the mechanism of injury, patient age, fall risk, underlying malignancy, and associated injuries.
Physical Examination
A complete examination of the affected extremity is essential. Inspection should assess for deformity, shortening, swelling, and open wounds. Range of motion at the shoulder and elbow should be evaluated as tolerated. A detailed neurovascular examination is mandatory.
Essential Evaluation
Individual nerve function must be assessed, with special attention to the radial nerve, particularly in midshaft fractures. Median, ulnar, axillary (sensation over the lateral shoulder), and musculocutaneous nerves (sensation over the lateral forearm) should also be evaluated.
Vascular assessment includes palpation of radial, ulnar, and brachial pulses and confirmation of adequate capillary refill. Imaging is required to define the extent and type of injury.
Pediatric Considerations
Humerus fractures are most common in children younger than 3 years or older than 12 years. Neonatal fractures may occur due to birth trauma, especially in infants weighing more than 4.5 kg or in breech deliveries, and may present as pseudoparalysis.
In older children, mechanisms are similar to adults. The thicker periosteum in children often limits displacement of humeral shaft fractures. Proximal humeral Salter–Harris type I injuries should be suspected when radiographs are normal but significant pain persists, with Salter–Harris type II being most common. Nonaccidental trauma must be considered, particularly in children younger than 3 years, especially with suspicious fracture patterns.
Diagnostic Studies And Interpretation
Imaging
Plain radiographs are the initial imaging modality. Proximal humeral fractures require at least three views: anteroposterior, lateral, and axillary. The axillary view is critical for evaluating tuberosity displacement, glenoid involvement, and humeral head alignment.
Humeral shaft fractures require anteroposterior and lateral views of the entire humerus, including both the shoulder and elbow joints to rule out associated injuries.
CT scanning is useful in complex or comminuted proximal humeral fractures and in suspected fracture–dislocations, helping define fracture anatomy and surgical planning.
Differential Diagnosis
Acute hemorrhagic bursitis
Traumatic rotator cuff tear
Shoulder dislocation
Acromioclavicular joint separation
Calcific tendinitis
Contusion
Tendon rupture
Neurapraxia
Pathologic fracture
Management
Prehospital Care
Excessive movement of the injured arm should be avoided to prevent further neurovascular injury. Immobilization with a sling and swath is recommended, with rapid transport for patients exhibiting neurologic or vascular deficits.
Initial Stabilization
Primary and secondary trauma surveys should be performed to identify associated injuries. Immobilization helps reduce pain, prevent displacement, and minimize neurovascular injury. An axillary pad may improve comfort. Ice application helps limit swelling. Open fractures require sterile coverage, tetanus prophylaxis, and parenteral antibiotics.
Emergency Department Management
Adequate analgesia is essential, with narcotics administered orally, intramuscularly, or intravenously as first-line therapy.
Most proximal humeral fractures are single-part injuries and can be managed nonoperatively with sling and swath immobilization and early range-of-motion exercises. Displaced or multipart fractures should be described using the Neer classification. Fractures with more than 1 cm of displacement or more than 45 degrees of angulation are considered displaced and require orthopedic consultation.
Two-part fractures may often be managed nonoperatively after reduction, whereas three- and four-part fractures may require operative fixation or hemiarthroplasty, depending on patient age, comorbidities, and functional expectations. Emergent orthopedic consultation is indicated for open fractures, irreducible fracture–dislocations, or vascular compromise.
Most humeral shaft fractures can be managed nonoperatively without reduction. Up to 20 degrees of anterior angulation, 30 degrees of varus angulation, and 3 cm of shortening are generally well tolerated. Nondisplaced fractures may be treated with a coaptation splint, except for transverse fractures, which are better managed with a sling and swath. Displaced fractures may require a hanging cast under orthopedic guidance. Emergent consultation is required for neurovascular compromise, open fractures, segmental fractures, articular involvement, or a “floating elbow.”
Medications
Pain control is achieved primarily with narcotic analgesics. NSAIDs may be used as adjunctive therapy. Procedural sedation may be required for closed reductions.
Follow-Up And Disposition
Admission Criteria
Open fractures
Fractures with vascular compromise
Displaced fractures not amenable to closed management
Significant associated injuries requiring observation
Discharge Criteria
Nondisplaced fractures
Fractures successfully treated with closed reduction
Most isolated humeral shaft fractures
Selected complex proximal humeral fractures after orthopedic consultation
Referral Considerations
Most patients require outpatient orthopedic follow-up. Proximal humeral fractures classified as Neer type 2–4 should be reviewed with orthopedics for definitive planning. Displaced humeral shaft fractures require orthopedic management with functional bracing, casting, or surgical fixation.
Follow-Up Recommendations
Early follow-up is recommended to reassess neurovascular status, pain control, and fracture alignment. Stable proximal humeral fractures should be evaluated for early range-of-motion therapy to reduce the risk of adhesive capsulitis.
Key Points And Common Pitfalls
A thorough neurovascular examination is essential for all humeral fractures and should be repeated after manipulation. Radial nerve injury is the most common neurologic deficit associated with humeral shaft fractures and typically resolves spontaneously over months. Proximal humeral fractures involving the surgical neck or articular surface carry a risk of avascular necrosis. Multipart proximal humeral fractures often do not require admission but must have a clear orthopedic management plan due to the potential need for surgical intervention.


- Published on
Emergency And Acute Medicine – Horner’s Syndrome
Basics
Condition Summary
Horner’s syndrome results from unilateral interruption of the sympathetic pathway to the eye and face. Loss of sympathetic innervation produces a characteristic triad. Relaxation of the upper and lower eyelid retractors leads to ptosis (drooping of the eyelid). Disruption of pupillary dilator fibers causes miosis, with unopposed pupillary constriction. Loss of sympathetic input to facial sweat glands results in anhidrosis on the affected side.
Etiology And Causes
In approximately 40% of cases, no cause is identified. Neoplastic disease, particularly lung tumors or metastases to cervical lymph nodes, may interrupt preganglionic sympathetic fibers between the thoracic sympathetic trunk and the superior cervical ganglion.
Trauma, including penetrating neck injuries, may directly damage sympathetic fibers. Pneumothorax, especially tension pneumothorax, can cause traction on the sympathetic chain due to mediastinal shift.
Infiltration or infection of cervical lymph nodes, such as from sarcoidosis or tuberculosis, may also disrupt the pathway.
Vascular etiologies include migraine or cluster headaches and carotid artery dissection. Lateral medullary (Wallenberg) infarction may present with Horner’s syndrome accompanied by vertigo and ataxia, which can overshadow ocular findings. Cavernous sinus thrombosis may produce partial Horner-like features along with headache, eye pain, ocular motor palsies, chemosis, and proptosis.
Pediatric Considerations
Congenital or hereditary Horner’s syndrome may present with heterochromia iridis, characterized by a lighter (often blue) iris on the affected side and a darker iris on the unaffected side. Birth trauma can injure the sympathetic chain. New-onset Horner’s syndrome in a child warrants evaluation for an underlying tumor, particularly neuroblastoma.
Diagnosis
Clinical Features
Horner’s syndrome is defined by a classic triad: mild ptosis on the affected side, miosis with pupillary asymmetry of at least 1 mm, and ipsilateral facial anhidrosis. The clinical importance lies in its association with potentially serious underlying conditions rather than the ocular findings alone.
History
History should focus on conditions that predispose to Horner’s syndrome or its causes, including malignancy, vascular disease, and trauma. Minor trauma may precede carotid artery dissection. Cardiovascular risk factors and relevant exposures should be assessed. The presence of pain, particularly neck or facial pain, raises concern for carotid dissection.
Alert
Acute onset Horner’s syndrome associated with neck or facial pain should be presumed to be due to carotid artery dissection until proven otherwise, as approximately half of internal carotid dissections present with a painful Horner’s syndrome.
Physical Examination
A focused neurologic examination is essential to confirm Horner’s syndrome and identify additional neurologic deficits. The general examination should look for signs of associated conditions such as tumors, trauma, or pulmonary pathology.
Essential Evaluation
Assessment includes a thorough history and neurologic examination. A chest radiograph is recommended to screen for apical lung tumors or pneumothorax.
Diagnostic Studies And Interpretation
Provocative Testing
Pharmacologic confirmation can be achieved with ocular cocaine testing. One drop of 5% cocaine solution (2.5% in children) is instilled into each eye. Failure of the affected pupil to dilate compared with the unaffected pupil, resulting in increased anisocoria after approximately one hour, confirms a sympathetic denervation lesion.
Laboratory Testing
Laboratory studies are not useful for diagnosing Horner’s syndrome itself but may be indicated to evaluate suspected underlying conditions.
Imaging
Chest radiography is often indicated due to the association between Horner’s syndrome and intrathoracic pathology. CT or MRI of the head, neck, or chest should be guided by clinical findings.
When carotid artery dissection is suspected, CT angiography or MR angiography of the head and neck is appropriate, with the lesion expected on the same side as the Horner’s syndrome. If stroke is suspected, at minimum a noncontrast CT of the brain is required to exclude hemorrhage. Patients within the thrombolysis window should undergo emergent imaging per local stroke protocols.
Diagnostic Procedures
Ocular tonometry should be performed if acute glaucoma is a consideration.
Differential Diagnosis
Elevated intracranial pressure, typically associated with headache and altered consciousness
Physiologic anisocoria (pseudo–Horner’s syndrome), which is common and yields a negative cocaine test
Topical medications or exposures causing miosis
Migraine or cluster headache
Glaucoma, inflammatory eye disease, or ocular trauma
Management
Prehospital Considerations
Horner’s syndrome itself is benign, but associated life-threatening conditions must be rapidly identified. Increased intracranial pressure or tension pneumothorax requires immediate intervention. Patients with suspected acute stroke should be transported to a designated stroke center when feasible.
Initial Stabilization
If elevated intracranial pressure is suspected, initiate airway protection and intracranial pressure–lowering measures, including osmotic therapy. Tension pneumothorax requires immediate needle decompression followed by chest tube placement.
Emergency Department Care
Horner’s syndrome does not require direct treatment in the ED. Management is directed at identifying and treating the underlying cause.
Medications
Cocaine ophthalmic solution (5% in adults, 2.5% in children) is used diagnostically, with one drop placed in each eye.
Follow-Up And Disposition
Admission Criteria
Admission is not required for isolated Horner’s syndrome but may be necessary for associated conditions such as stroke, carotid dissection, malignancy, or infection.
Discharge Criteria
Stable patients with isolated Horner’s syndrome may be discharged with appropriate outpatient follow-up once emergent causes, particularly carotid dissection and stroke, have been reasonably excluded.
Follow-Up Recommendations
Ongoing evaluation often requires coordination with neurology and ophthalmology to identify the underlying etiology and guide further management.
Key Points And Common Pitfalls
The primary importance of Horner’s syndrome lies in recognizing its potential underlying causes. Failure to evaluate for serious etiologies such as carotid artery dissection, stroke, or malignancy is a critical pitfall.
Basics
Condition Summary
Horner’s syndrome results from unilateral interruption of the sympathetic pathway to the eye and face. Loss of sympathetic innervation produces a characteristic triad. Relaxation of the upper and lower eyelid retractors leads to ptosis (drooping of the eyelid). Disruption of pupillary dilator fibers causes miosis, with unopposed pupillary constriction. Loss of sympathetic input to facial sweat glands results in anhidrosis on the affected side.
Etiology And Causes
In approximately 40% of cases, no cause is identified. Neoplastic disease, particularly lung tumors or metastases to cervical lymph nodes, may interrupt preganglionic sympathetic fibers between the thoracic sympathetic trunk and the superior cervical ganglion.
Trauma, including penetrating neck injuries, may directly damage sympathetic fibers. Pneumothorax, especially tension pneumothorax, can cause traction on the sympathetic chain due to mediastinal shift.
Infiltration or infection of cervical lymph nodes, such as from sarcoidosis or tuberculosis, may also disrupt the pathway.
Vascular etiologies include migraine or cluster headaches and carotid artery dissection. Lateral medullary (Wallenberg) infarction may present with Horner’s syndrome accompanied by vertigo and ataxia, which can overshadow ocular findings. Cavernous sinus thrombosis may produce partial Horner-like features along with headache, eye pain, ocular motor palsies, chemosis, and proptosis.
Pediatric Considerations
Congenital or hereditary Horner’s syndrome may present with heterochromia iridis, characterized by a lighter (often blue) iris on the affected side and a darker iris on the unaffected side. Birth trauma can injure the sympathetic chain. New-onset Horner’s syndrome in a child warrants evaluation for an underlying tumor, particularly neuroblastoma.
Diagnosis
Clinical Features
Horner’s syndrome is defined by a classic triad: mild ptosis on the affected side, miosis with pupillary asymmetry of at least 1 mm, and ipsilateral facial anhidrosis. The clinical importance lies in its association with potentially serious underlying conditions rather than the ocular findings alone.
History
History should focus on conditions that predispose to Horner’s syndrome or its causes, including malignancy, vascular disease, and trauma. Minor trauma may precede carotid artery dissection. Cardiovascular risk factors and relevant exposures should be assessed. The presence of pain, particularly neck or facial pain, raises concern for carotid dissection.
Alert
Acute onset Horner’s syndrome associated with neck or facial pain should be presumed to be due to carotid artery dissection until proven otherwise, as approximately half of internal carotid dissections present with a painful Horner’s syndrome.
Physical Examination
A focused neurologic examination is essential to confirm Horner’s syndrome and identify additional neurologic deficits. The general examination should look for signs of associated conditions such as tumors, trauma, or pulmonary pathology.
Essential Evaluation
Assessment includes a thorough history and neurologic examination. A chest radiograph is recommended to screen for apical lung tumors or pneumothorax.
Diagnostic Studies And Interpretation
Provocative Testing
Pharmacologic confirmation can be achieved with ocular cocaine testing. One drop of 5% cocaine solution (2.5% in children) is instilled into each eye. Failure of the affected pupil to dilate compared with the unaffected pupil, resulting in increased anisocoria after approximately one hour, confirms a sympathetic denervation lesion.
Laboratory Testing
Laboratory studies are not useful for diagnosing Horner’s syndrome itself but may be indicated to evaluate suspected underlying conditions.
Imaging
Chest radiography is often indicated due to the association between Horner’s syndrome and intrathoracic pathology. CT or MRI of the head, neck, or chest should be guided by clinical findings.
When carotid artery dissection is suspected, CT angiography or MR angiography of the head and neck is appropriate, with the lesion expected on the same side as the Horner’s syndrome. If stroke is suspected, at minimum a noncontrast CT of the brain is required to exclude hemorrhage. Patients within the thrombolysis window should undergo emergent imaging per local stroke protocols.
Diagnostic Procedures
Ocular tonometry should be performed if acute glaucoma is a consideration.
Differential Diagnosis
Elevated intracranial pressure, typically associated with headache and altered consciousness
Physiologic anisocoria (pseudo–Horner’s syndrome), which is common and yields a negative cocaine test
Topical medications or exposures causing miosis
Migraine or cluster headache
Glaucoma, inflammatory eye disease, or ocular trauma
Management
Prehospital Considerations
Horner’s syndrome itself is benign, but associated life-threatening conditions must be rapidly identified. Increased intracranial pressure or tension pneumothorax requires immediate intervention. Patients with suspected acute stroke should be transported to a designated stroke center when feasible.
Initial Stabilization
If elevated intracranial pressure is suspected, initiate airway protection and intracranial pressure–lowering measures, including osmotic therapy. Tension pneumothorax requires immediate needle decompression followed by chest tube placement.
Emergency Department Care
Horner’s syndrome does not require direct treatment in the ED. Management is directed at identifying and treating the underlying cause.
Medications
Cocaine ophthalmic solution (5% in adults, 2.5% in children) is used diagnostically, with one drop placed in each eye.
Follow-Up And Disposition
Admission Criteria
Admission is not required for isolated Horner’s syndrome but may be necessary for associated conditions such as stroke, carotid dissection, malignancy, or infection.
Discharge Criteria
Stable patients with isolated Horner’s syndrome may be discharged with appropriate outpatient follow-up once emergent causes, particularly carotid dissection and stroke, have been reasonably excluded.
Follow-Up Recommendations
Ongoing evaluation often requires coordination with neurology and ophthalmology to identify the underlying etiology and guide further management.
Key Points And Common Pitfalls
The primary importance of Horner’s syndrome lies in recognizing its potential underlying causes. Failure to evaluate for serious etiologies such as carotid artery dissection, stroke, or malignancy is a critical pitfall.
- Published on
Emergency And Acute Medicine – Hordeolum And Chalazion
Basics
Clinical Overview
Hordeola and chalazia arise from inflammatory processes involving the eyelid glands along the lash margin. A hordeolum represents an acute obstruction of an eyelid gland that leads to inflammation and often abscess formation. A chalazion is the chronic consequence of retained, thickened glandular secretions, producing a granulomatous inflammatory response.
A hordeolum develops when outflow obstruction affects one or more eyelid glands. Secondary bacterial infection may occur, and progression to a localized abscess or, less commonly, periorbital cellulitis is possible.
A chalazion reflects chronic granulomatous inflammation of a meibomian gland. Blockage of the duct at the eyelid margin may cause glandular contents to leak into surrounding eyelid tissue, triggering a lipogranulomatous reaction. Chalazia are occasionally secondarily infected and may evolve from an incompletely resolved internal hordeolum.
Etiology And Risk Factors
Hordeola may become secondarily infected, most commonly with Staphylococcus species. Predisposing conditions include meibomian gland dysfunction, chronic blepharitis, rosacea, and a history of prior hordeola.
Diagnosis
Clinical Features
A hordeolum typically presents acutely as a red, tender, painful, swollen lesion along the eyelid margin. Lesions are usually solitary but may be multiple or recurrent. Inflammation is well localized, and presentation varies depending on the gland involved.
An external hordeolum (stye) originates from obstruction of superficial sebaceous or sweat glands with ducts between the eyelashes. It appears as an exquisitely tender lesion that often points anteriorly.
An internal hordeolum arises from obstruction of deeper sebaceous glands whose ducts open on the inner eyelid margin. It presents as a painful, palpable mass within the lid, may cause foreign body sensation or visual disturbance, and is often larger and more inflamed than external lesions. It may drain internally toward the conjunctiva or externally through the skin.
Hordeola are localized processes without systemic symptoms but may be complicated by conjunctivitis or periorbital cellulitis.
A chalazion presents as a firm, well-circumscribed, nontender or minimally tender eyelid nodule that is typically long-standing and noninflamed. Symptoms usually relate to its size and location, including cosmetic distortion, obstruction of the visual field, pressure on the globe, or corneal drying or injury from exposure. Chalazia are nonacute and nonemergent unless significant corneal compromise or globe pressure occurs.
History
Hordeolum is characterized by sudden onset of a well-localized, painful eyelid mass without systemic symptoms.
Physical Examination
Findings include focal tenderness and inflammation of an external or internal eyelid gland, with minimal surrounding edema. An abscess may point at the lash line, the palpebral conjunctiva, or externally through the skin.
Essential Evaluation
A complete ophthalmologic assessment should be performed, including slit-lamp examination and corneal evaluation. Patients should be assessed for associated cellulitis or systemic involvement.
For hordeola, identifying the gland of origin is important.
For chalazia, evaluation should focus on whether the lesion causes corneal exposure or injury.
Diagnostic Studies And Interpretation
Laboratory Testing
Cultures of expressed or draining material are rarely useful and typically do not alter management.
Differential Diagnosis
Blepharitis
Dacryocystitis
Dacryoadenitis
Pyogenic granuloma
Sebaceous cell carcinoma
Basal cell carcinoma
Squamous cell carcinoma
Management
Emergency Department Care
For hordeola, treatment focuses on relieving obstruction and preventing abscess formation. Warm compresses applied for 15 minutes, 4–6 times daily, are first-line therapy. Gentle massage of the lesion may help express obstructed material.
In rare severe cases, incision and drainage of an internal hordeolum may be required and is typically performed by an ophthalmologist. When drainage is toward the conjunctiva, a vertical incision is preferred to minimize meibomian gland injury and reduce the risk of corneal scarring. External skin incisions are rarely indicated; if required, a horizontal incision is used. In select severe external hordeola, removal of a single involved eyelash may be helpful.
Chalazia generally require no emergent intervention. Management is typically referral-based, with ophthalmologic options including incision and curettage or intralesional steroid injection. Lubricating eye drops may provide symptomatic relief.
Medications
Ophthalmic lubricating drops may be used as needed for comfort.
Follow-Up And Disposition
Discharge Criteria
Patients may be discharged if there is no evidence of secondary complications such as significant periorbital cellulitis with systemic symptoms.
Referral Considerations
Urgent ophthalmology consultation should be obtained if incision and drainage of an internal hordeolum is considered. Chalazia should be referred for definitive ophthalmologic management.
Follow-Up Recommendations
Ophthalmology follow-up within 1–2 days is recommended to assess response to conservative therapy. Most symptoms resolve completely within 1–2 weeks.
Key Points And Common Pitfalls
Conservative management with warm compresses and gentle massage is the standard of care for hordeola, with most cases resolving without further intervention.
Emergent incision and drainage is rarely necessary and carries risks including corneal injury, fistula formation, and cosmetic complications; ophthalmology consultation is preferred.
Chalazia do not require emergent treatment and are best managed with outpatient referral.
Basics
Clinical Overview
Hordeola and chalazia arise from inflammatory processes involving the eyelid glands along the lash margin. A hordeolum represents an acute obstruction of an eyelid gland that leads to inflammation and often abscess formation. A chalazion is the chronic consequence of retained, thickened glandular secretions, producing a granulomatous inflammatory response.
A hordeolum develops when outflow obstruction affects one or more eyelid glands. Secondary bacterial infection may occur, and progression to a localized abscess or, less commonly, periorbital cellulitis is possible.
A chalazion reflects chronic granulomatous inflammation of a meibomian gland. Blockage of the duct at the eyelid margin may cause glandular contents to leak into surrounding eyelid tissue, triggering a lipogranulomatous reaction. Chalazia are occasionally secondarily infected and may evolve from an incompletely resolved internal hordeolum.
Etiology And Risk Factors
Hordeola may become secondarily infected, most commonly with Staphylococcus species. Predisposing conditions include meibomian gland dysfunction, chronic blepharitis, rosacea, and a history of prior hordeola.
Diagnosis
Clinical Features
A hordeolum typically presents acutely as a red, tender, painful, swollen lesion along the eyelid margin. Lesions are usually solitary but may be multiple or recurrent. Inflammation is well localized, and presentation varies depending on the gland involved.
An external hordeolum (stye) originates from obstruction of superficial sebaceous or sweat glands with ducts between the eyelashes. It appears as an exquisitely tender lesion that often points anteriorly.
An internal hordeolum arises from obstruction of deeper sebaceous glands whose ducts open on the inner eyelid margin. It presents as a painful, palpable mass within the lid, may cause foreign body sensation or visual disturbance, and is often larger and more inflamed than external lesions. It may drain internally toward the conjunctiva or externally through the skin.
Hordeola are localized processes without systemic symptoms but may be complicated by conjunctivitis or periorbital cellulitis.
A chalazion presents as a firm, well-circumscribed, nontender or minimally tender eyelid nodule that is typically long-standing and noninflamed. Symptoms usually relate to its size and location, including cosmetic distortion, obstruction of the visual field, pressure on the globe, or corneal drying or injury from exposure. Chalazia are nonacute and nonemergent unless significant corneal compromise or globe pressure occurs.
History
Hordeolum is characterized by sudden onset of a well-localized, painful eyelid mass without systemic symptoms.
Physical Examination
Findings include focal tenderness and inflammation of an external or internal eyelid gland, with minimal surrounding edema. An abscess may point at the lash line, the palpebral conjunctiva, or externally through the skin.
Essential Evaluation
A complete ophthalmologic assessment should be performed, including slit-lamp examination and corneal evaluation. Patients should be assessed for associated cellulitis or systemic involvement.
For hordeola, identifying the gland of origin is important.
For chalazia, evaluation should focus on whether the lesion causes corneal exposure or injury.
Diagnostic Studies And Interpretation
Laboratory Testing
Cultures of expressed or draining material are rarely useful and typically do not alter management.
Differential Diagnosis
Blepharitis
Dacryocystitis
Dacryoadenitis
Pyogenic granuloma
Sebaceous cell carcinoma
Basal cell carcinoma
Squamous cell carcinoma
Management
Emergency Department Care
For hordeola, treatment focuses on relieving obstruction and preventing abscess formation. Warm compresses applied for 15 minutes, 4–6 times daily, are first-line therapy. Gentle massage of the lesion may help express obstructed material.
In rare severe cases, incision and drainage of an internal hordeolum may be required and is typically performed by an ophthalmologist. When drainage is toward the conjunctiva, a vertical incision is preferred to minimize meibomian gland injury and reduce the risk of corneal scarring. External skin incisions are rarely indicated; if required, a horizontal incision is used. In select severe external hordeola, removal of a single involved eyelash may be helpful.
Chalazia generally require no emergent intervention. Management is typically referral-based, with ophthalmologic options including incision and curettage or intralesional steroid injection. Lubricating eye drops may provide symptomatic relief.
Medications
Ophthalmic lubricating drops may be used as needed for comfort.
Follow-Up And Disposition
Discharge Criteria
Patients may be discharged if there is no evidence of secondary complications such as significant periorbital cellulitis with systemic symptoms.
Referral Considerations
Urgent ophthalmology consultation should be obtained if incision and drainage of an internal hordeolum is considered. Chalazia should be referred for definitive ophthalmologic management.
Follow-Up Recommendations
Ophthalmology follow-up within 1–2 days is recommended to assess response to conservative therapy. Most symptoms resolve completely within 1–2 weeks.
Key Points And Common Pitfalls
Conservative management with warm compresses and gentle massage is the standard of care for hordeola, with most cases resolving without further intervention.
Emergent incision and drainage is rarely necessary and carries risks including corneal injury, fistula formation, and cosmetic complications; ophthalmology consultation is preferred.
Chalazia do not require emergent treatment and are best managed with outpatient referral.
- Published on
Emergency And Acute Medicine – HIV And AIDS
Basics
Foundational Overview
Acquired immunodeficiency syndrome (AIDS) is defined by laboratory evidence of HIV infection with a CD4 count below 200 cells/mm³ or the presence of an AIDS-defining condition. These conditions include opportunistic infections (such as cryptosporidiosis), malignancies (including Kaposi sarcoma or invasive cervical cancer), and other HIV-related illnesses such as wasting syndrome or HIV-associated encephalopathy.
Opportunistic conditions correlate strongly with immune suppression:
At CD4 counts below 500 cells/mm³, patients are at risk for oroesophageal candidiasis, pneumococcal infections, oral hairy leukoplakia, and immune thrombocytopenic purpura.
At CD4 counts below 200 cells/mm³, common conditions include Pneumocystis jirovecii pneumonia (PCP), cryptococcal infection, disseminated tuberculosis, cryptosporidiosis, isosporiasis, toxoplasmosis, and histoplasmosis.
At CD4 counts below 50 cells/mm³, patients are vulnerable to central nervous system lymphoma, Mycobacterium avium complex (MAC), tuberculosis pericarditis or meningitis, cytomegalovirus (CMV) infection, and HIV-associated cholangiopathy, most commonly caused by Cryptosporidium parvum.
Diagnosis
Clinical Manifestations
Primary HIV infection typically occurs 2–6 weeks after exposure and may present with fever, malaise, a rash involving the face and trunk, flu-like symptoms with lymphadenopathy and hepatosplenomegaly, pharyngitis, and diarrhea. Up to 90% of patients may be asymptomatic during this stage.
Advanced HIV disease, usually defined by CD4 counts below 200 cells/mm³, commonly presents with fatigue, fevers, night sweats, weight loss or wasting, alopecia, chronic diarrhea, cough, dyspnea, hemoptysis, chronic low-grade headaches, altered mental status, seizures, dementia, neuropathy, painless visual loss, and various skin lesions.
History
Important risk factors include multiple sexual partners, unprotected intercourse with high-risk partners, men who have sex with men, intravenous drug use, blood transfusions prior to 1985, and lack of circumcision. Key historical elements include most recent and lowest recorded CD4 count, viral load, history of antiretroviral therapy and adherence, duration of HIV diagnosis, previous opportunistic infections, and prior hospitalizations or ICU admissions.
Initial Evaluation
HIV serologic testing is essential, recognizing a window period of up to 24 weeks between infection and seroconversion during which tests may be negative. HIV DNA amplification testing can detect infection within 1–2 weeks but is rarely available in the ED and requires careful follow-up.
Patients with respiratory symptoms require chest radiography, arterial blood gas analysis, sputum evaluation for Gram stain, acid-fast bacilli, and cultures, serum LDH levels, and blood cultures.
Cardiac symptoms warrant cardiac biomarkers, electrolytes, ECG, chest radiography, and blood cultures if endocarditis is suspected.
Neurologic symptoms require head CT with and without contrast and lumbar puncture with opening pressure and comprehensive CSF studies.
Gastrointestinal symptoms necessitate stool studies, urinalysis, pregnancy testing in women, pelvic examination when appropriate, liver enzymes, pancreatic enzymes, hepatitis serologies, and a low threshold for abdominal imaging or surgical consultation.
Fever of unknown origin requires broad infectious evaluation including bacterial, fungal, AFB, and MAC cultures.
Ocular complaints require slit-lamp examination with fluorescein staining.
Diagnostic Studies And Interpretation
Laboratory Testing
ELISA testing detects IgG antibodies against HIV with approximately 99% sensitivity and specificity but may be negative during the window period. Western blot testing confirms positive ELISA results by detecting antibodies to HIV proteins. Rapid HIV testing provides results within 5–20 minutes using oral swabs or blood samples but requires confirmatory testing.
Absolute lymphocyte count can estimate immune status: values above 2,000 cells/mm³ often correlate with CD4 counts above 200, while counts below 1,000 suggest advanced immunosuppression.
Imaging
Chest radiographs may show bilateral interstitial infiltrates in PCP, reticulonodular patterns in TB or fungal infections, hilar lymphadenopathy in TB or malignancy, lobar consolidation in bacterial pneumonia, or cavitary lesions in TB and necrotizing infections. A normal chest x-ray does not exclude PCP or TB.
Head CT may demonstrate multiple ring-enhancing lesions consistent with toxoplasmosis or CNS lymphoma, or nonenhancing subcortical lesions suggestive of progressive multifocal leukoencephalopathy.
Abdominal and pelvic CT imaging may reveal splenomegaly, intestinal perforation or obstruction, biliary disease, or pancreatitis related to infection, malignancy, or medications.
Differential Diagnosis
Pulmonary complaints may represent pulmonary embolism, pulmonary hypertension, TB, bacterial, viral, or fungal pneumonia, malignancy, or lymphocytic interstitial pneumonitis.
Neurologic symptoms raise concern for neurosyphilis, viral encephalitis, toxoplasmosis, CNS lymphoma, meningitis, stroke, metabolic encephalopathy, or progressive multifocal leukoencephalopathy.
Cardiac presentations include cardiomyopathy, myocarditis, pericarditis, endocarditis, acute coronary syndrome, or pericardial effusion.
Oral and esophageal symptoms may result from candidiasis, viral infections, bacterial disease, autoimmune conditions, or malignancy.
Chronic diarrhea, hepatomegaly, and renal dysfunction have broad infectious, metabolic, medication-related, and neoplastic etiologies in HIV-infected patients.
Treatment
Emergency Department Management
Patients appearing toxic or with rapidly progressive illness should receive empiric antibiotics in the ED. Initiation of antiretroviral therapy is recommended for patients with low CD4 counts, high viral loads, pregnancy, AIDS-defining illnesses, or HIV-associated nephropathy.
Highly active antiretroviral therapy (HAART) typically consists of triple therapy using combinations of non-nucleoside reverse transcriptase inhibitors, protease inhibitors, and nucleoside reverse transcriptase inhibitors.
Post-exposure prophylaxis should begin within 2 hours of exposure when possible and continue for 4 weeks, with two-drug regimens for most exposures and expanded three-drug regimens for high-risk cases.
Specific opportunistic infections require targeted therapy, including pyrimethamine-based regimens for toxoplasmosis, amphotericin B with flucytosine for cryptococcal meningitis, ganciclovir for CMV retinitis, fluconazole for esophageal candidiasis, clarithromycin-based therapy for MAC, trimethoprim-sulfamethoxazole for PCP with adjunctive steroids when hypoxemia is present, and plasmapheresis for acute HIV-related demyelinating neuropathy.
Medication-Related Considerations
Antiretroviral therapy is associated with numerous potential adverse effects including hypersensitivity reactions, pancreatitis, peripheral neuropathy, nephrolithiasis, hepatotoxicity, lactic acidosis, Stevens–Johnson syndrome, hemolytic anemia, neuropsychiatric effects, metabolic derangements, cardiomyopathy, and hematologic abnormalities.
Follow-Up And Disposition
Admission Criteria
Indications for hospitalization include unexplained fever with neurologic involvement, hypoxemia, suspected acute coronary syndrome, pericardial effusion, suspected bacterial pneumonia or TB, new neurologic deficits or seizures, hemodynamic instability, inability to ambulate or tolerate oral intake, and severe diarrhea with dehydration.
Discharge Criteria
Patients may be discharged if they can maintain oral intake, ambulate, perform self-care, and have reliable follow-up.
Referral Considerations
All patients should be referred to an HIV specialist for initiation and management of antiretroviral therapy. Screening for depression and psychiatric referral are essential to ensure treatment adherence. Patients with concerning symptoms should be referred for malignancy evaluation.
Key Clinical Insights And Common Pitfalls
Immune reconstitution inflammatory syndrome typically occurs within 8 weeks of initiating HAART. Occupational exposure carries a low but real risk of seroconversion. Patients on HAART have increased risk for metabolic disease and acute coronary syndromes. Exercise-induced desaturation may aid in diagnosing PCP when imaging is normal. HIV is an independent risk factor for COPDukar
COPD, pulmonary hypertension, stroke, venous thromboembolism, thrombotic thrombocytopenic purpura, osteoporosis, and osteonecrosis of the hip.
Basics
Foundational Overview
Acquired immunodeficiency syndrome (AIDS) is defined by laboratory evidence of HIV infection with a CD4 count below 200 cells/mm³ or the presence of an AIDS-defining condition. These conditions include opportunistic infections (such as cryptosporidiosis), malignancies (including Kaposi sarcoma or invasive cervical cancer), and other HIV-related illnesses such as wasting syndrome or HIV-associated encephalopathy.
Opportunistic conditions correlate strongly with immune suppression:
At CD4 counts below 500 cells/mm³, patients are at risk for oroesophageal candidiasis, pneumococcal infections, oral hairy leukoplakia, and immune thrombocytopenic purpura.
At CD4 counts below 200 cells/mm³, common conditions include Pneumocystis jirovecii pneumonia (PCP), cryptococcal infection, disseminated tuberculosis, cryptosporidiosis, isosporiasis, toxoplasmosis, and histoplasmosis.
At CD4 counts below 50 cells/mm³, patients are vulnerable to central nervous system lymphoma, Mycobacterium avium complex (MAC), tuberculosis pericarditis or meningitis, cytomegalovirus (CMV) infection, and HIV-associated cholangiopathy, most commonly caused by Cryptosporidium parvum.
Diagnosis
Clinical Manifestations
Primary HIV infection typically occurs 2–6 weeks after exposure and may present with fever, malaise, a rash involving the face and trunk, flu-like symptoms with lymphadenopathy and hepatosplenomegaly, pharyngitis, and diarrhea. Up to 90% of patients may be asymptomatic during this stage.
Advanced HIV disease, usually defined by CD4 counts below 200 cells/mm³, commonly presents with fatigue, fevers, night sweats, weight loss or wasting, alopecia, chronic diarrhea, cough, dyspnea, hemoptysis, chronic low-grade headaches, altered mental status, seizures, dementia, neuropathy, painless visual loss, and various skin lesions.
History
Important risk factors include multiple sexual partners, unprotected intercourse with high-risk partners, men who have sex with men, intravenous drug use, blood transfusions prior to 1985, and lack of circumcision. Key historical elements include most recent and lowest recorded CD4 count, viral load, history of antiretroviral therapy and adherence, duration of HIV diagnosis, previous opportunistic infections, and prior hospitalizations or ICU admissions.
Initial Evaluation
HIV serologic testing is essential, recognizing a window period of up to 24 weeks between infection and seroconversion during which tests may be negative. HIV DNA amplification testing can detect infection within 1–2 weeks but is rarely available in the ED and requires careful follow-up.
Patients with respiratory symptoms require chest radiography, arterial blood gas analysis, sputum evaluation for Gram stain, acid-fast bacilli, and cultures, serum LDH levels, and blood cultures.
Cardiac symptoms warrant cardiac biomarkers, electrolytes, ECG, chest radiography, and blood cultures if endocarditis is suspected.
Neurologic symptoms require head CT with and without contrast and lumbar puncture with opening pressure and comprehensive CSF studies.
Gastrointestinal symptoms necessitate stool studies, urinalysis, pregnancy testing in women, pelvic examination when appropriate, liver enzymes, pancreatic enzymes, hepatitis serologies, and a low threshold for abdominal imaging or surgical consultation.
Fever of unknown origin requires broad infectious evaluation including bacterial, fungal, AFB, and MAC cultures.
Ocular complaints require slit-lamp examination with fluorescein staining.
Diagnostic Studies And Interpretation
Laboratory Testing
ELISA testing detects IgG antibodies against HIV with approximately 99% sensitivity and specificity but may be negative during the window period. Western blot testing confirms positive ELISA results by detecting antibodies to HIV proteins. Rapid HIV testing provides results within 5–20 minutes using oral swabs or blood samples but requires confirmatory testing.
Absolute lymphocyte count can estimate immune status: values above 2,000 cells/mm³ often correlate with CD4 counts above 200, while counts below 1,000 suggest advanced immunosuppression.
Imaging
Chest radiographs may show bilateral interstitial infiltrates in PCP, reticulonodular patterns in TB or fungal infections, hilar lymphadenopathy in TB or malignancy, lobar consolidation in bacterial pneumonia, or cavitary lesions in TB and necrotizing infections. A normal chest x-ray does not exclude PCP or TB.
Head CT may demonstrate multiple ring-enhancing lesions consistent with toxoplasmosis or CNS lymphoma, or nonenhancing subcortical lesions suggestive of progressive multifocal leukoencephalopathy.
Abdominal and pelvic CT imaging may reveal splenomegaly, intestinal perforation or obstruction, biliary disease, or pancreatitis related to infection, malignancy, or medications.
Differential Diagnosis
Pulmonary complaints may represent pulmonary embolism, pulmonary hypertension, TB, bacterial, viral, or fungal pneumonia, malignancy, or lymphocytic interstitial pneumonitis.
Neurologic symptoms raise concern for neurosyphilis, viral encephalitis, toxoplasmosis, CNS lymphoma, meningitis, stroke, metabolic encephalopathy, or progressive multifocal leukoencephalopathy.
Cardiac presentations include cardiomyopathy, myocarditis, pericarditis, endocarditis, acute coronary syndrome, or pericardial effusion.
Oral and esophageal symptoms may result from candidiasis, viral infections, bacterial disease, autoimmune conditions, or malignancy.
Chronic diarrhea, hepatomegaly, and renal dysfunction have broad infectious, metabolic, medication-related, and neoplastic etiologies in HIV-infected patients.
Treatment
Emergency Department Management
Patients appearing toxic or with rapidly progressive illness should receive empiric antibiotics in the ED. Initiation of antiretroviral therapy is recommended for patients with low CD4 counts, high viral loads, pregnancy, AIDS-defining illnesses, or HIV-associated nephropathy.
Highly active antiretroviral therapy (HAART) typically consists of triple therapy using combinations of non-nucleoside reverse transcriptase inhibitors, protease inhibitors, and nucleoside reverse transcriptase inhibitors.
Post-exposure prophylaxis should begin within 2 hours of exposure when possible and continue for 4 weeks, with two-drug regimens for most exposures and expanded three-drug regimens for high-risk cases.
Specific opportunistic infections require targeted therapy, including pyrimethamine-based regimens for toxoplasmosis, amphotericin B with flucytosine for cryptococcal meningitis, ganciclovir for CMV retinitis, fluconazole for esophageal candidiasis, clarithromycin-based therapy for MAC, trimethoprim-sulfamethoxazole for PCP with adjunctive steroids when hypoxemia is present, and plasmapheresis for acute HIV-related demyelinating neuropathy.
Medication-Related Considerations
Antiretroviral therapy is associated with numerous potential adverse effects including hypersensitivity reactions, pancreatitis, peripheral neuropathy, nephrolithiasis, hepatotoxicity, lactic acidosis, Stevens–Johnson syndrome, hemolytic anemia, neuropsychiatric effects, metabolic derangements, cardiomyopathy, and hematologic abnormalities.
Follow-Up And Disposition
Admission Criteria
Indications for hospitalization include unexplained fever with neurologic involvement, hypoxemia, suspected acute coronary syndrome, pericardial effusion, suspected bacterial pneumonia or TB, new neurologic deficits or seizures, hemodynamic instability, inability to ambulate or tolerate oral intake, and severe diarrhea with dehydration.
Discharge Criteria
Patients may be discharged if they can maintain oral intake, ambulate, perform self-care, and have reliable follow-up.
Referral Considerations
All patients should be referred to an HIV specialist for initiation and management of antiretroviral therapy. Screening for depression and psychiatric referral are essential to ensure treatment adherence. Patients with concerning symptoms should be referred for malignancy evaluation.
Key Clinical Insights And Common Pitfalls
Immune reconstitution inflammatory syndrome typically occurs within 8 weeks of initiating HAART. Occupational exposure carries a low but real risk of seroconversion. Patients on HAART have increased risk for metabolic disease and acute coronary syndromes. Exercise-induced desaturation may aid in diagnosing PCP when imaging is normal. HIV is an independent risk factor for COPDukar
COPD, pulmonary hypertension, stroke, venous thromboembolism, thrombotic thrombocytopenic purpura, osteoporosis, and osteonecrosis of the hip.
- Published on
Emergency And Acute Medicine – Hirschsprung Disease
Basics
Condition Overview
First described in 1886 by Harold Hirschsprung as a cause of severe constipation in early infancy. Hirschsprung disease is a congenital aganglionic megacolon occurring in approximately 1:5,000 live births. Mortality associated with Hirschsprung-related enterocolitis remains high at 35–50%.
Etiology And Pathogenesis
The disease is caused by absence of enteric ganglion cells in the distal bowel. Normally, neural crest cells migrate along the gastrointestinal tract, reaching the proximal colon by 8 weeks of gestation and the rectum by 12 weeks. Failure of migration into the parasympathetic Meissner (submucosal) and Auerbach (myenteric) plexuses results in an aganglionic segment and clinical disease.
The affected bowel typically begins at the internal anal sphincter and involves the rectosigmoid colon in about 75% of cases, though it may extend proximally and, in rare cases, involve the entire GI tract, which is often fatal. The aganglionic segment remains chronically contracted, producing functional obstruction, while proximal bowel dilates to accommodate retained stool. Anal stimulation may temporarily allow stool passage.
Genetic associations include mutations of the RET proto-oncogene in both familial and sporadic forms. The male-to-female ratio is approximately 4:1. About 8% have a positive family history, with 5–12% of siblings affected. Chromosomal abnormalities occur in 5–15%, most commonly trisomy 21 (Down syndrome). Other congenital anomalies are present in approximately 18%, including gastrointestinal, cardiac, craniofacial abnormalities, cleft palate, and congenital deafness.
Diagnosis
Clinical Features
Most patients are diagnosed by 2 years of age, with presentation varying by age.
Neonatal presentation
Abdominal distension, failure to pass meconium within the first 48 hours of life, vomiting, enterocolitis characterized by abdominal pain, fever, foul-smelling and/or bloody diarrhea, vomiting progressing to sepsis and possible intestinal perforation, and sepsis.
Infancy
Chronic constipation, progressive abdominal distension, vomiting, failure to thrive, enterocolitis, and possible toxic megacolon.
Later childhood And Adulthood
Chronic constipation with obstruction, often refractory to standard treatment, rare overflow incontinence, abdominal distension, bloody foul-smelling diarrhea, malnutrition, and episodes of enterocolitis with systemic toxicity.
History
Frequent need for rectal stimulation or enemas to achieve bowel movements, narrow-caliber stools, encopresis and diarrhea are uncommon, and absence of typical triggers for functional constipation such as fissures, toilet training issues, or dietary factors.
Physical Examination
Possible palpable colon on the left, abdominal distension with signs of obstruction, findings consistent with malnutrition or failure to thrive, and an empty rectal vault on digital rectal examination.
Initial Evaluation
Plain abdominal radiographs commonly show distended small bowel and proximal colon (megacolon) with an empty rectum and a transition zone into a narrowed rectosigmoid segment. Neonates often demonstrate a distal obstructive pattern. In chronic constipation, imaging may show only fecal loading. In enterocolitis, bowel wall edema or pneumatosis intestinalis may be present.
Diagnostic Studies And Interpretation
Laboratory Studies
CBC, electrolytes, glucose, BUN, creatinine, urinalysis, and blood cultures if the patient appears toxic.
Imaging
Barium enema should be obtained after stabilization and is contraindicated if perforation or severe enterocolitis is suspected. Findings include a dilated proximal colon with a narrowed aganglionic distal segment, uncoordinated peristalsis, and a transition zone. A nondistensible rectum and delayed barium evacuation are classic findings. The transition zone may be absent in neonates or in infants who have undergone repeated rectal exams or enemas.
Procedures And Surgical Diagnosis
Rectal manometry may assist in diagnosis but is often abnormal in long-standing constipation; affected patients fail to demonstrate reflex relaxation of the internal anal sphincter with rectal balloon inflation. Definitive diagnosis requires a full-thickness rectal biopsy demonstrating absence of ganglion cells, which remains the diagnostic gold standard.
Differential Diagnosis
Neonates
Meconium ileus or meconium plug syndrome associated with cystic fibrosis, intestinal or anal atresia or hypoplasia, malrotation or duplication with volvulus, necrotizing enterocolitis, and sepsis.
Infants And Children
Functional constipation, toxic etiologies such as opiates or anticholinergics, infectious causes including botulism, acquired aganglionic colon, metabolic or endocrine disorders such as hypothyroidism, parathyroid or adrenal disease, electrolyte abnormalities, spinal cord defects, and abdominal masses.
Treatment
Initial Stabilization And Support
Airway, breathing, and circulation management with appropriate monitoring. Administer isotonic IV fluid bolus (20 mL/kg) for dehydration, shock, or sepsis.
Emergency Department Management
Infants should be treated as having bowel obstruction; nasogastric decompression is indicated if vomiting is present. Early consultation with a pediatric surgeon is essential. Broad-spectrum triple antibiotics are indicated for toxic patients or those with enterocolitis. Unstable patients may require emergent decompression with a loop colostomy. Stable patients may complete diagnostic evaluation as outpatients.
Definitive treatment consists of surgical resection of the aganglionic bowel with pull-through of normally innervated bowel to within 1 cm of the anal opening. Enterocolitis may occur before or after surgical intervention.
Medications
Ampicillin 50 mg/kg IV divided every 6 hours.
Gentamicin 2.5 mg/kg IV divided every 12–24 hours.
Metronidazole 7.5 mg/kg IV divided every 12–48 hours.
Follow-Up And Disposition
Admission Criteria
Neonates and infants with bowel obstruction, any patient with enterocolitis, and ill-appearing infants requiring NICU or PICU care with pediatric surgical support.
Discharge Criteria
Well-hydrated patients tolerating oral intake, typically older children presenting primarily with constipation, with reliable caregivers and close outpatient follow-up arranged.
Referral Considerations
Ongoing care should be coordinated with pediatric gastroenterology and pediatric surgery.
Key Clinical Insights And Common Pitfalls
Clinical presentation varies widely with age, ranging from neonatal obstruction to chronic constipation. The disease exists on a spectrum from mild constipation to life-threatening enterocolitis. Toxic patients require immediate stabilization, antibiotics, urgent imaging, and surgical consultation. Failure to recognize enterocolitis can result in rapid deterioration and death.
Basics
Condition Overview
First described in 1886 by Harold Hirschsprung as a cause of severe constipation in early infancy. Hirschsprung disease is a congenital aganglionic megacolon occurring in approximately 1:5,000 live births. Mortality associated with Hirschsprung-related enterocolitis remains high at 35–50%.
Etiology And Pathogenesis
The disease is caused by absence of enteric ganglion cells in the distal bowel. Normally, neural crest cells migrate along the gastrointestinal tract, reaching the proximal colon by 8 weeks of gestation and the rectum by 12 weeks. Failure of migration into the parasympathetic Meissner (submucosal) and Auerbach (myenteric) plexuses results in an aganglionic segment and clinical disease.
The affected bowel typically begins at the internal anal sphincter and involves the rectosigmoid colon in about 75% of cases, though it may extend proximally and, in rare cases, involve the entire GI tract, which is often fatal. The aganglionic segment remains chronically contracted, producing functional obstruction, while proximal bowel dilates to accommodate retained stool. Anal stimulation may temporarily allow stool passage.
Genetic associations include mutations of the RET proto-oncogene in both familial and sporadic forms. The male-to-female ratio is approximately 4:1. About 8% have a positive family history, with 5–12% of siblings affected. Chromosomal abnormalities occur in 5–15%, most commonly trisomy 21 (Down syndrome). Other congenital anomalies are present in approximately 18%, including gastrointestinal, cardiac, craniofacial abnormalities, cleft palate, and congenital deafness.
Diagnosis
Clinical Features
Most patients are diagnosed by 2 years of age, with presentation varying by age.
Neonatal presentation
Abdominal distension, failure to pass meconium within the first 48 hours of life, vomiting, enterocolitis characterized by abdominal pain, fever, foul-smelling and/or bloody diarrhea, vomiting progressing to sepsis and possible intestinal perforation, and sepsis.
Infancy
Chronic constipation, progressive abdominal distension, vomiting, failure to thrive, enterocolitis, and possible toxic megacolon.
Later childhood And Adulthood
Chronic constipation with obstruction, often refractory to standard treatment, rare overflow incontinence, abdominal distension, bloody foul-smelling diarrhea, malnutrition, and episodes of enterocolitis with systemic toxicity.
History
Frequent need for rectal stimulation or enemas to achieve bowel movements, narrow-caliber stools, encopresis and diarrhea are uncommon, and absence of typical triggers for functional constipation such as fissures, toilet training issues, or dietary factors.
Physical Examination
Possible palpable colon on the left, abdominal distension with signs of obstruction, findings consistent with malnutrition or failure to thrive, and an empty rectal vault on digital rectal examination.
Initial Evaluation
Plain abdominal radiographs commonly show distended small bowel and proximal colon (megacolon) with an empty rectum and a transition zone into a narrowed rectosigmoid segment. Neonates often demonstrate a distal obstructive pattern. In chronic constipation, imaging may show only fecal loading. In enterocolitis, bowel wall edema or pneumatosis intestinalis may be present.
Diagnostic Studies And Interpretation
Laboratory Studies
CBC, electrolytes, glucose, BUN, creatinine, urinalysis, and blood cultures if the patient appears toxic.
Imaging
Barium enema should be obtained after stabilization and is contraindicated if perforation or severe enterocolitis is suspected. Findings include a dilated proximal colon with a narrowed aganglionic distal segment, uncoordinated peristalsis, and a transition zone. A nondistensible rectum and delayed barium evacuation are classic findings. The transition zone may be absent in neonates or in infants who have undergone repeated rectal exams or enemas.
Procedures And Surgical Diagnosis
Rectal manometry may assist in diagnosis but is often abnormal in long-standing constipation; affected patients fail to demonstrate reflex relaxation of the internal anal sphincter with rectal balloon inflation. Definitive diagnosis requires a full-thickness rectal biopsy demonstrating absence of ganglion cells, which remains the diagnostic gold standard.
Differential Diagnosis
Neonates
Meconium ileus or meconium plug syndrome associated with cystic fibrosis, intestinal or anal atresia or hypoplasia, malrotation or duplication with volvulus, necrotizing enterocolitis, and sepsis.
Infants And Children
Functional constipation, toxic etiologies such as opiates or anticholinergics, infectious causes including botulism, acquired aganglionic colon, metabolic or endocrine disorders such as hypothyroidism, parathyroid or adrenal disease, electrolyte abnormalities, spinal cord defects, and abdominal masses.
Treatment
Initial Stabilization And Support
Airway, breathing, and circulation management with appropriate monitoring. Administer isotonic IV fluid bolus (20 mL/kg) for dehydration, shock, or sepsis.
Emergency Department Management
Infants should be treated as having bowel obstruction; nasogastric decompression is indicated if vomiting is present. Early consultation with a pediatric surgeon is essential. Broad-spectrum triple antibiotics are indicated for toxic patients or those with enterocolitis. Unstable patients may require emergent decompression with a loop colostomy. Stable patients may complete diagnostic evaluation as outpatients.
Definitive treatment consists of surgical resection of the aganglionic bowel with pull-through of normally innervated bowel to within 1 cm of the anal opening. Enterocolitis may occur before or after surgical intervention.
Medications
Ampicillin 50 mg/kg IV divided every 6 hours.
Gentamicin 2.5 mg/kg IV divided every 12–24 hours.
Metronidazole 7.5 mg/kg IV divided every 12–48 hours.
Follow-Up And Disposition
Admission Criteria
Neonates and infants with bowel obstruction, any patient with enterocolitis, and ill-appearing infants requiring NICU or PICU care with pediatric surgical support.
Discharge Criteria
Well-hydrated patients tolerating oral intake, typically older children presenting primarily with constipation, with reliable caregivers and close outpatient follow-up arranged.
Referral Considerations
Ongoing care should be coordinated with pediatric gastroenterology and pediatric surgery.
Key Clinical Insights And Common Pitfalls
Clinical presentation varies widely with age, ranging from neonatal obstruction to chronic constipation. The disease exists on a spectrum from mild constipation to life-threatening enterocolitis. Toxic patients require immediate stabilization, antibiotics, urgent imaging, and surgical consultation. Failure to recognize enterocolitis can result in rapid deterioration and death.
- Published on
Emergency And Acute Medicine – Hepatorenal Syndrome
Overview And Definition
Hepatorenal syndrome is a form of renal failure that occurs in patients with advanced acute or chronic liver disease in the absence of intrinsic renal pathology. It reflects a severe reduction in renal perfusion caused by advanced hepatic dysfunction. The kidneys are structurally normal, and renal failure does not improve despite adequate volume resuscitation.
Disease Classification And Mechanism
Type I hepatorenal syndrome is an acute and rapidly progressive condition characterized by a sudden decline in renal function, defined by a doubling of serum creatinine or a 50% reduction in creatinine clearance within two weeks. It is commonly associated with acute liver failure or severe alcoholic hepatitis, often presents with oliguria or anuria, and carries a mortality rate approaching 90% within three months.
Type II hepatorenal syndrome has a more indolent course and typically occurs in patients with cirrhosis and refractory ascites. Renal dysfunction progresses slowly, and overall survival is longer than in type I disease.
The underlying pathophysiology involves profound systemic vasodilation due to liver disease, resulting in reduced effective arterial blood volume. This triggers activation of the sympathetic nervous system and the renin–angiotensin–aldosterone system, along with increased production of vasoactive substances. The net effect is dominant renal vasoconstriction, reduced renal blood flow, decreased glomerular filtration rate, and markedly low urinary sodium excretion.
Etiology And Precipitating Factors
Hepatorenal syndrome most commonly arises in chronic liver disease, particularly cirrhosis and severe alcoholic hepatitis, but may also occur in fulminant hepatic failure. Common precipitating factors include gastrointestinal bleeding, aggressive diuresis, large-volume paracentesis without albumin replacement, exposure to nephrotoxic medications such as NSAIDs or aminoglycosides, and systemic infections. Spontaneous bacterial peritonitis is a particularly important trigger and significantly increases the risk of renal failure.
Clinical Features
Patients typically exhibit signs of advanced liver disease, including ascites, portal hypertension, jaundice, hepatic encephalopathy, and coagulopathy. Progressive oliguria is common. Vital signs may reveal hypotension or tachycardia, particularly in the presence of bleeding or sepsis. Dyspnea and tachypnea may occur due to tense ascites or volume overload.
Diagnostic Evaluation
Laboratory findings usually demonstrate rising blood urea nitrogen and creatinine, though creatinine may underestimate renal dysfunction due to low muscle mass or interference from hyperbilirubinemia. Urinalysis typically shows no casts or protein, helping distinguish hepatorenal syndrome from acute tubular necrosis. Urine sodium is characteristically very low, with a fractional excretion of sodium below 1% and concentrated urine relative to plasma.
Additional studies include coagulation profiles, cultures to evaluate for infection, and renal ultrasound to exclude obstructive uropathy. Hepatorenal syndrome remains a diagnosis of exclusion, requiring elimination of other causes of renal failure such as hypovolemia, intrinsic renal disease, obstruction, and drug toxicity.
Differential Considerations
Important alternatives include prerenal azotemia due to volume depletion, acute tubular necrosis, glomerulonephritis related to viral hepatitis, obstructive uropathy, medication-induced nephrotoxicity, sepsis-related renal failure, and post–liver transplant renal dysfunction.
Initial Stabilization And Support
Management begins with standard airway, breathing, and circulation assessment. Hypotension and hypovolemia should be corrected promptly using isotonic fluids and albumin. Close monitoring of urine output and hemodynamic status is essential. Life-threatening complications of renal failure, including hyperkalemia, metabolic acidosis, hypoxemia, and uremic complications, must be addressed immediately.
Emergency Department Management
Treatment focuses on identifying and correcting reversible contributors while providing supportive care. All potentially nephrotoxic medications should be discontinued. Infections must be treated aggressively with early antibiotics. Electrolyte abnormalities, hypoglycemia, hepatic encephalopathy, and other complications of liver failure should be corrected. Large-volume paracentesis with albumin replacement may transiently improve renal perfusion in patients with tense ascites.
Advanced therapies such as transjugular intrahepatic portosystemic shunt placement may improve renal function in selected patients. Dialysis is reserved for management of complications and as a bridge to recovery or transplantation. Liver transplantation remains the only definitive treatment.
Pharmacologic Options
No medication is considered definitive therapy. Vasoconstrictor-based regimens may be used in select cases after excluding other causes of renal failure. Options include low-dose dopamine, combinations of midodrine and octreotide, or prostaglandin analogs. Vasopressin analogs such as terlipressin show benefit but are not widely available in all regions.
Disposition And Prognosis
All patients with suspected hepatorenal syndrome require hospital admission with gastroenterology and nephrology consultation. Intensive care admission is indicated for those with encephalopathy, severe electrolyte disturbances, or cardiopulmonary compromise. There are no circumstances in which discharge from the emergency department is appropriate.
Key Clinical Insights And Common Errors
Any degree of renal dysfunction in a patient with advanced liver disease must be treated as a medical emergency. Delayed recognition, failure to exclude reversible causes, or continued exposure to nephrotoxic agents significantly worsens outcomes. Early consultation and consideration of transplant eligibility are critical.
Overview And Definition
Hepatorenal syndrome is a form of renal failure that occurs in patients with advanced acute or chronic liver disease in the absence of intrinsic renal pathology. It reflects a severe reduction in renal perfusion caused by advanced hepatic dysfunction. The kidneys are structurally normal, and renal failure does not improve despite adequate volume resuscitation.
Disease Classification And Mechanism
Type I hepatorenal syndrome is an acute and rapidly progressive condition characterized by a sudden decline in renal function, defined by a doubling of serum creatinine or a 50% reduction in creatinine clearance within two weeks. It is commonly associated with acute liver failure or severe alcoholic hepatitis, often presents with oliguria or anuria, and carries a mortality rate approaching 90% within three months.
Type II hepatorenal syndrome has a more indolent course and typically occurs in patients with cirrhosis and refractory ascites. Renal dysfunction progresses slowly, and overall survival is longer than in type I disease.
The underlying pathophysiology involves profound systemic vasodilation due to liver disease, resulting in reduced effective arterial blood volume. This triggers activation of the sympathetic nervous system and the renin–angiotensin–aldosterone system, along with increased production of vasoactive substances. The net effect is dominant renal vasoconstriction, reduced renal blood flow, decreased glomerular filtration rate, and markedly low urinary sodium excretion.
Etiology And Precipitating Factors
Hepatorenal syndrome most commonly arises in chronic liver disease, particularly cirrhosis and severe alcoholic hepatitis, but may also occur in fulminant hepatic failure. Common precipitating factors include gastrointestinal bleeding, aggressive diuresis, large-volume paracentesis without albumin replacement, exposure to nephrotoxic medications such as NSAIDs or aminoglycosides, and systemic infections. Spontaneous bacterial peritonitis is a particularly important trigger and significantly increases the risk of renal failure.
Clinical Features
Patients typically exhibit signs of advanced liver disease, including ascites, portal hypertension, jaundice, hepatic encephalopathy, and coagulopathy. Progressive oliguria is common. Vital signs may reveal hypotension or tachycardia, particularly in the presence of bleeding or sepsis. Dyspnea and tachypnea may occur due to tense ascites or volume overload.
Diagnostic Evaluation
Laboratory findings usually demonstrate rising blood urea nitrogen and creatinine, though creatinine may underestimate renal dysfunction due to low muscle mass or interference from hyperbilirubinemia. Urinalysis typically shows no casts or protein, helping distinguish hepatorenal syndrome from acute tubular necrosis. Urine sodium is characteristically very low, with a fractional excretion of sodium below 1% and concentrated urine relative to plasma.
Additional studies include coagulation profiles, cultures to evaluate for infection, and renal ultrasound to exclude obstructive uropathy. Hepatorenal syndrome remains a diagnosis of exclusion, requiring elimination of other causes of renal failure such as hypovolemia, intrinsic renal disease, obstruction, and drug toxicity.
Differential Considerations
Important alternatives include prerenal azotemia due to volume depletion, acute tubular necrosis, glomerulonephritis related to viral hepatitis, obstructive uropathy, medication-induced nephrotoxicity, sepsis-related renal failure, and post–liver transplant renal dysfunction.
Initial Stabilization And Support
Management begins with standard airway, breathing, and circulation assessment. Hypotension and hypovolemia should be corrected promptly using isotonic fluids and albumin. Close monitoring of urine output and hemodynamic status is essential. Life-threatening complications of renal failure, including hyperkalemia, metabolic acidosis, hypoxemia, and uremic complications, must be addressed immediately.
Emergency Department Management
Treatment focuses on identifying and correcting reversible contributors while providing supportive care. All potentially nephrotoxic medications should be discontinued. Infections must be treated aggressively with early antibiotics. Electrolyte abnormalities, hypoglycemia, hepatic encephalopathy, and other complications of liver failure should be corrected. Large-volume paracentesis with albumin replacement may transiently improve renal perfusion in patients with tense ascites.
Advanced therapies such as transjugular intrahepatic portosystemic shunt placement may improve renal function in selected patients. Dialysis is reserved for management of complications and as a bridge to recovery or transplantation. Liver transplantation remains the only definitive treatment.
Pharmacologic Options
No medication is considered definitive therapy. Vasoconstrictor-based regimens may be used in select cases after excluding other causes of renal failure. Options include low-dose dopamine, combinations of midodrine and octreotide, or prostaglandin analogs. Vasopressin analogs such as terlipressin show benefit but are not widely available in all regions.
Disposition And Prognosis
All patients with suspected hepatorenal syndrome require hospital admission with gastroenterology and nephrology consultation. Intensive care admission is indicated for those with encephalopathy, severe electrolyte disturbances, or cardiopulmonary compromise. There are no circumstances in which discharge from the emergency department is appropriate.
Key Clinical Insights And Common Errors
Any degree of renal dysfunction in a patient with advanced liver disease must be treated as a medical emergency. Delayed recognition, failure to exclude reversible causes, or continued exposure to nephrotoxic agents significantly worsens outcomes. Early consultation and consideration of transplant eligibility are critical.

